MEDICAL AND SURGICAL LANDMARKS
By the same Author.
MANUAL OF DISSECTION OF THE HUMAN BODY.
With numerous Illustrations.
HUMAN OSTEOLOGY.
Comprising a Description of the Bones with Delineations of the
Attachments of the Muscles. Sixth Edition in the press.
LANDMARKS
MEDICAL AND SURGICAL
BY
LUTHER HOLDEN
EX-PRESIDENT, MEMBER OF COUNCIL, AND MEMBER OF THE COURT OF EXAMINERS OF
THE ROYAL COLLEGE OF SURGEONS OF ENGLAND: CONSULTING SURGEON
TO SAINT BARTHOLOMEW’S AND THE FOUNDLING HOSPITALS
assisted by
JAMES SHUTER, M.A. Camb., F.R.C.S.
ASSISTANT SURGEON TO THE ROYAL FREE HOSPITAL: LATE DEMONSTRATOR
OF PHYSIOLOGY, AND LATE ASSISTANT DEMONSTRATOR OF
ANATOMY, AT SAINT BARTHOLOMEW’S HOSPITAL
THIRD EDITION

LONDON
J. & A. CHURCHILL, NEW BURLINGTON STREET
1881
[All rights reserved]
TO
THE STUDENTS
PAST AND PRESENT
OF
SAINT BARTHOLOMEW’S HOSPITAL
THESE ‘LANDMARKS’ ARE
Dedicated
BY THEIR SINCERE FRIEND
THE AUTHOR
PREFACE TO THE THIRD EDITION.
In the present Edition the author adheres to his decision not to
introduce Diagrams. Additional experience more than ever convinces
him that they would frustrate his original object, which is to teach
Students the habit of making the eye and the hand work together, and to
educate the ‘touch’ upon the normal living body.
Without such practical training, how can we reasonably expect to form a
correct diagnosis when called upon to examine an injury or to detect a
disease? In truth, the work is intended only for those who are desirous
of acquiring the habit recommended.
PREFACE TO THE FIRST EDITION.
These ‘Landmarks’ have already appeared in Saint Bartholomew’s Hospital
Reports. They are now republished, with some additions, in the hope
that they may be useful to others besides those for whom they were
originally intended.
My object has been to collect into a compact form the leading landmarks
which help practical surgeons in their daily work. Those relating to
the chest and abdomen have been ascertained, with as much precision as
natural variations permit, by needles introduced in various directions.
I have to express my acknowledgments to Mr. Walsham and to Dr.
Godson for their contributions.
65 Gower Street: March 1876.
CONTENTS.
[Pg 1]
‘CHIRURGUS MENTE PRIUS ET OCULIS AGAT QUAM MANU ARMATA.’
LANDMARKS
MEDICAL AND SURGICAL.
1. In clinical teaching, we often have occasion to point out, on
the surface of the living body, what may be called ‘medical and
surgical landmarks.’ By ‘landmarks’ we mean surface-marks, such as
lines, eminences, depressions, which are guides to, or indications
of, deeper-seated parts. This practice is not only most useful but
absolutely necessary; because many, even advanced students of anatomy,
are not so ready as they ought to be in their recognition of parts
when covered by skin. Students who may be familiar enough with bones,
muscles, blood-vessels, or viscera in the dissected subject, are often
sadly at fault when they come to put this knowledge into practice in
the living.
For instance, ask a student to put his finger on the exact place where
he would feel for the head of the radius, the coracoid process of
the scapula, the tubercle of the scaphoid bone in the foot; ask him
to compress effectually one of the main arteries; to chalk the line
of its course; to map on the chest the position of the heart and the
several valves at its base; to trace along the walls of the chest the
outline of the lungs and pleura; to point out the bony prominences
about the joints, and their relative position in the different motions
of the joints; test him about the muscles and tendons which can be
seen or felt as they stand out in relief or remain in repose; let him
introduce his finger into the several orifices of the body, and say
what parts are accessible to the touch:—questions such as these, even
a good anatomist, unaccustomed[Pg 2] to deal with the living subject, might
possibly find himself at a loss to answer.
2. Object in view.—Our main object, therefore, is to induce
in students the habit of looking at the living body with anatomical
eyes, and with eyes too at their fingers’ ends. The value of this habit
cannot be too highly estimated. Is it not of the utmost importance
to an operating surgeon that he should have in his mind’s eye the
various structures of the body as they lie grouped, connected, and
working together? Should he not try at least to see them with the same
clearness and accuracy as if they were perfectly transparent?
Moreover, the habit of examining the living body with ‘anatomical eyes’
and ‘surgical fingers’ teaches the eye and the hand to act together,
and trains that delicate sense of touch which every surgeon should
possess.
This habit is within easy reach of any one who has carefully dissected
for himself, and learned what to feel for. Plates will not give him
this knowledge. Let a student examine his own body with a skeleton
before him. Better still that two should work thus together, each
serving as a model to the other.
Teachers of anatomy should follow the example of Sir C. Bell, who was
in the habit of introducing, from time to time, a powerful muscular
fellow to his class, ‘in order to show how much of the structure of
the body, such as the articulations and the muscles, might be learned
without actual dissection.’[A][1]
At the same time, it is only fair to say that ‘landmarks’ cannot always
be defined with precision. A considerable latitude must be allowed for
natural variations in different persons. In some, their anatomy stands
out beautifully clear; in others, it is masked by obesity. Selecting,
therefore, for study a moderately lean person, let us begin with the
head.
[Pg 3]
THE HEAD.
3. Scalp: its density.—The great toughness of the scalp,
more especially at the back of the head, is owing to its intimate
connection with the cranial aponeurosis, the scalp vessels and hair
bulbs intervening. This density often obscures the diagnosis of tumours
on the cranium. A tumour growing upon the head may be either above
or below the aponeurosis of the scalp. If below, it will have a firm
resisting feel, being bound down by the aponeurosis. Nevertheless
its firmness and resistance may depend not simply on its confinement
beneath the aponeurosis, but on its having its origin within the
skull. Look with suspicion, then, on every tumour on the head that
will not readily permit you to move it about, so as to be sure of its
connections prior to an attempt at extirpation.
The scalp moves freely over the pericranium, to which it is very
loosely connected by areolar tissue. When suppuration takes place in
this tissue free incisions through the dense scalp must be made to let
the pus out.
4. Arteries of scalp.—The supra-orbital artery can be felt
beating just above the supra-orbital notch, and traced for some way up
the forehead; the temporal (anterior branch) ascends tortuously about
one inch and a quarter behind the external angular process of the
frontal bone; the occipital can be felt near the middle of a line drawn
from the occipital protuberance to the mastoid process; the posterior
auricular, near the apex of the mastoid process. All these arteries can
be effectually compressed against the subjacent bone.
5. Skull-cap.—The skull-cap is rarely quite symmetrical. This
want of symmetry is often obvious. It may occur in men highly gifted,
as in the celebrated French anatomist Bichat. As to shape and relative
dimensions, no two heads are exactly alike, any more than are two
faces. It is beside my present purpose to go into the question of
craniology more than to say that, although the cranium does not exactly
follow the brain in all its eminences and depressions so as to be like
a cast of its surface, yet it certainly indicates the[Pg 4] dimensions of
the great cerebral masses. The prominence of the frontal and parietal
‘eminences’ and of the occipital region may be taken as a general
indication of the development of the corresponding lobes of the brain.
To ascertain the relative proportions of these three regions, let a
thread be passed from one meatus auditorius to the other, across the
frontal, parietal and occipital eminences respectively.
Frontal sinuses.—The ‘frontal sinuses’ formed by the separation
of the two tables of the skull vary much in size in different persons
and at different periods of life. This fact has an important bearing
on wounds in the forehead and on trephining in this situation. These
‘bumps’ do not exist in children, because the tables of the skull do
not begin to separate before puberty. From an examination of many
skulls in the Hunterian Museum, I find that the absence of the ‘bumps,’
even in middle age, does not necessarily imply the absence of the
sinuses, since they may be formed by a retrocession of the inner wall
of the skull. In old persons, as a rule, when the sinuses enlarge, it
is by the encroachment of the inner table on the brain case. The inner
wall of the skull here follows the shrinking brain. It is, therefore,
important to bear in mind that an adult, and more especially an elderly
person, may have a large frontal sinus without any external indication
of it.
Neither does a very prominent bump necessarily imply the existence of
a large sinus, or indeed of even a small one. The ‘bump’ may be a mere
heaping up of bone, a degradation, as in some Australian skulls.
Mastoid process.—The mastoid process, which can be felt behind
the ear, contains air-cells, to which the above observations may also
be applied.
Occipital protuberance.—The occipital protuberance, and the
superior curved line, can be distinctly felt at the back of the head.
The protuberance is always the thickest part of the skull-cap, and more
prominent in some than in others.
The posterior inferior angle of the parietal bone, grooved by the
lateral sinus, is on a level with the zygoma, and a[Pg 5] trifle more than
one inch behind the front border of the mastoid process.
Lines of cerebral sinuses.—A line drawn over the head from the
root of the nose to the occipital protuberance corresponds with the
superior longitudinal sinus. Another line drawn from the occipital
protuberance to the front border of the mastoid process corresponds
with a part of the lateral sinus.
Middle meningeal artery.—The trunk of the middle meningeal
artery runs along the front lower corner of the parietal bone, about
one inch and a half behind, and half an inch above, the external
angular process of the frontal.
A straight line drawn from the front of one mastoid process to the
other would pass through the middle of the condyles of the occiput,
showing how nearly the skull is balanced on the top of the spine in the
erect posture.
6. Thickness of skull-cap.—The average thickness of the cap
of an adult skull is about ⅕ of an inch. The thickest part is at
the occipital protuberance, where it is often ¾ of an inch or more,
even in an otherwise thin skull. The thinnest part is at the temple,
where it may be almost as thin as parchment. Everyone in the habit of
making post-mortem examinations knows how much the skull-cap differs
in thickness in different persons and in different parts of the same
skull. In old persons it is often in some parts not thicker than a
shilling, owing to absorption of the diploë. Another point of interest
is that the inner plane of the cap is not always parallel with the
outer. Hence, in applying the trephine this is not a bad rule—‘Think
that you are operating on the thinnest skull ever seen, and thinner in
one half of the circle than the other.’
7. Levels of the brain.—The level of the anterior lobes in
front corresponds with a straight line drawn across the forehead, just
above the eyebrows. The lower level of the anterior and middle lobes of
the cerebrum corresponds with a line drawn from the external angular
process of the frontal bone to the upper part of the meatus auditorius.
Another line drawn from the meatus to the occipital protuberance[Pg 6]
corresponds with the lower level of the posterior lobe. The lower level
of the cerebellum cannot be defined by external examination. It depends
upon the extent to which the occipital fossæ bulge into the nape of the
neck; and this bulge varies in different skulls.
THE FACE.
8. The approaches to the organs of the senses, their ever-varying
expression, their numerous muscles, and their rich profusion of vessels
and nerves, give the face great anatomical importance, which has a
most valuable bearing, not only on the practice of surgery, but on the
physiognomy of health, and in the diagnosis of disease.
9. Foramina for branches of fifth nerve.—As a surgeon may be
called upon to divide any one of the three chief branches of the fifth
nerve upon the face, he looks with interest to the precise situations
where they leave their bony foramina with their corresponding arteries.
The supraorbital notch or foramen can be felt about the junction of the
inner with the middle third of the supraorbital margin. From this point
a perpendicular line drawn with a slight inclination outwards, so as to
cross the interval between the two bicuspid teeth in both jaws, passes
over the infraorbital and the mental foramina. The direction of these
two lower foramina looks towards the angle of the nose.
10. Pulley for superior oblique muscle.—By pressing the
thumb beneath the internal angular process of the frontal bone, the
cartilaginous pulley for the tendon of the superior oblique muscle can
be distinctly felt. We should be careful not to interfere with this
pulley in any operation about the orbit.
11. Lower jaw.—The working of the condyle of the jaw vertically
and from side to side can be distinctly felt in front of the ear. When
the mouth is opened wide, the condyle advances out of the glenoid
cavity on to the eminentia articularis, and returns into its socket
when the mouth is shut. The muscle which causes this advance is the
external[Pg 7] pterygoid; and it gives the jaw a greater freedom of grinding
motion.
The posterior margin of the ramus of the lower jaw corresponds with
a line drawn from the condyle to the angle. In opening abscesses in
the parotid region, the knife should not be introduced behind this
line for fear of wounding the external carotid artery. Punctures to
any depth may be safely made in front of it. They are often necessary
where inflammation of the parotid gland ensues after eruptive fevers,
and runs on to suppuration. The swelling, tension, and pain are most
distressing. Owing to the fibrous framework of the gland, the matter
is not circumscribed, but diffused. One puncture is not enough. Three
or more may be requisite. The blade of the knife should be held
horizontally, so as to be less likely to injure the branches of the
facial nerve. We are not to be disappointed if no matter flows. The
punctures give relief, and matter will probably exude the next day.
12. Parotid duct.—A line drawn from the bottom of the lobe of
the ear to midway between the nose and the mouth gives the course of
the parotid duct. Opposite the second upper molar, the duct opens by a
papilla into the mouth. The branch of the facial nerve which supplies
the buccinator runs with the duct.
13. Temporal and facial arteries.—The pulsation of the trunk
of the temporal artery can be felt, between the root of the zygoma and
the ear. This should be well known to and used by chloroformists. It
is also a convenient pulse to feel in a sleeping patient. The facial
artery can be distinctly felt as it passes over the body of the jaw at
the anterior edge of the masseter; again near the corner of the mouth
close to the mucous membrane: and, lastly, by the side of the ala nasi,
up to the inner side of the tendo oculi. By holding the lips between
the finger and thumb the coronary arteries are felt under the mucous
membrane. The facial vein does not accompany the tortuous artery, but
runs a straight course from the inner angle of the eye to the front
border of the masseter, just behind the artery.
[Pg 8]
14. Eyelids and eyes.—The opening between the eyelids varies in
size in different persons; hence more of the eyeball is seen in some
than in others, and the eye appears larger. Although human eyes do vary
a little in size, yet the actual difference is by no means so great as
is generally supposed. The size of the fissure has much to do with the
apparent size of the eye. Contrast the narrow fissure of the Chinese
and Mongolian races, and the apparent smallness of their eyes with
those of Europeans. As a rule the external angle of the lid is higher
than the internal. When not exaggerated, it gives the face an arch and
pleasing expression.
Evert the lids to see the Meibomian glands; observe their perpendicular
arrangement, in the substance of the tarsal cartilages.
The free borders of the lids are not bevelled, as described by J. L.
Petit and most anatomists, ‘so as to form with the globe of the closed
eye a triangular canal for the flow of the tears.’ On the contrary, it
is easily seen that the lid margins, when closed, come into accurate
contact. Their plane is not exactly horizontal, but slightly inclined
upwards.
Every time the eye is shut, the ball turns upwards and inwards, so that
the cornea is completely covered by the upper lid. This may be well
seen by raising the lid of a sleeping infant; also in cases of low
fever when the lid is not completely closed. This up-turning of the eye
obviously clears the cornea, and protects it from the light.
A careful examination of the motion of the lower lid in the act of
shutting the eye proves that it is a double motion. The lid is not only
slightly raised, but drawn inwards about 1/12 of an inch. This second
movement sweeps any particles of dust as well as moisture towards the
inner canthus.
15. Puncta lachrymalia.—The puncta lachrymalia are distinctly
visible at the inner angles of the lids. The lower punctum is larger
and a little more external than the upper, so that they are not exactly
opposite. The direction, too, of the puncta deserves notice. Their open
mouths look a little backwards, ready to imbibe the tears. When their
proper[Pg 9] bearing is lost, as in facial paralysis or by a cicatrix near
the lid, the tears overflow the cheek. The length of the lachrymal
canals is from three to four lines. The lower is a little shorter and
wider than the upper. As each makes a little angle in its course, about
a line from its orifice, the lid should be drawn outwards to straighten
the canal when we introduce a probe.
16. Lachrymal sac.—To find the lachrymal sac, draw outwards
the eyelids to tighten the tendo oculi, which crosses the sac a little
above its middle. A knife introduced just below the tendon close to
the edge of the orbit would enter the sac. The angular artery and vein
would be on the inner side of the incision. A probe directed in a line
with the inner edge of the orbit, i.e. downwards, outwards, and
backwards, would pass down the nasal duct, and appear in the inferior
meatus of the nose.
The tendo oculi serves many purposes besides giving attachment to the
cartilages and muscles of the lids. One purpose is said to be to pump
the tears into the lachrymal sac. Place a finger on the tendon, and
feel that it tightens every time the lids are closed. The tendon, being
intimately connected to the sac, draws, as it tightens, the sac wall
outwards and forwards, and in this way it may pump along the lachrymal
canals any fluid collected at the angle of the eye.
17. Nasal duct.—The nasal duct is from six to eight lines long,
and narrowest in the middle of its course. Its termination in the
inferior meatus lies under the inferior spongy bone, about a quarter
of an inch behind the bony edge of the nostril. The appearance of
the orifice in the dry bone conveys no idea of its size and shape in
life; for it is diminished by a valve-like fold of mucous membrane, so
that it becomes, in most cases, a mere slit, not exceeding a line in
diameter.
The facility with which instruments can be introduced into the nasal
opening of the duct depends upon its position as well as its size. This
position varies in different instances. Sometimes it opens directly
into the roof of the inferior meatus, in which case the hole is large
and round, so that tears readily[Pg 10] run into the nose. In other instances
the opening is situated on the outer wall of the meatus, and is then
always such a narrow fissure as to be hardly discernible. The practical
conclusion then is, that a probe can be easily introduced when the
opening is in the roof of the meatus, but not without difficulty
and laceration of the mucous membrane when on the outer wall. This
difficulty indeed may be increased by the narrowness of the meatus,
arising from an unusual curvature of the spongy bone.
18. Nose and nasal cavities.—The line where the cartilages
of the nose are attached to the nasal and superior maxillary bones
can be traced with precision. The close connection of the skin to
the cartilages admits of no stretching; hence the acute pain felt in
erysipelas and boils on the nose. The external aperture of the nose is
always placed a little lower than the floor of the nostril, so that the
nose must be pulled up before we can inspect its cavities.
Looking into the nostrils, we find that the left is, in the majority
of cases, narrower than the right, owing to an inclination of the
septum towards the left. A communication sometimes exists between
them, through a hole in the septum, as in the case of the celebrated
anatomist Hildebrandt. By stretching open the anterior nares we
can get a view of the end of the inferior spongy bone. The middle
spongy bone cannot be seen: its attachment to the ethmoid is high up,
nearly opposite the tendo oculi. The cavities are so much narrowed
transversely by the spongy bones, that in the extraction of polypi it
is better to dilate the blades of the forceps perpendicularly, and near
the septum.
19. Mouth.—What can be seen and felt through the mouth? The
upper surface of the tongue, ‘speculum primarum viarum,’ is a
study in itself. We notice, on its under surface, a median furrow,
on each side of which stands out the ranine vein, lying upon the
prominent fibres of the lingualis. In the middle line of the floor of
the mouth is the ‘frenum linguæ,’ with the orifice of the duct of the
submaxillary gland on each side of it. The gland itself can be detected
immediately beneath the mucous membrane[Pg 11] by feeling further back near
the angle of the jaw, at the same time pressing the gland upwards from
below.
The long ridge of mucous membrane on each side of the floor contains
the sublingual glands.
We can feel the attachment of the ‘genio-hyo-glossi’ behind the
symphysis of the jaw. The division of this attachment would enable a
surgeon to draw the tongue more freely out of the mouth in any attempt
to remove carcinoma extending far back into its root.
There is great difference in the shape of the hard palate; this
difference depends upon the depth of the alveolar processes. In some it
forms a broad arch; in others it is narrow, and rises almost to a point
like a Gothic arch, and materially impairs the tone of the voice.
Throat.—To examine the throat well, the nose should be held so
as to compel breathing through the mouth. Thus the soft palate will be
raised, the palatine arches widened, and the tonsils and the back of
the pharynx fairly exposed. Pressing the tongue downwards, provided it
be done very gently, is also of advantage. Rude treatment the tongue
at once resists. The forefinger can be passed into the throat, beyond
the epiglottis, as low as the bottom of the cricoid cartilage, and thus
search the pharynx down to the top of the œsophagus, and the hyoid
space (on each side) where foreign bodies are so apt to lodge. The
greater cornu of the hyoid bone can be felt as a distinct projection
on either side. In introducing a tube into the œsophagus the finger
should keep the instrument well against the back of the pharynx so as
to prevent its slipping into the larynx.
Pass the finger between the teeth and the cheek and feel the anterior
border of the coronoid process of the jaw. On the inner side of this
process, between it and the tuberosity of the upper jaw, is a recess,
where a deeply-seated temporal abscess might burst, or might be
opened. Behind the last molar on the inner side of the upper jaw we
can distinctly feel the hamular process of the sphenoid bone; also the
lower part of the pterygoid fossa, and the internal pterygoid plate.
Behind, and on the outer side of the last molar, can be felt[Pg 12] part of
the back of the antrum and of the lower part of the external pterygoid
plate.
On the roof of the mouth we can feel the pulsation of the posterior
palatine artery. Hæmorrhage from this vessel can be arrested by
plugging the orifice of the canal, which lies (not far from the
surface) on the inner side of the last molar, about 1/3 of an inch in
front of the hamular process.
When the mouth is wide open, the pterygo-maxillary ligament forms a
prominent fold readily seen and felt beneath the mucous membrane,
behind the last molar teeth. A little below the attachment of this
ligament to the lower jaw we can easily feel the gustatory nerve, as it
runs close to the bone below the last molar tooth. The exact position
of the nerve can be ascertained in one’s own person by the acute pain
on pressure. A division of the nerve, easily effected by a small
incision, gives much temporary relief in cases of advanced carcinoma of
the tongue.
To feed a patient in spasmodic closure of the jaw, it is well to know
that there is behind the last molar teeth a space sufficient for the
passage of a small tube into the mouth.
Antrum.—Lift up the upper lip and examine the front wall of
the antrum. The proper place in which to tap it is above the second
bicuspid tooth, about one inch above the margin of the gum.
20. Posterior nares.—A surgeon’s finger should be familiar
with the feel of the posterior nares, and of all that is within reach
behind the soft palate. This is important in relation to the attachment
of polypi, to plugging the nostrils, and to the proper size of the
plug. In the examination of this part of the back of the throat it
is necessary to throw the head well back, because, in this position,
nearly all the pharynx in front of the basilar process comes down below
the level of the hard palate, and can be seen as well as felt. But when
the skull is horizontal, i.e. at a right angle with the spine,
the hard palate is on a level with the margin of the foramen magnum,
and the parts covering the basilar process are concealed from view.
The head then being well back, introduce the forefinger[Pg 13] behind the
soft palate, and turn it up towards the base of the skull. You feel
the strong grip of the superior constrictor. Hooking the finger well
forwards, you can feel the contour of the posterior nares. Their size
depends upon the anterior, but rarely exceeds a small inch in the
vertical diameter, and a small half-inch in the transverse. The plug
for the posterior nares should not be larger than this. Their plane
is not perpendicular, but slopes a little forwards. You can feel the
septum formed by the vomer, and also the posterior end of the inferior
spongy bone in each nostril.
21. Tonsils.—Before taking leave of the throat, look well at
the position of the tonsils between the anterior and posterior half
arches of the palate. In a healthy state they should not project beyond
the level of these arches. In all operations upon the tonsils, we
should remember the close proximity of the internal carotid artery to
their outer side. Nothing intervenes but the pharyngeal aponeurosis,
and the superior constrictor of the pharynx. Hence the rule in
operating on the tonsils, always to keep the point of the knife inwards.
In troublesome hæmorrhage from the tonsils, after an incision or
removal, it is well to know that they are accessible to pressure if
necessary by means of a padded stick, or even a finger.
22. Features.—A word or two on the lines of the face as
indicative of expression. Everyone pays unconscious homage to the study
of physiognomy when, scanning the features of a stranger, he draws
conclusions concerning his intelligence, disposition, and character.
Without discussing how much physiognomy is really worth, there can
be no doubt that it is a mistake to place it in the same category as
phrenology, since the latter lacks that sound basis of physiology which
no one can deny to the former.
A person fond of observing cannot fail to have arrived at the
conclusion that a man’s daily calling moulds his features. Place a
soldier, a sailor, a compositor, and a clergyman side by side, and who
will not immediately detect a marked difference in their physiognomies?
[Pg 14]
The muscles of the features are generally described as arising from the
bony fabric of the face, and as inserted into the nose, the corners of
the mouth, and the lips. But this description gives a very inadequate
idea of their true insertion. They drop fibres into the skin all along
their course, so that there is hardly a point of the face which has not
its little fibre to move it. The habitual recurrence of good or evil
thoughts, the indulgence in particular modes of life, call into play
corresponding sets of muscles which, by producing folds and wrinkles,
give a permanent cast to the features, and speak a language which all
can understand, and which rarely misleads. Schiller puts this well when
he says that ‘it is an admirable proof of infinite wisdom that what is
noble and benevolent beautifies the human countenance; what is base and
hateful imprints upon it a revolting expression.’
THE NECK.
23. Subcutaneous veins.—Notice first the direction of the
subcutaneous veins. The chief subcutaneous vein is the external
jugular. Its course corresponds with a line drawn from the angle of the
jaw to the middle of the clavicle, where it joins the subclavian. It
is made more prominent by putting the sterno-mastoid into action, or
by gentle pressure on the lower end of the vein. It is exceptionally
joined by a branch which runs over the clavicle, and is termed
‘jugulo-cephalic.’ The anterior jugular generally runs along the front
border of the sterno-mastoid.
24. Parts in central line. Os-hyoides.—Immediately below
and nearly on a level with the lower jaw we feel the body of the
os-hyoides, and can trace backwards on each side the whole length of
the cornua. They might easily be broken by the grasp of a garotter.
Below the body of the os-hyoides is the gap above the thyroid
cartilage. This gap corresponds with the anterior thyro-hyoid ligament
and the apex of the epiglottis; so that in cases of cut throat in this
situation, nearly the whole of the epiglottis lies above the wound.
[Pg 15]
Thyroid cartilage.—The projection and depth of the notch in
the thyroid cartilage, or ‘pomum Adami,’ varies in different persons.
Between the notch and the hyoid bone there is a large bursa, which
facilitates the play of the cartilage beneath the bone in deglutition.
The notch does not appear till puberty, and is throughout life much
less distinct in the female than the male. The finger can trace the
upper borders and cornua of the thyroid cartilage: its lower cornua can
be felt by the side of the cricoid.
On each side of the thyroid cartilage we can recognise the lateral
lobes of the thyroid gland. On the upper and front part of the gland we
can distinctly feel the pulsation of the superior thyroid artery. This
pulsation, coupled with the fact that the gland rises and falls with
the larynx in deglutition, gives the best means of distinguishing a
bronchocele from other tumours resembling it.
Below the angle of the thyroid cartilage we feel the interval between
it and the cricoid, which is occupied by the cricothyroid membrane.
In laryngotomy we cut through this membrane transversely close to the
upper edge of the cricoid cartilage, in order that the incision may be
as far as possible from the attachment of the vocal cords.
25. Cricoid cartilage.—The projection of the cricoid cartilage
is a point of great interest to the surgeon, because it is his chief
guide in opening the air-passages, and can always be felt even
in infants, however young or fat. It corresponds to the interval
between the fifth and sixth cervical vertebræ. The commencement of
the œsophagus lies behind it: here, therefore, a foreign substance
too large to be swallowed would probably lodge, and might be felt
externally.
Again, a transverse line drawn from the cricoid cartilage horizontally
across the neck would pass over the spot where the omo-hyoid crosses
the common carotid. Just above this spot is the most convenient place
for tying the artery.
26. Those who have not directed their attention to the subject are
hardly aware what a little distance there is between the cricoid
cartilage and the upper part of the sternum. In a person of the average
height sitting with[Pg 16] the neck in an easy position, the distance is
barely one inch and a half. When the neck is well stretched, about
three-quarters of an inch more is gained. Thus, we have (generally) not
more than seven or eight rings of the trachea above the sternum. None
of these rings can be felt externally. The second, third, and fourth
are covered by the isthmus of the thyroid gland. The trachea, it should
be remembered, recedes from the surface more and more as it descends,
so that, just above the sternum in a short fat-necked adult, the front
of the trachea would be quite one inch and a half from the skin.
27. Trachea.—In the dead subject nothing is more easy than to
open the trachea: in the living, this operation may be attended with
the greatest difficulties. In urgent dyspnœa you must expect to find
the patient with his head bent forward, and the chin dropped, so as to
relax as much as possible the parts. On raising his head, a paroxysm
of dyspnœa is almost sure to come on, threatening instant suffocation.
The elevator and depressor muscles draw the trachea and larynx up and
down with a rapidity and a force which may bring the cricoid cartilage
within half an inch of the sternum. The great thyroid veins which
descend in front of the trachea are sure to be distended. There may
be a middle thyroid artery. In children the lobes of the thymus may
extend up in front of the trachea, and the left vena innominata may
cross it unusually high. Thus the air-tube may be covered by important
parts which ought not to be cut. Considering all these possible
complications, the least difficult and the best mode of proceeding
is to open the trachea just below the cricoid cartilage; and if more
room be requisite, to pull down the isthmus of the thyroid gland, or
in children to divide the cricoid itself. It is important that all the
incisions be made strictly in the middle line, the ‘line of safety.’
28. Sterno-mastoid muscle.—The sterno-mastoid muscle is the
great surgical landmark of the neck. It stands out in bold relief when
the head turns towards the opposite shoulder. Its inner border overlaps
the common carotid, which can be[Pg 17] easily compressed for a short time
against the spine about the level of the cricoid cartilage. The
artery extends (generally) as high as the upper border of the thyroid
cartilage and corresponds with a line drawn from the sterno-clavicular
joint to midway between the angle of the jaw and the mastoid process.
Between the sternal origins of the sterno-mastoid is the fossa above
the sternum, more or less perceptible in different necks. As it heaves
and sinks alternately, especially in distressed breathing, it was
called by the old anatomists ‘fonticulus gutturis.’ In beautiful necks,
as seen in the ‘Venus,’ it is filled up by fat.
Notice the interval between the sternal and clavicular origins of the
sterno-mastoid. A knife introduced a very little way into this interval
would wound, slanting inwards, the common carotid, slanting outwards,
the internal jugular vein. These facts are of importance in performing
the subcutaneous section of the tendon of this muscle.
29. Sterno-clavicular joint.—Many important parts lie behind
the sterno-clavicular joint. There is the commencement of the vena
innominata; behind this comes the common carotid on the left side, and
the division of the arteria innominata on the right. Deeper still, the
apex of the lung rises into the neck.
In a child the arteria innominata often lies in front of the trachea
and divides a little higher than the joint: a point to be remembered in
tracheotomy (27).
30. Apex of lung in the neck.—The extent to which the apex of
the lung rises into the neck is greater than is generally supposed.
Many observations in reference to this point lead to the conclusion
that the lung rises behind the sterno-mastoid, on an average, one
inch and a half above the clavicle; in persons with long necks, as
much as two inches. The apex of the lung and pleura is covered by the
clavicular origin of the sterno-mastoid, the sterno-thyroid, and a part
of the scalenus anticus. It is also crossed by the subclavian vessels
in the first part of their course. As this cervical portion of lung is
peculiarly liable to tubercular disease, it[Pg 18] should always be carefully
examined. Its condition may be ascertained by percussion near the
sternal end of the clavicle.
31. Supra-clavicular fossa.—The hollow above the clavicle,
between the sterno-mastoid and the trapezius, is very manifest in
emaciation and old age. Notice the termination here of the external
jugular vein. In some necks only a small depression is visible,
particularly when the trapezius has a broad insertion into the
clavicle, and comes well forwards, so that its front border gives a
graceful contour to the base of the neck.
32. Subclavian artery.—In the supra-clavicular fossa, near
the outer border of the sterno-mastoid, and about one inch above the
clavicle, we feel the pulsation of the subclavian artery. Here the
artery lies upon the first rib, and can be effectually compressed. A
little pressure is sufficient. But the pressure must be made in the
right direction, or the artery will be pressed off the rib instead
of against it. The plane of the rib is such that the pressure, to be
effectual, must be made in a direction downwards and a little inwards.
It is best to stand behind the shoulder and make the pressure with one
thumb.
It is worth remembering that the outer border of the sterno-mastoid
corresponds pretty nearly with the outer edge of the scalenus anticus,
which is the surgical guide to the subclavian artery.
By pressing deeply at the upper part of the supra-clavicular fossa, the
transverse process of the seventh cervical vertebra can be distinctly
felt.
In long and thin necks, a thin cord is perceptible, running nearly
parallel with and just above the clavicle. It is the posterior belly of
the omo-hyoideus. See it rising and falling in breathing, and making
tense during inspiration that part of the cervical fascia which lies
over the cervical portion of the lung. Thus it may be said to be in all
respects a muscle of inspiration, co-operating with the sterno-mastoid
and scaleni. In the language of transcendental anatomy, we may say that
the central tendon of the omo-hyoid represents a rudimentary cervical
rib. Its posterior belly is analogous to a serration of the serratus
magnus; its anterior belly to a sterno-hyoid.
[Pg 19]
THE CHEST.
33. As a rule, the right half of the chest is slightly larger than the
left. Of ninety-two persons of the male sex and good constitutions,
seventy-one had the right side the larger; eleven the left; ten had
both sides equal. The maximum of difference in favour of the right was
one inch and a quarter. The measurements were made on a plane with the
nipple.
34. Peculiarities in the female.—The chest of the female
differs from that of the male in the following points:—Its general
capacity is less; the sternum is shorter; the upper opening is larger
in proportion to the lower; the upper ribs are more movable, and
therefore permit a greater enlargement of the chest at its upper part,
in adaptation to the requirements of pregnancy.
35. The top of the sternum is on a level with the second dorsal
vertebra; and the available space between the top of the sternum and
the spine is hardly more than two inches.[2]
36. Parts behind first bone of sternum.—There is little or no
lung behind the first bone of the sternum, the space being occupied by
the trachea and large vessels as follows:—
The left vena innominata crosses the sternum just below the upper
border. Next come the great primary branches of the arch of the aorta.
Deeper still is the trachea dividing into its two bronchi opposite the
junction of the first and second bones of the sternum. Deepest of all
is the œsophagus.
About one inch from the upper border of the sternum is the highest part
of the arch of the aorta, which lies on the bifurcation of the trachea.
37. The course of the arteria innominata corresponds with a line drawn
from the middle of the junction of the first with the second bone of
the sternum, to the right sterno-clavicular joint. When the artery
rises higher than usual into the neck, its pulsation can be felt in the
fossa above the sternum.
38. Rules for counting the ribs.—In fat persons it is[Pg 20] often
difficult to count the ribs; hence the following rules may be useful:—
a. The finger passed down from the top of the sternum soon
comes to a transverse projection, slight, but always to be felt, at
the junction of the first with the second bone of the sternum. This
corresponds with the level of the cartilage of the second rib.
b. The nipple of the male is placed, in the great majority of
cases, between the fourth and the fifth ribs, about three-quarters of
an inch external to their cartilages.
c. The lower external border of the pectoralis major corresponds
with the direction of the fifth rib.
d. A line drawn horizontally from the nipple round the chest
cuts the sixth intercostal space midway between the sternum and the
spine. This is a useful rule in tapping the chest.
e. When the arm is raised, the highest visible digitation of the
serratus magnus corresponds with the sixth rib. The digitations below
this correspond respectively with the seventh and eighth ribs.
f. The scapula lies on the ribs from the second to the seventh,
inclusive.
g. The eleventh and twelfth ribs can be felt even in corpulent
persons, outside the erector spinæ, sloping downwards.
h. One should remember the fact that the sternal end of each rib
lies on a lower level than its corresponding vertebra. For instance, a
line drawn horizontally backwards from the middle of the third costal
cartilage at its junction with the sternum, to the spine, would touch
the body, not of the third dorsal vertebra, but of the sixth. Again,
the end of the sternum would be on about the level of the tenth dorsal
vertebra. Much latitude must be allowed here for variation in the
length of the sternum, especially in women.
39. Interval below clavicle.—Immediately below the clavicle
we recognise the triangular interval between the pectoralis major
and the deltoid. This space varies in different cases, depending on
the distance between the[Pg 21] muscles. It is important as a guide to the
coracoid process and the axillary artery. In a case of injury to the
shoulder, to ascertain whether the coracoid process is broken, carry
the arm outwards, to put the deltoid and pectoral muscles on the
stretch, and make manifest the space between their opposite borders.
Pressing the thumb into the space we can feel the inner side of the
coracoid process, the apex being under the fibres of the deltoid; thus
it is easy to ascertain whether it be broken. Moreover, this space
corresponds with the line of the axillary artery; here its pulsation
can be distinctly felt, and here it can be compressed (but not easily,
or for long) against the second rib.
40. Internal mammary artery.—The line of the internal mammary
artery runs perpendicularly behind the cartilages of the ribs, about
half an inch from the sternum. The perforating branch through the
second intercostal space is generally the largest.
41. Outline of heart on chest-wall.—To have a general idea of
the form and position of the heart, map its outline on the wall of the
chest, as follows:—
a. To define the base draw a transverse line across the sternum
corresponding with the upper borders of the third costal cartilages:
continue the line half an inch to the right of the sternum and one inch
to the left.
b. To find the apex, mark a point about two inches below the
left nipple, and one inch to its sternal side. This point will be
between the fifth and sixth ribs.
c. To find the lower border (which lies on the central tendon of
the diaphragm), draw a line, slightly curved downwards, from the apex
across the bottom of the sternum (not the ensiform cartilage) as far as
its right edge.
d. To define the right border (formed by the right auricle),
continue the last line upwards with an outward curve, so as to join the
right end of the base.
e. To define the left border (formed by the left ventricle),
draw a line curving to the left, but not including the nipple, from the
left end of the base to the apex.
Such an outline (seen in the cut, page 22, with the angles[Pg 22] rounded
off) shows that the apex of the heart points downwards and towards the
left, the base a little upwards and towards the right; that the greater
part of it lies in the left half of the chest, and that the only part
which lies to the right of the sternum is the right auricle. A needle
introduced in the third, the fourth, or the fifth right intercostal
space close to the sternum would penetrate the lung and the right
auricle.
A needle passed through the second intercostal space, close to the
right side of the sternum, would, after passing through the lung, enter
the pericardium and the most prominent part of the bulge of the aorta.
A needle passed through the first intercostal space, close to the right
side of the sternum, would pass through the lung and enter the superior
vena cava above the pericardium.
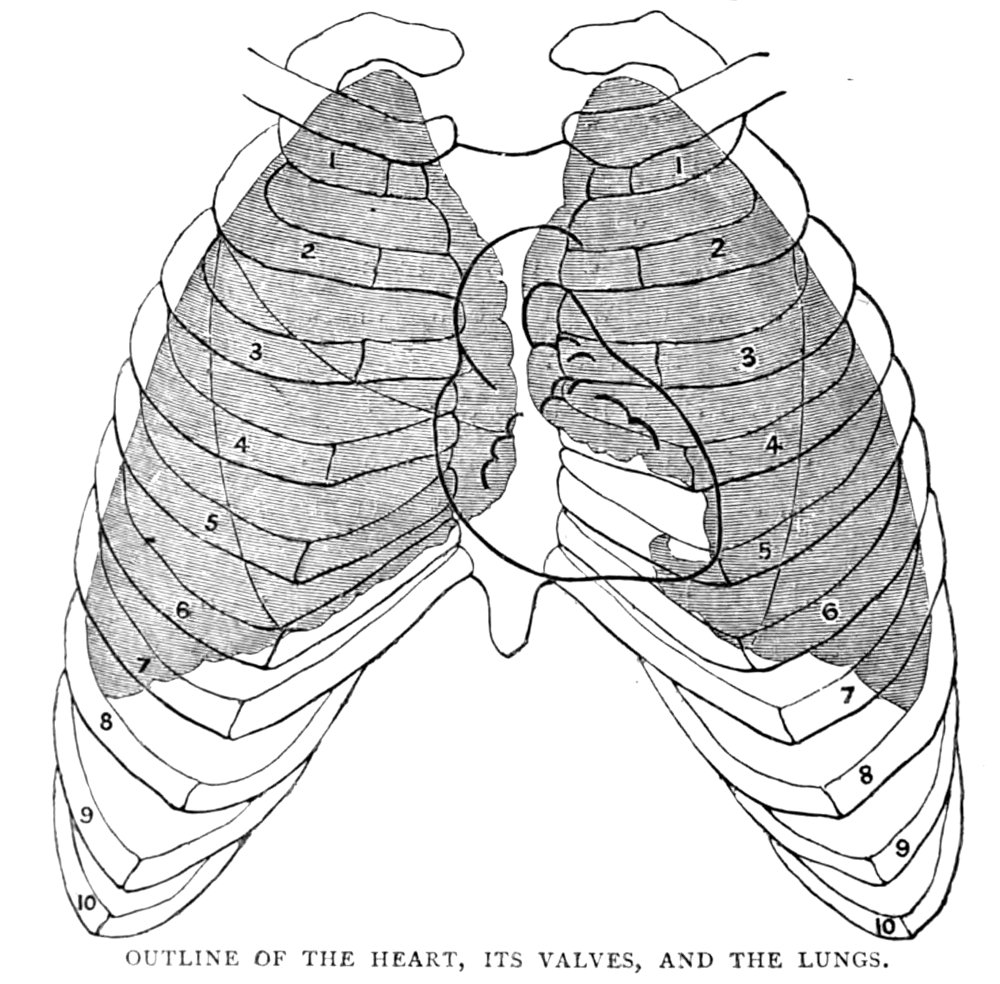
OUTLINE OF THE HEART, ITS VALVES, AND THE LUNGS.
42. The best definition of that part of the præcordial region which is
less resonant on percussion, was given by[Pg 23] Dr. Latham years ago in his
‘Clinical Lectures.’ ‘Make a circle of two inches in diameter round a
point midway between the nipple and the end of the sternum. This circle
will define, sufficiently for all practical purposes, that part of the
heart which lies immediately behind the wall of the chest, and is not
covered by lung or pleura.’
Apex of the heart.—The apex of the heart pulsates between the
fifth and sixth ribs, two inches below the nipple, and one inch to its
sternal side. The place and extent, however, of the heart’s impulse,
vary a little with the position of the body. Of this anyone may
convince himself by leaning forwards, backwards, on this side and on
that, feeling, at the same time, the heart. Inspiration and expiration
also alter the position of the heart. In a deep inspiration it may
descend half an inch, and can be felt beating at the pit of the stomach.
43. Valves of the heart.—The aortic valves lie behind the third
intercostal space, close to the left side of the sternum.
The pulmonary valves lie in front of the aortic behind the junction of
the third costal cartilage, on the left side, with the sternum.
The tricuspid valves lie behind the middle of the sternum, about the
level of the fourth costal cartilage.
The mitral valves (the deepest of all) lie behind the third intercostal
space, about one inch to the left of the sternum.
Thus these valves are so situated that the mouth of an ordinary sized
stethoscope will cover a portion of them all, if placed over the
sternal end of the third intercostal space, on the left side. All are
covered by a thin layer of lung; therefore we hear their action better
when the breathing is for a moment suspended.
44. Outline of the lungs.—Now let us trace on the chest the
outline of the lungs, with as much precision as their expansion and
contraction in breathing permit. (See the cut.)
45. The apex of each lung rises into the neck behind the sternal end of
the clavicle and sterno-mastoid muscle as much as an inch and a half:
in females rather higher than in males (30).[Pg 24] From the sternal ends of
the clavicles the lungs converge, so that their thin edges almost meet
in the mesial line on a level with the second costal cartilage. Thus
there is little or no lung behind the first bone of the sternum. From
the level of the second costal cartilage to the level of the fourth,
the margins of the lungs run parallel, or nearly so, close behind the
middle of the sternum: consequently their thin edges overlap the great
vessels and valves at the base of the heart.
Below the level of the fourth costal cartilage the margins of the
lungs diverge, but not in an equal degree. The margin of the right
corresponds with the direction of the cartilage of the sixth rib:
the margin of the left, being notched for the heart, runs behind the
cartilage of the fourth. A line drawn perpendicularly from the nipple
would find the lung margin about the lowest part of the sixth rib.
Laterally, i.e. in the axillary line, the lung margin comes down
as low as the eighth rib: posteriorly, i.e. in the dorsal or
scapular line, it descends as low as the tenth.
It should be remembered that, in a deep inspiration, the lung margins
descend about one inch and a half.
In children the lungs are separated in front by the thymus gland.
Allowance should be made for this. About the approach of puberty the
thymus disappears.
46. Anterior mediastinum.—The direction of the anterior
mediastinum is not straight down the middle of the sternum, but slants
a little to the left, owing to the position of the heart. The right
pleural sac generally encroaches a little upon the left, behind the
middle of the sternum. A needle introduced through the middle of the
sternum opposite the third or the fourth rib would go through the right
pleura.
47. Reflection of pleura.—The reflection of the pleura from the
wall of the chest on to the diaphragm corresponds with a sloping line
drawn from the bottom of the sternum over the cartilages of the ribs
down to the lower border of the last rib.
Since the pleura lines the inside of the last rib, a musket ball or
other foreign body, loose in the pleural sac, and rolling on the
diaphragm, might fall to the lowest part of the sac,[Pg 25] which would be
between the eleventh and twelfth ribs. The ball might be extracted
here. The chest might also be tapped here, but not with a trochar,
since a trochar would penetrate both layers of pleura, and go through
the diaphragm into the abdomen.
The operation should be done cautiously, by an incision beginning about
two inches from the spine, on the outer border of the ‘erector spinæ,’
on a level between the spines of the eleventh and twelfth dorsal
vertebræ. The intercostal artery will not be injured if the opening be
made below the middle of the space, which is very wide.[3]
THE BACK.
48. Median furrow.—In a muscular man, a furrow, caused by the
prominence of the erector spinæ on each side, runs down the middle of
the back. The lower end of the furrow corresponds with the interval
between the spine of the last lumbar and that of the first sacral
vertebra.
49. Spines of vertebræ.—A little friction with the fingers down
the backbone will cause the spines of the vertebræ to be tipped with
red, so that they can be easily counted, and any deviation from the
straight line detected. Still it is worth remembering that the spine of
the third dorsal is on a level with the commencement of the spine of
the scapula—that the spine of the seventh dorsal is on a level with
the inferior angle of the scapula—that the spine of the last dorsal is
on a level with the head of the last rib.
Division of the trachea.—The division of the trachea is
opposite the spine of the third, in some cases the fourth, dorsal
vertebra. In front this division is on the level of the junction of the
first with the second bone of the sternum.
The root of the spine of the scapula is marked by a slight dimple
in the skin. This is on a level with the third intercostal space. A
stethoscope placed on the inner side of this dimple would cover the
bronchus, more especially the right, since it is nearer to the chest
wall.
[Pg 26]
Make a man lean forwards, with his arms folded across the chest; this
will make prominent the spines of the vertebræ. The lower border of the
trapezius will guide you to the spine of the twelfth dorsal vertebra.
50. The place where the kidney is most accessible to pressure is below
the last rib, on the outer edge of the erector spinæ.
51. The highest part of the ilium is about the level of the fourth
lumbar spine. The best incision for opening the descending colon is
in a slightly sloping line beginning at the outer edge of the erector
spinæ, midway between the crest of the ilium and the last rib, and
continued across the flank for three inches or more, according to the
amount of subcutaneous fat.
52. In the pit of the neck we can feel the trapezius and the ligamentum
nuchæ. By pressing deeply we detect the forked and prominent spine of
the second cervical vertebra.
53. The spines of the third, fourth, and fifth cervical vertebræ recede
from the surface to permit free extension of the neck, and cannot often
be felt. But the spines of the sixth and seventh (v. prominens) stand
out well.
54. Notice that most of the spines of the dorsal vertebræ, owing to
their obliquity, do not tally with the heads of their corresponding
ribs. Thus, the spine of the second dorsal corresponds with the head
of the third rib; the spine of the third dorsal with the head of the
fourth rib, and so on till we come to the eleventh and twelfth dorsal
vertebræ, which do tally with their corresponding ribs. All this,
however, is best seen in the skeleton.
55. The spines of the vertebræ may be useful as landmarks indicative
of the levels of important organs. I have therefore arranged them in a
tabular form, thus:—
Tabular Plan of Parts opposite the Spines of the Vertebræ.
|
Cervical.
|
5th.
|
Cricoid cartilage. Œsophagus begins.[Pg 27]
|
|
7th.
|
Apex of lung: higher in the female than in the male. (30)
|
|
Dorsal.
|
1st.
| |
| 2nd.
|
|
| 3rd.
|
Aorta reaches spine. Apex of lower lobe of lung. Angle of bifurcation of trachea. (49)
|
| 4th.
|
Aortic arch ends. Upper level of heart.
|
| 5th.
|
| 6th.
|
| 7th.
|
|
|
8th.
|
Lower level of heart. Central tendon of diaphragm.
|
| 9th.
|
Œsophagus and vena cava through diaphragm. Upper edge of spleen.
|
|
10th.
|
Lower edge of lung. Liver comes to surface posteriorly. Cardiac orifice of stomach.
|
| 11th.
|
Lower border of spleen. Renal capsule.
|
| 12th.
|
Lowest part of pleura. Aorta through diaphragm. Pylorus.
|
|
Lumbar.
|
1st.
|
Renal arteries. Pelvis of kidney. (83) |
|
2nd.
|
Termination of spinal cord. Pancreas. Duodenum just below. Receptaculum chyli. |
| 3rd.
|
Umbilicus. Lower border of kidney. |
|
4th.
|
Division of aorta. (65) Highest part of ilium. |
|
5th. | |
56. Origins of the spinal nerves.—It is useful to know opposite
what vertebræ the spinal nerves in the different regions arise from the
spinal cord. They arise as follows:—
The origins of the eight cervical nerves correspond to the interval
between the occiput and the sixth cervical spine.
The origins of the first six dorsal nerves correspond to the interval
between the sixth cervical and the fourth dorsal spines.
The origins of the six lower dorsal nerves correspond to the interval
between the fourth and the eleventh dorsal spines.
The origins of the five lumbar nerves correspond to the interval
between the eleventh and twelfth dorsal spines.
The origins of the five sacral nerves correspond to the spines of the
last dorsal and the first lumbar vertebræ.
57. Movements of the spine.—The movements of which the spine
is capable are threefold: 1. Flexion and extension; 2. Lateral
inclination; 3. Torsion. Flexion and extension[Pg 28] are freest between the
third and the sixth cervical vertebræ, between the eleventh dorsal
and the second lumbar, and between the last lumbar and the sacrum.
This is well marked in severe cases of opisthotonos, where the body is
supported on the back of the head and heels.[4]
Still better may it be observed when a mountebank bends backwards, and
touches the ground with his head.
The lateral movement is freest in the neck and the loins.
The movement of torsion or rotation round its own axis may be proved by
the following experiment:—Seated upright, with the back and shoulders
well applied against the back of a chair, we can turn the head and neck
as far as 70°. Leaning forwards so as to let the dorsal and lumbar
vertebræ come into play, we can turn 30° more.
58. Position and motions of scapula.—There are a few points
worthy of observation about the scapula. It covers the ribs from the
second to the seventh inclusive. We can feel its superior angle covered
by the trapezius. The inferior angle is covered by the latissimus
dorsi, which keeps it well applied against the ribs in the strong and
athletic; but in weak and consumptive persons the lower angles of the
scapulæ project like wings—hence the term ‘scapulæ alatæ.’
A line drawn horizontally from the spine of the sixth dorsal vertebra
over the inferior angle of the scapula gives the upper border of the
latissimus dorsi. Another line drawn from the root of the spine of the
scapula to the spine of the last dorsal vertebra gives the lower border
of the trapezius, which stands a little in relief.
59. The sliding movement of the scapula on the chest can be properly
understood only on the living subject. It can move not only upwards
and downwards as in shrugging the shoulders—backwards and forwards
as in throwing back the shoulders—but it has a rotatory movement
round a movable centre. This rotation is seen while the arm is being
raised from the horizontal to the vertical position, and is effected
by the co-operation of the trapezius with the serratus magnus. The
glenoid cavity is thus made to look upwards,[Pg 29] the inferior angle slides
forwards, and is well held under the latissimus dorsi.
60. For the medical examination of the back, the patient should sit
with the arms hanging between his thighs, to lower the scapulæ as much
as possible. In this position the spine of the scapula corresponds
(nearly) with the fissure between the upper and lower lobes of the
lung; the apex of the lower lobe being about the level of the third rib.
THE ABDOMEN.
The student is assumed to be familiar with the conventional lines
dividing the abdomen into regions.
61. Abdominal lines.—The linea alba, or central line of the
abdomen, marks the union of the aponeuroses of the abdominal muscles.
It runs from the apex of the ensiform cartilage to the symphysis pubis.
As this line is the thinnest and least vascular part of the abdominal
wall, we make our incision along it in ovariotomy, and in the high
operation of lithotomy; in it, we tap the abdomen in ascites, and the
distended bladder in retention of urine.
The so-called ‘linea semilunaris,’ at the outer border of the sheath of
the rectus, corresponds with a line, drawn slightly curved (with the
concavity towards the linea alba), from the lowest part of the seventh
rib to the spine of the pubes. This line would be in an adult about
three inches from the umbilicus; but in an abdomen distended by dropsy
or other cause, the distance is increased in proportion.
It is important to know the position of the ‘lineæ transversæ,’ or
tendinous intersections across the rectus abdominis. There are rarely
any below the umbilicus, and generally three above it. The first is
about the level of the umbilicus. The second is about four inches
higher—that is, about the level of the lowest part of the tenth rib.
These are the principal lines, and they divide the upper part of each
rectus into two nearly quadrilateral portions, an upper and a lower:
of these, those on the right side are a trifle larger than on the
left. We[Pg 30] see these muscular squares pretty plainly in some athletic
subjects. Much more frequently we see them, too much exaggerated, on
canvas and in marble. Artists are apt to exaggerate them, and make the
front of the belly too much like a chess-board. It is lucky for them
that all the world do not see with anatomical eyes.
A familiarity with the shape and position of these divisions of the
rectus is of importance, lest we should, in ignorance, make a mistake
in our diagnosis. A spasmodic contraction of one of these divisions,
particularly the upper, or a collection of matter within its sheath,
has been frequently mistaken for deep-seated abdominal disease.
In the erect position, the anterior superior spines of the ilia are a
little below the level of the promontory of the sacrum. The bifurcation
of the aorta is on about the level of the highest part of the crest of
the ilium.
62. Umbilicus.—The umbilicus is not midway between the ensiform
cartilage and the pubes, but rather nearer to the pubes. In all cases
it is situated above the centre of a man’s height. It is a vulgar error
to say that when a man lies with legs and arms outstretched, and a
circle is drawn round him, the umbilicus lies in the centre of it. This
central point is in most persons just above the pubes.
In very corpulent persons two deep transverse furrows run across the
abdomen. One runs across the navel and completely conceals it. The
other is lower down, just above the fat of the pubes. In tapping
the bladder above the pubes in such a case, the trochar should be
introduced where this line intersects the linea alba.
Although the position of the umbilicus varies a little in different
persons, as the abdomen is unusually protuberant or the reverse, still,
as a general rule, it is placed about the level of the body of the
third lumbar vertebra. Now, since the aorta divides a little below the
middle of the fourth lumbar, it follows that the best place to apply
pressure on this great vessel is one inch below the umbilicus, and
slightly to the left of it (65). That the aorta can, under favourable
circumstances, be compressed under chloroform sufficiently to cure[Pg 31]
an aneurysm below it, is proved by recorded cases, and by none more
effectually than by a case related in the second volume of the ‘Reports
of St. Bartholomew’s Hospital.’
It may be asked, why not apply pressure on the aorta above the
umbilicus? The answer is, that the aorta above the umbilicus is farther
from the surface, and is, moreover, covered by important structures
upon which pressure would be dangerous.
63. Parts behind linea alba.—Let us next consider what viscera
lie immediately behind the linea alba. For two or three fingers’
breadth below the ensiform cartilage there is the left lobe of the
liver, which here crosses the middle line. Below the edge of the
liver comes the stomach, more or less in contact with the linea alba,
according to its degree of distension. In extreme distension the
stomach pushes everything out of the way, and occupies all the room
between the liver and the umbilicus. When empty and contracted, it
retreats behind the liver, and lies flat in front of the pancreas at
the back of the abdomen; thus giving rise to the hollow termed the ‘pit
of the stomach.’ But as the stomach distends, it makes a considerable
fulness where there was a pit. The middle of the transverse colon lies
above the umbilicus, occupying space (vertically two or three inches)
according to its distension. Behind and below the umbilicus, supposing
the bladder contracted, are the small intestines, covered by the great
omentum.
64. Peritoneum.—The peritoneum is in contact with the linea
alba all the way down to the pubes, when the bladder is empty. But
when the bladder distends, it raises the peritoneum from the middle
line above the pubes; so that with a bladder distended half-way up
to the umbilicus, there is a space of nearly two inches above the
symphysis where the bladder may be tapped without risk of injury to
the peritoneum. For the same reason, we have space sufficient for the
successful performance of the high operation for stone. This fact in
anatomy must have been well understood by Jean de Dot, the smith at
Amsterdam, who, in the seventeenth century, cut himself in the linea
alba above the pubes, and took out of his[Pg 32] bladder a stone as large as
a hen’s egg. The stone, the knife, and the portrait of the operator,
may be seen to this day in the museum at Leyden.
65. Division of Aorta.—The aorta generally divides at a point
one inch and a half below the umbilicus. A more reliable guide to this
division than the umbilicus, is a point (a very little to the left) of
the middle line about the level of the highest part of the crest of the
ilium. A line drawn with a slight curve outwards from this point to the
groin, where the pulsation of the common femoral can be distinctly felt
(rather nearer to the pubes than the ilium), gives the direction of the
common iliac and external iliac arteries. About the first two inches of
this line belong to the common iliac, the remainder to the external.
Slight pressure readily detects the pulsation of the external iliac
above ‘Poupart’s ligament.’
As a rule, the length of the common iliac is about two inches, but it
should be remembered there are frequent deviations. It may be between
three-quarters of an inch and three inches and a half long. These
varieties may arise either from a high division of the aorta, or a low
division of the common iliac, or both. It is impossible to ascertain
during life what is its length in a given instance, for there is no
necessary relation between its length and the height of the stature. It
is often short in tall men, and vice versâ. Anatomists generally
describe the right as a trifle longer than the left; but their average
length is pretty nearly the same.
66. Mr. Abernethy, who in the year 1796 first put a ligature round
the external iliac, made his incision in the line of the artery. But
the easiest and safest way to reach the vessel is by an incision
(recommended in the first instance by Sir Astley Cooper, and now
generally adopted), beginning just on the inner side of the artery, a
little above Poupart’s ligament, and continued upwards and outwards
a little beyond the spine of the ilium. The same incision extended
farther in the same direction would reach the common iliac.
[Pg 33]
67. Bony prominences.—The anterior superior spine of the
ilium, the spine of the pubes, and the line of Poupart’s ligament, are
landmarks with which every surgeon should be thoroughly familiar.
68. Spine of ilium.—The spine of the ilium is the spot from
which we measure the length of the lower extremity. It is a valuable
landmark in determining the nature of injuries to the pelvis and
the hip. The thumb easily feels the spine, even in fat persons. Its
position with regard to the trochanter major should be carefully
examined. The best way to do this is to place the thumbs firmly on the
opposite spines, and to grasp the trochanters with the fingers. Any
abnormal position on one side is thus easily ascertained with the sound
side as a guide.
69. Spine of pubes.—The spine of the pubes is the best guide
to the external abdominal ring. It cannot easily be felt by placing
the finger directly over it, since it is generally covered by fat. To
feel it distinctly, we should push up the skin of the scrotum and get
beneath the subcutaneous fat. If there be any difficulty in finding it,
abduct the thigh, and the tense tendon of the adductor longus will lead
up to it.
The position of the spine of the pubes is appealed to as a means of
diagnosis in doubt between inguinal and femoral hernia. The spine lies
on the outer side of the neck of an inguinal hernia, on the inner side
of the neck of a femoral.
The spine of the pubes is nearly on the same horizontal line as the
upper part of the trochanter major. In this line, about one full
inch external to the spine, is the femoral ring. Here is the seat of
stricture in a femoral hernia.
70. Poupart’s ligament, or crural arch.—The line of Poupart’s
ligament (crural arch) is in most persons indicated by a slight
crescent-like furrow along the skin. It corresponds with a line drawn
not straight, but with a gentle curve downwards from the spine of
the ilium to the spine of the pubes. With the help of the preceding
landmarks it is easy to find the exact position of the external and
internal abdominal rings, and the direction of the inguinal canal.
71. Abdominal rings.—The external abdominal ring is[Pg 34] situated
immediately above the spine of the pubes. It is an oval opening with
the long axis directed obliquely downwards and inwards. Though its size
varies a little in different persons, yet as a rule it will admit the
end of the little finger, so that we can tell by examination whether
it be free or otherwise. To ascertain this, the best way is to push up
the thin skin of the scrotum before the finger; then, by tracking the
spermatic cord, the finger readily glides over the crest of the pubes
and feels the sharp margins of the ring.
The position of the internal ring is about midway between the spine of
the ilium and the symphysis of the pubes, and about two-thirds of an
inch above Poupart’s ligament.
72. Inguinal canal.—The position of the external and internal
abdominal rings being ascertained, it is plain that the direction of
the inguinal canal must be obliquely downwards and inwards, and that
its length in a well-formed adult male is from one and a half to two
inches, according as we include the openings or not. In very young
children the canal is much shorter and less oblique, the inner ring
being behind the outer. With the growth of the pelvis in its transverse
direction, the anterior spines of the ilia become farther apart, and
thus draw the internal ring more and more away from (i.e. to the
outer side of) the external.
73. Spermatic cord.—The spermatic cord can be felt as it
emerges through the external ring, and its course can be tracked into
the scrotum. The vas deferens can be distinctly felt at the back of the
cord, and separated from its other component parts.
74. Epigastric artery.—The direction of the deep epigastric
artery corresponds with a line drawn from the inner border of the
internal ring up the middle of the rectus muscle, towards the chest.
In thin persons the absorbent glands which lie along Poupart’s ligament
can be distinctly felt. They are usually oval, with their long axes
parallel to the line of the ligament.
75. Abdominal viscera.—Now let us see how far we can make out
externally the position and size of the abdominal viscera.
[Pg 35]
To make this examination with anything like success, it is desirable to
relax the abdominal muscles. The man should be on his back, the head,
shoulders and thorax being well raised, to relax the recti muscles; and
the thighs bent on the abdomen, to relax the several fasciæ attached to
the crural arch. To induce complete relaxation, where a very careful
examination is desired, chloroform should be given.
In manipulating the abdomen we should not use the tips of the fingers.
This is sure to excite the contraction of the muscles. The flat hand
should be gently pressed upon it, and with an undulating movement.
76. It is well to bear in mind that the central tendon of the diaphragm
is about the level of the lower end of the sternum at its junction with
the seventh costal cartilage; that the right half of the diaphragm
rises to about the level of the fifth rib—that is, about an inch below
the nipple; that the left half does not rise quite so high. In tranquil
breathing the diaphragm descends about half an inch.
The position of the abdominal viscera varies, to a certain extent,
in different persons. In some of them, especially the stomach, their
position varies in the same person at different times.
Let us take, first, the largest of the abdominal viscera—the liver.
77. Liver.—The liver lies under the right hypochondrium,
and passes across the middle line over the stomach into the left
hypochondrium, generally speaking, as far as the left mammary line.
The extent to which it can be felt below the edges of the ribs depends
upon whether it is enlarged or not, as well as upon its texture, and
also upon the amount of flatus in the stomach and intestines. As a
rule, in health its lower thin border projects about half an inch
below the costal cartilages, and can be felt moving up and down with
the action of the diaphragm; but it requires an educated hand to feel
it. An uneducated hand would miss it altogether. That part of it,
however, which crosses the middle line below the ensiform cartilage is
much more accessible to the feel; here it lies immediately behind the
linea alba, and in front of[Pg 36] the stomach, nearly half-way down to the
umbilicus. Here, therefore, is the best place to feel whether the liver
be enlarged or pushed down lower than it ought to be. If it be much
enlarged and much lower, even the most untutored hand could detect its
edge.
Even if the edge of the liver be felt very much lower than is normal
below the ribs, it does not necessarily follow that the liver is
enlarged, since it may be pressed down by other causes—for instance,
the habit of wearing tight stays.
To what height does the liver ascend? This can only be ascertained by
careful percussion of the chest-wall. The highest part of its convexity
on the right side is about one inch below the nipple, or nearly on a
level with the external and inferior angle of the pectoralis major.
Posteriorly the liver comes to the surface below the base of the right
lung, about the level of the tenth dorsal spine.
Roughly speaking, the upper border of the liver corresponds with the
level of the tendinous centre of the diaphragm; that is, the level of
the lower end of the sternum. Thus a needle thrust into the right side,
between the sixth and seventh ribs, would traverse the lung, and then
go through the diaphragm into the liver.
78. Gall bladder.—The gall bladder, or rather the fundus of it,
is situated, but cannot be felt, just below the edge of the liver about
the ninth costal cartilage, outside the edge of the right rectus muscle.
79. Stomach.—The stomach varies in size more than any organ in
the body. When empty and contracted (63) it lies at the back of the
abdomen, overlapped by the left lobe of the liver, and in front of the
pancreas. When very full, it turns on its axis and swells up towards
the front, coming close behind the wall of the abdomen, occupying
most of the left hypochondrium and epigastrium, displacing the other
contiguous organs, pushing in every direction, and often interfering
with the action of the heart and left lung. Hence the palpitation and
distressing heart-symptoms in indigestion and flatulence.
The cardiac orifice of the stomach lies to the left of the[Pg 37] middle
line, just below the level of the junction of the seventh costal
cartilage with the sternum.
80. Pylorus.—The pylorus lies under the liver, on the right
side, near the end of the cartilage of the eighth rib; but it cannot be
felt unless occasionally when enlarged and hardened by disease.
81. Spleen.—The spleen, if healthy, cannot be felt, so
completely is it sheltered by the ribs. It lies on the left side,
connected to the great end of the stomach, beneath the ninth, tenth,
and eleventh ribs, between the axillary lines—lines drawn vertically
downwards from the anterior and posterior margins of the axilla. Its
upper edge is on a level with the spine of the ninth dorsal vertebra,
its lower with the spine of the eleventh.
Its position and size, therefore, in health can only be ascertained,
and not very accurately, by the extent of dulness on percussion.
The greatest amount of dulness would be over the tenth and eleventh
ribs; above this the thin edge of the lung would intervene between
the spleen and the abdominal wall. If, therefore, the spleen can be
distinctly felt below the ribs, it must be enlarged. In proportion to
its enlargement, so can its lower rounded border be detected below the
tenth and eleventh ribs, especially when forced downwards by a deep
inspiration.[5]
82. Pancreas.—The pancreas lies transversely behind the
stomach, and crosses the aorta and the spine about the junction of the
first and second lumbar vertebræ. The proper place to feel for it,
therefore, would be in the linea alba about two or three inches above
the umbilicus. Is it perceptible to the touch?—only under very deep
pressure, and very favourable circumstances, such as an emaciated and
empty abdomen. It is worth remembering that it may be felt under such
conditions. The pancreas of normal size, in thin persons, has been
mistaken for disease—disease of the transverse arch of the colon, or
aneurysm of the abdominal aorta.
83. Kidney.—The kidney lies at the back of the abdomen, on the
quadratus lumborum and psoas muscles, opposite the two lower dorsal and
two upper lumbar spines. The right,[Pg 38] owing to the size of the liver,
is a trifle—say, three-quarters of an inch—lower than the left. The
pelvis of the kidney is on about the level of the spine of the first
lumbar vertebra: the upper border is on about the level of the space
between the eleventh and twelfth dorsal spines; the lower border comes
as low as the third lumbar spine. During a deep inspiration both
kidneys are depressed by the diaphragm nearly half an inch.
Can we feel the normal kidney? The only place where it is accessible to
pressure is just below the last rib, on the outer edge of the ‘erector
spinæ.’ I say accessible to pressure, for I have never succeeded in
satisfying myself that I have distinctly felt its rounded lower border
in the living subject, nor even in the dead, with the advantage of
flaccid abdominal walls and the opportunity of making hard pressure
with both hands, placed simultaneously, one in front of the abdomen,
the other on the back. For these reasons, although we can easily
ascertain its degree of tenderness, we cannot actually feel it unless
it be considerably enlarged.
We must be on our guard not to mistake for the kidney an enlarged liver
or spleen, or an accumulation of fæces in the lumbar part of the colon.
84. Large intestine.—Let us now trace the large intestine and
see where it is accessible to pressure. The ‘cæcum,’ or ‘caput coli,’
and the ileo-cæcal valve lie in the right iliac fossa. The ascending
colon runs up the right lumbar region over the right kidney. The
transverse colon crosses the abdomen two or three inches above the
umbilicus. The descending colon lies in the left lumbar region in front
of the left kidney. The sigmoid flexure occupies the left iliac fossa.
Throughout this tortuous course, except at the hepatic and splenic
flexures, the colon is accessible to pressure, and we could, under
favourable circumstances, detect hardened fæces in it. In a case which
occurred in St. Bartholomew’s Hospital, a collection of fæces in the
transverse colon formed a distinct tumour in the abdomen. All the
symptoms yielded to large and repeated injections of olive oil. In[Pg 39]
another case an accumulation of fæcal matter in the sigmoid flexure
during life was mistaken for a malignant disease.
85. Colotomy.—The operation of opening the colon (colotomy) may
be done in the right or left loin, below the kidney, in that part of
the colon not covered by peritoneum.
The landmarks of the operation are:—(1) The last rib, of which feel
the sloping edge; (2) the crest of the ilium; (3) the outer border of
the ‘erector spinæ.’ The incision should be about three inches long,
midway between the rib and the ilium. It should begin at the outer
border of the ‘erector spinæ,’ and should slope downwards and outwards
in the direction of the rib. The edge of the ‘quadratus lumborum,’
which is the guide to the colon, is about one inch external to the edge
of the ‘erector spinæ,’ or three full inches from the lumbar spines.
The line of the gut is vertical, and runs for a good two inches between
the lower border of the kidney and the iliac crest on the left side;
rather less on the right.
Small intestines.—All the room below the umbilicus is occupied
by the small intestines. The coils of the jejunum lie nearer to the
umbilicus (one reason of the great fatality of umbilical herniæ). Those
of the ilium are lower down.
On the right side, a little below the ninth rib, the colon lies close
to the gall bladder, and is, after death, sometimes tinged with bile.
Posteriorly, this part of the colon is in contact with the kidney and
duodenum.
86. Bladder.—When the bladder distends, it gradually rises out
of the pelvis into the abdomen, pushes the small intestines out of the
way, and forms a swelling above the pubes, reaching in some instances
up to the navel. The outline of this swelling is perceptible to the
hand as well as to percussion. More than this, fluctuation can be
felt through the distended bladder by tapping on it in front with the
fingers of one hand, while the forefinger of the other passed up the
rectum feels the bottom of the ‘trigone.’
The body is supposed to be placed in the usual position for lithotomy.
87. Bony framework.—We can readily feel the osseous and
ligamentous boundaries of the perineum; namely, the rami of the pubes
and ischia, the tuberosities of the ischia, the great sacro-ischiatic
ligaments, and the apex of the coccyx. This framework forms a
lozenge-shaped space. If we draw an imaginary line across it from the
front of one tuber ischii to the other, we divide this space into an
anterior and a posterior triangle. The anterior is nearly equilateral,
and, in a well-formed pelvis, its sides are from three to three and a
half inches long. It is called the urethral triangle. The posterior,
containing the greater part of the anus and the ischio-rectal fossa on
each side, is called the anal triangle.
88. Raphé.—A slight central ridge of skin, called the ‘raphé,’
runs from the anus up the perineum, scrotum, and penis. This ‘raphé,’
or middle line of the perineum, is the ‘line of safety’ in making
incisions to let out matter or effused urine, or to divide a stricture.
89. Central point of perineum.—It is very important to know
that a point of the raphé about midway between the scrotum (where it
joins the perineum) and the centre of the anus, corresponds with the
so-called ‘central tendon’ where the perineal muscles meet. The bulb
of the urethra lies above this point, and never, at any age, comes
lower down. The artery of the bulb, too, never runs below this level.
Therefore the incision in lithotomy should never commence above it.
A knife introduced at this point, and pushed backwards with a very
slight inclination upwards, would enter the membranous part of the
urethra just in front of the prostate gland; pushed still farther it
would enter the neck of the bladder. This point, then, is a very good
landmark to the urethra in lithotomy, or, indeed, in any operations on
the perineum.
The incision in the lateral operation of lithotomy, beginning below
the point indicated, should be carried downwards[Pg 41] and outwards between
the anus and the tuberosity of the ischium, a little nearer to the
tuberosity than the anus. The lower end of the incision should reach a
point just below the anus.
90. Triangular ligament.—In a thin perineum, we can feel the
lower border of the deep perineal fascia or the ‘so-called’ triangular
ligament of the urethra. The urethra passes through it about one inch
below the lower part of the symphysis pubis, and about three-quarters
of an inch higher than the central tendon of the perineum. It is
important to bear in mind these landmarks in introducing a catheter.
If the catheter be depressed too soon, its passage will be resisted by
the triangular ligament; if too late, it will be likely to make a false
passage by running through the bulb.
91. Anus.—One of the most important landmarks which guide a
surgeon in his operations about the anus, is a white line[6] at the
junction of the skin and mucous membrane. It is easily recognised and
is of especial interest, because it marks with great precision the
linear interval between the external and internal sphincter muscles.
From this line the internal sphincter extends upwards, beneath the
mucous membrane, for about an inch, becoming gradually more and more
attenuated.
The wrinkled appearance of the anus is caused by the contraction of the
external sphincter. At the bottom of these cutaneous folds, especially
towards the coccyx, we look for ‘fissure of the anus.’
92. Landmarks in the rectum.—Many valuable landmarks may be
felt by introducing the finger into the rectum, with a catheter at the
same time in the urethra. The principal of these landmarks are the
following:—
a. The finger can feel the extent and powerful grasp of the
internal sphincter for about one inch up the bowel. (91)
b. Urethra.—Through the front wall of the bowel it can
most distinctly feel the track of the membranous part of the urethra,
exactly in the middle line. This is very important, because you can
ascertain with precision whether the catheter has deviated from the
proper track.
[Pg 42]
c. Prostate gland.—About an inch and a half or two
inches from the anus, the finger comes upon the prostate gland. The
gland lies in close contact with the bowel, and can be detected by its
shape and hard feel. The finger, moved from side to side, can examine
the size of its lateral lobes, their consistence and sensibility.
d. The finger, introduced still farther, can reach beyond the
prostate, as far as the apex of the trigone of the bladder. More than
this, it can feel the angle between the ‘ductus communes ejaculatorii,’
which forms the apex of the trigone. This is the precise spot where
the distended bladder should be punctured through the rectum. The more
distended the bladder, the easier can this spot be felt. Fluctuation
is at once detected by a gentle tap on the bladder above the pubes
(86). The trochar must be thrust in the direction of the axis of the
distended bladder; that is, roughly speaking, in a line drawn from the
anus through the pelvis to the umbilicus.
e. The fold of peritoneum, called the recto-vesical pouch, is
about four inches from the anus, therefore it is not within reach of
the finger; and we run no risk of wounding it in tapping the bladder if
the trochar be introduced near the angle of the trigone.
f. The finger can feel one of the ridges or folds of mucous
membrane which are situated at the lower part of the rectum. This
fold projects from the side, and sometimes from the upper part of the
rectum, near the prostate. When thickened or ulcerated, this fold
occasions great pain in defæcation; and great relief is afforded by its
division.
g. Lastly, the finger can examine the condition of the spaces
filled with fat on either side of the rectum, called the ischio-rectal
fossæ, with a view to ascertain the existence of deep-seated
collections of matter, or the internal communications of fistulæ.
Introduction of catheters.—In the introduction of catheters
the following are good rules. Keep the point of the instrument well
applied against the upper surface of the urethra;—depress the handle
at the right moment (90);—keep[Pg 43] the umbilicus in view;—in cases of
difficulty feel the urethra through the rectum, to ascertain whether
the instrument be in the right direction. Attention to these rules
diminishes the risk of making a false passage, an injury which under
great delicacy in manipulation ought never to happen.
Urethra in the child.—In children the membranous part of the
urethra is, relatively speaking, very long, owing to the smallness of
the prostate. It is also more sharply curved, because the bladder in
children is more in the abdomen than in the pelvis. It is, moreover,
composed of thin and delicate walls. The greatest gentleness,
therefore, should be used in passing a catheter; else the instrument
is likely to pass through the coats and make a false passage. Hence
the advantage of being able to ascertain through the rectum whether
the instrument be in the right track and moving freely in the bladder,
which can also be easily felt in children.
THE THIGH.
93. Poupart’s ligament, or crural arch.—Mark the anterior
superior spine of the ilium, the spine of the pubes, and define the
line of ‘Poupart’s ligament’ which extends between them. This line is
one of our guides in the diagnosis of inguinal and femoral herniæ.
If the bulk of the tumour be above the line, the hernia is probably
inguinal; if below it, femoral. The line is not a straight one drawn
from the spine of the ilium to the spine of the pubes, but slightly
curved, with the convexity downwards, owing to its close connection
with the fascia lata of the thigh. In many persons it can be distinctly
felt; in nearly all its precise course is indicated by a slight furrow
in the skin.
For the points about the spine of the pubes, refer to paragraph 69.
94. Furrow at the bend of the thigh.—When the thigh is even
slightly bent, there appears a second furrow in the skin below that at
the crural arch. This second[Pg 44] furrow begins at the angle between the
scrotum and the thigh, passes outwards, and is gradually lost between
the top of the trochanter and the anterior superior spine of the ilium.
It runs right across the front of the capsule of the hip-joint. For
this reason it is a valuable landmark in amputation at the hip-joint.
The point of the knife should be introduced externally where the furrow
begins, should run precisely along the line of it, and come out where
it ends; so that the capsule of the joint may be opened with the first
thrust. In suspected disease of the hip pressure made in this line,
just below the spine of the ilium, will tell us if the joint be tender.
Effusion into the joint obliterates all trace of the furrow, and makes
a fulness when contrasted with the opposite groin.
95. Saphenous opening.—In most persons there is a natural
depression over the saphenous opening in the fascia lata, where the
saphena vein joins the femoral. The position of this opening is just
below the inner third of Poupart’s ligament, and about an inch and a
half external to the spine of the pubes. This is the place where the
swelling of a femoral hernia first appears: therefore it ought to be
carefully examined in cases of doubt.
96. Femoral ring.—The position of the femoral ring, through
which the hernia escapes from the abdomen, is on a deeper plane, about
half an inch higher than the saphenous opening, and immediately under
Poupart’s ligament. As the plane of the ring is vertical in the supine
position of the body, the way in which we should try to reduce a
femoral hernia is by pressure, applied first in a downward direction,
afterwards in an upward. The intestine protruded has to pass back under
a sharp edge of fascia, namely, the upper horn of the saphenous opening
(known as Hey’s ligament). At the same time we bend the thigh, to relax
the fascia as much as possible.
A good way to find the seat of the femoral ring with precision is the
following:—Feel for the pulsation of the femoral artery on the pubes;
allow half an inch (on the inner side) for the femoral vein; then comes
the femoral ring.
[Pg 45]
In performing the operation for the relief of the stricture in femoral
hernia the incision through the skin should be about an inch and a half
external to the spine of the pubes. Its direction should be vertical,
and its middle should be just over the femoral ring.
97. Lymphatic glands in the groin.—The cluster of inguinal and
femoral lymphatic glands can sometimes be felt in thin persons. The
inguinal lie for the most part along the line of Poupart’s ligament:
they receive the absorbents from the wall of the abdomen, the urethra,
the penis, the scrotum, and the anus. The femoral glands lie chiefly
over the saphenous opening and along the outer side of the saphena
vein: they receive the absorbents of the lower extremity; they receive
some also from the scrotum—of which we have practical evidence in
cases of chimney-sweepers’ cancer.
98. Trochanter major.—The trochanter major is a most valuable
landmark, to which we are continually appealing in injuries and
diseases of the lower extremity. There is a natural depression over the
hip (in fat persons) where it lies very near the surface, and can be
plainly felt, especially when the thigh is rotated. Nothing intervenes
between the bone and the skin except the strong fascia of the gluteus
maximus and the great bursa underneath it.
The top of the trochanter lies pretty nearly on a level with the spine
of the pubes, and is about three-fourths of an inch lower than the top
of the head of the femur. A careful examination of the bearing of the
great trochanter to the other bony prominences of the pelvis, and a
comparison of its relative position with that of the opposite side, are
the best guides in the diagnosis of injuries about the hip, and the
position of the head of the femur.
99. Nélaton’s line.—‘If in the normal state you examine the
relations of the great trochanter to the other bony prominences of the
pelvis, you will find that the top of the trochanter corresponds to a
line drawn from the anterior superior spine of the ilium to the most
prominent part of the tuberosity of the ischium. This line also runs
through the centre of the acetabulum. The extent of displacement in[Pg 46]
dislocation or fracture is marked by the projection of the trochanter
behind and above this line.’[7]
‘Nélaton’s line,’ as it is termed, theoretically holds good. But in
stout persons it is not always easy to feel these bony points so as
to draw the line with precision. A surgeon must, after all, in many
cases trust to measurement by his eyes and his flat hands—his best
guides. Thus, let the thumbs be placed firmly on the spines of the
ilia, while the fingers grasp the trochanters on each side. Having the
sound side as a standard of comparison, the hand will easily detect
any displacement on the injured side. Hippocrates bids us compare the
sound parts with the parts affected (in fractures) and observe the
inequalities.
The top of the great trochanter is the guide in an operation recently
introduced by Mr. Adams, namely, the ‘subcutaneous section of the neck
of the femur.’ ‘The puncture should be made one inch above and nearly
one inch in front of the top of the trochanter. The neck of the bone
is to be sawn through at right angles to its axis, the saw working
parallel to Poupart’s ligament, and about one inch below it.’
Spine of the ilium.—The anterior superior spine of the ilium
is the point from which we measure the length of the lower limb. By
looking at the spines of opposite sides we can detect any slant in the
pelvis. By pressure on both spines simultaneously we examine if there
be a fracture of the pelvis, or disease at the sacro-iliac joint.
100. ‘In reducing a dislocation of the hip by manipulation it is
important to bear in mind that, in every position, the head of the
femur faces nearly in the direction of the inner aspect of its internal
condyle.’[8]
101. Compression of femoral artery.—About a point midway
between the spine of the ilium and the symphysis pubis, the femoral
artery can be felt beating, and effectually compressed, against the
pubes. How should the pressure be applied when the patient lies on
the back? In accordance with the slope of the bone—that is, with a
slight inclination upwards. A want of attention to this point is the
reason why so many fail when they undertake to command the circulation[Pg 47]
through the femoral artery in an amputation, or to cure an aneurysm by
digital compression.
If the Italian tourniquet be used, we should be careful to adjust
the counter-pad well under the tuberosity of the ischium. If digital
pressure be used, it is easy to command the femoral by slight pressure
of the thumb, provided the fingers have a firm hold on the great
trochanter.
102. Sartorius.—The sartorius is the great fleshy
landmark of the thigh, as the biceps is of the arm, and the
sterno-cleido-mastoideus of the neck. Its direction and borders may
easily be traced by asking the patient to raise his leg, a movement
which puts the muscle in action. The same action defines the boundaries
of the triangle (of Scarpa) formed by Poupart’s ligament, the adductor
longus and sartorius.
Line of femoral artery.—To define the course of the femoral
artery, draw a line from midway between the anterior superior spine of
the ilium and the symphysis pubis to the (spur-like) tubercle for the
adductor magnus on the inner side of the knee. The femoral artery lies
under the upper 2/3 of this line.
The sartorius begins to cross the artery, as a rule, from three to
four inches below Poupart’s ligament. The point at which the profunda
artery arises is about one and a half or two inches below the ligament.
Therefore the incision for tying the femoral in Scarpa’s triangle
should commence about a hand’s breadth below Poupart’s ligament, and be
continued for three inches in the line of the artery.
To command the femoral in Scarpa’s triangle, the pad of the tourniquet
should be placed at the apex, and the direction of the pressure should
be, not backwards, but outwards, so that the artery may be compressed
against the femur.
In the middle third of the thigh the femoral artery lies in Hunter’s
canal, overlapped by the sartorius. About the commencement of the lower
third the artery leaves the canal through the oval opening in the
adductor magnus, and, under the name of popliteal, enters the popliteal
space. The line for finding the artery in Hunter’s canal has been
already traced[Pg 48] (102). The incision to reach the artery in this part of
its course would fall in with the outer border of the sartorius.
To command the femoral artery in Hunter’s canal, the pressure should be
directed outwardly, so as to press the vessel against the bone.
THE BUTTOCKS.
103. Buttocks.—Bony landmarks.—The bony landmarks of the
buttocks which can be distinctly felt are: 1, the posterior superior
spines of the ilia; 2, the spines of the sacral vertebræ; 3, the two
tubercles of the last sacral vertebra; 4, the apex of the coccyx in the
deep groove leading to the anus; 5, the tuberosities of the ischia on
each side of the anus.
The posterior spines of the ilia are about the level of the second
sacral spine, and correspond with the middle of the sacro-iliac
symphysis.
The third sacral spine marks the lowest level to which the membranes of
the cord and the cerebro-spinal fluid descend in the spinal canal.
The tuberosities of the ischia, in the erect position, are covered by
the gluteus maximus. In the sitting position they support the weight of
the body, and are only covered by a thick pad of coarse fat. Between
this pad and the bones there is a bursa, which becomes occasionally
enlarged and inflamed in coachmen.
The prominence of the nates is one of the characteristics of man in
connection with his erect attitude. ‘Les fesses n’appartiennent qu’à
l’espèce humaine.’ They are formed of an accumulation of fat over the
great muscle of the buttock (gluteus maximus). From their appearance
we may gather some indication of the state of the constitution. They
are firm and globose in the vigorous; loose and flaccid in the infirm.
Wasting and flattening of one, compared with the other, is an early
symptom of disease in the hip.
104. Fold of the buttock.—The deep furrow, termed[Pg 49] ‘the fold
of the buttock,’ which separates the nates from the back of the
thigh, corresponds with the lower border of the gluteus maximus. Its
altered direction in disease of the hip is very characteristic. This
is the best place to feel for the great ischiatic nerve. We find it by
pressing deeply between the trochanter and the tuber ischii, rather
nearer to the latter. When we sit upright, the nerve is not liable to
pressure; but it becomes numbed when we sit long sideways.
105. Gluteal artery.—To find at what point the gluteal artery
comes out of the pelvis, draw a line from the posterior superior spine
of the ilium to the top of the trochanter major, rotated inwards. The
junction of the inner with the middle third of this line lies over the
artery as it emerges from the upper border of the great ischiatic notch.
The point of exit of the ischiatic artery from the pelvis is about half
an inch lower than that of the gluteal.
106. Pudic artery.—The pudic artery crosses the spine of the
ischium. To find it, draw a line from the outer side of the tuber
ischii to the posterior superior spine of the ilium. The junction of
the lower with the middle third gives the position of the artery. The
ischiatic artery lies close to it, but nearer the middle line.
Looking at the course of these arteries it appears that when we sit
on hard seats the pressure is sustained by the bones; when we recline
on soft seats the pressure is sustained more by the soft parts, and
reaches the arteries; hence the tendency of modern modes of reposing
to drive the blood into the interior of the pelvis and favour the
production of piles and uterine disorders. A celebrated French
accoucheur used to say that the fashion of high waists, tight lacing,
and easy chairs brought him many thousands a year.
THE KNEE.
107. Bony points.—The patella; the tuberosities of the
two condyles; the tubercle of the tibia for the attachment of the
ligamentum patellæ; another (the lateral) tubercle, on the[Pg 50] outer side
of the head of the tibia; and the head of the fibula are the chief bony
landmarks of the knee.
Observe that the head of the fibula lies at the outer and back part of
the tibia, and that it is pretty nearly on a level with the tubercle
for the attachment of the ligamentum patellæ.
We can also feel the adductor tubercle or spur-like projection of bone
above the internal condyle which gives attachment to the tendon of the
adductor magnus. This spur-like projection corresponds with the level
of the epiphysis of the lower end of the femur, and also with the level
of the highest part of the trochlea for the patella: facts worth notice
in performing excision of the knee.
‘In reducing a dislocation of the hip, it is important to bear in mind
that the inner aspect of the internal condyle in every position of the
limb faces nearly in the direction of the head of the femur.’ (100)
The tubercle on the outer side of the head of the tibia gives
attachment to the broad and strong aponeurosis (tendon of the tensor
fasciæ), which, acting like a brace for the support of the pelvis,
is well seen in emaciated persons down the outer side of the thigh.
This tubercle indicates the level to which the condyles of the femur
descend, and the lower level of the synovial membrane.
The patella, in extension of the knee, is nearly all above the
condyles; in flexion, it lies in the inter-condyloid fossa (more on the
external condyle), and thus protects the joint in kneeling. Its inner
border is thicker and more prominent than the outer, which slopes down
towards its condyle.
108. Ligamentum patellæ.—The line of the ligamentum patellæ is
vertical. Hence any deviation from this line, one way or the other,
indicates more or less dislocation of the tibia. There is a pellet of
fat under the ligament, which answers a ‘packing’ purpose—sinking in
when the knee is bent; rising when the knee is extended, and bulging
on either side of the tendon, almost enough to give the feel of
fluctuation.
In a well-formed leg the ligamentum patellæ, the tubercle[Pg 51] of the
tibia, and the middle of the ankle should be in the same straight line.
A useful point in the adjustment of fractures.
Behind the upper half of the ligamentum patellæ is the synovial
membrane of the knee-joint; behind the lower half is a synovial bursa
and a pad of fat. It is well to remember this in cases of injury to the
ligamentum patellæ.
109. Patellar bursa.—The patellar or housemaids’ bursa is
situated not only over the patella, but over the upper part of the
ligament. This is plain enough when the bursa becomes enlarged. There
is another subcutaneous bursa over the insertion of the ligament into
the tubercle of the tibia. This is quite independent of the deep bursa
between the tendon and the bone.
110. Synovial membrane of knee.—The synovial membrane of the
knee, when the joint is extended, rises like a cul-de-sac above the
upper border of the patella about two inches. It ascends, too, a
little higher under the vastus internus than the vastus externus—a
fact very manifest when the joint is distended. When the knee is bent
this cul-de-sac is drawn down—hence the rule of bending the knee in
operations near the lower end of the femur.
The lower level of the synovial membrane of the knee is just above the
level of the upper part of the head of the fibula. The tibio-fibular
synovial membrane is, with rare exceptions, independent of that of the
knee.
111. Popliteal tendons.—The tendons forming the boundaries of
the popliteal space can be distinctly felt when the muscles which bend
the knee are acting. On the outer side, we have the biceps running down
to the head of the fibula. On the inner side we feel three tendons,
disposed as follows:—nearest to the middle of the popliteal space
is the semitendinosus, very salient and traceable high up the thigh;
next comes the thick round tendon of the semimembranosus; still more
internally is the gracilis. The sartorius, which forms a graceful
muscular prominence on the inner side of the knee, does not become
tendinous until it gets below it.
112. Popliteal bursa.—The precise position of the bursa in
the popliteal space, which sometimes enlarges to the size[Pg 52] of a hen’s
egg, is between the tendon of the inner head of the gastrocnemius and
the tendon of the semimembranosus, just where they rub one against
the other. The bursa is from one and a half to two inches long. When
enlarged, it makes a swelling on the inner side of the popliteal space,
which bulges and becomes tense when the knee is extended, and vice
versâ. I examined 150 bodies with a view to ascertain how often
this bursa communicates with the synovial membrane of the knee. There
was a communication about once in five instances. This should make us
cautious in interfering too roughly with the bursa when enlarged.
113. Popliteal artery.—The popliteal artery can be felt beating
and can be compressed against the back of the femur, close to which
it lies. But pressure, sufficient to stop the blood, should be firm,
and should be made against the bone nearer to the inner than the outer
hamstrings. The line of the artery corresponds with the middle of the
ham. It lies under cover of the fleshy belly of the semimembranosus,
and the outer border of this muscle is the guide to it. An incision
down the middle of the ham would fall in with the vessel just above the
condyles.
114. Peroneal nerve.—The peroneal nerve runs parallel with and
close to the inner border of the tendon of the biceps. It can be felt
in thin persons. There is a risk of dividing it in tenotomy of the
biceps, unless the knife be carefully introduced from within outwards.
Below the knee the nerve can be felt close to the fibula just below the
head, and when pressed upon in this situation causes a sensation to run
down its branches to the foot.
THE LEG AND ANKLE.
115. Bony points.—The tubercle of the tibia (for the attachment
of the ligamentum patellæ), the sharp front edge called the shin, and
the broad flat subcutaneous surface of the bone can be felt all the way
down. The inner edge can be felt too, but not so plainly. The lower
third is the narrowest part of the bone and the most frequent seat of
fracture.
[Pg 53]
The head of the fibula is a good landmark on the outer side of the leg,
about one inch below the top of the tibia and nearly on a level with
the tubercle. Observe that it is placed well back, and that it forms no
part of the knee-joint, and takes no share in supporting the weight.
The shaft of the fibula arches backwards, the reverse of the shaft of
the tibia. The fact of the bones not being on the same plane should be
remembered in flap amputations. The shaft of the fibula is so buried
amongst the muscles, that the only part to be distinctly felt is the
lower fourth. Here there is a flat triangular subcutaneous surface,
between the peroneus tertius in front, and the two peronei (longus and
brevis) behind. Here is the most frequent seat of fracture.
116. Malleoli.—The shape and relative position of the malleoli
should be carefully studied, as the great landmarks of the ankle. The
inner malleolus does not descend so low as the outer, and advances more
to the front: at the same time, owing to its greater antero-posterior
depth, it is on the same plane as the outer behind. The lower border of
the inner malleolus is somewhat rounded, and the slight notch in it for
the attachment of the lateral ligament can be felt. The outer malleolus
descends lower than the inner, thus effectually locking the joint on
the outer side. Its shape is not unlike the head of a serpent. Viewed
in profile, it lies just in the middle of the joint.
In Syme’s amputation of the foot at the ankle, the line of the incision
should run from the apex of the outer malleolus, under the sole to the
centre of the inner.
In a well-formed leg, the inner edge of the patella, the inner ankle,
and the inner side of the great toe, should be in the same vertical
plane. Look to these landmarks in adjusting a fracture or dislocation,
keeping at the same time an eye upon the conformation of the opposite
limb.
There are several strong tendons to be seen and felt about the ankle.
117. Tendo Achillis.—Behind is the tendo Achillis. It forms a
high relief, with a shallow gutter on each side of it. The narrowest
part of the tendon, where it should be[Pg 54] divided in tenotomy, is about
the level of the inner ankle; below this it expands again to be
attached to the lower and back part of the os calcis. Seen in profile,
the tendon is not straight, but slightly concave—being drawn in by
an aponeurosis which forms a sort of girdle round it. This girdle
proceeds from the posterior ligament of the ankle; and, though most of
its fibres encircle the tendon, some of them adhere to and draw in its
sides. All this disappears when the tendon is laid bare by dissection.
118. Tendons behind inner ankle.—Above and behind the malleolus
internus we can feel the broad flat tendon of the tibialis posticus and
upon it that of the flexor longus digitorum. The tendon of the tibialis
posticus lies nearest to the bone and comes well up in relief in
adduction of the foot. It lies close to, and parallel with, the inner
edge of the tibia, so that this edge is the best guide to it. Therefore
in tenotomy the knife should be introduced first perpendicularly
between the tendon and the bone, and then turned at right angles to cut
the tendon. The tendon has a separate sheath and synovial membrane,
which commences about one inch and a half above the apex of the
malleolus, and is continued to its insertion into the tubercle of the
scaphoid bone. The proper place, then, for division of the tendon, is
about two inches above the end of the malleolus.
In a young and fat child, where the inner edge of the tibia cannot be
distinctly felt, the best guide to the tendon is a point midway between
the front and the back of the ankle. An incision in front of this
point might injure the internal saphena vein; behind this point, the
posterior tibial artery.
119. Tendons behind outer ankle.—Behind the malleolus externus
we feel the two peroneal (long and short) tendons. They lie close to
the edge of the fibula, the short one nearer to the bone. In dividing
these tendons, the knife should be introduced perpendicularly to the
surface, and about two inches above the apex of the ankle, so as to be
above the synovial sheaths of the tendons.
Tendons in front of ankle.—Over the front of the ankle, when
the muscles are in action, we can see and feel, beginning[Pg 55] on the
inner side, the tendons of the tibialis anticus, the extensor longus
pollicis, the extensor longus digitorum, and the peroneus tertius. They
start up like cords when the foot is raised, and are kept in their
proper relative position by strong pulleys formed by the anterior
annular ligament. Of these pulleys the strongest is that of the
extensor communis digitorum. When the ankle is sprained, the pain and
swelling arise from a stretching of these pulleys and effusion into
their synovial sheaths. A laceration of one of the pulleys and escape
of the tendon is extremely rare.
The place for the division of the tendon of the tibialis anticus, so as
to divide it below its synovial sheath, is about one inch before its
insertion into the cuneiform bone. The knife should be introduced on
the outer side, so as to avoid the dorsal artery of the foot.
Now trace the lines of the arteries, and the landmarks near which they
divide.
120. Popliteal artery.—About one inch and a quarter below the
head of the fibula, or say one inch below the tubercle of the tibia,
the popliteal artery divides into the anterior and posterior tibial.
The peroneal comes off from the posterior tibial about three inches
below the head of the fibula.
Consequently we may lay down, as a general rule, that, in amputations
one inch below the head of the fibula, only one main artery, the
popliteal, is divided. In amputations two inches below the head of
the fibula, two main arteries, the anterior and posterior tibial,
are divided. In amputations three inches below the head, three main
arteries, the two tibials and the peroneal, are divided.
121. Anterior tibial artery.—The anterior tibial artery
comes in front of the interosseous membrane, one inch and a quarter
below the head of the fibula, and here lies close to this bone. Its
subsequent course is defined by a line drawn from the front of the
head of the fibula to the middle of the front of the ankle. This
line corresponds pretty nearly with the outer border of the tibialis
anticus all the way down. If this muscle be put in action, its outer
border (the intermuscular line) is plainly seen, and the incision for
the ligature[Pg 56] of the artery in any part of its course may be defined
with the greatest precision. The artery can be felt beating and can be
compressed where it crosses the front of the tibia and ankle.
122. Posterior tibial artery.—The posterior tibial commences
about one inch and a quarter below the head of the fibula. Its
subsequent course corresponds with a line drawn from the middle of the
upper part of the calf to the hollow behind the inner ankle, where it
can be felt beating distinctly about half an inch behind the edge of
the tibia. A vertical incision down the middle of the calf would reach
the artery under cover of the gastrocnemius and soleus. A vertical
incision along the middle third of the leg, about half an inch from the
inner edge of the tibia, would enable the operator to reach the artery
sideways, by detaching from the bone the tibial origin of the soleus.
123. Saphena veins.—The subcutaneous veins on the dorsum of the
foot form an arch convex towards the toes (as on the back of the hand),
from which issue the two main subcutaneous trunks of the lower limb,
the internal and external saphena veins. The internal saphena vein can
be always plainly seen over the front of the inner ankle. Its further
course up the inner side of the leg, knee, and thigh to its termination
in the femoral is not in all persons manifest.
The external saphena vein runs behind the outer ankle and up the middle
of the calf to empty itself (generally) into the popliteal vein.
What are the bony landmarks which guide us in the surgery of the foot?
124. Points of bone.—Along the inner side of the foot,
beginning from behind, we can feel—1, the tuberosity of the os calcis;
2, the projection of the internal malleolus; 3, the projection of the
os calcis, termed ‘sustentaculum tali,’ about one full inch below the
malleolus; 4, about one inch in front of the malleolus internus, and a
little lower, is the tubercle[Pg 57] of the scaphoid bone; the gap between
it and the sustentaculum tali being filled by the calcaneo-scaphoid
ligament and the tendon of the tibialis posticus, in which there
is often a sesamoid bone; 5, the internal cuneiform bone; 6, the
projection of the first metatarsal bone; 7, the sesamoid bones of the
great toe.
Along the outer side of the foot we can feel—1, the external
tuberosity of the os calcis; 2, the external malleolus; 3, the peroneal
tubercle of the os calcis, one inch below the malleolus, with the long
peroneal tendon below it, and the short one above it; 4, the projection
of the base of the fifth metatarsal bone.
125. Lines of joints.—In fat persons the following rules for
finding the joints may be of service as regards the surgery of the
foot:—
The level of the ankle joint lies about half an inch above the end of
the inner malleolus. This is worth remembering in performing ‘Syme’s’
amputation.
The tubercle of the scaphoid bone is the best guide to the
astragalo-scaphoid joint which lies immediately behind it; and the
plane of this joint is in the same line as that of the calcaneo-cuboid.
Thus a line drawn transversely over the dorsum of the foot, behind
the tubercle of the scaphoid, would strike both the joints opened in
‘Chopart’s’ operation.
Place your thumb on the tubercle of the scaphoid, and measure about one
inch and a half in front: here you find the joint between the internal
cuneiform bone and the metatarsal bone of the great toe. This point is
useful in Lisfranc’s operation, which consists in the removal of the
metatarsal bones.
The line of the calcaneo-cuboid joint lies midway between the external
malleolus and the (tarsal) end of the metatarsal bone of the little toe.
The projection of the fifth metatarsal bone is the guide to the joint
between it and the cuboid.
Notice that the line of the joints between the metatarsal bones and the
first phalanges lies a full inch farther back than[Pg 58] the interdigital
folds of the skin. This is a point to be remembered in amputating the
toes.
126. Dorsal artery.—The line of the dorsal artery of the foot
is from the middle of the ankle to the interval between the first and
second metatarsal bones. The artery can be felt beating over the bones
along the outer side of the extensor longus pollicis, which is the best
guide to it.
127. Bursa.—The synovial sheath of the extensor longus pollicis
extends from the front of the ankle, over the instep (apex of the
internal cuneiform bone) as far as the metatarsal bone of the great
toe. There is generally a bursa over the instep, above, or it may be,
below, the tendon.
There is often a large irregular bursa between the tendons of the
extensor longus digitorum, and the projecting end of the astragalus,
over which the tendons play. There is much friction here. It is well to
be aware that this bursa sometimes communicates with the joint of the
head of the astragalus.
128. Plantar arteries.—The course of the external plantar
artery corresponds with a line drawn from the hollow behind the inner
ankle obliquely across the sole nearly to the base of the fifth
metatarsal bone; from thence the artery turns transversely across
the foot, lying (deeply) near the bases of the metatarsal bones,
till it inosculates with the dorsal artery of the foot in the first
interosseous space.
The course of the internal plantar corresponds with a line drawn from
the inner side of the os calcis to the middle of the great toe.
129. Plantar fascia.—To divide the plantar fascia
subcutaneously, the best place is about one inch in front of its
attachment to the os calcis. This is the narrowest part of it. The
knife should be introduced on the inner side; and the incision will be
behind the plantar artery.
The subcutaneous section of the tendon of the abductor pollicis should
be made about one inch before its insertion.
130. Clavicle.—The line of the clavicle and the projection of
the joint at either end of it can always be felt, even in the fattest
persons. Its direction is not perfectly horizontal, but slightly
inclined downwards, when the arm hangs quietly by the side. When the
body lies flat on the back, the shoulder not only falls back, but rises
a little, the weight of the limb being taken off. Hence the modern
practice of treating fractures of the clavicle (in the early stage) by
the supine position.
On the front surface of the clavicle, not far from its acromial end,
there is in many persons of mature age a spine-like projection of bone.
So far as I know, it has not been described. A gentleman, himself a
surgeon, showed me an instance in his own person. He suspected it was
an exostosis.
As a rule the acromio-clavicular joint forms an even plane. But there
is sometimes a knob of bone at the acromial end of the clavicle; or it
may be only a thickening of the fibro-cartilage, sometimes existing
in the joint. In either case this relief might be mistaken for a
dislocation, or even for a fracture. A reference to the other shoulder
might settle the question.
131. Bony points of the shoulder.—We can distinctly feel the
spine of the scapula and the acromion, more especially at the angle
where they join behind the shoulder. This angle is the best place from
which to measure in taking the comparative length of the arms.
In some shoulders, though very rarely, there is an abnormal symphysis
between the spine of the scapula and the acromion. There may indeed
be two symphyses and two acromial bones, the acromion having two
centres of ossification. These abnormal symphyses might be mistaken for
fractures, until we have examined the opposite shoulder, which is sure
to present a similar conformation.[9]
Tuberosities.—Projecting beyond the acromion (the arm hanging
by the side), we can feel, through the fibres of the[Pg 60] deltoid, the
upper part of the humerus. It distinctly moves under the hand when
the arm is rotated. It is not the head of the bone which is felt, but
the tuberosities, the greater externally, the lesser in front. These
tuberosities form the convexity of the shoulder. When the arm is
raised, this convexity disappears; there is a slight depression in its
place. The head of the bone can be felt by pressing the fingers high up
in the axilla.
The absence of this prominence formed by the upper part of the humerus
under the deltoid, and the presence of a prominence low in the hollow
of the axilla, or in front, below the coracoid process, or behind, on
the back of the scapula, bespeak dislocation of the head of the bone.
In examining obscure injuries about the shoulder, it is worth
remembering that, in the normal relation of the bones, and in every
position, the great tuberosity faces in the direction of the external
condyle. The head of the bone faces very much in the direction of the
internal condyle.
It is worth remembering also that the upper epiphysis of the humerus
includes the tuberosities; and that it does not unite by bone to the
shaft, till about the 20th year.
By making deep pressure in front of the shoulder, when the arm is
pendent and supine, we can feel the bicipital groove. It looks directly
forwards, and runs in a line drawn vertically downwards through the
middle of the biceps to its tendon at the elbow. We should be aware of
this, lest it be mistaken for a fracture.
132. Coraco-acromial ligament.—Under the anterior fibres of
the deltoid, we can distinctly feel the position and extent of the
coraco-acromial ligament. A knife, passed vertically through the middle
of it, goes at once into the shoulder joint and strikes the bicipital
groove with the tendon, a point to be remembered in excision.
In persons of an athletic build the triangular form and beautiful
structure of the deltoid become conspicuous when the muscle is in
action. The depression on the outer side of the arm, indicating its
insertion, is the place selected for issues or setons.
[Pg 61]
The arm being held up by an assistant, the anterior and posterior
borders of the relaxed deltoid admit of being raised so that in
amputation at the shoulder the knife can be introduced beneath the
muscle to make the flap.
133. Axilla.—The anterior border of the axilla, formed by the
pectoralis major, follows the line of the fifth rib. In counting the
ribs, or in tapping the chest, it is worth remembering that the highest
visible digitation of the serratus magnus is attached to the sixth rib.
The angle of the digitation is directed forwards, and corresponds to
the upper edge of the rib. The second visible digitation corresponds
to the seventh rib; the interval between these digitations, therefore,
corresponds to the sixth intercostal space—a convenient place for
tapping the chest. (38)
In the normal state no glands can be felt in the axilla.
134. Axillary artery.—When the arm is raised to a right
angle with the body, and the head of the humerus thereby depressed,
the axillary artery is plainly felt beating, and can be perfectly
compressed on the inner side of the coraco-brachialis. This muscle
stands out in relief along the humeral side of the axilla, and is the
best guide to the artery. A line drawn along its inner border—that
is, down the middle of the axilla—corresponds with the course of the
artery.
The depth and form of the axilla alter in different positions of the
arm. In the arm raised and abducted the axilla becomes nearly flat;
hence this position is always adopted in operations.
In opening abscesses in the axilla, the incision should be made midway
between the borders, and the point of the knife introduced from above
downwards.
135. Brachial artery.—When the arm is extended and supinated,
a line drawn from the deepest part of the middle of the axilla down
the inner side of the biceps to the middle of the bend of the elbow,
corresponds with the course of the brachial artery. The artery can be
felt and compressed all the way down; but nowhere so effectually as
midway, where it lies on the tendon of the coraco-brachialis close
to the inner side of the humerus. The only direction to apply the
pressure[Pg 62] effectually is outwards and a little backwards, else the
artery will slip off the bone.
The musculo-spiral nerve and superior profunda artery wind round
the back of the humerus about its middle, and come to the front of
the external condyloid ridge. Thus, for full three inches above the
condyles, there is nothing to interfere with operations on the back of
the bone, which is here broad and flat.
136. Bend of elbow.—At the bend of the elbow, the tendon of the
biceps can be plainly felt, as well as the pulsation of the brachial
artery close to its inner side, before dividing into the radial and
ulnar.
Cutaneous veins.—The bend of the elbow in young children and
in persons with fat and round arms, presents a semicircular fold of
which the curve embraces the lower part of the biceps; but in muscular
persons we see the distinct boundaries of the triangular space, formed
by the pronator teres on the inner side, and the supinator longus on
the outer. Here can be traced, standing out in strong relief under
the thin white skin, the superficial veins, which, in days gone by,
when bloodletting was the fashion, were of such great importance.
Their arrangement, although subject to variety, is very much like the
branches of the letter M, the middle of the M being at the middle
of the elbow. Of these branches the median basilic, which runs over
the tendon of the biceps, is the largest and most conspicuous, and
is generally selected for venesection; it crosses the course of the
brachial artery, nothing intervening but the semilunar aponeurosis from
the tendon of the biceps.
137. Landmarks of elbow.—It is of great importance to be
familiar with the relative positions of the various bony prominences
about the elbow. We can always feel the internal and external condyles.
The internal is the more prominent of the two, and a trifle higher.
Olecranon.—We can always feel the olecranon. This is somewhat
nearer to the inner than to the outer condyle. Between the olecranon
and the internal condyle is a deep depression in which lies the ulnar
nerve (vulgarly called the ‘funny bone’).
[Pg 63]
On the outer side of the olecranon, just below the external condyle,
is a pit in the skin, constant even in fat persons (when the elbow is
extended). This pit is considered one of the beauties of the elbow in a
graceful arm; it is seen in a child as a pretty little dimple. To the
surgeon it is most interesting, as in this valley behind the supinator
longus and the radial extensors of the wrist he can distinctly feel the
head of the radius rolling in pronation and supination of the forearm.
It is, therefore, one of the most important landmarks of the elbow,
since it enables us to say whether the head of the radius is in its
right place, and whether it rotates with the shaft.
Can the tubercle of the radius be felt? Yes, but only on the back of
the forearm in extreme pronation. Its projection is then distinctly
perceptible just below the head of the bone.
Relations of olecranon and condyles.—To examine the relative
positions of the olecranon and condyles in the different motions of
the elbow joint, place the thumb on one condyle, the tip of the middle
finger on the other, and the tip of the forefinger on the olecranon. In
extension, the highest point of the olecranon is never above the line
of the condyles; indeed, it is just in this line. With the elbow at
right angles the point of the olecranon is vertically below the line
of the condyles. In extreme flexion the point of the olecranon lies in
front of the line of the condyles.
All these relative positions would be altered in a dislocation of the
ulna, but not (necessarily) in a fracture of the lower end of the
humerus.
Sometimes, though rarely, we meet with a hook-like projection of bone
above the internal condyle. It is called a ‘supra-condyloid’ process;
it can be felt through the skin, with its concavity downwards, and is
a rudiment of the bony canal which, in many mammalia, transmits the
median nerve and ulnar artery. A third origin of the pronator teres is
always attached to it; this origin covers the brachial artery.[10]
Bursæ.—The subcutaneous bursa over the olecranon, if distended,
would be as large as a walnut. A second bursa sometimes exists a little
lower down upon the ulna. There[Pg 64] is also a small subcutaneous bursa
over each of the condyles.
The vertical extent of the elbow joint is limited, above by a line
drawn from one condyle to the other; below, by a line corresponding to
the lowest part of the head of the radius.
138. Interosseous arteries.—About one inch below the head of
the radius, the ulnar artery gives off the common interosseous; and
this divides, about half an inch lower, into the anterior and posterior
interosseous. Thus, in amputating the forearm, say two inches below the
head of the radius, four arteries at least would require ligature.
By flexion of the elbow to the utmost, the circulation through the
brachial artery can be arrested; but the position is painful, and can
be tolerated only for a short time.
Lymphatic gland.—There is a small lymphatic gland just above
the inner condyle, in front of the intermuscular septum. It is the
first to take alarm in poisoned wounds of the hand.
THE FOREARM AND WRIST.
139. Ulna.—The edge of the ulna can be felt subcutaneous from
the olecranon to the styloid process (in supination). Any irregularity
could be easily detected. The styloid process of the ulna does not
descend so low as the styloid process of the radius, or it would
impede the free abduction of the hand. Its apex is on a level with
the radio-carpal joint. The head of the ulna is plainly felt and seen
projecting at the back of the wrist, especially in pronation of the
forearm. It then lies between the tendons of the extensor carpi ulnaris
and extensor minimi digiti. There is often a subcutaneous bursa over it.
140. Radius.—The upper half of the shaft of the radius is so
covered by muscles that we cannot feel it; the lower half is more
accessible to the touch, especially just above and just below the part
where it is crossed by the extensors of the thumb. Its styloid process
is readily felt, and made all[Pg 65] the more manifest by being covered by
the first two extensor tendons of the thumb. It descends lower, and
lies more to the front than the corresponding process of the ulna. The
relative positions of these styloid processes can be best examined by
placing the thumb on one and the forefinger on the other.
Feel for the little bony pulley on the back of the radius near the
wrist, which keeps in place the third extensor tendon of the thumb.
This and the bone just above it is the place which we examine for a
suspected fracture (termed Colles’s) near the lower end of the radius.
141. Carpus.—Below the styloid process of the radius, just on
the inner side of the extensors of the thumb, we feel the tubercle of
the scaphoid bone. Between the styloid process and the tubercle is the
level of the radio-carpal joint. A little lower we feel the trapezium.
Just below the ulna on the palm of the hand we feel the pisiform bone;
and on the inner side of this, the cuneiform.
There are several transverse furrows on the palmar aspect of the
wrist. The lowest of these, which is slightly convex downwards,
corresponds with the upper edge of the anterior annular ligament and
the intercarpal joint. The line of the radio-carpal joint, as already
stated, is on a level with the apex of the styloid process of the ulna.
In forcible flexion of the wrist, the tendon of the flexor carpi
radialis and that of the palmaris longus come up in relief. On the
outer side of the first-named tendon we feel the pulse, the radial
artery here lying close to the radius.
The tendon of the palmaris longus runs near the middle of the wrist,
and close to its inner border runs the median nerve. In letting out
deep-seated matter near the wrist, the incision should be made close to
and parallel with the inner edge of the radial flexor tendon, so as to
avoid injury to the median nerve.
We can feel the tendon of the flexor carpi ulnaris for some distance
above the wrist. It overlies the ulnar artery, and somewhat masks its
pulsation.
142. Pulse.—The ‘pulse at the wrist’ is felt just outside[Pg 66] the
tendon of the flexor carpi radialis. In feeling the pulse it should
be remembered that, in some cases, the superficialis volæ arises
higher and is larger than usual. In such cases it runs by the side of
the radial artery, and gives additional volume to the pulse. The old
writers call it ‘pulsus duplex.’ When in doubt, therefore, it is well
to feel the pulse in each wrist.
143. Great carpal bursa.—The great synovial sheath under the
annular ligament common to the flexor tendons of the fingers and the
long flexor of the thumb, extends, upwards, about an inch and a half
above the edge of the ligament, and, downwards, as low as the middle of
the palm. This general synovial sheath communicates with the special
sheaths of the thumb and the little finger; not with that of the index,
middle, and ring fingers.
144. ‘Tabatière anatomique.’—On the outer side of the wrist we
can distinctly see and feel, when in action, the three extensor tendons
of the thumb. Between the second and third there is deep depression, at
the root of the thumb, which the French humorously call the ‘tabatière
anatomique.’ In this depression we can make out—1, the relief of the
superficial radial vein; 2, the radial artery, in its passage to the
back of the hand; 3, the upper end of the metacarpal bone of the thumb.
145. Tendons on back of wrist.—The relative positions of
the several extensor tendons of the wrist and fingers, as they play
in their grooves over the back of the radius and ulna, can all be
distinctly traced when the several muscles are put in action. The
length of their synovial sheaths should be remembered. They vary from
one inch and a half to two inches and a half. The longest of all are
those of the extensors of the thumb. When these sheaths are inflamed
and swollen, the motion of the tendons becomes painful and gives rise
to a feeling of crepitus, called ‘tenalgia crepitans’ by some writers.
It is said to be met with sometimes in pianists.
146. Lines of arteries.—The course of the radial artery
corresponds with a line drawn from the outer border of the tendon of
the biceps at the bend of the elbow down the front[Pg 67] of the forearm to
the front of the styloid process of the radius. In the upper third of
its course the artery is overlapped by the supinator longus. To make
allowance for this, the incision for the ligature of the artery in this
situation should be made, not precisely in the line of its course, but
rather nearer the middle of the forearm.
The line of the ulnar artery runs from the middle of the bend of the
elbow (slightly curving inwards) to the outer side of the pisiform
bone. The radial and ulnar arteries can, in most cases, be effectually
commanded by pressure well applied at the wrist, in wounds of the
palmar arch.
Before we make incisions along the forearm, it is always desirable
to ascertain whether the ulnar artery, which usually runs under the
superficial muscles, may not run abnormally over them; in which case
its pulsations can be felt all down the forearm.
THE HAND.
147. It is beside the purpose here to examine the question whether the
hand can tell more than the arm, the leg, or any other part of the
body, about the physical constitution of its owner, and to what use
it has been put. Those who are interested in this subject should read
a very elaborate treatise by Carus,[11] ‘On the Reason and Meaning of
the Different Forms of the Hand.’ Still less would I indulge curiosity
by inquiring whether the professors of chiromancy, relying on the text
‘erit signum in manu tua et quasi monumentum ante oculos tuos,’ can
advance any reasonable pretensions for their assertion that they can
read in the furrows of the palm the future destiny of its master.
148. Furrow in palm.—The only furrow in the palm useful as a
surgical landmark is that which runs transversely across its lower
third, and is well seen when the fingers are slightly bent. This
transverse furrow corresponds pretty nearly with the metacarpal joints
of the fingers, with the upper limit of the synovial sheaths of the
flexor tendons of the fingers (that of the little finger excepted
(143)); also with[Pg 68] the splitting of the palmar fascia into its four
slips. The transverse metacarpal ligament lies in the same line with
it. Again, a little below this furrow, the digital arteries bifurcate
to run along the opposite sides of the fingers.
149. Interdigital folds.—By pressing upon the interdigital
folds of skin, we can feel the transverse ligament of the fingers,
which prevents their too wide separation. The skin of these folds is
much thinner on the dorsal than the palmar aspect; hence deep-seated
abscesses in the palm very frequently burst on the back of the hand.
150. Digital furrows.—Concerning the transverse furrows on the
palmar surface of the fingers, notice that the first furrows, close to
the palm, do not correspond with the metacarpal joints. The second and
third furrows do correspond with their respective joints.
The slight depression observable between the ball of the thumb and
that of the little finger corresponds with the middle of the anterior
annular ligament.
151. Palmar arterial arches.—In opening abscesses in the palm,
it is important to bear in mind the position of the large arterial
arches which lie beneath the palmar fascia. The line of the superficial
palmar arch crosses the palm about the junction of the upper with the
lower two-thirds—that is, in the line of the thumb separated widely
from the fingers. From this, the digital arteries run straight between
the shafts of the metacarpal bones towards the clefts of the fingers.
Incisions, therefore, to let out pus beneath the palmar fascia may
safely be made in the lower two-thirds of the palm, provided they run
in the direction of the middle line of the fingers. The deep palmar
arch lies half an inch nearer the wrist than the superficial.
152. Digital arteries.—As the digital arteries run along the
sides of the fingers, the incision to open a thecal abscess should
be made strictly in the middle line. It should be made not over but
between the joints, since the sheath is strongest and thickest over
the shafts of the phalanges, and therefore more likely to produce
strangulation of the enclosed tendons.
[Pg 69]
153. Metacarpal joint of thumb.—The joint of the metacarpal
bone of the thumb with the trapezium can be distinctly felt by tracing
the dorsal surface of the bone upwards till we come to the prominence
which indicates the joint at the bottom of the ‘tabatière anatomique’
(144). Supposing, however, there be much swelling, the knife introduced
at the angle between the first and second metacarpal bones readily
finds the joint if the blade be directed outwards.
154. Sesamoid bones.—The sesamoid bones of the thumb can be
distinctly felt. Just above them—that is, nearer to the wrist—lies
the joint between the metacarpal bone and the first phalanx. We should
remember the position of these bones in amputation at this joint.
Mutatis mutandis the same observations apply to the sesamoid
bones of the great toe.
The extensor tendon of the last joint of the thumb crosses the apex
of the first interosseous space. Under the tendon, and in the angle
between the bones, we feel the radial artery just before it sinks into
the palm.
155. Subcutaneous veins.—The veins on the back of the hand,
and their arrangement in the form of arches which receive the digital
veins, is sufficiently obvious. The number and arrangement of the
arches may vary, but in all hands it is interesting to notice that
the veins from the fingers run up between the knuckles and are out of
harm’s way.
156. Interosseous arteries.—Since the dorsal interosseous
arteries, like the palmar, run along the interosseous spaces, incisions
to let out pus should always be made along the lines of the metacarpal
bones.
157. Digital bursæ.—Small subcutaneous bursæ are sometimes
developed over the knuckles and the backs of the joints of the fingers.
They often become enlarged and unseemly in persons of a rheumatic or
gouty tendency.
158. Knuckles and digital joints.—The three rows of projections
called ‘the knuckles’ are formed by the proximal bones of the several
joints: thus the first row is formed by the ends of the metacarpals;
the second by the ends of the[Pg 70] first phalanges, and so forth. In
amputations of the fingers it is well to remember that in all cases the
line of the joints is a little in advance of the knuckles, that is,
nearer the end of the fingers.
Long and graceful fingers, coupled with thickness and breadth of the
sentient pulp at their ends, and too great arching of the nails, have
been regarded, ever since the days of Hippocrates, as not unlikely
indications of a tendency to pulmonary disease.
PALPATION BY THE RECTUM.
The following report is from Mr. Walsham, of St. Bartholomew’s
Hospital, who, having a small hand (somewhat less than seven and a half
inches round), has had opportunities of introducing it up the rectum,
in the living subject, for the purpose of diagnosis:—
‘It is possible to introduce the hand (if small) into the rectum; in
many cases into the sigmoid flexure, and in rare instances into the
descending colon.
‘Once beyond the sphincter, the hand enters a capacious sac, and the
following important parts can be felt through its walls:—
‘Through the anterior wall the hand first recognises the prostate,
which feels like a moderately large chestnut. Immediately behind the
prostate, the vesiculæ seminales may be distinguished as two softish
masses situated one on either side of the middle line. Internal to
them, the whipcord-like feel of the vasa deferentia can be readily
traced over the bladder to the sides of the pelvis.
‘The bladder is easily recognised, when moderately distended, as a
soft fluctuating tumour behind the prostate; when empty it cannot be
distinguished from the intestines, which then descend between the
rectum and the pubes. The arch of the pubes can well be defined when
the bladder is empty.
‘Through the posterior wall of the bowel the coccyx and sacrum can be
felt, the curve of the sacrum being readily followed by the hand.
[Pg 71]
‘The projecting spine of the ischium on each side of the pelvis is a
valuable landmark. From this point the outlines of the greater and
lesser sacro-ischiatic foramina can be traced by the fingers; and any
new growth, encroaching on the pelvic cavity through these apertures,
could be easily detected.
‘If the hand be now pushed farther up the gut, the promontory of
the sacrum is reached; the pulsation of the iliac vessels becomes
manifest, and the course of the external iliac can be traced along the
brim of the pelvis to the crural arch, the loose attachments of the
rectum permitting very free movement in this direction. The internal
iliac artery can also be followed to the upper part of the great
sacro-ischiatic foramen.
‘By semi-rotatory movement, and alternately flexing and extending the
fingers, the hand can gradually be insinuated into the commencement of
the sigmoid flexure. In the sigmoid flexure the fingers can explore the
whole of the lower part of the abdomen, the loose attachment of this
portion of the gut permitting the hand to travel freely over the iliac
and hypogastric regions.
‘The parts that can here be felt are the bifurcation of the aorta, the
division of the common iliac arteries, the iliac fossa, and the crest
of the ilium.
‘In the female, the uterus in the middle line, and the ovaries on
either side, can be readily distinguished.
‘In the introduction of the hand into the rectum, in a patient under
chloroform, the dilatation of the sphincter ani should be very gradual:
first two fingers, then four, and finally the thumb should be passed.
It is necessary to use considerable force, and unless care be taken,
not only the integumentary edge of the anus, but the sphincter itself,
may be lacerated. The introduction is facilitated by the application of
the other hand upon the abdomen.
‘When the dilatation has been gradual and the hand not too large, no
incontinence of fæces and no very considerable amount of pain has
resulted.
[Pg 72]
‘We have been informed on reliable authority that permanent
incontinence of fæces has occasionally followed these examinations.’
Lastly, we think it right to insist upon the important fact that, in
some subjects, even a small hand cannot be passed up the rectum beyond
the reflection of the peritoneum over the second part of the gut. In
such instances the peritoneum offers a resistance like a tight garter,
and prevents the farther advance of the hand without great risk of
laceration of the parts.[12]
EXAMINATION PER VAGINAM.
For this report I am indebted to Dr. Godson, of St. Bartholomew’s
Hospital:—
‘The finger introduced into the vagina comes upon the carunculæ
myrtiformes, which are vascular membranous processes independent of the
hymen, variable in number, size, and form. It also feels the transverse
ridges known as “rugæ.”
‘Along the anterior wall of the vagina the finger readily detects the
track of the urethra, which feels like a prominent cord and forms an
excellent guide to the orifice of the meatus urinarius in passing a
catheter. The orifice is indicated by a slight semicircular prominence,
situated about one-third of an inch above the orifice of the vagina.
Behind the urethra the finger comes upon the posterior wall of the
bladder. But the bladder is not perceptible, as such, to the touch
unless distended. With a catheter previously introduced it is much more
readily explored.
‘The septum between the vagina and the rectum is so thin that, should
the rectum contain fæcal matter, its presence becomes at once apparent
to the finger.
‘The cervix uteri is felt protruding from the roof of the vagina in
a direction downwards and backwards—that is, in a line from the
umbilicus to the coccyx. The os uteri is felt, small and round, in the
centre of the cervix. The posterior lip feels a little lower than the
anterior. The cul-de-sac[Pg 73] formed by the vagina in front and behind the
cervix should be perfectly elastic to the touch, and not communicate
the sensation of a resisting body. Any resistance here bespeaks an
abnormal condition.
‘The bony landmarks within reach of a finger, or perhaps two, in a
woman who has not borne a child, are the symphysis pubis, the rami
of the pubes and ischia. The coccyx and part of the hollow of the
sacrum may also be felt, but not without exerting much pressure on the
posterior wall of the vagina, which gives considerable pain. If the
promontory of the sacrum can be felt, it is a sign that the conjugate
diameter of the pelvis is abnormal.
‘The finger in the rectum can detect almost everything which has been
mentioned in connection with the vagina. The shape and direction of
the cervix uteri are almost as perceptible, and the posterior wall of
the uterus can be examined. The peritoneal fold termed recto-vaginal
(Douglas’s space) can also be well explored, and anything abnormal
detected in this direction—a point of great importance in the
diagnosis of diseases and displacements of the uterus.
‘The ovary in its normal state and position cannot be detected by
the touch even with the hand firmly pressed on the hypogastrium. If
a movable body be felt through the vaginal roof on one side of the
cervix, if this body be exquisitely tender and recede at once from the
finger, it is an ovary in a state of prolapse.
‘The fundus of a healthy unimpregnated uterus never rises above the
level of the brim of the pelvis, and cannot therefore be felt by
pressing the hand on the hypogastrium.
‘The direction of the uterus is subject to changes which cannot be
looked upon as abnormal. The fundus may be thrown backwards by a
distended bladder, or forwards by a distended rectum. The axis of its
cavity is not a straight but a curved line; and uterine sounds should
be shaped to [Pg 74]suit it.’
Spottiswoode & Co., Printers, New-street Square, London.
Transcriber’s Notes
A few obvious errors in punctuation have been fixed.
The reference in section 153 to tabatière anatomique in section 140 has been corrected to 144.