Title: Social Work; Essays on the Meeting Ground of Doctor and Social Worker
Author: Richard C. Cabot
Release date: July 29, 2015 [eBook #49545]
Most recently updated: October 24, 2024
Language: English
Other information and formats: www.gutenberg.org/ebooks/49545
Credits: Produced by Bryan Ness, Martin Pettit and the Online
Distributed Proofreading Team at http://www.pgdp.net (This
file was produced from images generously made available
by The Internet Archive/Canadian Libraries)
Published by
HOUGHTON MIFFLIN COMPANY
A LAYMAN'S HANDBOOK OF MEDICINE. With Special Reference to Social Workers.
WHAT MEN LIVE BY.
SOCIAL WORK. Essays on the Meeting-Ground of Doctor and Social Worker.
SOCIAL WORK
ESSAYS ON THE MEETING-GROUND
OF DOCTOR AND SOCIAL WORKER
BY
RICHARD C. CABOT, M.D.
BOSTON AND NEW YORK
HOUGHTON MIFFLIN COMPANY
The Riverside Press Cambridge
1919
COPYRIGHT, 1919, BY RICHARD C. CABOT
All Rights Reserved
TO
MARY E. RICHMOND
WHOSE ILLUMINATING BOOK ON "SOCIAL DIAGNOSIS"
MARKS AN EPOCH IN THE DEVELOPMENT
OF SOCIAL WORK
Most writers who disclaim thoroughness are prone to describe their work as an outline, a sketch, or an introduction. But the chapters of this book are more like spot-lights intended to make a few points clear and leaving many associated topics wholly in the dark. Possibly such isolated glimpses may serve better than a clear outline to suggest the interest of the whole topic. At any rate, that is my hope.
Part of the same material has been used in lectures given at the Sorbonne in the early months of 1918 and published by Crès & Cie. under the title of Essais de Médecine Sociale.
| INTRODUCTION: HISTORICAL DEVELOPMENT OF SOCIAL ASSISTANCE IN MEDICAL WORK | vii | |
| Part I: Medical-Social Diagnosis | ||
| I. | THE MEDICAL STANDING, DUTIES, AND EQUIPMENT OF THE SOCIAL ASSISTANT | 3 |
| II. | HISTORY-TAKING BY THE SOCIAL ASSISTANT | 28 |
| III. | ECONOMIC INVESTIGATION BY THE SOCIAL ASSISTANT | 47 |
| IV. | MENTAL INVESTIGATION BY THE SOCIAL ASSISTANT | 66 |
| V. | MENTAL INVESTIGATION BY THE SOCIAL ASSISTANT, CONTINUED | 96 |
| VI. | THE SOCIAL WORKER'S INVESTIGATION OF FATIGUE, REST, AND INDUSTRIAL DISEASE | 112 |
| VII. | THE SOCIAL WORKER'S BEST ALLY—NATURE'S CURE OF DISEASE | 127 |
| Part II: Social Treatment | ||
| VIII. | SAMPLES OF SOCIAL THERAPEUTICS | 151 |
| IX. | THE MOTIVE OF SOCIAL WORK | 176 |
The profession of the social worker, which is the subject of this book, has developed in the United States mostly within the past twenty-five years. Probably ten thousand persons are now so employed. It is known by various titles—social worker, school nurse, home and school visitor, welfare worker, hospital social worker, probation officer—varying according to the particular institution—the hospital, the court, the factory, the school—from which it has developed. But although the use of these visitors has been developed independently by each institution, and largely without consciousness of what was going on in the others, yet the same fundamental motive power has been at work in each case. Because this is so, we shall do well, at the outset of our study of home visiting, to get a clear conception of the common trunk out of which various types of home visitor have come like branches.
Why has such an army of new assistants been called into existence? For this reason: In the school, in the court, in the hospital, in the factory, it has become more and more clear, in the last quarter of a century, that we are dealing with people in masses so[Pg viii] great that the individual is lost sight of. The individual becomes reduced to a type, a case, a specimen of a class. These group features, this type of character, of course the individual possesses. He must be paid as "a hand," he must be enrolled in a school as "a pupil," admitted to the dispensary as "a patient," summoned before the court as "a prisoner." But in this necessary process of grouping there is always danger of dehumanization. There is always danger that the individual traits, which admittedly must be appreciated if we are to treat the individual according to his deserts, or to get the most out of him, will be lost sight of. We shall fail to make the necessary distinction between A and B.
It is the recognition of this danger which has led, in the institutions which I have mentioned, to the institution of the social worker. Above all of her duties it is the function of the social worker to discover and to provide for those individual needs which are otherwise in danger of being lost sight of. How are these needs found? In schools, hospitals, factories, courts, and in the home visiting carried out in connection with them, one can discern the two great branches of work which in the medical sphere we call diagnosis and treatment.
Thus, in the school, it is for the individualization of educational diagnosis and of educational treatment that the home visitor exists. The educational authorities become aware that they need to understand certain children or all the children of a group[Pg ix] more in detail—each child's needs, difficulties, sources of retardation. This educational diagnosis is made possible through the home visitor's study of the child in the home and out of school hours. There follows a greater individualization of educational treatment. The teacher is enabled, through the reports of the home visitor, to fit his educational resources more accurately to the particular needs of the scholar, so that they will do the most good.
In the juvenile courts the judge needs to understand more in detail the child's individual characteristics, the circumstances, the temptations, which preceded and accompanied the commission of the offence which now brings the culprit before him. This is penological diagnosis, and the court visitor or probation officer, sometimes simply called the social worker, makes a study of the law-breaker in his home and in relation to all the influences, physical or moral, which may help to explain the commission of the particular offence which has brought him into trouble. All this leads to the greater precision of penological treatment. Understanding more in detail why this particular boy has committed this particular theft, how he differs from other boys who have stolen, the judge is much more likely to choose wisely those measures of treatment which in the long run will do most to reëstablish the individual as a healthy member of society.
In the factory the object of the employer in setting a home visitor or welfare worker at work is to create[Pg x] the maximum of satisfaction and good spirit among his employees, whereby each will do his best work and be as little likely as possible to change his employment. In the old days, when shops were small and the employer could know his employees personally, no intermediary such as a home visitor was necessary. The employer could keep human touch with his men. He could know not merely the amount of work done by each man, but something of the circumstances of his life, something of his personality, his adventures and misfortunes, so that help could be extended to him from time to time when special need occurred. It is only when the workshop has grown to the enormous size familiar in modern industrial plants that this relation of employer and employee has to be supplemented through the mediating offices of the home visitor.
It is this same process of evolution, the same heaping-up of groups till finally they become unmanageable, which has led to the employment of the social worker in other institutions. It is because the schoolmaster must teach so many that he can no longer know his pupils and their families individually that he has to employ the home visitor to keep him better in touch with them. It is because the judge tries so many prisoners that he cannot grasp and pursue all the detailed characteristics of those who come before him for judgment that he is compelled to get them at second-hand from a home visitor.
So finally when we approach the reasons for which[Pg xi] the medical home visitor has come in the better dispensaries of the United States to be an essential part of the institution, we find that the unmanageable increase in the number of patients to be treated by the doctor is one of the chief reasons why the home visitor has become necessary. In the old days and in country practice especially, it was doubtless possible for the doctor to follow the lives of his patients individually as acquaintances, and through many years, to watch the growth and development of families, to know their members as a friend and not merely in a professional capacity. He would meet them as a neighbor, in church, in town meetings, in agricultural fairs, in village sports and holidays. Thus he would touch the lives of his fellow citizens on many sides, and when he came to their aid in his narrower professional capacity he could supplement his diagnostic findings and his therapeutic resources out of the wealth of knowledge which years of association with them outside the sick-room had furnished him.
But in the evolution of the particular type of social worker who is the subject of this book, the home visitor connected with a dispensary, there are other forces besides those described above, other motives besides that common to the rise of all the types of home visitors in all the other institutions named. For in the dispensary, not only has the number of[Pg xii] applicants greatly increased, but it has increased because people realized that there was much more to be obtained by going to a dispensary than was formerly the case. The development of medical science and of the resources of diagnosis and treatment which can now be put at the service of the dispensary patient, has served to attract more patients there. But these new resources have also complicated the work of the physician in a dispensary, and made it more difficult for him to remember each patient and all the details about each patient as the physical, chemical, psychological, biological facts emerge in the complex ramifications of modern diagnosis and treatment.
In the old days the dispensary, as its name suggests, was a place to dispense, to give out medicine in bottles or boxes. The patient mentioned the name of his ailment, the corresponding remedy was given. It was a quick and simple business—no individual study, no prolonged labor was necessary. Moreover, one dealt only with a clearly defined class, the poor. There was no danger that the numbers applying for relief would swamp the institution or make it impossible for the dispenser to do his work properly.
But within the past quarter of a century the dispensary, especially in the United States, has received a new idea, an access of fresh life. Largely because it has become associated with universities and been used as an instrument of medical teaching, the influence of scientific medicine has begun to be felt there.[Pg xiii] This influence has enlarged and remodelled the dispensary in two respects. First it has compelled the introduction of modern accurate methods of diagnosis, instruments of precision, time-consuming processes of examination, specialization of labor, and subdivision of function, for the skilful application of these methods. The dispensary physician is no longer content to treat a headache or a cough as an entity, to dispense this or that drug as the remedy for such a symptom. He must discover if possible the underlying disease, and, moreover, the individual constitution and life-history in the course of which the patient's complaint now rises for the moment to the surface like a fleck of white foam on an ocean wave. But how is the physician to gain this radical and detailed knowledge of his patient's life outside the dispensary and enveloping the particular complaints for which he now demands relief?
His difficulties are only increased when diagnosis is complete and he turns to the labors of treatment. For with the advance of modern medical science there are left now but few physicians who believe that disease can often be cured by a drug. It is recognized by the better element of the medical profession all over the world that only in seven or eight out of about one hundred and fifty diseases clearly distinguished in our textbooks of medicine, have we a drug with any genuine pretensions to cure. What is to take the place of drugs in dispensary treatment? In hospital patients we have the hospital régime, the[Pg xiv] unrivalled therapeutic values of rest in bed, the services of the nurses; but in dispensary practice all this is impossible. What is to take its place?
For a good many years this question remained unanswered in American dispensaries, and as a result thereof there developed the pernicious habit of giving drugs no longer believed in by the physician, the custom of giving what we call placebos, remedies known to be without any genuine effect upon the disease, but believed to be justified because the patient must be given something and because we know not what else to do or how else to satisfy him.
It was at this very unfortunate and undignified stage in the development of our dispensary work in America that we received priceless help from France, help which I am all the more anxious to acknowledge to-day because it has not, I think, been fully appreciated in the past. We in America have not given to France the full expression of the gratitude which, for her services in the field of medicine, as in even more important phases of our national life, it is to-day particularly fitting that we should utter. The timely contribution made by France at this halting and unsatisfactory stage in the evolution of our dispensaries came through the work of the great Dr. Calmette, of Lille.
Calmette's introduction of the anti-tuberculosis dispensary as a focal centre of the fight against [Pg xv]tuberculosis contained among other important provisions the institution of the visite domiciliaire. The functions of the person making this visit were not precisely the same as those of the social worker whom I am describing in this book, but the latter may truly be said to have grown out of the former, nourished by some contributing elements from other sources. So far as I know, Calmette was the first to see that in the struggle of the dispensary against this particular disease, tuberculosis, it is essential to make contact with the home, and to treat the disease there as well as at the dispensary itself. In Calmette's view the function of the visite domiciliaire was an outgrowth of his bacteriological training and his bactericidal plan for treating tuberculosis. The home visitor was a part of the plan of antisepsis, a method of destroying the bacteria through disinfection and sterilization of the premises and of the patient's linen. In America the work of the home visitor in cases of tuberculosis has been concerned less with the disinfection and bactericidal procedures than with the positive measures of hygiene, such as the better housing of the patient, better nutrition, better provision for sunlight and fresh air, and above all instruction of the patient as to the nature of his disease and the methods to be pursued in combating it. But the great debt which we owe to Calmette was the linkage of the dispensary and the home by means of the home visitor. In America we have applied this principle, outside the field of tuberculosis, to all[Pg xvi] other diseases, and we have broadened the field of work assigned to the social worker. Nevertheless, the idea was primarily Calmette's.
There was another leading idea of Calmette's which we have followed first in relation to tuberculosis, later in dealing with other diseases. Like Calmette we have stopped wholesale drugging, and put our trust in those scientific hygienic procedures which carry out our knowledge of the nature of the disease which we are combating. Calmette's measures have the tone and the point of view of preventive medicine, and of that sound science which we have learned to associate with the Pasteur Institute and all that development of medicine which took its rise from Pasteur.
The focussing of interest upon a single disease which began, so far as I know, with Calmette's anti-tuberculosis dispensaries, has been fruitful in many ways. In the first place, it has enabled science once more to conquer by dividing the field, to help humanity by devoting itself to a single manageable task. Like others of Calmette's ideas, this isolation of a single disease for group treatment in dispensaries has been followed in fields with which he never concerned himself. Thus we have had special classes for cases of heart disease, for diabetes, for syphilis, for the digestive disturbances of infancy, and for poliomyelitis. A valuable measure of success has come in each of these diseases through the concentration of attention, at a special day and special hour[Pg xvii] by a special group of physicians and assistants, upon one disease at a time. We have even used class methods and taught the patients in groups as scholars are grouped and taught at school.
But there has come another signal advantage in the point of view adopted by Calmette in his dispensary campaign—the point of view, namely, of public health and public good. It has freed us from the limitations contained in the old idea that a dispensary is an institution concerned solely with the poor. Tuberculosis, of course, like every other infectious disease pays but little respect to distinctions of property. From the point of view of the State a tuberculous individual is as dangerous to others and a cured tuberculous patient is as valuable as a possible asset to the State, whether his income is above or below a certain figure, whether, in other words, he is inside or outside the imaginary group sometimes called the poor. From the institution of tuberculosis dispensaries with their home visitors in America, the poverty of the individual ceased to be a necessary badge for admission. Especially since many of our dispensaries have been instituted and maintained by the State, and therefore are paid for by all its citizens in their taxes, any one so unfortunate as to acquire tuberculosis, or be suspected of it, feels himself wholly justified in seeking help at a State-maintained tuberculosis dispensary. In this respect, as in many others, the campaign against tuberculosis has had a value far[Pg xviii] greater than its measure of success in checking that disease. It has introduced methods which were applicable outside the field of tuberculosis. One of these, as I have already said, was the utilization of the home visitor. A second was the disregarding of property lines. A third was the frank and confident reliance upon scientific measures and the relegation of eclecticism and quackery to the hands of those who make no pretence at scientific education or honest dealings with the public.
I must speak at this point of another great French contribution towards the occupation which in its fully developed state we now call social work. I mean that which at present receives ordinarily the name of the "Œuvre Grancher." Grancher proceeded upon the same sound bacteriological foundations which guided Calmette. Since children are especially susceptible to tuberculous infection (though they rarely show alarming signs of it till later years), he planned the separation of children from the neighborhood of tuberculous parents or other tuberculous persons as an essential measure for preventing contagion. I am not concerned now with the enormous benefit derived by the forces struggling against tuberculosis from this insight of Grancher's, nor with the part which it has played in such success as that fight has already attained in the United States and elsewhere. What interests me particularly in [Pg xix]connection with the topic of this book, is that the procedures suggested by Grancher led the physicians who came in contact with the tuberculous individual in a dispensary to extend their interest to other persons who did not present themselves at the dispensary as patients. It is not obvious at first sight how great a transforming principle is thereby introduced. Hitherto the doctor had been passive in his activities at the dispensary. He had concerned himself with such patients as chanced to appear there. He had never taken the active or aggressive attitude, searching for possible patients among those who had made no attempt to avail themselves of his services. Now he goes to find patients.
This is an epoch-making change. The physician becomes henceforth not merely a person who stands ready to treat disease when the accidental and incalculable forces of custom, hearsay, and natural propinquity bring the patient to him. He becomes now a person who actively wars against disease, who searches it out wherever it may be found. Thus he approaches for the first time the possibility of truly preventive action, the possibility of killing disease in its infancy or preventing its birth. For it is well known that preventive action in relation to disease is well-nigh impossible if we are forced or accustomed to wait until the disease has made such progress that the patient himself is aware of it and forced by its ravages to ask medical aid. Ordinarily the patient seeks the physician only when he has[Pg xx] broken down. From the point of view of public health and public good, this is grievously late, far too late. It is as if one inspected an elevator only after it had fallen and killed or maimed its passengers, instead of inspecting it at regular intervals so as to prevent its breaking down.
In this series of aggressive steps in the campaign against tuberculosis whereby one seeks out possibly infected children, brings them to a dispensary for examination, and separates them from their infected parents or house-mates, the social worker is the all-important executive. She finds the children, brings them or has them brought to the dispensary, and sees that financial aid or other assistance is given so as to carry out the isolation demanded by our bacteriological knowledge of the disease.
As far back as 1895 the reforms introduced by Calmette and Grancher in the field of tuberculosis had begun to modify and improve the treatment given in our dispensaries, not only to tuberculosis but to all other diseases. Especially it had favored the growth of home visiting, at first for the specific ends for which it was designed by Calmette and Grancher, but later for the prosecution of various related purposes which the very process of visiting brought to light. Not only in tuberculosis, but in other diseases, it was soon found that a knowledge of home conditions and of the family was essential for the [Pg xxi]treatment of the single patient who chanced to appear at the dispensary.
It was my good fortune during the ten years preceding 1905 to work as a member of the board of directors of a private charitable society caring for children deserted by their parents, orphaned, cruelly treated; also for children whose parents found them unmanageable or for children who had special difficulties in getting on at school. The work of this society brought to me detailed knowledge of the life-histories of a good many children. I watched the careful studies made by the paid agents of the society into the character, disposition, antecedents, and record of the child, his physical condition, his inheritance, his school standing. I noticed during these years how the agents of this society, to whom the child was first brought by its parents or by others interested in it, utilized to the full the knowledge and resources of others outside its own field; how, for example, they enlisted the full coöperation of the child's school-teacher, secured facts and advice from the teacher, and agreed with her upon a plan of action to be carried out both by her and by the home visitor in concert. Moreover, I saw how physicians were consulted about the child, and how their advice and expert skill contributed something quite different from that obtained from the teacher or that gained by the home visitor herself. The priest or clergyman connected with the family was also asked for aid, and sometimes could give very great help,[Pg xxii] differing essentially in kind from that given by the teacher or by the doctor. If there were problems involving poverty on the part of the parents, other societies concerning themselves particularly with the problems of financial relief were asked to aid, in order that indirectly the help given to the parents might make itself felt in the better condition of the child. Sometimes free legal advice was obtained from the legal aid society formed for the purpose of giving such advice to those who were unable to pay for it.
As I watched the application of this method over a period of a good many years and in the case of a great many children, I saw a good many failures in addition to some most encouraging successes. But what most of all impressed itself upon me was the method, the focussing of effort on the part of many experts upon the needs of a single child, the coöperation of many whose gifts and talents varied as widely as their interests, to the end that a single unfortunate child might receive benefit far beyond what the resources of any single individual, no matter how well intentioned, could secure.
I have said that the doctor was a member of the group whose efforts were focussed upon the needs of a single child, but he was never a very closely connected member of this group. A few charitably inclined physicians, personal friends of those directing the charities, were called upon again and again to help out in individual cases by examining a child, by[Pg xxiii] giving advice over the telephone or otherwise. Through the free hospitals and dispensaries help was also obtained for the physical needs of persons who had come to the notice of the different charitable associations by reason of economic need or other misfortune. But the medical charities, the hospitals, dispensaries, convalescent homes, and the benevolence of individual physicians were not well connected with the group of charitable associations which I have been referring to above.
At this period, in 1893 and 1894, I had been working for some years as a dispensary physician, concerning myself chiefly with perfecting the methods of diagnosis in a dispensary, so that the patient could obtain there a diagnosis as correct and scientifically founded as he could obtain from a private physician. But in the course of these efforts for a complete and exact diagnosis which should do justice to the actual needs of the patient, I found myself blocked. I needed information about the patient which I could not secure from him as I saw him in the dispensary—information about his home, about his lodgings, his work, his family, his worries, his nutrition. I had no time—no dispensary physician had time—for searching out this information through visiting the patient's home. Yet there was no one else to do it. My diagnoses, therefore, remained slipshod and superficial—unsatisfactory in many cases. Both in these cases and in the others where no diagnosis was possible from the physical examination alone, I[Pg xxiv] found myself constantly baffled and discouraged when it came to treatment. Treatment in more than half of the cases that I studied during these years of dispensary work involved an understanding of the patient's economic situation and economic means, but still more of his mentality, his character, his previous mental and industrial history, all that had brought him to his present condition, in which sickness, fear, worry, and poverty were found inextricably mingled. Much of the treatment which I prescribed was obviously out of the patient's reach. I would tell a man that he needed a vacation, or a woman that she should send her children to the country, but it was quite obvious, if I stopped to reflect a moment, that they could not possibly carry out my prescription, yet no other filled the need. To give medicine was often as irrational as it would be to give medicine to a tired horse dragging uphill a weight too great for him. What was needed was to unload the wagon or rest the horse; or, in human terms, to contrive methods for helping the individual to bear his own burdens in case they could not be lightened. Detailed individual study of the person, his history, circumstances, and character were frequently essential if one was to cure him of a headache, a stomach-ache, a back-ache, a cough, or any other apparently trivial ailment.
Facing my own failures day after day, seeing my diagnoses useless, not worth the time that I had spent in making them because I could not get the[Pg xxv] necessary treatment carried out, my work came to seem almost intolerable. I could not any longer face the patients when I had so little to give them. I felt like an impostor.
Then I saw that the need was for a home visitor or a social worker to complete my diagnosis through more careful study of the patient's malady and economic situation, to carry out my treatment through organizing the resources of the community, the charity of the benevolent, the forces of different agencies which I had previously seen working so harmoniously together outside the hospital. Thus I established in 1905 a full-time, paid social worker at the Massachusetts General Hospital, to coöperate with me and the other physicians in the dispensary, first in deepening and broadening our comprehensions of the patients and so improving our diagnoses, and second in helping to meet their needs, economic, mental, or moral, either by her own efforts, or through calling to her aid the group of allies already organized in the city for the relief of the unfortunate wherever found. To bring the succor of these allies into the hospital and apply it to the needs of my patients as they were studied jointly by doctor and home visitor, was the hope of the new work which I established at that time.
In the thirteen years which have elapsed since this period, about two hundred other hospitals in the United States have started social work, some of them employing forty or fifty paid social workers for[Pg xxvi] the needs of a single hospital. Unpaid volunteer work has always been associated with that of the paid workers in the better hospitals.
I should mention, in closing this chapter, three forms of medical-social work which had been undertaken previous to 1905, and which were more or less like the work which I have just described, though not identical with it:
(1) The after-care of the patients discharged as cured or convalescent from English hospitals for the insane (1880). The visitors employed in this work followed the patients in their homes and reported back to the institution which they had left. Their labors were directed chiefly to the prevention of relapses through the continuation in the home of the advice and régime advised by the hospital physician and previously carried out in the institution.
(2) The work of the Lady Almoners long existing in the English hospitals had begun about the time that I started medical-social-service work in America, to change its character so as to be more like the latter. Originally the purpose of the Lady Almoners was to investigate the finances of hospital patients in order to prevent the hospital from being imposed upon by persons who were able to pay something, but who represented themselves as destitute and therefore fit subjects for the aid of a charitable hospital. Gradually, however, the Lady Almoners had begun to be interested in the patients as well as in the hospital funds, and had begun to labor for the[Pg xxvii] patients' benefit as well as for the hospital's. This brought them near to the idea of hospital social service as practised in this country since 1905.
(3) The visiting nurses or public health nurses, employed by a Board of Health or by private agencies for the care of contagious diseases in the home and also for the nursing of the sick poor whatever their malady, have found it more and more difficult in late years to confine their work wholly to physical aid. They have been forced to take account of the patients' economic, mental, and moral difficulties, to extend their work beyond the field of nursing proper, and thus to approach very closely to the field of the social worker. It is my own belief that the frontier separating visiting nurse and medical social worker should be rubbed out as rapidly as possible, until the two groups are fused into one. The visiting nurse must study the economic and mental sides of the patients' needs, and the social worker must learn something of medicine and nursing. Then the two groups will be fused into one, as indeed they are fast fusing at the present time.
SOCIAL WORK
SOCIAL WORK
I have said in the Introduction that home visiting may easily and properly spring up in connection with various institutions; for example, in connection with the schools, courts, or factories of the city as well as with the dispensaries. But it is essential in home visiting, no matter what institution it is connected with, that the social assistant should be distinctly recognized as part of the machinery of that institution, or, in other words, as one of the means by which that institution does its work. If she is connected with the schools, she should be a part of the school system alone, not responsible to a Board of Health or to any other outside agency.
So in the type of home visiting which now particularly concerns us, it is essential to make it clear from the outset that the social worker is a part of the medical organization. She is one of the means for diagnosis and treatment. All that she does from the moment when she first scrapes acquaintance with the patient is to be connected with the condition of the patient's health. She is not to pursue [Pg 4]independent sociological or statistical inquiries. She is not to be the agent of any other non-medical society. It is unfortunate even if her salary should be paid from any source other than the medical institution itself.
There are great advantages in this apparently formal and obvious point of connection. In the first place the medical method of approach to close relations, to friendly relations, with a group of people, is decidedly the easiest. Persons who may be suspicious or resentful of our approach if we appear primarily as investigators, or primarily as persons concerned with economic or moral control, will welcome the visitor if she appears as the arm, the cordially extended hand, of the medical institution where they have already found welcome and relief. I know well that charity organization workers, court workers and others may establish just as close a relation with their clients in the end as is possible for the medical social worker. But the start is harder and needs more experience. Because disease is the common enemy of mankind, all sorts and conditions of men are instinctively drawn together when it becomes necessary to resist the attacks of disease as the enemy of the human family. Members of a family may disagree about many matters, and may be far from congenial with one another in ordinary times and upon ordinary subjects, but will draw together into the closest kind of unity if any one attacks the family, accuses or criticises the family. So human beings of[Pg 5] widely different environment, taste, economic status, heredity, may find it quite easy to begin and to maintain friendly relations when that which brings them together is their common interest in the struggle against disease. It is, indeed, almost too easy to get friendly with people when they are suffering physically and we are endeavoring, however lamely, to bring them relief.
The medical avenue of approach, then, the plan and hope of establishing intimate relations with a person or a family while we are trying to give them medical assistance, offers incomparable advantages. These advantages become clearer still if we compare them with the special difficulties which arise if one tries to begin an acquaintanceship with financial inquiries or with moral investigations. People who will agree on everything else will quarrel on money matters. There is nothing that so easily leads to friction, suspicion, and unfriendliness, as the interview in which one is trying to make out whether people are speaking the truth, the whole truth, and nothing but the truth, in relation to their income and expenditure. This matter very naturally seems to people their own business. They quite naturally resent inquiries on such matters by strangers. They feel attacked and in defence they are apt to conceal or color the truth. And yet, if a friendly relation has first been established through the patient's recognition of our genuine desire to help his physical difficulties, the financial inquiries which make a necessary part[Pg 6] of the home visitor's work can much more easily follow. One has to understand what money is available in order to make the best plans for nutrition, for home hygiene, for rest and vacation—all of which naturally form part of our medical interest. I wish to make quite clear here my appreciation that good social workers never begin their relationships with a client by assuming a moral fault on his part and never push the economic questionnaire into the first interview. All I wish to point out is that it is perhaps easier for the medical social worker than for others to avoid these blunders.
At the outset of a relationship which aims to be friendly, investigations which start with the assumption that there has been some moral fault or weakness in those whom we wish to help are even worse than financial inquiries. The instant that the social worker finds herself in the position of a moral critic, it becomes next to impossible that a friendly relation not hitherto established, shall be built up from the beginning. Late in the course of a friendship established long before, moral help, even moral criticism, may be welcome. But it cannot often or easily be one of the topics of conversation, one of the points of investigation, in the early stages of what we hope to make a friendly relation.
Everything stands or falls with this. We cannot even teach hygiene, we cannot even make medical principles clear unless we have succeeded to some extent, perhaps without any merit on our part, [Pg 7]perhaps through extraordinary good fortune, in acquiring a genuine liking for the person whom we want to help. Once that is attained, we can work miracles. But if it is wholly lacking, we cannot count upon accomplishing the simplest interchange of accurate information; we cannot achieve the most elemental hygienic instruction.
But there is another signal advantage in the medical point of approach to a relationship which, as I have said, must be friendly in fact, not merely in name, if it is to succeed in any of its ulterior objects. When the social worker begins the difficult task of acquiring her influence in a family, she starts with a great deal in her favor if she appears in the home as the agent of the physician. He has prestige. By reason of his profession, by reason of the institution which he represents, by reason of confidence already established by him in the patients' friends and neighbors, the new family is ready to have confidence in him. He is not thought to have any axe to grind. He is assumed to be genuine in his desire of helpfulness. Therefore any one who appears in his name, as his assistant, has a great deal in her favor, especially when compared with the visitors of societies which might be supposed to begin with economic or moral suspicions about the family. If the visitor appears in the home with the prestige of a medical institution enhancing the value of her own personality, she has a very definite advantage.
I have said that it is essential to the success of a medical visitor's work that she should be part of the medical machine, acknowledged as the doctor's agent, concerned wholly with helping to carry out his plans. But we must ask now, what part? And the answer is that the social worker is an assistant to the physician both in diagnosis and in treatment. I will begin with an account of what she is to do as his assistant in diagnosis.
She is to discover, so far as she can, what the disease is, how much the disease is, and why it is. I do not mean, of course, that she is to ape the doctor's scientific investigations, that she is to use instruments of precision, or to try to prescribe medicines. But she is to help the physician in some of the following ways:
He is often very much at a loss to be sure how bad the patient's symptoms really are, how much the patient suffers, how serious the case is. The social worker is often able to help in discovering why the patient really came to the dispensary, discovering, perhaps, that the reason is such as to show that the malady is really a trifling one. She may find, for instance, that the patient has come merely because her husband had to come, anyway, and she thought she would get the benefit of whatever there was to be had in the way of medical assistance at the dispensary, even though, unless her husband had been[Pg 9] going, anyway, it would not have occurred to her to make the independent visit upon her own account. Or, again, the visit may be due chiefly to curiosity, especially if the dispensary has been newly established or has added some new features to its methods of diagnosis and treatment. These facts are passed along from person to person; the person hearing of them may appear as a patient chiefly to see just what it is that her neighbors are getting when they go to the dispensary. I have known a patient to come merely because he was alarmed as a result of a recent conversation with a friend. His friend had been hearing about heart trouble and had mentioned some symptoms such as pain about the heart or cold extremities or dizziness. Any one sick or well on hearing such symptoms may easily remember that he has had them himself not long ago, or may even begin to feel them as a result of suggestion. Straightway, perhaps, he will betake himself to the dispensary, complaining of symptoms which never would have been noticed but for his talk with the friend.
Or, again, the patient may have some definite organic disease or some obstinate train of discomforts and physical inconveniences. But he has adapted himself to them tolerably; he has settled down to bear or forget them as best he may. He may know that his troubles are really incurable and yet not serious. He may have become as accustomed to them as he is to an uncomfortable lodging or to a modest income. Yet, as a result of some temporary[Pg 10] fatigue, some newspaper paragraph, some fragment of gossip overheard, there may arise in him a crisis of alarm and worry about his familiar discomforts or inconveniences. Thereupon he may betake himself to a dispensary, and give the physician an account which may be very difficult to interpret, because the physician does not understand the train of events which appear acute and new in that they have led the patient just now, rather than at any earlier time, to seek advice. After nearly twenty years' experience of dispensary work I should say that in no respect can a social worker give the doctor more welcome help than by discovering now and then reasons such as I have just suggested whereby the patient comes to the dispensary now rather than at any other time, and at a season not really connected in any special way with the nature of his disease.
Perhaps I can make this clearer by contrast with its opposite. A person who has just developed a scarlatinal rash, who has just coughed and raised a considerable quantity of blood, who has just lost the power to move half of his body, who has just begun to have swelling of the face, naturally consults a doctor at once. If he then comes to a dispensary for treatment, he has come at a time which is the right time, the reasonable time, considering the nature of his malady. Something new has happened. An attack has been made which should be foiled if possible at once. The clue for usefulness on the part of the[Pg 11] doctor is thus fairly clear. If, on the other hand, a person has had more or less back-ache all his life, and has grown used to getting along and doing his work, even enjoying life in spite of it, he may suddenly come to a dispensary for that back-ache because he has seen in the newspaper the wholly false statement that pain in the back means kidney trouble. Yet when he comes to the dispensary he may say nothing whatever about his having seen this newspaper advertisement. Indeed, it is very unlikely that he will mention this at all. He will describe his back-ache as something which demands immediate treatment, and the doctor may set in motion extensive and probably useless activities of investigation or treatment which never would have been undertaken had he known just what it was that brought the patient to the dispensary that day rather than months earlier or later.
So far I have spoken only of cases in which the visitor's studies in the home make it clear that the case is not as bad or not as manageable as it might have seemed if one had known only what the patient himself could reveal in the dispensary. But occasionally on reaching the patient's home the visitor may find reason to believe that the symptoms are much more serious, the disease much more urgent, than could have been realized from the story told and the facts obtained at the dispensary. The visitor may find in the home conditions of disorganization, dirt, disorder, serious malnutrition, [Pg 12]discouragement on the part of other members of the family, arguing a much more serious condition of the patient than one would have realized from talking with him at the dispensary. As a result of such findings the doctor, who must spend his energies for the patients who need him most, will see that he had better give more time and more effort to the patient than he would otherwise have thought right.
Still, again, the visitor may find that the symptoms are neither more serious nor less serious than he would have supposed from the dispensary interview; yet the clinical picture is different from the doctor's because the patient has thrust into the foreground of the clinical picture something which further knowledge shows to be really unimportant, while he has said almost nothing of some other feature of the trouble which is really much more serious. For example how much does the patient really eat, how does he do his work, are there complaints about him from his "boss," has he always had the cough which he has only just now begun to complain of? Such questions can be better answered after visits at the home and talks with the whole family.
Clearly the supplementary information thus secured by the social worker will count for nothing unless clearly explained to the doctor, and is taken up by him as part of the evidence on which he bases his diagnosis and his treatment. It is absolutely essential that the social worker should not merely make her visits and record them in her notebook, but[Pg 13] should incorporate her findings in the medical record and deliver them not formally but effectively to the doctor's mind.
Such help is needed because she can often learn far more in the quiet of an interview at home than would be possible for the doctor despite all his medical skill. For at the dispensary he questions the patient when he is confused and forgetful, alarmed, perhaps, by the sights and sounds of the clinic, and so very unlikely to give a correct and well-balanced account.
So far I have been describing the work of the social worker as a process of finding out how much ails the patient and what his symptoms signify. But it is also a part of the social worker's duty to find how much disease is present not only in the individual who appears in the clinic, but in his immediate environment, to discover nests, foci or hotbeds of disease. In the case of a disease like smallpox, this is obvious. If a patient presented himself at a dispensary with the pustules of smallpox upon his body, it would be criminal negligence on the part of the physician not to set on foot a search of that patient's home, his industrial environment, or, in the case of a child, his school environment, for evidence that others have been exposed to the same contagion and possibly already infected. This sort of duty cannot be abandoned merely because there is no health officer at[Pg 14] hand. It is a crying need and must be attended to at once.
Now in a minor degree this is true of many other diseases as well as smallpox. We are beginning to realize that it is true of tuberculosis, so that when one case of advanced and therefore contagious tuberculosis is seen at the dispensary, machinery should automatically and invariably be set in motion to search out possible paths of contagion from that patient to others, just as if he had smallpox.
This principle which is well established in the case of dangerous contagious diseases like smallpox and diphtheria, and is beginning to be established in relation to tuberculosis, is even more important in dealing with syphilis. Every case of syphilis means more cases of syphilis, and the danger of still more each day that the contagious patient is at large. No physician has done his duty unless, after seeing a case of syphilis, he attempts, through a social worker or otherwise, to get knowledge of others from whom this disease has been acquired, or to whom it may be freshly spread. At the Massachusetts General Hospital each patient with syphilis is asked to bring to the clinic for treatment the person who infected him. The method sounds impossible but in fact it works, and many cases are thus brought under treatment and prevented from infecting others.
With contagious skin diseases such as scabies or impetigo, the principle is obviously the same, though the dangers of disregarding it are not so great. With[Pg 15] typhoid fever, which not very infrequently shows itself even at a dispensary, the duty of the social worker is not so much to search for other persons through whom it may have been contracted or to whom it may be spread, as to investigate the water-supply and the milk-supply of the patient and of others in his environment. One case of typhoid always means more cases, usually more cases acquired, not by contact with one another, but through their share in a contaminated water-supply or milk-supply. The social worker, therefore, should know how to search out contaminated water-supplies, or at least to put in motion such machinery of public health investigation in the city or town where the case arises as may lead to good detective work in the attempt to track down the source of the trouble. It has been well said that every case of typhoid is some one's fault. It has even been asserted that for every case of typhoid some one should be punished. Certainly there are some grounds for such an assertion.
Commoner and not less important than the contagious diseases that I have just mentioned are industrial diseases, or diseases aggravated by the conditions of industry. A physician may serve for many months in a dispensary without seeing a case of smallpox, of trichiniasis, or of typhoid fever, or feeling it his duty to set in motion the forces that I have just mentioned for rooting out the sources of [Pg 16]contagion and preventing their further spread. But he cannot serve a month in any well-attended dispensary without seeing cases of industrial disease in the narrow sense, such as lead poisoning, or of independent disease aggravated by the conditions of industry, such as the functional neuroses of cigar-makers or of telephone operators. With such diseases, as with the infectious and contagious diseases, the presence of one case in the clinic should lead straight to the inference that there are others elsewhere, out of sight but no less important from the point of view of public good. This conclusion should lead in turn to the search through a social worker for the cases of disease which do not present themselves to any physician, which may be totally unknown even to the patient himself, yet which are important to the health of the nation.
Difficult though this field of industrial disease has shown itself to be, difficult though it is to separate out that portion of the patients' complaints which can justly be referred to the conditions of his work, and to distinguish it from the portions which are due to the way he lives, to his inheritance, to his habits or to diseases like tuberculosis and syphilis which may have been acquired without any connection with his work,—nevertheless we must try to disentangle and to recognize the elements in this knotty problem. And we can hardly fail to see that the social worker is an essential and logical assistant in the processes of investigation which we must carry out. If[Pg 17] we can ever unravel the tangled skein of causes and effects whereby the hours of work, the strain of work, the patients' heredity and his home conditions, all combine to produce the symptoms of disease, it will be through such intimate, prolonged, detailed studies as the social worker can carry out, especially if she becomes a friend of the family. The doctor in his hours of consultation at the dispensary certainly can never do it. The official agent of the Board of Health, perhaps feared, certainly not a natural confidant for the family, may easily miss the truth which the social worker unearths, provided always she succeeds in differentiating herself altogether from the impersonal and professional investigator, and gradually becomes in the mind of the family and in truth their friend.
I said above that the social worker should try to find out what disease, how much disease, and why this disease is present. The answers to these three questions cannot be kept separate. If one knows how much importance to attribute to a given symptom and whether it is as bad as it seems or worse than it seems in the dispensary interview, one may be steered straight to a correct diagnosis. To know how much disease may thus mean knowing what disease is present. Furthermore, the understanding of these questions, even though it be only partial and unsatisfactory, leads us a considerable distance towards understanding why the disease has arisen. The search for sources for contagion is an example of a[Pg 18] search for a why in disease. The search for psychical factors—groundless fears, misleading newspaper advertisements, distracting rumors—all this is also a search for the cause as well as for the nature of disease.
The social worker's investigations into the cause of disease may perhaps be still further exemplified. I once sent a social worker to my patient's home with the request that she try to find out what I had failed to find out, namely, why a young girl could not sleep. Physical examination of the girl had revealed no cause; the exploration of such parts of her mind as she would reveal to me had thrown no light upon the trouble. I was at a loss and asked for help through the more intimate knowledge of the patient sometimes to be gained through a social worker's studies. Such a search might easily have been fruitless—it often has been fruitless in my own experience. But in this case it was almost comically swift in reaching its goal. The visitor found that this girl was sleeping with two other girls of about her own age, in a bed hardly more than a metre wide. It needed only that she should acquire a separate bed for herself, which she was able to do without any financial assistance. She then regained her power to sleep. How often have such cases been treated with drugs or perhaps with more complicated physio-therapeutic or psycho-therapeutic procedures, when some simple fact like the size of the bed, the temperature of the sleeping-room, or the mental [Pg 19]activities of the evening immediately preceding bedtime, are really responsible for the whole trouble.
In order to carry out the particular procedures of diagnosis and treatment which belong within the province of the social worker, a certain amount of medical knowledge is needed. Because this is true, it has often been assumed that the social worker must be a trained nurse, prepared by months or years of experience in a hospital. But experience has shown that much of the knowledge possessed by nurses who have had this training cannot be used by the home visitor. On the other hand, the information which the social worker needs is often quite lacking even in well-trained nurses. Furthermore, it may be said with truth that the training of a nurse, as we know it in America at any rate, really unfits a woman in some respects for the work of a social worker, since it accustoms her to habitual obedience and subordination. These habits are very useful in their proper place, but they are antagonistic upon the whole to the temper and mental activity which is important in the social worker. I mean the temper of aggression in relation to disease, and the mental attitude of the teacher and leader in relation to the patient. But of this point it will be more in place to speak when I come to consider the functions of the social worker as a teacher.
Let us return, then, to the question, What [Pg 20]knowledge should the social worker possess in order to do her part in the "team-work" of the medical-social dispensary? Her knowledge should approximate that of the public health officer. Like him she should be, above all, familiar with what is known to medical science about the causes of disease. This is of great importance because it is especially in this field of medical science and medical ignorance that the public, the patients among whom the social worker will work, is most in need both of new knowledge and of the uprooting of old error and superstition. Medical science knows very little of the causes of many diseases. But our patients, especially the more ignorant of them, are very glib and confident in their assertions as to what has caused the particular disease from which they just now suffer. They tell us about their "torpid livers," their "congestive chills," their "ptomaine poisonings" and the like. Their supposed but unreal knowledge is extensive and detailed. Indeed, so stubborn are their beliefs upon such matters that they often present a firm wall of resistance which must be broken down by the social worker before any truth upon these matters can be introduced into their minds.
The social worker, then, should share such knowledge as the medical profession possesses about the causation of infectious disease, about direct personal contagion, and also about the indirect methods by which disease is conveyed from person to person through insects or through instruments and [Pg 21]utensils, such as the barber's razor, the family towel, or the public drinking-cup. She should be familiar with the small body of knowledge which we possess upon the transmission of disease by drinking-water, by milk, and other kinds of food. She should appreciate our still smaller body of knowledge about the relation of disease to climate, to weather, and to other physical agents such as the extreme heat and cold produced by some industrial processes, and the action of X-rays.
In addition to this definite and specific knowledge of causes, she should know the generally accepted views of the medical profession on the subject of bodily resistance, immunity, inheritance, the diseases and perversions of metabolism, and the other non-bacterial factors in the production of disease. Above all, she should realize the multiplicity of causes which science more and more clearly recognizes in their single result. She should learn both by precept and by experience that for a single fact such as disease or health there are always many causes, so that any one who points confidently to a single cause, such as cold, fatigue, bacteria, or worry as a sufficient explanation of a person's disease, is almost certain to be wrong. Obviously, this truth bears a close relation to what is to be said on the "historic and catastrophic points of view." Chapter III.
The importance of teaching the social worker all that is known about the transmission and causation of disease is due to the following fact: whatever we[Pg 22] succeed in accomplishing in our efforts at preventive medicine, whatever we do to nip disease in the bud or to check the spread of epidemics, is due to our knowledge of the causes of disease. The instructions of the doctor at the dispensary can accomplish but little in this field when compared with the detailed teaching of the social worker in the patient's house, in his workshop, in the schools and factories where disease is spread so much more frequently than in the dispensaries. If we hope to show people how they can avoid the disasters of illness, our teaching should be given in the very place where these disasters most often occur. There we can illustrate and demonstrate with the objects in sight what is to be done and to be avoided.
It is for this reason that the social worker is above all others the person who can convey life-saving information to the public in an effective way. A considerable amount of this precious knowledge is now possessed by the medical profession; but it is shut away useless, unavailable, in medical libraries and in doctors' minds. The social worker can fight disease by spreading the contagion of medical truth. She can multiply the foci from which truth can spread still more after she is gone, just as disease is redistributed again and again from new nests of infection.
The prognosis of disease, like its causation, is a subject on which the social worker should know almost as much as the doctor. This is possible because medical knowledge on this subject is still so very limited. For[Pg 23] the purposes of one who has to combat the poverty, sorrow, idleness, and corroding fears which disease produces, knowledge of prognosis is a most useful tool. For example: if one is to make plans for the care of a group of children during their mother's illness, one must have some idea how long that illness is going to last. If it affects the bread-winner of the family, how long will he or she be disabled, and how completely; what are the hopes of ultimate and complete recovery; will chronic invalidism follow; is it worth while in this particular disease to spend a great deal of money and time in trying to achieve a complete cure, or is cure so improbable and at best so incomplete that our resources can be expended more wisely in other directions?
A knowledge of prognosis will help the home visitor greatly in the solution of such problems. But it must be added that such knowledge as she already possesses about the prognosis of a disease, such as tuberculosis or heart trouble or kidney trouble, must always be supplemented by all the information that she can gain from the doctor as to the present prognosis in the case of the particular patient with whom the social worker has to deal. For the general prognosis of a disease is greatly modified by the particular circumstances in each individual case.
Physicians are not at all eager to impart their knowledge about prognosis, because this knowledge is so limited and so faulty. No scientific man likes to make definite statements upon so indefinite and hazy[Pg 24] a matter as prognosis. Nevertheless, it is essential for the patient's good that the doctor should be asked to give her as clear and definite a statement as is possible for him to make with the facts that he possesses. For it is only upon the basis of such a statement that an intelligent plan of social treatment can be constructed.
Besides acquiring all that she can learn of the causes and prognosis of disease, the social worker should be familiar with the symptoms of the more important and common types of disease. There are now several books written particularly with the object of conveying to social workers and others such knowledge as I have referred to, yet without any pretence of equipping the person either for nursing or for the practice of medicine. I will mention here a book by Dr. Roger I. Lee, Professor of Hygiene in Harvard University, "Health and Disease: Their Determining Factors" (Little, Brown & Co., Boston, 1917), and my own book, "The Layman's Handbook of Medicine" (Houghton Mifflin Co., Boston, 1916).
In order to understand such books, and to arrange her knowledge of disease in such form that it may be easily handled, the social worker must have a slight knowledge of anatomy and physiology, so that she can arrange the symptoms of disease in connection with the different systems of organs: circulatory, digestive, respiratory, urinary, nervous, and locomotive.
Finally, the social worker must know the principles of hygiene, in order that she may effectively combat medical quackery and the prevalent medical superstitions of the people. That portion of hygiene which is both securely founded upon scientific evidence and useful in the preservation of health, makes up only a very small body of knowledge, so that it can be easily mastered by any intelligent person. Our knowledge upon such matters as diet, exercise, bathing, sleep, ventilation, when such knowledge is both scientific and practically useful, could be written upon a very few pages. It consists largely of negatives which contradict the current superstitions.
In my own work in this field I have found it essential that there should be no mystery and concealment, no obscurantism and mediæval Latin in the methods of treatment which the social worker explains or carries out under the doctor's directions. She must be able to deal with the patients frankly, openly, without concealment or prevarication. Otherwise she will not have moral force enough behind her statements to bring them home to the patient so as to secure any reform in his hygienic habits. Such reforms are difficult enough in any case. They are usually impossible unless they can be initiated by one rendered eloquent and convincing by the consciousness that she leans upon the truth and has nothing to conceal. If she has mental reservations, if she is trying to protect the authority of the physician in a statement which she does not believe[Pg 26] to be wholly true, the force of her appeal will be so weakened that it will probably be ineffective.
There are some technical processes of diagnosis and treatment which are usually carried out by the visiting nurse, but which may well be performed after a brief training by the social worker who is not a nurse. Among these are:
(1) The accurate reading of the patient's temperature, pulse, and respiration, which she must often teach the patient to do for himself and to record accurately and clearly. This is of especial importance in tuberculosis, for in suspected cases of this disease one often needs daily measurements of the temperature as an aid in determining the diagnosis or in estimating the severity of the case and the fitness of the patient for work.
(2) The arrangement of a window tent or some other device for insuring the maximum of fresh air for the tuberculous patient both day and night. This device is also useful in pneumonia, typhoid fever, and other diseases, in case they are to be cared for at home and not in a hospital.
(3) The application of simple dressings to wounds, abscesses, and common skin diseases such as eczema, and impetigo.
(4) The care of the skin in bedridden patients. Our primary object here is the prevention of bedsores, those ulcerations which occur in very emaciated[Pg 27] patients at the points where their weight presses a bone against the bedclothes.
(5) The simpler procedures for the preparation of milk for sick children and of other foods commonly advised for patients who are confined to bed.
(6) The methods of emptying the lower bowel by means of an enema.
Into the details of these procedures this is not the place to enter, but I wish specially to assert that all of them may be learned within a few weeks by persons who have not studied medicine or had the full course for the training of a nurse. Any one who possesses these simple bits of skill can do all that is necessary for the physical care of the sick poor in their homes, unless continuous attendance upon the patient is necessary. Such attendance is not within the province of the social worker. But in the technical procedures just described it is all the more important that she be expert, because such skill makes her a welcome visitor and a trusted adviser outside the field of medicine. Because she has given relief by dressing a wound, curing a skin disease, or applying a poultice, she will be listened to with liking and with confidence when, later, she comes to give advice in economic, educational, or moral difficulties.
History-taking concerns the social assistant especially because history-taking is one of the things one does, if one is wise, in any matter in which one is trying to help a human being. Even if you were concerned to help not a stranger, but a member of your own family, still you would need a story or history of the person's life whether you wrote it down or not.
In our attempts to be of use to people in their misfortunes, there are two very common and quite opposite points of view (roughly the right and the wrong), which I call (a) the "historic" and (b) the "catastrophic," the accidental, or the emergency point of view.
Confronted with people's troubles, whether physical or mental or spiritual, we are tempted, and above all they are tempted to regard the sickness, the poverty, or the sorrow in the light of an emergency, an accident, and therefore as something to be treated at once and by means which have little to do with the past and the future. On the other hand, the standpoint of science and philosophy, and of any one who has labored long in the field of social work with[Pg 29] or without science or philosophy, is the point of view of history. This is the habit of mind which makes us believe that a supposed "accident" belongs in a long sequence, a long chain of events, so that it is impossible to understand or to help it without knowledge, as extensive as our time and our wisdom will allow, of that whole chain.
Consider a few examples which contrast these two points of view. When a boy is brought into court for stealing, it is almost always his attempt, and the attempt of those who defend him, to show that such a thing has never happened in his life before; he "just happened to steal." But as we inquire more closely into the facts, we almost always find that this is a fundamentally untrue statement of the case. For the offence which brought him into court is almost never the first offence. He has always stolen before. On the present occasion he was a member of a boy's gang; it was not in the least accidental that he got into that group of boys. As we search back in his history, and perhaps into his father's history, we find reasons why he is what he is now. Again, we are trying to help some wayward girl who has taken an immoral step. We are told what a wholly unforeseeable accident it was that got her into her trouble. But if we can get a good picture of her past, we find that we could have traced the tendency to weakness of this kind from the time she was born.
So it is in medical matters. Emergencies are rare. I remember being called out of a sound sleep one[Pg 30] night to go "as quickly as possible" to see a man who had discovered a lump upon his breast bone. He was quite sure that the swelling had appeared since the time when he went to bed. It was then one o'clock in the morning, and he had gone to bed at eleven. Well, I found a slight bony irregularity in his breast bone which doubtless had been there about forty-five years, as he was forty-six years old. He did not pretend that it hurt him, and did not undertake to show that he was ill in any other way. But this lump had come and naturally he wanted help at once.
The great importance of the contrast between the historic and the catastrophic points of view is, in the first place, that one way is on the whole right and the other on the whole wrong; but still more, that the patients whom we are going to deal with, and all the unfortunate or needy people whom the social assistant tries to help, are very fond of the wrong point of view and hang to it extraordinarily. It is the natural first impression of any untrained person that his troubles "simply happen" without any explanation that he knows. So that we have to start at once to tear down a structure of innocent and lifelong belief on the part of the patient, that troubles come suddenly and by accident. We have to disillusion him, a process which naturally he does not take to particularly pleasantly.
Our task in a dispensary is the same. The patient almost always starts with the catastrophic point of[Pg 31] view, and can only be very gradually engineered into the other. And yet our work in relation to public health is largely to be summed up as finding out how,—that is by what history, through what chain of events, people come to be sick. Repetition and extension of disease can be checked only in case we succeed in finding such clues. Hence our labors to change people's point of view in this particular respect are as worth while as anything we can do, and we must not be discouraged by the fact that, week after week and year after year, we come up against the same difficulties, the same conviction, that troubles "just come" and have no cause.
I have said that the historic prejudice is essentially right and the catastrophic prejudice essentially wrong. Of course, there are exceptions. A man may be run over in the street for reasons that we cannot discover to be connected in any possible way with his previous history; a man gets a burn, gets a broken leg, is hit by a missile in an air raid over London or Paris, in ways that are essentially catastrophic. And yet even in the field of accidents, industrial accidents for instance, the more we study, the more we find that injuries are not wholly accidental. The whole of science is the attempt to prove that nothing is an accident, that everything comes out of previous causes. The percentage of accident in the so-called "accidental" injuries decreases as we study industrial accidents. (a) They happen at certain hours of the day more than at other hours of[Pg 32] the day: if they were really accidental this would not be so. (b) They happen on certain days of the week, especially Mondays, for obvious reasons. (c) They happen especially to greenhorns, to the newcomers, who have not learned how to avoid them. One of the expenses incidental to hiring new help is the expense of accidents. Thus these events turn out to have a good deal of law and reason, a good deal in the history of the individual (alcoholism?), and the nature of the industrial process (speeding up?) which helps to explain them. By eliminating such causative factors, we may prevent some accidents.
The remedies that we apply fit the type of trouble; in so far as the trouble is accidental or catastrophic, the remedy is mechanical; in so far as the thing is historical and continuous, the remedy cannot be mechanical. When a man breaks his leg we put on a splint; that is mechanical. But if he is in a low state of health and the fracture won't unite, we have to do something non-mechanical, physiological, psychological. We may have to get him into a different state of nutrition or even into a better state of mind before his tissues will heal.
Our job, then, in taking histories—that is, in finding out how things happen that lead up to disease or misfortune—should begin by writing down the thing for which the patient comes—headache, cough, emaciation, poverty, desertion, unemployment. This is the "presenting symptom"; it should always be[Pg 33] the first thing written down in our history, not in terms of medical diagnosis such as asthma or anemia, but in the form of a complaint. Our attempt is first to put that down, to get a starting-point, and then to weave that into a chain of evidence which we call a history. That history makes it possible to make a diagnosis and to plan treatment.
But the particular event, the particular complaint for which the patient comes to us, is woven not merely into one chain of evidence, but into several. Let us carry out the metaphor of the chain. We must imagine many chains woven into one another like the chain-armor of the mediæval knight. Each link is a fact. But many chains of facts are interwoven in the history of one single patient. First there is the chain of medical evidence, the links (or symptoms) leading up to a diagnosis; second, the chain of social evidence, which we try to classify on our social history card. Third, we must trace the links in the chain of relationship with other people, other members of the family, with friends and fellow workers or schoolmates. Finally, the chain of heredity, of which we cannot make much at present except in relation to tuberculosis and mental disease or mental deficiency. But these studies of heredity in its bearing on character are going to be more important as the science of social work develops.
Our first attempt, then, after determining the[Pg 34] "presenting symptom," is to find out by a series of questions how this symptom is linked up into a tissue composed of many chains of facts. Our next task which is usually difficult, and frequently impossible, is to find out why this great tissue of evidence issues just now in one particular "presenting symptom." Why did the patient come to us to-day? This question is often impossible to answer because the patient does not know, though he may think he knows. Nevertheless, the social worker must try to find out. Often it is not until we have known and liked a person for days or weeks that we find out why he came to us at this particular time. Yet the answer to this question may be the most important thing that we can find out. For two reasons it is important; first, because it furnishes the clue to all our later investigation and assistance in this case; secondly, because it may show that the individual's complaints are not of any significance at all.
I can illustrate this by a case studied at the Massachusetts General Hospital in Boston. We looked up a series of patients at their homes in order to find out if we had really been of any service. The cases were not selected, but were taken from our files in numerical order. Among others we visited a lady whose malady had been diagnosed as "sacro-iliac strain." She had been given a prescription for a belt. We wanted to find out whether she had ever bought the belt and whether it had helped her. After some difficulty the visitor finally got the following details:[Pg 35] The lady had come from a city twenty miles distant from Boston. She had taken an early morning train, and could not get back to her home the same night. Hence she could not soon make another trip like that. She came to have her eyes examined. Now it happened that we had no eye clinic at the hospital at that time. But the lady had heard a great deal about the hospital and its efficiency. She was determined not to go home without having got something out of the hospital. So when she was told at the Admission Desk that she could get no treatment for diseases of the eye, she wandered into the medical clinic, trying to remember or imagine some symptoms for the relief of which she could be admitted to the clinic. Finally she managed to get out some sort of a story about a pain in her back; she was referred to the orthopedic division; there a diagnosis of sacro-iliac disease was made and a belt was advised. When she got home, of course, she laughed at the idea of buying a costly belt.
Now, if we could have found out in the beginning why she came to the hospital, we might have saved a good deal of bother for a good many people. It is astonishing how many patients turn out to have as little reason for coming now as this lady did. One of the things that shows the arbitrariness of choice in selecting a time for visiting the hospital, is the striking diminution in the number of patients in the week before Christmas. That suggests that there are many postponable visits. Or again, patients may[Pg 36] come merely because somebody else from the same neighborhood is coming.
As the history-taker traces out the symptoms of the patient's illness after finding an answer to this first question, Why to-day? two opposite habits of mind must be employed, one passive, the other active. We must be sure that the patient shall feel that he has had a good listener, that his troubles have really been appreciated. But if we are constantly putting in questions, as we certainly must later, the patient does not feel that he has been listened to. We desire first of all to get his own story in his own words, passively. We may not necessarily write down a single word of it. But I have found that the patient's own way of expressing the nature of his troubles is often important and characteristic. It helps to prevent our histories from looking too much alike, which is their commonest fault. Hence we should get into them somewhere a phrase or several phrases reported passively in the patient's own words; if possible a phrase in which he describes his "presenting symptom," the thing of which he chiefly complains.
But the second stage in the process of taking a patient's history is the most important. In this part we should be active, not passive. We must attack our task with a tool in our hand, a mental tool fitted to rake out of the mass of confused ideas in his mind[Pg 37] certain significant facts. That rake is a logical schedule of questions which you use upon him actively, not passively, and by using which you get answers either negative or positive. Whenever you think well, you think with a schedule of that kind in your mind. If you pack a trunk well, you pack it using a list, a schedule of the things that ought to go into that trunk. Our printed social face-card helps us to think and question with a schedule before us, to think in an orderly way, without forgetting our items, and thus to select what we need out of the mass of disorderly facts in the patient's memory.
In the second phase of history-taking, then, which begins after we have listened appreciatively but quietly to the patient's own version—usually catastrophic and full of fanciful theories—we lead him by questions (but not by "leading questions") along the paths which will open up a full view of the trouble, medical or social, which has been suggested to us by the patient's first statements. Suppose, for instance, one happened to know of an extraordinarily rare but curable disease, one symptom of which the patient had mentioned, "My hair comes out by handfuls." One would go on to ask, "Do you feel warmer or colder than usual this winter?" Then, "The expression of your face is not notably changed, is it, so that your friends comment on it?" "Is your skin drier or moister than usual?" "Does your tongue bother you in any way?" "Is your mind more or less active than usual?" Thus one would confirm[Pg 38] or refute the suggestion of the disease called myxœdema, a suggestion which was given to us by the patient's first complaint—rapid loss of hair. Given one symptom in a known group, one can trace out the others as the anatomist who finds a single fishbone may be able to reconstruct imaginatively the whole fish.
I said just now that we must not ask "leading questions." If we do, we can make a patient of a very suggestible type of mind say anything. If you ask him whether he has any symptom whatsoever he may obligingly say "yes." The way to avoid this is to put our questions in the negative: "You have no headache at all, have you?" "You do not cough?" "You never spit blood?" By these negatives we can get at the positive symptoms if they are present.
Schedules of questions to be used in history-taking may be medical or social. Some of the social question-lists are suggested in later chapters of this book. A masterly account of social questioning is contained in Miss Mary E. Richmond's "Social Diagnosis" (published by the Survey Associates, New York, 1917).
I wish now to illustrate the methods to be used by social workers in questioning patients about their symptoms so as to assist the doctor in his diagnosis.
Pain: How long? For a day, a month, a year, six years? Very chronic pains are seldom serious but seldom curable. Headache that has lasted years either has no cause known to medical science, or else[Pg 39] it means neurasthenia. In either event it is apt to be stubborn. A headache that has lasted only a day, and did not occur before, cannot possibly be due to migraine. This suggests how the length of time that a pain has lasted is very important in diagnosis. The patient will often say, "I have always had it"; but to this we should oppose a pretty strong cross-examination. The patient usually means that he has had it off and on throughout an indefinite period. We ask him then, "When did you first have it?" and then, "How much of the time—half the time, a quarter of the time, for one day a week or one day a month?"
Pain: Where? Patients rarely come to a doctor for a single point. But pain in several points is never as significant as pain in one point. One cannot learn much from scattered pains in relation to what ails the patient and what to do for him.
Pain: How bad? That is a very difficult question to get the answer to. There is no thermometer or measure for pain. I suppose every doctor has wished many times that he had one. But there are certain rough measures which are of some use in judging how bad a pain is. (1.) We ask, "Does it compel you to lose sleep?" Some headaches may be pretty severe and yet a person sleep despite the pain. It may link itself up with a dulling of consciousness leading to sleep. But most pains and even most headaches that do not keep a person awake are not as bad as those that do. (2.) We ask, "Does it prevent work?" Any[Pg 40] one can see all sorts of limitations to the use of that criterion. A man with a rugged type of mind will work with a pain that another weaker man will give up to. Yet the question does bring out evidence of some value.
(3.) Another criterion, more subtle and not quite so useful, is this, "Do you feel the pain more when you are quiet or when you are moving about?" The pains due to organic diseases are generally worse when one moves; while the functional type of pains are apt to be better when one moves about. One forgets it. Quite often patients are very lucid and candid about this.
Pain: How aggravated? How relieved? (a) A pain may be aggravated by position—for example, when the patient is on his feet—or worse when he is lying down—a headache, for instance. Most abdominal pains are worse when the patient is on his feet. (b) A pain may be aggravated by motion. Most of the surgical injuries, sprains, strains, tears of muscle or ligament, and fractures of bones are naturally made worse by motion. Pain may be aggravated by certain particular motions, as is the case with some of the innumerable pains in the back. Lumbago is a pain characteristically described as one that comes when the patient tries to lace his boots. Especially when he tries to get up from that position, the pain is intolerable. Pains in the chest are often worse on deep breathing—pleuritic pains, for example. But other thoracic pains may also be made worse by deep[Pg 41] breathing. (c) Pain may be aggravated by the taking of food, or by movements of the bowels.
Pain may also be relieved in any of these ways. The most important thing that one can know about a stomach pain is that it is relieved by food. The majority of all stomach pains are aggravated by food. Pains are also relieved by heat or cold or by drugs or by rest. But those are not very important points. They may be important in relation to what we do to help the patient, but not in relation to diagnosis. Some pains, whatever their cause, are relieved by cold, more by heat, and most are also relieved by rest.
Next to pain, Cough is the symptom, especially in the colder months of the year, that we have most to deal with. The question How long? is vastly the most important one about cough. One can also measure its severity by the question, "Does it keep you awake?" and to some extent by the question, "Does it prevent work?" More important is the question, "Is it dry or productive of sputum?" The patient's description of his sputa in gross, without any microscopic examination, is also of a good deal of use. There are usually three things a patient can tell us about it: either it is yellow, or it is white, or it is bloody. There are two other important questions about bloody sputa. Unless one gets these answered, the mere fact of spitting blood is not important. We must know whether there are merely streaks of blood[Pg 42] which one often sees in the sputa of anybody who coughs hard, are of no importance, and have nothing to do with tuberculosis. But if, in contrast with this, we can really establish evidence of the spitting of blood in quantity, we have almost proved a diagnosis of tuberculosis. In ninety-nine cases out of one hundred the spitting of blood in quantity means tuberculosis. "In quantity" means a cupful or thereabouts of pure blood. If the doctor does not find tuberculosis after that he should nevertheless assume it, for it is almost always there. I should pay no attention to negative physical finding in such a case.
The next point to ask about is whether the patient's breathing is wheezy. When a horse has become broken-winded we can hear his breathing in the street as he comes along. He has become emphysematous. We find this wheezing respiration in emphysema, asthma, and bronchitis, which are diseases important for us to distinguish from tuberculosis; we almost never get it in tuberculosis.
If the patient complains of dyspnea—difficult, rapid breathing, "short breath" as we say—we shall ask about œdema or swelling of any part, especially of the legs.
In every patient who has a cough we are concerned primarily with the diagnosis of one disease, that is, tuberculosis, its presence or absence. Hence every patient who coughs should be questioned about the other symptoms of tuberculosis and especially about emaciation. A man with a chronic bronchitis or [Pg 43]emphysema does not lose much flesh; he does not become emaciated. A person does not become thin from throat trouble. Hence emaciation, especially recent, is a helpful guide to the doctor in making up his mind. Fever we investigate for the same reason. The only disease that often causes cough and fever during a long period is tuberculosis. Unfortunately the patient's statement about fever is usually unreliable. We can believe most of what he says on the rest of these points. But he does not know whether he has fever or not.
In women we must ask also about the monthly sickness, because it is suppressed in cases of moderately advanced tuberculosis. Nephritis, anemia, heart trouble and emotional disturbances may have that same effect. It is a measure of the degree of disease, not its type.
For the purpose of dispensary consultations I do not think we should take any family histories except when we suspect tuberculosis. But when the history leads us to think that the person may have tuberculosis, the social worker can help the doctor by asking the patient questions about the possibility of the same disease in mother, father, or others who are in contact with the patient—grandfather, grandmother, or other relatives or friends living in the same house. We believe less and less in the heredity of tuberculosis, more and more in infection by contact. If separated from a tuberculous father or mother in early infancy we believe that the child[Pg 44] does not acquire tuberculosis. But the main mode of infection is by association in the same house, over a prolonged period, with people who have tuberculosis. Often the patients do not know or will not confess that anybody in the family now has tuberculosis or has died of it. But if we can establish the fact that one of the patient's family has died after having a cough for many years, that he grew very weak, and spit blood, we have established the diagnosis without the name. Not the degree of relationship to a tuberculous patient, but the amount of time spent in the same house with a tuberculous individual—what we call the degree of "exposure" to tuberculosis—is the important thing.
After getting the patient's present symptoms, one should ask, "Were you ever sick previous to this illness? If so, what troubles have you had?" That is of use in clearing up the limits or boundaries of the present illness. The sicknesses which the patient says he has had are not of very much use to us in diagnosis because we cannot get true answers. The patient's diagnoses or his doctor's are apt to be vague or meaningless. But the questions about the patient's past history tend to make him more clear as to the date when his present illness began. Hence his answers on these points should be written down very briefly, a word or two only about each, and usually in the words used by the patient.
In our written histories in hospitals we usually take a considerable body of notes about the patient's habits. I do not advise this for social workers. But there are certain routine questions which should be asked of all patients concerning their appetite, bowels, sleep, weight, and work. The answers should be recorded in a separate paragraph, at the end of the history.
What is printed here is meant to give a sample, not a full account, of medical-history-taking. Competence in this field takes long practice. Nevertheless the intelligent social worker can learn in a few weeks to be of great assistance to the doctor by taking either in the dispensary or in the home such histories as I have sketched.
In social-history-taking there is no single order or schedule of questions agreed upon by all social workers. But there should be some order and system determined partly by the personality of the worker and partly by the nature of the trouble. If poverty or destitution is the presenting symptom, one must find out the items in the family budget, the figures of income and outgo, paying especial attention as in medical histories to the question, "How long?" How long have you paid that rent, earned that wage, been without a job, taken boarders, been in debt?
Is sickness, childbirth, alcoholism, injury a factor?
Is there any family history of tuberculosis, pleurisy, insanity, epilepsy, feeble-mindedness? Of [Pg 46]miscarriages or of "scrofulous" children and "blood diseases"?
What previous hard times? What economic and moral high-water marks and low-water marks can we trace in the past history?
What relatives, friends, employers, doctors, teachers, neighbors, landlords, social agencies, public officials or records can be consulted for additional light on the person and his troubles?
From all these sources one arrives finally at an opinion on "what sort of person are we trying to help—what sort physically, mentally, and morally?" That is the central fact.
It should be clear from what I have said already that the work of the social assistant may have nothing to do with poverty. Her only business in visiting a family may be to assist the doctor in his diagnosis and treatment by bringing him additional facts about the nature, seriousness, or cause of the disease and about the means by which it may be combated.
But in many, perhaps most, of the families whom the social assistant attempts to befriend, there is a call for relief, for financial assistance, for money, food, coal, and clothes. This appeal like most medical appeals is apt to take the form of an emergency. Help (we are told over the telephone) is needed at once, or disaster will follow. The family is eager for immediate relief, not for a slow and painstaking investigation of the causes which have led up to the present state of things, or of the exact nature of their present troubles. They are like the sick in this respect. Prompt relief from pain is what the sick demand, not the tedious processes of questioning and examination. They want a remedy, a pain-killer, morphine or its equivalent.
But we all know the dangers of giving morphine for the relief of pain. It never cures a disease; it only stifles a symptom. It gives delicious ease; but the[Pg 48] need for its use soon recurs. Hence there is always danger that before long the patient will have to fight, not only the disease which originally caused him pain and made him call for morphine, but the morphine habit in addition. This is all familiar. But not every one realizes that the giving of money in case of poverty is as dangerous as the giving of morphine in sickness. Money like morphine satisfies an immediate need and hence is eagerly welcomed by the sufferer. But of money as of morphine it is true that a single dose soon makes the patient call for another, and often a larger dose; that it soon makes the patient dependent on this sort of relief, and so forms a dangerous habit. With the rarest exceptions, to give money or to give morphine does not cure. The state of things which produced the pain or the poverty is sure to recur. For (as I have said above) the patient's belief that his present troubles are an unforeseeable accident, a sudden catastrophe, is almost never true. The truth is that his pain or his poverty are but the last chapters in a long story produced by causes which can usually be traced out, and whose future action can often be foreseen. By giving money we are covering up a smouldering fire, not quenching it.
For economic bankruptcy or breakdown, like physical bankruptcy or breakdown, is generally the result of faulty organization in the system of income and expenditure. Physically a person breaks down because he has been spending more energy than he[Pg 49] can recoup by rest, food, and recreation. Economically he breaks down because his scale of expenses exceeds his regular income. Hence it gives but temporary relief to pay the bankrupt's debts, to cancel the sufferer's pain. The operation will soon have to be done over again unless some constructive plan for increasing his income or decreasing his expenditure can be worked out. Giving creates dependence because it atrophies industrial and moral initiative, just as a crutch or a splint causes muscles to waste. Powers unused atrophy. If we support a person, except temporarily, he will soon lose the power of self-support.
But the point of view impressed upon us by the sufferer himself is apt to be quite the opposite. What he wants is something immediate and temporary for the relief of something accidental. The beggar who meets us in the street has "accidentally" lost his purse and asks of us a small sum of money to reach his home. Often I have said to such an applicant, "Meet me at the railroad station half an hour before the train leaves for your home. I will buy you a ticket and see you on board." He never comes. This is an extreme instance and involves almost always a deliberate attempt to deceive us. In home visiting it is not like this. The sufferer does not usually intend to deceive. Nevertheless his misfortunes are pictured by him as accidental and temporary catastrophes, maiming a life which needs no general reconstruction. He is so sure of this that he is apt to force the idea upon us unless we are alert, bracing ourselves[Pg 50] to question it and to make sure that it is true. But actual experience has shown me and hundreds of others that this point of view is almost never true.
It is not chance that the family is just now poor. It is no emergency which we are summoned to meet. It could have been foreseen long before and it will certainly recur unless we can trace out its causes and prevent their acting as they have hitherto. Hence the detailed, prolonged, individual study of the family's economic state is necessary. One must find out, first of all, all the details of income and outgo. The family is likely to forget some of these, so that one must be ready to assist their memory.
Further, one must inquire carefully into possible sources of help from relations, friends, fellow members in some club or association, and so forth. For next to self-help the help from those naturally bound up with one is best. Compared with impersonal charity, it is less artificial. It is less destructive to the natural family relationships which it is always our ultimate ideal and our immediate job to maintain or to restore so far as possible. Whatever disturbs or threatens them is hostile to the social interests for which we labor.
Naturally one does not invoke the help even of family, friends, or fellow club members, unless it seems impossible for the individual, under the best plan that he and you can think out together, to get along without outside help. But if we are convinced that, for the present at any rate, this financial [Pg 51]self-maintenance is impossible, it is to securing help from those nearest to the sufferer that one should look with least regret. Gifts or loans from members of his family or from friends are more likely to be taken seriously by the recipient. He is less likely to feel (as he does with an impersonal agency or charity fund) that he can draw from a bottomless pit of money without making any one else the poorer. Moreover, when he takes money from his brother or the fellow member of some club, the pressure for regaining his economic balance is likely to be exerted from without him as well as from within. He feels the pressure of his debt and thereby is stimulated towards regaining his independence.
The sufferer's "catastrophic" point of view, which tends to isolate the present trouble from all its causes, to represent it as temporary and accidental, is related to his tendency to state that he has no friends, relations, or social connections through whom help could come to him. Without any deliberate attempt to deceive us, he quite naturally forgets some of his relations. He does not want to appeal to them. Hence they fall into the background of his mind, and are not easily recovered. When one finds them for him he is apt to say, "I did not think of him because I am not on speaking terms with him"; or, "I would not on any account take money from her, or allow you to ask her to help me." But such a sufferer may very properly be asked, "Why is it that you are willing to take money from me, a[Pg 52] stranger, or from this impersonal charitable agency, when you are not willing to call upon your own relations nor even to let them know that you are in trouble? You are concealing it from them, are you not? Is there really any good reason for this? Will it not be easier for you, as well as for them, that they should know at once? Are you not really storing up trouble for yourself, postponing the evil day which, when it comes, will be worse than anything which you would have to bear at present?"
Of course, in all such advice we intend to say nothing that we should not wish to have said to ourselves. The social worker tries to treat people always as she would wish to be treated. But one cannot always avoid giving pain or even estrangement. Because such interviews are necessarily difficult and may result in disaster to the relationship that we are trying to establish, they should be postponed if possible until we have already established in other ways a friendly understanding, a structure of friendship which will bear the strain of penetrating inquiries such as these economic matters necessarily entail.
I have said that the first guide to helpful economic relief is a realization of its danger. The next is awareness of the advantages of self-help and the truth that next to self-help, assistance from those naturally and nearly related to one is best.
The third principle, by following which we may hope to do the greatest good and run the least risk of[Pg 53] harm in our giving, is this: never give hastily except in extraordinarily rare emergencies such as acute hunger or exposure to the elements. In all other cases give in accordance with a plan worked out as carefully as may be, whereby we are confident that our giving can be temporary. Sometimes we can arrange that it shall come to an end automatically. That usually means that we arrange for a loan rather than a gift, with repayment either by instalments or in lump sum upon a definite date.
(a) Loans. It is in the hope of rendering service by these means that there have been organized philanthropic loan associations which lend money at low rates of interest and sometimes without interest or upon security which the commercial loan companies would not accept. The sufferer with whom we are dealing may know nothing of the existence of such agencies. If so, to connect him with one of them, to help in furnishing the security necessary to negotiate a loan, may perhaps be the best way in which we can help. Or one may buy some rather expensive article such as a piece of medical apparatus, with the clear understanding that we are to be repaid in instalments or at weekly intervals.
(b) Tools of a trade. Another example of the kind of giving which comes to an end and does not tend to form a habit like the morphine habit, is exemplified when we buy a man the necessary tools of his trade, or the stock and furniture necessary to start a store. The belief on which we rest in such cases is that after[Pg 54] the initial act of acceptance, after an initial period of dependence, the individual will become self-supporting and independent.
(c) Furniture. Or, again, one may give or loan a cooking-stove, so that the sufferer may no longer have to eat at restaurants, or some furniture in order that he may get the benefit of the lower rent to be had when one hires an unfurnished room. In all these cases the ideal thing is to arrange for repayment in small instalments. Failing this we try to think out a plan such that after the original expenditure the sufferer will be able to go on independently.
(d) Aid in illness. A fourth example of temporary interference in the form of financial aid, is a gift or loan of money to tide a person over an illness, to make his convalescence complete or to rest him when he is dangerously tired. Usually such aid can be rendered through services or institutions (nurses, hospitals, convalescent homes) which do not involve giving money outright.
(e) Aid during unemployment. A fifth good reason for giving money or other forms of relief temporarily is to tide the sufferer over a period of unemployment, during which he is actively looking for work or for better work than he now has. Sometimes we can assist him in this search. But there is danger in this. A man is less likely to keep a job that some one else finds for him than one which he finds for himself. Still, we may help him without harming him in case we can give him facts, names, positions, [Pg 55]employment agencies by means of which he may secure employment, he himself taking the active part in securing the job. Information, which is what we here furnish, is one of the least dangerous of gifts.
In all these cases the principle is like that whereby we do surgery. Surgery is a temporary injury to the body done with the expectation of ultimate good, a temporary interference of outside powers with the natural self-maintenance of the organism, in order that those functions may ultimately go on not only independently, but more satisfactorily than before. The surgery may kill the patient, or leave him worse than he was before. But our reasonable expectation is (in case our surgery is good) that his health—that is, the capacity of his body to maintain itself, or develop itself—will be improved. So in economic surgery we foresee a speedy end to the need for aid. The person is to be put upon his feet by our aid; our services can soon be dispensed with. The need will not recur. It is not chronic. It was not his fault and therefore is not likely to return upon him soon because of continuance of the same defect.
Obviously one must try to make clear—or, still better, try to have it clear without explanation, understood because of our previously established relation of trust, confidence, and affection—that it is not because of parsimony or close-fistedness that we are refusing to give quickly, constantly, and without inquiry. Medical analogies must constantly guide us and be in the minds of those whom we try to help.[Pg 56] We refuse money, as we refuse morphine, for the patient's good. We try to make our giving of money temporary and self-checking, for the same reason that we try never to begin giving morphine unless we can foresee a speedy termination of it, a speedy cessation of the need for it, as we do when we give it in gall-stone colic or acute diarrhea, or just before a surgical operation. If morphine were a possession of the doctor's, as money is a possession of the visitor or those whom she represents, then the doctor might often seem stingy, cruel, selfish in his refusal to give it. We must make it clear if we can that our hesitations, limitations, or refusals in relation to money have no more connection with our own control over that money, our own enjoyment of it, our own sense that we have any right to it, than the doctor's refusal to give morphine rests upon his desiring to take the morphine himself instead of giving it.
All this is difficult to make clear, and it is chiefly for this reason that I have repeatedly insisted that the financial approach, the financial ground for an entente cordiale, should not be used early in our dealings with the sufferer, but should if possible be postponed until, through medical service and personal intimacy, something approaching true friendship has been established.
It should be clear from what I have said that our judgments about giving financial aid can be sound, can result in doing good without harm or (as in[Pg 57] surgery) good with a small element of harm, only in case they are the fruit of detailed, prolonged, individual study. It cannot be a wholesale matter. It cannot be done in exactly the same way in the case of any two individuals.
Let us stop to realize for a moment how arduous, how bold a task we have undertaken. We hope to construct a person's economic future better than he can construct it himself. We hope to see what the individual himself, despite the vividness and pressure of his immediate need, has not been able to see for himself—namely, how he can get himself out of his financial difficulties. We who do not wear the shoe are venturing to say where it pinches and how the pressure may be relieved, and to know about this better than the sufferer who feels the pressure in his own person and longs for its relief as it is hardly possible for any one else to desire it. It is almost as if we were trying to use his mind for him. It must not be that. But if it is not to be that, we must be sure that our aid is given through stimulating the individual to think for himself. "What do you think," we must constantly be asking him, "is the best way out of this our difficulty?" He must feel that we know it to be our difficulty as well as his, that we are not looking on with the cold gaze of an outsider, that we suffer in his suffering, and still that it is at last his, and that with all our best efforts we can only contribute a little to what must be for the most part his own reconstruction, a reconstruction like that which the[Pg 58] body performs when it heals a wound which the surgeon or the physician can only encourage a little towards its natural healing.
Without being impudent enough to attempt to use the sufferer's mind for him, to force our wills upon him, to take his burdens off his shoulders, to fill his place or to assume his responsibilities, we must try to help him in all these respects, largely by the kind of sympathy which stimulates, the kind of affection which encourages, the affection which changes useless brooding, ineffectual worrying, destructive grieving, into their opposites. We can help him to think by suggesting resources, possibilities that he does not know or that he has forgotten, by furnishing new material on which his mind may work, by helping to generate the power, the hope, the concentration, the prolongation of thought out of which new solutions may be born. He must really think of something new. He must really invent something, if he is to get upon his feet and become independent once more. Ordinarily necessity is the mother of invention. We pull ourselves out of our difficulties when we finally realize that we must because disaster is otherwise imminent. But such pressure of necessity as would generate inventiveness in one person, may generate only despair in another. It is to avoid this tragedy, it is to make fruitful what were otherwise fruitless, that we hope to warm the sufferer into better life. We hope to rouse in him, by affection or by the stimulus of new facts (perhaps),[Pg 59] the courage necessary to see his situation afresh and to reshape it.
Because we are comfortable where he is suffering, because we have free power of thought whereas his mind is numb and cramped, we may be able to think of some possibilities, some changes, some sources of hopefulness which he could not even imagine. He cannot take them from us ready-made. If he does they will be useless to him. But if we have reached the central fire of his life, if we have stimulated not this faculty or that, but the centre of his personality, then by the grace of God we may be able to do with him what he alone could not do.
A part of the economic life of our patients, aside from the food and clothes for which they may most urgently ask our aid, is their housing.
(a) Is it hygienic?
(b) Is it as inexpensive as can be obtained with due consideration of health, decency, distance from work, from friends, from amusements?
(c) Is it large enough to safeguard the decencies of family life?
The last of these questions is the most important of all.
It should be among the medical duties of the visitor to investigate the hygienic aspects of the home in order to explain them to the doctor, who can then[Pg 60] include them among the facts on which his diagnosis, prognosis, and treatment are based. The social worker may then try to carry out such improvements in housing as the combined judgment of the doctor and the social worker suggests. More important than medicines, often, is the provision for proper warmth and proper ventilation of the patient's rooms during the day and especially at night. Darkness, dirt, poor ventilation, favor the growth of germs, vermin, parasites of all sorts. They also depress the vigor and power of the human organism to resist disease. Doctors and social workers cannot hold Utopian views in matters of housing, but must content themselves with trying to secure something a little better than they find in the worst of the patient's lodgings, especially when these lodgings represent conditions below the family's own standard of living at some previous time. People adapt themselves wonderfully to bad hygienic conditions, and once so adapted, they may be able to preserve their health for a long period. But if then a family is suddenly forced to crowd itself into smaller, darker, dirtier, noisier quarters than it has been used to, or if a family group increases its numbers within the same quarters, the adaptive powers of the human organism may be overstrained and break down.
It is against these conditions especially that the social worker and the doctor should labor. Housing problems are among the most difficult of all that confront society. Yet we should pledge ourselves to[Pg 61] attempt some improvement, not disdaining slight gains because we are enamored of distant Utopias.
Sometimes people are living beyond their means, are accepting bad quarters at high prices when they could get as good or better quarters for less money in some less crowded and popular district. Human beings have a strong tendency to stay wherever they find themselves, to settle down by chance and resent any suggestion of change even for their own greater comfort. After a few months any place soon comes to have the attractions of home merely because we have been there. Hence we stick in the same place, though we may know that it is chance and not choice or necessity that has put us there. Under these conditions a social worker may do real service by her greater knowledge of other lodgings at lower prices, or (what is essentially the same thing) better lodgings for the same price now paid. If the social worker is familiar, as she should be, with the lodging conditions in the neighborhood in which she works, she may be able to give a patient facts about lodgings which were either unknown to him, or more probably unrealized, because he has never seen them. Our mental horizon becomes restricted. Any one who enlarges it by presenting new and helpful possibilities serves us well.
So far I have spoken of the housing question mostly from the standpoint of health or cheapness, but, as I have already suggested, the moral aspects of the problem are still more important. It is [Pg 62]difficult, for many impossible, to preserve personal decency and to keep family morality at a proper level, when adults and grown-up children are forced to sleep in the same room. Lifelong injuries to body and soul may be forced upon innocent children in this way. Nothing can be more important than this. We must remember, however, that custom and previous habits play a vast part here. One race or one set of people may have so adjusted themselves as to preserve decency under conditions impossible for another. We cannot generalize. We must know the particular people with whom we are dealing, and we must know their previous habits and standards in case they have shifted their lodging or increased the number of persons in a room within a short time, as is so frequently the case.
Work and the conditions of work are among the most important and the most difficult of the economic problems in which a social assistant may find herself inevitably involved. These concern the patient's trade, the physical and moral conditions under which he practises it, his fitness or unfitness for it, the wages he receives, the future possibilities of advancement in pay and type of work which it offers. In all of these problems the social worker can sometimes help a little because of her greater freedom of mobility, mental and physical. She is not tied to her task as blindingly, as deafeningly, as the[Pg 63] manual worker is. She may know more or be able to find out more as to labor markets, as to other, possibly better, positions, shops, employers. She may be able to see, better than the worker himself, his fitness or unfitness for the work he is doing. She may be able to realize better than he that his trade presents an impasse, has in it no possibilities of development, personal or financial. She may realize better than he the bad effects of his work upon health or morality. In all these respects she may be able to give the safest, and in some ways the most satisfactory, of all help,—namely information.
I do not underestimate the difficulties of such help. It is not easy to know more about a man's business than he does. Yet if the social worker's education, her health, her circle of acquaintances, is greater than that of the wage-worker, she may really be of some assistance to him even in the field that is more specially his own and that she can understand but superficially. It is for this reason among others that the social worker cannot be too broadly educated, too fresh physically, too vigorous in her powers of thought and observation, too widely acquainted in her community.
Among the problems growing out of the basal economic needs of which I have just spoken, are others with which I cannot here deal adequately. Such are:
(a) The problem of industrial hygiene and industrial disease.
(b) The problems of school hygiene and school medicine, since school life is the industrial life of the child, who even receives wages for going to school in some communities.
(c) The industrial and psychological problems of those who are maimed by accident, war, or disease.
(d) The problem of industrial insurance and health insurance.
All of these questions involve matters of State action, legislative control, and economic reform with which I do not wish to deal. But I wish to make it clear, in closing this chapter, that the social worker as a citizen is as much interested in these hopes for radical economic reforms as any one else can be, though she does not regard them as her special business.
Preventive medicine and the daily fight against individual cases of disease which we hope some day to prevent—these two activities go on side by side, each helping the other. The social worker corresponds to the private practitioner of medicine; the economic reformer and discoverer corresponds to the laboratory student of preventive medicine or to the public health official. In social work as in medicine the case worker should bring to the inventor and reformer new facts and illustrations suggestive of the evils to be reformed or possibly of the ways of combating them. And in the difficult, often disappointing, task of trying to help individuals, the case worker will also take part of his inspiration from the[Pg 65] hopes and ideals of a better economic order sketched for him by the legislative reformer. The method and technique of economic investigation is complex and difficult. For a masterly treatment of this and all other aspects of social diagnosis Miss Mary E. Richmond's epoch-making book on "Social Diagnosis" should be consulted. (Published by the Survey Associates in New York City.)
Ever since the days of Charcot, France has been the land of medical psychology. France has never failed, as other countries have failed, to take full account of the mental factors, the mental causes and results in disease.
In America, on the other hand, the conspicuous disregard of medical psychology by physicians has led to widespread and serious revolt on the part of the public. Our physicians have too often treated the patient as if he were a walking disease, a body without a mind. Medical psychology has been neglected in our medical schools and in the practice of our most successful clinicians. The result has been a revolt upon the part of the laity, expressed in the popularity of the heretical healing cults such as Christian Science and New Thought. These unscientific and unchristian organizations illustrate an error opposite to that of the physicians, but no greater in degree. Indeed, I think that our physicians are more to be blamed than the leaders of these irrational cults, because our physicians having received a scientific training ought to be more thorough, more unprejudiced, more devoted to the truth, and therefore less inclined to shut their eyes to a huge body of facts. The physician often shuts[Pg 67] his eyes to the existence of the mind as a cause of disease. The Christian Scientist shuts his eyes to the existence of the body as a cause of disease. Both are equally and disastrously wrong. But the medical profession is on the whole more to blame, because they ought to know better, whereas the heretical healing cults have grown up among uneducated men who could not be expected to avoid the sort of narrowness and prejudice from which liberal education ought to free us.
The situation in America, then, is very different and on the whole worse than in France. There, scientific men, educated physicians have taken the leadership in the field of medical psychology. In America it has been left for ignorant enthusiasts, devoid of any scientific training or breadth of culture, to press upon our attention the neglected elements of medical practice, and to lead a revolt against the medical profession, an anti-scientific revolution which numbers its adherents by millions. But in neither country has our established knowledge of the mental elements of disease been properly incorporated into medical practice, especially into the practice of dispensary physicians, and it is here that the social worker forms an essential link in the chain of effective action. Let me describe more completely what I mean by the mental element in disease.
I refer not merely to the so-called nervous diseases, the neuroses and psychoses, the myriad forms of nervousness without recognizable basis in organic[Pg 68] disease, but also to the mental complications and results of serious organic diseases such as tuberculosis, arteriosclerosis, and surgical injuries. The classical studies of Charcot, Pierre Janet, and others have made clear to the whole world the existence of a body of diseases in which the mental functions are obviously deranged while still the patient is not insane in any legal sense, and does not show on physical examination any evidence of gross organic disease. Neurasthenia, psychasthenia, hysteria, are among the more common types marked out by the studies of great psychologists and clinicians. Little or nothing has been added by the studies of German, American, and English physicians to our knowledge of these diseases. But throughout the history and development of France's leadership in the study of these diseases, one cannot help noticing that interest is concentrated largely upon diagnosis; comparatively little attention is paid to treatment. The great leaders have not been extensively followed. Their suggestions have not been carried out on a large scale nor followed sufficiently into the field of practical therapeutics.
Especially is this true in the field of visceral neuroses or nervous symptoms referred by the patient to one or another organ—the stomach, the pelvic organs, the bowels—in which nevertheless no evidence of disease can be found. In these diseases English, French, and American physicians alike persist for the most part in humoring and soothing the[Pg 69] patient by the administration of remedies known to have no real influence upon disease and designed chiefly to make the patient feel that something is being done for him. This is superficial treatment. It makes no attempt to attack the determining causes of the disease. Whether or not there are any psychogenic diseases, whether or not purely psychical events can be proved to produce the group of symptoms known as neurasthenia, psychasthenia, or hysteria, or whether there are physical causes contributing to produce the symptoms, this at any rate may be said with confidence: that if we are to root out the patient's trouble, if we are to bring about anything approaching a radical cure, we must attack the mental symptoms directly and upon their own grounds, that is, by mental means, chiefly by reëducation. The mental element in these diseases is at any rate the most vulnerable point of attack. It is here that we can most profitably exert therapeutic pressure.
Even in organic disease, such as tuberculosis or arteriosclerosis, it may still be true that we can help the patient chiefly through psychotherapy. There may be little that we can do for his arteries or his lungs, and indeed the incurable destruction which has gone on in these organs may not at the time that we are treating the patient be producing any symptoms. All his symptoms just now may depend upon mental states which we can quite easily influence and thereby cure him of all that at present torments[Pg 70] him, though we recognize that the organic malady remains untouched, unimproved. Many a case of tuberculosis suffers chiefly from his fears of the disease or from his discouragement. If we can rid him of his constant dread that the disease will advance or will injure others, if we can give him courage, the natural healing power of his tissues may be all that is needed to bring about the arrest of the disease. On the other hand, even an incipient case of pulmonary tuberculosis may go steadily on from bad to worse, because the patient is constantly fretting and worrying about his own condition, or about the present sufferings of his family.
I remember a case of very early tuberculosis, but recently established at the summit of one lung, but unfortunately occurring in a patient of very active temperament, prone to fume and worry the instant that he was taken away from his work. He was devoted to his family, but as soon as he was aware of his trouble, he could think of them only as doomed to be dragged down by the contagion of his own disease or by the poverty resulting from his own inactivity. Unfortunately, no proper study was made of this patient's malady. No account was taken of his character and temperament. The condition of his lung occupied the whole field of the physician's vision. The condition of that lung demanded for the patient isolation and complete rest in a sanatorium. This was prescribed and carried out. The patient remained in the sanatorium about two months, [Pg 71]fuming and worrying constantly. He then refused to stay any longer, left the institution against the advice of his physician, returned to his family, and died about two months later.
Now I think it is at least probable that had we studied the patient's mind as carefully as we studied his lung in this case, his life might have been saved. But the physician who made the diagnosis and prescribed the treatment could spend but a few minutes upon the case, which formed but one of many trooping past him in his consultation hour at the dispensary. He had no time for the prolonged, detailed, wearisome studies necessary to win this patient's confidence, to make him feel that he was wholly understood, and bring him to the point when he would let himself be reëducated upon the mental side and receive docilely the advice given him. This work should have been carried out by the right type of social worker. Such a visitor would no doubt have realized that one must compromise to a certain extent with the difficulties of the patient's temperament. One must adapt and modify the treatment suitable for the average case because this particular patient differs from many others in important respects.
In the first place, he must be made to understand the importance of a correct mental attitude for the cure of his disease, must be taught that his recovery depends to a considerable extent upon his own efforts at self-control and self-education. Next he must be[Pg 72] convinced that his family will be adequately cared for during his absence from work. Furthermore, the complete rest in bed which would probably be advisable for him if one had only the condition of his lung to consider, should probably in his case be modified owing to the fact that his mental state makes it impossible for him to rest when he is confined to bed. In such cases one has the outward appearances of repose but not the reality, one clings to the form but misses the substance. What one has prescribed is in reality enforced impatience, enforced restlessness, because one has put the patient under a régime where no result can be expected except impatient struggling against restraint. Such a patient should be allowed a certain amount of work, carefully chosen and supervised, so as not to exercise the larger muscles of the body and thus produce fever, but sufficient to occupy an active mind and to make the patient forget himself. To find such occupation is difficult, no doubt, but it is not impossible. I have seen it done. In the case which I am now considering, no such effort was made. The patient was excessively lonely and isolated in the sanatorium to which he was sent. The doctor's visits were occupied with physical examination and the reiteration of commands that he should stop worrying and remain completely at rest.
Such treatment violated grossly one of the basal laws of medical psychology, which recognizes that no one ever stops worrying because he is told to do[Pg 73] so. To give such a command is as irrational as to tell an epileptic not to have convulsions or a choreic patient not to wriggle his hands. Yet this sort of error is constantly committed by physicians who have been well trained to understand the physical changes of disease, but have never concerned themselves to recognize the simplest and most obvious facts about the mental condition of the sick. As I have already said, it is impossible for the dispensary doctor to become acquainted with the details of the patient's malady, or to find out by investigation and experiment how the patient's mind may be made to aid his recovery rather than to impede it. This is the proper task for a social worker, partly because she has more time, partly because she is a woman, and is for that reason more fitted to get into close touch with the patient's mind and to use skill and tact in managing him.
Such studies of the social worker are equally important in the case of the functional neuroses; for example, in the cases where the patient's troubles can be most effectively attacked by ridding him of his fears. Fear plays a dominant role in the sufferings of many cases both of organic and of functional disease. In a recent examination of six hundred and sixty-two young men about to enter Harvard University, it was found that "there were more boys who thought they had a serious organic defect, usually of the heart, and were found entirely sound than boys who thought they were well and had disease." They[Pg 74] had been threatened with heart disease by gymnasium instructors or ill-trained physicians. They had in consequence restricted their physical activities and been haunted by the fear that they might by some unusual exercise of mind or body make themselves seriously ill or perhaps suddenly die. Such fears were all the more disastrous in these young men for being only half realized by themselves. It is exactly these shadowy apprehensions, these dreads which dwell in the half light, never quite faced in full consciousness, which torment and incapacitate us the most. Careful physical examination showed that the young men just referred to were free from all disease, and the clear and emphatic statement of this fact rendered a prompt and important service.
But if such fears haunt the students about to enter Harvard College, who are young men drawn from the better educated and more well-to-do classes, we may be sure that fear plays even a larger part in producing the sufferings of patients such as we examine and treat in a public dispensary. For such patients are very apt to be influenced by groundless rumors, panics, neighborhood gossip. They are prone to believe medical lies which they read in newspapers and in the leaflets and circulars sent to them by charlatans. Almost all their medical education comes to them from such sources, and is made up of a mass of systematic falsehoods designed to excite fear and to produce symptoms by suggestion.
Now if it is true that even among educated and relatively self-conscious classes the most troublesome and incapacitating fears are those which are but dimly known to the patient himself, this is sure to be still more frequently the case among dispensary patients. It is especially difficult and especially important, therefore, that their fears should be understood and brought to light through the investigations of some one who has time, patience, and tact to devote to the task. This cannot be the task of the physician who sees neurological cases in the dispensary, any more than the psychological twists and tangles of the tuberculous patient can be followed out by the specialist in tuberculosis who examines the patient's lungs. It is the proper task of the social worker. When she has brought the patient's fears to light, when she understands the details of his malady, she can communicate these facts to the physician. He then can exorcise the unclean spirits with the full authority of his medical position.
Just here one sees a good example of the proper coöperation between the physician and the social worker in the dispensary. Each brings to light certain elements in the diagnosis. But in the end the physician must unite all the knowledge accumulated either by himself or by his social assistants, and thus must be enabled to act for the patient's benefit on the basis of a body of information much larger than he could have secured alone.
The social worker is also an essential aid to the[Pg 76] physician in bringing to light the mental torments and errors which result from difficult personal relations within the family. These difficulties can only be understood by one who visits the patient in his home, becomes intimate and friendly with other members of his family, and understands, therefore, the difficulties that may arise from friction, rivalry, jealousy, and temperamental incompatibility within the home. In some cases the patient's friends and companions in work or school must also be understood. In other words, one must take account of the totality of influences in the patient's environment, the physical influences of nutrition, ventilation, clothing, but also the psychical influences exerted upon him by his family and friends, by his own half-conscious thoughts, by his worries, his remorse, his fears. Many a case of stomach trouble cannot be cured by diet or remedies until one can find out what it is that the patient is worrying about and can enable him to combat and subdue his mental enemies. Innumerable vague pains which the doctor cannot attribute to any organic disease, and for which the use of drugs is only too likely to do harm, yield only when one can study and influence the whole extent of the patient's mental, moral, and spiritual life. Nothing can be excluded here. It is utterly unscientific to close our eyes to any human interest no matter how little we may sympathize with it personally. It is one of the facts of the case, and must be understood and allowed for in our treatment.
More and more frequently in America the dispensary physician is consulted about the physical and mental condition of children and adolescents who are sent to him from courts. The judges, especially in our juvenile courts, are coming to realize that their legal training, their knowledge of the nature, the evidence, and the prescribed punishments for proved offences, is only a small part of their equipment if they are to deal with juvenile offenders in such a way as to promote the public good. The legal profession is beginning to realize that the physical, mental, and moral study of juvenile offenders is essential if one is to do anything to prevent their offending again. If penology is to be constructive and reformatory, if it is not merely to represent revenge, repression, and intimidation, our judges must know something of medicine and especially of medical psychology. In this field, as in the field of the functional and visceral neuroses, France has furnished the leaders, but apparently these leaders have been insufficiently followed. The work of Binet in the psychological measurements of school-children's intelligence seems to us in America to have been epoch-making. We recognize its limitations, we recognize that in its details it cannot be universally followed. But we have taken up the suggestions and the method of Binet, and gratefully acknowledging our indebtedness to him we have tried to carry these suggestions and methods much further, to apply them to the needs of older children and to the [Pg 78]examination of those who cannot read and write. Binet's tests depended altogether too much upon the use of books and upon linguistic facility. Yet with some modifications they seem to us in America to be of the greatest value, and in the remarkable book The Individual Delinquent (Macmillan Co.) by Dr. William Healy, of Boston, and in the books of his associates and followers, the science of medicine and medical psychology are intimately interwoven with the investigations and reports of the social worker.
In the first of the books to which I have just referred, Dr. Healy presents in detail the cases of over three hundred children who were sent to him as a physician and medical psychologist by the judge of the Juvenile Court in Chicago, who requested Dr. Healy to aid him in his legal treatment through a medical and psychological study of each case. Dr. Healy with his corps of assistants and social workers studied in each child the physical condition, especially the presence or absence of defects of sight and hearing, and the mental condition carefully measured by tests based upon those of Binet, but extended considerably by Dr. Healy himself and by others. But he adds to the facts thus ascertained a careful investigation of the child's social environment, both physical and psychological; that is, of all the influences—hereditary, domestic, economic, industrial, and personal—which have contributed to lead the child into crime. The influence of other boys and girls of the same age, of associates in work or school, is [Pg 79]investigated; also the good or bad example of parents, the amount and quality of schooling, and the presence or absence of religious instruction.
All these latter investigations are carried out for Dr. Healy by social workers. Their results are then pooled with those obtained by him after the physical and psychical examination of the child at the dispensary.
One sees, then, that Dr. Healy and the other Americans who have followed him in this field, insist upon covering in every case four classes of facts:
(1) The child's physical condition.
(2) The child's mental condition.
(3) His physical environment.
(4) His mental, moral, and spiritual environment.
All this investigation is necessary because it is now recognized that crime may be committed because the child is an epileptic; because he is feeble-minded; because he is strained and tortured by defects of sight and hearing; by inability to keep up in school on account of these defects; because he is abnormally susceptible, under the influence of comrades, cinema shows, and sensational literature; because his inheritance, his education, or his home training has been defective or bad.
Since there is no reasonable doubt that physicians and judges will more and more coöperate in the study of offences against the law, and will more and more need the assistance of social workers to complete[Pg 80] their studies and to carry out the reforms which those studies suggest, it can easily be appreciated that the social workers need to be familiar with the methods and results of psychological examination in this field of work.
The idea that social work necessarily concerns the poor is wholly wrong. It concerns the sick; it concerns the tuberculous; some of the sick and some of the tuberculous are poor. Others are not. The State provides dispensaries for tuberculosis, and the people pay for them out of the taxes. Hence all the people feel that they have the right to go there and that they are not in any sense accepting charity in going there. But social work is done in all these dispensaries. Thus the connection between medical and social studies is tending to upset the old idea that social work is necessarily concerned with poverty, and that economic studies are the main part of it.
In America our leading ideas about social work (formerly called charity), came originally from England and from the studies of English economists. Hence to a considerable extent economic considerations have governed the history and evolution of social work even up to the present day. Economists and people interested especially in political economy have studied, practised, and spoken and written upon these subjects, and all who are governed by the traditions inherited from England are still [Pg 81]obsessed by the idea that money and money troubles are the gist of social work.
Nobody should turn up his nose at economics. Anybody who is careless in money matters is sure to come to grief. But in my medical-social work, which has included a large number of cases where poverty existed, I have almost never found the economic trouble to be the essential one. Economics is everywhere present, everywhere subordinate. That is an adaptation of a saying of the German philosopher Lotze: "Mechanism everywhere present, everywhere subordinate." The idea applies also to economics which has many qualities in common with mechanics. I shall therefore lay especial stress in this book, not upon economic but mental deficiencies, which in most cases seem to me more fundamental than economic need or physical weakness.
A considerable portion of all social diagnoses should contain the word ignorance. I wish to distinguish ignorance from moral fault. It is true that somebody's sin, somebody's evil-doing is the fundamental thing in the social diagnosis of many cases. I have never yet studied carefully a case involving social work without finding some moral weakness as an important element in the trouble. Moral elements always enter into the study of a case of social work, but they are often not the main element, often subordinate.
Ignorance, of course, is permanent. If we were not ignorant we should never progress. Ignorance [Pg 82]therefore does not necessarily mean culpable ignorance, but still it may be the keynote to the trouble in which any of us finds himself. Consider industrial ignorance, ignorance of where best to turn one's forces. It would be impossible to say that any of us is free from that. Are we perfectly sure that we have found the place where the Lord intended us to work? This lack may not be such as to bring us into trouble. It may not force us to seek social aid. Yet the lack of a clear idea about where we ought to be working, how we can earn the most money, do the most good, and be happiest—that is a deficiency that none of us is free from.
Industrial ignorance has been the ultimate diagnosis in some of the cases that I have studied. The patient is an industrial misfit. He has not found his niche. Perhaps there is no niche existing for him. Some people seem to be made for another planet or another century. Evidently, then, conception of an industrial misfit is wide, perhaps vague. Yet it often dominates the economic situation. Your patient perhaps cannot earn his living because he is working with only about one quarter of his powers, and that the least useful quarter. That with which he is trying to earn his living may be a mere superficiality. Half the women that I know in industry are working with a wholly superficial part of themselves, unconnected with any of their deepest interests. That is less true of social workers than of any other body of women. They often can put the best of themselves[Pg 83] into their work. But many women in industry, in business, hate it. They may be earning enough, but are unhappy and unsatisfied, because the powers with which they were meant to labor for the service of their kind are not being used at all.
Medical ignorance: A quarter, perhaps, of our task as social workers, is medical instruction, the breaking-up of medical ignorance. Most well-trained physicians of the present day do not believe that many diseases can be cured by medicine or by surgery. We do not have great confidence in chemical, physical, or electrical therapeutics. We believe that when sick people are helped by a medical man or a social worker it is because they have learned something of what we call how to live, a large term which we usually limit to mean how to look after their physical machine.
As I talk with supposedly educated people, I am amazed to see how little people who have lived forty or fifty years in the same tenement of clay have learned about that structure. I do not mean that everybody ought to study physiology. I mean, for example, such a simple thing as how to rest. One cannot rest just as somebody else rests. We have individual finger-prints, no two alike, and individual hand-writing. So we have—and should have found—our own way of working and of resting, which is probably as individual as our finger-prints. But we follow each other like sheep.
The instructions we give to a tuberculous patient[Pg 84] are needed because of his medical ignorance or that of others. I once received a wonderfully touching letter from a middle-aged tuberculous lawyer who finally learned the medical facts necessary to save his life through reading a popular magazine. He was being treated for tuberculosis, about as badly as a human being could be treated, but he did not know this. He had gone to the best doctor in his vicinity. Through reading in a popular magazine an account of a medical conference on the treatment of tuberculosis he finally learned the truth and cured himself. Medical ignorance in relation to diabetes, to stomach trouble, to venereal disease, to heart disease, it may be one of our tasks to remove before inculcating the régime needed in these troubles.
Educational ignorance, ignorance of proper institutions and methods to give a man the power which he needs, is often exemplified in relation to industrial training. One sees people in industry who could do a great deal better work if they had better training. But they do not know where to get it. In many cities there are scholarships and funds for people who show ambition to be better trained. Educational ignorance, then, as well as industrial and medical ignorance, may bring people into economic trouble, even into physical trouble. Such people often turn up at a dispensary asking the doctor merely to cure a headache or a stomach-ache. Yet if the doctor is wise he will find this other trouble hidden in the background.
Obviously ignorance as a cause of trouble is a historic, not a catastrophic, cause. Ignorance does not happen suddenly. Its bad results accumulate gradually.
Another mental element in social diagnosis I call shiftlessness, in a particular sense that I want to define. Not shiftlessness in the sense of a general moral accusation, but as a failure of adjustment—maladjustment, due to shiftlessness in the sense of an inability to shift when there is a need for it. Professor Edouard Fuster[1] has spoken of social treatment as consisting almost entirely of helping people towards a better self-adjustment to their actual or attainable environment. People often make a failure of their lives because they do not shift when the proper time arrives. There are also people who shift too often, on the other hand. I shall speak of that later.
The physical analogies of these mental faults are interesting, I think. A person who has too great physical shiftlessness gets a bed-sore. Healthy people when they have lain in a certain position in bed for a time feel a discomfort and therefore instinctively turn over. We shift ourselves now and then in our chairs as we sit, and thus we relieve pressure which in turn would produce injury. But in chronic illness the patient sometimes lies in one position so long that he wears out his tissues till the raw flesh or even[Pg 86] the bone is exposed. That is just as true on the mental side of life, true of us all.
There is nothing I hate more than seeming to take a pharisaical attitude in our social diagnoses. All of us probably have failed to shift when we should. We might be more useful to-day if we had shifted more wisely. Still, we are getting along somehow, and some other people come to us for advice because they are even more shiftless than we. I never yet made a social diagnosis in anybody that I could not make also in myself. It is only a question of degree.
Industrial shiftlessness is an obvious example. A person gets into the wrong job and then does not get out of it. Most people choose their professions by the most irrational process or lack of process that can be conceived of. When a boy is ready to choose a profession, does he look around him, study the alternatives, and select one? Not at all. He does what the next man does, what his father did, what he happens to have heard most about. This is true whether people are pressed for money or not. They choose their job for no good reason; they are thrown into work by something pretty near to "chance." But they are often saved from the full consequence of their mindlessness because they shift. They shift either within the job or into another job. I got into medicine first on the laboratory side, began by writing a book on the blood and doing an unconscionable amount of work in the laboratory. It was wrong. I was not fitted for it, and luckily I knew enough to[Pg 87] shift. Social medicine was what I wanted. So many a man shifts within his profession. That is why the wrong choice made at the start does not always get people into serious trouble. But the chronically shiftless man remains immobile. He does not know where else he might be besides the place where he is. So he stays where he happens first to fall, gets bitter, hard, poor, drunken, all because he is in the wrong niche.
One sees racial shiftlessness when people cross the ocean and try to take root in a new country. This racial non-adjustment has very tragic results. We see it, for example, in the Armenians in America who have come from a civilization two centuries back, and cannot jump these two centuries. Hence comes the breaking-up of moral and industrial standards because they have come suddenly into a civilization to which they cannot adapt themselves.
A third kind of shiftlessness one might call domestic shiftlessness. An English servant girl married an Italian fruit-dealer. She was taken home into his Italian family in Boston and had to try to fit herself to Italian customs. She and her husband got along excellently. But it was very hard for her to understand the shifts which she must make in order to adapt herself to his family. She was an old patient of mine, and after her marriage she brought her physical troubles to me, quite ignorant of the fact that she was worn out by family friction. My efforts were devoted chiefly to teaching her Italian customs and defending her husband's family to her. I did not know[Pg 88] any too much about it. I had myself to learn the subject which I was set to teach, as one does so often in social work. I had to find out the meaning of many queer Italian customs in order to interpret them to her. At first she had no idea that when one crosses a racial line one must shift considerably. But she has finally learned it, and she is happy now.
I have spoken of two social deficiencies—ignorance and shiftlessness. I believe there are very few cases in the social worker's domain which fail to show some sort of ignorance, some sort of shiftlessness, as an element in the social diagnosis. Such diagnoses must usually be long. They are complicated and cannot often be expressed in one word. The word "feeble-minded" and the word "tramp" ("Wanderlust") are among the rare examples of a brief social diagnosis which explains all the physical, economical, moral misfortunes which one finds in a person. But generally one cannot find such a phrase. So one makes a number of statements as one makes a list of many diseased states in the different organs of the human body. I do not regret this. The best medical diagnoses, those made after death, contain from thirteen to seventeen items on the average. One of my chief tasks during the last fifteen years has been to study diagnoses made after death and compare them with those made in life. The real diagnosis as it is revealed at autopsy contains on the average thirteen to seventeen items. The diagnosis made during life contains often but two or three items. This [Pg 89]brevity is characteristic of the very partial truth contained in our clinical diagnoses. Therefore I do not altogether regret it when I see in a social diagnosis a long series of items referring one after another to the main departments of human life. When we are making our medical diagnoses we try to say what is wrong with the heart, the arteries, the kidneys, the stomach, etc., in each patient. So in making our social diagnoses we ought to go through some such list as I have begun to give here. Is ignorance a factor? If so, where? Is shiftlessness in this particular case a factor, and how? There are certain organs of the human soul which one can go through and check up. (Anything the matter here? Anything the matter there?) as one goes through the bodily organs to make a medical diagnosis.
The shiftless person, in the sense in which I define the words, is the person who does not move often enough, who rests too long on one particular set of habits so that he allows the world to move away from him while he is left high and dry. Or he allows himself to get fixed in one little set of habits and becomes a person with one idea. That is shiftlessness, the person who cannot accommodate or adapt himself.
The opposite of this is instability—the defect of the person who shifts too often, who cannot stay in one field long enough. In the physical field this [Pg 90]applies to people with motor nervousness, people who never can keep still. But we are more interested, of course, in the psychical side of it. Any piece of work can be said to have three phases, something like the phases that Sir Almoth Wright has emphasized in his writings on immunity. We have first a stage of interest and elation, then a slump, a depressed or negative phase, as Wright said, a stage when things are not going smoothly or when organization seems endlessly complicated. Then is the time when, if we are of an unstable type, we throw up our work. The unstable person cannot believe that the undertaking is going on and up to a third or positive phase, which in the end will be on a higher level than the phase in which we started. Normal people habitually expect these three phases in every human undertaking. They foresee the negative phase before they get out of the first one. Hence they are not astounded or bitter when the inevitable slump comes in the second phase. But the unstable person breaks off at that point and tries something else. It constitutes one of the most serious blots in any one's record if we find that he has changed his work four or five times already. "Why did you leave your first job?" we ask, and, "Why did you leave the second one?" There is never a satisfactory reason for so many changes. These people are rolling stones; they gather no moss. They never accumulate skill, power, and money as the result of having stuck long enough in one place.
We see mental instability also in temperament, in spirits. Many people get into trouble because they do not realize their own "negative" and "positive" phases. Most people, we say, have their ups and downs. But if we take our ups and downs too seriously, then we may talk about suicide as so many people do. It is in these emotionally unstable phases that people give offence to others, quarrel with their families, lose their jobs.
Instability is much less important in the adolescent stage. Many a parent has been in despair over his adolescent children. "Nothing good ever can come out of that boy. He is too unstable," the parent is apt to say. Yet great good often does come out of such a boy, simply because he grows older. Such a boy is generally between thirteen and nineteen. Tremendous physical changes are going on, which are rather more than he can manage. Hence he becomes for a time unreliable, capricious, moody. There is almost no degree of mental instability and unsatisfactory conduct which may not wholly disappear as we get past the adolescent stage.
On the other hand, the older a person is the more serious the outlook in a case of instability. A woman in the vicinity of sixty drifted into my hands some years ago, after having been the round of doctors whose diagnosis was essentially instability. Although I labored very long and prayerfully with that individual, I cannot say that I produced any considerable effect.
Remember always the possibility that such instability is due to drugs. Among the most unstable people are the morphine-takers, and because that has among other symptoms concealment and lying, it does not easily come to light. In the evening the morphine-taker is full of prowess, is full of hope, ready to make engagements for nine o'clock the next morning. But he almost never turns up for that engagement the next morning. This morning depression is common also in many other diseases, such as neurasthenia and that rare disease, anemia. The anemic patient has a hard time getting up in the morning, but it is the fault of his red corpuscles and not of his character.
Another phase of instability is abnormal suggestibility, abnormal openness to influence or "suggestion" in the psychological sense. I cannot count the number of fond but foolish mothers who have said to me about a child, "John is a good boy, only he is weak. He gets led astray by his companions." Everybody is and ought to be somewhat suggestible, normally suggestible. The man who is not suggestible is the person with a monomania, who can see nothing but his own view, is stupidly attached to one set of ideas and so cannot learn. But one can easily be too suggestible. Over-suggestible people run after every craze, are impressed with each new religion, or are tremendously excited with each new friend and think of each new experience: "Ah! This is what I have been looking for all my life. Nothing[Pg 93] else matters." This is especially common at the adolescent age, but it is a danger for all of us, men and women of every age. We get carried away by popular crazes, by influences, by suggestions, so that we cannot remember the good that there was in our previous beliefs and interests. If so we are mentally unstable in this respect.
We see in every dispensary many cases of abnormal physical suggestibility, people who think that they have caught every disease that they hear about. Among medical students and nurses in training there are always some who become convinced that they have the disease which they have just been studying in the hospital. In the social assistant's work as a taker of histories she must remember that. Highly suggestible people give curiously misleading histories because they become obsessed with the idea that they have some terrible disease. There are three examples of abnormal suggestibility which in my experience recur with especial frequency: heart disease, cancer, insanity. People are amazingly prone to fancy that they have heart disease. If they have any symptoms in that part of the body where they are taught to believe that the heart resides, or if they have heard anybody talk of heart disease, or especially if anybody whom they know has recently died of heart disease, there are many people likely first to believe that they have heart trouble, and then to have actual symptoms which they attribute to heart disease. They often say nothing[Pg 94] about this fear. That is just why it is so essential for social workers to dig it out in the course of their history-taking. When people are afraid of a thing they are especially apt to conceal that fear.
Insanity is feared, I think, even more often than heart disease. Every doctor is consulted by people who are sure on most trifling evidence that they are going insane. We hear people say, "Why my mind must be failing, for I read down a page and when I get to the bottom I cannot remember what I have read." Or, "I am losing all memory. I met a man recently suddenly and I could not remember his name." These two normal fatigue-products—failure of attention or failure of memory—often make people think that they are going insane. A third result of fatigue which often frightens people is the sense of unreality. Such people say, "I seem to be numb. Things do not seem real to me. I talk to people and I wonder if it is not all a dream. Am I not going crazy?" There have been interesting essays written by French psychologists on the "Sense of the Déjà Vu." For a few hours whatever we say or do seems a repetition; we have said, done, heard all that before we fancy. It is a very disquieting sense. But it is usually nothing but fatigue.
Cancer I suppose is the most dreaded of all diseases, but one of the most unnecessarily feared. Patients may appear at the dispensary for most trifling pains or stomach troubles, troubles that all of us would disregard, and when we inquire why it is that[Pg 95] they have come, sometimes a long distance and at considerable expense, we find out that it is because they have recently heard or read something about cancer, or remembered that there is cancer in the family. We cannot be too careful to tell people that cancer is not hereditary. People are apt to think it hereditary, but this is one of the medical fallacies that we should all of us do our part to eradicate from the public mind.
I will mention one or two other common groundless physical fears. We should teach people that if they have a pain in the left side of the chest the chances are about nine out of ten that the heart is perfectly sound. If they have a pain, as they say, "across the kidneys," the chances are ninety-nine out of one hundred that the kidneys are perfectly healthy. The newspaper advertisements of charlatans do all they can to make people think that a pain in the back must be kidney trouble. We must fight such poisonous influences.
[1] Conférence Interalliée des Mutilés. Paris, May, 1917.
It is not merely because of a doctor's mental habit that I speak of life in terms of diagnosis and treatment. For though those particular words are medical, any part of life can be thus conveniently summed up. One tries to find out the facts about some region of life in which one works or plays, fights, loves, or worships (diagnosis), and then one tries to do something about it (treatment). If one makes a friend one tries to find out something about him and then to treat him accordingly. If one comes to a new city one tries to diagnose its geography and to direct one's self accordingly. If there is anything not included in that set of phrases about the behavior of the human being towards the world, I do not know it. Therefore it seems natural to sum up social work also in terms of diagnosis and treatment.
I referred in the last chapter to social ignorance as a possible item in a social diagnosis. I meant to recall those parts of a person's outfit for dealing with life in which he is deficient because of ignorance, industrial ignorance, or educational ignorance, or physical ignorance. I went on to recall two other mental deficiencies or sources of incapacity, shiftlessness and instability.
In this chapter I want to exemplify fears as sources of inefficiency or deficiency, as causes of sickness, economic dependence, and unhappiness. Christian Scientists define almost all human ills in terms of fear. That is extreme. I know many people who do not seem to suffer from any fears whatever. I sometimes wish they suffered from a few more. I should not say at all that fears were the cause of all evil, or that the fearless person was perfect. Still, fear is a very great factor in social ills. I mentioned in the last chapter the three commonest physical fears as met with in medical practice: fears about the heart, about cancer, and about insanity. I sometimes feel that I will never let a patient go from me without saying, "You have not got heart disease, you have not got cancer, you are not going insane," even if he came to me for a cut forger or an ingrowing toe-nail. No one but a physician can appreciate how many people dread one of these three diseases.
But about physical fears as about other fears, the most important thing to know is that they are disabling, crippling, in proportion as they are not recognized, or only semi-conscious. I am one of those who believe that one should not talk about unconscious consciousness, although synonymous phrases are very popular among modern psychologists. But we all of us know that a large part of our mental life is in a half light, neither in full consciousness nor in oblivion. These half lights may be quite harmless, but often they are especially mischievous. Our[Pg 98] vague, undefined experiences produce the fears which trouble us most. Fear of the dark and fear of ghosts exemplify this rule, but it holds just as well for fears about disease.
Partly because of this vagueness, people often do not tell the doctor about their most serious fears. One has to go out of one's way to reassure people about their fears, because they so often conceal them. Of course there are exceptions to that. People come to a doctor often for nothing else except fears. But that is not true of the majority of patients nor of those suffering the most harmful and haunting fears. It is for that reason that I am trying to give some idea of where to look for facts that do not come spontaneously to you as patients tell their stories. If the social assistant has not the medical knowledge or the authority necessary to reassure the patient, she can bring him to somebody who has. At the present time there is no piece of medical service more clean-cut and satisfactory than the power to reassure a person about an illness that he thinks he has, half-consciously fears he has, and therefore tries to banish from his mind. To discover groundless fears, then, fears of poverty, of ridicule, of marital unhappiness, and to cure them by bringing them to light, is the task that I think every social worker should consider as part of her job, in so far as she is connected with medical work, as she must be always so far as I see.
It is astonishing how often people are relieved by[Pg 99] knowing a truth which we shrink from imparting. I recently examined at a Red Cross Dispensary in Paris an old lady in face of whose troubles I was a little daunted when I came to carrying out the principle of telling the truth as I have long preached and tried to practise it. She had a chronic asthma. She suffered a good deal from it both night and day, and I could not see the slightest prospect that she would ever be any better, because in people past middle life asthma is for all intents and purposes an incurable disease. When I had finished examining this old lady and faced my task of telling her the truth, I did not feel comfortable about it at all. But I gave her the facts. The outcome was striking. "Oh, yes," she said, "I rather thought that my asthma is incurable. I did not expect that you could do anything to cure it. All I wanted was to make sure that I had not got tuberculosis on top of it." About this fear of tuberculosis she had said not a word to the history-taker. It came to light quite unexpectedly. But when I assured her that she had not got tuberculosis on top of her asthma, she seemed quite contented and hobbled away very happily, puffing and blowing as she went.
That illustrates the relief that comes to people from finding that a deeper-concealed fear is groundless. Again and again I have pushed myself up to the task of telling people what I knew they had to know, and then found that instead of prostrating them I had relieved them of torturing uncertainty.
I will relate an experience which shows how far this truth extends. An elderly lady, whom I had known for nearly twenty-five years at the time this incident happened, was in the habit each spring of coming from New York, where she lived, to Boston, where she used to live, to make a round of visits among her friends. While still on one of these visits she telephoned me one day to come and see her. As I entered the house where she was staying, I was met, as I have been met so many times, by a member of the household, who, with finger on lip and every precaution for silence, beckoned me into a side room and proceeded to tell me "what nobody else must know." It was something like this: That my friend the old lady had begun the first of her round of visits about a month before this. On that first visit it had become pretty obvious to her friends that she was mentally queer. She was not a millionaire, yet she was spending and giving away an extraordinary amount of money. She was ordinarily a person of quiet habits and not prone to hurry about, but now she was making the dust fly all the time. She was ordinarily modest. She had now become boastful. The first friend with whom she stayed believed, as people usually do, that it would be dangerous to tell her anything about her mental condition, yet found it impossible to keep her in the house. Therefore the hostess made the excuse that she had a maid leaving and could not really keep a visitor just now. Would my friend mind moving on to the next visit? She[Pg 101] moved on to Number Two; naturally the same thing happened there. So the second hostess passed her along to Number Three. She was with Number Four at the time when she called me.
All this was given me in the strictest secrecy in the little anteroom close to the front door. My informant then tried to pledge me not to tell the old lady the truth, fearing an outbreak of violence. But as I had a good while ago sworn off all forms of lying, I refused to make any such promise.
I went upstairs to see the patient. She poured out to me one of the most pitiful stories I ever heard—the same story just given, but from her own point of view. So far as she could see, her friends were all playing her false in some way, or losing their affection for her. She knew that it was not by accident that one friend after another had politely shown her the door. Something was being concealed from her. What could it be? She was really worn out, she said with worry and sorrow about it.
I told her at once the whole truth. I told her that she was insane. I could also tell her truthfully that she would come out of it (as she did), but that I must now take her away from this house, shut her up, and take care of her. "Oh," she said, with immense relief in her voice, "is that all? Is it nothing worse than that? Insanity is nothing compared to losing all your friends." Insanity is one of the greatest of human fears, but for this old lady, as for most of us, there is something still worse—the fear that[Pg 102] one has not a friend in the world. Even to know that she was doomed to what most people would consider one of the worst of fates was to her a relief; for there was a worse fear in reserve, and that she now knew was groundless.
The treatment of fears, the only treatment that I know of, is that we face them, look straight at them, as we turn a skittish horse's head right towards the thing that he is going to shy at, so he can look at it squarely. So we try to turn the person's mental gaze straight upon the thing that he fears.
People frequently consult a doctor because they are afraid of fainting, fainting in church or in the street, for example. In such cases I have found it most effective to say, "Well, suppose you do—what harm will it do?" From the answers to this question I find generally that the patients have in the back of their minds, unconfessed, unrealized, the fear that if they faint and nothing adequate is done to cure them they will die. They do not know that people who faint come to just as well if they are let alone, and that all the fussing about that is usual when people faint is useful merely to keep the bystanders busy and not to revive the patient.
Make a person face "the worst" and you disarm its terrors.
"But suppose I get faint on the street?"
"Well, you probably will just sit down on the curbstone until you come to."
That remark does not sound as if it would reassure a person even if made with a laugh. But it does, because he is thereby freed of a fear of something much worse, a fear that lurks in the background of his mind.
There is one other thing to be said about the treatment of fears. If a person fears to do any particular act, such as going to church or into the subway, if he fears to be alone in crossing a big square, if he fears to get into a crowd (all these are common fears), the most important thing is to force him to do what he most fears.
"Do the thing you are afraid of, or soon you will be afraid of something else as well. And the more you do what you fear to do, the less you will be afraid of it, because your act will bring you evidence of the truth. Your act will prove to you that you can do the thing that you fear you cannot. That fact will convince you a great deal more than all the talking that your doctor or anybody else can do. You will get conviction by reality, the best of all witnesses."
Among the poor, with whom we deal part of the time in social work—though I insist that social work is concerned with the rich as well—we have to face economic fears. In America and England economic fears are a very real evil—fears of the work-house, fears of coming to be dependent, of having no place of their own, are what poor people often dread. Again, the clue for our usefulness is to find[Pg 104] out what people do not tell us of these economic fears, and then to see if we can make them groundless.
In a certain number of people (I do not feel competent to say how large a portion), life is rendered miserable by the fear of being found out. I happened, as I have already said, to get driven some years ago into a position where I thought it best to swear off medical lying. One of the surprising parts of this experience was the sense of relief which I felt when I knew that there was no longer anything in my medical work that I was afraid of having any one find out. It was in benevolent, unselfish medical lies that I had been dealing, according to the ordinary practice of the medical profession. But as soon as I decided that I could abandon these and need no longer fear that any patient might find out what was being done to him, I had the sense of a weight taken off my shoulders.
There is a very eloquent passage in one of Mrs. Bernard Bosanquet's books[2] about social work, in which she describes the psychology of the poorer classes among whom she worked in London, and dwells especially on their characteristic forgetfulness. They cannot learn because they cannot remember. They cannot learn how to avoid mistakes[Pg 105] in future because they cannot remember past mistakes. One well-known difference between a feeble-minded person and a person competent to manage the affairs of life, is that the former forgets so extraordinarily, and therefore cannot build up through remembrance of his past how to steer better through the future. Of course we all of us have this disease in varying degrees. We all forget, in the moral field as well as the physical, things that we ought to remember. There are things that we ought to forget. After we have started to jump a fence, we must not remember the possibility of our failing. The time to remember that is before we have begun to jump. Moreover, there is no particular benefit in remembering our own past mistakes if they are such that we cannot do anything about them, morally or any other way.
There are things, then, that we ought to forget, but allowing for these, forgetfulness means forgetting the things which we ought to remember. In alcoholism it is extraordinary how much the person forgets. One cannot fail to be struck by the fact that the alcoholic gets into trouble again and again because he cannot fully remember what happened before. In the field of sex faults this truth is equally obvious. A man is unfaithful to his wife because he allows himself to forget his wife—his memory of her is for the moment blotted out. Nobody could violate his own standards in this field if he could vividly remember them. Hence if we are to help any[Pg 106] one else to govern himself in matters of affection we must help him to remember, help him by planning devices that make it nearly impossible to forget.
Bad temper can ordinarily be explained by forgetfulness. We can hardly lose our temper with a person if we remember the other sides of his nature opposed to that with which we are just now about to quarrel. Nobody consists wholly of irritating characteristics. We all possess them; but we all possess something else besides. Hence if we can realize some of our own moments of wrath, I think we must confess that for the moment the person with whom we were enraged possessed for us but a single characteristic. The rest were forgotten.
My account of these five common types of mental deficiency: ignorance, shiftlessness, instability, fears, forgetfulness, is general and vague. I mean to make it so. If my suggestions are of any use to the reader it will be because he is able to make his own specific applications. I want, however, to mention one example of a much more specific fault, namely, nagging. In social work we often see families broken up or seriously cracked by some one's nagging. It consists in reminding people of their defects and shortcomings in season and out of season, until the reminder finally gets upon their nerves. You are aware that your husband, your wife, your child, has some very deleterious fault. Admittedly he has it and it is constantly getting him into trouble. So you want to[Pg 107] be quite sure that it never gets him into trouble again; and hence you keep reminding him of it again and again until you produce an irritation that only aggravates the original fault.
Why do I take so trivial and specific a case as this? Because I can remember several cases where I could not possibly leave out nagging when I came to make my social diagnosis. It was one of the chief factors. One cures this disease, in case one does help it at all, by making the nagging person conscious of what it is that he is doing. The nagging impulse is like an itch. It recurs and scratching does not stop it. The nagger does not know quite why he does it; he finds himself doing it almost in his sleep. Hence we try to wake him up, to make him conscious, if we can, of his foolishness, of the kind of harm he is doing, and of the degree of incurability he is inducing in the person whom he is trying to cure.
I will now sum up the last four chapters in a diagram which we have used in Boston at the Massachusetts General Hospital to assist us in making our social diagnoses. A social diagnosis can very seldom be made in one word, such as idiocy or tramp. It must include the patient's physical state. It must summarize a person's physical, moral, and economic needs. Our best social diagnoses, such as idiocy or feeble-mindedness, do not refer to the mind only. They refer to the body just as much. Feeble-mindedness is a statement about the child's body,[Pg 108] his brain, his voracious appetite, the diseases to which he is likely to succumb, his extraordinary susceptibility to cold, and his poor chances of growing up. One says a great deal about the physical side of a child as soon as one pronounces the word "feeble-minded." Also one says a great deal about his financial future. One knows that the feeble-minded child will never rise beyond a very low point in the economic scale. One says also a great deal about his moral future. We all know to what sexual dangers and temptations he is especially exposed. And on the purely psychological side one can predict his entire unteachability beyond a perfectly definite limit. All this is given in the medical-social diagnosis, "feeble-mindedness."
This is an example, then, of an ideally complete and compact, though a very sad, social diagnosis. It is almost the only good one we have worked out as yet. The only other is "tramp." The tramp in a technical sense is a person who has what the Germans call "Wanderlust." He is unable to stay in one place. Perpetually or periodically he desires to move and to keep moving. The tramp is a medical-social entity. He has certain physical limitations, certain economic limitations, certain moral deficiencies. But in America he is rather a rare being. One does not see many typical tramps here.
Since few social (or medical-social) diagnoses can be stated in a single word, one is usually forced to write down one's diagnosis in a great many different[Pg 109] items. As a guide I made four years ago a schedule for our use at the Massachusetts General Hospital. Use—the only test for that sort of thing—has shown this schedule to be of some value.
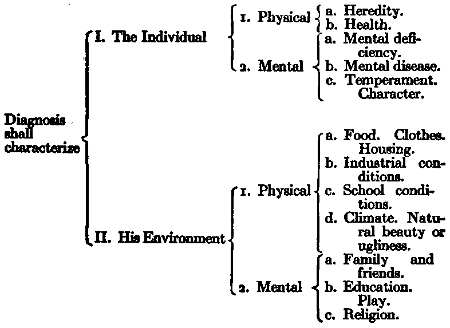
To make a social diagnosis we should make a summary statement about the individual in his environment. That summary is to include his mental and physical state, and the physical and mental characteristics of his environment. (I here use the word "mental" to include everything that is not physical; that is, to include the moral, the spiritual, every influence that does not come under physics or chemistry.)
When the investigation of a patient is divided between doctor and social worker, the doctor studies his physique; the social worker studies the rest. I [Pg 110]believe that there is nothing that we can want to know about any human being, rich or poor, that is not suggested in that schedule. Suppose, reader, that a friend of yours was engaged to be married. Suppose you wanted to know something about the fiancé. You would certainly want to know about his health and his heredity; then what sort of a person he was, his mentality, whether he had any money—what are the obvious physical facts about his environment. To what influences has he been subjected, and what mental supports, such as education and recreation, family, friends, and religion, can he count upon? You would not want to know any more and you ought not to want to know any less.
So in summing up a social diagnosis I think it is convenient to use the four main heads that I have put down here. I think these headings will remind us of everything that we want to put down, and of everything that we may have forgotten to look up. That is one function of such a schedule—to remind us of the things which we have forgotten.
Made up in such a way as this, of course the social diagnosis will have many items, and like medical diagnosis it will be subject to frequent revisions. The doctor who never changes his diagnosis is the doctor who never makes one, or who makes it so elastic that it means nothing. So social workers should never fear to add to, to subtract from or to modify their social diagnoses.
The best medical diagnoses—those made after[Pg 111] death—often contain fifteen or twenty items. Before death in a recent case we found pneumonia. After death we found in addition: meningitis, heart-valve disease, kidney trouble, gall-stones, healed tuberculosis, and ten minor troubles in various parts of the body.
So a good social diagnosis will name many misfortunes of mind, body, and estate, healed wounds of the spirit that have left their scar, ossifications, degenerations, contagious crazes which the person has caught, deformities which he has acquired.
[2] Bosanquet, Helen. The Standard of Life and Other Studies. (London, Macmillan & Co., 1898.) The Family. (London, Macmillan & Co., 1906.)
Fatigue is more important for medical-social workers to understand than any single matter in physiology or any aspect of the interworkings of the human body and soul, because it comes into almost every case from two sides: (a) from the workers' side because the quality of work that she puts into trying to help somebody else depends on how thoroughly she is rested, and how much she has to give; and (b) from the side of the patient, his physical, economic, and moral troubles, because fatigue is often at or near the root, of all these troubles. It is unfortunate that in spite of its importance, we do not know much about fatigue from the physiological point of view. Since the war of 1914-1918 we have prospects of knowing more about it than ever before; for one of the grains of good saved out of the war's enormous evils has been the fruitful studies of fatigue made in England, studies more valuable than any that I know of.
Let us take fatigue in some of its very simple phases, as it applies to your life and mine. The first thing to recognize is that it can affect any organ; our stomachs can get tired just as well as our legs.[Pg 113] When a patient complains of pain, vertigo, nausea, we first ask ourselves, "What disease has he got?" That is correct. Disease must be found if it is there. But the chances are he has no disease, but only a tired stomach, since fatigue easily and frequently affects that organ. When the whole person has been strained by physical, moral, and especially by emotional work, he may give out anywhere. He may give out in his weakest spot, as we say. That weak spot is different in different people. Therefore the study must be individual. We cannot do anything important with our own lives until we learn how and when we get tired. It is the same with people whom we try to help in social work.
Fatigue, then, may be referred to any particular spot in the body. People often go to an oculist to see what is the matter with their eyes, when there is nothing in the world the matter with their eyes: the honest oculist tells them that they are tired, and that for some reason unknown to him their fatigue expresses itself in the eyes.
This is a very common and very misleading fact. The patient finds it hard to believe that medicine ought seldom to be put on the spot where he feels his pain. If the pain is in his stomach he wants some medicine to put in his stomach and not a harangue on his habits, which is usually the only thing we can really do to help him. If he has a pain in his back he wants a plaster or a liniment for his back. It is very hard to get people out of that habit of mind, and[Pg 114] we shall surely fail unless we are clear about it ourselves. It must be perfectly clear in our minds, or better, in our own experience, that fatigue may be referred to one spot or to another, in such a way as seriously to mislead us. I suppose that half of all the pains that we try to deal with in a dispensary—and pain, of course, is the commonest of complaints—are not due to any local or organic disease in the part. Doubtless there are some wholly unexplored diseases or disturbances of nutrition in that part, as there may be in the eyes when they ache because you have been walking up a mountain. But medical science knows nothing about that. What we do know is that the pain, if it is to be helped, will be helped not by thinking about that spot or doctoring it, but by trying to get that person rested.
Fatigue, then, ought to be one of our commonest medical-social diagnoses, and to help people out of it, one of the attempts that we most often make. In Dec., 1917, a dozen or more Y.M.C.A. boys consulted me in France, all with coughs, all wanting medicine to stop the cough, and most of them a good deal disappointed because they were told to go home and go to bed, told that they were tired, and that this fact depressed their resistance against bacteria, so that bronchitis or broncho-pneumonia resulted.
The second point, then, that one wants to make about fatigue is, that it is the commonest cause of infectious disease. Pasteur's great discovery, which set modern medicine upon the right bases, [Pg 115]sometimes gets twisted out of perspective. Sometimes we fail to realize that the seed may fall upon stony ground. The seed, of course, is bacteria, and its discovery was Pasteur's immense service to humanity. But Pasteur was so busy that he did not emphasize the truth that a seed can fall upon good ground or upon bad ground. When bacteria fall upon bad ground, that is, upon healthy tissue, they do not grow, they do not spring up and multiply. Tired tissues, as has been abundantly proved by animal experimentation, are prone to infection. They are good soil for the growth of bacteria. It is true generally; it is true locally. A part that has been injured, for instance, a part that has been bruised without any break in the skin, without the entrance of any infection from the outside, is damaged by something that hurts its resisting power as fatigue does. Such a part will often become inflamed, will often become subject to the action of bacteria which must have been in the body already, but which had been kept on the frontier by our powers of resistance.
Our "powers of resistance," then, which we cannot more definitely name, which we do not as yet know to be identified with leucocytes or with anything else, can get tired. When they get tired we "catch" a cold or a diarrhea, or a hundred things which seem to have nothing to do with fatigue, but have nevertheless.
Accumulated fatigue or physical debt. If you go up a long flight of steps at a moderate rate, you can get[Pg 116] to the top without being tired; if you go up at a rapid rate, as most of us do, you are tired at the top. Physically you put out the same amount of energy, I suppose. I do not see that there can be any considerable difference in the energy consumed by the performance of that act whether we do it slowly or quickly. The difference is that in the first case we rest between each two steps as we rest between each two days at night. When our activities are so balanced as not to run in debt, we rest between each two steps. You and I can walk at our individual peculiar gait on the level for a long time without any accumulation of fatigue, often with refreshment. But push us and we are soon exhausted. Suppose that our normal walking rate is three and a half miles an hour; push us to four, and it may not be a quarter of a mile before we are done up, because we have not been able to avoid accumulated fatigue by resting between each two steps. It has been said that in rowing the crew that wins is the crew that rests between each two strokes. The person who does not get tired is the person who rests between each two days. He does not accumulate fatigue. It is the accumulation that finally breaks you, makes you bankrupt. It is the little unnoticed bit added day by day, week by week, month by month, that makes the break.
Fatigue we should think of as running in debt. One of the figures of speech that has served me best in teaching patients how to live is that figure of [Pg 117]income and outgo. I have often said to people, "Physically you are spending more than you earn, not to-day merely, but right along. You must earn more than you spend. You must get a plus balance in the bank. Then you can run along with fatigue or illness."
That figure of speech helps us also to express another fact about fatigue, which is important to recognize in ourselves and in our patients, because otherwise we get thrown off the track: delayed fatigue. The first day that your income begins to be less than your expenditures, nothing necessarily happens. The bank does not proclaim that there is no deposit there. It is some days later, usually, that you begin to reap your troubles. It is the same in physical fatigue. Patients say to us, "I slept ten hours last night. I spent a virtuous Sunday. Why should I be tired to-day?" We should answer, "Because of something you did last Tuesday or thereabouts." We all are familiar with this in relation to sleep. It is not the day after a bad night, but several days later that its effects depress us.
Delayed fatigue, then, is an important thing to notice in ourselves and to bring home to the people that we are trying to help. I suppose one could say that a great part of our business in social work is to call people's attention to things; if they have recognized them before, they will perhaps get a lesson out of what we say. Such matters are referred fatigue, delayed fatigue, accumulated fatigue,—familiar enough,[Pg 118] only the person does not act on them because he does not notice them.
The fatigue-rest rhythm, the alternation of fatigue and rest, I have already phrased by the metaphor of earning and spending. You can phrase it also by a metaphor very close to the physical facts as we know them, the metaphor of building up and tearing down. During the daytime, from the point of view of physiology and the workings of the body, we burn up tissue. In us oxidation processes are going on which are really burning, as really as if we saw the flame. Tissue is being destroyed, broken down, going off in the form of heat, energy, and life. That is good in case it is followed, as it should be, by a period of rest in which we build up. Presumably, if we could see with adequate powers of the microscope or powers of observation of some sort, what goes on during rest, we should see a perfect fever of rebuilding all that we have torn down during the day. People often say, "Shall I take exercise?" Yes, but remember that half of the process of taking exercise is getting rested afterwards. It will do you good provided you rest after it, provided what has been torn down in exercise is replaced by sufficient tissue or fresh power in rest.
The English studies of fatigue to which I have referred have been of great importance because, so far as I know, they are the first attempt we have had in the way of testing when men or women in industry are too tired and how much too tired they are. I do[Pg 119] not suppose that any employer of labor would want for his own profit or for more than a short time to overwork people in this sense, if he had the facts called to his attention. If he realized what he was doing, he would not want to break down his working force any more than he would to spoil his machinery. But some employers are careful of their steel machinery and careless of their human machinery. They will continue to be so, I fear, until we know more about fatigue.
It is one of the most difficult things to measure that I know. Take it in your own case: what tires you one day does not tire you another day. The individuality of it, the disturbing factors when we try to measure it, are perfectly extraordinary. Such a disturbing factor in our calculations is "second wind"—mental or physical. A number of men marching along will grow less tired as time goes on by the acquisition of what we call "second wind." We do not know what it is. We have tried to connect it with the condition of the heart, to say that the heart finally gets to deal with the volume of blood that is running through it so that there is no overplus of blood stored in any one chamber at any moment. But we do not really know anything about that. We do not know what second wind is; but it is important to know that it exists.
Moreover, as Professor William James pointed out in that essay called "The Energies of Men," there are "mental second winds." Just when a man[Pg 120] is worn out he often finds new strength. He often cannot get his best strength until he pushes himself even to despair. In the spiritual experiences of the world's saints and heroes we find that it was just when it seemed as if they were about to go under that this second wind, or third wind, for it sometimes comes again and again, this mitigation of fatigue without rest, comes to them. This is a most disturbing fact. If we were like a pitcher which is emptied out and filled up, we should know all about fatigue very soon. We are like a pitcher to a certain extent, but the similarity is disturbed by such factors as second wind, and disturbed, moreover, by mental and emotional intruders like music. A military band coming upon a body of marching men will give them strength when they had no strength. That is not a sentimental but a practical fact which army men have to take advantage of. Then the fact that many people can rest by change of work without stopping, is also disconcerting. We say to a person, "You have been working hard all day; you must stop, lie down, go to bed." That person disobeys, keeps going on something different, is altogether fresh next morning, and we have to confess that we were wrong.
It is a very familiar experience that one may be almost dead from one point of view, but quite fresh from another, as one wants no more meat, but has plenty of room for dessert. Some people can rest by change of work and some cannot. It is very important for us to keep finding out in a great number of[Pg 121] ways which of the classes into which people's bodies are divided we each belong to. Do we belong in the class of the people who must get their rest by giving up, by the abolition of all function, or in the class who rest by the change of function, by doing something different from the day's work? It is a question of fact and must be found out by each individual for himself.
Just here the individuality of fatigue, which I have been trying to make clear all along, becomes obvious. We are rested by making a success of something. If we have been making what seems to us a failure of something, it is amazing how it rests us to make a success of something. The boat crew that wins is almost never tired at the finish; the crew that loses is almost always dead tired. That is why it is so refreshing to go home, to have a home to go to, and somebody to go to in that home, because there you have a tiny success. You have built up that home; it represents your savings, perhaps, if you are a working-man, or your success in winning somebody's affections. That success is linked up with joy. Recreation re-creates us because it enables us to succeed when we have felt ourselves failures, or at any rate postponers. We are working for some "far-off divine event to which" (we hope) "creation moves," but moves very slowly. In recreation, in art, in beauty, in going to the theatre, dancing, music, we get at something where we can succeed, success by performance or by enjoyment and so be refreshed.[Pg 122] One of the things that is always exasperating to students of industrial fatigue is that a girl who is nearly dead from working in a factory is sometimes made totally fresh by dancing. After being tired out by standing, she gets rested by dancing. It is certainly puzzling but not inconceivable if we take into account the psychical factors, which we are so apt to ignore because they are invisible.
One of the things we want in rest is success where we have felt ourselves failures, achievement where we have felt we were postponing, trying to make goods which we never see finished, of which we do only a little piece. To balance all that, we want achievement, success, finish, the present delivery of something that is enjoyed now, of home, affection, or beauty.
From another point of view, a test of rest is forgetfulness. Forgetfulness ought to be achieved in our recreation and our time off. When people ask, "What form of exercise shall I take?" we have to bear in mind that the form of exercise which is most valuable is that which makes us forget. The easiest form of exercise, and the least valuable, usually, is walking. Many people carry on while walking just the same train of thought that has tired them. If so the walk is nearly useless. For other people the act of walking is different enough from what they do, so that it will break the continuity of thought and achieve forgetfulness and rest. Well-to-do people who can run an automobile usually can forget. That[Pg 123] has been a little good that has come out of the many evils of the automobile.
One of the good signs in modern education is that our old-fashioned gymnasiums are being stripped bare, the apparatus "scrapped," in order to give place to play a game. Playing a game gives us present joy, the first thing we want in recreation; and in the second place, it makes us forget.
I have spoken of rest through change of work. But the change ought to be such as sets free imprisoned, unused faculties that find no outlet in our daily work. It may be that marriages are made in heaven, but the marriage of a man to his job is very seldom made in heaven, and so mismating is common. The whole human race is too big for its jobs. The industrial system is altogether too small to fit us;—a large part of our powers remain unused. Therefore, the purpose of our time for rest and recreation, our evenings and our Sundays, should be to even up that balance, to use the part of us that is not used at other times. Sunday ought to be a family day, just because in the working world people do not see much of their families during the week; it ought to be a day in the country because we have organized these things called cities and live in them during the week. It ought to be a day of worship because we forget our religion so much in the week's work. Everything that we do on Sundays ought to be an evening-up of what gets crowded out of our week-day lives.
The English tests of fatigue are nowhere near being applied yet in America or anywhere else as we hope some day they will be, to solve this tremendous problem of industrial fatigue and industrial disease. In some of the ammunition works in England[3] they took a body of people of approximately the same age and sex, living under the same conditions approximately, doing the same work. They changed the working hours of one set and left the other set unchanged as a "control." In any scientific test we have to have what we call a "control," something that enables us to compare the changes that we bring about experimentally with the unchanged state of things.
(a) In one room the hours of labor were left unmodified, in the other modified, first increased, then decreased. They made interesting experiments to see whether a man produced as much output, in eight hours as he could in ten; they showed that he could produce as much in the shorter time as he could in the longer time, presumably because he was less tired, less bored, less strained. They made a further cut and found that then he did not produce as much. There is a limit, therefore. He could not probably produce as much in four as in eight hours.
Then they experimented on continuity and [Pg 125]discontinuity of work—whether a person could produce as much or more in five continuous hours as in two batches of two and a half hours with rest in between. They found that the shorter periods did distinctly better.
Output, then, was the first rough, but still serviceable, test that they used in relation to fatigue.
(b) Next they recorded the general look and feeling of the men as the foreman and other interested people could size it up—the look of listlessness, of boredness, of fatigue in the working-man when they varied the hours and continuity of work in the ways that I have spoken of.
(c) Next they took the amount of illness, of time off, away from work, as a measure of fatigue, and it was very definitely shown that with a diminished number of hours the number of sicknesses of all kinds, such as colds, were diminished, illustrating the point that I made a moment ago,—that accumulated fatigue diminishes our resistance to infection.
(d) Finally, they made some physiological tests of powers of sight, quickness of answer, etc., after fatigue, and showed that a man was less keen in his senses, less capable of accurate response, after a certain number of hours' work than before, and that fatigue could to a certain extent be measured in that way.
All these tests of fatigue can be applied in our lives and in the lives of people we are trying to help in[Pg 126] social work. We have to take account of the number of hours, the possible breaks, intervals, that can be made in otherwise continuous labor. Many people can get on very well if they break the day into manageable fragments. We must also take account of the effect of fatigue in producing infectious disease, of the general look of the person, and of such little physiological lapses as I have spoken of, weakened attention, the capacity for forgetting names, and mental numbness or the sense that things are unreal.
In dispensary work, when we try to give up the use of particular medicines which are useless (as contrasted with the medicines that are useful), one of the chief things to put in their place is the study of fatigue and of the methods for resting our patients. We cannot make the social work of a medical-social clinic successful unless, whenever we take away something which we know to be a fraud and an untruth, we put something else in its place. It is for that reason that I have devoted so much space to the subject of fatigue and rest.
[3] See Health of Munition Workers Committee. Final Report, Industrial Health and Efficiency. (London, 1918.)
Fatigue is a matter that seems to me of particular importance in social work for two reasons: first, because it concerns the visitor's own work and the way she does it; and second, because it concerns the troubles of a large proportion of all patients. The ultimate diagnosis, if we could make it, in probably half of all the people who come to a general clinic, is fatigue of some form, falling upon the weakest organ or function.
I want to connect this subject of fatigue with one of the policies which should govern medical-social work, namely, that we should be honest both in diagnosis and in treatment. That is a policy for which I have struggled and fought for a long time, but which we are still far from attaining. We have not yet an honest practice of medicine on any large scale, a frank declaration to patients of what ails them, how they may avoid its recurrence and so avoid coming to the doctor again. In the American Red Cross Dispensaries in France we tried to pursue the policy of honesty in diagnosis and treatment. We were told by wise people at the beginning that it would not work there, that with French patients it would not do to explain carefully and honestly[Pg 128] what was the matter or to refuse to give them drugs when we knew that drugs were no use. But one of the pleasantest experiences of our war work was to find that this warning was not true. We used the truth exclusively and successfully. Our success seemed to me natural because on the whole the French are the most intelligent race that I have ever come in contact with. Hence they took to this particular part of our policy even better than people take to it in America.
That policy links itself up with the management of diseased states due to fatigue and with the explanation of how to prevent getting into poor condition again. In newspaper advertisements and advertisements in the street-cars, it is the fashion to state that a given remedy, a given panacea, "will cure you in spite of yourself." That is exactly what the patient wants. He wants to be put in perfect condition by the first of March, we will say. Inquiring into his present distress we almost always find that he has been violating in some obvious way some hygienic law. But he wants to be cured without reform, in spite of persisting in his bad habits of eating, drinking, sleeping, working, worrying—to be cured by means of miraculous interference which he thinks a drug will produce. He wants a tonic, and he often does not take it well when you tell him that there is no such thing as a tonic. There never was and presumably there never will be such a thing. A tonic is a thing which does nature's work, which gives us in a[Pg 129] moment artificially what food and sleep and air and rest and recreation slowly and naturally give us. There is no such thing. The nearest thing we have to a tonic—a thing which we sometimes give when people ask for a tonic—is an appetizer. There are drugs which will help a little in giving an appetite. But only to that extent can we give a tonic. But this is not what people want to be told. They want something to take away "that tired feeling." There is one thing (as unfortunately people discover only too soon) which will take away the feeling of fatigue—alcohol. That is why people take it, because alcohol, a narcotic as it always is, dulls the sense of fatigue, and allows people to go ahead straining themselves, when they ought to have been compelled by nature's warnings to stop. Perhaps it is because so many "tonics" contain alcohol that people have not got over the idea that there is any such thing as a real tonic, which abolishes, not the awareness of fatigue, but the fatigue itself.
The promise to "cure you in spite of yourself," then, is the bait by which the quack attempts to tempt us, and his lie shows exactly the line in which we, as social workers or as physicians in a dispensary, ought to labor. We must try to show people that fatigue, strain, worry, and other natural causes have brought them where they are, and that there is no possible getting out of their troubles without following the line of common sense. No drug, no tonic, can take the place of obedience to common sense.
We see people who have varicose veins, for instance, and whose work forces them to stand a great deal on their feet. They often come to us hoping to get cured in spite of the fact that they are standing all the time, and inviting the force of gravity to produce stagnation of blood in their legs. In advising such people we have two courses open to us, quite characteristic of the courses which may be followed in all such matters:
1. We can say, "Well, I understand that you really cannot arrange to get off your feet. All right. The varicose veins will not get cured. But, on the other hand, they are not very dangerous; the consequences of neglecting them are not very serious. The number of cases when an over-distended vein breaks and causes a serious hemorrhage is not great. The chances of ulcer are not very great." Force the patient to face the danger and realize what will happen, in case he does not make any change in his habits; it is then perfectly proper in certain cases for a person to go on violating hygienic common sense provided he has counted the cost and faced it.
Each of us comes to some point in his life when he makes up his mind that for a good cause he will smash his health. I do not believe in the worship of health. There are many better things in the world than health. Many a man makes up his mind to do what he knows will probably cost him a number of weeks or a year of his life. That is all right; only we must face it, in peace as well as in war.
Or (2), when people come to us for the relief of skin abscesses, boils, and demand some drug which will cure these abscesses, we must ask the important questions, Whence did you get them? Why did they come? Presumably not because the patient has failed to take a drug. We must find the fault in hygiene, generally constipation or overwork, or lack of sleep, causing a lowering of the body's vital resistance, whereby the germs, the staphylococci, which are deep in our skin and never to be rubbed off by any washing or sterilization, begin to multiply. The soil has become such that they can multiply.
I have tried to suggest the importance that we ought to attribute to soil as well as to seed. Modern doctrine about the cause of disease has called our attention to the tremendous importance of seed, that is, germs, bacteria. But on the whole, if one had to say which is the most important single factor in disease, he would have to say, not the seed, but the soil. Take the tuberculosis bacillus, for instance. I do not think it is an exaggeration to say that nine tenths of all persons have had tuberculosis, usually in a harmless form, because the soil has been stony and so has killed off the bacteria. You know that the figures obtained by means of tests with the Von Pirquet reaction in almost any city or town, show that ninety per cent of the children of twelve years of age and on, have a positive reaction to this test for infection by tuberculosis. They have the tuberculosis bacillus somewhere in their bodies. That does not mean that[Pg 132] they have the disease, but they have the bacteria in their bodies, and mostly in the process of being killed off by the tissues of the body which resist this infection.
One of the reasons why I go into detail here about the changes that take place in the body through disease, is to make social workers feel as strongly as I feel, and convey to patients as strongly as I try to convey it, what nature does in curing disease. We have read of people who were walled up in masonry by way of vengeance, and left to die in a casket of stone. That is what nature does to a bacillus, literally walls it off in stone. After death when the pathologist's knife cuts down into a lung, the knife is sometimes broken by coming upon what feels like a stone. A stone it really is, a deposit of lime salts in the tissue, around a nest of tubercle bacilli. If one cuts such a stone in two, one finds in the centre bacilli often still alive and perfectly capable of increase, but harmless to the body because nature has built this wall around them. I do not think one can get the full force of this fact until one has seen it. That is one of the long list of things that the body is constantly doing in this process of resisting disease, and doing more intelligently than we can.
Since, then, it is chiefly the soil, the vital condition of our tissues, which resists disease, we must do our part in making that soil good or bad for disease. That is why our hygiene, our obedience to the individual laws of our own experience, which show us[Pg 133] how we can keep well and how we get sick, must be learned and taught by every one of us so far as we can in such a place as a dispensary or a patient's home.
For example: disease is often produced by lack of sleep; hence it is of central importance to teach people how to sleep. Excluding organic disease in the causation of most cases of sleeplessness—for most people suffering from insomnia do not have organic disease—one can say this: Insomnia usually depends on something wrong in the patient's day. The state of the night depends on the state of the day. If the day has been free not merely from gross sin, but free from hygienic blunder, then the night will go somewhere nearly right. If the day has been filled with concentrated work in which the mind has been wholly upon the thing it has in hand, if there have been no elements of strain through distraction or worry, causing double currents in the mind, then when night comes one can turn the mind off and go to sleep. On the other hand, the mind which has been intent half on its own job and half on its own worries, never wholly "turned on" during the day, cannot be "turned off" at night. Any physician or any patient succeeds in curing insomnia who succeeds in finding out what is wrong in the way the sleepless person lives, and how it can be corrected.
But most people want to go on living in just the same stupid way and yet to get rid of the sleeplessness "in spite of themselves." The obvious way is to[Pg 134] take a drug that for a while will stop insomnia even when life goes on as before. There are many drugs that will give sleep, but there are no harmless drugs that give sleep—none. Physicians receive about once a year advertisements of a drug for sleep which is "wholly without ill effects," but I do not think it shows undue skepticism or dogmatism to say that those drugs never do what they say, and never will. Sleep being a natural process, anything that forces it upon us hardly can be free from ill effects. Hence the first thing in attacking a case of insomnia is to say, "Never take a drug again." Natural processes whereby fatigue accumulates and puts us to sleep do not go on rightly if we are being artificially driven into sleep by a drug.
One gives drugs for sleeplessness rightly when there is some rare and special reason for being awake, some catastrophic reason which will never occur again. This exemplifies the principle which I have tried to emphasize throughout this book. We may give money for some catastrophic cause which puts the person down and out, and will not occur again. So we give a drug for sleeplessness if there has been some special thing to interfere with sleep—if, for instance, you have been talking very hard with a friend and you know by your own feelings that your mind will not stop that night. Then you may perfectly properly take a drug to put you to sleep, knowing that there is no reason to suppose that such a talk will occur again in the near future. Knowing[Pg 135] this, you do not need to waste that night. You take the drug. But it is only in rare catastrophic moments that one can be cured in spite of one's self, any more than one can give or take money safely.
It is the same in the matter of constipation. The first thing to make clear to a patient is that drugs must be abandoned before he can ever teach his bowels to behave as they should. But it is a great deal of trouble to do that, and because people shirk that trouble, and want to be "cured in spite of themselves," they come to a doctor to be cured by drugs. Alas, he is often weak enough to give them what they seek!
I have tried to make this drug-fearing practice one of the policies that honest medicine must always stand for, because it seems to me that when the doctor allows himself to be tempted into behaving as a considerable number of his profession do—that is, into giving people what they ask for—he very soon loses his ideals, gives things that he knows more and more clearly that he has no right to give, and goes downhill. Social assistants must help the doctor to avoid this disaster. They can do so by helping him to teach the truth.
I want to deal a little further with some examples of what nature does in the way of warding off disease. For a large part of what we call disease, and what we feel in ourselves as disease, is not the attack of the enemy, but is our defence against the enemy.
Take, for instance, inflammation. When germs are beneath the skin, one finds redness, swelling, heat, pain, as the symptoms of inflammation. What does that mean? It is all like the defences which were set up round Paris when the Germans were coming there, or that are set up anywhere when one is getting ready to repel attack. The inflamed finger gets red because a great deal of blood is going there. The blood cells, especially the white cells of the blood, are coming there to defend. The finger gets red for the same reason that the railroads get congested in time of battle, namely, because so many soldiers are being carried there for defence. The finger gets swollen because so many cells and fluids are coming to attack the enemy; it is their crowding outside the blood vessels that makes the swelling. There is heat in the finger because there is more blood in the part and therefore the part is hotter. There is pain because with the extra accumulation of defenders there is a squeezing of the little nerve terminations there. When a lot of soldiers are suddenly quartered, billeted in a town, it is a painful process. There is pain in having defence come to your city. There is pain in having defence come to your finger.
All of these symptoms, which we are apt to hate and to think of as misfortunes, we should realize are the thing which saves us from very serious illness. Suppose these things did not happen. Following out the metaphor, if it were not for these defences the[Pg 137] enemy would penetrate into the whole body and we should have blood poisoning. It is because this local heat, redness, swelling, pain, appears at the point where bacteria are attacking us, that they do not penetrate the whole body with a septicemia, which is one of the most dangerous of all diseases. So while suffering what we must suffer, we ought to be glad of all that nature is doing, because if she neglected it the consequences would be very serious to us.
But we may ask, "If this is true, where do medicine and surgery come in? Why do they ever interfere if nature is so very wise?" Because nature overdoes the thing every now and then. Nature is first enormously wise and then a little blind. In another example I can bring this out a little better. You have sprained your knee and the knee gets very stiff. That in itself is good; it is a defencive reaction. The stiffness is like a splint. The knee ought to be kept quiet. So far so good. But nature overdoes the thing. The knee ought to be kept quiet, but for how long? We will say three days more or less, according to the severity of the injury. Then you have to fight nature which stiffens the knee too much. You have to fight it by the use of the knee, by walking or by massage, which is not, however, so good as walking. If we respect blindly what nature does in stiffening the knee even to the exclusion of nature's other functions, such as walking, then the knee will get worse. One of the greatest improvements in the modern treatment of sprains, is that we no longer keep the[Pg 138] patient in bed and put plaster of Paris on, which makes the sprain last for months sometimes; but we let him walk at once on the sprained ankle, whereby the attempts of nature to cure by stiffening are not carried too far.
Another example of how nature overdoes things is in the formation of scar tissue. If a scar did not form to close the wound, the wound would remain open. Hence the scar is vastly better than nothing. But scar tissue is never as good as the original tissue. One of its known ill results is contraction, so that a scar on the hand or on the neck often draws the part out of place. Then we have to fight nature. We have to go against the workings of nature by surgery, in order to get the person right.
In suppurative disease, such as appendicitis, it is often difficult to decide when nature is doing better than we can do, and when we can do better than nature. The appendix is a hollow tube the size of one's little finger, and hangs off from one part of the large bowel. When it gets inflamed nature at once begins the defences which I have described in the lung, namely, the walling-off process, which tends to make the bacteria harmless. There is danger that they will spread from the neighborhood of the appendix and produce a very dangerous disease, general peritonitis. Hence nature begins to glue around the appendix the adjacent parts of the bowel and anything else at hand. This generally makes it harmless. Most of us physicians now believe that the great majority[Pg 139] of cases of appendicitis cure themselves, and that still more would cure themselves if given a chance. On the other hand, there are cases in which nature does not do her work rightly. Then if the surgeon did not interfere the person would die. That is why medical and surgical judgment, the particular, minute, individual study of the person from hour to hour, makes the difference between right and wrong treatment. The surgeon who operates every time he makes a diagnosis of appendicitis, or who says he will never operate, is just as wrong as the person who gives money the first time he sees a case, or who never gives money. But most surgeons are wiser than that.
I hope through these illustrations to make it clear that nature generally cures disease. When she does not, it is generally incurable. There is a small residuum left for the doctor. We have a function as physicians or nurses. We have a function, and that function is intermediate between two extremes. In disease or in other misfortune, there are three types of fortune, two extremes and a mean: (1) The people who will get out of their troubles whatever you do, get out of their misfortunes, rally to meet their griefs, pull themselves out of financial difficulties, get over their disease. Then (2) there are people on the other side, who will die whatever you do. Some cases of pneumonia, for instance, seem to be doomed from the start. It is the same with many other cases of disease and with some people's misfortunes. We have to face the fact in social work that there are[Pg 140] many people whose mental twists and agonies we cannot help in the least, and many people who will be in money difficulties as long as they live. But (3), intermediate between these two extremes—and our happiness and our success depend on our finding that group—are those cases where what we do makes the difference between success and failure. This triple division indicates a point of view which makes, not only for individual understanding of the situation, but for practical success.
Take the case of those maimed by war or accident. There are three classes of them: first, the people who will get back their jobs and get back into industry unaided; they are probably the majority. Then the people who cannot be put back by any process. Finally, there is the rather small intermediate class who, with our help, with a little extra education, with a hand in the back, will get back into work, but who never would succeed, humanly speaking, without our help.
So it is in disease. The vast majority of diseases get well without any help from anybody, and that is the thing we must teach most often and to most people, in season and out of season. In our day and generation few people get a chance of observing that fact, because somebody comes along and gives them a drug. And unless one has seen people get well without any drugs, one continues to believe that it was the last drug given that cured every case of illness one has known to get well. On the other hand, the[Pg 141] majority of illnesses that do not get well without drugs will not get well at all. I have mentioned before the figures which seem approximately true in relation to the cure of disease by drugs. Drugs will cure about six or eight diseases out of about one hundred and fifty diseases known to science. Anybody who fails to give a drug for one of those six or eight diseases is criminally negligent. We should press that drug upon the patient. I do not want anybody to think that I do not believe in drugs. I believe in them tremendously, in the particular cases where they are of use. But I do not stand for the habit of bolstering up people's beliefs that we have drugs all ready to cure most diseases.
I think the future of cure by drugs is very hopeful. I do not feel hopeless of our discovering drugs for the one hundred and forty-two out of one hundred and fifty diseases which we still cannot cure. But if we falsely suppose that we have a cure already, we do not hustle around to get it. It is not until we realize that we have not a cure already, that we do hustle around to get it. It is not until we realize that we are now very helpless in medicine that we shall labor in a way to become less so. At present the best that we can do for most patients is to explain what the trouble is, let them know what is going to happen, to preach some hygiene, and above all to make them realize that we care and suffer with them. That is the essence of medical work and of the social assistant's work in the dispensary and in the home.
Industrial disease is a phrase we have heard much in the last ten or fifteen years, meaning that diseases are caused—some of them—by the conditions to which people are exposed in industry. A great deal of indignation, some of it fruitful, much of it harmful, has been aroused against employers and against the whole system of industry—because we have now recognized the fact of industrial disease. Employers in the past have been more interested in their machinery than in their human help. That is not only bad, but very stupid. Most of us believe that because it is stupid it is not likely to continue indefinitely.
But aside from all these matters of controversy, there is one important distinction to make at the start. (a) Industrial disease in the narrow, strict sense, i.e., something produced by the industry, something which would never have occurred in any form if the person had not been in that industry. (b) Disease affected, modified, in some way by industry, but due in part to other causes.
There are very few clear-cut and common industrial diseases. Lead poisoning is almost the only one. Disease due to the inhalation or swallowing of other poisons and the penetration through the skin or irritation of the skin by definite poisons are real dangers, but not common. More common, more difficult to deal with, and therefore more within the province of the social worker, are the diseases in which [Pg 143]industry is only one factor in the complicated skein of causes. Take such matters as exposure to unusual heat or cold, unusual humidity or dryness in industry—very common conditions; or still more, exposure to unusual strain and hurry from what we call "speeding-up" or from the piece-work system. I do not think there is any good evidence that those things produce any single disease. I think there is excellent evidence that they often dip the scale whereby a person who has been in equilibrium, able to get along with his outside troubles, and to keep his balance, is finally knocked down into disease.
A person has tuberculosis. One of the favorite tricks of unscrupulous political orators is to say, "Look at all that tuberculosis due to the greed and the cruelty of employers!" Bad conditions of industry are doubtless a factor in the production of tuberculosis, but we must realize how many and important the other factors are. The eight or ten hours a person spends in industry is often a small factor in producing his ill health, compared to the fourteen or sixteen hours he spends outside the industry. Hence if we are to understand the diseases of workmen we must investigate these hours just as carefully as those in the factory. That is what we ordinarily omit. We find so many cases of tuberculosis in a given industry, and we say, "Ah, then, these cases are due to the hardships of that industry."
In refutation of this idea there is one more dogma packed for transportation, which I should like to[Pg 144] offer in the form of a logical fallacy which the mediæval logicians put down in Latin terms: "Post hoc, ergo propter hoc": "After this, therefore because of this." One of our duties as doctors and social workers is to combat fallacies, to teach people to think straight instead of crooked about their ill health and their other troubles. When thus occupied, a large part of our labors will consist in trying to overcome the popular fallacy quoted above. "You went into a particular industry and you had tuberculosis: therefore you had tuberculosis because you went into that industry." "You had a given disease and you took a certain remedy: you got better, therefore the remedy cured the disease." So the superstitions flourish. I do not believe it is easy for any of us to extricate ourselves from that particular fallacy, but we must try.
In industrial disease we have the causative factor of industrial hardship intimately mixed up with other factors. One of my colleagues, Dr. Roger I. Lee, of whose book I have already spoken, investigated, in our clinic at the Massachusetts General Hospital, the cases of one hundred young working-girls, factory employees, who either had tuberculosis or were suspected of tuberculosis—were in what is wrongly called the "pre-tubercular stage," when the doctor has not made up his mind whether the patient has tuberculosis or not. He studied these cases, as people ought to study them, always in proper coöperation with a social worker. He made his own careful observations in the dispensary. Then he [Pg 145]employed a social worker to study the girls in the home and outside the home, following up in their lives and personalities the tangles of disease. His total result was that he could not say in any given case that industry had produced a single one of the diseases which he found, though he was not willing to swear that it had not done so. He found that a certain number of these girls, in their perfectly natural search for recreation, were running around the streets or elsewhere until the small hours of the morning. That is an obvious factor in producing a diseased state. It is not that we want to blame people for seeking recreation; but the results cannot also serve as evidence of the harm done by industry, except in a very wide sense in which we might say that industry does harm because it does not provide for recreation, which is, I think, an extreme view.
Dr. Lee's social assistants found that a good many of these girls had no habits of eating. It was not that their habits were so bad, but that they had none of any kind. Sometimes they ate very well and sometimes they did not. Then he found, as of course one would know that he would, the psychical factors in many of these cases—their love affairs and other worries which were often much more deleterious to their health than their habits of sleep or food or even their industrial conditions.
When, therefore, one tries to consider industrial disease, one must realize how complex a thing it is, how essential it is to go beyond the inspection of the[Pg 146] factory and to study all the conditions of the lives of the people that one is concerned with.
In a big Western American town that I visited recently, where the automobile tire industry was employing some fifty thousand hands in factories, the most obvious cause for ill health was the tremendous congestion in that town, and as a result the fearful state of the available lodgings. Again most of the factory hands were foreigners; very few of them spoke English; they were wholly dislocated from normal family life, from any connection with their own countries and from their own previous interests. That is in itself a dangerous condition for hygiene as well as for morals. Factors like that must be taken account of when we want to help anybody to get free of the troubles, the fatigue or strain or debility, which we are apt to attribute to industry.
We are keen, and rightly keen, to find and to abolish poisons, such as lead, such as phosphorus, such as carbon monoxide. We ought to be keen to study poisons of that kind, and more interest has lately been concentrated upon them through war work and war industries than ever before. But there are moral poisons which we do not notice or mention. Monotony, for instance. Monotony is not altogether a horrible or hateful fact. Most of us want some monotony in our day. We want a rhythm and a certain recurrence in it, whereby our work comes to seem familiar to us and we do somewhere near the same thing each day. There is rest in that. But how much[Pg 147] we need is individual; the dose of monotony, the amount that is good for you and for me is limited. People often get too much, and when they get too much, then it is a moral poison. One of the most appalling things, I think, is its effect upon the mind. I have often wondered whether I ever had or ever would have any mind again, when I have come to the end of such a day. Any one of us, of course, can duplicate that experience, and it certainly ought to make us think hard about the lives of manual workers whose days are quite likely to be like that right along. At the end of such a monotonous day a person may be pretty reckless, may feel that he does not care what happens to him. I have met that in a great many histories. It is not so much that monotony makes machines of them as that it makes wild animals of them.
Another moral poisoning is the sense of injustice, a sense that it is not right that somebody else, whom the Lord did not make very different, has so much more of money and opportunity and happiness than the person himself has. It is altogether a secondary question to discuss whether that is true or not. I do not myself believe that the rich are any happier than the poor. On the whole, I think the evils of money are just as great as the evils of poverty. But the sense of injustice is often just as real even though the reasoning on which it is based is wrong; and the sense of injustice is a moral poison which breaks down health and spoils happiness.
Can we do anything about it? Sometimes. By going over the details of people's lives, by telling them stories of other people's lives, by confessing a great deal about our own life, we can help people to see things differently. When I was speaking of pains in the region of the heart I said that one of the most important things that one could learn is to distinguish between the pain and what we think of it. The pain often cannot be changed, but our interpretation of it often can. The patient often suffers chiefly from what he thinks of the pain, and when he knows that the pain is not due to heart disease and that he probably will live to be a hundred, that particular form of suffering leaves him. So in this matter of the sense of injustice, the causes for suffering may be unchangeable, but if we can change the patient's point of view we may help him a great deal.
A greater evil, I think, than any I have mentioned, and one that we are almost powerless to attack, is lowered sex standards, which come from the crowding of people of all ages and both sexes into industry. As in the housing problem, it is the moral rather than the physical side of crowding that is most serious.
That is why the visiting part of social work seems to me so much the most important. The important part is what we hope goes on in home visits, when the social assistant meets people where they will talk as of course they cannot talk in the dispensary.
The principles of linkage embodied in the work of the home visitor, in her cooperation with doctors and other social workers, and in good history-taking which avoids the fallacies of the catastrophic point of view, take on a little more impressiveness when we consider what a widely general law that "linking-up" law is. It is the essence of science; indeed, it is the essence of things still wider, for it is the essence of order.
There is an old phrase that "order is heaven's first law." It certainly is an impressively universal principle. How universal this linking-up process is, and how it applies to all possible situations medical and social, can be made to stick in our memories by the phrase, "In view of this, what next?" This is a prosaic and unimpressive-sounding dictum; but with some trivial and some important illustrations I can show that it is really useful.
1. A terrier dog is watching a rat-hole: in view of this, what next?—a question full of importance for the dog and for the rat.
2. A cobbler is working on his shoe: in view of what he has already done upon that shoe, what shall he do next? The value of the shoe, the value of the[Pg 152] cobbler's working time, depend upon his seeing truly, and then, in view of that vision, doing whatever is next called for by the conditions of the shoe which he is dealing with.
3. As we go down the bill of fare of a restaurant, we say, "In view of what I have eaten, what next?" Presumably there is a method, an order in our madness.
4. We may have known, in the course of our lives, a few people who, when we ask them a question, think before they answer. These are the people who habitually say to themselves, "In view of this question and of the truth which I should speak, what words should issue from my lips?"
5. The whole science of logic is the science of seeing truly: in view of certain premises, what is next? What follows and must follow, if we are to be logical.
6. Anybody who has got to a certain point in his profession says, "In view of my successes and my failures thus far, what is the next thing for me to do?" One can say the same, and I imagine that most people have often said it to themselves, in relation to friendships: in view of my present affection or dislike for that person, what next? We have come through the world's most gigantic war: in view of this, what next?
7. I tried to exemplify this principle also in our medical and social history-taking. Our histories should be orderly. There is a thing that rightly comes first and a thing that, in view of this, should come next.
8. When the musician composes or plays, he is guided in the writing-out or in the instrumental expression of his musical idea by his consciousness of the whole piece—what is done and still to be done. "In view of this whole," he asks himself, "what notes come next?"
9. When a man prays he says to himself, "In view of my sins and of God, what next?"
It appears, then, that the most trivial and the highest things that go through the human mind, if they go right, follow that formula, because it is simply a way of putting truth in order, and because order is as fundamental to a human mind that is working right and not wrong, as anything can be. The catastrophic point of view, on the other hand, is the point of view of disorder, the belief that things happen "as the result of accident," come upon us without order, were never in view beforehand, occurred for no known reason.
The principle of order is also closely knit to the principle of independence or integrity, which we want to achieve in social work when we give. Physically we want the person to be independent, not depending upon a drug, not needing to be jacked up by a stimulant, not dependent as a sick man is dependent, on nursing, special diets, and long rests. In the economic field we try to avoid making a person depend on a crutch, a support, a pension, which atrophies his economic powers instead of developing them. At least we desire not to weaken them. We[Pg 154] want to give and build, to give something that will go on by itself to make him independent of us.
But independence is not altogether a good phrase. No human being, linked up in a world-order as we all are, is ever independent. What we mean by that not altogether satisfactory phrase is that we want to be dependent only upon something that we can rely upon, only upon permanent, central, orderly powers of the universe. Physical independence does not mean independence of food or of rest; one soon comes to the end of his tether if one attempts such independence. Dependence means hanging. We must all hang. But we want to hang upon something that will not let us down, upon food, air, warmth, exercise, rest, such as are always available in an orderly life, or should be.
So in the economic field, no man is economically independent or ever will be. But we want his powers knit into an orderly system that is not dependent upon a protective tariff, on somebody's whim who pays his salary, or on political "pull." We want people to be independent in the sense that they get their living by connection with a well-ordered economic system. Even then, of course, we are not independent. A planet may run into us and we shall then be wrecked in spite of the fact that we are not dependent upon charity or a protective tariff.
Obviously literal independence is also impossible in moral and personal relations. We are never independent of society, never capable of going it alone.[Pg 155] The only question is, On what do we depend? Do we depend on one person, or one particular kind of entertainment or stimulation? Or can we find our food in any of a vast number of places and persons which in the natural order are fairly sure to be available? Or in the absence of all finite persons can we find our food in God? That is the fundamental question in relation to personal independence. Its answer states the degree in which our personal history is orderly and not catastrophic.
If one is habitually trying to order his own life in this way, the principles by which he lives will guide his attempts at social treatment and give him continuity and steadiness.
All our diagnostic duties, whether as doctor or social worker, are part of our search for truth, physical, economic, mental, and moral, as the basis for medical-social treatment. I have used again and again the figure of chains, each of them starting with the individual's present misfortune, need, or sorrow, as a central link, and radiating in different directions as we trace out the relevant physical and economic facts, the chain of the patient's relationships to family and friends, some of whom he is apt to forget, and finally the chain of mental and moral causes which lead up to the present moment. I believe in that method with all my heart. I also believe it can be employed so one-sidedly, so exclusively, as to[Pg 156] spoil social work. The criticism of social work which recurs most often and most justly, I think, is that we are not human enough, not big enough people to do social work, that we have not vision, that we get into mechanical and routine methods which spoil the whole adventure. I know that this is true. We fail because it is difficult for us to drive in span two strongly contrasted ideals only one of which I have yet laid great stress on. Truth and the following out of the links of truth, physical, economic, etc., is a process which we might call looking for the background of the fact that presents itself close to you. We need to see that background. We must not get our perspective distorted. It is the doctor's commonest fault, that he sees only the disease that is just now before him, and nothing of its "background," economic, mental, or moral. Hence he does not make a fundamental diagnosis or prescribe fundamental treatment.
We need in our dispensary work to find truth. Yes; but we need to find joy also in our work; we need to see the foreground. We do not want to have attached to us the stigma and the weakness which we think of in professional work. We are accustomed to believe that professional philanthropists find no joy in their work, which they do as a matter of routine, for pay, without vision and without a sense of the unexpected and momentary values which are precious.
The process of tracing chains, of looking off and away from the patient's present pain, sorrow or [Pg 157]poverty for its causes and relations, tends to make us look over the head of the present fact. We all know people who always look over our heads when they talk, and we know how little they get into touch with us. We must not stare into the physical, economic, or mental background so constantly or so fixedly that we cannot see the present fact before us. That is preoccupation. I have often accused myself and my assistants of going about their work with a care-worn air, because we are thinking so much of the fine, helpful plans which we are making and the truths which we are going to discover, or of bothersome details which we have not got round to finishing up. But we shall do no good in the long run unless we enjoy our work. There may be some professions where a man or a woman can be of use who does not draw joy from work, but certainly social work is not such a profession. We have with Stevenson the duty of happiness:
—What are we to do? We must wake up—
We are not awake. We are half asleep, dreaming over our plans, our worries, our visions. That is why we are preoccupied; looking over the head of the immediate fact, we miss the amazing beauty of face, word, and character tempered and enhanced by suffering.
Much as I hate the fault of never going beyond the fact that we see before us, I hate just as much the opposite error of not getting the full vision of the foreground. We ought always to be able to feel, at the end of any single home visit, that we have done something, accomplished something. Well: one of the things that we must make every effort to accomplish, and to feel ourselves a failure if we have not accomplished, is to find and to give pleasure, to enjoy ourselves, and if possible to give a little courage. The little embellishments of our work, the smile, the tone of voice, the jokes and courtesies of our fleeting contacts with individual patients, should be just as precious to us as any of our far-reaching plans and deep-plunging attempts to study into cases. How poignantly, how intensely Christ put this to us in saying that inasmuch as we did any good thing unto the least of his brethren we did it unto Him! I believe that He meant this not only of human beings, but of days, of moments. The least of these opportunities is infinitely precious and we are making a grievous mistake if we do not take it so.
I have known a few social assistants who make each little deed and each little moment a perfect work of art in itself. Art at its best this work is. It was my greatest single experience in 1917-18 to admire the French art for finding joy in little things, and of making beauty in little things. I asked recently a group of Americans what they had found the most admirable in their contact with the French[Pg 159] people. Everybody present had had the experience of finding in his own hotel or pension, a femme de chambre or some other domestic who, though starting to work at five o'clock in the morning and working until late at night, nevertheless always kept joy or the appearance of joy in her work. On the first night that I was in Paris I went with a friend to dine at a restaurant very late. There was but one waitress, who had nearly finished serving an enormous number of people. She ought to have been near the end of her day's work, which our arrival prolonged still more. But I never can forget the welcoming look and tone with which she said to us, "Now I shall have the pleasure of serving you."
We need the artistic spirit, the spirit of beauty in social work. It is not opposed to, but surely very different from, the spirit of science which I have been emphasizing in the earlier chapters of this book. I must confess my impression that, on the whole, thus far, social work has been ugly. Social workers have not kept beauty and the sense of beauty in the foreground of their work. Beauty and joy always tend to drop out in social work, but this must not be. There is an old story of an inspired social assistant in Boston who had been working for a long time with a needy family who were at that time much discouraged. One day she had an idea: "What that woman needs is a blue dress. She is extraordinarily fond of that color. She has not had a new dress for a long time." And it was true. She was given a[Pg 160] blue dress, and the history of that family afterwards began to show signs of the sort of change and upward constructive effort which had long been lacking. We cannot neglect that sort of thing, slight or sentimental though it may seem.
I remember another family in which flowers, and money spent on giving the children a chance to grow flowers, played a beneficent rôle; and still another discouraged family in which a canary bird seemed an essential element in the social work done.
There is something certainly very divine about the present moment. We shall never have it again. We are apt to think that next year we shall do something great. Then, we think, at last we shall gather up all the forces of our soul and do something worthy. But I do not believe we can tell ourselves too often in social work that now is the time, and that the opportunity of the present moment is priceless.
Hence, after trying to exemplify the backgrounds which we ought to seek out when a fellow being comes to us in trouble, I must now correct that overemphasis by paying homage to that state of mind which sees foregrounds. What we want is presence of mind—a very familiar and hackneyed phrase, but one which may grow precious to us after analysis. My complaint against the preoccupied, solemn look in the social worker's face is that the person's mind is not there with his fellow beings; it is aloof with his own troubles. He is not "in it," not all there on the[Pg 161] spot. The necessity of joy in one's work, and the necessity of seeing the momentary and infinitely precious opportunities, come to the same thing. If you are "in it," you get your chance. To have sufficient presence of mind to seize one's chance is surely the crucial act in social work or anywhere else, for that chance does not recur.
But presence of mind connects itself with an interesting fact in our grammar about the present tense. The present tense, in contrast with past and future tenses, expresses presence of mind, attention to the wonder of the moment, the opportunity of the moment. But it also expresses a wholly different thing, namely, the eternal. Some languages have an eternal tense and use it about facts that are not present or past or future. We use the present tense for the eternal. Two and two make four. When? Well, not of course at ten minutes before twelve on the 11th of November, 1918, more than at any other time. We might just as well use the future tense. Two and two always will make four. But by a peculiar accident we have hitched on to one tense the whole body of eternal truth. Why did we hitch the eternal to the present rather than to the past or to the future? Because anything that we really grasp now, as truth or as joy or as beauty, anything that we really comprehend, can be eternally ours. In the physical sense it is so. The electric light that I am now looking at and which might be turned off at any moment, is eternal, for its vibrations are travelling off through[Pg 162] space and always will be. The fact that those vibrations are going off through the ether is ever the same.
Any present fact, then, so far as we realize its truth or its wonder, is eternally ours. Hence presence of mind is the quality needed in social work to balance the scientific habit which looks for past and future, for what is not present. Investigation and history-taking must always be completed by appreciation, the other half of our mental life, which is acutely conscious of the present and therefore can be conscious of eternity.
I hope I have not put the contrast of science and art in social work so sharply that it seems as if one must take one extreme or the other. I do not feel any such contradiction. I believe that we can get courage for the long, discouraging search for causes out of the present joy which we find in speaking and listening to a person now. On the other hand, these momentary contacts are thin, capricious, and insufficient if we are not also planning some solid progress which will give us something to show for it at the end of a day or a year. One of the dreary things in human beings' work is that sometimes, after a month or a year, they cannot see that they have accomplished anything. It is all a mass of details. I remember a very marvellous social worker saying to me, "I do not want to die thinking that I have never done anything but case work." Case work seems to me as great a thing as any one can do. One might as[Pg 163] well say, "I have never done anything but miracles." But I know what she meant. She meant that through case work she wanted to feel that there was a thread of continuity which ought to be science or character or friendship, a thread whereon something accumulates. We ought each year to be able to say and to write what we have learned, or given.
Social treatment is giving and constructing. We want to give
Pleasure
Beauty
Money
Information
Education
Courage
and to help build the power to get more of each.
1. Pleasure. As we want to find pleasure in our work, we surely want to try, so far as our human capacities allow us, to give pleasure, to make people feel comfortable, to be always so polite to them and finally so fond of them, that they will enjoy the momentary contact no matter what it is about. As I look back over medical work of twenty-five years, I should say that in most of my cases I have failed from the medical point of view. Yet in a great many of those failures I can see some redeeming feature because of the friendships that the patient and I built while I was failing in my medical job.
Such a blending of success and failure is the rule, not the exception. We make elaborate social plans, but we know that many of them are going to fail. It is humanly impossible that they should not fail. But they will not be flat failures if along the way we have tried to treat people, not as they deserve, but a great deal better.[4]
But when we give pleasure we must try to provide that the stock shall go on. We want to try to build in and with the person some capacity to get that pleasure for himself after we have gone out of his life. This is just as true of course of Beauty which we surely want to try to bring into our patients' lives, and which is one of the things that redeems our failures on the other side of social work. Even people who are dying sometimes can get great enjoyment of beauty.
2. Money is, I suppose, on the whole, the thing we are asked for directly or indirectly most often in social work. If we are not doing direct medical work, if we are not giving a direct medical relief or trying to, we are more than likely to be asked for help in the way of money, clothes, food, or rent. Surely no one works long in social work who does not find the right place to give money. But I have to go back to the figure already used, the parallelism of money and morphine. A person comes to us with pain and[Pg 165] begs for money or its equivalent—direct, immediate relief. What makes us hesitate in the one case is the same that makes us hesitate in the other. We may relieve, yes; but have we constructed? In the long run we must both construct and give, else our giving may be useless or harmful.
When can we give money without doing harm?
In a general way, when it is not going to lead to the repetition of the same demand. When are we perfectly sure that we may safely give morphine? In gall-stone colic. For it may be weeks, months, years, perhaps, before there will be another such attack of colic. We give morphine once only. The person gets over the attack, and does not want morphine again for months or years. But if the patient's pain is chronic or likely to recur soon and frequently, it is cruel to give morphine, because soon the patient will have all that pain again, and more—the pain which is produced by morphine after it has been taken a little while. We never can tell that the pain suffered is not wholly due to morphine. So the person's trouble after we have given money may be due to the money itself, ill used. We should be able to say, after a careful, though not care-worn study of the case, that we know the patient's pecuniary need is not going to recur, because we are not dealing with a chronic difficulty like extravagance or alcoholism, which will recur and cannot be checked by money.
3. On the whole, the safest form of giving that I know, that which is surest to perpetuate itself, to be[Pg 166] planted like a seed and go on without our having to stand by it, is giving information—a cold-sounding thing, but sometimes very useful. One difference between the social worker and the person for whom she works ought to be that the social worker has had more education, more freedom, more friends, more opportunity to look around the world and see resources. Hence, when, for instance, she comes to find a job for a man, the social worker, because of the perfectly undeserved blessings that she happens to have, ought to be in a position to give information that is of value.
One of the most precious kinds of information is information how to secure more information. The difference between uneducated people and those whom we call educated, is not that the latter know very much, but that if they do not know something they know how to go to one who does. The uneducated person is helpless to improve his education. He does not know and cannot find out how to look up a subject.
I have distinguished information from education. Information as such never changes character in my opinion. This subject has been discussed in recent years in connection with what some call quite falsely sex hygiene. Information biological, pathological, physiological, talks about health and disease, never kept any man or woman straight morally. It never changes character. So our public school education sometimes represents only information,[Pg 167] only the facts, not the meaning, the interpretation, the use of those facts. Hence the public school is justly open to the criticism brought upon it by those who say that it does a child no lasting good to know facts. It may make him clever and so able (like German science in war) to do more harm than if he knew less.
But when we give education—for example, hygienic or economic education—we give something else than information. Education is that which, by reason of practice, by doing something again and again, and doing it if possible in the presence of a good model (living or dead, book or person), changes our character and our habits, as the use of a muscle changes the muscle. A person learns to write. That is not merely information—he has learned to do something. Learning to swim is not information. We learn it by practice, by doing it, and by the imitation of good models. How does one learn to think? By doing the thing, and if there is any model in sight, by trying to imitate that model.
4. Education is what social workers try to give most often, most consciously, over the longest time, and sometimes with the greatest results. We try to give people hygienic education. We try to give, not merely hygienic information, but motives fit to bring about a change in habits, a wholly different thing, and one which may be of signal value. We try to teach self-control, the control of sleep, the control of emotion, the control of appetite. It is hard, but it can be[Pg 168] done by prolonged effort, under such influences as give us courage to work at it. We try to give economic education, the power of foreseeing what is going to happen by reason of what has happened before. People are extraordinarily prone to forget things which they do not want to remember. We may help people by economic education, to economic foresight, to economic organization of their resources by practice, and by going over with them the cases of other people who have won out in similar difficulties.
5. Anybody who does much talking is asked a good many times, "Won't you please come round this evening and just give us a little inspiration?" There is no request that I look on more sadly, more wistfully, than I do on that. I know how little good such "inspiration" usually is because it can be given the same way as money or morphine can be given. Inspiration or courage means emotion of some kind. Nobody believes in emotion more than I do. I believe the greatest life is the life that feels the most, enjoys the most, suffers the most. But emotion is one of the most transient and unreliable of states. One may be in a most exalted and courageous state of mind at the end of a lecture, and a few hours later be as weak as an invalid, because, though courage has come, it is courage which does not provide for its reënforcement, for a new supply. We never give people help that has any permanence except when we give them reality. We try at first to help people[Pg 169] in their woes through our own personalities. But we are not strong enough to keep anybody else afloat. We have to transmit something greater than ourselves, if possible to bring people in touch with a life-preserver that will be there after we are gone.
I suppose that when we can teach people to work and give them something they can practise all their lives and get joy out of, when we teach people to play, to deal rightly with their affections, and to worship, we have given realities permanently buoyant.
Our social history cards at the Red Cross Refugees' Dispensary in Paris had a great many blanks on them, which represented the blanks in our knowledge of the patients and the defects of our social work. We rarely entered deeply into our patients' lives in relation to their education, family life, recreation, religion. In our work at that Dispensary we dealt chiefly with medical facts and economic facts. To go thus far and no farther cannot satisfy many nor remake lives. That Dispensary was open but a few months and within that time, of course, nobody could expect us to enter into intimate relations with a human being's life. But if we were to work in any Dispensary for years and still not one of those cards had any note about the patient's education, recreation, family relationships, and religion, I should feel that we had failed. I should feel not only that we had done superficial work (that is often inevitable), but that we had done nothing but superficial work, which is not satisfactory.
It is because we want to give people the best, not that we have but that the world contains, that we should have spaces on our social history card for notes about those things which we believe are fundamental in our own lives and which we want therefore to see constructed or increased in somebody else.
Social treatment, then, is chiefly, the giving and building of health, pleasure, money, beauty, information, education, courage. It is not because we have such a tremendous stock of those goods to give away, but because we know that we must somehow help a person to self-help in those directions or else be superficial, that I have phrased social treatment in those terms.
One of the simple and yet honestly useful things that we can do in social work is to give a man a hearing. Often he will solve his own problems with the aid of a little information from one whom he trusts and has talked things out with. But this implies unusual powers of listening on the social worker's part. It implies what Mr. R. H. Schauffler calls creative listening. Some of the most delightful friendships are those one makes through a magazine. In the "Atlantic Monthly" some years ago I saw an article on playing string quartets by a man whom I had never heard of, Mr. Robert H. Schauffler. Mr. Schauffler's writings, which I came to know through this article, contain many interesting points, but nothing so [Pg 171]valuable to me as the essay on "The Creative Listener."[5] It was founded upon an autobiographical incident. As a musical amateur he used to attend orchestral concerts in what was then his home city, Chicago. He used to go with a certain group of friends, his brother and others, who liked to sit together because they found that in this way they enjoyed the music more. Ordinarily they were very regular in their attendance. But one evening for some reason they had to miss the concert, and then it came to their knowledge that the orchestra had felt their absence very much, and really could not play their best without them. This is true. There are people whose attention makes us play or speak or act better than we could otherwise. We have known it in friendship We all know that some people when we talk with them, make us feel as if we really were worth something, had some ideas. Others are destructive listeners who make us feel as if we had no ideas; our personality seems destroyed.
I think it is perfectly within the province of any of us to make himself more of a creative listener than he has been before. For creative listening is due in part to the intensity of our sympathy, the whole-heartedness with which for the time being we give ourselves to the person we are with.
Under favorable conditions the power of the creative listener to enlarge and to remake a personality[Pg 172] is not capable of limit. The people whom I most often help are the people for whom I do nothing. They tell their tale, spread it all out before me; then they see the solution themselves. Just to state our difficulties clearly to another person who will listen not merely sympathetically but creatively, and with resistance as well as furtherance, is of value. With certain people we run against a stone wall every now and then, even though they are only listening silently. This is right and helpful. The right kind of listening is sympathetic when it ought to be and dissenting when it ought to be.
We help people out of trouble in other ways also; often by bringing new facts. A person tells us about his difficulties at work. He sees it perhaps more clearly after he has talked about it. But he may not know some facts that we know, and therefore we may be able to help in some ways that go beyond creative listening. But in the end a person has to make his own decision, to find his own solution; and in many cases he will find it without any more active or physical help than this.
It might well be objected by any thoughtful reader that if a person carried out the physical, economic, mental, moral, spiritual investigations that I have suggested in this book, he could take care of no more than one patient at a time, and would need years to finish up the tasks suggested by the history[Pg 173] of that one person. That is an objection that certainly deserves an answer. I will begin my answer by a comparison with medical work. A trained physician is supposed to know something of all the organs in the body. Even a dentist or an oculist has had some training on all the bodily organs and not merely on the special ones he treats. Among the organs of the body, the medical profession is supposed to include the brain and all the functions of the brain. This implies that he is supposed to have at his finger-ends the ability to make an examination so complete that a whole day would be needed to finish it. Obviously if he attempted anything like that he would soon be overwhelmed. But on the other hand if he limits himself to the professional examination of a single organ, the one perhaps which the patient complains of, he does so at his peril. He is in danger of making a wholly wrong diagnosis. But that can be diminished only in proportion to his knowledge of all the other organs that he does not examine. A well-trained physician must and can safely do some superficial work. So a very well-trained social worker can and must do some superficial social work. In the practice of any doctor who counts up a month's patients we will say to one hundred, there will be about fifty that he has examined and treated very slightly. Then there may be twenty-five whom he knows a little more about, fifteen perhaps that he could give a full account of, and possibly ten whom he has had to study from all the points of view that his medical[Pg 174] education has made possible for him. His professional life then is not wholly superficial yet does not attempt to deal exhaustively with every case.
As I see it, therefore, our work in the social or medical field ought to be something like a pyramid.
We should study and treat many cases superficially, a smaller number more intensively, and at the top of the pyramid which represents our case-work will come a few to which days or weeks of time are devoted. Such a distribution of time is not unsatisfactory or slipshod because not all the needs that come to our attention call for thorough study.
Such a pyramidal distribution of our energies is familiar and satisfactory in other fields of life, for instance in the field of friendship. Nobody wants only intimate personal relations. Everybody needs as a basis a host of acquaintances. Out of them all he makes a few friends whom he hopes to know as well as he can know any human being. Almost no one is satisfied to possess only acquaintances or only intimate friends. The properly balanced life has both.
Both among those for whom we attempt only slight study or slight service, and among those to whom we devote ourselves intensively, doctor and social assistant alike must count failures as well as successes. We do not try to balance failures and [Pg 175]successes if we are wise. The Lord only knows which of our seeming failures are really successes and which of our successes are failures. Some of the people with whom we seem to have made total failures, a more complete knowledge might show to have been actually helped. All this we must face from the start. Then we shall not be disappointed because we have to touch a great many people superficially and to fail a great many times. That is all right so long as we are not always superficial and do not always fail.
Such a philosophy is my defence for so elaborate and extensive a scheme of social investigation and social treatment as I have tried to explain in this book. The experienced physician and the well-trained social assistant can judge with some accuracy which cases to select for thorough study and continued devotion. But such a judgment is impossible unless one keeps always ready in the background of one's mind the whole apparatus of social diagnosis and treatment as it might be applied in toto, if time and strength were unlimited.
[4] Polonius (showing out the wandering actors):—My Lord, I will use them according to their desert.
Hamlet: Odd's bodikin, man, much better! Use every man after his desert and who shall 'scape whipping.
[5] In the volume called The Musical Amateur. (Houghton Mifflin Co., Boston.)
What is the motive of social work? Why do we do it? Why is it worth while? What will keep it going?
To me it seems like a head of energy behind a faucet or behind a dam, a pressure that has to be explained; and as we use the word motive, we may well think of it in a literal sense as something that pushes, something that moves. Then what moves? Energy, which is the source of our work, is perhaps the most general term that there is in the world. Behind everything, we say, there is energy. Behind the activities of our physical bodies there is energy to an extent that those who have not studied medicine or other physical sciences do not always recall.
Eighty per cent of any human being's body is made up of water. Where did it come from? It came from what he has taken in in the form of drink. Where did that come from? From the earth and the streams. Where did they get it? From the clouds. Where did the clouds get it? From the seas. Where did the seas get it? From the interplanetary spaces and God knows where. Eighty per cent of our bodies, of our available energy, comes out of something as far off as that, out of sources that have ultimately as little to do with us as that.
The other twenty per cent, the solids of every[Pg 177] organ in our body, the brain included, are alike widely distributed in source. We do not always stop to think how widely distributed are the foods out of which the body's solids are built. Grains, fruits, vegetables, meats, we get them out of every part of the globe. The minerals that are deposited in us as what we call bone, the lime and other salts, are something which a plant once sucked up out of the earth, or another animal took out of his food to pass on to us. The bones of a human being come out of the bones of the earth through his food, animal and vegetable. The breath of the trees, the oxygen which the trees give out every day and every night, we breathe in. They take up in turn the carbon that we give out, so that there is constantly an exchange between the animal and vegetable kingdom and ours. We are warmed by inheritance from thousands of years in the coal that plants have laid down their lives in layers and strata to form; we are warmed also by the constant literal burning up of food energy in ourselves. We are clothed with borrowings from sheep and cows and other animals; birds' feathers go to make our pillows, beds, and hats.
Sometimes I wonder whether we are worth all this destruction and all the other forms of destruction whose living incarnation we are. I described, in speaking of fatigue and rest, how our physical life is a constant process of burning up and breaking down tissue, hence of destruction. And of course the money and labor of our parents that kept us alive up to the[Pg 178] time that we call ourselves self-supporting, represents other stores of energy passed on through various way-stations, by the same sort of borrowing, from every part of the universe.
All that death, that suffering, that destruction, are we worth all that? One certainly could see a tragic aspect to this question if one were so minded. Many philosophers have so seen it. But the answer depends, I think, on what we do with that energy. It may easily be wasted. It may just run through us, as much of our information runs through us, uncaught, unused, sacrificed for us, and nothing come of it. But it may be used right.
When we come to think of our mental energies, are we any less incurably borrowers, incurably indebted to the universe, incurably wasters except in so far as we make use of what we borrow? Anybody who has not studied how the child learns to talk, does not realize what a borrowing the simplest acts of language are, what imitators we are from the earliest moments of our lives. And if we try to think back to the pieces out of which we have been actually made, our intellectual, moral, spiritual life, we could take ourselves apart like a piece of machinery and say where each piece came from. If we look into the generation of our own minds I think we shall be overcome with wonder as I often have been, by the consideration of how little there is left that is us if we take out what has been given us. I can say from[Pg 179] whom every idea I have had came, from whom I had it as a free gift. I believe the greatest of all our borrowings are from people we never saw, from books, from music, from art, from personalities to whom we feel inexpressibly near although we never saw them in the flesh.
Our spiritual borrowings are not only from sources such as I have mentioned, but from impersonal sources also, from beauty, from nature, that does not speak to us through any man. I have seen a hepatica on a rocky hillside under brown oak leaves, the sight of which made me conscious that I could never pay off my debts for life. I have heard a thrush singing in the early morning in wet dark woods, and known then and there that after the gift of that song I could never get even with the universe.
Most of us have had that sort of experience many times; it goes on and on piling up our debt. But our obligation grows and grows when we think of our country, of the traditions of our race, and of what has been given us by the church or university or family in which we have found ourselves without our doing anything about it. What should we be without those? What shred of personality would remain? I do not think the figure of the body, as I have tried to describe its borrowings, is any more striking than that of the mind, the spirit, and the inexhaustible debts that it has laid up.
All this energy poured into us from the material[Pg 180] and from the spiritual universe around us accumulates in us. It accumulates bodily in vital force, zest, animal spirits, or "pep"; the desire to shout and sing or jump or slap somebody on the back. That is the vital side of our unexpended borrowings, the bodily expression of the fact that we have received more than we can easily take care of. But mental energy accumulates too; and the sense of its pressure is expressed in what seems to me the greatest word in our language—gratitude. Gratitude is "happiness doubled by wonder," happiness such as anybody may contain almost unconsciously or may let out of him, if he is thoughtful, in action sprung from conscious gratitude. Gratitude seems to me ultimately the motive of social work. We find in ourselves this painful head of energy—to me often painful. The sense of an animal caged, of a dog in leash, is the figure that most often comes to me as I am aware of what has been given to me and of how little I have paid it back. The extra flood of physical energy which any healthy human being or animal has, is paralleled in this tension of gratitude for all the gifts which we have not properly handed back, have not passed on, and never shall.
The attempt to pay out, to pass on, this energy naturally divides itself up according to the ways in which we have received it. We have received the physical bounty of life. We know how good it is to get water when we are thirsty and food when we are hungry, and along with the full-flavored awareness[Pg 181] of this good we feel the pain of not being able to share it as swiftly as we would like to share it, as fully as we would like to share it, with people who have not got what we have. We call that pity, the sense of kind. I think of it as the sense of a common need. Other people are such as we. We are painfully aware of what has been given to us, and how much we and everybody else need it, and how little we deserve it. We are eager therefore to pass that on in any such form as it can be received. We are grateful for any good chance to pass it on. A homely but true image is that of the nursing mother. The baby needs milk and the mother needs to get rid of that milk. It is a painful pressure in her breast and a pressing need in her child. The two needs meet and satisfy each other.
We are just as eager, I think, to give back in kind all the different sorts of delight and of beauty for which we are grateful. But we have not well expressed this eagerness. I have dwelt already on the great lack of beauty and of art in social work, on its ugliness and drabness, and on the care-worn look in the social worker's face. But no one who is vividly conscious of the gifts of beauty which have come into his own life can continue to make his attempts at social work as unbeautiful as they have been hitherto.
If we have any sense of gratitude to the people that have cared for us, we want to pass on affection. We know the affection that was our physical [Pg 182]creation in the beginning and our upbringing through childhood and youth, yet most of us have never tried through most of our lives to pay back these debts to our parents. Indeed we usually do not become aware of those debts until it is too late. To know that would bring us to almost insupportable remorse after our parents have left us, if we were not aware that we could pay over to somebody else the affection and care which they once lavished on us.
As we know that the physical energies of water and oxygen and carbon, of the food, the lime salts, and whatever else goes to make up our physical being, all come out of one source, so we are aware that all spiritual gifts come out of one and the same source. To be vividly aware of that, to stop and face the facts, to stop and take a view of where we are, tells us what next to do. It makes us eager to pay back some of that gratitude directly in prayer, and also indirectly through all the way stations by which this help has come to us. If you want to please a mother you do something for her children. A human being lives in his children, in the people or the undertakings that are his children literally or figuratively. If you love him, you feed his lambs. So we get the impulse to pass on the best fruits of life, first to the one source of all that makes us grateful, and then to the children of this central Energy, the different way stations from which it has come to us.
We eat our heads off like stabled horses with too[Pg 183] much oats, if we do not get a chance to give away some of what has come to us. A man who tells funny stories is always grateful to the man who will listen to him. The same principle holds true all the way from story-telling to social work. It can be taken as humiliating, but properly viewed it is a sanifying and humbling fact.
I wrote a moment ago of the sense of what we owe to our parents, a debt that seems almost insupportable sometimes. It would be insupportable if we could not pay it on to somebody else. Were it not for this central fact our gratitude would be a curse not a blessing. But in fact those who gave to us, our parents and all the rest, are best pleased if we pay over their gifts to somebody else. That is how we can best repay them.
If this is a right conception of the source out of which comes the energy that has set us going and will keep us going, I think we can trace out a justification for the principles of social work which I have tried to present in this book and will now summarize:
1. We want to do social work because we have got something that we must share, something that is too hot to hold. There is a false emphasis, approaching sentimentality, in saying that our social work is done because of our love for the individual people to whom we give. We have a hope that some day we may know a few of these people well enough to say that we love them. But that is hope, not fact or [Pg 184]present impulse. Hence it is not right (although it is not a fearful error) to say that we do social work for love of the particular individuals whom we try to help. We are looking for an opportunity and are grateful for the opportunity that social work gives us, to pass on the gifts which we are grateful for, not as has sometimes been said, to people whom we love but to every one who needs them.
That may seem a very slight difference of emphasis. I think it is a very important difference of emphasis. We are in a much more self-respecting position if we do not have to think of ourselves as having already conquered at the beginning that which we aspire to win in the end, a personal affection for all our patients. If we remember that our patients are (unconsciously) doing us a favor in allowing us to pass on something to them, and that although we may have found a genuine need, still we are grateful to them because they want what we have to give, then our work is humble and free from taint of Pharisaism.
2. The second principle is: give as one passing on that which is not our own. That is familiar enough in relation to money. Any one who has any money and any capacity for thoughtfulness, knows that his money is not his own. Whether it happens to be literally in trust or not, the only right he has is the right of rightly choosing what he will do with it. He holds it rightfully just so long as he needs to find the chance, the best opportunity for passing it on.
Such a sense of trusteeship we ought to feel about everything that we have and want to give: beauty, information, education, affection, and courage. One should give them (if he can!) not as one who has any special merits, not as one having property which is one's own, but as one who has received without any possible deserts an incredible wealth and would like above all things to share it because it is not his own.
3. We ought to give and build, because the effects of any giving that is not also building will not last. Our bodies and our souls are what they are because of what has been given and built into them by nature and by man. The same energy which burns in our bodies and knows in our consciousness should make us desire always to give and build by giving, because we have ourselves been built up of such gifts.
4. We ought to give and take. That is another aspect of giving as one who passes on. We can give only what we have taken. Hence if we allow our lives to get cooped up, narrow and stifled, so that we are not taking in steadily, or not getting fresh energy out of what we have already taken in during the years that are past, we soon have nothing to give. I have written of the ugliness and the depression that I have seen too much in social workers' lives. That is partly because they are often led into giving without providing for any adequate source of renewal. They are not taking in enough to have anything to give out. They give until they are drained dry, squeezed out.
5. We give not as people who find the world so pitiable, so miserable that we want to diminish its misery. We give as people who find the world so glorious, so overflowing, in what it has done for us, that we want to even up, to pay out. We want to share our enthusiasms. Pity led Schopenhauer to pessimism. He pitied the world so much that he thought everybody ought to get out of it by suicide. Pity therefore does not necessarily lead us to social work.
But if we admire anybody, that fact gives us a duty to get our admiration over to somebody, to share our enthusiasm. The whole of a Christian's duty might be phrased as the duty to share his sense of the beauty and the wonder that is in Jesus Christ. Almost the only act that we can be sure will be of use in the world is the act of sharing what enthusiasm we have.
6. But this cannot be done without some care to shape it, without some labor to put it in a form in which somebody else will understand this sense of our admiration or gratitude. Without form and study to give it form, our enthusiasm is mere noise and good spirits. As I have described the fund of energy which comes into us, is felt as gratitude and then pours out of us in social work, one may have wondered, where does man's individual will and choice come in? Where does he begin and these tumultuous energies stop? What is he?
He is that which focusses, that which forms, which[Pg 187] makes comprehensible, which expresses the energies that have been given him as a free gift. And because miraculously he is made new—for everything that is new is a miracle—because miraculously he is different from every human being that ever was, so different from all others is the gift that he has to give. I think it is sometimes comforting to look at a finger-print. One gets doubtful whether there is any special reason that the individual called by one's name should persist on top of the earth. Then it is well to go back to simple, elemental facts like finger-prints, with the pretty nearly irresistible conclusion that the rest of our body and soul must be as unique as that, and so possesses something as original to contribute to the world. I have no doubt that there is waiting for each of us to-day a job much more individual than we have ever yet done.
Although, then, we can rightly give in social work merely as people who pass on to others in gratitude and wonder the energies which create our bodies and our souls, yet we can be perfectly sure that if we do what it is up to us to do, we shall in time be giving as people never gave before and never will again. We have missed rare chances in social work unless through presence of mind we find our chance to express differently from what we have ever heard it expressed before that which we feel pushing in us to get out.
7. Since it is our business to give as people who pass on, we want if we can to make it clear sooner or later to the people to whom we pass it on, that we[Pg 188] know this. Then they will feel no shame in taking since they know that they do not take from us. There will be no sense that a higher being is distributing what a lower being has to take, if we make it clear that we are sharing that which it is uncomfortable not to share. We are sharing that which we share because in view of all the bounty which we have received, in view of the beauty which has struck us dumb, in view of the flood of affection that we never have answered, we know what to do next. We know that we are branches of a vine, and that the sap of that vine can flow out in us and through us to other tendrils.
THE END
The Riverside Press
CAMBRIDGE. MASSACHUSETTS
U. S. A