
Title: The Ethics of Medical Homicide and Mutilation
Author: Austin O'Malley
Release date: May 22, 2013 [eBook #42764]
Most recently updated: October 23, 2024
Language: English
Other information and formats: www.gutenberg.org/ebooks/42764
Credits: E-text prepared by Dianna Adair, Julia Neufeld, and the Online Distributed Proofreading Team (http://www.pgdp.net) from page images generously made available by Internet Archive/Canadian Libraries (http://archive.org/details/toronto)
The Project Gutenberg eBook, The Ethics of Medical Homicide and Mutilation, by Austin O'Malley
| Note: | Images of the original pages are available through Internet Archive/Canadian Libraries. See http://archive.org/details/theethicsofmedic00omaluoft |
BY
NEW YORK
THE DEVIN-ADAIR COMPANY
1922
Nihil obstat
ARTHUR J. SCANLAN, S.T.D.
Censor Librorum
Imprimatur
✠ JOHN CARDINAL FARLEY
Archbishop of New York
Copyright, 1919, by
The Devin-Adair Company
——
All Rights Reserved by
The Devin-Adair Company
Third Printing
PRINTED IN U.S.A.
| CHAPTER I | |
| GENERAL PRINCIPLES CONCERNING SUICIDE AND HOMICIDE | |
| PAGE | |
There is a Supreme Being who alone is master of life. The Natural Law. The nature and determinants of morality. Probabilism. Permissive suicide. Suicide is illicit. Conscience. Homicide, direct and indirect. Self-defence. Formal and material aggressors. Legalized homicide. Bibliography | 1-22 |
| CHAPTER II | |
| GENERAL PRINCIPLES CONCERNING MUTILATION | |
Mutilation. Canonical irregularity. Self-mutilation. The double effect in morality. Direct and indirect mutilation. The State and mutilation. The dominion of the State | 23-32 |
| CHAPTER III | |
| WHEN DOES HUMAN LIFE BEGIN? | |
Ancient and modern opinions. The fetus is animated at the moment of conception. The single cell as the primal life-organ. Cell growth and division. Germ cells. The development of the embryo. Fetal viability. Theories of development. The Aristotelian and Thomistic opinions. The formal principle. A soul exists. The primordial cell is a sufficient organ for the soul. Metabolism in the cell. Cell motion. Animal heat and energy. Life in separated tissues. The soul in monsters | 33-82 |
| CHAPTER IV | |
| WHEN DOES HUMAN LIFE END? | |
The heart and life. Resuscitation after apparent death. The last sacraments in apparent death. Suspended animation. The living fetus in the womb of a dying or dead mother. Methods of resuscitation. Signs of death | 83-91 |
| [iv]CHAPTER V | |
| ABORTION | |
Abortion and miscarriage. Causes of abortion, fetal, maternal and paternal. Surgical operations and abortion. The debitum in pregnancy. Premature labor. Threatened, inevitable, and incomplete abortions. Treatment. The use of the tampon. Precautions against abortion. Therapeutic abortion. Methods of inducing abortion. Artificial abortion of an inviable fetus is never licit. Decrees of the church concerning abortion. The civil law on abortion | 92-123 |
| CHAPTER VI | |
| ECTOPIC GESTATION | |
Ectopic gestation or extrauterine pregnancy. Anatomy of the uterus and its adnexa. Place of fecundation. The abnormal uterus. Tubal rupture and tubal abortion. Diagnosis. Decrees of the church on ectopic gestation. Removal of an inviable ectopic fetus except in present peril of life is illicit | 124-132 |
| CHAPTER VII | |
| CESAREAN DELIVERY | |
Indications for cesarean delivery. Abnormal pelves. Symphyseotomy. Varieties of cesarean delivery. Morality. Amputation of the uterus after cesarean delivery. Precautionary sterilization of a cesarean case is illicit | 133-142 |
| CHAPTER VIII | |
| PLACENTA PRAEVIA AND ABRUPTIO PLACENTAE | |
Nature and effects of placenta praevia. Treatment. Morality and methods of treatment. Abruptio placentae. Morality of fetal removal | 143-146 |
| CHAPTER IX | |
| ABDOMINAL TUMORS IN PREGNANCY | |
Tumors blocking parturition. Fibroids or myomata. Ovarian tumors. Cancer. Effects and morality of operation | 147-152 |
| [v]CHAPTER X | |
| APPENDICITIS IN PREGNANCY | |
Occurrence. Time of operation. Diagnosis | 153-154 |
| CHAPTER XI | |
| PUERPERAL INSANITY AND STERILIZATION | |
Causes. Varieties. Prognosis. Precautionary sterilization of puerperal psychopaths is illicit | 155-157 |
| CHAPTER XII | |
| NEPHRITIS IN PREGNANCY | |
Frequency. Effects. Abortion as a treatment. Varieties of nephritis. Pyelitis. Catalepsy | 158-161 |
| CHAPTER XIII | |
| ECLAMPSIA PARTURIENTIUM | |
Definition. Symptoms. Prognosis. Causes. Precautions against eclampsia. Forced delivery. The expectant treatment. Relative mortality and morality of the methods. Cesarean delivery as a treatment. The expectant treatment is apparently the best | 162-169 |
| CHAPTER XIV | |
| HEART DISEASES IN PREGNANCY | |
Factors in abnormal gestation. The use of pituitrin. Weak pains and the diseased heart. The diseased heart in actual parturition. Operative risk in cardiopaths. Heart block and mitral regurgitation in labor. Prognosis | 170-176 |
| CHAPTER XV | |
| HYPEREMESIS GRAVIDARUM | |
Pernicious vomiting. Occurrence. Symptoms. Stages. Effects. Causes. Therapeutic abortion in pernicious vomiting. Treatment | 177-181 |
| [vi]CHAPTER XVI | |
| CHOREA GRAVIDARUM AND HYSTERIA | |
Varieties of chorea. Differentiation. Prognosis. Hysteria. Causes. Epidemics of hysteria. Symptoms. Prognosis | 182-186 |
| CHAPTER XVII | |
| ACUTE YELLOW ATROPHY OF THE LIVER IN PREGNANCY | |
Icterus gravis. Causes. Symptoms. Prognosis | 187-188 |
| CHAPTER XVIII | |
| INFECTIOUS DISEASES IN PREGNANCY | |
Effects on mother and fetus. Abortions in infectious diseases. Placental permeability. Typhoid. Smallpox. Pneumonia. Influenza. Scarlatina. Measles. Cholera. Tuberculosis. Artificial abortion in tuberculosis | 189-200 |
| CHAPTER XIX | |
| SYPHILIS IN PREGNANCY AND MARRIAGE | |
Prognosis. Abortion. Infection of mother and fetus. Colles' Law. Erroneous notions on the curability of syphilis. Once a syphilitic probably always a syphilitic. The professional secret in syphilis. Nature of secrets. The physician may warn an innocent person | 201-211 |
| CHAPTER XX | |
| GONORRHOEA IN MARRIAGE | |
The cause of gonorrhoea. Tests of cure. Effects on a woman. Chronicity. Prevalence. Surgical treatment in women. Morality of the surgical treatment. Conservative surgery. Salpingotomy. Ovariotomy. Evil effects of ovariotomy. Internal secretion of the ovary. Results of various operations. Pregnancy after operation. Morality of infection. General effects of gonorrhoea. Ophthalmia neonatorum and gonorrhoea | 212-229 |
| [vii]CHAPTER XXI | |
| DIABETES IN PREGNANCY | |
Fatality of diabetes in pregnancy. Diagnosis. Sterility of diabetics. Prognosis. Heredity in diabetes. Therapeutic abortion in diabetes | 230-231 |
| CHAPTER XXII | |
| CHILDBIRTH IN TWILIGHT SLEEP | |
Twilight sleep to avert pain in parturition. Stages of labor. Drugs used. Scopolamine and morphine. Danger in the use of these drugs in labor. Contradictory report of physicians on twilight sleep. Eminent authorities opposed to the methods. Baer's report on the evil effects. The methods are morally illicit and useless | 232-244 |
| CHAPTER XXIII | |
| VASECTOMY, OR STERILIZATION, BY STATE LAW | |
The States that have this law. Reasons for the law. Hereditary transmission of certain diseases. The operation. Its effects. Restoration of the function of the interrupted vas deferens. Vasectomy and impotence. Onanism. Vasectomy effects impotence from the moral point of view. Other conditions in the male that effect moral impotence. Immorality of artificial impregnation. Vasectomy a grave mutilation. Vasectomy as ordinarily practised is illicit. The State and vasectomy. The limitations of the State's dominion. The State surgeon and vasectomy. Bibliography | 245-268 |
| CHAPTER XXIV | |
| THE ETHICS OF BIRTH CONTROL | 269 |
| Index | 281 |
In this book is discussed the morality involved in the ordinary cases of medical homicide and mutilation. Craniotomy has been omitted because this operation on the living child is never morally licit, and when done on the dead fetus it has no moral quality that requires explanation.
The articles may seem to be intended for Catholic physicians and spiritual directors alone, but the desire in writing them was to reach all practitioners, to the end that the Natural Law which binds every man may be observed. Morality is not made such in its fundamental principles by any religious creed, but by the requirements of Divine Order, which finally prevails no matter what the opposition. Killing and maiming without sufficient extenuation did not become unlawful solely by the establishment of Christianity. Practically, however, physicians who have no religion, or a religion which is so illogical as to pay no attention to dogma, or even to rail at it as obtrusive, necessarily gravitates to the emotional in morality, and the principles of this book will not even interest them. Dogmas are abstract propositions, and all human society rests on abstract propositions. The most vital facts in morality, the basic distinction between crime and all that is virtuous or indifferent morally, is in abstract principle alone, but physicians and pastors who are not trained in philosophy and rational religion cannot appreciate an abstract principle—they are influenced only by the concrete.
Obstetrical text-books, unfortunately, are written by such emotional men; by men who lack all training in ethics other than that inculcated in childhood out of the mental vagaries of the women in the household; and these authors prescribe therapeutic homicide as if it were a drug in the American Pharmacopœia. The reader is told that if the patient is a Catholic he is to respect her religious "prejudices"; if she is not a Catholic one need not bother about moral scruples when it is necessary to take a life to stop fits. Since the civil law does not prosecute a physician for therapeutic abortion on an inviable child, most physicians deem such an act not only permissible but scientific, and they hold that if a man's conscience will not let him kill a fetus to alleviate maternal distress he is guilty of malpractice.
Decrees of the Catholic Church are cited in these pages, not because morality is an asset of the Catholic Church alone, but because it alone pronounces officially on these medical subjects after careful consideration by competent specialists. This Church has made decisions in comparatively few medico-moral cases, and the questions still undecided authoritatively are very numerous. They are quite difficult, too, because judgment supposes a knowledge of both medicine and ethics, a combination seldom found in one person. As physicians do not know ethics, and moralists do not know medicine, there is often trouble in getting at even a statement of the questions at issue between them. In the preface to Essays in Pastoral Medicine, in 1906, I mentioned a noted case of this kind, and in 1911 a similar incident occurred in a discussion of the morality involved in the sterilization of criminals and the defective by the state. This dispute was taken up by the leading canonists and moral theologians in the United States, Belgium, Holland, Austria, Spain, Italy and France, and for nearly two years these men wrote article after article based upon utterly erroneous physical data.
The books we have on medico-moral subjects are either obsolete at present, or insufficient; or, more commonly, they are the work of amateurs in medicine. These last are worthless when they are not harmful. If, however, I may judge from the questions sent to me for answer by clergymen and physicians from all parts of the country, our theological seminaries and medical schools are in grave need of courses on the morality of medical practice. In this book, to the preparation of which I have given years of anxious thought because of the extreme responsibility involved in its decisions, the data for the most important parts of such courses are presented.
Austin O'Malley.
THE ETHICS OF
MEDICAL HOMICIDE AND MUTILATION
A Discussion of euthanasia through the use of narcotics in cases of incurable diseases periodically recurs, and the opinions of those in favor of putting the patient out of his misery are expressions of mere sentimentality, as in Maeterlinck's essay, Our Eternity. They think either that the passing of a law by a legislature removes all moral difficulty, or that morality is a trifle which should never stand in the way of expediency. Those who oppose this method of euthanasia base their argument, first, on the fact that many patients supposed by even clever diagnosticians to be incurable recover health; and, secondly, on the fact that the giving power of life and death to physicians is liable to grave abuse. This side misses the central truth and argues from accidental and secondary premises. Whether it is expedient, humane, or impolitic to kill incurable patients are almost irrelevant considerations: the fundamental question to be answered here is, Is there a Supreme Being who alone is master of life, to give it or to take it?
By its very definition such a Being is necessary (as opposed to contingent), self-existent; its essence always has been and always will be actualized into existence, and that from itself alone; it is an individual substance of an intelligent nature, and therefore a person. A contingent being is one that happens to be (contingere); it is of necessity neither existent nor non-existent; it has no logical aversion to existence, but in itself it has no more than a possibility[2] of actuality. A necessary Being, on the contrary, essentially must be; it cannot not be; it is absolutely and essentially its own existence.
There must be such a Necessary Being. If there were not, all things would be contingent, which is an absurdity. The absurdity arises from the fact that if all things were contingent nothing would be actual, nothing could ever come into existence, because there would be nothing to bring the primitive potentiality of the contingent beings into actual existence. The sufficient reason for the existence of contingent beings is either in themselves or in something outside themselves. It cannot be in themselves, because as they do not yet exist they are nothing; therefore it is in a Being which is not contingent, but whatever is not contingent is necessary. Therefore the existence of contingent beings absolutely requires the existence of a Necessary Being, which always was in existence. The ordinary name for this Necessary Being is God. Contingent beings are all creatures, all organic and inorganic beings without exception. There is, then, a God, the first cause or creator of all contingent beings, among whom is man; and since God created man wholly, this creature is wholly subservient to God, under the dominion of God, and his life is owned solely by God; God alone is the master of life and death, and he alone can delegate such mastery.
From the relation between the Creator and the creatures arises the natural law. Violation of this law is the source of all moral evil in the world, and of much of the physical evil. Reason shows us this law, and the method of observing it; and reason and unreason, observance or disregard, of the order fixed by the natural law are the foundation of happiness and unhappiness. Whatever a human being is or does, he must seek happiness; that is an essential quality of his being. Happiness is the satisfying of our desires; but as our desires are limitless, only infinite good can satisfy them. The sole sufficient good that sates all human longing is the infinite Necessary Being, and to be happy we must be united with that Being. Obviously the only possible method of possessing[3] this infinite God is through mental union, by undisturbable contemplation of his infinite truth, goodness, being, beauty, and his other attributes. If perfect, everlasting happiness is not in that, in what can it be? Is it in human fame, honor, riches, science, art, man, woman, or child? None of these can give lasting happiness, and no other happiness is real happiness.
Now, the only means we have to obtain union with infinite good is to follow out the condition inexorably placed by God, which is to act in life in keeping with right reason, to obey the law. Man's supreme honor is in freedom from the tyranny of unreason, and in a full obedience to external and immovable order, with the belief that his chief duty is to apprehend and to conform thereto.
This is morality. From the beginning men have held that certain acts are wrong and to be avoided, and that others are to be done. What is wrong, moreover, is such of its own nature, not from our will: we deem the fulfillment of duty, obedience to law, the first, highest, and last necessity of life. If we deny this truth we let in chaos. What is right or wrong is one or the other on its own merits, prescinding from its pleasurableness or pain.
We must seek good whether we will or not. Good is the sole object upon which the will operates, it is the raw material of the will's business. The ultimate standard of this good is God himself as its exemplary cause, but proximately the standard of moral good is our rational nature. Through our reason we judge whether a thing is good or bad; that is, whether it perfects or injures us; and as it is good or bad for us our will's tendency toward it is good or bad. Many acts are indifferent in themselves, but take on a good or bad quality from our intention; others are good or bad in themselves apart from our volition: charity is good, lying is bad, whether they are willed by us or not.
The morality of any action is determined (1) by the object of the action; (2) by the circumstances that accompany the action; (3) by the end the agent had in view.
1. The term object has various meanings, but here it[4] means the deed performed in the action, the thing which the will chooses. That deed by its very nature may be good, or it may be bad, or it may be indifferent morally. To help the afflicted is in itself a good action, to blaspheme is a bad action, to walk is an indifferent action. Some bad actions are absolutely bad; they never can become good or indifferent—blasphemy or adultery, for example; others, as stealing, are evil because of a lack of right in the agent: these may become indifferent or good by acquiring the missing right. Others are evil because of the danger necessarily connected with their performance,—the danger of sin connected with them, or the unnecessary peril to life. An action, to have a moral quality, must be voluntary, deliberate; and mere repugnance in doing an act does not in itself make the act involuntary.
2. Circumstances sometimes, though not always, may add a new element of good or evil to an action. The circumstances of an action are the Agent, the Object, the Place in which the action is done, the Means used, the End in view, the Method observed in using the means, and the Time in which the deed is done. If a judge in his official capacity tells a sheriff to hang a criminal, and a private citizen gives the same command, the actions are very different morally because of the circumstance of the agent giving the command. The object—it changes the morality of the deed whether one steals a cent or a thousand dollars. The place—what might be an offensive action in a residence might be a sacrilege in a church. The means—to support a family by labor or thievery. The end in view—to give alms in obedience to divine command or to give them to buy votes. The method used in employing the means—kindly, say, or cruelly. The time—to do manual labor on Sunday or on Monday. Some circumstances aggravate the evil in a deed, others excuse or attenuate it. Others may so color the deed that they specify it, make it some special virtue or vice. The circumstance that a murderer is the son of the man he kills specifies the deed as parricide.
3. The end also determines the morality of an action. Since the end is the first thing in the intention of the agent,[5] he passes from the object wished for in the end to choosing the means for obtaining it. Without the end the means cannot exist as such. There are occasions when an end is only a circumstance: for example, if it is a concomitant or extrinsic end. When this extrinsic end is in keeping with right reason or when it is discordant thereto, it may become a determinant of morality. In every voluntary, or human, act there is an interior and exterior act of the will, and each of these acts has its own object. The end is the proper object of the interior act of the will; the exterior object acted upon is the object of the exterior act of the will; both specify the morality, but the interior object or end specifies more importantly, as a rule, than the exterior object does. The will uses the body as an instrument on the external object, and the action of the body is connected with morality only through the will. We judge the morality of a blow not by the physical stroke, but from the intention of the striker. The exterior object of the will is, in a way, the matter of the morality, and the interior object of the will, or the end, is the form. Aristotle said: "He that steals to be able to commit adultery is more of an adulterer than a thief."[1] The thievery is a means to the principal end, and this principal end chiefly specifies or informs the action.
The means used to obtain an end are very important in a consideration of the morality of an act. There are four classes of means—the good, bad, indifferent, and excusable. Good means may be absolutely good, but commonly they are liable to become vitiated by circumstances,—almsgiving is an example. Some means are bad always and inexcusable—lying, for instance. The excusable means are those which are bad, but justifiable through circumstances. To save a man's life by cutting off his leg is an excusable means. The end sometimes may vitiate or hallow indifferent means, but it does not in itself justify all means. Means, like other circumstances, are accidents of an action, but they are in the action just as much as color is in a man. Color is not of a man's essence, but we cannot have a man without color.
The effect of an action, the result or product of an effective cause or agency, may in itself be an end or an object or a circumstance, and it has influence in the determination of morality. Sometimes an act has two immediate effects, one good and the other bad. For example, ligating the blood-vessels going to the uterus to stop a hemorrhage and so save a woman's life, a good effect, has also in ectopic gestation while the fetus is living another immediate effect, namely, to shut off the blood supply from the fetus and so kill it, a bad effect. To make such a double-effect action licit there are four conditions which are explained in the chapter on Mutilation.
The doctrine of Probabilism is very important in morality. Any law must be promulgated before it really becomes a law, and promulgation in a rational conscience is sufficient. Sometimes there is rational doubt of the existence, the interpretation, or the application of a law in a given case. Here probability is the only rule we can follow. A law which is doubtful after honest and capable investigation has not been sufficiently promulgated, and therefore it cannot impose a certain obligation because it lacks an essential element of a law. When we have used such moral diligence as the gravity of the matter calls for, but still the applicability of the law is doubtful in the action in view, the law does not bind; and what a law does not forbid it leaves open. Probabilism is not permissible where there is question of the worth of an action as compared with another, or of issues like the physical consequences of an act. If a physician knows a remedy for a disease that is certainly efficacious and another that is doubtfully efficacious, he may not choose this probable cure. Probabilism has to do only with the existence, interpretation, or applicability of a law, not with the differentiation of actions. The term probable means provable, not guessed at, not jumped at without reason. The doubt must be positive, founded on reason, not a matter of mere ignorance, suspicion, emotional bias. The opinion against a law to permit probabilism must be solid. It must rest upon an intrinsic reason from the nature of the case, or an extrinsic reason from authority, always supposing the authority is really an authority. The probability is to be comparative[7] also. What seems to be a very good reason when standing alone may be weak when compared with reasons on the other side. When we have weighed the arguments on both sides, and we still have a good reason for holding our opinion in a doubtful case, our opinion is probable. The probability is, moreover, to be practical. It must have considered all the circumstances of the case.
There is, then, a Supreme Being whom we must obey, who created and owns human life primarily; there is also a moral law. On these facts rests the argument relating to the destruction of human life. How far, then, has a human being dominion over his own life, and, secondly, over the life of any one else?
St. Thomas,[2] Lessius,[3] and others offer as one argument to prove suicide is not licit, that it is an injury to society or the state of which the suicide is part, and to which the use and profit of his service rightly belong. Lessius, while developing this proof, acknowledges its weakness.
If there were only one man in the world, and no society or state, suicide would still be illicit, because its basic deordination lies deeper than society or the state. If suicide were a moral evil solely because it deprives the state of the suicide's life, then for the same reason no one might become a citizen of another state, emigrate, nor might man abandon society and live as a recluse. Moreover, if a man were detrimental to the state rather than beneficial, in this point of view that fact alone would justify suicide, and the state would then be justified in permitting or even commanding suicide; and we shall show later that the state has not this power.
It is true that the injury done the state or society by loss of use and profit, by scandal and similar evils, is a solid argument against suicide, as such injury aggravates the deordination of suicide, but in itself the injury done to the state and society is not the fundamental reason against suicide.
St. Thomas[4] argues against suicide because it is contrary to the charity a human being should have for himself. This[8] is true ordinarily, and suicide takes on part of its guilt just because it is an offence against the rational regard a person should have for himself; yet this argument is not basic. We are told that if one sins against charity in killing his neighbor, a fortiori he sins in killing himself. Yet suppose just what the advocates of euthanasia suggest, viz., that a neighbor is in great agony and incurable: then the act of killing him takes on a quality of charity rather than of uncharity. And so for the suicide: if the patient is willing to be killed, there would be no uncharity; if he were unwilling, then homicide in any form would be uncharitable and unjust. The argument from charity, therefore, is too narrow to fit the whole case; and its very weakness is a source of error for the advocates of euthanasia.
Still another argument is often advanced against suicide, viz., that a man is obliged to love his own life, since it is the foundation, or the necessary condition, to him, of all good and every virtue, and this circumstance makes the destruction of that life unlawful. That argument has solid truth, but if it held absolutely it would prevent us from desiring death in any case, and no one denies that there are conditions in which a desire for death is fully legitimate. No desire for death, however, can give the slightest justification for the destruction of life.
Again, the argument that suicide is cowardice is not broad enough. Fortitude is a mean between fear and rashness, and this argument maintains that the suicide sins against fortitude by rashness. If we have good reason it is not rash to expose ourselves to death; the soldier may do so, the person struggling to save a neighbor's life, and so on; it may be the highest form of fortitude thus to expose oneself to death. If the suicide can persuade himself that by his act he is seeking greater good than the life he possesses he would have reason for his act, and at least be above cowardice. This argument is one that can be turned at times so as to cut the fingers of the man that uses it. The fundamental reason that suicide is not lawful is that man cannot be master of his own life, and therefore he may not dispose of it as he pleases.
Suicide is the direct killing of oneself on one's own authority.[9] A killing is direct when death is intended as an end, or chosen as a means to an end. Direct killing is positive by commission, or negative by omission. In such cases the will directly rests in the death as a voluntary and free act. A killing is indirect when the act of which death is the effect by its nature and the intent of the agent is directed toward another end, but concomitantly, or as a consequence, results in death. In such case death is an accidental effect, and comes indirectly from the activity of the will—it is not necessarily voluntary. If one has a right to do that other deed, or if it is his duty to do it, and there is a proportion between it and his life, he may do the deed and permit the consequent death.
A direct homicide may be done on one's own authority, or on that of another person. It is done on one's own authority if the agent assumes a natural individual dominion over life, and by virtue of such dominion directly kills himself or another; it is done on the authority of another when a man directly kills himself or another by the mandate of a positive divine or human law, and in the name and on the authority of a positive divine or human legislator. It is evident that God, as Creator, has supreme dominion over human life, and therefore by his positive authority he may command a man directly to kill himself. God, however, does not by the natural law confer on man the right thus to kill. The question here is of the natural duty or right which comes from the natural law alone.
Direct suicide on one's own authority may happen in two ways: positively, that is, by doing an act which is directly homicidal; or negatively, by omitting an act necessary for the preservation of life. That a negative homicide be direct, death must be intended as an end or means. If, however, one voluntarily intends an end or a means, but for the sake of antecedent good or evil omits some act necessary to preserve life, his suicide is indirect, per accidens, and not always illicit unless there is a precept against just such an omission. Man has no dominion over his own life, he has only the use of it; and the natural law obliges us while using a thing which is under the dominion of another not to omit ordinary means for its preservation. We are not, however, held to extraordinary[10] means. His own death is criminally imputable to him who negatively and indirectly kills himself by omitting the ordinary means for preserving his life, because the precept he is under to preserve his own life makes his act voluntary. If he omits extraordinary means, the death is not criminally imputable to him because there is no precept obliging such means. Certain circumstances may by accident oblige one to use extraordinary means to preserve one's own life—a dependent family, a public office in perilous times, or the like. The proposition, then, is: The natural law does not give a man absolute dominion over his own life.
I. The natural law gives no rights except such as are finally founded in human nature itself; but human nature cannot give a title to dominion over one's own life; therefore the natural law does not give man such a right.
Every natural right is either congenital or acquired. The title to a congenital right is human nature itself; the title to an acquired right is some act consequent to the exercise of human activity. The right to such exercise is, in turn, congenital and founded in human nature.
If nature established the title to dominion over one's own life it would thereby establish the power of destroying that life, and thus of removing the fundamental title to all rights; but nature exists as the foundation for rights, not for the subversion of rights; therefore human nature cannot give a final title to dominion over our own life.
Again, this minor of the first argument is confirmed by the fact that if nature even remotely established the power of self-destruction there should be in nature itself some natural tendency to such destruction, but the direct contrary is the fact.
II. The natural law cannot grant a right to man which is not a means to the common end of human life; but absolute dominion over one's own life is not such a means, therefore the natural law cannot give one dominion over his own life.
The natural law is only an ordination of man to that common end of human life and to the means toward that end. As regards the minor of this second argument, an absolute dominion[11] over his own life would give man power to stop all his human activity, yet the common end of human life is attainable only by man's activity. The stopping, or the power of stopping, all activity cannot be a means to that end.
III. The natural law cannot give man a power which is opposed to the essential needs of human nature itself; but that a man should have absolute dominion over his own life is opposed to an essential need of human nature itself, therefore the natural law cannot give such a power.
Dominion over his own life implies the power in man of rebelling against the subjection which he owes to God; but human nature essentially demands that man be in subjection to God, since dominion over one's own life and subjection to God are contradictory.
Again, if man had absolute dominion over his own life he could stand aloof from all influx of the natural law and avoid every duty arising from that law. A law, however, cannot give a power which nullifies itself.
The objection that suicide is licit because no injury can be done a man by an act if the man is willing to submit to the act, is irrelevant. The injury in suicide is not to man at all, but to God.
There is also nothing in the objection that a gratuitous gift may be renounced. Life is not a gratuitous gift; it is an onerous gift with obligations inseparably affixed thereto which forbid the destruction of the gift.
IV. Destruction is an act proper to a master alone. Man cannot be master of his own life; he can have dominion of things that are outside himself, distinguishable from himself, but not of the very existence of himself, which is not really distinguishable from himself. The definition of dominion supposes relation. The offices of master, father, magistrate, are relative conditions which suppose superiority over another person, not over oneself. Even God is not a superior over himself, although he has all perfection. For this reason a man cannot sell himself; he can sell only his labor.
God, who should have absolute dominion over all creatures, and who has, wills to confine these creatures to certain lines of[12] action in keeping with the creature's nature. This is the law underlying even the moral law when it touches humanity; it is the eternal law coeternal with God's decree of creation, but not necessary as God is. When this law exists in the mind of God it is the eternal law; when it exists in the minds of creatures it is the natural law, governing the free acts of intellectual creatures. When the natural law becomes a motive to the human will, obliging but not forcing it, a law through knowledge within the consciousness of a man regulating his behavior, it is called the law of conscience.
Conscience is an act, a practical judgment on one's own action in some particular case. It testifies, accuses, excuses, restrains, urges. It is a rational faculty, not an emotional, sentimental power. Emotion blinds its judgments. Yet mere emotion, and that foolish deordination of emotion called sentimentality, are promptings which the ignorant mistake for conscience and obey. Conscience is the enlightened eye of the heart, not the vagary of any appetite that blunders into action. It must be educated; left to itself, it is guilty of all the perversions of the streets.
The natural law is immutable, not subject to recall by every rascal under the goad of the flesh. In morality what was, is; what was once right because reasonable, always will be right and reasonable. Since opposition to the natural law as applied to man is repugnant to human nature, no power can make opposition to that law licit. For the same reason this law is not subject to evolution. Truth in morality is eternal. What is ugly now was ugly a millennium ago; what was immoral yesterday was immoral in the sixth century. If our ancestors thought permissible what we know to be illicit, our ancestors were ignorant; the fact has not changed. It was as immoral to steal, lie, or murder in the day of Abraham as it is to-day.
The ultimate tendency of man is toward happiness, and, of course, happiness, or any other perfection, is impossible without existence; hence the instinctive recoil from the destruction of our life, which is the requisite condition for happiness. Even those that abnormally destroy their own life do[13] so with horror for the destruction itself, and act thus unreasonably to escape evil, not to escape life; or they seek what they think will be a better life. We can do no other injury to a man so great as the depriving him of his life, for that deprivation destroys every right and possession he has. He can recover from all other evil, or hold his soul above every other evil, but death is the absolute conqueror. No matter how debased or how diseased a man's body may be, no one may dissociate that body from its soul, except in defence of individual or social life under peculiarly abnormal conditions; but even such defence is permissible only while the defender respects other human life and the social life, while he is innocent, has done no harm to society commensurate with the loss of his own life.
Existence, no matter how sordid, is immeasurably better than non-existence, for non-existence is nothing; and when we consider eternal life after separation from the body, even as a probability, that raises existence to infinite possibilities above the void of non-existence. A human life, even in an Australian Bushman, in a tuberculous pauper, in the vilest criminal, is in itself so stupendously noble a thing that the whole universe exists for its upholding toward betterment. The raising of human life toward a higher condition has been the sole tendency of all the magnificent charity, sacrifice, patriotism, and heroism the best men and women of the world since time began have striven in. The necessary first cause itself is life, and life is by far the most sacred thing possible for the first cause to effect. Eternal life is the greatest reward of the just.
It is not permissible under any possible circumstance directly to kill an innocent human being. By killing directly is meant either (1) as an end desirable in itself, as when a man is killed for revenge; or (2) as a means to an end. By an innocent human being is meant a person who has not by[14] any voluntary act of his own done harm commensurate with the loss of his own life.
To kill a human being is to destroy human nature, by separating the vital principle from the body; to destroy anything is to subordinate and sacrifice that thing absolutely to the purposes of the slayer; but (1) no one has a right so to subordinate another human being, because man and his life are solely under the dominion of God. If a man may not kill himself, as we proved above, because he is not master of his own life, he surely may not kill another to whom he is no more closely related as master than he is to himself. (2) No man has a right to subordinate another human being as is done in slaying him, because this other human being is a person, an intelligent nature, and consequently free, independent, referring its operations solely to itself as to their centre. This very freedom differentiates man from brutes and inanimate things. These are not independent; they are rightly possessed by man; but man may be possessed by no one except God. Even extrinsic human slavery is abhorrent to us as a corollary of the intrinsic freedom of man, which is absolute. This intrinsic freedom is such that we may not under any circumstances lawfully resign it to another's possession. This is one of the chief moral objections to oath-bound secret societies which exact blind obedience. All morality depends on that freedom, all peace in life, all civilization, and society itself.
The end of our struggles, toil, fortitude, temperance, thrift, is freedom,—freedom to do and to hold, freedom from the thraldom of vice and barbarity. The rational endeavor of every civilized nation is that it be free; and this means solely that every citizen thereof, from the highest to the lowest, is made secure in his rights as a human being. It intends that justice should prevail. Nearly all the unhappiness, crime, moral misery, and much of the physical misery in the world are due to a disregard for liberty, for the safeguarding of men in their inalienable rights. Give every man his bare rights as a man and all troubles of capital and labor, all race problems would cease, the prisons would be empty, war would be unknown. Our struggle toward justice, toward the protection[15] of the rights of man, toward liberty, must go on, or anarchy and social destruction will ensue. Now, as there is nothing greater and nobler than liberty, the freedom of the sons of God to do what they have a right to do, and as every human being has a right to that liberty, so there is nothing baser than its contrary, the destruction of that liberty; and no destruction is so final as that of killing the man, no usurpation so abhorrent to human nature and all liberty. Abhorrence for such a destruction is the primal instinct of all human beings; even the irrational reflexes of our bodies react quickest in protecting us from that destruction.
Justice and order must prevail; that is a fundamental natural law to which all other laws are subordinate. Justice, moreover, is a moral equation, and whenever one right transcends another it must be superior to the right it holds in abeyance. The right an innocent human being has to his life, however, is so great that no other human right can be superior to it while he remains innocent. Subversion of this right by creatures is intrinsically evil, as blasphemy and perjury are evil, although not in exactly the same degree.
There are occasions upon which it is permissible to kill, indirectly, innocent persons. An effect is brought about indirectly when it is neither intended as an end for its own sake, nor chosen as means toward an end, but is attached as a circumstance to the end or the means. Means help to an end, circumstances often do not, although they may affect the morality of an act.
Suppose two swimmers, Peter and Paul, are trying to save Thomas, who dies in the water; as he dies Thomas grips Peter and Paul so tightly that they cannot shake the corpse off. Peter is weak, and he will soon sink and drown, owing to his weakness and the weight of the corpse; Paul also will go down later, owing to the weight of Peter and Thomas. Peter, however, cuts his own clothing loose from the grip of the corpse and is saved; but Paul immediately is drowned, owing to the fact that the full weight of the corpse comes upon him. Is Peter justified in cutting himself loose? Certainly he is. This is an example of indirect killing, a case of double effect,[16] one good, the saving of Peter's life, the other evil, the loss of Paul's life, both proceeding immediately and equally from the causal act, the cutting loose of the clothing. The good effect is intended, the bad effect is reluctantly permitted.
Again, let us set the same condition for Peter, Paul, and Thomas; but Peter is not able to cut himself loose. John, a fourth person, can cut Peter loose and save him, but can do no more; he must let Paul go down with the corpse of Thomas. May John cut Peter loose? Certainly he may, on the principle quod liceat per se licet per alium. This is another case of double effect, with the extenuating circumstances as above.
Suppose, however, Peter represents a living infant in the womb of Ann, and that she is in labor; further, this infant cannot be delivered owing to the contraction of Ann's pelvis. May John, a physician, cut away Peter by craniotomy and so save Ann's life? Certainly he may not. John here directly brains Peter to save Ann, although Peter is not an unjust aggressor; he does a murder to get a good effect, and the end does not justify the means. There are two effects, but the good effect follows from the bad one, and not immediately from the causal act.
Take another example: Peter is a swimmer disabled by cramps and about to drown; Paul, going to save Peter, is seized by Peter, and both are now in danger of drowning; John goes to help Peter and Paul. He cannot get Peter's grip loose by ordinary means, and he sees he can save only one man, either Peter or Paul. May John knock Peter senseless to loosen his grip from Paul, bring in Paul, and thus leave Peter to drown? Certainly he may. You have the double effect here also. Moreover, Peter is a materially unjust aggressor; he is like a maniac trying to kill Paul. In the craniotomy case the child is not a materially or formally unjust aggressor, it is not doing anything at all. It is where the mother put it, and it has a full right to its position and its life.
John most probably might also knock Paul senseless and save Peter, if through affection or similar motive he preferred this course. He would then be justified by the double-effect principle alone, although Paul is in no sense an aggressor. The[17] intention of the blow would have to be solely to loosen Paul's hold.
In a just war a commander may shell an enemy's works and indirectly thereby kill non-combatants. The gunners that cause the death of the non-combatants do not intend this death; they permit it as the evil effect which comes immediately with the good effect (the capture of the works) from the causal act of firing the guns.
If we keep within the bounds of a just defence we may protect ourselves against an unjust aggressor to the effusion of his blood, or even, if need be, to killing him. An aggressor is any one who does injury to us contrary to our rights and the ordination of right. A formally unjust aggressor is a sane intelligent person who intentionally attacks us; a materially unjust aggressor is one who is not intelligent, not responsible, as an insane person, a child, or a sane person who is injuring us unintentionally. This question is important in medicine because the fetus in utero is often erroneously called an unjust aggressor.
It is a primary law of nature that every human being should and will strive to resist injury and destruction. Justice requires a moral equation, and if one right prevails over another it must be superior to the right it supersedes. At the outset both the aggressor and the intended victim have equal rights to life, but the fact that the aggressor uses his own life for the destruction of a fellow man sets the aggressor in a condition of juridic inferiority to the victim. The moral power of the aggressor here is equal to his inborn right to life, less the unrighteous use he makes of it; while the moral power of the intended victim remains in its integrity, and has therefore a higher juridic value.
The right of self-defence is not annulled by the fact that the aggressor is irresponsible. The absence of knowledge saves him from moral guilt, but it does not alter the character of the act considered objectively; it is yet an unjust aggression, and in the conflict the life assailed has still a superior juridic value. In any case the right of wounding or of killing in self-defence[18] is not based on the ill will of the aggressor, but on the illegitimate character of the aggression.
The condition's of a blameless defence (moderamen inculpatae tutelae) are: (1) that the aggressor really threatens the defender's life, and there is no means of offsetting that violence except like violence; (2) that no more violence is used than is adequately required: if the aggression can be stopped by wounding the aggressor the defender is not to kill him; (3) that the violence in the defence is used with the intention of defence, not in revenge, hatred, anger, or the like motives.
We may do an act good in itself from which a double effect immediately follows, one good, to which the agent has a right, and the other bad, which the agent is not obliged to omit if permitted by him and not intended; but in the case of a necessary defence of life against an unjust aggressor, made even with the death of the aggressor, the defence is such an act, provided the moderation of a blameless defence is observed.
The evil effect here is not a means to the good effect, nor does it more immediately follow from the act done. The evil effect is an effect per accidens, and thus not directly voluntary, either in itself, because it is not intended, or in its cause. It lacks the condition necessary to make it voluntary in cause as regards the accidental effect since the act is not prohibited precisely because this accidental effect follows.
The act in the case is good in itself; it is an application of physical force in defence of a proper right, and any right supposes a compulsive power. The two effects of this double-effect act are: (a) the preservation of the defender's life, and (b) the death of the aggressor. The first effect is good because the defender has a right to his own life; the other effect is evil, not only physically for the one who dies, but morally inasmuch as the death conflicts with the dominion of God. This death, however, is an accidental effect of the act, because in general the defensive act is not directed by its nature to that death but to the preservation of the defender's life; nor does the death follow more immediately than the preservation. Thus it[19] is not a means of the defence. Finally, the defensive act is not prohibited precisely lest that death follow: not in justice, for there is no justice in any right of the aggressor which requires from the defender an omission of defence unto the loss of life; there is no obligation in charity, since charity does not oblige us to love another more than ourselves, or to exalt the good of another above our own.
In an aggression which is merely material—say, in an attack by an insane man—the defender has a right to the infliction of such damage as is necessary and proportionate to an efficacious defence. The right of the aggressor yields to the superior right of the defender, not through the fault of the aggressor but through his misfortune. There is a collision where both rights cannot be exercised at the same time, and there is no reason obliging the defendant to forego his own right.
We may defend another against an unjust aggressor because we can assume that the attacked person communicates to us the use of his own coactive right. If the aggressor is our own father, mother, son, or daughter, or in general any one to whom charity obliges us more than to the person attacked, we are not permitted to kill our own kin because charity does not oblige us to prefer the good of an alien to the good of one of our blood. Ordinarily we are not obliged in justice or charity to defend another at the risk of our own life.
We may kill an unjust aggressor, servatis servandis, in defence of good equivalent in value to life: for example, to prevent life imprisonment, the loss of reason, a mutilation which would render us useless, the loss of a woman's chastity.
There are cases of accidental homicide, in medicine and elsewhere, which have an element of guilt in them. If a death follows accidentally upon an act which in itself is licit, and the agent uses all proper precautions, he is not morally guilty in case of an accidental death following his act. This is true even if the agent foresaw a probable death but did not intend it. If, however, the agent's primary act is illicit in itself, and an accidental death follows from this act, the agent may be guilty of homicide, provided the first act in itself is naturally[20] likely to cause homicide. Should the first act be always dangerous, such that death commonly follows from it, like rocking a row-boat, aiming a supposedly unloaded gun at a person and pulling the trigger, striking a pregnant woman, drinking whiskey and then overlying an infant in the bed, throwing building material from a roof to a street, racing an automobile through a crowded thoroughfare, sending a crew out in a rotten ship, and so on, the accidental homicide that follows is imputable to the agent no matter how much precaution he may say he has used to avert such a death.
Suppose, secondly, the original act of the agent is illicit but such that accidental death rarely follows from it; then if he takes due precaution he is not ordinarily guilty of homicide. He has, say, stolen an automobile, and is going along the street leisurely, when a careless child runs off the sidewalk under the machine and is killed.
1. No person, then, may hasten his own death or permit any one else to hasten it.
2. No physician may in any possible condition kill a patient merely to effect euthanasia.
3. The state has no more right than the physician to permit the killing of patients to bring about euthanasia.
Were such permission given to physicians it would immediately be abused by men with even the best intentions. In all countries and in the largest cities the medical profession is swarming with quacks. What is done in crass ignorance by licensed physicians and specialists every day in the name of medicine is appalling. Professor Orth of the Pathologic Institute in Berlin makes the statement that of all the appendices that have been submitted to him for microscopic examination after removal by conservative and supposedly skilled physicians, 17 per cent. showed no disease at all, and should not have been removed. In this country the percentage of normal appendices removed because of vague abdominal pains is much larger.
The Journal of the American Medical Association (June 7, 1913) gave a list of post-mortem examinations where the[21] diagnosis made by men with a reputation for fair work had been correct in only the following ratios:
| Diagnosis | Diagnosis | |
| correct. | incorrect. | |
| Per cent. | Per cent. | |
| Diabetes Mellitus | 95 | 5 |
| Typhoid Fever | 92 | 8 |
| Aortic Regurgitation | 84 | 16 |
| Cancer of Colon | 74 | 26 |
| Lobar Pneumonia | 74 | 26 |
| Chronic Glomerular Nephritis | 74 | 26 |
| Cerebral Tumor | 72.8 | 27.2 |
| Tuberculous Meningitis | 72 | 28 |
| Gastric Cancer | 72 | 28 |
| Mitral Stenosis | 69 | 31 |
| Brain Hemorrhage | 67 | 33 |
| Septic Meningitis | 64 | 36 |
| Aortic Stenosis | 61 | 39 |
| Phthisis, Active | 59 | 41 |
| Miliary Tuberculosis | 52 | 48 |
| Chronic Interstitial Nephritis | 50 | 50 |
| Thoracic Aneurism | 50 | 50 |
| Hepatic Cirrhosis | 39 | 61 |
| Acute Endocarditis | 39 | 61 |
| Peptic Ulcer | 36 | 64 |
| Suppurative Nephritis | 35 | 65 |
| Renal Tuberculosis | 33.3 | 66.7 |
| Bronchopneumonia | 33 | 66 |
| Vertebral Tuberculosis | 23 | 77 |
| Chronic Myocarditis | 22 | 78 |
| Hepatic Abscess | 20 | 80 |
| Acute Pericarditis | 20 | 80 |
| Acute Nephritis | 16 | 84 |
Pneumonia is a very common disease, extremely dangerous, and by skilful treatment it is very often cured, yet of these 100 cases 66 were not diagnosed. I recently saw a severe case of double pneumonia which a physician was treating as "indigestion," and he was giving pepsin tablets for the supposed indigestion. There is such a thing as extraordinary scientific precision in medical work, but it is rare; the ordinary physician treats symptoms without knowing the cause of the symptoms; that is, the symptom-treater is a quack, and if euthanasia were legalized thousands of such quacks would be permitted to murder with an overdose of morphine any querulous old man or woman who might fall into their[22] hands. Osteopaths and chiropractors are masseurs, and they know very little of massage, but they are licensed by legislatures to practise medicine, and some of them even try obstetrical malpractice. They, too, would be licensed to inflict euthanasia. Pure homeopathy is little more than a name at present; it is faith-healing without prayer. It attenuates its drugs 100 per cent. for thirty repetitions, to a degree expressible by one with sixty ciphers. Consequently it gives sugar of milk or alcohol in minute quantities plus a label, and one cannot make much of an impression on any disease with a label. Such practitioners also would come under the euthanasia act.
BIBLIOGRAPHY
Cardinal John de Lugo. Disputationes Scholasticae et Morales, vol. vi; De Justitia et Jure, disputatio x.
St. Augustine. I Contra Petilianum, cap. 24; Ad Marcellianum Comitem, cap. 21; De Civitate Dei, cap. 17 to 28.
Aristotle. III Ethicorum, cap. 7, and lib. v, cap. ii. Plato. Phaedo.
Cicero. Quaestiones Tusculanae. I, lib. v; De Somno Scipionis.
Lessius. De Justitia et Jure, lib. ii, c. 9, dub. 6, 7.
Molina. De Justitia et Jure, vol. i, tr. 2, disp. 119; vol. iv, tr. 3, disp. 1 and 9.
St. Thomas Aquinas. Summa Theologica, 2, 2, q. 64, a. 5, 7.
St. Alphonsus Liguori. Theologia Moralis, vol. iv, tr. 4. See this book for opposed opinions and a bibliography.
Costa-Rossetti. Philosophia Moralis, thesis 120.
Ferretti. Philosophia Moralis, theses xci, xciv.
Macksey. De Ethica Naturali, theses xxxiv et seq.
The members of the human body may be injured (1) by a blow, which without bloodshed causes pain or a bruise; (2) by a wound, which breaks the continuity of the tissues; (3) by mutilation, which, without killing, removes some member requisite for the integrity of the body. The term Mutilation as applied to the human body has various meanings. In the civil law mutilation of a person is called Mayhem, an old form of the word Maim, and is defined by Blackstone[5] as "such hurt of any part of a man's body as renders him less able in fighting to defend himself or annoy his adversary." By statute in the United States and Great Britain the scope of the offence has been so extended as to include injuries to a person which merely disfigure or disable. Mutilation in the civil law now implies the taking away of some part of a legal instrument, as a will, contract, or the like, by any one who has no right to make this alteration.
In canon law mutilation is like malicious or accidental mayhem in the civil law, and it has also a technical phase in relation to irregularity as affecting the reception of ecclesiastical orders. The mutilation requisite to irregularity as affecting the reception of Holy Orders may differ from mutilation in its purely moral and accidental aspects. Broadly, an irregularity is a canonical and permanent impediment to the reception and exercise of ecclesiastical orders. It does not exist unless it is actually promulgated in some canon, and it is not necessarily grounded on corporal deformity. Defects of the body that cause canonical irregularity are such as would render the public ministration of a clergyman either impossible or indecent.
Molina, treating of mutilation, says[6] it does not exist unless there is an amputation or shortening (detruncatio) of a member. When a foot or hand is so weakened without amputation that it cannot exercise its function the person is said to be maimed or lame, not mutilated. He holds that a finger, and a fortiori a phalanx of a finger, are not properly members. In defining mutilation as a cause of canonical irregularity[7] he contends that the weakening of a member so that it cannot perform its function is not a true mutilation canonically. He does not agree[8] with Cajetan, de Soto, and others who hold that an important part of a whole member is equivalent to a member so far as technical canonical mutilation is concerned. Molina says that a part of the body as a member to fulfil the requirements of the law on mutilation as a cause of irregularity must have a distinct, complete function of its own, not be a mere part conducing to the function. Ballerini[9] agrees with Molina, but he draws attention to a decretal of Innocent I. which makes an amputation by oneself of even a part of one's own finger a full canonical irregularity, because of the unnatural quality of the act.
Suarez defines mutilation thus: "Mutilare significat proprie membrum aliquod abscindere"[10]—to mutilate means, strictly speaking, to cut off any member. He holds with Cajetan that an important part of a member is in itself equivalent to a member. A reason he offers for his opinion is that a eunuch is enumerated among those who are canonically mutilated, but the eunuch, he tells us, "does not lack any member which in itself has a function in the body independent of all other organs." This is not true. The testicles, which the eunuch lacks, have two distinct functions, independent of other organs—they make the spermatozoa and an important internal glandular secretion. These facts were not known in Suarez's time (1548-1617). Suarez adds this remark: "There can be a grave sin in a marring [diminutio] of any chief member,[25] although there may be no grave mutilation; as, for example, to cut off a part of a finger is undoubtedly a mortal sin, yet, in the opinion of all moralists, it is not enough to cause irregularity."
St. Alphonsus Liguori defines mutilation thus: "Mutilation here signifies that some principal member be separated from the body; that is, a part of the body that has in itself a distinct function, as a foot, hand, eye, ear, etc."[11] He says[12] canonical irregularity as a punishment is not incurred by a person who cuts off another man's finger, thumb, lips, nose, auricle, or who knocks out teeth, because these are supposed by canonists not to be properly members of the body, but parts of members. To blind a man in one eye is not enough to cause canonical irregularity; the eye must be taken out.[13] All these injuries are of course mutilations in the moral sense of the term. To blind a man without removing the eye, to cut out his spleen in the treatment of Banti's disease, to remove a woman's ovary or uterus, to cut off part of the point of a finger, to crop the top of an auricle, to knock out a tooth, and any other permanent marring of the body, even to cause an unsightly scar across the face, are all mutilations in the moral sense of the term. A physician, midwife, nurse, or parent who neglects an infant's eyes, and so permits ophthalmia neonatorum to blind the child, is guilty of grave mutilation. In the year 1914, in the Chicago schools, 45,176 children were found suffering from various defects, and 35,425 were advised by the examining physicians to seek treatment; in each of these cases the parents were informed of the nature of the disease and the necessity for treatment, but only 40 per cent. of the parents paid any attention to the notices. Of 5754 cases of diseased tonsils, which are likely to affect the heart permanently, only 4 per cent. were treated; of 1254 cases of discharging ears only 10 per cent. were treated, although such a condition may go on to deafness if not attended to. These[26] parents were criminally guilty of grave neglect in permitting the mutilation of the heart and ears.
Any notable mutilation inflicted upon oneself is akin to the malice of suicide, and when perpetrated on another it is related to homicide. The dominion over the members of the body, as over the whole body, belongs to God alone. Man is constituted by his parts, members, taken together, and if he were master of his members he would be master of himself. Again, each member of the body is naturally united to that body and ordained for determined organic functions; so it is wrong to render these members unfit for their natural function or to separate them from the body, unless such actions are necessary for the preservation of life itself. Although man is not master of himself, he is the administrator of himself; and therefore when the amputation of any member is necessary for the preservation of the life of the whole body it is licit to subordinate this part to the good of the whole.
A direct mutilation is one intended as an end, or as a means to an end; it is a voluntary and free act. An indirect mutilation is one in which the mutilation is the natural effect of the act, but the intention of the agent is directed toward another end. The mutilation follows indirectly from the activity of the will, but there is a satisfying proportion between the accidental effect (the mutilation) and the end intended. In such an act there are two effects which follow the causal act aeque immediate, or directly (not indirectly, that is, not all from the other effect, but each immediately from this cause): one effect is good (to save life, avoid unbearable pain, or the like), and the other evil (the mutilation), but the good effect is the end intended, the evil effect is reluctantly permitted. Such an act is licit provided the usual conditions of the double effect are present, that is:
1. The action that is the cause of the good and bad effects must be itself good or indifferent morally.
2. The good and the bad effects must each be an immediate result of the causal act; the good effect may be not so subordinated to the evil effect as to be obtainable only through the evil effect.
3. The bad effect must not be intended, either immediately or remotely; it may at most be tolerated as unavoidable.
4. There must be a sufficiently grave reason for the act.
Indirect mutilation may be licit when the evil to be avoided is proportional to the mutilation. Direct mutilation, where there is one direct effect of, say, the surgical operation, namely, to remove the somatic organ, is not licit, except for the good of the whole body; and that good to the whole body must be juridically equivalent to the damage done the body by the mutilation. There is to be a direct effect in such mutilation, which is the good of the whole body. It is not permitted to kill directly to save the life of another, but it is permissible to mutilate directly to save the whole body. Direct mutilation, however, is never unavoidable because the agent can always correctly order his intention before the operation.
All direct mutilation, unless for the good of the whole body, implies deordination: it offends against the supreme dominion of God, who reserves to himself, as Creator, ownership of human life and its organs. As we may not destroy life, which belongs to God, we may not amputate a member to suppress any vital function. The exception which permits us to mutilate a member or organ is, as has been said, the adequate good of the whole body. The reason for this is that man is the administrator of his members, to the good of the whole person. Each member is not for itself but for the whole body.
The good of the body is the sole cause that renders direct mutilation licit. The members of the body by their nature are not immediately subordinate to anything except the conservation of the total natural good, or that of the body. Therefore direct mutilation is not permissible to effect immediately spiritual good, or the good of the soul. We may not castrate a man, or do vasectomy on him, to preserve his continence, because there is no immediate subordination and connection between the members of the body and the salvation of the[28] soul. Moreover, as St. Thomas says,[14] "Spiritual health can always be preserved by means other than amputation of bodily members," that is, through moderating by the will the use of these members. If a mutilation that immediately conduces to the good of the whole body, happens also to do good to the soul, this second effect is then legitimate. (The various mutilations of the body by surgical operations will be considered separately hereafter.)
May the state, then, sterilize criminals, and persons afflicted with dangerous hereditary diseases, to prevent the propagation of moral and physical defectives? This question is considered specially in another chapter.
There is an error gradually infecting all nations of late which is that the state, as such, is above morality; that what the civil authority permits or orders is by that fact alone made licit or obligatory. Hence the interference with individual liberty, with the rights of man, shown by laws for the mutilation of the physically degenerate, laws conferring privileges on one part of the community to the detriment of another, meddling in parental rights, and so on. Political error has come to such a pass that the men on the street think any majority is justified, solely because it is a majority, in recalling a judge or a law, in overriding authority for the satisfaction of appetite. The sovereign people tries to be subject and sovereign at the same time, and it deems its rulers mere hired men who may be discharged at will like cooks.
A law is a rule and standard of action; a just, permanent, and rational ordination for the good of the community, promulgated by one who has charge of that community. Dominion is the power of claiming a thing as one's own, the right of ownership; and if this possessor has created the object, his dominion may be absolute. A governor, lawgiver, judge, has power or jurisdiction for the good of the governed. The business of government, of the state, is to protect each citizen in the pursuit of temporal happiness, to develop his natural faculties, establish and preserve social order, wherein each citizen is secured in his natural and legal rights, and is[29] held up to the fulfilment of his own duties so far as they bear on the good of the community as such; and also to put within the reach of all citizens, as far as possible, a fair allowance of means to acquire temporal happiness, or external peace and prosperity. This is the whole business of the state. The state is for the people, and it may not transgress an inch beyond its proper limits, which are as hard and fast as those that bind the individual citizen. The citizen is not to be treated solely as an industrial or military unit; nor are material progress and military power, or even sheer intellectual civilization, to be the sole aim of the state. The state should develop a man's entire nature, physical, mental, and moral.
We must obey civil authority, but we are not slaves or chattels of that authority. The state's authority over us is not dominative; it is only a power for our good and utility. The civil authority has no more right to invade the rights of its meanest citizen than it has to lie or to blaspheme. God gives civil authority to the established community, and the community entrusts this to its ruler; authority is a divine institution, rulers are directly a human institution and only indirectly divine. When the ruler has once been set up, has had authority entrusted to him, obedience must be given to him while he acts in keeping with his contract. Kant and his followers erroneously separate the juridic from the moral order; they deny that beyond the state there are any rights preeminent to the state's rights, yet they say there is an innate liberty which belongs to every human being equally and inalienably. The moral order comprehends all factors that are necessary to make the free activity of man in every respect well disposed, and among these factors is the juridic order itself. Man is naturally social, and whatever means are necessary to preserve human society are also naturally befitting man. Such means are to preserve for each man what are his, and to abstain from injuring other men. Now, so to act, that is, to abstain from murder, theft, and the like, to fulfil contracts, are strictly juridic duties, and at the same time moral duties. Therefore the moral order comprehends the juridic order.
The end of the state, then, is not the public good considered[30] as an end in itself. The individual citizen is not his own end in life, and so no mere multitude of men ever can become their own end. If the end of the state is the public good, then private good is subordinate to this, and the public good becomes man's final end, which is subversive of human dignity and is despotism.
A clear definition of the power of the state to interfere with the rights to life and limb of the individual citizen is very important, because, as has been said, of late there is an alarming tendency on the part of the civil authority to override the rights of private citizens, even in the most democratic forms of government. Encroachment on the liberty of the individual is characteristic of unchristian political societies, and all states are now receding from Christianity. A striking example of this tyranny is the laws recently passed in ten American states for the mutilation of degenerates. This definition is more readily made by considering concrete examples of public conduct.
Suppose an enemy demands from a city the surrender for execution of an innocent man on pain of the burning of the city and the destruction of its inhabitants. May the city cut off that member for the safety of the whole body politic, as a person may cut off his own hand to save his life? The state has not dominion over the life of a citizen, nevertheless it may kill a citizen in punishment of crime, because the punishment is useful to the whole people, is for the common good, is preservative of the social life. Why, however, should the state be permitted to kill a criminal rather than an innocent man, since it has no dominion over the life of either, and we suppose the death of each is necessary for the public good? If you answer by saying a man may cut off a diseased member but not a sound one to save his body, and the state in like manner may cut off a criminal, unsound member, but not an innocent one, this answer does not remove the difficulty: we may cut off even a sound member to save the body. Suppose, for example, a man caught by the arm and in danger of death from a flood; he might sever a sound arm to escape death if no other means presented. In like manner the state might cut[31] off an innocent, sound member to save its life from the enemy, as described above.
This reasoning, however, is open to objection. The state has no dominion over the life of its members, and there is a vast difference between the members of the human body and those of a body politic. A member of a human body has no right in itself against the other members; nor is it capable of natural injury, since it is not separable from the whole suppositum, or person. The suppositum, or person, has a right to the use of the members; it alone is injured when a member is amputated; and the members are solely for the utility of the suppositum. Therefore we may licitly destroy a member to save the suppositum for which this member exists.
The state, however, is not a suppositum in this sense; it may not wrest the life of its members to its own utility, because the citizens are not for the state; on the contrary, the state is for them and their utility. That a rational being should be for the utility of another person or a society makes him a slave and supposes dominion in the user. A slave is differentiated from a subject by the fact that the subject is only politically governed—that is, governed for his own utility and good; the slave is governed despotically—that is, for the utility and good of his master. The state may not, as a master, use the life of a subject for its own utility alone. Although the suppositum does not own its members, yet since the members are not separable from the man, are not self-centred as are the citizens in a state, the man may use them for his own utility. They are as slaves under a master, not as subjects in a body politic; therefore they may be sacrificed for the good of the suppositum.
This is the argument used by De Lugo; Molina follows the same line of thought; but both authorities finally reach the conclusion, in the case of the enemy and the citizen whose life is required, that the state may at least drive this citizen out of the city to save its own existence. Molina also draws attention to the fact that there is a great difference between a member of a body politic and a member of the human body; this[32] identification, if pushed far enough, becomes an analogical quibble.
Some hold that a judge or the civil authority in general may kill or maim a criminal by gubernatorial power alone, prescinding from dominative power, and this not to the utility of the criminal but for the utility of society. The killing of a criminal, these objectors say, is not for the good of the criminal; it is a deterrent, a protective act, for the good of society. This is not true. The penal law which the criminal breaks was not made solely for society; it was intended also for the utility of the person who becomes a criminal. The law was made and the punishment established that all subjects indiscriminately should be helped to live honestly and blamelessly, and to this end it was necessary to decree and inflict punishment as affecting all offenders. The obligation to receive punishment is in a manner essential to man. As he naturally requires direction and government unto virtue in his political and social life, he has a connatural obligation to endure punishment when he violates the law made for his advantage—one condition cannot exist without the other. Hence punishment really is to the utility of the criminal.
By the embryologists from the moment the spermatozoön joins the nucleus of the ovum until the end of the second week of gestation the product of conception is called the Ovum; from the end of the second week to the end of the fourth week it is the Embryo; from the end of the fourth week to birth it is the Fetus. At what moment during these three stages does the human soul, the substantial form of a man in the full comprehension of the term, enter the product of conception? When does the thing become a human being?
The question is evidently one of the greatest importance. If the rational soul does not enter until the ovum has developed into an embryo, or only after the embryo has passed on into the fetal condition, the destruction of this ovum, by artificial abortion or otherwise, would be a very different act morally from such destruction after the soul had turned the new growth into a living man. If the product of conception has first only a vegetative vital principle, and this is later replaced by a vital principle that is merely sensitive, and this again is finally superseded by a rational vital principle, the destruction by abortion or otherwise of the vegetative or sensitive life would not be a destruction of a rational life. In this hypothesis the killing of the embryo would be a great crime, because the embryo would be in potency for the reception of human life, but the act would not be murder.
The discussion concerning the moment the human soul enters the body is older than Christianity, and it was taken up by many of the early Greek and Latin Fathers of the Church, and revived again and again down to the present day. Plato thought the soul enters at birth; Asclepias, Heraclites, and the Stoics held it is not infused until the time of puberty; Aristotle[34][15] said the soul is infused in the male fetus about the fortieth day after conception, and into the female fetus about the eightieth day.
Tertullian,[16] Apollinaris, and a few others advocated Traducianism,[17] or a transmission of the spiritual soul by the parents. He said souls are carried over by conception and by the parents, so that the soul of the father is the soul of the son, and from one man comes the whole overflow of souls. St. Augustine used the metaphor, one soul lit from another as flame from flame, without decay in either. Augustine was in doubt as to the origin of the soul, and inclined to traducianism, because it seemed to him better to explain the doctrine of the transmission of original sin. "Tell me," he wrote to St. Jerome in 415,[18] "if souls are created singly for each person born to-day, when do infants sin so that they need remission in the sacrament of Christ, sin in Adam from whom the flesh of sin is propagated?... Since we cannot say that God makes of souls sinners, or punishes the innocent, nor may we hold that souls even of infants which without baptism leave the body are saved, I ask you how that opinion can be defended which thinks that all souls are not made from the single soul of the first man, yet as that soul was one to one man, these are particular to particular individuals."
Again, St. Augustine said:[19] "I do not know how the soul came into my body; he knows who gave it, whether he drew it [traxerit] from my father, or created it new as in the first man." In the Book of Retractions,[20] speaking of the articles he had written against the Academicians before he was a bishop, he says: "As to the origin of the soul, how it is set in the body—whether it is from that one man who first was created ... or, as in his case, is made particularly for each particular individual, I did not then know, and I do not know now." St. Gregory the Great also said he could not tell[35] whether the human soul descends from Adam or is given particularly to each man.
St. Gregory of Nyssa, however, who died about 385, thirty years before St. Augustine wrote the letter to St. Jerome, held that the soul is infused into the body at the moment of conception, and he argues with absolute precision for his opinion.[21] St. Maximus the Theologian, who was martyred in 662, inveighs[22] against the notion that the soul is vegetative at first, then sensitive, and finally intellectual, and he thinks the assertion of Aristotle that the fetus is not animated before the fortieth day is altogether untrue.
St. Anselm, who died in 1109, very dogmatically denied that the fetus is animated at conception,[23] and after his time the doctrine of Aristotle, which is commonly called the Thomistic opinion, became almost general. Vincent of Beauvais, however, a contemporary of St. Thomas, opposed the Thomistic doctrine. Albertus Magnus[24] had the same opinion as St. Thomas, and probably taught it to St. Thomas. In the middle ages all held that each soul is directly created by God, and is infused into the embryo, not at the instant of conception, but when the embryo is sufficiently formed to receive it, which, as Aristotle said, happens at about the fortieth day in males and the eightieth day in females. The Thomists maintained the succession of the three souls; many others opposed this particular opinion.
Thomas Fienus, a physician and a professor in the University of Louvain, in 1620 published a book[25] in which he held that the soul is infused about the third day after conception, and his argument for the early advent of the soul is very sound. As a result of Fienus's revolutionary argument, Florentinus in 1658 brought out a book at Lyons, called De Hominibus Dubiis Baptizandis, in which he held that no matter what the age of the aborted fetus, if it could be differentiated from a mole it should be baptized. This book was brought before the Congregation[36] of the Index. The congregation did not condemn the book, but the author was forbidden to teach that his doctrine holds sub gravi. The book went through many editions and was approved by the faculties of the principal universities and the theologians of the leading religious orders.
Zacchias, chief physician to Innocent X., in 1661 published his Questiones Medico-Legales, and in this he maintained that "the human fetus has not at any time any kind of soul other than a rational, and this is created by God at the first moment of conception, and is then infused."[26] By 1745 the opinion of Zacchias as to the moment life begins was virtually general among physicians, and has since remained the doctrine of physicists. Modern discoveries by biologists have confirmed the fact that human life exists in the impregnated ovum exactly as it does in all stages of life, and no scientist holds any other opinion. There are, however, a few moralists at the present day who incline to the old Thomistic doctrine or to modifications of it.
St. Alphonsus Liguori[27] was a follower of the Thomistic opinion. He affirmed: "They are wrong that say the fetus is animated at the instant of conception, because the fetus certainly is not animated before it is formed, as is proved from Exod. xxi: 22, where in the Septuagint version we find: 'He that strikes a gravid woman and causes abortion, will give life for life if the child was formed; if it was not formed, he will be fined.'" This argument by St. Alphonsus is invalid apart from any facts that may bear upon either the Thomistic or the modern opinion concerning the quickening of the fetus. The text from the Septuagint Exodus is (1) too doubtful in itself to be the basis of any argument; but (2) even if it were authentic just as it stands, the conclusion St. Alphonsus draws from it is not warranted by the premises. The Septuagint text differs from the Vulgate and the Hebrew texts. The Vulgate has it thus: "Si rixati fuerint viri et percusserit quis mulierem praegnantem, et abortum quidem fercerit, sed ipsa vixerit, subjacebit damno quantum maritus mulieris expetierit et[37] arbitri judicaverint; sin autem mors fuerit subsecuta, reddit animam pro anima, oculum pro oculo, dentem pro dente, manum pro manu, pedem pro pede, adustionem pro adustione, vulnus pro vulnere, livorem pro livore."[28] This version has nothing whatever to say about the foetus formatus or non formatus; it is merely an application of the Semitic Lex Talionis, and the form of the law is clearly corrupt and inaccurate.
The passage quoted by St. Alphonsus as that of the Septuagint is not exact even as the Septuagint has it. The full text is: "If two men fight, and one strike a woman that hath [a child] in the womb, and her babe come forth not yet fully formed,[29] in a fine he shall be mulcted; whatsoever the husband layeth upon him he shall give according to decision [i.e., of the judges]. But if it [the babe] be fully formed he will give life for life, eye for eye, tooth for tooth, hand for hand, foot for foot, burning for burning, wound for wound, stripe for stripe."
This is (1) evidently nothing but an application of the Lex Talionis, with no thought whatever of the biological animation, as such, of the fetus. It means that if a fully formed fetus be aborted, either no real damage is done, as such a child is viable; or the formed child may be maimed, and then the Lex Talionis is to be applied. If the fetus is not fully formed it is not a fit subject of the Lex Talionis since it cannot lose an eye, a tooth, and so on, because it lacks these organs and therefore the law of retaliation is not to be enforced.
(2) Suppose, however, the writer of the text as the Septuagint has it did think with St. Alphonsus that the formed fetus is animated, and the unformed is not animated, even then the conclusion drawn by St. Alphonsus is not warranted by the text. The laws of Exodus do not teach embryology, physiology, or any other part of physical science; and no[38] authority worth a hearing holds that the Scriptures were intended to be infallible treatises on obstetrics or astronomy. Like the other parts of the Bible, the laws of Exodus presuppose the unscientific biological, astronomical, and other physical notions of the time in which they were written—the moral truth is the matter the Scripture is dealing with; there no inaccuracy is to be found. St. John (1:13) speaks of those who believe in Christ's name, "Qui non ex sanguinibus, neque ex voluntate carnis, neque ex voluntate viri, sed ex Deo nati sunt." Here he expresses the contemporary notion, which is also the Thomistic opinion, that men are generated from the specialized blood of their parents. He was interested solely in conveying the truth that those who received Christ were regenerated by him, not through heredity; and he does so, although the biology is inexact. If St. Alphonsus's conclusion is valid as from the text of Exodus, then men are generated ex sanguinibus, and so on indefinitely.
The Massoretic text of this passage seems to be the best preserved: "If men fight, and one hurt a woman who is with child, and her child come forth, yet there is no mischief, he [who struck her] shall be mulcted in a fine; whatsoever the husband of the woman layeth upon him he shall pay according to the judges. But if there be mischief, then he shall give life for life, eye for eye, tooth for tooth, hand for hand, foot for foot, burning for burning, wound for wound, stripe for stripe." Here the Hebrew text follows the Lex Talionis exactly. If, in a brawl, a man's pregnant wife is struck and abortion results, the offender pays the penalty. If the abortion does not kill or maim the child, the culprit is fined by the Sanhedrim; if the child is killed or maimed, then the penalty is according to the Lex Talionis. In the Hebrew text also there is no mention of a distinction between a foetus formatus and non formatus.
Whether the fetus is animated at conception or some time later, there is no foundation whatever for the notion that the female is quickened later than the male. As was said before, Aristotle held that the human male fetus is animated at the fortieth day, the female at the ninetieth day, and the[39] old moralists accepted his statement. At the fortieth day, however, no one can differentiate sex unless the microscope is used, and this particular use of the microscope is altogether modern—the knowledge requisite for such use was not in existence sixty years ago. At the twentieth day, with the microscope and a stained specimen, a biologist can recognize whether the primordial ova are present or absent and thus determine sex. Only at the eighty-fourth day can sex now be differentiated without the aid of the microscope, but then the embryo must be dissected: nothing can be told from its external appearance. Sex can first be distinguished by the external appearance only at about the one hundred and twelfth day, the end of the fourth month of gestation. Therefore when Aristotle said the male fetus is animated at the fortieth day, and the female at the eightieth or ninetieth day, he was romancing.
The question, then, narrows to this: Is any human fetus animated immediately at conception, or from forty to eighty days after conception? The reason given by the followers of Aristotle for deferring animation is that the vital principle requires organs in the receptive material, but the embryo in the early stages, they say, lacks these organs. This notion, however, as to the lack of organs is altogether erroneous, and the rational soul enters the embryo in the oval stage, immediately after the pronuclei unite: there is organization in that stage of human life sufficient to receive the substantial form or soul. We do not know how long after insemination the pronuclei unite, but the proposition here is that as soon as they unite the human soul enters. Fecundation usually occurs after a menstruation, but not necessarily so; the spermatozoön may live in the tube for seventeen days awaiting the ovum.
The human body is made up of billions of microscopic living cells, all of which are derived by fission and differentiation from the two original single germ-cells, the ovum and the spermatozoön. Some nerve-cells have long processes running along the white fibres through the entire length of the body, but they cannot be differentiated except by the microscope.[40] In the body are also various liquids which are not cellular, as water, saliva, tears, urine, blood and lymph plasma, and the gastric, intestinal, and glandular juices, and these are secreted or excreted by the somatic cells. The cells assimilate nutritive material carried to them by the blood, excrete refuse substances, secrete glandular products, and are the media for all human operations below certain acts of the intellect.
A typical animal cell is commonly spherical in shape, but it may take a great variety of forms through compression. It has a cell-body or protoplasm, which is called also cytoplasm, especially when contrasted with the nuclear karyoplasm, and a nucleus. A few cells, like fat-cells and the human ovum, have an external covering membrane, or cell-wall. There is a part called the Centrosome observable in many cells, and this is made up of one or two minute dots surrounded by a radiating aster called the Attraction-Sphere. The centrosome is concerned in the process of cell-division and in the fertilization of the ovum; it is an important organ in the production of cell from cell, though its full nature and function are not yet known. The Plastid, or Protoplast, is another less important part found in certain cells; and in this by enlargement and differentiation are formed starch, pigment, and in some cases chlorophyl. Vacuoles are seen in cells; and there is an opinion that these may be a special kind of plastid: some vacuoles pulsate.
The Nucleus is the most important part of a cell, the centre of its activity. The specific qualities of organism in origin and development are based upon nuclei, so far as the material element of the living cells is concerned. Vital stimuli pass through the nucleus into the surrounding protoplasm, and these stimuli control metabolism. The nutritive cytoplasm assimilates, but the vital principle energizes this assimilation through the nucleus, for a part of a cell deprived of the nucleus may live for a time, but it cannot repair itself. Constructive metabolism ceases when the nucleus is lost. A toxic disease like diphtheria kills by disintegrating cellular nuclei.
In the nucleus are several elements, the chief among which[41] is Chromatin. Chromatin takes various forms, but commonly it is an irregular network. From the chromatin are derived the Chromosomes in the prophases of indirect cell-division which is the process of cell-division in the human body, except in lymph-cells and white blood-corpuscles, which split directly, or by Amitosis. Indirect cell-division is called Mitosis or Karyokinesis. In the male and female chromosomes, according to a common opinion of biologists, all the elements of parental and phyletic physical heredity are transmitted to the embryo.
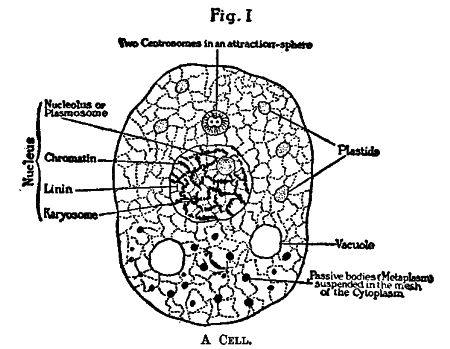
Fig. I
A Cell.
Throughout the Cytoplasm is a mesh containing numerous minute granules called Microsomes.
The production of cell from cell is accomplished either by direct splitting of the nucleus and cytoplasm into two new cells, or by indirect division through a series of stages. In a typical direct, or amitotic, division the nucleus is constricted in the middle and divides into two daughter-nuclei. These by amoeboid movements withdraw to the poles of the cell; the cell finally divides between them, and thus two cells are formed. These, again, split into four, the four into eight, and so on. An amoeba by direct division can separate into two distinct new animals in ten minutes.
Heredity here is simple. In unicellular organisms, such as Rhizopoda and Infusoria, each individual grows to a certain stage, and then divides into two parts, which are exactly alike in size and structure, so that it is not possible to decide whether one is older or younger than the other. These organisms reduce the size of their overgrown bodies by division. Each individual of any such unicellular species is a part split off serially from an organism which started into life ages ago. Some of them have come down in uninterrupted life from geological epochs that passed away eons before the first man was created. Many of these unicellular plants and animals have immeasurably the most ancient form of life on earth. Heredity with them depends upon the fact that each offspring is merely half of its parent. In some cases the division has a sexual quality: two cells in Paramecium, and, like Infusoria fuse and then divide if they come into contact; they can, however, split without this sexual process.
Multicellular plants and animals do not reproduce by simple division, and the half of the parental body does not pass over into the progeny. Sexual reproduction is the chief means of multiplication in multicellular organisms, and in no case is it completely wanting; in most it is the only method of reproduction. In multicellular animals the power of reproduction is in the germ-cells, which differ from the somatic cells. Germ-cells do not maintain individual life as the body-cells do, but the germ-cells alone preserve the species. From two of these germ-cells under certain conditions is developed a complete bodily organism of the same species as the parents. These two cells are in a sense the undying cells; the somatic cells die.
Multicellular animals—Man, for example—grow embryologically by Mitosis or Indirect Division. As in Direct Division, typically, the nucleus in mitosis splits first and the cytoplasm secondly; but before the nucleus divides its content undergoes a series of changes. The chromatin loses its reticular arrangement and gives rise to a definite number of separate bodies, usually rod-shaped, known as Chromosomes. In this process the chromatin becomes a convoluted thread, called the[43] Skein or Spireme. The thread thickens and opens out somewhat, and finally breaks transversely to form the chromosomes, which may be rods, straight, curved, ovoid, and sometimes annular. Commonly the nuclear material fades away and leaves the chromosomes in the cell-plasm. (Fig. II, 2 and 3.)
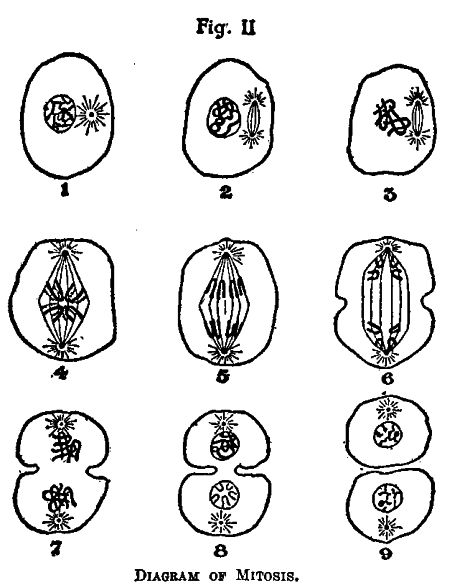
Fig. II
Diagram of Mitosis.
1. Cell with resting Nucleus. 2. Prophase: Chromatin in thickened convoluted threads, beginning of Spindle. 3. Prophase: Chromosomes. 4. Prophase: Spindle in long axis of the Nucleus, Chromosomes dividing. 5. Anaphase: Chromosomes moving toward the Centrosomes. 6. Chromosomes at the poles forming the Diaster, beginning splitting of the Cell-body. 7. Telophase, Daughter-Nuclei returning to resting state. 8. Daughter-Nuclei showing Monaster below. 9. The two new Cells.
It is almost an established fact that each species of animal and plant has a fixed and characteristic number of chromosomes, which regularly recurs in the division of all its cells. In forms arising by sexual production the number is even. The number of chromosomes in the human cell is said to be[44] forty-eight. There are, according to some observers, forty-seven chromosomes in man and forty-eight in woman. There seem to be twice as many chromosomes in white men as in negroes. Wilson gives the number[30] of specific chromosomes for seventy-four animals and plants. Germ-cells as differentiated from the somatic cells have in the perfected cell always half the number of chromosomes found in a somatic cell.
While these changes are going on in the chromatin the Amphiaster forms. This consists of a fibrous spindle-shaped body, the Spindle, at either pole of which is an Aster made up of rays. In the centre of each aster is a Centrosome, and this may have a Centrosphere about it. As the amphiaster grows the centrosomes are grouped in a plane at the equator of the spindle, forming the Equatorial Plate. (Fig. II, No. 4.) The process so far makes up the Prophases of the Mitosis.
In the Metaphases of the Karyokinesis begins the actual division of the cell. Each chromosome splits lengthwise into exactly similar halves, and these, in the Anaphases of the mitosis, drift out to the opposite poles of the spindle to form the daughter-nuclei of the new cells. The daughter-nuclei receive precisely equivalent portions of chromatin from the mother-nucleus, and this is an important fact in mitosis. As the chromosomes go toward the poles the cell-body begins to constrict at the equator.
In the final phases, the Telophases, the cell divides in a plane passing through the equator of the spindle, and each daughter-cell receives half the chromosomes, half the spindle, and one of the asters with its centrosome. A daughter-nucleus is reconstructed in each cell from the chromosomes. The aster commonly disappears and the centrosome persists, usually outside the new nucleus, but sometimes within it. Every phase of mitosis is subject to variation in different kinds of cells, but the outline of the division given here is the fundamental method.
The germ-cells differ from the body-cells in general by[45] containing half the number of chromosomes characteristic of a given animal or plant. If the body-cell has, say, twenty-four chromosomes, the spermatozoön of the animal or plant from which the cells are taken will have twelve chromosomes and the ovum will have twelve. When the nuclei of these two cells unite in fertilization the resulting primordial cell will have the twenty-four chromosomes restored, the specific number for this plant or animal. In oögenesis and spermatogenesis the phases of "Reduction," wherein the ovum and spermatozoön get rid of half the chromosomes during the stages of maturation of these germ-cells, are somewhat similar for both sexes. The process is very complicated, but it is of importance in the theories of inheritance. All the physical characteristics in a human being that come to him from his parents and remoter ancestors are supposed, by the biologists, to reach him through the chromosomes in the nuclei of the single parental germ-cells. The maternal physical heredity is handed on through the chromosomes in the ovum. The fetus in the womb is a parasite, autocentric, feeding at the start from the deutoplasm, or yolk, in the ovum, and later from the supplies brought to it by the maternal blood. The physical material it gets directly from the mother is very probably all in the chromosomes of the fecundated ovum. Some weeks elapse, and the embryo is quite advanced before it begins to draw food from the mother at all. So far as the father is concerned, there is no doubt whatever that every physical and pathological characteristic that can be handed down—and there are many such qualities—must come through the chromosomes of the paternal spermatozoön. Certain physical characteristics are passed on for centuries in a family—the Norseman's body in northeastern Ireland, the skin-pigment in the American negro, and so on indefinitely—and these qualities cannot come down except through the chromosomes. The germ-plasm has come to us from the first man, and it will be passed on to the last person of the race—we are all literally uterine brothers.
In the reduction of the germ-cells, if the primordial cell that finally produces the ovum has, say, four chromosomes,[46] these four chromosomes first split longitudinally and reduce into two tetrads, or two groups of four chromosomes. Outside the nucleus is a spindle toward which the two tetrads move; they pass out of the nucleus and become the equatorial plane of the spindle; each tetrad divides into dyads (pairs of chromosomes), and one pair of these dyads remains in the ovum, while the other pair leaves the ovum entirely and becomes the nucleus of an abortive cell, called the First Polar Body. Later a second polar body forms and carries another dyad (two chromosomes) out of the ovum, leaving only one dyad, or two chromosomes, in the germ-cells; that is, half the number of chromosomes that were in the primordial cell.
The reduction-division in spermatozoa is similar, but the end process leaves four active spermatozoa, whereas in the ovum the final result is one ovum and three practically inert and cast-off polar bodies. The reduction-division in both ovum and spermatozoön is in reality far more complicated than the broad summary given here. In parthenogenetic insects and animals a polar body takes the place of the spermatozoön, and fuses with the egg-nucleus to start mitosis.
In general, the new nuclei in the cells formed by division are not made de novo, but arise from the splitting of the nucleus in the mother-cell. The new nucleus assimilates material, grows to maturity, and divides again into two daughter-nuclei. Whatever be the number of chromosomes that enter a new nucleus as it forms, the same number issues from it in mitosis. Boveri said,[31] "We may identify every chromatic element arising from a resting nucleus with a definite element that enters into the formation of that nucleus, from which the remarkable conclusion follows that in all cells derived in the regular course of division from the fertilized egg, one half of the chromosomes are of strictly paternal origin, the other half of maternal." It is not strictly true to say that the germ-nuclei fuse: they send in two sets of chromosomes that lie side by side, as has been frequently demonstrated since[47] 1892[32] in many of the lower forms of life, and this law almost certainly extends also to man.
The primordial germ-cells appear in the human fetus about the twentieth day and finally mature at puberty. Then an ovum at menstruation breaks out through the surface of the ovary, and is taken by the fimbriae of the Fallopian tube into the lumen of this tube. Fecundation happens near the outer or ovarian end of the Fallopian tube, and the fecundated ovum finally is passed on to fasten on the wall of the uterus. The spermatozoön is a ciliated cell with the power of locomotion, through the movement of the tail of the cell. It can move 0.05 to 0.06 mm., or its own length, in a second. It thus passes up through the uterus and out through the Fallopian tube, against the cilary motion of the tubal cells, until it meets the ovum.
A human ovum is a typical cell, but it has a covering membrane, and a minute quantity of deutoplasm or yolk, which is not alive, and is food for the growing embryo before the embryo begins to draw sustenance through the placenta. The eggs of birds have a large quantity of food stored in the yolk, since their embryos live in the ovum and draw food therefrom during the entire period which corresponds to the time of gestation in mammals. The "white" and the calcareous shell of a hen's egg are adventitious parts, added in the oviduct after the egg leaves the ovary.
The spermatozoön is a complicated organism. The head is partly covered with a thin protoplasmic cap, and it contains the nucleus with the chromatin. In the neck are two centrosomes. The tail is in three parts with an axial filament throughout, which is a bundle of extremely minute fibrils. In the middle part the axial filament is surrounded by an inner sheath; outside this sheath is a spiral filament lying in a clear substance; and outside the spiral filament is a finely granular layer of protoplasm, called the Mitochondria. This organism is a living animal cell, and it can live in an incubator, or in the Fallopian tube for two or three weeks, altogether removed from the living male body that produced it. Sir[48] John Lubbock[33] says he kept a queen ant alive for thirteen years. This ant, which died in 1888, had been fertilized in 1874, and never afterward. She laid fertile eggs for thirteen years; that is, the spermatozoa in her oviduct retained their vitality for thirteen years.
The human spermatozoön is a living cell: it has (1) the requisite structure; (2) the chemical composition of an organic being; (3) a figure in keeping with its species; (4) an origin from a living progenitor; (5) the explicatio naturae; (6) the power of assimilation; (7) the duratio viventium; (8) the power of reproduction; (9) motion and locomotion. As soon as the ovum breaks through the surface of the ovary it has all the qualities of the spermatozoön except locomotion. These two cells are animal cells, not vegetable; just as single-celled protozoa, like Actinophrys, Actinosphaerium, Closterium, Stentor, and the Amoebas are animals, not plants. It is not possible in our present knowledge sharply to differentiate ultimate forms of plants from animals. To say that animals have the qualities of plants plus a sentient vital principle is not enough. It is very doubtful that even the so-called sensitive plants feel, and it is practically certain that many low forms of animal life do not feel—they have no sentient mechanism. Plants have the qualities enumerated above plus the power of drawing nutriment directly from inorganic material, while animals can draw nutriment directly only from organic material; yet some fungi, bacteria for example, will grow and thrive only on organic material, and animals will take up mineral drugs. It is questionable, however, that minerals which thus find a way into animal cells are really assimilated. They excite or irritate these cells into intenser action, and thus cause growth, rather than affect development by direction. The so-called mineral tonics used in medicine act by irritation.
This irritation or stimulation by drugs can in certain very low forms of animal life start mitosis in the unfertilized ovum, and thus build up part, at the least, of a specific embryo parthenogenetically: here probably a polar body takes the place[49] of the spermatozoön. Loeb, by treating the unfertilized egg of Arbacia (a sea-urchin) with magnesium chloride, started mitosis that resulted, it is said, in a perfect Pluteus larva.[34]
The human ovum is about half the size of a period in the type of this page, and two hundred and fifty spermatozoa will fit side by side along the horizontal diameter of the lowercase letter o here. The nuclei of these cells are extremely minute: they must be stained and be observed with a high-power objective on the microscope before they become visible. This small nucleus of the spermatozoön penetrates the covering membrane of the ovum, enlarges, and becomes the male pronucleus. The pronucleus unites permanently with the pronucleus of the ovum, and together they form the Cleavage or Segmentation Nucleus of the fertilized ovum. This new nucleus gives rise by division to the innumerable myriads of nuclei in the growing body. Hence every nucleus of the child apparently contains nuclear material derived from both parents, as has been said.
The two perfected germ-cells before fecundation are in a state of nuclear rest after the numerous mitotic changes that have taken place in the maturation of these cells. When these nuclei unite in the ovum an intense activity at once is set up. Biologists offer very many theories to explain this awakening force. Herbert Spencer, Herting, and others held that protoplasm when perfected tends to pass into a state of stable equilibrium and consequent lessened activity, but fertilization restores it to a labile state. This and similar theories are verbose amplifications of the obvious fact that the cells start to divide and the biologists do not know the cause. The soul, of course, cannot have anything to do with the matter, because you cannot smell a soul. "Senescence and rejuvenescence" is another sonorous explanation that does not explain, used by Minot, Engelmann, and Hansen. Weismann rejects these theories for his own "Fertilization as a Source of Variation." Anyhow, the fertilized cell starts to divide regardless of the biologists. Adult cells may be stimulated to divide by chemical irritation, by mechanical pressure as in[50] the formation of calluses, traumatism, by any agency that brings about an abnormal condition of the body, but this fact does not explain the normal fission of the fecundated ovum.
In about fifteen days from the date of fertilization the ovum passes through the following stages:
1. The ovum, with a full series of mitotic changes of the ordinary somatic type described above, divides, subdivides, and grows within the cell-wall until a rounded mass of cells is formed, which is called the Morula or Blastula—the original cell-wall, of course, stretches to hold these new cells. They are of unequal size, and they divide at unequal rates.
2. An albuminous fluid collects within the morula, and thus the Vesicle or Blastocyst is formed. The blastocyst is called more commonly the Cleavage Cavity or the Segmentation Cavity. As this cavity widens the cells are seen to be arranged in two groups—(a) an enveloping layer, the epiblast, from the outermost plate of which develops later the Trophoblast, or the nourishing and protecting covering of the embryo; (b) an Inner Cell Mass, made up of granular cells, attached to the epiblastic layer at the Embryonic Pole of the Vesicle. These two stages probably take place in the Fallopian tube, and thereafter the embryo is in the cavity of the uterus.
3. In the third stage the Inner Cell-Mass separates into two layers derived from the inner cell-plate of the blastula. The mass flattens and spreads peripherally, until finally it is divided into two layers. The outer is the Ectoderm and the inner is the Endoderm or Hypoblast. The three steps just described have not yet been seen in the human species by any one, but they are inferred very confidently from what is well known of the development in mammals most closely resembling man in physical formation.
4. By the conversion of the one-layered blastula into two layers of cells, the Gastrula stage of the embryo is attained. The Gastrula consists of two layers of cells surrounding a central cavity, which is the Archenteron, or the body-cavity that will hold the intestines. During the past twelve years many specimens of human gastrulas have been observed. The[51] earliest form was that seen in 1908 by Teacher and Boyce.[35] This embryo was 1.95 mm. in length by 0.95 mm. in width, about twice the size of a pin-head. It showed on section the endoderm, the ectoderm, and the beginning mesoderm, enclosed in a spherical mass of trophoblastic cells. The mesoderm is a plate of cells lying between the endodermic and ectodermic plates. When the mesoderm develops into two plates, a cavity, called the Primitive Coelom, appears between the plates. The Coelom becomes the space between the viscera and the body-walls in later development.
From the primary embryonic layers of cells, the ectoderm, the endoderm, and mesoderm, all the parts of the body are built up. From the ectoderm are produced the skin, nails, hair, the epithelium of the sebaceous, sweat, and mammary glands, the epithelium of the mouth and salivary glands, the teeth-enamel, the epithelium of the nasal tract, of the ear, of the front of the eye, and the whole spinal cord and the brain, with their outgrowths.
From the endoderm come the epithelium of the respiratory tract, of most of the digestive tract with the liver and pancreas, the epithelium of the thyroid body, the bladder, and other minor parts.
From the mesoderm are developed bone, dentine, cartilage, lymph, blood, fibrous and alveolar tissues, muscles, all endothelial cells, as of joint-cavities, blood-vessels, the pleura and peritoneum, the spleen, kidneys and ureters, and the reproductive bodies.
The epiblast now with its mesoblastic lining begins to form the Chorion, an embryonic intrauterine appendage; and the endoderm encloses the Archenteron or primitive gut. Before the end of the second week of gestation the heart is indicated as two tubes in the mesoderm, and the blood-vessels begin to be produced in the yolk-sac. About the twelfth day the mouth-pit shows, and the gut-tract is partly separated from the yolk-sac. The medullary plate of the nervous system is laid down about the fourteenth day, and the nasal area is[52] observable. The maternal blood escapes into spaces about the embryo enclosed by masses of embryonic cells, which have not separated from one another, but which are known collectively as Syncytium.
5. With the third week the stage of the embryo, technically so called, begins. During this week the body of the embryo is indicated. There are three layers of cells, already mentioned, the ectoderm, mesoderm, and endoderm, and these lie on the floor of the enveloping Amnion. The amnion is a loose fluid-filled sac (the caul) enveloping the fetus to protect it from jarring. The fluid in it is the "waters" that escape in parturition when the infant breaks through the caul. The archenteron in the third week shows the beginning of a division into two parts: the part that will go to the body proper of the embryo, and the part outside the body of the embryo which will form the yolk-sac, or umbilical vesicle, from which the embryo will draw sustenance until the placental vessels have been formed. The part of the archenteron that remains within the embryo proper begins in this third week to be moulded into the head-cavity. The forepart of the archenteron will later make the alimentary tract from the mouth to the middle of the duodenum, or small intestine beyond the stomach. The other part of the archenteron wall make the Allantois, the hind gut and the bladder. The allantois becomes a part of the fetal umbilical cord after the formation of the placenta.
During this third week the dorsal outline of the embryo is concave; the heart has a single cavity, which will begin to divide during the fourth week; the vitelline blood circulation begins, and the blood-vessels of the visceral arch are laid down. The digestive system is advanced to a gut-tract, which is a straight tube connected with the yolk-sac. The liver evagination is present and the oral pit is a five-sided fossa. The respiratory system is represented by the anlage of the lungs, a longitudinal protrusion of the ventral wall of the esophagus. The genito-urinary system begins as the Wolffian bodies. The mesoderm starts to segment to form the skin, and the neural canal (from which develop the spinal cord[53] and brain) for the nervous system forms. The fourth ventricle of the brain is indicated, and the vesicles of the fore brain, mid brain, and hind brain are recognizable. The ears, nose, and eyes, muscular system, skeleton, and limbs are also beginning to be recognizable. At about the sixteenth or eighteenth day of gestation the various parts of the embryo rapidly differentiate.
In the fourth week all these parts advance. The atrium cavity of the heart begins to divide; the alimentary tract shows the pharynx and esophagus, stomach, and gut; the pancreas starts, the liver diverticulum divides, and the bile-ducts appear. The lung anlage bifurcates and the primitive trachea is seen. The ventral roots of the spinal nerves appear, the interior ear is indicated, and the eye is deeper. The buds of the legs and arms appear about the twenty-first day—by the thirty-second day even the fingers are present. The four heart-cavities are formed, the intestinal canal is nearly closed, the first indications of the liver and kidneys appear. The child now has reached the fetal stage, and its living body is made up of myriads of cells all derived from the original fertilized ovum. The fetus is then one centimetre, or two-fifths of an inch, in length—about the length of the word "fetus" here.
At the end of the second month the fetus is two and a half centimetres long. The ears appear, and the tail-like process at the lower end of the spine disappears. The arms show the three parts, arm, forearm, and hand; and a little later the thigh, leg, and foot are differentiated. The navel begins to close, the liver develops, the abdomen is yet partly open.
At the end of the third lunar month the fetus is seven to nine centimetres long. The intestinal canal is formed and contains bile. The body resembles that of a human being, but the head is proportionately very large. Bony tissue begins to appear.
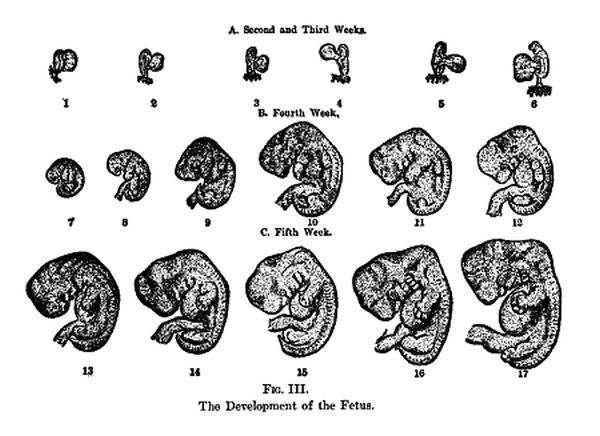
Fig. III.
The Development of the Fetus.
At the end of the fourth lunar month the fetus is ten to seventeen centimetres long. Some muscles are movable. The heart-beat is strong. Sex is distinguishable externally. [55] The skin is bright red, and so transparent that the blood-vessels are visible through it.
Toward the close of the fifth lunar month the head is about the size of a hen's egg. The skin is somewhat less transparent. There are indications of hair and nails. The eyelids are closed. Parts of the brain and spinal cord are formed. Such a fetus may live for five or ten minutes if removed from the womb, and it may make attempts at respiration.
At the end of the sixth lunar month the fetus, if born, may live for several hours under favorable circumstances. Its respiratory, digestive, and related organs are not developed, and no artificial feeding will keep such a child alive. The brain cortex, the organ of consciousness, begins to laminate into three strata of nerve-cells at the beginning of the sixth month.
Here the time of fetal viability outside the womb may be considered. Langstein, of the Augusta Victoria Hospital in Berlin, reported[36] a study of the growth and nutrition of 250 prematurely born infants, and he found that a weight of 1000 grammes (21⁄5 pounds) and a full body length of 34 centimetres (133⁄5 inches) are the lowest limits for viability under proper circumstances. A fetus 1000 grammes in weight and 34 centimetres in length has completed the sixth solar month, or the sixth and a half lunar month; that is, it is viable at the beginning of its seventh month, servatis servandis.
The child at term, as a rough average, is from 48 to 52 centimetres (19 to 201⁄2 inches) in length, and it weighs from about 63⁄5 to 71⁄2 pounds. It is impossible, however, to obtain the sizes and weights of infants in utero with scientific accuracy, because the date of conception cannot be determined with absolute certainty, and individual fetuses vary as do infants after birth. A full-term infant sometimes may weigh only 31⁄2 pounds when the mother is diseased, and again an eight-month fetus will weigh as much as 8 pounds. Large muscular and fat women have large babies; women of the well-to-do classes have larger babies than do the poor; women who work during gestation bear smaller babies than do those women that rest. Mothers who work in tobacco, lead, or phosphorus[56] have puny babies; white children are larger at birth than negro children; boys at term are 3 to 5 ounces heavier than girls.
Langstein says that prematurely born infants weighing from 900 grammes (311⁄2 ounces) to 1500 grammes (31⁄2 pounds)—that is, all born before the seventh solar month—must be kept in hot-water incubators in a room with ordinary ventilation. Babies weighing 2000 grammes (41⁄2 pounds) or more get along in an ordinary crib if they are kept surrounded with hot-water bags. Such children are to be fed with human milk through a catheter passed into the mouth or they die of inanition. Only a few of them are strong enough to suck from a bottle, and these give up the effort after a few days and die. They cannot utilize fat, even from milk; and all artificial food is dangerous.
Most of the prematurely born become rachitic, and even human milk is not preventive of this condition. Rachitis is a constitutional disease, characterized by impaired nutrition of the bones and changes in their shape. In the third or fourth month craniotabes is frequent—that is, an atrophy of the skull bones with the formation of small conical pits. These infants show also a morbid tendency to convulsions—spasmophilia. Such diseases are caused by a lack of mineral salts, which normally are carried to the fetus by the placental blood during the last two months of gestation. Because of this lack premature infants require the administration of lime salts in their food; they also need iron because they are anemic.
A fetus, then, of six calendar, or solar, months (not lunar) is viable if treated in a hospital by competent physicians. Otherwise it is not viable, except in a strictly technical sense; it will not live more than a few days or weeks. Reports of infants younger than six months as having been successfully reared are not credible—it is easy to make an error in the reckoning.
A full seven-months infant may be reared with proper feeding and skilled care; a six-months infant may be reared (with difficulty) in a hospital with skilled care. If it is certain that the removal of a six-months fetus will here and now[57] save the life of a mother (a very difficult matter to judge by the best diagnosticians), this removal may be done, provided the infant is delivered in circumstances where skilled care, incubator, and proper food are obtainable; otherwise the removal is not justifiable. That the ordinary physician says it is necessary to empty the uterus is not a sufficient reason, as he is likely to act from ill-digested information set forth by professorial pagans, who place no value whatever on human life in an infant.
A most important and essential circumstance in the matter of inducing abortion at the end of the sixth month of gestation to save a mother's life is that in practically every case requiring such interference the diseased condition of the mother has checked the growth of the fetus, and the fetus therefore is really not a six-months child in development. Such an undeveloped fetus is not viable. Eclamptic women, and those who have nephritis, are most likely to have undeveloped fetuses. In cases of this kind the seventh month should be completed before interference.
How is this human body in all its complexity developed from the microscopic germ-cells? There has been a vast deal of ink spilled in striving to solve this mystery, but we come out empty by the same door wherein we went. The early Preformationists guessed that the ovum contains an embryo fully formed in miniature, and development is a mere unfolding of what had already existed. The biologists of to-day mention the Preformationists with superior scorn, and then present Preformationism under other names. Weismann's theory is the most fashionable at present.
In a paper read at the Darwinian Memorial Congress in 1909, Weismann said: "With others I regard the minimal amount of substance which is contained within the nucleus of the germ-cells in the form of rods, bands, or granules, as the germ-substance, or germ-plasm, and I call the individual granules[37] ids. There is always a multiplicity of such ids present in the nucleus, either occurring individually or united in[58] the forms of rods and bands (chromosomes). Each id contains the primary constituents of the whole individual, so that several ids are concerned in the development of a new individual." Actually there are such things as chromosomes, and when these are stained and are under the highest power of the microscope they appear to be granular. These granules Weismann calls ids. Beyond the fact that there are such granules, all else is sheer guessing.
He says further: "In every complex structure thousands of primary constituents must go to make up a single id; these I call determinants, and I mean by this name very small individual particles, far beyond the limit of microscopic visibility, vital units, which feed, grow, and multiply by division. These determinants control the parts of the developing embryo,—in what manner need not here concern us."
There is some truth here. The id is made up of molecules and atoms, ions and electrons, and in some manner, of course, these have to do with the development of the embryo; but as to the manner we have not the slightest knowledge, and just this knowledge is what we need to make the theory anything more dignified than a child's game at guessing. There is a structural differentiation in the unsegmented ovum, with all the embryonal axes foreshadowed in it, but this tells us nothing more than that the egg contains the man in germ.
He goes on: "The determinants differ among themselves; those of a muscle are differently constituted from those of a nerve-cell or a glandular cell, etc., and each determinant is in its turn made up of minute vital units, which I call biophors, or the bearers of life."
That these so-called determinants differ among themselves may be true, if they exist at all, which is just the point to be proved. Giving Greek names to inventions does not turn invention into fact. These supposed determinants, he says, "may vary quantitatively if the elements of which they are composed vary; they ... and their variations may give rise to corresponding variations of the organ, cell, or cell-group which they determine." Professor Dwight said:[59][38] "This is what is palmed off on us for science!" Weismann assures us we must admit this farrago of clumsy fiction, otherwise we should be forced "to assume the help of a principle of design."[39] In the name of common sense, then, admit a principle of design, and be done with it!
Darwin's Gemmule Theory is the same guessing; and Weismann rejects it because he did not think of it first. As a theory the gemmule plot is just as good and just as bad scientifically as Weismann's. The chief objection to such imagining is that after its authors have put it into print a few times they lose all sense of humor, and mistake phantasms for facts.
Up to the present time we have discovered no living organism lower in grade than the cell. If life ever originated from inorganic matter, it appeared in an organized cell. The Weismann ids, biophors, and the rest, supposing they existed outside his own imagination, are not more capable of independent life than is a chromatin granule. In any event, these biophors could not have originated spontaneously in the first living being; and if they could not so have come into existence, life could never have begun. However primitive any organism is, it must be able to nourish itself and to develop into a higher specific form; but such a variety of functions supposes differentiated structure, composed of unstable chemical substances, a correlation of parts, a purposeful anticipation of ends. Inorganic substances, crystals, and the like are characteristically stable, not unstable; and these could not have been brought into the organic state on an earth burnt to a cinder and devoid of chlorophyl, which itself presupposes organic cells. Whence came also the absolutely essential form of energy, directive of vegetative life? The only possible explanation is that life was created, not evolved by a stranger miracle from a lump of lava.
We know the successive steps in the growth of the embryo from the time of fertilization to the end of gestation, but how this vital process is effected is not so evident. What we are certain of is that there is a vital principle of some kind from[60] the beginning, and this is the matter of real importance in the present discussion. The old moralists held that this principle in the human being is at first vegetative; after a while that vegetative vital principle is expelled by a sensitive principle; and finally this sensitive soul is expelled by the rational vital principle, or human soul. St. Thomas[40] says: "Some tell us the vital acts that appear in the embyro are not from its soul, but from the soul of the mother, or from the primitive force in the semen. Both these statements are false. Vital operations, as sensation, nutrition, growth, cannot come from an extrinsic principle; therefore it must be admitted that a soul preëxisted in the embryo, nutritive at first, then sensitive, and finally intellectual." After showing that an intellectual soul cannot be evolved from lower forms, he concludes: "Therefore we say that since the generation of one thing is always the corruption of another, in man as in other animals, when a more perfect form comes in this supposes the corruption of any precedent form; so, however, that the sequent form has all perfection that was in the destroyed forms, and something in addition: and thus through many generations and corruptions the final substantial form is attained in man and other animals. This is apparent to the senses in animals generated from putrefaction. Therefore the intellectual soul is created by God at the end of human generation, and this soul is both sensitive and nutritive, all precedent forms having been destroyed."
There is no such thing as the generation of any animal or other living being from putrefaction; but that is irrelevant. St. Thomas's argument proves conclusively that if man has first a merely vegetative soul, and secondly a merely sensitive soul, which includes the power of the vegetative soul, and thirdly an intellectual soul, which does the work of all three, that this final intellectual soul is not an evolution of the first two, but a new form that replaces these after they have served their purpose and have been annihilated. It does not even attempt to prove that man really has first a merely vegetative soul, and secondly a sensitive, and lastly an intellectual soul;[61] it supposes all this. It starts out with the erroneous Aristotelian theory and takes it for granted. The reason for this statement is that the rational substantial form requires disposed matter to work upon, and the Thomists suppose (again erroneously) that in the human embryo during the period immediately after conception there is not enough matter to be a receptacle for the rational soul.
The soul according to the Thomists, who use the Aristotelian definition, is the first entelechy of a natural organic body that has life in potency.[41] It is the determination that gives the body its specific and substantial being; the primal actuation of a body or matter, since only in matter is there a distinction between potency for substantial being and substantial actuality. An entelechy is a realization, actuality, full perfection; sight, for example, is the entelechy of the eye. This body is natural, not merely instrumental; it is energized by an immanent principle, not moved by an external force like a tool. The body is also organic; it must have organs, faculties, parts destined to perform definite functions. To say the entelechy has life in potency means that since life, or the operation of the soul, is an immanent act, there must be a receptacle within which it can be immanent, and the soul is the primal actualization of that organic body, which is in potency to produce those immanent actions in which life consists. A body might be in potency while it still has no principle of operation, or, secondly, while it has such a principle but is not using it. In the second condition the human body is in potency for life at the moment of actualization.
A form fixes a thing in its prχοντοσoper species, and the rational soul is such a form for the human body. This substantial form is the completion, perfection, in operability and existence, of the matter that receives it. It is the formal cause of man, not the efficient cause, although it is the efficient cause of subsequent vital operations. An efficient cause makes something numerically different from itself by its own real and physical action; a formal cause and a material cause do[62] not make anything different from themselves numerically, but they intrinsically constitute the effect—they are intrinsic causes.
The human soul as the substantial form virtually contains vegetative and sensory faculties, and through these lower organic capacities it informs and animates the body. That form, together with the matter, the body, does the vital acts of the composite human nature. The rational soul enters the body at the beginning, and first uses its vegetative faculty until the fetus is far enough advanced to be a subject for the action of the sensory faculty of the soul. Later, some time after the birth of the child, when the body is sufficiently formed, the intellectual faculty comes into use.
The nature of a vital principle is that in which it normally issues. If it issues as a rational substantial form, as in man, it was rational from the beginning. If it was not rational from the beginning, a rational principle replaced a sensory vital principle, and that sensory vital principle replaced a vegetative vital principle. The only reason for these replacements would be that the early human embryo, as has been said, lacks organization sufficient to sustain a form higher than a vegetative principle. If this were sufficient reason for deferring the advent of the rational soul, then a baby six months after birth would have no rational soul because it certainly lacks the supposedly requisite organs. However, as the rational soul is whole in each part of the adult body in the totality of its essence and perfection, but not in the totality of its virtue, because certain organs are lacking in particular parts of the body, it is in the embryo whole in the totality of its essence and perfection, but not in its virtue because certain organs are not yet formed, and it is thus from the moment of conception.
As to the soul itself, Kant held that the soul is not a real, but only a logical substance. The Pantheists, Transcendentalists, and Neo-Hegelians try to identify the soul with the divine consciousness. The Associationists (Hume, Davis, Höffding, Sully) say that the soul is a mere group of sensations. The Agnostics and Positivists (Locke, Herbert Spencer,[63] James, Comte) write volume after volume on the soul to prove that they know nothing about it. Then the Materialists assert that there is no soul of any kind; that we secrete thought as a mule secretes sweat. Yet the vital operations of man are inexplicable as resultants of the physical and chemical properties of matter. There is an intrinsic energy that unifies the actions of man, directs processes, controls the tendency of organic matter to pass into the fixity of the inorganic, and effects metabolism. This intrinsic energy is the entelechy, substantial form, or what is popularly called the soul.
In any organic body there is a formal principle. We know that there are activities that proceed from organic bodies, and a formal principle of such activity is a substantial entity whence the organism derives basically its own kind of action, which determines and orders the activity. There are acts of perception in animals such that an external object becomes so internal to the organism of these animals that it is known by one expressed and immanent image, not only as something objectively existing but as good or hurtful to the perceiving animal. The innate and elicited appetites by which the animal tends toward or away from the object are recognized, as are the spontaneous motions which are directed by that knowledge. There must be a principle whence these actions proceed, and this is either an accident of matter or something substantial. It is not an accident of matter, because action can never arise from an accident; it must proceed from a substance. If you say this principle whence these actions arise is not an accident of matter, but matter itself, you would have an extended, composite, inert mass acting; but even if such thing could act, it could never effect a simple immanent image of an object or group of objects external to itself.
No mere machine can build up itself, can make any remote approach to metabolism as an organized body can; and the principle of this immanent action is not matter itself, because it uses, makes, subordinates matter to itself. That principle is positively one, not one by continuity as matter is. Matter as in a crystal grows by mere aggregation, an organism[64] grows by assimilation; a crystal loses force in formation and growth, an organism accumulates force.
The theory that denies the existence of this formal principle does not explain the phenomena of life in organic beings. Uniformity of tendency toward an end is not a characteristic of mere matter; neither is a harmonious interaction of parts, nor the dependence of parts on the unit, nor motion, nor the reproduction of the species.
Moreover, most of the greatest physical scientists strongly maintain that there must be a formal substantial principle in all living things. Among these are Wallace, Nägeli, Askenasy, Preyer, Fechner, Agassiz, von Baer, E. de Beaumont, Blanchard, A. Braun, Brongniart, Bronn, Burmeister, Delff, Milne-Edwardes, Flourens, Goeppert, Griesbach, Heer, Koelliker, Mivart, Quatrefages, Quenstedt, Spiers, Volger, R. Wagner, Liebig, and Joseph Hyrtl.
The formal principle which coexists with matter in the organic body is really though not perfectly distinguished from matter. A formal principle which is necessary for sensation should be either perfectly simple, or at the least so one that its parts together make up one essence: matter, however, cannot have such unity, and as a consequence the formal principle must be distinct from matter. Anything is like its operation, and the parts of any sensitive activity always result in an activity that is essentially one. If we touch a table, by that single touch we at once know that the object is one, wooden, hard, angular, smooth, extended, and so on, and we also know that one subject perceives all these varied qualities. One eye can convey knowledge at once of a thousand objects miles apart, and these objects can be brought into one perception only by a simple subject. An extended complex subject like matter would get one impression (if it could perceive any impression) on one side, one on another, and so on, but it could not unite these.
The formal principle which is in organic bodies is a true substantial form, actuating the body both as to its nature and substance. Together with the body, this principle makes a being one in itself, such that the matter and the form separably[65] are incomplete as regards operation and being. Now, a form is that principle through which anything is established in its own species; light, for example, is the form of a luminous body, heat of a hot substance. A body, however, is established in the human species by receiving a rational soul, and this soul, then, is its form. It is also a substantial form because the soul itself is a substance, not an accident dependent upon another subject. Moreover, from its union with the body another substance—man—arises, and not a thing added to a substance. Man's body is alive, therefore it is a living substance; but life in its secondary actuality is an operation; in its primary actuality it is an essence. The body is made a living substance, not from itself, but from the soul which is added to it. When the soul departs the body is no longer alive. Now, a principle which by a communication of itself determines the body in its essence and differentiates it as a living substance from everything else, is a substantial form. A substantial form, then, or a soul, exists.
The soul, however, must have disposed matter for most of its operations; it cannot exist as a substantial form bombinans in vacuo; but it does not need a human organism complete in all its parts as a necessary condition for its indwelling. There is organized matter enough in the first cell that comes into existence after the fusion of the germ-nuclei to hold this rational form, or soul, as perfectly as it needs to be held in this first stage of human life.
To inform the embryo any principle, whether it is the rational soul or a force derived from the parental organism, must have organs; and if organs are present, then the embryo is fit to receive the human soul, as the only objection to its presence is a supposed lack of organs. To use other principles when the human soul itself could be present would be a multiplicatio entium sine necessitate, which is a condition repugnant to the universal method of the Creator.
It has been said that the vital activity in the fertilized ovum does not proceed from the rational soul because, "in the first place, it results from the fusion of two vital activities, neither of which is rational; secondly, it results in the formation,[66] by fission, and differentiation, of two distinct and separate living cells, each containing within itself a principle of vital activity. Now this principle of vital activity cannot be a rational soul, for each cell has its own principle of activity, and in man there is but one soul."
In the first place, that vital activity does not result from the fusion of two vital activities neither of which is rational. It results after the nuclei come together, by particular creation, and replaces their activity—the generation of the last vital force is the corruption of the first that existed in the separate nuclei, not a derivative of that first force. Again, when the embryo is in the two, four, eight cell stage, and so on, there are not two, four, eight vital principles present, but one. Substantial unity is essential to life of any kind, no matter how low its grade; and if each cell had an independent vital principle, any form of resultant life in the mass would be impossible. An aggregation has no unity of substance; there would be as many substances or natures as there are individual beings in the aggregate, no matter whether ordered or in a mob, consequently no life at all as a life.
The embryo in the two-cell stage is not made up of two independent organisms, any more than the right and left halves of an adult man are two independent organisms. The cells in the two-cell stage of the embryo are the right and left halves of the body, not two individuals, as has been proved repeatedly by biologists. Roux[42] punctured with a hot needle one of the cells in the two-cell stage of a frog embryo without killing the embryo, and it grew into a half-frog larva. Analogous results were obtained by operating in the four-cell stage. Later, Pflüger, Schultze, Enders, and Morgan corroborated the work of Roux. Newport[43] discovered this fact sixty years ago.
In analyzing the structure and functions of the individual cell we regard it as an independent elementary organic unit, but this view is solely a matter of convenience, almost a convention. All the billions of cell's in an adult man are[67] inseparable parts of the single living person. No cell exists as an independent organism in multicellular animals, except the germ-cells, and these only after separation from the gland of origin. Indeed, the biological theory of heredity, already mentioned here, wherein the germ-cell is supposed to carry forward the entire heredity, is now changing toward the view which makes all the somatic cells influence the germ-cells; that is, the body-mass of cells sends on heredity through the germ-cell as the instrument. Adult organisms do not make cells de novo. New cells are formed by division from preëxisting cells, but some biologists think the body-cells so affect the new germ-cells as to influence heredity.
The cells are organs, nodal points, of a single formative power which pervades the mass of cells as a whole. The protoplasm of each cell is not only in direct apposition with its neighbors, but nearly all biologists are now inclining to the opinion, which Heitzmann proposed in 1873, that division of cell from cell is incomplete in nearly all forms of tissue; and that even where cell-walls are present (an exceptional condition in mammals) they are traversed by strands of protoplasm, by means of which the cells are in organic continuity. The whole body, he contended, is thus a syncytium (a mass of continuous protoplasm stippled with nuclei), with the cells as mere nodal points in an almost homogeneous protoplasmic mass. There are cell-bridges between the sieve-tubes of plants. In 1879 Tangl discovered such connection between the endosperm cells of plants, and later Gardiner, Kienitz-Gerloff, A. Meyer, and many others demonstrated that in nearly all plant tissues the cell-walls are connected by intracellular bridges. Ranvier, Bizzozero, Retzius, Fleming, Pfitzner, and many other observers have found these protoplasmic bridges in animal epithelium. In the skin of a larval salamander they are quite conspicuous. They are known to occur also in smooth muscle-fibre, in cartilage cells, in connective-tissue cells, and in some nerve-cells. Harrison found, in 1908, that in frogs the nerve-fibres develop out of these intracellular bridges. Dendy in 1888, Retzius in 1889, and Palladino in 1890 have shown that the follicle cells of the ovary[68] are connected by protoplasmic bridges, not only with one another, but also with the ovum; and similar connection between somatic cells and germ-cells has been found in a number of plants. Thus even the germ-cell is not independent until it has actually broken away from the gland. A. Meyer holds that both the plant and animal individual are continuous masses of protoplasm, in which the cytoplasmic substance forms a morphological unit, no matter what the cell is. That opinion is not finally settled as regards the animal after the fetal stage, but it is much stronger as regards embryos. In the early stages of many arthropods it is certain that the whole embryo is at first an unmistakable syncytium. This is almost established also for Amphioxus, the Echinoderm Volvox, and other animals. Adam Sedgwick holds that it is true for vertebrates up to a late embryonic stage. Mitosis, then, is a form of growth of a mass, not a generation of new individuals.
Whether chromatin or any other element in the germ-cell be the idioplasm in which heredity inheres, differentiation is a progressive transformation, through physical and chemical changes, of the substance of the ovum, and this transformation occurs in a definite order and a definite distribution in the ovum. The changes result in a cleavage of the egg into cells, the boundaries of which sharply mark the areas of differentiation. These cells take on specific characters. In the four-celled stage of an annelid egg these four cells contribute equally to the formation of the alimentary canal and the cephalic nervous system, but only one of them, the left-hand posterior cell, gives rise to the nervous system of the trunk and to the muscles, connective tissues, and germ-cells. The relation between the four original cells, or blastomeres, and the adult parts arising from them, is not fixed, because in some eggs these relations may be artificially changed. A portion of the egg which normally would develop into a fragment of the body will, if split off from the others, give rise to an entire body of a diminished size.
Conklin says[44] that in the ascidian Styela "there are four or five substances in the egg which differ in color, so that their[69] distribution to different regions of the egg and to different cleavage cells may be easily followed, and even photographed, while in the living condition. The peripheral layer of protoplasm is yellow and it gathers at the lower pole of the egg, where the sperm enters, forming a yellow cap. This yellow substance then moves, following the sperm nucleus, up to the equator of the egg on the posterior side, and there forms a yellow crescent extending around the posterior side of the egg. On the anterior side of the egg a gray crescent is formed in a somewhat similar manner, and at the lower pole between these two crescents is a slate-blue substance, while at the upper pole is an area of colorless protoplasm. The yellow crescent goes into cleavage cells which become muscle and mesoderm, the gray crescent into cells which become nervous system and notochord, the slate-blue substance into endoderm cells, and the colorless substance into ectoderm cells. Thus within a few minutes after the fertilization of the egg, and before or immediately after the first cleavage, the anterior and posterior, dorsal and ventral, right and left poles are clearly distinguishable, and the substances which will give rise to ectoderm, endoderm, mesoderm, muscles, notochord, and nervous system are plainly visible in their characteristic positions." Conklin followed these cells in every division until the embryo was developed, making a complete genealogy up to the ovum proper.
De Vries[45] assumed that the character of each cell is determined by "Pangens" that migrate from the nucleus into the protoplasm. Driesch and Oscar Hertwig held that the peculiar development of a given blastomere is a result of its relation to the remainder of the cell-mass, an outcome of the action upon it by the whole system of cells of which it is a part. Hertwig said:[46] "Each of the first two blastomeres contains the formative and differentiating forces not simply for the production of a half-body, but for the entire organism; the left blastomere develops into the left half of the body only because it is placed in relation to a right blastomere."[70] Wilson[47] and Driesch[48] came to the same conclusion about the time Hertwig wrote. Driesch said:[49] "The relative position of a blastomere in the whole determines in general what develops from it; if its position be changed it gives rise to something different; in other words, its prospective value is a function of its position."
A discussion of this matter will be found in Wilson,[50] but the many experiments made in the study of this subject show conclusively that the cells, singly, grouped, and in mass, are a morphological unit, not an aggregation of distinct individuals. They are not, of course, absolutely homogeneous, because such a body could not have organs. The substantial form, therefore, is not confined to the first cell.
The cell-mass, then, has a unity sufficient to be the receptacle of a human vital principle; again, the basic vital operation of the human body at any age is metabolism, and this is actually carried on in the first somatic cell of the embryo as in the cells of the adult man. In the development of the human body in the embryonal stage the energy of cell-division is most intense in the early cleavage stage, and this diminishes as the limit of growth approaches because further division is not needed. When that limit is attained a more or less definite equilibrium is established. Some of the cells in the fully formed body cease to divide, the nerve-cells, for example; others divide under special conditions, as the blood-cells, the connective-tissue cells, gland-cells, epithelial and muscle cells; others continue to divide throughout life and thus replace worn-out cells of the same tissue, as the Malpighian layer of the skin. Cells grow, divide, function, reproduce themselves, and so on, all through their vital activity, sustained by the material brought to them by the blood. Weismann[51] and other biologists think that the vital processes of the higher animals are accompanied by a renewal of the morphological[71] elements in most tissues. The material is carried to the fetus in the womb by various agents, but mostly by the maternal blood after the embryo uses up the yolk; and when the fetal circulation has been established the nutritive material is taken from the maternal blood into the fetal circulation through the placenta, and then carried to the cells by the fetal circulation itself. After the child has been born the stomach and intestines take in the food. The stomach does very little with it except in a preparatory manner; the intestines further prepare it, pass it into the body, where it is again modified by other organs, and finally it is carried by the blood to the cells. The cells really use it; the other organs are the farmers, grocers, railways, and the like; the cells are the consumers. So far as the essential processes are concerned, the embryological cells act as do the adult cells.
The first cell has contractility, protoplasmic motion; it can absorb perfectly all food-stuffs necessary for it from the deutoplasm of the ovum, and the water that passes in from without to the ovum. In a few days the embryonic cells have used up the deutoplasm and are taking up food from the maternal blood as perfectly as any adult cell does, and are exercising their function of building up and sustaining whatever part of the body they are destined for; and this with all the complicated metabolism of the adult cell. Cell metabolism is the fundamental, chief, organic act of any human body at any age. That the embryo does this impelled by the virtus formativa transmitted from the parents is a mere gratuitous assumption to fit the theory that the embryonic cell lacks organic power. The fundamental organ that conserves the body in its very existence under the government of the soul is the apparatus which effects metabolism. Incessant chemico-vital change is a characteristic of all living substances, from the single cell up to the adult man; and in all cases this activity has to do with a transformation of the complex molecules which build up the protoplasm or are associated with its operations. The totality of the chemical changes, or exchanges, in living cells, the transformation of unorganized food materials so that these may be assimilated, and the chemical processes[72] in the tissues themselves, all are metabolism. Growth and repair (anabolism) occur side by side with the destruction of elementary tissue substance (katabolism), and the duration of life rests on these processes; and all are mere cell activities. Food-stuffs (water, inorganic salts, proteids, albuminoids, carbohydrates, and fats) undergo more or less combustion or oxidation. Oxygen unites with carbon to form carbon dioxide, and with hydrogen to form water; the nitrogen of the highly complex proteid substances reappears in combination with carbon, hydrogen, and oxygen as urea, uric acid, and other compounds; and other ingesta are thus transformed through oxidation. All maintain the temperature of the body, replace outworn parts, and accomplish the body's work. Oxidation occurs to a slight extent in the blood, but the specific reactions are intracellular. Even when nothing exists but the cells and the blood, as in the beginning embryo, the cells really do the work, and they do the work as they do in the adult.
The cells also from the very beginning are the organs that make the animal heat necessary for life. Rubner[52] proved that the source of at least 90 per cent. of the animal heat in the body is a result of the chemical changes—oxidation—in the food ingested: the other 10 per cent. is caused by muscular contractions, the flow of blood, the friction of joints, and like motions. This oxidation is more active in young animals than in adults, and in each it is, of course, a cellular process.
Living matter contains hydrogen, oxygen, sulphur, chlorine, iodine, fluorine, nitrogen, phosphorus, carbon, silicon, potassium, sodium, calcium, magnesium, and iron. The removal of one of these elements causes the death of the body. They must be arranged in a definite, prescribed order to constitute cellular protoplasm, and any disarrangement of this order causes intoxication, disease, or death. Hydrogen is a constant product in the putrefaction of animal matter, of animal food, and is present in the intestinal tract. Oxygen is found dissolved in water and loosely combined in blood as oxyhemoglobin. All the elements, except fluorine, combine with oxygen, forming oxides, and the process is called oxidation. The production[73] of heat and all vital motion depend on oxidation, decomposition of matter. In the nuclei of cells there is a so-called "oxygen-carrier," a nucleo-proteid, which contains iron, and this appears to be the chief oxidizing agent in the body. Chlorine, which in hydrochloric acid is essential to digestion, is ingested as chloride, and leaves the body chiefly through the urine and sweat. Iodine is a necessary part of the thyroid gland, an indispensable vital organ. Fluorine is found in all cells. Nitrogen goes into the body combined in proteids; and phosphorus, combined in the alkalies and alkaline earths of the foods. Carbon occurs in all cells and leaves them through the lungs as carbon dioxide.
The amount of energy set in action in the body in the decomposition of any food is equal to the energy that had been expended in the synthesis of that food from its organic elements, and the liberated energy set free in the body appears as heat, work, and nervous impulse. In a plant the chlorophyl and the sun's rays combine water and the carbon dioxide of the air into sugar and free oxygen. This sugar is changed in a plant into starch, cellulose, and fat, and also, when combined with some nitrogen, into proteid. An animal eats this plant, which contains starch, cellulose, fat, and proteid, and it either adds these ingredients to its own substance or oxidizes them so as to prevent the destruction of its own substance. These are the ends of all food. Broadly speaking, plants synthesize elements; animals analyze them, reduce them into simpler bodies.
Such processes, and those of the other elements of the body, which have to do with the changing constituents of the human organism, are all cellular processes—metabolism. Hence the chief organic act of the body is metabolic; the basic organ of man is the cell. Arms, legs, heart, brain, stomach, and similar organs are secondary, though some of the latter are essential for certain operations. Now, one cell is an organ amply sufficient for metabolism, for the chief organic act of the body; hence it is a fitting receptacle for a substantial form, a soul. Therefore there is no reason why the soul may not be present in the one-cell stage of the embryo; and since there is no reason[74] why it should not be present, but many why it should, it is present.
Conklin says:[53] "The fertilized egg of a star-fish, or frog, or man is not a different individual from the adult form into which it develops, rather it is a star-fish, a frog, or a human being in the one-celled stage. This fertilized egg fuses with no other cells, it takes into itself no living substance, but manufactures its own protoplasm from food substances; it receives food and oxygen from without and it gives out carbonic acid and other waste products; it is sensitive to certain alterations in the environment, such as thermal, chemical, and electrical changes—it is, in short, a distinct living thing, an individuality. Under proper environmental conditions this fertilized egg-cell develops, step by step, without the addition of anything from the outside except food, water, oxygen, and such other raw materials as are necessary to the life of any adult animal, into the immensely complex body of a star-fish, a frog, or a man. At the same time, from the relatively simple reactions and activities of the fertilized egg there develop, step by step, without the addition of anything from without except raw materials and environmental stimuli, the multifarious activities, reactions, instincts, habits, and intelligence of the mature animal."
An objection to the opinion that the soul is in the embryo from the beginning is made from a consideration of the facts that there appears to be an aptitude for life in certain animal cells and tissues after removal from the original host, or after the death of the host; and, secondly, that in other separated tissues life is undoubtedly made evident under proper conditions. Some parts of the human body can be grafted upon another human body, and human sarcomatous cells have been made to grow in vitro. Hair often lengthens after the death of a person, if no embalming fluid has been injected. Dr. Alexis Carrel[54] substituted a piece of a popliteal artery, taken from an amputated human leg and kept in cold storage for[75] twenty-four days, for a part of the aorta of a small bitch, and the dog lived for four years afterward and died in parturition. Magitot of Paris, in 1911, took a piece of the cornea from an extirpated human eye, and with it replaced a part of an opaque cornea on another man, and this second man could see through the new cornea. Surgeons now remove skin, bone, and other tissues from still-born infants and accident cases, preserve these, for weeks if necessary, in petrolate and Ringer's solution in cold storage, and then graft them on patients to repair lesions in skin, bone, cartilage, or other parts of the body.
If these separated tissues are alive, what is the origin and nature of the life? Again, if there is a low form of life in these separated tissues, remaining after the departure of the human soul, why could not such a low form of life precede in the embryo the advent of the human soul?
What is the nature of the "life" in the parasitic sarcomatous tissue which has been seen to proliferate for a short time in vitro? We do not know, nor is it relevant to the question. That there is life of any kind in the cold-storage graft of bone and skin is certainly not evident; rather every evidence points to the absence of all life. When taken out of cold storage, and the ordinary forces which corrupt a dead body are permitted to work, these grafts corrupt exactly as any part of a corpse does. That there is life of any kind in these grafts is a gratuitous assumption. In cold storage they are kept ready for assimilation into the body as food may be kept. Bone and skin grafting is merely a peculiar form of assimilation. Food taken into the body through the stomach and entrails is prepared in the body and assimilated into the substance of the bones or skin or other tissues; the graft is ready for assimilation without this preparation because it is already bone or skin.
The vital principle in a man, or in anything else, is at the end, when it normally issues, of the same nature as it was in the beginning. If it is at perfection a substantial primary form, it always was such—a substantial form cannot issue from an accidental form. If the substantial form is the form of the cells in the completed organism, it was such before that[76] organism was perfected, unless it replaced a lower substantial form; but there is, we repeat, absolutely no need for such a secondary form at the beginning. If the cells of the embryo (not the infused germ-cells, which are not the embryo) had a forma corporeitatis, or cellularis, or whatever you wish to call it, the human soul when it did come would not confer primal existence, would not be a forma substantialis, but an accidental form. "In proof of which," says St. Thomas,[55] "we must consider that a substantial form differs from an accidental form in this, that an accidental form does not give being simply, but such or such being; as heat does not give being simply, but heated being. So when an accidental form comes in, a thing is not said to come into existence or to be generated, simply, but to become such or such an object, or to find itself in such or such a condition. So, also, when an accidental form disappears, a thing is not said to be destroyed simply, but only to a certain degree. A substantial form, however, gives being simply; and therefore by its advent a thing is said to be generated simply, and by its recession to be destroyed simply. If, therefore, it happened that any substantial form other than the intellectual soul preëxisted in matter, by which the subject of that soul would come into actual being, it would follow that the soul would not confer being simply, and therefore would not be a substantial form; also that the coming of the soul would not be a generation simply, but only secundum quid—all of which is evidently false." Again, St. Thomas says:[56] "Some tell us the vital acts that appear in the embryo are not from the soul, but from the soul of the mother, or from the primitive force in the semen. Both these statements are false."
An application of the opinion offered here—that is, that the human soul is infused at the instant of conception—to multiple and monstrous embryos offers no real difficulty. There are two kinds of human twins—those from two distinct ova and those from one ovum. Two ova may come from one or different ovaries, or even from one Graafian follicle, be fertilized[77] at the same time and develop synchronously. If the ova are placed at some distance apart in the uterus, two placentas appear; if the ova are near each other the placentas may fuse, but their circulations do not. Each child will have its own fetal envelope.
In twins from two distinct ova there is no difficulty in seeing that the souls are placed in these in the same manner as the soul is put in the normal single embryo. When the twins come from one ovum the condition is not so simple. The oval nucleus is the essential part that goes from the maternal side, and human ova at times contain two nuclei, as occasionally hens' eggs do; a double-yoked hen's egg has two nuclei, and two nuclei have been found in a single yolk. Kölliker, Stöckel, and von Franque have observed double germinal vesicles in single human ova. In such a condition two spermatozoa could fecundate the two nuclei and the development go on as in the case of twins from distinct ova.
There is a theory which holds that homologous twins (uni-oval) can develop from a single germinal vesicle which splits into two primitive streaks and two gastrulas. According to this opinion, if the germinal vesicle divide entirely, two fetuses develop which are always of the same sex, and which resemble each other so closely in appearance that it is very difficult to differentiate them. This theory holds also that should the germinal vesicle not split fully, the lack of fission causes the various kinds of double monsters. The germinal vesicle that supposedly splits into two is not fecundated by two spermatozoa, they say, because where there is only one nucleus in the beginning, the entrance of a second spermatozoön commonly kills the ovum. This last assertion has been disproved of late.
Some followers of the splitting theory hold that double monsters arise from the union of two originally separate primitive traces (Verwachsungstheorie). Others say that a single primitive trace of blastoderm cleaves more or less thoroughly and makes the double monster (Spaltungstheorie). The earliest human double monster (Ahlfeld's case) was in the fourth week of gestation; therefore whatever is held in these theories[78] as regards human monsters is only through analogy with lower animals.
Gerlach[57] saw bifurcation at the cephalic end of a chicken embryo sixteen hours old. In this case the first change was a broadening of the anterior end of the primitive streak; next a forked divergence appeared, and by the twenty-sixth hour the bifurcation was half as long as the undivided posterior part. Whether this was a case of two nuclei or not is not known.
What seems to make for the fission theory is that in non-parasitic double terata, no matter how unequally nourished or how variable in extent, the union between the halves of double monsters is symmetric, and the same part of each twin is joined. This fact is used as a reason to exclude a fortuitous growing together of dissimilar areas of cell-masses, at least in non-parasitic cases. Born,[58a] in a study of fish ova, found that eggs which produce double monsters begin with a segmentation like that of the simple normal ovum. Composite spermatozoa have been observed with two and three heads and one body and tail-piece, but the significance of these abnormal cells is not known.
Embryos of sea-urchins in the two-cell and four-cell stages can be separated by shaking into isolated blastomeres, and the segments will grow into full though dwarfed larvae. The same division with the growth of dwarfed larvae has been made in Amphioxus, in the teleost Fundulus, in Triton, in a number of Hydromedusae and several other low forms of life. When the division is not made completely double monsters result.
Up to a certain stage of development the blastomeres of the Medusa embryo are totipotent, or capable of developing into any part of the body. The limitation of development in a particular case lies in the cytoplasm rather than in the nuclei of the cells. If frogs' eggs are fastened in abnormal positions, inverted or on the side, a rearrangement of the egg material results, wherein the nucleus and cytoplasm rise and the deutoplasm sinks. This change of axis shifts the embryo.[79] If an egg is turned upside down in the two-cell stage, a whole embryo, or half a double embryo, may arise from each of the two blastomeres, instead of a normal half-embryo. A half-embryo or a whole dwarf may arise according to the artificial position of the blastomere. Each of the two blastomeres contains all the materials potentially for the formation of the whole body, and these materials build up a whole body or a half body according to the grouping they take on. Primarily the egg cytoplasm, in low forms of animal life, is totipotent; it has no fixed relation with the parts to which it gives rise, and may be artificially modified or differentiated. These effects, from position and traumatic dislocation, suggest explanations for teratic forms in higher animals.
Human terata are now commonly classified in four groups: (1) Hemiteratic; (2) Heterotaxic; (3) Hermaphroditic; and (4) Monstrous. Hemiterata are giants, dwarfs, persons showing anomalies in shape, color, closure of embryonal clefts, in absence or excess of digits, or like defects. The Heterotaxic group are persons whose left or right organs are reversed in position. A true Hermaphrodite would have the complete reproductive organs of both sexes, but such an individual has not been observed. There is never any question of double personality in hermaphrodites.
Terata more properly so called may be single, double, or triple; and single monsters may be autositic or independent of another fetus, or they may be omphalositic, dependent upon another which is commonly well developed and which supplies blood for both through the umbilical vessels. There are four genera of autositic single monsters, with eight species and thirty-four varieties. Of the monstra per defectum the commonest are caused by a failure of closure in the embryonal medullary canal, which leaves part of the brain and spinal cord or their bony covering lacking. Some terata, as the Acephalia, have no brain or spinal cord, but they die in the fetal stage. The Anencephalia may have a spinal cord, a medulla oblongata, and parts of the basal ganglia, but the cerebral hemispheres are wanting. Such monsters are sometimes born at [80] term and live for several days: they cry, suckle, show some reflexes and a sense of pain, and move the arms and legs.
I described the various kinds of terata in Essays in Pastoral medicine,[58b] and of these the most important in the matter under discussion here are the double and triple monsters. Many of the double monsters evidently were two persons. There is only one well authenticated case of a triple human monster, and this happened in Italy in 1831. It had a single broad body with three distinct heads and two necks, and was killed in delivery. There is no proof as to whether it was one or more persons. The standard of judgment in such cases as regards the presence of one or two souls in the monster is the evidence of one or more distinct consciousnesses. A monster double from the navel or breast downward (terata anadidyma) is, I think, one person. There was an example of a monster in this group which was divided from the foreheads downward; or better, the distinct twins were united by their foreheads only; but such a form is very exceptional. In my article on "Human Terata and the Sacraments," in Essays in Pastoral Medicine, in 1906, I expressed the opinion that a monster which is single to the navel and double below is composed of two persons, but I now am of the opinion that such a monster is only one person, because there is apparently only one consciousness. There are about eight cases of two-headed monsters known which were evidently two persons in each case, and several terata kata-anadidyma, divided above and below but joined at the sternum, abdomen or sacrum. Several ischiopagic twins, joined at the pelvis with the heads at the opposite ends of the double body, are grouped with either the katadidyma or kata-anadidyma. It is commonly not difficult to recognize individuality or duality of personality in monsters, but it is not easy to explain the origin of life, to point out the moment the second soul enters these fused or undivided twins.
We can artificially obtain double embryos of frogs by inverting the blastomeres in the two-cell stage.[58c] We thus get [81]united twins with heads turned in opposite directions, twins united back to back like the Blazek Sisters, twins united by their ventral sides, and double-headed tadpoles, but we have no knowledge of how similar doubling in human monsters takes place; we must guess vaguely from analogy. There was one soul, at least, present from the one-cell stage of the human monster; when the second soul is created and infused we do not know, but the moment of the creation of this second soul has no practical significance in this discussion.
The presence of certain kinds of monsters in the uterus can be diagnosed before labor, but double monsters are mistaken for ordinary twins. A woman who has given birth to a monster is likely to have subsequent monstrous fetuses. Where the intrauterine existence of a single monster is suspected the X-ray will at times clear up the diagnosis. Women gravid with monsters commonly abort early in pregnancy, but even united twins may go on to term. Those monsters that offer an obstacle to delivery by the abnormal bulk of one or the other end are mostly twins joined above or below the navel; those joined at the middle are easier of delivery. Monsters that are joined at the pelves are commonly in a straight line, and may not be difficult to deliver. Most double monsters cannot be delivered alive except by cesarean section, and the fact that the content of the uterus is monstrous is, as a rule, not diagnosed until it is impossible to attempt cesarean section without killing the mother through infection. In such a condition the double monster would, in the ordinary medical practice, be delivered by craniotomy, exenteration, cleidotomy, or the like operation.
The Rituale Romanum Pauli V[59] gives the following directions for the baptizing of human terata:
"18. In monstris vero baptizandis, si casus eveniat, magna cautio, adhibenda est, de quo si opus fuerit, ordinarius loci, vel alii periti consulantur, nisi mortis periculum immineat.
"19. Monstrum, quod humanam speciem non praeseferat baptizari non debet; de quo si dubium fuerit, baptizatur sub hac conditione; Si tu es homo ego te baptizo, etc.
"20. Illud vero, de quo dubium est, una ne, aut plures sint personae non baptizetur, donee id discernatur: discerni autem potest si habeat unum vel plura capita, unum vel plura pectora; tune enim totidem erunt corda et animae, hominesque distincti, et eo casu singuli seorsim sunt baptizandi, unicuique dicendo: Ego te baptizo, etc. Si vero periculum mortis immineat, tempusque non suppetat, ut singuli separatim baptizentur, poterit minister singulorum capitibus aquam infundens omnes simul baptizari, dicendo: Ego vos baptizo in nomine Patris, et Filii, et Spiritus Sancti. Quam tamen formam in iis solum, et in aliis similibus mortis periculis, ad plures simul baptizandos, et ubi tempus non patitur, ut singuli separatim baptizentur, aliis nunquam, licet adhibere.
"21. Quando vero non est certum in monstro duas esse personas, ut quia duo capita et duo pectora non habet distincta; tune debet primus unus absolute baptizari, et postea alter sub conditione, hoc modo: Si non es baptizatus, ego te baptizo in nomine Patris, et Filii, et Spiritus Sancti."
Any kind of monster coming from the human womb, if it is only a head and lacks a body (Acardiacus Acormus), or is a body and lacks a head and heart (Acardiacus Acephalus), or is a Foetus Anideus, which is a shapeless mass of flesh covered with skin, should be baptized, provided it shows signs of life. Number 19 in the Ritual would be liable to an interpretation which is too narrow if it were not that very monstrous fetuses, which appear to a lay observer to be not human, are as a rule delivered dead. Here it may be worth while to mention that a hybrid between a human being and a lower animal is impossible. As to number 20, the rule for differentiating unity or duality of personality is not the number of heads, but the number of evident consciousnesses, and this differentiation commonly cannot be made at birth. There have been examples of two-headed monsters delivered alive, which were single as to soul because the consciousness evidently was one.
The moment human life begins in the human fetus is a subject of dispute, but the moment human life ends is a mystery—we have no method of determining exactly just when the soul leaves the body. Daily throughout the world the priest reaches a patient who has just died. Conditional absolution, extreme unction, baptism might have been administered if there were signs of life, but the heart and lungs are still, "the patient is dead," and the priest leaves without doing anything. Yet it is always probable that the patient does not die at once even in a case of decapitation.
Bichat, at the beginning of the last century, called the brain, lungs, and heart "the tripod of life," and from time immemorial we have based our judgment of the presence of somatic death on the lack of consciousness, respiration, and circulation in the patient. The heart, however, beats after consciousness and respiration cease (and sometimes respiration continues after the pulse cannot be felt), and this cardiac activity may go on for more than a half hour after all the normal clinical signs of death have appeared—after respiration has quit, when no heart-sounds can be heard by the stethoscope and muscular relaxation indicates death.
The stimulus of the heart-beat probably starts at the juncture of the superior vena cava with the right auricle of the heart. Some biologists think that in this spot life takes its last stand before the final retreat, but that fact is disputed of late. In the hospital of the Rockefeller Institute for Medical Research in New York, Dr. G. Canby Robinson[60] made records[84] from about eight patients before and during the actual stopping of the heart, using the electrocardiograph, which can be employed without disturbing the patient. He thus found—only in one case, however—that the heart may beat for a half hour after all vascular and circulatory sounds have ceased to be audible. In a letter to me Dr. Robinson said: "Undoubtedly the heart continues to show activity sufficient to be recorded by the string galvanometer very frequently after respiration has ceased, both in man and the lower animals; but this does not necessarily mean that it continues to be an efficient pump, maintaining the circulation. Undoubtedly also in other instances the cardiac activity ceases before the respiration, but I have never obtained electrocardiographic records of such cases."
Crile's experiments upon dogs show that it is possible to resuscitate these animals after they have been apparently dead for periods of time up to seven and a half minutes. The cessation of the blood circulation causes degenerations in the nerve cells and fibres, and these lesions may last even if the animal has been resuscitated. Crile thinks the human respiratory centre may survive anemia from thirty to fifty minutes; the vasomotor and cardiac centres, about twenty to thirty minutes; the spinal cord, eight to ten minutes; the motor cortex, eight to ten minutes; the portion of the brain used in conscious activity as such, six to seven minutes. The higher neurons have been stimulated into reflex activity twenty-five minutes after complete clinical cardiac cessation of activity.
In any attempt to resuscitate a person apparently dead the maintenance of the blood circulation is the chief end. If, however, the blood is not oxygenated the circulation will not go on automatically. Artificial respiration is used, and the active principle of the adrenal gland is injected to stimulate the heart. If the heart has stopped in diastole,—that is, when distended with blood,—this distention must be relieved by cardiac massage, commonly through an opening in the thoracic wall. Intratracheal insufflation of oxygen is also to be employed, as a rule.
In Essays in Pastoral Medicine[61] I mentioned several cases of resuscitation after what had appeared to be certain death. Two of these had been "dead" for forty-five minutes before they were revived temporarily. Wayne Babcock[62] reported a number of new cases of his own. One was a resuscitation which lasted for forty-three hours, and which was begun twenty-five minutes after respiration had ceased. The patient was a very fat negress who had collapsed after the use of scopolamine. A man whose arm had been torn off died from shock in the operating-room. After fifteen minutes of artificial respiration the circulation started again, and he was kept alive for six hours in this manner, but he died as soon as the artificial respiration was discontinued. An exactly similar case was kept alive for seven hours by artificial respiration. One of Babcock's cases was a woman of eighty-seven years of age, who apparently died on the table during an operation for strangulated hernia. After ten minutes of cardiac and respiratory cessation she was revived. She died four days later of peritonitis. A man fifty-six years of age undergoing the same operation ceased breathing and his heart stopped. He was completely revived and cured.
Father Juan Ferreres[63] holds that aborted and newly born children should be baptized, although they give no sign of life, if they show no clear evidence of putrefaction. This opinion is mine also, but the word maceration should be substituted as more exact. Eschbach[64] says: "Infantes recenter natos et in vitae discrimine positos, aut foetus abortivos plane formatos, cum vel levissimus in eis motus apprehenditur, absolute baptizari oportet: cum autem sine motu et sensu iidem videantur neque tamen adhuc corrupti aut putrefacti sint, sine mora baptizentur conditionate: Si vivis, ego te baptizo, etc." These quotations give the common opinion of moralists at present, and this opinion is fully safe. Eschbach, however, would have the fetus "plane formatus," which is erroneous and an echo of the old Aristotelian notion. If the fetus is visible at all,[86] open the membranes and baptize it conditionally, even if it is not as big as a pea.
An infant born apparently dead may be resuscitated after a delay very much longer than would be possible in an older person, provided always the infant has not begun to breathe.
Ferreres mistakes cases of catalepsy which have recovered consciousness for cases of apparent somatic death. In these cataleptic conditions the blood circulation does not completely cease—if it did the nervous centres would be disintegrated. The case he reports on p. 26,[65] of the woman resuscitated by Rigaudeaux in 1748, was one of catalepsy, if it ever happened. The same is true of the case from Gaspar de los Reyes,[66] which probably had some foundation in a condition of catalepsy, but which more probably is a sheer invention by Reyes. It looks like an anecdote from a medieval Florentine novella.
Old writers speak of cessation of the pulse for long periods. Ballonius[67] mentions a person in whom there was no pulse for fourteen days before death; Ramazzini[68] describes a cessation of the pulse for four days before dissolution; Schenck[69] tells of a disappearance of the pulse for three days, with recovery. These all were apparently cataleptic cases, where the circulation was very feeble and the radial pulse was not palpable. Cheyne gives an account of a Colonel Townsend who had the power of apparently dying at will. He could so suspend the heart action that no pulse could be felt, and after a short while the circulation would become normal again. The longest period in which he remained in this condition was about thirty minutes. St. Augustine mentions a priest named Rutilutus who had a power like that of Colonel Townsend, and Caillé[70] reported a similar case.
The fakirs of India carry this power to great lengths. Braid,[71] on the authority of a Sir Claude Wade, says a fakir was buried unconscious at Lahore in 1837, and the grave was[87] guarded day and night by sentinels from an English regiment. Six weeks after the burial the man was dug up and he presented all the appearance of a corpse. The legs and arms were shrunken and stiff, and the head reclined on the shoulder, as happens in corpses. There was no perceptible circulation anywhere, yet he revived.
Honigberger, a German physician in the service of Runjeet Singh, described[72] a fakir of the Punjaub who was put into a sealed vault for forty days, and the seal of Runjeet Singh was on the coffin. Grain was sown above the vault and it was well above the ground when the man was taken out of the vault and resuscitated. Sir Henry Lawrence testified to the truth of this story. The fakir's chin was shaved, Honigberger says, before the burial, and the beard did not grow while he was in the vault.
In keeping with these stories are many curious accounts of recovery after hanging. These are frequent in writings of the sixteenth and seventeenth centuries, when hanging was almost an every-day occurrence. These narratives are much more authentic than the anecdotes told of recovery after premature burial, which are as old as literature. Paul Zacchias[73] tells of a young man who died of the plague and was set out with the corpses for burial. He revived and was taken back to the pest-house. He "died" again and was again prepared for the grave, but he came to a second time. The stock story in these premature burial cases is that of the woman who is revived by a thief who cuts her finger in an effort to steal the rings buried with her.
The important fact, however, is that in any case of death the exact moment in which the soul leaves the body is not knowable by any means we have at present, and where there is question of giving the sacraments the person apparently dead should have the benefit of the doubt. He is to receive conditional baptism, absolution, or extreme unction (preferably by the short method), in case these sacraments are required. For a whole hour after apparent death the probability that the[88] soul has not departed is so strong that, in my opinion, a priest who does not give the necessary sacraments is virtually as guilty as if he neglected to administer them to a person evidently alive. Crile, one of the best medical authorities on this matter of somatic death, holds that the human respiratory system may survive anemia for from thirty to fifty minutes. How long after the hour a priest may administer the sacraments is not known, but a second hour, or even a third, are not unreasonable periods of time during which the sacraments may be administered conditionally. The sacraments are for man, and there is no irreverence if they are administered conditionally and the priest explains to the bystanders the reason he has for his action.
If a pregnant woman dies slowly, the fetus in her womb is likely to die owing to lack of oxygen; if she dies suddenly, the child may live for variable periods in various cases. Brotherton reported a case where a living child was taken from a woman twenty-three minutes after the death of the mother. Tarnier, the noted French obstetrician, told of a remarkable incident which happened in Paris during the rioting by the Commune after the war of 1870. The rioters fired on a maternity hospital, and a pregnant woman sitting on a bed in a ward was instantly killed by a bullet through her head. After a while she was discovered dead, and Tarnier was sent for to save the fetus, as its heart-sounds could be heard through the abdominal wall. When he began the operation the hospital was fired upon again, and it was necessary to carry the corpse to the cellar of the building. There Tarnier, an hour and three quarters at least after the death of the women, extracted a living child from the corpse. Hirst[74] tells of another case which was narrated to him by an American naval surgeon who saw it in the harbor of Rio Janeiro during the revolution at the beginning of the present republic of Brazil. A woman near term was killed instantly by a piece of shell. As soon as she fell to the ground a Brazilian surgeon, who was standing near by, cut open her abdomen with a penknife and drew out the child, but it was already dead.
Mack[75] was called to a pregnant woman, and he found she had died suddenly about five minutes before he arrived. He at once opened the uterus with a small lancet and extracted a child which was beyond the livid stage and had no heart-sound. He worked on the child for forty minutes, using the ordinary methods for reviving asphyxiated children, but got no sign of life. Then he injected a hypodermic syringeful of a 1:1000 epinephrin solution through the umbilical cord into the abdomen and continued the reviving motions. In ten minutes the child was crying vigorously, and it was a healthy baby afterward.
Gunn and Martin,[76] in experiments on rabbits poisoned by chloroform and apparently dead, found they could resuscitate about 70 per cent. of the animals if treatment was begun within ten minutes after the heart ceased beating. They started artificial respiration through a tube in the trachea, then injected epinephrin into the pericardium, and afterward massaged the heart through an opening in the abdomen. The rate of compression of the heart in this massage must be somewhat less than half that of the normal beat, and at short intervals the massage is to be stopped to allow the spontaneous beats to develop. Compression should be gradual and the relaxation abrupt. The massage is applied by one of these four methods, and they are arranged here in the order of their efficiency: (1) by direct compression of the heart through an opening in the thorax; (2) by compression above the diaphragm through an opening in the belly-wall; (3) by simple compression of the abdomen; (4) by simple compression of the thorax. Epinephrin, or pituitary extract, is used as an adjuvant intravenously to increase the cardiac movement after it has been started. The same methods will probably be effective in man, and have been used successfully.
When a woman is in articulo mortis with a living fetus in her womb, one should not wait for her death. If one waits, he[90] will nearly always lose the child. The cervix should be dilated forcibly, the child turned and delivered. Even if this forcible delivery should happen to hasten somewhat the mother's death, the action would be morally licit. It would be a double-effect action; the two effects would proceed immediately and equally from the act, which is indifferent morally; one effect, the good one, is to save the child for baptism at least, and possibly permanently; the second, evil but reluctantly permitted, is the possible hastening of the maternal death. I should be willing even to slit the cervix, if necessary, provided the diagnosis were certain, with the possibility of tearing the uterus, in a case where the dilatation of the cervix would be too slow a method; but this supposition is scarcely practical.
Zsako[77] gives a method for determining the interval since death by muscular phenomena. Tapping with a percussion hammer on certain muscles of the body excites a reflex contraction up to from an hour and a half to two hours after death. The contraction may be elicited in the same manner on the living, but it is more evident on a cadaver owing to the absence of antagonistic tonus in the muscles. Some muscles may move for four hours after death. Tapping along the radius from the elbow downward, he says, a point is found where the stroke causes extension of the hand; tapping along the radius above the wrist makes the thumb bend; tapping on the spaces between the bones of the hand closes up the corresponding fingers; tapping on the back of the foot extends the toes, on the leg adducts the foot, on the tibia along the middle third extends the leg. When the lower third of the thigh is tapped across the muscles move, and if the back is struck between the scapula and the spine the shoulder blades move toward each other. If there is no response the person must be dead from two to four hours. I have had no experience with this method.
Satre[78] reported that many soldiers brought into the dressing-stations apparently dead from shock, head or spinal wounds, or gas asphyxiation, were revived after artificial respiration[91] had been applied, sometimes for even six hours before results were obtained. Two tests were used to find out whether the patient was alive or not. In such cases ten c.c. of a 20 per cent. alkaline solution of fluorescine is injected subcutaneously, and if there is any circulation this dye will be carried to the eye and turn the conjunctiva green. The second test is to push a fine puncture-needle into the spleen or liver and thus remove a particle of the pulp. This pulp is put on blue litmus-paper and drawn free from blood. If the litmus-paper turns red the man is dead; if it remains blue he is alive. The reaction of the living pulp is alkaline, blue; this becomes acid, red, a half-hour after death; an hour after death the acid reaction is quite marked.
Abortion, as the term is used by physicians, in its widest sense is the ejection or extraction of a fetus from the womb at any time before term. The word is popularly contrasted with miscarriage, where the fetus is ejected through disease or accident; abortion in the lay sense supposes artificial, and commonly criminal, extraction of the fetus. Abortion (from aboriri, to perish) etymologically has an association with destruction of life, but the name is given by physicians to a removal of any premature fetus, even if it is viable. Strictly, however, abortion is an interruption of pregnancy before the fetus is viable, and premature labor is such an interruption after the fetus is viable. Throughout this chapter the words are used in this sense.
Abortion as a medical and moral consideration may be considered from several points of view.
First, involuntary pathologic and accidental interruptions of pregnancy are to be averted, if it is possible to do so, to save the life of the child; and when the abortion is inevitable the treatment has moral qualities which involve the physician and the mother.
Secondly, voluntary and therapeutic abortion has peculiar moral and medical qualities arising (a) from the period of gestation or the viability of the child; (b) from the truth or error in the diagnosis as regards the necessity for interference, and the advantage or damage resulting from the interference.
Thirdly, the technical skill or ignorance of the physician, and the methods he employs may in themselves in any case avert or cause the death of the mother or grave injury to her, and in the forced delivery of premature infants may save, kill, or maim the child.
Fourthly, voluntary criminal abortion has a special malice of its own, which makes it somewhat more criminal than the therapeutic removal of an inviable infant.
Fifthly, there are positive canonical and civil penalties against abortion as it affects the inviable infant.
Pathologic abortions, and those arising from accident or carelessness, are extremely common. Hegar estimated that there is one of these abortions to every eight normal parturitions, and specialists in obstetrics find as many as one abortion to four deliveries at term. These abortions are most frequent from the eighth to the twelfth week of gestation, because the ovum is then not firmly attached to the uterus, and it readily succumbs to external influence. Moreover, the woman is not certain she is pregnant and neglects precautions. Many women, again, are under the error that there is no moral evil in getting rid of the ovum before quickening, and they think quickening occurs only when they feel the fetal movements. Others, erroneously again, fancy that abortion in the early months is not dangerous or injurious to themselves.
The causes of pathologic and accidental abortion are very numerous and often interactive. They may arise from the fetus, the mother, the father, or from violence. The death of the fetus, or diseases of the fetus itself or of its appendages, cause abortion. Weakness of the fetus from alcoholism in the parents, anemia, carbon monoxide and lead poisoning, tobacco poisoning in women who are cigar-makers, and similar conditions in one or both parents, will bring on abortion. Monsters rarely go on to term. Acute or chronic affections in the mother, as typhoid, malaria, smallpox, cholera, scarlatina, measles, tuberculosis, and the like, and syphilis in the mother or father, effect abortion. Other abnormal states that bring on abortion are low blood-pressure in maternal anemia, shock, syncope; hemorrhages into the placenta in maternal nephritis; hemorrhages between the placenta and uterus from diseases of the placenta and decidua, or from traumatism, which detach the placenta; sun or heat stroke; sudden high temperature in fever; toxemias, as in some forms of hyperemesis[94] gravidarum, eclampsia, chorea, hepatic autolysis, and impetigo herpetiformis.
Chronic endometritis, or inflammation of the lining membrane of the uterine cavity, is the commonest maternal cause of abortion, especially of habitual abortion. In this condition hemorrhages in the decidua, or uterine fold that holds the fetus, kill the fetus, or force the ovum off the uterine wall, or excite expulsive uterine contractions. Without hemorrhage endometritis prevents a firm fixation of the ovum, or it may bring about a malposition of the placenta, called placenta praevia. Endometritis at the decidua may cause hydrorrhoea gravidarum, and the accumulated serous secretions from this source are likely to start uterine contraction. Chronic metritis, or inflammation of the deeper tissues of the uterus, is commonly found with endometritis, and it prevents the expansion of the uterine muscle. This condition is more likely to cause abortion than endometritis alone.
Acute gonorrhea, inflammations of the Fallopian tubes, and appendicitis sometimes interrupt pregnancy. Other causes are malformations and diseases of the uterus, infantilism, fibroids, polyps, uterine horns, lacerations and amputation of the cervix, and retroversions and retroflexions of the uterus. At times a replacement of the uterus will avert an abortion.
When the mother has an infectious disease like typhoid, smallpox, cholera, or typhus, the infection may reach the fetus and kill it, or may cause an endometritis with a hemorrhagic tendency. Maternal sepsis may kill the fetus directly or secondarily, and this is true also of maternal syphilis. A sudden rise in temperature may excite expulsive uterine contraction. In pneumonia the excess of carbon dioxide in the blood may bring on abortion. Like pneumonia, anesthesia may kill the fetus if kept up for a long time, or if marked by cyanosis. Prolonged nitrous-oxide anesthesia is especially dangerous to a fetus, but a brief nitrous-oxide anesthesia for the extraction of a tooth may not bring on abortion. The worst tooth stump can be extracted painlessly after local injection of novocain, with no danger to the fetus. The gums remain somewhat sore for a day or two after novocain infiltration, but this[95] inconvenience is a much less evil than total anesthesia, even when there is no pregnancy. It is probable that total anesthesia is morally unjustifiable for the extraction of a single tooth if the tooth is not wedged in.
Violence, accidental or intentional, is a frequent primary or secondary cause of abortion. Sometimes a slight jar, a misstep on a stairway, a nervous shock, a jump from a carriage-step, lifting weights, running sewing-machines, sea-bathing, a rough automobile ride, will bring on an abortion where there is a predisposition. Often in healthy women, on the other hand, extreme violence does not interrupt pregnancy. Surgical operations are classed here with violence. In a neurotic woman a slight operation on an organ not directly connected with the uterus will start expulsive contractions. Again, 66 per cent. of operations on ovarian tumors during pregnancy have left the uterus undisturbed. De Lee says he has removed fibroids from the pregnant uterus, once even exposing the chorion, and has amputated the cervix of a gravid uterus, without interrupting pregnancy. Several cases have occurred where both ovaries have been removed during pregnancy without abortion. The breast has been amputated and a kidney removed from a pregnant woman[79] without disturbing the pregnancy. Wiener[80] did eleven operations for ovarian tumors during pregnancy with only two abortions. Von Holst[81] removed a myoma weighing two and a half pounds from the uterus at the seventh month of gestation without abortion. Davis of Birmingham, Alabama, reported[82] that a woman three and a half months pregnant was shot in the abdomen. The rifle bullet made twenty-five perforations in her intestines. She was taken eighty-five miles, and then Davis cut out five feet of the intestine. She recovered and gave birth to a living child at term.
Double ovariotomy brings on abortion in the early months of pregnancy oftener than in the later, probably from the loss of the corpus luteum, which, it appears, is necessary for the[96] growth of the uterus. Appendicitis and appendectomy are especially likely to interrupt gestation, apparently as a result of infection and because pregnant women are prone to defer operation. The traumatism of criminal abortion, punctures and lacerations from bougies and curettes, and the exhibition of drugs like ergot and cantharides, are sources and results of abortion. Drugs will not empty the uterus unless they are given in poisonous doses which endanger the woman's life.
In the father, syphilis, tuberculosis, general paresis, general debility from alcoholism, unchastity, and senility, and septic conditions of the generative tract, may cause abortion. Many men who work with lead, phosphorus, mercury, or X-rays are sterile, and before they become totally sterile their condition appears to cause debility in the fetus which leads to abortion. In paternal lead poisoning there is a reduction of about 20 per cent. in the weight of the infants at birth, and a general weakness and retardation of the child. The children of lead-poisoned fathers are frequently permanently under weight.
Coition during gestation is a cause of abortion, and the fault here, as a rule, lies with the husband. St. Thomas[83] said: "St. Jerome protests against the sexual approach of the husband to his gravid wife, not that in this condition such an act is always a mortal sin, unless there is probable danger of abortion." St. Alphonsus[84] says if there is danger of abortion the use of the debitum is a grave sin. In n. 924 he again teaches that while it is true that if by the use of the debitum the life or formation of the fetus is endangered or checked the right to the use of the debitum is, in such circumstances, lost, yet he thinks that in pregnancy there is little danger of abortion from this cause, especially near term.
Sabetti-Barrett[85] says the wife is excused from the debitum conjugale if the husband is drunk, or if there is a rational dread of grave injury, or grave danger to health. Genicot[97][86] thinks that in pregnancy it "can scarcely be shown that there is a notable danger of abortion." Lehmkuhl[87] holds that a married person is not obliged to grant the debitum if there is great danger of abortion; but, he adds, "Even then, if there is a grave danger of incontinence I do not think it certain that there is an absolute obligation to abstain."
Unlike Lehmkuhl, moralists agree that if there is real danger of abortion from marital congress, such an act is illicit, but they are inclined to think that there is little or no danger of abortion, especially at the end of gestation. Authorities on obstetrics, on the contrary, say that one of the causes of abortion in the early months of pregnancy is marital congress; and one of the sources of sepsis in women, which may result in the death of both mother and child, is certainly congress at the end of gestation. This causation of abortion is found especially in neurotic irritable women, in such as have diseases of the generative tract, or a tendency to habitual abortion. Whenever a woman shows any tendency to bleeding during gestation the use of the debitum is undoubtedly contraindicated, because of the proximate danger of both abortion and septic infection. Toward the end of pregnancy the danger from sexual commerce is the risk of infecting the woman's vagina with bacteria which may bring on sepsis through the abrasions incident to parturition. The staphylococcus pyogenes albus, a dangerous septic microörganism, exists as a saprophyte in 50 per cent. of male urethras, and the bacillus coli communis is another source of infection from the father during pregnancy. De Lee saw two cases of sepsis that killed both mother and child from such an infection shortly before term. If a physician now examines a woman before delivery without using all the precautions known to prevent sepsis, such as wearing a sterile rubber glove, he is guilty of malpractice; yet certain moralists are inclined to let a husband do what he likes. Moralists talk about the fetus as protected in the membranes. That is nonsense, because it has no relevancy to the question. It can have the slight relevancy of untruth when the woman[98] is rendered septic, because then the membranes are no protection at all.
The mortality statistics of the United States Census Bureau show that a little more than 42 per cent. of the infants who died in the registration area in 1911 did not last throughout the first month of extrauterine life, and of these babies almost seven-tenths died of prenatal and delivery abnormalities. In 1912, in the registration area, which then took in 63.2 per cent. of our population, the total death-rate of infants under a year old was 9035, and of these 3905 died of puerperal infection. In the entire country a very conservative estimate of the annual number of deaths of infants from puerperal sepsis is 5000; and about 15,000 women die here yearly from this etiology alone. Of course most of these deaths are caused by unclean midwives and quacks, but a large number of them are brought about by incontinent husbands. Invalidism from puerperal sepsis happens many times 15,000. Moreover, one-third of all the blindness in the world is caused by septic infection of the eyes at birth and virtually all this septic infection of the eyes is carried in by diseased husbands, although not necessarily by coitus during gestation.
Coition during pregnancy is unnatural because it necessarily fails of the end of coition, which is procreation. Curiously, too, all the lower animals instinctively appear to avoid this act during pregnancy. Men should be told that marriage has restraints as well as celibacy. Women are reminded of the law of the debitum, but not of the occasions when they are even obliged to deny it. If a man cannot keep continent in the presence of his pregnant wife, let him live in another part of the house. Regard for the woman is lacking in many ways. Young girls often marry without having the faintest notion of sexual life, and they are panic-stricken when assaulted. I have known two who were frightened into insanity. Priests should tell young married men that they are human beings, not animals; that they should act like rational beings when they are first married; and that after the wife has become pregnant the husband should not be the cause of abortion in the first three months, nor of puerperal sepsis in the last three[99] months. Priestley,[88] in 2325 pregnancies, found one abortion in every four pregnancies; Guillemot and Devilliers in France, Hirst in Philadelphia, and others report the same proportion. These are natural, not criminal, abortions. If, then, in normal pregnancies about one child in five is lost before birth, husbands should be taught a continence which would to some degree avert this calamity. Superfetation has occurred by coition during pregnancy, and this results commonly in abortion and the death of both fetuses.
Premature labor in cases where the child is viable is produced by the same agencies that interrupt gestation in the early months. Obstetricians think that syphilis is the commonest cause of premature labor, and they estimate that from 50 to 80 per cent. of these premature births are due to syphilis. In a series of 705 fetal deaths in Johns Hopkins Hospital, 26.4 per cent. were due to syphilis. After syphilis the cause of premature labor next in frequency is nephritis with placental hemorrhages and infarcts. Twins are not seldom delivered prematurely because of lack of room in the uterus. For the same reason any tumor of the uterus or abdomen may cause an abortion.
When successive pregnancies are interrupted prematurely the abortion is said to be habitual, and again the commonest cause is syphilis. In this disease, as the virulence of the infection decreases, the gestation is prolonged until a child is born infected with congenital syphilis. This child commonly dies, and later a child strong enough to live appears. Correct treatment of the parents will avert this slaughter of the innocents. Sometimes the syphilis is latent so far as clinical symptoms are concerned, but we may find a positive Wassermann reaction. Hubert reported[89] that 8.8 per cent. of 8652 patients in a clinic at Munich where all were subjected to the Wassermann test had latent syphilis, and in 52 per cent. of these cases in men, and 75 per cent. in women, the infection was altogether unknown to the patients.
Chronic endometritis, where there is no syphilis, will permit[100] habitual abortion, and each abortion makes the condition worse. Nephritis, diabetes, and other constitutional diseases cause habitual abortion.
In the first two months of gestation the decidual fold which holds the ovum against the uterine wall is thick, vascular, and friable. The contracting uterus in abortion expels the decidua with considerable difficulty, but the ovum containing the fetus may slip out easily and be lost. A fetus two months old is about three-fourths of an inch in length. If a physician, nurse, or other person finds the ovum, no matter how small it is, they should open it at once with a scalpel or scissors and baptize the fetus conditionally, even if no sign of life is perceptible. If the fetus is unmistakably dead—a diagnosis not easily made—there is no use in attempting baptism; but always give the fetus the benefit of the doubt. In the first six or eight weeks the whole ovum is usually born developed in decidual tissue; sometimes the ovum will slip out of the decidua and be covered only with shaggy villi, suggestive of a chestnut burr.
During the third and fourth months there may be (1) an abortion of the whole ovum; or (2) the membranes may rupture, the fetus be expelled, and the secundines remain in the uterus, and these may have to be removed by instrument or finger; or (3) the decidua reflexa and the chorion may split and let out the fetus into the amniotic sac: here again the remaining secundines, if they do not come away spontaneously, must be removed. Abortion after the fifth month is like a regular labor at term, but not so energetic.
An abortion may be threatened, inevitable, or incomplete. In each of these conditions there is uterine pain and hemorrhage. In inevitable and incomplete abortions we find softening and dilatation of the cervix, and a presentation or expulsion of part or all of the ovum.
In pregnancy uterine hemorrhage and uterine pain are symptoms of a threatened abortion, but not certain symptoms. Fromme found that 17.9 per cent. of 157 women who had these signs in the early months went on to term. If the fact of pregnancy is not known it is not always easy to differentiate[101] a threatened abortion from other uterine conditions, like chronic metritis, ectopic gestation, a fibroid or other tumor, hemorrhage from cervical erosions or varices, or malposition of the uterus. If the abortion is inevitable the diagnosis is made more readily. The cervix is then more or less dilated and the ovum is palpable. There is rather profuse hemorrhage, flooding, and painful uterine contractions are evident. The rupture of the bag of waters may be simulated by the escape of secretions in hydrorrhoea gravidarum, or the escape of waters may be a primary symptom of graviditas exochorialis. Hydrorrhoea gravidarum is an intermittent discharge of clear or bloody fluid from a catarrhal endometritis under the decidua. It occurs in anemic, weak women, especially multiparae. In graviditas exochorialis the fetus is left within the womb but outside the ruptured chorion, and it may remain there for some time.
When an abortion is incomplete it is absolutely necessary to learn whether the entire ovum and decidual tissue have been expelled or not. When a part or all of the dead ovum is retained the consequences are so grave that they may result in the death of the woman or cause chronic invalidism. Sepsis may result, a placental polyp may form, and even syncytioma malignum may start—this fatal tumor, however, is not so common after incomplete abortion as after hydatid mole formation.
The prognosis as regards health is worse after abortion than after normal pregnancy. The involution of the uterus is slower than in full-term cases, and if infection has occurred there is great likelihood of a chronic endometritis and metritis. The woman may be rendered sterile, or she may become a chronic invalid to be cured only by capital operations.
In threatened abortion examination is to be avoided unless it is absolutely necessary for diagnosis, and then great gentleness is required so as not to excite uterine contractions. The woman is to rest in bed, not so much as raising her head to take a drink of water (which is given to her through a tube), and she is morally obliged to submit to this inconvenience. If she refuses she is accountable for the death of the fetus. If there[102] is bleeding the foot of the bed should be elevated as in hemorrhage in typhoid fever. The routine practice is to quiet the woman and the uterine irritability with morphine and other opium derivatives. Children are readily overwhelmed by opium because their circulation is not sufficient to neutralize the deoxidizing effects of the drug up to safety. While the embryo is connected with the maternal circulation through the placenta the mother's circulation often safeguards the fetus from the effects of the opium. The danger to the child in such cases begins from the opium remaining in its circulation after the child has been separated from the mother. Often, however, fetuses in cases where scopolamine and morphine have been used on the mother during labor are born badly, and even fatally narcotized, despite the connection with the maternal circulation. Nevertheless, even if there is some real danger to the fetus from the use of morphine in a threatened abortion, the cautious use of this drug would be morally justifiable. Should the threatened abortion go on to actual abortion, the fetus will certainly be killed, but the use of morphine on the woman is the best and virtually the only means we have to avert a threatened abortion and so save the fetal life. The immediate double effect from the morally indifferent act of giving a dose of morphine is, on the good side, the saving of the fetal life, and on the other, the evil side, the danger of fetal narcosis, which is not at all certain to follow. Evidently, the good intended effect far overbalances the evil and somewhat hypothetical effect.
After about five days, if the bleeding ceases, the woman may be permitted to go back to her ordinary routine of life, but with extreme caution, and she must return to bed at the slightest show of blood. Morphine is used at the beginning to quiet the patient and the irritable uterus. If the cervix is eroded, applications of a 10 per cent. nitrate of silver solution are made. The bowels are kept locked for three days and a softening enema of olive-oil is used before emptying the bowel.
If the bleeding starts again every time the woman goes about her duties, the abortion may be inevitable. When the[103] cervix is shortened and dilated so that the ovum is palpable and pieces of the decidua or ovum are expelled, the hemorrhage is more or less profuse, and especially if the bag of waters has ruptured and uterine contractions show, the abortion is deemed inevitable. In such a case the fetus may be alive, or it may be dead; and, again, conditions which show all the classic symptoms of inevitable abortion sometimes, though rarely, do not go on to abortion. It is extremely difficult, and often impossible, to tell whether an early fetus is dead or alive. A high, lasting fever sometimes kills the child; so do low blood-pressure, profuse hemorrhages, deoxidation of the blood in pneumonia, separation of the placenta, fatty degeneration of the placenta, and the severe infections—in such cases there is always strong probability that the child is dead when the abortion shows its symptoms. If the fetal tissues that appear indicate maceration, or if the discharge is fetid or purulent, the fetus is dead. Should the fetus be alive, tamponing the vagina to check the hemorrhage often separates the fetus from the uterus by the dissecting force of the blood dammed back, or in any case tamponing is almost certain to excite uterine contractions; thus there is an indirect killing of the fetus.
The treatment of inevitable abortion after the fifth month differs very much from the methods used in the early months. The prime principle is, never interfere until forced to do so. When the hemorrhage is dangerously profuse, so that the woman's life is endangered (an exceptional condition), the uterine cervix and the vagina must be tamponed with sterile gauze and cotton to check the bleeding, but this is a last resort. If the fetus is alive, or probably alive, nothing short of a necessity to save the woman's life by this means justifies the use of the tampon. De Lee advises the routine use of the tampon in threatened abortion, but this doctrine is erroneous medically and altogether false morally. If the physician knows the fetus is dead, he should, of course, tampon at once to get rid of the fetus. The tampon excites uterine contractions and causes destruction of a living fetus by dissecting it loose from the uterine wall through the dammed blood. Elevation[104] of the foot of the bed and the use of morphine will, as a rule, check the bleeding.
When the woman is bleeding to the risk of her life, the tampon is put in to check the bleeding and so save her life. The double effect immediately following this indifferent act is on one side good, the saving of her life; on the other side evil, the killing of the fetus. The good effect is intended, the evil effect is reluctantly permitted. Such a procedure is morally licit.
Where a tampon must be put in, it is left in from sixteen to twenty-four hours, even if the temperature goes up. During this time there are painful contractions of the uterus, as a rule, and these are expulsive. No drug is to be given to allay these pains if the intention is to have a dead or viable fetus expelled. If the pains cease suddenly, this is usually a sign that the fetus has been expelled above the tampon. When the tampon is removed and the entire ovum is found, it is best for the ordinary physician not to meddle with the uterus in any manner. Some advise that the physician should go over the uterine lining with a half-sharp curette to make certain that nothing has been left behind, but this is dangerous advice to any one who is not an expert obstetrician. Should the temperature remain above 100 degrees, the uterus must be cleaned out, and flushing with uterine catheters is not enough: if the gloved finger cannot remove the secundines, the curette is needed.
If, when the tampon has been removed, no ovum is found and the cervix is still closed, another tampon is to be put in for another twenty-four hours, supposing the removal of the ovum is licit. Forcible dilatation of the cervix is always a dangerous operation, and should never be employed when avoidable. Steel dilators have ruptured the uterus and killed the patients again and again even when used by experts. Laminaria tents are not to be recommended; the tamponade is enough.
When the retained ovum cannot be removed by the finger or squeezed out, the free portion of the ovum is to be grasped by an ovum forceps and gently drawn out. The operator[105] should be sure he has a part of the ovum in the forceps and not a part of the uterine wall. If he bites into the uterine wall (a common catastrophe), he may pull a hole in that wall, and then the woman will probably die unless the rent can be closed immediately after opening the belly. When the abdominal cavity has been opened in such an event, the uterus is also to be opened, cleansed, and sutured. This method is safer than curetting where there is a rent. If one is certain the gut has not been injured—and it is extremely difficult to be certain—vaginal anterior hysterotomy may be substituted. Sometimes perforations, when the uterus is not septic and the instruments are clean, are not dangerous. Rest in bed, ice-bags, ergot, and opium cure without operation.
Physicians who are called into an abortion case should always be certain that no one has attempted to pass sounds, curettes, or similar instruments, because a perforation may have been made by the meddler which will be charged to the second man himself.
If a uterus is flexed it is easy to poke a curette or like instrument through it at the bend, especially if the uterus is thin or friable from sepsis. Again, the placental site is raised, it feels rough, and the furrows in it lead one to think part of the placenta is still adherent, whereas all has been removed. Repeated scraping, due to this error, may dig a hole through the uterine wall. Perforation in a septic case is practically always fatal to the woman. The use of the curette supposes a special technic, and no physician should presume to try its use unless he has been carefully and practically instructed.
In inevitable abortion after the third month it may be very difficult to get the embryo out. The cervix, in primiparae especially, may be long, thick, and hard. If the fetus is dead, it may then be removed by morcellement—i. e., by cutting and breaking it into pieces, and then taking out these pieces with an ovum or stone forceps. Sometimes, though rarely, the operator may find it impossible to get the entire fetus away. Then the uterus is packed with weak iodine gauze, and after twenty-four hours the fetal remains are expelled.
In every abortion the presence or absence of extrauterine[106] pregnancy is to be made out. If there is an extrauterine pregnancy, curettage will cause rupture of the sac.
When the interior of the aborting uterus has become septic the old treatment was to empty the uterus at once, but now the treatment is expectant, because the traumatism of the curetting makes the sepsis worse. The commonest and worst infections are of the streptococcus putridus, a pus staphylococcus, and the bacterium coli communis. Curettage lets these microörganisms enter the circulation. The cause of this condition is often unskilful attempts at artificial abortion. When the womb contains decomposing material bleeding usually obliges tamponing, and thus often the uterine contents come away in twenty-four hours with the gauze. If there is no hemorrhage there should be no tamponing: it is then better to get dilatation by packing and drain the uterus with gauze. The curette should not be used at all.
Where there is habitual abortion the cause must be found. During gestation syphilis and displacements of the uterus, as causes, may be treated. Endometritis can be cured only when the uterus is empty. Rest in bed at the time when these abortions usually occur, and at the time when menstruation customarily appears, is required. Treatment of the husband is often necessary, as he is virtually always the source of luetic infection.
Attention or inattention to the mother's own hygiene during pregnancy has great effect on the fetus, and care of hygiene may avert abortion. The woman's dress should be simple and warm enough to prevent congestion from changes in temperature. Congestions are likely to affect the kidneys, and care of the renal function is always one of the most important facts connected with pregnancy. No circular constrictions of the trunk by lacing or stiff corsets should be attempted. The corset forces the uterus and child downward into the pelvis and against the lower abdominal wall, causing congestion of the pelvic veins and strain on the abdominal muscles. Tight corsets, preventing the expansion of the uterus and the growth of the fetus, may cause mutilations like club-foot and wry-neck, or even kill the child. The woman who would "preserve[107] her figure" by corsets, to the mutilation, weakening, or killing of her unborn infant, and this is an every-day evil, is either a criminal fool or an unmitigated scoundrel. Tight lacing to conceal pregnancy is a method of murder. High-heeled shoes are somewhat injurious because of the constrained position into which they throw the woman. X-ray photographing of pregnant women is very likely to cause abortion.
The woman's diet should be simple. She must abstain from all alcoholic liquors even if she has been accustomed to their use at meals. She should not overeat on the supposition that she has to feed two persons. Some popular books advise a special diet to reduce the bone-salts and thus get a smaller baby and one more easily delivered. Such advice is criminal. The constipation of pregnancy is not to be treated by strong cathartics like Epsom salt. The kidneys are to be watched; therefore the urine should be examined every three weeks up to the seventh month, then oftener. If there is any suspicion of toxemia or nephritis, the urine should be examined daily. Obstetricians who have any regard for their own conscience and reputation will have nothing to do with a woman who refuses to take this precaution.
Physical exercise should be gentle—say, walking, up to two miles in the daytime. The vast majority of women are too lazy to take physical exercise as a hygienic duty at any time, and during pregnancy their aversion to all effort to overcome indolence is so great they make even themselves believe they cannot. Just as most professional men think they think, most women think they work. There are thousands of women who have servants, yet make not only their families and friends but themselves believe they are worked to death, and their work is the spreading of four or five beds, and the ordering of groceries over the telephone. When these women are pregnant they quit even the bed-making.
Cold and hot baths, Turkish and Russian baths, hot sitz-baths and ocean bathing are not permissible during gestation. Tepid baths and spongings are to be substituted. Near term the bath-tub is not safe because of danger of uterine infection from unclean water. Then shower-baths are better, but these[108] are dangerous if the woman must step over an enameled bath-tub side to take them, because she may slip and fall. Vaginal douches are not to be used in pregnancy except in certain diseased conditions, under the direction of a competent physician.
Therapeutic abortion and therapeutic induction of premature labor are employed in five chief groups of conditions: (1) contracted pelvis; (2) diseases caused by pregnancy; (3) diseases coincident with pregnancy; (4) habitual death of the child after viability but before term; (5) prolonged pregnancy. There is no such act as therapeutic abortion of an inviable child; all abortions of inviable children, when direct, are criminal, and nothing criminal is therapeutic. The consideration of narrow pelvis, and the diseases caused by pregnancy and coincident therewith, will be treated in detail.
When the child dies after viability but before term the cause is most commonly syphilis. In such cases a Wassermann reaction should be made from both parents; and even if it is negative, and no other definite cause for the fetal death can be found, syphilitic treatment should be tried on the father and mother. Bright's disease, even when scarcely diagnosable, anemia, diabetes, adiposity, and hypothyroidism are other lethal causes of habitually still-born infants. Not seldom the cause is in the husband. If he is an alcoholic (and two or three drinks of whiskey a day make any man an alcoholic), if he is especially susceptible to the toxin of tobacco (and tobacco alone may render some men not only sterile but impotent), if he is a worker in poisonous metals, an X-ray operator, a user of narcotics, exhausted with overwork and worry, affected with weakening systemic disease, his germ-cells are unfit for their function. Such men are not technically sterile, but they are practically sterile.
Some women carry the child beyond term, with the effect that the baby is overgrown for normal delivery. The head is harder and more angular than it should be, the long bones stiffer and less pliable, the muscles tenser. All these changes make the delivery so difficult that the overgrown child may be fatally injured at birth. Physicians must be cautious in believing histories of enormous children at previous births at[109] which they were not present. Mothers and nurses are likely to exaggerate the size of infants.
In cases where the children die at a particular time before term, premature labor should be induced to save the child, and when the child has been carried over term it may be necessary to induce labor. In the first condition labor is not to be induced a week earlier than is necessary. We talk so much of a seven months' child as viable that we forget that any child born before the thirtieth week of gestation has very small chance for survival. From 30 to 60 per cent. of all prematurely delivered infants die. The maternal passages do not dilate normally and the child is unformed; its bones fracture readily; it cannot sustain pressures and strains. All induced labors are dangerous to the mother by shock and possible infection, and only very grave necessity justifies any such procedure.
In inducing necessary premature labor the technical method may take on a moral quality. There are over a score of methods, and many of these, although used, are dangerous and should be obsolete. A very common method, begun in 1855, is to insert one or two elastic solid bougies into the uterus between the membranes and the uterine wall. This is a dangerous method and should be obsolete. Other dangerous and obsolete methods are the puncture of the membranes with a trocar high up in the uterus; intrauterine injections of hot or cold water, glycerine, milk, and other liquids; vaginal tamponade alone; irrigation of the vagina with carbon-dioxide water; a stream of hot water directed against the cervix, electricity, X-ray, dilatation of the vagina with a rubber bag, irritation of the nipples, the use of drugs like quinine, cimicifuga, ergot, or cantharides.
If haste is not necessary, packing the cervical canal and the lower uterine segment antiseptically with a strip of gauze three to five yards long and three inches wide and leaving it in for about twenty-four hours is one of the best methods. Where rapid delivery is required, cesarean section must be employed. In cases of somewhat less urgency the membranes are first punctured and balloon dilators are used. In any case puncture[110] of the membranes is the most certain method to start labor, but it has many bad disadvantages. A dry labor in a primipara with an undilated cervix is a grave condition. If the fetal head is not engaged in the pelvis, puncture must not be attempted. When the head is not engaged in the pelvis like a ball-valve, the cord will prolapse, be pinched, and thus the blood supply will be cut off from the child and the loss will kill it. For the same reason, the waters must not be run off too quickly. Many operators insert a bag, dilate, and so start the labor, without puncturing the membranes, where there is no reason for haste.
Therapeutic abortion, as has been said, is never permissible, under any circumstances, if the child is not viable. In certain conditions, say, when a uterine tumor clearly threatens the life of the pregnant woman, or if in extrauterine gestation there is a rupture of the tube, an operation may be permissible, or even obligatory, which has for its direct end the removal of the tumor or the stopping of the hemorrhage. If such a removal or ligation, under these conditions, indirectly causes the abortion of the inviable fetus, or its death from a lack of blood, these indirect effects may be reluctantly permitted. They are cases of an equally immediate double effect, one good and one evil, where all the requirements are fulfilled. A direct abortion of an inviable fetus, however, is never licit even to save the mother's life, and in abortion the killing is direct because it is used as a means to an end. In a ruptured ectopic gestation the primary effect of the physical operation is to ligate the torn arteries to save the woman's life here and now; the secondary effect is the permitted death of the fetus from the shutting off of the blood supply. In the abortion of a premature fetus the primary effect of the operation is to separate the placenta from the uterus, to cut off the child's blood supply, and as a direct consequence of this act, which is essentially evil, the woman's life is saved. The original act in this abortion is evil, and evil may not be done even if good follows. Even in self-defence against an unjust aggressor one may not kill a man to save his own life—he tries to save his own life and reluctantly permits the death of the aggressor. In a killing[111] in self-defence there are two distinct effects; in abortion there is only one effect, and the killing is a means to this one effect. That you may kill an irresponsible insane man who is attacking your life, or the life of one entrusted to your care, is no reason that you may attack a fetus in the womb. There is no parity. The insane man is a materially unjust aggressor; the fetus is not an aggressor at all. The mother placed it where it is; and if any one is an aggressor, she is. In the abortion you directly kill the fetus and indirectly save the woman's life, and this indirection uses the death of the fetus as a means to the end of saving the woman's life. In killing the insane aggressor you directly save the life of yourself or your ward, and reluctantly permit the death of the aggressor. The proofs of the essential immorality of direct homicide have already been established in the general chapter on Homicide.
The assertion that an undeveloped fetus in the womb is not as valuable as the mother of a family is beside the question, and in certain vital distinctions it is untrue. Any human life, as such, whether in a fetus or an adult, is as valuable as another, inasmuch as no one but God has any authority to destroy it, except when it has lost its right to existence through culpable action. Secondly, the quality of motherhood is an accidental addition to a mother's life, not substantial as is the life itself. This quality of motherhood does not create any juridic imbalance of values which justifies the destruction of the rights inherent in the fetus. That the fetus may not be able to enjoy these rights if the mother dies is, again, an irrelevant consideration. There is no question of a comparison of values. A life is a life, whether in mother or fetus, and the destruction of an innocent life by any one except its creator, God, is essentially an evil thing, like blasphemy. An innocent fetus an hour old may not be directly killed to save the lives of all the mothers in the world. Insisting on such comparisons supposes ignorance and sentimental opposition to truth. It is a good deed to save a mother's life; but such saving by killing an innocent human being ceases to be good and becomes indescribably evil, an enormous subversion of[112] the order of the natural law, as it is a usurpation of the dominion over life possessed by God alone. If I owe a man a vast sum of money and the payment of this debt will ruin me and my children, it would be a good thing for me and them to have this creditor put out of the way by death, but that fact is no justification whatever for me to kill the man. The fetus in the womb in a case where there is question of therapeutic abortion is like this creditor: it would be well for the mother to have this fetus out of the way, but that is no justification whatever for her to kill the fetus, or to let it be killed by a physician. The physician who kills such a fetus is exactly like a hired bravo who assassinates a troublesome creditor for a fee, except that the physician does the nasty job for less money.
To hasten even an inevitable death is homicide, and that quality of merely hastening adds nothing for extenuation: every murder is merely a hastening of inevitable death. To give a dying man a fatal dose of morphine "to put him out of misery" is as criminal a murder as to blow out his brains while he is walking the streets in health; to ease pain is not commensurate with the horrible deordination of taking a human life. This subversion of the moral law in the interest of mawkish sentimentality is one of the gravest evils of modern social ignorance. Physicians are constantly mistaking inclination, or the mental vagaries of the nurses who influenced their childhood, for rules of moral conduct. A physician is not a public executioner, nor a judge with the power of life and death: his business is solely to save human life, never to destroy it.
If there were anything in the objection that refusal to do abortion opposes the life of a useless fetus to that of a useful mother of a family, where would such false logic stop? If it held for the taking of life in an unpleasant condition, it would hold a fortiori in every other less unpleasant condition where a life would not be at stake. When a note that you had given falls due and it would bankrupt you to pay it, does this inconvenience let you out of the difficulty in honor, in the moral law, or in the civil law? It certainly does not; but it[113] should if the doctrine of the sentimentalists on abortion were true. An eclamptic woman, or one with hyperemesis gravidarum, conceived the child, got into the difficulty, and she and her physician have no right to tear up the note they have given to the Creator, especially when such tearing implies murder. Suppose, again, a woman has done a deed for which she has in due process of just law been condemned to death; suppose, also, there is only one man available to put her to death, and if this man were killed she could escape. Would her physician be permitted to shoot that executioner to let her out of the difficulty? Certainly not. That, however, is just what the physician does who empties an eclamptic uterus of an unviable fetus. You may not do essential evil that anything under the sun, good, bad, or indifferent, may come of it.
If I may kill a so-called "useless fetus" to save a useful mother, do gross evil to effect great good, why should I stop there? Why, then, may I not rob a church to make my children rich, murder a useless miser to employ his money in founding orphanages, shoot any oppressor of the poor, kick out of doors my senile and bothersome father, reject all my most sacred promises whenever their observance makes me suffer? Where will the sentimental moralist draw the line? That the civil law permits therapeutic abortion is no excuse at all; it is merely a disgrace of the civil law. The American civil law permits many things that are contrary to morality and the law of God: it absolves bankrupts even if they afterward become solvent; it permits the marriage of divorced persons; it levies unjust school taxes; it gives unjust privileges; it squanders the money of the citizens; and so on.
If a woman marries in good faith a man she deemed a gentleman, but who turns out to be a syphilitic sot who disgraces her and makes her life a perpetual misery, immeasurably worse than the condition of any eclamptic woman, no greater blessing could come to her and her children than his death. Would she therefore be justified before any tribunal of God or man in murdering him to get rid of her trouble? No;[114] she must bear with her evil for the sake of social order and of eternal right. So must the eclamptic woman.
If it is murder to kill a child outside the womb, and mere therapeutics to kill it inside the womb, then it is murder to shoot a man on the street, and mere good marksmanship to shoot him to death inside his house, especially if he is an undesirable citizen. All reputable physicians deem a fetus in a normal pregnancy so good that they will not dream of destroying this fetus. They absolutely refuse to effect an abortion to get rid of a fetus which may disgrace an unmarried woman and her family, and they are perfectly right in this refusal. They talk and write with genuine indignation of race suicide. The only reason they have for the refusal to do what they call criminal abortion is that the disgrace or inconvenience of the woman is not commensurate with the destruction of a human life. They observe the natural human instinctive repugnance to murder in this special speech and writing, and then go home and get their obstetrical bags and complacently murder the first baby they find in the womb of a married matron who has a disturbed stomach or kidneys. They show here the fine intellectual acumen and reasoning ability of a chronic lunatic. The first fact in the social order is that justice, law, order, should prevail, no matter what the cost. It might be better that the fetus should die than that the mother should die, though that is not always true. It is not better that an unbaptized fetus should die than that a mother in the state of grace should die. But these are irrelevant considerations. It is never better that the fetus should be killed than that the mother should die. That is a very different matter.
The Mignonette case in 1884, tried in England by Lord Coleridge, is a good example of evaluation of lives as in therapeutic abortion, which came to grief. A ship called the Mignonette foundered 1600 miles from the Cape of Good Hope, and three of its crew, with a boy, were for a long time at sea in an open boat without provisions. When they were almost starved the boy lay on the bottom of the boat, asleep or half conscious from weakness. Two of the men plotted to[115] kill the boy for therapeutic purposes; they needed his flesh to save their own lives. They killed the poor lad just as the therapeutic abortionist kills a fetus. They got his uncooked flesh for four days. Later Lord Coleridge got them and he sentenced both of them to death. Another Lord will get the therapeutic abortionists.
What, then, is the physician to do who meets a case that imperatively calls for therapeutic abortion according to the common medical practice? He can do nothing. The law may seem hard in certain circumstances to those who cannot see beyond the physical; yet that fact does not abrogate the law, which is one of essential morality.
May the physician call in a physician who, he knows, will not scruple to perform the therapeutic abortion on an unviable fetus? If he does, he is as much a murderer as if he did the deed himself. He may not so much as suggest the name of some one who will do the deed. He simply tells the family he can do nothing. If they insist on the abortion he withdraws from the case.
In this connection it is necessary to mention again the question of viability. Langstein reported[90] a study of the growth and nutrition of 250 prematurely born infants, and he found a confirmation of what was already known, that a weight of 1000 grammes (21⁄5 pounds) and a full body length of 34 centimetres (133⁄5 inches) are the lowest limits for viability under proper circumstances. A fetus 1000 grammes in weight and 34 centimetres in length has completed the sixth solar or calendar month, or the sixth and a half lunar month—it is beginning its seventh month, not ending it, yet it is viable under proper conditions.
The child at term, on a rough average, is from 48 to 52 centimetres (19 to 201⁄2 inches) in length, and it weighs from about 63⁄5 to 71⁄2 pounds. It is impossible, however, to obtain the sizes and weights of infants in utero with scientific accuracy, because the date of conception cannot be determined with absolute certainty, and infants in utero vary as they do after birth. A full-term infant sometimes may weigh[116] only 31⁄2 pounds when the mother is diseased, and at times an eight-months fetus will weigh as much as 8 pounds.
As was said in Chapter III, a fetus of six completed calendar or solar months (not lunar—the duration of gestation is often reckoned in lunar months by obstetricians) is viable provided it is cared for by competent physicians in a hospital. Otherwise it is not viable, except in a strictly technical sense; it will not live more than a few days or weeks.
A full seven-months infant may be reared with proper feeding and skilled care; a six-months infant may be reared (with difficulty) in a hospital with skilled care. If it is certain that the removal of a six-months fetus will here and now save the life of a mother (a very difficult matter to judge by the best diagnosticians), this removal may be done, provided the infant is delivered in circumstances where skilled care, incubator, and proper food are obtainable; otherwise the removal is not justifiable.
The Council of Lerida, in Catalonia, in the year 524, decreed that abortionists of any kind must do penance all their lives, and if they are clerics they are to be suspended perpetually from all ecclesiastical ministration.
The Council of Worms, under Hadrian II., in the year 868,[91] also judged women who procure abortion as certainly guilty of murder.
In the Corpus Juris,[92] among the decretals of Gregory, there is the following law: "If any one, through lust or hatred, does anything to a man or woman, or gives them any drug, so that they cannot either generate or conceive, or bear children, he is to be treated as a murderer."
Sixtus V., in the Constitution Effraenatam, October 29, 1588, mentions a decree of the Sixth Synod of Constantinople, in session in 680 and 681, which subjects those who perform abortion, or kill a fetus, to the punishment inflicted on murderers. Sixtus then decreed that any one who effects the abortion, directly or indirectly, of an immature fetus, whether the fetus is animated, formed, or not, either by blows, poison,[117] drugs, or potions, or tasks of hard labor imposed on pregnant women, or any other method, however subtle or obscure it be, is guilty of murder, and is to be punished accordingly. He recalls all ecclesiastical privileges from clerics who cause abortion, and says that they are to be reckoned as murderers according to the decree of the Council of Trent,[93] and he makes a law that abortionists may never be promoted to orders.
In the fifth paragraph he says: "Moreover, we decree that the same penalties are incurred (1) by those who give potions and poisons to women to induce sterility or prevent conception, or who cause these drugs to be administered, and (2) by the women themselves who freely and consciously take these drinks."
In paragraph seventh he decrees that any one, man or woman, cleric or lay, who procures abortion by counsel, favor, drinks, letters of advice, signs, or in any way whatever, are ipso facto excommunicated, and the excommunication is reserved to the Pope himself.
Gregory XIV., in the constitution Sedes Apostolica, May 31, 1591, gave to priests who have special faculties for the purpose from the bishop, permission to absolve from this excommunication, but only in foro conscientiae. Sixtus V. and Gregory XIV. used the term foetus animatus, in keeping with the old Aristotelian notion of animation.
Pius IX., in the constitution Apostolicae Sedis Moderationi, deleted the epithet animatus, and extended the excommunication to all abortions, no matter at what time of the gestation they occur. He ordered that only the actual physical abortionist is to be excommunicated, not those who counsel the crime. Some moralists hold that those who order abortion are direct abortionists and fall under this excommunication; other moralists oppose this opinion. Pius IX.[94] excommunicates procurators of abortion if actual abortion is effected, and this excommunication is reserved to the bishops, not to the Pope.
In this decree occur the words "Procurantes abortum, effectu[118] secuto," and there has been considerable discussion of the question who are the procurantes, the agents who fall under the excommunication? Again, are craniotomy, cephalotrypsis, decapitation, embryotomy, and exenteration, when performed on the living child, abortions in the sense of the decree, and thus matter of the excommunication?
Those who do abortion are the principal agents who physically, immediately, of themselves, in their own name, or who morally, through others, perform an abortion. The common opinion of moralists is that all those who of themselves or through others bring on an abortion are excommunicated, but that assistants, although guilty of crime, are not excommunicated.
Many eminent moralists are of the opinion that the mother herself who seeks an abortion does not fall under the excommunication because Sixtus V. does not explicitly mention her in this penal law, and a penal law is to be interpreted literally. If a pregnant woman goes to an abortionist and persuades him by speech and pay to do an abortion, she is the direct moral cause of that abortion. If it were not for her, the abortion would not take place. Virtually all abortions done on married women are effected morally by the woman herself. In my opinion, and the new canon law states this explicitly, the woman who procures an abortion on herself or on another woman is excommunicated.
Sabetti-Barrett[95] holds that craniotomy on a living child and the removal of an inviable extrauterine fetus are not abortion in the scope of this excommunication, because as a penal law these operations are not specifically mentioned. All mutilating operations, like craniotomy and the others enumerated above, first kill the fetus, then extract its body from the womb; abortion first extracts the fetus and then lets its die. The result is the same, but the operations differ technically, and a penal law is ad literam. A cleric who procures abortion of an inviable fetus at any time of gestation falls under the excommunication and suspension a sacris perpetually, although he probably is not technically irregular canonically if[119] he procures the abortion before the Aristotelian date of animation. The bull Effraenatam makes the canonical irregularity at the Aristotelian date obsolete practically.
In the church the Holy Office (that is, the Inquisitors-General in matters of faith and morals) is the official authority which interprets, under the approval of the Pope, the morality of acts like abortion and related operations. In 1895 the following difficulty was proposed to the Holy Office for solution:
A physician is treating a woman with a disease which will certainly be fatal to her unless cured medically, and the disease is due to the presence of a fetus in her womb. To save her it is necessary to empty the uterus, but the fetus is not yet viable. The question is, May the physician perform therapeutic abortion in such circumstances?
On July 24, 1895, the Holy Office answered: "The Inquisitors-General in matters of faith and morals, with the vote of their Consultors, decree: Negatively, in accord with the other decrees of May 28, 1884, and August 19, 1888."
In May, 1898, the following questions were proposed to the Holy Office:
I. Is the induction of premature labor licit when a contracted maternal pelvis prevents the birth of a child at term?
II. If the maternal pelvis is so narrow that premature delivery is impossible, is it licit to perform abortion, or to effect cesarean delivery at the proper time?
III. Is laparotomy in extrauterine gestation licit?
May 4, 1898, the Holy Office answered, with the assent of Leo XIII:
I. Premature labor in itself is not illicit, provided it is done for sufficient reason, and at the time and by such methods as will under ordinary circumstances preserve the life of the mother and the fetus.
II. As to the first part, the answer is negative, according to the decree of July 24, 1895, on the unlawfulness of abortion. As to the second part, there is no objection to the cesarean delivery at the proper time.
III. In a case of necessity, a laparotomy to remove an[120] ectopic fetus from the mother is licit, provided the lives of both mother and fetus are, so far as is possible, carefully and opportunely preserved.[96]
March 5, 1902, this question was asked the Holy Office: "Is it ever licit to remove an ectopic fetus from the mother while the fetus is under six months of age from the time of conception?"
The answer was: "Negatively, in accord with the decree of May 4, 1898, by which the lives of the fetus and mother, as far as possible, are carefully and opportunely preserved. As to the time, the questioner is reminded by the same decree that no premature delivery is licit unless effected at the time and by the methods which, under ordinary circumstances, will preserve the lives of mother and fetus."
The English civil law concerning abortion[97] is:
"Whoever shall unlawfully supply or procure any poison or other noxious thing, or any instrument or thing whatsoever, knowing that the same is intended to be unlawfully used or employed with intent to procure the miscarriage of any woman, whether she be or be not with child, shall be guilty of a misdemeanor, and being convicted thereof shall be liable, at the discretion of the court, to be kept in penal servitude for the term of three years, or to be imprisoned for any term not exceeding two years, with or without hard labor."
Alfred Susaine Taylor,[98] commenting on this law, said: "Strictly speaking, there is no such thing as justifiable abortion; the law recognizes no such possibility. A medical man must always remember this when he contemplates emptying a pregnant uterus.
"It is obvious that the only reasons that can be thought of by an honorable man as justifying the induction of labor are (1) to save the life of the mother; (2) to save the life of the child. (Some religions will not contemplate the first reason, but that we are not now concerned with.) It cannot be[121] done for the sake of family honor nor for any similar ethical reason....
"The golden rule is never to empty a uterus without first having a second professional opinion as to its necessity; if this opinion be adverse, do not do it; if it be favorable, it is well to get it in writing, and it is well also to get the written or attested consent of the woman and her husband, and then proceed to do it with all the skill and care possible. The death of the fetus is at any time the most certain means of causing the womb to empty itself, but after the sixth month the operation is performed necessarily with a view to preserving this life, and steps must be taken accordingly." Coke, about 1615, judged that to kill a child in the womb is not murder, but if it is expelled by violence and dies after it leaves the womb, that is murder.
The law in Pennsylvania[99] is: "If any person, with intent to procure the miscarriage of any woman, shall unlawfully administer to her any poison, drug, or substance whatsoever, or shall unlawfully use any instrument, or other means whatsoever, with the like intent, such person shall be guilty of felony, and being thereof convicted, shall be sentenced to pay a fine not exceeding five hundred dollars, and undergo an imprisonment, by separate or solitary confinement at labor, not exceeding three years." It makes no difference in Pennsylvania law whether the child is quickened or not.
The New Jersey, Massachusetts, and Wisconsin laws are like the Pennsylvania law. The law in Iowa[100] is: "If any person, with intent to procure the miscarriage of any pregnant woman, wilfully administer to her any drug or substance whatever, or, with such intent, use any instrument or other means whatever, unless such miscarriage shall be necessary to save her life, he shall be imprisoned in the penitentiary for a term not exceeding five years, and be fined in a sum not exceeding one thousand dollars." To the same effect are the laws in Connecticut, Maine, New York, Ohio, Michigan, Minnesota, Colorado, Texas, and Maryland.
Frank Winthrop Draper, professor of legal medicine in Harvard University,[101] commenting on the Massachusetts law of October, 1903, cap. 212, secs. 15, 16, says: "It is important to recognize the fact that the law does not make any exception or formal recognition in favor of justifiable operations to procure premature labor. The statute is general in its application. It is, of course, obvious that the best sentiment of the medical profession and of obstetric teachers is favorable to interference of pregnancy, (1) whenever there is such anatomical deviation or mechanical obstruction in the mother's pelvis that the birth of a child is impossible; or (2) whenever the mother is suffering from such grave disease that her life is in imminent peril and can be saved only by the arrest of gestation. Under such conditions the physician is not only warranted in inducing premature labor, but is required to do so by a sense of duty to his patient, with a view thereby to save one life at least, and, if possible, the lives of both mother and offspring.
"Nevertheless, as the law now stands, a prudent practitioner will not expose himself to any risk, if a few precautions will save him. In the event of the death of the mother and child in such an emergency, the attending physician might find himself in jeopardy, with the imputation of gross carelessness and criminal neglect hanging over him, an imputation which requires years to remove. So the attending physician should never undertake to do an instrumental operation without these precautions: 1. The consent of the patient, with that of her husband or family. 2. Especially, a consultation with some other physician or physicians in whom there is full confidence. Attention to these simple and sensible safeguards, by making the conduct appear by its candor and openness in the strongest possible contrast with the secret methods of the abortionist, may save great embarrassment."
The ethics of this doctrine is, of course, absurd, as has been shown, and it is cited here only to show how the civil law considers abortion. Wharton and Stille[102] give the same[123] information in a more technical manner. "It is a general rule," they say, "independent of statute, that the act of a physician in aiding a miscarriage is not unlawful, where the miscarriage was the inevitable result of other causes. And the act is justified where the circumstances were such as to induce in the mind of a competent person the belief that a miscarriage was necessary to preserve the life of the mother. And the statutes of many of the States penalize the causing, or attempting to cause, an abortion, unless necessary to preserve the life of the woman, or unless advised by a designated number of physicians to be necessary for such purpose, the absence of both the necessity and the advice being an essential ingredient in the crime. The physician by whom the deed is done, however, cannot act as his own adviser in the matter. And an indictment under the statute must not only allege that the act was not necessary to preserve the woman's life, but must also negative the advice of physicians; and such averments cannot be inserted as an amendment after demurrer.
"The burden of proof rests with the state to show that the means used were not necessary to preserve the life of the woman in question; and the absence of necessity may be determined from circumstantial evidence. But the burden of proof as to the advice of physicians would not fall within the rule controlling the production of proof as to negative matters in general, and would rest with the accused; though it may be proved by a preponderance of the evidence and need not be established beyond a reasonable doubt. But either that the act was necessary to preserve the life of another, or that it was advised by physicians to be necessary for that purpose, is of equally good defence; and the destruction of the child need not have been both necessary and advised by physicians. And statutes of this class apply only in cases in which the death of the mother could reasonably be expected to result from natural cause, unless the child was destroyed, and do not apply to a case in which the mother threatened suicide unless she was relieved from her trouble."
Ectopic Gestation, called also extrauterine pregnancy, is gestation outside the uterus in the adnexa or the peritoneal cavity. Pregnancy in the horn of an abnormal or rudimentary uterus is classed with ectopic gestation because the effects are similar, although pregnancy at times in a rudimentary uterus goes on to term normally. The uterus is in the pelvic cavity, between the bladder and the rectum, and above the vagina, into which it opens. It is a hollow, pear-shaped, muscular organ, somewhat flattened, and about three inches long, two inches broad, and an inch thick. The fundus or base is upward, and the neck is downward. Passing horizontally out from the corners or horns of the uterus, which are at the fundus, are the two Fallopian tubes, one on either side. These are about five inches in length and somewhat convoluted. They are true tubes, opening into the uterus, and they are about one-sixteenth of an inch in diameter throughout the greater part of their extent. The ends farthest from the uterus are fringed and funnel-shaped; and this funnel end, called the Infundibulum or Fimbriated Extremity, opens into the abdominal or peritoneal cavity. Near the Fimbriated Extremity of each tube is an Ovary, an oval body about one and a half inches long by three-quarters of an inch in width. For convenience in description, each tube is divided into four parts: (1) the Uterine Portion, which is that part included in the wall of the uterus itself: it extends from the outer end of the horn into the upper angle of the uterine cavity, and its lumen is so small that it will admit only a very fine probe; (2) the Isthmus, or the narrow part of the tube which lies nearest the uterus: it gradually widens into the broader part called (3) the Ampulla; (4) the Infundibulum, or the funnel-shaped end of[125] the Ampulla. One of the fimbriae, the Fimbria Ovarica, is longer than the others, and it forms a shallow gutter which extends to the ovary.
The uterus, tubes, and ovaries lie in a septum which reaches across the pelvis from hip to hip. This septum is called the Broad Ligament. If a man's soft hat, of the style called "Fedora," is inverted, the fold along the crown coming up into the cavity of the hat is like the broad ligament. As the crown is held downward the uterus would be in the middle, its fundus upward, and outside the hat, representing the pelvic cavity, but in the crown fold. The tubes and ovaries would also be in the crown fold, or broad ligament, and the fimbriated extremities would open into the interior of the pelvic cavity through holes. The ovum breaks through the surface of the ovary into the pelvic cavity, passes, probably on a capillary layer of fluid, into the fimbria ovarica and thence into the infundibulum, whence it moves along slowly into the uterus.
Ovulation and menstruation occur about the same time ordinarily, and if the ovum produced is not fecundated it gradually shrivels and passes off through the uterus and vagina. Fecundation of the ovum rarely occurs in the uterus, but ordinarily in the Fallopian tube. After fecundation the ovum is pushed on through the Fallopian tube into the uterus in from five to seven days, where it fastens to the wall and develops normally. Hyrtl described an ovum which appeared to reach the uterus in three days. If from some abnormal condition of the Fallopian tube the fecundated ovum is blocked and held in the tube, the embryo grows where the ovum stopped, and we have a case of Ectopic Gestation. In normal pregnancy in the uterus, the uterus grows with the embryo, but a tube does not. In the latter condition, when the ovum is big enough it bursts the tube or slips out through the ampulla, causing hemorrhage or other pathological symptoms.
There are certain rare abnormalities of the uterus through imperfect embryological development, and pregnancy in such a uterus may result in symptoms like those of ectopic gestation. Normally the uterus and vagina are formed by the[126] fusion of the two Müllerian ducts. When these ducts do not fuse perfectly, or when one develops partly, the various kinds of abnormal wombs and vaginas are the results. There may be a double uterus with a single or double vagina, a uterus with a complete or partial septum down the middle, a uterus with one horn, a uterus with a developed horn and a rudimentary horn, and the rudimentary horn may be open or shut, and so on. In many of these conditions the ovum becomes blocked and rupture follows as in ectopic gestation.
When the ectopic ovum begins to develop in the Fallopian tube the placental villi erode the tubal wall and the blood-vessels. At length the ovum slips out of the ampulla—the common result—or the tube bursts. The break may be traumatic in origin, from jarring or a like accident, or it may be spontaneous. If the rupture is through the tube there is hemorrhage into the pelvic cavity; if the ovum slips out of the ampulla the tubal abortion causes hemorrhage as in uterine abortion. In either case the blood with peritoneal fibrin forms a hematocele, and this, with the ovum, may be finally absorbed; or the woman may bleed to death unless the hemorrhage is checked surgically; or the child may live for varying periods up to term. The tube rarely ruptures into the fold of the broad ligament.
The fetus usually dies after rupture or tubal abortion, and if it has not advanced beyond the eighth week it is absorbed. Sometimes it lives. When the rupture or abortion does not tear the placental site the fetus may develop in the abdominal cavity. Between 1889 and 1896 Haines[103] found 40 operations for ectopic gestation done after the seventh month of pregnancy with 10 maternal deaths. Of the children, 27 survived the operation from a few moments to fifteen years. Sittner, in 1903, compiled from the medical reports 142 cases of viable ectopic fetuses, and Essen found 25 additional cases. Since Essen's article more have been reported, about 173 to my knowledge, but the number is considerably larger.
Hirst says an experienced obstetrical specialist sees from 12 to 24 cases of ectopic pregnancy annually. Küstner himself[127] operated on 105 cases in five years. About 78 per cent. of all ectopic gestations result in tubal abortion and 22 per cent. in rupture.
Many specialists now are of the opinion that the diagnosis of ectopic gestation ordinarily is not difficult, but most physicians find it very difficult. Before rupture of the tube or a hemorrhage diagnosis is hardly ever made by any one, and no pelvic condition gives rise to more diagnostic errors. When there is rupture or tubal abortion the symptoms may lead the physician to mistake the condition for uterine abortion. In uterine abortion the onset of the symptoms is quiet, with gradually intensifying and regular pains, resembling labor, in the lower abdomen. In ectopic pregnancy the symptoms of a rupture or tubal abortion arise quickly, with irregular and colicky or very violent pains, localized on one side. In uterine abortion the external hemorrhage is more or less profuse, with clots; in ectopic gestation the external hemorrhage is slight or absent; the shock in the latter case is out of proportion to the visible blood loss. Parts of the ovum, or the presence of the whole ovum, as uterine, are found in ordinary abortion, but in the ectopic condition the ovum proper does not appear. An intrauterine angular pregnancy, or pregnancy in a uterine horn, causing the upper corner of the womb to bulge sidewise, may be mistaken for ectopic gestation. Pregnancy in a retroflexed uterus, tumors of the adnexa, the twisted pedicle of an ovarian tumor, a burst pyosalpinx, an appendicitis in pregnancy, or a combined intrauterine and ectopic gestation, also may confuse the diagnosis. When there is a dangerous hemorrhage from rupture or tubal abortion the diagnosis is usually made without difficulty from the collapse and other signs.
The diagnosis as to whether the fetus in the pelvis is dead or alive may be made (1) from the absence or presence of symptoms of tubal rupture during the second and third months, or of mild symptoms indicating only slight bleeding; (2) from the continuation and progress of the evidences of pregnancy, as nausea, mammary changes, fetal movements, or audibility of the fetal heart; (3) from the presence of a loud uterine blood souffle; (4) from the absence of toxemia or suppuration;[128] (5) from a growth of the uterus and a softening of the cervix; (6) from a gradual increase in the size of the suspected ectopic fetal tumor. In making the diagnosis great caution must be observed, as roughness in manipulation may start hemorrhage or rupture a thinned tube.
The diagnosis may be made: (1) that ectopic gestation exists without symptoms of maternal hemorrhage, and the fetus is not viable; (2) that the same maternal condition may be present, but the fetus is viable; (3) that there may be symptoms of slight bleeding, and the fetus is inviable; (4) that there may be symptoms of grave maternal hemorrhage at any stage of the gestation.
The ordinary medical doctrine in the text-books is that as soon as a diagnosis of ectopic gestation is made laparotomy should be done and the sac with the ectopic fetus removed. If the fetus is alive and inviable this procedure will, of course, kill it. Only a few obstetricians of authority advise an expectant treatment. Schauta found 75 recoveries and 166 maternal deaths in 241 cases treated expectantly—a mortality of 69 per cent.
If there are no symptoms of maternal hemorrhage but the fetus is evidently dead, the fetus is to be removed. If it is evidently alive, or doubtfully alive, the treatment must be expectant. The woman is to be removed to a hospital and kept under constant watch, day and night, with everything prepared for immediate operation. Any woman while bearing an ectopic fetus is in constant grave danger of death, but the moralists hold that her danger is not so imminent before actual rupture as to justify the death of the fetus by precautionary removal.
In 1886 the Archbishop of Cambrai proposed the following list of questions to the Holy Office for decision:
1. May a pregnant woman in danger of death from eclampsia or hemorrhage be prematurely delivered of a viable child?
2. May a woman in the same condition be delivered in urgency by means which will kill the infant?
3. May a woman in articulo mortis be delivered of a[129] viable child if the delivery will somewhat hasten her death?
4. May the woman in question 1 be delivered of an inviable fetus?
5. May the woman in question 3 be delivered of an inviable fetus?
6. May a woman who is about to become blind, paralytic, or insane from her pregnancy be prematurely delivered of a viable child?
7. May the woman in question 6 be delivered by means which will kill the fetus?
8. May the woman in question 6 be delivered of an inviable child?
9. May the woman in question 6 be delivered of an inviable child, supposing the child to be in articulo mortis?
10. May an ectopic fetus be killed by operation, electricity, or poison, to avert possible danger of death from the mother?
11. May a surgeon who has opened the abdomen for some condition not uterine incidentally remove a viable ectopic fetus?
12. With conditions like those in question 11, except that the fetus is not viable, may the surgeon remove the inviable ectopic fetus?
Three years later, August 19, 1889, the Holy Office answered these questions comprehensively: "In Catholic schools it may not be safely taught that craniotomy is licit, as was decided May 28, 1884, or any other surgical operation which directly kills the fetus or the pregnant mother." Safely taught here is a somewhat technical expression which has been interpreted by the Holy Office in another connection as meaning that the act is illicit morally.
The Holy Office, May 4, 1898, again decreed: "Necessitate cogente, licitam esse laparotomiam ad extrahendos e sinu matris ectopicos conceptus, dummodo et foetus et matris vitae, quantum fieri potest, serio et opportune provideatur."[104] This[130] decision was not clearly understood, and on March 5, 1902, the same congregation reported the following question: "Is it ever licit to remove from the maternal pelvis an ectopic fetus which is still immature; that is, which has not yet completed the sixth month after conception?" The answer was, "No; according to the decree of May 4, 1898, which prescribes that the life of the fetus and the mother must as far as possible be carefully safeguarded. As to the time, according to the same decree, the questioner will remember that no premature delivery is permissible unless it is effected at such a time and by those methods which in ordinary circumstances safeguard the life of the mother and fetus."[105]
If the fetus is removed and so killed to avert a threatened danger to the maternal life, but not an actually operative destruction of her life, this removal or homicide is an evil means used to avert the danger. There is no question of a double effect, that is, of two effects, one good and the other evil, coming with equal directness from the cause, which is the removal or killing of the fetus; but of a good effect, the averting of the danger to the mother, issuing from an evil cause, the removal and death of the fetus. A good effect does not justify the use of evil means; it is not permitted morally directly to kill the fetus, as in this case, to save the mother from a threatened grave danger.
The case is not like that of the woman who has an operable cervical cancer while she is bearing an inviable fetus. If the cancerous uterus is not removed the woman will surely die; if it is removed she has a reasonable chance of cure; but if the inviable ectopic fetus is not removed it is by no means certain that the woman will die. In the cancer the uterus is directly removed, the fetus is indirectly killed; in the ectopic case the fetus is directly killed, and the danger to the woman's life is removed as a direct effect of the killing.
Again, the killing of the inviable ectopic fetus cannot be[131] justified by maintaining that the fetus is an unjust aggressor against the life of the mother. An aggressor against life may be such formally or materially. A formally unjust aggressor consciously and voluntarily attacks the life of the victim unjustly. This perversion, or evil, in the aggressor's consciously actuated will sets his own right to life in juridic inferiority to that of the victim's right to life, and the victim may defend his own life, even unto the indirect death of the aggressor in necessity.
The materially unjust aggressor attacks the victim's life unjustly, but whether the aggressor is sane or insane, the attack is not voluntary. When an insane aggressor appears to use his will, such use lacks all moral quality because of the absence of intellect and reason; he wills improperly, as a brute is said to will. In either case, nevertheless, there is active aggression directed against the victim's life, which also sets the aggressor in juridic inferiority to the victim, and permits the victim to defend his own life to extremes. As great an authority as De Lugo holds that in such defence, whether the aggressor is formally or only materially such, the victim may directly kill, but direct killing is never necessary, as it is all a matter of intention.
The ectopic fetus cannot, of course, be a formal aggressor because it cannot exercise either intelligence or will. It is not a materially unjust aggressor, because the only action it is capable of is to increase in size in obedience to the natural law of growth. It is not trying in any manner to tear the maternal blood-vessels. It has a right to its own life and a right to grow. Its growth may finally bring about a maternal hemorrhage, but just now it is not causing that hemorrhage. An aggressor is such only while there is an actual attack going on here and now, directed against the victim's life. The fetus is necessarily passive always, never aggressive in any sense of the term, until the actual rupture occurs. If it may be deemed materially aggressive when the actual rupture is taking place, the question becomes irrelevant, because at that time the fetus may be removed for other reasons altogether. If an insane man is in a room with a loaded revolver which he may[132] not use against me, but which he probably will, I may not kill him in self-defence until he actually begins the aggression. The opinion expressed here is the contrary of the opinion I expressed, in 1906, in Essays in Pastoral Medicine.
The second condition proposed is that the ectopic gestation exists without symptoms of maternal hemorrhage, but the child is viable. In such a case it is probably better to remove the fetus at once, but only a skilled abdominal surgeon should attempt the operation because it is likely to be difficult from adhesions. A viable ectopic fetus is usually deformed. Winckel found 50 per cent. of them deformed—the head in 75 per cent., the pelvic end in 50 per cent., the arms in 40 per cent. Compression, infraction, hydrocephalus, and meningocele are common. The longer the fetus is left in, the worse for the mother so far as peritoneal adhesions and danger and difficulty in removing the fetus are concerned.
The third case supposed that the fetus is not viable but the symptoms of maternal hemorrhage are slight. The danger to the mother in waiting is greater here than in case one, and the decision must be made in keeping with evidences in the particular case. The surgeon who assumes responsibility is obliged to remain ready for instant operation.
Where there are symptoms of grave hemorrhage in the mother at any stage of ectopic gestation the surgeon must operate at once, and ligate the bleeding vessels to save the woman's life. The ligation will shut off the blood supply to the fetus, and thus indirectly, permissively, the fetus must be unavoidably allowed to die. This is a clear case of double effect immediately issuing from the same cause, and the operation is morally licit. No matter how young the fetus is, the surgeon or an assistant is to baptize it; if it is very young it may be necessary to split the envelopes to get at the fetus.
In the cesarean delivery (partus cesareus, celiohysterotomy) the infant is brought out through an opening made in the abdominal and uterine walls. The chief indications for this operation may be a contracted maternal pelvis, an abnormally large fetal head or body, death of the pregnant mother before delivery, certain forms of rigidity of the cervix uteri, some cases of stenosis of the vagina, relative vaginal narrowness, blocking tumors, or a ventrofixed uterus. Sometimes abruptio placentae, eclampsia, placenta praevia, and other accidents of pregnancy are taken as indications for cesarean delivery.
An abnormal bony pelvic girdle is the most frequent obstruction to delivery of the fetus. The lower part of the pelvis, called the pelvis minor or true pelvis, supports the muscles of the pelvic floor, and gives shape and trend to the parturient canal. The inlet and outlet of the true pelvis are narrower than its middle portion and are called the superior and inferior straits. The inlet is somewhat cordate in outline, and normally from front to back, at its so-called conjugata vera, it averages 11 centimetres (45⁄16 inches) in depth; from side to side it measures 13 centimetres (51⁄8 inches); obliquely from the right posteriorly to the left anteriorly it is 121⁄2 centimetres (nearly 5 inches), and the other oblique conjugate is 12 centimetres (43⁄4 inches) long. The transverse diameter of the outlet, from right to left, is 11 centimetres; the diameter from front to back, because the coccyx can be pushed back in labor, is from 91⁄2 (33⁄4 inches) to 12 cm. Normal fetal head measurements average from side to side at the widest part, 91⁄2 cm. (33⁄4 inches); from the root of the nose to the occiput, 11 cm.; from the chin to the occiput, 13 cm.; from the vertex to[134] the neck behind, 91⁄2 cm. The size of the fetal head is the most important factor in delivery, so far as the child is concerned, because, as a rule, when the head is delivered the compressible trunk follows readily. Normally the child presents in delivery with the vertex of the head first; other presentations are transitional, abnormal or pathologic. In 48,499 cases Karl Braun found vertex presentations in 95.9 per cent., and Schroeder in 250,000 cases found an average of 95 per cent. The child's head is "engaged" when its largest diameter has passed the plane of the inlet.
An abnormal pelvis may be generally contracted, dwarfed, in all its diameters; it may be flat or narrow from front to back; it may be contracted from side to side; it may be generally contracted and flat at the same time; it may be obliquely contracted (Nägeli's pelvis); or it may be crowded together irregularly. Rachitis, osteomalacia, curvature of the spine, habit scoliosis, hip dislocation, and similar pathologic states cause these distortions and contractions.
Contraction of the pelvis affects the mother and child in parturition in proportion to the degree of the narrowing. Besides this, the prognosis depends on the size of the child, its presentation, position, and attitude, the strength of the pains, the skill and surgical cleanliness of the operator, and the presence or absence of complications. Obstruction may bring about rupture of the uterus, septicemia, exhaustion and shock, pressure narcosis, or tears of the cervix or vagina. If the child's head becomes impacted the vagina and vulva may become even gangrenous. Pressure may cause areas of necrosis resulting in fistulas into the bladder, rectum, or between the uterus and the vagina. When the contracture is sufficient to let the fetus just engage, pressure may interfere with the placental circulation and kill the child. Compression of the vagus nerve may slow the child's pulse and asphyxiate it through lack of oxygen in the blood. The cord may prolapse. The pressure on the child's head may cause fatal intracranial hemorrhage, or effect permanent injury to the brain.
Often it is extremely difficult to find out the best plan for delivering a woman who has a contracted pelvis. Where[135] the conjugata vera is 9.5 cm. (35⁄8 inches) or above, Ludwig and Savor found that 75 per cent. were delivered without instrumental help. At 9 cm. (31⁄2 inches), 58 per cent. so end; at 8 cm. (33⁄16 inches), 25 per cent. Should the conjugata vera be less than 51⁄2 cm. (23⁄16 inches) in a flat pelvis, or 6 cm. (23⁄8 inches) in a generally contracted pelvis, this is an absolutely contracted pelvis according to the old standard, and the delivery must be by cesarean section, whether the child is living or dead. The minimal requirements have been gradually extended. In 1901 Williams of Johns Hopkins University advocated that the absolute indication for cesarean section be changed to 7 cm. in the generally contracted pelvis, and to 7.5 cm. in the simple flat pelvis. His opinion was accepted by Webster, Jewett, Edgar, and others. Now some obstetricians of authority extend the measurements to 8 cm. If the woman is seen before labor, or early in labor, cesarean delivery alone is done. When the uterus is infected it is usually necessary to remove it after taking away the child, because an infected uterus left in place causes death by sepsis, as a rule.
Text-books on obstetrics have a series of rules, based on pelvic measurements, concerning the indications for cesarean or other methods of delivery in cases of contracted pelvis, but the problems are not so simple and uniform as to be always accurately solved by the data derived from measurements. One woman with a contracted pelvis may require cesarean delivery; another woman with the same measurements may have a normal parturition because the child happens to be small or its skull compressible. The best pelvic measurement is made with the fetal head. A difficult decision as to whether a cesarean delivery is necessary or not comes up in the majority of cases in primiparae; in multiparae the physician has the experience from former births to guide him. In over 90 per cent. of primiparae the fetal head normally is found engaged in the pelvis in the last week of gestation, and can be felt by a vaginal examination. In multiparae the head usually is not engaged until labor begins. If the fetal head does not engage in a primipara, this fact at once suggests an absolutely or relatively[136] narrow pelvis. When labor has begun, if the fetal head cannot be pushed into the true pelvis of a primipara, especially after anesthesia, the necessity for cesarean delivery may be clearly evident.
In the cases where there is doubt that the child can get through the pelvis, but good reason to think that it can, many obstetrical experts try the effect of labor for two hours or a little more, and if there is no real progress they deliver through laparotomy. There is considerable objection now to version or the application of high forceps, but many skilful men prefer these methods at times. When version has been done and it fails there is no chance to save the child's life. In the trial of labor, the expectant treatment, extraordinary watchfulness is required and a full knowledge of the special procedure that may be necessary.
In minor degrees of pelvic contraction the obstetrical practice is either to induce premature labor at the thirty-second week, or to deliver by a cesarean operation, or to delay and try labor. In the last event there may be one of the following issues: spontaneous delivery, version and delivery, extraction by high forceps, cesarean delivery, symphyseotomy, hebosteotomy, or craniotomy. Craniotomy on a living child is never to be considered under any circumstances. Symphyseotomy is a cutting of the maternal pelvic girdle through the symphysis pubis, the rigid joint at the front middle part of the pelvis, and thus letting the bony girdle dilate. Hebosteotomy or pubiotomy is a sawing through the pelvis near that joint to get the dilatation. Symphyseotomy has been replaced by hebosteotomy because the maternal mortality and morbidity are somewhat lessened by the latter method. Schläfli in 1908 reported 700 hebosteotomies with a maternal mortality of 4.96 per cent. and a fetal of 9.18 per cent. Other operators have a better average; still others a worse. This operation is done very seldom of late except in a case where the fetal head is caught low in the pelvis, or there is a chin-posterior or brow or face presentation, and the cesarean operation would not deliver the child.
The varieties of the cesarean delivery as practised at present[137] are the classic cesarean, called also celiohysterotomy, the Porro cesarean, or celiohysterectomy, where the uterus is removed after the extraction of the child, and the two sections in the cervical end of the uterus, viz., the extraperitoneal cesarean and the transperitoneal cervical cesarean. Before the days of antiseptic surgery cesarean delivery was practically always fatal to the mother. Tarnier could not find one successful outcome for the mother in Paris during the nineteenth century up to his own time, and Spaeth said the same for Vienna up to 1877. In 1877 Porro of Pavia advised the supravaginal amputation of the uterus after the child was delivered to avoid hemorrhage and peritoneal infection. This operation replaced the classic cesarean until 1882, when Sänger invented a suture which would keep the uterine incision shut, and applied antisepsis. Sänger's operation has been improved so much that cesarean delivery, when performed by skilled obstetricians, has an extremely low mortality in cases which have not been infected. Routh, in 1910, collected the statistics of Great Britain, comprising 1282 cases, which may be taken as a standard for all civilized countries, and he found a steady decrease in the mortality until now it is near 2 per cent. in uninfected cases. The dangers in the operation increase with every hour the woman is in labor, but even then the general mortality is now down to about 8.1 per cent. This, it must be remembered, is the rate when competent men operate.
When the ordinary practitioner in small cities, towns, and country places operates the mortality is very high. Newell[106] said that in four cities of from 25,000 to 40,000 inhabitants within forty miles of Boston he collected the following data: in A no patient on whom cesarean section had been done is known to have recovered—a mortality of 100 per cent. In B the mortality is from 60 to 70 per cent. In C the operation is invariably fatal when done by the local surgeons. In D the fatality is from 10 to 20 per cent. in average cases, but since cesarean section has become popular as a method of treatment for eclampsia the mortality is over 50 per cent.
In spite of perfect technic by the best obstetricians, the operation has a high morbidity: fever, peritonitis, pneumonia, dilatation of the stomach, and other bad results are common.
Before antiseptic surgery began, opening the abdominal cavity was almost always fatal, and some obstetricians tried to get the child out of the uterus in cases where cesarean delivery is indicated by going in above the pelvis without opening the peritoneum. The uterus was incised near its cervical end. This method, called extraperitoneal cesarean delivery, has been restored for use in cases where there is some infection of the uterus and the operator wishes to save the child without removing the womb. The technic is more difficult than in the classic cesarean, and the operation was not kindly received, but of late some men are having so much success with it that it is reviving, and rightly so. Baisch[107] says that the first eleven women he delivered by extraperitoneal cesarean section recovered more readily than they would from an ordinary laparotomy. In nineteen cases of transperitoneal but cervical section he had no trouble, and six of these were infected cases. The technic of this low incision protects the peritoneal cavity better than the classic incision, apparently. Two of the nineteen women were in slight fever and the uterine fluids were fetid. Two primiparae forty years of age had been in labor seventy hours. Eight of the women were able to leave the clinic on the tenth day. Only one child was lost, and that was a delayed case. Hofmeier[108] compiled 194 cases of transperitoneal cervical cesarean section with three deaths. Küstner did 110 extraperitoneal cesarean sections with no mortality. This makes 304 cases of cesarean cervical section, not the classic operation, with only three deaths, less than 1 per cent. mortality; and fully 50 per cent. of these cases were not surgically clean. From these statistics it is evident that the cervical operation in the hands of competent surgeons should be the operation of choice.
The ordinary practitioner, however, is utterly unfitted to do a cesarean section of any kind. In large cities it is easy[139] to find a trained surgeon to do the operation, but in small towns and in country places there is seldom any one available. The physician who chooses to practise medicine in an isolated place knows that he will almost certainly be called upon to do a cesarean section some day, and he should not take up the responsibility of the general practitioner in such a place until he is competent to do that operation when life depends upon him. This is as things should be; but unfortunately a man who is trained well enough to do major surgery will not live in a small town if he can get into a large city. The physician in any case should be able at least to make the diagnosis in time, before labor sets in, and have the woman sent to the nearest city, if possible. Dr. Bull[109] reported that he had traveled seventy-five miles to see a woman who was having severe hemorrhages at term. He found her in a log cabin, with a centrally implanted placenta (i.e., right across the opening of the cervix uteri), and she had had three hemorrhages before his arrival. He narcotized her, took her in a train to a hospital, delivered her by cesarean section, and saved her and the child. If he had delivered her by version in the log cabin, he would almost certainly have lost both the mother and the child.
The question of removing the uterus comes up when the uterus is infected, or as a method of sterilizing the woman to avoid the danger of a subsequent gestation. Whenever a uterus is gravely infected and a cesarean delivery is finally necessary, the infection is commonly due to ignorance or carelessness, and the physician or midwife is guilty. There should be no such business as that of the midwife who actually delivers the patient. The state should provide physicians for the poor. Even the midwife who calls herself "a practical nurse," but who is not a licensed trained nurse, is commonly a public danger, although some so-called practical nurses are better than the ordinary trained nurses.
Suppose, however, that the uterus is infected unavoidably. If this infection has been done by a competent obstetrician working in a hospital with sterile instruments, it may be safe to deliver the woman by an extraperitoneal or cervical trans-peritoneal[140] cesarean section. If the practitioner has tried to deliver the woman at her home with forceps and has failed, especially if repeated attempts have been made by the physician and an assistant or consultant, the uterus should be amputated. It will not do to deliver by a low cesarean and await developments, because if the infection is serious no subsequent removal of the uterus will save the woman's life. The grave mutilation of removing the uterus is, of course, licit, as it is the only means of saving the woman's life. Some moralists hold that a woman from whom the uterus has been removed is impotent, but this question has never been decided authoritatively, as we shall show in the chapter on Vasectomy; and until it has been so decided the woman must be given the benefit of the doubt.
The question of removing the uterus solely to prevent the danger of subsequent deliveries differs from the condition just considered. If the woman has had a cesarean delivery for an absolutely narrow pelvis, her subsequent deliveries must be by the same method. After a cesarean section there is more or less danger of rupture at the scar in other labors. Some think the danger is greater if the placenta becomes implanted on the scar; others think this implantation does not weaken a good scar. If the convalescence after the cesarean section already done has been abnormal, the prognosis for rupture is not good. Where there has been an abnormal convalescence, each new pregnancy must be watched closely, and often an early subsequent cesarean is indicated to prevent rupture. No matter how well the section has been done, latent gonorrhea may prevent perfect healing of the wound. Twins, hydramnios, and overtime gestation are other causes of rupture. The tendency with obstetricians in the future will probably be to do the section toward the cervical end of the uterus; and as the uterus is thinnest there, it might be thought that it will be more likely to break, but Spalding[110] found the contrary true—the rupturing was usually in the thick part of the uterus. Version, high forceps, uterine tampons, hydrostatic bags, and pituitary extract should be avoided where an old cesarean scar exists, but[141] Vogt and Kroback have done version a few times without rupture. Vogt had one patient with a true conjugate of 63⁄4 cm. (28⁄16 inches) to 7 cm. (23⁄4 inches). She was delivered in the first three labors by craniotomy; in the fourth by version; in the fifth and sixth by cesarean section; in the seventh she had twins one of which was born spontaneously; in the eighth by version and perforation of the after-coming head; in the ninth she refused operation and was delivered spontaneously. Skilful operators have the fewest ruptures after cesarean delivery. Olshausen had one in 120 cases, Leopold none in 232 cases, Schauta none in 177 cases, Küstner none in 100 cases. Olshausen, in a series of 29 cases, operated on two patients twice and upon three patients three times. As early as 1875, Nancrede of Philadelphia had operated the sixth time on the same woman. In such cases the uterus is commonly so broadly attached by adhesions to the belly-wall that it is opened without getting into the peritoneal cavity. In 150 cases of repeated section collected by Polak in 1909 the mortality was only 5 per cent.
A woman may not be sterilized by having the uterus removed, by fallectomy, or otherwise, solely to obviate danger or morbidity from subsequent pregnancies and cesarean deliveries. Such a sterilization would be a grave mutilation without a present excusing danger, and it would render the primary end of marriage always impossible. Such sterilization of a woman is in contravention to the decretal of Gregory[111] as given in the chapter on Vasectomy. It is also against the bull Effraenatam of Sixtus V., who extended all penalties prescribed for abortionists to those who give women drugs which cause sterility, and to those who purposely prevent the development of the fetus or in any manner abet the deed; and the penalties are to be applied to the women themselves who willingly use these means. These penalties are enumerated in the chapter on Abortion. The Congregation of the Holy Office, May 22, 1895, answered negatively the following question: "Si sia lecita la practica sia attiva sia passiva di un procedimento il[142] quale si propone intenzionalmente come fine espresso la sterilizatione della donne?"[112]
The reason for these laws is that any act which deprives one of the power to generate, and which prevents conception and makes the semen fail of its end, is against the chief intrinsic end of marriage and any benefit that arises therefrom, which is the good of offspring. The act is also against the intrinsic end of the semen, which is to generate; and since the semen cannot possibly effect its end, the conjugal act degenerates into an equivalent of onanism. This act of sterilization, done not to save the whole body from immediate danger, is intrinsically evil, and therefore unjustifiable.
To say that marriage is also a licit remedy of concupiscence is no excuse. Marriage is such only in a secondary sense, and this secondary end is necessarily subordinate to the primary end, and coexistent with that primary end, which is the generation of children. Even when a surgeon is doing a Porro operation, his main intention may not be to sterilize the woman. He must directly intend to save her life by removing the infected uterus, and reluctantly permit the sterilization as an evil part of the double effect coming from the causal amputation.
Cesarean delivery is used frequently of late in placenta praevia. It may be necessary also in abruptio placentae, gunshot wounds of the abdomen during pregnancy, sometimes in appendicitis complicating gestation, rarely in prolapse of the cord to save the child, and when twins become interlocked in delivery. Placenta praevia is a development of the placenta in that part of the uterus which dilates at the end of gestation or during delivery. This dilatation, with the mechanical pressure of the child, detaches the placenta enough to cause a hemorrhage which may be fatal to the woman if not checked. The hemorrhages begin sometimes as early as the sixth month of gestation, but most frequently in the eighth month. Premature labor is a common effect. The position of the placenta may cause malposition of the fetus, prolapse of the cord, weak pains, air embolism into the blood, rupture of the uterus, sepsis, profound anemia, and other evils. The child may be premature, puny, have collapsed lungs, hemorrhages, and it is very likely to be killed in delivery. The mortality of the women varies, but it averages about 7 per cent; that of the children averages 61 per cent.
The tendency with obstetricians is to deliver the child as soon as the diagnosis has been made. When the bleeding is slight, and the child is viable, one may delay delivery provided the woman will remain in bed in a good maternity hospital without moving. At home the woman may "flood" and bleed to death before a physician can reach her. If the woman refuses to go to a hospital, and to permit the induction of labor, any physician who has regard for his own reputation will drop the case and leave the woman to her own devices.
There are various methods of treatment, and much depends on the position of the abnormally placed placenta. The treatments all consist in stopping the hemorrhage for the instant, emptying the uterus, insuring permanent hemostasis, and meeting the anemia. The Braxton-Hicks version is one method. The child is quickly turned so that the head is upward in the uterus, and a leg is pulled down to plug the cervix uteri until there is enough dilatation to extract the child. Very many children are lost by this method. When the placenta praevia is marginal to the cervix or lateral in the uterus the child has a better chance when a colpeurynter, or inflatable rubber bag, is inserted in the cervix as a plug. Much skill and discrimination is required in the management of this bag until the child is delivered. The obstetrician may be obliged to sit by the bed and hold on to the bag for from three to twelve hours. Hasty extraction through a poorly dilated cervix is a very dangerous process, as a tear cannot be repaired quickly enough, as a rule, to check the hemorrhage, which will be fatal. When version has been done haste may compress the head in the tight cervix and asphyxiate the child.
When the child is viable a cesarean section is by far the best method for the child, as it lowers the fetal mortality from 61 to about 5 per cent. The mother, too, has a better chance by the cesarean section, provided it is done by a competent man, early in labor before infection has set in, and in a hospital.
If the child is not viable the hemorrhage must be stopped to save the woman's life. As a rule, the hemorrhages are not dangerous before the seventh month. In the 128 deaths of Müller's statistics there was not one before the seventh month of gestation. Hirst, however, says he has been obliged to empty the uterus at the fifth month for placenta praevia. The woman must be kept in bed, the foot of the bed elevated, sedatives used, and so on, as in threatened abortion, and the vagina tamponed securely with cotton. If it is evident that the fetus is dead, it must be extracted as in the case of a viable fetus. If it is probable that the fetus is alive, it is to be treated as in a case of inevitable abortion as described in the[145] chapter on Abortion. The tamponing of the vagina to stop the hemorrhage will cause the abortion of the fetus indirectly. This is another double-effect case, and the tamponing is morally permissible provided the intention is correct.
Abruptio placentae is a tearing loose of a placenta which is situated in the normal position, not abnormally as in placenta praevia. The cause may be a disease of the placenta or decidua; for example, syphilis, chronic metritis, traumatism from a blow or fall, jumping from a carriage-step, and so on. Nephritis is often found where there is abruptio placentae. In labor the placenta may be torn loose by a version, by the delivery of the first of a pair of twins, or because the cord is too short.
There is always profuse hemorrhage, which is usually concealed at first, but finally external. It is possible at times for a woman to bleed to death into her own uterus, when it is distensible. The mortality is about 50 per cent. for the women, and where there is concealed hemorrhage about 95 per cent. of the children are lost. A differential diagnosis is to be made to exclude placenta praevia, rupture of the uterus, extrauterine pregnancy, rupture of an appendical abscess, gall-stone colic, or intraäbdominal injury.
If the child is viable it must be delivered as quickly as possible. If it is dead and the head is developed, craniotomy should be done to hasten extraction. When the abruptio takes place before the seventh month of gestation the fetus will die in about ten minutes, whether in the uterus or outside it; no matter what method might be adopted to empty the uterus, the child would be dead before delivery. The diagnosis would have to be made and instruments prepared, and this would take up more than the ten minutes of life left to the fetus. It is necessary to get the fetus out to stop the bleeding of the open sinuses by contraction of the uterus.
The removal of the fetus here is not like an artificial abortion. In abortion the abortionist separates the placenta from the uterine sinuses and so kills the fetus; the removal from the uterus is secondary to that separation which kills. The common notion of moralists that death is caused in abortion by[146] taking the child out of the uterus is inexact—tearing loose the placenta is the real cause. In a removal of the fetus after an abruptio placentae the death of the fetus is not caused by the physician at all, but by the force that effected the abruptio. As the child will be dead before sufficient dilatation of the cervix to deliver it can be attained, there is no objection to beginning the delivery as soon as the diagnosis is clear.
Tumors in or near the uterus may be obstacles to delivery or they may through malignancy endanger the woman's life. The commonest tumors complicating pregnancy are fibroids, cancers, and ovarian tumors, especially cysts and dermoids, but tumors of other kinds are not frequently met. Schauta, in 111,112 pregnant women, found fibroids in 86, one in 1292 cases; Pinard, in 13,915, found 84, one in 165 cases; Pozzi, in 12,050, had 83, one in 133 cases; in St. Petersburg, in 13,076 deliveries, there were only 4, one in 3269 cases; and in the Charité in Berlin, 6 in 19,052 births, one in 3175 cases. The ovarian cyst in pregnancy is rarer than the fibroid—5 in 17,832 births, one in 3566 cases, in the Berlin Frauenklinik. Cancer of the cervix also seldom appears—once in about 2000 cases. Other very rare conditions, related to these, are polyps of the cervix, enlarged and prolapsed kidneys, extrauterine pregnancy combined with intrauterine, echinococcus cysts, parametric abscesses, cancers of the rectum, rectal strictures, tumors of the bladder, stones in the bladder, tumors of the pelvic bones or cartilages, and tumors of the vagina or vulva.
Fibroids, called also fibromyomata, fibromata, and myomata, in the uterine muscle or adnexa commonly enlarge during pregnancy, and if they are big enough and low in the pelvis may block the parturient canal. These tumors may suppurate, grow gangrenous, or take on red degeneration; they may cause abortion, peritoneal adhesions, pain, or hemorrhage; simulate threatened abortion; bring on retroflexion of the uterus, placenta praevia, abnormal presentations, sometimes weak pains or pains so strong as to rupture the uterus, and they may check contraction after delivery so as to start hemorrhage. They[148] may so kink the uterus as to incarcerate the placenta and cause sepsis. The percentage of degeneration in fibroids taken generally is 22, according to William Mayo.[113]
Myomata often obscure the diagnosis in pregnancy. The tumor may be mistaken for a twin child, or vice versa. A large symmetrical interstitial myoma may be mistaken for pregnancy, or vice versa. Sometimes, even after the belly has been opened, it is difficult to be sure whether the condition is pregnancy or a tumor. As eminent a surgeon as Deaver says this diagnosis cannot always be made by any one no matter what his experience.
We cannot give a general mortality average for myomata in pregnancy because only bad cases are reported, but in bad cases the mortality is very high—50 per cent. for the mother and about 60 per cent. for the children, with almost 30 per cent. of abortions. The majority of women who have myomata go on to delivery without trouble. In some there is much pain or hemorrhage, and these conditions may finally oblige the obstetrician to operate, but the operation should be deferred as long as possible. Where there are signs of necrosis of the tumor, operation is necessary at once to prevent sepsis. Removal of a myoma during pregnancy does not always cause abortion. The statistics are that about 83 per cent. of those operated upon are removed without abortion. In the Mayo Clinic[114] fourteen cases of degenerating fibroids in pregnant wombs were removed and the majority went on to term. The removal is always a very bloody operation, and it requires great surgical skill. Where enucleation of the tumor alone was intended it may finally become necessary to amputate the uterus to stop hemorrhage.
When the case has gone on to labor at term the diagnosis as to position and size of the tumor is to be made, and what the effects will be as to blocking the canal or crushing the tumor so as to bring on sloughing. If a tumor blocking the canal cannot be pushed up out of the way of the child, a cesarean section should be done immediately. In such an outcome as[149] section the experience of the operator must decide whether the tumor is to be removed then or at a more favorable opportunity. It may be necessary to do cesarean section to liberate an incarcerated placenta.
Sometimes the fetus is so involved with a gangrenous myoma that enucleation of the tumor will kill or hasten the death of the fetus. When, in such a complication, it is evident that the life of the woman depends on the immediate removal of the tumor, yet a second but evil effect follows from the operation, namely, the unavoidable death of the fetus, the removal is morally licit provided the operator has the proper intention. The death of the child as an effect in this case is only indirectly voluntary from the physical point of view, and only permissively voluntary from the moral aspect.[115]
Ovarian tumors in pregnancy are, as has been said, rarer than myomata. Such tumors are mostly cysts and dermoids. In 862 cases collected by MacKerron, 68 per cent. were cysts, 23 per cent. dermoids, 5 per cent. malignant tumors, and a few were myomata. Cysts and dermoids do not, like the myomata, grow bigger during pregnancy, but they may hinder delivery or grow gangrenous and septic. When treated early the mortality in pregnancy is from 2.1 to 5.9 per cent for the women, but delay gives a maternal mortality of from 31 to 39 per cent. The fetal mortality in Heiberg's statistics of 271 cases was 66 per cent.
Most obstetricians advise the removal of an ovarian tumor in pregnancy as soon as diagnosed, provided it is of a size to cause difficulty in parturition, but such a removal causes abortion in over 20 per cent. of the cases. The expectant treatment causes abortion in about 17 per cent. If the child is viable, Fehling, Martin, Norris, and De Lee are in favor of the expectant treatment. Late operators leave weak scars at labor. When there are symptoms of torsion of the pedicle of the tumor, infection, incarceration in the pelvis, involvement of the uterine broad ligament, or overdistention of the belly, the tumor[150] must be removed immediately. Whether vaginal puncture or laparotomy is the better method is to be decided particularly. Dermoid cysts are likely to bring on sepsis if they are broken in enucleation, and the diagnosis and operation must be carefully made. When it is necessary to save the life of the woman to remove an ovarian tumor, the risk of abortion may be taken permissively.
Cancers of the cervix uteri are always malignant and cause death if they are not removed before they have gone on to metastasis. As this tumor commonly appears after the child-bearing age, it is rare in pregnancy; the ordinary ratio is one in 2000 deliveries, but De Lee saw only one in Chicago in 16,000 consecutive labors. Abortion occurs in from 30 to 40 per cent. of the cases. Spontaneous rupture of the uterus may happen, and placenta praevia is frequent relatively. Pregnancy hastens the growth and spread of cancer very much. Eight per cent. of the women die undelivered, and 43 per cent. die during labor or immediately afterward. Of all uterine cancers, 80 per cent. are cervical.
The diagnosis should be as certain as possible. Rarely nodules which are not cancerous appear in the cervix during pregnancy, and these are to be examined microscopically. Snipping out of a piece of the nodule for examination does not cause abortion. Vaughan of Michigan University, who is a skilful and careful observer, said[116] that in an investigation of 200 cases of cancer, upon which more than 30,000 differential blood-counts were made, he discovered a method of diagnosing the operability of a cancer as follows: He makes a blood-count and then injects intraperitoneally one c.c. of placental residue. The next day he begins a series of blood-counts, and if the number of polymorphonuclear cells decreases the case is operable, no metastasis has occurred; if there is no change in the number of the polymorphonuclears, or an increase with a corresponding decrease of the large mononuclears, the case is inoperable, metastasis has begun.
In cancer of the cervix operability does not mean curability always. Inoperability signifies that the woman has no chance[151] at all for life and that it is useless to do anything; operability means that she has one chance in four and that it is worth while taking the chance. The following conditions may be met:
1. The case may be operable and the child inviable.
2. The case may be operable and the child viable.
3. The case may be inoperable and the child inviable.
4. The case may be inoperable and the child viable.
In the first case the supposition is that the case is operable but the child inviable. To save the woman the uterus, with its adnexa, must be removed, and this, of course, kills the fetus. The case differs from the enucleation of a gangrenous myoma which involves the death of an inviable fetus. In the myoma case the woman has practically every chance for her life through operation; in this cancer case the woman has only one chance in four, as 75 per cent. of such operations fail through recurrence of the cancer.
The child has about one chance in two of going on to viability, owing to the tendency to abortion, if no operation is done; but the mother loses her chance for life if the operation is not done at once, as the cancer will spread beyond cure. Zweifel has seen such a growth extend a finger's breadth in one week. The one chance in four in immediate operation gives the mother a solid ground for hope, and the probability is sufficient, in my opinion, to permit the operation with a permissive loss of the fetus.
In the second case the cancer is operable and the child is viable. The child should at once be delivered by cesarean section, and the uterus with its adnexa removed.
The third case is that of an inoperable cancer and an inviable child. There the operation should be deferred, if possible, until the child becomes viable.
The fourth case supposes the cancer is inoperable but the child viable. In the interest of the child, immediate cesarean section is the best thing to do; it is much better than waiting until term. At term this operation will have to be done anyhow, and the earlier it is done, the better the woman can stand the strain. There is a risk that she will die from the[152] first operation done to deliver the viable child, but she may licitly take this risk, as she might licitly run into a burning house to save a child, even if not her own. She may also licitly refuse the first operation.
Primary appendicitis in pregnancy is very rare; recurrent appendicitis is not so rare. When appendicitis goes on to suppuration and perforative peritonitis the condition is worse in pregnant women than in the non-pregnant. In pregnancy protective adhesions, walling off, are less likely to occur; the inflammation is more intense owing to increased vascularity; thrombosis and phlebitis are more frequent; drainage may be obstructed and the burrowing of pus widespread; tympany, too, causes dyspnoea earlier. About 75 per cent. of the cases occur after the third month, and the earlier the appendicitis appears, the better the prognosis. During labor the contracting uterus sometimes tears open an adhesive appendix, or ruptures a pus sac and starts a general peritonitis. This condition may be mistaken for a general sepsis which is puerperal. Acute appendicitis is likely to be confused with an inflammation of a Fallopian tube. When the appendicitis is perforative abortion, infection of the uterine contents and death of the child happen in most cases. Labor is very painful when appendicitis is present, and the uterine contractions are often weak. After delivery many forms of infection of the uterus and its adnexa are possible.
Operation is much less difficult in the first half of gestation than in the latter months. At the beginning of gestation the operation does not, as a rule, cause abortion. Late in pregnancy appendicitis rapidly goes on to suppuration and perforation, with a high mortality. Hirst says that where there is reason to suspect suppuration a median incision should be made and the pelvic cavity examined for possible areas of infection. John Deaver says, "Always cut down on the sore[154] spot and do not handle the uterus." An infected uterus after cesarean section complicated with appendicitis has to be amputated.
The diagnosis between appendicitis, ectopic gestation, twisted ovarian tumors, ureteritis, and ureteral stone is to be made. In a discussion of a paper by Finley on Appendicitis in Pregnancy,[117] Dr. John Murphy of Chicago, a great authority, advised operation as soon as the diagnosis is made, and he was of the opinion that this diagnosis is not difficult to make in pregnancy. Deaver said a diagnosis of catarrhal appendicitis is not seldom very difficult to make. This form is very rare in pregnancy. Deaver is not of the same opinion as Murphy as to operating as soon as the diagnosis is made in all cases. Where there is a general peritonitis, operation commonly only makes matters worse by spreading infection. The mortality of cases of appendicitis in pregnancy left without operation is as high as 77 per cent.; where the cases are operated upon within forty-eight hours after diagnosis the mortality is 6.7 per cent. and it would be better if the operation were done within twenty-four hours. Finley says that in the fifteen cases reviewed in his paper the operation did not cause abortion. Deaver tells us the muscular rigidity in the right groin characteristic of appendicitis is often missing in pregnancy, and that sometimes the pain is on the left side of the belly.
From 8 to 10 per cent. of all insanity in women develops during the puerperium—the incidence is about one case to 400 births. Puerperal insanity in nearly 70 per cent. of the cases begins within the first two weeks after parturition. Next in frequency of occurrence is the period of lactation, especially in multiparae. Insanity during pregnancy itself is relatively rare, and it begins usually after the fourth month.
As in other forms of insanity, hereditary predisposition is found in from 25 to 30 per cent. of the cases. Alcoholism, sepsis, and neuroses like hysteria, chorea, and epilepsy, are the predisposing elements. The most common immediate exciting cause during pregnancy is toxemia from faulty metabolism and excretion. Other frequent direct excitants are mental worry from poverty, desertion, seduction, and the like troubles.
Prolongation of the lactation period beyond the usual time for weaning, from the ninth to the twelfth month, is common among ignorant and lazy women. Some women prolong lactation in the erroneous notion that it prevents renewed impregnation. Such lactation is injurious to the child, as a rule. Ploss says hyperlactation is frequent in Spain, and that some Japanese, Chinese, and Armenian women may nurse their children for years, but this practice is undoubtedly injurious, especially among European races. The women get tabes lactea with emaciation, asthenia, anemia, backache, pain in the breasts, neurasthenia, cramps, and blindness. The uterus atrophies in some cases and may be permanently injured. Insanity is not unusual.
The forms of mental disturbance commonest in puerperal insanity are mania with or without delirium, melancholia, and[156] dementia. Dementia is the final stage in the cases that become chronic. Mania is the prevailing type in insanity after labor, and melancholia in insanity during gestation. The melancholy of insanity during gestation is often suicidal, and must always be watched. Religious and erotic symptoms are also observed.
The onset may be very sudden during labor. An outbreak after labor may be suicidal or homicidal. Maniacal puerperal women are dangerous. They have delusions and hallucinations, with very rapid and incessant changes that range from obscenity to prayer. Melancholy in the puerperium is likely to be suicidal.
About 75 per cent. of puerperal insanity cases recover within five or six months. From 2 to 10 per cent. die from sepsis, exhaustion, or intercurrent diseases; the remainder become permanently insane. The nearer the delivery the insanity appears, the better the prognosis. Menzies found that of cases which began during gestation 56.7 per cent. remained insane; of those that began during the puerperium 25 per cent. did not recover; of those that began during lactation 43.5 per cent. remained insane. Melancholia is more favorable than mania in pregnancy, but after labor mania gives the better prognosis. The maniacal patient is more likely to die, but the melancholic is more likely to remain insane. The older the woman, the greater the number of her pregnancies, the more the depression, and the higher the temperature, the worse the prognosis. Alcoholism is an added risk always.
All puerperal insanities should be treated in sanatoria or asylums and not at home. When a woman with puerperal insanity is allowed to remain at home she cannot get proper treatment, and is a constant menace to her own life and the lives of her family.
A woman who has had puerperal insanity and has recovered her mental health is likely to have a recurrence of her malady at subsequent pregnancies. The question has been asked me a few times, "Would it not be justifiable to sterilize such a woman to prevent this recurrence, with its dangers and terrors?"
It would not be justifiable: 1. Because it is not licit to[157] inflict a grave mutilation to avert a possible or probable future evil. 2. There are other means to escape the danger: a woman with this tendency is justified in denying the debitum. 3. Once crazy, always crazy, is an aphorism with much truth in it, and it is doubtful that sterilization in itself will prevent ultimate insanity. 4. The conjugal relation of a sterilized woman would be no better than onanistic. 5. The sterilization would fall under the decrees and penalties described at the end of the chapter on Cesarean Section.
In pregnancy the kidneys always give evidence of a constant congestion, and the chief symptom of this is the great quantity of renal epithelium shed with the urine. This engorgement has given rise to the term "kidney of pregnancy." There has been much discussion of this condition, especially as to the possibility of differentiating it from beginning nephritis. In 227 consecutive cases of pregnancy in which the urine was examined at short intervals by myself throughout the entire gestation, there was always an enormous quantity of epithelium, and this presence of epithelium is so constant that its absence is a proof that pregnancy does not exist. It is as physiological as any other somatic change in the puerperium. Von Leyden and other German observers look upon the degenerative alteration in the epithelium of the renal tubules as pathological, but apparently more definite symptoms are necessary to make a diagnosis of significant nephritis.
Williams[118] says that in the examination of 1000 pregnant women at Johns Hopkins Hospital in Baltimore traces of albumin were found in 50 per cent. without subsequent serious disturbance, but where considerable albumin with casts other than hyaline was seen there were symptoms of toxemia later, and several of these went on into eclampsia. Fisher[119] held that red blood-corpuscles in these cases indicate acute nephritis; and granular and epithelial casts, chronic nephritis. Like the Johns Hopkins cases, he found albumin in 50 per cent. of his patients. Albumin in slight quantities is found to be extremely common toward the end of pregnancy. Meyer,[120] in an extensive[159] study of the kidney in pregnancy, made at Copenhagen, found albumin in 5.4 per cent. of the women. During the last month of gestation 71 per cent. of the women showed albumin. Premature births occurred in 8 per cent. of the patients who had had albuminuria, but in 21.5 per cent. of the women who had had casts. Delicate tests for albumin are used by men who find these high averages, as a few leucocytes from leucorrhoea will give the reaction. Most of these cases have no clinical significance.
It is usually impossible to differentiate in pregnancy a lighting up of an old nephritis from a toxemia. Where there is a history of nephritis before the pregnancy, this often clears up the diagnosis. Nephritis is likely to manifest itself in pregnancy earlier than toxemia; albuminuric retinitis is commoner in nephritis, but these facts are no real help in differentiation.
The position of the uterus may be a cause of nephritis, according to the American Text-Book of Obstetrics; but De Lee and others hold that the growing womb cannot possibly be a cause. Many other origins have been suggested, but without sufficient proof.
The treatment of the nephritides of pregnancy is that described in chap. xiii for eclamptic symptoms. When albuminuric retinitis occurs, the medical tendency is to empty the uterus. All text-books counsel this procedure, but they give no convincing reasons for the advice. If the child is viable the therapeutic abortion might be done when necessary; if the child is not viable the operation is, of course, not licit. In the nephritis of pregnancy it is not certain that emptying the uterus artificially, with the entailed shock, is the best method of treatment; but, as a rule, nephritis is made worse by pregnancy, and the irritation lessens with the termination of gestation in some cases, but not in true chronic nephritis. Eclampsia is more toxic than nephritis, and the treatment may differ in important details: it certainly is doubtful that artificial abortion in eclampsia is the method of choice at present. I saw a case of albuminuric retinitis ten years ago, which could not have been worse. The woman was in the seventh month of gestation;[160] she was nearly blind and half comatose. The albumin in her urine always was so great that it would not fully precipitate in a centrifuge tube, and every field under the microscope was covered with large casts in such enormous quantities that they were felted together. Yet the woman was carried on to term by Dr. Joseph O'Malley and delivered of a fully developed child. She since has had two other children at term who are perfectly healthy, and she herself could pass a life insurance examination. This is, of course, only one case, and it is exceptional; but it is impossible to say what will happen in any particular case—whether it will go on to death or recovery.
Both subacute and chronic parenchymatous nephritis show clinically much albumin, many casts, marked edema (except in very emaciated cases), absence of high blood-pressure, and the heart is not enlarged. This condition is caused commonly by chronic tuberculosis, syphilis, sepsis, and malignant tumors. With these clinical symptoms and the history, we may differentiate the nephritis of pregnancy from Bright's disease. Again, acute intestinal nephritis or glomerulonephritis has urinary findings like the nephritides just described, and there may be edema. The heart and the blood-vessels are normal. The cause is usually a pus microörganism, and there may be anemia from the sepsis. In subacute glomerulonephritis, or intestinal nephritis, the urinary findings are marked (much albumin and many casts), anemia is rather constant, the blood-pressure gradually goes up to 180 or 200, edema may be marked or absent. The cause is usually a pus microörganism. Chronic glomerulonephritis shows much epithelium and many casts (sometimes in showers), the blood-pressure is high, the heart is usually somewhat enlarged, there is polyuria and some blood, edema is common (but there are dry cases), albuminuric retinitis is rare, and anemia is marked and secondary. It may be difficult to find the cause of this chronic glomerulonephritis, but there is, as a rule, a history of tonsillitis, septic rheumatism, endocarditis, a true influenza, or the like infection. Primary arteriosclerotic contracted kidney shows hypertension and secondary circulatory disturbance. The urinary findings are comparatively slight and transient, and there is little or no[161] anemia. The development is insidious, and the etiology is not known.
There is evidence of late to find a septic cause for most of the nephritides, such as infectious fevers, pyorrhea of the teeth, and like bacterial intoxications; in pregnancy the nephritis may be toxemic from sources that are not bacterial. It is extremely difficult, and not seldom impossible, to make any differentiation, as has been said. When the child is viable, whether the uterus should be emptied or not must be decided for the individual case; no general rule can be set down to cover all conditions.
One of the kidneys may be dislocated during pregnancy—usually the right kidney. If a floating kidney becomes twisted on its pedicle, abortion may be a consequence. The torsion may compress the renal blood-vessels and bring on acute hydronephrosis with high fever, great abdominal tenderness, and a peritonic facial expression.
Pyelitis of the renal pelvis is not seldom met in pregnancy. The gonococcus, colon bacillus, or some other pyogenic bacterium gets a nidus after pressure and lowered power of resistance. This condition is sometimes mistaken for appendicitis.
Catalepsy is a rare complication of pregnancy, in which the woman lies in an unconscious condition. The disease is a neurosis, but it might be mistaken for a toxic or uremic condition by a superficial observer. The infants of such women may be cataleptic, and may die as a consequence of the condition.
The term Eclampsia was first used to describe the sudden exaltation, flashing forth (eklampsis), of the vital faculties at puberty; later it was applied to convulsions, but now it is restricted to convulsions in pregnancy which sometimes begin suddenly, as in a flash. The disease is characterized by a series of violent convulsive movements, loss of consciousness, and coma, and is one of the most dangerous complications of gestation. All convulsions and comas in pregnancy, not due to hysteria, epilepsy, cervical tuberculosis, apoplexy, pneumonia, phosphorus, strychnia and like poisons, uremia, and meningitis, are commonly classed as eclamptic. When the symptoms of eclampsia are present with the exception of the convulsions, a rare condition, this state also is said to be eclampsia. Reineke[121] reported a case like this. After death the heart, kidneys, and liver showed all the signs of eclampsia.
The eclamptic attack may occur without warning, but almost always there are premonitory symptoms for from a few hours to some weeks. The preëclamptic symptoms are headache (commonly frontal), nausea and vomiting, vertigo, nervous excitement or somnolence, muscle twitching, occasional delirium, cramps in the calves, disturbances of sight, tinnitus, and pain in the epigastrium. Epigastric pain, headache, and disturbances of the optic tract are important symptoms. If these last signs are present in a woman who has some edema and nephritis, the eclampsia will certainly occur, if proper means to relieve the condition are not promptly taken. When the prodromata appear there is nephritis, as a rule, but exceptions are observed.
When the attack comes, if the patient is standing she falls unconscious. The pupils dilate, the eyes and head are turned to the side. She opens her mouth, and the jaw is pulled laterally. The woman stiffens, her face is distorted, her arms bent, and the whole body curves sidewise in a tonic spasm. After a few seconds her jaws chop, and if her tongue is between the teeth it is lacerated; twitching runs down from the face and ends in a violent convulsion of the whole body, which may toss the patient from the bed, and she may even fracture her skull or long bones in the fall. The breathing stops, the bloodshot eyes stick out, the face swells and darkens, the lips become purple. Gradually the convulsions wane, and the woman appears to be dying; but after deep sighing she begins to breathe stertorously; then she sinks into a coma, or, in favorable cases, revives.
After a few minutes to an hour or more another convulsion may befall her, or she may have no more than one. In very grave cases consciousness may never return after the first fit. The convulsions may run up into extraordinary numbers—a hundred or more. There is a pseudoeclampsia where the convulsions have been as many as two hundred. If there are many attacks in the first twenty-four hours with no clear evidence of subsidence, the woman nearly always dies. Fever begins in such cases, and goes up to 103 or even 107 degrees. In an untreated case Black found a temperature of 110 degrees before death. The average number of attacks in these cases is from five to fifteen, and the convulsions are from a half minute to two or three minutes apart. Olshausen had six patients who recovered after having had from twenty-two to thirty-six convulsions, but those who have above fifteen commonly die.
If the convulsions are severe the woman as a rule aborts, and often rapidly. After the child is delivered the eclamptic symptoms may subside, or they may come on again, even a week after labor. Often the fetus dies during the attack; rarely it survives and is carried to term; again, it may die and the eclampsia may subside, but the fetus remains in the uterus for some time.
If the woman is to die the eclamptic attacks usually increase[164] in frequency and violence; the temperature runs up very high, or it sinks; the pulse becomes weak and running, edema of the lungs comes on, with rattling and cyanosis, and the urine ceases to flow. The woman may die in a convulsion from apoplexy or heart paralysis. At times the child is delivered, but the coma deepens and the woman dies. In other cases there are coma and death without convulsions. Rarely there is a condition akin to acute yellow atrophy of the liver, with delirium, twitchings, coma, and death.
Women who have chronic nephritis seldom have convulsions in pregnancy unless there happens to be cerebral hemorrhage as an effect, but they suffer the other results of chronic Bright's disease—dropsy, uremia, edema of the lungs, paralysis of the heart, and albuminuric retinitis; they also are inclined to premature labor, and to hemorrhages that loosen the placenta. When acute nephritis happens in pregnancy convulsions are quite common, and when there are convulsions as a result of either chronic or acute nephritis it is very difficult to differentiate between these convulsions and genuine eclampsia.
The real cause of eclampsia is unknown, but the most plausible explanation of this "disease of theories," as Zweifel of Leipsic called it, is that it is a toxemia which attacks the liver, and directly or indirectly the kidneys, and brings on convulsions by toxic action on the anterior cerebral cortex. The great difficulty is to explain how these toxins originate. One authority suggests that the poison comes from the liver; another, from the fetus; a third, from the placenta, the intestines, the general metabolism, disturbed glandular balance, bacteria, and so on, but nothing is certain as to the etiology except that it is an intoxication.
On an average, 20 per cent. of the women who have eclampsia die,—but statistics vary from 5.31 per cent. to 45.7 for the mother and from 30 to 42 per cent. for the child. Eclampsia occurring ante-partum has the worst mortality; intra-partum, less; post-partum, least. About half the children die from prematurity, toxemia, asphyxiation, narcotics administered to the mother, or injuries at birth.
If the patient's pulse remains full and hard and below 120,[165] there is no immediate danger of death; but if faster, weaker, and running, the prognosis is bad. High fever is not necessarily fatal to the mother, but it is very dangerous to the fetus. Edema of the lungs is a very grave symptom, but recovery is possible. When the convulsions have gone beyond twenty the prognosis is bad, but there have been recoveries. Deep cyanosis, marked restlessness, anuria, and intense albuminuria are all bad symptoms. Apoplexy is nearly always fatal. After delivery the recovery of the woman is by no means certain. She may get pneumonia, sepsis, or another eclamptic attack. Hirst finds that if the diastolic pressure does not rise above a ratio of 1 to 3 times the pulse pressure (i. e., the difference between the systolic and diastolic pressures), the prognosis is good.
Every pregnant woman should be watched to prevent eclampsia, if possible, because all are liable to this outcome. The hygienic methods mentioned in the chapter on Abortion are most important here. The family history is of weight—if the women of the patient's family have been eclamptic, if her parents were alcoholic or insane, these facts increase her liability to the disease. If she has had eclampsia before, if her kidneys are acutely diseased,—especially if injured by infections,—if she is inclined to digestive disturbance, she is disposed to eclampsia. Albuminuria, diminishing amounts in the daily excretion of urine, and decrease in the total solids of the urine, casts or blood in the urine, are serious symptoms. If albumin increases and urea decreases, this is a grave sign.
The blood should be examined for the various anemias. If the thyroid gland is deficient or altered in activity, thyroid extract may be indicated—this acts also as a diuretic. Uterine malpositions should be corrected. Treatment should be given where there is any evidence of toxemia, as headache, altered secretion and excretion, neuralgia, mental eccentricity, increased vasomotor stimulation, high tension, disturbance in the sensory apparatus, obstinate constipation and jaundice. Toxemia is not necessarily renal in origin.
In any of these conditions the proteids should be kept low in the diet, so that the kidneys may not be overtaxed. To throw[166] off toxins, the emunctories should be stimulated by laxatives, water for diuresis, tepid bathing. If the symptoms grow threatening, and the kidneys are involved, the woman should be put to bed, on water alone. After three days an absolute milk diet should be begun. As she improves, starches are added, then the vegetables containing proteid, vegetable oils, and butter. As the improvement goes on, the diet may be vegetables, fruit easy of digestion, and one egg a day. Later fish and chicken are used, but never a full meat diet. Beef, mutton, veal, and similar heavy meats are not to be eaten. The drink is to be water, buttermilk, or koumiss.
When the eclampsia is inevitable the question of inducing labor arises. If the child is not viable, abortion is out of the question, as has been proved in the chapter on Abortion and the general chapter on Homicide. If the child is viable, there are three opinions: one, that the premature delivery should be effected as soon as possible; a second, that this delivery should be delayed as long as possible; and a third, that it should not be attempted at all. Those who hold that the uterus should be emptied as soon as possible, induce labor at the first convulsion, rapidly and under deep narcosis. Chloroform is dangerous to the heart in such cases for full anesthesia; ether is better. Braun first observed that the convulsions cease or are lessened after delivery. Dührssen found these results in 93.72 per cent., Olshausen in 85 per cent., Zweifel in 66 per cent. Peterson said that in 615 cases of early delivery—as soon as possible after the first convulsion—the maternal mortality was 15.9 per cent., but 28.9 per cent. in the same maternities under the expectant method.
Olshausen was not in favor of forced delivery. Charpentier[122] held that forced delivery is dangerous and should be absolutely proscribed. His statistics of mortality are: after spontaneous labor, 18.96; after artificial labor, 30.04; after forced delivery, 40.74.
Lichtenstein[123] reported, from Zweifel's clinic in Leipsic, the results of 400 cases of eclampsia, and he found that the eclamptic[167] convulsions cease in only one-third of the cases after any form of delivery. He says the mortality of induced labor is no better than that after forced delivery, and that the mortality of both methods does not materially differ from the mortality of a long series of cases where there was no such intervention. The difference in the mortality between eclampsia without delivery or with delivery seems to depend on the relative loss of blood. In 40 per cent. of eclamptic cases operated upon, the loss of blood was 500 c.c. above the loss in cases of spontaneous delivery. The loss of blood tends to produce collapse when the blood comes from the uterus, although it may be beneficial if removed by venesection before delivery. Five hundred c.c. of blood is one-eighth to one-ninth of the entire blood supply of the body in a woman of average size. If 500 c.c. of blood is withdrawn before the shock of forced delivery and replaced by an equal quantity of normal salt solution, the toxin is thus reduced by one-fourth or one-third and then diluted by the normal salt solution, so that it has less poisonous effect.
Lichtenstein[124] describes the expectant treatment by phlebotomy and narcotics to replace operative interference, and this method has revolutionized the mortality of the treatment of eclampsia. In ninety-four cases of eclampsia his mortality was only 5.3 per cent., and none of the deaths could be ascribed to the treatment. The infant mortality was 37.3 per cent., as against his 38.8 per cent. in active operative interference during preceding years. Werner, in the Second Gynecological Clinic in the University of Vienna,[125] by this new method in thirty-eight cases of eclampsia had a maternal mortality of 5.2, as Lichtenstein had, but his infant mortality was only 14.65 per cent., an enormous advance for the better. Formerly the mortality in the Viennese clinic was 15.8 for the women and 44.3 for the children, in a series of 120 cases of eclampsia. A mortality of 50 per cent. in the children is common in the old method. In Lichtenstein's cases there were mental disturbances[168] in 2.1 per cent. of the women, as against 6.75 per cent. in the old method. Eclamptics may go insane and kill the child after delivery. Lichtenstein treated 74 consecutive cases without a single death. In 54 per cent. of his cases the convulsions ceased after one venesection, and 42 per cent. of the women with ante-partum attacks recovered before labor came on. Engelmann[126] reported a case where a woman who had had 188 convulsions recovered after the third venesection.
In this method the woman is put in a dark, quiet room; 400 to 600 c.c. of blood are withdrawn by venesection, and 0.002 gm. morphine is injected; two hours later 3 gm. chloral is given in an enema. If the fetus presents in a position for prompt delivery it is removed with forceps, or by expression to spare the mother; but expression is a dangerous process always.
Zinke[127] of Cincinnati has a method which reduces the maternal mortality, but it has an enormous infantile mortality. He depresses the maternal pulse by veratrum viride, and this depression is probably the cause of the infantile mortality through asphyxia. Veit introduced the use of morphine in eclampsia, and Winckel the use of chloral. It has been found that narcotics check the action of toxins on the nuclei of cells, and in eclampsia the action of narcotics may be of this nature. Baker of Alabama in 1859 first gave veratrum viride in eclampsia. The drug lowers arterial tension by depressing the vasomotor centres and the heart itself. In eclampsia it diverts blood from the brain and depresses the motor neurons of the spinal cord. Aconite has the same effect in acute cerebral congestion without depressing the vasomotor centres or irritating the stomach as veratrum viride does.
Cesarean delivery is used frequently of late in eclampsia. The mortality of the children is lowered somewhat by a cesarean section, but the mortality of the mothers is much worse than in the expectant method described by Lichtenstein. Eclamptic women usually have badly affected kidneys, and the anesthetic used in the section may be a cause of the raised mortality. Peterson reviewed 500 cases of cesarean section[169] for eclampsia[128] done by 259 operators in various countries. Up to 1908 the maternal mortality was 47.97 per cent. in 198 cases; from 1908 to 1913 it was 25.79 per cent. in 283 cases. Convulsions ceased in only 54.92 per cent. of the women after cesarean delivery, and in those cases in which the convulsions continued the mortality was 31.53 per cent. In 146 cases where the convulsions ceased the mortality was still 19.8 per cent. for the mothers. The fetal mortality was 10.69 per cent., counting all children who died within three days after delivery by section. The maternal mortality after cesarean section increases with the age of the patient. The cesarean delivery, then, has a maternal mortality of late of 25.79, with a tendency to increase as unskilled men attempt it; the expectant method has a maternal mortality of only 5.3 per cent. The cesarean delivery has a fetal mortality of 10.69 per cent.; the expectant, 14.65 per cent. The expectant method is preferable.
Over 20,000 women die in childbirth each year in the United States, and about 100,000 infants, and more or less permanent injury from parturition is almost general in mothers. The mortality in the trenches during the present great war is 2 per cent.; the mortality of infants during the first year is 14 per cent. Very much of this mortality and invalidism is attributable to lack of skill in the licensed unfit. We commonly deem parturition merely a physiological process, and for that reason the state permits ignorant midwives and quacks to take upon themselves with impunity the responsibility and the risks of delivery.
It is difficult to draw the line between normal and abnormal parturition, but every labor, as women now are in civilized countries, should be regarded as a grave surgical operation, and the indications that must be met in a surgical operation are likely to occur in almost any parturition. The strength of the patient, the condition of the heart, lungs, kidneys, and blood, sepsis and antisepsis, the nature and technic of the various operations that may be required, and the complications that may arise, are all to be understood and met conscientiously. No physician who has any regard for morality and his own reputation now will accept an obstetrical case unless he has had the woman under frequent observation for months before delivery. If the mother or child dies because of the bungling or surgical uncleanness of the physician or midwife,—and unfortunately such deaths occur almost hourly,—this physician or midwife is guilty of murder. There may be an abnormality of the uterine or abdominal muscles used in parturition, a disproportion between the parturient canal and the child, or various[171] accidents of labor; and these conditions are so frequent in occurrence and so grave that their removal requires great medical skill, fine discernment, quick and exact judgment, and often decidedly courageous purpose.
New methods of treatment frequently appear, and the quack is likely to be among the first by which the new is tried. The use and abuse of pituitrin is an example of such a method. About 1909, pituitary extract as a uterine stimulant was first described and it was immediately taken up by competent men and more frequently, perhaps, by the quack. The extract is from the posterior lobe of the pituitary gland, and when injected subcutaneously or into a muscle it is a very powerful oxytocic. In a few minutes the injection markedly increases the intensity and duration of the pains. The effect lasts for an hour or an hour and a half. Whitridge Williams[129] says a judicious administration of the drug will do away with the use of low forceps in from one-third to one-half of the cases, but its ignorant use places the life of the mother and child in jeopardy. Mundell[130] found twelve cases of rupture of the uterus, thirty-four cases of fetal death, and forty-one cases of fetal asphyxia pallida in which resuscitation was effected only after prolonged and vigorous efforts, sometimes for over an hour.
If there is any serious obstacle at all to delivery in the parturient canal or in the fetal position, or the like, pituitrin is likely to cause rupture of the uterus and asphyxiation of the child. It should never be used when there is the slightest danger of rupture of the uterus; or when the child is suffering; or in a shoulder and most pelvic presentations; or in elderly primiparae with rigid muscles; or when the cervix is not fully dilated, lest the undilated cervix be torn off; or where there is inertia after prolonged effort to overcome an obstacle to delivery. It is never to be used in a normal delivery merely to hasten the birth. Obstetrical cases are tedious, and an impatient physician with an atonic conscience is likely to use pituitrin so that he can get back to his bed.
Comparisons between the fetal mortality after the use of[172] pituitrin or the forceps are erroneous. Quigley[131] contrasted the fetal mortality in these conditions. In 147 pituitrin cases it was 2.7 per cent., in about five or six times the number of forceps cases it varied from 5.7 to 15.63 per cent.; but wherever there is any real need at all for the forceps, pituitrin at once is contraindicated except in easy low forceps deliveries, where in the hands of a skilled man pituitrin may safely replace the forceps to avoid possible instrumental infection of the uterus. There are contractions of the uterus toward the end of gestation, before labor proper sets in, which cause what are called False Pains, and these must not be mistaken for the beginning of labor, as unnecessary examinations and meddlesome interference may bring on great harm. Uterine atony, or weak pains, may affect the patient in the first stage of labor, in which the cervix of the uterus should be dilated; or the second stage, in which the child is delivered; or the third stage, the post-partum period, when the placenta is thrown off. Contractions of the uterine muscle cause pain, and these contractions themselves are called the Pains. In the first stage weak pains may prolong the dilatation of the cervix for days and expose the mother to sepsis or exhaustion, and the child to consequent danger.
In the second stage the abdominal muscles, which push the child out of the uterus, fail to work if the pains are weak. Causes of unsuccessful pains in the second stage are: an infantile uterus, fibroids or other tumors in or near the uterus, peritoneal adhesions, a full rectum or bladder, abnormal position of the uterus, a pendulous abdomen, diseases of the uterine wall, scars from past operations, chronic metritis or endometritis, primiparity in relatively advanced age, twins, distention of the bag of waters, gas in the uterus, abnormal position of the child, contracted pelvis, adhesions of the membranes about the os uteri, fatigue of the woman, and tetany or stricture of the uterus. The obstetrician must be able to diagnose the special cause and treat the indications.
One of the causes of weak pains is a diseased heart. Systolic murmurs at the base of the heart and an accentuated second[173] aortic sound are quite common in pregnancy and may not be of grave importance. If there is a genuine cardiac lesion with good compensation, the labor is usually successful and without notable damage to the woman, although obstetricians like De Lee think that such patients appear to develop decompensation sooner than do women who are not pregnant. If the heart disease is advanced and the heart is in unstable equilibrium, especially if there is myocarditis or fatty degeneration, the heart is likely to break down in pregnancy or labor. In chronic cardiac lesions, pregnancy, through venous congestion, tends to renal and hepatic disturbance, or to dyspnoea and carbonic acid narcosis. The uplifting of the diaphragm by the enlarged uterus increases the respiratory difficulty. There may be edema of the lungs, hypostatic pneumonia, dropsy, insomnia, albuminuria, and other serious symptoms.
During labor a diseased heart may fail and cause sudden death, especially if the second stage is prolonged. At times there is collapse and death shortly after delivery. The mortality of heart disease in pregnancy varies in the reports on various series from 4 to 85 per cent. Babcock[132] says that the mortality in mitral disease in pregnancy is 50 per cent.; that in disease of the aortic valve is 23 per cent. These figures are far above those given by later obstetricians of skill. Fellner and Demelin, in ninety-four and forty-one cases respectively, had a mortality of only 6.3 and 5 per cent. Hirst says he never lost a case. Jaschke[133] found a mortality of only 4 per cent. in 1548 cases of pregnant cardiopaths. A great danger is in treating heart conditions by general rules, and in giving digitalis and other drugs without discrimination. In uncompensated heart conditions many of the children die from prematurity, abruptio placentae, diseases of the placenta, or asphyxiation.
Even those obstetricians who induce abortion at any stage of gestation when they deem the woman's life in danger say that heart disease in itself is not an indication for abortion[174] unless there is chronic decompensation with myodegeneration and renal or hepatic insufficiency. Expectancy is the rule. Lusk advises abortion as soon as mitral stenosis is discovered.
Surgeons of the Mayo Clinic, in a report[134] on Operative Risk in Cardiac Disease, hold that a valvular lesion is not a rational basis for judging a cardiopath so far as prognosis in a surgical operation is concerned, but this statement is not true for an obstetrical case. If we except angina pectoris and related diseases, the four disorders of the heart's mechanism that surgeons deem the worst risks in operation are auricular fibrillation, auricular flutter, impaired auriculoventricular conduction, and impaired intraventricular conduction. These conditions are usually accompanied by extensive lesions of the heart muscle.
In auricular fibrillation there are rapid incoördinate contractions, twitchings in individual muscle bundles of the auricular wall. The auricle loses its power to pump the blood and dilates. The pulse is commonly arhythmic and rapid. A permanent fibrillation is worse than a paroxysmal state. The condition is found especially in advanced cases of exophthalmic goitre. In the Mayo Clinic the operative mortality in seventy cases of exophthalmic goitre with auricular fibrillation was only 2.8 per cent.
In auricular flutter, or heart block, there are foci of irritation in the auricular wall which cause rapid coördinate contractions. The auricle may contract twice as often as the ventricle, and the pulse may be regular or markedly irregular. The stimulus for heart contraction normally reaches the ventricle from the auricle by passing along the bridge of primitive tissue which connects the auricle and ventricle. This bridge may be so affected that the stimulus is delayed, or prevented at times from crossing over, or completely blocked. One patient with complete heart block was operated upon at the Mayo Clinic three times in eleven years for appendicitis, cancer of the breast, and the excision of recurring skin nodules, and is still alive and reasonably well. In intraventricular block the risk of operation is worth taking, according to the opinion at the[175] Mayo Clinic, where there is exophthalmic goitre or tonsillitis.
In general, where there is question of surgical operation on a cardiopath, no such operation should be done unless there is definite ground to believe that the operation is essential to improve the heart condition or restore reasonable health. Extremely severe cardiac disease can be relieved or even completely cured by the surgical removal of infectious, mechanical, or toxic sources of heart degeneration, especially goitre. When the myocardial insufficiency is so marked that no medical treatment reëstablishes a reasonable compensation, no surgical operation is permissible. The medical treatment is the only test to learn whether the heart can be put into a condition wherein it will withstand the anesthesia and the operation. Life depends on ventricular action, not on auricular, and the ventricular reserve is the standard for judgment in these cases.
Fibrillation and heart block are grave conditions when found in pregnancy, but disease of the mitral valve because of frequency is more important, and when compensation is unstable mitral lesions are dangerous. In mitral stenosis the enlarged uterus in the last months of gestation, by crowding the intestines and diaphragm, embarrasses the heart. As the diaphragm cannot descend well, the flow of blood out of the right ventricle is not aided by respiration as in normal conditions. Pressure on the abdominal veins increases the blood tension and throws greater work on the left ventricle. In the expulsive stage of labor there is danger of the right ventricle giving way under the added strain.
In mitral regurgitation the left ventricle is dilated, and in pregnancy the regurgitation is increased by the peripheral resistance or obstruction. If the dilated ventricle is also hypertrophied it stands the strain much better. In the second stage of labor the danger is the same as in mitral stenosis. In disease of the aortic valve the strain of child-bearing is on the left ventricle, but patients in this condition undergo labor more successfully than do those with mitral disease.
Labor in any cardiac disease requires close watching even when the compensation is good. There is always a possibility of collapse in the third stage or during the puerperium. The[176] obstetrician must stay by the bedside, and he is to have everything ready for a sudden emergency, which is likely to result in death if not instantly met. All the instruments for operative delivery are to be kept sterilized and ready for immediate use. When symptoms of imminent collapse appear, delivery is to be done at once. If a cardiopath collapses in the early stages of gestation, before the child is viable, the rule explained in the chapter on Abortion holds—the child may not be killed by removal to save the woman's life.
Jaschke,[135] in his consideration of 1548 pregnant cardiopaths, found that seven-eighths went to term, and that the women were prematurely delivered in only about 9 per cent. of the total number of cases. Therapeutic interruption of pregnancy was necessary in only about 1 per cent. The high mortality reported by many good obstetricians is a proof that the treatment of cardiac conditions requires an experience in clinical medicine and a skill lacking, as a rule, in specialists who are not internists.
A combined mitral and aortic disease with great enlargement of the heart, heaving of the chest wall, and some protrusion makes pregnancy very dangerous. Osler thinks mitral insufficiency in itself not very dangerous. He had one patient with such a condition, a loud apex systolic murmur, and some enlargement, who bore nine children and lived to past sixty years of age. Mitral stenosis is not so favorable, but even in extreme stenosis some women bear several children without collapse.
Hyperemesis Gravidarum, the Pernicious Vomiting of Pregnancy, is commonly classified among the toxemias; but as the etiology is not known definitely, this classification is one of convenience more than exactness. Nausea and vomiting occur so frequently in the early months of gestation that they are deemed almost physiological, but when these symptoms become very grave and persistent they are undoubtedly pathologic, and are said to be pernicious, as they may lead to abortion, or to the death of the woman. In 1813, Simmond first successfully employed artificial abortion to save the woman in this condition, and thus added a possible moral quality to the disease. Therapeutic abortion was used in 1608, and Soranus of Ephesus, in the second century, mentions it.
The pernicious nausea commonly begins in the second month of pregnancy, less frequently in the fourth month, but it may be delayed until the sixth month; if it occurs after the sixth month it is, almost as a rule, an evidence of nephritis. It may last from about a month and a half to three months, but in toxemic cases it may result in death in two weeks. Sometimes remissions occur.
In 1852, Paul Dubois described the disease, and his division into three stages is still used in articles on pernicious vomiting, although these stages are not clearly marked clinically. In the early months of gestation the stomach may become unable to retain food, and there is notable loss of appetite; the condition is then grave. There may be retching at the sight of food, at any change of position, or at the entrance of a person into the room. The emesis may recur so often at night as to cause exhaustion from insomnia. Hiccough, thirst, pain in the[178] stomach, and soreness of the thoracic muscles are frequent and troublesome symptoms. In some cases there is salivation.
The vomitus is food, mucus, and some bile at first; later mucus and bile; finally it contains blood. The blood may come from the mouth, pharynx, or stomach, and it is serious if it is gastric. The urine is scanty, and shows nephritic irritation. At times it contains blood, bile, acetone, diacetic acid, indican, and rarely sugar.
In the second stage of the disease all symptoms are aggravated, and the stomach will not retain anything. There is extreme thirst; the patient faints often, and loses weight rapidly. In chronic cases there is much emaciation. The mouth is like that in a case of typhoid. Sometimes there is a low fever; again, the temperature is subnormal, with a rise before death. The pulse is rapid and weak, and the post-mortem heart shows fatty degeneration as in a fatal sepsis.
In the third stage the mind is affected, there is delirium, stupor, and coma; the vomiting ceases, the pulse grows more rapid and feebler, and the weakness becomes more and more overwhelming until the patient dies. This third stage is commonly short. In these conditions it is too late to empty the uterus, and any attempt to do so then only hastens death.
In some cases the fetus is apparently not affected; in toxic cases it is affected, and then there may be miscarriage. If the fetus dies the vomiting ceases, as a rule.
The liver enlarges in the first stage and later diminishes. There may be a general hemorrhagic hepatitis and acute yellow atrophy, or partial fatty degeneration around the central lobular veins. Necrosis also occurs. Acute parenchymatous nephritis and hemorrhages into the kidneys are often observed.
Neurotic and hysteric women are more liable to this disease than the nervously stable. There is a direct communication by the sympathetic and vagus nerves between the stomach and the uterus and its adnexa, and thus reflex irritations readily pass to the stomach. Through this path vomiting is caused by any unusual distention of the uterus, as when the fetus grows too rapidly; or when the size of the ovum is larger than normal, as in twin pregnancies; or in irritations like hydramnios,[179] displacement of the uterus, acute anteversions, retroversions, or flexions which pinch and stretch the nerves. Inflammations, as metritis, endrometritis, and cervicitis; tumors of the uterus; diseases of the adnexa or of the pelvic connective tissue or peritoneum are other sources of reflex vomiting. The proof that such are causes is that the vomit ceases when the conditions mentioned are cured. Such conditions exist, however, in women who are not pregnant without causing vomit; there is therefore some special disposition in the pregnant.
Diseases which in themselves have vomiting as a symptom will in pregnancy make the vomit pernicious. Such are chronic gastritis, gastric ulcer, enteritis, cancer, helminthiasis, large fecal concretions, enteroptosis, tubercular peritonitis, and gall-stones. What is apparently pernicious vomiting in pregnancy may be the beginning of acute miliary tuberculosis. Diseases of the air passages—hypertrophied turbinates, septal spurs, laryngeal and apical tuberculosis—seem to cause the vomiting or to dispose to it. When vomit is associated with uremia, this occurs, as a rule, in the last months of pregnancy.
The cause, again, may be in the nervous system, from either a demonstrable lesion or a functional imbalance—paresis, locomotor ataxia, tumors or tubercle of the brain, meningitis, polyneuritis. Even when the nervous system is not directly the cause of the emesis, the remote irritant may work through the nervous system. A bad neurotic inheritance, as from alcoholic, insane, or weak parents, disposes to neurotic hyperemesis.
Toxins from the fetal syncytium appear to be another cause of the vomit. The syncytium is a mass of protoplasm without cell demarkation but with nuclei scattered throughout the substance. Sometimes this embryological cellular material starts to grow after the manner of a cancer, and then it is very malignant (syncytioma malignum), but its connection with the pernicious vomit of pregnancy is more theoretical than established. In physiological conditions the toxins in the blood are neutralized by the secretions of the ductless glands of the body, and in pregnancy probably these same glands by intensified activity effect the same result. Injection of blood serum taken[180] from healthy pregnant women has cured cases of toxemic pernicious vomit, and this makes the theory much more probable.
To diagnose the etiology of pernicious vomiting is not always easy. We must decide first whether the emesis is really pernicious or not; secondly, we have to determine whether or not it is due to the presence of the fetus; thirdly, we are to differentiate the primary and adjuvant causes for intelligent treatment. The age of the fetus must be known to determine whether we may licitly interfere so as to remove the fetus from the uterus if necessary, in medical opinion, to do so.
Trousseau emptied the uterus of a woman to stop her pernicious vomit, but she died, and at the autopsy he found a cancer of the stomach. Caseaux discovered tubercular peritonitis in a woman who had died after a diagnosis of hyperemesis gravidarum; Beau, tubercular meningitis in a like case. Williams of Johns Hopkins University stopped a very grave case of pernicious vomiting in a neurotic woman merely by telling her of the dangers of artificial abortion.
There is no settled mortality percentage in hyperemesis gravidarum because so much depends on diagnosis and treatment. Braun, in 150,000 obstetrical cases, never had a death from pernicious vomit; others have a mortality of 40 per cent.
The treatment is technical, and is given in detail in books like De Lee's Principles and Practice of Obstetrics.[136] Suggestion and the environment are important elements in the treatment. Local anesthetics, mechanical drugs like cerium oxalate and bismuth, depressomotors, external applications, and gastric lavage are indicated in the early stages of the disease, but are rather harmful than useful in later stages. Adrenalin, ten drops of a 1:1000 solution by mouth, or three drops hypodermically as doses, often cures. Sergent and Lian reported six such cases in one paper in 1913. Hypodermic injection of the extract of corpus luteum in 1 c.c. doses has been effective in some cases. So has the injection of defibrinated serum from a healthy pregnant woman. Curtis describes the technic in the Journal of the American Medical Association, February 28, 1914. The gynecologist must adjust uterine displacements[181] and heal cervical erosions. The oculist, laryngologist, and otologist are to remedy refractive errors and remove irritants in the air passages and the ear.
The treatment of last resort is to empty the uterus. This will cure all cases of neurotic and reflex origin if done early enough. In these cases, if the therapeutic abortion is deferred until very late, the patient will die of exhaustion. Toxemic cases do not react well after therapeutic abortion because of the damage previously done by the circulating poison, especially in the liver. A positive diagnosis of toxemia cannot always be made, and many patients in whom the diagnosis has been made correctly recover without abortion. Apart from moral considerations, it is very difficult to determine the proper time to empty the uterus. A test is made of the glycolytic power of the liver by giving two ounces of levulose internally; and if sugar shows in the urine, this means that the liver is unable to act normally, that it has been attacked and disabled by the toxin, and therefore the therapeutic abortion should be done. Again, a marked concentration of the blood, shown by erythrocytosis and leucocytosis, indicates starvation. Some obstetricians perform abortion when the pulse remains above 100, at the appearance of fever, blood from the stomach, jaundice, albuminuria, mellituria, acetonuria, indicanuria, or marked loss of weight. Polyneuritis, with icterus and bile in the urine, is another indication for abortion; a patient may die from polyneuritis alone after the hyperemesis has ceased. Not one but all these facts must be considered, together with one's own clinical experience.
In hyperemesis gravidarum, as elsewhere, therapeutic abortion is never permissible, under any circumstances, if the child is not viable. If the mother cannot be saved without emptying the uterus, the mother must die; there is no way out of the difficulty. The proof that this doctrine is correct has been given in the introductory chapter on Homicide and when considering abortion in general.
Recurring, permanent, localized spasms of facial or other groups of muscles, which are often called chorea, are tics,—convulsive tic, painful tic, accessorius spasm, and so on. Chorea is also characterized by various recurrent spasmodic movements, but the origin of the disease is commonly an infectious endocarditis, rheumatism, tonsillitis, or the like disease. This is Chorea Minor, St. Vitus's Dance, or Infectious Chorea. There is also a common chorea, which is not from an infection but from some nervous irritation, usually eye-strain, and disappears with the removal of the irritation. The chorea of pregnancy is often an infectious chorea, and then it is an extremely dangerous condition: the mortality in some collections of toxic cases is as high as 22 per cent. We meet, too, in pregnancy hysterical chorea, and a form which is partly hysterical and partly infectious in origin.
Primigravidae are more susceptible to infectious chorea in pregnancy than multigravidae. If a woman has not had true rheumatism she very rarely gets chorea after the first gestation. Rheumatism in the patient or in her immediate ancestors, epilepsy, fright and other emotions, and anemia are predisposing causes. The patients are all very neurotic; and if they had chorea in childhood, the condition is likely to recur in pregnancy.
Mild cases may be cured without damage to the woman or fetus, but many cases go on to abortion and death in coma and fever. Some severe cases result in a mania which may last for months; again, there is paralysis and delirium. The earlier in pregnancy the attack, the greater the danger to the fetus.
It is very important to differentiate infectious chorea from[183] hysterical chorea—the latter may or may not be dangerous; chorea always is dangerous. In hysterical chorea the movements are sudden, isolated, and sometimes rhythmical, especially in the fingers; there are zones of anesthesia, and the perversity of the hysteric soon manifests itself. The movements in hysteria are never so intense as to exhaust the patient. In true chorea the movements are irregular, spasmodic, and increased by motion and voluntary effort, especially if the effort is sustained; they exhaust the patient.
Maniacal chorea differs from the mania of the puerperium from other causes: in maniacal chorea the woman is not so sullen, and is more garrulous than the patient with puerperal mania. The prognosis is better in maniacal chorea as to recovery of reason. Sometimes, however, the mania of puerperal chorea persists for months, or it may become even permanent.
If the fetus is viable and the choreic woman, with a clear toxic chorea, shows signs of exhaustion from the spasms and insomnia, or if her mania is becoming fixed and her delusions are dangerous (such women are likely to kill the infant), or if she has endocarditis, the uterus should be emptied, as a rule. If, however, the symptoms show a recession on treatment, the uterus should not be emptied. Albrecht[137] reported a case of chorea cured by an injection of serum from a normal pregnant woman. Each case must be judged by its own characteristics. The last sacraments should be given as soon as the symptoms grow grave.
Hysteria in a woman, even when mild, may grow serious in pregnancy when it takes the form of melancholia; but it is dangerous when it passes into maniacal excitement. In mania there may be exhaustion from a refusal to take food, and in labor maniacal hysteria may wreak grave injury on both mother and child. Hysterical women should be treated before pregnancy; indeed, the process of avoiding hysteria should have begun in the patient's grandparents.
The term hysteria has been handed down from the days when physicians thought there was a connection between uterine disorders and the set of nervous symptoms grouped about the[184] title hysteria. It is now etymologically meaningless—men also grow hysterical. Briquet found 11 male to 204 female hysterics, and later statistics increase the number of males.
The disease is not readily definable. The patient is usually a young emotional woman, oftenest between fifteen and twenty years of age. She commonly has anesthetic spots on her body, concentric limitations of the fields of vision and reversals in the color fields, hysterogenetic zones, or tender points, which when pressed appear to inhibit the hysterical fit. The symptoms enumerated here are not, however, found in every case of hysteria, and it is difficult at times to diagnose the case. There is a popular notion that hysteria is a disease of malingerers, but it is as real as typhoid fever or a broken leg, and a much greater affliction than either of these conditions. Malingering is only a symptom of the disease.
The conditions that bring about hysteria are hysteria in a parent, or insanity, alcoholism, or some similar neurotic taint in an ancestor. Immediate causes are acute depressive emotions, shocks from danger, sudden grief, severe revulsions of feeling, as from disappointment in love or abandonment by a husband; and, secondly, cumulative emotional disturbance, as from worry, poverty, ill treatment, unhappy marriage, or religious revivals. Certain diseased conditions, as anemia, chronic intoxications, pelvic trouble, start it into activity when it is latent. It is also communicated by imitation and it may become epidemic.
After the great plague, the Black Death, in the fourteenth century, there were very remarkable epidemics of imitative hysteria in Germany and elsewhere. In 1374, at Aix-la-Chapelle, crowds of men and women danced together in the streets until they fell exhausted in a cataleptic state. These dances spread over Holland and Belgium and extended to Cologne and Metz. The "Dancing Plague" broke out again, in 1418, at Strasburg and in Belgium and along the lower Rhine. In 1237 there was a similar outbreak among children at Erfurt and many died from exhaustion. The tarantism in Italy from the fifteenth to the eighteenth century is another example of epidemic hysteria. There were epidemics of hysteria in Tennessee, Kentucky, and a part of Virginia, which[185] began in 1800 and recurred for a number of years. These outbreaks started in revivals and camp meetings. The majority of the cases were in youths from fifteen to twenty-five years of age, but the hysteria was observed in persons from six to sixty years old. The muscles affected were those of the neck, trunk, and arms, and the convulsions were so strong that the patients were thrown to the ground and often leaped about like a live fish tossed out of the water on a bank.
Convulsions, tremors, paralyses of various forms and degrees are common in hysteria. In major hysteria the patient falls into a convulsion gently. There is checked breathing, up to apparent danger of suffocation. Then follows a furious convulsion, even with a bloody froth at the mouth, but there is a trace of wilfulness or purpose in the movements. Next may come a stage of opisthotonos, in which the body is bent back in a rigid arch until the patient rests on her head and heels only, like a wrestler; and this is followed by relaxation and a recurrence of the contortions. An ecstatic phase succeeds this at times, the so-called crucifix position, with outbursts of various emotions, and a final regaining of the normal state. Any of these stages, however, may constitute the entire fit. Some major hysterics can simulate demoniacal possession with extraordinary ingenuity. In minor hysteria there is commonly a sensation of a rising ball in the throat—the globus hystericus. There may be uncontrollable laughter or weeping, and muscular rigidity is frequent. The patient, especially if she is a child, may mimic dogs and other animals. The snarling, biting, and barking of false rabies are hysterical; such symptoms do not occur at all in real hydrophobia.
There are innumerable physical symptoms of the disease, but the mental phases have most to do with the treatment. The hysterical person is characterized by an overmastering desire to be an object of sympathy, interest, admiration, rather than by a tendency to baser instincts. The will is weak, the emotions explosive, the patient is impulsive and lacking in self-control. She readily goes from absurd laughter into floods of tears. She simulates pains and other symptoms of disease, and[186] she is always a liar, no matter what her state in life, from nurse-girl to nun.
Acquired hysteria may be cured, but the congenital form is virtually hopeless; yet even with this latter kind much can be done by patient training. Such a girl or boy must be reared carefully and with a firm hand. A marked congenital hysteric should not marry. Marriage makes them worse, and they beget other hysterics. When a hysterical girl gets one of her fits the chief obstacle to cure is sympathetic visits from relatives and friends. If a patient in the vapors is taken from school and wept over, she will never come down to earth again. The girl who faints at the communion-rail regularly is always a hysteric, and the cure for her is a bucket of cold water in the sacristy, or a threat to turn her over to the police. You will find these fainters with a perfect pulse despite the faint. But there are other cases in which rough treatment is harmful, and the only method is patient tact. Such persons are objects of great pity and should be dealt with as one would deal with any deficient mind.
Acute yellow atrophy of the liver in pregnancy was formerly called Icterus Gravis. The disease is not necessarily connected with pregnancy, but half the cases are in pregnant women, and with them it may appear at any time in gestation or shortly after delivery. Pernicious vomiting, eclampsia, sepsis, chloroform poisoning, typhoid, osteomyelitis, diphtheria, erysipelas, alcoholism, or phosphorus poisoning in pregnant women may end in this acute yellow atrophy. Bendig[138] reported two cases, both fatal, which were caused by syphilis.
The liver lessens in size, is friable, yellow-streaked, mottled with red; the heart degenerates, and all tissues are stained with bile, icteric. If the hepatic atrophy is a consequence of the diseases enumerated above, the symptoms of these diseases precede those of the atrophy. In chloroform poisoning the attack may end fatally within six hours, or it may last for five or six days before death.
If a pregnant woman has had gastric catarrh with weakness and headache, and then suddenly becomes delirious, begins to toss about the bed with rolling of the head from side to side, is jaundiced, shows epigastric tenderness, and a diminution of the liver dullness, the diagnosis is almost certain. The reflexes are exaggerated, there are minute petechiae on the trunk, arms, and legs, the tongue is dry and brown, the breath is foul, the pulse is fast and weak, the temperature is usually high (102-104 degrees), and the urine shows nephritis.
The prognosis is always bad. The fetus nearly always dies. If the fetus is viable the uterus should be emptied at once even if the woman is so near death that the procedure appears useless: it may at least give a chance to baptize the infant. Suppose[188] in a particular case a consultant or the physician in charge holds that the mother is so ill that therapeutic abortion will only hasten her death, yet the fetal heart-sounds can be heard through her abdominal wall. In that case I should be in favor of performing the abortion to baptize the infant, reluctantly permitting the chance of hastening the mother's death. But this hastening is by no means certain.
When a diagnosis of acute yellow atrophy has been made the patient should receive the last sacraments as soon as possible.
Any of the acute infections, as typhoid, typhus, smallpox, measles, scarlatina, and the others, attacks a pregnant woman as readily as one who is not pregnant. Pregnancy, as a rule, lessens the resistance to the infection, and the infection is likely to cause abortion. The toxin of the infection is added to the physiological toxins of pregnancy, the kidneys often are overwhelmed, and there is a tendency to hemorrhage. After the exhaustion from the disease, delivery, whether premature or at term, is liable to end in collapse, especially if the heart or lungs have been injured. Puerperal sepsis, either general or local, is a common effect of these bacterial diseases. In smallpox there is infection from the pustules and the virus itself; in typhoid the typhoid bacillus and the streptococci in Peyer's patches get into the blood; in influenza, pneumonia, erysipelas, and diphtheria the bacteria directly cause sepsis, and in scarlatina the pus organisms from the throat are found in the septic foci.
In these infections the fetus may be killed by the high temperature; it may die from asphyxia brought on by feeble maternal blood-pressure and consequent stagnation of the circulation in the uterine sinuses; it may be overwhelmed by maternal hemorrhage; by deoxidation of the maternal blood, as in pneumonia; by a hemorrhage in the placenta, and a consequent separation of the placenta itself from the uterine wall; by fatty degeneration of the fetal villi, which renders respiration of gases impossible. Again, the child may be infected by the disease of the mother, or it may be killed by the toxins in the maternal circulation.
The communication between the fetal and the maternal blood systems is as indirect as that between the air in a man's[190] lungs and his blood. The communication between mother and fetus is by osmosis, but certain toxins, drugs, and bacteria may also pass from the maternal to the fetal circulation through the placenta. Strychnia injected directly into the embryos of animals by Savory and Gussarow killed the mother after passing to her through the placenta. There is no direct communication (except by osmosis) between the fetal chorionic villi and the maternal intervillous blood spaces. In the first half of pregnancy fetal and maternal blood are separated by the syncytium, Langhan's layer of cells, the stroma of the villi, and the walls of the fetal capillaries; in the second half of gestation Langhan's layer gradually disappears. In the fetal blood-vessels are found many nucleated red corpuscles, but these are lacking in the maternal intervillous spaces. Sänger also discovered that in pernicious leucemia the leucocytes of the mother are not present in the fetal circulation.
That gaseous substances pass through the fetal barrier of tissues was proved by Zweifel, Cohnstein, and Zuntz. Zweifel showed that chloroform administered to the mother rapidly reaches the fetus. As early as 1817, Mayer proved the passage of cyanide of potassium. Since then we have been made certain of the transmission of iodide and ferrocyanide of potassium, salicylic acid, bichloride of mercury, methylene blue, and many other substances. Krönig and Futh, in 1901, determined that the maternal and the fetal blood freeze at the same temperature, which indicates that they possess equal osmotic power, and that osmosis may occur in either direction.
Some bacteria do not get through to the fetus, but a few do get in. Tubercle bacilli were found in the fetus by Birch-Hirschfeld[139] in 1891, and Schmorl[140] demonstrated them in 50 per cent. of the placentas in one series of examinations. Bar and Renon[141] found them in the blood of the umbilical cord in two of five cases. Actual congenital tuberculosis is possible, though very exceptional: the bacteria either pass through the wall between mother and fetus, or destroy this wall and then[191] get in. Smallpox, measles, and scarlatina, the causes of which have not yet been demonstrated; typhoid, cholera Asiatica, pneumonia, bubonic plague, erysipelas, pus infection, anthrax, syphilis, febris recurrens, and malaria have already been demonstrated in the fetus. Lynch of Johns Hopkins collected sixteen cases of typhoid in the fetus. I found the typhoid bacillus in the liver and kidneys of a still-born fetus whose mother was ill with typhoid fever; this case was not among those collected by Lynch.
The majority of writers give unfavorable prognoses for typhoid in pregnancy. Abortion or premature labor is extremely common, with great danger to the mother's life. When labor begins in these cases the last sacraments should be administered early. Therapeutic abortion in typhoid is very likely to cause death, yet a number of women recover after abortion. As regards the woman's life, cases of premature labor have a worse prognosis than early abortion. The greatest danger is while the fever is high, and abortion is commoner in the first week of fever than in the second or third. In protracted typhoid abortion is likely to occur in the fourth week or later. After defervescence the prognosis is better, but there is always danger. Different physicians have markedly varying results. There is no medical condition where skill in the physician counts more than in typhoid; it is the supreme test of the therapeutist. Sacquin[142] collected from various sources the statistics of 233 cases of pregnancy during typhoid, and abortion or premature labor occurred in 150 of these, with death in 16 per cent. Many skilful men have a mortality as low as 3 per cent. in typhoid not complicated with pregnancy.
The subject of typhoid is too vast for complete treatment here: the article on Typhoid in the American edition of Nothnagel's Encyclopedia of Practical Medicine covers 472 large octavo pages. A very important point is not to mistake typhoid for a septicemia in its early stage. A Widal reaction should be made in apparently septic cases to exclude typhoid. Sometimes, however, a streptococcic infection will give a positive[192] Widal, and there may be a mixed typhoid and streptococcic infection.
Smallpox in pregnancy causes abortion or premature labor in the majority of cases, and the child usually dies. The child may be born in the eruptive stage, or pockmarked. Franklin reported a case where a vaccinated woman was delivered of a child while her husband was in the house ill with smallpox. The mother did not take the infection, but the child was born dead of smallpox: the contagion had passed to the child through the unaffected mother. Vaccinated women at times bear children which are after birth immune to vaccinia and smallpox—vaccinia, in the commonly held opinion at present, is an attenuated smallpox. Pregnant women should be vaccinated, when there is smallpox in their neighborhood, to protect themselves and their children, unless they have been successfully vaccinated within four or five years.
Vaccination prevents smallpox in more than 90 per cent. of the exposures to the disease. The death-rate was 58 per cent. in the unvaccinated cases and 16 per cent. in the vaccinated in a group of 5000 cases of smallpox studied by Welch in 1894. During the eighteenth century, according to Bernouilli's calculation, one-twelfth of all the children born succumbed to this disease. In 1707, in Iceland, 18,000 of the entire population of 50,000 died of smallpox. As late as 1885, 3164 persons died of the disease in Montreal in one epidemic brought on at a time when vaccination had been neglected. In Prussia, from 1851 to 1860, without compulsory vaccination for civilians, there were 36,577 deaths from smallpox; in the Prussian army during the same time, with compulsory vaccination, there were only fourteen deaths. During the war of 1870 the French armies, without vaccination, lost 23,469 men from smallpox; the German armies lost only 459 men and there was a great epidemic of the disease in Germany at the time.
The efficiency and necessity of vaccination against smallpox, which is as virulent now as it ever was, is so certainly established that a parent or guardian who neglects or refuses to have children vaccinated when exposed to the disease is guilty of homicide through neglect if an unvaccinated child[193] under his care dies of smallpox. Revaccination is necessary every eighth year if smallpox reappears. Agitation against vaccination is not mere ignorance: it is a dangerous crime, exactly like loosing a mad dog; and it is combined with the insolence of ignorance. Persons who have seen smallpox are very much afraid of it, because it is one of the most dreadful afflictions humanity is exposed to; those who have not seen it, yet say they are not afraid of it, are mere fools.
A pregnant woman who is infected with smallpox should receive the last sacraments as soon as possible. If she aborts she may die very quickly in collapse. If she is evidently in articulo mortis and the fetal heart can be heard, her cervix should be forcibly dilated, the child turned, and delivered for baptism. If the physician waits for death, the child will be dead also, and sectional delivery will be too late for any good.
Pneumonia in pregnancy is a rare but very dangerous disease. In one series of 13,611 pregnancies there were 120 cases of pneumonia—eight-tenths of one per cent.; in another series of 1842 pregnancies two and three-tenths had pneumonia. Wallich,[143] in a study of the mortality of this condition, found that pneumonia causes abortion in one-third of the cases that occur during the first six months of gestation, and in two-thirds of the cases that happen between the sixth month and term. On the third day of the pneumonia the abortions are most likely to occur. The maternal mortality varies between 50 and 100 per cent. in the groups studied, and the fetal mortality is 80 per cent. in general, but about 40 per cent. for viable fetuses. The large size of the uterus in the last months of pregnancy interferes with the descent of the diaphragm in respiration, and the heart is likely to fail. The more advanced the pregnancy, the greater the danger to both mother and child from pneumonia. Among the dangers to the child is the imperfect oxygenation of its blood, and in a few cases the pneumococci reach the fetus.
Randall, in a study of 190 pregnant women who had pneumonia, found a somewhat lower mortality than that observed by Wallich. In Randall's series 70 died (36.7 per cent.); of[194] 118 who did not abort, only 12 died (10.7 per cent.). In a second group of 352 cases abortion happened in 58.8 per cent. Of 144 patients in the first six months of gestation, 22.08 per cent. died, but of those that aborted 52.08 per cent. died. Again, of 164 cases in the last three months, 30.49 per cent. died, but 70.12 per cent. died of those that aborted during these three months. Of 82 that aborted, 87.8 per cent. died. The mortality in women under 25 years of age was 13.33 per cent.; in women from 25 to 35 years, 23.2 per cent.; over 35, 22 per cent.
Pneumonia in pregnancy is made worse by the mechanical interference with respiration brought about by the enlargement of the uterus, and the heart, which is overburdened in ordinary pneumonia, is still more exhausted by the additional strain of pregnancy in the pneumonia of gestation; moreover, the lungs, which are obliged to do enhanced labor in pregnancy in eliminating, are clogged by the pneumonia; it would seem, then, that, if the fetus is viable, the womb should be emptied to give the mother a better chance for recovery. Statistics, however, are against therapeutic abortion. The evacuation of the uterus determines blood to the inflamed lungs, which are already overburdened. The exhaustion of labor weakens the patient, and makes her liable to general septic infection. Matton[144] found that in eighteen cases where pregnancy was artificially interrupted, nine women died (50 per cent.); while in twenty cases where no interference was attempted, only one woman died. This comparison is not exact, perhaps, because we do not know the gravity of the infection in each group, but in any consideration the difference is remarkable. In a group studied by Chatelain[145] the results in natural and artificial delivery were virtually the same. Inasmuch as therapeutic abortion at the best is no better than non-interference, there is no justification for therapeutic abortion, unless in unusual circumstances.
Pneumonia is an infectious disease, and a pregnant woman should, for her own sake and the sake of the fetus, avoid exposure[195] to infection. When the disease is present the last sacraments should not be deferred, as it may be impossible to make a confession when near death.
Influenza in pregnancy is more severe than it is in the non-gravid state. By the laity, and sometimes even by physicians, influenza is confused with la grippe, but there is an influenza vera and an influenza nostras, or la grippe, and this latter is not nearly so serious a disease. The real influenza is caused by a specific bacillus; it appears in epidemics which have a tendency to become pandemic, and then the disease disappears for a generation. La grippe is a bronchitis or coryza with some fever and muscle-soreness. True influenza (the name is Italian, influenza di freddo) is very infectious. The pandemic of 1889-90 started in Turkestan in June, 1889, and by October, 1890, influenza had gone westward and encircled the earth along the trade routes. The preceding pandemic occurred in 1847-48.
There is no clear proof that pregnant women are especially liable to infection by influenza, but there is always a notable fall in the birth-rate after marked epidemics of the disease. This has been observed in France, Germany, and Switzerland. When it does occur in pregnancy it is likely to cause abortion. Pasquier, as early as 1410, noticed this fact. The disease is likely to cause hemorrhage from the uterus in non-gravid women, especially in those who are past the climacteric, and menorrhagia in younger women who are not pregnant. Moeller[146] found abortion or premature labor in 28.3 per cent. of twenty-one severe cases. In severe influenza where there is diffuse capillary bronchitis, pleuropneumonia, or spasmodic cough, abortion is most likely to occur, and such abortion is always dangerous. The hemorrhages in abortions from influenza are often alarmingly profuse.
In threatened respiratory or cardiac failure in influenza complicating pregnancy there may be question of therapeutic abortion, but in such an event great care must be taken to avoid exhaustion and shock. The child should be extracted; the woman should not be made to labor. One of the important[196] moral considerations in this matter of influenza and pregnancy is that the woman commits grave sin if she needlessly exposes herself to infection, because of the danger to the child's life and the risk of its loss without baptism, and also because of the danger to her own life.
Scarlatina (Italian scarlattina, Low Latin febris scarlatina), or Scarlet Fever, is very rare in pregnancy. Popularly, scarlatina is used for a light form of scarlet fever, as varioloid is used for a light attack of smallpox; but physicians do not make this distinction between scarlatina and scarlet fever: they use the terms synonymously. In Nothnagel's Encyclopedia of Practical Medicine Juergensen has an elaborate discussion on the differentiation between genuine scarlet fever in the puerperium and the relatively frequent septic erythema found in that state, but the received opinion now is that real scarlet fever is very rare in pregnancy. Those who report large numbers of scarlet fever cases in pregnancy err in diagnosis.
The mortality in the scarlatina of pregnancy may be very high—52 per cent. in some epidemics; and if the infection happens immediately after delivery, the mortality is still higher. A septic rash is sometimes mistaken for scarlatina, but where the genuine disease is present the pregnant woman is gravely obliged to avoid exposure to it, both for her own sake and for that of the fetus. In the early months of gestation scarlatina commonly causes abortion.
Measles in pregnancy is also very rare, but when it does occur it is a serious disease. Gestation is interrupted in 55 per cent. of the cases, and the mortality is 15 per cent. for the women. The same moral and related conditions that obtain in scarlatina are found in measles. There is a marked tendency to hemorrhage and pneumonia. Of eleven cases reported by Klotz,[147] nine aborted.
In epidemics of Asiatic cholera the mortality among pregnant women is extremely high. In the Hamburg epidemic of 1897, fifty-seven per cent. of the pregnant women affected died. Abortion is very frequent because of the hemorrhagic endometritis. The mortality for all patients in Asiatic cholera is very[197] great—almost 50 per cent. at the beginning of the epidemic.
Typhus fever is the ship or famine fever of 1847. It is very rare now. When it does occur it is about three times as fatal as typhoid. It is a disease of poverty and war, and is spread largely by the body-louse, as happened in Serbia in 1915. Skilled hygiene, however, soon gains control of the epidemic.
Erysipelas in pregnancy is rare, but not infrequent after delivery. In the puerperium it appears commonly as a septic infection in abrasions about the parturient canal. When it starts on the face, scalp, or breast the prognosis is relatively favorable, but even then it causes death; when it starts on the genitalia it has a mortality of 43 per cent. Erysipelas causes abortion. As it begins from pus bacteria, it is not seen so frequently now as formerly, owing to greater attention to asepsis. In the puerperium it is often an infection brought on by dirty midwives or physicians.
Malaria, if severe, may interrupt gestation through fever or cachexia. During labor in such cases the uterine action is feeble, and hemorrhages are common after delivery. By proper treatment during pregnancy these evils can be averted. The infection is spread from one malaria patient to another by a mosquito (Anopheles), as yellow fever is spread by another mosquito (Stegomyia fasciata).
Pulmonary tuberculosis in pregnancy is somewhat frequent; the estimate is that about 32,000 tubercular women become pregnant annually in the United States; and obstetricians incline to the opinion that pregnancy commonly, though not always, makes the tuberculosis worse. Nearly all agree that the combined effect of pregnancy, the puerperium, and lactation is a grave burden on the consumptive and lowers the power of resistance.
Trembley of the Saranac Lake Sanitarium reported that 63 per cent. of 240 tubercular married women under his observation gave a history which showed that the disease was first recognized during pregnancy or the puerperium. Schauta's clinic found such origins in 29 per cent. Fisberg, Funk, Jacob, Panwitz, and other observers, in a series of 1100 cases,[198] said 39 per cent. of these women thought the disease began during pregnancy or the puerperium.
Some tubercular women during pregnancy give no clinical evidence of an aggravation of the pulmonary disease, but these cases are exceptional. Tubercular women who apparently improve during pregnancy are likely to have a subsequent detrimental reaction. As tubercular cases, however, are prone to show exacerbations even if not pregnant, it is not possible to say that pregnancy is the sole cause of the progressive lesions in particular instances. Where there are no wide or deep areas of infection, there may be no recognizable damage from pregnancy, but advanced and active tuberculosis, with fever or cavity formation, does badly, especially if the throat is involved. The pressure of the enlarged uterus causes dyspnoea; the cough and fever may bring on miscarriage. Miscarriage, however, is rare in tuberculosis; it is more common in cardiac and renal diseases. Bernheim, in a series of 315 tubercular pregnancies, found that abortion occurred in 23 per cent. The later in gestation the tuberculosis becomes florid, the more likely it is that abortion will happen. Conception may take place at any stage of the tuberculosis, although women in the final stage are commonly sterile. Sometimes a woman will give birth to a sound child and die herself of tuberculosis a few days after the parturition.
Pregnancy in consumptive women is not necessarily detrimental to each particular patient, nor is it, as a rule, a justification for emptying the uterus of even the viable fetus. Even when the tubercular condition grows worse during pregnancy it is not always possible to prove that the pregnancy itself is the cause of the deterioration. If the woman conceives in the final stage of pulmonary tuberculosis she will die, whether she goes on to term or not. Bonney[148] describes three cases of advanced pulmonary tuberculosis which were cured during pregnancy, by the bodily changes peculiar to that condition, but such results are altogether exceptional.
Artificially induced premature labor sometimes causes more damage than normal parturition at term. Much depends upon[199] the methods used for the induction of the abortion. The insertion of bougies, catheters, or sounds is always contraindicated in advanced tuberculosis. Hirst of the University of Pennsylvania[149] thinks the notion that tubercular women improve in pregnancy is "a superstition," and that such women should neither marry nor have children. De Lee[150] holds that tubercular women should not marry because the woman is likely to infect her husband and children. He thinks the disease grows worse in pregnancy, and that hemorrhage is frequent except in chronic ulcerative tuberculosis. In this last condition pregnancy does not ordinarily aggravate the condition. In tubercular laryngitis complicating pregnancy, Küttner found the mortality to be 90 per cent. Such laryngitis is usually fatal, whether pregnancy is present or not. When there is a miscarriage in tuberculosis, the infection often becomes florid and resembles pneumonia. Advanced cases have a tedious and dangerous labor, with dyspnoea and occasionally hemorrhage or cardiac exhaustion. Edema of the lungs is not infrequent.
Williams of Johns Hopkins University, in the 1903 edition of his Obstetrics, tells of a woman who died of tuberculous peritonitis a short time after parturition. The uterus was studded with tubercles and its interior was covered with tuberculous ulcers. The tubercle bacillus had been found in cultures taken from the interior of the uterus during life. Her child was born perfectly healthy and remained so. Williams says in the same place that the induction of premature labor because of tuberculosis is justifiable only in the interests of the child, and this only in those rare cases in which the woman is so ill that she probably will die before term. Norris[151] of Philadelphia agrees with Williams that induction of premature labor is useless, and he says all authorities unite in this opinion.
A tubercular woman should not nurse her infant because she will infect it and exhaust herself. Infants are very susceptible to tuberculosis. Birch-Hirschfeld, in 1891, first demonstrated tuberculosis in the fetus, and Schmorl found it in[200] the placenta in 50 per cent. of a series of cases that he examined. Infection of the child in utero, however, is extremely rare even by the placental way. There is a high death-rate from tuberculosis among infants, but the infection is postnatal. Dietrich of Berlin found that the death-rate from tuberculosis among children in Prussia is higher during the first year of life than in any other year.
The moral conclusion is that artificial abortion in pregnancy complicated with tuberculosis is never indicated except when the good of the child is at stake in the last stage of gestation.
Syphilis in pregnancy at times assumes peculiar malignancy. The virulence depends on the patient's power of resistance, and whether or not there are septic microörganisms mixed with the syphilitic spirochetes. There are, moreover, varying strains of spirochetes which differ in virulence, or there are familial idiosyncrasies. Tropical syphilis is worse than northern infections, and syphilis of the nervous system is often incurable. Fournier was of the opinion that a syphilitic woman who becomes pregnant is more likely to abort than a pregnant woman who becomes syphilitic. The percentage of fetal deaths is also greater in the first class than in the second. The longer a woman has been syphilitic, provided she has not been treated for the disease, the worse the prognosis for the duration of the pregnancy and the life of the fetus. The earlier in pregnancy the syphilis appears, the worse the prognosis for gestation. General fetal mortality in syphilis under the best circumstances is 75 per cent. Syphilis should be looked for in every case where the cause of an abortion is not evident. Ruge holds that in 83 per cent. of repeated abortions syphilis is at fault; late abortions are characteristic of this disease.
Inoculation with syphilis before conception almost always results in abortion. In 130 women studied by Le Pileur there were 3.8 per cent. still-births before infection by syphilis, but 78 per cent. after infection. In premature labor the child is, as a rule, born dead; less frequently it is born syphilitic; still less frequently it is born apparently sound, but the syphilis appears later; in a few cases, when the maternal syphilis is old, the child may be born normal. Interruption of gestation is the commonest symptom in syphilis complicating pregnancy.[202] The labor itself is affected: the pains are weak and tardy. Abnormal presentations occur frequently when the fetus is dead. Chancres on the cervix may cause obstruction, and there may be indurations so dense as to necessitate cesarean delivery. The perineum may become so friable as to tear, as De Lee says, "like wet paper."
When the mother is infected at the time of conception the child is always syphilitic. If the mother is infected early in pregnancy the child is almost always infected. If she is infected late in pregnancy the child may escape infection. Men with tertiary syphilis have begotten children without, to all clinical appearance, inoculating the wife. In such a case the mother may nurse the child with safety to herself, but the child will infect a wet nurse other than its own mother, and in very rare instances mothers in this condition have been floridly infected. The condition here described is called Colles's Law.[152] The doctrine of Colles's Law has fallen into disuse because we can now demonstrate by the Wassermann reaction that almost all apparently healthy mothers of this class are in reality infected. The term now used is "Syphilis by Conception."[153] The virus passes through the fetal placenta to the mother, although immunizing substances are held back by the placenta. A fetus cannot make immunizing bodies before its eighth month, and on that account the earlier the fetus is infected, the more likely it is to die. Recently, however, some scanty testimony has been collected which sustains Colles's Law in a few cases. Ledermann reported three cases, and Nonne others, in which the wives of men with tabes or paralysis bore syphilitic children and yet never responded positively themselves to the Wassermann test, or showed any symptoms suggesting syphilis. To this list Kroon[154] adds a case corresponding fully to the requirements of Colles's Law. A woman of twenty-eight years who had had eight abortions was delivered of a child with undoubted congenital syphilis. The child's father had been infected with syphilis twelve years before.[203] The woman showed no signs of syphilis, two Wassermann tests were negative, and she nursed the child without injury to herself.
Should the husband have florid primary or secondary syphilis, and infect his wife at impregnation, abortion is the rule. The commonest cases are those where the husband has been treated for syphilis more or less thoroughly before marriage. Even if at the time of impregnation the husband has no apparent infective lesion, the child is usually syphilitic, or it may show signs of the disease later in life. Ibsen's Ghosts is founded on a case like this. If the syphilis is recent, or uncured, the child dies, macerates, and is expelled. These conditions recur in pregnancy after pregnancy, until the virus is removed by time or drugs. As the nucleus of the spermatozoön is too small to carry the spirochete of syphilis, the infection is through the semen in a manner not yet clear to us.
Wolff[155] studied a group of nine syphilitic women and their children. There were sixty-six pregnancies, but only thirty-three viable children were born. Of these last fourteen died in childhood, three committed suicide at twelve, twenty, and twenty-eight years of age; and of the thirteen still living only two were normal. The others are all feeble-minded, epileptic, hysteric, or otherwise neurotic. Post[156] tabulated the mortality in thirty syphilitic families in which there were 168 pregnancies. Of these fifty-three ended in still-birth or miscarriage and there were forty-four early deaths—a total loss of 57 per cent. Of the children that were born alive 38 per cent. are now dead, and of the seventy-one that are alive only thirty-nine are apparently healthy. There are very many cases of diseased children and adults with serious lesions of obscure etiology, and in a great number of instances of anemia, malnutrition, extreme nervousness, aortitis, bone diseases, vague pain, and similar conditions, the origin is congenital syphilis. Stoll,[157] in sixty-eight such cases, found a positive luetin syphilitic reaction, and a positive Wassermann in 17 per cent.
Gottheil,[158] professor of dermatology and syphilography in Fordham University, holds that if a man has gone through a modern treatment for syphilis, given by a competent physician and extended over three years, and if during the fourth year, without treatment, he repeatedly shows a negative Wassermann reaction, he may marry. That is the common opinion of physicians, but it is decidedly erroneous.
In one series of 562 cases of hereditary syphilis observed by the great syphilographer Fournier, sixty children, or over 10 per cent., were infected more than six years after the primary parental inoculation. He tells of one woman who had nineteen consecutive still-births from syphilis. Gowers[159] says: "There is no evidence that the disease ever is or ever has been cured, the word 'disease' being here used to designate that which causes the various manifestations of the malady." This statement is too sweeping, but it is very near the truth.
Bruhns recently reported the outcome of the Wassermann test repeated about yearly from 1908 to 1915 in one hundred private cases infected with syphilis ten or more years before the time of the report. In forty-two the test was constantly negative; in thirty-two, positive at first but negative later; in seven, constantly positive notwithstanding repeated courses of treatment; in three, positive at first, then long negative, but finally changing to positive again; in eight, negative at first, then positive, and finally negative; and in eight, negative at first but finally positive. The last three groups are particularly significant. In some the long negative reaction, for five or six years, indicated cure, and physicians would pronounce such cases positively cured; but suddenly they changed to a positive reaction without any clinical manifestations showing at the time. After renewed courses of treatment in the following two years the reaction became negative. Among the cases with constant negative reaction there were some who developed brain syphilis, or tabes, proving that they were not cured despite the absence of clinical manifestations of the disease and the negative[205] Wassermann reactions. Professor Blaschko of Berlin, at the seventeenth International Medical Congress in 1913, in the presence of Ehrlich, Wassermann and Hata, said no one could even talk of a cure of syphilis until an interval of ten years without symptoms had occurred. Where a blood Wassermann is negative a spinal fluid reaction may be positive.
In from 60 to 75 per cent. of all cases of tabes or paresis members of the family other than the patient have shown infection. The proportion of infections in the families of tabetics and paretics is far larger than that found in families in which the syphilis does not go on to these extremes. Tabes is also called locomotor ataxia. It is a degeneration of a part of the spinal cord, with unsteadiness and incoördination of motion, lightning pains, disorders of vision, and other symptoms. Paresis is softening of the brain, with insanity and death.
These and other facts strongly indicate that the form of syphilis which ends in tabes or paresis remains infectious over a much longer time than ordinary syphilis does. No one has cured either tabes or paresis. Raven reported in 1914 an investigation of ninety families in each of which a case of metalues had developed. The interval between the date of infection and the marriage was known in about half of these, and it was four years in two families, five years in one, and from six to twenty-one years in ten! Fournier, in 4400 cases of syphilis, saw three cases where the tertiary symptoms appeared fifty years after infection, and in one case fifty-five years after infection. Bonnet[160] reported such a case which came to him for treatment fifty-four years after infection. The man had no children.
Syphilis that affects the nervous system as in tabes and paresis is an incurable syphilis, and there is no means whereby any physician, no matter how skilful he may be, can tell whether or not a given patient has such an infection. The physician, then, who tells a syphilitic that he or she is cured and lets such a person marry is responsible for all the evils that result from his rashness. Once a syphilitic, not necessarily always a syphilitic; but once a syphilitic, possibly and probably always a[206] syphilitic, and that no matter what the treatment or the lack of clinical symptoms. Damaged goods of this kind are to be looked upon as damaged goods forever.
Any man or woman, then, who has ever had a clear case of syphilis (and the diagnosis is easy, as a rule) is likely to be for the remainder of life a source of syphilitic infection. There is even question of late of spirochete-carriers, as there are typhoid-carriers and diphtheria-carriers, who may infect others while not suffering themselves. If one who has been a syphilitic marries without informing the other party to the contract of the condition, the injustice is, without doubt, very grave. I should call such concealment a mortal sin, and a condition exposing the sacrament to sacrilege.
Suppose the second party is informed of the old infection and is then foolish enough to risk the marriage. No one but an experienced physician has any notion of the indescribable horror that may come of taking this risk, and no one has the right to expose his own body to infection by syphilis for the advantage of marriage. There is no approach to a juridic equilibrium between these two conditions. If in such a marriage children are begotten and infected, (1) embryos will die without baptism; (2) later possible children will be born who will die of congenital syphilis; (3) possible children who will escape syphilis; (4) children who may have to pass through tabes or paresis to death, after begetting other degenerates.
A syphilitic embryo which dies without baptism is better than no child at all. It will live in a state of natural happiness after abortion. A baptized child which has congenital syphilis is immeasurably better off than a sound child that lacks baptism. Eugenics as a prudent investigation of conditions before marriage is a good thing; eugenics as the drivel of agitators, who cannot tell the difference between a gentleman and a corn-fed hog, is quite another thing. The marriage, therefore, of a person who has been syphilitic to one who knows or does not know of this condition gets its mortality chiefly from the damage to one of the contracting parties which is imminent. It is difficult to estimate the morality of the act as it refers to the children infected congenitally, and to society.
The natural order, charity, justice, and related principles give every child the right to be born with bodily health, if such an event is possible. If it is not possible in particular circumstances, then melius esse quam non esse, and the decision in each case depends on its own qualities.
If a physician knows that a person who has been infected with syphilis is about to marry, should the physician warn the innocent party?
There are several conditions: (1) the infected person about to marry may be actively infectious; (2) the person may be probably infective, as any one is who has once had syphilis; (3) the physician may know the fact of the infection officially or unofficially; (4) the infective person may have gone to the physician for treatment for a condition not connected with the syphilis—say, for a bronchitis or a broken bone—and the physician in the examination discovers syphilis.
Again, there are various kinds of secrets. St. Alphonsus Liguori[161] classifies secrets in three groups: (1) natural; (2) promised; (3) entrusted secrets. A natural secret is one which obliges us in justice to observe it if divulging it will gravely injure any one in reputation or possessions. We are not obliged to observe a secret of this kind at the risk of our lives unless the damage from the divulging would affect the community gravely. A promised secret obliges to silence either gravely or lightly, according to the intention of the promiser. Where reasonable doubt exists as to grave obligation, such obligation does not exist. A promise to secrecy made even under oath is not binding if one is obliged in justice to reveal the secret; therefore we must testify to the crime of another when a judge legitimately demands our testimony, even if we have promised not to tell anything. If a secret is entrusted to one, and divulging would cause grave damage, but justice, or similar circumstances, do not oblige us to reveal it, we are bound to observe it even when questioned by legitimate authority. Then we may answer we know nothing about it, at least for revelation. St. Alphonsus's text is: "Potes respondere te nihil scire, scilicet ad revelandum." His meaning seems to be: "You may say you[208] know nothing about the matter inquired into." Any other signification would be futile. To say literally, "I do not know anything I may tell," would only expose one to punishment for contempt. He seems to make the answer a conventional denial, like the "not guilty" of a criminal. A judge may not abrogate the natural right by which an entrusted secret is protected, unless the secret is already known in some other way, or there is a just cause for revealing it.[162]
When an entrusted secret, however, which is also called a strict or absolutely natural secret, is imparted expressly or tacitly, say, to physicians, lawyers, or priests, and becomes a professional secret, it obliges more strictly than any other. There are four conditions under which such an entrusted secret may be revealed, at least without mortal sin (except by a confessor): (1) If we have the presumed consent of the principal. (2) If the material of the secret is trivial, or if it is known from another source, or is already public. Is it a mortal sin to divulge a grave entrusted secret to a responsible person who is under the same bond? St. Alphonsus, De Lugo, and others say probably it is not, provided the secret is not divulged to the particular person from whom the principal wished it to be concealed. The term probably here is technical and refers more to the absolute truth of an assertion than to its practical application. (3) One might reveal such a secret without mortal sin, through inadvertence or thoughtlessness, or under the supposition that it is not a grave secret. Some moralists hold, however, that to excuse from mortal sin, the revealer must be certain that the matter of the secret is not grave. (4) Such a secret may be revealed if keeping it would cause public injury, or injury to an innocent person, or injury to the person to whom the secret has been entrusted; then the law of charity demands that it be revealed. Therefore, even if one has bound himself under oath, he may reveal the secret—always excepting a priest or confessor. This is the common doctrine of moral theologians. It is for the common good of human society that entrusted secrets be absolutely kept unless so grave a damage befalls another from such observance that it becomes more conducive[209] to the public good to reveal than to conceal. To let an infective syphilitic, for example, spread his contagion merely because an entrusted secret should be kept is a much greater damage to the public than a good.
Barrett[163] says a physician may not divulge the diseases of a family to an insurance company unless the family assents; he may not tell the man before marriage that the woman had been operated upon, say, for ovariotomy, unless the woman gives permission; nor may he let the woman know, before marriage, of those diseases of the man which are not contagious. Ho says further that if a man has had syphilis and is now completely cured, the physician may not reveal this previous condition to the woman.
That doctrine about ovariotomy, if it includes double ovariotomy, is disputed by physicians because, they say, such a woman is sterile and she knowingly is going to deprive the man of his chances of having children; secondly, a woman upon whom double ovariotomy has been performed is almost always a neurasthenic invalid with a marked tendency to insanity, and it is a grave injustice to any man to saddle such a degenerate upon him for life by treachery. The prospective injury to the man is so great that the physician should first try to induce the woman to divulge her condition, and if she does not, the physician at least may divulge it.
Secondly, I deny most emphatically that any physician can tell that a man who once has had syphilis is completely cured and is not a source of infection. The facts I have cited in this chapter prove conclusively that once a syphilitic always probably a syphilitic, and the risk is always so great that the physician is obliged first to insist that the man does not marry, and if the man persists the physician may let the woman know. If preparations for the marriage have been made publicly, the physician will, as a rule, for his pains from the woman and her family get only a rebuff and the woman will later get her syphilis more or less certainly. If the man is actively infective the physician is bound to let the woman know, through[210] her confessor if no other way presents, provided the man cannot be frightened out of his scoundrelism. If nothing else avails, the physician would be justified in reporting such a man to the Board of Health or the sanitary police. Barrett says the physician may be excused from divulging that the man has infective syphilis if such a revelation would cause the physician to lose the confidence of his patients. It never does have such an effect, although physicians constantly expose such cases in the interests of humanity. Because a man who is apparently cured of syphilis may or may not infect the woman, this doubt probably excuses the physician from the strict obligation of divulging the condition, although he may tell her if he wishes to do so, salvo meliore consilio, as far as the release from strict obligation to divulge is concerned.
If a patient with syphilis goes to a physician for the treatment of some other physical disability, and the physician discovers the syphilis in the course of the examination, this knowledge of the syphilis would be a tacitly entrusted secret. Whether, however, a secret that a man is actively infective or very probably infective is entrusted either tacitly or directly, it is not a privileged secret owing to the danger or certainty of extraordinary calamity to the innocent second party.
The fact that in these cases of active or latent syphilis the disease has been acquired criminally does not in itself affect the state of the question one way or another—a criminal syphilitic has a right to his reputation and goods despite his moral condition; but even where the disease has been acquired without moral guilt the syphilitic is always a formally or materially unjust aggressor in a prospective marriage to an innocent and uninfected woman, and is to be treated accordingly. If a woman may kill an unjust aggressor in defence of her chastity, and if quod liceat per se licet per alium, her natural protectors, kin, physician, and so on, may at least divulge the secret of the man's condition in defence of her from a fate which in many respects is worse than rape.
In keeping with this matter of entrusted secrets it is worth noting that physicians should remember that the case histories they leave after them at death, or which they leave unguarded[211] in their offices, are likely to be read by some third party who has no right to the secrets they contain. Case histories which the patients would not have divulged should be kept in cipher so far as proper names and addresses are concerned.
Gonorrhea is caused by the gonococcus discovered by Neisser in 1879. The name was given to the disease in the second century by Galen, who supposed that the condition is a spermatorrhea. The infection begins as a surface inflammation and gradually penetrates more or less deeply into the underlying tissues. In the male, gonorrhea may affect any part of the body; and when the disease is chronic it is a source of infection for years. If a man who has had gonorrhea wishes to marry after careful treatment, most physicians will permit him to do so if he passes the customary tests which indicate cure, but he is always dangerous. The tests are: (1) the microscopic and cultural examinations of the centrifugalized morning urine—the washings from the urethra must be negative after repeated trials and over a space of months; (2) the microscopic and cultural examinations of urethral spontaneous and artificial discharges must be negative in the same manner; (3) the microscopic and cultural findings of the secretion expressed from the prostate and seminal vesicles must be negative in the same manner; (4) urethroscopic examinations of the anterior and posterior urethra must show no unhealed lesions; (5) the complement fixation test is to be repeatedly negative. The complement fixation test is like a Wassermann reaction, but the antigen should be polyvalent. This test does not give a positive reaction where no gonorrhea is present, but it is often negative where the gonococcus is present. Hence a positive result has value, but a negative result has little or no value. All these tests are to be tried repeatedly, and if negative for months, the physician may say the man is probably cured, but no physician can guarantee the cure so as to take the responsibility of[213] the decision. Not one physician in five hundred can make these tests himself, because physicians in general lack the special training and the means to make them. As the effects of gonorrheic infection in a woman are so appalling, any woman who wittingly marries a man who has had gonorrhea is very rash, and the man who takes the risk of infecting such a woman is a rascal.
A physician is obliged to let a woman who innocently is about to marry a "cured" gonorrheic know of the man's condition, as in a case of supposedly cured syphilis. Taber Johnson, Noble, and other authorities, say no one can tell when a gonorrheic is absolutely cured.
In women infection of the cervix uteri occurs in about 80 per cent. of the cases of acute gonorrhea, and in 95 per cent. of all chronic cases. The infection may extend up into the uterus at the menstrual period or just after parturition. In the cervix, owing to the histologic formation, the disease tends to chronicity, but the inflammation within the uterus is much more likely to subside naturally. Chronic gonorrhea of the endometrium is usually accompanied by tubular infection. The infection of the uterus may be superficial or it may extend down into the underlying myometrium.
The inflammation extends from the endometrium to the Fallopian tubes and beyond, causing salpingitis, pyosalpinx, hydrosalpinx, tuboövarian abscess, tuboövarian cysts, and pelvic peritonitis. The most frequent form of tubal gonorrhea is pyosalpinx, or pus tube.
In the acute stage of tubal infection the tubes become elongated and swollen, and the mucous surfaces within are covered with a seropurulent exudate. This condition is called salpinx or salpingitis. When the condition advances so far that the external abdominal ostium of the tube is closed, a pyosalpinx forms. The pyosalpinx may be quite large. A hydrosalpinx is like a pyosalpinx, with both tubal ends sealed, except that its content is a serous or watery fluid. When infected material escapes through the distal end of the tube, perioöphoritis develops, and the ovary becomes adherent to the tube and other adnexa. More commonly only the surface of the ovary[214] is affected, but frequently the infection gets into the body of the ovary and causes oöphoritis. The ovary then swells and there is a tendency to the formation of retention and other cysts, or an abscess of the ovary. A tuboövarian cyst is a hydrosalpinx in communication with an ovarian retention cyst, and a tuboövarian abscess is a like formation.
Gonorrhea, especially in women, is likely to be very chronic. Emil Noeggerath, who in 1872 published a book[164] which changed the medical doctrine on the disease, said of women, "Once infected, always infected." Norris[165] reports a case where the gonococcus was latent in a man for twenty years, and he then infected his wife and wished to divorce her until he found that he himself was at fault. Sax[166] reported an infection after fourteen years; MacMunn,[167] one after fifteen years. These are exceptional durations in the male for virulence, though not for continuance of the diplococcus.
Neisser, who discovered the cause of gonorrhea, holds that, with the exception of measles, gonorrhea is the most widespread of all maladies. By sterilizing men and women and by abortion it holds down the birth-rate more than any other disease. The number of deaths from the consequences of gonorrhea (pelvic abscess, peritonitis, septicemia, endocarditis, and so on) is enormous. Norris thinks that 12,000 prostitutes die annually from the effects of gonorrhea alone. Woodruff[168] holds that 60,000 is nearer the truth. The estimate, too, is that 50 per cent. of all pelvic inflammatory diseases in women is gonorrheic; and Neisser, Bumm, and Fürbinger hold that from 20 to 50 per cent. of childless marriages are due to gonorrhea. Probably more than 20 per cent. of all the blindness in the world is from the same cause. The Committee of Seven,[169] in 1901, after examining most of the hospital records in New York and hearing from 4750 physicians, estimated that there were more than 220,000 venereal patients in New York City.[215] Bierhoff[170] reckoned that in 1910 there were about 800,000 gonorrheics in that city. In 1906, in Baltimore, there were 3310 cases of the infectious diseases like measles, diphtheria, scarlet fever, and tuberculosis combined, but 9450 cases of venereal diseases. In New York City, in round numbers, there are annually about 41,000 cases of infectious diseases, excluding the venereal group, but 243,000 cases of venereal diseases—over five times more cases of venereal diseases than of all the other infectious diseases together. Of 12,000,000 persons insured in Germany, 750,000 annually are infected with venereal diseases. In the United States navy between 1904 and 1908, with an average of 43,165 men in the navy and marine corps, there were 32,852 admissions to the hospitals for venereal diseases, and of these 11,526 were cases of gonorrhea. This report is far below the actual numbers, as only men incapacitated for work are included in the list. In the English navy in 1906 the daily number of men rendered inefficient by venereal diseases was 867. In the total relative number of venereal diseases the American army and navy, before the present war, were the worst in the world, the Japanese navy next, the English army and navy next.
Sullivan and Spaulding[171] reported on the prevalence and effects of gonorrhea in 522 women and girls in a Massachusetts reformatory for women. Of these women 75.7 per cent. had gonorrhea by positive diagnosis. The average length of time the infection had existed when diagnosed was four years and five months, but one woman had had the disease for twenty-six years, and seven had had it for over twenty years. In 82.7 per cent. there had been no cessation of the clinical symptoms from the time of infection to the time of diagnosis. Of the total number 68 per cent. had pelvic inflammation on one side, and 27 per cent. had it on both sides. There were 41 per cent. of the cases which had had surgical operations or which required such treatment.
Of 63 women committed for alcoholism 52.4 per cent. had gonorrhea, 42.8 per cent. had syphilis, and 9.6 per cent. had[216] doubtful syphilis; but of 400 women who had been at some time prostitutes 98.2 per cent. had gonorrhea, 65.5 per cent. had syphilis, and 9.5 per cent. had doubtful syphilis. Of 119 mental defectives among these women, 90.8 per cent. had gonorrhea, 61.3 per cent. had syphilis, and 6.7 per cent. had doubtful syphilis.
Dr. Thomas Haines[172] reported on 365 cases of boys and girls under eighteen years of age committed to an Ohio reformatory, and of these 20.8 per cent. had syphilis, and it was mostly acquired syphilis, not congenital—over one-fourth of the boys were so affected. McNeil[173] examined 1200 adult negroes in Galveston, Texas, for syphilis and found the disease in 30 per cent. of the 1200.
Howard Kelly[174] estimated that venereal diseases cost the United States three billion dollars annually, and Norris thinks this estimate too low. The ravages of the disease are so frightful, physically and morally, that any one who spreads it by infection, especially of an innocent woman, is guilty of the gravest moral injustice. Morrow[175] thinks that 250,000 married women in the United States are suffering from gonorrhea. As most of these unfortunate women are infected by immoral husbands, and as the invalidism and suffering they undergo are indescribable and cure is often impossible, the physician who permits a gonorrheic to marry without a protest is responsible for the evil as an accomplice; and, as has been said, once a gonorrheic, probably always a gonorrheic.
Pelvic inflammatory disease includes in the uterus and its adnexa alone metritis, salpingitis, oöphoritis, pelvic peritonitis, cellulitis, lymphangitis, and perimetritis. Pus may rupture into the pelvic cavity and set up local or general peritonitis or septicemia. It may burrow through from behind the uterus into the vagina, rectum, or other parts of the intestines, or into the bladder, and leave fistulas. Pus has been known to get through the abdominal wall itself. When the disease advances beyond the tubes there is, as a rule, invalidism until after the[217] menopause, although the woman may be cured by surgery. Even skilled surgery does not always cure, because it is practically impossible to get rid of the gonococcus once it has been fixed in the tissues.
In cases where the gonorrheic or other bacterial infection has been chronic in the uterine adnexa, palliative treatment will in a certain percentage of cases make surgical intervention unnecessary, and when such treatment does not avail we must decide between the total removal of organs and the partial removal. Partial removal is called conservative surgery, and the term conservative is used as a synonym of preservative. Prochownick[176] reported 420 cases where pus in the tubes or ovaries was let out extraperitoneally, and no organs were removed. Of these cases, one hundred and sixty, or 38 per cent., were permanently cured. Fourteen of the one hundred and sixty who had received only one treatment subsequently gave birth to children, and three aborted. After a second treatment twenty-seven remained well and three became pregnant, of whom one aborted. Olshausen,[177] a great authority in gynecology, used the palliative treatment, and he commonly waited for nine months after the infection and until the temperature was normal. Goth[178] reported excellent results in seven hundred cases of pelvic disease treated by the palliative method. The chief objections to this method are the time required to get the result, and the difficulty of controlling the patients and their chronically diseased husbands, who reinfect them despite the medical prohibition of marital intercourse.
In cases of chronic pelvic peritonitis the question comes up frequently whether the womb and both tubes and ovaries should be removed wholly or in part. The text-books decide the question without any heed whatever to the notion of the morality of mutilation as such. They take into account the age of the patient, whether she has children or is desirous of maternity, whether or not she supports herself by manual labor, her temperament[218] and character, and the results attained by men who have tried various methods of operating.
The conservative surgery of the uterus and its adnexa in gonococcal pelvic peritonitis was for many years looked upon with disfavor by surgeons. These conservative operations often failed or later required secondary intervention. Preliminary palliative treatment as now used greatly lessened the number of failures. Operations in peritonic conditions are dangerous because they may let loose encysted bacteria and start up a general septic peritonitis, which may be fatal. By delay and palliative treatment the virulence of the bacteria subsides, except where the woman is reinfected by her husband. In any case the blood-count should have been normal for at least a month and a half before any surgical interference is attempted. Olshausen waited nine months to let nature disinfect the pus.
The removal of a part of a tube is called salpingotomy; the taking out of the whole tube is salpingectomy; the opening up of a shut tube is salpingostomy. The presence of pus in a tube is absolute indication for removal according to the gynecologists at present. Howard Kelly and others have succeeded at times in such cases with conservative surgery, yet such treatment is now deemed obsolete—the dangers and failures seem to overbalance the little good effected. The end of conservative surgery is to try to restore function without pain, to preserve menstruation and ovulation, to put the organs in a condition to make pregnancy possible, and to preserve the internal secretion of the ovaries. The ovaries, so far as the woman's health is concerned, are the most important of her generative organs. If a woman is at the end of her child-bearing age there is no reason to preserve the tubes when they are affected, and conservation is likely to fail; but the ovaries should always be preserved, wholly or in part, when possible.
If one tube is infected from the uterus many gynecologists are inclined to remove both tubes. When a single tube is affected the cause is seldom the gonococcus, but some other bacteria which are not persistent. When both tubes are affected the cause is commonly the gonococcus, and attempts at preservation then fail, as a rule. Norris, who is a reliable authority,[219] holds that "the only cases in which a salpingostomy is justifiable is on old, non-active hydrosalpinges, and in those cases of tubal occlusion or phimosis resulting from extratubal inflammation, such as sometimes result from appendicitis or ectopic pregnancies."[179] When a tube is shut, if it can be opened the opening tends to close again. A few cases of subsequent pregnancy have occurred after salpingostomy, but such a result is exceptional, because the origin is usually the gonococcus, which destroys tissue and is very persistent.
The ovary corresponds to the testicle, and the Fallopian tube to the vas deferens. Removal of the ovaries, or removal or closure of the Fallopian tubes, renders the woman sterile, but removal of the ovaries has other profound effects beside sterility. Loss of the ovaries brings on suppression of ovulation, menstruation, pregnancy, and ovarian internal secretion, various neuroses, and a tendency to insanity in certain cases.
The testicles and prostate gland produce an internal secretion containing spermin, and the ovaries a similar nitrogenous base called ovarin, which acts like spermin. The suprarenal glands secrete epinephrin; the thyroid gland and the pituitary body also make internal secretions, and these secretions sustain the tone of the blood-vessels and effect immunity against those toxins that arise from metabolic waste substances while these are in the body before elimination. If there is a hypersecretion from one or more of these glands, the excess causes congestion of the cerebrum and cerebellum and of the nerve centres there, and one effect may then be a sexual erethism that leads to masturbation and similar deordination.
Castration in the male or ovariotomy in the female stops all production of spermin and ovarin. In man the prostate gland also ceases its function after castration, and vasectomy lessens the production of spermin. In castration or spaying, again, when we remove the power of producing spermin or ovarin, that function of the testes and ovaries whereby the body is immunized against poisoning by its own effete material is also inhibited, and evil effects arise from this waste material. These toxins act just as would an excess of spermin or ovarin—they[220] congest the cranial nerve centres, excite fever, neuroses, or temporary sexual erethism. This excitement may gradually subside as equilibrium is restored and neutralization effected, through a compensatory overproduction of the internal secretions by the other glands remaining in the body. Cimoroni[180] found after ovariotomy an increase in size of the pituitary body with dilatation of the blood-vessels. Goldstein[181] reported a case of gigantism from overactivity of the pituitary gland after castration. Acromegaly in cases where there was no castration has been accompanied by atrophy of testicles and ovaries. Cecca[182] found like effects in the thyroid, and several have observed these effects in the adrenals. All these results have also been produced experimentally on animals.
Women at the menopause frequently are observed who have become neurasthenic from the irritation of waste material intoxication which is not neutralized because the ovaries are ceasing to function. Ovariotomy in younger women produces this menopause artificially and suddenly; and women from whom both ovaries have been removed, as a rule, become neurotic invalids with a tendency to insanity if they are unstable in character or have a bad inheritance. If the whole thyroid gland is removed, death results from intoxication. Extreme obesity is an effect of undersecretion by the glands and a consequent lack of oxidation. Fat children have deficient glands, as a rule, and eunuchs grow fat as capons do. Removal of the ovaries before puberty arrests or prevents the development of the uterus; removal after puberty stops menstruation, the breasts atrophy, and there is an arrest of general physical growth.
Gordon[183] reported on 112 cases of oöphorectomy. Of these thirty-four had had before operation various symptoms of neurasthenia, hysteria, or psychasthenia, and vague abdominal disturbances. Surgeons in each of these thirty-four cases blamed the ovaries for the symptoms; and although these organs were not diseased in any degree, the surgeons removed them. In twenty-five of these cases there was no improvement whatever;[221] in the remaining nine there was improvement for a few weeks, but complete relapse later, and finally their symptoms grew worse. The obsessions became permanent and expanded. Those women in the group who had hysterical paroxysms began to have stronger and more frequent attacks. Several psychasthenics had to be confined in asylums for the insane. Three of the women who had complained merely of vague nervous symptoms, as pain in the abdomen, head, or back, or of constipation or diarrhea, after oöphorectomy grew irritable, highly nervous, quarrelsome, fickle, restless, showed a tendency to travel about, to complain of others; finally there was insomnia, and loss of appetite or voracity. In the remaining seventy-five cases one or both the ovaries were diseased, but both ovaries were completely removed. All these women developed symptoms like those described above, but several grew much worse in their mental condition than the psychasthenics among the first thirty-four women. The generally observed symptoms are: restlessness with a tendency to move from place to place; loss of self-control; dissatisfaction with all persons and things; want of interest in work; indolence; pessimism. Sometimes there are outbursts of anger, with a tendency to attack. The mental conditions do not, as a rule, become clearly developed melancholias or manias, although a few do grow definitely insane. The morbid symptoms, however, persist obstinately. After ten years' observation Gordon found no improvement in some of these psychasthenics.
When the ovaries must be removed for diseases like cystic degeneration or abscess, the surgeon leaves, if possible, part of an ovary, or he engrafts part of an ovary in the abdominal wound, under the skin, or elsewhere. This grafting is beneficial in many cases, but it has little or no effect in many others. The graft is absorbed and it disappears in a year or two, but before it is absorbed it makes the onset of the surgical menopause gradual and thus prevents much suffering. In thirty-two cases reported by Chalfant[184] the graft gave evidence of functioning in five of seventeen women from whom the uterus and ovaries had been removed; in others it acted for months[222] and then failed; in others it lessened the unfavorable symptoms; in others it had no effect at all. Stocker[185] reported two successful implantations of ovarian grafts and one testicular graft.
Giles[186] says that in his series of 157 cases of double oöphorectomy severe mental depression occurred in various groups in from 10 to 33 per cent., and two women became insane. Sex instinct was abolished in 16 per cent. Dickinson[187] found, in 200 cases where one or both ovaries had been removed, that not more than 20 per cent. fell into the surgical menopause even when the uterus had been taken out; but Giles, in 50 removals of one ovary, found irregularity, diminution, or cessation of the menses in 16 per cent. Carmichael, Valtorta, and McIlroy[188] discovered in animals a compensatory hypertrophy of the remaining ovary after one ovary had been removed. The internal function and nutrition seem to depend upon the ovarian secretion, as atrophy occurs after bilateral oöphorectomy. In all operations upon or near the ovaries there is likelihood of interference with the blood supply of the ovary, either by including ovarian arteries in the ligatures, or by tension of these vessels, which occludes them, or by malposition and prolapse of the ovary, which kinks them: these accidents result in degeneration or retention cysts. In most cases of pelvic peritonitis the uterus is retrodisplaced, and this position prevents cure until it is corrected.
When there is pus in the ovary, resection, in the opinion of gynecologists at present, is not an advisable operation; the ovary should be removed. Watkins,[189] however, says he resects small ovarian abscesses in young women with good results. In resection the blood supply is, as has been said, usually disturbed, and the cause for the operation is, as a rule, the gonococcus, and both these circumstances make the prognosis bad. The stitches necessarily used in resection operations are an additional[223] source of irritation. Turetta[190] speaks in favor of resection in certain cases. A single retention cyst may be resected, especially when pedunculated. Boldt[191] had only one bad result in forty-five resections where a part of the ovary was saved. If the blood supply after the resection is evidently to be poor, resection is useless. Skill in surgical technic has much to do with success in all these cases. When the uterus is removed because of tumors, even near the time of the menopause, if one or both ovaries can be left in, this should be done. In such conservative operations Dickinson found 80 per cent. of the patients free from nervous disturbance at the time of the menopause.
Polak[192] describes an operation for the preservation of the menstrual function in double suppurative disease of the tubes and chronic metritis. He maintains that even if only one tube is infected, both should be removed because this apparently sound second tube will later, almost as a rule, show infection—probably by extension from the fundus of the uterus inside. Ordinarily inflammation of the tubes happens to be bilateral. Owing to the persistence of the gonococcus in the uterine muscle, surgeons are inclined to the removal of the whole uterus and both tubes. After such an operation menstruation ceases, and in the removal of the uterus the blood supply to the ovary is interfered with so that the ovaries degenerate. The consequent artificial menopause has a decidedly injurious effect on the woman's general physical and mental health. The parts of the uterus permanently infected by chronic gonorrhea are the cervical region, the fundus and the partes interstitiales of the Fallopian tubes. Polak advises that in cases where surgeons usually remove the tubes and the whole uterus they should instead cure the cervical infection by the cautery and take out the tubes, but in place of the removal of the whole uterus they should cut out a wedge including the fundus and the partes interstitiales of the tubes. This leaves the body of the uterus and does not injure the circulation to the ovaries. In the last[224] seventeen cases thus operated upon by him he had success.
When it is necessary to remove both ovaries and tubes an opinion very common now is that it is better to take out the uterus also, because in such cases the uterus and vagina atrophy and this condition later causes trouble. Giles came upon such trouble in 11 per cent. of sixty-two cases. As the uterus is useless after the removal of the ovaries and tubes, there is no reason why it should not be removed. The danger of atrophy is sufficient reason for the mutilation. In operations for pelvic peritonitis it is well to remove also the appendix, because it is nearly always diseased, or it will give trouble from adhesions later and cause a secondary operation. It has no function we know of at present.
In conservative surgery of the uterus and adnexa for pelvic inflammatory diseases, the results attained by four skilled surgeons are: Giles cured 90 per cent. of 132 cases; Polak cured 35 per cent. of 300 cases; Robins cured 100 per cent. of 20 cases; Norris cured 73 per cent. of 191 cases. Polak's patients became pregnant after operation much oftener than those of the other operators. Seventeen per cent. of his patients, from whom he removed one ovary and resected the other, became pregnant. Giles found that of his married patients under fifty years of age at the time of the operation 25 per cent. became pregnant and went to term. They bore twenty-five children. Five of these also miscarried. In sixty-eight of Morris's cases seventeen were delivered of living children after the operation; three had two children each, one had three children, and there were seven miscarriages. In one of his cases where he removed one ovary and both tubes, the woman bore a healthy full-term child two years after the operation. Dudley[193] found that about 10 per cent. of 2168 cases of resection became pregnant after operation. Ectopic gestation is likely to occur in a few cases after conservative operations. Giles had seven such cases in his series of 132 operations, Polak one, and Norris two.
When it is necessary to remove the uterus, the choice between supravaginal hysterectomy, where the cervix is left in after the destruction of its mucosa, and panhysterectomy,[225] where the cervix and the body of the uterus are removed, offers no moral problem except the necessity of deciding upon what will be best for the woman. Rupture of a pus tube is a very dangerous accident—all the patients suffering from such a rupture die if not operated upon, and fifty per cent. die even after operation. A physician may do this damage by ignorant or careless examination, and he may be morally responsible for the death. The accident happens not unfrequently from marital congress, and if the husband has been warned by a physician but does not heed this warning, he is guilty of murder if the woman dies after rupture of the pus tube.
Pregnant women are more liable to infection by the gonococcus than non-gravid women, because of the increased blood supply to the generative organs in gestation, and the softening of these organs. For the same reason, latent gonorrhea is likely to become active and to spread during pregnancy. A like activity and extension of latent gonorrhea often occurs during menstruation. Women with gonorrhea are commonly sterile—this is the chief reason why prostitutes are usually sterile. In married women gonorrhea may cause dyspareunia; it may bring on abortion through endometritis; it may shut the tubes and prevent conception; it may destroy the ovaries.
The disease is extremely frequent during pregnancy. Gurd[194] isolated the gonococcus in 52 of 113 pregnant women who came to his dispensary service because of pelvic pain. Leopold, Stephenson, Fruhinholtz, and many others estimated that about 20 per cent. of all pregnant women have gonorrhea, but more recent observers think that from 5 to 10 per cent. is nearer the truth.
When a pregnant woman has gonorrhea great care must be taken in treatment to prevent abortion. Powerful antiseptics in the cervix, or dilatation of the cervix, are not permissible, and operative interference is to be delayed as long as possible—in each instance to avoid abortion. The vaginal douche as a routine treatment is not used now by obstetricians in these cases. When the gonorrhea is in the uterus douches of hot bichloride solution, 1 to 10,000, are used twice daily during the[226] last few weeks of gestation, with the intention of saving the infant's eyes from infection during delivery. After delivery the cavity of the uterus should not be entered with instruments lest infection be carried in, unless absolute necessity requires this instrumental procedure. Post-partum gonorrheal sepsis is differentiated from other septic conditions chiefly by the history of gonorrhea in the husband, by bacteriological examinations, and by the technical differentiation of symptoms.
The moral guilt of a person who infects another with gonorrhea is affected by the extent of the physical injury done. Gonorrhea causes, besides the effects already described: (1) chronic cystitis, with all the suffering, loss of work, and danger of renal infection in such a condition; (2) lymphadenitis of the inguinal canal, and rarely of other places; (3) proctitis, or inflammation of the rectum, especially in women and young children; (4) ophthalmia, vaginitis, and proctitis in infants and children, and metastatic conjunctivitis; (5) stomatitis or inflammation of the mouth in adults and children; (6) nasal gonorrhea (a doubtful condition); (7) gonorrheal septicemia, bacteremia, or toxemia, which may affect any organ in the entire body; (8) bone and joint lesions: (a) gonorrheal arthritis in any joint in the body (this condition may be fatal, or it may leave permanent disability, or it may disappear); (b) tenosynovitis, or pain, swelling, and edema along affected tendon sheaths; (c) gonorrheal periostitis, where the bone and periosteum near a joint are affected; (d) perichondritis and chondritis, a rare condition, where cartilage is attacked; (9) endocarditis, or inflammation of the lining membrane of the heart (one of the most frequent secondary lesions of gonorrhea); (10) pericarditis, or inflammation of the sac which contains the heart; (11) myocarditis, an inflammation of the heart muscle itself, usually as an extension of endocarditis; (12) aortitis, or inflammation of the aorta—a rare condition; (13) phlebitis, an inflammation of the veins—a very rare condition; (14) thrombosis, or blocking of a blood-vessel by exudate (this may be fatal); (15) skin lesions, as erythema, erythema nodosum, bullous and hemorrhagic eruptions, hyperceratosis, and ulcers; (16) gonorrhea of the lungs in septicemia; (17) gonorrheal[227] pleurisy in septicemia; (18) gonorrheal nephritis, which is frequent in gonorrheal septicemia—the condition is often fatal; (19) perinephritis, a very rare condition; (20) gonorrhea of the nervous system, as neuritis or neuralgia, or neuroses, which vary from slight melancholia to severe mental disturbances; (21) parotiditis, a very rare condition; (22) otitis, or inflammation of the middle ear, a very rare condition; (23) suppuration in muscles, or under the skin; (24) wound septicemia; (25) venereal warts; and (26) epididymitis, which often causes not only sterility but impotence.
Campbell[195] reported a gonorrheal infection of a compound fracture at the ankle—it required four months to get the wound free of the infection. Gonorrheal obliterating epididymitis is quite common. Delbet and Chevassu[196] found 114 cases of male sterility in 131 cases of epididymitis. More than half of such cases are left permanently sterile, and if the function of the testicle cannot be restored by the surgeon the patient is impotent, and any marriage he would make, ... is rendered void. These two surgeons have restored function in six such cases by uniting the vas with the epididymis by Martin's operation. It is much easier to restore function after vasectomy than after obliterating epididymitis.
There are frequent cases of arthritic rheumatism in which the source of the infection is a chronic gonorrhea of the seminal vesicles. Fuller[197] has done 101 vesiculotomies for this condition, and of these twenty-three were gonorrheal. In these twenty-three the excision of the infected vesicles cured the rheumatism. In vesiculotomy great care must be taken not to cut the vas deferens. If it is cut the man is impotent until the vas is restored, and it would be a very difficult operation to reunite the vas if cut near the vesicles.
Of all the gonorrheal affections of the body the most dangerous and important are the cardiac inflammations and ophthalmia neonatorum. This ophthalmia is a purulent infection of the external parts of the eye in infants. It may be caused[228] by many kinds of toxic bacteria, but the worst cases are from the diphtheria bacillus (a very rare condition) and the gonococcus (a very frequent condition). Before 1881, when Credé introduced prophylactic treatment for ophthalmia neonatorum, every maternity hospital had a department isolated for the care of babies suffering with this disease. At the present day, however, despite the precautions taken, this disease is quite common. Pennsylvania and New York alone spent $242,000 annually for the support of asylums for the blind, and about 40 per cent. of the children in these institutions were blinded by gonorrheal ophthalmia. The United States spends $1,800,000 yearly on victims of ophthalmia neonatorum. Stephenson[198] tells us that in the practice of forty-one oculists who reported to him the gonococcus was found in 67.14 per cent. of their 1658 cases of ophthalmia. Mayou found the gonococcus in 63.5 per cent. of 1483 cases.
There is an infection of the child's eyes by gonococci possible even while the child is in the womb, but this is very exceptional; the infection happens in the vagina during delivery, as a rule. When the child's head is born its lids and eyelashes should be cleansed with vaseline, or 1 to 5000 bichloride, or carbolized oil, before the eyes are opened to put in the silver nitrate solution. This solution should be made from a pure drug or it will injure the eyes. A one per cent. solution is strong enough for routine work, but if the gonococcus is suspected, or if it is known that the mother has gonorrhea, then the lids of the infant must be everted and touched everywhere with a five per cent. solution of silver nitrate. This is neutralized with a salt solution and washed out before the lids are turned back. It is rash to trust any of the albuminoid preparations of silver, like argyrol, silvol, or protargol, in gonorrhea or suspected gonorrhea of the eyes.
If the child develops ophthalmia the treatment should be turned over to an oculist when possible. When a child can have a day and a night nurse, this method should be adopted, but ordinarily there is no nurse except some woman about the house or the mother. In such cases one eye, commonly the[229] right, does better than the other because the first eye treated is opened readily, but after the infant has been irritated it shuts the eyes so strongly that it is difficult to open them at all. The first eye treated is habitually the same. The nurse should begin to treat the eyes alternately on this account, or wait to treat the second eye until after the baby has quieted down. Iced compresses should be used, but not so long as to chill the eye very much—five to ten minutes at a time is enough. If the physician himself makes the applications of silver nitrate, the nurse should use some silver salt like argyrol. Three to eight grains of zinc sulphate to eight ounces of boric solution is a good regular eye-wash in these cases. Atropine must also be instilled to protect the iris. If only one eye is affected, the other eye should be protected under a watch glass sealed over it. All persons who have gonorrhea, or who treat gonorrhea, must be warned of the danger they are in of infecting their own eyes.
A new treatment of gonorrhea is described by Weiss.[199] The gonococci are killed by a temperature of 107.6 degrees Fahrenheit, and in eleven cases Weiss subjected men to a hot bath for forty to fifty-five minutes, with the temperature of the water gradually increased from 104 to 110 degrees Fahrenheit. In one instance the body temperature was raised to 108.5 degrees F. in a forty-minute bath and the gonococci disappeared at once. In the other cases the body temperature did not go up so high, but the vitality of the gonococcus was evidently reduced, and under a few local injections they all disappeared.
Diabetes Mellitus is rare in pregnancy, but when it does occur the disease is fatal in three-fourths of the children, and it hastens the death of the woman, according to the common opinion of obstetricians, but this opinion is disputed. In making the diagnosis we must exclude lactosuria and other pseudodiabetic conditions. A sugar reaction which is often mistaken for the glycosuria of true diabetes is from lactose in excessive milk secretion. This lactosuria is harmless. Again, when women are taking tonics or cough mixtures containing derivatives of wild cherry their urine may give a sugar reaction from the phloridzin of the wild cherry. The phloridzin so acts on the epithelium of the kidneys that it lets the blood-sugar escape into the urine. Medical writers who report diabetes in large numbers of pregnant women mistake these reactions for the reaction of true glycosuria.
In the genuine diabetes of pregnancy there is a high mortality. Offergeld,[200] in sixty cases, found that the women died within two and a half years, and that 76 per cent. of the children were lost. Diabetics commonly are sterile from atrophy of the uterus and ovaries: in a series of 114 diabetic married women, Lacorché found only seven pregnancies. In a third of such as do become pregnant abortion or premature labor occurs. Coma happens in 30 per cent. of these pregnancies, and it is almost always fatal. Delivery frequently causes collapse, coma, or sudden death. The liver in any gestation has more work than it has in the unimpregnated state, but a diabetic liver is unfit for almost any normal function. If albuminuria is found the prognosis becomes very bad. Diabetic women have poor resistance against a tubercular infection. Half their children[231] are still-born, and 10 per cent. more die within a few days after birth (many of these children are diabetic).
There is some evidence of heredity in diabetes—it is likely "to run in a family." Heiberg[201] reported one family in which five of thirteen children had diabetes; in another, four of eight children, the mother, two of the mother's brothers, and the maternal grandfather had diabetes. In another, two brothers, the father, and grandfather died of it. I know of a case where the only two sons and the father in a family died of it. Heiberg did not find any essential difference in the histology between the hereditary cases and those which were not hereditary.
Joslin[202] reported seven cases of diabetes associated with pregnancy. Four of the seven are now dead, one by suicide, one from uremia, one from coma, one from tuberculosis. Of the three living one is in good condition, one is not well and she has lost two of three children, and one is very ill with diabetes. In persons beyond middle age diabetes with proper treatment may go on for from ten to fifteen years before it is fatal, but it quickly kills young patients. A young woman at the marriageable age who has diabetes will die anyhow in two or three years, and if she marries and becomes pregnant she will die very probably in her first pregnancy.
When the child is viable, and the diabetic mother shows albuminuria, progressive weakness, or diacetic acid in marked quantity, it may be necessary to perform therapeutic abortion; but if this is done no anesthetic may be used, and great precautions should be taken to avert physical and mental shock. Even ergot acts badly with these cases. The last sacraments should be given in good time, especially if coma threatens. When labor begins in a diabetic and everything appears to be normal the sacraments should be given, because there is always danger of sudden collapse and death.
A method of effecting painless childbirth through the use of scopolamine and morphine was first used in 1902 by Steinbuechel, and in 1906 Gauss, of the University of Freiburg in Baden, reported a series of five hundred obstetrical cases in which scopolamine and morphine had been used. The woman's condition was called in Freiburg a Dämmerschlaf, a Twilight Sleep, because she is somnolent and forgetful of pain. In 1903 the chief obstetricians in several of the leading American and German universities tried the drugs, but they quickly abandoned the method because they found it dangerous and unscientific. The process was exploited here by McClure's Magazine,[203] The Ladies' Home Journal, and other lay periodicals. The articles in these magazines were written by persons who are not physicians, and their erroneous statements are misleading. The Ladies' Home Journal, however, while favoring the method, published letters from several leading obstetricians in the United States, all of whom are opposed to the use of these drugs during parturition because they had tried them and found them unscientific. The method is illicit morally, and it is unscientific.
Obstetricians divide a parturition into three stages. In most primiparae and many multiparae there is a prodromal stage, in which false labor pains (dolores praesagientes) are the most evident symptom. When the real labor sets in there are rhythmic uterine contractions about every fifteen minutes, which cause pain to the woman by the pressure of the fetus on the uterine nerves—dolores praeparantes. From the time the pains become rhythmic, and are effective in dilating[233] the neck and mouth of the womb, until the mouth of the womb is completely stretched and flush with the vaginal wall, thus completing the continuous parturient canal, is the first stage of labor. The fetal enveloping membranes (the "bag of waters") usually rupture at the end of this stage, but sometimes the bag bursts before the end, or as late as the second stage of labor. The first period is the stage of dilatation.
The second stage extends from the end of the dilatation until the expulsion of the child is completed. This is the stage of expulsion.
The third stage lasts from the delivery of the child until after the expulsion of the placenta and membranes and the retraction of the uterus has ended—the period of the afterbirth.
Normal parturition is always painful to the woman. As the labor progresses the pains gradually grow more intense, and the interval between them shorter. After a few hours the pain is strong enough to cause the woman to cry out, but there is a great variety in the endurance of these pains, as the women's characters differ. Neurotic women begin to scream and act hysterically even in the early part of the first stage. When the pains are fully developed each lasts about half a minute.
In most cases the infant comes out head first, but almost any part of its body may present. Before the advancing child part of the liquor amnii within the fetal enveloping membranes is forced down into the neck of the womb, and causes dilatation. In primiparae especially the bag of waters may rupture prematurely and thus cause what is called a dry labor, which is commonly tedious and painful. Often operative interference is required in dry labors.
In the second stage the pains are stronger, recur every two or three minutes, and are expulsive. The woman then strives to expel the child. She strains violently with the abdominal muscles—literally labors; her pulse is high, the veins of her neck stand out, her face is turgid, and her body is covered with sweat. When at last the head of the child is driven out the woman feels as if she were being torn asunder in the dolores conquassantes. The pain is so great that the woman may faint from it, but that is not the rule. After a pause the shoulders[234] are forced out, and then the trunk in one long convulsive effort. The umbilical cord is tied and cut, and the child is born.
After from five to twenty minutes the womb begins to contract again, but the pains (dolores ad secundum partum) are not nearly so intense as they were during labor. Then in from fifteen minutes to about three hours the placenta is expelled.
The pains of labor are so evident that the expulsive contractions of the uterus, of which the pains are symptoms, are themselves called "the pains." These pains in all scientific exactness of statement are, as has been said, agonizing. "In dolore paries filios" is a very literal text. The scopolamine-morphine method was devised with the intention of mitigating them, or mercifully rendering the woman unconscious of them during at least a part of the labor. If she is unconscious of pain she is thus saved also from shock and depression, which render her susceptible to infection. Such results certainly are immeasurably valuable if attainable without taint of moral evil, but as the method stands just now, they are not free from that taint.
Scopolamine hydrobromide, one of the drugs used in this method, is an alkaloid obtained from the roots of Scopolia (or Scopola) carniolica, and it cannot be differentiated chemically from hyoscine hydrobromide, which is made from henbane and other plants of the Solanaceae group. Rusby was of the opinion that scopolamine is really a mixture of hyoscine, hyoscyamine, and atropine: one-tenth hyoscine and nine-tenths hyoscyamine and atropine. Cushny and others find different proportions of these alkaloids. As the leaves of Scopolia are used to adulterate the belladonna leaves from which atropine is derived, hyoscine and scopolamine are substituted for each other—if, indeed, there is an any real difference between them. Some of the largest drug-houses in Germany before the war supplied hyoscine and scopolamine from the same stock bottle—the name depended on the asker. Even in a pure state hyoscine and scopolamine have the same chemical formula (C17H21NO4), and their physiological action is the same. Each can exist in three isomeric forms, and in one of these forms they turn polarized light to the left, in another to the right, while in a third[235] form they do not affect the light at all. The higher the rotatory power of the drugs, the more active they are physiologically. The levorotatory scopolamine has, according to Cushny, Peebles, and Hug, double the action of the inactive scopolamine on the cardiac inhibitory fibres of the vagus, but the levoactive and the inactive scopolamine produce the same effect on the central nervous system. The drug on the market is usually composed of a mixture of the levoactive and the inactive forms, and as one or the other predominates the results differ: the rotatory power of a given specimen should be known. Old solutions of scopolamine decompose and give rise to toxic substances. Gauss attributed post-partum hemorrhages in the women and asphyxia in infants to these decomposition products, but he avoided these untoward effects somewhat by cutting down the morphine dose. He had five infant deaths before he cut down the morphine, and 25 per cent. of the children were intoxicated. The chief action of scopolamine or hyoscine is upon the cerebral cortex, producing sleep, which is accompanied often by a low delirium. They depress the centre of respiration, and have a depressant effect also on that part of the spinal cord which governs the motions of the body. They intensify the action of morphine and other narcotics.
Morphine, which is used to prevent pain, is the chief drug in the twilight sleep method, and it is greatly intensified in action by the presence of scopolamine. When, however, morphine and scopolamine are given to a pregnant woman hypodermically, these drugs are at once carried by the blood to the fetus. Children for years after birth all withstand the action of morphine badly, and a fetus in utero may be overwhelmed by it. Just in this fact lies the chief moral crux in the use of the twilight sleep method of obstetrical delivery. The woman may go on to the end more or less safely in competent hands, but if constant watch is not kept at the bedside by a skilled observer the infant is liable to be killed, and the danger comes to it not solely from the drug directly—it may be drowned in the amniotic fluid, its condition may be masked by the restlessness of the mother, which prevents proper observation: when a woman is plunging all over the bed, as is extremely common in twilight[236] sleep, the pulse-rate of the baby cannot be properly watched.
If the mother happens to be particularly susceptible to scopolamine or morphine, the first will cause delirium and the second coma; or the respirations may become arhythmic and be reduced to only five or six a minute. The kidneys may be affected by the morphine so as to bring on total suppression of urine. Labor is prolonged, and it may be very much prolonged. In some women uterine atony is induced by the morphine, with very dangerous consequent post-partum hemorrhage. Morphine relaxes all musculature, and it relaxes the muscle of the arterial walls and so disposes to hemorrhage. There is little or no premonitory symptom of these idiosyncrasies (except in the case of an injured kidney) to inform the physician that he should avoid the scopolamine-morphine treatment.
Dr. Polak, professor of obstetrics at the Long Island College Hospital, reported[204] on 155 cases of the twilight sleep method, and he is in favor of it under several restrictions. He uses the drugs from ampules which contain one two-hundredth of a grain of scopolamine and half a grain of narcophin, which is a proprietary drug said to be composed of the meconate of morphine with the meconate of narcotin in molecular proportion. Morphine itself is a tribasic meconate, and narcotin, of course, another opium derivative. The American Council on Pharmacy and Chemistry was unable to accept the claims made for narcophin.[205] Polak says he finds no difference between morphine and narcophin.
In the twilight sleep treatment the patient, especially if she is a primipara, should be definitely in labor before any injection is given. She should have pains occurring at regular intervals, preferably every four or five minutes, before the first injection of scopolamine and morphine is administered; that is, the first stage of labor should be well advanced. Gauss gives one-sixth of a grain of morphine at the first injection, and Polak nearly three-fourths of a grain of narcophin, with one two-hundredth of a grain of scopolamine. If the woman is a[237] multipara, Polak begins the treatment at the very beginning of the pains. The patient is kept in bed, in a darkened room, removed from all noise and excitement. Some stop the ears and blindfold the patient, and, according to Baer of Chicago, the women are put into restraining sheets as a routine practice in certain clinics to keep them from infecting themselves. The ordinary practice is to give a half dose of scopolamine an hour after the first dose and about every two hours thereafter, according to the indications. The morphine may be discontinued, or used approximately every six hours in a long labor. Smaller doses are required if the first is given early in the labor, and larger if the pains have been well developed. In these latter cases the danger to the child is, of course, greater.
The condition of the patient's pulse, respiration, pupillary reaction, and the frequency and character of the uterine contractions are constantly watched, to guard against poisoning. Fonyo[206] reported two fatal poisonings by the scopolamine-morphine method as used in surgery. Both were operations for the delivery of women by laparotomy, and in each case the centre of respiration was overwhelmed. In each of these operations only one-hundredth of a grain of scopolamine and one-third of a grain of morphine had been used, but chloroform was administered later. Robinson recently reported the fatal poisoning of a negress by scopolamine, and Chandler of Philadelphia two more where one thirty-third of a grain of scopolamine had been used. One-ninetieth of a grain given hypodermically has caused severe toxic disturbance which lasted for twenty-eight hours, and Root[207] reported a case where one three-hundredth of a grain given by mouth poisoned violently.
In Freiburg, Gauss tests the consciousness of the women about every half hour by showing them some object, and if they remember having seen this object he gives an additional dose of scopolamine. Polak says this memory test is not necessary: even if the patient gives outward evidence of pain by cries and motion, she is apparently but very dimly conscious in his opinion.
The progress of the delivery must be constantly watched by repeated extraäbdominal or rectal examinations, following the fetal shoulder as it rotates—and not by vaginal examinations—to avoid sepsis. The fetal heart must be auscultated every half hour at most, between and during the pains. If the child's pulse grows arhythmic or slow between pains, these are bad prognostic signs. All use of the drugs is to be discontinued, and the child is to be delivered at once to save its life, by the most suitable method and route.
Polak holds that the solutions of the drugs must be absolutely pure, and that hyoscine cannot be substituted for scopolamine, but that narcophin is no better than morphine: the American preparations have produced delirium. As I have shown, no one can possibly tell the difference between hyoscine and scopolamine, even by chemical analysis. All we can do is to take the druggist's word that the drug at hand was made from Scopolia and not from Hyoscyamus niger. It does not make any difference which is the source of the supply.
Polak says the morphine shortens the first stage of labor by softening the cervix, but that the treatment lengthens the second stage. Other observers have not found that it shortens the first period. He tells us that if this second stage—that is, the time from the full dilatation of the os until the delivery of the child—lasts over an hour in multiparae, or over two hours in primiparae, delivery must be effected by the Kristeller expression or by low forceps. In the Kristeller expression the child is pushed out of the canal by the hands of the physician applied to the fundus uteri. It should be a method of last resort, because there is danger of rupturing the uterus, of tearing the placenta loose, or of crushing an ovary.
In his report Polak says he has had no failures; the patients had no recollection of the labor; in the first series of fifty-one the children showed no sign of asphyxiation or even cyanosis except in two cases. In this first series one patient had a long second stage and the child had to be resuscitated. There were, he said, no post-partum hemorrhages; no low forceps; the placentas were delivered without difficulty; none of the women showed signs of tire or exhaustion the next day; in[239] fact, they were better off than the women who have normal labor. This report is different from that made by other men just as competent, and in exactly the same circumstances; even Gauss confesses many failures. The lay journals say Gauss had no failures, but he himself should know. In April, 1915, I was told in New York City that there had been no failures there, yet in May, Dr. Broadhead, professor of obstetrics at the Postgraduate School of Medicine in that city, after observing seventy-two cases confessed[208] several failures where the child was concerned. One Catholic woman, a member of the executive committee in a Twilight Sleep League of married and unmarried women, was killed in Brooklyn by the method in the summer of 1915.
Dr. Charles M. Green, professor of obstetrics in Harvard University, tells us:[209] "My own observations, published in 1903, led me at the time to favor this therapeutic means of producing the 'Twilight Sleep,' and removing the consciousness of pain, or at least preventing all remembrance of it. I have long since abandoned this agent, however, for two reasons: First, because it has apparently been the cause, occasionally, of fetal asphyxia. Second, because the effect of the drug on the mother is often uncertain, and unless used with great care may cause unfavorable or dangerous results. Moreover, we have other and safer measures for the relief of pain in labor. So I have given up teaching the use of scopolamine in my lectures."
Dr. Williams, professor of obstetrics in Johns Hopkins University, and the author of a book on obstetrics which is very valuable, says:[210] "We have used the scopolamine treatment of childbirth in two separate series of cases at the Johns Hopkins Hospital, but in neither series were the results satisfactory, nor did they in any way approach the claims made for the treatment. We expect to do more with it next year." In the fourth edition of his Obstetrics, published in 1917, he thinks that the twilight sleep method will fall into disuse, or at least that its use will be restricted to a small group of neurotic patients.[240] From his experience, he says, the method is not adapted for private practice.
Dr. Hirst, professor of obstetrics in the University of Pennsylvania, tried the scopolamine treatment in the maternity hospital of the university in about 300 cases at three different times. He tried it first in 1903, but he found that if sufficient morphine is given to abolish pain there is danger of hemorrhage in the mother and of asphyxia in the child. At a meeting of the Obstetrical Society of Philadelphia[211] Hirst, commenting on a paper by Polak, said: "I am sorry to say I cannot agree with my friend Dr. Polak in his conclusions ... I had to discontinue morphia and scopolamine because there were too many cases of post-partum hemorrhage, too many cases in which forceps had to be used, too many asphyxiated babies. So I am not an enthusiast for 'twilight sleep.'"
Dr. Joseph B. De Lee, professor of obstetrics in the Northwestern University Medical School, Chicago, and the author of a book on obstetrics which is now one of the best we have in English, tells us[212] that the impressions he received from studying ten cases of childbirth in Professor Krönig's clinic at Freiburg were "decidedly unfavorable to the method of 'Twilight Sleep.'" In all the ten cases, he testifies, the birth pains were weakened, and labor prolonged—in two instances for forty-eight hours. In three cases pituitrin, which is in itself a dangerous drug to use before the uterus has been almost emptied, had to be given to save the child from imminent asphyxia. In five of the cases forceps had to be used owing to the paralyzing effects of the drug, and all these forceps cases were extensively lacerated. Several of the women became so delirious and violent that ether had to be used to quiet them, with the result that the infants were born "narcotized and asphyxiated to a degree." One child had convulsions for several days.
The complete failure in these ten cases is so obvious as to be a scandal, although De Lee does not say so. He abandoned[241] the use of the method twelve years ago, and in 1913 he visited the maternities at Berlin, Vienna, Munich, and Heidelberg, and found that all had tried the method and had rejected it.
Several so-called detoxicated substitutes for morphine, like "tocanalgine" and "analgine," have been tried; but these turned out to be morphine, and to be equal in strength to morphine as we ordinarily have it. These were the drugs that were advocated in the Cosmopolitan Magazine as "having nothing to do with the morphine-scopolamine treatment originating some years ago in Freiburg." They are morphine treacherously disguised, and the assertions in the Cosmopolitan were never retracted when attention was called to the untruth by the Journal of the American Medical Association. In the American Journal of Obstetrics for May, 1915, is a full description of these drugs (page 772).
Dr. Joseph Baer reported[213] sixty cases of the morphine-scopolamine treatment at the Michael Reese Maternity Hospital in Chicago, and his results were diametrically opposed to those Dr. Polak himself obtains. The rooms used were large, and had cork-lined sound-proof walls and doors; obstetricians and specially trained nurses were present day and night. The circumstances, then, were the best that could be had.
He used Merck's scopolamine at first, and later a solution made up after the formula of Straub of Freiburg, which is more stable. His doses of morphine were from one-eighth to one-fourth of a grain; Gauss uses one-eighth to one-sixth of a grain; Polak, as much as three-fourths of a grain of narcophin for his first dose.
Baer's series ended on February 5, 1915, and of his sixty cases only five were successful. Three of the successful cases received one-fiftieth of a grain of scopolamine in all, and some of the unsuccessful cases got as high as one-sixteenth of a grain, with only wild delirium as a result.
The labor was lengthened by about seven hours over untreated cases. As to the amnesia, in twenty-six cases the memory[242] was not dulled at all, although they received more scopolamine than thirty-nine cases in which the memory was cloudy.
Thirty-two women had unbearable thirst throughout the labor, and nothing would slake this thirst. Their incessant cries for water were very distressing to the attendants. Headache was present in twenty-seven cases and vertigo in thirty-one, and the headache, which was very intense in some women, lasted for several days after delivery.
Pain was diminished in thirty-nine cases, absent in one, as severe as in the average untreated woman in nineteen, and increased in one. That is, only one woman in sixty did not suffer the pain for which the treatment was devised. The reason evidently is that his dose of morphine was too small, yet if he went above this dose he ran the risk of post-partum hemorrhage and of narcotizing the baby. As it was, he had seven post-partum hemorrhages, but in a series of sixty unselected normal delivery cases he had only one hemorrhage.
Restlessness was present in eighteen cases, and delirium in nine; six of these women had to be wrapped in restraining sheets, and one had to be shackled for four days after she had overpowered a nurse in an effort to jump out of a window. It took three attendants to get her into the strait-jacket. Chandler of Philadelphia saw a woman in a like delirium who was shackled only after six attendants together had tackled her. Two physicians in the Chicago maternity were severely beaten by women in a twilight sleep delirium.
Baer says the serious risk of self-infection during labor through the uncontrollable motion of these women is a source of constant anxiety. They sit cross-legged, and the heel infects them with coli communis from the expressed feces. The dazed women constantly try to get at the vague pain with their hands, and on this account, according to Baer, some clinics that practise the twilight sleep method keep all the women in strait-jackets, but they omit to publish this fact.
One of Baer's patients died from a ruptured uterus, and her dead baby was taken from her belly-cavity. The drug will mask symptoms in a case like this. Sudden cessation of puerperal pain as a symptom of rupture, and the peculiar pain of[243] a premature loosening of the placenta, are both covered from observation by the drugs, the darkening of the room, and the tossing of the patient, which prevent proper examinations.
One patient had a mitral insufficiency and myocarditis. This should be an ideal case for the treatment, according to the twilight sleep men. The woman, however, after three doses of the scopolamine developed pulmonary edema. Her child was delivered in asphyxia pallida and resuscitated with difficulty.
Thirteen of the children did not breathe at delivery, six were asphyctic, and two cases relapsed into asphyxia. One child was killed, as we said, when the mother's uterus ruptured. Avarffy[214] had one fatal case in fifty, and Chrobak one in one hundred and seven.
Eight of the women had blurred vision after delivery, which lasted for over twenty-four hours; two had marked delirium for from two to four days after childbirth. As to exhaustion after labor, Baer says he found no difference between the twilight sleep women and the normal cases.
Some advocates of the twilight sleep method say that there is less use of the forceps in this method than in normal delivery. At Freiburg, for example, operative delivery has been "reduced" to six or seven per cent. Six per cent., as a matter of truth, is two per cent. above the normal average for forceps delivery in eighteen German maternities. In 95,025 deliveries in these hospitals the average forceps delivery was 4.5 per cent., and some were small teaching hospitals where the forceps were used on any provocation for class demonstration. The twilight sleep method has a much higher operative delivery, and this varies, of course, according to the skill and judgment of the operators.
Holmes, one of the first in Chicago to try the newly revived method, says[215] that in July, 1914, before the great war broke out, there were twenty-five malpractice suits pending in one German city as a result of the morphine-scopolamine fad. He quotes a noted obstetrician on this subject: "If you will[244] use the method, have the patient in the best hospital possible, with all the appurtenances requisite for the revival of the child; if you do not know, learn at once the differences between asphyxia, oligoapneia, and narcotic poisoning, and the methods of treating them; get the best and the most reliable product called scopolamine; and then be sure you are in a position to be adequately defended by a lawyer versed in malpractice suits."
This is the state of the question. Two or three men in the best circumstances say they get one hundred perfect results; other men, equally or far more skilled and in equally favorable circumstances, get one hundred results which are anything but successful, often a disgrace to science, and undoubtedly immoral. They are immoral because they risk human life in an attempt to ease a physiological pain, and this is not a sufficient reason; moreover, these attempts fail oftener than they succeed. The second group of practitioners have no motive except honesty to induce them to make their unfavorable reports of failure. The reports of the two groups are directly contradictory, and the judgment is thus a matter of motives. Testimony from women who have gone through the process is not to be taken into account. They were dazed, and in any case they are not competent to judge a matter which is wholly technical.
We know the limitation of morphine and scopolamine and we cannot improve their use. If enough is given to still pain, we take a criminal risk; if we do not give enough to remove the sense of pain, why not use the safer nitrous oxide, ether, and chloroform? If enough morphine and scopolamine are administered early in labor to a multipara, the labor is commonly stopped; if this dosage is given after the pains are developed, the baby is born, as a rule, before they take effect.
The State of Indiana in 1907 enacted a vasectomy law which obliges the superintendents of some prisons and asylums to appoint two surgeons whose office is to sterilize sexually criminals, idiots, imbeciles, and similar persons, if these surgeons, in consultation with the chief physician of the institution, deem the propagation of children by such so-called degenerates detrimental to society. The same law has been incorporated in the statutes by New York, New Jersey, Washington, Iowa, Nevada, Wisconsin, Connecticut, California, Utah, Kansas, Oregon, and Minnesota. The law has been proposed several times in the Legislature of Pennsylvania, but it was vetoed twice and held up once in the Assembly.
In New Jersey there was question of sterilizing an epileptic girl, and the Supreme Court of that State[216] decided in 1913 that the law is contrary to the State and Federal constitutions. In 1916 Probate Judge Lapeer of Michigan declared the law as passed in his State in 1913 unconstitutional, but the State appealed against this decision. The Supreme Court of Washington[217] decided in favor of the law in a case where a man convicted of rape was sentenced by the trial judge to life imprisonment and to vasectomy as a punishment. The constitutionality of the Iowa law is on appeal to the United States Supreme Court after a Federal judge had declared it unconstitutional. The law in Indiana was put into effect in hundreds of cases, but Governor Marshall set the law in abeyance. Two Federal judges in Kansas said the law is unconstitutional[246] and granted an injunction against its application in a particular case. In 1808 the superintendent of a Kansan institution for the feeble-minded castrated forty-eight boys. Up to April, 1916, about twenty-five feeble-minded boys in the Wisconsin institution at Chippewa Falls were sterilized, and the authorities then said they intended to sterilize the girls. The law has been advocated by alienists in Switzerland, and French and English physicians have advocated it.
The reason given by the advocates of this law is the alarming prevalence of feeble-mindedness with its tendency to criminality; and as, they say, heredity accounts for 65 per cent. of feeble-mindedness, the feeble-minded should be prevented from propagating their kind. Sweden, with 5,500,000 inhabitants, has 18,000 insane, 14,000 idiots, 20,000 imbeciles, and 7,000 epileptics. Much of this degeneracy is due to the notorious alcoholism of the Swedes, which only lately has been brought under some control. Pennsylvania had about 17,000 feeble-minded in 1913. In a single county almshouse in that State were 105 women who had given birth to 101 defective children. One feeble-minded couple in the same State had 19 defective children; two other families had 9 imbeciles and 7 idiots. In New Jersey the history of 480 individuals of the famous "Kallikak" family (a pseudonym), descended from a feeble-minded woman who lived at the time of the Revolutionary War, has been traced out, and of these descendants only 40 were normal. New York State has 32,000 known feeble-minded persons. One State school for the feeble-minded in Indiana in 1908 had 1054 inmates. There are 6000 mentally defective children in the schools of Chicago. An investigation made in Illinois about 1907 brought out the conclusion that all the defectives and delinquents in that State at the time could be traced to 150 families. Poehlmann of Bonn traced the descendants of one female drunkard through six generations in 800 individuals, and of these 107 were illegitimate, 102 were beggars, 181 were prostitutes, 76 were criminals in a grave degree, 7 were murderers, and they had cost the State $1,206,000. The Jukes sisters, two illegitimate prostitutes in New York State, in five generations bred 709 criminals. Fifty-two[247] per cent. of the women were prostitutes, whereas the ordinary ratio of prostitutes to other women is 1.66 per cent. Alcoholics engender degenerates. In three generations of 215 French alcoholic families, Legrand found that 60 per cent. of the children were degenerates. Bourneville found that 62 per cent. of 1000 idiotic, epileptic, and feeble-minded children in Paris had alcoholic parents.
Hereditary transmission is certainly a cause also of many diseases of the nervous system. Friedrich's ataxia is hereditary. It is an incurable progressive incoördination of the limbs, tongue, larynx, and eyes, which attacks commonly between the tenth and the twentieth year, and the patient dies from some intercurrent disease, usually an infection. Progressive muscular dystrophy is also hereditary and incurable. The legs and trunk atrophy, and death comes from an intercurrent disease. Related to this malady are hereditary progressive neurotic muscular atrophy, progressive spinal muscular atrophy in infants, and progressive spinal amyotrophy in adults. Amaurotic (amaurosis, blindness) family idiocy is hereditary, and the child dies at about two years of age. Huntington's chorea appears in every generation of an affected family. Its symptoms show between the ages of thirty and forty years, and it progresses from choreic and ataxic signs to dementia and death. The death is often by suicide. In eastern Long Island, southwestern Connecticut, and eastern Massachusetts 962 cases were all traced back to six persons, three of whom were probably brothers, who came to America in the seventeenth century. In the 3000 relatives of these choreics were 39 cases of epilepsy, 51 cases of cerebral inflammation, 41 cases of hydrocephaly, 73 feeble-minded children, and other evidences of neuroses. The heredity in this disease is apparently Mendelian. Besides the diseases enumerated here, there are several pathologic conditions of the eyes which are hereditary—presenile cataract, stationary night blindness, and retinitis pigmentosa. If the persons who have these diseases are sexually sterile, evidently the heredity so far as they are concerned will be cut across; hence the advocates of legal sterilization wish to have these patients sterilized to protect society.
The surgical operation by which the man is sterilized according to the State laws mentioned above is an interruption of the continuity of the vasa deferentia near the testicles. This interruption may be a severing of each vas, a cutting out of a part of each vas, or a ligation of the vasa. The term vasectomy is now used loosely to cover all these methods. The vas deferens, or seminal duct, passes from the testicle up along the groin on each side, in through the belly-wall by the inguinal canal, down along the pelvis and under the bladder, where it opens into the bottom of the urethra a short distance in front of the bladder exit. Each vas is about two feet in length, and it has a diameter of one-tenth of an inch throughout the greater part of its length, but its lumen is extremely narrow.
There are two essential parts in the semen, the spermatozoa and the carrying liquid. The spermatozoa, which fructify the ovum, are formed in the testicle; the liquid, which is the essential vehicle of the spermatozoa, and without which the spermatozoa are inert and sterile, is secreted, except a few drops from the testicles, at the distal end of the vasa deferentia under the base of the bladder, in the seminal vesicles, the prostate gland, and Cowper's and Littré's glands. The semen is made up of 90 per cent. water and 10 per cent. solids, and in these solids is the nitrogenous base called spermin, which is produced by the interstitial cells of the testicles and the prostate gland. Ovarin, secreted from the ovaries, corresponds in the woman to spermin in the man. The ductless glands, and some that have ducts, produce secretions which sustain the tone of the blood-vessels and neutralize the toxins from waste substances while these are in the body before excretion. An excess of spermin or ovarin causes congestion of the cerebrum and cerebellum and the nerve centres there, with consequent sexual erethism. When there is a pathologic sexual erethism from an excess of spermin or ovarin, vasectomy, castration, spaying, or the menopause cuts off this excess and the erethism disappears. Sometimes the waste product toxins excite the patient when the spermin or ovarin has been eliminated, just as the excess of spermin or ovarin excites, and the neurotic disturbance or[249] sexual erethism continues until compensation by other glands neutralizes the irritating substance.
The testicles in man are by no means the sole organ of generation. There are at least seventeen distinct organs in the male generative system. The seminal vesicles with the prostate gland are as necessary in generation as the testicles, as their removal sterilizes the spermatozoa and prevents the formation of the liquid vehicle. Castration effects an atrophy of several parts of the generative tract, and an irremediable degeneration; vasectomy cuts off the spermatozoa but causes no atrophy or degeneration, and the condition is remediable. Dr. Edward Martin of Philadelphia found active living spermatozoa in a testicle that had been ligated off for twenty years.
Running along the vasa deferentia, within the sheath of the two spermatic cords, are the spermatic arteries, the pampiniform plexus of veins, and the deferential arteries. These vessels, with the vas deferens and the sheath enveloping the bundle, make up the spermatic cord. In vasectomy, under local anesthesia, a slit is made through the skin of the scrotum behind, the sheath of the spermatic cord is opened, and the vas is isolated and tied or cut. The skin wound is left to heal. This operation is repeated on the second vas. If the blood-vessels in the cord are ligated or cut with the vas, the testicle will atrophy; if the vas alone is operated upon, the testicle is not injured. The person upon whom vasectomy has been done is conscious of no change. The semen is discharged as before the operation, but in a slightly less quantity, and it is, of course, sterile from the lack of spermatozoa.
Dr. Carrington of Virginia reported, in 1910,[218] twelve cases of vasectomy on convicts. He said ten of this dozen had been confirmed masturbators, and all were cured by vasectomy. One masturbating epileptic was cured of both conditions. Two dangerous homicides were rendered harmless and peaceable. One of these two homicides was a negro under a long sentence for murder. He grew insane in prison, and while insane killed a second person. A confirmed masturbator and sodomist, and a dangerous savage, he became lucid and relapsed into insanity[250] several times. A year after vasectomy he was "a sleek, fat, docile, intelligent fellow, a trusty about the yard."
Dr. Sharp of Indianapolis, after ten years' experience with the operation, during which time he did 456 vasectomies, says:[219] "There is no atrophy of the testicle, no cystic degeneration, no disturbed mental or nervous condition following." He says, further, that 176 men in the Indiana Reformatory asked him to perform the operation on them. Vasectomy tends to check masturbation, and the minds of the masturbators frequently improve after the operation.
If a man has been sterilized by vasectomy, restoration of function and removal of the sterility seems practically always possible. If a ligature has been used, releasing the ligature restores function. Dr. William T. Belfield of Chicago[220] restored function fully by removing the ligature eight weeks after it had been applied. In a letter to me, Dr. Belfield said: "My observation accords with the general experimental and clinical experience that the restoration of the lumen after vasectomy or ligation, or both, is more certain than the lasting occlusion of the vasa by these measures. The perseverance of natural forces in restoring the lumen of the vas—and the success achieved over such obstacles as silk ligatures—is surprising until one reflects upon the natural factors favoring such restoration. In one case I tied a waxed (to avoid cutting through) silk ligature tightly around the sheath of each vas; a specimen examined a month later was devoid of sperms; one six months later contained plenty of them. I cut down upon the ligatures, found them in place and neatly encysted, and removed them. Evidently the pressure from behind had squeezed a passage on at least one side. The gynecologists have learned that ligatures around the Fallopian tubes are apt to cut through, whereupon the tubal lumen is restored, though pressure must be less than in the vas. Even when a piece of the vas has been excised cases of spontaneous restoration have been observed in men and dogs."[221]
When the ends of a cut vas are released from cicatricial tissue, these ends may be sutured together; but as the lumen of the vas is extremely small, there is sometimes obliteration by occlusion at the juncture. Christian and Sanderson[222] described a method of preventing this obliteration. A piece of No. 0 twenty-day catgut is inserted three-eighths of an inch into each end of the vas, and these ends are brought together by two catgut sutures, leaving the inserted catgut in the canal. The ends heal together and the catgut in the canal is absorbed. This method has been used successfully to join the cut end of a Fallopian tube.
Gemelli[223] did vasectomy on eleven dogs and seven cats; about six months later he reunited the cut ends, and on dissection found restoration perfect, anatomically and functionally, in the eighteen animals. The vas deferens in these animals is smaller than in man; and therefore offers greater difficulty in the suturing. He used no inserted catgut, but told me he employed the method Carrel applies in joining cut arteries. In one case, where the dissection was broad, he successfully inserted a piece of a vas taken from another animal. Whether there is occlusion or not after end-to-end suturing depends largely on the skill of the surgeon.
Dr. Edward Martin of the Pennsylvania University[224] and Delbet[225] have removed sterility by effecting a patulous anastomosis between the vas and the epididymis, and this method is applicable after vasectomy by cutting, but it is not successful, as a rule. It has been done effectively where the vas had no stricture. McKenna,[226] in five attempts on men, succeeded once. Fürbringer[227] said that in his experience with a thousand cases of double epididymis, the condition is incurable in 80 per cent. of the gonorrheal infections.
Apart from the so-called vasectomy law, gynecologists quite frequently sterilize women who have chronic heart disease, tuberculosis, nephritis, diabetes, or hereditary mental taints. Some men, like Spinelli, Cramer, Polak, and others, would sterilize also in chronic anemia, persistent albuminuria, epilepsy, syphilis, contracted pelvis, diseases of metabolism, infections, and cirrhosis of the liver. There are several methods of sterilizing women—removal of the ovaries, ligation of the Fallopian tubes, resection of portions of the tubes, resection of the whole tube on each side, cutting the tubes and burying the cut end in the tissues by various methods, and destruction of the lining of the uterus by vaporization or the thermocautery. De Tarnowsky[228] describes the various methods. Some ligations and short resections have failed to sterilize. When the ovaries or uterus are removed, or the major part of the tubes are resected, or the lining of the uterus has been destroyed, the sterilization is permanent. Almost certainly function could be restored where the resection of the tubes is not too destructive. Apart from the matter of mutilation, the effects of double oöphorectomy are very grave,[229] and removal of the uterus or the ovaries merely for sterilization is not only immoral, but altogether unjustifiable scientifically.
A phase of this subject which is important and has occasioned much discussion is whether vasectomy causes sexual impotence or not. From a medical point of view, there is no question of impotence; physicians would say it causes sterility only. Most canonists, however, hold that the condition after vasectomy is technically impotence in the canonical sense. Ferreres of Tortosa, a leading Spanish canonist, in several articles in the Ecclesiastical Review, in Razon y Fe (xxviii, 376; xxxi, 496), and in his book De Vasectomia Duplici (Madrid, 1913), opposed my opinion published in 1912 and 1913, which then was that vasectomy does not cause canonical impotence. De Smet of Bruges[230] holds that it causes impotence. So do[253] Ojetti,[231] René Michaud,[232] Wouters,[233] Eschbach,[234] Capello,[235] Stucchi,[236] De Becker, Vermeersch, De Villers, and Salsmans of the University of Louvain, and others. Gemelli of Milan[237] agreed with me. The weight of authority is certainly in favor of the notion of impotence, but the arguments are by no means convincing, as virtually every canonist who has discussed the question has made gross misstatements of the physical facts in the case.
If a man or woman is impotent, the disability is an impedimentum juris naturalis, and as such it would nullify any marriage, no matter what the dispensation. There are two opinions among moralists as to the essence of canonical impotence.
I. Some hold that any permanent obstruction to fecundation, no matter in what stage of the physiological process or in what part of the genital tract it occurs, constitutes impotence. They maintain that a woman whose ovaries or uterus have been removed is impotent. Roman Congregations have promulgated several decrees in peculiar cases permitting the marriage of spayed women; but, these moralists say, it is not clear that in those special cases the entire ovary on each side of the whole uterus was taken out; they hold there is doubt as to the fact. And, since there is disagreement of moralists, the Holy Office or other congregations would give the same decision because of the dubium juris.
April 2, 1909, the Congregation on the Discipline of the Sacraments decreed that the marriage of a Spanish woman, from whom, according to the physician in charge of the case, the uterus and both ovaries had certainly been removed, should not be prevented.
February 3, 1887, the Holy Office made the same decree in the case of a woman from whom the uterus and both ovaries had been removed.
July 23, 1890, the Holy Office made the like decree under the same conditions.
July 31, 1895, the Holy Office permitted the marriage of a woman from whom both ovaries had been removed.
Another case, in 1902, in which the physician was not certain that the whole ovary on each side had been removed, was decided in the same manner.
There have been, then, four decisions so far permitting the marriage of women who lacked both ovaries, and three of these women lacked the uterus also. The Congregation of the Council has made four decisions in recent time forbidding the marriage of women because of impotence; March 21, 1863, a case in which there was neither vagina nor uterus; January 24, 1871, a case in which the vagina was only two inches in depth; September 7, 1895, a case in which the vagina was obliterated in greater part; December 16, 1899, a case in which the vagina was only five centimetres in depth.
That a woman who certainly lacks both ovaries is canonically impotent is the opinion of Antonelli,[238] Lehmkuhl,[239] Rosset,[240] Alberti,[241] Bucceroni,[242] and others. These men meet the decisions of the congregations concerning the spayed women by saying it is not certain the whole ovarian tissue or the entire uterus was removed, although as a matter of fact the physician in one case testified explicitly that both ovaries and the whole uterus were undoubtedly removed. That a woman lacking both ovaries is not impotent is the opinion of Gasparri, D'Annibale, Génicot, Berardi, Aertnys, Tanquerey, Ojetti, De Smet, and others.[243]
II. The second opinion on impotence is that this condition is caused exclusively by those permanent disabilities which exist in the copula itself. If the sexual act contains in itself all that is essential to generation, if the copula is de se apta ad[255] generationem, prescinding from all antecedent and subsequent, temporary or permanent, obstructions to generation, there is no impotence. In this opinion the woman without ovaries is not impotent, but the vasectomized man is; in the first opinion both the mulier excisa and the vasectomized man are impotent. The second group says the vasectomized man is incapable of performing an act de se apta ad generationem because his semen lacks the essential spermatozoa. If one objects that the spayed woman, who is not impotent according to some moralists that so interpret the decisions of the congregations, lacks the essential ovum, so that she cannot perform an act de se apta ad generationem because she has nothing to generate with, they answer that her copula is per se apta, that there happens in it everything which takes place in a copula from which generation actually follows. The vasectomized man cannot go through the form of the act with all the elements which, so far as the act is concerned, are required and sufficient for generation because he lacks the spermatozoa, but the mulier excisa can. His inability is intrinsic to the act, it vitiates the very substance of the act; her inability to present ova is not intrinsic to the act, they say. All that is necessary in her case is that she be capable of receiving the semen.
Marriage was instituted to beget children; that is the proper end of the contract, its basic justification. Whenever the debitum is used it must be with the intention of generating children. Even the use of marriage as a remedy of concupiscence is so secondary an end that it alone is not enough to legitimize marriage. Because a woman does not always have ova present in the tubes,—and there is no means of knowing just when the ova are present,—it is justifiable to repeat the conjugal act until the woman is impregnated; secondarily and dependently, the repetition may be a remedy of concupiscence. The sexual act does not form either the spermatozoa or the ova; these pre-exist. The spermatozoa are always released in a normal sexual act; the ova are not always present when the spermatozoa are released. A copula which is perfectly de se apta ad generationem supposes not at the time the presence of both sperm and ovum, but it does suppose[256] the possibility of the ovum, otherwise generation is utterly impossible; and every copula becomes justifiable solely because there is a hope that it may be present. It is a mere quibble to say that an act is de se apta ad generationem if by no possibility generation ever can take place; nevertheless the congregations in four cases have apparently judged to the contrary. In these special decisions, however, Rosset, Antonelli, Bucceroni, and Palmieri hold there was a doubt in the minds of the members of the congregation as to the complete removal of the ovaries or uterus. Bucceroni expressly states[244] that the Cardinal Secretary of the Holy Office told him personally the members of the congregation supposed in the particular cases that generation could follow. Therefore these decisions do not say that the mulier excisa in general is not impotent or potent; they merely gave the women of these cases the benefit of the doubt. Tho question is entirely open so far as these decisions are concerned.
Those who hold that vasectomy causes canonical impotence say also the constitution of Sixtus V. forbidding the marriage of eunuchs is applicable necessarily to the vasectomized man, because the semen from the vasectomized man, inasmuch as it lacks spermatozoa, is not genuine semen, and Sixtus V. said eunuchs cannot produce true semen. The relevant passage in the constitution is: "Cum frequenter in istis regionibus eunuchi et spadones, qui utroque teste carent, et ideo certum ac manifestum est eos verum semen emittere non posse; quia impura carnis tentigine atque immundis complexibus cum mulieribus se comiscent, et humorem forsan quemdam similem semini, licet ad generationem et ad matrimonii causam minime aptam, effundunt, matrimonium ... contrahere praesumant ... mandamus ut conjugia per dictos et alios quoscumque eunuchos ... contrahi prohibeas."
Sixtus V. says here: (1) that eunuchs "who lack both testicles certainly and evidently cannot emit true semen"; (2) that "although eunuchs may perhaps produce a kind of liquid resembling semen, this is by no means fit for generation or marriage"; (3) therefore eunuchs are forbidden to marry. The[257] effects of castration in the eunuch are: (a) that all spermatozoa are absent; (b) that, as a consequence of the absence of the testicles, the power of penetration is lost; (c) that, as another consequence, the liquor seminis, which normally is formed in the seminal vesicles, the prostate and other glands, is no longer secreted. The eunuch, then, is completely impotent, in the full sense of the term. Ferreres is of the opinion, erroneously, that eunuchs, as a rule, have the power of penetration and of emitting a humor semini similis, and that amputation of the penis is requisite to cause impotence in eunuchs. There are only five authentic cases of temporary apparent potence in eunuchs in modern medical records, and these are explicable as cases of erethism from waste-product intoxication.
The canonists who hold that the vasectomized man is impotent interpret the words of Sixtus V. to fit their opinion, although the vasectomized man has all the sexual potency of the normal man except that his spermatozoa are occluded. The potestas coeundi is not lost in any degree; neither he nor the woman is conscious of any change whatever. Only the microscope can tell that the spermatozoa are absent if the fact that he has been vasectomized is not told. Moreover, if vasectomy has been done by mere cutting without considerable resection, and especially if the vasa have been shut by ligation alone, no one can be certain that the occlusion is either certain or permanent. There is always doubt that the spermatozoa are present if the microscope is not used, and these canonists all disclaim the use of the microscope in such circumstances. The argument Ferreres uses, to the effect that the absence of spermatozoa is seriously injurious to the woman, is a supposition of his own arising from an erroneous notion of potency in the vasectomized. This absence is not injurious to her, but it is probably injurious to the vasectomized man because of the partial ejaculation. Onanism, which is different, is decidedly injurious to both the man and the woman.
Onanism, coitus interruptus, or withdrawal before ejaculation, which takes place extra vas, is intended to prevent impregnation. In the normal sexual act the male genital tract suddenly becomes congested with blood through nervous action[258] of centres in the lumbar cord and the cerebrum. Cowper's and Littré's glands secret an alkaline fluid which neutralizes the acid urine in the urethra and thus prevents killing of the spermatozoa. Muscular peristaltic action presses out the spermatozoa and the secretions of the seminal vesicles and the prostate. When the act is normal there is a complete emptying of the tract of semen and of the blood engorgement; in coitus interruptus there is incomplete ejaculation and only partial deplethorization. The seminal vesicles remain distended, and this distention, with the congestion of the prostate, causes continual excitation of the sexual centres without relief. There is irritability and exhaustion of the centres, and this state brings on premature ejaculation and final impotentia coeundi. Other common effects are tenesmus of the urinary bladder, incontinence of urine, nocturnal pollutions, sexual neurasthenia, pain in the legs, over the eyes, and in almost any part of the body, general weakness, headache, vertigo, cardiac palpitation, neurotic dyspepsia, and a train of psychic symptoms which not seldom end in suicide.
In the woman there is the like blood engorgement and a pouring out of the secretions of Bartholin's and the other glands, but deplethorization takes place later in the woman than in the man, and for this reason the woman suffers more from coitus interruptus than the man does. In onanism, as in masturbation, after the diseased conditions have been established it is extremely difficult to induce the patient to resist the almost overwhelming irritation.
The canonists have interpreted the text of Sixtus V. to the effect that the eunuch is impotent precisely and solely because he cannot produce semen "elaboratum in testibus." No man produces semen elaboratum in testibus—more than 93 per cent. of the semen is produced entirely outside the testicle; nothing but the spermatozoa and two or three drops of a lubricating fluid are produced in the testicles. The eunuch really is impotent because the removal of the testicles and their nervous system so breaks the genital circuit, which consists of at least seventeen distinct parts, that erection is prevented, the formation of spermatozoa is impossible, the secretion of the essential vehicle[259] of the sperm and of the fluids which render it fertile is cut off. The eunuch cannot penetrate and he cannot form any semen; he is impotent; the vasectomized man can penetrate, and he forms a semen which is sterile.
I think now the vasectomized man is really impotent for the reason that I think the mulier excisa is impotent, but he is not impotent because of the constitution of Sixtus V., which is not relevant at all to his case.
If the vasectomized man is impotent, the following cases are also impotent:
1. A man whose germ-cells have been destroyed by the action of the X-ray.
2. A man with double permanent occluding epididymitis.
3. A man whose vasa deferentia open into the ureters and not into the urethra.
4. A man whose vasa are shut by surgical operations for stone, or cysts of the prostate, or seminal vesicles.
5. A man whose seminal vesicles are shut by concretions, cysts, or tumors.
6. A man with bilateral cryptorchidism.
7. A man with a tuberculous condition of the testicles.
8. A man with absolute neurotic aspermia.
9. A man with congenital lack of development of the testicles or vasa.
Sterility in the male would exist only in advanced diabetes, general tuberculosis, senility, or in cases of absent or diseased prostate gland or seminal vesicles.
Here it is worth noting that since the copula must be natural, fit for generation in the natural manner, artificial impregnation by the use of instruments is immoral, and forbidden by a decree of the Holy Office, promulgated March 24, 1897. Artificial impregnation does not effect a copula which is by its nature proper to generation, but is an act contrary to nature, one from which generation does not follow in a natural manner, secundum communem speciem actus. It supposes deliberate pollution and semination outside the vagina, both of which actions are intrinsically evil.
In discussing the morality of vasectomy the following points must be considered:
1. In what degree of mutilation is vasectomy?
2. Vasectomy may be done either at the request or by the permission of the vasectomized person; or by order of the State.
(a) If done by the request or permission of the vasectomized person, it may be either (1) as a means to use the debitum without the inconvenience of having children; or (2) as a therapeutic measure to cure some malady.
(b) If done by order of the State, it may be (1) a punishment; or (2) a prophylactic measure to avert physical or moral evil in society.
If vasectomy causes canonical impotence, that fact adds a special moral quality. The weight of authority is on the side that it does cause canonical impotence, as has already been mentioned.
A slight mutilation, in the sense of the term as commonly used, can be any permanent effect of a wound, bruise, or similar cause, from a mere scar to an amputation or other injury whereby any member of the body is rendered unfit for normal action. That the causal wound or injury is trivial in itself, apart from its effect, as in vasectomy, has little or no direct bearing on the morality of the mutilation. It is possible to have a very gross mutilation without extensive wounding. We can blind a man permanently by putting the point of a fine cambric needle one-twentieth of an inch within the pupil.
Vasectomy is a grave mutilation because (1) it removes from the man the power of generation; (2) it inhibits the function of the testicle, which is an important organ of the body. Although they are not the entire organ of generation, the testicles are together a complete organ in themselves, the function of which is to produce the spermatozoa essential to the procreation of the human species. If by a wound one inhibits the function of the testicles, he gravely mutilates the human body, for a grave mutilation is nothing but an inhibition[261] of the function of a distinct organ through a wound.
A mutilation of this kind, since it frustrates the production and action of the human generative semen and prevents generation, is what is technically called a mortal sin against nature, unless there is sufficient cause to necessitate the frustration, such as to save life, to restore as a sole means the health of the whole body, to protect society, or a similar reason. What is said here of vasectomy is true for fallectomy or other methods of sterilizing the woman. Fallectomy, however, is in itself a dangerous operation, and oöphorectomy is never justifiable as a mere method of sterilization because of its very injurious effects on the whole body and mind of the woman.
Among the decretals of Gregory in Corpus Juris (lib. v, tit. xii, c. 5) is the following canon: "If any one, for the sake of indulging lust, or through revenge, does anything to a man or woman, or gives them anything to drink, whereby they cannot generate, or conceive, or bear children, he is to be treated as a homicide." Any one who sterilizes a man by vasectomy or a woman by fallectomy or oöphorectomy, for an improper motive, ipso facto falls under this decree, and is before the canon law classed in the same category as a murderer; that is, the agent is deemed guilty of a grave crime against nature.
If a man has vasectomy done upon himself, his intention may be (1) to use the debitum without the inconvenience of having children; or (2) to avert from a wife with a narrow pelvis the dangers of the cesarean section or other obstetrical operation to herself and the child; or (3) to avoid the transmission to possible offspring of a hereditary disease like Huntington's chorea or one of the others mentioned at the beginning of this chapter; or (4) to cure himself of some malady.
1. If vasectomy is done merely to be able to use the debitum without the inconvenience of having children, it is evidently illicit. It is in that condition the same as onanism; it is contrary to the basic justification of marriage; it is a frustration of nature; and so on.
2. If it is done to safeguard a wife with a narrow pelvis it is a means, evil in itself, used directly to effect a good end; and a good end, or any end or effect, never justifies a direct[262] evil means or cause. There is in reality no such thing as a good effect from an evil means or cause; the evil means or cause essentially and substantially vitiates the effect. There is no question here of a double effect, one good and one evil, wherein the good effect is intended and the evil permitted, both coming with equal directness from the single causal act. On the contrary, from the vasectomy here there is the single direct effect that the man is sterilized, and then directly from this sterility comes the desired effect, the protection of the wife. For exactly the same reason, vasectomy done to prevent the transmission of a hereditary disease is illicit; it is an evil means used directly to effect an end intended. In artificial abortion when the fetus is inviable the act done is to empty the uterus, and this act itself kills the fetus, which is not an unjust aggressor, and is murder. This murder may save the mother's life, but the end does not justify the means. The vasectomy to protect the mother's life or to avert an evil heredity is a parallel case.[245]
The fourth case supposes that the vasectomy was done to cure the man of some malady. If there were a malady that endangered the patient's life, or destroyed the health of the body and it could be cured by vasectomy, the operation would of course be licit for the reasons given in the chapter on General Principles concerning Mutilation. Dr. Carrington tells us[246] that he did vasectomy on an epileptic convict and cured him. Such a cure is doubtful as to permanence. He describes two dangerous insane negro homicides who were rendered harmless by vasectomy. In cases like those of the homicides any one responsible for them would probably be justified in having the operation done, although these two cases are the only direct ones on record. Epileptics sometimes show a homicidal tendency, but it is doubtful that vasectomy would help them. The operation of vasectomy as a cure for bodily ill has a very limited field. There are very many conditions in women where it is necessary to remove the ovaries or the tubes to save life, or to[263] cure chronic invalidism of an unbearable nature. These conditions are discussed in the chapter on Gonorrhea. There is no objection to the removal of a tube or an ovary when such removal is absolutely necessary, but the necessity must be clearly evident. There is a tendency in some surgeons to mutilate women in this manner without sufficient reason or to follow out a therapeutic theory.
Men, like Sharp, who have done hundreds of vasectomies, say the operation commonly removes the inclination to masturbation. Masturbation is, as a rule, a moral condition, but it can, like alcoholism, come to have a large physical element. Idiots almost unexceptionally have this vice, and in them there is no morality possible. If by vasectomy they can be cured of this vice, which injures their health and is a social indecency and a source of sin in observers, the operation would be licit in their case. When the patient is morally responsible vasectomy would not be licit, as there is no adequation between a physical evil like sterilization and a moral vice. There are cases of pathological sexual erethism which are so violent that the patients must be put into strait-jackets to prevent constant masturbation. The semen of such patients is usually devoid of spermatozoa. If the patient is confined in a strait-jacket he will die, and vasectomy, according to Sharp, will quiet such a man. Vasectomy would be permissible in these circumstances.
The question has arisen in the case of a sane masturbator who is neurotic, weak-willed, and a confirmed addict to his vice, whether or not his vasa might be tied off by ligatures, temporarily, with the intention of removing the ligature later and restoring function. I think not. Even temporary sterilization is sterilization, a grave mutilation, while it lasts, and the condition is really moral fundamentally, and therefore not a fitting object for physical remedies.
When vasectomy is done by the State, it is done either as a penal or as a prophylactic measure. As a general statement we can say the State in certain conditions has the right to kill or mutilate a criminal in defence of the social order; but even then any punishment, to be justifiable, must be effective and necessary, and it has to be either reformative, exemplary, or[264] reparative in regard to the crime for which it is inflicted. Capital punishment and mutilation are effective usually, and are necessary for the preservation of society. The natural law permits the State to preserve itself against the unjust encroachments of individuals by curtailing their rights in so far as that curtailment is effective and necessary: since the natural law requires the existence of civil society, it must allow what is necessary for the preservation of that society. There is no question here of a good end justifying evil means; the means which otherwise would be evil in these conditions become good. Homicide and mutilation are not mere killing or mere maiming, but unjust killing or unjust maiming. Killing or maiming is not intrinsically wrong under all circumstances, as lying, blasphemy, and some other crimes are; nevertheless, as a punishment by maiming, vasectomy is ordinarily wrong, and therefore a law making it an ordinary mode of punishment for certain whole classes of criminals, or all criminals, is unjust.
It is wrong because as a punishment it is neither effective nor necessary nor reformatory nor exemplary nor reparative—it lacks every quality of a justifiable punishment. In Dr. Sharp's list of vasectomies done in Indiana prisons, 176 operations were done on men who voluntarily asked for vasectomy. There is no pain, no inconvenience caused by the operation, no sexual change perceptible, but a fitting of the criminal to indulge his lust without the various inconveniences of impregnation. Instead of being reformatory, it is conducive to crime. I find only one man who objected to vasectomy.[247] In this man vasectomy was added to life imprisonment as a punishment for rape.
The legislators in the States which have passed the vasectomy law all seem to have been influenced by the pseudoscientific notion that criminality is a hereditary condition, a physical disease, and not a matter of volition. This Lombrosan absurdity is now held by no physical scientist, and from an ethical point of view it is nonsense. Moreover, if the State vasectomized all the criminals in the jails, this method would not appreciably affect the supply of criminals, nor reach an appreciable[265] minority of the criminal class, as the most dangerous criminals are not in jails.
The operation is not a punishment to the men upon whom it is done, but it is an unnecessary deprivation of an essential right of these men, an excessive, ill-ordered attack on a primary right of man, and an act of violence against human nature and its Author without adequate reason. The law is against the natural order because it directly deprives a man, and that against his will, of functions which are at times a moral necessity to him, and puts him into the occasion of sin. Vasectomy does not remove his venereal desires, but gives opportunity to lust; it turns the conjugal relation into mere onanism and degrades marriage into a crime. Other conditions, like military service, in which necessity obliges the State to place its citizens and thus prevent the conjugal relation, cause an indirect temporary prevention, reluctantly permitted, not directly intended. Vasectomy is an evil directly intended.
It is to the interest of the State to prevent the transmission of hereditary disease, and in doing so it may to a certain degree curtail the natural liberty of its citizens. When the peril is great, as in a plague, the State may isolate infected individuals, and thus indirectly, but temporarily, prevent a natural right—namely, the conjugal relation. It may even perpetually isolate, as in leprosy. Vasectomy, however, is a direct prevention without reason, and it is done as a direct evil means to effect a so-called end which it never attains.
A man with Huntington's chorea, if married and if he has children, will surely transmit the disease to some of these children, and they to their children. Vasectomy on him will prevent a propagation of his kind but will cure no disease. Moreover, he is not a criminal and not amenable to punishment. The bad effect, sterilization, must be perpetual in his case or it is foolish, but the sterilization is not a punishment, nor a means of saving the health of the patient. Whatever good comes of the act comes out of an evil cause. If such a man persists in marrying, his marriage might be prevented, but that is different from mutilating him.
The State has no direct dominion over the lives or members[266] of its citizens, nor are citizens naturally mere instruments for the good of the government; on the contrary, the government exists solely for the good and utility of the citizen. The State may not take the life of an innocent person, nor mutilate him, unless these acts are necessary either (1) to protect the life or rights of individuals; or (2) to preserve the social life of the commonwealth. Now, neither of these two requisites is present when there is question of vasectomizing a man.
The right or life of no individual is at stake. The rights of the possible children, yet unborn, are not injured, because, as these children are not in existence, they have no rights. Should they come into being, it is always better to be, even though diseased, than not to be. The methods of cattle-breeders in dealing with human beings is not a virtue in the State, but an outrage and a degradation of human nature.
The rights of the wife are not injured, because she personally receives no injury; and if her possible children have chorea, for example, she either voluntarily took that risk when she married, or if she did not, through ignorance, there are other means to avoid the trouble than the evil of sterilization, which in itself would render the use of marriage onanistic. If the husband has syphilis, gonorrhea, leprosy, tuberculosis, or any other infectious disease, vasectomy is no protection for the wife.
May a physician employed by the State in a prison, an institution for the feeble-minded, or a like place, do vasectomy at the command of the law? Certainly he may not, except in those rare cases where vasectomy is permissible as described above.
The advocates of freakish legislation harp on the assertion that insanity and imbecility are increasing alarmingly, and as a consequence the entire nation is degenerating. To cure this evil we are to mutilate certain criminals and the mentally defective. It is not true that insanity and mental imbecility are increasing in a very marked degree in the United States. The number of inhabitants in this country is increasing rapidly, and as there are more people here than there were a few years ago, the number of the insane and the mentally defective has[267] increased pari passu, but the percentage does not increase to any degree that calls for immoral and ineffective legislation. Only of late years have the State governments begun to classify, diagnose, and gather up the insane and the imbecile, whom we always have had with us, and these processes have brought the defectives into the light.
Our late immigrants are not equal in race, in mental and moral strength, to the old northern European immigrants. In Philadelphia the foreign-born population is 24.7 per cent. of the whole, but that foreign-born population gives us 44 per cent. of the indigent insane. In New York State 27 per cent. of the registered insane are not American citizens. What we need here is not sterilization, but a better control of the immigrant, a keeping out of the unfit. Again, our insanity percentage is increased avoidably by the undoubted increase of insanity among negroes. We are accountable for this because we do not care for our helpless negroes. These people are prevented by trades-unions from learning and working at elevating trades, and they are thus forced unjustly into a poverty and degradation which lead to vice and mental deterioration. The cure is not a jail surgeon's scalpel, evidently.
A system of education that ignores the will, upon which morality and virtue are based, and substitutes a sham intellectuality as elaborated by ignorant boards of education and administered by emotional, half-educated women, together with a lack of genuine religion, is a prolific source of mental and moral deterioration and consequent degeneracy in the physical and moral orders. Our American public-school system is such, and its deity is the unwashed and crassly depraved god Demos, whose bible is the evening newspaper. If we could civilize our schools, we should have no mention of legislation by vagary.
BIBLIOGRAPHY
Ecclesiastical Review, vols, xlii, xliii, xliv, xlvi, xlvii, xlviii, passim. Philadelphia.
Gemelli. La Scuola Cattolica, November, 1911. Milan.
Stucchi. Ibid.
Eschbach. Ibid., February, 1912; Analecta Ecclesiastica, September and October, 1911.
Capello. La Scuola Cattolica, February, 1912.
Michaud. Nouvelle Revue Théologique. Paris, 1914.
Schmidt. Zeitschrift für katholische Theologie, nn. 1 and 4, 1911.
Ferreres. De Vasectomia Duplici necnon de Matrimonio Mulieris Excisae. Madrid, 1913.
De Smet. Collationes Brugenses, December, 1910.
Wouters. Nederlandische kathol. Stemmen, January 15, 1911.
Waffelaert. De Virtutibus Cardinalibus, vol. ii. Bruges, 1889.
Sharp. Journal of the American Medical Association, December 4, 1909. This is the article which started the entire vasectomy controversy.
Barker. Maryland Medical Journal, April, 1910.
Bell. Hereditary Criminality. Medico-Legal Journal, vol. xvii. New York.
Desfosses. Presse Méd., vol. xviii.
Rentoul. St. Thomas Hospital Gazette, vol. xx. London.
Swift. Maine Medical Association Journal, December, 1914.
Lydston. Medical Record, November 8, 1913. New York.
A corollary of the doctrine which treats of the destruction in medical practice of existent human life, is a consideration of what is called Birth Control, or the criminal prevention of possible human life by onanistic contraceptive methods. There has been an agitation for several years past in western and northwestern Europe and in the United States to bring about the repeal of laws which forbid the spreading of information on the methods of preventing conception. The laws which the agitators wish to have abrogated declare that contraceptive information is indecent and should be classed with the circulation of obscene literature, pornographic pictures, and instruction in abortion. The birth control advocates pay no attention to accusations like those expressed in the laws, or to those made by persons who have accurate notions of morality and common decency, but assert that the spread of contraceptive information tends to benefit the individual and human society.
Birth control as advocated by its perpetrators is intrinsically contrary to the natural law, and therefore immoral; it mentally and physically debases those that are guilty of the practice; it does not benefit the poor as its advocates claim it does; the arguments urged by its supporters are foolish and frequently deliberate untruths; and it is destructive of society and the state. Broadly speaking the natural law rests on the principle that order, reason, justice, what is congruous with the nature of a being or faculty and tends to its perfection in being or action, should prevail, and that disorder, unreason, injustice, the unnatural, must be avoided. The right order of nature as established by the Supreme Creator of nature is the standard of action; what is contrary to that order is evil,[270] wrong, destructive, criminal, injurious, or the like, in different circumstances, but altogether these deordinate conditions must be removed, not accepted. Morality also depends on these facts. Morality is merely the observance of the natural law, and immorality is revolt against that law.
Since the natural law evidently prescribes that man must live in society and that the human race which constitutes this society, is to be preserved by the generation of new human beings who will replace those that die, or are made useless by disease or other accident, whatever tends to this sustention of humanity according to the natural law, and in the proper conditions, is good, and whatever tends to the destruction of humanity is evil and to be avoided.
The generation of new replacing human beings must take place only in the state of marriage, because thus solely the wife and the child are protected, the children are educated physically, mentally and morally, and the degradation and bestiality of promiscuous sexual relationship are averted. The first and principal end of marriage is the procreation of children. That end of marriage must be the end on which is founded primarily the natural necessity for this contract, but the natural necessity for the contract is the propagation of the human kind through lawful generation and education. Marriage, too, in its very nature is fitted for that chief end, and for that end it was instituted by the Author of nature—a stable, perpetual association of the sexes for the attainment of what is requisite for the propagation of mankind. There are secondary ends of marriage, such as a reciprocal love and help of the husband and wife, and also that aspect of marriage which makes it a restraint upon promiscuous lust. These last, however, are not enough to justify marriage in themselves without the first or chief end, which is the procreation of children.
Whatever is subversive of the end of marriage, and that is the propagation of mankind, is subversive of the very foundation of human society, is contrary to the nature of man, frustrates the primal function of nature, and is therefore essentially and always evil, as bestiality, sodomy, or incest are evil. Such is birth control as ordinarily practised. Birth control if it is[271] effective through a reciprocal consent of a wedded couple, for grave reason, and solely by mutual abstention from the debitum may be in certain conditions an indifferent act morally. If, however, birth control is effected by contraceptive drugs, or like methods, it is a crime against nature, and always a crime which no circumstance can excuse, no more than no circumstance can excuse bestiality, sodomy, or incest. Secondly, marriage, which was instituted primarily to perpetuate the creative act of God, when such practices prevail degenerates to mere concubinage, a gratification of lust protected from the police. Such practices, moreover, lower man and woman below the brutes, because brutes do not frustrate the natural law except in the case of the male rat and a few other low grade rodents and boar pigs. Onan is the patron of Birth Control advocates. The Book of Genesis said Onan, the son of Judah, "did a detestable thing, therefore the Lord slew him."
These are the fundamental reasons those of us recognize who do not wish that the ignorant and vicious should be taught to act contrary to the natural law. Furthermore, there is always another way out of the difficulties, mostly imaginary, the birth control advocates conjure up. Granting that all the difficulties from multiple births are real, no end justifies essentially evil means, and a subversion of the natural law is always essentially evil. War, homicide, and like acts are not always evil; under certain circumstances both war and homicide may be holy deeds; but to act contrary to nature is never justifiable in any condition. If I owe a man a large sum of money it may be to the advantage of myself or my children that this man be removed, but that good end does not justify murder; no more does any condition of poverty justify a contraceptive act against nature, especially when such an act is never the sole means of evasion. We must protect the married state, but in America we are destroying it. Human society had its origin in marriage, and it depends on marriage for its preservation, but our American divorce laws have made marriage a travesty. In New York alone in 1916 there were 74,893 women divorced, nearly twenty-eight times as many as were[272] divorced in England and Wales in that year, and over forty-nine per cent. of these women were childless, very significantly. Probably ninety-five per cent. of the childless women had used contraceptive methods, yet there are few forces better able to hold the marriage knot tied as it should be tied than a child's fingers. In England and Wales, too, in 1916, forty per cent. of the divorced couples were also birth controllers, at least they had no children. Pennsylvania is much more shameless than New York in granting divorces for no reason at all.
Among the arguments used by those in favor of spreading contraceptive information is that large families keep the laboring classes down to low living standards, and it would be better for those families and the state that these children were not born. Large families as such do not keep the laboring classes down to low standards of living; bad legislation which allows profiteering, which criminally permits extortion in the prices of food, clothing, in taxes, rents, the cost of coal, and the like, which does not force employers to give laborers an honest price for labor, or check the extortions of monopolists, and a hundred similar economic deeds of injustice, together with a parental shiftlessness, unthrift, alcoholism, lack of education through neglect, and so on indefinitely, are the causes. Big families have more wages than small families, and as a rule they do better than the small families when the children are old enough to work. Society is at fault, not the size of the family; the active and the passive selfish are at fault, not the babies; the liars, hypocrites, and the buttoned pockets are at fault, not the holy innocents; the professional meddlers in the business of better folk are the nuisance, not the blessed children, who are the brightest things in this darkened world until we spoil them, and make them like ourselves instead of better. One decent mother is worth a hundred shirkers who raise nothing but lap dogs.
The children of large families, the birth controllers say, are more afflicted by infectious diseases than those of small families. I was for years in charge of the infectious diseases Bureau of the Washington Health Department, and I have had ample opportunity here and in Europe to study this matter.[273] Large families in proper economic positions are not different from small families as regards the infectious diseases. These diseases spread among the poor because the houses of the poor are commonly owned by land sharks and politicians who laugh at health regulations; our health departments can not get enough money away from the political ringleaders in power to employ capable sanitary experts; our laws for the regulation of medical practice and education are a disgrace to our civilization, and every town is swarming with quacks who can not recognize even smallpox when they see it. The fault here is in ourselves not in the large families. Control the professional politicians and quacks and there will be no occasion for foolish talk about birth control.
Again, the children of poor but large families, we are told, have slight or no chance to rise in the social order. Benjamin Franklin, however, one of the greatest men America has produced, was the youngest of seventeen children in a poor family; Lyman Beecher, a poor man, had eleven children, and every man and woman among them became famous; Theodore Schwann, the father of the cell doctrine and of all modern biology, was one of thirteen poor children; John Mueller, one of the greatest of modern scientists, and the Father of German medicine, was one of five children of a very poor family; Emerson was one of five sons, so was Farragut; John Wesley the founder of Methodism, was the eighteenth child of his parents; Ignatius Loyola was the eighth; Saint Catherine of Sienna, among the greatest women intellectually and morally that Europe ever produced, was the twenty-fourth child of her parents. This list can be extended indefinitely from the biographical dictionaries. Every enormous fortune made in America was built up originally by a man who arose from the depths—Rockefeller, Carnegie, Vanderbilt, Astor, Ryan, Havemeyer, Schwab, Ford, Gould, and so on. Poverty is a necessary foundation for a great fortune. The great soldiers of the world almost without exception rose from the ranks of poverty—Napoleon, Washington, Sheridan, Grant, Sherman, Pershing, De Lacy in Russia, Prim in Spain, O'Higgins in Chili, Stonewall Jackson, and others. The powerful Dukes of Tetuan in[274] Spain came from an Irish adventurer, the fifth of eight sons of a poor man. Big families make for strength of character in the struggle for existence; the solitary child in a family is pampered, spoiled.
Advocates of birth control say that Holland has had a Neomalthusian League openly operative since 1881, with fifty-two clinics where contraceptive information is publicly given. As a direct consequence, and solely from the work of this League, Holland has a dropping death rate and an increase in population, and even the stature of the Dutch has increased four inches since 1881. The main objection to these statements about Holland is that they are absolutely false in every particular except that the population of Holland has increased—from other causes. Before the great war every civilized nation had a dropping death rate and an increase in population except France where birth control worked against the increase made by the progress of preventive medicine and a diffusion of sanitary methods. The assertion about the fifty-two clinics in Holland was investigated. An army officer sent out by the committee searched fourteen days before he could find even one secret birth control propaganda station. The present prime minister of Holland, de Beerenbrouk, is an earnest Catholic man, and if anyone talks birth control in Holland during his administration he guarantees them a long term in jail. There was really a Neomalthusian League with 6,704 members, now greatly decreased in number, in the northern Protestant provinces of Holland. As a matter of fact just where this league exists the birth rate decreased and the death rate increased and where it did not exist the direct opposite is true. As to the increase of four inches in stature—since this is a physical impossibility the spinner of the original yarn was an ignorant romancer, lacking plausibility in his untruth. Where there is birth control there are no children to increase or maintain the population, but the New York birth controller who invented the Dutch story says that in Holland where there are no children born through birth control the population increases through birth control.
The birth control movement assumes that the world suffers[275] from overpopulation. It does not; it suffers from incorrect distribution of populations, and no doctrine of birth control will ever affect this fact. All the authorities on the statistics of population tell us it requires an average of four children to each family to keep the population even stationary, not to talk of overcrowding. Two children reaching maturity replace their parents, and because of the high mortality in infancy, and the large number of the unmarried and the birth controllers and abortionists, four children are needed to a family to make a new generation as large as the old. An average of one, two, or even three children to a family means a loss in population, unless the loss is supplied, as in the United States, by immigration. An average of five or six children means an increase in the population. Having none or two children to a family and relying on immigration to preserve the nations means political annihilation, as can be readily shown. In New York State in 1919 instead of the required four children to keep the population stationary, as far as the native Americans are concerned, there was one child to every ten families.
The American nation was founded and built up wholly by Nordic races, immigrants from Great Britain and Ireland, Germany, and a few from France, Holland and Sweden. All our national traditions are from these Nordic immigrants, our notions of self government, our peculiar democracy, our constitution, our language and literature. These Nordic peoples are dying out here in appalling numbers for two chief reasons, one of which is birth control and the other is the American climate. The civilization which affects us has always existed along a geographical belt reaching from the British Isles to above Rome, and covering Great Britain, Ireland, France, Spain, middle and western Germany, and Italy to below Florence. The Grecian civilization was not indigenous, but the result of a Nordic occupation, and it ceased centuries before Christ. Huntington of Yale and several others have shown, by studying the production of thousands of piece workers and students over a long time, that man does his best work physically and mentally under four climatic conditions: a mean temperature[276] of about sixty-two degrees Fahrenheit for physical work and about forty degrees for mental work; secondly, there must be a humidity of about seventy-five per cent.; thirdly, the climate must be variable, be that of the belt of cyclonic storms; fourthly, there must be a quantity of sunlight such as that found in the European racial habitat of the person considered. These conditions are found curiously in exactly these degrees in the civilized parts of Europe and not elsewhere. Above and below that area they are lacking and there has never been any civilization where they are wanting. The reason physical and mental productivity lessen annually with us in December, January, and February is because these climatic conditions are absent during these three months.
Again, men are differentiated into races, thrive, develop, and reach and maintain mental and physical perfection within well defined climatic areas. Nature preserves the race that has acquired through countless ages acclimatization in a given environment, and kills off very quickly immigrants coming from far north or south of the given latitudes. The natural geographical position for the black man is from the equator to the thirtieth parallel of north or south latitude. The thirtieth parallel in America runs through upper Florida, southern Louisiana, and the lowest third of Texas. From the thirtieth to the thirty-fifth parallel is the zone of the brown man, like the Malay. The thirty-fifth parallel runs along the southern border of North Carolina and Tennessee, through the middle of Arkansas, New Mexico, Arizona, and the lowest third of California. From the thirty-fifth to the forty-fifth parallel is the zone of the brune Mediterranean races. The forty-fifth parallel passes near Halifax, Bangor in Maine, Ogdensburg, Ottawa, and St. Paul. In Europe it runs near Bordeaux, Turin, Bosnia, and the Crimea. New York is as far south as Naples, Philadelphia is sixty miles south of Naples, and has the sun of southern Italy. The Nordic races that we are interested in as our origins all live above the United States, and the summer temperatures they have been accustomed to are above the United States. An immigrant coming from northern Ireland to Philadelphia moves southward a thousand miles; a Norwegian[277] going to Texas moves southward two thousand miles, and his family disappears as a rule in two generations.
In historic times there have been sudden movements southward of European races for about seven hundred miles and all ended disastrously. The Lombards went south from upper Prussia to middle Italy at the level of Boston and disappeared in two hundred years. The Teutonic Goths went from the Baltic to Italy and Spain. They lasted sixty-two years in Italy. Eighty thousand Vandals with their families went down from Brandenburg to North Africa at the level of Virginia. They were annihilated by the climate in one hundred and eight years. The Burgundians disappeared in sixty years from Greece, as the Celts who had carried the Homeric sagas to Greece also disappeared. Rome was great while the Nordic Cisalpine Celt ruled it, and died forever with the Celt. Italian art ended at Florence, the southern boundary of Cisalpine Gaul. The Slav disappeared the same way from southeastern Europe and left only language traces to the Turanian and Semite there. No European race of pure blood has ever had grandchildren in the tropics.
The northern races of Europe die out with amazing rapidity in the northern United States. The Irish death rate at the level of New York is double the death rate in Ireland under much worse economic conditions; the death rate of the southern Italian and the southern Russian is much better in New York than it is in their European racial habitats.
In 1910 our English immigration was only six per cent. of the whole, and the Irish immigration is now negligible because there are no more people in Ireland to leave it, but we have seven million Slavs who came in during the ten years before the war. We have three million southern Italians, three million Poles, and hundreds of thousands of nondescript folk from all the back alleys of the old world. At an army camp in Massachusetts during the late war there were thirty languages other than English spoken, and seven thousand men there never had heard the term Anglo-Saxon. The extreme southern, eastern, and southeastern European hordes are overwhelming us, and these hordes never knew a single political principle that[278] even remotely resembles what we understand as American principles. They come of races who were ruled, if they had any rule at all, by despots, but we shall make "Anglo-Saxons," Americans, or whatever you like to call the final metamorphosis we effect, out of these barbarians. Never! Even in a millenium. Centuries from today the Slav here will be a Slav, the Sicilian a Sicilian, the Russian a Russian, all with a veneer of American slang on the tongue of an eternal racial character. Whole counties of Pennsylvania are filled with Germans who have been here since before the Revolution and they have not so much as learned English yet. The Nordic peoples die out here. Only the dark-skinned southern Germans last with us; the sun kills out the red and blond in two or three generations. I recently went over fifty Irish families which I knew perfectly, and they have degenerated eighty-six per cent. numerically and otherwise in my own lifetime: killed off by the climate which keeps our southern states empty of white men. By two American censuses and one English we know that fifty per cent. of Washington's army was born in Ireland, but there are no Irish in the revolutionary societies because the Revolutionary Irish have disappeared.
If there is any chance at all for our civilization, flimsy as it is, this world must be ruled by the Nordic European races, not by the southern, eastern and southeastern European barbarian Semite. We must rule for our own sake and for their sake; they can not rule anything. If we do not rule them, then welcome the final curtain as soon as possible. How can we rule America, not to think of the rest of the world, unless we have Nordic children to take our place, and how can we have such children if we let sex-brained misfits run about spreading contraceptive drivel? The rascal that preaches such doctrine is a traitor to America, the worst enemy our country ever has had, more treacherous than any spy that sneaked in among us during the war just past. The French have had their lesson in birth control, and we should learn from their misfortune. In the first six months of 1914 when Europe was still at peace the total number of births in France was 381,398; a decrease of 4,000 on the year 1913. At the same time[279] the deaths increased 20,845. Thus the population of France during the first six months of 1914 decreased 24,816. For the past thirty years the birth rate of that country has steadily decreased by contraceptive methods, while the death rate has increased proportionately to the number of inhabitants. January, 1916, found France with about seven hundred thousand less people than she had in January, 1914, and then came the horrible carnage of the great war. No matter what change of heart war may bring to France no increase in her population can be expected for many years yet to come. She is daily crying out to the world for treaties to protect her from Germany, despite the prostration of Germany, because she knows Germany had a birth rate of two males for her one, and for twenty years to come Germany probably can put twice as many men into the field as France can. If France will give over her unclean birth control she will not need to whine for protection.
The advocates of birth control assert that it lessens venereal diseases. It does not; it increases the spread of venereal disease. The more reasonable among the birth control propagandists are anxious lest their public talks suggest temptation to the young. There is at present for youth the deterrent of the natural consequences of lust; with birth control knowledge spread broadcast that check is removed and promiscuity will become more general, because safer socially. Venereal diseases will spread also as incontinence spreads. Nowhere in the world has the crime of birth control been practised as in France nor for a longer time, and in that country together with the lowest birth rate in the world there is the highest death rate from venereal diseases according to Dr. Dublin the statistician of the New York Metropolitan Life Insurance Company. Not long ago one of the leading medical writers of France, Doyen, said in the Academy of Medicine in Paris that syphilis is the chief cause of death in France. France now asserts she has given over birth control, but that is a hard disease to cure after it has been established. Unchastity is its own punishment, and if France goes the way of those nations that have died along the pathway of civilization, and great[280] would be the pity, she has nothing to blame for it but this abominable moral leprosy, birth control. She is as striking an example of the insanity of birth control as Russia is of the insanity of communism.
One of the most successful of teachers is a Montreal Principal—successful because she insistently teaches undergraduates to THINK. Force of thought is better than force of will. A triphammer is all force, but unless guided by a THINKER strikes a pile or a cream-puff with equal power. Then there is the nagger with a tongue-will of poiseless perpetual power but—thought-proof.
Do you as host, hostess or guest want a spur to cleverness of thought, wit and repartee?
Do you fail in clearness of thought and expression—especially in conversation?
Do you teach, preach—or lecture?
Do you dictate at home(?) at office—or both?
Do you want to give straight-to-the-point advice to your children, your friends, your employees and YOURSELF?
If an employer you will commend KEYSTONES OF THOUGHT to your employees—surely to the stenographers.
If easily discouraged, a victim of worry, fear, the blues, "Keystones" is your prescription.
Is Christianity a Failure? Have you an active or passive grouch against the clergy (a now fashionable disease usually confined to the middle aisle) because of "what they say and do and because of the way they live"?
Do you want something to "crib" for public dinners and other occasions? The "greatest after-dinner speaker in the world" is a New Yorker. Never lengthy, always aphoristic, he says more in five minutes than all the "wax-works" on the dais drone or spout in hours.
THEN READ
KEYSTONES of THOUGHT
By AUSTIN O'MALLEY, M.D., Ph.D., LL.D.
The only book of original and genuine aphorisms in English.
Written by "the World's master of aphoristic thought
and expression."
"The successful aphorist is about ten thousand times scarcer than the successful essayist, or story teller, or Assyriologist. Humor without effort, wit without bitterness, philosophy without pretension! Dr. O'Malley has written a book that is worth possessing."—From a review of the book written by the editor of the N. Y. Sun himself.
Special gift book edition, suède, gold edges, in box—a very useful
ornament for Den, Desk, or Drawing Room, $4.00 net, Postpaid.
Cloth, gold letters and design, $2.00 net, Postpaid.
NOTE: Whether young or old, Sage or Seer, Poet, Philosopher, or what-not, if you think YOU can match KEYSTONES OF THOUGHT in aphoristic originality, in depth, deftness, wit, wisdom and humor—in tonic-cheer for all of life's worries, troubles and adversities, you are welcome to try. If successful The Devin-Adair Company will send you a check for an acceptable but well-earned sum, and your work will be promptly published.
THE DEVIN-ADAIR COMPANY, Publishers
437 FIFTH AVENUE, NEW YORK
[1] Ethics, v, c. 2.
[2] Summa Theologica, 1, 2, q. 64, a. 5.
[3] De Justitia et Jure, lib. 2, cap. 9.
[4] Ibid.
[5] Commentary, bk. iv, p. 205.
[6] De Justitia et Jure, disp. 19, tr. 3.
[7] Ibid., disp. 68, tr. 3.
[8] Ibid., n. 69.
[9] Theol. Moral. vol. vii.
[10] De Censuris, etc., disp. 44, sec. 2, 2.
[11] Theol. Moral., lib. 7, cap. 5, disp. 4, n. 365.
[12] Ibid., n. 378.
[13] Ibid., n. 382.
[14] 2, 2, q. lxv, a. 1, ad 3.
[15] IX, De Animalibus.
[16] De Anima, cap. 27.
[17] From tradux, a planted vine-shoot made to take root.
[18] Migne, vol. xxxiii, col. 720.
[19] De Anima et ejus Origine, i, xv.
[20] I, cap. i, n. 3.
[21] Migne, Patrologia Graeca, vols. xliv and xlvi.
[22] Migne, Ibid., vol. xci, col. 1335.
[23] De Conceptione Virginis, cap. xii.
[24] Summa, De Homine, q. xvi, art. 3.
[25] De Vi Formatrice Foetus Liber.
[26] Tom. ii, lib. ix, tr. 1.
[27] Theologia Moralis, lib. iv, tr. 4, n. 594.
[28] If men quarrel, and one strike a woman with child, and she miscarry indeed, but live herself, he shall be answerable for so much damage as the woman's husband shall require and as arbiters shall award. But if her death ensue thereupon, he shall render life for life, eye for eye, tooth for tooth, hand for hand, foot for foot, burning for burning, wound for wound, stripe for stripe.
[29] καὶ ἐξέλθη παιδίον αὐτῆσ μὴ ἐξεικονισμένον—not moulded out into form; ἐξεικονίζειν, to mould out into form: εἰκων, an icon, image, likeness.
[30] The Cell in Development and Inheritance, p. 207.
[31] Jenaische Zeitschrift, 1891, p. 410.
[32] See Wilson, op. cit., p. 299.
[33] Journal of the Linnean Society, vol. xx, p. 133.
[34] American Journal of Physiology, 1899, iii, 3.
[35] Contributions to the Study of the Early Development and Embedding of the Human Embryo. Glasgow, 1911.
[36] Berliner klinische Wochenschrift, June 14, 1915.
[37] Id is a word derived from Nägeli's term idioplasm, which means the chromosome granule.
[38] Thoughts of a Catholic Anatomist, p. 48.
[39] Contemporary Review, September, 1893.
[40] I, q. 118, a. 2, ad 2.
[41] ἡ ψυχή ἐστιν ἐντελέχεια ἡ πρώτη σώματος ψυσικοῦ ὀργανικοῦ δυνάμει ζωὴν ἔχοντοσ (De Anima, ii, 1).
[42] Virchow's Archiv (1888), 114.
[43] Phil. Trans., 1854.
[44] Heredity and Environment, p. 123, Oxford Press.
[45] Intracelluläre Pangenesis. Jena, 1889.
[46] Jenaische Zeitschrift, 1892, 1.
[47] Journal of Morphology, 1893, 1894.
[48] Studien, iv, p. 25.
[49] Ibid., p. 39.
[50] The Cell in Development and Inheritance, pp. 413 et seq. New York, 1906.
[51] The Duration of Life.
[52] Zeitschrift f. Biologie, 1893, bd. 30, p. 73.
[53] Heredity and Environment.
[54] Journal of the American Medical Association, vol. lix, n. 7, p. 523.
[55] I, q. 76, corp.
[56] Ia, q. 118, a. 2, ad 2.
[57] U. d. Entstchungsweise der vordern Verdoppelung. Deutsch. Archiv. f. klin. Med., 1887.
[58a] U. d. Furchung des Eies bei Doppelbildungen. Breslauer Aertzliche Zeitschrift, 1887.
[58b] Chap. vi, p. 69. New York, 1906.
[58c] See Wilson, op cit., p. 421.
[59] Tit. ii, cap. 1, nn. 18, 19, 20, 21.
[60] A Study with the Electrocardiograph of the Mode of Death of the Human Heart. Journal of Experimental Medicine, 1912, xvi, 291.
[61] New York, 1906, p. 164.
[62] Proceedings of the American Therapeutic Society, 1912.
[63] La Muerte Real y Apparente, 4th ed., p. 21. Madrid, 1911.
[64] Quaestiones Physiologicae-Theologicae, disp. 3, p. 2, c. 3, a. 3.
[65] P. 30 in the English translation.
[66] P. 35; p. 39, English translation.
[67] Opera Medica Omnia. Geneva, 1762.
[68] Epistolae, 1692.
[69] Observationum Medicarum, etc. Frankfort, 1600.
[70] New Orleans Medical and Surgical Journal, xvi.
[71] Treatise on Human Hibernation, 1850.
[72] Medical Times and Gazette, vol. i. London, 1870.
[73] Quaestiones Medico-Legales, 1701.
[74] A Textbook of Obstetrics, 7th ed., p. 643. Philadelphia, 1912.
[75] Journal of the American Medical Association, August 28, 1915.
[76] Journal of Pharmacology and Experimental Therapeutics. Baltimore, July, 1915.
[77] Münchener medizinische Wochenschrift, January 18, 1916.
[78] Presse Médicale, Paris, xxiv, 66.
[79] Cronk, Oklahoma State Med. Assoc. Jour., July, 1816.
[80] Amer. Jour. Obstet., August, 1915.
[81] Upsala Läkareforenings Förhandlingar, xxi, 8.
[82] Journal Amer. Med. Assoc., October 28, 1916.
[83] In. 4, dist. 81.
[84] Theologia Moralis, n. 943.
[85] Theologia Moralis, n. 936.
[86] Theologiae Moralis Institutiones, vol. ii, n. 544.
[87] Compendium Theologiae Moralis, n. 1114.
[88] Pathology of Intrauterine Death. London, 1887.
[89] Münchener medizinische Wochenschrift, lxii, 39.
[90] Berliner klinische Wochenschrift, June 14, 1915.
[91] Cap. 35.
[92] Lib. v, tit. xii, c. 5.
[93] Session xiv, De Reformatione, cap. 7.
[94] Sect, iii, cap. ii.
[95] Compendium Theologiae Moralis, 1915, n. 1009.
[96] "Dummodo et foetus et matris vitae serio et opportune provideatur."
[97] Statutes 24 and 25, Victoria, cap. 100, sec. 59.
[98] Principles and Practice of Medical Jurisprudence. London, 1905.
[99] Laws of Pennsylvania, Act of March 31, 1860, sec. 88. p. 404.
[100] Laws of 1897, Iowa Code, 4759.
[101] Legal Medicine, 1905.
[102] Medical Jurisprudence, vol. iii, sec. 526.
[103] Kelly's Operative Gynaecology. New York, 1898.
[104] "In a case of necessity, it is licit to do a laparotomy for the removal of an ectopic gestation sac from the maternal pelvis, provided the life of both fetus and mother be carefully safeguarded."
[105] "Negative, juxta decretum 4 Maii, 1898, vi cujus, foetus et matris vitae, quantum fieri potest serio et opportune providendum est: quod vero tempus, juxta idem decretum, orator meminerit, nullam partus accelerationem licitam esse, nisi perficiatur tempore et modis, quibus ex ordinarie contingentibus, matris ac foetus vitae consulatur."
[106] Jour. Amer. Med. Assoc., February 24, 1917.
[107] Zentralblatt f. Gynäkologie. Leipsic, October 30, 1915.
[108] Münchener medizinische Wochenschrift, January 4, 1916.
[109] Jour. Amer. Med. Assoc., September 30, 1916.
[110] Jour. Amer. Med. Assoc., December 1, 1917.
[111] Corpus Juris, lib. v, tit. xii, c. 5.
[112] Is any active or passive procedure licit which is undertaken with the express end of sterilizing a woman?
[113] Jour. Amer. Med. Assoc., March 24, 1917.
[114] Ibid.
[115] Cf. Ferreres, Nouvelle Revue Théologique, September and October, 1912, and the appendix of his book De Vasectomia Duplici, Madrid, 1913.
[116] Jour. Amer. Med. Assoc., December 8, 1917.
[117] Jour. Amer. Med. Assoc., December 24, 1912.
[118] Obstetrics, p. 456.
[119] Praeger medizinische Wochenschrift, 1892 n. 17.
[120] Zeitschrift für Geburtshülfe, bd. 16, n. 2.
[121] Münchener medizinische Wochenschrift, July 30, 1907.
[122] Nouvelle Archives d'Obstétrique et de Gynécologie, 1893.
[123] Archiv für Gynäkologie, 1911, xcv, 1.
[124] Monatsschrift für Geburtshülfe und Gynäkologie, xxxviii, 2. Berlin.
[125] Münchener medizinische Wochenschrift, November 23, 1915.
[126] Centralbl. f. Gynäk. xxxi, 11.
[127] New York State Journal of Medicine, xiii, 8.
[128] Amer. Jour. Obstetrics and Diseases of Women and Children, lxix, 6.
[129] Obstetrics, 4th ed. New York, 1917.
[130] Jour. Amer. Med. Assoc., June 2, 1917.
[131] Jour. Amer. Med. Assoc., April 10, 1915.
[132] Diseases of the Heart. New York, 1905.
[133] Medizin. Klinik, February 25, 1912.
[134] Jour. Amer. Med. Assoc., lxix, 24.
[135] Loc. cit.
[136] Philadelphia, 1913.
[137] Zeitschr. f. Geburtshülfe u. Gynäk., lxxvi, 3, p. 677. Stuttgart.
[138] Münchener medizinische Wochenschrift, August, 1915.
[139] Arbeiten d. pathologisch. Instit. zu Leipsig. Jena, 1891.
[140] Münchener medizinische Wochenschrift, 1904, vol. li, p. 1676.
[141] L'Obstétrique, vol. i, p. 69.
[142] Thèse. Nancy, 1885.
[143] Annales de Gynécologie. June, 1889
[144] Jour. de Méd. de Bruxelles, 1872, p. 412.
[145] Ibid., 1870, vol. l, pp. 430, 516, and vol. li, p. 11.
[146] Deutsch. med. Wochensch., 1900, No. 28.
[147] Archiv. f. Gyn., vol. xxix, p. 448.
[148] Pulmonary Tuberculosis, p. 550. Philadelphia, 1908.
[149] A Text-book of Obstetrics, p. 427. Philadelphia, 1912.
[150] The Principles and Practice of Obstetrics, p. 480. Philadelphia, 1913.
[151] Pennsylvania Medical Journal, February, 1916.
[152] From Abraham Colles, Dublin, 1837.
[153] Wolff, 1879.
[154] Nederlandisch Tijdschrift voor Geneeskunde, i, 9.
[155] Zeitschr. f. klinisch. Med., vol. lxxvi. Berlin.
[156] Boston Med. and Surg. Jour., vol. clvii, n. 4.
[157] Jour. Amer. Med. Assoc., October 31, 1914.
[158] Forchheimer's Therapeusis of Internal Diseases, vol. ii, p. 421. New York, 1913.
[159] Syphilis and the Nervous System, 1892.
[160] Lyon Med., November 7, 1907.
[161] Theologia Moralis, iv, n. 970 et seq.
[162] Cf. De Lugo, De Justitia et Jure, disp. 14, n. 141.
[163] Sabetti-Barrett, Compend. Theol. Moral., n. 565. New York, 1915.
[164] Die latente Gonorrhoea in weib. Geschlect. Bonn.
[165] Gonorrhea in Women, p. 123. Philadelphia, 1913.
[166] Trans. Amer. Urological Assoc., vol. iii.
[167] Lancet, November 24, 1906.
[168] Expansion of Races. New York, 1909.
[169] Medical News, December 21, 1909.
[170] New York Med. Jour., November 12, 1910.
[171] Jour. Amer. Med. Assoc., January 8, 1916.
[172] Jour. Amer. Med. Assoc., January 8, 1916.
[173] Jour. Amer. Med. Assoc., September 30, 1916.
[174] Jour. Amer. Med. Assoc., October 6, 1912.
[175] Social Diseases and Marriage, 1904.
[176] Monatschrift f. Geburt. u. Gynä., 1909, n. 20.
[177] Zeitschr. f. Geb. u. Gyn., 1907, vol. lix, n. 1.
[178] Archiv. f. Gyn., vol. xcii, n. 2.
[179] Gonorrhea in Women, p. 285. Philadelphia, 1913.
[180] Policlinico, 1907, p. 16.
[181] Münchener medizinische Wochenschrift, April 8, 1913.
[182] Soc. Med.-Chir. de Bologne, 1904.
[183] Jour. Amer. Med. Assoc., October 17, 1914.
[184] Surgery, Gynecology, and Obstetrics, November, 1915. Chicago.
[185] Correspondenz-Blatt f. Schweizer Aerzte, February 12, 1916.
[186] Jour. Obstet. and Gynecol. of Brit. Empire, March and April, 1910.
[187] Trans. Amer. Gyn. Soc., vol. xxxvi, p. 324.
[188] Norris, Gonorrhea in Women, p. 289.
[189] Jour. Amer. Med. Assoc., January, 1913.
[190] Il Policlinico, January 3, 1919.
[191] Trans. Amer. Gynecol. Soc., vol. xxxiv, p. 327. Philadelphia, 1909.
[192] Jour. Amer. Med. Assoc., December 8, 1917.
[193] Jour. Amer. Med. Assoc., vol. xli, n. 24.
[194] Montreal Med. Jour., vol. xxxvii.
[195] New York Medical Journal, February 22, 1908.
[196] Canadian Presse Médic., July, 1908.
[197] New York Medical Journal, May 30, 1908.
[198] Ophthalmia Neonatorum. London. 1907.
[199] Münchener medizinische Wochenschrift, November 2, 1915.
[200] Archiv. f. Gyn., bd. 86, n. 1.
[201] Deutsche medizinische Wochenschrift, xlii, 9.
[202] Boston Medical and Surgical Journal, November 25, 1915.
[203] June, 1911.
[204] Long Island Medical Journal, December, 1914, and American Journal of Obstetrics, May, 1915.
[205] Jour. Amer. Med. Assoc., November 21, 1914.
[206] Zentralblatt f. Gynäkologie, September 19, 1914. Leipsic.
[207] Therapeutic Gazette, vol. ii.
[208] The Postgraduate, May, 1915.
[209] Ladies' Home Journal.
[210] Ibid.
[211] Proceedings printed in American Journal of Obstetrics, May, 1915.
[212] Ladies' Home Journal.
[213] Jour. Amer. Med. Assoc., May 22, 1915, lxiv, 21, p. 1723.
[214] Gynäkol. Rundschau, 1909, iii.
[215] American Journal of Obstetrics, May, 1915.
[216] Smith vs. Board of Examiners of the Feeble-minded, 88 alt. R. 963.
[217] State vs. Feilen, 126 Pac. R. 75.
[218] Virginia Medical Semi-monthly, vols. xiv, xv.
[219] Jour. Amer. Med. Assoc., December 4, 1909.
[220] Jour. Amer. Med. Assoc., October 19, 1912.
[221] Belfield, loc. cit.
[222] Jour. Amer. Med. Assoc., December 13, 1913.
[223] La Scuola Cattolica, November, 1911.
[224] University of Pennsylvania Medical Bulletin, 1902, p. 388; 1903, xv, 2; Therapeutic Gazette, December 15, 1909.
[225] Revue de Thérapeutique Médico-chirurgicale, January 15, 1912.
[226] Journal Amer. Med. Assoc., January 26, 1915.
[227] Deutsche med. Wochenschrift, xxxix, 29.
[228] Jour. Amer. Med. Assoc., April 19, 1913.
[229] See the chapter on Gonorrhea.
[230] Ecclesiastical Review, September, 1912.
[231] Synopsis Rerum Moralium et Juris Pontificii, 31st ed., n. 2425.
[232] Nouvelle Revue Théologique.
[233] Nederlandische Katholische Stemmen, January 15, 1911.
[234] Analecta Ecclesiastica, September, 1911, and La Scuola Cattolica, February, 1912.
[235] La Scuola Cattolica, February, 1912.
[236] Ibid., November, 1911.
[237] Ibid., November, 1911.
[238] Medicina Pastoralis, vol. ii, n. 43.
[239] Theologia Moralis, 8th ed., ii, n. 744.
[240] De Matrimonio.
[241] Theologia Pastoralis, p. iv, n. 88.
[242] Theologia Moralis, ii, n. 994.
[243] See Ferreres, De Vasectomia Duplici necnon de Matrimonio Mulieris Excisae, p. 110. Madrid, 1913.
[244] Theologia Moralis, 5th ed., vol. ii, p. 391, n. 994.
[245] See the chapter on General Principles concerning Mutilation for an explanation of the act with a double effect.
[246] Virginia Medical Semi-monthly, vols, xiv, xv.
[247] State of Washington vs. Feilen, 126 Pac. R. 75.
Variations in spelling, punctuation and hyphenation have been retained except in obvious cases of typographical error.
The cover for the eBook version of this book was created by the transcriber and is placed in the public domain.
Page 151: "3. The case may be inoperable and the child inviable." The word "be" was added by the transcriber.
Page 194: Footnote 145 "Ibid., 1970, vol. l, pp. 430, 516, and vol. li, p. 11." The transcriber has changed 1970 changed to 1870.
Page 215: A missing anchor was added by the transcriber for Footnote 170 "New York Med. Jour., November 12, 1910."
Page 222 Footnote 185 "Correspondenz-Blatt f. Schweizer Aertze" The transcriber has changed "Aertze" to "Aerzte".