The Project Gutenberg eBook of The history & traditions of the Moorfields Eye Hospital
This eBook is for the use of anyone anywhere in the United States and
most other parts of the world at no cost and with almost no restrictions
whatsoever. You may copy it, give it away or re-use it under the terms
of the Project Gutenberg License included with this eBook or online
at www.gutenberg.org. If you are not located in the United States,
you will have to check the laws of the country where you are located
before using this eBook.
Title: The history & traditions of the Moorfields Eye Hospital
One hundred years of ophthalmic discovery & development
Author: E. Treacher Collins
Release date: May 6, 2026 [eBook #78625]
Language: English
Original publication: London: H. K. Lewis & Co. Ltd, 1929
Credits: Thiers Halliwell (This file was produced from images generously made available by The Internet Archive)
*** START OF THE PROJECT GUTENBERG EBOOK THE HISTORY & TRADITIONS OF THE MOORFIELDS EYE HOSPITAL ***
Transcriber’s notes:
As the title indicates, this book recounts the history
of Moorfields Eye Hospital over the first one hundred years following
its founding in 1805, the significance of which is that it was the
world’s first hospital created to service a single specialty, viz.
ophthalmology. In recent times, two more volumes have been published
to bring the history up to date but copyright constraints prevent them
being available in digitised format.
The text of this e-transcription has been preserved as in the
original, including inconsistent spelling (storey/story) and
hyphenation (inpatient/in-patient, and ‘retching’ being misspelt as
’reaching’ on p.165. Plate XXIV has been rendered in normal text as the
original image is barely legible, and hyperlinks have been added to
assist readers navigate the text.
New original cover art included with this eBook is granted to the
public domain.
THE HISTORY AND TRADITIONS OF THE
MOORFIELDS EYE HOSPITAL
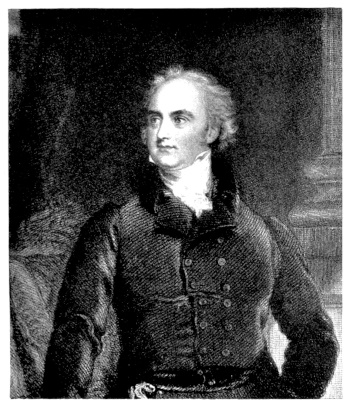
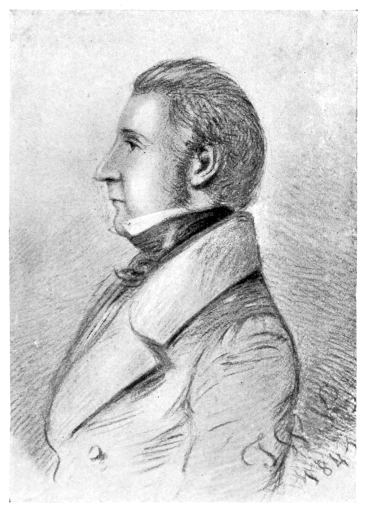
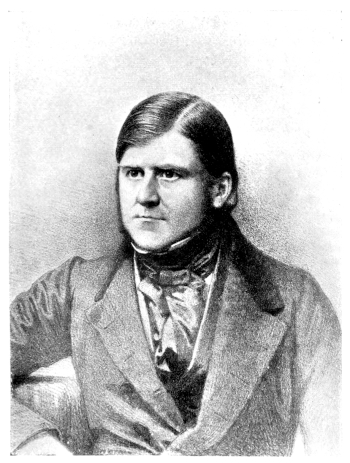
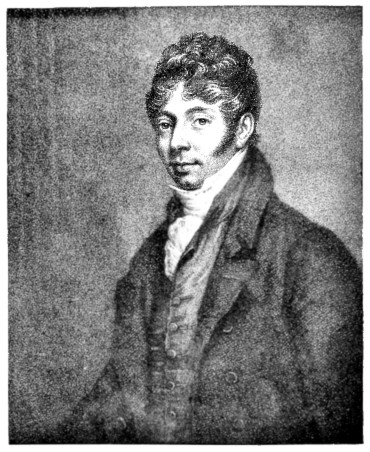
PLATE I.
JOHN CUNNINGHAM SAUNDERS. From an engraving by Anthony Cardon, after a picture by A. W. Devis.
THE HISTORY & TRADITIONS OF THE MOORFIELDS EYE HOSPITAL
ONE HUNDRED YEARS OF
OPHTHALMIC DISCOVERY & DEVELOPMENT
BY
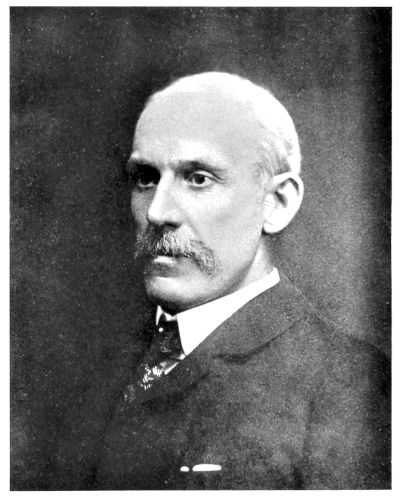
E. TREACHER COLLINS
CONSULTING SURGEON; MEMBER OF THE COMMITTEE OF MANAGEMENT;
FORMERLY, CLINICAL ASSISTANT; JUNIOR AND SENIOR HOUSE
SURGEON; CURATOR OF THE MUSEUM AND LIBRARIAN;
ASSISTANT SURGEON AND SURGEON
WITH TWENTY-SEVEN PLATES
LONDON
H. K. LEWIS CO. LTD.
1929
DEDICATED TO THE MEMORY
OF THE
MEMBERS OF THE SURGICAL STAFF
OF THE
MOORFIELDS EYE HOSPITAL
IN THE YEARS 1883 TO 1887
TO WHOSE INFLUENCE AND INSTRUCTION
THE AUTHOR IS SO DEEPLY INDEBTED
vii
PREFACE
Great traditions are the most valuable assets which a hospital
or a teaching establishment can possess. They give it a
personality which makes it beloved and respected. Traditions
are made up of the energies and enterprise of those
who have gone before, and will live on from generation to
generation long after the bones of those who have created
them have crumbled into dust. The primary aim of this
book is to put on record the traditions of the Moorfields
Eye Hospital for the benefit of past, present, and future
workers within its walls.
So intimately associated has this Hospital been with all
the discoveries and developments which have taken place
in connection with ophthalmology during the nineteenth
century, that it was not possible to write a history of the
first hundred years of its existence without giving an account
of them also. By having done this, it is hoped that the book
may find a wider circle of readers than those for whom it
was in the first instance intended.
An endeavour has been made to give an account of events
as they have happened in chronological order, and by so
doing to produce the effect of a cinematograph film, rather
than that of an album of photographs.
For the facts recorded, numerous different sources have
been tapped. Much information as to the commencement
of the Institution has been derived from Barnsby Cooper’s
biography of his uncle, Sir Astley Cooper. Great use has
been made of the minute books of the Committee of Management
of the Hospital, and of its annual reports.
For biographical details, the Dictionary of National
Biography has been consulted, and also the articles on the
viii“British Masters of Ophthalmology” which have been
published in the British Journal of Ophthalmology.
It has been said that “when a medical man begins to
write on the history of his subject it is a sure sign of senility.”
The writer of these traditions does not claim that his case
is any exception to this rule. In early life a man has to
learn history. In middle life he is engaged in making
history; and it is in his later years that he becomes best
qualified to write history. It is then that, on looking back,
he obtains the most comprehensive view, and is able to
regard objects in their truest perspective.
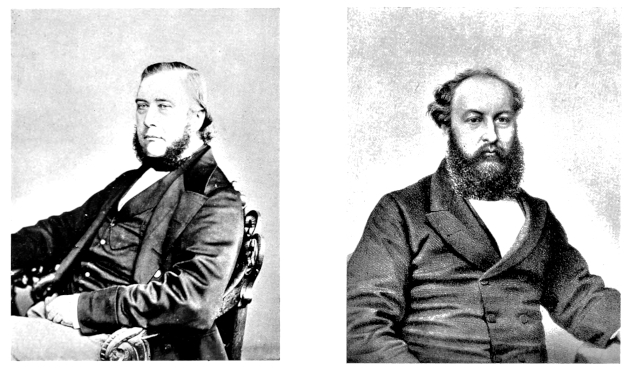
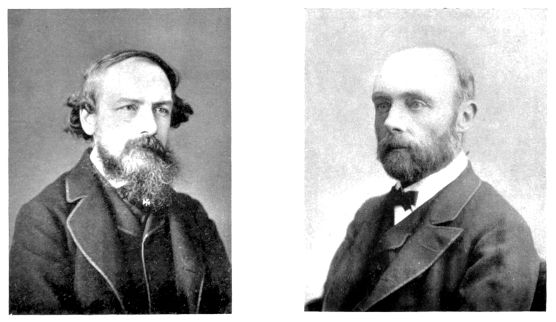
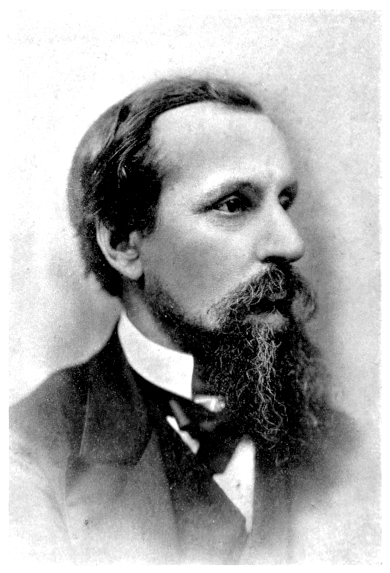
In conclusion I have to thank the Committee of Management
of the Hospital for its permission to reproduce the
portraits of several former members of the surgical staff,
which hang in its Board Room; also the British Journal of
Ophthalmology for permission to use the blocks of some of
the illustrations which have been published in its pages;
and lastly my friend Mr. Frank Juler for kindly reading
through and correcting the proof-sheets.
THE HISTORY AND TRADITIONS OF THE
MOORFIELDS EYE HOSPITAL
CHAPTER I
THE FOUNDERS AND FOUNDATION
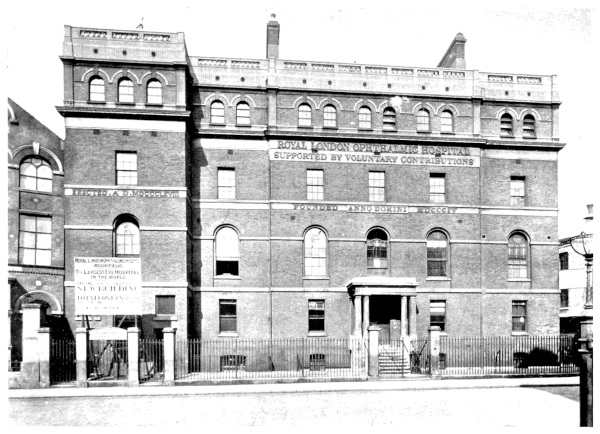
In the board room of the Royal London Ophthalmic
Hospital hangs a framed document in which the names of
Saunders, Farre, and Battley are associated as being the first
promoters of the institution.
Who were these three men? What brought them together?
And how came they to establish an institution
unlike any which had previously existed?
John Cunningham Saunders was born and bred in
Devonshire; he first saw the light of day at Levistone on
October 10th, 1773. He went to school at Tavistock and
South Molton, and at the age of seventeen commenced a
five years’ apprenticeship to Mr. John Hill, surgeon, of
Barnstaple. It was during his apprenticeship that he had
his first introduction to ophthalmic surgery, for Mr. Hill,
though only a country practitioner, was bold enough in those
pre-anæsthetic days to operate for cataract. It was from
him also that Saunders first learnt the value of the use of
belladonna for dilatation of the pupil. William Adams,
who also became an ophthalmic surgeon, was likewise a
pupil of Mr. John Hill, but of him more anon.
Saunders, at the expiration of his apprenticeship, came to
London to complete his medical education at the then
combined borough schools of St. Thomas’s and Guy’s
Hospitals. The skill and diligence which he displayed in
the dissecting room, together with his deftness as a draftsman,
2soon attracted the attention of Astley Cooper, who was
then rapidly rising into fame. On Cooper’s election to the
chair of anatomy in 1797, he offered to take Saunders into
his house and make him a demonstrator of anatomy on the
terms shown in the following letter:
“Dear Sir,
“I ought long since to have informed you of my plan
for the winter, so far as it concerns you, and as I have been
able to decide.
“It is my wish that you should lodge and board in my
house. I have informed you that I live in a plain and
economical style, and that you are only to expect a joint of
meat and a pudding; if this will satisfy you, a bed will be
ready whenever you return to London.
“I can say nothing about the salary you are to receive,
for I have not been able to form any idea of what will be
proper, or how much you may expect; all I can say is that
the sum shall be annually increased, which at the same time
as it may act as a stimulus to you, and make it an object to
proceed in your career, will be more convenient to myself,
because, if no stroke of adverse fortune prevents it, my
income must be yearly improving.
“It is my wish that you should dissect for lecture-work
in Comparative Anatomy, and assist in my preparations.
With respect to the first of these, the labour is certain, and
all other occupations and objects must yield to it; with
regard to the latter, the quantum of employment shall be
guided by your feelings. It is a duty I have performed,
without injury to my health, with much amusement, and
great advantage.
“I am in hopes that you will have no objection to giving
me three months’ information if any other pursuit should
lead you to quit the situation, as otherwise, I may be unable
to procure a substitute, and suffer great inconvenience from
the want of one.”
Saunders accepted the offer, and was shortly afterwards
appointed the demonstrator of anatomy at St. Thomas’s
Hospital. His association with Astley Cooper proved an exceedingly
happy one, he on several occasions being entrusted
with the charge of Cooper’s patients during his absence
3in the country. Saunders was evidently a good teacher,
and possessed of a most attractive personality, so that he
became exceedingly popular with the students, who on
several occasions presented him with pieces of plate as
a token of their regard.
John Richard Farre was two years younger than Saunders,
being born in Barbados in 1775, where he was educated,
and commenced the study of medicine under his father.
He came to England in 1792 to complete his studies at
St. Thomas’s and Guy’s Hospitals. The commencement
of his acquaintance with Saunders and Battley may best
be given in his own words:
“In 1792 I entered as a dresser at Guy’s Hospital. At
that time Sir Astley Cooper had, by his open manner, become
well known among the pupils, but I was not intimate with
him, until after my return, in 1794, from the expedition in
which I served under Lord Moria. I then became more
particularly acquainted with him in the following manner.
“About the year 1798, Sir Astley excited great zeal in the
prosecution of minute anatomy, and the order of the day
became the injection of the absorbents, and the dissection
of parts concerned in operations, especially those of hernia.
It was at this time that my acquaintance commenced with
Mr. Saunders and Mr. Battley, who were both engaged in
the dissecting room. So earnest were we all in the pursuit
of the subjects above described, that Mr. Saunders and
myself became jaundiced, in consequence of the continually
constrained position to which we were subjected, while
leaning over bodies under dissection.
“Mr. Saunders also suffered from a punctured wound
of the finger received while dissecting, which was followed
by extensive inflammation of the arm; nor did this subside
until nearly two hundred leeches had been applied.”
Richard Battley was older than his two friends, having
been born at Wakefield in 1770; he was educated at the
Grammar School there, and subsequently became the pupil
of a physician in that town. For a while he studied at the
Infirmary in Newcastle-on-Tyne, and came to London in
1795. Entering as a pupil at St. Thomas’s Hospital at the
4same time as Saunders, a close and lasting intimacy sprang
up between the two men.
Having thus brought these three men together from
Devonshire, Bermuda, and Wakefield to the dissecting room
at St. Thomas’s Hospital, it next becomes necessary to trace
the circumstances which led them to start the “London
Dispensary for Curing Diseases of the Eye and Ear,” the name
by which the present “Royal London Ophthalmic Hospital”
was first known.
In 1800, when twenty-seven years of age, Saunders became
anxious about his future prospects. His ambition prompted
him with the desire to practise as a surgeon in London;
probably also about this time influences began to work which
made him desire to settle down with an assured income,
so that he might enter into the state of matrimony. There
was little prospect of his obtaining any higher appointment
than that of demonstrator of anatomy in the hospital at
which he was working, the custom in the old-established
hospitals at that time being to select for the staff appointments
a pupil of one of their surgeons, and one who had
been articled at the Royal College of Surgeons for at least
six years. Saunders had not been so articled, having served
his apprenticeship in the country. He was not, therefore,
eligible to compete against those who had proceeded in the
recognised manner, no matter how great his merits. This
was pointed out to him by Astley Cooper, who advised him
in his own interests to seek some other means of support.
Saunders then resigned his post as demonstrator of anatomy
and took over the practice of a surgeon in Gravesend.
Astley Cooper, however, soon began to miss his able
assistant, and found that the other arrangements he had
made, which had to some extent caused Saunders to take
offence, did not work smoothly. He therefore wrote him
the following letter, and induced Saunders’ friend Battley to
go to Gravesend to use his influence in persuading him to
resume his old post:
5
“London,
“July 28th, 1801.
“Dear Sir,
“I have so often explained my reasons for the change
which I made last winter at the Hospital, that I consider it
as almost unnecessary to say anything further upon the
subject. The trial has been made; Mr. D——has been
weighed against you in the balance, and been found wanting.
“His excessive vanity has disgusted, his want of perseverance
has disappointed me, and I feel most thoroughly
convinced that his abilities are inadequate to the task which
has been assigned to him.
“I felt it my duty to act as I have done, and my conduct,
I fear, has been the cause of uneasiness to you; but as our
separation was not the effect of misconduct upon your part,
or of any disapprobation on mine, I hope we shall be again
united in the pursuit of medical science, and that we shall
entertain for each other that respect and esteem which I must
ever feel for you.
“As I told you in our last conversation, I have ever felt
a degree of veneration for your acquirements and abilities,
which has made me diffident in expressing my wishes. But
as you have now courted it, I will say, that I have wished to
see you join in the debates of Guy’s Medical Society. The
capability of expressing our ideas in public is a source of
more power than anything with which I am acquainted.
It is the road to bring a public teacher to character and to
fortune.
“Secondly, I should much wish for your assistance in
making experiments upon animals. I am certain that
everything valuable in physiology is only to be so obtained.
What is every day under observation of the senses is well
known, but few men have sufficient knowledge of anatomy
to be capable of making the interior parts of the body the
subject of inquiry.
“Thirdly, you will do me a favour by making my collection
in comparative anatomy more complete. This, I am aware,
is the greatest favour I can ask, as you are neither captivated
by its splendour nor convinced of its utility; but as I have
embarked on it, you will confer an obligation upon me by
assisting me in making it complete.
“I shall endeavour to make your situation comfortable
6in a pecuniary point of view, but I had rather make that the
subject of conversation when I see you.
“I am, dear Sir,
“Yours, with the utmost esteem,
“A. C. ”
Battley had a high appreciation of his friend’s talents, and
felt strongly that they would not have sufficient scope in
such a confined sphere as Gravesend. The combined
effect of his persuasive influence, and of Cooper’s letter,
ultimately induced Saunders to resume the duties of demonstrator
of anatomy at St. Thomas’s.
Shortly afterwards he took a house in Ely Place, with the
intention of practising as a surgeon, and on April 7th, 1803,
married Miss Jane Louisa Colkett.
During the last years of the eighteenth and the first years
of the nineteenth centuries England was at war with France.
Farre, in 1793, went with Lord Moira’s expedition to France,
returning, however, to London on its failure. Battley for
a time served in the Navy as an assistant surgeon, and was
present at several engagements under Sir Sidney Smith.
In 1799 Napoleon invaded Egypt, and after the destruction
of his fleet by Nelson at the Battle of the Nile, English
troops under Sir Ralph Abercrombie were landed at Aboukir,
in 1800. Almost all were attacked by what was called
“Egyptian ophthalmia,” but which we now know must
have been a mixed infection of purulent ophthalmia and
trachoma. After the evacuation of Egypt by the English
in 1803, the troops were disbanded, and spread this very
infectious form of eye disease in all the stations at which
they stopped and throughout Great Britain.
Mr. Patrick Macgregor, surgeon to the Royal Military
Asylum, writes of the effects of the disease in the Army as
follows:
“The progress of the ophthalmia since its first introduction
into this country in the year 1800 has, in the Army, been very
rapid and extensive, and has at different periods materially
7interfered with its discipline and efficiency. It has crippled
many of our best regular regiments to such a degree as for
a time to render them unfit for service; and though the
regiments which were in Egypt have, in general, suffered
most from the disease, yet it has prevailed extensively in
others which have never served in that country.”
The terribly destructive character of the disease may be
shown by its effects on the second battalion of the 52nd
Light Infantry, which are recorded by Dr. Vetch: out of
636 cases 50 were dismissed with the loss of both eyes, and
40 with that of one.
The spread of the disease was not confined to the Army,
but extended widely throughout the country in the towns
and villages, when the disbanded troops returned to their
homes carrying infection with them.
That the medical men and the hospitals in this country
were badly prepared to deal with such an immense increase
in eye diseases may be shown by quoting a description of
the condition of things which then existed, written by Sir
William Lawrence some thirty years later:
“The diseases of the eye, in general hospitals, are inadequate,
from the smallness of their number, to the purposes
of practical study, particularly that of exemplifying the
various operations. Thus these institutions have been
inefficient in reference to this important department. As
the general body of surgeons did not understand diseases
of the eye, the public naturally resorted to ‘oculists’” [in
speaking of “oculists” he refers to those that have bestowed
that title on themselves without having had any regular
medical training] “who, seeing such cases in greater numbers,
became better acquainted with the symptoms, diagnosis,
and treatment; and especially more skilful in the operative
department. At the same time, the subject, being imperfectly
understood, was neglected in the general surgical courses,
in which many important affections were entirely unnoticed,
and the whole very inadequately explained. Thus students,
who resorted to London for the completion of their professional
studies, had no means of learning this important
8department of the profession, which was tacitly abandoned,
even by the hospital surgeons, and turned over to the
‘oculists.’ The latter, not being conversant with the
principles derived from anatomy, physiology, and general
pathology, attended merely to the organ, and relied almost
exclusively on what is comparatively of little importance,
local treatment. Hence ophthalmic surgery, being in a
manner dismembered from the general science, was reduced
to a very low ebb. Until within a few years, it was, in this
country at least, in a state of almost total darkness.”
It will thus be seen that at the time Saunders established
himself as a surgeon in London there was an immense
increase in the amount of eye disease, but that very few
medical men were in any way trained or competent to deal
with it, and scanty, if any, provision was made for its treatment
in the hospitals.
Saunders’ attention had early in his career been attracted
to diseases of the eye during his apprenticeship under
Mr. John Hill, and his studies in the dissecting room had
afforded him a sound basis for their treatment, in an intimate
knowledge of the anatomy of the organ and its surrounding
structures. His association with Astley Cooper had also
led him to devote special attention to the anatomy of the ear
and to disorders of hearing. Astley Cooper in 1800 made
a communication to the Royal Society, on the effects of
destruction of the tympanic membrane of the ear. He had
found that considerable openings might be made in it
without impairment of the hearing power, and was thereby
led to perform the operation of puncturing the membrane
in cases of deafness resulting from obstruction in the Eustachian
tube, with a remarkably good result in the restoration
of hearing, in the first cases in which he employed it. Subsequent
experience, however, showed it not to be so generally
useful as he had originally anticipated. He made a second
communication on the same subject in the following year,
and in 1802 was elected a Fellow of the Royal Society, and
awarded the Copley Medal.
9
Whilst these papers were being written the subject of them
must have been much discussed by Cooper and his assistant
Saunders, the latter’s interest in ear disease being thereby
awakened.
On starting in practice at Ely Place, Saunders decided to
devote himself to the treatment of diseases of the eye and
ear, a decision which must have required considerable
courage at that time by one who wished to remain of good
repute with other members of his profession. Up to that
time the treatment of eye diseases had been mainly in the
hands of itinerant quacks, who dubbed themselves oculists.
George Coats, who has written an account of the lives and
practices of many of these worthies, has well described the
condition of things which then existed. He says:
“In the eighteenth century ophthalmology had not yet
vindicated, in England, its position as a separate branch of
practice. It was the province of a set of ambulant practitioners
who toured the country accompanied by all the
apparatus of shameless advertisement (including ‘monkies,’
we are told), couching cataracts, and selling infallible salves
and eyewashes. This taint of quackery appears to have
deterred respectable surgeons from meddling much with
the subject; their operative experience was probably small,
and the procedure of couching, attended frequently with
brilliant immediate, but disastrous after, results, was likely
to be performed with fewer scruples by itinerant oculists,
here to-day and gone to-morrow, than by settled practitioners
who had to abide the consequences of their handiwork.”
Such men were naturally looked upon as charlatans by
the medical profession, but that did not prevent them becoming
the recipients of royal favours.
One William Read, who commenced life as a tailor, and
became a mountebank and itinerant quack oculist, settled
in London in 1694, advertising in the Tatler “that he had
been thirty-five years in the practice of couching cataracts,
taking off all sorts of wens, curing wry necks and hair-lips
[sic] without blemish.” In 1705 he was knighted, “as
10a mark of royal favour for his great services, done in curing
great numbers of seamen and soldiers of blindness gratis”;
and about the same time was appointed oculist-in-ordinary
to Queen Anne. It is stated that the wealth he acquired
enabled him to mix with the best literary society of the day.
Swift, in writing to Stella, commented on the quality of his
punch which he served in golden vessels. One sample of
his methods of treatment need only be quoted—“the putting
of a louse into the eye when it is dull and obscure, and
wanteth humours and spirits. This,” he says, “tickleth
and pricketh, so that it maketh the eye moist and rheumatick
and quickeneth the spirits.”
On Sir William Read’s death in 1715, his rival, Roger
Grant, succeeded to the post of oculist to Queen Anne, and
afterwards to George I. Grant, originally a cobbler and
later a Baptist minister, lost one eye as a soldier in the service
of the German Emperor, and then set up as an oculist in
Mouse Alley, Wapping. He advertised profusely in the
journals of the day, giving accounts of his cures, with
certificates attached from the patients themselves and
others.
George II. appointed as his oculist-in-ordinary John
Taylor, better known as “Chevalier Taylor,” of whom
Coats says:
“Amongst travelling quacks the name of the ‘Chevalier’
Taylor stands pre-eminent for unblushing effrontery, blatant
self-laudation, and all the methods of the charlatan, but also
for mental endowments far above the average of his tribe,
and for real acquaintance with the contemporary state of
ophthalmic knowledge. His fame extended to every country
in Europe; his boast of having conversed with kings and
princes is no idle one; he had an acquaintance, not always
felicitous, with some of the best known men, medical and
lay, of his time; counting translations and minor works he
was the author of nearly fifty books; and in later life he wrote
an autobiography, which, if it gives few and unreliable
particulars as to his actions, does much to reveal the character
of the man.”
11
The Chevalier’s talents seem to have been hereditary, for
his son and two grandsons followed the same line of practice,
and were each in turn the recipients of royal favours.
It was with such prating mountebanks that Saunders ran
the risk of being confused in devoting himself specially to the
treatment of eye diseases. He was not, however, the first
reputable medical practitioner in London to specialise in this
line of work, having been preceded by both Wathen and
James Ware. Dr. Wathen published, in 1785, A Dissertation
on the Theory and Cure of Cataract, and held the appointment
of oculist to George III. He took Ware when a young man
into partnership with him, a partnership which lasted for
fourteen years, during which time Ware acquired such a
liking for eye work that he decided to devote himself exclusively
to it.
Ware, like Saunders, had studied at St. Thomas’s Hospital,
and held there the post of demonstrator of anatomy, so it
would seem highly probable that his example may have had
some influence in determining Saunders to take up surgery
of the eye as a special branch of practice.
In 1801 Ware contributed to the Royal Society a paper
dealing with the case of a boy of seven years of age upon
whom he had operated for cataract, and as the result of this
communication he was elected a Fellow of the Royal Society.
It was one of Saunders’ most noteworthy achievements, as
we shall see later, to introduce an operation for cataract in
infants who are born blind.
The suggestion that Saunders should start a special institution
for the treatment of diseases of the eye and ear is
stated by Battley to have originated with Astley Cooper,
whose own experience, in the treatment of diseases of the
ear, had shown him what insufficient accommodation the
General Hospitals offered for the treatment of diseases of the
special organs. As his letters show, he held a very high
opinion of Saunders’ professional abilities, and he saw only
too clearly that the nature of Saunders’ apprenticeship would
12prevent him being promoted to any surgical post at either
of the Borough Hospitals. Consequently the idea suggested
itself to him that a special hospital might be established
for diseases of the eye and ear, at which Saunders might find
a suitable field for the exercise of his skill and ingenuity.
Before taking any action in the matter, Saunders first sought
the advice of the physicians and surgeons of St. Thomas’s
and Guy’s Hospitals, and having obtained from them a testimonial
of their approbation, on October 1st, 1804, he published
the following proposal for instituting “A Dispensary
for the Poor afflicted with Diseases of the Eye and Ear,” with
their testimonial attached:
“Among the many charitable institutions which mark the
wisdom and benevolence of the inhabitants of this Metropolis
there is none particularly appropriated to the relief of
the poor afflicted with diseases of the Eye and Ear. No
diseases which do not affect the life of the patient are more
distressing than such as are incident to these organs or
demand greater dexterity and skill in their treatment. The
structure of the Eye and Ear is so delicate and complex and
their irritability under injury so extreme, that they cannot
easily be treated but by those who make them the objects of
peculiar study and attention. The acknowledged difficulty
in the treatment of the diseases to which they are liable has
induced a few to separate themselves from the general
practice of professional duties and to devote themselves to
the exercise of this branch alone, a fact which sufficiently
establishes the necessity of making them the objects of a
specific institution. Every surgeon must allow that most
unremitting care and attention is necessary after some of
the capital operations on the eye, and that through the want
of it some of the most dexterous operations are frequently
defeated. In large hospitals and dispensaries which embrace
a variety of objects, where the medical attendants are deeply
interested in the most formidable and excruciating diseases,
it can rarely happen that sufficient leisure is afforded
for the exercise of that strict care and attention which
operations on the eye demand, much less will it happen,
when patients are the subjects of fortuitous operations and
retire afterwards to their own homes where they experience
13a miserable want of every comfort and convenience, that such
operation can be successful. Impressed with these considerations
the author of this address, who devotes himself
to the treatments of diseases of the Eye and the Ear, solicits
the public to patronise an institution which will enable him
to extend relief to the poor afflicted with these diseases. An
institution of this kind will be the means of restoring to
society the exertions of many industrious individuals and will
be established and carried on at a very moderate expense.
The author of this address offers his services to the Charity
without any emolument to himself and he pledges himself
to the promoters of the institution, that the public shall reap
the fruits of their beneficence.
“J. C. Saunders,
“Surgeon and Demonstrator of Practical
Anatomy at St. Thomas’s Hospital.
“24, Ely Place, Holborn,
“October 1st, 1804.”
“We are of the opinion that the establishment of the
dispensary will prove beneficial, and is therefore worthy of
public support, and that the author of the proposal is qualified
to procure the accomplishment of its object.
Signed:
Physicians of St. Thomas’s.
Physicians of Guy’s.
Wm. Lister, M.D.
Wm. Babington, M.D.
W. C. Wills, M.D.
James Curry, M.D.
Thos. Turner, M.D.
M. Alexander, M.D.
G. Gilbert Currey, M.D.
Surgeons of St. Thomas’s.
Surgeons of Guy’s.
G. Chander.
T. Foster.
I. Birch.
Wm. Lucas.
H. Cline.
Astley Cooper.”
As the outcome of the issue of this circular a committee
was formed which held its first meeting at the City Coffee
House on January 4th, 1805, Mr. Benjamin Travers, a
wealthy City merchant and the father of the surgeon of the
same name, being in the chair.
This Mr. Benjamin Travers, Sen., in the keen pursuit
of knowledge, had attended Astley Cooper’s lectures on
14anatomy, and had become so interested in them and the
lecturer, that he apprenticed his son to him as a pupil, and
later extended his patronage to the project of founding an
eye dispensary put forward by Cooper’s demonstrator and
protégé.
At the meeting the following resolutions were moved and
unanimously agreed to:
“That a dispensary be instituted under the name of the
London Dispensary for the Relief of the Poor afflicted with
Diseases of the Eye and the Ear, where they may apply and
obtain advice and medicines gratis.
“That the dispensary be situated in a central part of this
city and contain beds for the reception of patients who
undergo the operation for the cataract or any other operation
of the eye requiring minute care.
“That the Charity consist of a Treasurer, Governors,
Secretary, and Medical Officers.
“That Henry Kensington, Esq., be appointed Treasurer.
“That a person contributing an annual subscription of one
guinea be a governor and have the right of recommending
and keeping under the care of the charity one out-patient,
and if two guineas, two out-patients, and so in proportion to
his subscription.
“That patients admitted into the house be admitted according
to priority of recommendation, except in cases of emergency,
when the medical officers must determine.
“That Mr. J. C. Saunders be appointed Surgeon of the
Dispensary, and that Dr. Farre be appointed Consulting
Physician in cases requiring medical aid.”
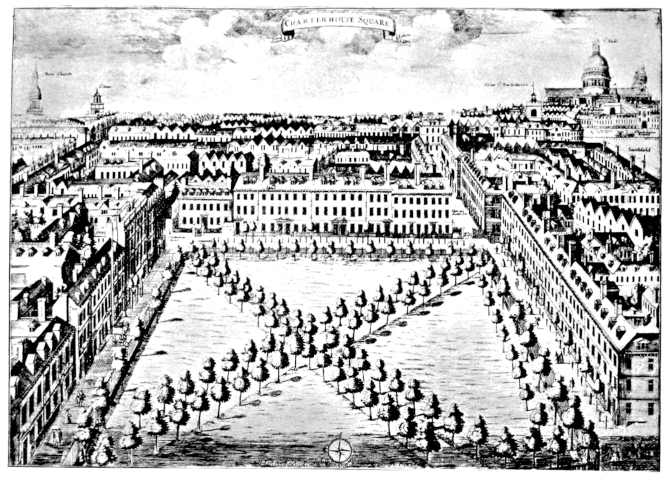
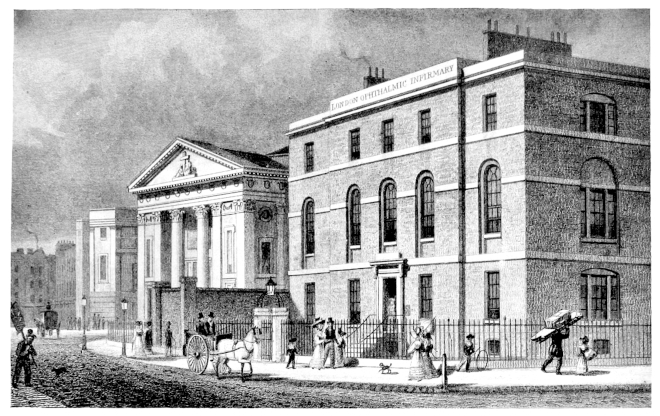
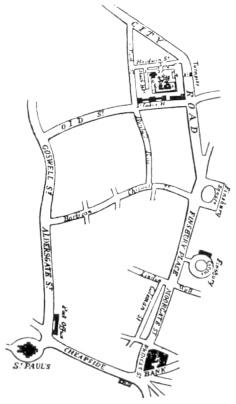
PLATE II.
SHOWING THE SOUTH SIDE OF CHARTERHOUSE SQUARE AND NO. 40
Where the London Dispensary for Curing Diseases of the Eye and Ear
was first opened in 1805.
Richard Battley, who was then practising as an apothecary
in St. Paul’s Churchyard, undertook the duties of Secretary,
which he continued to discharge in an honorary capacity,
with the utmost assiduity, for fourteen years.
Many City merchants, with whom Saunders had no
previous acquaintance, became subscribers, and sufficient
funds were soon forthcoming to provide for the purchase of
the lease of No. 40, Charterhouse Square, for eighteen years,
for the sum of £300 and an annual rental of £65.
15
On March 25th, 1805, The London Dispensary for Curing
Diseases of the Eye and Ear was opened for the reception of
patients.
Sir Charles Price, Bart., a former Lord Mayor, and Member
of Parliament for the City of London, accepted the post of
President of the Institution, and several of the Aldermen
of107
the City became its Vice-Presidents.
One Sarah Clark was appointed nurse and housekeeper,
she being required to act under the control of the Surgeon,
who had power to dismiss her for misconduct. She was
allowed coals and candles and a gratuity at the end of the
year “such as the Committee may deem proportionate to her
services.” Her husband was subsequently engaged to dispense
drugs, and the two of them received £50 a year for their
services, together with the aforesaid coals and candles.
In 1804, after Saunders had brought forward his proposal
for the establishment of an Eye Dispensary, Mr. Wathen
(afterwards Sir Wathen Waller), an oculist of eminence,
described to King George III. the sad state of the soldiers
and sailors who had returned from the campaign in Egypt
suffering from ophthalmia, and suggested the desirability of
establishing an Infirmary exclusively for eye diseases: “Their
Majesties and the Royal Family graciously and humanely
approved of the plan, and honoured it with their patronage
and benefactions.” Such was the origin of the Royal Infirmary
for Diseases of the Eye, in Cork Street, which commenced
under Mr. Wathen, and was subsequently carried
on as a comparatively private institution, under the charge of
Mr. Charles Alexander, up to the time of his death in 1872.
This institution must not be confused with that started
in the Western district of London, by the Army surgeon
Guthrie, in 1816, which exists to-day as the Royal Westminster
Ophthalmic Hospital.
That Wathen’s Infirmary was opened for the reception of
patients three months before the London Dispensary, though
the proposal for its establishment was not made until after
16the publication of Saunders’ circular, evidently caused the
latter considerable annoyance, for in a letter addressed to the
Committee of the Dispensary in 1808 Saunders writes:
“Subsequently to the date of my Proposal, a similar
Institution, honoured with the Royal Patronage, was formed
and established in Westminster. Although the Prospectus
of the Royal Infirmary was not heard of until many months
after the Publication of my Proposal, yet it must be admitted
that that Institution first appeared before the Public in a
regular and organised form, and this, which is the original,
is consequently considered by all who are unacquainted with
the facts as the copy. Apprehensive of this impression, I
immediately claimed by public advertisements, which were
never answered, the priority of my Proposal.
“I should be excused for thus obtruding on your notice if
I sought merely the indulgence of honest pride, by maintaining
this just claim to respect, but I shall yet more readily be
excused, when you reflect, that if I had abandoned this claim,
the Public would continue to regard me as an humble
copyist.”
This Royal Infirmary, whose rivalry at its commencement
caused Saunders so much annoyance, continued in existence
until Alexander’s death in 1872. It was then resolved at a
meeting of its Life Governors and Subscribers to close the
Institution and to hand over the balance of its funds, after
the settlement of all its liabilities, to the Royal London
Ophthalmic Hospital. Two hundred pounds was ultimately
received by the Hospital, and three of the Committee of the
old Infirmary were elected as Life Governors, one of them
being a relative of the late Mr. Alexander.
17
CHAPTER II
THE WORK OF JOHN CUNNINGHAM SAUNDERS
That the Institution which Saunders had founded provided
a much felt want is evident from the following statement of
the number of patients with eye diseases dealt with, and the
numbers stated to be “cured,” during the first four years of
its existence.
It must be admitted that it is somewhat doubtful what the
term cured actually implied, for in a list of the diseases
which those “cured” suffered from are included some, such
as total opacity of the cornea, for which even to-day no
absolute cure is known.
Successful as the Institution proved to be in dealing
with eye disease, it was far less so in connection with ear
disease.
Saunders’ first publication was a book entitled The
Anatomy of the Ear: A Treatise on the Diseases of that Organ.
The Causes of Deafness and their Treatment. It must
evidently have met with much demand, for a third edition
was published after his death, in 1829. Although he had
devoted so much study to the treatment of diseases of this
organ, he seems soon to have realised that the interests of his
Institution would be best served by restricting its aims to the
treatment of diseases of the eye only. His reasons for doing
so are set out in the following letter which he sent to the
Committee in December, 1807:
18
“Gentlemen,
“Antecedent to the establishment of this Dispensary
the diseases of the Eye and Ear had never been made the
object of a specific institution, although their great variety
and complexity seem to require the most minute and attentive
investigation. Those who have practised on the eye have
always partially cultivated the ear, and when I chose the
former for professed pursuit, the latter also became the
subject of my serious enquiry. I had ascertained by observation
that certain cases of disease are alleviable. Still I was
aware how little would be the success, as the most complicated
structure of the organ, which occupies an inaccessible part
of our frame, is most frequently the seat of disease. Regardless
of this conviction and solely influenced by a knowledge
of the positive good which the deaf occasionally receive, I did
combine in my proposal for the institution of this charity,
the ear with the eye, solicitous of gaining public esteem by
doing for the public all the good in my power. But the
experience which this institution affords demonstrated the
proportion of curable and incurable cases, a proportion much
smaller than was expected, at most exceeding (obstruction
from inspissated wax excepted) one in a hundred. It grieves
me now to state, this branch of our institution exhausts the
funds without an adequate advantage, and consumes a
portion of my time on an impracticable point, that must
ultimately tend to diminish my reputation. The performance
of this part of my duty is, therefore, irksome to me, not
because it is laborious, but because it neither leads to distinction
nor obtains even the common reward of benevolent
institutions. To be thankful for intended benefits demands
a refinement of reason which none but liberal minds possess.
Of those who are dismissed incurable more are made vindictive
by disappointment than are grateful for the care
bestowed upon them, and the former almost universally
represent him who has ineffectually attempted their relief
as the author of their misfortunes.
“My attention to the vast number of irremediably deaf
which are accumulated at the Charity is not merely disagreeable
to my feelings, but absolutely injurious to my
interest by causing me to be considered as an Aurist when
I am in fact an Oculist. The branch of the profession has
always been in my private practice a secondary object. In
this light I should wish it to be placed in the Dispensary.
19The Ear may consistently with the preservation of those
privileges which the Governors have acquired be withdrawn
from public notice. Then, whilst I render the same
service to those for whom they may individually be interested,
it will cease to operate to my prejudice. The mode to be
adopted for the accomplishment of this object is implicitly
submitted to your judgment.
“I am, gentlemen,
“Your obedient servant,
“J. C. Saunders.”
After consideration of this letter by the Governors it was
resolved, at a General Meeting in the following January:
“That diseases of the Eye shall in future be the sole object
of the Charity, and that its name be changed to that of
The London Infirmary for Curing Diseases of the Eye.”
In June, 1806, Saunders published an Essay “On Inflammation
of the Iris, and the Influence of the Extract of Belladonna
to prevent the Consequent Obliteration of the Pupil.”
In it he gives an accurate description of the clinical characteristics
of the affection, and records several cases treated at the
Dispensary in which he had prevented loss of sight from
closure of the pupils by keeping them dilated with the
extract of belladonna, applied to the conjunctiva whilst the
inflammation lasted.
In January, 1809, he advertised in the medical journals
his intention of publishing a treatise on some practical points
relating to the diseases of the eye, and particularly on the
nature and cure of cataract in persons born blind.
Up to the beginning of the nineteenth century only two
forms of operation for cataract were in vogue: that of displacing
the opaque lens downwards with a needle out of the
axis of vision, the operation of “couching,” which may be
regarded as one of the most ancient of surgical procedures;
and that of removal of the opaque lens out of the eye, the
operation of “extraction,” first performed by the French
surgeon Daviel in 1745.
20
It was observed by several operators who couched cataracts
that if they failed in displacing the lens down it was sometimes
possible to break it up with the needle, and that the
fragments so formed tended in time to disappear. Percival
Pott, a surgeon at St. Bartholomew’s Hospital, in 1775, first
pointed out that this disappearance of the fragments of lens
substance was due to them becoming dissolved in the fluids
of the eye, and he advocated a procedure to facilitate their
solution.
To Conradi, a surgeon at Nordheim in Hanover, seems
to be due the merit of first proposing a distinct method of
operating for cataract by its division with a needle through
the cornea, and he published an account of his method in 1797.
Neither the operation of couching nor that of extraction
were found suitable for small children afflicted with cataract,
and it was customary in cases of congenital cataract to advise
postponement of operation until the patient had arrived at
the more manageable age of twelve to fourteen. As has
been already mentioned, James Ware, in 1801, contributed
a paper to the Royal Society, describing how he had removed
a cataract from a boy, aged seven, by breaking it up with
a couching needle.
In the medical report of the Dispensary at the end of its
second year it is recorded that three children born blind with
cataract had been cured at the respective ages of seven, five,
and four years. On its receipt by the Governors the following
resolution was passed:
“That the thanks of this General Meeting be given to
Mr. Saunders for the ability and care by which he has cured
so great a number of patients, many of them labouring under
the most complicated diseases of the eye, and more especially
for having been the first to establish by repeated success the
propriety of performing the operation for the cataract at the
earliest ages in children born blind of that disease.”
So pleased were the Governors with this proof of the value
of their charitable institution that they directed that these
21three small children whose sight had been restored should
be introduced at the anniversary dinner. These anniversary
dinners were held each year for the purpose of increasing
the number of subscribers to the Charity. The dinner
at which these children were exhibited was held at the London
Tavern, Bishopsgate Street, in May, 1807, at 5 p.m. It is
recorded that the price of the dinner was 7s. per head,
including beer, bread, cheese, and radishes. The dessert
was 1s. 6d. extra, and the wines, port and sherry. The
President, Sir Charles Price, Bart., M.P., was in the chair,
and about one hundred gentlemen were present; sixty new
subscribers were obtained.
At a similar dinner held in the following year the number
of Governors and their friends who attended was 277,
and new subscriptions to the amount of £708 15s. were
received.
In a letter to the Committee, dated March, 1808, Saunders
wrote as follows with reference to his work in connection with
congenital cataract:
“By the adaptation of an operation on the cataract to the
condition of childhood I have successively cured without
a failure fourteen persons born blind, some of them even
in infancy, and it has just been performed on an infant only
two months old who is in a state of convalescence. As
I reserve for another occasion the communication of the
method which I pursue for the cure of very young children,
I shall no further compare it with extraction, than by observing
that extraction is wholly inapplicable to children, or only
fortuitously successful. Those who on all occasions adhere
to this operation, and have never turned their thoughts
towards the application of means more suitable to this tender
age, have been obliged to wait until the patient has acquired
sufficient reason to be tractable; otherwise when they have
deviated from this conduct, the event has afforded little cause
of self-congratulation.
“How great the advantage of an early cure is a question
of no difficult solution. Eyes originally affected with
cataracts contract an unsteady and rolling motion, which
22remains after their removal, and retards, even when it does
not ultimately prevent, the full benefit of the operation.
A person cured at a late period cannot overcome this awkward
habit by the utmost exertion of reason or efforts of the will.
But the actions of infants are instinctive. Surrounding
objects attract attention, and the eye naturally follows them.
The management of the eye is therefore readily acquired,
his vision rapidly improves, and he will most probably be
susceptible of education about the usual period.”
During 1809 Saunders, in preparation for the publication
of his advertised treatise, wrote essays “On the Inflammation
of the Conjunctiva in Infants” and “On the Cure of the Inversion
of the Eyelids by Excision of the Tarsus.” He also
commenced to put together his notes on congenital cataracts
and of his methods of operating on them. His work,
however, in these matters became much impeded by recurrent,
violent, acute attacks of headache due to brain disease,
which in February of the following year proved fatal.
Saunders had realised that congenital cataracts varied
considerably in character and consistency, and also that they
might be dealt with either by passing the needle, as in couching,
through the sclerotic and behind the iris in its approach
to the pupillary area, or through the cornea, the so-called
anterior operation. He was wisely waiting to gain experience
as to which form of procedure was better suited for the
different forms of cataract before rushing into print on the
matter. He had two pupils working with him at the Dispensary,
both of whom subsequently became ophthalmic
surgeons, and both of whom in later years wrote in glowing
appreciation of all they learnt from him. The one was
William (afterwards Sir William) Adams, and the other John
Stevenson. Two letters addressed to the latter in April and
August, 1808, are the only authentic documents in Saunders’
writing descriptive of his operation for cataract; with the
first he enclosed two of his improved needles for Stevenson’s
own use. Needles of a similar pattern are still employed,
and known by Saunders’ name, at the present time.
23
“My dear Friend,
“I confide the method of operating which I pursue
for cataract to your honour, and I am very certain that it is
safely deposited. I shall not have time to point out all the
advantages which result from this deviation from the old
method of couching; but simple as they appear, they are
very important, as you will perceive when I detail all the
circumstances, which I shall sometime do, in a treatise on the
cataract.
“I always use the solution of Belladonna, and never begin
the operation until the pupil is as much dilated as it will
admit of, keeping the eye, by means of Pellier’s elevator, or
else my own fingers, as steady as possible. The object of my
introducing the instrument into the eye is, to cut the capsule
in the anterior part of the crystalline; and therefore, as the
lens is generally more dense towards the centre, I take care
that it shall pass through the crystalline as near to the capsule
as possible. That the instrument may traverse the lens
freely, you will observe that it is made of the greatest tenuity,
and flat, and that it cuts towards the point on each side. I
find by experience that it can be conducted, with care,
through the hardest lens; whereas the needles, such as
Scarpa’s and Hey’s, only push the whole lens before them,
and without being able to carry the instrument to the capsule,
the lens is made to press on and protrude the iris; whence
results the consequent inflammation. As for the crystalline
itself, you may or may not meddle with that; it may be well
to loosen its texture in some instances, but you ought never
to depress it....
“The instrument should enter the sclerotica about a line
behind the ciliary ligament, and should be conducted through
the anterior part of the crystalline which is softest. You
may loosen the texture of the cataract before you divide the
capsule, or after, as in the operation seems most convenient,
but the capsule must be divided at all events. I do not much
care what becomes of the substance of the crystalline. I
sometimes let it go in considerable quantity into the anterior
chamber, if it seems tending that way, but I never push it,
because that must press the iris. N. B.—Follow Hey’s rule,
to be careful not to do too much. After the operation the
plan with me is purely antiphlogistic, and I believe you
well know what that is. If your operation should not
succeed at the first attempt, describe to me the appearances,
24and I will gladly give you my sentiments as to repeating it.
“With respect to congenital cataracts, from the repeated
conversations we have had on the subject, it seems scarcely
necessary for me to remind you, that they are generally
capsular, the whole or greater part of the lens having probably
been, at some antecedent period during the foetal state,
spontaneously absorbed. I shall only add to what I have
already stated, that the steps to be pursued in the operation
are nearly similar to those adopted for lenticular cataract;
the great object being either to make a sufficiently large
central aperture for the rays of light to pass freely through it
to the retina, or also to endeavour to tear the condensed
capsule into as small fragments as possible, and be gradually
absorbed; for which purpose, you may use the needle with
much more freedom than in the former case.
“With our united regards,
“I am yours faithfully,
“J. C. Saunders.”
It is interesting to note how in these pre-anæsthetic days
the small children were kept sufficiently still to allow of
operations for cataract to be performed on their eyes. The
following is the description of the method employed given
by Dr. Farre:
“Four assistants, and in stouter children five, are required
to confine the patient. The first fixes the head with reversed
hands, the second not only depresses the lower lid with his
forefinger, but also receives the chin of the child between
his thumb and forefinger, as in a crutch. By this means the
play of the head on the breast is prevented, a motion which
the child incessantly attempts, and which will very much
embarrass the surgeon. The third assistant confines the
upper extremities and body; the fourth the lower extremities.
The surgeon, seated on a high chair behind the patient,
takes Pellier’s elevator in his left hand, and the needle in his
right, if he is about to operate on the right eye, or the speculum
in his right hand and the needle in his left, if the operation
is to be performed on the left eye.”
The following is the commencement of an unfinished
medical report which Saunders had in preparation to
25present to the Committee of the Infirmary at the time of
his death.
“Gentlemen,
“Five years have now passed since my proposal for
establishing this Infirmary was submitted to your notice,
during which I have incessantly and anxiously laboured to
redeem the pledge then given to make it a beneficial Institution
to Society. My anxiety has been relieved, and my
labour consoled in the progress of this Institution, by repeated
instances of your respect; and the recollection of them at
present only heightens the satisfaction I feel, on finding
myself confirmed as the conductor of an establishment
supported by liberal and zealous advocates, and possessed
of the means of performing an important part in Society,
and esteemed by Society for it.
“In prosecuting the object of attracting public attention
towards this Institution, I trust I have kept free from the
practice of any disingenuous art. Popularity has not been
snatched; but studiously and unremittingly sought: it was
expected only as a reward of service; and the share of it which
has been gained, is ascribable to the estimation in which the
Governors have been pleased to hold this service. I have
confided the character of the Institution to the quantum of
professional good—excepting you may be pleased to add, that
mindful of being an agent for liberal and philanthropic men,
I have always administered with humanity and attention to
the feelings of the poor that relief which their bounty has
supplied.”
Owing to the early death of Saunders, before the publication
of his promised book on diseases of the eye, and of any
description of his operation for cataract, there was much
heated controversy for many years afterwards, in which the
Committee of Management of the Infirmary became involved.
The chief matters around which dispute arose were: the
publication of Saunders’ unfinished manuscripts; his claim
to having introduced a new form of treatment for cataract;
the advertisement of his successful results prior to making
known to the profession his method of procedure; and the
priority of his invention of an operation for the restoration
26of sight in those in whom it had become impaired from
Egyptian ophthalmia.
Saunders died intestate, and there was nothing left for his
widow but what might result from the publication of his
unfinished manuscripts. The Governors of the Institution
decided, in the first instance, that the book should be published
at its expense, and that the proceeds of the work
(without any deduction) should be appropriated to the sole
use and benefit of Mrs. Saunders. It was afterwards found
that Mr. Saunders’ brother and sister could claim legal
rights to the proceeds. It was, therefore, decided in lieu
to present £50 to Mrs. Saunders and an annuity of £40.
Dr. Farre, at the request of the widow and of Mr. Saunders’
brother, consented to edit the book and make good its deficiencies,
and it was published by Messrs. Longman and
Company in 1811, delay being caused in connection with
the question of copyright. Eighteen months after Saunders’
death his widow married again, under which circumstances
the Committee considered they had reserved to themselves
the right of reconsidering her annuity, and it was discontinued.
It was agreed, however, that she should retain the
copyright of her late husband’s book and receive any further
proceeds that might arise from its sale; these rights she later
parted with to Messrs. Longman and Company for the sum
of £50. When a second edition of the book was called
for, Longmans offered the copyright to Dr. Farre; he refused
it for himself, but accepted it on behalf of the Infirmary.
The discontinuance of the annuity to Saunders’ widow
after her second marriage was the subject of an attack by
those at enmity with Farre and Battley up to the time of her
death in 1817.
The book, entitled A Treatise on some Practical Points
relating to the Diseases of the Eye, opens with a short account
of Saunders’ life, a rather detailed account of his last illness,
and a statement of the morbid appearances found by Astley
Cooper on the examination of his body. The account of
27his illness suggests that he suffered from a tumour of the
brain, which had affected one of his optic nerves and caused
impairment of the sight of his right eye. At the post-mortem
examination, however, no tumour was found, the
immediate cause of death being cerebral haemorrhage.
The first two chapters of the book consist of the three
previously published essays already referred to; the other
three of unfinished notes which were arranged and added to
by Dr. Farre, and which deal with “Cases illustrating
Changes of Structure in the Eye,” and with “Congenital
Cataract.”
In the course of events it not infrequently happens that
circumstances lead up to an epoch when some new development
becomes ripe for discovery, and that then more than
one mind independently “hits the moment” at about the
same time. Later on, when history steps in to record the
event, considerable discussion is liable to arise as to whom
the palm of priority is to be awarded. This is what occurred
in connection with the introduction of the operation of
solution for the removal of congenital cataracts.
The solubility of the substance of the crystalline lens in
the aqueous humour of the eye had been recognised long
before Saunders began to operate for cataract. But in introducing
the method of solution for the dispersion of cataracts
in infancy he undoubtedly believed he had discovered a new
method of treatment. He appears to have been unaware
of Conradi’s method of needling cataracts in adults, published
in Germany. The real value of his contribution to ophthalmology
in this matter is well estimated in the following
extract from a lecture published in the Lancet by Mr. Green,
a surgeon at St. Thomas’s Hospital, in 1823:
“I do not mean to say that this operation is entirely new;
if you read Mr. Pott’s works, you will find that, in some
instances, he performed a very similar operation. He tells
you, that in cases where the cataract was too soft for depression,
he sometimes lacerated the anterior layers of the capsule,
28so as to admit the aqueous humour, and procure the
solution of the cataract. Hey, Scarpa, and Ware have
performed similar operations. We are not, however, to
consider those as inventors of any practice who have merely
employed it here and there, without stating any certain rules
for its general applicability. It is to Dr. Saunders that we
are indebted for having shown the principle on which he
performed this particular operation, its applicability to
cataract in children, and to some cases of cataract in adults.
Dr. Saunders, therefore, may be justly considered as the
inventor of this operation, and entitled to our respect and
admiration of so material an improvement in this branch of
surgery.”
It must, however, be admitted that it was an error of
judgment on Saunders’ part to have allowed the Committee
of Management to advertise in the public press, stating that
operations were being performed at the Infirmary on children
born blind of cataract, before the nature of the operation
had been made known to the medical profession. Such
a practice, together with the exhibition of the children who
had been operated on at a public dinner, savoured rather of
the methods of the quack oculists, though Saunders himself
derived no pecuniary benefit and died a poor man.
Benjamin Gibson in Manchester, independently of
Saunders, recognised the possibility of operating successfully
on congenital cataracts in infancy, and in the October
number, for 1811, of the Edinburgh Medical and Surgical
Journal, published a description of his methods in an article
entitled “On the Use of the Couching-needle in Infants of
a Few Months Old.” The description of his operation was,
therefore, published almost at the same time as Dr. Farre’s
description of Saunders’ methods of procedure.
Saunders’ two pupils, William Adams (afterwards Sir
William) and John Stevenson, followed the example of their
teacher, both claiming to having introduced new methods of
operating on the eye, and both founding institutions for the
treatment of its diseases.
29
William Adams, as already mentioned, had, like Saunders,
served his apprenticeship with John Hill, of Barnstaple, and
had completed his medical education at St. Thomas’s and
Guy’s Hospitals. He worked under Saunders in the dissecting
room and also at the Eye Infirmary, assisting him
for a year and a half in both his public and private operations.
After obtaining the diploma M.R.C.S. in 1807, he went to
reside in Exeter, where he founded the West of England
Eye Infirmary for curing diseases of the eye, on the same
lines as the one in London; this Institution continues its
work to-day under the same name. To it Saunders allowed
his name to be attached as Consulting Surgeon, and wrote
advice on several occasions to Adams concerning his work
there.
Saunders had pledged Adams not to reveal the nature of
the operations he had learnt from him before he had had
time to publish a description of them. Even before Saunders’
death Adams resented being bound to observe this pledge,
and after his death considered himself exonerated from its
further observance. Most operators in the course of their
practice introduce modifications in their procedures. Adams
considered that the modifications which he introduced in the
operations he had learnt from Saunders justified him in
claiming them as his own. It was on the strength of these
claims, that on his return to London, after Saunders’ death
in 1810, he was appointed to operate on pensioners dismissed
from the Army as blind through Egyptian ophthalmia.
The operation he performed was a modification of that
introduced by Saunders of excision of the tarsus of the eyelid.
He was also appointed to operate for cataract on seamen
at Greenwich, and later an Ophthalmic Institution was
founded for him in part of the York Hospital, Chelsea, which
was afterwards transferred to Regent’s Park.
He became oculist extraordinary to the Prince Regent
and to the Dukes of Kent and Sussex, and in 1814 was
knighted. A Select Committee of Parliament reported on his
30work at the Ophthalmic Institution and on his claim to public
money, and with Lord Palmerston’s support he was voted
the sum of £4,000.
Sir William Adams’ claims to the invention of new operative
procedures was much resented by Farre and Battley,
who regarded them as piracy of their deceased friend’s work
at the Eye Infirmary. In 1814 the Committee of Management
of that Institution requested its medical directors to
furnish them with a report on the matter, showing how
Sir William Adams’ claims had been anticipated. This
report was sent to His Royal Highness the Duke of York,
the Commander-in-Chief of the Army, and to His Majesty’s
Ministers, with the request that deputations from those connected
with the Infirmary might be received. As an outcome
of the deputation to the Duke of York, His Royal
Highness graciously condescended to become a Patron of the
Infirmary.
In 1817, when the question of a monetary grant to Sir
William Adams was raised in Parliament, further deputations
waited on Lord Palmerston and on the Chancellor of the
Exchequer with the object of refuting his claims, and of
obtaining some pecuniary assistance for the Infirmary’s
building fund, but no success in the latter direction was
met with.
In later life Adams became interested in Anglo-Mexican
mines, but his speculations do not appear to have been
attended with success. Two years before his death he
changed his name to Rawson in compliance with the will of
his wife’s mother, the widow of Colonel Rawson.[A]
[A] It is due to this change of name that a writer of a life
of Sir William Adams, in Vol. II. of the British Journal ofOphthalmology, failed to find a notice of him in the Dictionary of National Biography.
It is from the description there given of
Sir William Rawson that most of the above facts respecting him have
been taken.
John Stevenson, like Adams, worked under Saunders in
the dissecting room at St. Thomas’s Hospital and at the Eye
31Infirmary. Having obtained the diploma of M.R.C.S., he
settled in or near Nottingham, but on Saunders’ death returned
to London to practise there as an oculist and aurist.
In 1813 he was appointed as such to the Prince of Wales and
to Leopold, the Duke of Saxe-Coburg.
He wrote several treatises on the structure and functions
of the eye and ear, and much on the subject of cataract and
its treatment. Whilst always acknowledging his obligations
to Saunders and his admiration for his genius and industry,
he claimed credit for having introduced a method of successfully
removing cataracts in adults at an earlier stage in their
development than was then usual, and thereby obviating
a prolonged period of semi-blindness.
In 1830 he founded at 13, Little Portland Street, Cavendish
Square, the Royal Infirmary for Cataract and other
Diseases of the Eye, under the Patronage of His Majesty
King William IV., to whom he was soon after appointed
oculist and aurist. This Infirmary, besides the patronage
of the King, had a long list of Royal Patronesses and of noble
supporters. The indigent poor suffering from all forms of
diseases of the eye were treated gratis as out-patients, but
only cataract cases were admitted as in-patients. In the
Dictionary of National Biography it is stated that after 1844
all trace of Stevenson is lost.
It is noteworthy that both this Infirmary and Wathen’s
Institution, which were established under Royal Patronage
in the West End of London, existed for only a comparatively
brief time, whilst that founded by Saunders, with the
approval and support of the medical and surgical staffs of
the Borough Hospitals, and under the patronage of the City
fathers, has continued to flourish and grow in the manner
which the following pages will relate.
Farre described Saunders as a man of middle size, well
made and of an engaging mien, with an active mind,
generous in his private practice, and perfectly unreserved in
stating his opinion in cases submitted to his judgment. That
32he had the capacity of forming firm friendships is shown by
the marked respect which Farre describes as having been paid
to him at his funeral, and the steps which were taken to perpetuate
his memory. At a General Meeting of the Governors
of the Eye Infirmary it was unanimously agreed that a
portrait and bust of Mr. Saunders should be obtained and
placed in the Committee Room. In accordance with this
resolution a portrait was painted by Devis, and a bust was
executed by Henry Weekes. The former hangs to-day in
the Board Room of the present Hospital, and an engraving
of it by Anthony Cardon was inserted as a frontispiece to
Saunders’ treatise, and is still used to adorn the certificates
which are presented to students who have completed a course
of instruction at the Hospital.
This portrait shows Saunders with a mass of brown
curly hair coming low down over his forehead, with mutton-chop
whiskers, pronounced features and a mouth shaped
like a Cupid’s bow. He wears a high white stock round his
neck, has a frill to his shirt, and a blue coat.
33
CHAPTER III
BENJAMIN TRAVERS AND SIR WILLIAM LAWRENCE
The death of the founder of the Charity only five years after
it was first opened placed its Committee of Management in
a most difficult and unexpected position. Astley Cooper
came to its immediate assistance, conducting the operating
department and frequently attending in the receiving room
until a new surgeon was appointed. Being keenly interested
in all branches of surgery, he was probably pleased to have
this opportunity of gaining experience in the surgery of the
eye.
The vacancy was advertised in three leading London
newspapers, several applications being received in response.
Amongst the candidates were Saunders’ former pupil at the
Infirmary, John Stevenson, and William Lawrence (afterwards
Sir William), who was then demonstrator of anatomy
at St. Bartholomew’s Hospital; both of these, however,
withdrew their applications in favour of Benjamin Travers’
who was unanimously elected at a ballot of the General
Committee.
Benjamin Travers was then twenty-seven years of age,
and had been a house pupil of Astley Cooper’s, of whom
evidently he was a great admirer, for in later years he wrote
this description of him:
“Astley Cooper, when I first knew him, had the decidedly
handsomest, that is the most intelligent and finely formed
countenance and person of any man I remember to have
seen. He wore his hair powdered, with a queue, then the
custom, and having dark hair and always a fine, healthy
glow in his cheeks, this fashion became him well. His
34frequent costume during the summer when taking horse
exercise (for at this season he rode daily on horseback) was
a blue coat, yellow buckskin breeches and top-boots, then
much in vogue.”
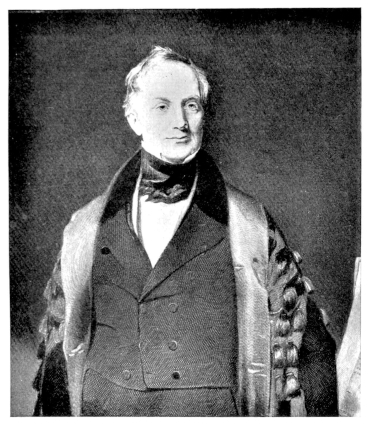
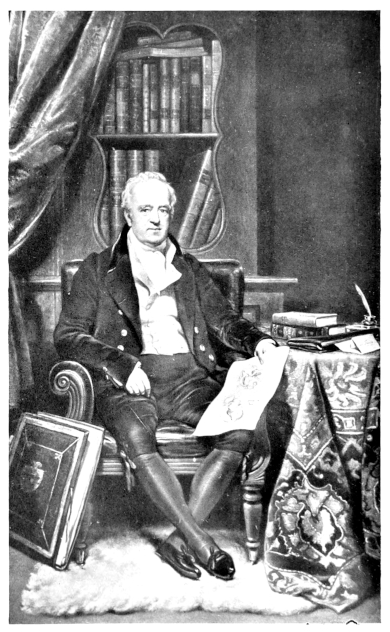
PLATE III.
SIR ASTLEY PASTON COOPER, BART., F.R.S.
From an engraving by W. H. Mote, after a picture by Sir T. Lawrence, P.R.A.
Travers had been articled at the Royal College of Surgeons
for six years; he was, therefore, unlike Saunders, eligible
for appointment as surgeon to a general hospital when
a vacancy arose, and was so appointed to St. Thomas’s
Hospital in 1815. At the time of Saunders’ death he was
demonstrator of anatomy at Guy’s Hospital and surgeon
to the East India Company.
In accepting the post of surgeon to the Eye Infirmary he
did not, like Saunders, devote himself exclusively to treating
diseases of the eye and ear, but combined the practice of
ophthalmic surgery with that of general surgery. In the
preface of a book he subsequently wrote, entitled A Synopsis
of Disease of the Eye, he claims to have been the first general
hospital surgeon in this country to have given more than
a cursory attention to diseases of the eye. In doing so he
incurred no small risk to his reputation as a general surgeon,
for, as already stated, those who practised as oculists at that
time were of but low repute. His courageous and disinterested
action in this matter served, however, to raise the surgery
of the eye out of the condition of quackery into which it
had fallen.
Shortly after Travers was appointed surgeon to the
Infirmary it was decided to increase its accommodation by
providing eight additional beds, so that other than cataract
cases might be admitted.
In 1811, in accordance with the recommendation of
Dr. Farre and Mr. Travers, the practice of the Infirmary
was opened to medical students, and permission was granted
to the medical officers to deliver lectures on the subject of
their profession. Thus was started the school of ophthalmology
which has since developed into a teaching centre of
worldwide renown.
35
Amongst the earliest students to avail themselves of the
instruction given were two young Americans, who had
recently graduated in medicine at the College of Physicians
and Surgeons in New York, and who had come to London
to complete their training: Dr. Edward Delafield and
Dr. J. Kearney Rodgers. So impressed were they with the
Institution and its teaching that, on their return to New York
in 1818, they determined to establish one on similar lines in
that city. In August, 1820, “The New York Eye and Ear
Infirmary” was opened, and continues as one of the leading
special hospitals of the sort in America at the present time.
It is interesting to note that whilst the parent Institution has
changed its title from that of “Infirmary” to that of “Hospital,”
the daughter Institutions both in Exeter and New
York retain the older name.
Dr. Delafield later showed his appreciation of Travers’
teaching by editing an edition of his Synopsis of Diseases of
the Eye, which was published in New York. As one of the
first surgeons in the United States to devote himself to the
study of diseases of the eye, he was, when the American
Ophthalmological Society was founded in 1864, most appropriately
elected its first President.
A few years later Dr. Edward Reynolds came from Boston,
Mass., to London to pursue his medical studies. He attended
the practice and lectures at the Eye Infirmary under Benjamin
Travers and William Lawrence, and, in a letter written
home to Dr. J. C. Warren, gave the following description
of the former:
“He is not a very pleasant lecturer—his voice is low and
his manner is very inanimate and uninteresting, but his
matter, however, is very valuable.”
On Dr. Reynolds’ return from Europe he found his father
blind from cataract in both eyes. There were no specialists
in that part of the country at that time, so, fortified by his
recent experiences in London, he decided to operate, happily
36with complete success. The following is an interesting
description of this event, written by Dr. Edward Reynolds’
grandson in 1910:
“I well remember my grandfather’s telling me of his
operation on his father’s eye. He told me that his father,
finding his eyesight failing, made great efforts to accustom
himself to its gradual disappearance and to the performance
of his ordinary duties without the aid of sight, and that
upon one occasion, after finishing the process of shaving
between two windows in his room, he put away his razor
and, turning to his wife, said to her: ‘My dear, I am at last
totally blind, I can see nothing.’ My grandfather said that
his father had written him nothing of this infirmity, which
came on while he was a student in London; that it was, in
consequence, a great shock to him to find his father blind.
He said that on looking at the eyes, and satisfying himself
that the blindness was due to cataracts, he thought the
situation over; that his father was too old to take the sailing
voyage to London and, so far as he knew, no operation for
cataracts had been performed in America, and certainly none
in this locality; that he was therefore probably better qualified
than any one available for the performance of the operation;
and that he decided to attempt it. He said: ‘I went into my
closet and offered a prayer to Deity for success, took a glass
of sherry and went ahead to do my best.’ The three phrases
of this sentence have always seemed to me exceedingly
characteristic of the man as I knew him.”
The success of the operation becoming widely known led
to the foundation of Dr. Reynolds’ reputation as the leading
surgeon in Boston in diseases of the eye, and to the foundation
in 1824 of “The Massachusetts Charitable Eye and Ear
Infirmary.”
As already mentioned, Travers held the appointment of
surgeon in London to the East India Company. In 1819
its Honourable Directors became impressed by the great
prevalence of eye disease in the large and populous districts
over which they ruled, and applied to Travers in the matter.
He pointed out to them the excellent results which had
37followed the establishment of the Eye Infirmary in London,
and that similar Institutions might be started in India. This
advice was accepted, and Mr. R. Richardson, one of the
Company’s surgeons, who had studied ophthalmology
under Travers, was sent to Madras, where he founded
“The Madras Eye Infirmary,” which was each year resorted
to by increasing numbers of patients. The Infirmary has
been several times enlarged, and in 1888 its name was altered
to that by which it is now known, “The Government Ophthalmic
Hospital.”
Stimulated by the success which attended the establishment
of the Eye Infirmary in Madras, the East India Company
determined to start similar Institutions in other provinces.
In 1824 two other surgeons who had studied at
the London Eye Infirmary were sent out to India for this
purpose: Mr. Jeafferson went to Bombay and Mr. C. J.
Egerton to Calcutta, where each of them founded an Eye
Hospital.
During the first seven years that the London Eye Infirmary
was open for medical students 412 pupils received instruction
there, of whom fifty were physicians and the rest surgeons.
They came not only from the three divisions of the United
Kingdom, but also from India, America, Germany, Portugal,
and other countries; many of them held important posts in
the Army and Navy. Ten years later still it is recorded that
the number who had received instruction at the Institution
considerably exceeded one thousand, and that they were
spread over every part of the world.
In 1814 Travers found the increasing number of patients
coming to the Infirmary made the work so arduous that it
was impossible for one individual to cope with it satisfactorily,
and he wrote to the Committee requesting them to
appoint a second surgeon to co-operate with him. This
they readily agreed to, and, at a meeting of the General
Committee, with whom the election of members of the
medical staff then rested, William Lawrence, demonstrator
38of anatomy and assistant surgeon to St. Bartholomew’s
Hospital, was appointed.
PLATE IV.
BENJAMIN TRAVERS, F.R.S.
One of Travers’ earliest surgical achievements was the
cure of a pulsating tumour of the orbit, described as an
aneurism by anastomosis, by ligature of the common carotid
artery. It was the first case in which such treatment had
been employed, and the second case on record of successful
ligature of that artery. He communicated the case to the
newly formed Medico-Chirurgical Society in 1809. He was
possessed of considerable literary ability, and rendered
Sir Astley Cooper considerable assistance in collaborating
with him in the production of a volume of surgical essays.
In 1815 Travers was elected a Fellow of the Royal Society,
and in 1820, after he had resigned his appointment at the
London Eye Infirmary, published the treatise already referred
to, entitled A Synopsis of Diseases of the Eye, which he
dedicated to Dr. J. R. Farre, in esteem for his character,
admiration of his talents, and gratitude for his friendship.
This book had the merit of being entirely the outcome of
his own observations at the Eye Infirmary, and was not
a compilation of the work of others. It is stated to have been
the application of Hunterian principles of inflammation to
the diseases of the eye. That it met with a wide appreciation
is shown by its having passed through three editions, by its
having been translated into Italian, and by its being reedited
and reproduced in New York by Travers’ former
pupil, Dr. Delafield.
From a writer of an obituary notice we get the following
description of Travers as a man:
“He was tall, large formed, and well proportioned, with
a highly intelligent and pleasing countenance. His manners
were prepossessing, and in consultation with his professional
brethren he showed a high-bred courtesy which marked the
refinement of his mind.”
Pressure of work, and some fears as to his health, necessitated
his retirement from the staff of the Eye Infirmary
39in 1817. He lived, however, until 1858, and was twice
elected President of the Royal College of Surgeons. The
year before his death he was appointed serjeant surgeon to
Queen Victoria.
The chief financial support of the Infirmary for many
years after its foundation was derived from subscriptions
and donations received at its anniversary dinners. The
exhibition of patients at these dinners was apparently continued
until 1812, for a minute of that year states that their
attendance was in future to be dispensed with.
Another method of raising funds in support of the Charity
was to obtain the services of some eminent divine to preach
a sermon on its behalf on the Sunday before the dinner,
with permission for him to do so at one of the City churches.
Alderman Ansley, who had been one of the Infirmary’s most
jealous supporters since its conception, in the year of his
Mayoralty, not only presided at its annual meeting of
Governors and at the anniversary dinner, but also attended
in state at Bow Church when the Rev. Henry White preached
a sermon in support of the Charity.
It is interesting further to note that, in spite of the Peninsular
War, which is said to have cost England £100,000,000,
and of the European campaign which followed Napoleon’s
escape from Elba and ended with the Battle of Waterloo,
the funds of the Charity showed a steady increase, both that
for general purposes and one started in 1813 for purchase
of a freehold and the erection of a suitable building. In
1815, the Waterloo year, the anniversary dinner was held
in May, presided over by the President, Sir Charles Price,
Bart., and the anniversary sermon was preached at St.
Botolph’s, Aldersgate Street, before the Lord Mayor. The
invested fund for general purposes in April that year amounted
to £2,415, and the building fund to £852; in October the
general purposes fund had increased to £2,800 and the
building fund to £1,160.
The rapid increase in the work of the Infirmary, both in
40the in- and out-patients’ departments, necessitated in 1816
a reorganization of its resident staff, and it was arranged
that this should consist of a housekeeper and sister with
a salary of 25 guineas per annum, a housemaid at 10 guineas,
a cook at 12 guineas and a resident apothecary and sub-secretary
at £50 per annum. A year previously a dispenser
had been appointed to make up and distribute drugs for the
patients in place of Mr. Clarke, the porter; it was now decided
that these duties should be performed by a resident officer.
From the rules drawn up detailing the apothecary’s duties,
they would seem to have included all those now performed
by the house surgeons, dispensers, and the assistant secretary.
His first and most important occupation is defined as
follows:
“To compound and dispense the medicines, to cup,
bleed, apply leeches, dress setons, etc., and to obey orders
of the Medical Directors relative to the business of the
Infirmary.”
The withdrawal of blood was regarded at that time as of
the utmost importance for the reduction of inflammatory
conditions of the eye, and the apothecary must have had his
time fully occupied in this way. Respecting the general
principles for its employment, Lawrence wrote:
“Of the means of reducing inflammation, abstraction of
blood is the most powerful. Blood is the material by which
the increasing action of the part is maintained. In the
figurative language, which the obviously increased heat has
suggested, we may say that it is the fuel by which the fire
is kept up. If we could completely command the supply of
blood, the increased action might be effectively controlled
or arrested. In comparison with the loss of blood, all other
means are of minor importance in lessening the local disorder
and quieting the general disturbance.”
Regarding the quantity of blood to be drawn from the arm,
he says:
41
“We cannot determine the amount beforehand; we cannot
decide that ten, twelve, or sixteen ounces will be sufficient;
it may be necessary to take twenty, thirty, or forty ounces, or
to produce syncope, if you cannot otherwise make the requisite
impression on the vascular system.”
After venesection the next best method of taking blood is:
“By cupping from the back of the neck or the temple,
especially the latter, from which blood can be obtained
quickly and in large quantity. Branches of the temporal
artery are commonly wounded in this operation, facilitating
the abstraction of the blood, and causing neither danger nor
inconvenience.”
With regard to the use of leeches he writes:
“It is a common error here, as in other inflammations, to
apply them in too small a number; if the disease be active
and the patient adult, it will seldom be proper to put on
fewer than twelve, while eighteen or twenty-four will more
frequently be necessary, in order to produce decided benefit.”
In a book published “on the traffic with leeches” in 1826,
it is stated that not less than seven million two hundred
thousand of these animals were annually sent to England.
This so-called “antiphlogistic treatment,” which was so
implicitly relied upon in those times for the relief of inflammation
in the eye, consisted, not only in the withdrawal of
blood, but also in purging, dieting and the administration of
tartar emetic to excite perspiration, nausea, or vomiting
Lawrence writes:
“It is not sufficient in the treatment of inflammation to
diminish the quantity of the circulating fluid by the abstraction
of blood, we must prevent the introduction of further
supplies into the vascular system by the use of purgatives
and the regulation of diet.”
The diet of the patients in the Infirmary, from the table
then in use, seems, according to our present standards, to
have been both meagre and monotonous. It was arranged
42under three headings, “Low diet”; “Reduced diet”;
and “Full diet.” Low diet consisted of milk pottage or
gruel, with 12 oz. of bread for women, and 1 lb. for men.
Reduced diet consisted of the same allowance of bread, but
included broth in addition to milk pottage. Full diet had,
in addition to the milk pottage and bread, 8 oz. of meat,
broth and vegetables for dinner, and one pint of small beer.
In 1817 new regulations were drawn up for the election
of medical officers. The qualifications required of candidates
for the offices of physician, surgeon, and apothecary
were as follows: Physician: that he be a Fellow or Licentiate
of the London College of Physicians, or a Bachelor of
Medicine of one of the English Universities. Surgeon:
that he be a Member of the College of Surgeons, and have
served an apprenticeship at one of the hospitals of this
Metropolis. Apothecary: that he be a Member of the
College of Surgeons, and a Licentiate of the Society of
Apothecaries. It was further arranged that the election of
medical officers should be vested in the Governors, and not
left to the General Committee, as was previously the case.
After these regulations had been passed Travers resigned
the post of surgeon, which he had held for seven years, and
was elected a Vice-President. It had been a source of great
satisfaction to him to have had a man of William Lawrence’s
professional attainments appointed as his colleague on the
staff. In the year previous to his joining the Infirmary Lawrence
had been elected a Fellow of the Royal Society, and
appointed assistant-surgeon to St. Bartholomew’s Hospital.
Travers felt that, with Lawrence’s co-operation, his unprecedented
step of associating the practice of an oculist with
that of a general surgeon was being justified. The Infirmary
also gained a better reputation in the profession, by showing
that it was not merely the offshoot of one hospital, but was
prepared to appoint as members of its staff those educated
at, and connected with, other institutions.
William Lawrence not only became the leading ophthalmic
43surgeon of his time, but also a leading general surgeon,
a philosophic writer, an eloquent teacher and lecturer, and
a strongly combative medical politician. It is unnecessary
here to go into the inconsistencies in his career, such as the
withdrawal from publication of his book on the Comparative
Anatomy, Physiology, Zoology, and Natural History of Man,
when it aroused an angry outcry from the orthodox religious
folk of the day; and his change from being a leading reformer
of the constitution of the College of Surgeons to one of its
most vigorous supporters. In his recognition of the importance
of a knowledge of diseases of the eye by medical men he
always remained firm, being the first to advocate that a course
of instruction in it should be included in the medical curriculum.
In an introductory chapter to his Treatise on Diseases of
the Eye, he urged that the course of procedure in the study
of ophthalmology should be the same as that for diseases in
general, and be founded on the science of anatomy, physiology,
pathology, and therapeutics. He pointed out that the
instruction given at the Eye Infirmary was intended to impart
to physicians and surgeons a knowledge of ophthalmic
disease, and not merely to make oculists.
In this same introductory chapter he gives a short history
of ophthalmology, from which some points may here be
quoted. Amongst the ancient Egyptians there were specialists
for affections of the eye, as there were for every other class
of disease. Herodotus tells us that Cyrus, King of Persia,
sent to Amasis, King of Egypt, for an oculist. The extent
of the Greeks’ knowledge of eye disease is evidenced by the
imperishable records of language, for many of them still
bear the names given to them by the ancient Greek writers.
That the Roman Emperors Augustus and Tiberius had
oculists is evident from inscriptions on seals. In the fifteenth,
sixteenth, seventeenth, and first half of the eighteenth centuries,
the management of diseases of the eye was left to
quacks, mountebanks, and itinerant practitioners, the French
44writers on the subject, Maitre-Jan, St. Yves, and Janin, being
more respectable than their contemporary brethren in other
countries. The anatomy of the organ began to be more
carefully cultivated by the Germans about the middle of the
eighteenth century, when Zinn, Professor of Anatomy at
Gottingen, published his excellent Descriptio Anatomic Oculi
Humani, and later Soemerring his Icones Oculi Humani, with
its beautiful and accurate engravings. Boerhaave of Leyden
made some study of the pathology of the eye in his De Morbus
Oculorum. But the most important era in the history of
ophthalmic surgery was the establishment of the Vienna
school of ophthalmology in 1773, by Joseph Barth, who was
appointed lecturer on ophthalmic surgery in the University
of Vienna in that year. He was succeeded by Schmidt, and
afterwards by Beer, who held the post of Professor of Ophthalmic
Medicine in the University for many years, wrote several
theses on the subject, and attracted students to his clinic from
all parts of Europe.
PLATE V.
SIR WILLIAM LAWRENCE BART., F.R.S.
From an engraving by E. R. Whitfield, after a picture by Pickersgill, R.A.
If a man’s worth is to be judged by the estimates of those
who were his pupils and assistants, then indeed Sir William
Lawrence must be described as great. Sir James Paget,
who in his day was the most fluent and mellifluous orator
in the medical profession, said in describing Lawrence’s
teaching:
“It was the best method of scientific speaking that I ever
heard, and there was no one, at that time in England, if I may
not say in Europe, who had more completely studied the
whole principle and practice of surgery.”
Sir William Savory, Lawrence’s most devoted disciple,
who described him as “a model of intellectual beauty,”
speaks of
“his natural grace and dignity of bearing,” of “his vast and
capacious intellect,” of “his unfailing fluency of pure and
perspicuous language,” and says “he touched nothing that
he did not adorn.”
45
On the vacancy on the staff being advertised after Travers’
retirement, applications were received from Edward Stanley,
a former pupil at the Infirmary, who was then demonstrator
of anatomy at St. Bartholomew’s Hospital; Frederick
Tyrrell, who had served his apprenticeship under Sir Astley
Cooper at Guy’s and St. Thomas’s Hospitals, who had also
studied at Edinburgh University, and worked in the Military
Hospital at Brussels after Waterloo; Samuel Cooper,
whose name is famous in connection with his Dictionary of
Surgery, Henry Earle, surgeon of the Foundling Hospital
and assistant-surgeon to St. Bartholomew’s Hospital.
It soon became evident that the Governors were in favour
of a candidate coming from St. Thomas’s Hospital, with
which Travers, who was retiring, was connected, and the
other candidates withdrew their applications, expressing their
wish to come forward again on some future occasion, so that
Tyrrell was elected.
Lawrence continued as senior surgeon to the Infirmary
until 1826, retiring at the age of forty-three. Both he and
Dr. Farre were regular attendants at the meetings of the
Committee of Management, and lent valuable aid and advice
in the arrangements connected with the building of the new
Infirmary at Moorfields.
After his retirement he published a book on The Venereal
Diseases of the Eye. Previous to its appearance, affections
of the eye had received but scant attention from writers on
venereal diseases in this country, though they had been dealt
with more extensively by Schmidt and Beer in Vienna.
The former seems to have been the first to describe inflammation
of the iris, and to have used the term “iritis.”
In the first chapter of the book Lawrence says:
“The venereal diseases of the eye have been mentioned
by many writers, but, for the most part, in such general
terms as to convey no clear information respecting the circumstances
under which they arise, their characteristic
appearances, their progress, effects, or treatment. Hence,
46although one of these affections, namely acute gonorrhœal
inflammation of the conjunctiva, is of the most violent and
rapidly destructive kind, and another, syphilitic iritis, produces,
more or less speedily, changes of structure which injure
or destroy sight, they have entirely escaped the notice of
some modern writers in this country, who have been regarded
as the principal authorities on the venereal diseases.”
The book gives a full account of the nature, symptoms, and
treatment of these diseases, based entirely on Lawrence’s
own experience. The notes of the cases from which his
descriptions were drawn are appended, most of them having
been under his care at the Eye Infirmary, thus bearing
evidence to the advantage of a special hospital in supplying
material for the study of the natural history of disease.
In 1833 he published his Treatise on Diseases of the Eye,
a most scholarly work, based, as he says in the advertisement,
on the lectures on Anatomy, Physiology, and Diseases of the
Eye, which he delivered at the London Ophthalmic Infirmary,
and which were reported at the time in the Lancet. It
contained not only the outcome of his matured experience,
but also references to the views and practice of all the best
known European writers. It is probably one of the best,
if not the best, book dealing with eye disease in pre-ophthalmoscopic
times; two further editions were published in
England and one in America. It was also translated into
several foreign languages, part even into Arabic.
Lawrence continued to hold his post of surgeon to St.
Bartholomew’s Hospital until 1865, when he retired at the
age of eighty-two, no age limit having been fixed previous
to his appointment. In 1867 he was appointed serjeant
surgeon to Queen Victoria, and in 1867 was made a Baronet,
but died the following year.
In 1818 Richard Battley, who had gratuitously performed
the duties of secretary to the Institution since its establishment,
found it necessary to resign. He did not, however,
cease to interest himself in the work of the Charity he had
47helped to found; he continued to attend its Committees,
and, as we shall see later, he taught and lectured to students
on matters connected with pharmaceutical subjects.
In the same year the Infirmary lost, through death, two of
its earliest and most enthusiastic supporters, its first President,
Sir Charles Price, Bart., and the Chairman of its Committee,
Mr. Harry Sedgwick. To the post of President thus left
vacant Mr. William Mellish, M.P., was elected. The name
of Sedgwick is still held in grateful remembrance at the
Hospital, and will be as long as it continues, for in his will he
provided for its endowment, as is shown by the following
extract:
“I leave the interest of the remainder of my Property to
my wife and children or the survivors of them for their lives,
and to my sister if she survives them for her life. After her
decease, I leave in trust the principal, to be invested in the
3 Per Cent. Consols, in the names of the President, Treasurer,
Physician, and Surgeon of the London Infirmary for Curing
Diseases of the Eyes, now situated in Charterhouse Square,
the principal on no account whatever to be touched, but the
interest as it arises to be applied to the benefit of that truly
benevolent and valuable Institution for ever.”
48
CHAPTER IV
REMOVAL TO MOORFIELDS
The lease of the house in Charterhouse Square was purchased
for a period of eighteen years; at the end of nine years it
became obvious that, to cope with the continuously increasing
work of the Charity, it would be necessary when the lease
expired to provide larger and more commodious premises.
It was, therefore, decided in 1813 to open a fund for the
provision of a suitable freehold and building. To this fund
the Lord Mayor, Aldermen, and Common Council of the
City of London, as a mark of their approval, contributed
£100.
In March, 1819, a Building Committee was appointed to
find a suitable site and to draw up plans. The possibility
of acquiring from the City a piece of ground in Moorfields
soon came under consideration. Frederick Tyrrell was the
son of Timothy Tyrrell, who was the City Remembrancer
and resided at the Guildhall, and it was with his aid that
negotiations for this site were entered into. Timothy Tyrrell
became a member of the General Committee of the Infirmary,
and his eldest son, John Tyrrell, a barrister, became an
active member of the Building Committee.
Though the option for refusal of a plot of land to the north
of the Roman Catholic Chapel in Moorfields was then
obtained from the City, it was not until more than a year
later that an agreement to acquire the freehold was decided
upon. In the meantime, several other possible sites had
been inspected and rejected.
It was in October, 1820, that, at a meeting at the Guildhall
with the Committee of the City Lands, the following terms
were finally entered into:
49
“That the Infirmary should acquire the freehold of a plot
of land on the North-East side of Moorfields, to the extent
of 88 ft. in width and 85 ft. in depth, for the sum of £800,
to be paid at the time of the roof of the intended building
being complete, and that a pepper-corn rent only be paid
from Christmas next until Lady Day 1822. The Institution
to be at the expense of preparing the Title.”
Robert Smirke, F.R.S., F.A.S., R.A. (afterwards Sir
Robert), was commissioned to prepare plans for the building,
the expenses of which were to be limited to £5,000. Subsequently
Smirke found that, in consequence of the unexpected
loose nature of the land of the site chosen, extra
expense would be incurred in forming the foundations of
the proposed building, and the limit of the amount was
increased to £5,500.
On May 2nd, 1821, the General Committee of the Infirmary,
after having assembled at the City of London Tavern,
proceeded with the President to the ground in Moorfields
to lay the foundation stone of the new building, in which
stone was deposited the following coins: 1 sovereign, 1 half-sovereign,
1 crown, 1 half-crown, of the reign of
George IV.; 1 shilling, 1 sixpence, and in silver, one piece
value each 4d., 3d., 2d., 1d., of the reign of George III.;
upon these was placed a brass plate having the following
inscription engraved thereon:
“London Infirmary for Curing Diseases of the Eye,
founded by the late John Cunningham Saunders Esq.,
A.D. MDCCCIV. The foundation-stone of the new building
for the same Institution, henceforth to be entitled
The London Ophthalmic Infirmary, was laid in Moorfields,
on the second day of May, 1821, by the President.
50
Patron: Field-Marshal His Royal Highness the Duke of York, K.G., etc.
President: William Mellish, Esq.
Vice-Presidents:
St. Asaph, The Right Rev.
Sir Charles Flower, Bart., Ald.
Lord Bishop of.
Thos. F. Foster, Esq.
John Ansley, Esq., Ald.
Sir William Leighton, Ald.
John Julius Angerstein, Esq.
Sir Charles Price, Bart.
William Babington, M.D., F.R.S.
Jeremiah Olive, Esq.
George Bainbridge, Esq.
Thomas Rowcroft, Esq.
Thomas Boddington, Esq.
Sir James Shaw, Bart., Ald.
George Byng, Esq., M.P.
John Thompson, Esq.
Henry Cline, Esq, F.R.S.
Benjamin Travers, Esq., F.R.S.
Astley Cooper, Esq., F.R.S.
Sir Robert Wingram, Bart.
Treasurer: Michael Bland, Esq., F.R.S.
Medical Directors.
Physician: John Richard Farre, M.D.
Surgeons: William Lawrence, Esq., F.R.S. Frederick Tyrrell, Esq.
Committee:
Aaron, Lewis, Esq.
Kerr, Niven, Esq.
Bainbridge, John, Esq.
Mackie, John, Esq.
Bonsor, Joseph, Esq.
Mellish, Thos., Esq.
Blades, John, Esq.
Ommanney, Sir F. M. , M.P.
Brandain, Samuel, Esq.
Pearce, J. M. , Esq.
Brown, Thomas, Esq.
Price, Ralph, Esq.
Browning, William, Esq.
Price, Richard, Esq.
Brydon, William, Esq.
Price, Charles, Esq.
Battley, Richard, Esq.
Russell, Rev. John, D.D.
Cazenove, John, Esq.
Read, Samuel, Esq.
Clarke, John, Esq.
Row, William, Esq.
Cohen, Joseph, Esq.
Rudge, Rev. Jas., D.D., F.R.S.
Crawley, William, Esq.
Smirke, Robert, Esq.
Croskey, J. D. , Esq.
Solly, Thomas, Esq.
Curtis, Timothy, Esq.
Sparks, R. W. , Esq.
Dean, John, Esq.
Towle, Thomas, Esq.
Elgie, William, Esq.
Thomas, John, Esq.
Gamble, Robert, Esq.
Tyrrell, John, Esq.
Hartshorne, John, Esq.
Tyrrell, Timothy, Esq.
Heathfield, Richard, Esq.
Warburton, Thos., Esq.
Hodgkinson, John, Esq.
Ward, Samuel, Esq.
Horner, John, Esq.
Yates, William, Jun., Esq.51
Hon. Chaplain: The Rev. Thos. Gill, M.A.
Solicitor: Robert Pitches, Esq.
Secretary: Matthew Heathfield, Esq.
Apothecary: Mr. Charles Craddock.
Architect: Robert Smirke, Esq., F.R.S., F.A.S., R.A.”
A prayer suitable to the occasion was offered up to Almighty
God by the Chaplain.
At six o’clock the Governors and friends of the Charity
dined at the City of London Tavern, when contributions
since January 1st of that year were announced to the amount
of about £1,200 for the building fund.
Moorfields was originally a piece of moorland lying to the
north of the old City wall, access to which was obtained
through the Moorgate. Early in the seventeenth century it
was drained, laid out in walks, and planted with trees. For
a long time it remained a place of recreation and jollification
for the City folk—a place of swings and roundabouts, as is
described in the following verses in the vade mecum for
malt worms:
“In Moor’s most pleasant Field, where Northern Lads
With Western Youths contend for broken Heads,
And where our Weal thy Citizens repair
To lengthen out their Lives with wholesome Air;
Jointing to Trotter’s famous Castle, stands
A noted Mansion built by artful Hands;
Where Young and Old, at small Expense can find
Delightful Pastimes to refresh the Mind.
Hither the sprightly Genius has recourse
To practise Riding on the Flying-Horse;
Where danger-free, he through the Air may scow’r,
And, void the Wings, fly fifty miles an Hour;
Nor that has this Courser, tho’ he runs so fast,
One living Leg to expediate him hast,
Yet carries double, treble, if requir’d,
But never stumbles or is ever tir’d.
As for the pregnant Wife, or tim’rous Maid,
Here’s a true South-Sea Coach, that sporting flies
Between the humble Earth and lofty skyes,
Manag’d to rise and fall with little Pains, 52 Like the uncertain Stock that turns our Brains.
Liquors, the best, are also vended here,
From Heav’nly Punch to Halsey’s Noble Beer,
By gen’rous Whitehead, who deserves the Bays
From all the Sons of Malt that Merit praise;
Therefore, if any will prove the Poet just,
Thither repair and you will surely find
Your entertainment good and Landlord kind.”
In a map of London of the middle of the eighteenth century
Moorfields is shown divided up into three sectors, Upper,
Middle, and Lower. The site of the Upper Moorfields is
now marked by Finsbury Square, and that of Lower Moorfields
by Finsbury Circus; Middle Moorfields lay between
the two.
It was at the north-east corner of Lower Moorfields that
the Infirmary was erected. No paved roads led up to it, only
tracks: one of these to the north, then called Broker Row,
became Eldon Street, another leading out of London Wall
to Broker Row became Blomfield Street. It was in the angle
between these two streets that the Infirmary was situated.
The site now occupied by Broad Street Station, directly
opposite the Infirmary, was then an open space.
PLATE VI.
THE LONDON OPHTHALMIC INFIRMARY AS FIRST ERECTED AT MOORFIELDS IN 1822.
From an engraving by R. Acon, after a drawing by Tho. H. Shepherd.
On the laying of the foundation-stone of the new building
its name was changed, for the third time, to that of “The
London Ophthalmic Infirmary and this was yet again
altered in 1837, under circumstances that will be mentioned
later, to that which it now bears, “The Royal London
Ophthalmic Hospital.” The name, however, by which it is
most generally known is “The Moorfields Eye Hospital,”
though it has never been officially so designated.
It was not the first “Moorfields Hospital”; if a patient
had said that he had been an inmate of “The Moorfields
Hospital” in the eighteenth century he would have been
regarded as an escaped lunatic. “The Bethlehem Royal
Hospital” for lunatics was built on the south side of
Lower Moorfields in 1675; it was a substantial building
accommodating 150 patients, and remained in existence
53until 1815, when it was removed to Lambeth. To go and
see the lunatics at Moorfields was for over 200 years one of
the sights of London, the public being admitted to view the
poor wretches on the payment of a small charge. It is stated
that as much as £400 a year was received towards the upkeep
of the Institution in this way; the chains with which the
patients were secured and the other sufferings to which
they were subjected is, however, not part of this history.
The architect of the Ophthalmic Infirmary, Robert Smirke,
R.A., who was knighted in 1832, has left his mark deeply
impressed on London; to him we owe, amongst other important
London buildings, the British Museum, Covent
Garden Theatre, the East Wing of Somerset House, the
College of Physicians, and the Carlton and other Clubs.
The Infirmary in its original state was a plain, unpretentious,
but not unpleasing structure; in later years, whatever merits
its external appearances originally possessed were destroyed
by the addition of a new wing on one side and an upper
storey. It originally consisted of three floors, a flight of
stone steps leading up to the entrance hall in the centre of
the ground floor. The out-patient consulting room was on
the right of the entrance hall, and a room was specially set
apart for Dr. Farre’s use on the left. In the basement,
besides the kitchen, etc., there were the porters’and maids’
rooms, and the one bathroom and wash-house. On the
first floor, in the centre, was the operating theatre, on the
right a committee room, and on the left a room designated
as the library, but not used as such for some years. The
apothecary and the nurse-housekeeper also had their apartments
on this floor, the second floor being devoted to wards
for the patients.
The in-patients in the house in Charterhouse Square were
restricted to operation cases, and cases of purulent ophthalmia;
with increased accommodation in the new building no
such restrictions were made, and a nurse was engaged to
assist the nurse-housekeeper. To relieve the apothecary of
54some of his duties, a professional cupper was appointed to
attend three days a week, and a room was set apart for
him in the basement in which to carry on his sanguinary
proceedings.
Smirke, the architect, advised the Committee of the
Infirmary, and as afterwards turned out most wisely, to secure
the vacant land in its immediate vicinity with a view to
possible future extensions. The ground immediately behind
the Infirmary, having a frontage of 36 feet to the north and
a depth of 69 feet, had already been disposed of by the City
to a Mr. Turner, who consented to part with his purchase
for £15 per annum, or at twenty years’ purchase, £300, for
which latter it was ultimately secured.
When the building of the new Infirmary was completed,
work commenced there without any ceremonial opening
procedure. The first committee meeting held in it was on
October 2nd, 1822, and it must have been opened for the
reception of patients the same month.
On November 12th, 1822, Dr. Farre delivered to the
pupils an introductory lecture in which he announced the
arrangement of the following courses of instruction:
Lectures on Morbid Anatomy illustrative of the Practice
of Physic in general, as well as Ophthalmic Medicine in particular.
To be given occasionally and separately announced.
By Dr. J. R. Farre, Physician to the Infirmary.
Lectures of the Anatomy, Physiology, and Diseases of the
Eye. First Course on Tuesdays, Thursdays, and Saturdays
at half-past 5 o’clock. Second and subsequent courses on
Tuesdays and Saturdays at the same hour.
By Mr. William Lawrence, F.R.S., Senior Surgeon to the
Infirmary.
Clinical Lectures, on select cases of Ophthalmic Diseases
occurring in the In- or Out-Patients of the Infirmary. To be
given on days and at hours adapted to the convenience of the
pupils.
By Mr. F. Tyrrell, Junior Surgeon of the Infirmary.
55
Lectures in Optics. To be given on Thursdays at 7
o’clock in the evening.
By the Rev. T. Gill, M.A., Hon. Chaplain to the Infirmary.
Dr. Farre concluded his announcement of these lectures
with the following remarks:
“There remains one subject of great interest—The
Chemistry of Light—to which I have invited the attention
of Mr. Battley, not because he was the oldest and most faithful
friend of Mr. Saunders, but because he has actually worked
for a long time at that part of the subject which respects the
vegetable kingdom, and his labour has deservedly attracted
the attention of the College of Physicians. I think that the
profession is much obliged to him, and I shall do everything
in my power to promote his very interesting enquiries
respecting the composition and decomposition of those more
important vegetable substances which form a part of the
Materia Medica. His success in the decomposition of
opium, and in the discovering the Liquor Opii Sedativus, one
of the most valuable preparations of opium, whether externally
applied for the mitigation of extreme suffering, as in
the cancerous fungi of the eye and other parts of the body,
or internally administered for the cure of various irritative
diseases, and his beautiful preservation of the natural green
pigment and medical virtues of other preparations of the
narcotic tribe, as Digitalis Conium, and the like, induced me,
in July last, to invite him to communicate his thoughts on
those subjects to the class of the Infirmary, and, in a letter
received only this day, he has led me to hope that he will
indulge my wishes in the spring of the ensuing year.”
To what extent this ambitious programme of instructions
was carried out is uncertain. Of Dr. Farre’s teaching but
few records remain; with regard to it, Lawrence said in the
introductory chapter of his treatise:
“Dr. Farre set the example at the Infirmary, of applying
the general principles of pathology and therapeutics to the
elucidation and treatment of ophthalmic diseases. In the
clinical illustration of cases, the exposition of curative indications
and simplicity of treatment, he could not be surpassed.
56All who have had the advantage of his instructions will
remember them with gratitude and respect, and will regret
that he has not communicated to the public, through the
Press, the interesting results of his long practice, his close
observation and mature reflection.”
The report of one of his lectures at the Infirmary in the
Lancet gives anything but a good impression of him as
a teacher; it is a long rambling discourse, professedly on the
cardiac system, with but scant reference to eye disease, and
set out with scriptural quotations and protests against
materialism. We learn, however, from it that he had previously
delivered a course of lectures on the gastric system
as applicable to ophthalmic medicine.
Lawrence’s lectures were reported as they were delivered
in the Lancet in 1825–26, and subsequently formed the basis
of his treatise. The Rev. T. Gill resigned his appointment
as Chaplain to the Infirmary in February, 1823, owing to some
disrespectful behaviour to him on the part of the housekeeper,
for which she was duly reprimanded. So he could only
have given one course of instruction on optics; there is no
record of any of his successors taking on a similar duty.
A room in the basement, which it had been suggested to
Battley might be used by him as a laboratory and museum,
was not found suitable for that purpose, and the courses of
instruction which it was suggested that he might give in
Materia Medica seem to have been left in abeyance until
the establishment of what was termed “The Saunderian
Institution.”
Besides the unoccupied land behind the Infirmary, already
referred to, there was another piece to the south of it, lying
between it and the Roman Catholic Chapel. The leasehold
of this was offered to, and secured by, Dr. Farre, who subsequently
transferred it to the Infirmary. Part of the
agreement permitted the previous owner of the lease to erect
a stable for his own use on about two-thirds of the site, for
which he was to pay only a peppercorn rent. On the
57remaining one-third, Dr. Farre obtained permission to erect,
at the expense of the Saunderian Fund, which had been
established by him, a building to be called “The Saunderian
Institution.” The purpose of this Institution was the
cultivation of minute anatomy, especially of the eye, and a
general analysis of the Materia Medica to increase the
remedial agents of the Hospital, as well as benefit the profession.
The management of the Institution was to remain
entirely in the hands of Dr. Farre during his life.
“The Saunderian Fund” was one specially established for
the erection of a monument to John Cunningham Saunders;
to it Dr. Farre himself contributed £120, and to it also were
added the proceeds of the sale of the second edition of
Saunders’ book edited by Dr. Farre. Out of the fund a
bust of the late J. C. Saunders was constructed, which now
stands in the entrance hall of the present Hospital; the
remainder of it seems to have been devoted to this Institution.
In the year 1827, the Laboratory of the Institution was
opened by Mr. Battley for the analysis of the vegetable substances
of the Materia Medica, with a view to the improvement
of Pharmacy, by showing wherein the efficient powers
of these substances reside and by what means the most useful
preparations of them may be obtained. It appears that he
held large classes of students there, more than 2,000 from
various Medical Schools, British and foreign, having attended
for instruction.
Dr. Farre, in an Introductory Lecture entitled “Apology
for British Anatomy,” at the opening of the pathological
department of the Institute, or Academy, as he sometimes
described it, pointed out that the objects which it had in
view were: the study of the anatomy of structure; the performance
of post-mortem examinations; the study of minute
morbid anatomy; the publication of a journal; the publication
of separate essays; the cultivation of the Fine Arts of
drawing and modelling as connected with minute practical
and morbid anatomy.
58
John Dalrymple, who afterwards became a surgeon to
the Ophthalmic Infirmary, was appointed demonstrator and
secretary to the Academy.
In connection with the announcement of Lawrence’s
resignation of his post of surgeon to the Ophthalmic Infirmary
in 1826, there commenced a series of editorial articles in the
Lancet, attacking members of the Committee of Management
and imputing to them the most base and degrading motives.
The Lancet had been founded in 1823 by Thomas Wakley,
and at first, as his biographer says, “Some men read it,
some men laughed at it, and some men wondered at it, but
nobody much marked it, for its views were not sufficiently
condensed and its objects not definitely defined.”
In 1825 Tyrrell summoned Wakley for libel, claiming
£2,000 damages, in that the Lancet had accused Tyrrell of
plagiarism in connection with his publication of Astley
Cooper’s Surgical Lectures. Though the jury gave their
verdict in Tyrrell’s favour, they only assessed his damages
at £50.
Gradually after this trial the policy of the Lancet became
directed to three main objects:
(1) The maintenance of a right to publish, for the benefit
of the profession at large, the sayings and doings of members
of the Hospital Staff’s, with or without their permission.
(2) A fight against nepotism in the matter of staff appointments
at the Hospitals.
(3) An exposure of, what Wakley delighted in calling,
a “Hole in the Corner Policy” by members of Hospital
Staffs—i.e., the employment of secretive methods in their
practice.
In the affairs of the Ophthalmic Infirmary Wakley found
a suitable field for attack in these three directions, and,
though his objects may have been excellent, his mode of
conducting his campaign was inconsiderately bitter and
personal.
For the unauthorised publication in his Journal of the notes
59of cases at St. Thomas’s Hospital, Wakley had been expelled
from that Institution, where he had studied as a student,
the letter of expulsion being signed by the three surgeons,
Travers, Tyrrell, and Green.
Lawrence, who was at that time a prominent medical
reformer, and for whom Wakley evidently had a great admiration,
welcomed the publication of his lectures, delivered at
the Ophthalmic Infirmary, in the Lancet.
Tyrrell, who had been prominent in the fight against
Wakley at St. Thomas’s and who had also taken legal proceedings
against him, resented having his demonstrations at the
Ophthalmic Infirmary reported in the Journal. On this
matter there may very likely have been some disagreement
between the two surgeons of the Infirmary. There is no note
in the minute book of the Committee of any discussion on
the matter having taken place, or of any bye-law being
passed to the effect that “no pupil should be allowed in
future to take notes of cases.” Wakley, therefore, seems to
have been wrong in attributing Lawrence’s resignation of his
post on the staff of the Infirmary to his disgust with the
Committee for having passed such a bye-law. When the
Lancet’s first attacks on Dr. Farre and Mr. Battley were
brought to the notice of the Committee, Lawrence protested
emphatically that neither directly nor indirectly had he been
in any way concerned in them. The real reason of his
resignation probably was that he had become connected with
the newly constituted Aldersgate Street School of Medicine,
where he delivered a course of lectures on Surgery.
As has been mentioned, the idea of establishing a special
institution for treating diseases of the eye was originally
suggested to Saunders by Sir Astley Cooper, who always
took a fatherly interest in it. It was, therefore, inevitable
that, to commence with, it should be mainly staffed by his
disciples and followers. Saunders had been his house
pupil and demonstrator; Travers and Tyrrell were both his
articled pupils, the latter having also married his niece.
60Farre and Battley had both studied under him. In making
his charge of nepotism, Wakley complained chiefly of the
rule which made it obligatory that a candidate for the post
of surgeon should have served an apprenticeship at one of
the Hospitals of the Metropolis. He pointed out that for
these apprenticeships to the London Hospital surgeons
a premium of as much as £1,000 was sometimes demanded
and received, and that those for whom these large sums were
paid thereby obtained an unfair advantage when competing for
staff appointments likely to lead to renown and emoluments.
He also commented on a rumour that a post of assistant-physician
to the Infirmary was about to be created, to which
Dr. Frederick Farre, Dr. J. R. Farre’s son, was to be
appointed. This, as we shall see, did ultimately take place,
but not until ten years later and after the post had been duly
advertised, Dr. Frederick Farre being the only applicant.
The Infirmary’s announcement of Saunders’ operation
for cataract in infancy, before he had made known to the
profession his method of procedure, afforded Wakley an
excellent illustration of secret surgery, or “Hole in the
Corner methods” as he termed them. He eagerly made the
most of it, raking up what he considered the misdeeds of
Saunders, who had been dead seventeen years, and whom he
had never known personally. He reprinted much of Gibson’s
article on operations for congenital cataract from the Edinburgh
Medical and Surgical Journal, to show that the publication
of his procedure actually preceded Farre’s publication
of Saunders’ posthumous work by two months. He even
accused Dr. Farre of wilful delay in the matter, a delay which
was entirely due to the difficulties which arose in connection
with the copyright.
The Committee of the Infirmary took legal advice in
connection with these defamatory articles, but contented
itself with the insertion of the following letter in The Times
and other leading papers:
61
“London Ophthalmic Infirmary, Moorfields.
“At a meeting of the Committee, 6th November, 1826,
Ralph Price, Esq., in the Chair, five numbers of a weekly
publication, called the Lancet, dated the 7th, 14th, 21st and
28th October last, and 4th instant, and The Times newspaper
of the 28th October, were laid before the Meeting; the
former containing false statements and offensive reflections
upon the Members of this Committee in their official capacities,
but in a particular manner calculated to insult the
memory of the late Mr. Saunders, and wound the feelings
of Dr. Farre and Mr. Battley; and the latter echoing similar
calumnies in the form of a letter, directed ‘to the Editor
of The Times’ and signed ‘A Governor’; when it was resolved:
That the freedom of the Press has been violated, by
becoming, in the instances referred to, an instrument of
gross malignity and abuse, and of the foulest injustice towards
two of the earliest and most tried supporters of the Charity;
that this Meeting experiences the greatest satisfaction in
again bearing testimony to the high value of Dr. Farre’s
and Mr. Battley’s undeviating and disinterested exertions
during a period of twenty-two years, which, in conjunction
with their liberal pecuniary subscriptions, have largely
contributed to the rise and establishment of this Institution.
That, this Resolution, signed by the Chairman, be
inserted in four of the Morning and two of the Evening
Papers.
“Ralph Price, Chairman.”
On the retirement of Lawrence from the post of surgeon
to the Infirmary, John Scott, who had served his apprenticeship
at the London Hospital with Sir William Blizard, was
appointed as Tyrrell’s colleague.
Lawrence, as has been shown in the previous chapter, was
what may be described as “a whole hogger,” so far as
withdrawal of blood was concerned for the relief of inflammation
in the eye. Tyrrell, though he employed it in many
cases, was evidently doubtful as to its general utility; thus
he writes in his textbook:
“It is a great mistake to suppose that it is necessary to
take away large quantities of blood; or to bleed to such an
62extent as to occasion faintness, in order to check severe local
disease: I am confident that more harm than good results
from such practice.”
He advocated the importance of promoting and maintaining
power in the circulation, the principal means on
which he relied being “diet, stimuli, and tonics, which
are materially aided by quietude, proper clothing, and pure
air.”
In the preparation for extraction of cataract, to prevent
subsequent inflammation, especially in the robust and
plethoric, Lawrence practised depletion, taking blood freely
and repeatedly by venesection before operation. Gradually
this preliminary measure seems to have been less and less
resorted to, and, in a small monograph on Cataract and its
Treatment, published by Scott in 1843, he writes:
“Of the last fifty cases of extraction, taken in succession,
which I have performed at the Ophthalmic Hospital, where
an accurate record of the treatment is kept, I have not had
occasion to draw blood from the arm in a single instance,
either before or after the operation.”
PLATE VII.
FREDERICK TYRRELL.
An anonymous writer has recorded his personal recollections
of Tyrrell thus:
“His appearance was prepossessing, his manner to his
patients kind and reassuring, and his calmness was conspicuous
in circumstances of difficulty. It is a singular
fact that, when first attached to Moorfields, his ill success
as an operator was so great that he was suspended from
performing the major operations for a year; yet by steady
perseverance he acquired a dexterity with either hand that
could not be surpassed. In extraction of cataract his neatness
was remarkable, and we well remember an instance of his
coolness. The point of the section knife broke off, and
dropped into the anterior chamber. Mr. Tyrrell withdrew
the knife, and without the least expression of impatience,
asked for the blunt-pointed knife, with which he enlarged
the section. He then removed the bit of steel and proceeded
to extract the lens with such perfect sang froid that no one
who had not seen the breaking of the knife would have
known that anything untoward had occurred.
“Mr. Tyrrell’s great success depended fully as much on
his judicious after-treatment as on his manual dexterity;
and his secret lay in not exhausting the systems of his patients
unnecessarily, but keeping the balance of power precisely
at healing point.
“On a hot day in May, 1843, whilst an active competition
for a house was going on at the Auction Mart, an alarm was
raised that a gentleman had fainted. He was carried out.
Alas! it was Frederick Tyrrell, who had attended the sale
for the purpose of purchasing the very lot then under competition,
which, indeed, was the house he occupied. His
heart was diseased and thus he died!”
In 1840 he published a book in two volumes entitled
A Practical Work on the Diseases of the Eye and their Treatment,
Medically, Topically, and by Operation. It was dedicated
to his ophthalmic pupils, and contained the outcome
of the extensive experience which he had gained at the
Infirmary. His memory has, however, become enshrined
in the annals of ophthalmology, not so much by his writings,
as by a blunt hook which he introduced for the operation
of making an artificial pupil, which is still known as
“Tyrrell’s hook,” and without which no ophthalmic armamentarium
is complete.
It is interesting here to note how far more frequent
operations to produce an artificial pupil were one hundred
years ago than they are now. In all the early treatises on
eye disease much space was devoted to the discussion of
the various methods of producing such artificial openings
for the restoration of sight. The only inference is that
occlusion of the natural pupil by inflammatory membranes
was then of more frequent occurrence, and that the improved
methods of treating inflammatory eye affections, and the
more successful operative procedures for cataract, have
reduced the number of such occlusions.
In 1828 a body of ladies interested in the Charity carried
64out a most successful sale of useful and ornamental work
on its behalf. The President of the Infirmary, Mr. William
Mellish, obtained for the sale the patronage of the Lord and
Lady Mayoress, and permission to hold it in the Egyptian
Hall at the Mansion House. The sale commenced on
April 30th, and lasted three days; stalls were presided over
by thirteen ladies, and the sum of £2,309 9s. 6d. was realised.
On the announcement of this result at a General Meeting
of Governors a long and flowery resolution of thanks was
passed to all concerned, of which the opening sentence will
suffice as an example of the rest:
“That this unprecedented success of the plan conceived
with so much benevolence and executed with so much zeal
and ability by the ladies who have honoured the Institution
with their patronage on this occasion, whilst it reflects the
highest honour on the ingenuity, industry and charity,
which combined to produce so beneficial a result, is eminently
conducive to the best interests of the Infirmary and
highly gratifying to its Governors and friends.”
In 1830 Tyrrell, who had been carrying on the duties of
surgeon to the Institution for twelve years, became desirous
of receiving some aid, and applied to the Committee for the
appointment of an assistant-surgeon; this was agreed to,
and after the post had been advertised two applicants came
forward, Gilbert Mackmurdo and John Dalrymple. In the
ballot which ensued 591 Governors voted, Mackmurdo, who
had served his apprenticeship under Travers at St. Thomas’s
Hospital, obtaining a majority of 143.
Two years later it was found desirable to open the Infirmary
for out-patients on four days a week instead of three,
as had up to then been the custom, and also to make the
hours of attendance from 8 a.m. until 10 a.m. instead of
from 12 noon to 2 p.m. A second assistant-surgeon was
then appointed to act with John Scott, and John Dalrymple,
who was the only applicant, was elected.
John Scott, shortly after his appointment as surgeon to
65the Infirmary, was appointed assistant-surgeon to the
London Hospital, becoming full surgeon there in 1831.
He continued his work at the Ophthalmic Infirmary until
shortly before his death, which occurred after a prolonged
illness in 1846.
PLATE VIII.
JOHN SCOTT.
From an engraving, after a picture by H. Howard, R.A.
His name is best remembered in General Surgery in connection with
his treatment of joints and chronic ulcers of the leg. “Scott’s
dressing” and “Scott’s ointment” are still well known, the latter being
a camphorated mercurial ointment. He was the first surgeon in England
to remove the upper jaw, and was renowned for his skill in bandaging.
His only published contribution to ophthalmology was a small monograph
on _Cataract and its Treatment_, in which he described a new method of
making the section of the cornea in the operation of extraction. It
had previously been the custom to use a wedge-shaped knife for this
purpose, which was made to cut by thrusting it through the anterior
chamber of the eye; the force necessary to do so tended to rotate the
eyeball in an objectionable manner. Scott devised a knife, shaped like
a sickle, with which he was able to transfix the cornea and then cut
upwards. Though his knife has fallen completely out of use, the general
principle of first transfixing and then cutting out is now almost
universally employed. The writer of his obituary notice, his junior
colleague at the London Hospital, Walter Rivington, describes him as
“an honest but very irritable man,” and one who had no sympathy with
humanity.
Another writer who knew him says:
“A colleague of Frederick Tyrrell’s at Moorfields was
John Scott, who presented as great a contrast to the former
as could well be imagined. Impatient and irritable in
manner, he could not bear anything to go wrong; no man
lost vitreous humour more frequently during extraction, at
which he was invariably annoyed, ascribing it, however, to
fluidity of that body.”
66
A great loss to the Infirmary in 1835 was occasioned by
the death of its secretary, Matthew Heathfield, who had
served it in that capacity with marked assiduity and enthusiasm
for fifteen years. His successor only held the
office for a few months before he was obliged to give it up
on account of ill-health. In April, 1835, Francis William
Bircham was appointed secretary at a salary of £52 10s.
annually. It is noteworthy that the firm of solicitors to
which he belonged, Messrs. Bircham, Dalrymple and Drake,
now Messrs. Bircham and Co., of 46, Parliament Street,
S.W.1, still act as honorary solicitors to the Hospital.
67
CHAPTER V
THE ROYAL LONDON OPHTHALMIC HOSPITAL
His Royal Highness the Duke of York, the Infirmary’s first
Patron, died in 1827.
At the three days’ sale at the Mansion House in 1828
the Duchess of Kent was one of the Lady Patronesses. In
1836 the Rev. Dr. Blomberg, a member of the General
Committee of the Infirmary, stated that he had reasons to
hope that an application to their Royal Highnesses the
Duchess of Kent and the Princess Victoria to become
Patronesses of the Institution would be likely to meet with
success. A letter was then drawn up, addressed to the
Rev. Dr. Blomberg, and signed by the President, with a
statement of the following claims by the Institution to so
high a distinction: That the grand total of patients admitted
since its establishment to the end of 1835 (a period of about
thirty years) was 116,890, during which time 1,070 cases of
cataract or closed pupil (including 136 born blind) had had
their sight restored. That the annual number of patients
admitted of late years had varied from 5,000 to 5,500. That
74 capital operations were performed in 1834, 69 of which
were successful, and of 78 performed in 1835 four only
failed to produce the desired effect. That no less than
1,320 physicians and surgeons had been pupils at the
Infirmary, and were now dispensing its benefits in various
parts of the globe. That it was the parent institution of
the numerous hospitals since established throughout the
kingdom for the same benevolent purpose.
It was requested that the Rev. Dr. Blomberg would
bring these facts before the notice of the Duchess of Kent
and her illustrious daughter, the Heiress-Presumptive to
68the Throne, requesting their gracious permission to place
the Institution under their august patronage.
In response to this petition the following letters were
received:
“Kensington Palace,
“12th March, 1836.
“My dear Sir,
“By the accompanying letter which you will be so
good as to forward you will see that the Duchess of Kent
has lent her aid and that of the Princess Victoria to the
excellent charity whose cause was so ably advocated in
Mr. Mellish’s letter.
“Her Royal Highness is very happy to find an occasion
to meet a wish of yours.
“Believe me always, my dear Sir,
“Yours very faithfully,
“John Conroy.
“The Rev. Dr. Blomberg.”
“Kensington Palace,
“12th March, 1836.
“Sir,
“I have the honour to lay before the Duchess of
Kent your letter of yesterday’s date, and Her Royal Highness
begs you will assure the Committee of the London Ophthalmic
Infirmary, Moorfields, that it will be very gratifying to
her to allow her name and that of Her Royal Highness the
Princess Victoria to be placed as Patronesses of so benevolent
an Institution.
“I have the honour to be, Sir,
“Your most obedient servant,
“John Conroy.
“Wm. Mellish, Esq.,
“112, Bishopsgate Street Without.”
As the outcome of the Royal Patronage, it was agreed at
a General Meeting of Governors, on April 20th, 1836, that
the name of the Institution should be changed to “The
Royal London Ophthalmic Hospital, Moorfields.”
In 1837, on Queen Victoria’s accession to the Throne, the
Chairman of the Committee of the Hospital applied to Lord
John Russell, the Secretary of State for the Home Department,
69to ascertain Her Majesty’s pleasure as to continuing
Patroness of the Hospital, and received from him the following
reply:
“Whitehall,
“August 29th, 1837.
Sir,
“I have the honour to lay before the Queen the
petition of the Committee of Management of the Royal
Ophthalmic Hospital.
“And I have the satisfaction to inform you that Her
Majesty has been graciously pleased to be the Patroness of
that Hospital.
“I have the honour to be, Sir,
“Your obedient servant,
“J. Russell.
The Rev. J. Russell, D.D., etc.,
“Rectory House,
“Devonshire Square.”
The Patronage of the Queen, thus commenced, continued
throughout the whole of her long reign.
In 1838 William Mellish, who had been President of the
Hospital for twenty years, died, and the Committee placed
on record their gratitude and respect for the uninterrupted
paternal care and attention he had shown to the interests of
the Institution during his time of office. He was what may
be described as a real live President, having been always
ready to take the Chair at the annual meetings of Governors
and at the anniversary dinners. He was succeeded in the
office of President by Earl Fitzwilliam, who resided mainly
in the country, and but seldom visited the Hospital, so that
the control of its affairs fell largely into the hands of the
Chairman of the General Committee, who was at that time
the Rev. J. Russell, D.D.
It was obvious at the foundation of a special institution
devoted to eye diseases that the treatment would be mainly
surgical, but the importance of the medical side of ophthalmology
was recognised by the appointment of a physician.
With the expansion of the work of the Institution during
70the first thirty years of its existence the number of surgeons
on the staff had to be increased from one to four. During
all that time Dr. J. R. Farre acted alone as consulting
physician, having referred to him for his advice and aid
cases requiring medical treatment. In 1836, when he had
reached the age of sixty-one, a special Committee, of which
he was not a member, decided that it was desirable to
appoint an assistant-physician; the post was advertised in
the daily journals, and Dr. Frederick John Farre, assistant-physician
at St. Bartholomew’s Hospital, son of Dr. J.
R. Farre, was appointed, he being the only candidate. It
was then arranged that the Hospital should be opened for
out-patients, to be seen by the assistant-physician, on
Wednesday mornings at eight o’clock, and that notices to
that effect should be advertised.
In turning over the leaves of the minute books recording
the doings of the various Committees, it is remarkable to
find how much time and attention Dr. J. R. Farre devoted
to the management and administration of the Infirmary
during its first thirty years. Travers aptly described him
as “the foster-father of the London Ophthalmic Infirmary.”
He has also aptly been described as “the father of Ophthalmic
Medicine.” He was most regular in his attendance,
and when a petition, a report, or any letter of importance
had to be composed, his assistance was always sought for.
Though his style now seems florid and verbose, it met the
requirements of the time, and generally effected the purpose
for which it was intended.
With remarkable foresight he endeavoured to establish,
with varying degrees of success, many of the developments
which have in later years become some of the most prominent
features of the Hospital’s work. Thus the Saunderian
Institute, one of the purposes of which was the investigation
of the minute anatomy of the eye, foreshadowed the Pathological
Laboratory and Museum which were established
later.
71
In 1828 Dr. Farre started the publication of a Journal, of
which, however, only one number appeared, but in a way
it may be considered the precursor of the Royal London
Ophthalmic Hospital Reports, which commenced in 1857.
Farre’s Journal contained a most remarkable mixture of
subjects, and serves to show him as a man of wide and varied
interests.
It was entitled, Journal of Morbid Anatomy, Ophthalmic
Medicine and Pharmaceutical Analysis, with Medico-Botanical
Transactions communicated by the Medico-Botanical
Society.
It contained reports from the Calcutta and Madras Eye
Infirmaries; notes on cases and pathological examinations
of rupture of the heart, angina pectoris, aneurysm, etc., by
various observers; a paper by Richard Battley on experiments
on Chinchona; the Transactions of the Medico-Botanical
Society; observations on the climate of the Azores,
of Hastings, and Penzance; a paper by John Dalrymple,
‘On the Muscularity of the Iris,” which, Dr. Farre said,
in some introductory remarks, met the principal object for
which his Academy was instituted—
“the inquiry having been physiologically conducted and
pathologically directed, assumed the very spirit which he
most desired to encourage amongst the many British candidates
for anatomical character.”
It was announced that:
“Parts of the Journal will be published at fixed periods
of Midsummer and Christmas, and also intervening parts,
as opportunity may admit, for the completion of each
volume, if the Editor’s health should, by God’s permission,
enable him to separate from the hours of his repose a portion
of time adequate to the service announced in this notice to
contributors.”
These good intentions were, however, not realised, no
further number of the Journal being issued.
72
The Library, for which a special room had been set apart
in the new building, was started by Dr. J. R. Farre’s presentation
of eighteen volumes of the Philosophical Transactions
and various works on optics. These formed a
nucleus around which has been built up one of the most
extensive and valuable collections of books dealing with
ophthalmology, a collection which has proved of inestimable
service for purposes of reference and research to several
successive generations of workers at the Hospital.
In 1837 Dr. J. R. Farre advised the Committee that it
was desirable that a Pharmacopœia should be constructed
for the use of the Hospital; in its compilation Dr. Frederick
Farre, who was lecturer on Botany at St. Bartholomew’s
Hospital, and later lecturer there on Materia Medica,
rendered valuable assistance.
Dr. Farre, senior, seems to have been a man who inspired
the warmest regard and affection in all who became associated
with him; in 1838 a full-length portrait of him was
presented to the Hospital by some of his friends with the
accompanying letter:
“London, 18th August, 1838.
“34, Montagu Square.
“Gentlemen,
“I have the honour on behalf of my brothers and
myself to present to the Royal London Ophthalmic Hospital,
of which he has so long been a liberal patron and zealous
benefactor, a portrait of our esteemed friend Dr. John
Richard Farre, painted by T. Phillips, R.A.
“To those who appreciate the character and services of
the worthy original we feel assured that we need only offer
in order to obtain for it a welcome reception.
“I am, Gentlemen,
“Your most obedient servant,
“J. Roach Bovell.
“The President, Vice-Presidents,
Treasurer and Committee of the R.L.O.H.”
On receiving it the Committee passed the following
resolution:
73
“That recognising in Dr. Farre not only one of the
Founders of the Institution but a munificent contributor to
its funds, and the able physician by whom the science
communicated and dispensed within its walls has been
effectively upheld and enlarged, the Committee accepts the
testimonial of private esteem and affection with peculiar
pleasure as the means of publicly manifesting, and of
transmitting to posterity, the high claims of public
respect and gratitude for that highly distinguished public
benefactor.”
PLATE IX.
DR. JOHN RICHARD FARRE.
From an engraving by Frank Bromley, after a picture by Thomas Phillips, R.A.
Thomas Phillips, R.A., painted the portraits of most of
the celebrated literary and scientific men of his time; that
of Dr. Farre must certainly have been one of his largest
works of this description. It now occupies a dominating
position in the Board Room of the Hospital, and shows Dr.
Farre clothed in stockings and knee-breeches, with a buff-coloured
waistcoat, stock, and blue coat with brass buttons.
He is represented seated at a table with the drawing of a
malformed heart in one hand, and a portfolio beside him,
evidently containing his valuable collection of drawings
of pathological specimens, which was afterwards presented
to St. Bartholomew’s Hospital Museum.
Dr. Farre was a religiously devout man, and most appropriately
there is conspicuously shown amongst the books on
his table a copy of the Holy Bible. He continued to serve
the Hospital in the capacity of consulting physician until
1843, but lived on until 1862, when he died in his eighty-eighth
year, having outlived all those who had been associated
with him in the Hospital’s foundation.
His son, Dr. Frederick J. Farre, was educated at Charterhouse
School, and was the captain of it during Thackeray’s
first year there. Thackeray afterwards introduced him in
The Adventures of Philip as Sampson Major, the cock of the
whole school.
Mackmurdo and Dalrymple’s duties as assistant-surgeons
consisted mainly in the treatment of the out-patients. After
having been so employed for several years, they not unnaturally
74aspired to gaining skill and experience in the
performance of the major operations of ophthalmic surgery
on the in-patients. With such aspirations several members
of the Committee of Management were in sympathy, and
much discussion took place as to some alteration in the rules
which would permit of them acting as full surgeons. Tyrrell
and Scott, however, were opposed to any proposal which
was likely to lead to a curtailment of their privileges as senior
officers.
The following return was drawn up and laid before the
Committee to show how the work of the Institution was
distributed amongst the different members of the medical
staff in the year 1842.
Out-patients:
Dr. F. Farre
607
(one day a week)
Mr. Tyrrell
1,090
Mr. Scott
1,037
(two days a week)
Mr. Mackmurdo
1,274
Mr. Dalrymple
1,714
Operations performed:
Extraction of Cataract.
Needling of Cataract.
Artificial Pupil.
Mr. Tyrrell
42
20
7
Mr. Scott
29
9
7
Mr. Mackmurdo
0
4
0
Mr. Dalrymple
0
5
0
The matter was brought to a head by the death of Tyrrell
in June, 1843. By that time Mackmurdo had served the
Hospital as assistant-surgeon for a period of thirteen years,
and Dalrymple for eleven years.
After due notice had been given it was then agreed, at
a special General Meeting of the Governors, that the laws
regarding the appointment of the medical officers should
be suspended, and that Mr. Mackmurdo and Mr. Dalrymple
should forthwith be appointed surgeons to the Hospital;
also that two new assistant-surgeons should be elected.
75Mr. John Scott strongly protested against such an increase
in the surgical staff, pointing out, quite correctly, that such
an increase was out of proportion to the increase in the
number of patients.
Shortly afterwards Dr. Frederick J. Farre was likewise
promoted from assistant-physician to physician to the
Hospital, his father, Dr. J. R. Farre, being described as
consulting physician, the capacity in which he claimed to
have always served as a member of the staff.
The candidates for the two posts of assistant-surgeon
were:
Mr. James Dixon, who had been articled as apprentice
to Tyrrell, and who was demonstrator of anatomy at St.
Thomas’s Hospital.
Mr. George Critchett, who had been articled to Scott,
and who was demonstrator of anatomy at the London
Hospital.
Mr. William Bowman, who had served his apprenticeship
at the Birmingham Hospital, and who was demonstrator of
anatomy at King’s College Hospital.
The latter withdrew his candidature in favour of the two
former when he found that they had been already working
at the Hospital, but at the same time intimated his intention
of applying again when a further vacancy arose. This
occurred in 1846, due to Scott’s retirement from ill-health,
and Bowman was then elected assistant-surgeon
unopposed.
Dr. J. R. Farre was, as already shown, a man of ideas as
well as of affairs; the time, however, occupied by the latter
precluded his putting many of the former into practice.
He was, therefore, exceedingly fortunate in finding in John
Dalrymple a most energetic and capable disciple.
John Dalrymple, who was related to the Stair family, was
born in 1803. His father, William Dalrymple, who had
studied under Astley Cooper, was surgeon to the Norfolk
and Norwich Hospital. He was a liberal-minded man as
76well as a skilful surgeon, and attracted considerable attention
in 1813 by repeating successfully Travers’ operation of
tying the common carotid artery in a case of “aneurism by
anastomosis” of the orbit. He had also devoted some
attention to ocular pathology, and had made a valuable
collection of anatomical and pathological preparations,
which he presented to the Norfolk and Norwich Hospital.
John seems to have served his apprenticeship under his
father, and to have acquired from him a liking for both
pathology and ophthalmology. He studied for a time at
Edinburgh University, and came to London, where he
qualified as M.R.C.S. in 1827.
His association with Dr. Farre and with the Moorfields
Hospital then commenced, with his appointment already
mentioned, as demonstrator and secretary to the newly
opened Saunderian Institution, where he carried out anatomical
and pathological investigations. In 1834, as the
outcome of his work at the Institute, he published a treatise
on the Anatomy of the Human Eye, which he dedicated
to Dr. J. R. Farre, Frederick Tyrrell, and John Scott, his
colleagues at the Infirmary, to which he had been appointed
assistant-surgeon the previous year. This book, besides
containing a description of his own dissections, gives an
excellent review of the work of previous investigators,
and is illustrated by five engraved plates from his own
anatomical drawings. Dalrymple’s investigations were not
restricted to ophthalmology; between the years 1840 and
1849 he contributed several papers to the Medico-Chirurgical
Society’s Transactions relating to general pathology,
and also wrote articles dealing with Natural History.
Tyrrell’s unexpected decease, and later Scott’s retirement,
left Dalrymple in a leading position in ophthalmology,
and his reputation and practice rapidly increased. In 1847
he found the state of his health to be such as to render it
impossible for him to keep up his attendance at the Hospital
during the winter months. As he was the only surgeon in
77attendance on Wednesdays and Saturdays, whereas on the
other days of the week both a surgeon and an assistant-surgeon
were on duty, the Governors agreed to appoint a
third assistant-surgeon, and thereby relieve Dalrymple of
his duties during the winter. Alfred Poland, who had
served his apprenticeship under Aston Key at Guy’s
Hospital, and who was a demonstrator of anatomy there,
was elected to the post.
Dalrymple’s health did not tend to improve, and in 1849
he felt compelled to resign his appointment on the active
staff, and was appointed consulting surgeon. On his
retirement no fresh appointment was made to the staff,
Critchett being promoted to the post of surgeon in his
place. In 1850 Dalrymple was elected a Fellow of the Royal
Society.
For a number of years John Scott and Dalrymple had
been collecting water-coloured drawings of diseases of the
eye, made from patients under their care at the Hospital
by the best artists. Scott, at his death, bequeathed to
Dalrymple the drawings he had collected, and these, added
to Dalrymple’s own, amounted to several hundred. It was
from a selection of them that in 1852 Dalrymple was able
to produce his great Atlas of Pathology of the Eye. The
publication of the volume was entrusted to Mr. Churchill,
and every advantage that fine paper and artistic skill could
afford was supplied. The Atlas consisted of thirty-six
plates, some containing six figures, and others full-page
illustrations, with explanatory letterpress. The original
drawings were made by W. H. Kearney and Leonard, and
the drawings on stone by W. Bragg. It can safely be
asserted that no illustrations of eye diseases ever surpassed
or even equalled those in this Atlas, both as regards artistic
merits and faithfulness in the depiction of the characteristics
of the conditions they represent. The cost of the production
of the Atlas was nearly fifteen hundred pounds, and
copies of it now are exceedingly scarce. Dalrymple only
78lived a few weeks after its completion, dying in the zenith
of his fame and the full tide of prosperity. The whole
collection of drawings, from which those reproduced in the
Atlas were selected, was bequeathed by him in his will to
the library of the Royal London Ophthalmic Hospital,
where they are still preserved.
It is perhaps remarkable that, though Dalrymple did so
much for ophthalmology by his anatomical investigations
and the production of this Atlas, his name is best known
by ophthalmic surgeons at the present day in connection
with the symptom of retraction of the upper lids in “Graves’
disease” or “exophthalmic goitre,” which produces the
peculiar staring look that forms one of its most characteristic
features. This symptom is spoken of in textbooks as
“Dalrymple’s sign,” but to his description of it Dalrymple
himself apparently attached but little importance.
PLATE X.
JOHN DALRYMPLE, F.R.S.
John Dalrymple was one of a family of nine; two of his
brothers became medical men and practised in Norwich;
another, named Robert Francis, was a solicitor in the firm
of Bircham, Dalrymple, and Draise, and on the retirement
of Francis Bircham, his partner, from the post of secretary
to the Hospital in 1844, R. F. Dalrymple was appointed in
his place. He discharged the duties of the office most
efficiently for two years, and was then succeeded by Mr.
F. A. Curling.
Richard Battley married one of Dalrymple’s sisters. John
Dalrymple died in May, 1852, and Battley in 1856. The
latter’s widow, after the death of her husband, presented
to the Hospital a bust of her brother, which now stands
in the hall of the present building. In the same year, 1856,
Robert Dalrymple was elected a member of the Committee
of Management of the Hospital, and presented to it an
engraving of his brother, which still hangs in the Board
Room of the Hospital, mounted in what was described at
the time as “an elegant gilt frame.” Another presentation
to the Hospital that year was a copy of Dalrymple’s Atlas
79from John Churchill, the publisher, with the following
inscription on the flyleaf:
“Presented to the Royal London Ophthalmic Hospital,
in honour of that sight-saving Institution, and as a memorial
of the highest respect and esteem for the memory of the
author, whose lamented death took place soon after the
completion of his immortal work, the subscriber having
enjoyed the friendship of the author, as well as being his
publisher.
“(Signed) John Churchill.
“6th October, 1856.”
At the Annual General Meeting of the Governors of the
Hospital, after the death of Richard Battley, the following
resolution was passed:
“That this Meeting most gratefully acknowledge the
eminent services to this Hospital of the late Mr. Richard
Battley; that to his energy and perseverance are attributed
more especially the establishment of the Hospital; that in
its origin, when checked by impediments and surrounded
by difficulties, it was fostered by his influence and exertions
and, in the arduous circumstances which ensued and continued
during many years, was succoured and sustained
by his active zeal; and that it is especially to be recorded
that he upheld the Institution by an undeviating regard to
the professional appointments by which the Hospital has
been distinguished from its foundation.
“That this memorial be engraved and placed in the
committee room of the Hospital with the portraits of his
early friends, Saunders and Farre.”
Gilbert M. Mackmurdo was Dalrymple’s senior; he remained
a member of the active staff of the Hospital until
1856, and died at an advanced age in 1869. In his obituary
notice he is said to have had a fine appearance, a fair patrimony,
and to have enjoyed great City and mercantile influence;
it was largely due to the latter that he obtained
his early appointment to the staff at Moorfields, and that of
surgeon to St. Thomas’s Hospital and to Newgate Prison.
80The last appointment gave him for many years a handsome
salary, with a commensurate retiring allowance.
Being well provided for with this world’s goods, he seems
to have contented himself with the practice of the art of
his profession without making contributions to its science.
Early in life he was elected a Fellow of the Royal Society,
but for what particular reason no record can be found.
His only contribution to ophthalmic literature seems to be
a short description of a case of recurrent haemorrhage from
the inferior palpebral artery. He is said to have been
thoroughly popular with his pupils and with his patients of
all degrees, and never, never to have made an enemy in his
life, either willingly or wilfully.
In 1849 Mrs. Dodson, who had held the post of matron
at the Hospital for a number of years, died, and a Committee
was appointed to report on the general arrangements and
accommodation of the Institution. The following extract
from it serves to show what these were, after the Hospital
had been in existence for half a century:
“The establishment consists of a Resident Apothecary,
a Matron, one Nurse, one Housemaid, and one Cook, all of
whom reside upon the premises, and a Porter or Messenger
who neither sleeps nor takes his meals in the building.
“There are 23 beds for patients in five separate wards,
and during the winter only from one to five are occupied,
whilst during the summer, or from May to October, when
the season is propitious for the various operations, the
whole of the beds are occupied.
“The Committee recommends that the new Matron to
be appointed should be discreet and mild in her manner,
whose standing and carriage is superior to a servant, of
about 40 years of age and without encumbrances, and whose
duties shall be to render assistance to and alleviate the
sufferings of the patients by a regular oversight of them.
“Her salary to be 30 guineas a year, with an allowance
of £5 for tea and sugar.”
As the fame of the Hospital extended there was a rapid
increase in the patients who came to it seeking relief. The
81annual number of new out-patients became doubled in the
course of ten years; in 1841 there were 5,643, and in 1851,
11,384.
This large increase made it necessary to provide for increased
accommodation in the out-patient department. In
a letter to the Committee, Dr. J. R. Farre drew attention
to the early age at which the death of several of the members
of the surgical staff had taken place. Saunders died at the
age of thirty-six; Tyrrell at forty-nine; Scott at forty-eight;
and Dalrymple at forty-nine. Farre suggested that this
might to some extent be due to the tainted atmosphere of
the receiving rooms for patients, and to the strain involved
in having to attend to such large numbers.
A rearrangement of the rooms of the ground floor of the
Hospital was then made to provide more space for those
waiting to be attended to; an assistant was engaged to aid
in the dispensing; and the staff was increased by the appointment
of another assistant-surgeon.
The candidates for this post were Mr. H. H. Mackmurdo
and Mr. T. N. Nunn; the former received 330 votes and
the latter 160. The former probably, like his brother
Gilbert, was able to bring considerable City and mercantile
influence to assist him; he, however, only held the post for
a year, and then resigned. Mr. J. C. Wordsworth, who
was a descendant of a collateral branch of the poet’s family,
and who was an assistant-surgeon at the London Hospital,
was appointed in his place.
82
CHAPTER VI
THE INTRODUCTION OF INHALATION ANÆSTHESIA
AND OPHTHALMIC SURGERY
Ether was first employed as an anæsthetic for surgical
operations in England on December 19th, 1846, when
Robert Liston performed an amputation of the thigh, and
the removal of a great toe-nail, on patients under its influence,
at University College Hospital, Gower Street. In
Edinburgh, Sir James Simpson first gave a description of
his use of chloroform, at the Medico-Chirurgical Society in
that city, in November, 1847.
The adoption of anæsthetics for general surgical procedures
rapidly followed, but, due to the sickness by which
they were often followed, their employment in ophthalmic
surgery was for some time delayed. Thus, Mackenzie of
Glasgow, writing in 1854, says:
“Needle operations may be performed on timid adults
under the influence of chloroform. In extraction I have not
ventured to use it, being afraid lest the vomiting which is
apt to follow might cause rupture of the internal structures
of the eye.”
In a review of Haynes Walton’s textbook on eye diseases
in 1853, an anonymous writer says:
“We agree with Mr. Walton that it is not advisable to
use chloroform in the extraction of cataract, and we would
remark that a surgeon with a sharp eye, a cool head, and
a steady hand will usually prefer to have the command of
his patient’s voluntary motions, and to avoid the danger
which may arise from his restlessness on awaking from his
drunken sleep.”
Hulke, writing of his reminiscences of Sir William
Bowman’s work, said:
83
“In London, so far as my knowledge extends, Sir William
Bowman was the first surgeon who employed chloroform
in ‘extraction.’ In his first case the administration of
chloroform was followed by vomiting after the completion
of the operation—which could not have been more perfectly
performed—and the violent straining induced choroidal
hæmorrhage with extrusion of the vitreous humour and the
retina through the corneal incision—the eye was lost. So
serious a disaster would have deterred many men from the
further trial of chloroform, but its advantages in respect of
the performance of the operation were so manifest that Sir
William Bowman persevered in its use, and in order to
inspire confidence in his patients he experimentally inhaled
it to complete anæsthesia himself. His conviction of its
extreme usefulness in extraction was soon shared by others,
and its employment quickly became general.”
The practice as regards the use of chloroform at Moorfields
Hospital during the first decade after its introduction
is summed up in the following extract on the subject from
the second edition of James Dixon’s Guide to the Practical
Study of the Diseases of the Eye:
“We may regard it under two aspects: as saving the
patient from pain, and as facilitating the manipulations of
the surgeon. Now, it is notorious that operations performed
on the globe itself cause very little pain, and last
but a very short time. Those on the lids, involving as they
do the wounding of the skin, are of course more painful;
but, in respect of the suffering they cause, none of these
are comparable to the larger operations in General Surgery,
and there are few adults who, if thoroughly informed as
to the real nature of such operations as those for cataract,
artificial pupil and strabismus or even entropion and
ectropion in their slighter forms, will not readily undergo
them without the aid of anæsthetics.
“A perfect passive condition of the eye is so desirable
in the delicate operations of cataract and artificial pupil,
that one would naturally expect to find chloroform universally
applicable in such cases; and specially indicated
in the most delicate of all—extraction. But this forms a
peculiar and exceptional case, and for the following reasons:
We have seen that—provided the operation has been properly
84performed—the successful result of an extraction chiefly
depends upon the rapidity with which the union of the
corneal wound can be effected. Now, with every precaution
it will sometimes happen that chloroform induces vomiting,
and the violent efforts which attend this might disturb the
lips of the wound, and cause the vitreous body to escape
between them, thus inducing a prolapse of the iris, with
all its accompanying irritation and retarded union. But,
without taking such an extreme case as this, we shall
find a very serious objection to the use of chloroform in
the fact, that the squeamishness and disrelish for food
which it induces may interfere with the reparative process,
by impairing the nutrition of the cornea during
the critical twenty-four hours immediately following the
operation.
“In adults who are extremely fearful and unsteady,
chloroform may be required in the operations for artificial
pupil and strabismus; it will always be indicated in cases
of extirpation of the globe, and it may greatly facilitate the
examination of eyes rendered irritable by disease or by the
presence of foreign bodies.
“In children all these manipulations will be greatly
facilitated by the use of chloroform, and some can hardly
be performed at all without its aid.”
White Cooper, who was a great friend and follower of
Dalrymple, wrote in 1853 as follows:
“In common with many others, I for some time hesitated
before using chloroform in extraction of cataract, from a
fear that the object of the operation might be defeated by
the eye receiving injury during the return of consciousness,
or by vomiting afterwards. It appeared to me, however, so
deserving of a trial that nearly two years ago I first employed
it, and since that time have availed myself of it very frequently
in operations on the eye, including 16 cases of extraction of
cataract, 9 of artificial pupil, 4 of foreign body in the eyeball,
and 2 of tumours of the globe, besides numerous needle
cases.
“The advantage obtained by the use of chloroform in
operations on the eye are a perfectly quiescent condition
of the globe or the lids, absence of congestion of the eye,
and mental tranquillity for the patient. To the operator
85the perfect repose of the eye affords a manifest advantage,
the various steps of the operation being performed with as
much facility as in a demonstration on the dead subject;
the risk of prolapse of the iris (which is usually caused by
muscular action) is greatly diminished, and the corneal flap
can be accurately adjusted.”
By improved methods of preparation of patients before
the administration of chloroform the risks of vomiting
became reduced. By a modification of the operation of
extraction so that a piece of the iris was removed, either
at the time of the extraction of the cataract or as a preliminary
procedure, the risk of its protrusion into the wound
was avoided; and by the modification of the opening made in
the eye, so that it formed a straight linear incision instead of a
flap, the risk of its gaping open subsequently was diminished.
Ultimately, up to the time of the introduction of cocaine in
1884, the employment of chloroform for extraction of
cataract became the general custom, and the performance
of the operation without its aid the exception.
The following return of the number of cases to which
chloroform was administered during the first six months
in 1868 shows how general its use in operative procedures
on the eye had then become: Cataract, 74; removal of eye,
67; iridectomy, 99; iriddesis, 11; syringe, 15; entropion
and ectropion, 36; abscission, 5; strabismus, 166; tumours
of lid and orbit, 8. Total, 481.
After the introduction of anæsthetics many new operative
procedures on the eye were invented, and those formerly
in use, like that of extraction of cataract, became modified
and improved. In all these changes and advances Critchett
and Bowman, at Moorfields Hospital, played a conspicuous
part.
Excision of the eyeball was at one time a most formidable
procedure, and was only resorted to in cases of malignant
growths. Hulke has recorded the following graphic description
of his recollections of it at the time of his pupillage:
86
“The first excision of the eyeball that I saw was to me,
a novice, so horrible and distressing a scene that the impression
it made still lingers in my recollection. No anæsthesia.
The surgeon first passed through the eyeball a
stout needle armed with stout silk, and knotting the ends,
formed a loop. Next, with this he dragged forwards the
eyeball, and then scooped it out of its socket with a double-edged
scalpel curved on the flat of the blade. This done
an assistant, who stood ready with a large brass clyster-syringe,
checked the profuse bleeding by squirting into the
orbit iced water. How different this from enucleation as
now done—methodical circular division of the conjunctiva,
severance of the muscles at their insertions into the globe,
careful section of the optic nerve with scissors!”
The suggestion that the eyeball might thus neatly and
safely be dissected out of its encircling capsule originated
with an anatomist, O’Ferrall, in Dublin in 1841, and was
first put into practice by Bonnet in France in the following
year. George Critchett independently adopted it, and
gave a description of the proceeding in 1851. After that,
excision of the eye became an increasingly frequent operation
for the relief of pain, when the sight was irretrievably
destroyed, or for the improvement of appearances where
the eye had become unsightly and disfiguring. The consequent
increased demand for artificial eyes resulted in
their improvement in construction and appearance. Their
manufacture became a highly specialised art, and a Mr.
Gray was appointed purveyor of artificial eyes to the
Hospital.
PLATE XI.
GEORGE CRITCHETT
In 1844 Lawrence wrote:
“The influence of one eye upon the other is not confined
to cases of disease. When an eye has been lost by accident,
the other often becomes diseased sooner or later, without
any imprudence or any external influence that would be
injurious under ordinary circumstances. This kind of
occurrence is so common, that it is necessary to warn those
who have lost an eye of this danger, and the necessary
precautions for avoiding it.”
87
The prophylactic treatment of removal of eyes injured
in such a way as to provoke this sympathetic disease does
not, however, seem to have been put into practice until
1854, when it was first adopted by Prichard of Bristol. So
effectual did this prophylactic measure prove that it soon
became generally adopted, and excision of the eyeball at
Moorfields Hospital, from being a rarely performed operation,
as it was in the pre-anæsthetic days, became one of
the commonest operations.
The operation for squint, before the introduction of
anæsthetics, was a very crude procedure, and was performed
often in what seems to-day a very indiscriminate manner.
The patient was seated in an armchair with a high back,
against which the head was fixed by an assistant who stood
behind it. The same, or another assistant, held the eyelids
apart. The operator, standing in front, exposed the muscle
to be dealt with by making a long incision in the membrane
overlying it. He then passed a curved grooved director
beneath it, and divided the muscle by running a sharp-pointed
bistoury, or knife, along the groove in the director,
no special attention being paid as to whether the tendon
or the muscle itself was cut across. Loss of mobility with
an unsightly prominence of the eye not infrequently resulted;
whilst the large, open wound which was left often
developed a mass of granulation tissue which considerably
delayed healing.
Through the ingenuity of George Critchett, a much
neater and simpler procedure was devised, by which many
of the disadvantages of the older method were obviated.
Only a small opening was made in the conjunctiva, the whole
proceeding for division of the tendon being carried on
beneath it, a hook was inserted under the muscle in place
of the director, and scissors were used to cut through the
tendon close to its insertion into the eyeball.
Disorders arising in connection with the drainage apparatus
for the passage of the tears from the eye to the nose
88have attracted the attention of those engaged in the healing
art since very ancient times. In 1833 Sir William Lawrence
wrote that to give a description of all the proceedings
which have been proposed for removing obstruction to the
tear duct would fill a moderate volume, but that the greater
part were obsolete. The collection of all those which have
been proposed since that date would fill a second volume.
Amongst all these different methods of treatment, that
devised by Bowman in 1851 of slitting up the openings into
the tear sac at the inner angle of the eyelids, the lacrymal
puncta and canaliculi, represented a considerable advance
on those which had been previously employed. He first
practised it in cases of overflow of tears caused by closure
or displacement of the lacrymal puncta; afterwards, in the
treatment of obstruction of the nasal duct, he passed probes
through the slit canaliculus to dilate the stricture in the duct,
and introduced through it styles to be worn for a time in
order to maintain the dilatation. The introduction of styles
worn in this way avoided the disfigurement entailed when, as
formerly, they were introduced through the skin of the nose
overlying the tear sac.
Gibson of Manchester (as mentioned in Chapter II.),
independently of Saunders, introduced in 1811 a method
of operating on cataracts in infants. He first broke up the
lens, and reduced it to a pulp, with a couching needle;
then, two or three weeks later, evacuated it through a small
incision in the cornea by the introduction of a curette.
This operation, though practised for some time in Manchester,
fell into disuse. At Moorfields, the Saunderian
tradition was still adhered to, allowing the lens matter
slowly to become dissolved in the fluids of the eye. In 1851
Bowman revived and improved upon Gibson’s operation,
and in 1864, in the Ophthalmic Hospital Reports, T.
Pridgin Teale, junr., described how, in order to aid the
removal of softened lens matter, he had employed a suction
curette. The curette was converted into a tube by having
89its groove roofed over to within a line of its extremity; it
was connected with an indiarubber tube, and the suction
was made by the mouth of the operator. The idea of
extraction by suction can, he said, “boast of considerable
antiquity, as the following quotation, kindly sent me by
Mr. Bowman, will show
“According to Avicenna a similar proceeding (viz.,
excision of cataract, by opening in the cornea and drawing
out the cataract by a needle) was practised by the Persians
in the fourth century, and Albucasis reports that the procedure
was gradually displaced by the ‘suctions-method,’ in
which the cataract was sucked out through a hollow needle.”
Bowman himself, later on, had constructed a suction
apparatus for soft cataracts, which could be manipulated
with one hand, the suction being made by the movement
upwards of a piston with the thumb.
After the introduction of anæsthetics, which allowed of
patients being kept perfectly quiet during the performance
of operations on the eye, procedures requiring great precision
and skill were introduced by both Bowman and
Critchett for the formation of artificial pupils.
Bowman, in order to produce an enlargement of the pupil
of a limited extent, in a suitable direction, whilst still keeping
it as central as possible, made use of canula-scissors. These
were scissors with delicate blades expanding from a stem
which moved up and down in a canula, the size of a cataract
needle, by means of a spring in the handle. When the
spring was pressed the scissors were closed by being drawn
partly into the canula, and when it was relaxed they opened,
being protruded by the spiral wire. One blade of the
scissors, which protruded beyond the other, was pointed with
a sharp cutting edge capable of penetrating the cornea and
allowing the whole of the closed scissors being introduced
into the anterior chamber of the eye. The other shorter
blade of the scissors was blunt-pointed. When within the
eye, the blades of the scissors were opened and made to
90cut the pupillary border of the iris, the blunt-pointed blade
being passed behind and the sharp-pointed one in front.
The calibre of the canula was so graduated as to plug the
wound through which it was introduced, and prevent the
escape of the aqueous humour.
For use in other cases he had constructed a modified form
of Tyrrell’s hook. It was of the same size, but sharp and
flattened at the point. Its stem was cylindrical so as exactly
to occupy the corneal wound and prevent the escape of the
aqueous humour. With this “needle hook,” as he termed
it, the necessity of making a preliminary incision with the
loss of the aqueous humour, before the introduction of the
hook, was avoided; the needle hook introduced itself into
the eye, the retention of the aqueous humour facilitating
the precision with which the hook could be passed round
the pupillary border.
Critchett invented an operation which he called “iriddesis,”
or the formation of artificial pupil by tying the iris.
The purpose of the procedure he described as follows:
“The formation of what is commonly called an artificial
pupil is required under various morbid or abnormal conditions
of the eye, and demands a corresponding variety in
the modes by which it is accomplished. In some cases, a
restoration of the original pupil as regards size and situation
is all that is wanted; in others, a change in the size, shape,
and situation of the natural pupil is required; or, again, it
may be necessary to form a new pupil in an abnormal
situation and in the very substance or tissue of the iris.
In each of these different cases the object is the same—viz.,
to establish a clear pupil or aperture in the iris opposite to
a transparent part of the cornea.
“It is very desirable that, in the formation of an artificial
pupil, the conditions upon which the perfection of the natural
pupil depends should be as nearly as possible preserved and
imitated, both as regards its position and defined border,
its size, mobility, and sensitiveness to light. In the methods
usually employed these conditions are frequently unattainable,
and the circular fibres of the natural pupil are either
91cut or torn through, and an opening is formed which is
very probably large and irregular in shape, fixed and insensible
to light, ill-defined and extending to the margin
of the cornea—thus admitting rays of light that are too
much refracted by the margin of the lens, and having the
effect altogether of confusion of vision.”
His operation, designed to overcome the disadvantages
above mentioned, consisted in drawing into a wound at the
margin of the cornea, with canula-forceps, a small piece of
the periphery of the iris and fixing it there by tying a loop
of silk around it. In this way an alteration of the position
of the pupil was effected without its margin being cut or
the sphincter muscle interfered with.
The operation was for some time extensively practised at
Moorfields, not only by Critchett, but also by Bowman
and Poland. In cases of conical cornea, Bowman, by performing
this operation at the outer and inner margin of
the cornea, produced a laterally elongated slit-like opening;
in order to create the same beneficial visual effect, in such
cases, as is sometimes derived by holding a slit-shaped
opening in a metal disc in close proximity to the eye.
Later on, it was found that this ingenious operation of
iriddesis was liable to be followed by inflammation in the
eye of a type which might spread to the fellow eye: it became,
therefore, entirely abandoned.
Another discovery which largely extended the range of
operative ophthalmic surgery was that glaucoma could be
relieved by the removal of a piece of the iris.
A. von Graefe first performed an operation of this description
for glaucoma in Berlin in June, 1856. His study of
the natural history of the disease, and of its ophthalmoscopical
appearances, had led him to the conclusion that
increased hardness, or tension, of the eyeball was the leading
factor in its causation, and that, if some means could be
devised of permanently lowering the tension, its cure might
be effected. Experience had shown him that after the
92removal of a piece of the iris to form an artificial pupil, in
eyes where the tension was increased, normal tension
became restored. After having performed experimental
iridectomies on animals’ eyes, he felt justified in trying the
effect of the operation on patients suffering from glaucoma,
and with the most gratifying results. Up to that time the
disease inevitably resulted in blindness, and in some of its
forms was accompanied by the most agonising pain and
distress. The discovery of a means whereby not only could
the pain be relieved, but the loss of sight also prevented,
must always be regarded as one of the greatest triumphs of
ophthalmic surgery.
The successful performance of iridectomy for glaucoma
requires a steadier hand and more skill than any other
operation on the eye. It is also necessary to have the
patient absolutely quiet. The acute pain to which the affection
gives rise renders the eye exceedingly sensitive, and
even to-day most surgeons prefer to perform it on patients
under the influence of a general anæsthetic. Indeed, the
introduction of inhalation anæsthesia may be said to have
paved the way for the operative treatment of glaucoma.
1851 was the year of the first Great Exhibition in London,
held in the Crystal Palace in Hyde Park. Visitors from all
parts of the world flocked to see it, and amongst them came
Albrecht von Graefe, then twenty-three years of age, full
of enthusiastic ardour and fresh from his studies in the
clinics of Germany, Vienna, and Paris; also Frans Cornelius
Donders, thirty-three years of age, whom his friend Moleschott
described with fervid admiration as “a swelling rose-bud,
whose calix leaves signified nothing but pure science;
the flower leaves hidden glory. In one word, he was a
man complete—perfect for his time of life.” He was at
that time Professor Extraordinary at the University of
Utrecht, and lectured on no less than four subjects—viz.,
Forensic Medicine, Anthropology, General Biology, and
Ophthalmology.
93
These two men and Sir William Bowman, destined to
revolutionise the practice of ophthalmology, met for the
first time in London in that eventful year, and remained on
terms of the most intimate friendship for the rest of their
lives. Donders and Bowman have left on record the following
interesting descriptions of their first meeting; the
first wrote:
“In August, 1851, at the International Exhibition, chance
threw von Graefe and myself together in London. I had
already enjoyed the companionship of Friedrich von Jaeger,
when one morning a young man in Alpine costume rushed
into Guthrie’s eye hospital—he had reached London but
two hours before—and threw himself into Jaeger’s arms.
With the words, ‘You are made for each other,’ the latter
literally threw him into mine. And he was not mistaken.
From early morning, when, on our way to Moorfields
Hospital, we took our modest breakfast in Oxford Street
amongst the workmen going to their work, till late evening,
when we gratefully quitted the hospitable home of our
friend William Bowman, we remained inseparably united
in common objects of pursuit. Von Graefe was my guide
in practical work, of which I had as yet but little experience,
and I again could impart to him much from the physiological
side. This mutual instruction constituted for us a great
attraction. These days in which von Graefe unfolded the
whole charm of his nature belong to the happiest recollections
of my life.”
Bowman, in describing Donders’ visit to London that
year, says:
“It was his first travel, and it brought him, at least, one
thing for which he had great reason to be thankful—the
personal friendship of Albrecht von Graefe, an association
soon to be fraught with splendid results for the expanding
science of ophthalmology; for these two men, both of the
first capacity, laboured ever afterwards to advance it as
brothers in council, and alike fruitfully; freely communicating
their ideas to each other, always in perfect harmony
of aim. While von Graefe, a stranger in London, was able
to tell Donders of the European hospitals he had been
94visiting, and of the new clinical ideas he was maturing, as
well as of the construction in that year, by Helmholtz at
Konigsberg, of a dioptric apparatus for rendering visible
the fundus of the eye, Donders, a stranger there too, could
on his side explain many discoveries of his own in the
physiological field, and, amongst other things, declare the
true nature of the act of accommodation, quite recently
disclosed with certainty by his countryman Cramer, under,
it may be added, his own inspiration and in his own
laboratory.”
Sir William Bowman at the time of this memorable
meeting was older than his two friends, being thirty-five
years of age. His biographer wrote of him:
“At a period of life when most men are only beginning
to apply their powers of observation and reflection, he,
exercising both in a high degree, had already done work
quite unexampled for its novelty, interest, variety, and above
all for its accuracy. Before attaining the age of twenty-six,
he had won for himself a leading position amongst the most
eminent anatomists of his time as a microscopist of first-rate
ability, and the discoveries he had made, with the conclusions
he drew from them, have ever since exercised an important
influence in practical medicine, and have served as models
for all subsequent and similar investigations. Later in
life he became distinguished as an original investigator in
physiology, and as a teacher in that subject, and, at a still
later period, devoting himself to a special branch of his
profession, he stepped naturally and easily into the position
of leader and representative of ophthalmic medicine and
surgery, holding the same position in this country, though
for a far longer period, that was occupied in Germany by
his friend von Graefe, and in Holland by his still more
intimate associate Donders.”
PLATE XII.
SIR WILLIAM BOWMAN, BART., F.R.S.
As the immediate result of his histological work on muscle,
Bowman was in 1841, at the unusually early age of twenty-five,
elected a Fellow of the Royal Society. At the Oxford
meeting of the British Medical Association, in 1847, he
read a paper entitled, “On some Points in the Anatomy
of the Eye, chiefly in Reference to the Power of Adjustment,”
95in which he demonstrated, simultaneously with and independently
of Bruecke, the structure and function of the
ciliary muscle.
In the same year, he delivered to the students at Moorfields
Hospital a series of six lectures dealing with the
parts concerned in operations on the eye and on the structure
of the retina. They contained an account of his
investigations into the microscopical anatomy of the eye,
and were published in book form two years later, a book
which ever since has been regarded as one of the classics
of ophthalmology; a French translation of it by M. Testelin
was published in the Annales d’Oculistiques in 1855.
Bowman’s discovery of the ciliary muscle, bearing as it
did on Donders’ investigations on the accommodation of
the eye, formed from the first a bond of intellectual union
between the two men, which, with the growth of years,
ripened into the warmest esteem and friendship. Donders
wrote on the front leaf of his great work, On the Anomalies
of Accommodation and Refraction of the Eye:
“To William Bowman, F.R.S., whose merits in the
advancement of Physiology and Ophthalmology are equally
recognised and honoured in every country, this work on
the anomalies of refraction and accommodation is, in testimony
of the warmest friendship and of the highest esteem,
inscribed by the Author.”
Though Graefe first performed the operation of iridectomy
for glaucoma in June, 1856, it was not until the following
year that he published an account of his great discovery.
He wisely waited until he had tested it in the different
varieties and stages of the disease until he gave an account
of it to the world at large.
Dr. Bader, the curator and registrar at Moorfields,
wrote in 1859:
“The first instance of glaucoma treated by excision of
a portion of iris by von Graefe’s method was in a case of
chronic glaucoma, operated upon May 1st, 1857; a second
96case was treated in the same manner in October in the same
year. Both were cases of chronic glaucoma in an advanced
stage, and the immediate result for vision was not such as
would recommend the operation. Then came several cases
of acute and subacute glaucoma, in which a striking improvement
followed shortly after the operation. Since then
iridectomy has been tried extensively at Moorfields, and with
good and lasting results in many cases.”
In the second number of the Ophthalmic Hospital Reports,
published in January, 1858, Critchett recorded some cases
of acute glaucoma which he had treated successfully by
iridectomy, though not quite in accordance with Graefe’s
method.
Some years later Bowman wrote the following description
of the introduction of the operation into this country:
“Since the winter of 1856–7, the splendid researches of
von Graefe on the nature and treatment of glaucoma have
prominently attracted attention. On the Continent, his
proposal to arrest the disease by the excision of a portion
of the circle of the iris has been adopted and practised by
the ablest men, including especially Professors Donders of
Utrecht, Arlt of Vienna, and Desmarres of Paris. In May,
1857, I first performed it in England. At the Ophthalmological
Congress at Brussels, in September following, von
Graefe gave an account of his researches, and distributed
amongst his friends an essay on the subject, then just presented
to the French Institute. In the ensuing autumn,
iridectomy as a remedy for glaucoma was, in my opinion,
and in that of my friend and colleague, Mr. Critchett,
established by the facts we had ourselves observed, as a
proceeding competent to cope with the disease, by reducing
that tension of the eyeball, and compression of the retina
and its vessels, which is the cause of the loss of sight.
“It was our earnest wish that the value of von Graefe’s
discovery should be early and extensively acknowledged by
medical men, so that those suffering from so serious a malady
might no longer be drifting, as before, into hopeless blindness.
Since then we have with no faltering voice continued
to advocate the practice, and have performed the operation
on all suitable occasions, both in private and in public.
97At Moorfields, iridectomy has been exhibited and tested
on a very large scale, scarcely a week having passed since
1858 without one or more instances of it; and a host of
competent observers, both students and practitioners, have
witnessed the method of performing it, and its results, in
the hands of several of my colleagues and myself.”
Both Critchett and Bowman began as general surgeons
as well as ophthalmic surgeons. Critchett was appointed
assistant-surgeon at the London Hospital in 1846, and
became full surgeon in 1861. Bowman was appointed
assistant-surgeon at King’s College Hospital in 1840, and
became full surgeon in 1856.
So extensive and absorbing became their work in ophthalmology
that both of them ultimately found it necessary to
resign their general surgical appointments and devote themselves
exclusively to the treatment of eye diseases.
Their reputation as masters in their speciality was not
confined to their own country, but became world-wide.
George Critchett, who was an admirable French scholar
frequently attended the meetings of the International
Ophthalmological Congress, and his son, Sir Anderson, was
fond of relating how, at one of its meetings held in Paris
in 1867, he performed the operation of extraction of cataract
before the assembled Congress, on the two eyes of a patient,
using his right hand for the one eye and his left hand for
the other. So great was his dexterity that at the conclusion
of the operation, Graefe, who was presiding at the Congress
threw his arms round his neck and kissed him on both
cheeks.
Both Critchett and Bowman were men with strong and
attractive personalities, and collected around them at Moorfields
not only a large body of students, but also practitioners
who were devoting themselves to ophthalmology
from all parts of the world. In 1859 they commenced to
supplement their clinical teaching by giving a systematic
three months course of lectures on Ophthalmic Surgery,
98attendance at which course enabled students to comply
with the rules of the Royal College of Surgeons for obtaining
a certificate.
Most foreign missionaries from this country have endeavoured
to promote the spread of Christianity by practising
gratuitously the healing art. David Livingstone was a
qualified medical man, and administered medical relief to
large numbers of the African natives amongst whom he
lived. From some remarks of Sir J. Risdon Bennett, with
reference to Livingstone’s medical studies in London in
1839, it seems probable that he was then in attendance at
Moorfields Hospital. Many missionaries have not sufficient
medical training to entitle them to practise in this country,
but, when abroad, feel themselves called upon to administer
such European drugs as they possess, having greater knowledge
of their uses than the inhabitants of the district in
which they are situated. It was to aid such persons to
alleviate affections of the eye that the Committee of Management
of the Hospital obtained the consent of the medical
staff, in 1854—
“To admit gratuitously to the practice of the Hospital
gentlemen qualified to derive advantage from it, by the
possession of some amount of preliminary medical knowledge;
provided they be duly authenticated to them by a
Missionary Society or otherwise, as being about to proceed
on missionary labours abroad.”
A letter was then drawn up and printed, embodying this
resolution, for circulation amongst those whom it might
interest. Large numbers of missionaries, both men and
women, have since availed themselves of the opportunities
thus afforded them before taking up their duties abroad,
and in this way the teaching and benefits of Moorfields have
been spread to remote regions and to many uncivilised people.
99
CHAPTER VII
THE DISCOVERY OF THE OPHTHALMOSCOPE
The two decades from 1850 to 1870 may well be described
as the golden age of ophthalmology, on account of the
many new discoveries and developments made in connection
with it during that epoch.
In the last chapter the surgical improvements which were
effected have been spoken of, together with the crowning
achievement of them all—the introduction of the operation
of iridectomy for the relief of glaucoma.
In this chapter will be described an event, destined not
only to change the whole outlook of ophthalmology, but also
to add a valuable means for the detection of disease in many
of the organs and tissues of the body—the discovery of the
ophthalmoscope. Following on its discovery, and to some
extent incidental to it, came the recognition of the different
forms of errors of refraction, and the building up of the
methods for their correction with glasses, with which the
name of Donders will for all time be associated.
The merit of discovering the ophthalmoscope, and of
having given it to the world in 1851, belongs to Professor
von Helmholtz, who, having commenced his career as an
army surgeon, was, by his mathematical talents, led on from
the study of physiology to that of physics, and to the production
of his greatest work, his Manual of Physiological
Optics.
The ophthalmoscope was, he said,
“a discovery rather than an invention; that is to say, when
a well-trained physicist came and grasped the importance
of such an instrument, nothing more was wanted, since all
the knowledge had been developed which was required for
its construction.”
100
In speaking of his discovery in later years he said:
“The ophthalmoscope has unfolded itself to me simply
out of the necessity of discussing, in my lectures on physiology,
the theory of emission of light by the eye. Why
does the human eye not glisten under ordinary circumstances,
since in its background there is situated a spot—
small, indeed, but clear white; that is to say, the end of
the optic nerve, which must reflect light in the same way
as the most sparkling tapetum of animals’ eyes? Why do
animals’ eyes sometimes shine with such remarkable lustre,
though they may only be illuminated by a small distant
flame? These questions, when once proposed, were not
difficult to answer, and now the answer is known to everybody.
Once answered, they furnished the means of
lighting up the eye of another human being, and of seeing it
plainly.”
It not infrequently happens, that when time is pregnant
with some new discovery, more than one person is found
to have been hopefully striving to become its accoucheur.
So it was with the discovery of the ophthalmoscope. Here
in England, in 1846, William Cumming, a young surgeon
who was working at the Royal London Ophthalmic Hospital,
had noticed that a reflex could be obtained from the fundus
of the human eye under certain conditions of illumination.
At the Medico-Chirurgical Society that year he read a paper
entitled “On a Luminous Appearance of the Human Eye,”
the conditions for obtaining which he described as follows:
“(a) That the eye must be at some distance from the
source of light, the distance being greater in proportion to
the intensity; (b) that the rays of light diffused around the
patient (and sometimes around the eye itself) should be
excluded; (c) that the observer should occupy a position
as near as possible to the direct line between the source of
light and the eye examined.”
With remarkable prospection he foreshadowed some of
the results which were ultimately obtained from the use of
the ophthalmoscope; thus he wrote:
101
“The establishment of the fact of a similar reflection
from the human eye to that from the eyes of animals appears
to be chiefly important in its adoption as a mode of examining
the posterior part of the eye. The retina and choroid
hitherto concealed in the living eye, and little opportunity
being afforded of examining their condition after life, in
consequence of their diseases not terminating fatally, considerable
uncertainty had hitherto attended the diseases
ascribed to these structures; but the existence of this
luminosity, its non-existence, or abnormal appearance may
enable us to detect changes in these structures hitherto
unknown, or satisfactorily to see those which we only
suspected.
“If we dilate the pupil with atropine, we have the means
afforded of seeing the condition of the retina and choroid
in every case. The cases I have examined in this way
have confirmed the general impression that the retina is
not frequently the seat of changes in amaurosis; for, out
of several cases of amaurosis, in which the non-opacity of
the cornea, lens, and humours allowed this mode of examination,
I found but two in which the retina was so changed
that the reflection was not seen.”
Cumming discussed these matters with Dixon and Bowman,
the latter suggesting to him that the choroid and its
pigment was probably the reflecting surface. Another
quotation from his article will show how near he actually
came to the discovery of the ophthalmoscope; thus he
wrote:
“On approaching within a few inches of the eye the
reflection is not visible, for, before our eye can be brought
within range of the reflected rays, the incident rays are
excluded.”
Cumming died in 1855, at the early age of thirty-three,
but just lived sufficiently long to see that what he had fore-told
was being realised. In 1862 a portrait in oil-colours
of him was presented to the Hospital by one of his relatives
with the following letter:
102
“2, Vittoria Place, Limehouse,
“November 11th, 1862.
“Sir,
“I have the pleasure of presenting to the Hospital
a portrait of the late William Cumming of Limehouse. It
is from a painting in possession of the family.
“William Cumming was honourably connected with the
Institution, was discoverer that the fundus of the living eye
could be explored, and a pioneer in the recent advances in
Eye Surgery.
“He died in 1855 at the early age of 33 years.
“I am, etc.,
“John Stewart Cumming.”
This portrait still hangs in the Board Room of the
Hospital.
PLATE XIII.
WILLIAM CUMMING.
From a painting in the Board Room of the Hospital.
In 1847 Charles Babbage, a distinguished mathematician
and scientific mechanician, who held the Lucasian Chair of
Mathematics at Cambridge, and who spent a large part of
his life in the construction of a calculating machine, actually
invented an ophthalmoscope. He himself published no
description of it, and we know nothing of the circumstances
which led up to this invention; the only record we have
concerning it is that published by Wharton Jones in 1854,
in a “Report on the Ophthalmoscope” in the Medico-Chirurgical
Review. He wrote:
“It is but justice that I should here state, however, that
seven years ago Mr. Babbage showed me the model of an
instrument that he had contrived for the purpose of looking
into the interior of the eye. It consisted of a bit of plain
mirror, with the silver scraped off at two or three spots
in the middle, fixed within a tube at such an angle that the
rays of light, falling on it through the side of the tube, were
reflected to the eye to be observed, and to which one end
of the tube was directed. The observer looked through
the clear spot of the mirror from the other end.”
Probably Wharton Jones, who was himself short-sighted,
in using Babbage’s reflecting mirror, without any lens, only
obtained a red glow from the fundus of the eye, and saw
103nothing of the optic nerve or of the retinal bloodvessels,
for, had he done so, it seems unlikely that a man of his
powers of observation and scientific attainments would not
have realised the possibilities of such an instrument.
Anyhow, he gave Babbage no encouragement, and the
instrument was laid aside as a mere toy.
Indeed, it seems doubtful if Helmholtz himself at first
fully realised the possibilities of his great discovery. On
the occasion of the presentation to him of the first Graefe
medal in Heidelberg in 1886, Donders spoke as follows:
“How the ophthalmoscope could be serviceable to
ophthalmologists, how the eye under examination, whilst
its fundus becomes visible, constitutes for the emmetropic
examiner a lens, too weak in myopia, in hypermetropia too
strong; and how simultaneously with the examination of
the fundus, the refraction can be determined; all this was
clearly indicated by von Helmholtz. But he never thought,
or at least he never said, that the new instrument implied
the dawning of a new era for ophthalmology. Von Graefe
felt it immediately. When he, for the first time, saw the
background of the eye, with its nerve-entrance and its
bloodvessels, his cheeks reddened, and he called out excitedly.
‘Helmholtz has unfolded to us a new world,’ and
then, ‘What remains there to be discovered?’ added he
thoughtfully.
“It was, indeed, humiliating to hear it said, banteringly,
that black cataract was that disease in which the patient saw
nothing, nor the surgeon either. Treatment was then but
a groping in the dark. Under the same name were thrown
together the most diverse affections of the fundus oculi
and of the nerve apparatus; and even disturbances of refraction
and accommodation, such as astigmatism and
muscular asthenopia, were reckoned with amblyopia. And,
against these most diverse disturbances, the same empirical
remedies were employed many of them a real torment to
the patient not only with little beneficial result, but sometimes
at the cost of health.”
The increasing number of operative procedures performed
at the Hospital, and the coming of the ophthalmoscope,
104created a demand for more accommodation in both
the in- and out-patient departments. The alterations necessary
to supply these wants extended over several years, but
ultimately resulted in the transference of the out-patient
department, together with the dispensary and a dark room
for ophthalmoscopic work, to newly erected buildings on
the site of the Saunderian Institute, and the yard at the back
of the main building. The ground floor of the latter was
then utilised for rooms for the resident staff and for a
committee room, and the first floor was turned into wards
for in-patients.
Battley having ceased his pharmaceutical investigations
and teaching, and Dr. Farre his pathological researches,
they consented to hand over all their rights in the Saunderian
Institute so that it might be made use of by the Hospital.
Shortly before Tyrrell’s death, the Committee of Management
had under consideration the hardship of an assistant-surgeon
remaining on the staff for a number of years without
the opportunity of gaining experience in performing the
major operations on the eye. When Tyrrell died, both
Mackmurdo and Dalrymple became full surgeons, and the
matter was left for a time in abeyance. In 1854, however,
at a meeting of the Governors, the rules were altered so that—
“any assistant-surgeon who shall have served the Hospital
five years shall, provided he be a Fellow of the College of
Surgeons, become, if the Committee think fit, a surgeon.”
At the same time the title of the resident medical officer
was changed from apothecary to house surgeon.
In 1854 the Crimean War commenced; its immediate
effect on the Hospital was a reduction in its receipts from
donations and subscriptions, which together amounted to
£614 in 1853, and only to £236 in 1854. A Jubilee dinner
to commemorate the fiftieth anniversary of the foundation
of the Hospital was abandoned, and the building operations
of the new out-patient department postponed.
105
PLATE XIV.
JAMES DIXON. JOHN CAWOOD WORDSWORTH.
In 1855 Wordsworth, the junior assistant-surgeon,
answered Mr. Sydney Herbert’s call for volunteers in aid
of the overtaxed military medical officers in the East, and,
having obtained leave of absence from the Committee of
Management, went as surgeon to the Civil Hospital at
Smyrna. Later he was transferred to the Crimea, which
he reached just in time to render good service “in the
front” to those wounded in the attack upon the Redan.
For three months of the following winter he was attached
to the Castle Hospital on the heights above Balaclava.
On the conclusion of the war, at the annual general meeting
of the Governors, the following resolutions were passed:
“That this meeting, holding in the highest respect and
esteem the humane and benevolent consideration and
sympathy manifested for the Army in the East, during the
late War with Russia, by the Right Honourable Sydney
Herbert, M.P., respectfully requests Mr. Herbert to accept
the nomination of Honorary Life Governor and Vice-President
of this Hospital.
“That this meeting appreciates most highly the humane
and benevolent ministrations of Miss Florence Nightingale
to the sick and wounded in the service of the country in
the East during the late War with Russia, and it is hereby
resolved that Miss Nightingale be a Life Governor of this
Hospital.”
Miss Nightingale and Mr. Sydney Herbert both replied
accepting with pleasure these nominations.
Though Miss Nightingale was made a Life Governor of
the Hospital, it was not until many years later that the
reforms in the system of sick nursing, which she was instrumental
in bringing about, were introduced at Moorfields.
In 1859, in consequence of the increased accommodation
for in-patients, it was arranged that there should be a nurse
with an assistant on each of the two floors. It was also
ordered “that in future every patient on admission to the
wards be bathed, unless otherwise ordered by the admitting
officer.” But that much was left to be desired in the matter
106of nursing will be gathered from a note directed to the
Committee by the Medical Council in 1861, in which it
requested the Committee to consider the advisability of
providing proper receptacles for keeping the in-patients’
clothes, “which are now generally put under the bedding,
the consequence of which is that the beds occasionally get
infested with vermin, to the serious discomfort of the
patients who subsequently occupy them.”
In 1856 Dr. Frederick Farre, who had become full
physician at St. Bartholomew’s Hospital, found that pressure
of work necessitated his resigning his post on the active
staff at Moorfields. His father, Dr. J. R. Farre, at the same
time withdrew from his position of consulting physician,
and Dr. Frederick Farre was appointed in his place. The
family’s connection with the Hospital was still further maintained
by the appointment of Dr. J. R. Farre’s younger
son, Dr. Arthur Farre, a distinguished physician accoucheur,
as a member of the Committee of Management.
Dr. Robert Martin, an assistant-physician at St. Bartholomew’s
Hospital, being the only candidate, was elected
physician.
In the same year Gilbert Mackmurdo, who had served on
the staff of the Hospital for a period of thirty-six years, resigned
and was appointed consulting surgeon. The appointment
of a new assistant-surgeon to fill the vacancy thus created
gave rise to a most keenly contested election, in which 458
Governors recorded their votes. One of the daily papers,
describing the event, stated “that the usually quiet neighbourhood
of Finsbury was the scene of great excitement.”
There were four candidates, and, at the close of the poll,
the scrutineers announced that the votes had been distributed
as follows:
Mr. J. S. Gamgee
3
Mr. J. W. Hulke
148
Mr. J. F. Streatfield
214
Mr. Walter Tyrrell
93
107
This method of election by Governors of the members of
the medical staff was the general practice at most hospitals
at that time; but though it helped to increase the funds
of those institutions, it was not well calculated to secure
the services of the most suitable candidate, and, as we shall
see later, was subsequently abandoned.
The Governors consisted of “Life Governors”—i.e. those
who had contributed ten guineas in the course of one year,
and annual subscribers of one guinea. A body of electors
so formed was not well qualified to judge of the relative
merits of rival candidates; and a candidate, with a number
of friends willing to promote his interests by becoming
subscribers, might thereby bring about a preponderating
influence in his favour. Moreover, where more than two
candidates presented themselves, the successful candidate
might, as in this 1856 election, be elected without having
received a majority of the votes recorded.
With an electorate of between 400 and 500 Governors,
a candidate who set out to canvass them had a formidable
task before him, and one which often proved an expensive
proceeding. The last surgeon elected to the staff in this
way estimated his costs at nearly £100, which seems an
inordinate amount to expend for obtaining the privilege of
giving one’s time and service to the relief of the poor and
needy. It can, therefore, be easily understood why a candidate
who found his chances of election doubtful, frequently
withdrew in favour of one of the others, and contented
himself with announcing his intention of applying again on
a future occasion.
John Fremlyn Streatfield was the son of a well-known
antiquarian, the Rev. Thomas Streatfield, of Charts Edge,
Westerham, Kent. He inherited his father’s antiquarian
instincts and was also a staunch Churchman. He studied
medicine at the London Hospital, and, like several of the
other oncoming surgeons at Moorfields, served in the East
at one of the British hospitals during the Crimean War.
108In 1862 he was appointed assistant ophthalmic surgeon at
the University College Hospital, and shortly afterwards, on
the retirement from the staff there of Wharton Jones, succeeded
him as full surgeon.
Streatfield was gifted with remarkable manipulative
dexterity, and delighted in using his fingers in a way which
most people would have regarded as impracticable. There
was, indeed, something almost acrobatic in his method of
operating, and George Critchett used jokingly to remark
that he expected one day, on going into the operating
theatre, to find Streatfield removing a cataract whilst at the
same time he balanced a feather on his nose.
On the death of Earl Fitzwilliam, in 1857, the post of
President of the Hospital became vacant, and Mr. William
Cotton, D.C.L., F.R.S., an eminent merchant and philanthropist,
having consented to be nominated for the post,
was elected by the Governors. He was at one time Governor
of the Bank of England, and invented a most ingenious
machine, which has ever since been in use, for weighing
sovereigns at the rate of twenty-three per minute; it is
capable of discriminating to a ten-thousandth part of a
grain, discharging the full-weight and the under-weight
into different compartments. He was, perhaps, even more
noted for his philanthropy than his ingenuity: he founded
several churches and gave assistance to many charitable
institutions.
At the same time H.R.H. the Duke of Cambridge was
invited to become a Patron of the Hospital, which invitation
he most graciously accepted.
As the medical staff became enlarged, its members formed
themselves into a “Medical Council,” to give collective
consideration to matters referred to it by the Committee of
Management, or to initiate measures for promoting the
prosperity of the Hospital and the progress of ophthalmology.
In 1857, when several regulations and practices which
109had been introduced were being codified, the following
rule became included amongst those governing the Institution:
“The physicians, if any, surgical officers, with the consulting
physicians and consulting surgeons, if any, shall
constitute a Medical Board empowered to consult on all
matters connected with the medical department, with the
admission and conduct of pupils, and shall report to the
Committee from time to time.”
In 1856 this Medical Council made the following proposal
to the Committee which led to the establishment of the posts
of clinical assistants:
“That with a view to aid in treating the less important
cases, to assist the clinical work of the out-patient room
and in case-taking, it might be worthy of the consideration
of the Committee, whether advantage might not be taken
of the zeal and knowledge of some of the younger surgeons
attending the Hospital, by electing them for a period of six
or twelve months, as assistants to the surgeons. The
Committee might appoint such assistants to any of the
surgeons who might require aid. They should be qualified
to practise, and of such established character that perfect
confidence could be placed in them for the steady performance
of their duties. Many of these men, after completing
their term of office, would carry skill to various parts
of the country in which they settle, while from them the
Governors would be gradually furnished with highly competent
candidates for the vacancies which from time to
time occur in the staff. Their title might be that of ‘clinical
assistants,’ and they would be entitled on retirement to a
superior certificate.”
These recommendations of the Medical Council were put
into practice, and have continued ever since to work out
in the ways which it had forecast. The first clinical assistants
to be appointed were Mr. J. W. Hulke, Mr. Jonathan
Hutchinson, and Mr. Walter Tyrrell; and a year or so
later, Mr. G. Lawson, Mr. Harkness, Mr. Hughlings Jackson,
Mr. J. S. Wells, and Mr. J. Couper.
110
The following rule with regard to these appointments
became embodied in the laws of the Hospital in 1861:
“That the appointment of clinical assistants be held for
one year, and that these officers be annually re-eligible when
approved by the Medical Council and sanctioned by the
Committee of Management.”
The increasing number of eyes which were removed for
the relief of pain, on account of disfigurement, to prevent
inflammation spreading to the fellow eye, or on account
of the presence of a new growth, supplied a large amount
of material for pathological investigation, and for the formation
of a museum of pathological specimens.
When the Saunderian Institute was converted into a
waiting room for out-patients, a room was set apart elsewhere
for a museum and library; and with some of the money
left over from the Saunderian Fund a microscope was
purchased. In 1857 Dr. Charles Bader, a young German
skilled in the use of the ophthalmoscope, was appointed
curator and registrar, with an annual honorarium of 25
guineas.
The increasing interest excited in the various changes in
the fundus of the eye revealed by the ophthalmoscope made
it desirable to have a collection of water-coloured drawings
depicting them for preservation in the museum. An artist,
Mr. Schweizer, was employed to make such drawings under
the superintendence of Bader. A long list of those which
he produced is recorded in the early numbers of the
Ophthalmic Hospital Reports, where also some of them are
published in lithographic plates. The changes represented
are all drawn on a very small scale, the pictures themselves
only measuring inches in diameter. They are, however,
very faithful representations of the changes shown, and contain
a remarkable amount of fine detail. There can be little
doubt that Mr. Schweizer must himself have been short-sighted.
The interpretation of the nature of the changes revealed
111by the ophthalmoscope called for much careful dissection
and microscopical investigation. The two chief pioneers in
this work at Moorfields were Hulke and Bader. The former,
in an article on the morbid anatomy and pathology of the
choroid and retina in 1857, wrote:
“Since the discovery of the ophthalmoscope great advances
have been made in our knowledge of the diseases
of the deeper parts of the eyeball. We are daily becoming
more familiar with the morbid appearances which characterise
the various affections of the choroid, the retina the
vitreous humour, and the lens. We read these appearances
during life, as if portrayed upon the pages of a book; but
our knowledge of them, of their exact situation and precise
natures must remain very imperfect without the explanation
afforded by dissections and the microscope. The extensive
practice of the Moorfields Ophthalmic Hospital has, by the
liberality of the medical staff, for a long time afforded me
great opportunities for working with the ophthalmoscope,
and for making microscopical examinations of diseased
eyeballs immediately after their removal.”
PLATE XV.
JOHN WHITAKER HULKE, F.R.S. GEORGE LAWSON
In 1859 the Royal College of Surgeons chose as the subject
for the Jacksonian Prize Essay of that year:
“The morbid changes in the retina as seen in the eye of
the living person, and after removal from the body, together
with the symptoms associated with several morbid conditions.”
John Whitaker Hulke’s essay was awarded the prize, and
he subsequently published it in a somewhat altered form as
a handbook to the use of the ophthalmoscope.
Hulke, who was born in 1830, was educated at the
Moravian College at Neuwied, and became a fluent German
linguist; he studied medicine at King’s College Hospital
where he early became associated with Bowman. During
the Crimean War he was attached to the hospitals at Smyrna
and Sebastopol. In 1857 he was appointed assistant-surgeon
to King’s College Hospital, and in 1858, when an
additional post of assistant-surgeon was created at Moorfields,
112he was elected unopposed, the only other candidate,
Jonathan Hutchinson, retiring in his favour. In 1862 he
transferred his services as a general surgeon to the Middlesex
Hospital, where he became full surgeon in 1870. In 1867
he was elected a Fellow of the Royal Society for his researches
relating to the anatomy and physiology of the
retina in man and the lower animals, particularly the reptiles.
Hulke not only distinguished himself as a general surgeon,
an ophthalmologist, a pathologist, but also as a geologist;
he contributed several papers to the Royal Society on
Palæontology, more especially in connection with the great
extinct land reptiles (Dinosauria) of the secondary period.
In 1887 he was presented the Walleston Medal, the greatest
honour in the power of the Royal Society to bestow.
To those familiar with an Ophthalmic Hospital at the
present time, it is difficult to conceive of its work being
carried on without the devotion of much time and attention
to the correction of errors of refraction with glasses. Yet
it was only during the latter part of the nineteenth century
that the scientific principles for the correction of such errors
became recognised.
Hulke, in some reminiscences of his youth, remarked:
“In my earliest student days the ophthalmoscope was
unknown, and errors of refraction were so little understood
that a small tortoise-shell case, which could be easily carried
in the trousers pocket, containing half a dozen convex and
concave spherical lenses, was held to comprise a sufficient
stock for every trial.”
The simultaneous but independent discovery by Bowman
and Bruecke of the muscular nature of what was formerly
known as the ciliary ligament, the change in the form of
the lens in accommodation demonstrated by Cramer, and
the discovery of the ophthalmoscope by Helmholtz, prepared
the way for Donders’ great work, On the Anomalies of
Accommodation and Refraction of the Eye, which was published
in English by the New Sydenham Society in 1864.
113
James Ware, to whom reference has already been made,
was one of the first surgeons in England to devote himself
specially to the treatment of eye diseases (vide Chapter I.,
p. 11). He is entitled, Donders says, to be described as
the discoverer of hypermetropia or long-sightedness. In a
paper on “Observations Relative to the Near and Distant
Sight of Different Persons,” which Ware read before the
Royal Society in 1812, he said:
“There are also instances of young persons, who have
so disproportionate a convexity of the cornea or crystalline,
or of both, to the distance of these parts from the retina,
that a glass of considerable convexity is required to enable
them to see distinctly, not only near objects, but also those
that are distant; and it is remarkable that the same glass will
enable many such persons to see both near and distant
objects, thus proving that the defect in their sight is occasioned
solely by too small a convexity in one of the parts
above-mentioned, and that it does not influence the power
by which their eyes are adapted to see at distances variously
remote. In this respect such persons differ from those
who had the crystalline humour removed by an operation,
since the latter always require a glass to enable them to
discern distant objects, different from that which they use
to see those that are near.”
These early and accurate observations of Ware’s were
forgotten, and it was not until 1859, at a meeting at Heidelberg,
that Donders first clearly differentiated long-sightedness
or over-sightedness as some then termed it, from
presbyopia, and suggested the term “hypermetropia” as an
appropriate name for it. The importance of understanding
correctly the nature of this affection of the eye was summed
up thus by Donders:
“He who knows by experience how commonly hypermetropia
occurs, how necessary a knowledge of it is to the
correct diagnosis of the various defects of the eye, and how
deeply it affects the whole treatment of the oculist, will
come to the sad conviction that an incredible number of
114patients have been tormented with all sorts of remedies
and have been given over to painful anxiety, who
have found immediate relief and deliverance in suitable
spectacles.”
What is termed “asthenopia,” or tiredness of the eyes
with confusion of vision after close work, without any alteration
in their external appearance, had been attributed to
a variety of causes by different observers. Lawrence spoke
of it as an affection of the retina from excessive employment.
Tyrrell endeavoured to prove that it was due to congestion
of the choroid. It became recognised that it was not caused
by contrasts of light and shade:
“All day the vacant eye without fatigue
Strays o’er the heaven and earth; but long intent
On microscopic arts, its vigour fails.”
That it was produced by application of the eyes to near
objects suggested that the muscles that move the eyeballs
might be concerned, and some even practised tenotomy of
them for its relief. It was not until Donders demonstrated
its association with hypermetropia that the circumstances
under which it may arise were made clear, and the way
shown in which it could be relieved by the use of spectacles.
Though we are indebted to Kepler for the earliest knowledge
of short-sight, or myopia, it was not until after the discovery
of the ophthalmoscope that the peculiar changes in
the fundus of the eye associated with it, and due to enlargement
of the posterior part of the eyeball, became recognised.
At Moorfields they were described and pictured by Bader
in the Ophthalmic Hospital Reports in 1858.
The elongation of the visual axis in myopic eyes, formed
at the expense of the posterior wall, was first demonstrated
by dissection by Arlt in Vienna in 1856.
The asymmetry of the dioptric system of the eye which
we call astigmatism was first observed by that versatile
genius, Thomas Young, in his own eyes in 1793; and later
115by Airy, the Astronomer Royal, in 1827, who introduced
the use of cylindrical lenses for its correction. Airy’s
colleague, Whewell, suggested the term “astigmatism.”
That it was due to a difference in the curvature of the
cornea in its two meridians was asserted by Wharton Jones
in 1855 and by Wilde of Dublin. It was, however, Donders
who by measurement first certainly proved that such
asymmetry of the cornea actually existed.
The introduction of systematic sight-testing for errors of
refraction at Moorfields was of gradual growth. In 1860
J. Soelberg Wells, who was then working there as a clinical
assistant, wrote as follows:
“There are perhaps few subjects connected with ophthalmic
practice which demand greater care and exactitude
than the choice of a pair of spectacles. The very frequency
with which we are called upon to improve vision by means
of glasses is but too apt to make us somewhat careless and
empirical in our mode of selection, and to prescribe those
which the patient himself most fancies, even although they
may not quite accord with the range of his accommodation,
or with the scientific principles which should influence our
choice. But how much more does not this inefficiency in
selecting spectacles obtain among quasi-opticians, jewellers, etc.
This is doubtlessly often attended with the most disastrous
results, and eyes, which might with proper glasses have
lasted a number of years, are soon recklessly and unwittingly
destroyed through ignorance and carelessness of
unscientific opticians. In order to obviate this, I would
urgently advise the adoption of a method practised in many
parts of the Continent. In Berlin, for instance, von Graefe
has spectacle boxes, containing convex and concave glasses
(whose number corresponds exactly with those kept by the
opticians); from these he selects the proper glasses, and
puts the number of their focal distance on a slip of paper,
which the patient takes to an optician, who supplies him
with the spectacles thereon prescribed.
“I am fully aware that this proceeding would, at present,
be carried out with some difficulty in England, owing to
the fact that different opticians often number their glasses
116differently; but I have doubt, that if the leading opticians
would adopt a certain standard, the others would soon
follow their example.”
In order to overcome the difficulties caused by the inaccurate
dispensing of glasses, it was agreed in 1861, on
the recommendation of the Medical Council, to appoint
Thomas Doublet, optician, of 7, City Road, Finsbury
Square, the official optician to the Hospital. This appointment
led to a letter of protest from William Hawes, optician,
of 79, Leadenhall Street, in which he said that for the
past twenty years he had been supplying spectacles ordered
by the surgeons to patients of the Hospital at an agreed
price. It is interesting to note this, as his son, Alfred
Hawes, was later on appointed optician to the Hospital, an
appointment which William’s grandson still holds.
The system then in vogue for numbering lenses was the
“inch system,” the unit on which it was based being a
lens having a principal focal distance of 1 inch. It was
inconvenient, as it necessitated the refractive power of any
lens of a weaker strength being expressed by a fraction,
whose denominator represented its principal focal distance.
Complications also arose owing to the variations of
the inch in different countries. Thus in ordering glasses it
was necessary to state if the trial lenses employed were
graduated in English, Paris, or Prussian inches. It was
Nagel in 1866 who proposed a metre system of numbering
lenses—i.e., taking a lens with the principal focal distance
of 1 metre as the unit, and speaking of it as having the
refractive power of 1 diopter. The advantages of this new
system soon became evident, and, after it had been considered
and reported on favourably at the International
Congress of Ophthalmology in 1872, its adoption became
general.
Letters or figures have always been employed by ophthalmologists
as the most convenient method for testing the
power of vision. Alfred Smee, F.R.S., surgeon to the
117Bank of England and to the Central London Ophthalmic
Hospital, in a book entitled Vision in Health and Disease;
the Value of Glasses for its Restoration and the Mischief
caused by their Abuse, the first edition of which was published
in 1847, gave a series of graduated sized prints for the
testing of vision, and described an optometer he had constructed
for “the adaption of glasses.”
Ed. von Jaeger of Vienna, in 1854, published a series
of typographical specimens, distinguishing the various sizes
of the letters by numbers instead of technical names, which
allowed of their use by all nations. These have ever since
remained the most generally used test for near vision. It
was Snellen of Utrecht, however, who first constructed
test types on a definite scientific principle, so that the
strokes composing the letters are all drawn on a regularly
proportional scale of thickness, the letters exhibiting themselves
under an angle of five minutes at the distance at which
they should normally be seen.
In 1860 the Committee of Management of Moorfields, at
the request of the Medical Council, had drawn up and
printed test types for use in the out-patient room.
By the death of Mr. Richard Heathfield in 1859 the
Hospital lost one of its oldest supporters, who had been
a friend of Saunders and associated with him in its foundation.
When the Rev. J. Russell retired from the Chairmanship of
the Committee of Management, Heathfield had
succeeded him, and was a vigorous promoter of the
extensions of the institution rendered necessary by the advance
of knowledge.
Mr. F. G. Sambrooke was appointed Chairman in his place.
On the death of Miss Marian Sedgwick, the last
surviving daughter of the late Harry Sedgwick, in January,
1860, the Hospital came into possession of the reversion
bequeathed by him (as mentioned in Chapter III.) of the
sum of £19,841 Three per Cent. Stock, subject to 10 per cent.
118legacy duty. A portrait of this early supporter and munificent
benefactor of the Charity had been previously presented
by his family, and now hangs in the Board Room.
In 1853 the Committee had commissioned Mr. Henry
Weekes to construct a marble bust of Mr. Harry Sedgwick
at the cost of £120, to be designed as a companion to that
by the same artist of J. Cunningham Saunders. These
two busts, together with that of Dalrymple, now adorn the
entrance hall of the present building.
119
CHAPTER VIII
THE COMMENCEMENT OF “THE OPHTHALMIC HOSPITAL REPORTS”
The first English journal devoted specially to the subject
of ophthalmology originated with the medical staff of the
Moorfields Hospital. The first number of the Ophthalmic
Hospital Reports, as the journal was called, was published
in October, 1857. Its origin and aims were set forth as
follows:
“At a meeting of the Medical Council of the Hospital
on the 25th of August last, it was determined to issue a
periodical record of ophthalmic observation and experience;
it was thought that, not only at Moorfields, much valuable
information was gained and lost that should be preserved,
and that such a journal might obtain favour throughout
the country. Mr. Streatfield was appointed to collect and
arrange, from time to time, the material and order its
publication.
“The Ophthalmic Journal will be, for the present, issued
quarterly. It will give short monographs by members of
the staff, and of the profession generally (if we are so fortunate
as to engage their attention), on any physiological or
pathological subjects connected with our especial study;
with, it is hoped, occasional engravings, or photographs as
illustrations. It will also contain a summary reprint of the
monthly reports of the Registrar of the Hospital, and titles
of books and preparations presented to the Ophthalmic
Library and Museum of the Hospital. It will not contain
reviews of books as such, or any correspondence, or
anonymous publications. The opinions expressed in it
must be understood to be those of individual authors. The
editor will collect minor noteworthy observations, and
record novelties and illustrative cases, with regard to
consecutive detail.”
120
A list of the subscribers given in the fifth part, published
a year later, shows them to have then numbered 195. By
its establishment the Library at the Hospital became enriched,
for exchanges were effected between it and several
other journals dealing directly or indirectly with ophthalmology.
Though the highly specialised subject of the journal
prevented it from gaining a very extensive circulation, it
became the medium for publication of original articles
which are now regarded as among the classics of ophthalmic
science.
The first volume is composed of six parts, published at
intervals between October, 1857, and January, 1859. The
first part opened with an article by Bowman, giving an
extended account of his investigations into the treatment
of lacrymal obstruction by slitting up the lacrymal punctum
and the use of probes, which has already been referred to
in Chapter VI. Poland also commenced a series of articles,
which were continued in subsequent parts, on “Protrusion
of the Eyeball.” They contain a number of well recorded
cases with interesting remarks, giving a vivid description
of the treatment of inflammatory affection in pre-antiseptic
days, by what was termed “antiphlogistic measures.” In
the third volume of the Reports Poland contributed an
article on “Medico-legal Observations in Connection with
Lesions of the Eye.” Much has been written on this
subject since, but little has been added, as regards matters
in this country, which is not dealt with by Poland. He
quotes Mr. Harry Bodkin Poland, barrister-at-law, no doubt
a relative of his, as stating the legal position in the assessment
of damages for accidents to be as follows:
“There is no fixed mode of assessing damages from
accident. When it can be shown that a particular person
is liable for causing an accident, etc., the jury decide as
to the amount of damages to which the injured person is
entitled, and neither the medical man nor the lawyer interferes,
121except to put before the jury the real nature of the
injuries inflicted.”
The following precautionary remarks, which he wrote
some seventy years ago, evidently as the outcome of his
experiences at Moorfields, are so applicable to-day that they
may well be quoted:
“The causes which may lead to the loss of an eye through
carelessness and negligence ought well to be borne in mind
by the thoughtless, so that should any person be employed
in any of the following acts, he should pay due regard to
the passers-by, or those standing near, and thus obviate
any necessity for rendering himself liable for the damages
committed.
“The carrying or whirling about of sticks, umbrellas,
guns, etc., in the public thoroughfares, the slashing about
of whips, the careless use of the line and rod in fishing, the
letting off of fireworks, the shooting of arrows, the throwing
of missiles such as stones, lime, etc.; the chipping of wood,
stone, and metals in the public highways, without adequate
protection; the playing at tip-cat; the uncorking of effervescing
draughts; the explosion of chemicals and gunpowder;
and numerous other acts each and all of which have caused
the loss of an eye or of both, and have been the means
of litigation.”
In 1861 Alfred Poland was elected surgeon to Guy’s
Hospital with charge of the large ophthalmic department,
and, in accepting the appointment, was required by the
Governors of Guy’s to resign his post of surgeon at Moorfields,
which he did most reluctantly. Many competent
observers described him as the best operator on the eye
they had ever seen. He was a spare, thin man, and made
remarkable recoveries from several severe illnesses, but died
ultimately of consumption at the age of fifty-two. The
following account of some of his other characteristics have
been recorded by one of his colleagues at Guy’s:
“Poland had a remarkable power of gathering together
detailed knowledge, including dry facts and figures, so that
122his essays are complete treaties on the subjects in hand,
and are of permanent value.
“It was said with great truth that if Poland had been
shut in a room containing not a single book, but with only
pens and paper, he could have written a complete work on
surgery, not in a vague way, giving merely general descriptions
and treatment, but in a systematic manner, detailing
the distinct forms and varieties of the disease then in his
mind.
“He was utterly careless as to his personal appearance.
He would leave the dissecting room without changing his
coat, and it was often the subject of surmise whether he
washed his hands.
“On his appointment to the surgeoncy at Guy’s, the
Treasurer had no hesitation in telling him he would have
to dress himself more decently and cleanly. It is not,
therefore, surprising that Poland never had any practice
to speak of. There was nothing in his manner to give confidence,
but he was a great favourite with students.
“His marriage a few years before his death was a misalliance,
and added much to his misfortunes.”
One of the most conspicuous features of the Reports
since their commencement has been the contributions
made to them by the several occupants in succession of the
post of curator of the Museum, beginning with Charles
Bader. This post has afforded the holders of it a most
valuable field for pathological research, as all the eyes
removed by the members of the staff are entrusted to
the curator for his investigation, and often also a large
number of specimens from elsewhere. The articles written
by the several curators contain most of the valuable
original work which has been done in this country on the
subject.
In the fourth part of the journal, published in July, 1858,
Jonathan Hutchinson, who was then working as a clinical
assistant at the Hospital, commenced his ever memorable
series of articles “On the Different Forms of Inflammation
of the Eye consequent on Inherited Syphilis.” In these
articles he first definitely established the connection of
123interstitial keratitis with inherited syphilis, and showed its
frequent connection with certain characteristics of the complexion
and physiognomy, and with peculiarities in the
formation of the permanent teeth. Which latter are now
universally known as “Hutchinson’s teeth.”
PLATE XVI.
SIR JONATHAN HUTCHINSON, F.R.S.
Jonathan Hutchinson was born in Yorkshire in 1828, of
Quaker ancestors. For four years he studied at the York
School of Medicine, and then came to London, when he
attended at St. Bartholomew’s Hospital. He there came
under the influence of Sir William Lawrence, to whom he
dedicated his book entitled Diseases of the Eye and Ear
consequent on Inherited Syphilis, published in 1863, consisting
mainly of his reprinted articles in the Ophthalmic
Hospital Reports.
It has already been mentioned in Chapter III. how much
Lawrence did to increase the knowledge of venereal diseases
of the eye by the careful collection and collation of notes
of cases at the Ophthalmic Hospital. It was by the same
careful collection and collation that Hutchinson was able to
establish the connection of certain inflammatory eye affections
with inherited syphilis, and he likewise found the most
fruitful field for his investigations in the out-patient department
at Moorfields. He was a most patient and elaborate
note-taker and, in apologising for the lengthy notes of some
or his published cases, remarked:
“I must plead that they are the stones out of which the
edifice is to be built, and that unless care be devoted to their
preparation in the first instance, it will be useless to expend
it on the subsequent elaboration.”
Jonathan Hutchinson was a man intensely interested in
the study of the natural history of disease in all its manifestations,
and it may be added not only in the natural
history of the disease, but of natural history generally. He
was a great collector of facts, and had a remarkable flair for
grouping them so as to draw new and unsuspected inferences.
124
He was not inaptly described as “the greatest general
practitioner in Europe,” and also as “the universal
specialist.” He was appointed assistant-surgeon to the
London Hospital in 1859 and full surgeon in 1862; he was
also surgeon at the Blackfriars Skin Hospital.
He attracted around him a large number of able assistants
of whose devoted services he was able to make very material
use. His biographer writes:
“His teaching was made impressive by ingenious arguments,
apt illustrations, vivid metaphors, and quaint expressions,
and was driven home by the simplicity and
solemnity with which they were delivered.”
On the retirement of Alfred Poland from the staff in 1861,
it was decided that the surgical staff should be increased
to eight in number by the appointment of two new assistant-surgeons.
George Lawson and Jonathan Hutchinson were
the only two candidates who came forward, and were both
elected. Lawson, receiving a few more votes than Hutchinson,
was appointed the senior of the two.
George Lawson, like Hulke, received his medical education
at King’s College Hospital. There was a remarkable
parallelism between the careers of these two men. Both
served as house surgeons under Sir William Ferguson.
Both served as surgeons at the Crimea. Both became
assistants to Bowman, and inspired by him combined
ophthalmic surgery with general surgery. Both became
general surgeons at the Middlesex Hospital, and ophthalmic
surgeons at Moorfields.
Though their careers were so similar, temperamentally
they were very different. Hulke was an austere, conscientious
disciplinarian, who seemed to have had no youth.
Lawson, on the other hand, was full of kindly sympathy for
the weaknesses of mankind, and never seemed to grow old.
This difference was no doubt to some extent attributable,
as Lawson himself suggested, to Hulke having had no
children, whilst Lawson had a large family of boys.
125
Hulke earned for himself the greater scientific reputation,
but Lawson had by far the larger private practice. Hulke’s
articles in the early numbers of the Reports were numerous,
some of them clinical records, but many of them dealing
with histological and pathological investigations. Lawson’s
contributions were also numerous, and dealt mostly with
injuries of the eye and sympathetic ophthalmitis. In 1867
he published his collected experience on these matters in
a book entitled Injuries of the Eye, Orbit, and Eyelids. His
attention had doubtless been specially attracted to such
injuries during his service with the Army in connection with
the Crimean War. Early in 1854, when war was threatening,
Lawson joined the Army as an assistant-surgeon, and
went in March of that year with the first batch of troops
to Malta. He landed with the first troops in the Crimea,
and was present at the battles of Alma and Inkerman. He
was invalided home in July, 1855, with typhus fever, which
he contracted from some mule drivers whom he was attending,
and which left his circulation permanently impaired.
In Part III. of the Reports, Streatfield gave a description
of his operation of grooving the fibro-cartilage of the eyelid
in cases where its margin or the eyelashes turned inwards:
an operation which is still frequently performed as originally
described, or in a modified form.
In the last part of the first volume, which appeared in
January, 1859, Dixon recorded a case in which he successfully
removed a chip of steel from the vitreous chamber by
grasping it with a pair of forceps. The case is of particular
interest because it seems to have been the first in which an
attempt to remove a foreign body from the interior of the
eyeball with a powerful magnet was made, a line of practice
which has since reached a high degree of usefulness. In
Dixon’s case, the effect of the magnet was only to drag the
chip of steel into a less desirable position, so that a pair of
forceps had to be used in order to effect its removal.
Amongst the numerous interesting articles in the second
126volume of the Reports are some short contributions from
the celebrated Glasgow ophthalmic surgeon, William
Mackenzie, then in his fifty-ninth year, whose masterly
Practical Treatise on the Diseases of the Eye had obtained
world-wide reputation. After serving his apprenticeship
and passing his qualifying examination in Glasgow, he
visited the medical schools of Paris, Pavia, and Vienna; at
the latter he studied ophthalmology under Professor Beer.
In 1818 he settled for a time in practice in London, in
Newman Street, Oxford Street, and delivered a systematic
course of lectures on “Diseases and Operative Surgery of
the Eye.” Though we have no definite record of his attendance
at the Eye Infirmary, then in Charterhouse Square,
there can be little doubt that his keen interest in ophthalmology
must have taken him there. In 1820 he returned
to Glasgow to fill the Anatomical Chair in the Andersonian
University, and in 1824 he established the Glasgow Eye
Infirmary. One of his articles in the Reports deals with
glaucoma, and he was the first to point out its connection
with the increased tension of the eye—an increase of tension
which he endeavoured to relieve by paracentesis of the eye
through the sclerotic or cornea.
To those familiar with the operation for removal of
cataract, the fixing of the eyeball whilst making the incision,
by grasping the conjunctiva with a pair of toothed forceps,
seems such an obvious procedure that it is surprising that
it should not have always been employed. We find, however,
in the second volume of the Reports, an article by
France advocating such fixation as a new departure. France
was surgeon in charge of the ophthalmic department at Guy’s
Hospital. When Saunders first established a special institution
for the treatment of eye diseases, and for many years
afterwards, there were no such special departments at any
of the London general hospitals. Guy’s Hospital was the
first of the general hospitals to establish an ophthalmic
department, and by 1858 similar departments had been
127started at University College Hospital under Wharton Jones,
and at St. Mary’s Hospital under White Cooper. These
two latter surgeons also contributed articles to the Ophthalmic
Hospital Reports, which in its early days was not restricted
to work carried on at Moorfields.
With the second volume of the journal the use of paper
of a slightly yellow tint, instead of white, was commenced.
Streatfield, the editor, explained that Charles Babbage, the
mathematician, in printing his logarithmic tables, had experimented
with specimens set up on paper of various shades
and colours, and found that almost all those whom he
consulted agreed with him in giving preference to the
coloured papers. The particular tint, however, was not so
unanimously fixed upon, though yellow appeared to have
the preference. Several editions of Babbage’s Tables of
Logarithms were printed on the yellow and the white paper;
the former were always in most demand. This slightly
yellow tinted paper was apparently approved of by the
contributors and readers of the journal, as it continued in
use for several years.
In this same volume there commenced a series of articles
on “Paralytic Affections of the Muscles of the Eye,” by
John Soelberg Wells, who in 1860 became one of Bowman’s
clinical assistants.
Soelberg Wells was a tall, handsome man, of splendid
physique, and possessed of ample private means. He
graduated in medicine at Edinburgh University in 1856,
but much of his education and training, general and professional,
was conducted by German teachers, for he was
partly German by extraction. For two years previous to
his commencing work at Moorfields he studied under
Graefe in Berlin, and was for a time one of his assistants.
In his lectures and in his clinique Graefe devoted much
time and patience to teaching the diagnosis of paralytic
affections of the eye muscles, and Wells’ articles on the
subject dealt with the rules he had learnt from Graefe, to
128the great accuracy and value of which he was able to
testify.
In the third volume of the Reports commenced the publication
of a “Periscope” of foreign ophthalmological literature;
in this production Soelberg Wells’ knowledge of
German and of the Continental cliniques was of great service,
and he translated for the use of English readers articles by
Müller, Donders, and Graefe. By such means international
scientific intimacy, which is so eminently desirable, was
stimulated and promoted.
After the issue of the thirteenth number of the Reports,
Streatfield resigned his editorship, and in April, 1861, what
was termed a New Series was commenced, with the following
prefatory remarks:
“The first number was issued October, 1857, and the
publication, though not strictly quarterly, has subsequently
appeared with regularity sufficient to complete two volumes.
“The later numbers, however, have assumed a very
different appearance to those which were at first submitted
to the profession, and it has therefore been deemed necessary
to remodel the journal: at the same time, as it is the
only periodical in England specially devoted to ophthalmic
medicine and surgery, it is thought desirable to extend its
limits, by admitting reviews and periscopes, and thus to
make it more generally useful.
“It will be edited by members of the staff, and appear
under the title Ophthalmic Hospital Reports, and Journal of
Ophthalmic Medicine and Surgery.”
Apparently very heavy expenses had been incurred in
former numbers for engravings and coloured lithographs,
which made a change of management desirable, for it was
noted:
“In future the amount of illustration will much depend
on the support of the professional public, the medical
officers of the Royal London Ophthalmic Hospital having
led the way by devoting their fees, received from pupils,
to the interests of the journal.”
129
The art of perimetry or of taking the field of vision, which
has now reached such a high degree of accuracy and importance,
seems to have originated with von Graefe in 1856,
and to have been first employed at Moorfields by Hulke in
1859. In the third volume of the Reports he described
some cases, as he says, “to illustrate some forms of limitation
of the field of vision.”
Hulke’s method of procedure was similar to Graefe’s.
He placed the patient before a large blackboard at a distance
of 8 inches, covered one of his eyes, and made him fix a
chalked dot in the centre of the board, on a level with his
eyes, with the other. He then moved a white object over
the board in various directions from its margins towards
the centre and marked the places where it was first seen.
A line connecting these marks gave the outline of the field
of vision.
The obvious defect of using a flat surface, like a blackboard,
was that the various parts of the retina were not
situated at an equal distance from it. To Forster belongs
the credit of having introduced an instrument in which the
field was projected on a hollow sphere. His perimeter
consisted of a metallic semicircle capable of rotation in
various meridians, and on this general principle all other
models since produced have been constructed. Forster’s
perimeter first came into use at Moorfields in 1870.
The rapid development of surgical procedures in ophthalmology
eclipsed for a time at Moorfields the medical side.
Dr. Robert Martin, who held the post of physician from
1856 to 1884, made but little use of the opportunities it
afforded him. He did not have patients allotted to him or
any fixed time of attendance, like his predecessor. In 1867
he suffered from a severe illness which seemed to threaten
his mind, and necessitated his temporary retirement from
work; he, however, completely recovered, and no one
was appointed in his place at Moorfields during his absence.
The discovery of the ophthalmoscope opened up a new
130field for medical investigation, which was fully taken advantage
of by that distinguished neurologist, Dr. Hughlings
Jackson, who at the commencement of his career
worked at Moorfields, first with Poland and afterwards with
Jonathan Hutchinson. In a Presidential Address which
he delivered at the Ophthalmological Society in 1889, he
remarked:
“It was the luckiest thing in my early life that I began
the scientific study of my profession at an Ophthalmic
Hospital. Many years ago I had the good fortune to be
Mr. Hutchinson’s clinical assistant at Moorfields. I suppose
it is to his example and teaching that I owe the beginning
of the little scientific development I may have. At an
Ophthalmic Hospital one has the opportunity of being well
disciplined in exact observation. When a physician sees
how carefully and precisely ophthalmic surgeons investigate
the simplest case of ocular paralysis, he is getting a lesson
in exactness, and will be less likely in his own department
of practice to deal in such generalities as that a patient’s fit
‘had all the characters of an ordinary epileptic fit,’ and
more likely to take pains to describe the convulsion, the
place of onset, the march and the range of the spasm.”
Dr. Hughlings Jackson contributed many most valuable
papers to the Reports dealing with ophthalmoscopic findings
in connection with brain disease. He wrote, as he said in
one of them, “as a physician and not as an ophthalmologist,”
having studied ophthalmic medicine merely as a
help to the study of diseases of the nervous system. And,
again, in another article he remarked:
“The physician is quite as much indebted to Helmholtz
as the ophthalmologist. Defects of sight of all kinds occur
so often in affections of the nervous system that it is not
too much to say that to the student of these diseases a knowledge
of amaurosis, both in the widest and loosest, and in
the narrowest and most precise use of the word, is of
more importance than a knowledge of any other class
of symptoms.”
131
He was never tired of impressing on physicians the value
of the routine use of the ophthalmoscope. Thus he wrote
in 1889:
“I urge young physicians to study eye diseases at an
Ophthalmic Hospital or at an ophthalmic department of a
General Hospital; this nowadays needs no urging on physicians
especially interested in neurology.”
In 1863 Dr. Argyll Robertson contributed a paper from
Edinburgh to the Reports, “On the Effects of Calabar Bean
on the Eye,” in which he stated that the miotic action of
this drug had been first discovered by Dr. Thomas R.
Fraser. Besides describing its effects on the normal eye,
he enumerates several affections in which he had found its
use beneficial, but makes no mention of glaucoma. It was
apparently not until 1876 that it became employed for the
reduction of increased intraocular tension, Adolph Weber
and Laquer describing its use for this purpose about the same
time.
132
CHAPTER IX
GROWTH AND EXTENSION
When the Eye Infirmary was first built in lower Moorfields
in 1821 the district was an exceedingly quiet one; in front
of it was a large open space, which had been the old Bethlehem
Hospital burial-ground, but had not been used as such
after the removal of that Hospital to the other side of the
river in 1814.
In 1899, when the Eye Hospital was transferred to the
City Road, the district had become one of the busiest and
noisiest in the City of London. The cause of this change
was the erection of the Broad Street and Liverpool Street
Stations on the site of the old burial-ground, and on that of
a large number of courts and alleys in its vicinity, which
were cleared away for the purpose. Out of these terminal
stations there poured forth every morning the various City
workers, and back to them they streamed in the afternoons
and evenings. The railway termini became the starting-points
of various omnibuses, the roll of the wheels of which
on stony streets and the clatter of the horses’ hoofs kept up
a continuous roar. The erection of the London and North-Western
Railway’s Goods Station, to the north of the
Hospital on the opposite side of Eldon Street, added noises
at night, as well as day, in the rattle and banging of milk-cans.
To patients coming from country districts this continuous
noise proved very disturbing and detrimental. In
1870 some mitigation of the trouble was obtained by the
substitution of asphalt paving in the streets around the
Hospital in place of cobble-stones.
The increased facilities which the railways and omnibuses
afforded for approach to the Hospital tended largely to
133increase the number of patients coming to it for relief. In
1851 new out-patients numbered 11,384, and in 1878
they had increased to 19,177. To provide accommodation
for this increase, and for the larger number of patients
requiring operative treatment, it became obvious that a
new wing would have to be added on the south side of the
Hospital. A lease for the land on which it was to be erected
had, through the foresight of Dr. Farre, been obtained in
1823 for a period of seventy-seven years from the Corporation
of London. On it a stables had been built and let
off until such time as the Hospital found it necessary to
take possession. When the new building was contemplated,
an attempt was made to obtain a freehold of the site from
the Bridge House Estate, but owing to the Hospital not
being an incorporated body the negotiations fell through.
The original London terminus of the Great Eastern
Railway, opened in 1839, was at Shoreditch. In 1863 a
Bill was introduced into the House of Lords to give the
Great Eastern Railway power to extend their line to Finsbury
Circus, and to make a station there which would absorb
all the surrounding houses and the recently erected London
Institution. It was obvious that such an undertaking
would seriously interfere with the amenities of the Hospital,
and the Committee of Management drew up a petition
against the Bill pointing out how the work of the Hospital
would be interfered with if it was passed. This petition
they confided to Mr. Alfred Smee, who at that time resided
in Finsbury Circus, to be forwarded to the Earl of Shaftesbury
for presentation to the House of Lords.
The Bill was rejected and the Committee of the Hospital
passed a vote of thanks to the Right Hon. the Earl of Shaftesbury
for his important services in the matter.
Pending the final selection of sites by the different railways
for their terminal stations, the Committee of the Hospital
had to postpone their plans for enlargement, but ultimately,
early in 1868, the long contemplated building was
commenced; it did not, however, become ready for occupation
134until July, 1870; the total cost was £7,226, towards which
Her Majesty the Queen graciously contributed £100.
The reform in hospital architecture which commenced
after the Crimean War with the publication of Miss
Nightingale’s celebrated Notes on Hospitals was then still
in its infancy. St. Thomas’s Hospital, which was being
erected on the Thames Embankment at the same time as
the new wing at Moorfields, was the embodiment of her
ideas; adequate cubic space, not only in the wards but also
in the passages, being considered the most essential factor.
It has been jokingly said that, at St. Thomas’s, so large and
lofty is the children’s ward that it is difficult to find the
children. Listerism, with its passion for aseptic cleanliness,
rounded corners, and polished surfaces, had not then dawned.
The new wing at Moorfields was designed by Mr. Robert
Brass, and consisted of three floors. The ground floor was
devoted to out-patients. The first and second floor each
contained three small six-bedded wards leading out of a
long passage. Their arrangement was neither good for
administration or for ventilation. The curious device was
adopted of placing the fireplaces immediately beneath the
windows, which necessitated an elbow-shaped bend in the
chimneys. The consequence was that soot which collected
in the bends caught fire, causing from time to time considerable
consternation and excitement amongst the patients
and resident staff.
In 1866 the staff of the Hospital consisted of four surgeons
and four assistant-surgeons, but Critchett was desirous of
having an assistant-surgeon to work with him on his days
of attendance, and it was mainly at his instigation that it
was decided to appoint a fifth assistant-surgeon. To this
post John Couper, who for several years had acted as
Critchett’s clinical assistant, and who was an assistant-surgeon
at the London Hospital, was unanimously elected.
In 1867 the President of the Hospital, Mr. William
135Cotton, D.C.L., F.R.S., died, and the Governors obtained
the consent of the distinguished banker, scientist, and
statesman, Sir John Lubbock, F.R.S., M.P. (afterwards
Lord Avebury), to take his place.
In that year yet another addition was made to the surgical
staff by the election as assistant-surgeon of John Soelberg
Wells, to whose early career and scientific attainments
reference has already been made. By that time several of
the assistant-surgeons, by acting as such for five years, had
become eligible for promotion to surgeons; it was not,
however, until the new wing was opened, which provided
an additional thirty-six beds, that they were able to obtain
the full advantages of such promotion.
The establishment of special ophthalmic departments at
the several general hospitals in London caused the Governors
of Moorfields some alarm as to the ultimate welfare of their
own institution, or as Critchett picturesquely put it, “they
feared that the heart of the parent would be sucked out for
the benefit of their children, without any corresponding
advantage to the public.” It was for this reason that in
1864, at a meeting of the Governors, the following rule was
passed:
“No surgeon of the Hospital shall hold an ophthalmic
appointment in any other institution, and if any surgeon,
at the time when he becomes such, holds any ophthalmic
appointment, he shall resign the same within three months.”
The first time this rule came into operation was when
Streatfield and Hulke became surgeons. The rule only
applied to surgeons, not to assistant-surgeons. Streatfield
held the post of ophthalmic surgeon at University College
Hospital, and Hulke that of ophthalmic surgeon at Middlesex
Hospital. On their promotion at Moorfields, the Committee
of Management requested them to resign their
appointments as ophthalmic surgeons elsewhere. Hulke
readily complied with the request, as he was still able to
136maintain his connection as a general surgeon with the
Middlesex. Streatfield, however, who only practised as
an ophthalmic surgeon, was very reluctant to resign his
connection with University College. On the matter being
discussed by the Medical Council, it was found that its
members were divided in their opinions: some, like
Critchett, feared rivalry from the newly developing ophthalmic
departments at general hospitals; others welcomed
their up-growth, and saw that they were essential parts
of such institutions, both from the patients’ and the
students’ point of view. They considered it desirable that
those who enjoyed the exceptional experience afforded as
surgeons at Moorfields should be encouraged to join them,
and that, as has proved to be the case, their connection
with them would induce students requiring extended
ophthalmic training to come to Moorfields. With such
division of opinion on the surgical staff the Committee did
not at that time consider themselves able to advise any
alteration in the rule, and Streatfield had to resign his
appointment at University College Hospital.
When Couper and Soelberg Wells became eligible for
promotion as surgeons in 1873, the matter again came under
consideration; in the interval several members of the staff
had altered their opinions, and the Medical Council unanimously
recommended the abolition of the rule, stating that
“it felt assured that the cultivation of intimate relation with
General Hospitals through members of the staff is conducive
to the interests of Moorfields.” A special meeting
of the Governors was then summoned, at which the rule was
rescinded. Streatfield was fortunate enough to be reappointed
to the post he had had to resign at University
College.
James Dixon retired from the active staff of the Hospital
in 1868, after having been connected with it for twenty-five
years, and the senior surgeon for a period of twelve years.
As such he had a seat on the Committee of Management,
137where he was a regular attendant and rendered valuable
assistance. In 1870, owing to domestic bereavements, he
gave up practice and lived in retirement, occupying himself
with the study of English history and English literature.
He published a small handbook, entitled A Guide to the
Practical Study of the Diseases of the Eye, in which he said
he aimed at supplying a useful guide to those commencing
the study of eye diseases. That it fulfilled this purpose
is shown by its having passed through three editions. The
last which appeared in 1866, was brought well up to date
with the numerous developments which had taken place
since it first made its appearance.
Dixon was particularly scathing on the dry and pedantic
use of unnecessarily complicated names in the description
of affections of the eye. Thus he writes:
“It requires a more intimate knowledge of Greek than
one has a right to expect from every student of medicine
to recognise in ‘Iridoperiphakitis’ an inflamed iris and
capsule, or at once to detect the operation for closing lacrymal
fistula under such a disguise as that of ‘Dacryocystosyringokatlesis.’”
Though the world-wide reputation of Moorfields is mainly
due to the skill and scientific attainments of the medical
staff, its progress and prosperity have been to a large extent
promoted by the services of the able and devoted workers
who have in succession held the post of Chairman of the
Committee of Management. Conspicuous among them
for the interest they took in everything connected with the
Institution were Mr. F. G. Sambrooke, who died in 1871,
after having held the post for eleven years, and Mr. Philip
Cazenove, who succeeded him.
The medical staff of a hospital are the distributors of its
benefits, but in order that benefits may be distributed a
collecting department is essential, and the work of raising
funds for its maintenance falls upon the Committee of
Management and the secretary.
138
Some individuals seem to have a special flair for begging
successfully for funds for charitable purposes. The united
efforts of Mr. Sambrooke, the Chairman at Moorfields, and
of Mr. Mogford, its secretary, during the sixties, met with
a most excellent response. In the early days of the Hospital
funds were raised by means of festival dinners and special
sermons; but during the sixties, without such aid, subscriptions
flowed in both for the maintenance of the Institution
and for its building fund. Mr. Mogford attributed his
success in this matter entirely to his letters of appeal; but
it must be remembered that it was a time of peace and considerable
commercial prosperity, under which conditions
philanthropic efforts stand the best chance of success.
Excellent as Mr. Mogford was as a collector of funds, he
had certain weaknesses which in 1872 necessitated his
resignation, Mr. Robert J. Newstead being appointed to
fill his place.
In Mr. Sambrooke the medical staff had a most sympathetic
supporter in the promotion of the scientific side of
ophthalmology. During his chairmanship most liberal
grants of money were made towards the development and
upkeep of the Museum and Library. Thus a grant of £72
was made in 1864 for the purchase of a collection of ophthalmoscopic
drawings of the fundus of the eye, and when the
new museum was completed in 1870 a grant of £235 was
expended in book-cases and suitable fittings for the display
of specimens.
Charles Bader, who continued to hold the post of curator
of the Museum up to 1867, as the outcome of his experiences
published a book entitled The Natural and Morbid Changes
in the Human Eye. He was very dexterous in the mounting
of museum specimens of the eye, but unfortunately the only
two methods then known of preserving such specimens were
by means of spirit or by the use of glycerine. The former
caused them to shrink and rendered the transparent parts
opaque, and the latter, though to some extent preserving
139their transparency, caused them to swell. The introduction
of the glycerine jelly method of preserving museum specimens
of eyes by Nettleship in 1871, and elaborated by
Priestley Smith in 1883, was a great improvement; but even
with this method considerable care and attention was necessary
to prevent deterioration. It was not until the introduction
of formaline as a hardening and preserving agent,
by Professor Leber in 1894, that a really satisfactory medium
for museum specimens was found—one which would retain
indefinitely the relative degrees of transparency and colour
of the different parts which they presented during life.
On the resignation of Bader of the post of curator, Bowater
Vernon, who had been working as clinical assistant to Wordsworth,
was appointed in his place with a salary of £50 per
annum. The duties of the post were defined as follows:
“That he shall attend daily from 10 to 1, and on the
evenings of the ophthalmoscopic demonstrations, and at
such other times as may be necessary to put up and display
the morbid specimens presented.
“That he be responsible for the due keeping, cataloguing
and giving out under regulations of the books and plates
under his charge.
“That he shall prepare gradually a complete series of
preparations illustrating the normal anatomy of the human
eye and its appendages, and proceed as far as possible with
a similar series illustrative of the comparative anatomy and
pathology of the same.
“That he shall be required to report upon the microscopic
appearances of all specimens requiring such examination
and to keep a register of such examinations, if possible,
illustrated by drawings.”
The evening ophthalmoscopic demonstrations above referred
to had been started for the benefit of the students
attending the Hospital in 1864, and were conducted in turn
by the different members of the staff.
In the records of pathological specimens, published by
Vernon in the Reports in 1868, is the description of what
140must have been one of the first cases of tubercle of the
choroid which, having been seen ophthalmoscopically, was
later examined microscopically. In 1871 Vernon, being
appointed ophthalmic surgeon to St. Bartholomew’s Hospital,
resigned the post of curator of the Museum; he was succeeded
by Edward Nettleship, who held it for two years in conjunction
with that of clinical assistant to Jonathan Hutchinson.
The extensive reports of the specimens committed
to his care which Nettleship published in the Hospital
Reports for those years show with what care and diligence
he discharged the duties of the office. This, together with
the stimulating influence of his chief, Jonathan Hutchinson,
formed an excellent training for the important work which
Nettleship did in connection with ophthalmology in later
years.
PLATE XVII.
EDWARD NETTLESHIP, F.R.S.
In the middle of the nineteenth century a number of
residential schools were established in London for the children
of parents in receipt of Poor Law relief. Almost from their
commencement outbreaks of ophthalmia became very
prevalent in these schools. In 1870 Critchett was asked
to visit and advise as to the ophthalmia in one of them at
Anerley. He stated in his report that he
“found a large proportion of mild ophthalmia, which in
most cases did not render the patients incapable of following
the usual educational course, and he advised the establishment
of a ward or separate school, where all such cases
might be kept for an indefinite time until it was quite certain
that they would not relapse, where they might be under
such hygienic and medical treatment as seemed necessary,
where their instruction and education should go on as if
they were in the body of the school, and where, by prolonged
isolation, they might be prevented from acting as
sources of contagion to the healthy children in the school.”
Action was taken in accordance with this advice in 1873,
when 400 children who showed signs of ophthalmia at the
Anerley School were isolated in an unoccupied workhouse
141at Bow, which was kept going as a combined infirmary and
school with an efficient staff of teachers and nurses for
twelve months. Nettleship, having resigned his appointment
as curator at Moorfields, acted as its resident superintendent.
The experiment proved the soundness of Critchett’s
advice, but it became obvious that in some cases, more
especially those of trachoma, isolation and treatment would
have to be continued for more than a year. In 1889 a
special isolation school was erected for children affected
with ophthalmia in the Central District School at Hanwell
and placed under the charge of Sydney Stephenson. Here,
again, the success of Critchett’s policy was so marked,
that in 1897 the Local Government Board instructed the
Metropolitan Asylums Board to provide accommodation
for children suffering from ophthalmia in all the Poor Law
Schools of London. The result has been a steady and continuous
diminution in the number of cases to be dealt with
and the practical extinction altogether in these schools of
that at most intractable of all forms of ophthalmia—trachoma.
The salary for the curator of the Museum, whilst Vernon
and Nettleship held the office, seems to have been disproportionately
small to the liberal grants made for the
upkeep of the Museum itself. During his first year of
office Nettleship’s salary was only £50 per annum; at the
end of that time, “in consideration of his very valuable and
arduous services in the work of the Museum,” it was raised
to £75. When W. A. Brailey was appointed to the post
in 1874 it was found necessary to increase the salary of it
to £100, and in 1877 to £120. After increased accommodation
was made in connection with the laboratory in 1879,
courses of instruction in practical pathology of the eye were
commenced by the curator.
In 1870 ophthalmic science sustained a heavy loss by the
death of Albert von Graefe, its most zealous and successful
cultivator, in his forty-third year. His last extensive article
dealing with “The Pathology and Treatment of Glaucoma”
142was translated and published in full in the Ophthalmic
Hospital Reports at the beginning of 1871. Much as Graefe
did to extend our knowledge of the conditions which lead
to an increased hardness of the eyeball, the disasters to
which such hardness gives rise, and the means by which
they may be avoided, much was still left unexplained.
Even now, in spite of the reams which have since been
written, there is still much in connection with the subject
requiring further elucidation. In 1878 a stimulus was
given to research in this country in connection with glaucoma
by the Royal College of Surgeons setting as the subject for
the Jacksonian Prize Essay for that year, “Glaucoma: its
Causes, Symptoms, Pathology, and Treatment.” The
prize was awarded to Priestley Smith, of Birmingham, and
articles dealing with its causation were published in the
Hospital Reports for 1881 by him, and by the curator of the
Museum, W. A. Brailey. The following year Brailey
resigned the curatorship on his being appointed assistant
ophthalmic surgeon at Guy’s Hospital. His successor was
W. Jennings Milles, who had previously been house surgeon;
he, however, only held the post for eighteen months, resigning
it to go to Shanghai. He thus carried the practice
and training of Moorfields to the Far East, as others had
done to all parts of the British Empire, and to many of the
leading cities in the United States of America.
In 1873 a Canadian, Frank Buller, was appointed house
surgeon, and, returning subsequently to Montreal, became
the pioneer of ophthalmic surgery in that colony. Incidentally,
it is of interest to note that in doing so he forestalled
another young Canadian named Osler (afterwards Sir William
Osler, Bart.), who had come to Moorfields to study eye
diseases with the same end in view, but, learning there of
Buller’s intentions, he abandoned the practice of ophthalmology
for that of general medicine.
The length of time which those holding office at Moorfields
retained their posts, and the reluctance with which
143they resigned them, bears eloquent testimony to their
interest in the work of the Institution. There was then no
limit to the time that a house surgeon might retain his post,
and some continued to do so for more than three years. In
1870 Miss Boycott, who had held the post of matron for
twenty-one years, died at the Hospital. Miss Harnet
succeeded her, but not being herself a trained nurse did
little to raise the standard of nursing, which remained
during her term of office in a very primitive condition.
As the number of new out-patients attending the Hospital
continued to increase—from 19,177 in 1868 to 20,687 in
1875—it soon became evident that the newly erected wing
did not supply all the in-patient accommodation that was
required. In 1875 a plan was drawn up and adopted for
the erection of another storey on the main building at a cost
of £2,430. This was completed the following year, when
the accommodation of the Hospital became increased to
45 beds for male patients, 51 for women and children, and
4 for occasional use.
PLATE XVIII.
THE HOSPITAL AT MOORFIELDS AFTER THE ADDITION OF A NEW WING IN 1868, AND
A NEW STORY IN 1875.
Bowman and Critchett were nearly of the same age,
Bowman being a little the senior. So much had they done
to add to the fame and reputation of Moorfields that as
they approached the age of sixty, when in accordance with
the rules of the Hospital they would have to retire from the
active staff and become consulting surgeons, the Committee
of Management became anxious to find some way in which
their services could be retained. Both Bowman and
Critchett, like many of those who have come after them,
felt very reluctant to sever their intimate association with
the Hospital’s work and welfare.
Bowman, in writing to the Chairman of the Committee
in July, 1876, to inform him that the time for his retirement
was nearly due, requested that the duties of a consulting
surgeon might be defined, as so far nothing had been laid
down concerning them. Critchett also wrote at the same
time as follows:
144
“I believe that Mr. Bowman is about to send in his
resignation, and I wish to reiterate my conviction that it will
be a serious loss to the Hospital. Every week I am a witness
to the brilliant operations he performs, they are to me and
to a crowded theatre a source of pleasure and profit; professors
and students gather round him from far and near;
the prestige of the Hospital and its value both in a scientific
and benevolent aspect are enhanced by his presence, and
by the admirable work that he does. I am sure that if he
had voluntarily left us, or if he had been snatched from us,
every one attached to the Institution, whether lay or professional,
would have felt that they had sustained an irreparable
loss. I would therefore suggest that some effort
should be made to retain his services. In appointing him
to be consulting surgeon, it seems desirable that he should
have a few beds placed at his disposal for the admission of
cases that may be sent up to him or that any of his professional
colleagues may wish to place under his care; also
that he should be invited to continue his clinical teaching
and if possible give some clinical lectures at stated times.
This would be a great service to us all.”
The Committee then, in accepting Bowman’s resignation,
passed the following resolution:
“That in acknowledgment of his high reputation and
long services to this Institution the Committee request him
to continue his clinical instructions, which they are sure
will be as acceptable to the staff as to themselves, and for
that purpose are pleased for the present to place five beds
at his disposal.”
In passing this resolution and forwarding it to Bowman
the Committee acted without first consulting the Medical
Council. That body at once notified the Committee that
it was unanimously of opinion that it was an infringement
of the existing laws to assign beds thus to Bowman on
his becoming consulting surgeon. The Committee replied
by requesting the Medical Council to consider regulations
as to the duties of a consulting surgeon. The Medical
Council then proceeded to collect information as to the
145customs in force with reference to such officers at the
principal Metropolitan Hospitals. It found that in all of
them their duties were simply consultative, and that they
attended only when specially summoned at the request of
the officer in charge of the patient. The Medical Council
then advised that a similar practice should be adhered to
at Moorfields, and that arrangements might be made for
the consulting surgeons to deliver clinical lectures. The
Committee were very loath to withdraw the offer of the
use of beds which they had made to Bowman, and had
likewise extended to Critchett. The whole matter was
discussed at the Annual Meeting of the Governors, with
Sir John Lubbock, the President, in the Chair. In the end
Bowman and Critchett withdrew from all active participation
in the work of the Hospital with somewhat embittered
feelings.
Bowman died in 1892 at the age of seventy-six. In one
of his obituary notices we read the following account of his
doings after he left Moorfields:
“Fortunately, the opportunities for professional intercourse
with Bowman did not cease with his retirement
from Moorfields. Until some years later he held the leading
place at all the chief meetings connected with our specialty.
In 1880, when the British Medical Association held its
Annual Meeting at Cambridge, Bowman was President of
the ophthalmological section. Donders was present also.
The Senate of the University conferred its honorary degree
of LL.D. on both. In the following year Bowman presided
over a still more important gathering in London—the
ophthalmological section of the Seventh International
Medical Congress. The fine nature of the man, his high
ideals, simplicity, and modesty, are perhaps nowhere more
clearly shown than in the inaugural address given by him
on that occasion.
“The Ophthalmological Society of the United Kingdom
was founded in 1880, and was fortunate in having Bowman
as its president during its first three years—it was largely
through his influence that the Society rose so rapidly into
146strength and importance. Its funds, moreover, were largely
increased by his generosity. He was an ideal president:
speaking little, but always with purpose and effect, showing
interest in every communication and encouraging every
effort at good work.
“In the year 1883 the Council of the Ophthalmological
Society resolved to establish an annual lecture—the Bowman
lecture—‘in recognition of Mr. Bowman’s distinguished
scientific position in ophthalmology and other branches of
medicine, and in commemoration of his valuable services
to the Ophthalmological Society, of which he was the first
president.’ In the following year he was made a baronet
in recognition of his scientific attainments and professional
eminence. A little later, the suggestion that his portrait
should be painted and presented to him was welcomed by
a large number of his friends, in this and other countries,
and the well-known portrait by Ouless, which was exhibited
in the Royal Academy in 1889, was the result.
“Not until he was seventy years of age did Sir William
Bowman relinquish active practice, and even for some years
longer he was still at times accessible to those who specially
desired his opinion and advice.”
Critchett died in 1882 at the age of sixty-five. After
retiring from Moorfields he was appointed ophthalmic
surgeon and lecturer on ophthalmology at the Middlesex
Hospital, an appointment which he held for four years.
It afforded him a few beds for needy patients, and his son
Anderson assisted him with the out-patients. He soon
endeared himself to the students there, who valued his
teaching and the opportunity of watching his operative
dexterity. For some years he suffered from enlarged
prostate, cystitis, and granular kidney, but it did not prevent
his attending to his practice with unabated vigour, and
performing his numerous social engagements with his
customary hospitality up to the time of his death.
Several candidates who had acted as clinical assistants
presented themselves for the appointments on the staff
rendered vacant by the retirement of Bowman and Critchett,
but all withdrew in favour of Waren Tay and James Adams,
147both of whom were assistant general surgeons at the London
Hospital.
After the publication of Donders’ great work in English
On the Anomalies of Accommodation and Refraction of the
Eye, by the New Sydenham Society in 1864, and Soelberg
Wells’ smaller book, which embodied Donders’ teaching,
On Long, Short, and Weak Sight, sight-testing and the
correction of errors of refraction with glasses grew progressively
in importance.
The prescription of lotions or ointments for the eyes
took far less time than the estimation of refractive errors
and the prescription of glasses, and with the increase of
sight-testing the length of time occupied in dealing with
out-patients became considerably prolonged. At first it
was only the correction of the grosser errors of refraction
which received attention, but as the methods for their
estimation improved, and the importance of even small
errors became recognised, the amount of refractive work
steadily increased.
The length of time many out-patients had to wait before
they received attention became a source of anxiety, extending
over many years, not only to the Committee of
Management, but also to the surgical staff. The surgeons’
time was fully occupied with the investigation of diseased
conditions and with operating; they had to depend mainly
for the carrying out of this refraction work on the devotion
and goodwill of their clinical assistants, who, being purely
voluntary workers, could not always be relied upon to stay
for an indefinite time.
Many measures were tried to overcome the difficulty.
Hulke, who had a passion for punctuality, was never tired
of urging the value of his special virtue on all concerned.
Though a painfully punctual individual on a medical staff
may at times be very trying to his colleagues and assistants
it is no doubt that he is a valuable asset to the institution
with which he is connected. Everybody knew at Moorfields
148that on Hulke’s days of attendance they had to be early
risers, with the result that the work was finished more
expeditiously.
Much trouble in connection with the refraction work of
the Hospital would probably have been avoided if the plan
which has recently been adopted, of paying an honorarium
to one clinical assistant for each surgeon, had been sooner
resorted to. It was originally recommended by the Medical
Council in 1877, but the Committee could not for a long
time see its way to increase so considerably the Hospital’s
annual expenditure.
Jonathan Hutchinson, as has already been mentioned, was
a man who took the widest interest in all diseased conditions;
the one subject which did not specially attract him
was refraction work. As the amount and importance of it
increased, and after he became deprived of the zealous help
of his two able assistants, Tay and Nettleship, he felt he
could no longer conscientiously carry out all the duties of
his post, and in 1878 resigned his appointment on the staff.
No man at Moorfields ever made more thorough and
effectual use of the clinical work which it placed at his
disposal than Jonathan Hutchinson. For several years he,
together with Wordsworth, edited the Hospital Reports,
and it was during that time that they were conducted
with the highest degree of efficiency and regularity. The
“Periscope” in those years, which was mainly the work
of Waren Tay, formed an excellent and very complete
review of foreign ophthalmic literature. Hutchinson’s own
articles were numerous, containing groups of well-recorded
cases, designed to illustrate new and interesting observations.
In the November number of the Reports for 1871 he
published “Statistical Details of Four Years’ Experience in
Respect to the Form of Amaurosis supposed to be due to
Tobacco.” It was his third article on the subject; the first,
in which he suggested a connection between excessive
149smoking and affections of the optic nerve, having appeared
in 1864. His attention became attracted by the almost
exclusive occurrence of what was then called “idiopathic
symmetrical amaurosis” in the male sex. He considered
all the possible causes which might account for such a
prevalence in one sex only, and found the tobacco hypothesis
the most probable. His researches showed that there
was little evidence of any other affection of the nervous
system in these cases, and that all of them were excessive
smokers, most of them having used shag tobacco. Having
watched them for some time, he discovered that when the
disuse of tobacco was real and complete vision generally
improved.
The less frequent issue of the Reports after Hutchinson’s
departure, and the abandonment of the “Periscope,” was
due to two things—the establishment of the Ophthalmological
Society in 1881, and the commencement of the
Ophthalmic Review in 1882.
The unexpected vacancy on the staff caused by Hutchinson’s
resignation was filled by the election of John Tweedy
who was a clinical assistant to Streatfield, and held the
post of assistant ophthalmic surgeon at University College
Hospital.
In 1879 Philip Cazenove resigned the post of Chairman
of the Committee of Management which he had held for
eight years, and in doing so presented the Hospital with
a gift of £1,000. Charles Gordon, whose name was, and is
still, well known in connection with gin, was appointed to
succeed him.
The Hospital suffered a severe loss by the death of
Soelberg Wells in December, 1879; his health had been
failing for some time, and he had been granted repeated
periods of leave from his work at the Hospital on account
of it. His Treatise on the Diseases of the Eye, first published
in 1869, ran through three editions, and was translated into
German and French. It was for a long time the standard
150textbook on ophthalmology, having the supreme virtue of
combining the best teaching and practice of continental
writers on the subject with those of our own country, an
undertaking for which Soelberg Wells was particularly well
fitted, owing to his familiarity with the continental clinics
and his linguistic abilities.
Robert Lyell, who had worked as Hulke’s clinical assistant
and who was an assistant general surgeon at the Middlesex
Hospital, was elected in Wells’ place. He was a man who,
as a student, had had a brilliant career and had obtained
the highest qualifications and distinctions. With his appointments
at the Middlesex and Moorfields, the way seemed
open to him for a successful and prosperous future. Unfortunately,
in the summer holiday of 1882, he contracted
pneumonia, and the opening session at the Middlesex
Hospital Medical School in October, at which he was to
have delivered the Introductory Address, was saddened by
the news of his death.
For the vacancy created by Lyell’s death several candidates
presented themselves, but ultimately withdrew their
applications in favour of Nettleship, who already held the
post of ophthalmic surgeon at St. Thomas’s Hospital. This
was the last appointment on the staff at Moorfields which
was created by a vote of the Governors. In 1883 the
Medical Council informed the Committee of Management
that in its opinion “the present mode of election of the
honorary medical officers did not secure the best interests
of the Hospital.” A joint conference was held at which
it was decided to recommend that in future the election of
honorary officers should be invested in a committee, and
that this election committee should consist of the Board
of Management, together with six honorary medical officers,
the quorum to consist of seven; and that canvassing should
be prohibited on the part of any candidate under pain of
disqualification. These recommendations were agreed to
at a meeting of the Governors, and in this way all subsequent
151elections have been conducted. At the same time it was
also agreed that the Fellowship of the Royal College of
Surgeons of England should be the only requisite necessary
for eligibility as a candidate for a post on the surgical staff.
PLATE XIX.
WAREN TAY
Manners and characteristics, besides being inherited by
children from parents, are also often acquired by pupils
from teachers. The latter most frequently occurs where
the teacher possesses a strong and impressive personality,
and the taught are earnest and devout. This transmission
of traits is not uncommonly met with in the medical profession,
where some dominating member of a hospital staff
impresses his individuality on those who work under him.
A conspicuous example of this occurred at Moorfields, where
Waren Tay and Edward Nettleship, who worked as clinical
assistants to Jonathan Hutchinson, acquired, probably
quite unconsciously, not only his mannerisms, but even his
method of speech. Tay, like Hutchinson, became skilled
in the practice of several different branches of his profession;
like him, he became a general surgeon at the London
Hospital, a specialist in skin diseases at the Blackfriars’
Hospital and in eye diseases at Moorfields. It has already
been mentioned how Hutchinson worked under Sir William
Lawrence, and acquired from him the habit of collecting
and collating the notes of clinical cases; in this most valuable
method of advancing our knowledge of the natural history
of disease Hutchinson found a most able disciple in Edward
Nettleship, who, in the excellent field for its employment
which Moorfields Hospital afforded him, made the most
extensive use of it, more especially in tracing out the hereditary
transmission of diseases and deformities.
152
CHAPTER X
ANTISEPTICS, BACTERIOLOGY, AND LOCAL ANÆSTHESIA
Joseph Lister’s first paper on his method of preventing
the access to wounds of germs which cause putrefaction
appeared in the Lancet in 1867. It was not, however, until
several years later that London surgeons began to adopt
his methods, and it was not until the teaching and training
of bacteriological laboratories exerted their influence that
the practice of Listerian principles became generally and
efficiently carried out.
Wounds of the eye, due to the protective influence
afforded by the eyelids, and to their continuous irrigation
with tears, which normally possess bactericidal powers,
were less liable to septic infection than those in other parts
of the body. Hence, prior to the introduction of antiseptic
methods, the operations of ophthalmic surgery were less
frequently complicated by septic troubles than those of
general surgery.
Where the tear duct became obstructed and discharge
from the tear sac regurgitated into the eye, and where contaminated
instruments were introduced into the interior of
the eyeball, wounds became infected and disastrous consequences
ensued. The danger of operating for cataract
when there was obstruction to the tear duct was soon
recognised, and it became a routine practice to investigate
the condition of the tear passages before embarking on such
operations. It was not until some time after the introduction
of antiseptic surgery that the sterilisation of the
instruments used in ophthalmic operations became general.
In the third edition of Soelberg Wells’ Treatise on Eye
153Diseases, published in 1873, which may certainly be taken
as picturing the high-water mark of ophthalmic practice
at that date, no mention is made of the use of any antiseptic
precautions in connection with operations on the eye.
The after-treatment of eyes operated on for extraction of
cataract at Moorfields in 1876 is described by A. S. Morton,
who was then house surgeon, as follows:
“As soon as the operation was completed the lids of each
eye were fastened by a very narrow vertical strip of plaster
to prevent involuntary opening of the eye during recovery
from the anæsthetic, then a piece of lint, on which was
placed a layer of cotton-wool for each eye, and over all a
bandage. The eyes were dressed each morning and evening
after the operation, being gently bathed with tepid water
and the lids oiled with a soft brush to prevent the dressing
sticking to them. The patients were kept in bed till the
third day, and the lids never opened till the fourth or fifth
day after the operation, unless there were indications of
mischief. About the end of a week they were handed over
to the nurse to dress, and in about nine or ten days were
allowed to have their eyes open, but very carefully shaded.”
Confinement in a dark room was for a long time regarded
as an essential part of the treatment of certain eye diseases.
Some elderly people still retain vivid recollections of having
to submit to this unpleasant form of treatment for some
inflammatory eye affection in their youth. The admission
of light to the eye during the first few days after an operation
for cataract was believed to excite inflammation, and
elaborate precautions were taken to avoid it.
The cataract wards at Moorfields were darkened with
double blinds, and when the dressings on the eyes were
being changed, a nurse stood at the end of the bed holding
a candle which she cautiously shaded with her hand to
prevent any of its rays falling on the patient’s eyes. Some
of the senior members of the staff received rather a shock
when a venturesome house surgeon, mindful of Florence
Nightingale’s dictum that “a dark room is always a dirty
154room,” had the blinds in the cataract wards drawn up,
letting the sun’s blessed rays stream in, whilst the patient’s
eyes were tied up or shaded with dark glasses.
The practice with regard to the instruments in the pre-antiseptic
days was for the nurse to wash them when used
in ordinary tap-water, after which they were stored in their
velvet-lined cases. From these they were transferred
without further preparation, and handed to the surgeon for
the next operation on a tray lined with green baize.
Out-patients and in-patients were operated on in the
same theatre, the former coming to it just as they presented
themselves at the Hospital, without any change of clothing.
The surgeons themselves made no change in their costume
when operating, and the nurses wore no regular uniform.
The former violent “antiphlogistic” treatment of extensive
bleeding, sweating, vomiting, and purging, for inflammatory
affections of the eyes, had in the seventies been
given up, chief reliance being then placed on the use of
belladonna and poppy-head fomentations, “astringents,”
and the application of leeches, blisters, and setons to the
temples.
The year 1872 was an unusually disastrous one at Moorfields
as regards operations for the removal of cataract, as
many as 20 per cent. having resulted in failure. A joint
meeting of the Committee and the medical staff was held
to consider the matter, and the disasters were attributed
to the presence in the Hospital at the time of a large number
of infectious cases, changes in the nursing staff, and the
absence of the house surgeon on a holiday. Measures to
improve the ventilation of the wards were taken, an assistant
house surgeon was appointed, and a long standing request
of the Medical Council for the appointment of a special
night nurse was at last acceded to.
At the International Congress of Medicine held in London
in 1881, a discussion took place at the ophthalmological
section on the employment of antiseptics in ophthalmic
155surgery. Antiseptic surgery at that time consisted in the
use of carbolic acid in the form of a spray, as a lotion, and
in the dressings. Professor Horner of Zurich, who opened
the discussion, quoted his statistics of cataract operations
from 1867 to 1881 to show that by the use of antiseptics
there had been a decrease in the number of cases of suppuration
from 6·6 to 1·1 per cent. Some speakers thought
the good obtained from the use of carbolic acid was counter-balanced
by its irritating properties. Bowman, who presided
over the section, in his Inaugural Address, made the following
wise remarks which may be taken as foreshadowing the
adoption of aseptic as opposed to antiseptic measures:
“I presume that no one nowadays will question the evils
we are so familiar with in our practice, and which have
so often marred the intention of well-devised operations
skilfully performed, but where, as we hear it said, Nature
has failed to do her part, to second the effort of the surgeon
by a process of repair. The study of the causes of such
failures and of the means of obviating them, constitutes far
the most brilliant page of modern surgery; and in other
sections of this Congress, while the name of Lister will be
applauded, the wide questions he has raised, and in raising
has so often cleared up, will receive the full consideration
they call for.
“In the case of the organ of sight, specially constituted,
and in some respects screened from injury as it unquestionably
is, there are reasons why the application of precautionary
antiseptic measures, though the principle of them must
still assert itself, should take a somewhat special form.
Owing to the local structural conditions they may apparently
be often more simple, though the possible need of the more
elaborate of them should never be allowed to fall out of
view.
“The tears are a secretion as pure from extraneous
particles as is the filtered air in the recesses of the lungs.
They are poured out under cover, in the right place, in
quantity suitable to the need; while the lids diffuse them
over the conjunctival surface ere they escape to their proper
channels. Their useful and multiple office is performed in
a way so simple and so perfect, that no art, however skilful,
156could pretend to equal it. We should ponder well the deep
marvels of adaptation of means to ends, and take heed that
we do not hinder exquisite Nature by meddlesome or
needless interference, by the nimia diligentia Chirurgorum,
but only lend it tender and judicious help by our dressings
and our methods. We should always still be able
to apply the words of our great poet, ‘The Art itself
is Nature.’”
In 1876 A. S. Morton, the house surgeon at Moorfields,
recorded that out of 146 cases of extraction of cataract
5·47 per cent, had suppurated, and that 12·3 per cent, had
suffered from severe iritis. In an analysis of the results
of cataract extraction at Moorfields for five years, from
1889 to 1893, the house surgeon, C. D. Marshall, records
the number in which suppuration occurred as 1·69 per cent.
The preparation and after-treatment of patients undergoing
this operation during those years he describes as follows:
“I shall here only mention the special points connected
with the eye, the general examination and preparation of
the patient being precisely the same as that adopted previous
to the performance of any surgical operation. The lids
and parts around the eye are carefully washed with soap
and hot water over-night, and a pad which has been wrung
out in a 1/4000 solution of the perchloride of mercury is
applied. On removing this the next morning one is able
to obtain a good idea as to the state of the conjunctiva; if
the lids be gummed together, the operation is deferred until
a more satisfactory state of things is obtained. If, however,
there is nothing to contraindicate the performance of the
operation the eye is anæsthetised with a 2 per cent. solution
of freshly prepared cocaine and the conjunctival sac is washed
out with a good stream of either warm boracic or perchloride
lotion. The instruments are boiled before being used and
kept in carbolic acid lotion 1 to 40.
“After the operation both eyes are as a rule closed for
a day or two, and tied up with pads of Gamgee tissue made
of the double cyanide wool. The operated eye is kept
bandaged for about a week, and after that dark goggles are
worn.”
157
John Couper, who was a general surgeon at the London
Hospital as well as an ophthalmic surgeon at Moorfields,
was one of the earliest and most enthusiastic pioneers of
antiseptic surgery, practising it consistently before Lister
came to London. At Moorfields he was one of the first to
welcome its application to ophthalmic surgery.
PLATE XX.
JOHN COUPER.
In the following appreciation, written by Sir John Tweedy,
we have recorded a most faithful and striking word-picture
of John Couper’s characteristics:
“When I first knew John Couper he was assistant-surgeon
to the London Hospital and assistant-surgeon to the Royal
London Ophthalmic Hospital, Moorfields. With his work
as a general surgeon I was but slightly acquainted, but I
do know that he was one of the first and most ardent of the
disciples of the Listerian doctrine, and practised the Listerian
method with patient confidence. It was my happy privilege
to have as colleagues at Moorfields George Lawson and
John Couper, and to work side by side with them for many
years. Lawson was one of the best ophthalmic surgeons I
have ever known. Couper’s gifts were of a different order.
Although a good surgeon and skilled operator, his qualities
were those of an ophthalmic physician. Facile princeps
among the ophthalmoscopists of the day, he was one of the
first in this country seriously and scientifically to study
problems of the errors of refraction, and especially of
astigmatism. His diagnostic skill and his careful method
of investigation attracted a body of thoughtful pupils, not
a few of whom afterwards attained a notable distinction.
Couper’s was a charming personality; he was gentle, courteous,
conciliatory, but strong in opinion and tenacious of
principle. His mental temperament was essentially sceptical.
Not unbelief, not mis-belief, but hardness of belief was his
intellectual attitude to all surgical and scientific questions.
He did not believe easily or lightly, but only when convinced
by the force of reason and by the potency of well
observed facts. His scepticism may not have been an
unmixed benefit as a teacher to beginners, but it was a
real advantage at a Hospital like Moorfields, where many
of the pupils, assistants, and visitors were actual or potent
experts. His hardness of belief often provoked keen but
158friendly controversy, sharp but generous differences of
opinion, which rarely failed to elucidate truth, and open up
fresh avenues of knowledge. No man was ever the worse
for a difference of opinion with Couper, and most of us
were often much the better. Thought was stimulated,
reasons were clarified, opinions modified and amended, or
maybe strengthened and confirmed; and, above all, a valuable
lesson was learnt in mutual respect and tolerance.
Couper was indeed a lovable man, a true friend, a staunch
and loyal colleague. To have known him, and to have
been so long associated with him, is an abiding satisfaction,
and the recollection of a friendship unclouded throughout
many years is a precious possession.”
John Couper was not only a pioneer in the use of antiseptics
in ophthalmic surgery, but also in the accurate
correction of even small errors of refraction with glasses.
He was most emphatic and uncompromising in advising
his patients to wear their glasses constantly. A young lady
with a very pretty face, who felt very loath to detract from
its charms by wearing glasses, asked pitifully: “Please,
Mr. Couper, how long shall I have to wear these glasses?”
Couper replied by asking her her age, which was eighteen.
“Well,” said Couper, “the average age of woman is three
score years and ten: eighteen from that makes how long?”
Couper made use of his ophthalmoscope not only to
explore the fundus of the eye, but also as an optometer for
the estimation of refractive errors. He commenced to do
so before the practice of “retinoscopy” came into use,
and having acquired considerable skill in the method, continued
to employ it in preference to the easier one. To
render the ophthalmoscope as serviceable as possible as an
optometer, he introduced several modifications in it. He
found it most desirable to have only one lens to look through
behind the sight hole in the mirror at a time, and to be
able to bring the eye of the observer as near as possible
to that of the one being examined. For these purposes he
substituted a chain of lenses in place of the usual disc, and,
159as he considered it necessary to have as many separate lenses
available as are contained in an ordinary trial case, the
handle of his ophthalmoscope in which the lenses circulated
became of considerable length. So long, indeed, was it
that Couper had to arrange with his tailor for the construction
of a special coat pocket in which he could carry it.
The method of estimating errors of refraction of the eye
by what is now known as “retinoscopy” was first introduced
as a systematic method by Cuignet in 1874, under
the inappropriate name of “keratoscopy.” Bowman had,
however, ten years previously called attention to the possibility
of diagnosing regular astigmatism by using the
mirror of the ophthalmoscope to reflect light into the eye,
much in the same way as for detecting slight degrees of
conical cornea.
An article advocating the use of Cuignet’s method, by
Litton Forbes, appeared in the Ophthalmic Hospital Reports
in 1880, and another, descriptive of its optical basis, by
W. Charnley, in 1882.
In 1883 John Cawood Wordsworth, having reached the
age of sixty, retired from the active staff after thirty-one
years of service, and died three years later from angina
pectoris. He was described as an admirable example of
the genuine “dignity and reputation of the profession,”
and as “unobtrusive almost to a fault.” Though, together
with Hutchinson, he was for several years editor of the
Hospital Reports, he contributed but little himself to the
literature of ophthalmology.
He resided and commenced to practise in Finsbury Square;
for some time his private patients were but few and far
between. He employed a page boy who was instructed to
fetch him from the Hospital if any patient should happen
to come whilst he was engaged there. One day the boy
came to the Hospital in hot haste to announce the arrival
of a patient. “Will he wait until I get round?” Wordsworth
asked the boy. “I am quite sure he will,” replied
160the boy, “for I have locked him in.” Wordsworth then
explained to the house surgeon and his assistants how they
must carry on the work for a time as he had been called
away to see a private patient; they helped him on with his
coat, and away he went with the boy. To their great
surprise he returned after only a few minutes. Noting the
surprised look in their faces, he sadly explained that it was
only the tax collector.
PLATE XXI.
R. MARCUS GUNN.
Marcus Gunn, who had previously been the house surgeon,
was appointed to succeed Wordsworth; he was the first
officer who had so served the Hospital to become elected
as a member of its honorary staff. He had been a particularly
able and energetic house surgeon, having instituted
a new system of note-taking for the in-patients, which has
proved so satisfactory that it is still in use at the present
time. His intimate acquaintance with the nursing and
domestic arrangements of the Hospital proved of considerable
value in the reforms and general upheaval which took
place shortly after he was appointed. Previous to his
becoming house surgeon, he had studied ophthalmology in
Vienna under Jaeger; so impressed was he with the systematic
courses of instruction carried on at that school,
that on his appointment as assistant-surgeon he at once
set to work to institute more regular and systematic teaching
at Moorfields. He himself conducted regular classes in
ophthalmoscopic examination at stated intervals, which
became so popular that the list of students which could be
taken at any one class was always filled up some time in
advance.
Early in 1884 Dr. Martin resigned the post of physician,
and Dr. Stephen Mackenzie (afterwards Sir Stephen
Mackenzie), a physician at the London Hospital, was
appointed in his place. He resided at that time in Finsbury
Square, and it was easy, therefore, for him to attend at the
Hospital when requested to do so either by a member of
the surgical staff or the house surgeon. He took a keen
161interest in medical ophthalmology, and contributed several
communications on the subject to the Ophthalmological
Society, of which he was one of the first secretaries.
During a large part of the nineteenth century the district
of Finsbury was a fashionable residential medical quarter
of London; Finsbury Square, Finsbury Pavement, Finsbury
Circus, Broad Street, and St. Helen’s Place, at one time
swarmed with physicians and surgeons. The City and its
adjacent districts were then largely inhabited by prosperous
business folk and their families; as these migrated westwards,
the doctors naturally followed suit. Many of the
younger members of the staffs of St. Bartholomew’s, Guy’s
and the London Hospital lingered on so as to be within
easy distance of those Institutions. It gradually became
the custom for those residing around Moorfields Hospital,
who were interested in ophthalmology, to foregather
there in the house surgeon’s room on certain evenings
in the week to discuss cases and other matters of mutual
interest. So far back as 1866 Jonathan Hutchinson records
in the Ophthalmic Hospital Reports how he read a paper at
the “Moorfields Club,” It was at one of such informal
meetings that early in 1880 a circular was drawn up suggesting
the formation of an Ophthalmological Society. This
was sent to the leading ophthalmic surgeons in the three
divisions of the United Kingdom, and met with a cordial
response. In June of that year the first meeting of “The
Ophthalmological Society of the United Kingdom” was
held, at which William Bowman, who had been appointed
President, delivered an Inaugural Address.
Pasteur’s researches on fermentation and putrefaction,
and Lister’s application of them to the treatment of
wounds, raised the study of bacteriology to the dignity of
a science.
Improvements in the microscope by the introduction of
high power oil-immersion lenses made it possible to study
the morphology of micro-organisms, and the introduction
162by Koch of improved methods for obtaining pure cultivations
of them paved the way to the investigation of their
life-history and bio-chemical reactions.
During the eighth decade of the nineteenth century the
connection of several different micro-organisms with diseases
of the eye was discovered, which aided in the study of their
natural history and treatment.
In 1884 incubators and other bacteriological apparatus
were installed in the pathological laboratory at Moorfields
to allow of these new methods of investigation being carried
out.
In 1882 Koch demonstrated that a specific organism
could be separated from tuberculous tissue and cultivated
outside the body, which would reproduce tuberculosis when
inoculated. A new test was thus supplied for the recognition
of tuberculous lesions, and some affections of the eye,
of which the real nature up to that time had been doubtful,
were by its means proved to be tubercular. J. B. Lawford,
who, on the resignation of Jennings Milles, had become
curator of the Museum, was among the first to detect Koch’s
bacillus in the tissues of the eye.
In 1890 Koch introduced his original form of tuberculin
treatment, which, before its effects had been adequately
investigated, raised the greatest expectations, and caused
a rush to Berlin of consumptives from all parts of the world.
This treatment was tested in January, 1891, on a patient
at Moorfields, under Waren Tay, with tubercular nodules
in the iris at the margin of the pupil. So situated it was
possible to watch the effects of the treatment on them with
the greatest precision. The nodules, which were at first
separate, gradually increased in size and became confluent,
ultimately invading neighbouring parts and necessitating the
removal of the eye. Besides demonstrating the failure of
the treatment, this case was of interest, because the administration
of an injection of the tuberculin after the eye
was removed produced a general reaction, thus showing the
163presence of some other focus of tuberculosis which had not
been detected, and from which most probably the eye had
become secondarily affected.
PLATE XXII.
JAMES E. ADAMS.
From a painting by a patient upon whom he had performed the
operation of extraction of cataract.
The employment of bacteriological investigation in connection
with the discharge from eyes affected with ophthalmia
resulted in the discovery of two new forms of bacilli—the
Koch-Weeks bacillus in 1887, and the Morax-Axenfeld
diplo-bacillus in 1896—each receiving a dual name due to
their independent and almost simultaneous recognition by
two different workers.
The recognition of these and other micro-organisms
which had been discovered in connection with other affections
(such as the gonococci, Klebs-Löffler bacilli, pneumococci,
streptococci, and staphylococci), as the specific
agents in the causation of the different forms of ophthalmia,
led to a new means of classifying them, the previous
classifications being based on the clinical appearances
alone.
The rapid advance in bacteriology, and the introduction
of vaccine treatment arising out of it, tended to make its
study and practice more and more a special branch of
medicine. In 1907, after the Hospital had been removed
to the City Road, it was found necessary to erect a special
laboratory for its development and to appoint a special
officer to take charge of it.
The premature decease of several members of the surgical
staff just as they had attained the acme of a successful
career has already been referred to; the cruellest fate of
all was that which befell James Adams, who, whilst engaged
in restoring and saving the sight of others, was doomed to
watch the gradual failure of his own to complete and
irremediable blindness. This, too, whilst he was in the hey-day
of life, a successful general surgeon at the London Hospital
and ophthalmic surgeon at Moorfields. A man full of the
joy of life, deservedly popular with his colleagues and
students, he combined scientific with spotting interests,
164and was able to snatch a day here and there from his arduous
duties to follow the hounds.
A complete rest having failed to prove of any benefit to
his gradually increasing darkness, he, in the latter part of
1884, found it necessary to resign all his appointments.
William Lang, who had for some time worked with him as
clinical assistant, and who held the appointment of ophthalmic
surgeon at the Middlesex Hospital, was elected as his
successor at Moorfields.
Cocaine is derived from the leaves of a plant, Erythroxylon
coca, which grows in Peru and Bolivia. It was originally
named “khoka,” meaning “the tree of trees.” Joseph
de Jussieu first sent a specimen of the plant to Europe in
1750. The practice of chewing its leaves as a means of
appeasing hunger and thirst, and relieving fatigue, had for
long been a custom among the natives of South America.
The famous long-distance walker, Weston, employed them
in this way when, in the seventies, he trudged round and
round the Agricultural Hall in his efforts to cover the longest
possible distance in the shortest possible time. In 1872
Dr. Hughes Bennett of Edinburgh showed that cocaine,
when applied to a mucous membrane, produced anæsthesia,
but no use was made of it in practice.
It was Karl Roller of Vienna, in 1884, who first made
applications of it to the eye, which resulted in its employment
in ophthalmic surgery. Koller’s original article,
describing the physiological effects of the drug on the eye,
was so complete that there was but little left to be added.
A description of it was given at the meeting of the Heidelberg
Ophthalmological Society in 1884, and a solution of
the drug was brought straight from there to Moorfields in
the latter part of September of that year. The first operation
performed under its influence in this country was a
tattooing of the cornea by Marcus Gunn. Its employment
soon became general in all operations on the eye in which
there was not much congestion, and in which the tension
165of the globe was not increased. The supply at first was so
small and the demand so great that its price rapidly rose
to a guinea a grain.
The substitution of local for general anæsthesia in cataract
operations aided materially in their safety and success.
The dreaded effects on the eye of vomiting and reaching
on the recovery from the administration of ether or chloroform
were avoided, and the aid of the patient in turning the
eye in any direction did away with the necessity of dragging
it into suitable positions, which was frequently requisite
when the patient was unconscious. The immediate result
was a considerable decrease in the number of cases in which
the vitreous humour escaped, and the possibility of greater
precision in the adjustment of parts after the removal of
the cataract.
At first nothing was known of its toxic effects, and the
small amount absorbed when dropped into the eye did not
give rise to them. It was only when attempts were made
to anæsthetise large areas of the skin by subcutaneous
injection that they became manifest.
In 1884 the surgical staff had become so dissatisfied with
the system of nursing at the Hospital, and with the standard
of the nurses employed, that they requested a conference
with the Committee of Management on the matter. At
this conference it was agreed that no satisfactory improvement
could be effected without having at the head of the
establishment a lady who had herself been efficiently trained
as a nurse. Miss Harnet, who then held the post of matron,
was advised to tender her resignation. This she did, a
pension being granted her. The new matron, selected from
a number of candidates for the post, was Mrs. Peel, who
had been trained at the London Hospital, where she had
also held the post of sister: later she had been matron at
the Newcastle Infirmary.
Shortly after her appointment, the head nurse was detected
receiving money from a patient; this being her second
166offence of the sort she was at once dismissed. After her
departure it was discovered to have been a common form
of corruption, notwithstanding the warning notices concerning
it posted about the Hospital. The forced resignation
of the former matron and the summary dismissal of the
head nurse caused consternation amongst the other members
of the nursing staff, who combined together to make things
unpleasant for the new matron. She received, however,
the support of the medical staff and the Committee of
Management, and ultimately a complete change of the
nursing staff was effected, fully trained nurses being engaged
to fill all the most important posts.
In April, 1885, occurred the sudden and unexpected
death of Streatfield, who was at that time the senior surgeon.
As has already been mentioned, he was a most dexterous
operator, and also possessed of considerable ingenuity,
which manifested itself sometimes in peculiar ways. A
few years before his death he had had constructed a gigantic
model of an eye, on which he could demonstrate to students
mechanically the various stages of operative procedures.
As he truly pointed out, in operations on the eye, the smallness
of the organ and of the parts dealt with renders it impossible
for any, except those in close proximity to the
operator, to see clearly what is taking place. He, therefore,
devised this model, constructed with all its dimensions
ten times the size of the normal eye. The eyelids and
sclerotic were of white felt spread over wire, the cornea of
glass, the iris of indiarubber, the lens of xylonite, and the
external muscles of the eye of linen. Models of the instruments
employed were of wood, also ten times their actual
size, except as regards their handles, which to allow of the
manipulation of such weapons had to be reduced. By
various artfully arranged mechanical contrivances, the lens
could be made to present and escape from the eye above
the cornea when a certain spot on the sclerotic was touched,
and the cornea then roll back into position. Ingenious as
167all these contrivances were, the effect of the model when
exhibited was to excite mirth more than anything else. It
passed into the possession of the Hospital after Streatfield’s
death, but no further use was made of it.
PLATE XXIII.
A. QUARRY SILCOCK.
A. Quarry Silcock was elected to succeed Streatfield;
besides being an ophthalmic surgeon he was a general
surgeon attached to St. Mary’s Hospital. At one time, as
has been shown, all members of the surgical staff of the
Hospital had to be either a general surgeon or a demonstrator
of anatomy connected with a general hospital. This
rule had, however, been altered, it being thought only
necessary to insist on candidates possessing the diploma of
Fellowship of the College of Surgeons of England, as a
guarantee that they had attained a high standard of general
surgical efficiency. Silcock was the last member of the
staff appointed who combined the practice of ophthalmology
with that of general surgery; all those since appointed,
though Fellows of the College of Surgeons, have restricted
their practice to ophthalmology. With the growth of knowledge
the speciality of ophthalmology had come to consist
of much besides mere dexterity in the performance of
certain surgical operations. Here may be aptly quoted
what the late Dr. James Anderson wrote with reference to
it in 1889:
“It seems to me the best and most hopeful feature of
ophthalmology that it has relations, closer or more remote,
with every branch of medicine and surgery—indeed, with
almost every branch of science.”
168
CHAPTER XI
THE SELECTION OF A NEW SITE, AND THE
ERECTION OF THE NEW HOSPITAL
The condition of the Moorfields Hospital in 1884 may be
compared to that of a man wearing a suit of clothes fitted to
him in his youth, which had since been added to, patched,
and darned, to cover his nakedness. The result was that he
not only presented an incongruous appearance, but lived in
constant fear of fresh dilapidations.
To carry the analogy still further, those who would be
called upon to find funds for a fresh suit, and who had
taken pains to make the patches, desired to leave matters
as they were. Whilst the man himself, who had to wear
and work in his old-fashioned clothes, was all agog for a
new rig-out.
The Hospital erected in 1821 was in keeping with the conceptions
of the time and adapted for the accommodation
then required. With the new ideas which arose out of
Florence Nightingale’s teaching, and later as the outcome
of bacteriological investigations, the general principles for
hospital construction became completely changed. Though
the original Moorfields Hospital was added to and altered
to meet new requirements, it became obvious to the rising
generation of medical men working there that it could
never be converted into an up-to-date institution. It took
time, however, before the Committee of Management as
a body could be induced to look at the matter in the same
light, especially its older members who had taken part in
raising funds and arranging for the additions.
In 1884 a piece of building land in Eldon Street to the
west of the Hospital became vacant, and the Controller of
169the City of London offered to lay any proposal the Committee
of Management might feel inclined to make concerning it
before the Bridge House Estates Committee. Though
urged by the Medical Council to acquire it, the Committee
of Management replied that it did not feel able to
tender.
During the next three years circumstances arose which
gradually convinced the Committee that there were irremediable
defects in the Hospital as regards accommodation,
ventilation and sanitation. The beds were always
full, and the waiting-list of patients requiring in-patient
treatment grew in dimensions. The cubic space per patient
in the wards was very deficient, and no cross-ventilation of
them was possible. There were no day rooms in which
patients not confined to bed could take their meals. There
was no passenger lift to convey patients who had been
operated on to the upper floors, so that they had to walk
up a narrow staircase. There were no bath rooms, and
very inefficient accommodation, for the resident staff. The
drainage, laid down without any general plan, and in piecemeal
fashion, was constantly being attended to and tinkered
with.
In 1887 the Medical Council complained of the defective
sanitation of the Hospital, and requested that a sanitary
expert might be asked to examine the drainage and advise
in the matter. At the same time it submitted to the Committee
a report entitled, Some Defects in the Royal London
Ophthalmic Hospital, in which the above mentioned deficiencies
and others were set out in detail. From the
consideration of this report, and that received from the
sanitary expert, it became obvious that nothing but a new
building would meet all the requirements.
The building land in the rear of the Hospital facing
Eldon Street still remained temptingly vacant, and, in 1887,
a suggestion was received, emanating from the City architect,
that an exchange might possibly be effected—i.e., the
170taking of the existing site of the Hospital for the vacant site
in Eldon Street together with a sum of £15,000.
Though this suggestion did not come to anything, it
served to awaken the Committee of Management to the
valuable assets the Hospital possessed in the greatly enhanced
value of its freehold and leasehold properties, due to the
changes which had taken place in its environment since it
was first built—unearned increment, which was eventually
put to the best possible use by an extension of the means
for the relief of suffering in the community.
Mr. Lander, the Hospital’s surveyor, was then requested
to obtain valuations of the Hospital’s site and of that of the
vacant land adjoining it. No very precise figures were
obtained, the site of the Hospital being valued at anything
between £50,000 and £100,000. The Committee still,
however, hesitated to make any tender for the vacant
land.
In July, 1888, after a consultation of representatives of
the Medical Council with Sir John Lubbock, the President
of the Hospital, he agreed to introduce a deputation to the
Lord Mayor to request him to use his influence in obtaining
for the Hospital a gift of the vacant land adjoining it from
the Corporation. The Lord Mayor pointed out that it
was trust property held by the Bridge House Estates, which
had no power to comply with the appeal of the deputation
“so earnestly and reasonably made.” The deputation next
waited on the Bridge House Estates Committee, who replied
that it was unable to pledge itself not to accept any tender,
but the matter would receive its most favourable consideration.
Matters were still further advanced in that year: firstly,
by the receipt of an unsolicited donation of fifty guineas from
the trustees of St. Stephen’s, Coleman Street, towards a
Building Fund, which led to the opening of such a fund
for subscriptions, to which the surgeons of the Hospital in
the following year promised a gift of £1,000; secondly, by
171the desire of the City to effect a street improvement, so as
to widen the junction of Blomfield Street and Eldon Street,
which would necessitate a surrender of a slice of the Hospital’s
ground.
A complication arose, due to the Hospital’s land not
directly adjoining that vacant in Eldon Street—a Welsh
chapel, with a lease of four years yet to run, intervening
between them.
Ultimately, the Bridge House Estates Committee offered
the Hospital the vacant area, including that of the Welsh
chapel, comprising in all 7,180 feet, on lease for ninety-nine
years at a peppercorn rent of £311 per annum until the
chapel’s lease expired, and then at £388 per annum, with,
however, the provision that the Committee of the Hospital
or its trustees were made personally responsible for the
payment of the rent and the observance of the conditions
of the lease. This provision neither the members of the
Committee nor the trustees of the Hospital were prepared
to accept, and the whole of the year 1889 was spent in
endeavouring to come to terms with the Law Guarantee
and Trust Society to take on these responsibilities. These
negotiations not proving satisfactory, it was decided, in
1890, that application should be made to the Privy Council
for a Charter of Incorporation. A Petition for Incorporating
the Hospital by Royal Charter was prepared and presented
to Her Majesty the Queen in Council, together
with a draft form of the Charter which would empower
the Hospital to hold land in mortmain, and thereby enable
it to proceed with negotiations for the lease. The Charter
of Incorporation under the Great Seal was passed in
December, 1890, to which a common seal, that had been
designed for the Hospital, was appended.
In the lease obtained for the ground in Eldon Street it
was laid down that building was to commence before
January, 1893, and it became necessary at once to appoint
a suitable architect to draw up plans. Messrs. Lander
172and Bedell were at that time acting as surveyors to the
Hospital, but hospital construction had developed into a
very specialised branch of architecture, and it was thought
desirable to employ for the new building one who had a
large experience of that kind of work. In August, 1891,
Mr. Keith Young, who had already designed several hospitals,
was appointed, to be assisted by Mr. Lander, and
after his death in 1892 by Mr. Bedell.
After due and deliberate consideration, the architects
arrived at the opinion that the site, even including that of
the Welsh chapel, would not allow of sufficient space to
meet all the requirements of the new Hospital. They
suggested that a larger one might be acquired in a less
valuable locality. Investigations were made, and a site
which seemed to offer many advantages was discovered in
the City Road. Many of those associated with the Hospital
felt very loath to move the Institution from the neighbourhood
of Moorfields, with which it had become so intimately
associated. The matter was discussed at length at a joint
meeting of the Committee of Management and the medical
staff, and in July, 1892, the latter passed the following
resolution:
“That considering the alleged great value of the present
site and the difficulty of constructing a suitable building
upon it, the Medical Council is of opinion that the present
site should be sold and that, so far as the information at
present at its disposal goes, the City Road site is best
adapted for a new Hospital provided that the whole of that
site can be acquired.”
With the sanction of the Bridge House Estates Committee,
the lease of the Eldon Street site with all its obligation
was transferred to a substantial tenant, who was willing
to pay the Hospital a premium of £1,000.
The lease was then obtained for 999 years from March,
1894, of what was termed the City Road and Peerless Street
site of some 35,000 feet, in the parish of St. Luke’s, Old
173Street, in the county of Middlesex, at a rent of £1,210 per
annum, from the Ecclesiastical Commissioners.
It is rather a remarkable coincidence that another hospital,
which was originally situated at Moorfields, should have
previously removed to the neighbourhood of the City Road,
and not very far from the Peerless Street site. St. Luke’s
Hospital, which, though independent of Bethlehem Hospital,
dealt with the same class of ailments, was originally established
in 1750 on the north side of Moorfields. In 1782
a new building was erected near the junction of Old Street
and the City Road, it being recorded that at that time
green fields could be seen in every direction. The building
continued as a hospital for the mentally defective until the
time of the Great War, when it was taken over by the Bank
of England, of which it continues to be a branch.
Peerless Street runs between the City Road and Bath
Street. It is lined by a row of small, mean houses, which,
but for the Rent Restriction Act, would have been swept
away ere this by the ground landlord, St. Bartholomew’s
Hospital. Anyone unacquainted with the history of the
neighbourhood may well wonder how such a poverty-stricken
street could have acquired such a high-sounding
name. It is the last remaining sign of the delectable
attractions which formerly existed in its neighbourhood.
In ancient times some springs overflowed and formed a
pond between what is now Peerless Street and St. Luke’s
Hospital; from it water was conducted through pipes to
Lothbury for the benefit of the inhabitants of that district.
Stowe describes it in 1603 as “cleare water called the
Perilous Pond because divers youths by swimming therein
have been drowned.” In consequence of such accidents
(the inhabitants of Lothbury having obtained water from
elsewhere), the Perilous Pond was entirely filled in. In
1743 Mr. William Kemp, an eminent jeweller and citizen
of London, having derived relief from violent pains in the
174head from which he had suffered for several years by bathing
in the water from the spring, converted it into what William
Maitland, in his History of London, 1775, describes as “the
completest swimming bath in the whole world.” “He
spared,” Maitland says, “no expense nor contrivances to
render it quite private and retired from public inspection,
decent in its regulations and as genteel in its furniture as
such a place could be made.” At the same time he changed
its name from the disagreeable one of the “Perilous Pond,”
which it no longer was, to the pleasing one of the “Peerless
Pool,” which, owing to its size and surroundings, it had undoubtedly
become. The swimming bath measured 170 feet
in length and 100 feet in width, and varied from 5 to 3 feet
in depth. The entrance to it was through a marble pavilion
30 feet in length and across a bowling green; it was surrounded
by dressing compartments, outside which were
lofty banks covered with shrubs and a terraced walk planted
with lime trees. Four pairs of marble steps descended to
the bath, which had a fine gravel bottom. Besides this
open swimming bath, there was a covered cold bath, supplied
with water from a specially cold spring, faced with marble
and paved with stone. The most remarkable feature,
however, of the Peerless Pool was “a noble fish pond
constructed by Kemp due east and west. It was 320 feet
long, 93 feet broad, and 11 feet deep, stocked with carp,
tench, and a great variety of the finney tribe, wherein subscribers
and frequenters of either the pleasure or the cold
bath were privileged to angle.” William Hone, in his
Every-day Book, published in 1831, gives engravings of the
fish pond (showing the lime walk and Kemp’s house in the
distance) and of the swimming bath, made by Mr. John
Cleghorn, an architectural draftsman and engraver, who for
many years resided near the Pool.
In the Daily Advertiser of August, 1748, are some doggerel
verses extolling the attractions of the Peerless Pool, and
also a statement that—
175
“any gentleman, who subscribes only one guinea per annum,
is entitled to the pleasure and cold bath, and to the diversion
of angling and skating at proper seasons; and that if any
occasional visitor, who must pay 2s. each time he bathes,
thinks proper to become a subscriber in the fourteen days
from his first visit, he shall be allowed that he has paid it
as part of his subscription.”
PLATE XXIV
THE PLEASURE BATH,
PEERLESS POOL, CITY ROAD.
TERMS OF
──────
PLEASURE BATH
──────
£.
s.
d.
Month
0
9
0
Two Months
0
10
0
Year
1
1
0
──────
Single Bathe
with Towels
0
1
0
and Box
Ditto without
0
0
6
SUBSCRIPTION
──────
COLD BATH
──────
£.
s.
d.
Month
0
10
0
Two Months
0
17
0
Year
1
1
0
──────
Single Bathe
0
1
0
THE PLEASURE BATH
OF PEERLESS POOL,
The largest in England, is situated in the immediate neighbourhood
of the heart of the City, within Ten minutes direct
walk of the bank and Exchange, (vide plan.) Surrounded by trees
and shrubberies, open to the air, although entirely screened
from observation, and most ample in its dimensions—170 feet
in length, by 108 in breadth—it offers to the Bather the very
advantages he would least expect to find at so short a distance
from the centre of the metropolis. Its depth, which increases
gradually from 3 feet 6 inches to 4 feet 8 inches, is such as to afford
free scope to the Swimmer, while it precludes all fear of
accident to any and the temperature of the water rises to a
height sufficient to ensure all the comfort and luxury of Bathing,
without the risk of injury to health, from a too violent contrast
with the external air.
THE COLD BATH,
Thirty-Six feet by Eighteen, is the largest of its kind in
London, and both Baths are entirely supplied by Springs,
which are constantly overflowing.
The City Road is the line from all parts of the West
End to the City. Omnibuses pass both ways nearly
every minute throughout the day.
BILL OF PEERLESS POOL. Circ. 1846.
After Kemp’s death the Pool seems to have changed
hands several times. On the expiration of the lease in
1805, a new one was obtained from St. Bartholomew’s
Hospital by Mr. Joseph Watt, at an annual rental of £600.
To remunerate himself Mr. Watt drained the fish pond,
felled the trees around it, and built Baldwin Street, which
lies just south of Peerless Street, on its former site. He
also erected Bath Buildings on the ground occupied by
Kemp’s orchard, but left the pleasure bath intact. In 1831
William Hone wrote:
“The pleasure bath is still a pleasant spot, and both
that and the cold bath retain their ancient capabilities.
Indeed, the attractions of the pleasure bath are undiminished.
Its size is the same as in Kemp’s time, and trees enough
remain to shade the visitor from the heat of the sun while
on the brink, irresolute whether to plunge gloriously in,
or ignobly walk down the steps.... Every fine Thursday
and Saturday afternoon in the summer, columns of blue-coat
boys, more than three score in each, headed by their
respective beadles, arrive, and some half strip themselves
ere they reach their destination; the rapid plunge they make
into the pool, and their hilarity in the bath, testify their
enjoyment of the tepid fluid.”
The Peerless Pool continued in existence as a public bath
until 1850, the site occupied by it being built over between
that date and 1860.
Out of the City Road, on the opposite side to Peerless
Street, leads Shepherdess Walk, which marks the site of
the Shepherd and Shepherdess ale-house and tea-garden,
built some time before 1745. The gardens were frequented
by visitors who regaled themselves with cream, cakes and
176fromity. Invalids sometimes stayed at the inn to benefit
by the pure air of the neighbourhood.
“To the Shepherd and Shepherdess then they go
To tea with their wives, for a constant rule;
And next cross the road to the Fountain also,
And there they all sit, so pleasant and cool,
And see, in and out,
The folk walk about,
And the gentlemen angling in Peerless Pool.”
In Baldwin Street there is still a public-house called “The
Fountain,” which is probably the survival of the one referred
to in this old rhyme, and of one which Franklin wrote of, “a
very genteel public house at the east end of Kemp’s garden.”
The City Road, which was opened in 1761, cut through
the meadow grounds which surrounded the Shepherd and
Shepherdess, so that the place lost its rural isolation. The
inn was pulled down in 1825, and the Eagle Tavern, which
formed the nucleus of the famous Eagle establishment,
with its Grecian saloon and theatre, and its garden and
dancing pavilion, was erected near its site. It was this
establishment which was celebrated in the refrain of the
popular song;
“Up and down the City Road,
In and out the Eagle,
That’s the way the money goes,
Pop goes the weasel.”
It has been suggested that this refrain might be paraphrased
by those employed at the Moorfields Hospital as
follows:
“Up and down the City Road,
In and out Moorfields,
That’s the way we spend our lives,
Oh! the joy it yields.”
Whilst the above discussions and negotiations with regard
to the erection of a new Hospital were in progress several
changes took place in the personnel of the staff.
177
In 1890 John Whitaker Hulke, having reached the age of
sixty, retired. He died five years later whilst holding the
highest position in his profession, that of President of the
Royal College of Surgeons in England. John Browning
Lawford, who had already held the posts of house surgeon
and of curator of the Museum, was elected in his place.
In 1891 George Lawson also had to retire under the age
limit rule. In 1869 he had published a Manual on Diseases
and Injuries of the Eye, which, owing to its practical character,
became exceedingly popular amongst medical students, and
rapidly ran through five editions. Lawson endeared himself
to his patients by the personal interest he manifested
in their welfare. His treatment went far beyond the mere
prescription of drugs or the performance of operations.
He would instruct a mother how to feed, clothe, and train
her child. He would tell a patient, for whom nothing
could be done to restore the lost sight, what his future might
be and how to get to work to earn a livelihood. Many of
those engaged in seeing out-patients often wish they could
prescribe food for them instead of medicine. Lawson
actually did this, having an arrangement with a neighbouring
butcher by which he could at his own expense order
patients so many pounds of meat. Nor did his generosity
to Hospital patients end with supplying sound advice and
meat; many to whom some unusually disastrous circumstance
had occurred would be led quietly aside and return
with a smiling face and a closed palm.
In 1886 Lawson was appointed surgeon oculist to Her
Majesty Queen Victoria, which appointment he held until
her death. He himself died in 1903 at the age of seventy-two,
having had the satisfaction of seeing his son Arnold
(now Sir Arnold Lawson) appointed on the staff at Moorfields,
where he himself had worked for so long.
The vacancy caused by Lawson’s retirement was filled
by the election of A. Stanford Morton, who was educated
at Edinburgh University. He had served the Hospital first
178as house surgeon and later as clinical assistant for a period
of sixteen years. He did not take the necessary qualification
of the Fellowship of the Royal College of Surgeons of
England, which would qualify him as a candidate for the
staff, until 1888, and was forty-eight years of age at the time
of his election. His name has become widely known
throughout the ophthalmic world in connection with the
very serviceable and popular pattern of ophthalmoscope
which he had constructed for him by Messrs. Curry and
Paxton. It happily combined all the best features and
adaptations which had previously been suggested.
For dexterity and neatness as an operator on the eye
Morton was unsurpassed in his time. He enthusiastically
instructed others in the art, holding classes of operative
ophthalmic surgery in which he employed pigs’ eyes fixed
in a frame to enable students to obtain the necessary manipulative
dexterity. Whilst he was working as a clinical
assistant, the practice of retinoscopy for the correction of
errors of refraction came into use, and he wrote a small
book on Refraction of the Eye, describing it in such an
easily assimilated manner that the book had a large sale,
several editions being called for.
Being a good draftsman, and having an excellent eye
for colour, Morton made many beautiful coloured drawings
of ophthalmoscopic changes, the originals of which he
presented to the Hospital on his retirement. The extreme
care which he took in their production often necessitated
several sittings on the part of the patient. In one interesting
and complicated case, the drawing of which took a very long
time, Morton found it necessary to remunerate the patient
liberally after each sitting to ensure his subsequent attendance.
When the drawing was finished the man found that
Morton’s interest in his case had evaporated, and, being
hard up, appeared at the Hospital one morning offering to
sell him one of his eyes if he would like to take it out—an
offer which it is perhaps needless to say was not accepted.
179The man afterwards went about to various ophthalmic
clinics calling himself the celebrated Moorfields case, and
he informed those who examined him “that gentlemen
generally gave him something after looking at the backs of
his eyes,”
Though it had been the custom for a long time to print
on the letters given to patients, and to have posted up in
the out-patient department, a notice to the effect that the
Hospital was only open for the reception of really indigent
patients, it was a rule which the medical staff found very
difficult to enforce, and which was obviously very frequently
infringed. In 1893 on the advice of the Medical Council,
the Committee of Management adopted the plan in use at
several of the other London hospitals of appointing an
“inquiry officer” to attend daily and make necessary
inquiries, so that “no person should be admitted in the first
instance to Hospital relief who can afford to pay a fee of
one guinea for a consultation (except in cases of accident)”
The officer appointed for this Purpose was one selected by
the Charity Organisation Society, who had been trained
under its superintendance. As the result of his investigations,
from about 500 applicants were refused yearly, it
being found that they were able to pay a surgeon’s fee,
many of them stating that they were unaware that the
Hospital was open for the poor only.
John Couper’s time for retirement from the staff came in
1895. He continued in active practice for several years afterwards,
and died in 1918, in his eighty-third year. He had
always been a firm supporter of the movement for the admission
of women to the medical profession, and welcomed Miss
Elizabeth Garrett (afterwards Mrs. Garrett Anderson) as
an onlooker at his clinic at Moorfields. It was not, however,
until after he had left the staff, in 1898, that the eligibility
of women to become pupils and clinical assistants at the
Hospital became officially recognised.
E. Treacher Collins, who, like Lawford, had been both
180house surgeon and curator of the Museum at the Hospital
was appointed as Couper’s successor.
The premature and unexpected resignation from the staff
of Edward Nettleship took place in 1898; his keen interest
in the scientific side of ophthalmology, however, did not
slacken. He gave the Hospital a donation of £250, to be
expended on scientific apparatus and appliances for the
laboratory in the new building. With more time at his
disposal for research work, his valuable scientific contributions
increased in number. With indefatigable ardour and
strenuous accuracy he worked out pedigrees of hereditary
diseases, the value of which work was recognised in 1912
by his election as a Fellow of the Royal Society. On his
retirement from practice in 1901, his friends and pupils
inaugurated a fund to found the “Edward Nettleship
Prize” for the encouragement of scientific ophthalmic work.
It took the form of a Gold Medal to be awarded at intervals,
at the discretion of the Council of the Ophthalmological
Society, British subjects alone being eligible. He died in
October, 1913, being actively employed up to the time of
his death, in conjunction with Karl Pearson and C. H.
Usher, on a large monograph upon “Albinism in Man.”
To fill the surprise vacancy caused by Nettleship’s retirement,
W. T. Holmes Spicer was appointed.
Three matrons at the Hospital resigned from ill-health
in the course of a few years, and, in 1895, Miss Ada Robertson,
a former sister at the London Hospital, was appointed
to the post. She not only carried through the difficult task
of transferring the work of the Hospital from the old to the
new building, but also, with skill and tact, raised the nursing
to a higher standard of efficiency than it had reached
before.
In 1897 Mr. Charles Gordon, who had acted as Chairman
of the Committee of Management for eighteen years, and
who had taken an active part in all the negotiations for the
removal of the Hospital to a new site, on the eve of the
181laying of the foundation stone, found it incumbent upon
him to resign owing to his advanced years; he died two years
later. Thus, like Moses, having led his colleagues to
within sight of the promised land, he left it for them to
enter into its occupation.
Mr. H. P. Sturgis, a director of the London and Westminster
Bank, was elected Chairman in his place.
About the same time, Mr. Robert J. Newstead, after
twenty-five years’ service as secretary, had to resign from
ill-health, and died at the end of the year. Mr. Robert J.
Bland was appointed as his successor.
On the 28th of May, 1897, the work of clearing and preparing
the foundations being sufficiently advanced His
Royal Highness the Prince of Wales (afterwards King
Edward VII.), on behalf of Her Majesty Queen Victoria,
laid the foundation stone of the new Hospital. His Royal
Highness was accompanied by their Royal Highnesses the
Princess of Wales (afterwards Queen Alexandra) and
Princess Victoria, the former graciously consenting to receive
purses containing donations in aid of the Hospital. The
silver trowel used on the occasion, which was provided by
Mr. E. Hogg, one of the members of the Committee of
Management, was presented to His Royal Highness, who
stated “it is Her Majesty’s great and earnest wish that
this Hospital may be prosperous and successful in every
way.” Her Majesty further manifested her continual
interest in the Charity by giving a donation of £100 to the
Budding Fund. The Prince of Wales on his departure
signified his intention to become a Patron of the Hospital.
In the removal of the Hospital from a prominent situation
which had developed into a great business centre to a less
known district easily accessible to those to whose needs it
ministered the Committee of Management hoped to defray
the cost of the building by the proceeds of the sale of the
old site, and in doing so it was not far out in its reckoning.
The old Hospital was sold for £78,500, and the new Hospital
182cost about £80,000. To provide the funds for the new
building, whilst the work was being carried on in the old
one, large loans had to be negotiated on the security of its
freehold and leasehold property. In addition to the cost
of the building the Committee had to provide funds for
furnishing the new building, and equipping it with appliances
and apparatus in keeping with its position as the leading
ophthalmic institution in the British Empire. For this
purpose it made a special appeal which was liberally responded
to by the Corporation of the City of London and
the following City Companies: The Worshipful Company
of Carpenters, of Clothworkers, of Drapers, of Dyers, of
Fishmongers, of Goldsmiths, of Grocers, of Leather Sellers,
of Mercers, of Merchant Taylors, of Sadlers, of Salters, and
of Skinners.
The fund was further augmented by a festival dinner
held at the Grand Hotel, Charing Cross, on the 6th of May,
1898, over which His Royal Highness the Duke of Cambridge
graciously presided, he himself making a liberal contribution
to the cause for which he pleaded. In the following
year a large and influential number of ladies promoted a
ball in the Empress Rooms at the Royal Palace Hotel,
Kensington, on the Hospital’s behalf, and Sir Squire Bancroft
generously gave to it the proceeds of one of his inimitable
readings.
When the clearance of the site for the new Hospital in
the City Road was commenced, a Building Committee was
appointed, consisting of certain members of the Committee
of Management, with Mr. H. Davidson as chairman, and
three representatives of the Medical Council, Tweedy,
Gunn, and its honorary secretary, at first Morton, and later
Treacher Collins.
One of the first questions this Committee had to consider
was the dual one of the ventilation and warming of the new
building. Was the system of ventilation to be “natural”
or “artificial”? If artificial, was it to take the form of
183propulsion or extraction, or a combination of both? It
has been well said “that theories in ventilation and warming
are as numerous as trees in a forest,” and so the Building
Committee discovered when they commenced to consider
the problem. Several hospitals in which artificial ventilation
was in use were inspected; ultimately it was decided
that artificial ventilation on the planum system should be
adopted for the out-patient department, and that natural
ventilation should be relied upon for the wards.
The air forced into the out-patient department is first
filtered, and then warmed or cooled as required. A shaft
is provided which allows the foul air to escape. The force
employed is a large rotating fan-wheel which propels the
air along underground passages, and through gratings
which open into the various compartments. It is filtered
by passing through a coke-screen, which is cleaned with
a stream of water flowing over it automatically at periodic
intervals. It is warmed by passing over hot-water radiators
situated close to the gratings opening into the compartments.
It can be cooled by substituting blocks of ice placed on the
radiators for the hot water contained in them.
In the wards the position of the windows is arranged to
allow of cross ventilation, and the main sources of heat
are open fires. Additional sources for warmth and ventilation
are provided by hot water radiators, past which fresh
air is allowed to enter through gratings near the floor. A
separate sanitary block running through the centre of the
building is cut off from it by cross-ventilation lobbies.
Only those who worked in the old Hospital in Blomfield
Street can fully appreciate the amenities afforded by the
new one in the City Road. Daily at noon the whole in-patient
department in the old building became permeated
with the odour of cooked meat. In the new Hospital all
such disagreeable smells have been avoided by having the
kitchen placed on the top floor. Most of the cooking is
carried on by steam, supplied from boilers in the basement.
184A special service lift conveys goods to the kitchen, and also
permits of the distribution of food and fuel to various parts
of the building. Both this lift and the passenger lift are
worked by hydraulic power; the latter allows of the conveyance
of a patient on a wheeled trolley, in the recumbent
position, to his bed from the operating table.
The lighting arrangements in the out-patient department,
for the examination of the patients and the testing of their
eyesight, and in the operating theatre to meet its varied
requirements, engaged the architect’s and the Committee’s
prolonged consideration. For the examination of patients
in the first instance, and for many operations, uninterrupted
direct skylight from a northern aspect was regarded as
essential, and the new building was so planned as to allow
of this in the large consulting room and in the operating
theatre. As the work of the Hospital has to be carried
out on dark days as well as bright ones, adequate means
for the examination of patients by artificial light, in the
absence of daylight, had to be provided. In the old
Hospital, where gas was the main source of artificial illumination,
there were various contrivances rendering it
more or less efficient by the use of reflectors. In the
operating theatre, a device used by the Nottingham lace
workers had been employed. It consisted of a large hollow
glass globe filled with water and suspended from the ceiling,
which concentrated light from a lamp placed behind it on
to the face of a patient lying on the operating table. The
introduction of electricity for illuminating purposes throughout
the new building simplified matters considerably. In
the consulting room, movable flexes and adjustments permit
light being easily brought into the most suitable position in
which to conduct an examination. The employment of
electric light globes for ophthalmoscopic examinations in
the dark room, in place of argand gas burners, renders the
atmosphere in it far more healthy and pleasant to work
in, but it is doubtful if any form of electric bulb supplies
185quite such a uniform and satisfactory area of illumination
for these examinations as the old argand gas burner.
The electric current supplied to the Hospital for lighting
purposes is an alternating one; fortunately a constant
current was also available in the district, being used in
neighbouring factories. One of the chief purposes for
which it is required is for working electro-magnets for
the extraction of chips of iron or steel implanted in the
interior of the eyeball.
It has been already mentioned how in 1858 Dixon tried
unsuccessfully to remove a chip off the edge of a chisel,
seen floating in the vitreous chamber, by a permanent
magnet. In a similar case, McKeown of Belfast, in 1874,
succeeded in the removal of the foreign body by the introduction
of the tip of a permanent magnet into the interior
of the eye.
In 1878 Malcolm McHardy, who was later ophthalmic
surgeon to King’s College Hospital, employed for the first
time an electro-magnet, and with it successfully removed
a chip of steel which had become embedded in the crystalline
lens. A few years later, Snell of Sheffield, Hirschberg
of Berlin, and Bradford of Boston, U.S.A., had constructed
electro-magnets which could be held in the hand, and have
suitable terminals attached to them for introduction into the
interior of the eye. Considerable success attended the use
of such instruments when fragments of iron were situated
in the front parts of the eye, but only on rare occasions
when they had become deeply placed in the vitreous humour.
In these latter cases, the foreign body was often hid from
view, due to opacity of the lens caused by the injury, so that
its exact position was unknown, and there was some doubt
as to whether it had lodged in the eyeball or not. It was
only when the nozzle of the hand magnet came close to the
foreign body that it possessed sufficient traction power to
draw it out, and in searching for it much damage was liable
to be inflicted on the structures in the interior of the eyeball.
186
On the discovery of the X-rays by Professor Röntgen in
1895 it occurred to many ophthalmic surgeons that they
might be utilised for the detection of foreign bodies in the
eye. Two practical difficulties at first presented themselves,
both of which were ultimately overcome. One was
the density of the bony structures around the eyeball, and
the other that of locating accurately the position of a foreign
body when detected. It was found that excellent skiagrams,
showing exceedingly minute pieces of metallic substances
in the orbit, could be obtained if the sensitive plate was
placed against the temple on the side of the injured eye, and
the Crookes tube 10 to 15 mm. distant from the opposite
temple. The most accurate localisation of foreign bodies
implanted in the body was effected by an ingenious device
of Mackenzie Davidson’s in which, after superimposing
two skiagrams taken at slightly different positions, he followed
the tract taken by the rays from the Crookes tube
to the foreign body by means of threads, noting where they
crossed in relation to the position of other known points.
Mackenzie Davidson (afterwards Sir James Mackenzie
Davidson) worked at Moorfields as clinical assistant, and
subsequently practised as an ophthalmic surgeon in Aberdeen.
Soon after the discovery of X-rays, he removed
to London and devoted himself specially to their application
to surgery and medicine. His combined interest in
ophthalmology and X-rays made him desirous of testing
his method of localising foreign bodies in connection with
eye injuries. Several members of the staff at Moorfields
sent cases to him to report on, and such accurate and helpful
information did he supply, not only as to the presence or
absence of a foreign body in the eye, but also as to the
exact position in which, when present, it could be found,
that a desire arose to establish a special X-ray department
and to secure his services in connection therewith. On the
recommendation of the Medical Council, this was agreed to
by the Committee of Management in November, 1898, £80
187being voted for the cost of apparatus and an annual expenditure
of £20 for the working expenses of the department.
Mackenzie Davidson consented to accept the appointment
of honorary medical officer in charge of the X-ray department,
and a special room was fitted up in the new Hospital
with the necessary conveniences for carrying on the work.
The introduction of the constant electric current into the
operating theatre allowed of the employment of far more
powerful magnets for the extraction of fragments of iron
from the eyeball than had previously been used in this
country. These powerful magnets have appropriately been
described as “giant magnets”: they were originally introduced
into ophthalmic practice by Professor Haab of Zurich.
Their traction force is so great that a chip of iron hidden
in the back part of the eyeball can be drawn forward into
view in the front part.
In the Hospital Reports, H. V. McKenzie, the house
surgeon in 1895, collected notes of all the cases in which
a foreign body had been removed from the eye by the small
hand magnet—i.e., prior to the introduction of X-ray
localisation, and found that in 26 per cent, of those in which
it was lodged in the vitreous the eye was saved. In 1902
the house surgeon, A. F. MacCallan, tabulated the results
obtained by the use of Haab’s Giant Magnet, and found
that in a similar class of cases by its use 58 per cent. of the
eyes were saved, and that in half of these good vision was
obtained. If accurate localisation of the foreign body by
X-rays was carried out previous to the use of the magnet,
a still larger percentage of success resulted.
The operating theatre in the new Hospital has been
designed to make possible the practice of aseptic surgery.
Antiseptic surgery, as first introduced, relied on the destruction
of micro-organisms by chemical agents, and it was
thought essential, whilst an operation was in progress, to
have a spray of carbolic acid playing to prevent aerial
infection of the wound. Later, as the result of experience
188gained in bacteriological laboratories, it became realised
that such a precaution was unnecessary; micro-organisms
being like dust particles subject to the law of gravitation,
all that was required was to prevent any accumulation of
dust and to avoid currents of air.
To avoid any accumulation of dust in the new operating
theatre, its walls, ceilings, and floor are so constructed that
at any time they can be washed over with a hose. The
wall and ceiling are lined with glass tiles, technically known
as “opalite,” the floor is paved with terazzo, and all the
corners are rounded. All the pipes are of copper, and the
radiators of the same metal. The latter are constructed so
that they can be swung out on a pivot, and no dirt be
allowed to accumulate behind them; they are in three divisions,
which allow of variations in the amount of warmth
given out as may be required.
To permit as many onlookers as possible being able to
watch the operator’s procedures, without inconveniencing
him or his assistants, fixed stands are erected on each side
of the operating table, each stand being composed of three
tiers, and each tier accommodating four persons.
The colour of the tiles on the walls and ceiling is a
creamy-white with a dado of pale green. As some operations
have to be conducted in a darkened room by artificial
light concentrated on the eye, a dark blind is provided
which can be drawn up from below, being enclosed when
not in use in a brass box.
The case in which the instruments are stored is constructed
entirely of brass and glass, and apparatus is provided
to allow of the instruments being sterilised by boiling them
before use. A special steriliser for dressings is also provided,
with an outer jacket for steam, which permits of them
being delivered dry when required for use.
In the wards, passages, and other parts of the building,
all possible precautions are taken to avoid any lodgments
for the accumulation of dust, the floors of all the wards
189being constructed of polished teak, and wherever possible
the corners are rounded. All cupboards have sloping tops,
and are fixed to the walls at such a height that the highest
part of them is easily within reach. Arrangements are
made for the storage of the patients’ clothes, when in bed,
in special cupboards outside the wards, and the small
marble-topped lockers placed beside their beds were
specially designed just to contain a few of their possessions.
A special eye hospital differs from a general hospital in
the large proportion of its patients who are able to be up
out of bed during the daytime. It is, therefore, desirable
to have special day rooms in which they can congregate
away from the wards, and have their meals. In the new
Hospital, on each floor, such day room accommodation is
provided.
Notwithstanding the enormous amount of work involved
in the removal to the new building, it was effected with
scarcely any interruption in the routine work of the Institution.
The new building was opened for the reception of
patients on September 4th, 1899, the work in the old
Hospital being carried on for in-patients up to August 19th,
and for out-patients up to August 26th.
190
CHAPTER XII
THE HOSPITAL IN THE CITY ROAD
On June 28th, 1899, the now dreary neighbourhood of the
former “Peerless Pool” once again awoke to life and
notoriety with a visit from their present Majesties King
George V. and Queen Mary, then the Duke and Duchess
of York, to open the new “Peerless” Eye Hospital. A
lengthy description of the ceremony appeared in The Times
on the following day.
The Duke and Duchess of York, attended by Sir Charles
Cust and Lady Katherine Coke, arrived at the Hospital
shortly after half-past 3 o’clock, and were received by Sir
John Lubbock, the President, Mr. H. P. Sturgis, Chairman
of the Committee of Management, and the architects,
Messrs. Keith Young and H. Hall. The Duke, who received
a gold key from the architects, unlocked the door of the main
entrance hall, where the surgeons of the Hospital, the matron,
Miss Robinson, and the secretary, Mr. R. J. Bland, were
presented to their Royal Highnesses. The Royal party
were then conducted over the building, and after completing
their inspection they entered the out-patients’ hall, which
had been prettily decorated for the opening ceremony, and
where a large company had assembled. Among the visitors,
in addition to those already named, were the Lord Mayor
and Lady Mayoress, Mr. Alderman and Sheriff Alliston,
Lieutenant-Colonel and Sheriff Probyn and Mrs. Probyn,
the Bishop of Islington and Mrs. Turner, the Rev. Prebendary
Whittington (chaplain), Sir J. Whittaker Ellis and
Lady Ellis, Lady Faudel-Phillips, Sir Squire and Lady
Bancroft, Mr. J. Lea Smith (trustee), Mrs. Sturgis, Sir
T. Lipton, and the Rev. Dr. Hermann Adler and Mrs.
191Adler, Mr. H. Davison (chairman of the Building Committee)
and Mrs. Davison, Mr. A. G. Pollock (chairman
of the Special Appeal Committee) and Mrs. Pollock. The
little daughter of Mr. John Tweedy, the senior surgeon,
presented a handsome bouquet of pink roses to the Duchess,
who was dressed in pale green eau de Nil silk with a toque
of pink roses. Prayers having been said by the Bishop of
Islington, Sir John Lubbock called upon Mr. Sturgis to
make a statement.
PLATE XXV.
THE ROYAL LONDON OPHTHALMIC HOSPITAL IN THE CITY ROAD, OPENED IN 1899.
Mr. Sturgis said that they valued extremely the presence
of the Duke and Duchess of York, inasmuch as their Royal
Highnesses represented the fourth generation of the Royal
Family who had shown interest in the Hospital. He related
the circumstances which had necessitated its removal from
its old site at Moorfields and the erection of the present
building, which the Committee had endeavoured to make as
perfect as possible, and which they would come into free
from debt. This, however, he went on to say, was only
the beginning of their task. They had to consider the
maintenance of the establishment. The cost of maintenance
at the old building was about £8,000 a year, and their regular
income, including grants from the Hospital funds, did not
reach the sum of £3,000 a year, so that they had to make
up the difference in other ways. But the cost of maintenance
in the new building would be as much as £11,000
a year. He hoped their income would increase to a corresponding
extent. What they wanted more than anything
else was an increase in annual subscriptions, and they
wished to raise a fund of £50,000 which would be a guarantee
for the large ground rent which they now had to pay.
Sir John Lubbock, after expressing indebtedness to all
those concerned in the work of the Institution, asked the
Duke of York to declare the building open.
The Duke of York said:
“Sir John Lubbock, Mr. Sturgis, Ladies and Gentlemen,
I am grateful to Sir John Lubbock for the kind words he
192has used with regard to our coming here to-day, and I have
been very much interested in all I have heard from Mr.
Sturgis, the Chairman of the Committee. I thank you all
in the Duchess’ name as well as my own for the very kind
reception you have given us. It is an especial pleasure to
the Duchess and myself to come here to-day, as my father
laid the foundation stone of the new building in 1897, and
therefore we are completing the work, so to speak, which
he inaugurated.” (Cheers.) “As Mr. Sturgis told us just
now, of late years the number of patients increased so
enormously that the old buildings were found quite inadequate
to their wants, and the Committee were compelled
to seek a larger site for this new building. And, if I may
be allowed to do so, I wish to congratulate the architects
on the excellent result of their labours, and I also wish to
congratulate the Committee and the medical staff on occupying
a new Hospital designed and equipped according to
the most modern requirements. The cost of maintenance
of these new buildings, which cover three-quarters of an
acre, will be, I fear, as Mr. Sturgis has just told us, very
heavy, but I am sure the Committee deserve the generous
support of the charitable public to enable them to continue
the useful work that has been so ably carried out by this
Hospital for nearly a century, and I can only say that I
trust that the public will come forward and help this
Hospital and prevent it from getting into debt by their
annual subscriptions. I have now much pleasure in declaring
this new building open, and the Duchess joins with
me in wishing the Royal London Ophthalmic Hospital
continued prosperity in this new building, and a long career
in its great and important work.” (Cheers.)
Their Royal Highnesses then left the building, and were
heartily cheered by a large crowd in the street as they drove
away.
As a lasting memorial of the visit of their Royal Highnesses
the Children’s Ward was named the “Princess May”
Ward. After their visit, they consented to become Patrons,
and presented copies of their portraits to the Hospital, with
their autographs attached.
The hopes expressed by Mr. Sturgis, the Chairman of the
193Committee, at this opening ceremony, that increased financial
support would be forthcoming to meet the additional
annual expenditure, were completely shattered for a time
by the outbreak of the South African War. As at the time
of the Crimean War, the sympathies and contributions
of the public became diverted to funds for soldiers and
sailors, and the donations and new subscriptions to the
Hospital almost ceased to come in, the result being that the
Hospital, in September, 1900, found itself £5,000 in debt.
One of the largest and most unforeseen items in increased
expenditure, resulting from the removal of the Hospital,
was the enormous addition to the amount in rates which it
was called upon to pay. The Hospital at Moorfields was
assessed by the City of London Union at a nominal amount
the rates for the year 1897 being only £88. The Holborn
Union, in whose area the new building was situated, adopted
a different course, and the rates for 1900 amounted to £870
nearly an eleventh part of the Hospital’s annual total expenditure.
In 1901 they increased to £948, and in 1902
to £972. No other hospital in London was assessed so
highly in proportion to its income and size, St. Thomas’s and
Guy’s being the only London hospitals paying heavier rates.
In answer to an appeal against such excessive rating the
authorities replied that, as the Hospital relieves patients
from every part of London, as well as many parts of the
country, they could not treat it on the footing of a local
charity.
In 1900 the Hospital, owing to its embarrassed financial
condition, was in arrears with the payment of two instalments
of rates, amounting to £324, and a summons was
served on it. The Justice of the Peace who had to deal
with the matter stated “that he had no other course but
to order payment within fourteen days.” This summons
became widely reported and commented on in the public
press; considerable sympathy with the Hospital was thereby
evoked, and in the course of three days donations and
subscriptions came in, amounting to £300, which enabled it
194temporarily to meet its difficulties. Ever since, however, the
annual amount which it has had to pay in rates has fluctuated
between £800 and £1,000. Thus this Institution, which
every year rescues numbers of people from loss of sight
and from becoming rate-supported, has to raise this large
sum in voluntary contributions from the benevolent public
to pay out in rates.
Until the year 1875 hospitals were not regarded as ratable,
as there was no obvious person connected with them to be
assessed. In that year, however, the House of Lords ruled
that voluntary hospitals had no right to such exemption
and must pay rates as other premises, though no one’s
sense of justice had appeared to be offended. If, as they
so frequently profess, public bodies wish to aid and support
the work of voluntary hospitals, no more efficient method
could be found than to exempt them again from this inconsistent
and burdensome form of taxation. In connection
with the Rating and Valuation Bill, which was before
the House of Commons in July, 1928, a discussion on the
rating of hospitals took place, being raised in connection
with an amendment proposed by Mr. Harris, Member for
South-West Bethnal Green, and seconded by Mr. Briant,
Member for North Lambeth. The Minister of Health,
Mr. Neville Chamberlain, whilst expressing his sympathy
with the matter, did not consider the Bill to be one in which
relief of that kind to hospitals could be given effect, it being
for the stimulation of industries, and he refused to consider
that the maintenance of the health of the community was
likely to give such stimulation.
What at first seemed likely to be a most severe blow to
the Hospital’s means of maintenance ultimately resulted in
its salvation. This was the establishment of the Prince of
Wales’ Hospital Fund (afterwards King Edward’s Hospital
Fund), and the diversion to it of annual subscriptions
previously paid to the Hospital—e.g., the Drapers’ Company,
195which had for several years given a subscription of
ten guineas, notified in 1900 that it would in future be discontinued
as the Company was subscribing annually to the
Prince of Wales’ Fund. The receipt of the following letter
was, therefore, a source of immense relief and satisfaction
to all connected with the Hospital:
“THE PRINCE OF WALES’ HOSPITAL FUND FOR
LONDON.
“The Bank of England,
“27th December, 1901.
“The Treasurer,
“Royal London Ophthalmic Hospital
“City Road, E.C.
“Sir,
“By the desire of His Royal Highness, the President,
I have the honour to enclose a cheque for £2,850.
“Of this sum, £900 is an annual grant to open eighteen
closed beds, on the condition that by the opening of these
beds eighteen more are made available for the sick poor in
your Hospital; and the balance of £1,250 is a special donation
for this year.
“I am also directed to inform you that your building is
reported on as a very fine new building. The Visitors state
that all the Wards, Operating Rooms, etc., are thoroughly
practical and up-to-date, and that your very complete
Hospital requires considerable additional funds to carry on
its useful work.
“Kindly acknowledge the receipt of the above.
“Yours faithfully,
“(Signed) S. Crossley,
“Honorary Secretary.”
In June, 1902, His Majesty the King himself became an
annual subscriber of ten guineas to the Hospital.
In December, 1902, a still more liberal grant was made
by the King Edward’s Hospital Fund for London, as shown
by the following letter:
“Sir,
“I am directed by His Royal Highness the President
to enclose a cheque for £4,500.
196
“Of this sum, £900 is an annual grant to support 18
beds opened by the aid of this Fund. The balance, which
consists of £1,100 as an annual grant and £2,500 as a special
donation for this year, is given on the condition that 30
more beds are opened in your Hospital so that by opening
those beds 30 more are made available for the sick poor
in your Institution.
“Kindly acknowledge the receipt of the above.
“Yours faithfully,
“(Signed) Savile Crossley,
“Honorary Secretary.”
The wards in the new Hospital were constructed to hold
138 beds, but at first, owing to its serious financial deficiency,
only 70 could be made available for use. By the help of
the King’s Hospital Fund in 1901, 18 more were opened
up, and, in the following year, by the help of the same fund,
an additional 30, leaving only 20 vacant. The opening
of the wards containing the additional 30 beds in 1902
was made a ceremonial occasion by the visit to the Hospital
in state of the Lord Mayor and some of the Sheriffs of the
City of London.
In order to pay off its liabilities, the Committee of Management,
during 1902, had to obtain a loan of £5,000 on the
security of the Harry Sedgwick Trust Fund, £7,000 of which
was retained by the Charity Commissioners until such time
as the compound interest on it had sufficiently accumulated
to repay the loan. The annual income of the Hospital was
thereby temporarily reduced by the interest on these two
amounts. In 1909, by the realisation of certain legacies,
the Hospital was enabled to repay this loan, the dividends
on the fund then reverting to it.
To find some fresh source of income it was agreed, at
a joint meeting of the Committee of Management and the
Medical Council, to try experimentally what could be
obtained by asking each out-patient on admission to make
a voluntary contribution, no compulsion to do so on any
account being used. At the end of three months it was
197found that an annual amount of £1,150 could be obtained in
this way, without giving any offence to those solicited for help.
The way in which the new building was constructed
necessitated some changes in the customs of the staff. The
out-patient department was entirely separated from the
in-patients, and it was thought desirable that the two classes
of patients should be kept completely apart. This necessitated
a second operating room specially for out-patients,
for which provision had been made, and over which a
special sister was appointed to preside. In the immaculate
in-patient operating theatre it became the established custom
for the surgeons working there to wear sterilised white cotton
coats, instead of their ordinary ones, as they had done
previously.
It may also be noted how customs have changed with
regard to the hirsute appendages of the face in the members
of the medical staff at different epochs. In the first half of
the nineteenth century, all the members of the staff wore
side whiskers. During the Crimean War our soldiers grew
beards, and on their return beards became the fashion of
the time. The surgeons at Moorfields, from the middle of
the century up to the commencement of what may be
described as the aseptic era, all wore beards. No surgeon
on the staff now wears a beard; they are all either clean-shaven,
or at most wear a closely-cut moustache.
The costume of the in-patients when taken into the
operating theatre also needed consideration, and in the
provision for them of special overalls the idea of a ladies’
working guild first originated. The following description
of its commencement and early progress was given in its
Fifth Annual Report, dated December 31st, 1904:
“In the winter of the year 1900, Mrs. Quarry Silcock,
Mrs. Treacher Collins, and the matron, Miss Richards,
with a few other ladies who had special opportunities of
knowing the difficulties with which the Hospital had to
contend for lack of funds and public interest, banded
themselves together and determined to help the Institution.
198They formed themselves into a Committee under the
Presidency of Lady John Tweedy, and were fortunate in
inducing many of their friends to join them. They determined
to take upon themselves the essentially womanly task
of supplying all the clothing, house and bed linen required
in the Hospital for the use of the patients, and so successful
were they that, not only were they able to do this, but by the
end of the second year they were in a position to hand the
sum of £50 to the general funds. The movement has since
so far grown that many more necessaries have been added.
The beds in the new wards, opened in 1903, were supplied
with blankets, coverlets, and sheets from the fund, and the
Guild has for the past two years maintained a Cot and a
Woman’s bed in the wards. It also extends its operations
in other directions that can be of help to the Hospital.
Through the consideration of several members, the Nurses’
library has been replenished with interesting and useful
books. Other members have rendered personal service by
visiting at the Hospital, and have thus relieved the monotony
of the hours spent by the suffering patients by reading
pleasant books, entering into kindly conversation with them,
and amusing them with singing and music. The cheering
effect of such visits and the assistance they are in the work
of recovery cannot be overestimated.”
Extensive as were the improvements in the new Hospital
over the old, in course of time fresh requirements cropped
up, and it was discovered that some of the arrangements
might have been better still. Any imperfections cannot,
however, be attributed to oversight on the part of the
architect, but rather to want of foresight and imagination
on the part of those from whom he received instructions
as to what to provide for. When first the rebuilding of the
Hospital was decided on, the question was discussed as to
whether the out-patient consulting room should be constructed
to allow for accommodation of an increase in the
number of the surgical staff, and the decision was deliberately
arrived at that no such increase was desirable or likely to
be required.
199
By the appointment of Soelberg Wells as an additional
assistant-surgeon in 1867, the number of the surgical staff
became increased to nine. Three surgeons attended each
day and each came twice a week. Such an evenly balanced
arrangement worked satisfactorily for a number of years.
In 1867 the number of new out-patients was 17,211; in
1900 the number had increased to 36,932—i.e., more than
double. The work entailed in dealing with this large
increase of patients was, however, far more than double in
amount to what it was in 1867, because sight-testing and the
correction of errors of refraction had increased both in
extent and accuracy. It is not surprising, therefore, that
those surgeons who had but few clinical assistants found
themselves unable to cope with all the demands made on
them. In 1890 the post of paid refraction assistant had
been created to aid the staff in that class of work. T.
Phillips held this post for a number of years: he attended
daily and became exceedingly expert in dealing with a large
number of cases in a very short time. When, however,
he was absent on a holiday or from illness, those who relied
upon his assistance experienced great difficulties in getting
through their work, patients even sometimes having to be
sent away unseen.
In 1900 the Committee of Management determined that
some fresh arrangement was essential, and advocated the
appointment of additional assistant-surgeons: after considerable
discussion this was agreed to, and the surgical
staff was increased to twelve. The three new members to
be appointed were to rank as assistant-surgeons, and their
work was to be confined to the out-patients, except in the
absence of the surgeon of the day. This was a reversion
to a former plan, which after a short trial broke down,
each member of the staff again attending to both out- and
in-patients. Fortunately at that time there were a large
number of able clinical assistants, who became candidates
for the new posts, from amongst whom Percy Flemming,
200assistant ophthalmic surgeon at University College Hospital,
J. Herbert Fisher, assistant ophthalmic surgeon at St.
Thomas’s Hospital, and Arnold Lawson (afterwards Sir
Arnold, and ophthalmic surgeon at the Middlesex Hospital)
were elected.
The result of this increase of the staff was that the out-patient
consulting room, originally designed to accommodate
three surgeons and their clinical assistants, had to accommodate
four.
When the number of beds in use became increased to
118, the services of a third house surgeon were found
requisite, those of the two senior being required for the
in-patients, and those of the junior being confined to the
out-patients. No accommodation had been made in the
new building for an increase in the resident staff, and some
reconstruction of rooms became necessary.
The accommodation required for the nursing staff had
been sadly underestimated, and a part of the building which
had been designed as an isolation quarters for sick nurses
had to be taken into general use. At the present time,
even with these additional rooms, it would be impossible
to make use of all the beds for in-patients with which the
Hospital is provided without first securing increased accommodation
for nurses.
A nurse may have completed three years’ training at a
general hospital and have acquired sufficient theoretical
knowledge to pass the examination which is considered
essential before she is granted a certificate, and yet be
incompetent to nurse a case of eye disease.
Moorfields Hospital has become, not only a special
training school for ophthalmic surgeons, but also for
ophthalmic nurses. Many who have been trained there
have subsequently been appointed to take charge of ophthalmic
institutions or departments in various parts of the
United Kingdom, in the Colonies, and in America.
In 1896 courses of lectures given by members of the
201surgical staff were instituted for nurses, in addition to the
instruction which they received from the matron: such
courses have been regularly carried on ever since. In 1907
arrangements were made with the authorities of the Queen
Victoria’s Jubilee Institute for Nurses to allow of the district
nurses employed by them to attend at the Hospital and
receive practical instruction in ophthalmic nursing free of
charge. Fifty-three such nurses attended at the Hospital
in 1907, and fresh ones have continued to attend ever since.
A large room was set apart in the new Hospital as a lecture
theatre, and, as the teaching became more systematised and
the number of students steadily increased, it became desirable
to have a Dean appointed to advise the students as to
their studies, and to superintend the classes: to this post
W. T. Holmes Spicer was elected in 1899. The teaching
at Moorfields up to 1920, when the Royal Colleges of
Physicians and Surgeons established a Diploma of Ophthalmology,
had been post-graduate and almost entirely clinical
and pathological, the laboratory and museum affording
excellent facilities for the latter. In order to obtain the
Diploma of Ophthalmology it became necessary for students
to pass a first examination in optics, and in the anatomy
and physiology of the parts concerned in ophthalmic surgery.
To meet the requirements of candidates for this examination,
Moorfields then instituted special courses of instruction
in these scientific subjects, upon which the practice of
ophthalmology must always be based. In so doing it has
become a complete school of ophthalmology.
Graefe, in his work on the ocular muscles, described what
are termed latent squints—i.e., squints which only become
manifest when the desire to see singly with the two eyes
is removed. Increased attention to them was awakened in
1886 when Stevens of New York suggested a convenient
form of nomenclature to describe their different varieties,
and in 1890 when Maddox of Bournemouth introduced a
simple and expeditious method for their detection and
202measurement. Some enthusiasts at first tended to
exaggerate the importance of these defects in the balance of the
ocular muscles, attributing to them numerous ills to which
the flesh is heir, and practising operative procedures for
their correction. On the other hand, some were slow in
devoting sufficient attention to them. Had more importance
been attached to them at Moorfields, at the time the
new building was under construction, better provision
might have been made in it for their investigation.
PLATE XXVI.
SIR JOHN TWEEDY, LL.D.
In the closing years of the nineteenth century the science
of bacteriology increased both in its importance and in its
technique by leaps and bounds. In 1901 the medical staff,
finding that more bacteriological investigations were required
than the pathologist had time to devote to them in association
with his other duties, recommended the establishment
of a special bacteriological department and the appointment
of a special bacteriologist. This entailed the provision
of additional laboratory accommodation, and it was
not until six years later that the Committee could see their
way to the erection of a new laboratory above that part
of the pathological department occupied by the Museum
and curator’s room, part of a legacy left to the Hospital
by the late Mr. Samuel Lewis being used to defray the
cost.
John Tweedy, who had been elected on the staff at the
comparatively early age of twenty-nine, resigned in 1900
at the age of fifty-one, and was appointed consulting surgeon,
the Committee of Management putting on record at the
time its appreciation of the “numerous occasions he had
pleaded the cause of the Hospital in powerful and most
interesting public addresses, endorsing his advocacy with
liberal donations to its funds.” Tweedy was a fluent and
learned writer; he served for a long time on the editorial
staff of the Lancet, so that most of his contributions appeared
anonymously. He did not contribute much to the literature
of ophthalmology, though he had had a very large
203experience and was frequently called into consultation by
his colleagues in difficult cases. An American student once
asked him which he considered the best textbook on ophthalmology.
Tweedy took a deep breath, with which, on
account of some chest affection, he always preceded any
oratorical remark, and, with a dramatic wave of the arm
towards a crowd of patients that were waiting to see him,
said: “There, that is the best textbook.”
Three years after his retirement from the staff of the
Hospital, he became President of the Royal College of
Surgeons; he held that post for three years, and was
knighted in 1906. He possessed remarkable administrative
capacity, and was skilful in putting through the business of
a meeting with efficiency and dispatch. He also presided
over the Ophthalmological and Medico-Legal Societies, the
Medical Defence Union, and the Royal Medical Benevolent
Fund. He died in 1924 at the age of seventy-five.
With the discovery of the ophthalmoscope the interests
of ophthalmologists became largely medical as well as
surgical; though they still style themselves ophthalmic
surgeons, some might more aptly be termed ophthalmic
physicians; Marcus Gunn was one of these. The distinguished
neurologist, Sir William Gowers, in 1879, wrote a
book on Medical Ophthalmoscopy, which was the leading
manual of its kind for many years; its third edition, which
appeared in 1890, was edited by Marcus Gunn. He was
a most careful ophthalmoscopic observer, and for several
years devoted his attention to certain changes in the retinal
bloodvessels. Writing on the outcome of these observations
in 1898, he said:
“The chief importance of this retinal arterial change lies
in its association with a more general arterial disease of a
similar nature, particularly in the kidneys and brain, and in
its prognostic value in regard to the results which may
follow in cerebral vessels. It has been well said that ‘a
man is as old as his arteries.’ I would urge that ophthalmoscopic
204observation is one of the most ready clinical
means for the early detection of important arterial
changes.”
Rheumatism is a term which is applied to a multiple of
ills, and during the nineteenth century a number of cases
of inflammation of the iris were so classified. The most
typical and well-defined form of rheumatism is rheumatic
fever or acute articular rheumatism, and investigations of a
number of such cases at general hospitals, and of cases of
iritis at Moorfields, showed that the two affections were
but rarely associated. Iritis not uncommonly occurs in
connection with inflammation of the joints due to gonorrhœa,
which is sometimes termed “gonorrhœal rheumatism,” but
a very large number of cases of iritis are met with unassociated
with any joint affection or any venereal disease. Of
recent years, largely as the outcome of the observations and
teaching of William Lang, it has become recognised that
such cases are secondary to some focus of inflammation
elsewhere in the body, very often a septic condition in
connection with the teeth. Seeing how many people suffer
from septic teeth who never develop iritis, considerable
scepticism at first prevailed as to its being the cause of the
disease. The satisfactory way in which iritis subsides and
ceases to recur after the septic focus in the mouth has been
removed seems, however, to have definitely established the
relation of the one to the other, and provided a means of
eradicating a very potent cause of suffering and destruction
of sight.
PLATE XXVII.
WILLIAM LANG
The reawakening of the importance of the medical side
of ophthalmology made the surgical staff desirous in 1899
of securing for their patients at the Hospital the aid and
assistance of a physician who had had a special training as
a neurologist. For this purpose, it was decided to appoint
a second physician who should be required to attend the
Hospital once a week to examine and report on such cases
as were selected for him by the surgical staff. Dr. James
205Taylor, who had studied under Dr. Hughlings Jackson, and
who may be regarded as one of his most ardent disciples,
was elected to this post.
The systematic and orderly keeping at Moorfields of the
clinical records of in-patients, and of the pathological
examination of the eyes removed, over a number of years
by successive house surgeons and curators of the Museum,
has provided a large amount of valuable material for the
investigation of the natural history of certain diseases from
which useful inferences as to their incidence and prognosis
can be drawn. Such method of investigation has been
applied by a succession of workers, over a period of fifty-seven
years, to the different forms of malignant growths
originating in the eyeball, and has added considerably to
our knowledge concerning them, the results being published
in the Hospital Reports.
A distinguished ophthalmic surgeon from New York
who visited Moorfields went away much impressed by
Nettleship, because he showed and discussed with him
nothing but his failures. Most operating surgeons like to
exhibit their successes and keep their disasters in the background,
but by the study of our failures lies the road to
future success. The curator of the Museum at Moorfields,
or pathologist as he is now called, has the opportunity of
examining critically all the eyes removed after the failure
of operative procedures by the various members of the staff.
From such examinations much valuable information has
been collected and published, both in connection with
operations for the removal of cataract and for the relief
of glaucoma. To have had the advantage of carrying out
these examinations must necessarily be an excellent training
for one who is to become an operator himself. It is not,
therefore, surprising that all those who have in recent years
held the post of pathologist have subsequently been promoted
to the surgical staff.
C. Devereux Marshall, who held the post of curator of
206the Museum from 1894 to 1899, was elected assistant-
surgeon on the retirement of Tweedy from the staff. William
T. Lister (now Sir William Lister, K.C.M.G.) was the
curator from 1899 to 1901, and was elected assistant-surgeon
on the retirement of Waren Tay in 1904. John
Herbert Parsons (now Sir John Parsons, C.B., F.R.S.) was
curator from 1901 to 1905, and was elected assistant-surgeon
to fill the vacancy caused by the death of A. Quarry Silcock
in 1904.
When, in 1891, elementary education was made universal
and compulsory, those responsible for the measure little
realised all that it would involve. They little thought
that in 1927 it would lead to the provision of 16,000,000
meals for school-children, and the medical examination of
2,000,000, involving the employment of about 2,000 doctors,
600 dentists, and 5,000 nurses, or that it would develop
into what Sir George Newman, the chief medical officer
of the Board of Education, describes as “the grand inquest
of the nation directed towards laying the foundation of the
nation’s health.”
It soon became evident that it was futile to compel
children to study if their physical condition was such that
they would not profit thereby, or if it was likely to lead to
their physical deterioration. The question of their eyesight
and its possible impairment from study early attracted
attention. At first the teachers of the London School Board
were given instructions to test the children’s eyesight, and
to give the parents of those in whom they found it defective
a printed paper, stating that their child was suffering from
a defect of vision, and, in the child’s interests, they were
strongly advised to consult an oculist without delay. To
this notice was attached a list of hospitals with eye clinics
and the times at which they were open for patients. The
periodic rush of school-children with their parents to
these clinics created chaos in their ordinary working
routine.
207
In 1908 the Board of Education issued a circular stating
that suitable provision can be made by a local education
authority for the prescription and purchase of spectacles;
and that, in this connection, the Board will be prepared to
entertain proposals for contributions to the funds of hospitals
on terms of adequate advantage, and the contributions are
specially desirable in the case of eye hospitals. Also that
“it is permissible to include among the conditions of contribution
a provision allocating a reasonable remuneration
to the medical men working for such institutions.”
In the following year, in response to the invitation of the
London County Council Education Committee, the Committee
of the Hospital agreed to co-operate with it for the
treatment of children whose eyes required attention, on the
basis that not less than 3,000 nor more than 6,000 children
be sent during the year, and that the Council would pay
for the extra assistants which the Committee would have
to appoint to carry out the work.
When the new Hospital was built, a portion of it on the
ground floor had been left uncompleted, it being thought
that it might ultimately be used as a chapel. The chaplain
found it most convenient to conduct his services in the
day wards. So, in 1909, through the generous help of
some friends of the Hospital, donations were collected for
the special purposes of carrying out certain alterations to
this unoccupied part of the building to provide and equip
a refraction department for school-children, separate from
the other out-patients. This school-children’s department
was completed and became ready for use in 1910. While
the majority of the children which attend require spectacles
for the correction of errors of refraction, some are found
to be suffering from some other affections of the eye, and
these are referred for treatment to the ordinary out-patient
department.
On the death of Queen Victoria, who had been a Patron
throughout the whole of her long reign, in 1901, King
208Edward VII, and Queen Alexandra consented to continue
the patronage of the Institution which they had extended
to it as Prince and Princess of Wales. In the same way,
the Prince and Princess of Wales agreed to continue the
patronage which they had bestowed on it when Duke and
Duchess of York.
On the removal to the new Hospital, it had been foreseen
that special steps would have to be taken to provide for the
payment of the ground rent of £1,210 a year, and in 1899
John Tweedy started the “Rent Fund” with a generous
donation of £150, to which he later added a further donation
of £50. Owing, however, to the South African War and
the pressing need to defray current expenses, but very slow
progress was made in the collection of donations to this
fund. In 1904, to celebrate the centenary of the foundation
of the Hospital, the Committee decided to change the name
of the fund to that of the “Centenary Fund,” and to make
a special appeal for contributions to it, all donations to be
invested and the interest on it devoted to the payment of
the rent.
A Centenary Festival Dinner was held at the Hotel
Cecil on May 10th, over which Sir Charles Wyndham
presided, delivering a most eloquent appeal on behalf of
the Charity. The following ladies kindly acted as hostesses
on the occasion: Princess Alexis Dolgorouki, the Hon.
Helen Henniker, Lady Critchett, Lady Burnand, Lady
Wyndham, Lady Walker, Mrs. Marcus Gunn, Mrs. Widenham
Fosbery, Mrs. Edward Nettleship, Mrs. F. C. Scotter,
Mrs. Beerbohm Tree, Mrs. Brooman-White of Arddaroch,
Mrs. J. S. Wood. Three hundred guests were present,
and the proceeds of the dinner, amounting to £2,270, were
added to the Centenary Fund.
In former times it was the custom to end a story by drawing
a moral; all such moral conclusions are nowadays regarded
as out of fashion, and even a plot is no longer considered
as essential in a story. All that is required is just to describe
209a slice out of life, beginning anywhere and ending when the
requisite number of pages have been filled. This story of
the Moorfields Eye Hospital describes a slice out of the life
of an institution, commencing with its foundation in 1804,
and ending, whilst it is still full of progressive vigour, with
the celebration of its centenary.
Most people will agree that the chief object of raking
over the ashes of the past should be to acquire inspirations
for the future; and so, though it may be hopelessly out of
fashion, this story will conclude with some maxims which
may be deduced from all that has gone before.
The general principle on which the Hospital was established
was that the treatment of diseases of the eye and
visual disorders should be recognised as a branch of medicine
and surgery, and not left in the hands of unqualified and
imperfectly trained practitioners. With this end in view,
it has always been insisted on that the members of its medical
staff should hold the highest possible qualifications as
physicians and surgeons, and that every encouragement
should be given to qualified medical men to come to it to
study the treatment of eye diseases as a branch of medicine
and surgery. The necessity for the recognition of this
general principle, now in 1929, is just as necessary as in
1804, there being, as then, no short road to the efficient
treatment of visual defects apart from a complete training
as a medical practitioner.
The question is sometimes asked: Do special hospitals
justify their existence? The perusal of this book, it is
hoped, will at any rate show that the Moorfields Eye Hospital
has justified its existence.
One of the incomparable advantages afforded by a special
hospital is the field which it offers for mass observation,
both clinical and pathological. It was by taking advantage
of the extensive opportunities for clinical research which
Moorfields Hospital affords that Sir William Lawrence,
Sir Jonathan Hutchinson, Dr. Hughlings Jackson, Edward
210Nettleship, and others have been able to make their most
valuable contributions to our knowledge of the natural
history of eye diseases.
Pathological research in connection with eye disease
depends almost entirely on the investigation of eyes which
have had to be removed during life, and at Moorfields the
custom of placing the mass of such material at the disposal
of one man, the curator of the Museum, whilst he holds
office, has proved to be of inestimable advantage in the
promotion of that line of research.
To arrive at an accurate estimate of the benefits to be
derived from any special line of treatment or from some
operative procedure, it is necessary that it should be tried
in the various varieties and phases of a disease; inferences
drawn from isolated cases must always prove fallible. The
mass of cases provided by a special hospital allows of reliable
estimates being arrived at.
The facilities for mass observation which a special hospital
affords are of as great advantage to the student as to the
investigator. It enables him, not only to get a comprehensive
picture of a disease in all its manifestations firmly
impressed on his mind, but also to see in a comparatively
short time several examples of what, in a more restricted
sphere, would be regarded as rare affections. It has been
the recognition of such advantages that has induced medical
men from all parts of the world, for over a hundred years,
to congregate at Moorfields to gain instruction and
experience.
It has not, however, been only the size of the clinic which
has attracted students of ophthalmology to Moorfields, but
also to a large extent the personnel of its medical staff. To
listen to discussions on debatable matters by able exponents,
holding forth day after day from the same pulpits, and to
watch varying forms of procedure on similar conditions
carried out in the same theatre by different operators,
stimulates students to observe and to think for themselves
211—a form of training which is far preferable to the absorption
of dogmatic aphorisms from a single teacher, or the
attendance at courses of didactic oratory.
Medicine and surgery are not exact sciences, and probably
never will be; any increase in exactitude in connection with
them may, however, be regarded as synonymous with progress.
The immense increase in exactitude in connection
with ophthalmology which has taken place since the discovery
of the ophthalmoscope can be realised, if we consider
the number of well understood conditions which are now
differentiated, and which were formerly grouped under the
vague heading of “Amaurosis.” Ophthalmology is closely
associated with such exact sciences as mathematics, chemistry,
and physics. It was, indeed, from the association of the
latter with ophthalmology that the discovery of the ophthalmoscope
resulted; for, as Helmholtz himself said, “When
a well-trained physicist came and grasped the importance
of such an instrument, nothing more was wanted, since all
the knowledge had been developed which was required for
its construction.”
William Cumming had grasped the possibilities of such
a discovery, but, lacking himself the necessary training in
physics and failing to consult anyone who had, missed
the way to the end for which he was striving.
It was the fortunate circumstance of Sir James Mackenzie
Davidson being interested in both physics and ophthalmology,
at the time of Professor Röntgen’s discovery of the
X-rays in 1895, that led to their early employment at Moorfields
in connection with foreign bodies implanted in the
eyeball, and the introduction of an accurate method for their
localisation.
Of the intimate association of mathematics with ophthalmology
we have evidence in Helmholtz’s great work on
physiological dioptrics. Donders, in the preface to his
book On the Anomalies of Accommodation and Refraction of
the Eye, with a Preliminary Essay on Physiological Dioptrics,
212published by the New Sydenham Society in 1844, writes
as follows:
“In the doctrine of the anomalies of refraction and accommodation,
the connection between science and practice
is more closely drawn together than in any part of medicine.
“Science here celebrates her triumph, for it is at her
hand that this branch has acquired the exact character
which makes it also worthy of the attention of natural
philosophers and physiologists. It is, indeed, satisfactory
to see, how in the accurate distinction between anomalies
of refraction and accommodation with exclusion of every
condition foreign to those anomalies, the system assumed,
as if spontaneously, an elegant simplicity; and how the cause
and mode of origin of many an obscure type of disease
emerged into the clearest light.
“Practice, in connection with science, here enjoys the
rare but splendid satisfaction of not only being able to give
infallible precepts based upon fixed rules, but also of being
guided by a clear insight into the principles of her actions—
advantages the more highly to be estimated as the anomalies
in question are of more frequent occurrence, and as they
more deeply affect the use and functions of the eyes.
“Is it, then, strange that the study and treatment of my
subject have been to me a labour of love? the more so, as
I felt proud in having been called upon to elaborate it for
a country in which Young, Wells, Ware, Brewster, and Airy
have pointed out to us the track which we had only to follow,
and happy in being able to offer my work in this form to
my highly esteemed friends and colleagues, whose proofs
of kindness and affection have left with me the most agreeable
recollections of my visits to England.”
In its indebtedness to chemistry, ophthalmology shares
with all other branches of medicine and surgery. It was
to the chemist Louis Pasteur that we owe the upgrowth of
the new science of bacteriology. It is to Madame Curie’s
chemical researches that we are indebted for radium, which
promises to be the most effectual means for dealing with
malignant neoplasms apart from operations.
It is to Wassermann that we owe the possibility of a
213chemical means of diagnosing syphilis, and to Ehrlich a
chemical compound which will kill the invading organism
without damaging the tissue of the infected host.
From what has gone before it would seem that measures,
which tend to bring about a close association between the
clinical work in the Hospital and the laboratory work of the
trained observers in these exact sciences, are those most
likely to prove fruitful in the promotion of the progress of
ophthalmology in the future.
Hospitals in the first part of the nineteenth century were
institutions founded and supported by the rich for the relief
of suffering in the indigent poor, the inmates admitted to
which were given everything for nothing.
Under altered conditions, they are now rapidly becoming
institutions for the relief of suffering in the community at
large, supported in part by donations from munificent
persons, and in part by contributions from those who receive
benefits in them.
In former times the word “hospital” raised in the mind
a picture of a barrack-like building, associated with pain
and suffering, with poverty and death.
John Couper, when senior surgeon at the London Hospital,
was journeying to it down the Mile End Road in one of the
old horse-drawn omnibuses, and asked the conductor to
put him down at the London Hospital; the conductor
shouted out to the driver, “Stop at the slaughter-house
Bill.”
Since the introduction of anæsthetics and antiseptics
hospitals are no longer regarded as slaughter-houses by the
general public, but as places where pain and suffering are
relieved, and health and vigour are restored. No longer are
they forbidding barrack-like structures, but temples of
hygienic cleanliness. No longer is it a luxury to be ill,
or to have an operation performed in one’s own home,
where all the necessary appliances have to be imported or
improvised. Far preferable has it become to go to an institution
214specially constructed for such purposes, furnished
with the most up-to-date contrivances, and with a staff
efficiently trained to meet all emergencies.
In a Report of a Special Committee of the King Edward’s
Hospital Fund for London on “Pay Beds,” dated July,
1928, the present relation of various sections of the general
public to hospitals is set out as follows:
“During recent years there has been a considerable extension,
both of the classes included amongst Voluntary
Hospital patients and of the payments made by ordinary
patients. There was a time when the Hospitals were only
called upon to provide comparatively simple treatments for
the necessitous poor, which meant those who were unable
to pay for medical attendance. With the development of
expensive methods of treatment and diagnoses, large numbers
of the middle and professional classes are now unable
to pay the full cost of these services, some of which, according
to our evidence, are often difficult to obtain outside the
Hospital.
“At the same time, experience has shown that large
numbers of the ordinary Hospital patients are both able and
willing to contribute towards their cost. At present,
therefore, there is a demand for Hospital treatment from
several different classes which may be grouped into three:
First, those who cannot afford to pay anything, and who
receive, when in the ordinary wards, free maintenance and
treatment; second, those who can and do contribute
according to their means towards their cost of maintenance
in the ordinary wards, though still receiving free medical
attendance from the visiting staff of physicians and surgeons;
third, those whose standard of living causes them to desire
better accommodation, or at all events more privacy, than
is provided in the ordinary wards, and who are prepared to
pay for it according to their means, and also to pay something
for medical attendance. Beyond these, there is a
fourth class, those who can afford to obtain their treatment
in private nursing homes and to pay full medical fees.”
Institutions, like individuals, if they wish to survive in
the struggle for existence, have to obey the universal law
of adaptation to environment. Moorfields Hospital, during
215the first hundred years of its existence, has undergone
reconstruction, had additions made to it, and has twice
been removed to a new site, in response to the demands
made upon it by the increasing number of patients attending
for relief, and to the developments and discoveries in the
methods of applying relief.
To be capable of such frequent fresh adaptations, an
institution must be prepared to obey another biological
law—that of retaining a high degree of plasticity, which,
in the case of an institution, is equivalent to maintaining
a big margin for expansion.
As has been shown, Moorfields is largely indebted to the
foresight of its architects for having retained such a margin
for expansion to meet new requirements. When first a
new Hospital was erected on the Moorfields site, Sir Robert
Smirke, the architect, advised the Committee to secure the
freehold of a piece of vacant ground immediately behind
the Hospital, upon which, after the discovery of the ophthalmoscope,
a new out-patient department with a large dark-room
was built. It was also, probably by his advice, that
Dr. Farre secured the lease of the piece of ground on its
south side, part of which he for a time let off for a stables
and in part used for the Saunderian Institute, but upon
which a new wing of the Hospital was subsequently built,
when the demand for more in-patient accommodation
became urgent, after the introduction of anæsthetics and the
great increase in the number of operative procedures. When
the removal to a new site again became necessary, it was
the proceeds derived from the greatly enhanced value of
these sites, which had been so fortunately obtained, that
supplied the funds for the erection of the new building.
It was due to the advice of the architects, Keith Young
and Bedell, that the large site in the City Road was chosen
for the present Hospital, instead of the cramped one in
Eldon Street adjoining the former building, to which at
the time sentiment made a strong appeal.
216
In the twenty-five years which have elapsed since the
celebration of the Hospital’s centenary, fresh discoveries and
altered economic conditions have produced further changes
in environment, calling for more expansion in one direction
and another. Fortunately, the plasticity of the present large
site is by no means exhausted, and with suitable adaptation
it is capable of providing all the demands likely to be made
upon it for several years to come.
The last maxim, however, to be drawn from the past
history of the Hospital is the necessity of keeping ever alert
for adaptations to meet fresh changes in its environment
as they arise.
217
APPENDIX
Presidents
Date of Appointment.
Date of Resignation.
Sir Charles Price, Bart.
1804
1818
Mr. William Mellish
1818
1838
Rt. Hon. Earl Fitzwilliam
1838
1856
Mr. William Cotton, D.C.L., F.R.S.
1857
1867
Sir John Lubbock, F.R.S., M.P. (afterwards Lord Avebury)
1867
1913
His Royal Highness Prince Arthur of Connaught, K.G.
1914
Chairmen of the Committee of Management
Mr. Harry Sedgwick
1804
1818
Mr. Ralph Price
1818
1830
Mr. Stuart Donaldson
1831
1837
Rev. J. Russell, D.D.
1837
1857
Mr. Richard Heathfield
1857
1859
Mr. F. G. Sambrooke
1860
1871
Mr. Philip Cazenove
1871
1879
Mr. Charles Gordon
1879
1897
Mr. H. P. Sturgis
1897
1921
Mr. Theodore W. Luling
1921
Honorary Medical and Surgical Officers
Physicians
John Richard Farre, M.D.
1805
1857
Frederick J. Farre, M.D.
1843
1880
Robert Martin, M.D.
1856
1884
Sir Stephen Mackenzie, M.D.
1884
1905218
James Taylor, C.B.E., M.D.
1899
1919
Gordon M. Holmes, C.M.G., C.B.E., M.D.
1914
1927
William J. Adie, M.D.
1927
Surgeons
J. Cunningham Saunders (Founder)
1804
Died 1810
Benjamin Travers, F.R.S.
1810
1817
Sir William Lawrence, Bart., F.R.S.
1814
1826
Frederick Tyrrell
1817
Died 1843
John Scott
1826
1846
Gilbert Mackmurdo, F.R.S.
1830
1856
John Dalrymple, F.R.S.
1832
1849
James Dixon
1843
1868
George Critchett
1843
1877
Sir William Bowman, Bart., F.R.S.
1846
1876
Alfred Poland
1848
1861
H. H. Mackmurdo
1851
1852
John C. Wordsworth
1852
1883
J. F. Streatfield
1856
Died 1886
J. W. Hulke, F.R.S.
1858
1890
George Lawson
1862
1891
Sir Jonathan Hutchinson, F.R.S.
1862
1878
John Couper
1866
1895
J. Soelberg Wells
1867
Died 1880
Waren Tay
1877
1904
James E. Adams
1877
1884
Sir John Tweedy, LL.D.
1878
1900
Robert Lyall
1880
Died 1882
Edward Nettleship, F.R.S.
1882
1898
R. Marcus Gunn
1883
1909
W. Lang
1884
1912
A. Quarry Silcock
1886
Died 1904
J. B. Lawford, LL.D.
1890
1918
A. Stanford Morton
1891
1909
E. Treacher Collins
1895
1922
W. T. Holmes Spicer
1898
1920
Percy Fleming
1900
1919
J. Herbert Fisher
1900
1927219
Sir Arnold Lawson, K.B.E.
1900
1914
C. Devereux Marshall
1900
Died on active service, 1918
Sir William T. Lister, K.C.M.G.
1904
1905
1919
Sir John Herbert Parsons, C.B.E., F.R.S.
1905
Claud Worth
1905
1921
W. Ilbert Hancock
1909
Died 1910
George Coats
1909
Died 1915
Malcolm L. Hepburn
1910
1926
A. Cyril Hudson
1913
1928
R. Foster Moore, O.B.E.
1914
R. Affleck Greeves
1915
F. A. Juler
1918
Charles Goulden, O.B.E.
1919
B. T. Lang
1920
Died 1928
M. H. Whiting, O.B.E
1921
P. G. Doyne
1922
Humphrey Neame
1926
Miss Ida C. Mann
1927
W. Stewart Duke-Elder
1928
Rupert S. Scott
1928
Ear, Nose, and Throat Surgeon
G. Seccombe Hett
1923
1929
Medical Officer to the X-Ray Department
Sir James Mackenzie Davidson
1899
1910
Albert Bowie
1910
Dental Surgeons
Arthur E. Relph
1913
1915
R. M. Fickling
1915
1928
Stanley A. Riddett
1928
Medical Officer to the Ultra-Violet Ray Department