The Project Gutenberg EBook of The Matron's Manual of Midwifery, and the
Diseases of Women During Pregnancy and in, by Frederick Hollick
This eBook is for the use of anyone anywhere in the United States and most
other parts of the world at no cost and with almost no restrictions
whatsoever. You may copy it, give it away or re-use it under the terms of
the Project Gutenberg License included with this eBook or online at
www.gutenberg.org. If you are not located in the United States, you'll have
to check the laws of the country where you are located before using this ebook.
Title: The Matron's Manual of Midwifery, and the Diseases of Women During Pregnancy and in Childbed
Being a Familiar and Practical Treatise, more especially
intended for the Instruction of Females themselves, but
adapted also for Popular Use among Students and
Practitioners of Medicine
Author: Frederick Hollick
Release Date: January 1, 2015 [EBook #47836]
Language: English
Character set encoding: UTF-8
*** START OF THIS PROJECT GUTENBERG EBOOK MATRON'S MANUAL OF MIDWIFERY ***
Produced by Cindy Horton, Sarah Jensen and the Online
Distributed Proofreading Team at http://www.pgdp.net (This
file was produced from images generously made available
by The Internet Archive/American Libraries.)
The cover image was created by the transcriber, using the book's original title page, and is placed in the public domain.
BEING A FAMILIAR AND PRACTICAL TREATISE, MORE
ESPECIALLY INTENDED FOR THE INSTRUCTION OF
FEMALES THEMSELVES, BUT ADAPTED ALSO
FOR POPULAR USE AMONG STUDENTS
AND PRACTITIONERS OF MEDICINE.
By FREDERICK HOLLICK, M. D.,
LECTURER ON PHYSIOLOGY AND FEMALE DISEASES,—
AND AUTHOR OF THE DISEASES OF WOMAN,—
OUTLINES OF ANATOMY AND PHYSIOLOGY
FOR POPULAR USE,—NEUROPATHY,—
AND THE ORIGIN OF LIFE.
ILLUSTRATED BY OVER 50 SPLENDID ENGRAVINGS.
NEW YORK:
PUBLISHED BY T. W. STRONG,
NO. 98 NASSAU STREET.
BOSTON:—NO. 64 CORNHILL.
1849.
Entered according to Act of Congress, in the year 1848,
By FREDERICK HOLLICK, M. D.,
in the Clerk's office of the District Court of the United States for the
Southern District of New York.
The price of this Book is One Dollar.—It may be obtained of all Booksellers, or of T. W. Strong, 98 Nassau-st., N. Y., who will also send it by Post to any part of the country, on receiving One Dollar and the Address.—N. B. All Dr. Hollick's other Books will be sent by T. W. Strong in the same way.
A short time ago I published a popular treatise on The Diseases of Woman, in the non pregnant state, and in that work I announced my intention of shortly publishing a similar one on Pregnancy and its diseases. This book is the fulfilment of that promise.
Being the first popular, and yet strictly scientific and practical book on Midwifery ever published, its preparation has necessarily been a work of great labour and difficulty. Everything had to be simplified; familiar explanations had to be given of complicated processes, and illustrations had to be designed that could be understood by my readers. Little or no assistance could be obtained from other works on the subject, because they were either designed for professional men; and therefore too technical, or else were too general in their explanations, and too unsystematical, to be of any practical use. I therefore had to write every part afresh myself, and plan a new arrangement; and so difficult was this to do, satisfactorily, that I have twice before completed the whole work, and then commenced at the beginning again, before I was satisfied with my own production.
As it now stands, I trust this treatise answers the purposes for which it was intended. I have taken care to make it so complete, and scientific, that a medical student may take it for his text book; and at the same time I have endeavoured to so simplify it that any female, of ordinary capacity, can fully understand both its explanations and practical directions. All purely technical words have been avoided, or, when absolutely necessary, they have been carefully explained. Every topic connected with the main subjects has been discussed, and the latest information given on every point, and from every source.
Such a work as this has long been needed. Females have been kept in shameful ignorance, of everything connected with their own systems, and of the wonderful phenomena in which they play so important a part. That ignorance has led to untold evils, which can never be corrected till they become more enlightened respecting themselves. Fortunately many of them begin to see this, and they request, in behalf of themselves and their sisters, that such knowledge be no longer withheld. I have been now, for a long time, engaged in this pleasing task of female instruction, both by my Lectures and books, and in my daily communion with them as patients; I am therefore aware both of their great lack of proper information, and of their strong desire for it, and I flatter myself I also know, from experience and careful observation, the best mode of imparting it to them. In fact, I have made it a matter of careful study, not only to render my subject[iv] plain, but also pleasing and unobjectionable; so that the most unreflecting shall feel an interest in it, and the most sensitive be able to study it without pain or repugnance.
The object of this book is not to make every woman a professional Midwife, nor to induce her to dispense with proper assistance in her hour of difficulty, but simply to explain to her the nature and manner of child-birth, and the means by which she is to be assisted. This will disabuse her mind of many pernicious errors—make her more patient under her unavoidable difficulties and pains—more docile to what is required of her, since she will see the reason for it—and it will also enable her to avoid much positive suffering, and to render great help, in many cases, to her attendant.—In a case of emergency also, when other assistance cannot be procured time enough, or not at all, it will teach one female how to assist another in delivery, which every one of them ought to be able to do. Very often it happens that a case of this kind occurs, and the Females around, instead of knowing how to help the sufferer, are utterly useless, and even make her worse by their evident terror and ignorance. I have known women die in child-bed, for want of the most trivial assistance, which even a child could understand how to give, though there were elderly females, mothers themselves, around her; but they knew not what to do. Such a state of things is disgraceful to the boasted intelligence of the age, and should be remedied as speedily as possible. Every Adult female, or at least every married one, should be instructed in these things, so that she may know how to regulate her own conduct and how to render useful assistance to others in case of need. Ill informed women are generally as apprehensive of danger as they are incapable of avoiding it; and as regardless of proper advice as they are ignorant of the reason for it.
The time, I trust, is fast coming, when every female will be taught, as of paramount importance, everything which concerns her own welfare; and when ignorance will no longer be considered necessary to propriety and virtue, nor useful knowledge incompatible with the most refined delicacy and the strictest morality. I consider it my duty to assist in hastening that time, and I feel much pleased that my previous efforts have been so much commended. This book I hope will be equally acceptable, and, if possible, more useful, than those which have preceded it.
F. HOLLICK, M. D.,
New York
Parturition, or the expulsion of the perfectly formed human being from the body of its mother, is a most wonderful natural function, for the complete and safe performance of which at the proper time, every requisite is found to exist. Notwithstanding the contrary experience of society, as it now exists, it is well known that extreme suffering, and danger to life, are not necessary nor even probable accompaniments to child-birth; for it is invariably found, when females live under circumstances favourable to their full physical development and health, that it occurs speedily, and with little or no difficulty or pain. Numerous proofs of this could be given in accounts of the Indians, and other uncivilized females, among whom parturition is regarded as an ordinary occurrence, for which no preparation need be made, and about which no apprehension need be felt; such facts, however, are so well known that they only need be referred to here.
As the organization and requirements of society changes, by the adoption of what is called civilization, the condition of woman becomes very different to what it was originally. In many respects her lot is much meliorated, and she has great reason to be pleased with the change, but in other respects she has not been so fortunate.
One great evil resulting from her altered position is, a neglect of proper physical education while young, and of the various requirements for bodily health in after life. In consequence of which she becomes constitutionally weaker, and more sensitive to various injurious influences, which she possesses diminished powers to withstand. This evil increases in proportion as civilization advances, until at last females become so imperfectly organized, and so enervated, that they are utterly unable to fulfil the duties assigned them, and they either die prematurely, or pass their whole lives in suffering and complaint. So universally is this the case at the present time, particularly in cities, that the exempt are very rare exceptions to a rule most lamentably general. Unfortunately, custom and false notions have given this melancholy state the stamp of propriety, and thrown around it the charm of fashion. The suffering invalid is called interesting, and the pale faced debilitated creature, scarcely able to crawl about, is styled genteel, while robust health and physical capability is termed coarseness and vulgarity. So infatuated, and weak minded, have females been made on this point, that I have actually known some of them quite chagrined because people could see they were well and strong; and I have known others quite alarmed for fear that they should look so. A short time ago I knew a lady who, by the adoption of a proper course of training and treatment, passed through her confinement so quickly, and with so little exhaustion, that she was up and travelling about in three days after, not only without inconvenience but with pleasure and advantage. But what was the impression made on her female friends by such a speedy recovery? did they feel quite pleased at it, and desirous that all others should be equally fortunate? No; but quite the contrary! She was actually thought deserving of reprehension, and was stigmatized as vulgar in the extreme. One person even made the remark, that she must be a very common person, and no Lady! Now what a pitiable state of ignorance, and mental imbecility, these females must be in, to be actually proud of their infirmities;[vi] and yet they are but like the majority of their sex. If they were not so unfortunate in not knowing their true interests, they would be highly culpable, but as it is they are truly deserving of our pity.
It must be admitted, however, that though civilization has, so far, entailed these evils on women, it has also done much to alleviate them. Many diseases are beneficially modified, and some are even cured, by medical treatment; surgical science has also attained a high point of perfection; and the difficulties attendant on child birth are overcome to a great extent by obstetrical skill. But notwithstanding all this alleviation, these evils are still deplorably great. The utmost scientific skill to which society can ever attain, will do but little towards effectually relieving human suffering, and removing disease, so long as it is entirely devoted to the mere art of curing and palliating as it chiefly is now. Our knowledge of the human system, and of the causes which produce in it disease and deterioration, must be universally disseminated, so that the whole people may see how these evils arise, and how they should live, and conduct themselves, so as to avoid them altogether! or, in other words, science should teach us how to prevent disease and suffering, instead of merely how to alleviate them. Eventually this will be done, and our females will then pass through their travail as easily as their savage sisters do now. Let us hope that time will soon come; and let every one esteem it his duty, who possesses the ability, to hasten its coming, by doing all he can to spread the necessary information to those who need it.
The happy exemption from difficulty and suffering which females enjoy in more uncultivated states of society, and which we believe they will ultimately enjoy universally, does not however obviate the necessity for assistance now, in our state of society, and we have therefore to explain how it can best be rendered.
It has often been a matter of dispute, both with medical men and with moralists, whether Men or Women ought to assist in child-birth. The discussion has called forth a great deal of declamation, but very little has been said to the point on either side. It appears to me, however, that the question may be very easily settled, if it be rightly considered. The first requisite, and the most indispensable, in those who are to assist in child birth is, that they should know how to assist. This is paramount to every thing else. Now, if females really did know what to do in such cases, and were fully competent to do it, I think there is no question but they would be the best assistants, to say nothing of their being the most proper. There are many things experienced by females in such situations, which can never be understood by a man at all, though they are readily appreciated by one of their own sex, particularly if she has been a mother herself. With each other also there would be less disposition and less occasion for reserve in delicate communications, and less repugnance to necessary examination or manipulation, which could therefore be more efficiently practised. In short, if women were undoubtedly equally competent with men in this art, and full confidence was felt in them by their own sex, I think it is evident they would, in every respect, be the most fitting practitioners, and I have no doubt but they would be preferred. The question simply arises then, whether they are so competent? And every one able to judge, who speaks honestly, must admit that very few, if any of them really are so. It has not been possible for them to acquire the requisite information, nor to pursue the necessary investigations, and therefore we cannot expect that they can be equal to those who have. There are some women[vii] I know, who have been careful observers, and who have had great experience, that can render all needful help in most cases, but even they are apt to meet with difficulties, which require more skill than they possess to overcome; therefore very few like to depend upon them altogether. It is naturally argued that, as a physician may be needed, it is better to have him at first, and so be ready for every contingency.
That females can make competent Accoucheurs is proved by numerous well known instances, among which I need only refer to Madame Boivin, and Madame Lachapelle, both of whom, as practitioners and as authors, stand in the very highest rank. These ladies are referred to as authorities, and their works are quoted by the most eminent Professors of the day; in fact, on many points, they have surpassed all competitors. Further on in our work we shall have occasion to refer to their labours, the value of which will then be seen.
It is therefore evident that females can officiate, if they are properly instructed, which I think they ought to be, independent of the reasons already given. That they will eventually be competent I have no doubt, and I am proud to throw my mite of instruction in their way to assist in making them so.
In regard to the alledged immorality resulting from the present system of men acting as Midwives, there is much exaggeration, and much unnecessary alarm. That it is, in some respects, indelicate, and only to be justified by necessity is true, but there is no foundation for saying, as some do, that it leads to wide spread Profligacy and Adultery. I should prefer to see females always able to assist each other; but I cannot nevertheless consider the present system a necessary cause of licentiousness.
That females were always depended upon in old times, and are now in certain rude communities, is true, but that is no reason why they should be depended upon under all circumstances. In our present highly artificial state there are numerous causes at work, and numerous difficulties experienced, unknown to more primitive times and conditions, and we therefore require greater skill and more extensive resources. Females have in fact become more in want of help, and less able to assist.
At what time, and in what country, men first began to assist in cases of labour is not recorded. They have done so however for a long time, much longer than most people suppose. In the time of Hippocrates, called the Father of Medicine, who lived more than four hundred years before Christ, it appears that physicians were commonly resorted to. In his writings we find cases described, which show that he was well acquainted with the process of parturition, and even with some of the most difficult operations now practised. The Israelites appear to have employed women, as most eastern nations in fact do at the present day.
Midwifery, however, did not attract much attention, nor make much progress, till about the middle of the sixteenth century, since when it has been studied and practised by the most eminent Physicians and Surgeons, and has arrived at great perfection.
Many new discoveries have been made lately, which enable us to facilitate delivery and ease its pains, so that it is now robbed of many of its former terrors and dangers. Some of these discoveries are of easy application, and promise much future good; I shall carefully describe them all, in the following pages.
F. H.
FRONTISPIECE, Eve in the Garden of Eden.
PLATE I.—Lateral Section, of the Female Pelvis, to show the position of the Organs in their natural state, 5. PLATE II.—Front View of the Female Pelvis, with the External Walls removed, 9. PLATE III.—The Uterus and its Appendages, 13. PLATE IV.—Vertical Section of the Womb and Vagina, natural size, 18. PLATE V.—The Muscular Fibres of the Womb, 23. PLATE VI.—Muscular Fibres of the Womb, 27. PLATE VII.—Bones of the Pelvis, 33. PLATE VII.-a.—Male Pelvis, to show the difference in structure, 35. PLATE VIII.—Section of the Pelvis, 37. PLATE IX.—Diameters of the Upper Strait, 41. PLATE X.—The Bones of the Pelvis viewed from below, 45. PLATE XI.—The Direction of the Pelvis, 49. PLATE XII.—Section of the Uterus, with the Ovum and appendages, at about one month, 65. PLATE XII.-a.—Female Breast, 77. PLATE XIII.—Breast about the Fourth Month, 90. PLATE XIV.—Womb, at about the third, seventh and ninth months, 99. PLATE XV.—Primipara, or the First Pregnancy.—Woman who has borne children before, 101. PLATE XVI.—Mode of performing the Ballotment, to detect Pregnancy, 107. PLATE XVII.—At the end of the Fifth Month, 111. PLATE XVIII.—The neck of the Womb in a first pregnancy, and in a female who has borne children before, at the end of the seventh month, 116. PLATE XIX.—Fœtus in the most usual position, 121. PLATE XX.—Fœtus in the next most frequent position, 125. PLATE XXI.—Presentation of the Pelvis, or breech, 129. PLATE XXII.—The position of Twins, as most usually observed, 133. PLATE XXIII.—End of the Ninth Month, 135. PLATE XXIV.—The Fœtal head, 147. PLATE XXV.—Diameters of the Head, 151. PLATE XXVI.—Attitude of the Fœtus, 153. PLATE XXVII.—Head just entering the upper strait, 173. PLATE XXVIII.—Head lower in the Pelvis, 177. PLATE XXIX.—Head beginning to Rotate, 181. PLATE XXX.—Rotation of the Head, 183. PLATE XXXI.—Head in the right anterior occipito iliac position, 187. PLATE XXXII.—Delivery in a breech presentation, 194. PLATE XXXIII.—Anterior posterior position of the head, 195. PLATE XXXIV.—The chin just passed in presentation of the face, 200. PLATE XXXV.—Presentation of right shoulder, 205. PLATE XXXVI.—Descent of shoulder, 206. PLATE XXXVII.—Descent of shoulder, 207. PLATE XXXVIII.—Trunk descended, 208. PLATE XXXVIII.-a.—State of the parts at beginning of labor, 215. PLATE XXXIX.—Manner of supporting the perineum, 233. PLATE XL.—Standard form of Pelvis, 271. PLATE XLI.—Masculine Pelvis, 271. PLATES XLII, XLIII, XLIV, XLV.—Deformed Pelves, 275-279. PLATE XLVI.—Head fixed in a narrow pelvis, 282. PLATE XLVII.—Case of Tumor, 289. PLATE XLVIII.—Case of Polypus, 293. PLATE XLIX.—Limbs cut off by the Cord, 301. PLATE L.—Forceps, 346. PLATE LI.—Head extracted by Forceps, 353.
| PART I.—MIDWIFERY. | ||
| Section I. | ||
| position and uses of the female organs. | ||
| Page | ||
| CHAPTER I.— | Position of the Organs and Parts, | 13 |
| Internal Organs, | 14 | |
| External Organs, | 16 | |
| CHAPTER II.— | Structure of the Principal Organs and Parts, | 18 |
| The Womb, | 19 | |
| The Vagina.—Vulva.—Perineum, | 29 | |
| The Pelvis, | 30 | |
| CHAPTER III.— | Functions of the Principal Female Organs, | 50 |
| The Womb, | 50 | |
| The Ovaries.—Menstruation, | 51 | |
| Conception, | 54 | |
| CHAPTER IV.— | Fœtal Development, | 57 |
| Fœtal Nutrition, | 67 | |
| Peculiarities of the Fœtal Circulation, | 70 | |
| The Breast, | 74 | |
| Section II. | ||
| signs of pregnancy, and
the means of detecting it; its duration, and the period at which the fœtus can live. |
||
| CHAPTER V.— | Presumptive Signs, | 83 |
| Probable Signs, | 94 | |
| CHAPTER VI.— | Duration of Pregnancy, | 137 |
| CHAPTER VII.— | Period when the Child can live, | 142 |
| Section III. | ||
| the form, size
and position of the fœtus, and its appendages, at full term. |
||
| CHAPTER VIII.— | Form and Size of the Body, | 144 |
| Size and Form of the Head, | 144 | |
| Attitude of the Fœtus at Full term, | 152 | |
| [x] CHAPTER IX.— | The Appendages of the Fœtus at term, | 155 |
| CHAPTER IX.— | The Membranes, | 155 |
| The Placenta, | 156 | |
| The Umbilical Cord, | 157 | |
| Section IV. | ||
| the mechanism of
delivery in all the different presentations and positions of the fœtus. |
||
| CHAPTER X.— | Presentations, | 160 |
| Positions, | 161 | |
| Mode of ascertaining the Presentation and | ||
| Position, | 164 | |
| CHAPTER XI.— | The Mechanism of Delivery, in a Presentation | |
| of the Head, | 170 | |
| The Left Anterior Occipito Iliac Position, | 170 | |
| Mechanism of Delivery in all other Positions | ||
| of the Head, | 185 | |
| General Remarks on the Different Positions | ||
| of the Head, | 189 | |
| CHAPTER XII.— | Mechanism of Delivery in Presentations of | |
| the Lower Extremities, | 191 | |
| Delivery in a Breech Presentation in the left | ||
| Anterior Sacro-Iliac Position, | 192 | |
| Delivery by the Breech in the Right Posterior | ||
| Sacro Iliac Position, | 196 | |
| Delivery by the Breech in the Full Posterior, | ||
| or Sacro Sacral Position, | 196 | |
| General Remarks on the Presentation of the | ||
| Lower Extremities, | 197 | |
| CHAPTER XIII.— | Mechanism of Delivery in Presentations of | |
| the Face, | 199 | |
| Delivery in the Right Posterior Mento Iliac | ||
| Position of the Face, | 199 | |
| Delivery in other positions of the face, | 200 | |
| CHAPTER XIV.— | Mechanism of Delivery in Presentations of | |
| the Trunk, | 203 | |
| Mechanism of Delivery in Presentations of | ||
| the Trunk by Spontaneous Evolution, | 204 | |
| Section V. | ||
| the physiology of
spontaneous delivery, or childbirth, and the manner of conducting a natural labor. |
||
| CHAPTER XV.— | Of Delivery in General.—Different Kinds of | |
| Delivery.—Causes of Labor, | 211 | |
| Signs of Delivery, | 212 | |
| CHAPTER XVI.— | The Progress, Phenomena, and Duration of | |
| Natural Labor.—First Period, | 214 | |
| Second Period, | 216 | |
| Duration of Natural Labor, | 220 | |
| [xi] CHAPTER XVII.— | The Conduct or Management of a Natural | |
| Labor.—Preliminary Requisites, | 222 | |
| Preliminary Proceedings, | 223 | |
| Preparations for the Delivery, | 226 | |
| Attendance after the Preparations are made, | ||
| and during the Delivery, | 229 | |
| CHAPTER XVII.— | Delivery of the After Birth, or Placenta and | |
| Membranes, | 239 | |
| Attentions to the Female after the Delivery | ||
| of the After Birth, | 242 | |
| Attentions to the Child, | 243 | |
| Accidents which may happen, | 246 | |
| Subsequent Attentions to Mother and Child, | 249 | |
| Concluding Remarks, | 255 | |
| Section VI. | ||
| protracted and difficult labors. | ||
| CHAPTER XVIII.— | The Causes and Consequences of Prolonged | |
| Labor to both Mother and Child, | 259 | |
| The Consequences of Prolonged Labor, | 259 | |
| CHAPTER XIX.— | Causes connected with the Mother which | |
| may impede labor, or make it difficult, | 260 | |
| Inertia, or Want of sufficiently Powerful | ||
| Contraction in the Womb, | 260 | |
| Rigidity of the Mouth of the Womb, Vagina | ||
| and Vulva, | 264 | |
| Obliquities of the Womb, | 266 | |
| Prolapsus Uteri.—Smallness or Deformity of | ||
| the Pelvis, | 267 | |
| Tumors in the Pelvis, | 286 | |
| Tumors externally.—Obstructions in the Vagina, | 295 | |
| CHAPTER XX.— | Causes connected with the child, or children, | |
| which may impede delivery. | 297 | |
| Procidentia of the Umbilical Cord, | 297 | |
| Shortness of the Cord, | 300 | |
| Descent of other parts with the head, | 301 | |
| Twins and Triplets, | 302 | |
| Excessive size of the Fœtus, or the diseased | ||
| development of certain parts, | 304 | |
| Ossification of the Head, | 305 | |
| Various presentations and positions of the | ||
| Fœtus, | 306 | |
| Presentations of the Lower Extremities, | 307 | |
| Presentations of the Shoulder, | 311 | |
| Section VII. | ||
| accidents during labor which may compromise the mother's life. | ||
| CHAPTER XXI.— | Uterine Hemorrhage, or Flooding, during | |
| Labor, | 315 | |
| CHAPTER XXII.— | Eclampsia, or Convulsions during Labor, | 336 |
| CHAPTER XXIII.— | Rupture of the Womb or Vagina, | 341 |
| Section VIII. | ||
| operations with the hand and with instruments. | ||
| CHAPTER XXIV.— | Operations with Instruments.—The Forceps, | 345 |
| Other Instruments, | 355 | |
| CHAPTER XXV.— | Operations with the Hand.—Turning, | 357 |
| [xii] PART II. | ||
| the diseases of women during pregnancy, and in childbed. | ||
| Section IX. | ||
| the diseases of pregnancy. | ||
| CHAPTER XXVI.— | Sympathetic Diseases occurring during | |
| Pregnancy.—Sickness and Vomiting, | 366 | |
| Ptyalism, or Excessive Salivation, | 369 | |
| Odontalgia, or Toothache, | 369 | |
| Derangements of the Appetite, | 371 | |
| Pyrosis.—Dysphagia, | 374 | |
| Gastralgia, | 375 | |
| Constipation, | 377 | |
| Dysentery and Diarrhœa, | 378 | |
| Dyspnœa, or Difficulty of Breathing, | 380 | |
| Cough, | 381 | |
| Palpitation of the Heart, | 383 | |
| Syncope, or Fainting, | 384 | |
| Headache and Dizziness in the Head, | 386 | |
| Insomnia, or Sleeplessness, | 388 | |
| Temporary Affection of the Sight, Hearing, | ||
| and Smell, | 389 | |
| Disordered Judgment, Inclinations, and | ||
| Propensities, | 391 | |
| Hæmoptysis, Hæmatemesis and Epistaxis, | 393 | |
| Varicose Veins, | 395 | |
| Hæmorrhoids, or Piles, | 397 | |
| Œdema, or Watery Swellings, | 399 | |
| Hydrorrhea, or Profuse Discharge of Water, | 400 | |
| Pustules, and Mucous Discharges, | 400 | |
| Derangements of the Urinary Organs, | 401 | |
| Cramps.—Pruritus, or Itching of the External | ||
| Parts, | 403 | |
| CHAPTER XXVII.— | Idiopathic, or Primary Diseases Incident | |
| to Pregnancy.—Flooding, | 406 | |
| Abortion, or Miscarriage, | 409 | |
| Section X. | ||
| the diseases of women in childbed, after lying in. | ||
| CHAPTER XXVIII.— | Diseases of Childbed.—Puerperal | |
| Fever, or Childbed Fever, | 420 | |
| Affections of the Breast occurring after | ||
| Pregnancy, | 430 | |
| Bronchocele, or swelling in the Throat, | 438 | |
| Phlegmasia Alba Dolens, or Milk Leg, | 439 | |
| Trouble with the Urine, | 441 | |
| APPENDIX. | ||
| on preventing pain in childbirth, | 443 | |
PLATE I.
Lateral Section, or side view of the Female Pelvis, to show the position of the Organs.
A. The Bladder.
B. The Womb.
C. The Vagina.
D. The Rectum.
e. The Right Ovary.
f. The Right Fallopian Tube.
g. The Os Tincæ, or Mouth of the Womb.
h. The Meatus Urinarius, or Mouth of the Bladder.
i. i. The Small Intestines.
j. j. The Back Bone.
k. The Pubic or Front Bone.
l. The Right External Lip, or Labium.
m. The Right Internal Lip, or Nymphæ.
n. The Hymen.
o. The Opening through the Hymen.
q. The Perineum.
p. The Clitoris.
(This of course shows the half of all the single Organs and the right one only of those that are double.)
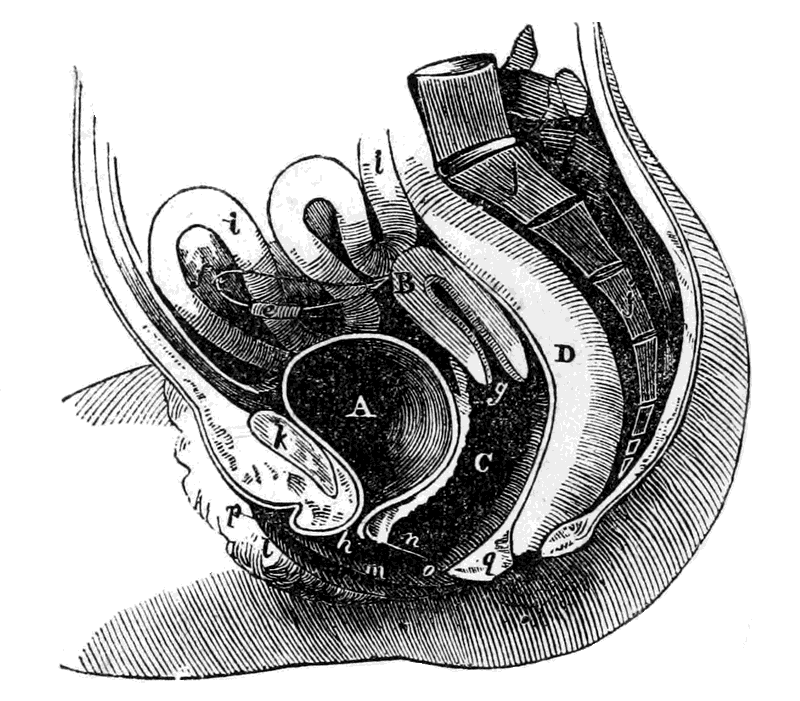
Plate I.
Lateral Section, or side view of the Female Pelvis, to show the position of the Organs in their natural state.
PLATE II.
Front View of the Female Pelvis, with the External Walls removed.
A. The Bladder.
B. The Womb.
D. The Rectum.
e. e. The Ovaries.
f. f. The Fallopian Tubes.
i. i. The Small Intestines.
r. r. The Round Ligaments.
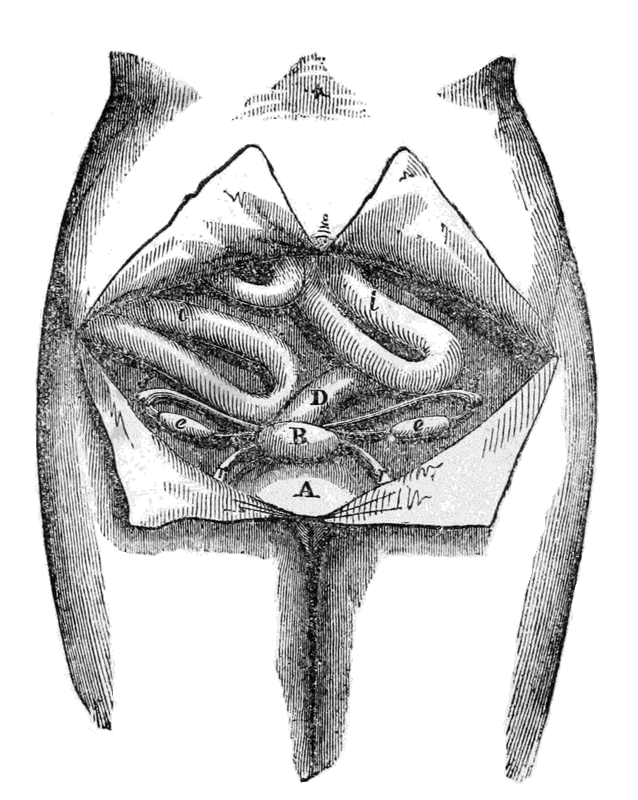
Plate II.
Front View of the Female Pelvis, with the External Walls removed.
MIDWIFERY.
POSITION, STRUCTURE, AND FUNCTIONS OF THE ORGANS AND PARTS OF THE FEMALE BODY CONCERNED IN GENERATION AND PARTURITION.
To understand the subjects treated upon in the present work, it is necessary to have at least a general acquaintance with the structure, position, and special uses of the principal organs and parts of the female system. A complete acquaintance, so far as our knowledge extends, would be advisable, but is not absolutely required, and could not with convenience be given here. The following explanations therefore, chiefly taken from my book on the Diseases of Woman, are merely sufficient for the present occasion, and for reference—full details being reserved for a separate and complete work, now preparing, on the Philosophy and Physiology of the Reproductive Functions.
Plate I, represents one half of the Female body, supposing it to be cut down the middle, and gives an accurate representation of the relative position of the different organs.
Plate II, represents a front view of the Female body, with the external walls removed, to show the relative position of the organs.
Plate III, represents the uterus and its appendages removed from the body, so that their connections with each other may be seen.
PLATE III.
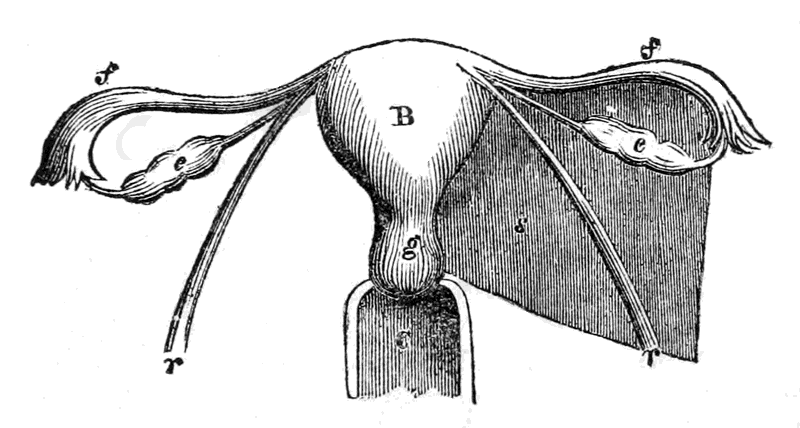
B. The Womb.—C. The Vagina.—e. e. The Ovaries.—f. f. The Fallopian Tubes.—s. The left broad Ligament, the right one being removed.—r. r. The Round Ligaments.—g. The Os Tincæ, or Mouth of the Womb.
The Ovaries.—(e. e. Plates I, II and III.)—These are two oval shaped bodies, about the size of an almond nut, placed one on each side, nearly in the groin. They contain a number of small round grains, or granules, called the ovæ, or eggs, which are the germs of human beings, as the eggs of birds are of their particular kind. They are connected with the uterus by two short arms, or prolongations, and are enclosed in the folds of the broad ligaments.
The Fallopian Tubes.—(f. f. Plates I and II.)—These are two Tubes, one on each side, beneath the Ovaries, and extending farther. Each of them has a small passage which opens into the uterus at one end, and opposite the Ovaries at the other. Their use is to convey the impregnating principle to the Ovaries, at the time of conception, and to convey the Ovæ, when impregnated, to the interior of the Womb.
The Uterus, or Womb.—(B. Plates I, II.)—This is a hollow organ, placed between the Bladder, which is in front, and the Rectum, which is behind. It is connected with the Vagina, and opens into it by the small orifice called the mouth of the womb.—(g. Plate I.)—The Uterus is the organ which receives the impregnated ovum, and in which it is developed into the human being. It is connected with the Ovaries by the Fallopian Tubes, and with the Vagina by the Os Tincæ, and is retained in its situation partly by its connections with other organs, and partly by the round and broad ligaments.
The Vagina.—(C. Plate I.)—This is the passage which leads to the Womb from the external opening.
The Os Tincæ, or Mouth of the Womb.—(g. Plates I and II.)—This is the small orifice, opening into the Vagina, by which communication is established with the Uterus from without.
The Bladder.—(A. Plates I and II.)—The Receptacle of the Urine. It is placed immediately in front, on the pubic bone, the Uterus lying nearly on the top of it.
The Rectum, or Termination of the large Intestine. (D. Plates I and II.)—This is situated behind the Vagina, and between it and the back bone.
The Broad Ligaments.—(s. Plate III.)—These are two broad folds of membrane, which serve partly to enclose the Fallopian Tubes and Ovaries, and partly to sustain the Womb in its place. They adhere to the Uterus and to the walls of the Pelvis.
The Round Ligaments.—(r. r. Plates II and III.) These two cords arise from each upper corner of the Uterus, and curving downwards are fixed by their other extremities to the pubic bone. They are partly enclosed in the Broad Ligaments. They assist in sustaining the Uterus in its position, and probably also they strengthen the Broad Ligaments and prevent their rupture when the strain upon them is too great.
Fimbriæ of the Fallopian Tubes.—(t. t. Plate III.) These Fimbriæ are like Tentaculæ, or fingers, springing from the extreme ends of the Tubes, and floating loosely in the cavity of the pelvis. Their use is to clasp hold of the ovaries at the time of conception, so that the fecundating principle can reach them, and also to take up the ovæ when impregnated, and convey them into the Tube, down which they pass into the Womb.
The External Lips.—(l. Plate I.)—These are commonly termed the Labiæ externa. They are two broad folds of membranous and adipose substance, forming the portals to the Vulva, or entrance to the Vagina.
The Internal Lips.—(m. Plate I.)—These are two smaller labiæ, sometimes called the Nymphæ, within the first, the chief use of which appears to be to direct the flow of the urine from the urethra.
The Hymen.—(n. Plate I.)—This is a membrane generally found in virgins, which grows over and closes more or less completely the entrance to the Vagina. Use unknown. When it exists there is generally a small orifice through it, by which the menses escape at each monthly period.—(o. Plate I.)
The Clitoris.—(p. Plate I.)—This is a small prominent organ, about the size of a large pea, placed in the upper part of the opening between the external lips, and immediately above the Meatus Urinarius. It is the principal seat of venereal excitement, and is subject to many annoying diseases.
The Perineum.—(q. Plate I.)—The part between the Vulva, or entrance to the Vagina, and the fundament. It is chiefly composed of the muscles belonging to the neighboring parts, and assists very much in supporting the womb.
The Meatus Urinarius, or Mouth of the Bladder, (h. Plate I.)—A small opening by which the urine escapes, placed between the lips, and immediately above the Vulva, or entrance to the Vagina.
These organs are all placed within, or in contact with, the lower part of the Trunk, called the pelvis.[17] They are all intimately connected with each other, and some of them have most extensive and strong sympathies with almost every other part of the system. So much so is this the case in fact, that probably the great majority of diseases to which females are liable arise, directly or indirectly, from Uterine or Ovarian derangement. Very often the heart, the stomach, or some other organ, though perfectly healthy, is thought to be diseased, and appears to be so, merely from its sympathy with the diseased womb.
PLATE IV.
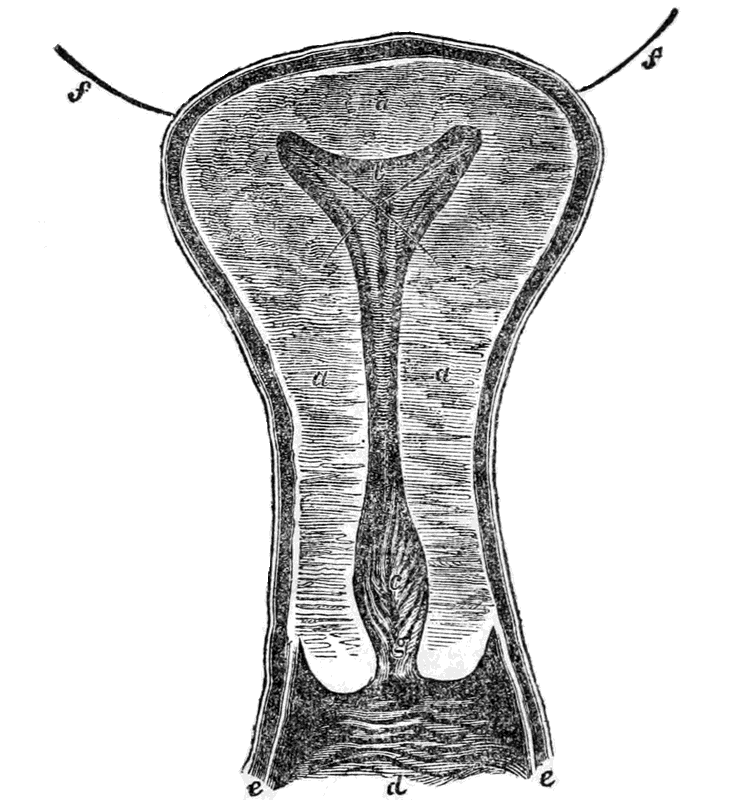
Vertical Section of the Womb and Vagina, natural size.
a. a. a. The solid walls of the Womb cut through. b. That part of the cavity, or hollow of the Womb, which is in the fundus, or top. c. That part of the cavity which is in the lower part, or neck, of the Womb. d. The Vagina. e. e. The cut edges of the Vagina. f. f. The positions of the Fallopian Tubes, which are cut off, and down the passages of which two needles are passed. g. The Os Tincæ, or Mouth of the Womb.
In addition to the general explanation already given, there are some of the Female organs whose peculiar structure requires to be more fully noticed, on account of its important influence on some of the processes hereafter to be described.
The external appearance of the womb, viewed in front, and in connection with its appendages, is shown in Plate III. It is placed in the Pelvis, between the bladder and the Rectum, and at the top of the Vagina, as seen in Plates I and II. Its internal structure is represented in Plate IV.
The length of the Womb, after puberty, is about three inches; its breadth at the upper part, or fundus, about two inches; and at the cervix, or neck, about one inch. The cavity in the interior is small, owing to the thickness of the walls, and its form is triangular. The shape of the Womb resembles a pear, somewhat flattened, from before backward. Previous to puberty its size is much smaller, and with those who have had children it often exceeds the dimensions we have given.
The Neck, or narrow part, (c. Plate IV.) is much changed by pregnancy. In virgins it is long and pointed, and somewhat enlarged in the middle. In those who have borne children it is considerably shorter, more obtuse, and less regular in its form. The cavity in the Neck is larger in the middle than at either end, as will be seen in Plate IV.
The Os Tincæ, or mouth of the Womb, also undergoes considerable change from the same cause. In the young person it is merely like a small slit, scarcely to be felt, but after pregnancy it much enlarges,[20] and remains more or less permanently open. The anterior lip, or the one in front, is somewhat larger than the posterior one.
The body of the Uterus is formed of a very dense, gray colored, muscular substance, possessing astonishing contractile power. The interior is lined, like the Vagina, with a mucus membrane, and the whole organ is plentifully supplied with arteries, veins, and nerves.
One of the most remarkable properties of the Womb is that of being able to distend to an extraordinary degree, and then retract again to nearly its original size. The force which it sometimes exhibits during its contraction is very great, being sufficient to separate, and even break, the bones of the mother's pelvis, and paralyze the hand of the operator when introduced. The Muscular Fibres on which this contractile force depends are most obvious during gestation; they then appear very numerous, and very curiously disposed, some of them ramifying in almost every direction, as will be seen by Plates V, VI. It is owing to this that the Womb contracts in every conceivable direction, and thus presses, during labor, on every part of the child's body.
PLATE V.
Figures 1 and 2.
Fig. 1. In this plate represents the Muscular Fibres a little exaggerated, so that they can be more distinctly seen.—a. a. are the orifices of the Fallopian Tubes.
Fig. 2. Represents the natural appearance, the fibres not being quite so distinct, though sufficiently obvious.—a. a. The orifices of the Fallopian Tubes.
In both Figures the Womb is supposed to be turned inside out, its peculiar structure being more readily seen interiorly than exteriorly.
Fig. 1 Fig. 2
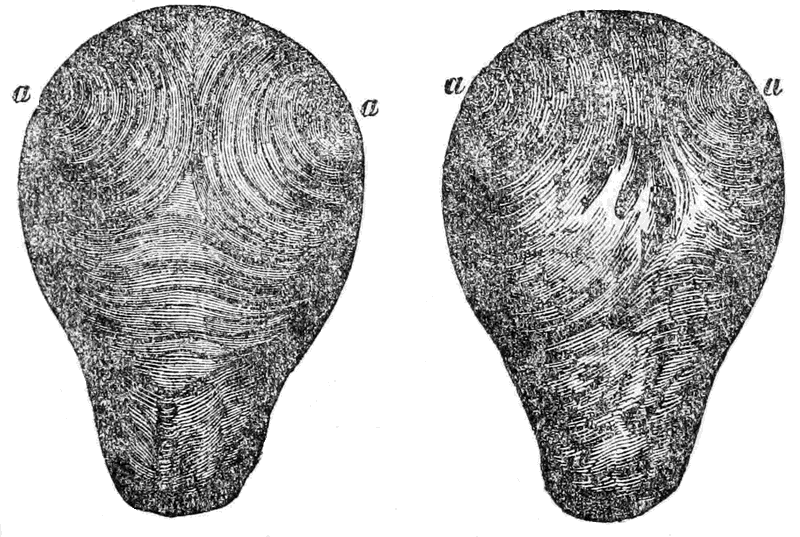
Plate V.
The Muscular Fibres of the Womb.
PLATE VI.
Figures 1 and 2.
Fig 1. This represents the appearance of the Fibres externally, and shows how they terminate in the round ligament a. b.
Fig. 2. The lines a. b. represent the direction of the force of the Fundul Fibres; c. d. That of the Circular Muscles of the body of the Uterus; d. e. The combined force of the Muscles.
The dotted lines represent the force reflected by the liquor amnii. The dotted curved lines the direction of the circular fibres of the body of the Uterus.
Fig. 1
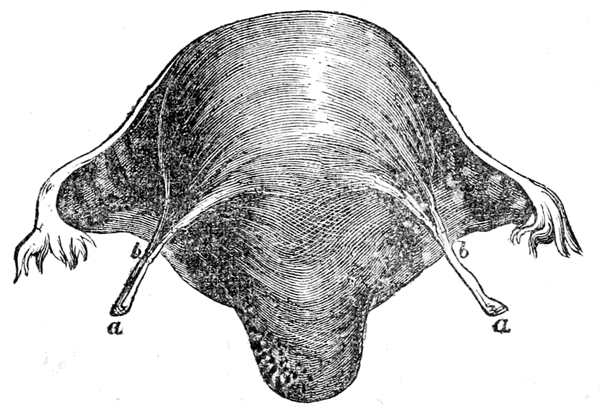
Fig. 2
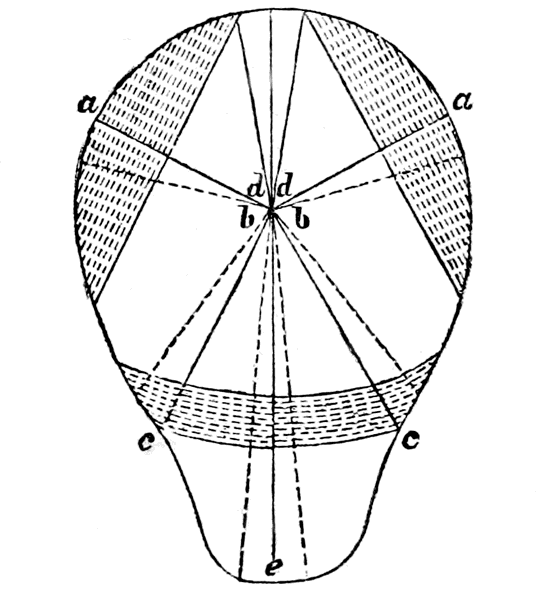
Plate VI.
The Muscular Fibres of the Womb.
The Vagina (c. Plate I.) is a membranous canal, lined with a mucus membrane like the Uterus. By its upper part it is attached to the neck of the Womb, at about two-thirds of its height—so that two-thirds of the neck hang within the Vagina. Below, it terminates in the Vulva, or external mouth. The upper part of the Vagina is much larger than the lower part, particularly in those who have borne children. It is capable of considerable distension, and after retraction, to allow of the child passing down it from the Womb. The external mouth is called the Vulva, and is usually partly closed, in the virgin state, by the membrane called the Hymen, (n. Plate I.) The length of the Vagina is from three to five inches, and its diameter from one inch to one and a half, or even two inches in those who have borne many children.
This is the external opening, or mouth of the Vagina, through which the child has to pass at the termination of delivery. The external and internal lips, with the muscular and membranous tissue surrounding it, are all capable of great distension, without injury, to allow of the passage of the child.
This is the part situated between the Vulva and the Rectum. (p. Plate I.) It is composed of a somewhat dense and firm substance, chiefly muscular, and, like all the other parts mentioned, is capable of great distension. It is important, in many of the manipulations[30] during labor, to be well acquainted with it; and when the child's head is passing the perineum requires supporting, to prevent its being lacerated or broken through, an accident which often happens from want of due attention, and which leads to the most serious consequences.
The Pelvis is that part of the bony structure, or skeleton, of the female, in which the generative organs are placed, and through which the process of parturition is effected. An acquaintance with its natural structure, and with the changes which may be produced in its form and size, by disease and other accidents, is indispensable to those who wish to practise or understand midwifery.
In early life the Pelvis is composed of several bones, many of which, after puberty, grow together. In the adult female it is customary to speak of but four bones, the sacrum, the coccygis, and the two innominata, or hip bones, (see Plates VII, VIII.) In the young female these are divided into several distinct parts.
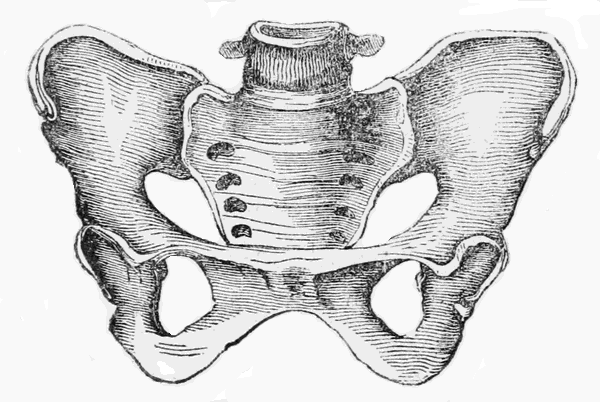
PLATE VII.
Bones of the Pelvis.
The four principal bones, as found in Mature life.—A. A. The Ossa Ilii, or Ossa Innominata, commonly called the haunch, or hip bones.—B. The Os Sacrum, or lower part of the back bone.—C. The extreme termination of the back bone, called the Os Coccygis.
The divisions into parts, as in Early life.—The Ilium, A, on each side, is in three parts; the Ilium, properly so called, marked a. a.; the Pubis, marked b. b.; and the Ischium, marked c. c. The Sacrum is in five parts, marked 1, 2, 3, 4, 5.
d. Is the last bone of the spine, which joins the Sacrum.—e. e. Are the Sockets in which the upper parts of the thigh bones fit, forming the hip joints.—g. g. The two rings, formed by the bones of the Pubis and Ischium, each called the Foramen Magnum.
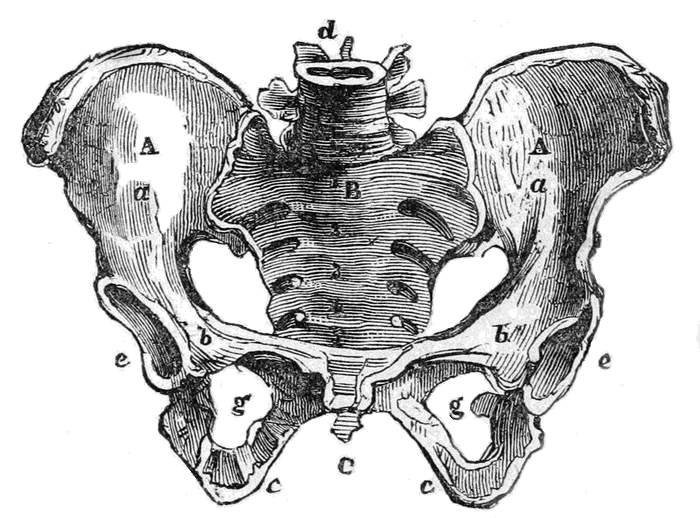
Plate VII.
Bones of the Pelvis.
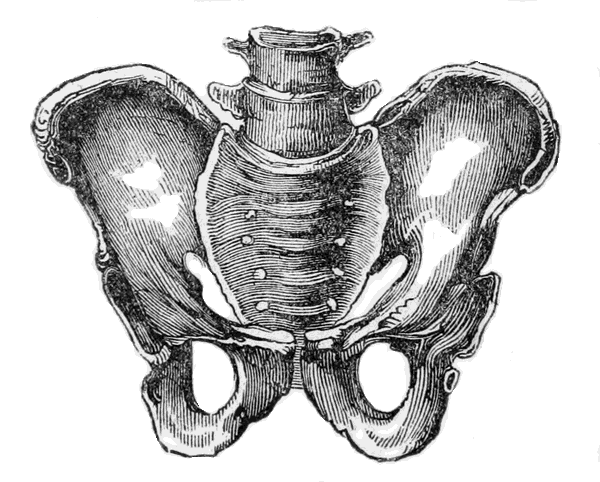
PLATE VII.—a.
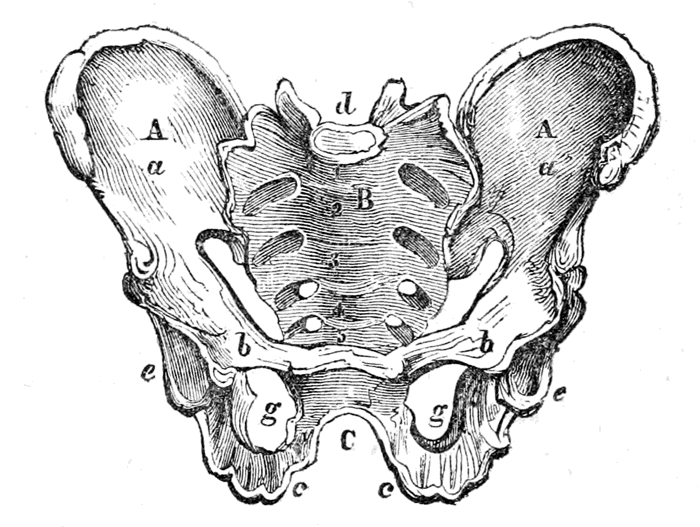
This represents the Male Pelvis, to show the difference in structure.
The letters correspond with those in Plate VII.
PLATE VIII.
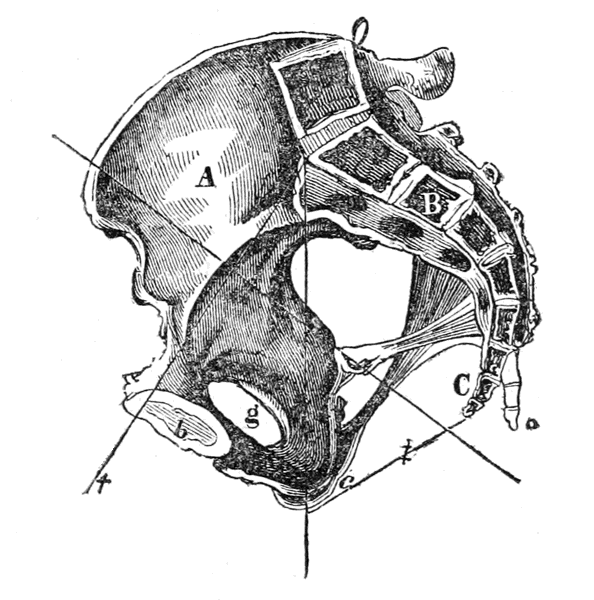
Section of the Pelvis, to show the shape and connection of those parts not distinctly visible in the full view. The section is made down the middle of the back bone, and through the symphysis pubes, in front. The letters correspond with those in Plate VII.
A. The right Ilium.—B. The Sacrum.—C. The Coccygis.—b. The Os Pubis.—c. The Os Ischinum.—g. The Foramen Magnum.—o. shows the manner in which the coccygis is bent back through labor.
These bones are all firmly bound together by a cartilaginous substance, which is placed between where they touch, and is firmly attached to each one. This union is called a symphysis. The one at front which joins the pubic bones is called the symphysis pubis; the two which join the Ossa Illii to the Sacrum are called the sacro iliac symphyses;[38] and that which joins the Coccygis to the Sacrum, is called the Sacro coccygeal symphysis. The two pubic bones are separated a little in Plate VIII, simply to show them better. The reader will bear in mind that they are naturally connected by the cartilaginous substance which forms the symphysis.
These articulations, or joinings, become much softened during labor, and give way a little, but not to any extent sufficient to assist delivery. It is a mistake to suppose that the bones separate at that time. The only part which gives way is the sacro coccygeal symphysis, which does relax, and allows the Os Coccygis to be pushed back by the child's head a full inch or more, thus enlarging the inferior strait.—(See c. and o. Plate VIII.) Sometimes this little bone will be even broken off, when there is great disproportion between the head and the strait. I have heard it snap like a stick breaking. There is nothing serious nor alarming in this, however, unless it be a first delivery late in life, though it may cause some pain at the time, and a little difficulty in sitting for some time after. In young persons the symphysis is soft, and gives way easily, so that they have little difficulty during delivery from this cause; but if a female marry late in life, after it becomes hardened, she may suffer considerably. In this case the coccygis is usually curved inwards considerably, and being firmly fixed the head cannot push it back, and on that account cannot pass, without great difficulty, and with the risk of rupturing some of the soft parts, or breaking the coccygis completely off. There is in fact great difficulty, and some danger, if the first pregnancy takes place late in life.
The Pelvis is usually divided into two parts,—the great pelvis, or upper part, enclosed between the[39] wide flanges of the Ossa illii and the upper part of the sacrum; and the small pelvis, or basin, which is enclosed between the lower part of the sacrum and coccygis behind, and the ossa ischii and ossa pubes in front. The basin is nearly cylindrical, larger in the middle, and curved towards the front.
The Straits of the Pelvis.—The bones of the Pelvis, it will be seen, form a kind of broad ring, or cylinder, particularly in the basin; and the straits are two passages, one by which the child passes into the basin from the upper Pelvis, and the other by which it passes out from the basin into the world.
In Plate VIII. the line marked † is the antero posterior diameter of the upper strait, through which the child first passes, called also the brim, or entrance to the Pelvis. The line marked ‡ is the diameter of the lower strait, through which the child passes into the world, called also the outlet of the Pelvis. In Plate VII. the line marked † crosses the upper strait, or brim of the Pelvis.
The diameters of the Pelvis are the distances between the prominent points of each strait, and are four in number for each, those for the upper strait being represented below.
PLATE IX.
Diameters of the Upper Strait.
A B, which extends from the most prominent point of the Sacrum, to the top of the Symphysis pubes, is called the antero posterior diameter, or that from before to behind.—C D, and E F, are called the two oblique diameters; they extend from each sacro iliac symphysis, to the most prominent point of the Os Ilium on the opposite side.—G H, is called the Transverse, or bis iliac diameter, it crosses the Pelvis nearly from one hip joint to the other.
The Sacro Antero posterior diameter measures four inches. The two oblique diameters four inches and a half each. The bis iliac diameter measures five inches.
(By comparing this with Plate VII. the various points will be still more apparent.)
The inferior strait has also four diameters, represented in Plate X.
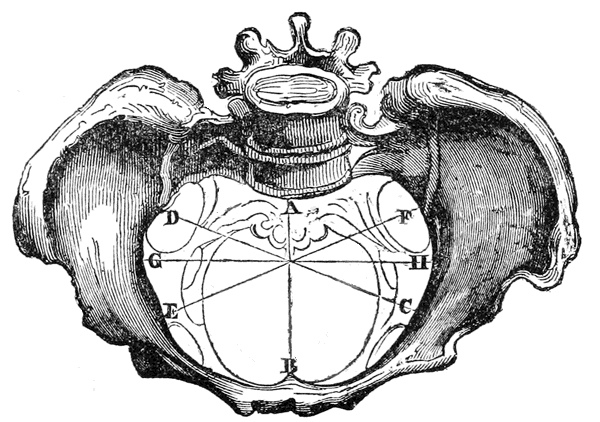
Plate IX.
Diameters of the Upper Strait.
PLATE X.
The Bones of the Pelvis viewed from below, looking through the inferior strait, to show its diameters.
A B, which extends from the end of the Coccygis to the lower part of the Symphysis Pubis, is called the antero posterior diameter; it measures four inches, like that of the upper strait, but is increased a little by the bending back of the Coccygis.—C D, and E F, are the two oblique diameters, also corresponding to those in the upper strait; they measure four inches, but are increased a little by the giving way of the soft parts.—G H, is the transverse, or bis-ischiatic diameter; it measures four inches.
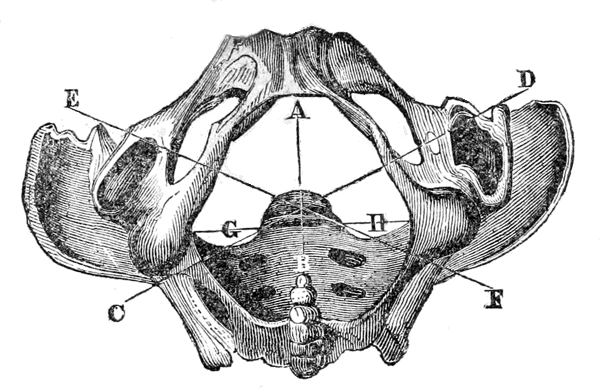
Plate X.
The Bones of the Pelvis viewed from below, looking through the inferior strait, to show its diameters.
It will thus be seen that the diameters only average from four to five inches, but it must be remembered that the soft parts, and even one of the bones, very readily give way, and thus they are slightly increased.
When we come to describe the form and size of the fœtal child's head, it will be found that its diameters correspond very nearly with those of the pelvic straits through which it has to pass, so that ordinarily labor presents no serious difficulty. If the head be larger than natural, from any cause, or if the Pelvis be too small, or deformed, this mutual adaptation does not exist, and delivery of course becomes difficult, or dangerous, and sometimes impossible. The only obstacle therefore, which can seriously impede the expulsion of the fœtus, or prevent it altogether, is this want of conformity, in size and shape, between its head and the bones of the Pelvis. The soft parts may retard labor considerably, by being contracted or rigid, but can generally be made to give way, either by the efforts of nature or by manual assistance; and the fœtal head can be reduced in size if necessary; but insufficient size, or faulty form, in the bones, is irremediable.
The various causes which produce deformity, or imperfect development, in the Pelvis, and unnatural growth of the child's head, will be stated in a subsequent section. For the present, we have only to do with both in the normal state.
The importance of an accurate knowledge of the structure of the Pelvis, and of the changes which may be induced in it, will now be obvious; neither the theory nor the practice of Midwifery can in fact be understood without such knowledge. It is also frequently of the first importance to know, previous[48] to marriage, whether the pelvis of a young person is so formed that delivery can be safely effected! Inattention to this has sacrificed the lives of many, and caused others to live for years suffering and helpless. In another place we shall give some plain rules and directions by which this important point may be determined.
The floor of the Pelvis.—The soft parts at the bottom of the basin of the Pelvis, consisting of the perineum and various muscles, are called the floor of the Pelvis—the only passage through which is by the Vulva, or mouth of the Vagina. As the head of the child descends to the bottom of the basin, it presses upon this floor, and gradually distends it, until the Vulva is sufficiently enlarged. This delay is advantageous, for if the passage was always large enough, or increased in size without any difficulty, the child would pass too suddenly, and much mischief might often result from its sudden expulsion—such as pulling down of the womb, flooding, and the falling of the child upon the ground.
Direction of the passage of the Pelvis.—In most of the lower animals the passage of the Pelvis is straight, and on a line with the body, the two straits being opposite each other, which makes delivery much more easy with them. Even in the negroes, and other inferior races, the passage is much straighter than in the whites. The more perfect the organization therefore, the more difficult is parturition; and the more imperfect or simple the organization, the more easy is parturition. The dotted line in Plate XI. shows the direction of the passage of the Pelvis, in the human female, to be a curve, so that the child has to move, during its passage, in a circle.
PLATE XI.
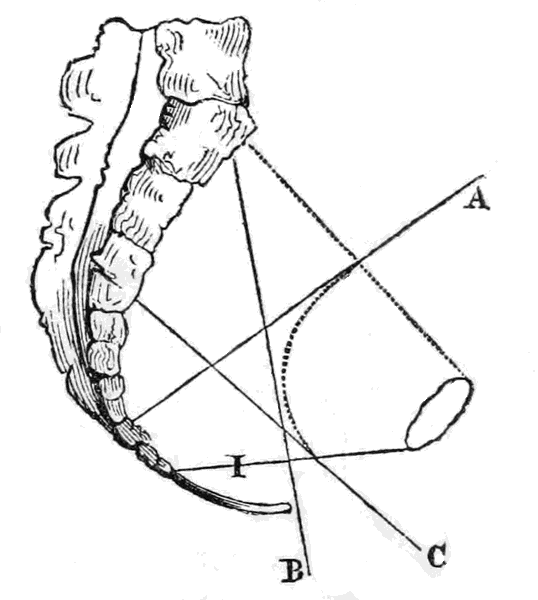
The axis, or direction, of the upper strait is denoted by the line A, that of the lower strait by the line B, and that of the Vulva by the line C. The force of expulsion tending to push the child in each direction, it has to traverse a path intermediate with them all, or compounded of them all, not being able to move in either alone. This aggregate direction is denoted by the dotted curved line, which shows the direction in which the child passes, and in which the hand must be passed when introduced.
I is the Perineum.—The dotted line which crosses A denotes the upper strait, and the line I the lower strait.
The great object for which the whole of the Female organs perform their several functions is, that of bringing into existence a new being! For this purpose they act both separately and conjointly, each one having its specific part to play in the grand phenomenon. As already remarked, it would not be in place here to give all the details of this wonderful event, but merely such a description of its principal stages, as will suffice for an understanding of the main subject of the present treatise. I shall therefore, first give the uses of the principal organs separately, and then explain the processes of conception, and fœtal development.
The Womb is nothing more than the receptacle in which the impregnated egg is placed, and in which it undergoes all the wonderful changes by which it eventually is developed into a perfect human being. The womb is not therefore absolutely needed in conception, and indeed several cases have been known where the new being was formed without the womb altogether, though not perfectly. Its principal use is in fœtal development, which cannot take place perfectly in any other part of the body.
The Ovaries, as already remarked, are two oval-shaped bodies, placed one on each side of the womb, and connected with it, whose use is to form the germ or rudiment, called the ovum, or egg, from which the new being is developed. The structure of the Ovaries is very simple, and the manner in which they produce the ovum is not very well understood. It is certain however, that they are indispensable to conception, being in fact the most essential parts of the female generative system.
Menstruation appears to be a process resulting from the development and healthy action of the Female organs, and is essential to their well being. The following brief account of its nature and origin is extracted from my Diseases of Woman, page 152 to 155:
"Until very recently but little was known, with any certainty, respecting this remarkable and important phenomenon of the female system. The most crude and visionary theories have been advanced to explain it, and our works on medicine and physiology do nothing more than repeat them, one after the other. The investigations of several distinguished physiologists however, within the last few years, have thrown a new light on this hitherto obscure subject, and explained much that was previously unknown, or, at best, merely conjectured upon. A brief statement of the result of those investigations will not only be highly interesting in itself, but will materially assist in explaining what we shall afterwards speak upon.
"It is well known that the female organs are liable, at regular periods, to assume a peculiar action, which results in the discharge of a fluid termed the menses. The secretion and excretion of which are highly essential, both to the proper performance of many other functions, and to the maintenance of the general health. Whence comes this fluid, and what causes it to flow? These were questions unanswered, except by mere supposition, previous to the discoveries referred to, which we now proceed to make known.
"In the first chapter it was stated that the Ovæ, or eggs, contained the rudiments or germs, from which, when impregnated by the male principle, new human beings were developed. These ovæ, however, are not prepared to undergo this development before the age of puberty, nor after the change of life, nor are the whole of them fit for conception even during the prolific period. It appears that they become fit for fecundation in succession, during the menstrual period, one ovum, or more, being ripened every month! When fully perfected it separates from the ovary and is lost, unless conception occurs, in which case it passes along the fallopian tube into the Womb, and then develops into the fœtus. Here then we see the cause of the menses; the ripening of the ovum causes a local excitement, and congestion, in the ovary and womb, which increases till the period when it is thrown off, and then the accumulated fluid is discharged, the excitement subsides, and a new development commences.
"This curious process is termed by some physiologists the monthly ponte, or laying of eggs, and by others the Ovarian labor, or birth! A small scar is left on the ovary at the point where the ovum separates,[53] which fades away after a time, but a number of them may always be observed on the ovaries of those who have long menstruated. In those who die during menstruation the ovaries are found very red, and full of blood, and sometimes one of the ovæ will be found swelled, and just ready to burst through, or the ruptured opening may be seen through which it has actually escaped.
"Precisely the same phenomenon occurs in the lower animals, excepting that their periods are more extended; some of them occurring annually, and others at still longer intervals. Some of the monkeys even have a species of real menstruation.
"These important facts, by enabling us to understand what causes menstruation, give us an insight also into the nature of its derangements, and the conditions required for their regulation. When we call to mind also the close sympathy between the uterine organs and every other part of the system, it shows us how important a proper menstruation is to the general health, because without it those organs must be diseased, and consequently every other part of the system liable to suffer with them.
"Formerly many absurd notions prevailed respecting menstruation, which in fact are not quite removed even now. Thus some authors asserted that a female, while unwell, could cause various diseases, by merely touching persons! Others supposed they would curdle milk, and nearly all believed that the menstrual fluid itself was highly poisonous, so that females, at those times, were compelled to live apart and approach no one. In the Old Testament there are many regulations given, for females while menstruating, which show the prevalence of such notions in olden times. It is scarcely necessary to say that[54] there is no foundation whatever for all this, as the fluid itself differs but little from ordinary blood, and is equally innocuous.
"In like manner it was supposed, that menstruation was influenced by the Moon, and only occurred at a certain period of her age. We know, however, that females are unwell almost every hour of every day in the year.
"The due establishment of the menstrual function is absolutely necessary, to the perfection both of mind and body, and its regular performance is quite as essential to the continuance of health, for there is scarcely a single disease that its derangement will not either cause, or at least seriously aggravate.
"It is therefore vitally important to attend to this matter, particularly in young persons approaching puberty! A little care at that time, properly bestowed, may prevent years of disease and suffering, if not untimely death!"
Conception is the union of the male principle with the female ovum, or egg, after that is perfected in the manner described in the article on Menstruation. The precise manner in which this union is effected is unknown, though our information in regard to it is much more extensive, and precise, than formerly. As nearly as can be stated it occurs in the following way:
At the time of a fruitful connection, which can only occur, it must be remembered, when the ovum is ripe, the male principle is carried into the Womb, (B, Plates I. and III.) and is then supposed, by some, to meet with the ovum which has descended down[55] the Fallopian Tube (f, Plates I. and III.) from the Ovary, so that the union of the two takes place, according to this view, either in the Fallopian Tube or in the Womb. Others, however, suppose that the ovum does not leave the Ovary before conception, but that the male principle passes down the Fallopian Tube and meets it there, and that it is several days after before it reaches the Womb. There are many facts and arguments brought forward in support of each view, all of which will be set forth in my forthcoming work on the reproductive functions. All that is known for certain is, that the two principles must unite in one place or the other, and that the ovum must pass down the Tube into the Womb, either before impregnation, or after.
The union of the two principles in the Womb appears so likely an event that it is scarcely possible to avoid thinking that it really does then take place, but at the same time there are very strong reasons for adopting the opinion that it takes place in the Ovary. Among others may be mentioned the phenomenon of extra uterine conception, which will be more fully alluded to in another place. In these cases the fœtus is found outside of the Womb, in the Tube, or the Ovary, or even in the Abdomen, among the intestines. Such an occurrence seems to render it almost certain that the ovum must have been fecundated in the Ovary, because we cannot well conceive, if it were not so, how it could reach the outside of the Womb. This difficulty is not, however, regarded as insuperable, by the advocates of the opposite theory. Possibly conception may occur in both ways.
There are many causes which prevent conception, or, in other words, which produce barrenness and[56] sterility. These various causes cannot be all explained, except in connection with a full explanation of the process of reproduction, and of the nature of many female diseases. In my work on "The Diseases of Woman," I have given a chapter on this subject, and have also referred to the present work as one in which it would be more fully treated. This reference, however, was made in mistake; the subject is not needed here, but will be in the other work, on the reproductive functions in which it will be discussed at length.
FŒTAL DEVELOPMENT.
The last Chapter brought us up to the point of conception, or the first commencement of the new being. The next step is to exhibit its various stages of development, and to show how it is nourished and maintained in its proper position. This is requisite in order to understand the origin of many diseases and accidents which occur during gestation, and also to explain the various signs by which it is determined whether a female is pregnant or not.
The development of a perfectly formed human being from the egg in which it originates, is one of the most astonishing phenomena that can come under our observation, and is eminently deserving the study of every rational being. The present explanation of it must necessarily be brief, being merely intended to make the main subject more clear.
It has already been remarked that it is uncertain whether the ovum is impregnated before it is brought into the Uterus, or after it arrives there; but be that as it may, nothing has yet been discovered in the Womb till several days after conception. Some physiologists tell us that the rudiment of the new being may be found there about the sixth day; but others again assure us that it cannot be found before the twelfth, at which period our explanation of its development will commence.
At the twelfth day the ovum is about the size of a large pea, it is composed of a vesicle containing a thick fluid, called the germ, which corresponds to the opaque substance seen in the white of a fecundated bird's egg, and of a yellowish substance, in which it floats, called the vitellus, which answers to the yelk. The whole being surrounded by two membranous coverings, the outer one called the chorion, and the inner one the amnion. Between these is a gelatinous substance, and within the amnion is a fluid, called the liquor amnii. The two membranes, the liquor amnii, and the inclosed ovum, are called the ovulum! Immediately after conception the uterus begins to secrete, from its inner walls, another membrane, very delicate, called the decidua. This lines the whole cavity, so that when the ovulum passes out of the tube it is met by this lining which seems to prevent its entrance into the womb. The ovulum, however, presses upon it and so makes a depression, like a nest, in which it lies. This prevents its moving about, or falling to the bottom of the womb.
The weight of the entire ovulum is about one grain. The embryo commences in the germ, and may now be seen about the size of a pin's point. The vitellus removes away from it, but remains connected by a small pedicel or thread-like tube, down which it is gradually absorbed as nutriment. A small white thread, scarcely perceptible, may be seen sometimes as early as this period, being the commencement of the brain and spinal marrow. The mouth is visible also from the twelfth to the twentieth day, and frequently the eyes. These are placed at first on the side of the head, like those of quadrupeds, and move round to the front afterwards.
At twenty-five days, the embryo is about the size[59] of a large ant, which it also resembles in form. It begins to have a little more consistence, and the future bones begin to resemble cartilage, or gristle. A small groove may be seen denoting the neck, which thus indicates the separation of the head from the trunk. The weight is three or four grains.
The first month, it is about the size of a Bee, and is somewhat like a small worm bent together. The arms may be seen like two little warts. They are first formed under the skin, and shoot out like buds, growing straight from the body; afterwards they become folded together, in a curious manner, upon the breast. The head is as large as the rest of the body, and upon it we can now see distinctly the eyes, like two black dots, the mouth, like a line, and also the nose. The lower extremity is lengthened out like a tail. Weight about ten grains.
The second month. Every part has now become much more developed, and the general form is that of a human being. The superior members are much more elongated, and the inferior ones begin to be distinguished, forming in the same manner as the others. The fingers are united together by a membrane, like the web on a Frog's foot. In the ribs, clavicles, and jaw bones, a few points can be seen ossified, the cartilage beginning; to harden into bone. The rudiments of the first teeth are also visible. The weight is about one drachm, and the length one inch.
At about seventy days the eyelids are visible, the nose becomes prominent, the mouth enlarges, and the external ear may be seen. The neck is well defined. The brain is soft and pulpy, and the heart is perfectly developed.
Every organ is originally formed without either blood or blood vessels. The circulation which afterwards[60] takes place in them is merely for their subsequent development. The heart is perfect in all its parts, and even has a slight motion, before the blood is found in it.
Three months. All the essential parts are well defined. The eyelids distinct, but firmly closed. The lips perfect, but drawn tightly together. The heart beats forcibly, and in the larger vessels red blood is seen. The fingers and toes are defined, and the muscles begin to be apparent. The organs of generation are remarkably prominent, but still it is somewhat difficult, at first, to distinguish the sex by these organs, notwithstanding their development, as the principal parts in both are nearly identical in form. It can, however, be ascertained by other circumstances, as the form of the head, dorsal spine, thorax, and abdomen. It now weighs about two ounces and a half, and measures four or five inches in length.
Four months. The development is remarkably increased. The brain and spinal marrow becomes firmer, the muscles distinct, and a little cellular tissue is formed. The abdomen is fully covered in and the intestines are no longer visible. A little of the substance called meconium even collects in the intestines, the same as is found in at birth. It now weighs seven or eight ounces, and measures six or seven inches. The bones are ossified in a great part of their extent, and the rudiments of the second set of teeth are visible, under the first.
The uterus now is so large that it can no longer remain in the lower part of the pelvis, but is compelled to rise up into the abdomen for more room. This change of position is improperly called quickening! Sometimes it takes place very gradually, so[61] that it is scarcely noticed, but more frequently it rises suddenly, disturbing all the internal organs, and causing in them considerable derangement till they accommodate themselves to the change. This occurrence often causes unnecessary alarm, though the sickness, and other unpleasant sensations, are always sufficiently annoying.
This stage corresponds with that in which the young of oviparous animals breaks the shell and escapes. The human being however, undergoes a remarkable change, and remains in the womb for a period longer than that already past, in order to become more perfected.
From four to nine months the development is proportionally much more rapid than during the first four months, owing to the circulation of perfect red blood, which is now found the same as in the adult, and is probably derived from the mother's blood vessels.
Five months. Every part is considerably increased in size, and become more perfect. The lungs enlarge, and are even capable of being, to a certain extent, dilated. The skin becomes much stronger. The situation of the nails can be discerned. The meconium is more abundant, and lower down in the intestines. The length is now eight or ten inches, and the weight fifteen or sixteen ounces.
Six months. The nails are marked. The head becomes downy, from the first development of the hair. A little fat is formed. Length twelve inches, weight from one and a half to two pounds. No indications of intellectual faculties.
Seven months. The whole being has rapidly progressed. The nails are formed, the hair is perfect, in the male the testicles descend to the scrotum, and[62] in the female the ovaries reach the brim of the pelvis. The bones are tolerably firm, and the meconium collects in the large intestines. Length fourteen inches, weight about three pounds. Intellectual functions not yet exercised.
The two remaining months are merely devoted to further increase in size and weight. No new phenomena present themselves.
Nine months. Every function has become active. The skin becomes colored, and perspiration occurs. There are no indications of the intellectual functions, but the animal functions are remarkably active, particularly that of taste, which no doubt leads to the act of sucking, from the natural desire for its gratification. The child can now experience all the ordinary sensations of pain, hunger, heat, and cold, and is capable of preserving an independent existence if brought into the world.
Plate XII. represents a section of the Uterus at about one month of gestation, so as to show all the parts in their proper situation.
PLATE XII.
Section of the Uterus, with the Ovum and appendages, at about one month of gestation.—a. a. a. The substance of the walls of the Womb.—b. b. The Embryo.—c. The different vessels by which it is connected with the Placenta.—d. d. The Placenta.—e. The Vitellus.—f. f. f. The Membrane lining the Uterus, called the Decidua; it is seen to be bent double, or reflected, the Embryo being on the outside of it.—g. g. The Chorion, or Middle Membrane, which is studded over with villosities, or small blood vessels.—h. h. The Amnion, or inner membrane, which contains the fluid called the liquor amnii, in which the Embryo floats.—i. i. The blood vessels which connect the Placenta with the Womb.—j. Is a plug of Mucus, by which the mouth of the Womb is now blocked up.—k. k. The ends of the Fallopian Tubes, which are cut off; these are also blocked up with mucus, the same as the Os Tincæ.—l. The Os Tincæ, or mouth of the Womb.—m. The Vagina.
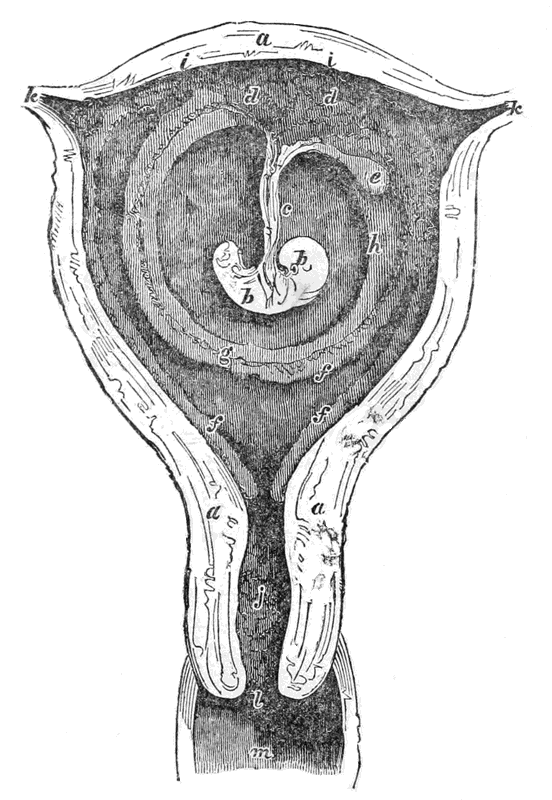
Plate XII.
Section of the Uterus, with the Ovum and appendages, at about one month of gestation.
The manner in which the new being derives its nutriment, or the material by which it grows, is, in a great measure, unknown to us, though we certainly obtain some little information about it by a study of the apparatus employed in the process.
For the first fifteen or twenty days the substance called the Vitellus, (e. Plate XII.) which is analagous to the yelk of the ordinary egg, appears to supply most, if not all of the material that is required in the formation of the new being; and indeed this substance does not totally disappear till after the third month, though we cannot suppose it to be the sole source of nutriment then. It is also supposed, by some, that the amniotic liquor, in which the fœtus floats, may afford some nutriment, either by being swallowed, or by being absorbed through the skin. It is certain that this fluid is nutritive, and there is nothing impossible in its absorption, though it is not very likely to occur to a sufficient extent. The idea that it can be swallowed however, is erroneous, because the mouth of the Fœtus is firmly closed while in the Womb; and besides, children have been born alive without mouths, and even without heads, and of course they could not have swallowed anything. It is now generally conceded by physiologists that the material required by the Fœtus, for its nutrition, is obtained from the blood of the mother, through the medium of the Placenta, and the vessels in the Umbilical cord. It is, however, a matter of dispute whether the maternal blood is sent directly, in its ordinary state, into the body of the child, or whether it first undergoes a preparatory process, which most modern authors suppose it does.
From the earliest period of gestation, the middle membrane, called the chorion, (g. g. P. XII.) is covered, on its outer surface, with a number of small protuberances called villosities, which subsequently become true blood vessels. About the fourth month these have increased very much in size and number, and have all become conglomerated into one mass, in form like a mushroom. This is called the Placenta. It is almost entirely formed of blood vessels, which seem to attach themselves at one end, by open mouths, to the open mouths of other blood vessels on the inner walls of the uterus (i. i. Plate XII.) At the other end these vessels are drawn together and lengthened out into a long tube, called the umbilical cord, or navel string, which finally enters the body of the child at the navel and so establishes the connexion between it and the mother.—(c. Plate XII.)
The blood vessels in the placenta, umbilicus, and fœtus, like those in the maternal body, are of two kinds, Arteries and veins. The arteries, which come from the left side of the heart, carry the pure blood, which contains all the materials for forming and nourishing every part of the system. The veins contain the blood in its impure state, and take it to the right side of the heart, from whence it is forced into the lungs to be purified by the act of breathing. The blood is made impure by some of its constituents being absorbed, to form the different parts of the body, and by having thrown into it a quantity of waste and poisonous matter no longer needed.
The course of the blood, therefore, is from the left side of the mother's heart along her arteries till it reaches the arteries of the uterus, from them it passes into those of the placenta, and thence into those of the umbilicus which convey it into the body of the child.[69] When there it circulates in its arteries, supplies the material for its further increase and development, becomes in consequence impure, and passes into its veins, the same as in the maternal body. From these veins it passes into those of the umbilicus and placenta, and, apparently, into those of the mother, by which it is conveyed to the right side of her heart, and by its action to her lungs, to be again purified when she breathes. This explains what was previously stated, that the child uses the mother's heart, lungs, and stomach, while in the womb, and has, therefore, no occasion to use its own.
The diameter of the placenta is about six inches, and its thickness about one inch and a half. The length of the umbilical cord is from eighteen to twenty-four inches, its diameter about half an inch. These dimensions are, however, subject to great variation. Instances are mentioned of the cord being five feet long, and as thick as the child's arm. I have seen one myself four feet long. Sometimes it will be very short, not more than eight or ten inches. It is composed of one artery and two veins, twisted together like the strands of a cable, and of a sheath surrounding them composed of the chorion and amnion. Between the sheath and the vessels is a thick gelatinous fluid called the Gelatine of Wharton.
This explanation, it must be remembered, is in fact merely hypothetical. The direct passage of the blood through the Placenta, from the mother's vessels into those of the cord, is denied by many physiologists, who contend that there is an intermediate set of vessels in the Placenta, in which it first undergoes important changes. They also contend that the impure blood does not pass through into the mother's veins at all, but is purified in the Placenta,[70] and immediately returned. Some have even averred that the Placenta is not required at all, to supply nourishment, but is merely a purifying organ. It is now known, however, that it is not absolutely essential to either process, for children have been born alive, and perfectly formed, which merely floated loosely in the amniotic liquor, having neither Placenta nor cord, nor any other connection with the mother. How they were nourished we cannot tell. These, however, must be regarded merely as curious exceptions, there being little doubt but that fœtal nutrition is ordinarily effected through the Placenta and cord, by means of the mother's blood, somewhat in the manner we have described.
From the circumstance of the fœtus not using its heart and lungs, like the adult, its circulation has several modifications.
The engine by which the blood is forced along its vessels is the heart! This is divided into two distinct parts, each of which has two cavities, the upper one called the auricle, and the lower one the ventricle, which communicate with each other by curious valves. In the adult the whole of the impure blood is poured into the right auricle, that from the lower part of the body by the inferior vena cava, and that from the upper part by the superior vena cava. From the right auricle it passes into the right ventricle, which pumps it into the lungs, by way of the pulmonary artery; here it is purified by the act of respiration, and then brought, when pure, by the pulmonary veins, into the left auricle, and passes from[71] thence into the left ventricle, which pumps it into the great aorta, and from thence into the smaller arteries all over the body. The two sides of the heart, therefore, do not communicate directly with each other, but there is a strong partition between them. In the fœtus the arterial blood from the mother, when it leaves the umbilical artery, enters first the liver, runs through its vessels, gives off the bile found in it, and then joins the vena cava inferior. By this passage it is taken into the right auricle, along with the impure blood of the vena cava. From the right auricle it passes through a hole in the partition directly into the left auricle, instead of taking the indirect route by the lungs as in the adult. From the left auricle it passes into the left ventricle, and is from thence distributed by the arteries all over the body. This opening in the partition is called the foramen ovale!
After birth, when the blood begins to pass through the lungs, this passage closes up. By the eighth day it is generally obliterated, often much sooner, though occasionally it has remained open longer without inconvenience. In some cases the foramen ovale does not close at all. The child then has what is called the blue disease! The whole body is of a uniform leaden, or blue color, and the whole system is generally languid and sluggish. The blue color is caused by the dark blood of the veins mixing with that of the arteries. These children mostly die early, but some live to be five or six years old, and one I saw twelve, but this is rare. No remedy can be had for this affliction, and I have never known it to cure spontaneously. Some children are so very dark for a few days after birth as to cause great alarm. This is owing to the foramen ovale being very open and[72] closing slowly. No apprehension need be experienced in such cases, as it soon subsides.
The impure blood from the upper part of the fœtal body, which is brought down by the superior vena cava, also enters the right auricle, but does not pass from thence through the foramen, like that from the inferior vena cava. By a peculiar arrangement this blood is made to pass down into the right ventricle, and from thence along the pulmonary artery, the same as in the adult state. Only a very small portion, however, passes into the lungs, the great part being taken along a tube called the ductus arteriosus into the great artery called the aorta, where it begins to turn down to the lower part of the body. In consequence of this, the arterial blood going down to the lower part of the body, is mixed with this portion of impure, venous blood, brought by the ductus arteriosus from the superior vena cava; while that going to the head, and upper part of the body remains pure. And this is the reason why the lower part is always so much smaller than the upper part, previous to birth; it receives less pure nourishment. The head and chest appear, at an early period, almost as large as the rest of the body.
This circumstance also explains why, in the great majority of cases, the right arm is preferred to the left, and has more real power. The place where the ductus arteriosus pours the impure blood into the aorta, is almost immediately opposite to where the artery is given off which feeds the left arm. In consequence of which, in most cases, a small portion of this impure blood becomes mixed with the arterial blood, and the left arm is, therefore, in the same situation as the lower limbs, and like them is comparatively imperfectly developed. The right arm is[73] not liable to any such deprivation. In some cases the insertion of the ductus arteriosus is lower down, so that no such mixture occurs. Both arms are then equal, and this accounts for the fact that in some persons there appears to be no difference. In some cases, no doubt, early habit, or imitation, may overcome this natural inferiority, and even give the preference to the left arm; but such instances are rare; the general rule is the contrary, and for the reason stated.
The ductus arteriosus closes up about the same time as the foramen ovale.
The two veins which convey the impure blood back to the mother, to be purified, originate from the iliac artery, in the pelvis. They pass up the sides of the bladder towards the navel, enter the sheath of the cord, and so reach the placenta. These vessels are obliterated about the third or fourth day after birth, and remain afterwards in the form of a fibrous cord.
The real source of all the blood in the body of the child is a mystery; it would certainly appear most likely for the whole of it to be derived from the mother's vessels, but there are many circumstances which make it probable that the child may form some itself, by digesting the fluid it is supposed to absorb. This view is supported by the fact that there is found in its bowels at birth, and even before, a greenish substance like excrement, called Meconium. This has every appearance of being the product of digestion, though some suppose it to be derived from the liver. It occasionally contains hair, and other anomalous substances.
CHAPTER IV.
The Breasts, or Mammæ, are not needed in the process of generation, nor are they absolutely necessary even after birth; but as they are naturally associated, in the majority of cases, with infantile nutrition, and are besides liable to many derangements and diseases during pregnancy and child-birth, it is advisable to give some account of them.
When one of the breasts is dissected it is found to be composed chiefly of a singular body called the Mammary Gland, which resembles somewhat a very firm piece of fat, of a yellowish drab color. In the substance of this Gland are an immense number of little cells, or vessels, in which, by some unexplainable process, the milk is secreted, or made from the blood. From these little vessels there proceeds small tubes which gradually unite into larger ones, and these again into larger ones still, until at last all the milk is poured into a few tubes, or canals, which terminate in the nipple. The outer mouths of these terminal canals are only slightly contracted together, so that the suction of the child's mouth, or even the pressure of the milk, when the breast is full, will force them open and allow the fluid to flow out.
The following plate represents the structure of the Breast, and explains, as far as it can be explained, the manner in which it performs its functions.
PLATE XII.—a.
a. a. The cut edges of the skin.—b. b. The flaps of the skin thrown back.—c. c. c. The fat which covers the breast.—d. d. The cells of the Mammary gland.—e. e. e. The Tubes or canals, which convey the milk from the Gland to the Nipple.—f. The Nipple, cut down the middle, to show the ends of the milk tubes terminating in it; these are usually about fifteen or eighteen in number.—x. Shows a bunch of the little cells, with the tubes proceeding from them, as they appear when injected.
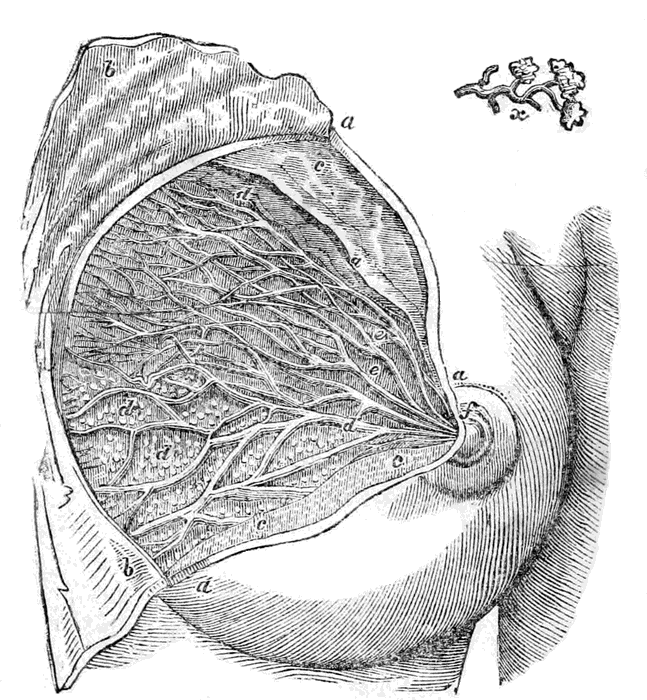
THE FEMALE BREAST.
Plate XII.—a.
This Plate represents the structure of the Breast, and explains the manner in which it performs its functions.
Sometimes there has been seen two and even three nipples on one breast, and in a few cases one of the breasts has had no nipple at all. The two glands are not immediately connected, but have a very intimate sympathy with each other. The size of the breast depends more upon the thickness of the layer of fatty substance, than upon the development of the gland, so that one female, with a very full bosom, may have but little milk, while another, whose breast is but little prominent, may have a superabundance. The graceful swell of the fully developed breast is, however, a matter of positive utility, as well as of beauty, because it better adapts it to the use of the child, and probably also adds to its pleasure, as any one may readily conceive who will observe the delight with which an infant, even when not nursing, will often caress it. Sir Astley Cooper says, "The natural obliquity of the Mamella, or nipple, forwards and outwards, with a slight turn of the nipple upwards, is one of the most beautiful provisions in nature, both for the mother and the child. To the mother, because the child rests upon her arm and lap in the most convenient position for sucking; for if the nipple and breast had projected directly forwards, the child must have been supported before her, in the mother's hands, in a most inconvenient and fatiguing position, instead of it reclining upon her side and arm. But it is wisely provided by nature, that when the child reposes upon its mother's arm it has its mouth directly applied to the nipple, which is turned outwards to receive it, whilst the lower part of the breast forms a cushion, upon which the cheek of the infant tranquilly reposes."
With the exception of the dark areola, or circle, and the little tubercles around the nipple, the breast[80] is of the most delicate structure and color, so that it blushes, or reddens, like the cheek, from any sudden emotion, and goes pale during fainting.
As a general rule no milk is secreted in those who have not become pregnant, nor in those who have passed the turn of life, but occasionally exceptions are observed to this rule.
Bandelocque tells us of a girl only eight years of age, who suckled her little brother more than a month! And Sir Hans Sloane tells us of a lady aged sixty eight, who nursed several of her grandchildren, though she had had no child herself for twenty years! Dr. Francis, of New York, describes the case of a lady who continued to secrete milk regularly for fourteen years after having lost her child, so that she could always nurse an infant; and Dr. Kennedy relates an instance of another who continued to suckle children, uninterruptedly, for forty-seven years, and who had milk perfectly sweet and good even when eighty-one years old! Dr. Clark, of Alabama, informs us that a married lady, who had never been pregnant, was requested to take charge of an infant during the night, and that to quiet it she had put her nipple in its mouth. This was done frequently, and to the great surprise of all it induced a flow of milk. A singular circumstance connected with this was that the lady soon after became pregnant, though previously barren! This will not appear so surprising, however, to those who know the connection between the breasts and the womb, and who have observed the mysterious bond of sympathy by which their functions are united.—(See the articles on Menstruation, and on Sterility, in my "Diseases of Woman," for other instances of this kind.)
The structure of the male breast is precisely the[81] same as that of the female, but it is seldom developed. Instances have been known, however, of the milk being secreted in men, and of children having been nourished by it! Humboldt gives us an instance of this kind, and Professor Hull, of Maryland, exhibited a colored man to his class, in the year 1827, who had a large full bosom, like a female, and who had often officiated as wet nurse in the family of his mistress. The secretion appears to have been established by his putting the children that he had to nurse to the nipple, to quiet them. When the milk was not needed it was found as difficult to dry it up as it is in some females, but it was soon made to flow again, by applying a child to the breast for a few times. This man differed in no other respect from any other man!
In the females of some races of the human kind, the mammæ attain a surprising length, and become very flaccid, so that they hang down to the hips, or lower, and may be thrown over the shoulder for the child to nurse from while carried on the back. Some suppose this to constitute a real variety of the human race, but others suppose it to result merely from habit, which is probably correct.
When the breasts are small sized in young females, their growth may often be promoted, but the means need not be pointed out here.
SIGNS OF PREGNANCY, AND THE MEANS OF DETECTING IT; ITS DURATION, AND THE PERIOD AT WHICH THE FŒTUS CAN LIVE.
It is always desirable, and frequently of the first importance, to be able to know whether a female is pregnant or not, both to the accoucheur and to the individual, or even to be able to judge whether she is probably or possibly so, or not. Sometimes this can be decided positively, but more frequently it is a matter of great uncertainty. The presumptive and positive signs on which a judgment can be formed are of various kinds, most of which can be readily observed, and easily made use of by any person in possession of the information already given in the preceding section. They will be set forth in the following Chapters, together with such other matter as appertains to this part of the subject, in such a manner as will make them available either for professional or for private use.
SIGNS OF PREGNANCY, AND THE MEANS OF DETECTING IT.
The signs of Pregnancy are of three kinds—Presumptive, Probable, and Certain.
The presumptive signs of pregnancy are only of value in the first three months. They consist mainly of certain nervous and organic derangements, and of certain changes in personal appearance. It is scarcely possible to enumerate all these, nor is it necessary; we shall therefore only specify those most important, and most generally met with.
Colic pains, and creeping of the skin, with shuddering and fainting fits, very frequently follow immediately on conception, and in many females inform them when that event occurs. Some persons speak of other sensations, of a peculiar nature, by which they always know, in their own cases, when they conceive; but these sensations are felt by so few, and are so little capable of being explained or observed, that they are of no general use. In most cases, within the first three months, and sometimes in the first three days, the face changes remarkably. The eyes are sunk and dull, and surrounded by a black circle, the nose seems pinched up, the skin turns pale, and red spots, or freckles, frequently appear. Many females also complain of a husky dry throat, numbness in the hands and feet, and a sudden[84] sinking at the heart. These signs, however, are very uncertain guides; very often none of these are felt at all during pregnancy, and sometimes they are all experienced from other causes. One of the most constant signs, according to some, and the most to be relied upon, is an increase in the size of the neck. This I know is often very apparent, and at a very early period. I am acquainted with females who, by simply keeping the measure of their necks, can always tell when they are pregnant. The increase is often considerable in a few days. In young persons of a certain temperament however, the neck is apt to swell merely from marriage, though they do not conceive; and some old nurses, we are told, being acquainted with this fact, judge of the honesty of their unmarried charges by such admeasurements!
This singular development is owing, probably, to a sympathetic connection between the uterine organs and certain parts of the brain, and large nerves in the neck.
Suppression of the Menses is one of the strongest presumptive signs of pregnancy that can be observed, but does not always accompany it, and frequently arises from other causes. In the great majority of cases, it is true, the menses cease to flow, immediately conception occurs; sometimes they will continue for one or more periods after, and occasionally during the whole time of gestation, even up to a few days before delivery. This, however, is a very unusual occurrence, and the stoppage of the menses is by no means so strong a sign that pregnancy has occurred, as their continuance is that it has not. Some females are always irregular, so that pregnancy makes little difference, and in them of course these signs are even less to be depended upon than usual. There have[85] cases been known even of women who have conceived without having menstruated, and of others who never menstruated except when they were pregnant; and it is not at all unusual to see others who will conceive while nursing, and never menstruate between the two pregnancies. Therefore we can only say that the menses usually stop when conception occurs, and that their continuance is strong evidence that it has not occurred, but still both signs may fail.
It is also proper to remark that several medical men have advanced the opinion that the discharge which appears during pregnancy is not the menstrual fluid, but real blood. It has however been accurately examined, and found in no respect to differ from the usual discharge. In my own opinion there is no doubt but that some females really do menstruate while pregnant.
As an instance that the presence of the menses is no proof that pregnancy has not occurred, I give the following case:—Not long since I was requested to see a lady who was supposed to labor under a polypus in the womb. She had been married six years, but had no offspring. On seeing her I suggested, from certain peculiarities in her appearance and manner, that possibly she might be pregnant. The suggestion was met with a smile, particularly by the medical attendant who was present, and I was told that there was no sign of such a thing, and moreover it could not be, for she had never stopped menstruating, nor was there the slightest change in the breasts, nor any disturbance in the stomach, mind, or feelings. On making the usual examination however, I felt fully convinced I was right, and told them so, but my opinion had no other effect than to induce them not to interfere for a time. They had been talking[86] of an operation immediately. She still continued to menstruate for three months after, but in six weeks from her last period was safely delivered, without assistance, of a very fine living child. No part of the body had undergone any material change, except the abdomen, though many of the usual changes occurred after delivery. In this case the delay probably saved the lives of both mother and child, and deeply grateful they all were for the escape. In my work on the Diseases of Woman many fatal cases will be found of pregnant females who have been killed from mistakes of this kind, owing to a blind reliance on such uncertain signs.
Disturbance of the Digestive Functions.—It is very seldom, indeed, that pregnancy does not produce more or less disturbance in these functions, though it must be remarked that marriage also does the same sometimes, even without conception. These disturbances are generally manifested by loss of appetite; sickness, particularly in the morning; vomiting, and depraved taste; the individual frequently taking a fancy to the most extraordinary articles, and making herself extremely unhappy if she cannot obtain them. Thus some have eaten flies, spiders, mice, and other living things, and others again have regaled themselves upon charcoal, chalk, slate pencils, and even earth or ashes. Such freaks are called longings, and it is thought highly improper not to indulge them, which is certainly right when they are for articles not positively injurious; but I have known this notion carried to a very injurious and absurd extent. There is no doubt but these vagaries of the stomach arise, mainly, from its sympathy with the uterus, but it is highly probable that they are often exaggerated, and frequently even produced, by a[87] morbid state of the sensibilities, and by vacuity of mind. The tendency to imitation also, so strong in most females, often leads to the same result. A young female who is declared to be, or who fancies herself, pregnant, listens eagerly to all that is said about that interesting state, by older acquaintances, and when told that they always longed, immediately begins to long also. I have known young persons considerably advanced in gestation, who had never longed at all before, do so immediately after a conversation of this kind. It must be remembered however, that the sympathies of the digestive organs with the womb are very strong, and that the appetite and taste are frequently rendered very capricious at this time, so that the female really likes or dislikes many things that she did not before; but still I feel convinced that the absurd ways in which this caprice exhibits itself, are often owing to the causes I have stated. The wondering ignorance, in which most females are kept, makes them disposed to be led away by a morbid imagination, and constantly liable to be imposed upon by silly and erroneous statements, which they of course implicitly believe. These longings are always the strangest, and most frequently met with, among the most uninformed and unthinking, though they are occasionally met with under all circumstances. As a sign of pregnancy this longing is not much to be relied upon alone, because marriage alone often produces it, and so do many uterine derangements.
Usually all these disturbances disappear by the third or fourth month, the appetite becomes regular, and sometimes even voracious, and the digestion improves, so that the individual may become quite fat, though previously she was very thin.
Some suffer from constipation, and others from diarrhœa, but this is more rare.
Nervous Derangements.—The changes produced in the minds and feelings of pregnant females are sometimes of the most extraordinary character. Individuals who possess, ordinarily, the most agreeable tempers, and the most amiable dispositions, will become peevish and fretful, and often even violently passionate and malicious. Some have even been known to have a disposition to commit various crimes, of which they had the greatest horror in their natural state. Others, on the contrary, who are usually ill-tempered and unhappy, attain a charming tenderness of manner, and a most pleasing serenity of mind. Their likings and dislikings also change very much, so that their most valued friends will become hateful to them, and those whom they habitually dislike will seem endowed with every loveable quality. Some will become perfect misanthropes, or weep and fret without intermission, while others will exhibit the most reckless and boisterous gaiety. I have known some much disposed to study while pregnant, and others who would draw, or paint, most excellently, though at other times they were but indifferent artists. In short, it is impossible to denote half the singular changes of this kind that are thus produced. Suffice it to say that, when well marked, they are strong presumptive signs of pregnancy, especially when coming in connection with other evidences. It must be remembered however, that hysteria, and some other uterine diseases, are often accompanied by similar changes.
Alteration in the appearance of the Breast.—The direct, and sympathetic connection between the womb and the breast is so great that pregnancy usually[89] causes corresponding changes in both, though not always. In most cases however, the breasts swell, and become painful. The nipple becomes elevated, and the circle around it assumes a dark brown color, and is dotted with small tubercles, from which a thin watery liquor may often be pressed. The nipple will also enlarge, or become erect on being rubbed, and, as gestation advances, milk may be forced from it. Most of these signs however, may be wanting in pregnancy, and may arise independent of it. Chronic inflammation, and other diseases of the womb, will frequently produce them, as may be seen in my "Diseases of Woman." Marriage alone frequently causes such symptoms, particularly in certain temperaments, and deranged menstruation will frequently produce them.
The alteration in the color of the areola, or circle round the nipple, is a sign much relied upon by some, but is frequently a deceptive one, merely from want of close observation. I have known many females, though frequently mothers, whose breasts always retained the bright rosy color they had previous to marriage; and I have known young unmarried females with the breasts quite dark. The peculiar hue that arises from pregnancy however, is different from anything I ever saw in non-pregnant females; and, though not always to be met with, is, in my opinion, an infallible sign when present. The celebrated John Hunter regarded this sign as an unmistakeable one, and he gave a remarkable instance of it in his lectures. In making a post mortem examination of the body of a young female, he observed this peculiar color, and at once proclaimed her pregnant, though the hymen was unbroken. On dissection he was found to be correct—she was four[90] months advanced. If this sign were constant, pregnancy could nearly always be ascertained, but frequently it does not appear. The peculiar color must be seen to be recognized, as it cannot be accurately described; perhaps the nearest approach to it is the shell of a fresh ripe chestnut, but it is much darker in some than in others. The dark circle is nearly always more elevated than the rest of the breast, as may be seen by taking a profile view.
PLATE XIII.
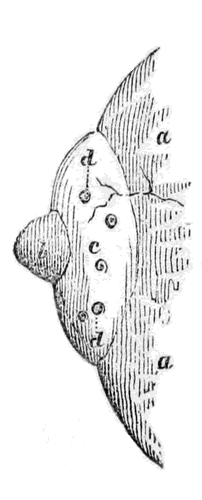
View of the Breast about the Fourth Month.—a. a. The Breast.—b. The Nipple.—c. The Areola, or part which becomes brown; it is elevated above the rest of the Breast, as may be seen.—d. d. The little Tubercles.
Most frequently the breasts do not swell, nor the areola change color, nor the tubercles appear, till about the fourth month, and frequently much later.
All these changes in the breast are also liable to become more or less permanent, after the first pregnancy, so that they are of much less service, and less to be depended upon, in all succeeding ones. They also remain, with most females, during nursing, and are therefore not available in those who conceive while they are nursing. On the whole however, these signs, especially in those not previously pregnant,[91] may be pretty confidently relied upon, and will seldom deceive an experienced observer.
The secretion of milk is, by most persons, considered a positive sign of pregnancy, but it is not so, for it sometimes takes place in young girls merely from the establishment of puberty, and in some females it always occurs at each monthly period, though they have never been pregnant. Instances have been known of women nursing other people's children though they had never conceived themselves.
Miscellaneous signs.—There are a few other presumptive signs, not easily classified, some of which are of value, while others are so uncertain, or so little available, as to be almost worthless. All these however, it is necessary to point out, because some of them may be made use of in cases where the more ordinary signs are absent.
In the unimpregnated state the mucus membrane, which lines the Vagina, is of a bright rose color, but in nearly every case of pregnancy it changes to a bluish, or purplish hue. I do not recollect a single instance, in the course of my own observation, in which this change has not occurred, and the same statement is made by several eminent authors. It is true that in some young females the mucus lining is naturally darker than it is in others, but, like the areola round the nipple, this natural tinge is not like that produced by pregnancy. It is of course impossible to say whether this blue tinge is always produced, though I am inclined to think it is, and I should certainly consider it an almost infallible sign when present. Parent Duchatelet states that he was present when M. Jacquemin proved this, without a single failure, in four thousand five hundred cases.
Many females are also warned of their condition[92] by pains in various parts of their bodies, the most frequent of which is one felt at the top of the head. Some always have palpitation at the heart, and others experience a singular kind of fluttering in the womb.
Many medical men rely altogether on certain peculiarities in the urine, and as this sign is really a valuable one, in some cases, I will describe the mode of examination fully. The urine is put in a clean vessel, and allowed to stand perfectly still. In a short time, varying from two to six days, a number of little opaque bodies begin to rise from the bottom, like flocks of cotton, which unite together at the top into a thin but firm layer, or pellicle, like cream on the top of milk. This layer is frequently so consistent that it can almost be raised out of the vessel, by taking hold of one edge, and may be easily drawn out by passing the finger under it. This substance is called kyestein. It is of a whitish color, semi-transparent, and looks as if it were partly crystalized. After a few days, if left undisturbed, the urine becomes thick and muddy, and the pellicle of kyestein breaks up and falls to the bottom. According to the experience of many medical men, and so far as I have seen myself, this peculiar substance is always to be found in the urine of pregnant females, after the first month, and frequently even earlier. Sometimes a substance similar to it is observed in the urine of those not pregnant, but there is, in most of these cases, sufficient difference between them to enable any one, who has seen both, to distinguish one from the other. The only time, except during gestation, when real kyestein appears to be formed, is while the milk is being secreted and not freely discharged. Thus it may often be found when the female is weaning, and, some writers assure us, in some cases[93] during the whole period of nursing. On the whole this sign is a very valuable one, and may be much relied upon.
The changes in the pulse, on which some persons rely, are of no value whatever as a sign of pregnancy, since they are no more frequent, and not at all different, so far as I have seen, from what ordinarily occur from other causes.
The development of the abdomen, though an invariable accompaniment of pregnancy, is by no means a certain sign of it, since it may be produced by other causes; and besides, it is sometimes but little to be observed till a late period. The peculiar manner of the development however, is usually somewhat different from that produced by tumors, and other diseases. Very often the abdomen will be tolerably large by the second month, and then again become so much smaller that the female will think she is certainly not pregnant. This is owing chiefly to flatulence, produced by digestive disturbance during the early periods, but which afterwards subsides. In a short time however, the uterus not only enlarges more, but rises, and the development becomes permanent. This circumstance of there being often two developments has deceived many, and I have known females declared to be not pregnant, simply because the development of the abdomen went down, who, in a short time after, exhibited unequivocal evidences of being in that condition. The first development, or swelling, is merely similar to what often arises from indigestion, and other causes, and is therefore no sign of pregnancy; but the second development is accompanied by other changes, besides being more permanent.
The linea alba, or white line, which may be seen[94] extending from the navel to the pubis, in the ordinary state, becomes much darker, the skin of the abdomen wrinkles, and the umbilicus, or navel, becomes prominent.
Swelling of the eyelids, and puffing of the face, are experienced by some females, but are not very general, and so frequently result from other causes that they are of little value as evidences in this case.
This, I believe, comprises all the presumptive signs of Pregnancy that are worthy of notice. Some of them are valuable and may be depended upon, particularly the presence of kyestein in the urine, which may almost be called a certain sign. Others of them are of little value alone, but are useful in the way of corroboration. The more there are of them observed together, in any case, of course the more grounds there are for the presumption that pregnancy exists, and the reverse.
It must be carefully remembered however, that these presumptive signs are precisely those most likely to be produced by other causes, particularly by marriage only; they must therefore be well weighed, and unless very numerous, or very distinctly marked, must not be regarded as conclusive. As already remarked, it is only during the first three months that most of these presumptive signs are taken much notice of; after that we have others that can be more depended upon, and which will be described in the succeeding articles.
End of the third month.—The probable signs now to be described are seldom recognized before this time, and not generally with distinctness till a still[95] later period. They chiefly consist of certain changes in the form, development, and position of different parts of the uterus, to ascertain which requires an internal examination. These changes are not observable till the end of the third month, previous to which time we cannot be certain that the womb has really increased beyond its normal size. And even then, when the increase is obvious, we cannot tell how it has been produced; it is not till a much later period, till five or six, or even seven months are elapsed, that pregnancy can be ascertained with anything like certainty.
The changes to be noticed are in the form, and size, of the neck and body of the womb, and in its mouth, and also in the weight of the whole organ. No one, of course, can expect to recognize these changes who is not acquainted with the parts in the unimpregnated state, both in the virgin and in those who have borne children.
The mode of conducting the requisite examination is, by introducing the index finger of the right hand, covered with oil or mucilage, into the Vagina, and then carrying it upwards till it reaches the Os Tincæ. By means of this finger the position and length of the neck of the womb are ascertained, and also the state of its mouth, whether it is opened or closed, and to what extent. If it be then placed at the top of the neck, on the under side, and the other hand upon the fundus of the womb externally, and pressing firmly upon it, the organ is enclosed as it were between the two hands, so that its size and form may be pretty accurately ascertained, and also its degree of firmness, by which a judgment may be formed as to whether it is occupied by any solid body, or fluid, or whether it is empty. In addition to this a pretty[96] accurate estimate may be made of its comparative weight, by balancing, and raising it up on the finger. This is called by the French Ballotment, and, as will be shown further on, is a valuable means, at certain stages, of ascertaining pregnancy.—(See Plate XVI.)
The female may be examined either standing or lying down, though the recumbent position is best, except in certain displacements of the womb, when it is most likely to be thrown into a position in which the neck can easily be reached by the female standing. The position of the neck is very different in many of these displacements, and during pregnancy, to what it is in the ordinary state, and a person not acquainted with these changes might frequently be much puzzled to find it. As we have already remarked, also, there are certain differences between those who have had children and those who have not. The following three diagrams represent the changes just spoken of at three different periods:—
PLATE XIV.
Figure 1, represents the form and size of the body, neck, and mouth of the Womb, at about the third month.
Figure 2, the same at about the seventh month.
Figure 3, the same at the ninth month.
The references are the same in all. a. The Neck of the Womb.—b. b. The Body of the Womb.—c. The Os Tincæ, or Mouth of the Womb.—d. d. The cut edges of the Vagina.
Fig. 1.
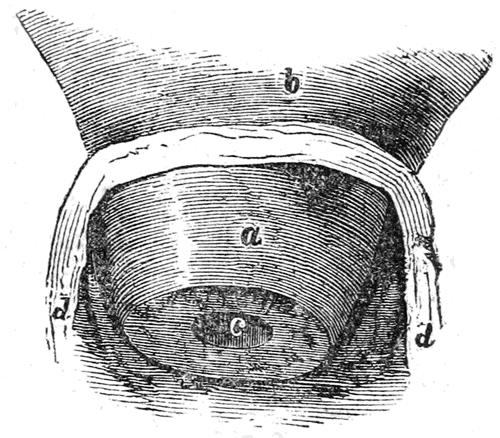
Fig. 2.
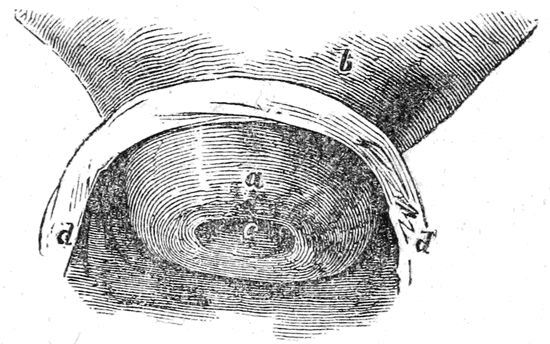
Fig. 3.
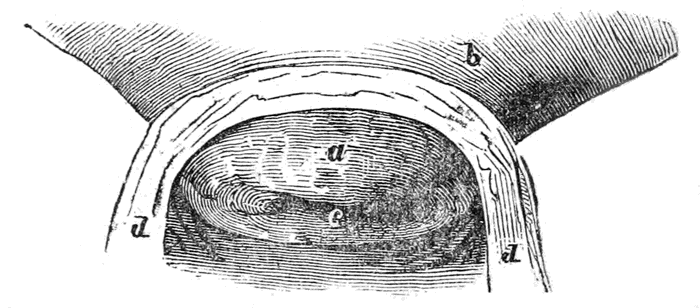
Plate XIV.
The form and size of the body, neck, and mouth of the Womb, at about the third, seventh and ninth months.
It will readily be seen by these diagrams that the alterations in the neck and mouth of the womb are very marked, and of a character easily to be ascertained by the touch. These three should be compared with the section of the womb in Plate IV, which represents it in the unimpregnated state.
The difference between those who have borne children, and those who have not, is well represented in Plate XV,—the drawings being one-third of the natural size, and representing the appearance at about three months.
PLATE XV.
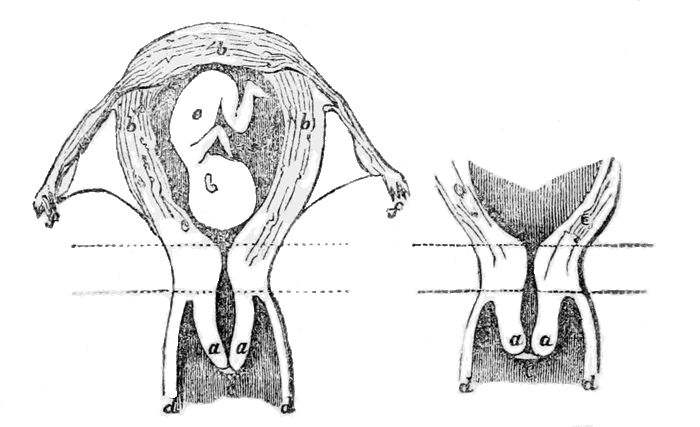
a. a. The neck of the Womb.—b. b. b. The body of the Womb.—c. The Os Tincæ, or mouth of the Womb.—d. d. The cut edges of the Vagina.—e. The Fœtus.—f. f. The Fallopian Tubes, Ovaries, and Round Ligaments.—g. The Placenta.
Most of the changes produced can be readily distinguished by the finger, after seeing this representation, and making a proper comparison between it and the natural state in Plate IV.
The Neck is not much enlarged at this period, but its lower part is somewhat soft to the feeling. The Os Tincæ is more rounded than in the unimpregnated state, particularly in the Primipara, in whom in fact it is nearly circular, the lips being quite smooth and closed. In the female who has already borne children it is somewhat open, so that the finger may often be introduced; and the lips feel rough, owing to scars and laceration in previous deliveries. It is also larger altogether, and softer, than in the primipara. The whole length of the neck at this stage is about two inches.
The body of the uterus, when pressed between the two hands, will be found much larger than ordinary, and more round, and it will feel heavy when pushed up by the finger.
In regard to the precise value of these probable signs, it can only be said, when they are observed, that it is certain that the womb is enlarged, and most probably from pregnancy. But at the same time it must be remembered that several diseases, and particularly suppressed and irregular menstruation, or the development of tumors and polypi, will effect very similar changes, and that it is not always possible to say whether they arise from these abnormal growths or from pregnancy, though it can generally be done. But though we cannot, in every case, say when these signs exist, that the female must be pregnant, we can nearly always say, when they do not exist, that she cannot be so, particularly if the other usual signs are absent.
End of the fourth month.—By this time the neck has become a little shorter still, and the mouth more open, but on the whole there is not much change to be felt internally. The body of the womb however, has now ascended above the superior strait of the Pelvis, and begins permanently to enlarge the Abdomen. It may be distinctly felt between the two hands, like a firm round ball, somewhat elastic, and resisting when pressed. This is the period when the motions of the fœtus are usually felt first, and these motions, with the ascension of the womb, are sometimes experienced very suddenly, so as to alarm the female, and produce certain curious sensations, with much nervous derangement. This is called quickening, and, with some persons, is always so well marked as to indicate not only their condition, but the very period, with great precision. Many however, never experience anything at all peculiar at this time.
It is customary for the medical attendant, as a means of making the child move, to put his hand first in cold water, and then over the fundus of the uterus; the sensation of cold thus conveyed usually causing it to move immediately. Great care must be taken however, that other motions be not mistaken for those of the child, an error not at all uncommon. Many a female, and many a medical man also, has been deceived in this way, particularly in cases of uterine or ovarian dropsy, and tumor, and even in ordinary flatulence and hysteria. Females who much desire offspring frequently deceive themselves in this way, and it is sometimes next to impossible to convince them of their error. Some women possess the power of imitating the movements of the child, with great exactness; and instances have been known where[104] they have successfully imposed, both on their friends and medical attendants, for a long time, in this way. Mr. Dubois mentions instances of females who possessed this extraordinary power, and who, though not pregnant, used to present themselves to his class, for the pupils to ascertain the motions of the child. In short, this sign must not be too much relied upon, nor too confidently expected, for many females observe no fœtal motions at all till the sixth or seventh month, and even then very indistinctly. Sometimes also, after having been distinctly felt, these motions will altogether stop for a long time, and then appear again.
At this time however, Ballotment can begin to be practised, though it is not quite so certain as at a month later. The manner of performing this important manipulation has already been partly described, and by examining Plate XVI, and attending to the following remarks, it may be readily understood and practised.
PLATE XVI.
This Plate represents the mode of performing the Ballotment, to detect pregnancy. The outline of the figure is the same as in Plate I, and most of the organs are lettered the same.
The index finger of the right hand is passed into the Vagina till it touches the body of the Womb, the neck being thrown back, owing to the tilting of the Fundus forward. The left hand is pressed firmly upon the Abdomen, just over the pubic bone.
1, Is the Fœtus.—2, The Placenta, connected with the Fœtus by the cord.—3, Is the index finger of the right hand, within the Vagina.—4, Is the left hand.
The development of the Womb, and the change in its position, are very well represented in the Plate, and so are the alterations in some of the other organs. The manner in which the Bladder, A, is pressed out of its usual shape and size, may be seen by comparing this with Plate I. The shortening of the Vagina, and the expansion of its upper part, are also equally obvious, and the manner in which the mouth of the Womb is thrown back against the Rectum.
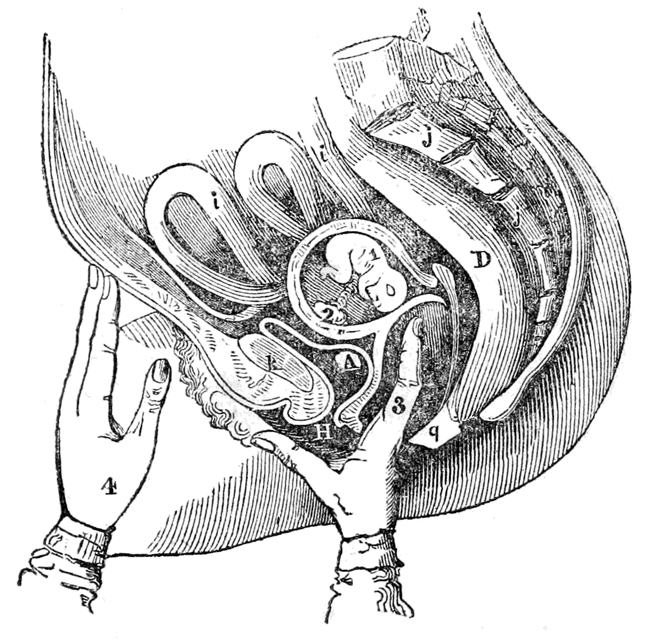
Plate XVI.
This Plate represents the mode of performing the Ballotment, to detect pregnancy. The outline of the figure is the same as in Plate I, and most of the organs are lettered the same.
When the right hand finger (1 Plate XVI,) is carried to the top of the Vagina, it meets with a round soft tumor, which is the head of the child felt through the walls of the womb. As soon as this is distinctly felt, the finger must be withdrawn a little, and then pushed suddenly against the tumor with a jerk; this will displace the fœtus, and cause it to rise in the liquor amnii towards the Fundus, so that the round tumor will have disappeared. In a few moments it will sink down and may be again felt, and again displaced in the same manner. This is called the Ballotment, or balancing it on the end of the finger. The sensation conveyed on touching the Fœtus, and when it rises after being pushed, are so peculiar that they are not likely to be overlooked, or mistaken for anything else, after being once experienced. The jerk is not required to be at all violent, and had better be made at first very slight, as it can easily be repeated a little more forcibly if the tumor does not rise at first. Some practitioners practice the Ballotment in this way, using the one hand only; but others place the left hand also on the Abdomen, (4 Plate XVI,) at the same time, and immediately after jerking upwards with the right hand, they suddenly depress the Abdomen, just over the pubes, with the fingers of the left, so as to send the Fœtus down again more quickly and more forcibly. This is seldom needed, but if the first way does not succeed the two hands may be tried.
A species of ballotment may even be practised externally, in the following way:—The fingers of the right hand are placed on the Abdomen, just over the fundus of the womb, like the left hand in Plate XVI, and a smart jerk is given downwards and backwards, several times in quick succession. This also displaces[110] the Fœtus, which may be distinctly felt to float away, each time the percussion is made. No one can mistake this peculiar motion who has once felt it.
Sometimes one of these manœuvres will succeed when the other fails, so that it is well to practise them all. They may be performed with the female either standing or lying down, and will sometimes succeed one way when they will not the other.
It is requisite to remember that in presentations of the breech, or trunk, the ballotment may not succeed as well as when the head presents; or it may even fail altogether, so that when it is unsuccessful we must not immediately conclude there is no pregnancy. Tumors in the womb, stone in the bladder, and various uterine displacements, may also create uncertainty, or cause failure, but these accidents are rarely met with, and only interfere materially at an early stage; afterwards ballotment can be practised notwithstanding them, or auscultation may be resorted to.
In short, this mode of detecting pregnancy is one of the most certain, and the most generally applicable, that we possess.
End of the fifth month.—At this time the Uterus has increased considerably in size, and has ascended so high in the Abdomen that the Fundus is level with the umbilicus, or navel, in a first pregnancy, though somewhat lower in those who have borne children before. This rising of the womb makes the Vagina longer, and brings the neck of the womb nearer to its centre. In the previous stage the neck was thrown so far back that it was difficult to reach, but now it is much more favorably situated, though much higher. Its substance is softer than before, and the two lips are nearly on a level, and somewhat[111] opened, particularly in those who have borne children before. Indeed, in them the point of the finger may be introduced, as seen below:—
PLATE XVII.
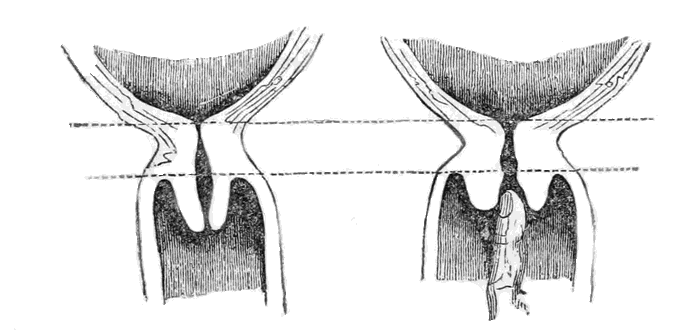
This is at the end of the Fifth Month, and the drawings are about one-third of the natural size.
Ballotment is now much more easily practised, and is more conclusive. A new sign is also to be distinguished, by which we are furnished with another valuable means of detecting pregnancy. The child's heart begins to beat so strongly, and its circulation is so vigorous, that the sound of it can be heard externally. The same means are taken to ascertain this that are used in sounding the chest of an adult. If the ear be placed on the Abdomen, over the womb, the beating of the fœtal heart may[112] be heard quite plainly; and if the stethoscope be used it will be still more distinct. This practice is called Auscultation. The signs furnished by it are certainly of the greatest value, and frequently enable us to detect pregnancy with unerring certainty. Indeed, not only can we tell by them that a child is in the womb, but often even the very position in which it lies, and whether there be twins, or more. This is done by noting where the heart is situated, by the sound, and whether the beating is single or double.
The nature of these sounds, and the manner of detecting them, require to be carefully explained.
If the person wishing to notice this sign is not already familiar with the beating of the adult heart, he had better become so first. The ear should be placed on the left side of a grown up person, on the skin, just beneath the breast, and held very still. The heart will then be heard to beat very distinctly, there being two sounds, a long one and a short one, alternating with each other. When this has been listened to for some time, the ear will be able to catch any similar sound, and the auscultation may then be practised to detect pregnancy.
The ear must be placed on the Abdomen, about midway between the Pubes and the umbilicus, and towards the left side. No weight should be borne on the body, but the ear must be laid sufficiently close to exclude all external sounds, and no motion should take place, particularly with the clothes. If the sound be not heard in the position first assumed, move a little, in different directions, till that point is attained where it is most distinct. It can scarcely fail to be heard, with ordinary care. A practised ear will sometimes distinguish the sound as early as the fourth month, but generally it cannot be heard[113] before the end of the fifth, or even till the sixth month. There are several sounds that may either be mistaken for it, or that may confuse the ear. The beating of the mother's heart will sometimes be very distinct, as far as the lower part of the Abdomen, but it is much slower; the child's heart throbbing nearly twice as fast. The movements of the Fœtus, and the rumbling of the intestines, will also interfere; but when once the proper sound has been caught it may be kept independently of all these.
The manner in which the child lies in the womb will determine where the heart shall be opposite, and as its position frequently varies, both in different individuals, and at different periods, in the same person, the sound must be sought for at several points, till the right one is found. The most usual position will be seen in several of our plates, and they will give sufficient indication to enable almost any one to practise this mode of detection with success. During the early months the child moves about a good deal, so that the sound may be heard one day in one place, and the next in another. About the seventh month however, it becomes more fixed, so that the place of the heart can be pretty certainly ascertained, and thus the position of the whole body is made out, whether the head is downwards or upward, and a tolerable idea can be formed even as to the direction of each part.
Many persons have failed in their attempts to hear the Fœtal pulsation, but I cannot but think it must have been either from inattention, or from not being acquainted with the sound of the heart at all. I never recollect an instance when I could not do so, at the proper time. M. Chailly says he does not hesitate to affirm that in every instance they can be[114] detected; and M. P. Dubois distinctly heard them in one hundred and eighty-five females, out of one hundred and ninety-five, in the other ten the child being probably dead. Indeed, the absence of this sound is the most certain sign of the death of the Fœtus, as its existence is of its being alive; and medical men now tell whether the child is dead or not by these very means.
In conducting the auscultation the female must recline, and keep as still as possible, breathing low. The Abdomen may be covered with a single thin garment, if absolutely insisted upon; but the judgment will be so much the more uncertain, owing both to the deadening of the sound and to the friction of the material. The experimenter must also recollect that if the head be held down too long, the blood will rush to it, and cause a humming in the ears, which will confuse him; it will therefore be better if the bed be high.
It is always best to use the stethoscope, as it covers only a small space, conveys the sound more directly, and shuts out external noises more effectually. This instrument is extremely simple, consisting merely of a tube of wood, glass, metal, gum elastic, or almost any other material. One end should be expanded a little, like a bell, and the other made small, so as to fit close in the ear—the large end being placed on the Abdomen. It may be about a foot in length, though a little shorter or longer will not make much difference. I once used a child's tin trumpet, having no regular stethoscope with me, and succeeded with it perfectly. The large end should be pressed on the Abdomen, and the smaller one into the ear, sufficiently close to shut out all other sounds but those coming from the body. This is the same instrument[115] that the lungs are sounded with, when we want to judge of their action and condition.
This is an invaluable means of detecting pregnancy; in fact, at the proper time, and with due care, it may be said to be certain.
End of the sixth month.—This is the period when, according to the law, the child can live. There are no new signs at this time, but those previously noticed are now more distinct. The neck of the womb is still softer and shorter, and the finger can penetrate further in the passage than before. The fundus of the womb is now above the umbilicus, in primipara, though not so high in those who have borne children; and the bladder is above the superior strait.
Ballotment can now be practised with certainty, the falling and rising of the Fœtus being very distinct.
Auscultation also becomes more positive, the sounds being louder and more easily ascertained.
End of the seventh month.—The fundus of the womb has now risen still higher, and the Bladder is pushed completely above the upper strait, so that the whole length of the Urethra lies behind the pubic bone. It is then much pressed upon and swollen, and being much longer, and bent out of its usual course, the urine is often passed with difficulty, and the catheter can scarcely be introduced. The upper part of the Womb now lies over towards the right side of the body, very evidently. This direction is nearly constant, in all females, but the reason for it is not known. There have been many theories to account for the peculiarity, but none of them are either so plausible, or so well supported by facts, as to be generally adopted.
The upper part of the Womb being tilted to the[116] right side, the neck of course points to the left, and backwards. It is now very short, even in primipara, but in those who have borne children it is scarcely to be distinguished at all. The finger may now be introduced, even in primipara, half way up the neck; and in others it will reach even into the uterine cavity.
PLATE XVIII.
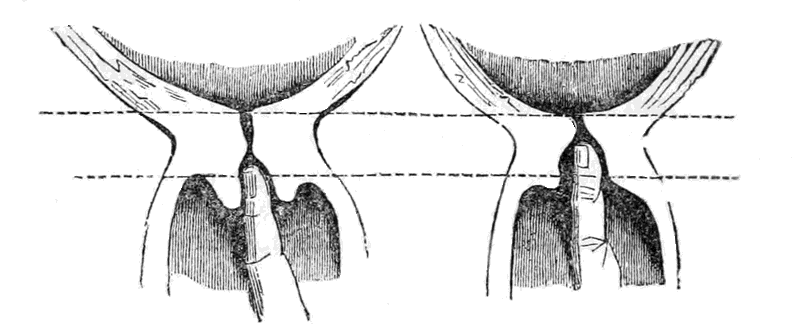
The neck of the Womb in a first pregnancy, and in a female who has borne children before, at the end of the seventh month.
The part below the lower line here, shows that part of the neck which is contained in the Vagina. It will easily be seen how much shorter this part is, and how much more open the passage is, in the female who has borne children, than in a first pregnancy.
Ballotment and Auscultation both, now afford unmistakeable evidences as to the condition of the patient.
End of the eighth month.—By referring to the preceding[117] Plates, it will be seen that the part of the neck of the Womb above the Vagina, which is placed between the two dotted cross lines, remains almost unchanged, while the part within the Vagina, or that below the lowest line, becomes less and less, till at this time, in those who have borne children, it can scarcely be felt at all; and even in a primipara it is merely like a small tubercle. About this time however, the upper part of the neck begins to shorten also, though that is not so obvious, and therefore not so useful for our present purpose.
On making an examination, the mouth of the Womb itself may now be felt, at the upper part of the Vagina, and far back. It is however, very difficult to reach, on account of its position. The finger will now pass, in those who have previously borne children, into the cavity of the Womb itself, but in others it will scarcely reach so far.
The linea alba becomes darker at this period, and so does the areola around the nipple. Certain peculiar marks also appear on the Abdomen, and upper part of the thighs, almost like the pits from small pox. They are usually diamond shaped, slightly depressed, and dark in color. They appear to be owing to the over stretching of some of the parts under the cuticle, and which give way in consequence. In first pregnancies, and in those who enlarge very much, these marks are sometimes very numerous, and remain for a long time after delivery, sometimes even they never disappear. As signs of pregnancy however, they are but of little value, because they are often produced by other causes that distend the Womb. None of these presumptive signs are now needed, and therefore they are of little consequence, because there are others more certain.
The motions of the child itself can now be generally both felt and seen, and an experienced observer may even predicate from them, with tolerable certainty, the position in which it lies. Ballotment, by one hand on the Abdomen, may still be practised with success; but in the Vagina it is difficult, because the Fœtus is both more fixed and heavier.
Auscultation is now the surest dependence however, and may be advantageously resorted to also as a means of determining beforehand the position of the child. This may be done even a month earlier, but not so certainly as now.
To understand how this important point is determined, it is only necessary to recollect, as will be very evident, that the pulsation will be heard the loudest immediately over the heart; and as we know the form and general size of the Fœtus, and the manner in which it usually lies, it becomes possible, when the position of its heart is discovered, to trace out, from that, the position of every other part. This will be evident by referring to Plates XIX, XX, and XXI. It will then be seen that, if a line be drawn across the middle of the Abdomen, the heart will be above that line when the breech presents, and below it when the head presents, and on the right or left side, as the case may be, in each position.
In case of twins there will be two pulsations, and they so much interfere with each other that it is difficult to distinguish either. The two children being generally disposed with the head of one to the heels of the other, one heart will be above the line, and the other below, on opposite sides, as shown in Plate XXII.
PLATE XIX.
This Plate represents the Fœtus in the most usual position, the head downwards, and the back of it presenting to the left side.
The black spot a, shows the situation of the heart; usually immediately under that part where the sound is heard the strongest.—It is below the line.
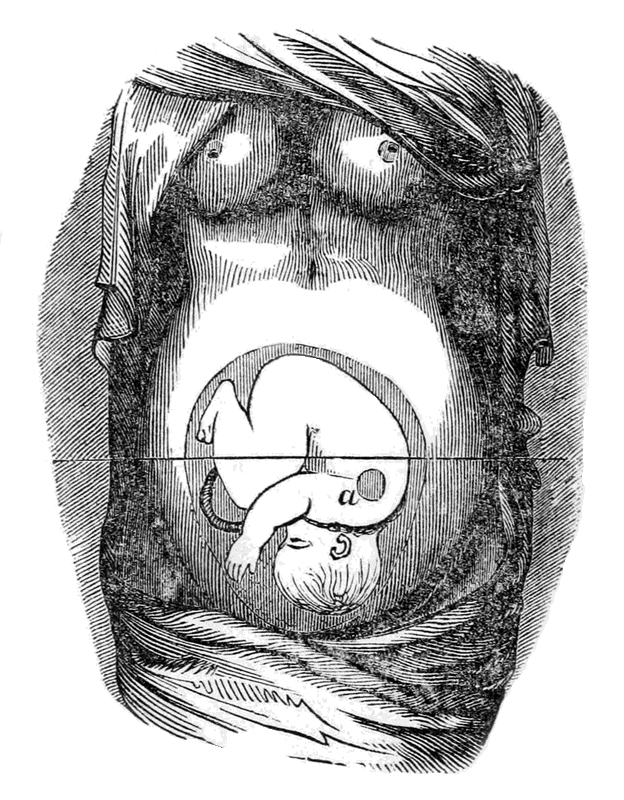
Plate XIX.
This Plate represents the Fœtus in the most usual position, the head downwards, and the back of it presenting to the left side.
PLATE XX.
This Plate represents the Fœtus in the next most frequent position, the head downwards, but the back of it presenting to the right side.
The black spot a, shows the situation of the heart as in the previous Plate. It is now below the line, as before, but on the opposite side.
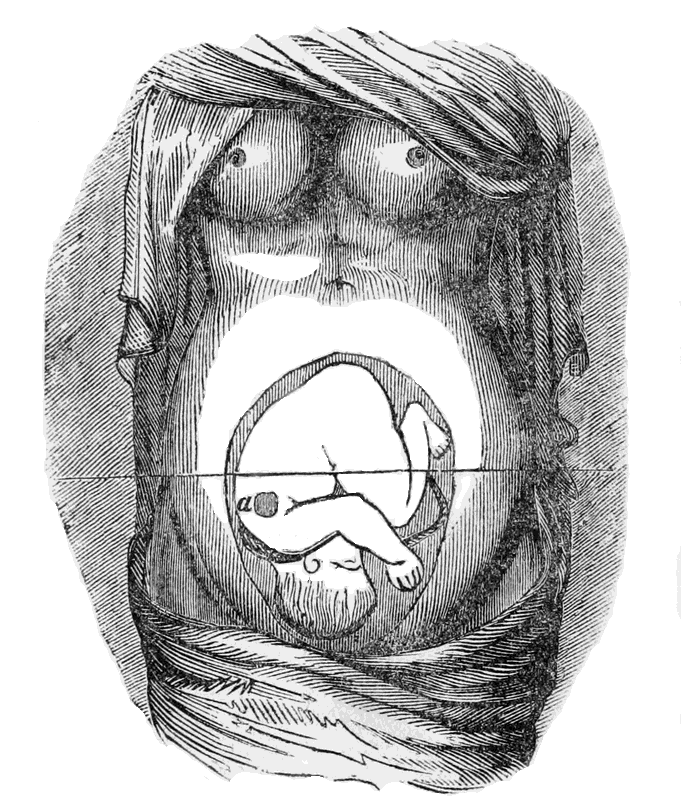
Plate XX.
This Plate represents the Fœtus in the next most frequent position, the head downwards, but the back of it presenting to the right side.
PLATE XXI.
This Plate shows the position of the Fœtus in a presentation of the Pelvis, or breech, which happens, comparatively, but seldom.
The black spot a, denotes the situation of the heart, which is here above the line, instead of below.
In this case, as in the others, the heart may be on either side of the body, according as the child faces, but always above the line.
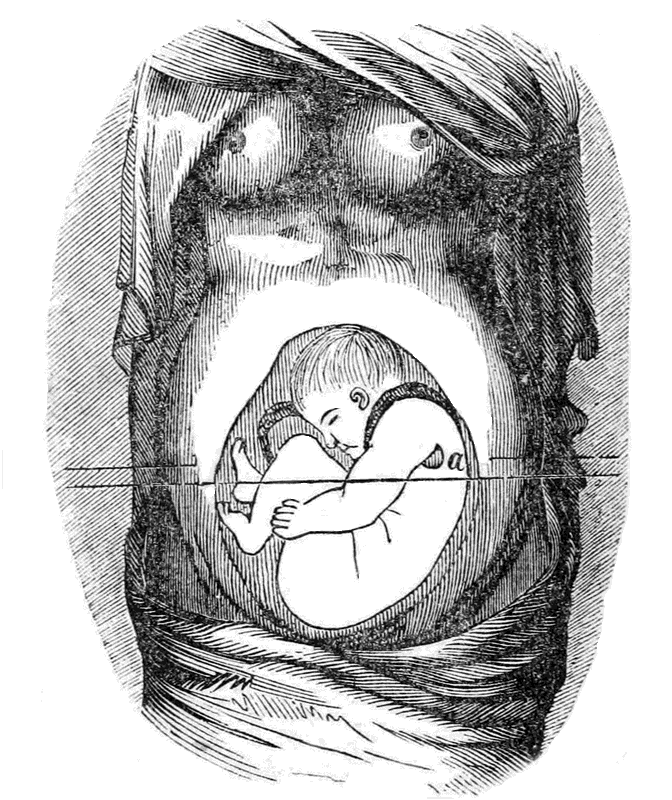
Plate XXI.
This Plate shows the position of the Fœtus in a presentation of the Pelvis, or breech, which happens, comparatively, but seldom.
PLATE XXII.
This represents the position of Twins, as most usually observed, one having a head presentation, and the other a breech.
The black spot a, on both, denotes the position of the heart, which in one case is above the line, and in the other below.
The head however, may be on the right side instead of the left, and so reverse the position of the two hearts, but this is very seldom the case.
When there are more than two, the confusion and uncertainty becomes still greater.
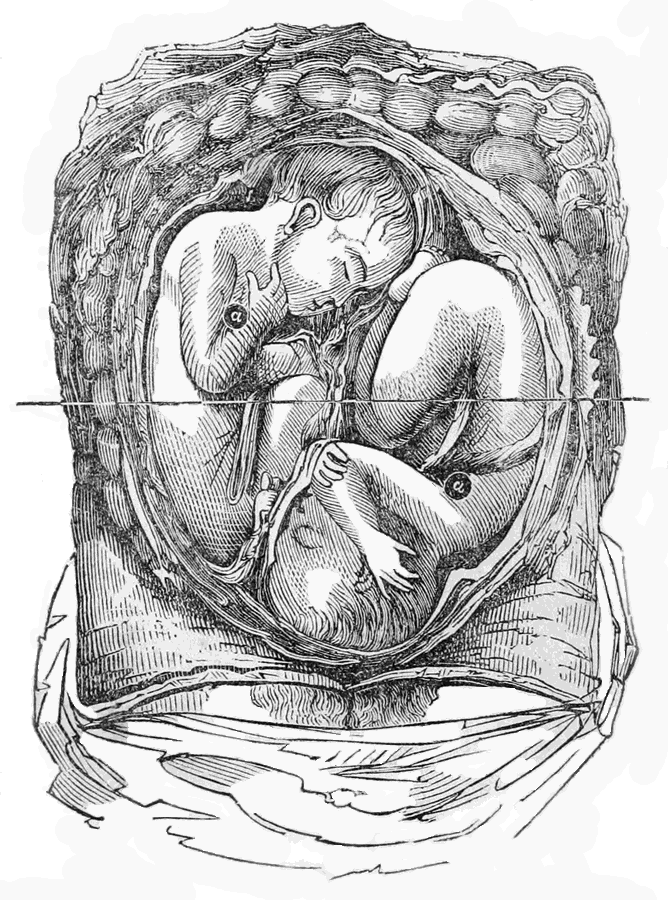
Plate XXII.
This represents the position of Twins, as most usually observed, one having a head presentation, and the other a breech.
At this period the signs previously observed become more distinct, but there are few new ones. The external lips sometimes swell, and the breathing becomes more difficult, owing to pressure on the diaphragm. The trouble with the urine is also apt to increase, and little mucus tubercles, like pimples, occasionally form around the Os Tincæ, and on the upper part of the Vagina.
End of the ninth month.—There is but little difference between this and the previous period. The mouth of the Uterus is more open, and, in those who have had children, the finger will pass directly into the Womb, and feel the child, but in primipara there is still a small portion of the neck left.
PLATE XXIII.
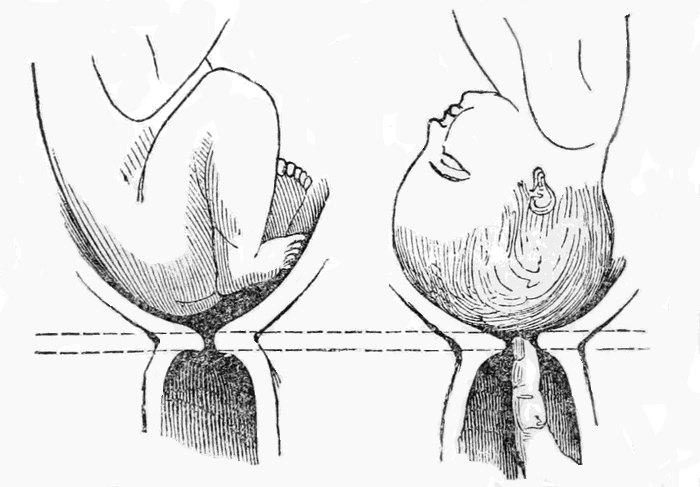
Ballotment is now more obscure than before, as the Fœtus is very heavy, and quite low down, and pretty firmly fixed. Auscultation is distinct enough, but not more so than at the previous period. The swelling of the lips, and of the veins of the legs, may increase, and so may the difficulty with the urine; but the breathing generally becomes easier, owing to the Womb having descended a little, and so pressing the diaphragm less.
These comprise all the signs and indications of pregnancy that possess any real value. Some of them, at certain times, and under particular circumstances, may be called positive; such as those discovered by Ballotment and Auscultation, and also the presence of Kyestein in the urine. Most of the others merely make it probable that pregnancy exists, or warrant us in presuming as much. They are not to be depended on implicitly alone, but when many of them are observed together, and no other cause can be assigned for their production, the presumption becomes so well supported as almost to be called a moral certainty. A person of experience, who is familiar with all these signs, and with the others produced by disease which resemble them, will seldom find it difficult to decide; but still there are cases in which pregnancy proceeds, even to its termination, with but few unusual symptoms, so that both patient and attendant are completely at fault. This however is very rare, and many eminent authors contend that it is always possible to detect pregnancy, after the sixth month, and I think so myself, unless the child be dead, in which case it will soon be evident in another way.
The duration of pregnancy, or the precise term of Utero Gestation, is not fixed. It appears, from accurate observation, that there is no absolute period determined by natural laws, and therefore there is none laid down by human enactments. An approximation can be made, by taking the average of a number of cases, and the period of limitation may also be determined in the same way. The most usual period is about nine months, or from thirty-five to forty weeks, some females going beyond the thirty-six weeks, and others not so long. First children are frequently born under the nine months, and more so than those that come after; this is a fact not generally known, and ignorance of it has often given rise to unjust suspicions. It is quite possible for a female to be delivered, with the child at full period, in a little over eight months after marriage, without there being any just grounds whatever for suspecting unfaithfulness.
Dr. R. Lee, in his Lectures on the Theory and Practice of Midwifery, gives the best summary that we have in the language, of our information on this subject; I will therefore quote from his work, making such comments and additions as I may think advisable.
"The Roman law fixed the period of gestation at ten lunar months. The civil code of Prussia ordains that a child born 302 days after the death of the[138] husband shall be considered legitimate. By the law of France, the legitimacy of a child cannot be called in question who is born 300 days after the death or departure of the husband. The laws of England declare that the usual period of human utero-gestation is nine calendar months, or forty weeks; farther than this they do not fix a definite period: the law is not exact as to a few days. Nine calendar months contain only 275 days, and only 273 or 272 if February be included. To fix bastardy on a child in Scotland, absence must continue till within six months of the birth, and a child born after the tenth month is accounted illegitimate.
"The difficulty of determining the precise time when impregnation takes place in the human subject, renders it almost impossible, in any case, to calculate with absolute certainty the duration of pregnancy. We are, however, in possession of a sufficient number of observations to establish the fact that the ordinary period is about forty weeks, or 280 days; but it is certain that it does occasionally exceed or fall short of this period by several days. As we can never be certain of the precise day, between the periods of menstruation, when conception occurs—whether it takes place immediately after the last period, or before the expected period, or midway between these—it is obvious that all calculations founded upon the cessation of the catamenia must be extremely uncertain. The error of the calculation will be still greater if the catamenia should have appeared, or a discharge like the catamenia should have occurred once or twice after conception. Impregnation most frequently takes place soon after menstruation, but in others it does not happen till a few days before the expected period; so that two[139] women may have menstruated at the same time, and one may have reached the full period three weeks before the other; and to this extent, or nearly so, an opinion founded on the disappearance of the catamenia may be erroneous.
"Calculations of the duration of pregnancy, founded upon what has been observed to occur after casual intercourse, or perhaps a single act, in individuals who can have no motive to tell us what is false, are likely to be much more correct; and the conclusion to be drawn from these is, that labor usually, but not invariably, comes on about 280 days after conception, a mature child being sometimes born before the expiration of forty weeks, and at other times not until the forty weeks have been exceeded by several days. A case came under my observation very lately, in which I had no doubt the pregnancy existed 287 days: the labor did not take place till 287 days had elapsed from the departure of the husband of this lady for the East Indies. Some women are always delivered before the end of the forty weeks, according to the usual calculation, and their children are mature.
"In the evidence given on the Gardner Peerage cause, the period of utero-gestation was limited, but not strictly, by some of the witnesses, to forty weeks, or 280 days; by others it was extended to 311 days. Dr. Merriman, whose opinion is always entitled to much respect, thinks the greatest number of women complete gestation in the 40th week, and next to that in the 41st. Of 114 pregnancies, calculated by him from the last day of menstruation, and in which the children appeared to be mature, 3 deliveries took place at the end of the 37th week; 13 in the 38th; 14 in the 39th; 33 in the 40th; 22 in the 41st;[140] 15 in the 42d; 10 in the 43d; and 4 in the 44th week.
"How long before the expiration of the 40 weeks a child may be born with the power of supporting life has not been determined. Where I have induced premature labor for distortion of the pelvis before the end of the seventh calendar month from the last menstruation, I have never seen a child reared. The lady of the clergyman in Fife, whose case has lately given rise to so much discussion, was delivered 175 days after marriage, and the child lived five months. To what extent gestation may be protracted in some cases beyond the 280 days it is very difficult to determine, and the opinions of the most eminent writers differ upon the subject. I should suspect some great error in the calculation where the period of gestation exceeded 300 days. But the experiments made on the lower animals prove that there exists in them a great variation between the shortest and the longest gestation; and it is difficult to comprehend why there should be a difference in this respect in the human species."
In a trial which took place in this country, in the county of Lancaster, Pa., as reported in the Medical Examiner for June, 1846, it was decided that Gestation may be prolonged to three hundred and thirteen days! The female swore that conception must have taken place on the twenty-third of March, 1845, and the child was not born till the thirtieth of January, 1846, or over eleven months. The judge directed the jury to return a verdict in her favor, and I suppose this case establishes a precedent for America.
In a recent number of the Medical Gazette, I find a case reported wherein the period was said to be[141] prolonged still farther. A man left his wife in New South Wales, he coming to England, and twelve months after he left she was delivered of a child, which she claimed to be legitimate. He denied this however, and the judge in the Consistory Court decided, without hesitation, in his favor. Taking the medium between these two cases therefore, it appears to be decided that the extreme limits is somewhere between eleven and twelve months! It must be recollected however, that both were perfectly arbitrary, and that, for anything known positively on the subject, both may be either right or wrong.
Except when labor is brought on prematurely by violence, it always commences at what would have been one of the monthly periods; or in other words, after a certain number of full months, and never at any time between! If therefore a female passes over the ninth month, she will probably go to the tenth. This has been proved by extensive observation, and is only another proof of the regular method in which nature conducts all her operations. The same law is also observed in abortions, which generally take place at one of the months, unless brought on suddenly by violence.
The precise period when the child can live, if brought into the world, is not determined, any more than the time it may remain in the Womb. Some children may be able to live a considerable time before the full period of Gestation, and others may not till some time after, there being a great difference in regard to their development.
One may be as fully developed at six, as another at seven months. The common opinion is that the child cannot live if born before seven months. This, however, is incorrect. Many instances have been known of births at six months, and even earlier, in which the child lived, and became strong and healthy. Van Swieten mentions the case of one Fortunio Liceti, who was born before the sixth month. He was not larger than the hand, but grew to the average size, and lived to be seventy-one years old. Dr. Gunning Bedford mentions a similar case, in his translation of Chailly's Midwifery. There are even cases mentioned of children living at five months, but it must be borne in mind that it is seldom possible to determine the exact period. As a general rule however, the child does not live till after the seventh month, though there undoubtedly have been cases where it has lived before the end of the sixth month. The law adopts the medium period, and declares the child capable of living at the end of the sixth month, and not before. There is no reason whatever for supposing that it is less likely to live at eight months than at seven, or that it will not live at all at eight months, as some do.
THE FORM, SIZE, AND POSITION OF THE FŒTUS, AND ITS APPENDAGES, AT FULL TERM.
FORM AND SIZE OF THE FŒTUS AT FULL TERM.
The average length of the Fœtus, at full term, is about twelve inches from the head to the breech, and about eighteen inches from the head to the feet. Its weight varies from five to eight pounds, perhaps averaging about six, though some have been born weighing only three pounds, or less, and some even as high as twelve. The breadth across the shoulders is about four inches, and the same across the hips, but both are so easily compressed that during delivery they only measure about three inches, or three and a half at most.
The head is the most important part, because it is the largest, and usually present first. It is therefore necessary to describe it fully, and with special reference to its importance, in the early stages of labor, as the part by which the position is usually determined.
PLATE XXIV.
The head is generally divided into the Cranium, or that part which contains the brain, and the Face.
The Bones of the Cranium.—These are seven in number, viz., two Frontal Bones, or those forming the forehead; 1, 1, Figs. 1 and 2, (Plate XXIV.)—Two Parietal bones, or those forming the sides of the head; 2, 2, Figs. 1 and 2.—The Occipital bone, or that forming the back of the head; 3, 3, Figs. 1 and 2.—And two Temporal bones, which lie over and between the ear and the eye; 4, Fig. 2.
The Bones of the Face.—These are five in number, viz., two Superior Maxillary, or upper jaw bones; 5, Fig. 2.—Two Malar, or cheek bones; 6, Fig. 2.—And one Inferior Maxillary, or lower jaw bone; 7, Fig. 2.
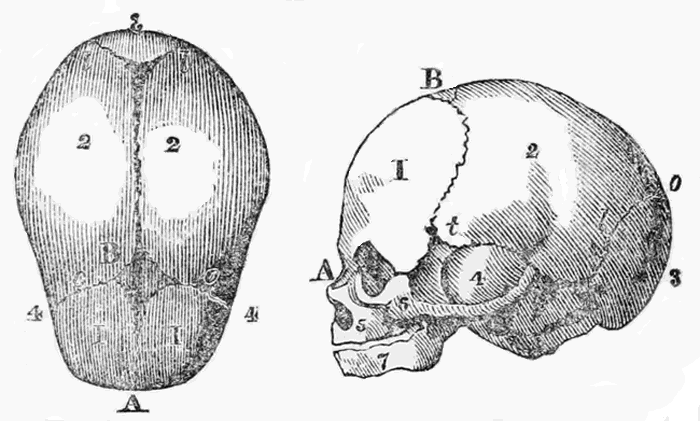
the fœtal head.
Plate XXIV.
The head is generally divided into the Cranium, or that part which contains the brain, and the Face.
The bones of the cranium are not closed together, as they are in the adult, but are separated to a considerable distance, in certain parts, and connected by a strong membrane. These membranous spaces are called Sutures and Fontanelles, and a knowledge of them is absolutely necessary, as a means of ascertaining the position of the head.
The Sutures.—The first of these spaces, which extends from the lowest part of the middle of the forehead to the occipital bone, is called the Sagittal Suture, or antero posterior Suture: A, B, C, Figs. 1 and 2. It separates the two frontal, and the two parietal bones. The spaces between the two frontal and the two parietal bones are called the Frontal Parietal Sutures, o. o. Fig. 1; and those between the two parietal bones and the occipital, l. l. Figs. 1 and 2, are called the Lambdoidal Sutures.
The Fontanelles.—When the different Sutures meet at a point, the membranous space is greater than at other parts, and is called a Fontanelle. Thus when the two Frontal Parietal Sutures meet the Sagittal Suture, at B, Figs. 1 and 2, there is quite a large diamond shaped space between the different bones, filled up with membrane. This is called the Anterior Fontanelle, or bregma. Where the Sagittal Suture joins the two Lambdoidal there is another space, not so large, and different in shape, being triangular; this is called the Posterior Fontanelle, c. Figs. 1 and 2. And where each of the temporal bones joins the parietal there are two other spaces, called the Temporal Fontanelles, t. Fig. 2, which are also irregularly diamond shaped, but not nearly so large as the anterior fontanelle.
It is evident that if a person can distinguish these Fontanelles, when he touches them with his finger, he[150] can tell what part of the head is presenting, and hence their use.
These spaces allow of the bones lapping over each other, during delivery, and thus the head is made smaller. They do not disappear till sometime after birth, and in very young children the brain may be felt, and seen to work, at the anterior fontanelle. Eventually however, the bones come close together, and are joined by a curious kind of dovetailing. The two frontal bones however, completely coalesce, and form but one, in the adult.
Sometimes the bones will be very perfectly formed, and the fontanelles nearly filled up, before birth, and then the head cannot be crushed much smaller, and so the labor becomes both painful and difficult. This is usually called an ossified, or solid head.
Diameters of the Head.—The diameters of the head are the distances between its most prominent points. They are necessary to be known before we can judge as to the possibility of its passing the straits of the Pelvis, in the various positions.
Generally there are reckoned ten diameters, and they are represented in the following Plate:—
PLATE XXV.
Diameters of the Head.
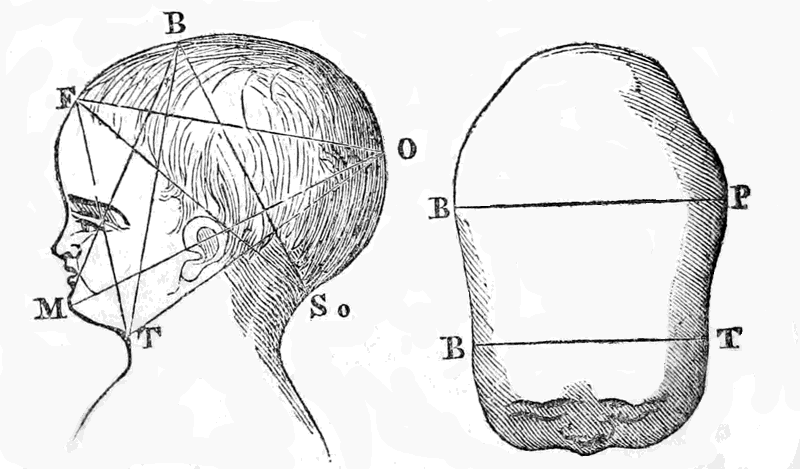
1. The Occipito Mental, or from the back of the head to the chin, M, O, Fig. 1, five inches.
2. The Mento Bregmatic, or from the chin to the anterior fontanelle at the top of the head, M, O, Fig. 1, four inches.
3. The Occipito Frontal, or from the back of the head to the top of the forehead, O, F, Fig. 1, four inches.
4. The Trachelo Occipital, or from the throat to the back of the head, T, O, Fig. 1, four inches.
5. The Sub Occipito Bregmatic, or from the nape of the neck to the top of the head, S, B, Fig. 1, three inches and a half.
6. The Trachelo Bregmatic, or from the top of the throat to the top of the head, T, B, Fig. 1, about three inches and a half.
7. The Trachelo Frontal, or from the top of the throat to the top of the forehead, T, F, Fig. 1, about three inches.
8. The Sub Occipito Frontal, or from the nape of the neck to the top of the forehead, S, F, Fig. 1, about three inches.
9. The Bi Parietal, or across the head from one side to the other at the middle of the parietal bones, the widest part, B, P, Fig. 2, three inches and a quarter to three and a half.
10. The Bi Temporal, or across the head from one temporal bone to the other, B, T, Fig. 2, about two inches and a half.
The necessity for knowing these diameters will be obvious. It is only by being acquainted with them, and with the straits of the Pelvis, already described, that we can tell whether the child can pass or not in certain positions, and how we must change its position, when possible, to give relief.
On comparing the diameters of the head with those of the Pelvis, it will be seen that some of them correspond in size while others do not, so that in one position delivery can take place spontaneously, while in another it will be difficult, and in some nearly impossible, without assistance. Thus, for instance, if the head should present by the occipito mental diameter, (O, M, Fig. 1,) it evidently could not pass while in that position, because by this diameter it is five inches in width, and the greatest diameter of the Pelvis is only about four inches and a half. Its position must therefore be changed, and the accoucheur must know how to change it with advantage.
The attitude of the Fœtus is represented in the following Plate:—
PLATE XXVI.
Attitude of the Fœtus.
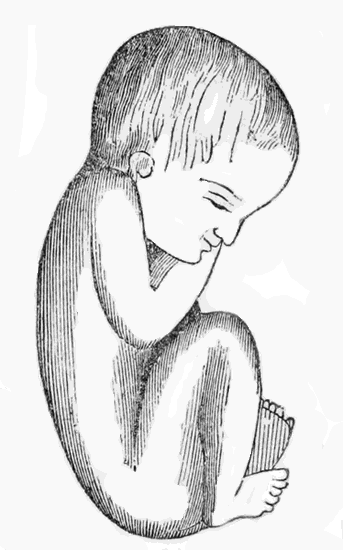
The arms, it will be seen, are crossed on the breast, upon which the chin is also bent; the thighs are close together, and brought against the Abdomen; the legs are close bent on the Thighs, and the feet are turned up against the front of the legs, the whole body being curved forward.
The position in which the Fœtus most usually lies in the Womb has already been shown, particularly in Plate XII, and in Plate XVI. The head is downwards, and the back part of it turned to the mother's left side. What is the cause of this almost universal position is not certainly known. It was formerly thought to depend on the head being heavier than the other parts, and thus sinking down; but this[154] supposition has been shown to be entirely without foundation. M. P. Dubois has lately advanced the notion that it depends on an instinctive feeling in the Fœtus itself, which directs it to take that position by which it can most easily make its exit. This opinion appears very reasonable, and is apparently well founded. It is well known that the Fœtus is susceptible of various impressions while in the Womb, and impelled by unerring instinct to take the breast immediately it is born; nay, it has even been known to suck the finger of the assistant, in cases of face presentation, even before birth! We can readily believe, therefore, that it is directed to place itself in the Womb, in the best position, the same as it is directed to take the finger in its mouth.
In the young of many of the lower animals this is also strikingly exemplified. The young duck in the shell taps with its little beak against the part that is to be broken, and rushes into the water even with a part of the shell still on its back. The young oppossums, who are born imperfect from the Womb, shelter themselves, immediately they come into the world, in the pouch on the mother's breast, and fasten themselves to the mammæ till they are more perfectly grown.
It must be remarked however, that the head does not always present first, though it usually does so. Occasionally we have the breech present, and still rarer even other parts; but these are merely exceptional deviations, the causes of which are unknown. Out of every sixteen children born, fifteen usually come head first. This however, will be shown better further on.
The uses and arrangements of the membranes surrounding the Fœtus have already been explained, so that little more is needed to be said here, because they are not much different at the full term from what they are at an earlier period, excepting perhaps that the amnion is a little more dense and firm. This membrane appears not only to surround the Fœtus like a bag, to contain the waters, but is also reflected close on to its body, like its skin, with which in fact it is thought by some to be connected. The child is certainly born with this membrane still on its body, and does not part with it till some days after birth, when it peels off like a thin dead skin, or powder.
The waters, enclosed within the Amnion, (see Plate XII,) have now increased to their greatest quantity; and there is also, in most cases, a second body of fluid between the Amnion and the Chorion, which coming away before the real discharge, is called the false waters.—(See Plate XII.)
The quantity of the true waters, at birth, is about twenty, or from that to thirty ounces, but is very variable. It is of a greenish color, rather muddy, and heavier than water. It contains albumen, (white of egg,) sulphate of soda, and lime. Ninety-eight per cent. of it however, is pure water. It appears to be excreted, like perspiration, from the surface of[156] the membranes, and most likely is merely the watery portion of the blood exuded through. The uses of this fluid are various. As already stated, it probably supplies some nutriment to the fœtus, which it also protects, in a great measure, from pressure and from concussions. It also prevents the limbs from adhering, and helps to distend the mouth of the Womb, in the earlier stages of labor, besides affording an abundant slippery fluid for the purpose of lubricating the passages, thus making the passage of the child more easy.—(See Plate XII.)
The other two membranes, the Chorion and Decidua, are not of much importance in our present explanation; and practically, in fact, the whole three may be regarded as one envelope, surrounding the child and the waters in which it floats.
At the full term the Placenta, (See Plate XII,) is about six or seven inches in diameter, and nearly circular, though often irregular. Its thickness varies from one to two inches, and is greatest where the cord is inserted. Sometimes it is very large, or very thick, and may then be difficult to extract, and even cause serious accidents.
As already explained the Placenta is composed of a mass of blood-vessels, by means of which the blood of the fœtus is, in some way, brought into contact, or commingled with that of the mother. Its uterine face is irregular, being broken into lobes, or cotyledons, on which may be seen a vast number of little veins and arteries, corresponding with others on the inner surface of the Womb. Its outer surface is of a grey red color, and covered with the fœtal membranes,[157] under which the large blood-vessels can be traced. The Placenta is usually attached to one side of the Uterus, near the fundus, or at the fundus, but sometimes it grows wholly, or in part, over the mouth of the Womb; an occurrence which may cause serious consequences.
When there is more than one child each usually has a separate placenta, and they are all intimately connected. In some rare cases however, one placenta only exists with twins. Each child has also a separate amnion, and waters; but there may be only one chorion and decidua for the whole, or each may have a complete set of membranes itself. Instances have been known however, of two children being enclosed in the same amnion, and surrounded by the same waters, having but one placenta between them.
These possible diversities show the accoucheur how necessary it is for him, in any case of multiple pregnancy, to be sure that he has abstracted all the after birth; and they also caution him not to proceed to unnecessary manipulations merely because it is not the same as in other cases.
This is composed, as already stated, of an artery and two veins, which twist round the artery, like the strands of a rope. These are all enclosed in a sheath, and surrounded by a thick kind of mucus, called the Gelatine of Wharton. Its thickness is about that of the little finger, though it may be much larger, having been seen as thick as the child's body. Its usual length is about eighteen or twenty inches, but it has measured as much as five feet. Then again it has been found so small that the vessels in it[158] could not nourish the child. These exceptional variations however, are very rare. The veins may also be enlarged, or full of knots, and the circulation may be so much impeded thereby as to cause abortion. The various accidents which may result from anomalies in the cord will however, engage our attention in another place.
THE MECHANISM OF DELIVERY IN ALL THE DIFFERENT PRESENTATIONS AND POSITIONS OF THE FŒTUS.
PRESENTATIONS AND POSITIONS OF THE FŒTUS.
The child may present several different parts of its body, at the commencement of delivery, and they may be in different positions relatively to the different parts of the Pelvis. All these require to be known.
Different authors have made different classifications of the presentations and positions, and have differently named them; but this is of little consequence, since they are still the same, no matter how they are named. I shall follow the arrangement of M. Chailly, because I think it equally perfect, and much more simple and practical, than any other yet proposed.
The fœtus may present at the mouth of the Womb either by the head, the most usual way—by the lower extremities, which is the most frequent way after the head—or by various parts of the trunk, which is the least frequent way of all.
In each of these three full presentations there may be certain variations, which require to be noticed. The head, for instance, may present either by the cranium or by the face; the lower part of the body may present either by the feet, the knees, or the breech, according as the legs and thighs are flexed or extended; and the trunk may present either on the right or left side, and inclined towards the back or[161] towards the chest, though neither the back nor abdomen ever fully present.
Each of these variations may also have slight variations again. Thus the face may present full, or by one or the other cheek, and so on. These variations however, are of little practical consequence, because we only find them at the very commencement of the labor, and they always change to the full presentation.
Practically speaking therefore, there are five full presentations, viz., the Cranium, the Face, the Breech, the Feet, or knees, and the Trunk, either by the right or left side.
The varieties of these, as already remarked, not requiring any special attention from the accoucheur, providing he is not puzzled or misled by them.
The position means the particular direction in which the presenting part of the Fœtus is placed in relation to the Pelvic straits. The Pelvis itself is supposed to be divided into two similar halves, the right and the left, and each presenting part has one particular place which is referred to as the indicating point. Thus, for instance, in the Cranium the Occipit, or behind part of the head, is the indicating point; and we therefore say, in Cranium presentations, that it is a right or left Occipital position, according as the back of the head is to the right or left side of the Pelvis. In face presentations, the chin (mentor) is the indicating point, and we therefore say it is a right or left mento position, according as the chin is towards the right or left side. In breech presentations, the child's sacrum is the indicating[162] point, and we then say it is a right or left sacral position, according as the Sacrum is towards the right or left side of the Pelvis. In trunk presentations, which are always crosswise, the head (cephalo) is the indicating point, and we therefore say it is a right or left cephalo position, according as the head lies towards the right or left side of the mother's body.
In Cranium presentations also, the back of the head is not merely on the right or left side, but may be at two different points on each side. It may be either nearest to the Sacrum (posterior), or nearest to the pubes (anterior), but still against the Ilium; it is therefore called a right or left anterior, or posterior, occipito iliac position, as the case may be. Sometimes also, the occiput lodges immediately on the pubis, instead of going to either side, and that is called an occipito pubic position; at other times, on the contrary, it is placed against the Sacrum, instead of being on either side, and that is called an occipito sacral position.
In presentations of the head therefore, we may reckon six positions—the right and left anterior and posterior occipito iliac, and the pubic and sacral.
In presentations of the face the same; they being mento iliac and so on, instead of occipito.
In presentations of the lower extremities also the same, excepting that they are sacro iliac and so on, instead of occipito.
In presentations of the trunk we have but two positions for each side, the right and left cephalo iliac; according as the head is on the right or left side of the mother's body. The child always lying, in presentations of the trunk, crosswise—the feet on one side and the head on the other.
Most authors enumerate many more presentations and positions, but they are of little practical utility. When the head presents, for instance, the delivery takes place in nearly the same manner, let it be in what position it may. And in presentations of the face, or of the lower extremities, the particular position is of little consequence, the delivery being usually effected much the same in them all. Some of the positions are, it is true, much more favorable than others, but a spontaneous delivery, generally speaking, occurs in all of them, when the head, face, or lower extremities presents. Very frequently indeed, the less favorable positions are changed to the more favorable ones, and the worst seldom do more than impede delivery for a time, unless there be some malformation, or loss of power. I therefore refer to them more for convenience in future explanations, and to enable my readers to know what is meant by them, when they read other books; not because they are really necessary to be understood, or of any great practical use.
The celebrated Baudelocque admitted seventy-four positions, and twenty-two presentations; and the number might be made still greater, if all the variations were to be enumerated. Such classifications however, are more ingenious than useful, and they are but little noticed even by medical men.
I shall merely describe the mechanism of labor in the most frequent positions, in each presentation, because the others usually change into these; and even when they do not, the process of delivery is essentially the same, and also the mode of assisting it.
The Presentation.—Although in general it is not possible to ascertain with certainty, what part of the fœtus presents to the mouth of the Womb, until labor commences, yet a tolerable judgment can frequently be formed before. In head presentations, on performing ballotment, the head is felt, like a firm round tumor, occupying all the space which the finger can reach, very differently from any other part. The peculiar cramps in the female's lower limbs, and frequent inclination to urinate, mentioned in the signs of labor, are also strong indications of this presentation, being seldom experienced in any other. When the labor has actually commenced there can be but little uncertainty in these cases, for, immediately the mouth of the Womb is sufficiently open, the finger can be introduced, and the head felt like a smooth, round, and elastic bony tumor, not likely to be mistaken for anything else, if ordinary care be taken. After the waters have escaped, it can of course be felt still more distinctly. If even an inexperienced person bears in mind the shape of the head, and reflects how it must fill up the passage, and how it must feel, from being composed of separated thin bony plates, lying on a soft yielding substance like the brain, he can scarcely fail to recognize it. The sensation is very much like that of pressing a piece of firm card board on an inflated bladder, which forms a tolerable representative of the fœtal head. Sometimes there is a difficulty from a great quantity of water being intruded between the membranes and the head, which somewhat obscures the touch, but this only necessitates greater care. The[165] water however, may be in such quantity as to entirely prevent the touch, in which case nothing can be done till the membranes break; the presentation can then be ascertained with certainty, and it will be quite early enough to render assistance, if it should be an unfavorable one. I have known some inexperienced persons mistake the bag of water itself for the head, and commit great errors in consequence.
The Face can seldom be mistaken, because the nose, or mouth, may be felt; and, by passing the finger up the side of the head, the ears also.
The trunk is in general easy of recognition. Nearly always the right or left shoulder occupies the passage, or is near to it, so that the finger may be readily passed under the arm pit. The shoulder joints, the ribs, or the shoulder blade bone, all feel very different to the head, and are not likely to be taken for it.
In presentations of the lower extremities there is still less danger of error. If the feet, or knees, occupy the passage, they can scarcely be mistaken. The breech is certainly something like the head in its form, but feels different, and is divided down the middle by the indentation between the two cheeks, along which the finger can be passed till it enters between the limbs.
In irregular presentations, as of the arms for instance, or of one leg, or an arm and leg, it is only necessary to carefully feel them, so as to ascertain their form, and the relation of their parts. Thus the fingers can be distinguished from the toes, and the feet from the hands, particularly if the ankle can be felt.
The accoucheur should ascertain the particular presentation as early as possible, because he may[166] sometimes be of service in correcting an unfavorable one, if he is certain of it in time, and knows what he is about. He should not however, use any degree of force to ascertain it, in case he cannot do so without, but wait till the conditions are more favorable. Neither should he, with the same object, rupture the membranes too soon, for he may thereby cause considerable delay and difficulty, without any good to counterbalance it.
All the above-named presentations may, and usually do, terminate spontaneously, except those of the trunk, and even they do occasionally, though more frequently they require assistance.
Relative frequency of the different presentations.—The most favorable presentations, and positions also, are always the most frequent, while the unfavorable ones are but seldom met with. According to Madame Lachapelle, in fifteen thousand six hundred and fifty-two labors there are about fourteen thousand seven hundred and forty-nine presentations of the head and face; about five hundred and eighty-six of the breech, knees, and feet; and only about sixty-eight of the trunk, or shoulders.
Positions.—The position is generally of but little consequence, because in all the favorable presentations spontaneous delivery occurs in every position alike, and in the unfavorable presentations the same assistance is required in one position as in another. In some cases an unfavorable position of the head may be changed however, to a better one; and therefore, so far as the head is concerned, the positions are worth ascertaining.
The mode of determining the position is by feeling for the sutures and fontanelles, described in Chapter VIII; and this cannot be usually done till after the[167] membranes are broken, when the head can be distinctly touched. By referring to Plate XXIV, the shape and position of the Fontanelles will be seen, and if the head be supposed placed with the top downwards, and the back of it to the mother's left side, they may be readily found with the finger.
In the left anterior occipito iliac position, or that when the back of the child's head is against the left side of the mother's pelvis, and nearest the pubes, while its forehead is against the right side, and nearest the sacrum,—the sagittal suture, or opening along the top, will of course run across from right to left. This opening may be distinctly felt with the finger, which should be passed along it towards the right side, and it will then reach the anterior fontanelle; afterwards it should also be passed to the left side, and then it will reach the posterior fontanelle. The difference between these two openings, in shape and size, is shown in Plate XXIV, and even if a person has never seen, or felt, the head of a newborn child, they can scarcely be taken for each other, after noticing that Plate.
If the anterior fontanelle should be felt on the left side instead of the right, and near the pubes, while the posterior fontanelles is to the right, and near the sacrum, the position must be the right posterior occipito iliac, or just the reverse of the former.
If the sagittal suture should be found to run across from the pubes to the sacrum, instead of from one side to the other, it will then indicate either an occipito pubic, or occipito sacral position, according as the back of the head is behind or before; and this can be readily ascertained by finding either of the fontanelles.
In short, if the relative position, forms, and directions[168] of these openings in the child's head be clearly understood, the position of the head can nearly always be determined by feeling them, as will be evident by referring to our former explanation of them.
Sometimes however, the bones overlap a good deal, from the head being pressed, and then instead of an opening along the top, a seam will be felt. And sometimes, from long continued pressure, a quantity of blood, and watery fluid, will be effused under the scalp, so as to prevent the bone being distinctly touched. But these accidents seldom happen, and with ordinary care and perseverance, need not prevent the position being determined, after a little delay.
The position of other presenting parts is easily ascertained, by feeling for some known point—as the nose, or the face, the depression between the cheeks, or the breech, and so on.
Relative frequency of the different positions.—The most favorable positions, like the most favorable presentations, are also the most frequent. According to Baudelocque, in ten thousand three hundred and twenty-two cases, of head presentation, there were eight thousand five hundred and twenty-two cases when the back of the child's head was on the mother's left side, and towards the front, (or in the left anterior occipito iliac position); one thousand seven hundred and fifty-four when it was on the right side towards the front, (right anterior occipito iliac); twenty-five times to the right side, but towards the Sacrum, (right posterior occipito iliac); and nineteen times on the left, but towards the Sacrum, (left posterior occipito iliac.) Being most frequently with the back of the head towards the front on the left side, as shown in Plate XXVII; next towards the front on the right[169] side; and but seldom towards the Sacrum, or back, on either side. In all these ten thousand cases we do not find a single instance of the head lying from back to front, in the occipito pubic, or occipito sacral positions, commonly called transverse; neither do we find a single instance in fifteen thousand six hundred and fifty-two cases recorded by Madame Lachapelle; which will show how rare such unfortunate positions must be. What this great frequency of one particular position depends upon we do not know—possibly on that cause, previously alluded to, which determines the most frequent presentation.
In the next Chapter, the mechanism of delivery, or the manner in which the child escapes out of the body, as it most frequently occurs, will be fully explained.
This is the presentation and position most frequently observed, perhaps fifteen out of sixteen times. In most Obstetrical works it is called the first position.
By observing the following Plates, and referring to the previous explanations of the diameters of the Pelvis, and fœtal head, in Plates IX and XXV, it will be seen that through all its changes of position, while making its exit, the head always presents by one of its shortest diameters to one of the largest diameters of the Pelvis, so that the relation between them is invariably the best that could be established; and many peculiar turnings and revolutions occur, apparently for the express purpose of bringing this about.
Before the rupture of the membranes the head presents its occipito frontal diameter, which measures four inches, to the right oblique diameter of the Pelvis, which measures four inches and a half; while its bi-parietal diameter, which measures only about three inches and a half, is presented to the other oblique diameter, also measuring four and a half—(See Plate XIX.) Even here it will be seen that the passage is larger than the head which has to pass through it, but a more favorable position still can be obtained, by a slight movement of the Fœtus, which[171] nature accordingly accomplishes, and also follows by others, to preserve the advantage, which will next be described.
Movements of the Fœtal Head.—There are three of these peculiar movements, each of which takes place at a particular period of the labor, and must be described separately.
First movement, flexion, and descent.—Immediately after the Membranes are broken, the contractions of the Uterus force the head into the upper strait, by the occipito frontal diameter of four inches, as already shown; but then commences the first movement, which consists in a bending of the child's chin down upon its breast, so that the forehead is carried up into the Womb; and the most prominent point of the back of the head presents to the middle of the passage, by the occipito bregmatic diameter, which is only about three inches instead of four. This of course makes the passage so much easier, and generally, immediately after this change, the head descends into the basin of the Pelvis.
It is not absolutely necessary however, for this movement to occur, for in a well formed Pelvis the head can descend without it, though not so easily; and sometimes, in fact, it does not take place, but this is unusual.
It must be recollected that this shifting of the head alters the position of the fontanelles—the posterior one being brought more to the centre of the strait, and the anterior one carried up out of reach, while previous to the movement they were both on a level. If an examination is not made therefore, till after this change, it may be difficult to determine the position, unless this is borne in mind. The following Plates show this very well.
PLATE XXVII.
It will be seen here that the neck is straightened out, and that the two fontanelles are on a line with each other.
Note.—The front of the bones are represented in this and the two following Plates, as if transparent, so that the head may be seen through them.
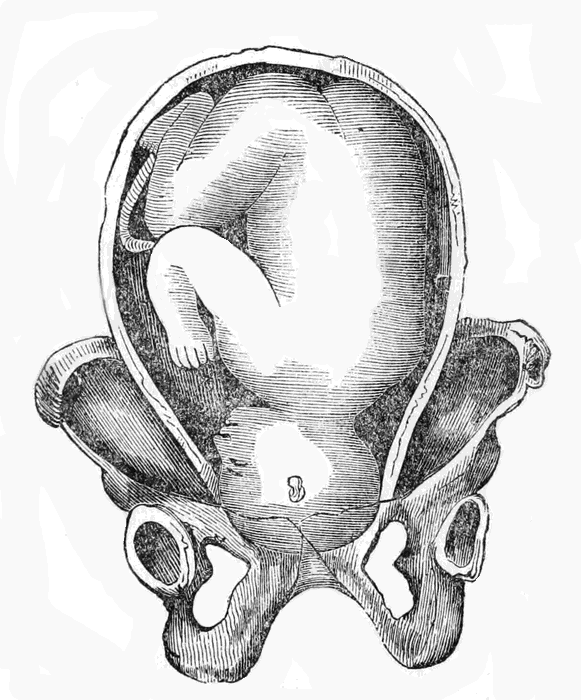
Plate XXVII.
This Plate represents the head just entering the upper Strait.
PLATE XXVIII.
At this time the anterior fontanelle can scarcely be reached, but the posterior one is easily to be reached, being in the open passage, on the left side. The head is now fairly within the Pelvic cavity, but still lies across from right to left.
Second Movement, Rotation of the Head.—When the Fœtus is thus brought to the bottom of the Pelvis, its head turns completely round, the back of it being brought to the front, or under the pubes of the mother, and its forehead turned against her Sacrum, as represented in Plate XXIX.
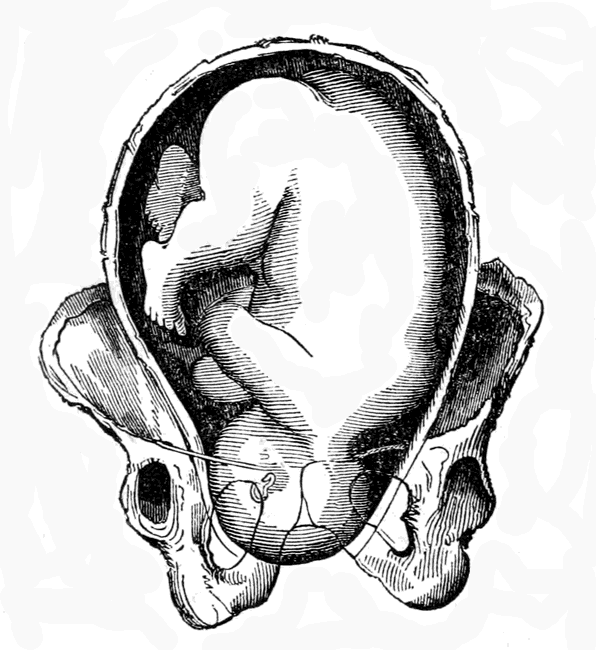
Plate XXVIII.
This Plate represents the head descended still lower in the Pelvis.
PLATE XXIX.
Here the head is seen just beginning to turn—the right side, and part of the back of it, just passing under the pubes. As the rotation becomes complete the neck straightens, so that the two fontanelles are again found on the same level. Finally the back of the head fully emerges from under the pubic arch, and the chin slides gradually out after it beneath, so that the neck of the child is encircled by the ring of the Vulva.
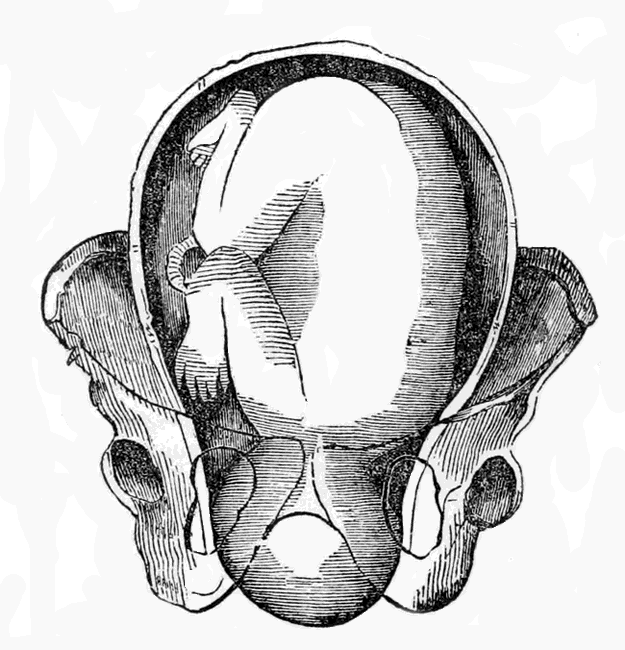
Plate XXIX.
This Plate represents the head still further down, and beginning to Rotate.
PLATE XXX.
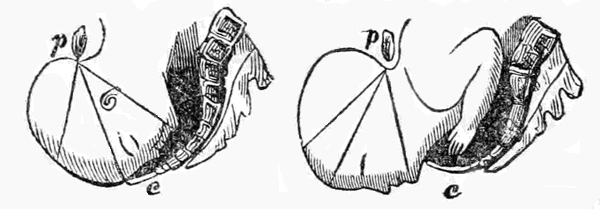
In Fig. 1, the back of the head is nearly under the pubic bone, while the forehead is just passing the external opening below.
In Fig. 2, the back of the head is completely extruded, and also the chin, so that the whole head is now born.—(p. is the pubic bone, in front.)
In Fig. 1 it will be seen how the Os Coccygis, or lowest part of the back bone, (c,) is straitened out, backward, while the head is passing, as I explained before; and in Fig. 2 it has returned again to its natural position.
The reason for this rotation of the head will be obvious on calling to mind the form of the Pelvis and the external opening. On examining Plates IX and X, it will be seen that the longest diameter of the Vulva, or external opening, the antero posterior, is nearly at right angles to the longest diameters of the upper strait, the oblique. Now the longest diameter of the head is adapted to this oblique diameter, on entering the upper strait, as already explained, and it is necessary for it also to be adapted to the longest diameter of the external opening, the anterior posterior when making its exit; but as the two are not parallel the head is compelled to turn, or rotate, in order to pass from one to the other. To accomplish[184] this however, the neck has to be twisted considerably. But when the head is fully delivered, it is immediately straitened again, by the back of the head turning towards the mother's left side, so that its proper relations with the trunk is re-established.
Third Movement, Rotation of the Shoulders.—When the head is delivered the shoulders come next, which also require to turn round a little, to adjust themselves to the long diameter of the lower strait; and as they turn within the Pelvis the head also turns, to correspond, and thus the back of it is brought opposite the middle of the mother's left thigh. Immediately this movement is effected, the shoulders rapidly escape through the external opening, the right one being in front, a little to the left of the symphysis pubes, and the left one behind, a little to the right of the os coccygis. The body then curves upwards, to accommodate itself to the curved axis of the Pelvis, and speedily follows the shoulders.
These curious movements cause the child to pass in a spiral direction, so that each part may pass through the Pelvis in the most favorable position. Sometimes all these movements are not effected, and yet the delivery may occur, though not so speedily, or safely, as when they are. The shoulders do not always fully rotate, but may nevertheless pass the opening, if the parts be large, and well relaxed. It is questionable however, if the head can ever pass the lower strait without rotating, when it enters the Pelvis diagonally, the occipit on one side and the forehead on the other; as it is necessary for either one or the other of these parts to pass under the pubes.
The right posterior occipital position.—This position, called the second by some authors, and the fourth by others, is exactly the reverse of the one just described, the head lying in the same direction, but the back of it being behind, to the right of the Sacrum, and the forehead to the left of the pubes.
Precisely the same movements are gone through in this position as in the other, excepting that the head has to rotate considerably further. In the former position the back of the head is only a little to the left of the pubis, and therefore has not far to turn to pass under it; but in this position the back of the head is behind, and therefore has to turn very far round to reach the same position. The rotation is therefore more difficult, not so soon effected, and sometimes likely to be dangerous to the child.
In the other movements there are no difference worthy of notice, but it must be borne in mind that they all occur the reverse way, to what they do in the first position, because the occiput is on the right side instead of the left.
The right anterior occipital position.—This position is precisely the same as the first, but on the other side. The back of the head is in front, but to the right of the pubis instead of the left, while the forehead is behind, to the left of the Sacrum. This will be apparent enough by observing Plate XXXI.
PLATE XXXI.
This is the second most frequent position; the left anterior occipito iliac being the most frequent.
a. The Acetabulum, or socket of the hip joint.
c. The cut edge of the Womb.
c. The Foramen Ovale.
d. The top of the ilium bone, called the crest.
h. The Symphysis Pubes.
i. The ischium.
k. k. The pubic bones.
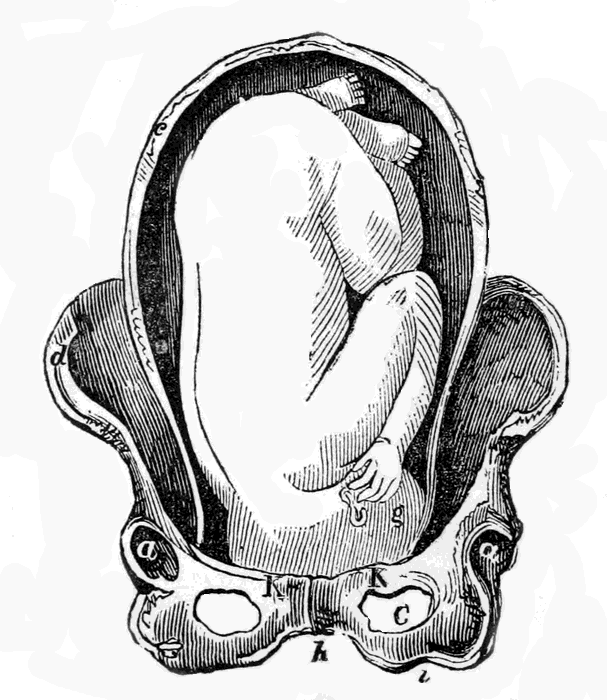
Plate XXXI.
Head in the right anterior occiput iliac position.
The mechanism of delivery is precisely the same, and all the movements occur in the same order and manner, as in the first position, but the reverse way. The rotation, for instance, being from right to left, instead of from left to right, and so of all the others.
The left posterior occipital position.—Delivery is effected the same in this as in the left anterior, or first position, excepting that the rotation is more extended, owing to the occiput being behind, as explained in the right posterior occipital position.
In all the other positions, and their varieties, there is nothing that calls for special notice, or that is material in practice, the delivery being nearly the same in them all. No matter what position the head is placed in, the back of it nearly always comes to the front, under the pubes, even though it have to turn half round to do so. The cause of this is supposed to be the peculiar form of the parts, which give it a screw like motion, in its descent, and the shape of the external opening, which, being longest from before to behind, can only allow the long diameter of the head to pass through in the same direction.
Sometimes, it is true, the occiput passes behind, instead of coming to the front, and then the chin comes under the pubes, while the occiput presses on the coccygis. This is very seldom observed, and when it occurs the labor is more difficult and tedious, though it may still terminate spontaneously.
The resistance of the soft parts, externally, appears to be the chief cause of the head turning; for when they are much relaxed, and the child's head small,[190] it will sometimes pass without, or in the anterior posterior position. And sometimes, when the head is large, so that it distends the parts very much, the shoulders will pass cross wise, there being room enough for them without turning. In some females, formed large, whose organs are excessively relaxed, and whose children are small, the delivery takes place without any of the movements being effected, the child passing straight through in whatever position it may happen to be: this is rarely seen however.
When there are twins they do not usually both present by the head, but one by the feet; and frequently the parts are so relaxed by the passage of the first, that the second is delivered without rotating at all, though in general it follows precisely the same movements. It sometimes happens however, that the second birth does not take place till some hours, or even days, after the first.
It may be said, in general, that all positions of the head are favorable to both mother and child, and may terminate spontaneously. It is seldom that anything more than ordinary assistance is required in any of them, and they could in general terminate without any at all, though sometimes with difficulty. The worst cases are those in which the head does not turn round, but remains across, or where the back of it turns behind, instead of coming to the front. In these cases there is great danger of the perineum, or external lips, being much lacerated, or even of an artificial passage being torn through the perineum, leading to the most serious after results. About one child also, out of every fifty, is lost in these unfavorable positions.
This presentation includes the feet, the knees, the breech, and also the hips, there being no difference in the delivery for all these parts. It is the same also whether there be one foot, or knee, or both feet and knees.
There are but two positions worthy of notice in this presentation, and they are determined by the child's sacrum. If the sacrum, or posteriors, are to the right of the mother's Pelvis, it is called the right sacro iliac position; but if they are on the left side it is called the left sacro iliac position. The direction in which the child's pelvis is placed, is analagous to that of the head, the sacrum answering to the occiput. Thus most frequently the sacrum is on the left side, a little to the left of the pubes, (left anterior) while the abdomen faces the right side near the sacrum. When on the right side however, it is most usually nearest the sacrum, with the abdomen facing the left side near the pubes.
The lower extremities present most frequently next after the head, but still they are but seldom met with. M. P. Dubois tells us that out of twenty thousand labors he only met with eighty-five such cases. In these eighty-five cases the breech presented fifty-four times, and the feet twenty-six, the knees being found but once.
A presentation of the lower extremities may generally be recognized at an early stage, by the head[192] being felt at the fundus of the Uterus, and by the pulsations of the fœtal heart being heard above the umbilicus, as explained in the section on Auscultation. After labor has commenced the part felt at the mouth of the Womb is irregular, and so different from the head, that it is not likely to be mistaken for it. If the knees or feet present, they can always be distinguished; and if the breech presents it can easily be recognized by its form, and particularly by the os coccygis, which can be distinctly felt at the bottom of the depression between the two cheeks. The side on which it is felt of course determines the position, and the same with the front of the knees, or the heels. The Rectum can also be reached with the finger, when the breech is touched; but great care must be taken not to intrude it too far, because with a female child the Vulva might be mistaken for it, and thus the hymen be broken, and other injury committed. The genitals of a male child are more obvious, so that the sex of the child may be usually ascertained, along with the position.
For want of proper care the breech has been mistaken for the head, and face, but this can scarcely happen if the accoucheur is attentive. It is simply necessary to call to mind what must be felt in each presentation, as the nose and mouth with the face; the two cheeks of the posteriors, with the opening between them; and also the genitals, with the breech; and it can be certainly ascertained which of these parts are really at the opening. With the knees or feet there can scarcely be a doubt.
In this position the legs and thighs are turned up[193] against the abdomen, the breech in full occupying the passage, with the sacrum to the left and in front of the mother's pelvis.
The descent of the breech usually takes place without much difficulty, into the Pelvis, it being small and easily compressed. It descends in the same direction in which it first presents—that is diagonally, like the head—and also rotates, or turns round, so that the left buttock comes in front, just to the right of the pubis, while the right one goes behind, to the left of the sacrum. The left buttock reaches the mouth of the Vulva first, in this position, and then remains stationary there while the right one slides along the curve of the sacrum and perineum, and passes out first at the lower part of the external opening. The left however, speedily follows, and when the whole breech is born it rotates again, one hip coming immediately in front, and the other going immediately behind. Owing to this movement the long diameter of the breech is adapted to the long diameter of the Pelvis, as in the case of the head. This will be evident from the following Plate:—
PLATE XXXII.
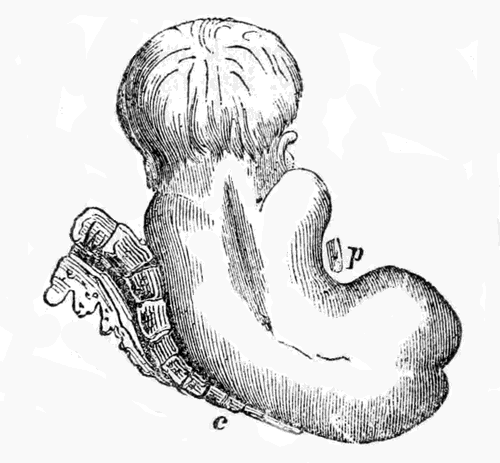
Delivery in a breech presentation, the buttocks having just passed the Vulva.
c. The Coccygis, much straightened.
p. The pubic bone, in front.
The rest of the body then rotates in the same way, and the arms and shoulders pass through the external opening in the same direction as the hips. The left shoulder first moves to the right of the pubes, while the left passes behind; and then, just when they are both passing out, one comes immediately in front, and the other immediately behind, placing themselves in the long diameter of the Vulva.
The head passes through the superior strait in the left, anterior occipital position, and is often delivered in that way; but sometimes it rotates, and the forehead passes into the curve of the sacrum, while the occiput is placed behind the pubes. When this occurs[195] the body also rotates, to accompany the head. This state of the parts is represented in the following Plate:—
PLATE XXXIII.
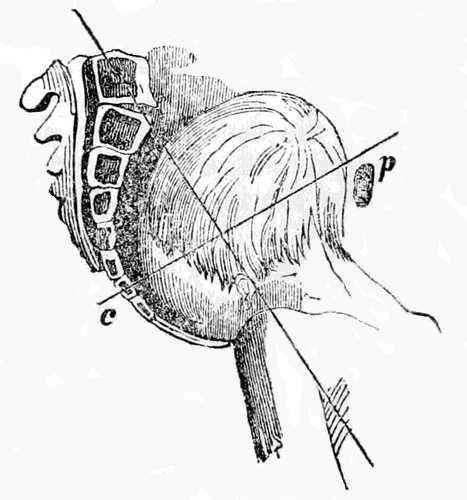
Anterior posterior position of the head, the occiput being in front, after the delivery of the body.
c. The Coccygis.
p. The pubic bone, in front.
At this period the head is passed the uterus, and there is therefore little or no contraction to expel it, so that it often remains a long time undelivered. It will be seen that the position is very unfavorable, the longest diameter of the head, the occipito frontal, being the presenting one, which makes it lie immoveably across. The means of assisting in such a case are plain enough, the forehead must be brought down while the body is raised, towards the mother's abdomen; this will throw the top of the head back, towards the sacrum, and change the presenting diameter.[196] The forehead and bregma rapidly escape below, and the occiput passes out last. This is the way in which nature herself also completes the delivery in such cases, when she has the power.
This position is the reverse of the preceding one, the Sacrum being behind, and to the right, while the Abdomen is to the left in front. The same movements are performed as in the first position, and the whole process is similar, only the reverse way. The Sacrum being behind however, has to rotate much further to come in front, precisely the same as with the head when in the posterior position.
The head generally follows the Sacrum, and the occiput comes under the pubes, as already explained; but sometimes only at the moment when being disengaged.
In this position there is no rotation at all, the back of the child being turned full to the back of the mother, and the whole body, and head, being expelled in that position. In general there is no particular difficulty from this position, but on the contrary it is thought by some to be rather favorable than otherwise. The longest diameter of the fœtal pelvis, and shoulders, are adapted to the longest diameter of the mother's pelvis, at the upper strait, and easily pass it. They will also generally pass the external opening in the same direction, unless it be very unyielding,[197] or the child very large; and if they pass the head usually follows, because the parts have been so much dilated by the passage of the body that they offer but little resistance.
As a general rule delivery by the breech, or by any other position of the lower extremities, is less favorable than by the head. The labor is usually longer, more painful, and more exhausting; still however, it is generally spontaneous, and not necessarily dangerous to the mother. To the child, on the contrary, it is dangerous, on many accounts.
It appears, from the observations of M. P. Dubois, that in this presentation one child is lost out of every twelve, while only one out of fifty is lost in head presentations! The chief cause for this greater mortality appears to be the compression of the umbilical cord, which is greater, and lasts much longer, than when the head presents, as will be evident on examining the circumstances under which delivery is effected in each case. When the head presents it passes, and also the shoulders, before the umbilicus is reached; the mother's organs are therefore much dilated, and only the smallest parts of the fœtus are left, when the cord is engaged in the passage; it cannot therefore be much compressed, nor for any long time, because the labor is then soon over. When the lower extremities present this is not the case, the smallest parts then pass before the umbilicus is reached, so that the cord has to pass along with the head and shoulders, which are both the largest and the longest in being delivered. This[198] compression of the cord stops the circulation of blood between the fœtus and the Placenta, as will be evident on referring to the description formerly given of Fœtal nutrition; and the stopping of this circulation is as fatal, to it, as stopping the breath is to an adult. When the breech presents altogether, there is not so much danger as with the feet, or knees, because it is large, and in its passage dilates the parts so much that the rest of the body, and the head, follow more quickly. There is, of course, no danger till after the hips have passed, because the cord is not reached before; but the delivery should be completed as soon after they are born as possible, for every minute's delay makes the chances for the child's life so much less.
Presentations of the face appear to result from the head being bent backwards, instead of forwards upon the chest. They are easily recognized, because the face has so many peculiar parts, as the nose and mouth, for instance, which are altogether unlike what can be felt in any other presentation. In a very early stage the forehead may be taken for the vortex, unless care be used, because it feels round and soft like it, but the mistake cannot last long.
The positions in this presentation, as formerly explained, are determined by the chin, and in practice only two are noticed—the right posterior mento iliac, and the left anterior mento iliac. In the first the chin is on the right side, near the sacrum, and in the second it is on the left side, near the pubes. These answer, it will be seen, to the two principal positions of the head itself. It is generally considered that, though the chin, like the head, may assume other positions, yet it does so in but very few cases, and these presenting no peculiarities which require special notice.
The head descends with the forehead and chin nearly on a level, and the nose occupying the middle[200] of the passage. When fairly in the cavity it rotates, the chin being brought under the pubes, while the back of the head passes into the curve of the sacrum. This is nearly always the process; no matter where the chin may be when the labor commences, it seldom fails to move under the pubes before it concludes. Occasionally it may rotate the other way, and pass into the hollow of the sacrum, while the occiput comes in front, but this is very rare.
The chin is born first, and then follows, below, the forehead, top of the head, and finally the occiput—the face turning upwards towards the mother's abdomen, as each part is successively delivered. When the head is fully born, the body rotates inside the same as in the head presentation, and the delivery concludes in precisely the same way.
PLATE XXXIV.
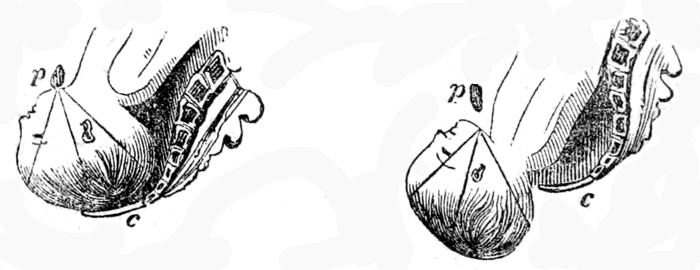
Fig. 1.—The chin just passed, in presentation of the face.
Fig. 2.—The head full born in presentation of the face.—p. The Pubic bone.—c. The Coccygis.
The delivery is precisely the same in all the other positions of the face, excepting that in some of them[201] the chin has further to rotate before it can pass under the pubes. In all cases however, it may be safely calculated that it will do so, there having been so few instances known in which it has rotated the other way, into the hollow of the sacrum, which is fortunate, for there is always more or less difficulty and danger when it does so.
Sometimes the rotation does not take place at all, but the face descends diagonally, as the head occasionally does.
On the whole presentations of the face are not particularly to be feared, as regards the mother. Some authors even consider them quite favorable, and reckon them only as varieties of the head presentation. Madame Lachapelle states as a principle, that face presentations should always be left to nature. And M. Chailly says he must admit that, in all positions of the face, the labor may terminate spontaneously, excepting when the chin passes behind, in which case it will be protracted, and most likely fatal to the child. The labor is generally a little longer, and more painful, owing to the face not being so perfectly adapted to the passage as the head is; but still it must be regarded as favorable to the mother, though assistance is oftener required than with the head. There is more or less danger to the child however, owing to the head being kept under pressure for an unusual time, which produces congestion. The neck is also forced against the pubic bone, as will be seen by Figs. 1 and 2, Plate XXXIV, and thus the jugular veins are compressed. If there be any delay, it is customary to observe the face closely, after the chin is born; and if it appears from any indications that congestion is taking place, assistance is rendered at once. The face will sometimes become[202] so tumefied, and engorged with blood, from this prolonged pressure, that it will not appear natural till several days after birth.
Probably about one child is lost in ten or twelve deliveries in these cases; and if the chin pass behind its death is almost certain.
It was formerly the practice to endeavor to turn the face upwards, when at the superior strait, and so change the presentation to one of the head. This however, is now abandoned, because the attempt is seldom successful, and does not materially improve the condition of things, besides being painful to the mother. The only extra danger with the face presenting is to the child, and this is not removed by the operation; to the mother the face is nearly as favorable as the cranium. In regard to the frequency of face presentations, we find that Madame Lachapelle met with but seventy-two cases in fifteen thousand six hundred and fifty-two deliveries.
It has already been stated that in presentations of the Trunk it is nearly always the right or left shoulder which occupies the passage. It is stated, by some authors, that they have felt the back, and abdomen, but others think they were mistaken; and most certainly such positions are extremely rare, if they actually do ever exist.
There are two presentations of the Trunk, determined by the side on which the fœtus lies, and denominated accordingly right or left lateral presentations.
Each of these presentations has two corresponding positions, determined by the side on which the child's head lies. If the head be on the mother's right side it is called the right cephalo iliac position, and if it be on the left side it is denominated the left cephalo iliac position. The mechanism of spontaneous delivery is the same in them both, and in all their varieties, and so is the mode of rendering assistance, so that a description of one will suffice.
Sometimes, when the labor has lasted long without assistance, one arm will be forced down first, and even appear externally. This used to be considered a separate presentation, and described as such, under the name of presentation of the hand and arm. There is no reason for describing it separately however, and no utility in doing so, as it differs in no essential particular from ordinary presentation of the shoulders, and must receive the same assistance.
What it is that produces presentations of the Trunk, and other unfavorable parts, is not known, though they are generally thought to be owing to excessive motion in the child, or obliquities of the Womb.
M. Lachapelle met with sixty-eight cases of Trunk presentation in fifteen thousand six hundred and fifty-two labors, which is nearly the same as the face. The right side presents more frequently than the left, and the head is on the left side oftener than on the right, as it is in ordinary head presentations.
As a general rule assistance is always rendered in presentations of the Trunk, and is generally considered absolutely necessary. It is undoubtedly true however, that nature has effected delivery in such cases unaided, though rarely, and such instances are considered as extremely fortunate exceptions to the general rule. M. Chailly says that the accoucheur should never leave such cases to nature alone, but always aid her; but other authors trust to her a little more. The most usual mode of rendering assistance is to turn the child, and bring down the feet, a manœuvre which will be fully described hereafter.
In some cases the child turns itself, from the contractions of the Womb, before it enters the upper strait; and in other cases, when very small, or long dead, it will pass folded double. This self-turning however, cannot take place after the escape of the waters, so that it seldom occurs when the membranes are broken.
This is the most usual mode for the fœtus to escape,[205] in each presentation, and in every position. By referring to the following Plates, and the accompanying descriptions, it will be readily understood.
PLATE XXXV.
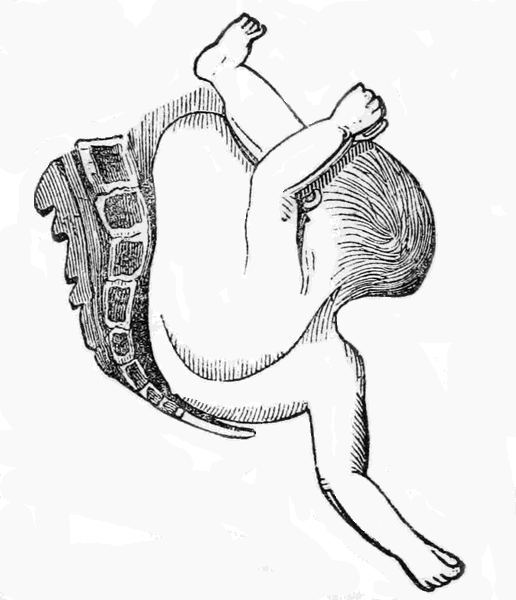
Position of the Fœtus in a presentation of the right shoulder, and in the left cephalo iliac position.
Previous to the rupture of the membranes the child's body lies across, as formerly explained; but immediately after the rupture the shoulders descend into the Pelvis, as seen in the above Plate, while the head remains above the pubes; the arm frequently, but not always, protruding externally.
The shoulder then continues to descend, the body following, bent up against the face, as seen in Plate XXXVI.
PLATE XXXVI.
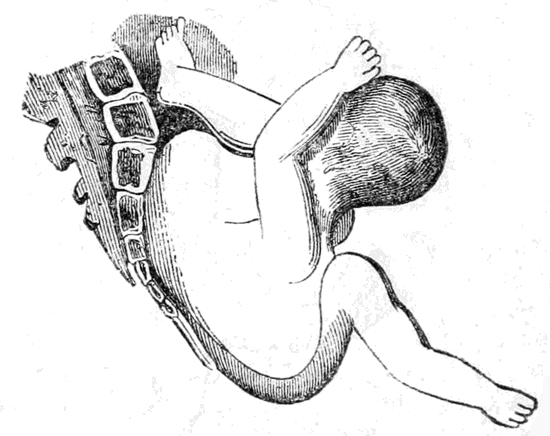
Descent of the shoulder in a Trunk presentation, at a more advanced period.
Here the shoulder is protruded from the Vulva, the back being nearly folded, and the knees turned up against the face.
PLATE XXXVII.
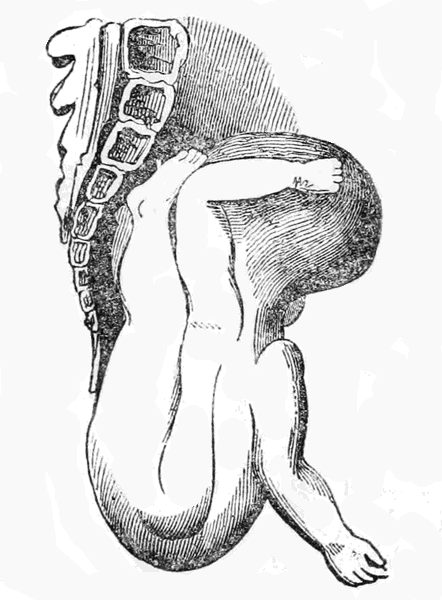
Descent of the shoulder and trunk at a still later period.
The whole Trunk is now fully delivered, folded almost double, and the legs and feet are turned up against the face. They speedily follow however, and then nothing is left but the head, and perhaps one or both arms, placed against the sides of it, as shown in Plate XXXVIII.
PLATE XXXVIII.
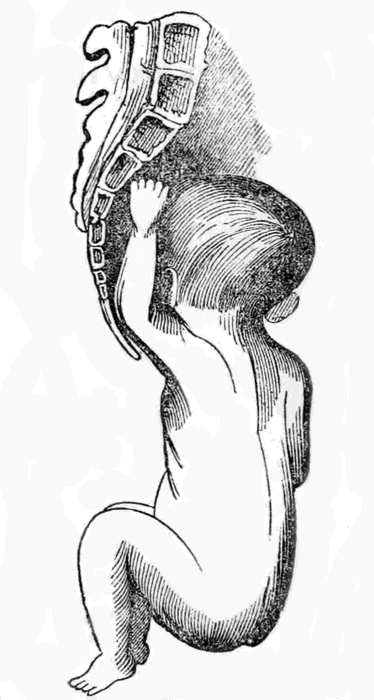
The Trunk has fully descended, and only the head is left, with one arm.
The arm is generally very easily brought down, or it may remain and come with the head. The delivery of the head is effected the same as in presentations of the pelvis, and is seldom attended with much difficulty, the parts having been so much distended. The body always rotates so that the back comes in front, and the chin passes into the curve of the Sacrum.
This is the way in which the delivery is effected[209] by nature in such cases, and it will readily be conceived how dangerous it is to both mother and child, and how seldom it can be accomplished. If the Fœtus be of a full size, and the mother's pelvis no larger than ordinary, it is almost impossible for this spontaneous evolution to take place; and even when it does, it is with the greatest difficulty, the mother suffering in an extreme degree, and running great risk, not only of the most serious after results, but even of death. To the child the danger is equally great, owing to the severe and long-continued compression it receives, and the unnatural position it assumes. M. Velpeau tells us that in one hundred and thirty-seven such cases, one hundred and twenty-five of the children died. The number of the mothers also, who either died or were made sufferers all their future lives, was undoubtedly great, though unknown.
It is evident therefore, that presentations of the Trunk are the most unfavorable known, and labor in them is but rarely spontaneous. Nature can but very seldom effect the delivery of the Fœtus herself, and even when she does it is with the greatest risk, both to it and the mother. The accoucheur should always assist therefore, if he can, because even if nature can complete the delivery it is with such danger. The means of assisting, by turning, will be described in another Chapter.
If the fœtus is not at full term, and of course is under the full size, its expulsion may be left to nature safely, but not otherwise.
THE PHYSIOLOGY OF SPONTANEOUS DELIVERY, OR CHILDBIRTH, AND THE MANNER OF CONDUCTING A NATURAL LABOR.
Having now completed the description of the Mechanism of Delivery, in all the various presentations and positions, it is necessary to explain the physiological phenomena attending a natural labor, and the duties of the accoucheur when conducting it, and to show what assistance he can render, and when he should or should not interfere.
When the child is brought into the world by the unaided efforts of nature, and without any accident to itself or the mother, it is called a Natural Delivery. When it occurs by the efforts of nature alone, but not advantageously for both, it is not called natural, but simply Spontaneous Delivery. And when assistance is required it is called an Artificial, or difficult Delivery. It is also called precocious, or tardy, according as it comes before or after the full term.
What it is that causes labor to commence, and proceed, is not fully known. At the proper time the Uterus prepares to cast out the fœtus it has so long retained, in the same manner that the tree casts off its fruit, and from some efficient cause which we have not yet discovered.
It is probable that, when the fœtus attains a certain size, it presses upon the nerves of the neck of the Uterus and irritates them, and they react again upon the muscular fibres of the Womb and cause them to contract, and so expel its contents. This is much the same action, in fact, as vomiting. When any body very repugnant to the stomach is swallowed, it irritates the nerves of that organ, and then they excite its muscular fibres, which, by forcible contractions, expel the offender.
It is possible, also, that the fœtus itself may instinctively assist in bringing about its own delivery, as was supposed of old by Hippocrates, and more lately by Harvey and others. It is certain that labor is both more difficult, and more dangerous, when the child is dead; though it may take place as usual after the death of the mother, providing the child be still alive. Several instances of this kind have been known, when the living child was expelled from the Womb, by the natural process, sometime after the mother had ceased to breathe.
The contraction of the muscular fibres of the Womb however, must be regarded as the immediate or efficient cause of fœtal expulsion, let them be brought on how they may. The muscles of the Abdomen, and the diaphragm, also assist, in the last stage, but are not essential.
The young of some of the lower animals are observed to perform certain peculiar motions, during delivery, by which it is much facilitated; and this is considered a proof, by some, that voluntary movements of the fœtus assist in the process. Certainly if it be supposed, as we have shown there is good grounds for doing, that the child assists in placing itself in the best position, it is equally probable that it also assists in its own expulsion, in other ways.
Premonitory Signs.—A few days before delivery the Uterus descends much lower, so that the diaphragm and stomach are less pressed upon, and the breathing and digestion becomes easier in consequence. The ease which is thus experienced is sometimes so great that the female becomes unusually[213] animated and cheerful, and cannot think she is so near her travail. This is not always the case however, for some on the contrary feel very uncomfortable and melancholy. The lips of the Vulva are also apt to swell and become painful, and the lower limbs numbed and cramped, owing to the child's head pressing on the large nerves. The neck of the bladder is also very liable to be compressed, so that a constant desire is felt to urinate, and a similar trouble may also be experienced in the Rectum. Most of these inconveniences, but particularly the numbness and cramps in the limbs, are not likely to be experienced except when the head presents, because no other part is so formed as to be able to descend sufficiently low; when they are felt therefore, the female may console herself by the reflection that they indicate, with tolerable certainty, that the child is presenting in the best position it can for a safe and speedy delivery.
Standing, or walking, usually become more difficult, and swelling of the external parts, or piles, are apt to occur. With some females also, a sudden diarrhœa, or vomiting, takes place, and troubles them up to the period when labor commences.
Finally the Uterus begins to contract, though insensibly at first; the Abdomen becomes unusually hard, and flying pains are experienced, particularly with first children. This continues with more or less of intermission, up to the actual period of labor, which is usually divided into three periods, each of which must be considered separately.
On making an examination the mouth of the Womb will be found to be dilating, and a discharge of mucus, tinged with blood, issuing from it. The membranes may also be felt protruding into the Vagina, and distended, like a bladder. The female complains of being drawn powerfully together in the inside; she trembles, and gasps for breath; her pulse sinks, and she often becomes sick and deadly faint; she complains of great thirst, and breaks out into profuse perspiration; frequently she will weep, and apparently suffer from some terrible apprehension, while her strength will be completely exhausted. Occasionally however, she will be perfectly passive, and almost immoveable, appearing as if in a dream.
The pains however, gradually become more and more acute, and closer together; the patient is excited and irritable; her pulse becomes quicker again, the thirst increases, and vomiting frequently ensues. Before each pain she frequently experiences a severe chill, with chattering of the teeth, and not unfrequently becomes perfectly delirious.
With each pain the mouth of the Womb expands more and more, till at last it totally disappears, and the cavity of the Uterus and the Vagina form but one uniform passage, which is completely occupied with the distended membranes, or bag of waters, which may be felt like a soft round tumor. This is well represented in the following Plate:—
PLATE XXXVIII.—a.
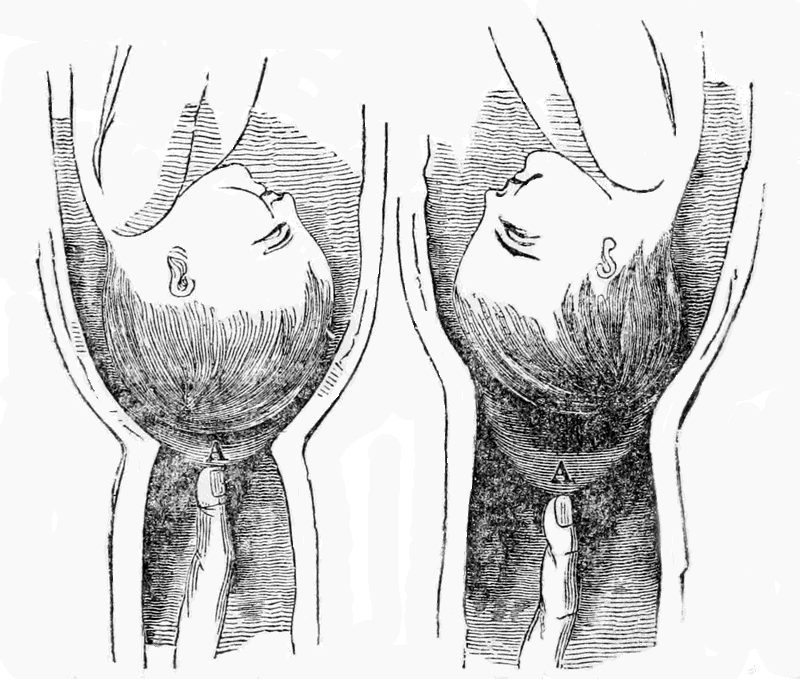
Fig. 1 shows the state of the parts at the beginning of labor. The mouth of the Womb is considerably dilated, and the Membranes, A, are protruding slightly.
Fig. 2 shows the state of the parts at the end of the first period. The neck of the Womb is now so fully dilated that it forms a continuous passage with the Vagina, while the bag of waters, A, projects far down and occupies the whole width of the canal.
The first period may be much protracted, and is generally very exhausting, though not attended with any danger or special difficulty.
At this stage all the previous symptoms become much exaggerated. The contractions are more powerful, and the pains more acute, but with a perfect period of repose between them, during which the female will feel quite easy, and even sometimes fall asleep, but only to be aroused by the pains coming on again. The muscles of the Abdomen, and the diaphragm, are now called into play; the patient strains, or violently bears down, and pants with exertion, while the perspiration streams from every pore, the pulse quickens, and the expression of the countenance betrays the wildest anxiety and excitement.
The bag of waters now descends, and enlarges more and more, until at last, being unable any longer to bear the strain to which it is subject, it bursts, and the waters flow away in a profuse gush. Immediately this takes place the head descends, and closes up the passage; the pains cease for a time, and the patient again has a respite, while the uterus apparently gains fresh power. Very soon the contractions recommence, more energetically even than before, the head passes the mouth of the Womb and enters the Vagina, which keeps enlarging as it descends, till it reaches the lower part, or floor of the pelvis. The pains now become more violent than ever, the patient screams with agony, clutches hold of any object near her, throws herself back, draws in her breath, and bears down with all the force she can command.
The fearful cries which most females emit at this time appear to assist the delivery, by the convulsive efforts at breathing which they necessitate, and the expulsive straining also does the same. These natural[217] efforts are much assisted by providing a firm support for the patient's feet, against which she can push, which she will do with tremendous force.
The head now presses, at each pain, against the perineum, which begins to project outwards, as also does the Rectum. The Vulva begins to dilate, the lips separate wider and wider, and part of the child's head becomes visible. Gradually the lips become thinner and thinner, and at last disappear nearly altogether, so that the mouth of the Vulva is only composed of thin ring, which seems ready to give way every moment. The head however recedes, and the parts again assume something like their natural condition for a short time, when the same process again takes place, and the distension proceeds still further, while the head does not retire so far. This alternate action is repeated perhaps many times, so that the external mouth is opened gradually, and without the lips or perineum being torn, which they would be if the head were to pass suddenly, before they were softened and dilated.
After this has been continued for a sufficient period a strong expulsive pain is felt, the female screams, the head passes clean through the external opening, and the lips close round the neck. This however, is only for an instant, the rest of the body speedily following the head, in the manner hereafter to be explained. Most usually, in fact, the whole body follows the head without any stoppage at all, but sometimes there is a delay of a few seconds.
The Third period of delivery comprises the delivery of the Placenta, which will occupy our attention in another place.
Differences in the process of Labor.—Although, in most cases, labor proceeds much in the way I have[218] just explained, and is attended with similar phenomena, yet still we occasionally see marked exceptions. This is particularly the case with regard to pain. Most females suffer severely at this time, and some even the most torturing agony, while others again experience scarcely anything to complain of, and some even feel nothing at all. I am acquainted with a lady at the present time, the mother of several children, who assures me she never felt any pain at all in her labors, nor was she in any ways exhausted by them. I have known her rise from her bed in the night, from feeling indications of the approaching event, make all her arrangements, and send for the nurse, as if it was the most ordinary affair imaginable. On one of these occasions, before her husband returned with the assistants, she was delivered while alone, without any difficulty, and they found her sitting up in bed nursing the child. She had cut it loose, and tied up the cord herself, having heard how to do so at one of my Lectures, and actually brought away the Placenta with her own hand. In two days after she was about as usual. And yet this lady was by no means strong, nor remarkably healthy; and what is very singular, she suffered severe pains at most of her monthly periods; much more, as she assured me, than from all her labors put together. M. Chailly also mentions an instance of a young girl of sixteen, with her first pregnancy, whose Vagina was also partly closed by an internal membrane, whose delivery nevertheless was almost painless. She woke up, he tells us, about four o'clock in the morning, with some very slight pains, which scarcely disturbed her, but which continued till about six, when the child was born suddenly and safely, without any assistance, and with scarcely any increase[219] of pain to the mother. I have known many other such cases as these, and plenty of them can be found recorded; but what this fortunate exemption from suffering, in such cases, depends upon, is not known.
The nature, and the seat of the pains, is also very variable. Some only feel a dull sort of aching, with powerful contraction, or drawing together, while others call it grinding, cutting, and burning pain. Some feel it in the back, and some at front, while others feel it most in the groins, and others again experience it in all these parts at once. The peculiar sharp pain which results from the extreme dilatation of the external mouth, when the head passes, is perhaps the most constantly felt, and the most alike in all.
The manner in which the mouth of the Womb opens, and the time required for its dilatation, differ much in different cases. In females who have previously borne children, as before explained, the mouth is always considerably opened at the full term, while in a first pregnancy it is nearly closed, even till some time after the labor actually commences. Sometimes the dilatation takes place rapidly, and at others very slowly; it is especially liable to be delayed if the Membranes break too soon, because then the pressure of the bag of waters is lost, and that is an important agent in expanding the Os Uteri. In some cases the neck of the Womb is very hard and rigid, so that a long time is required to make it give way. When any other part than the head presents also, the opening of the mouth will not take place so soon, because no other part so completely fills up the passage.
The breaking of the bag of waters will sometimes occur very early, almost as soon as it protrudes;[220] while at other times it will be delayed till the whole Vagina is filled up by it, or even till it appears externally. The quantity of the water discharged at the time of the rupture is also variable; if the presenting part of the fœtus does not completely block up the passage, the whole may pass away when the rupture takes place; but if it does, as is usually the case when the head presents, only a part flows then, and the rest comes in gushes, as the head is raised, and when the child is born. The too early escape of the waters, as already explained, may retard the delivery, by delaying the expansion of the mouth of the Womb; and in this way unskilful accoucheurs have caused lingering labors, by breaking the membranes too soon.
It is important to recollect also, as I explained before, that a portion of fluid sometimes exists between the amnion and chorion, which may pass first, and induce the belief that the true waters have escaped, when they have not. This is called the false waters, or shows, and is not connected with the true waters at all.
The general physiological phenomena of a natural delivery having thus been explained, we have now to state its duration, and then proceed to its conduct or management.
The duration of natural labor is not by any means constantly the same, nor can it be predicted with anything like certainty in any case; but still by keeping careful records, and by duly observing a vast number of cases, a tolerable approximation can [221]be made. There are various circumstances that tend to lengthen the duration of labor, some general, and others belonging to the individual. The mode of life and early habits of the female, the climate in which she lives, and the manner in which she has conducted herself during gestation, all have an important influence. As a general rule, the period becomes longer in proportion to the civilization of the community in which she lives. The first labor is generally more tedious than the succeeding ones, owing to the slower dilatation of the parts. It is also thought by some, that the labor is longer in proportion to the age of the female, particularly with the first child; but this opinion is not well founded.
The average duration of labor in our country, is from eight to twelve hours. In some parts it is longer than this, and in others again it is much shorter. I have good reason also to think, that it is longer in cities than in the country.
An experienced practitioner can sometimes predict with tolerable certainty, when called to a labor, how long it will be before it is over; but this is seldom the case, and most frequently his success is owing more to chance than to judgment. If the mouth of the womb be well dilated, the contractions powerful, and the patient vigorous, with the presentation natural, he is of course justified in predicting a speedy delivery; or the reverse, if these favorable conditions do not exist. Many unforeseen conditions may exist, however, and many accidents arise, that may falsify an apparently safe conclusion. No judicious practitioner, except in a few rare cases, will hazard his reputation by fixing any time, and no well informed patient would ask him to do so, because she would know that it was out of his power.
In most cases of natural labor there is not much assistance needed. The assistant should, however, possess a certain tact, or manner, calculated to make a favorable impression on the patient. This is especially needed when a man officiates. It must be recollected, that the situation of the female at such times is a very peculiar one, and that the presence of one of the other sex, however necessary, must be more or less objectionable to her. He should, therefore, carefully exhibit in his behavior the most refined delicacy, combined with a warm sympathy and kind consideration; thus soothing her scruples and enlisting her gratitude. He must also appear perfectly self-possessed under all circumstances, and then she will have full confidence in his skill and judgment. It may seem scarcely necessary to state these things, but I have often known men officiate without such qualifications, and also be perfectly unaware of their deficiencies. Such accoucheurs never officiate well; they may be skillful and attentive, but yet unsuccessful, and unappreciated. They are only tolerated, but not respected, and are never fully confided in.
When requested to see a woman supposed to be in labor, it is always advisable to be prompt in paying the visit, because delivery sometimes comes on suddenly and unexpectedly, and both mother and[223] child may be in great danger if no one is near to assist.
Some time before the event is expected, it is advisable to provide certain articles, which will or may be needed at the time, and which should not have to be looked for at the last moment. A pair of sharp scissors, with a piece of strong thread or cord, are indispensable, and a female catheter may be needed. A quill with the feather part on, may also be useful; and some pure lard or sweet oil is frequently called for. The professional accoucheur will also find it a good precaution to have his stethoscope in his pocket, and a lancet, if he ever relies upon bleeding in any contingency. A small box of extract of Belladonna also, may often be of great and immediate service.
The first thing required when visiting the patient, is of course to ascertain positively whether she be pregnant, and whether labor is really commenced, and if so how far it has progressed. This necessitates an examination, the proposal and making of which require the most delicate tact, particularly if it be with a comparative stranger, or in a first labor. No allusion to it should be made to the patient herself by the assistant; he should converse with her about indifferent matters, or merely upon her health, and state his wishes to the nurse or female friend, and then retire. This gives them time to inform her of what is required, and to make the necessary preparation. On entering the room again, he should not proceed abruptly, but resume the conversation, and make some of the necessary arrangements while carrying it on. He should seat himself by the side[224] of the bed, with his right hand next her, and his face opposite hers. Then passing his hand under the bed clothes, after having lubricated it with lard or oil, he can proceed with the examination as if it were a simple ordinary proceeding. By exhibiting no hurry, and appearing to think it nothing unusual or in any way strange, the female herself will cease to think it so, and will not be flurried or shocked.
The hand must be passed under the female's right thigh, her knees being elevated. She should, of course, lie on her back, and as near to the edge of the bed as convenient. Not the slightest exposure is necessary, nor allowable under ordinary circumstances.
The fore-finger being introduced, ballotment may be practised, to ascertain if pregnancy really exists; and if the evidence from this source is not sufficient, auscultation must be resorted to. After being satisfied on this point, the mouth of the womb must be carefully examined, and its degree of dilatation noticed. If the female has pains, their character and frequency must also be noticed, and the effects they produce on the parts. It will generally be possible by these means, to discover how far the labor has progressed, and even to form an opinion how long it is likely to last. The general form of the parts and their size, should also be noticed; particularly of the pelvis, so that any deformity or deficiency may be discovered. And lastly, the presentation should be ascertained, if possible, so that it may be known in time whether nature will be sufficient herself or will require helping. The position need not be cared for at present, because it is of little consequence when the presentation is favorable.
The time required to make the examination need[225] not be long, and should always be as short as possible.
While conversing with the patient, much useful information may be gained. The general state of her health, the nature of her pains, and the time they first commenced, should all be known; and if she has had children before, it will be highly useful to know what kind of a labor she had; whether it was long or short, easy or difficult, and particularly if attended with any accident likely to occur again.
It need scarcely be remarked that great caution is needed in these cases, many eminent men having been deceived as to the patient's condition, as already stated in our chapter on the signs of pregnancy. And many times the doctor has been summoned under the supposition that labor had begun, while it was yet far off. The pains may be false ones, such as frequently occur towards the end of pregnancy, and may all pass away. These false pains, however, can usually be distinguished, being continuous and irregular, while the true ones intermit with periods of almost perfect ease, and are tolerably regular. The false pains are also felt in various parts, while the true ones are chiefly fixed in the uterus and vagina. Sometimes, however, the difficulty in distinguishing them is very great, and the accoucheur has often waited for several hours and even days; the labor meanwhile making no progress; and eventually all has passed off, and the patient has risen again from her bed. I know one case, where a gentleman attended nearly three days, at the end of which time the patient rose and walked down stairs. She was not put to bed till six weeks after. I can scarcely think, however, that these mistakes can[226] happen very frequently, if the examination be properly conducted.
If it appears from the examination that labor has really commenced, or is about to do so, everything should be at once prepared. All useless persons should leave the room, and also those who would be likely to alarm or grieve the patient by uttering cries, or exhibiting fear; but no objection should be made to any one being present whom she wishes to see, unless they cannot be depended upon. Thus some females always wish to have their husbands with them, but others do not, though they are averse to saying so. In these cases the accoucheur, if he be an attentive observer, will soon see what is really desired by his patient, and will manage matters accordingly.
The dress of the female should be perfectly loose, consisting of a wrapper or night-gown, but sufficiently complete and warm to allow of her getting up to walk in the chamber, if she desires it, as some do. No corsets, garters, or other tight bandages, however, should be allowed.
The bed should be prepared by placing the mattress on the top, or by removing all from it; and then placing a thick layer of blankets or quilts, with a folded sheet over them. This is to provide a firm level surface, in which the body will not sink, and also to prevent the fluids soaking through. It is an excellent plan, if the material can be obtained, to place a thin oil-skin or India-rubber cloth under the folded sheets, as this keeps all perfectly dry underneath. Some persons also place another folded sheet,[227] or a cushion, under the pelvis, to keep it elevated; but this is not necessary, unless the bed sinks in very much. It is also advisable to leave a foot-board or other firm body, against which the female can press her feet when bearing down; and a long towel folded lengthways should be passed under the back, so that it can be raised up by a person lifting at each end. This will often be found a better mode of pressing the back, which nearly all patients call for, than by merely forcing the hand against it, which is both tiresome and insufficient. Another towel may also be firmly fixed to the bottom of the bed, so that she can pull by it, at the same time that she pushes with her feet.
Some persons are confined on a cot, but this is not a very good arrangement, because it sinks in too much in the middle, and is not sufficiently large and firm. It is advantageous in one respect, however, as it can be placed by the side of the bed, into which the patient can be lifted when all is over, and be comparatively dry and comfortable. This is the most frequent plan in France. If the bed be properly arranged however, the under sheet can be withdrawn, and clean warm napkins then passed under the body, which will be equally as good. The covering should consist of a sheet, with blanket or coverlid, according to temperature, and should, of course, never be removed, except under peculiar circumstances.
The chamber itself should be as quiet as possible, well ventilated, and not too warm. Nothing distresses the patient more than a close, hot atmosphere.
The accoucheur need not, of course, be present while these arrangements are being made; and when he retires he should suggest to the nurse that the[228] female may attend to the bowels and bladder during his absence. This precaution may both facilitate the labor, and prevent much future annoyance. It would even be advisable to administer an injection if necessary, of thin starch and a little castor oil, rather than leave the bowels unmoved.
In regard to nourishment, nothing is needed or proper in the shape of solid food; because all the energies of the system are concentrated in the uterus, and as digestion cannot therefore go on, it would only be an evil. If the labor is much protracted however, some broth or soup may be taken, or a little milk. As a general rule, no spirituous liquors or stimulating drinks of any kind should be taken; because they impart no real strength, and may produce inflammation, or congestion on the brain. Some females always prefer tea to drink, others lemonade, toast water, gruel, or barley water, and others again simple cold water, which is perhaps the best of all. In cases of great exhaustion it is sometimes advisable, and even necessary, to give a little wine, or brandy and water, but it should always be cautiously administered.
In some parts it is customary for the female to lie on her side during delivery, with a pillow between the knees; some even choose this mode, and others will desire to stand, or place themselves on their knees. The most frequent position however, and certainly the most convenient, is on the back, though it may often be changed with advantage under peculiar circumstances. In the early stages of labor she can lie, or move about, as she chooses, or even rise if more agreeable.
When everything is arranged the assistant should take his seat on the right hand of his patient and repeat the examination. If the head presents, he need not concern himself much further at present, but if it be any other part, he should prepare at once to change it, or assist, as the case may be. At this second examination the parties present, and the female herself are usually anxious to know if the child is coming right, and how long the labor is likely to last. The answer to these inquiries should be guarded and circumspect in regard to the duration, because of its uncertainty, but if the presentation is right, it is well to say so at once, because this gives great comfort and encouragement. If it be unfortunately wrong, it is best not to say so abruptly, but remark that it is rather obscure, or cannot yet be fully distinguished, and so keep up the spirits of the female while you await the proper time, or make the necessary arrangements, to interfere; and then tell her there is a little difficulty which requires to be righted, but which will not be serious, nor cause much delay.
If the labor steadily progresses it is necessary to remain with the female and attend to it; but if it be delayed, and everything remains natural, she may be left for a time with advantage. When the second stage is fairly commenced however, and especially after the membranes are broken, the attention should be unremitting. The state of the parts should be ascertained frequently, so that the actual progress may be known, and any necessary assistance rendered. The state of the bladder especially should[230] be observed, and if it be full and the female unable to urinate, the catheter should be passed. Neglect of this precaution may lead to serious accidents. While making the examinations, the hand should be introduced with great care, so as not to bruise or lacerate the parts, and it should not remain longer than absolutely necessary.
Many females exhaust themselves unnecessarily by bearing down, and straining, with great force, from the very commencement of labor, under the mistaken idea that it is necessary to do so, or will assist. They should be told not to do so however, till after the membranes are broken, and not even then unless the neck of the womb begins to dilate. They should also be told not to make any effort except during a pain, as it will not assist at any other time.
No attempt should be made, under ordinary circumstances, to rupture the membranes, or dilate the mouth of the womb, even though nature may be slow in doing so. Patience must be practised, both by the female and by her assistant, and sometimes it is severely tried.
When the waters have escaped, and the orifice is opened, an examination must be made, to discover whether the cord has descended, or either of the arms, as is sometimes the case, and if so, they must be returned if possible.
As the head descends to the bottom of the pelvis it compresses the rectum, and produces a feeling as if the bowels must be moved, or even causes them to be so. This is apt to distress the female, and make her wish to rise, which cannot be permitted. If anything of the kind occurs no notice should be taken of it, or she may even be assured she is mistaken,[231] while a clean napkin may be interposed. This, as Dr. Chailly observes, will soothe her delicacy. Such an accident is very apt to occur towards the end of the labor.
When the head has rotated, and presents at the external opening, or vulva, and begins to distend it, the greatest care is required. This is a critical period, during which the accoucheur can render more real assistance than at almost any other. There is danger at this time, as formerly explained, of the head passing through too quickly, before the parts are sufficiently relaxed, and so causing them to rupture. This is particularly the case with the perineum, against which the head presses with great force. It is necessary therefore to support the perineum, as it is termed, to prevent this accident. This is done by passing the right arm under the patient's right thigh, and placing the palm of the hand flat against the perineum, with the thumb encircling one side of the vulva, and the forefinger the other. The hand is then gently, but firmly, pressed against the part during every pain, so as to prevent the head passing too quickly, and also to elevate it, and thus relieve the perineum of part of the strain, and throw the occiput under the pubes.
Some practitioners also pass the left hand over the thigh, at the same time, and grasp the back of the head with it, thus holding the head as it were between the two hands, so as to direct it at pleasure.
The manner of doing this is represented in plate XXXIX.
PLATE XXXIX.
The manner of supporting the perineum, during the passage of the head.
The right hand is placed underneath, so as to push the head gently back, when it presses on the perineum too forcibly, before it is dilated; and also to elevate it towards the pubes.
The left hand is seen above, grasping the top of the head, to assist. This may be done or not, according to the necessities of the case, or the custom of the assistant.
It is also necessary to request the female at this time to moderate her efforts, and not bear down too strongly. If however she be too excited, and eager to do so, more care must be used, and the head pressed back still more forcibly, till the parts are fully relaxed. For want of these precautions there is often serious lacerations of the perineum and vulva, particularly in first labors, and when the parts are unusually rigid. If proper care be bestowed however, these accidents ought to occur but seldom, even in the worst cases, and nothing can be more hurtful to the reputation of an accoucheur than for them to happen. Sometimes it is necessary to support the perineum for hours, and to bestow constant attention the whole time. It is often useful to keep applying a little simple ointment, or lard, in the intervals of the pains, mixed with the extract of Belladonna, which will soften and relax the parts. Dr. Lee also advises the application of a sponge, dipped in warm water, and which would probably do much good in many cases.
It will of course be understood that the pressure only needs to be made during the pains; when the head draws back the ointment or warm sponge may be applied. The knees of the female should be held up by some one, if she bears down too much, so as to prevent her from doing so too powerfully.
When it is felt that the parts are fully relaxed, and sufficiently distended, the head is left at liberty, during a strong pain, and it immediately passes the outer ring, or is born.
It should then be held up, towards the pubes, and the mucus should be cleaned from the mouth with one of the fingers, so that the child may breathe. A careful examination should also be made round[236] the neck, to see if the umbilical cord is around it. If it be so, but is not tight, it may be left alone, or pulled a little over one shoulder, or even passed clean over the head, if it can be easily drawn out long enough. When it is very tight, and cannot be eased, it must be cut through, or it will strangle the child.
In most cases the shoulders follow immediately after the head, the uterus resting only a few moments; but if they do not the head may be slightly drawn upon, or the fore-finger of the right hand may be linked under the arm, and a little force employed, though very carefully. It is better however to wait even two or three minutes, and only resort to these means when there is evidently a partial suspension of the natural efforts. Sometimes also the contractions may be brought on again by merely pressing the hand over the fundus of the uterus, and this should therefore be tried first. In all cases it being better to let the uterus expel the child than to bring it away by manual force.
During the passage of the shoulders the perineum needs as much care as during the passage of the head, and must be supported in the same way. Indeed some authors are of opinion that most cases of laceration are caused by the shoulders.
After the shoulders are expelled the limbs and body speedily follow. The child should be received in the hands of the accoucheur, and laid on its side, at a little distance from the vulva, so that it may not be suffocated by the discharged fluids. He should then take a strong ligature and pass it twice round the umbilical cord, about two inches from the navel, and also at about four inches, and then cut the cord through, between the two bands, with a pair of sharp scissors. The child may then be handed to the nurse.
The tying of the cord is by some deemed unnecessary, and in most cases probably is so, but as children have been known to bleed to death, when it was not done, it should never be neglected. Some practitioners only tie it once, leaving that part open which is still attached to the placenta, and they suppose this is advantageous, inasmuch as it partly empties the placenta of its blood, and so helps to detach it. There is little or no fear, as some suppose, that this bleeding can be extensive enough to hurt the female, or second child if there be one, and even if it were likely to be so it could soon be stopped; it has the inconvenience however of soiling the bed more, and this is probably one great reason why the second ligature is applied, which certainly is not necessary.
In my directions I have said that the cord may be tied about two inches from the abdomen, and this will be sufficient if the child breathes; but if not it should be left about four inches long, so as to give room to cut it again, which is occasionally needed, as will be seen further on. The knot should be drawn very tight, and great care must be taken never to tie it so near as to pinch the skin of the abdomen, which passes a little distance up it. A small portion of the intestine will enter the cord sometimes, and swell it out for an inch or more; this must be pressed back with the thumb and finger, and carefully avoided by the ligature. Some practitioners cut the cord first and tie it after, but I think the other plan is decidedly the safest and the best.
After this is accomplished the accoucheur should place his hand again over the fundus of the uterus, to discover whether it contracts, and also to judge whether there be another fœtus. If the womb is felt[238] drawn up into a hard round ball, in the middle of the abdomen, all is right, and no apprehension need be felt; but if it remains unaltered in size, and is soft, flooding is to be feared, and the hand should be firmly pressed, or kneaded, over the fundus, to bring on contraction.
If there be another fœtus, the womb will remain much the same as before labor, and the child may also be felt. It is better however to make an examination internally, and then, in most cases, the membranes and presenting part of the second fœtus will be found at the upper strait. If there be any doubt after this it is even better to carry the hand a little way into the womb, than to remain in ignorance on such an important point. The delivery of the second fœtus usually follows close upon the first, though sometimes there will be a delay of some hours, or even days. And in general there is little or no difficulty with the second, owing to the parts having been already prepared; but the longer it is delayed the less easy it becomes.
Immediately the birth is fully effected the female feels, as most of them express it, in heaven; there is an almost instantaneous change, from the most agonizing pain to a state of perfect ease. She ceases her cries, and falls into a quiet and pleasing languor, strikingly at variance with the state of intense excitement she was in but a few moments before. This repose however, does not last long; the Placenta yet remains, and a new effort is required to expel that.
Unlike the Fœtus the Placenta is fast to the walls of the Womb, and can only become separated from them by the contraction of their substance, which usually commences soon after the birth of the child, and is indicated by new pains, and a slight discharge of blood. In about a quarter of an hour, or twenty minutes, the accoucheur should enquire of the patient whether she has felt any of these pains, and he should also examine whether the Placenta has reached the mouth of the Womb, or Vagina, so that he may remove it. If the pains have not yet come on, and the Placenta is not in the passage, he should press one hand on the fundus of the Womb, to promote its contraction still further, and then gently draw upon the cord with the other, holding it as high up as possible, either by a piece of linen around it, or by looping it around the finger. It should be pulled very gently, but steadily, downwards and backwards. If it be snatched, or drawn too hard, it may break, and cause great trouble; or it may pull down the Womb, and either invert it or bring on falling of the Womb afterwards. The hand placed over the fundus can detect this accident, and if the uterus be felt to sink down the cord must not be drawn upon any longer. Pulling away the Placenta too soon, and with rudeness, has often led to deplorable accidents. In nearly every case it will gradually separate itself, and be delivered in about half an hour, and should only be assisted by slight drawing on the cord, and by pressing the fundus.
When the Placenta is completely detached there is seldom any difficulty in its passing the neck of the[240] Womb, and down the Vagina, but it usually requires to be drawn through the external opening by the hand. In doing this the membranes may be twisted round the cord, so as to wind them altogether, and strengthen the cord.
In case the separation does not take place we must wait, and continue the slight strain on the cord and the friction over the fundus. It is not reckoned safe however, by most authors, to wait more than an hour; and if there is no sign of its coming by that time artificial delivery is resorted to. This is accomplished by carrying the hand carefully up into the Womb, and separating the Placenta from its walls with the fingers, and then bringing it down at once.
When the afterbirth has passed the Vulva, a careful examination should be made of it, to see that no part is left behind; and for still greater security it is advisable to explore the Vagina thoroughly, so that any detached portion may be removed. The membranes are very apt to become broken, and fragments of them left, which though ever so small may cause trouble. The finger should also be passed into the mouth of the Womb, so as to clear it; for sometimes a large clot of blood, or a piece of the membranes, will remain and keep it open, and thus cause severe flooding.
It is generally considered, by those who have bestowed attention on the subject, that assistance should always be rendered, if the afterbirth does not come very soon. There is danger, if it be left too long, of the mouth of the Womb contracting and retaining it; in which case it becomes absolutely necessary to abstract it, but exceedingly difficult, and even dangerous, to do so. Dr. Lee says it should never be[241] left more than an hour at most, and that it is best never to delay removing it even so long as that.
When left purposely, for observation, it is found to be expelled spontaneously, and soon, only in a few cases; usually it remains several hours, and most frequently it requires to be removed by hand. No doubt it is natural for it to be expelled unaided, but it must be borne in mind that our females are usually too weak, and deficient in energy, to perform any unusual natural function without assistance. The accoucheur must use great caution, so as neither to intrude his help when not required, nor yet to refuse it when really needed; and above all he must not substitute violence for skill.
When the afterbirth is brought away, a bandage should be passed round the body of the female, made of soft linen, twelve or fourteen inches wide. It should be drawn moderately tight, and fastened securely. If it pass round twice it will be all the better, and it should be drawn down as near the pubes as possible. I know many ladies who prefer the India Rubber bands, recently invented, as they press more equally and firmly, and are put on with less trouble, being all in one piece and drawn over the feet and limbs.
Some accoucheurs put on the wrapper immediately the child is born, before the afterbirth passes away; but I think this is not the best plan. When properly adjusted, the supporting band gives great comfort to the female, and is very useful.
Some ladies provide a curious kind of corset to put on, invented for the purpose, which however, as a celebrated author recently remarked, "Are usually stiff and unyielding, like the prejudices of their patrons, and often prove injurious." None of them[242] are equal to the simple contrivances above-mentioned.
When the afterbirth is removed the patient should be left to repose herself for about a quarter of an hour, during which time most of the blood escapes, and then she must be made as comfortable as possible. In France, and with many persons here, it is customary to cleanse the patient with a sponge dipped in warm water, pass a clean warm sheet under her, and then put on clean linen, after which she is lifted into the clean bed, previously well warmed; the accoucheur himself carrying her there. Most frequently however, the sponging is dispensed with till some time after, and also the changing of beds—the under sheet merely being withdrawn, and a warm dry one passed in its place, while the female's limbs are gently wiped. In either case the female should be disturbed as little as possible, particularly if there be danger of flooding, and she should be carefully guarded from cold. When the soiled and wet clothes are removed, as completely as possible, warm napkins should be placed under the Pelvis and between the limbs, to soak up the discharge, and they should be carefully changed as often as needed, without uncovering the patient. If she be disposed to sleep however, and is much exhausted, these attentions need not be pressed too much till she is recovered a little.
Many persons here have a dread of using the sponge immediately, and of being carried to another bed; but there is no danger from either practice, in[243] ordinary cases, when carefully performed; and it is so productive of comfort, that I never knew one but what was pleased with and benefitted by it, and desirous of its being done in their subsequent labors.
Some females will even rise and take a cold bath, or be wrapped in a wet sheet, not only without evil effect but with positive advantage. I would not advise any one to do this however, particularly if they are the least timid at it, or doubtful of its propriety. Without the mental stimulus of faith and hope it may be hazardous. It shows however, that many of the popular notions, as to the requirements and susceptibilities of females, in this state, are entirely unfounded.
The patient may either experience great comfort after being thus attended to, or she may complain very much. Some will even be attacked with a kind of chill. Their teeth will chatter, and their hands and feet grow quite cold. This however usually passes off, and she falls asleep. The accoucheur ought to remain for an hour or two, even though she sleeps soundly, and appears quite well, because she may become suddenly worse, or flooding may set in with such violence as to endanger life in a few minutes, when unchecked.
If the patient desires any nourishment she may take a little simple soup, or gruel, but nothing stimulating, unless a little wine be needed from extreme exhaustion.
Inspection when born.—As soon as the child is born its mouth and nose should be cleared from mucus, if that has not been done already; and if it has not breathed, means should be resorted to immediately[244] to make it do so. Sometimes the whole head is covered with a thin membrane, called the caul, or veil, which is most probably only a portion of the Amnion, and which may cause suffocation. I remember a case of this kind in my own practice, in which the caul was unnoticed at first, and the child came near dying from it. Nothing could be seen, and as it bent before the finger, when pressed into the mouth, it was totally unobserved. The nurse however, called out that the child did not breathe, and a close examination as to the cause soon revealed why. On passing the finger under the edge of the membrane, which was round the neck, it came off like a cap, and the child cried immediately.
Washing the child.—The cleansing of the child may usually be safely committed to the nurse, or other female attendants, though some of them have very absurd and injurious practices in this respect. Thus I have known them rub the whole body over with whiskey, or raw spirits, before washing it, which must cause great coldness from its evaporation, and also great irritation. The only thing required is perfect cleanliness, and this should be effected in the quickest and simplest manner. Some very mild soap, and moderately warm water, is all that is really needed, though a little sweet oil, or fresh lard, or butter, rubbed on first, appears to facilitate the operation. The drying should be done as quickly as possible, after all the mucus is washed off, and with great care; the napkin being as soft as it can be, and never rubbed hard, for it takes but little force to remove the skin. Many persons take great trouble, and are a long time over this infantile wash without succeeding well with it. They are deceived by the tough mucus slipping under the hand, but still clinging[245] to the body, where they leave it even after using the napkin; it then dries on and forms a hard skin, very difficult to remove, and very irritating. This can be avoided with care, and by using the oil first, which appears to soften the mucus. Some persons use flour, or Indian meal, and others starch, but none of these are so good as the simple means we have described.
Dressing the child.—After the washing and drying is completed the child must be dressed, and this is a process in which comfort and utility is frequently sacrificed to mere fashion and prejudice, as it is in adults. The article next the skin should be of soft line linen, which may be followed by others of warmer material, according to the temperature. They should all be perfectly loose in their make, and quite soft to the feel. As far as possible they should all be fastened with strings, rather than pins. These metallic points are troublesome to fix, and often injure the child, in spite of every precaution. They are also apt to be referred to as the cause of the child crying, and thus prevents other causes being sought for, which frequently exist.
Some people put a thick flannel cap on the head, over a linen one, but others leave this part altogether uncovered, which I think is the best plan. At most there should only be the linen covering; the head being better rather cool than otherwise.
The dressing of the cord is the next duty, and this is done by taking several pieces of soft linen, oiled a little, and cutting a small round hole in the middle of each, through which the cord is passed. The linen then lies flat on the abdomen of the child, and the cord on the top of that, the holes being just large enough for it to pass easily through. Five or six[246] pieces are usually put on, but very frequently only one is used, and is found quite sufficient. It should be very fine, and soft. When this is done another layer is laid over the cord, and then a bandage of soft linen, about four or five inches wide, is passed two or three times over it, and round the body. This completes the dressing, and the child may now be wrapped up warmly and laid down to sleep—remembering, as Dr. Chailly remarks, that if it be laid on a chair, or sofa, it may be accidentally sat upon and killed, an accident which has happened.
Before these dressings are needed however, there are frequently other things of more importance to be attended to. If the labor has been long, or the presentation unfavorable, the child may be born apoplectic, from the pressure it has received. The face will be puffed up, and of a blue color; the body will be swollen, and the limbs without motion, while the pulsation will scarcely be felt, either over the child's heart or in the cord. It will feel warm, and the limbs will be quite flexible, but still there will be no signs of life. In this case it should be exposed naked to the cool air, and even blown upon; and if that does not resuscitate it the cord may be cut through below the ligature, so as to let out two or three tea-spoonfuls of blood. After this it generally revives, and begins to move, while its face assumes a natural color, and the swelling goes down. The mouth and throat should also be carefully cleaned with a quill feather, of all mucus.
A more frequent accident is Asphyxia, or want of breathing, in which case the surface of the body is[247] cold and pale, and no breath whatever is drawn, though the heart beats quite naturally. Very weak children, or those born before their time, are most likely to become asphyxiated, or those delivered by instruments. The first thing to be done is to carry the child to the open window, if it be not exceedingly cold, and expose its head and chest to the air, while the rest of the body is wrapped up warm. This will often make it gasp, but if it does not a little cold water may be dashed on its face and chest, and the throat may be tickled with a feather. The breech may also be smartly slapped, and the chest well rubbed with the cold hand. When it begins to breathe a little it may be put into a warm bath up to the middle, and a warm injection may be given to it. In most cases these means will speedily bring it round, but if they do not the attendant should place his mouth close over that of the child and breathe into it, so as to fill the lungs, and then press down the chest to empty them again, repeating the process several times. This may be called artificial breathing, and if it succeed once only there is a probability of its effecting the desired object. The breath however, must not be blown in too hard, or it may injure the child's lungs, nor too rapidly. Sometimes a tube is used, which is passed down into the throat; but it is troublesome, and not much better than the mouth, if any at all. These efforts may be repeated twenty or thirty times if necessary, or even more. In some cases it is requisite to continue using some, or all of these means, for an hour or two without intermission, before the child begins to breathe freely. I knew an instance even, where the nurse continued to do so for five hours, and at last fully recovered the child, though all present, including the doctor, had[248] given it up. She said she did not despair while it continued warm, though it was doubtful whether the heart beat or not. This may show that the attempt should not be abandoned too soon.
In cases of asphyxia no blood should be lost at all, but on the contrary the cord should be carefully examined to see if it is tied fast; the bleeding from it frequently aggravating the evil.
Congenital weakness.—Some children are born extremely weak, and remain constantly debilitated and cold. This is very apt to be the case when they are born before the full term, or when the mother is diseased. They should be carefully wrapped in cotton, or very soft flannel, and kept warm by bottles of warm water. Many instances are on record of these weak children becoming afterwards extremely robust, so that they need not be regarded with unmixed apprehension, nor neglected from a supposition that they must die.
The child may be deformed.—The accoucheur should also carefully examine the child, to see if it be deformed in any way, or has met with any accident, because in some of these cases assistance is required immediately, and may be rendered at once.
The child's capability of endurance.—The capability of the new-born infant to endure extremes of cold is almost as great as that of its mother, and sometimes even it is benefitted by them. With many persons it is customary to plunge it in cold water, immediately when born; and in Russia, we are told, it is even rolled in the snow. In some cases these extremes may be beneficial, but in others I have no doubt they prove fatal. A medium course is best, in most instances, leaving the extreme to be resorted to when we wish a sudden stimulus.
When all these matters are carefully attended to, and both mother and child have remained for an hour or two without any unpleasant symptom, they may be left to the care of the ordinary attendants, giving them strict orders to send for proper assistance immediately, if anything unusual transpires.
The Bladder.—One of the most important points to attend to is the urine. A few hours after the delivery is fully effected, unless the female is reposing, she should be asked whether she has any desire to urinate; and, if she has, the convenience should be at once afforded to do so. There is always more or less danger of retention of urine, from the pressure that has been exerted on the bladder; and if it be allowed to continue too long its removal becomes exceedingly difficult. If on making the attempt the urine does not flow, the catheter must be used, and the sooner the better. The pain arising from retention of the urine has often been supposed to arise from inflammation of the womb, or bowels—neither patient nor physician knowing its real source, till the passage by the catheter gave relief. There have even been instances of females dying, merely from an overcharged bladder, while their attendants were industriously treating them for uterine inflammation. This accident therefore, should always be suspected, and a very little attention will prevent any mistake in regard to it. When allowed to become too full the swollen bladder may be felt, just above the pubes, hard and tender, so that the least pressure upon it causes great pain. If not relieved it will at last burst.
The Bowels.—If the bowels are not opened naturally, it will be well, the following day, to administer an injection of thin starch and water, or to prescribe a small dose of castor oil, or a seidlitz powder. This should also be repeated for two or three days, till the natural power is restored.
The Food.—But little solid food should be taken, and nothing stimulating. Gruel, milk, toast and water, Indian meal, light puddings, or broth, should be the chief articles for some time. Roast apples are also very good, being pleasant and relaxing. For refreshing drinks, if there be any fever, lemonade or tamarind tea may be taken.
The After Pains.—After the expulsion of the after-birth most females experience, more or less, severe pains, almost like those of labor, arising apparently from the further contraction of the uterine walls to expel the coagulated blood. These pains are seldom or never felt in first labors, but afterwards they are often most acute. I have known many patients suffer much more from them than they did during labor. They sometimes last only a few hours, or a day, and sometimes even extend to six or eight days. Nothing that we know of can prevent them, though many means are known of mitigating their severity. If there be no tendency to flooding, a large poultice may be placed over the abdomen, or it may be fomented, or covered with cloths wrung out in hot water. An injection may also be used, either in the Vagina or Rectum, consisting of warm thin starch, with about twenty drops of laudanum; or either of the following recipes may be used internally:—Pills of Gum Camphor, two, about the size of ordinary pills, to be repeated, if necessary, in an hour.—Or, Syrup of Poppies, two[251] drachms; Mucilage of Gum Arabic, two ounces; and Solution of Sulphate of Morphia, ten drops; to be made into a mixture, one-half of which may be taken at first, and the remainder in two hours, if the patient is not relieved. This seldom fails.—It is necessary to bear in mind that the pains arising from inflammation have been mistaken for ordinary after-pains, and serious consequences have resulted from the error. The after-pains however, are concentrated, and intermittent, while the sensations from inflammation are more diffused and constant, and are also usually attended by fever.
The Lochial Discharge.—From the time of delivery until the uterus has returned to its ordinary condition, there is poured from it a discharge, at first like blood, and afterwards thin and light colored, called the Lochia. The duration of this discharge varies from one week to a month, and its quantity from one ounce to six or eight ounces, daily. It gradually diminishes however, and frequently stops for a few days altogether. In women who do not nurse it is both more abundant, and lasts longer, than in those who do. The bloody color usually disappears after the first or second day, though sometimes it will show itself again, even when the discharge has nearly ceased, particularly if the female exert herself too soon.
It appears that this discharge is essential to health, and great attention should therefore be bestowed on the patient, if it be too small, or cease too soon, or too suddenly. In most cases it ceases naturally during the milk fever, and of course its disappearance then need not excite alarm. Sometimes also, it does not attain its full quantity till some days after its commencement. If however, it remains small past the[252] third day, or does not appear when the milk fever is over, means should be taken for increasing it. The best means for this purpose are warm poultices and fomentations over the abdomen, and injections in the rectum of simple warm water. Some practitioners advise two drachms of powdered Camphor to be sprinkled on each poultice, and probably it is an excellent addition. Occasionally the lochia is very offensive, and in that case a simple cleansing injection may be frequently used of thin starch, or Chammomile tea.
During the whole period of the Lochia in fact, even in ordinary cases, the female will be all the more comfortable, and better, for an occasional injection, and frequent washing. This is very much neglected, though it never ought to be so. The only care required is not to expose her to cold, which is quite unnecessary.
The Milk Fever.—About the second or third day there usually commences a peculiar temporary excitement in the system, called the milk fever, which requires to be described because it may be confounded with something more serious. It is generally ushered in by headache, flushed face, and a hot dry skin; the pulse beats slowly, and the breasts become hard, while the veins upon them appear very full. In a short time however, the pulse becomes quicker, a perspiration breaks out, and the breasts become still larger and fuller, so that the female can scarcely bring her arms to her body. These symptoms last about a day, or two days at most, and seldom become much aggravated.
Occasionally the milk fever is preceded by a slight chill, or by a furred tongue, or sick stomach, but not very frequently.
The precise causes of this temporary fever are unknown, though probably it is connected with the full establishment of the secretion of milk, and hence its name. It is seldom very severe in those who nurse, and frequently does not appear at all. During its continuance, and for some time after, the female must carefully avoid exposure to cold, and keep herself quiet; her diet should also be rather restricted, and light and unstimulating. An occasional seidlitz powder may also be of service, or a simple injection.
Making the Bed.—It is not customary to disturb the female, for the purpose of making her bed, till the milk fever is passed; or, if that does not appear, till the tenth or twelfth day; and then it should be done with care, and so as not to expose her unnecessarily.
First sitting up, and Going out.—This must of course be determined more by the condition of the patient, and the state of the weather, than by any rules. It may be as well to remark however, no matter how the patient may feel, that the first attempt should always be made with care. Very frequently she thinks herself stronger, and more capable, than she really is, and premature or undue exertion may do great injury. In most cases the female is allowed to rise within the first week, and sit for a short time in an arm chair; after which she begins to walk slowly about the room. The first going out is fixed, by fashion, at one month. Many females however, are unfit to leave the house till long after that time, and others should by no means be confined to it so long. Of course these proceedings should depend, as already remarked, upon the patient's strength and inclinations, and upon the state[254] of the weather, and not upon any fashionable observances. Some females are quite able to rise, and even walk out, in a few days, with benefit to themselves; and it exhibits as great a want of correct feeling, or common sense, for any one to make disparaging remarks on them for their early appearance, as it would if they were to blame the poor invalid for keeping her bed.
The apartment should be kept constantly well ventilated, particularly if the female is confined to it, and all soiled linen, or other sources of foul air, should be removed as quickly as possible. There is reason to believe that inattention to this, and to properly cleansing the person of the female, frequently produces child-bed fever.
Attentions to the Child.—If the infant's bowels are not opened by the end of the first day it should have a little sugar, or molasses and water, given to it, and if this does not succeed about half a tea-spoonful of syrup of Rhubarb may be added. This is however but seldom needed, if it be put to the breast within a few hours, as the first secretion of the milk possesses sufficient laxative power itself. It should also be observed whether it has urinated, and if not it should be placed in a warm bath immediately.
Some persons prefer to let the child wait till the milk fever is established, before they let it nurse, but this is very improper. The early feeding does it no good, and the purgatives it requires are injurious. As soon as the female is sufficiently reposed, if there is nothing special to forbid it, the child should go to the breast.
Sometimes the child will remain sleepy and dull, and not seem to require food at all, for several days, and even die at last of starvation, unless aroused.[255] If this lethargy continues it should be put in a warm bath, and afterwards well rubbed, while a little sugar and water is poured down its throat. These attentions may be required to be repeated for some time.
About the fourth or fifth day the portion of the cord above the knot usually separates and falls off, if it has not already done so. If the navel is inflamed, or suppurates, a little simple ointment may be rubbed on, and it should be regularly and carefully washed. In some infants it swells out very much, in which case a pad should be made of soft linen, and laid upon it, over which the ordinary bandage may be drawn. The complete healing of the part does not occur till about the twelfth day, and the bandage must be carefully worn till then at least, and is better continued a little longer, particularly if there is any swelling, or if the child cries much, or strains.
From the explanations given above of an ordinary natural labor, it will be evident that but little manual assistance is required, either to the mother or the child, and also what really is called for is of so simple a character as to be easily rendered. It would undoubtedly be improper, and cruel, to leave females at such times without aid altogether; but it is also equally improper and injurious to interfere too much. Excepting in cases of disease and deformity, or of very unfavorable presentations of the fœtus, Nature herself will nearly always effect the delivery; and much better, in most cases, when left to herself. Numerous females and infants have been killed, and still more have been grievously injured for life, by[256] rude and uncalled for manipulations; so that it has been a question with some accoucheurs, of great experience, whether as many would die, or seriously suffer, from receiving no assistance, as do now from being improperly handled. Without going so far, it is undoubtedly true that great mischief is done in this way, which can only be prevented by both accoucheur and patient bearing in mind that Nature herself is usually competent, and at most only requires skillful and gentle assistance. Some practitioners seem to think that labor is a mere mechanical process, like the removal of a block of stone, and hence they depend altogether upon force; overlooking altogether the wonderful vital powers inherent in the system, which operate with such certainty, and yet so safely; and which frequently succeed of themselves when brute force is completely foiled.
The nature of the assistance proper to be given, in any particular stage of labor, will be evident on inspecting the structure of those parts, of both mother and child, which are brought in connection at the time, and by considering how their mutual relations require to be changed and modified. If those relations are already such as are required, and the system retains sufficient force, nothing can be done with any advantage—we must wait, and let Nature operate herself. Even many unfavorable conditions may be spontaneously corrected, and it should always be a matter of consideration, when the means of assistance are not very obvious, whether it will not be better to rely upon the natural powers than to interfere. Great evil has resulted from teaching females that labor cannot terminate, safely, without a great deal of assistance, which can only be rendered properly by those who possess a vast amount[257] of skill and experience. They are thus led to think themselves totally dependent upon the accoucheur, and many of them actually seem to believe that he is as necessary to deliver the child as a dentist is to extract a bad tooth. If they were better informed they would feel more confidence in their own natural powers, and would not be so unnecessarily alarmed when unforeseen difficulties occur, or when professional aid cannot be immediately procured.
In most cases there is more danger after the labor is over, from puerperal fever, various local inflammations and other causes, than there was during its progress. Indeed the real danger may be said properly to commence several days after, and the physician is really needed then more than at the time.
PROTRACTED AND DIFFICULT LABORS.
The causes which may impede a labor, and increase its difficulties, are numerous, and they are of several different kinds—some depending upon the mother, and others upon the child. Some of these may be easily removed, or modified, but others present more serious difficulty. It is therefore necessary to enumerate and explain them separately.
A labor is usually called protracted or difficult, if the head presents, when it is not completed in about twenty-four hours from its actual commencement. There are many labors however, that last much longer, and yet terminate quite favorably, and many that are over much sooner and yet are very difficult. Still, generally speaking, the danger and difficulty increases as the time progresses, and it is seldom prolonged beyond twenty-four hours without serious inconvenience.
It appears, from the statistics of the Dublin Lying-in Hospital, that in seventy-eight thousand deliveries, one out of every ninety-two of the mothers died, and one out of every eighteen of the children was stillborn. Of those mothers who were in labor with first children, from thirty to forty hours, one in every thirty-four died, and one child in every five was stillborn. Of those who were in labor from forty to fifty hours, one died in every thirteen. Of those who were in labor from fifty to sixty hours, one died in every eleven. And of those who were in labor from sixty to seventy hours, one died in every eight, and nearly one-half of the children. It is evident therefore that, as a general rule, the danger increases with the length of time.
This is most likely to occur in delicate females, and in those who are debilitated by disease. The contractions are very feeble, and, as the nurses say do not tell; the mouth of the womb dilates but slowly, and the head descends with difficulty into the passage.
In many cases in fact the labor is so tedious, from this cause, that the female becomes completely worn out, and finally sinks, while the child is exposed to the greatest hazard from the delay.
It is in these cases that the patient's strength needs supporting, and that stimulants may be useful. A little wine, or brandy and water, will often rouse the failing energies, and bring on a series of strong contractions that will end the labor at once.
The most usual resort however is to the drug called Ergot, or Secale Cornutum, a fungus growth which is sometimes found on ears of rye. This possesses the peculiar property of exciting the womb to contract, the same as an emetic excites the stomach to vomit, and it seldom fails in its effect; but still there are many objections to its use. It not unfrequently causes delirium, great restlessness, and anxiety, sickness, headache, and convulsions, or complete prostration, from which the female may be long in recovering. It is also supposed by some to[261] be not altogether free from danger to the child. If however no other means were known of making the womb contract, in such cases, all the probable evils should be risked, because the labor must be completed at all hazards; but other means are known, which succeed even more certainly than ergot, and without any danger. The application of Galvanism, explained in my "Neuropathy," and "Practical Facts," will almost invariably cause the womb to contract, and speedily bring the labor to a safe termination, without the slightest risk or inconvenience, to either mother or child. Simple friction over the abdomen will also succeed in many cases, and gently rubbing the mouth of the womb with the finger in others. These simple means should therefore always be used in preference to the ergot, but in case they cannot be resorted to, or fail, the drug must be administered, and I will therefore explain the manner in which this is done. When gathered the ergot is in large irregular lumps, and should be so kept. When wanted for use a single drachm should be finely powdered, and divided into three parts; one of these parts to be taken first in a glass of sugar and water, and the others at intervals of ten minutes, unless the effects of the first are very powerful. It is often thrown from the stomach however even in still smaller quantities, and is then given, by some, as an injection by the rectum, in which mode it seems more powerful, so that a smaller dose is sufficient.
Great caution should always be observed in using this powerful drug, as it will sometimes act so energetically as to burst the womb; or expel the child so suddenly as to lacerate the perineum and other parts. The contractions produced by it are different from the natural ones, being almost constant, without any[262] interval, and gradually increasing in force. They usually come on in about ten or fifteen minutes after the last dose, and continue about an hour and a half. Some practitioners depend almost altogether on the ergot, in every protracted case, and even use it to bring on premature labor, when that is required. Thus M. P. Dubois was once called to a dwarf, whom he delivered with instruments, the first time, but with great difficulty and risk. The next time she became pregnant he determined to bring on premature labor, and accordingly he administered ergot, when she was about eight months gone. This brought on natural labor, and she was delivered without difficulty. M. Chailly says he believes it will bring on uterine contraction at any time, and that he has never known it to fail. I consider however that there is always more or less risk in its use, and I should certainly prefer any of the other means, particularly Galvanism.
It is of the first importance however to be certain, before using any forcing means whatever, that there is no physical impediment. If the pelvis should be deformed or small, if the child's head should be unusually large, or dropsical, or if the soft parts of the mother should be undilated and rigid, the most serious consequences must ensue from violent uterine contractions. In like manner if the presentation be unfavorable, particularly if it be one of the trunk, the danger is equally great. In every case the passage of the child must be physically possible, before it is attempted to force it away. A neglect of this rule has frequently led to fatal results. The ergot has been given and the uterus forced to contract, while the pelvis was too small for the child to pass through; and the consequence has been rupture of[263] the uterus, or complete exhaustion, with death to both mother and infant. In other cases the delivery has resulted so suddenly, from the violence of the expulsive efforts, that the vagina and perineum have been lacerated in the most shocking manner.
The ergot is also especially dangerous to very nervous women, or to those who are disposed to congestion, apoplexy, or inflammation.
Among the special causes which often paralyze the action of the womb, may be mentioned a full habit of body, great distention of the uterus from accumulations of fluid, and extreme thickness of the membranes. In some cases in fact, the membranes will be so strong that the most violent contractions fail to break them, and the uterus completely exhausts itself to no purpose. It is in such cases as these, when the mouth of the womb is fully dilated, that the accoucheur should rupture the membranes artificially. This is usually done with the finger nail by pinching them. Some practitioners however use a pointed instrument, or a sharp quill; but there is always more or less danger of injuring the child or the mother by such means. The best time for breaking them is during a strong pain, when they are fully distended. The mere scratching, or pushing on them will frequently suffice. I have known cases however in which they were so strong that an instrument was actually necessary to open them.
The death of the infant also seems sometimes to check uterine contraction, though probably not from the mere circumstance of its being dead, but because the womb suffers from the same morbid cause which produced its death.
Any strong moral impression may also produce the same state of things. Thus in some females the[264] womb will instantly cease its contractions, and the labor be arrested, from fright, or from strong repugnance to somebody, or something, in the room. Instances have been known of women being so alarmed on first seeing the accoucheur, or so displeased because he was not the one they wished, that the uterine efforts immediately ceased, and could not be again brought on for a long time. The presence of some person who is a subject of dislike may also have a very prejudicial effect, and if this is known they should be immediately removed. Dr. Merriman tells us of a female who was seized with a fit, from which she died, simply from seeing a strange doctor enter the room.
Whatever may be the cause which paralyzes the action of the womb we should endeavor, if possible, to discover and remove it. If however it be beyond our reach, the patient's strength must be supported as much as possible, and the simplest means of exciting the contractions tried first; if these fail the more powerful ones must be tried, always preferring the safest. Finally, if all fail, the hand must be introduced into the womb, the child turned, and brought away by the feet; or the forceps must be used if absolutely necessary.
Sometimes the mouth of the womb or other soft parts, will not give way, but remain obstinately rigid, so as to render the continued expulsive efforts of the womb of no avail. If this state continues too long the parts become swollen, hot, and dry, and extremely painful, so that the slightest touch causes[265] acute suffering. The abdomen also becomes exquisitely tender, fever sets in, with cold sweats, the head begins to wander, the features express great anxiety and suffering, and the voice alters so that it can scarcely be recognized. These symptoms will sometimes be established, and become rapidly worse in a remarkably short time, so that the patient will appear to pass suddenly from a condition of comparative ease and safety to one of extreme peril and suffering. The child also suffers in an equal degree, the continued pressure upon its head having a most injurious effect. The bones overlap to a great distance, the scalp is engorged with fluid, and all its blood-vessels are ready to burst; the brain is severely compressed; the circulation in it is suspended, and apoplexy frequently ensues. Even when one of these protracted cases eventually terminates without immediate mischief, there is much subsequent evil to be feared. The bruised parts frequently slough away, so that fistulas are formed, and the whole remain so permanently weak that they can never afterwards retain their places.
The most usual resort in these cases of obstinate rigidity is blood-letting. This frequently induces relaxation immediately, and also checks the tendency to inflammation and fever. In many cases however, if not in all, it may be dispensed with, and should always be so if possible. Very frequently it produces as much evil as good, by alarming the patient, and by creating a debility which cannot afterwards be removed. Simple warm fomentations will often make the rigid parts give way; and so will lubricating them with soothing ointment, or better still anointing them with the Extract of Belladonna. This frequently acts like a charm, and opens the rigid os[266] tincæ in a few minutes. Injections of thin starch and laudanum are also excellent, and may be advantageously administered before applying the Belladonna. The Galvanic Battery may also be employed, it having induced relaxation in many cases, when all other means failed; as will be seen by the cases quoted in "Practical Facts."
If the labor really does progress though slowly, it is generally best to have patience and let it take its course. If however the patient is likely to sink before it is completed, or if it is at a stand still, and cannot be accelerated, artificial delivery may be necessary. It is seldom however that all of the above mentioned means fail.
Sometimes the womb is so much inclined in a particular direction that its mouth does not present to the middle of the passage. Thus it may lean over so much to the right side that the mouth may open against the left wall of the Pelvis; or it may lean to the left side, or to the front. In all these cases the expulsion of the child may be totally prevented, because it is forced against the walls of the passage instead of down its axis.
Obliquity is sometimes righted spontaneously, but more frequently it requires the interference of art. The mode of rendering assistance is to support the womb on the side to which it falls, particularly during the pains, so that its mouth may be directed towards the middle of the passage.
Falling of the womb may retard labor, but is not likely to make it more than usually difficult, nor dangerous. It is requisite, however to bear in mind that the head of the child may, by this displacement, be found in the vagina, and even at the vulva, before it has passed through the mouth of the womb, because the neck itself is already in the passage. The head may therefore be felt low down, and the accoucheur may think the labor will soon be completed, when in reality it has scarcely begun. In such cases it merely requires patience and non-interference.
In my work on the Diseases of Women, will be found many curious cases of pregnancy and delivery, occurring during partial or complete prolapsus uteri; and also much information regarding obliquity, and other similar derangements.
These constitute by far the most serious obstacles to delivery, and are most to be dreaded. In treating upon them it will be first necessary to explain the chief kinds of deformities, and the cause from which they arise, after which it can be shown how they interfere with the progress of labor, and how they can be best remedied.
Deformities of the pelvis may either be congenital, or they may be produced by certain diseases in after life, and also by bad physical education. The principal causes however are two diseases, Rachitis, or Rickets, and Malacosteon, called also Mollites Ossium, or softening of the bones. Rachitis usually attacks children somewhere between nine months and two[268] years of age, and produces a variety of well marked symptoms; such as large head and belly, protrusion of the breast-bone, flattening of the ribs, emaciation of the limbs, and various deformities of the bones. The patient may recover from the disease, but the deformity of the bones often remains, and therefore no female should become pregnant, who has had rickets, till the shape and dimensions of her pelvis are known, or it may cost her life.
Malacosteon or softening of the bones, may come on at any period of life, and frequently occurs without any serious constitutional disturbance. It consists in a gradual absorption from the bones of all their solid matter, so that they become soft, and may be bent or twisted like horn. Sometimes this state will be reached very soon, but at other times the disease progresses very slowly. The causes of it are unknown, and it is incurable. I have seen a patient who could bend the bone of her leg nearly double, as if it were a piece of rope.
In my work on the Diseases of Woman, I have spoken upon various other causes which may deform the bones in young females, such as wearing corsets, improper attitudes in sitting, and want of sufficient unconstrained exertion of the body in the open air.
The deformities may be of various kinds, and may either alter the general appearance and the walk, or may not be discoverable except on examination. Sometimes the pelvis is too large, so that the womb and other parts are continually falling down into its cavity, but this is very rarely seen; more frequently it is either too small, or irregular in its form.
In all cases where the irregularity in form, or diminution in size, is such as to prevent the passage[269] of the child an operation becomes necessary, either upon the mother or her infant, and great danger is consequently incurred by both.
It is therefore the duty of every mother, if she has the slightest suspicion that her daughter is deformed, though it may not be apparent, to have her examined before she is allowed to marry. Many have lost their lives for want of this precaution. Severe blows or falls in early life may also create a pelvic deformity, and this, as a possible consequence of such accidents, should always be borne in mind. The means by which the form and size of the pelvis are ascertained, as before stated, are simple, and such as need not in any way be feared.
To enumerate all the varieties of deformed pelvis, as described by different authors, is unnecessary, and would not be useful here. I shall therefore only refer to them generally. Sometimes the pelvis is regular enough in its form, but singularly small altogether, not larger perhaps than that of a child eight or nine years of age. More frequently, however one part only is small, while the others are full sized, or the different parts are not in a proper position in regard to each other. Thus sometimes the pubic bones will be flattened backward, near to the sacrum, so as to narrow the antero posterior diameter of the upper strait; at other times one of the sides will be flattened towards the other, as if crushed in, and thus diminish all the diameters; and at other times one side will sink down lower than the other, and thus effect similar changes in another way.
By referring to the description of the perfect pelvis, given in the early part of the work, the nature of these changes will be readily understood, particularly if the plates given there are compared with those given here.
PLATE XL.
Represents the standard form, with which the rest must be compared.
PLATE XLI.
Represents a pelvis which resembles that of the male in its form, and is therefore called masculine. It is deeper, and less capacious altogether than the standard one. This form is occasionally met with in females of a peculiar general conformation, and temperament, approaching that of the other sex. It is not a sufficient deviation from the natural form to create any great difficulty, though it may cause delay.
PLATE XLII.
Represents the peculiar deformity most frequently produced by Mollites Ossium. The different parts are stretched out as it were, and crushed inwards toward each other. The size of each strait is diminished in nearly every diameter, and the whole form is very unfavorable to delivery. This is sometimes called a cordiform pelvis. Observe the difference between it and the standard one.
PLATE XLIII.
This is called an Ovate Pelvis. It appears as if it had been crushed by a heavy weight, from above downward, the sacrum being depressed below the plane of the pubes. In this case the antero posterior diameter of the upper strait is so much lessened that the two halves appear nearly separated, and form almost a figure of eight (8).
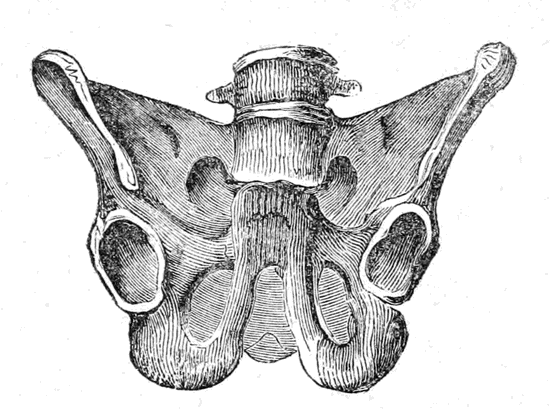
Plate XLII.
Represents the peculiar deformity most frequently produced by Mollites Ossium.
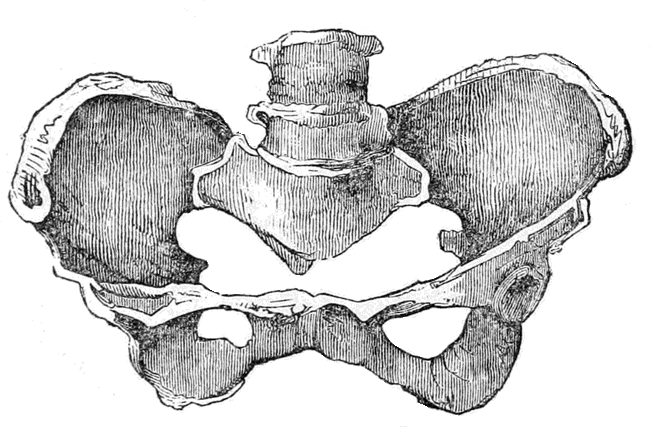
Plate XLIII.
This is called an Ovate Pelvis.
PLATE XLIV.
This is another kind of deformity, in which one side is sunk down below the other, while both are twisted as it were round the sacrum.
PLATE XLV.
This is a section of a Pelvis to show the effect of a corroding disease of another kind. The whole of this is such a mass of disease and deformity as to preclude any particular description.
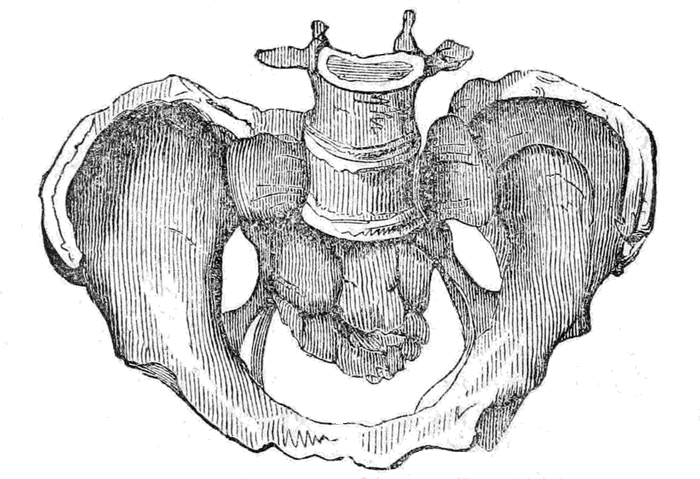
Plate XLIV.
This is another deformity, in which one side is sunk below the other, and both twisted round the sacrum.
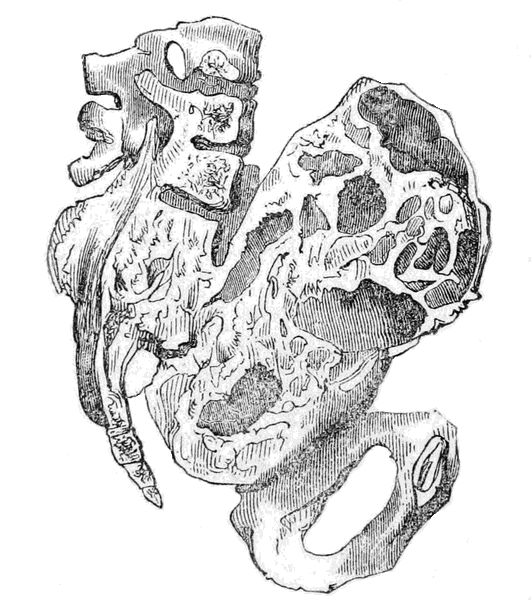
Plate XLV.
The effect of corroding disease.
Curvature of the spine sometimes affects the pelvis, when low down, and therefore if any female is affected with it she should not marry before being examined. Several diseases and lesions of the hip-joint, and of the thigh, may also do the same, and should therefore be suspected.
In the great majority of cases, deformities of the pelvis remain unknown, till the period of delivery, and all that can be then done is to combat in the best possible way the difficulties they create. It is evident that the amount of difficulty depends entirely on the disproportion between the head of the child, and the passage through which it has to be born. If the head be large and the passage small the difficulty will be greatest, but if the head be small it may pass through the pelvis though under its average size. The development of the head cannot be ascertained however, before birth, except when it is unusually large from dropsy, and it is therefore always assumed to be of an average development, and the pelvis is compared accordingly.
The kind of assistance required in these cases depends chiefly on the measure of the pelvic diameters, though it may be modified somewhat by other considerations.
When the smallest diameter of the pelvis measures from three inches and a half to three inches, it is customary to leave the expulsion of the fœtus to nature, and it is generally effected, though slowly and with difficulty. If however the patient becomes exhausted, or the head be unusually large, the forceps are generally used after waiting five or six hours. In these cases the head often becomes firmly fixed in the upper strait, so that great force is needed to dislodge it. The upper part passes through, owing to[282] the overlapping of the bones, and the scalp then bulges out like a large tumor, from being engorged with blood and serum, but the lower being more unyielding remains behind. It is therefore impossible for the head to move either way, as it is formed like a figure 8, and held by the narrow part, as will be seen by the following plate.
PLATE XLVI.
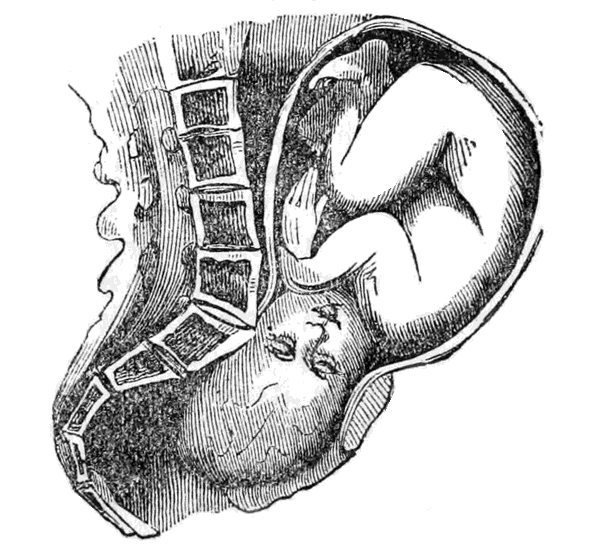
This Plate represents the head fixed, or impacted, at the upper strait of a narrow pelvis.
When the smallest diameter is not more than from three inches to two and a half, the birth is sometimes effected by nature, but with extreme difficulty. The accoucheur waits four or five hours, as in the former case, and then if no progress is made he applies the forceps, using great care in doing so. If the extraction is found impossible, with reasonable force, the head must be opened and made smaller, even[283] though the child be living, because it is more proper to sacrifice it than to risk the life of the mother. In a case like this however, no one person would like to decide, unless in a great emergency; there should always be a consultation if possible.
A dwarf, named Lepratt, who used to perform at the theatres, was delivered with the forceps by M. Dubois, though the pelvis only measured three inches. She perfectly recovered, though the child was born dead: it was of fair average size.
It is contended by some that the delivery may be effected, under peculiarly favorable circumstances, when the passage measures only two and a half inches, and at all events the effort should be made; but for the sake of the mother such cases should not be left long, as the chance is so small, and the risk of delay so great. When the passage is less than two and a half inches, spontaneous or artificial delivery is allowed to be impossible, and the only alternatives then are to dismember the child or open the mother. Which of these should be done depends on circumstances. Whenever the child can be brought away by the natural passages, though it be piecemeal, it always is so brought, unless the danger to the mother be greater than by the cesarian operation, in which case that operation is resorted to. By means of an instrument called the Cephalotribe, which crushes the head, the child may be brought away, unless very large, when the pelvis only measures two inches. When the passage is less than two inches, the only resort is to the cesarean operation, which sometimes succeeds, and saves both mother and child, though more frequently the mother sinks.
The necessity for all these frightful operations is now much less than formerly, and may be done away[284] with altogether. This important fact should be known universally, and also the means to be resorted to. In the first place, every young female should be examined, before marriage, by a competent person, if there be the slightest reason to suspect deformity; and in case the deformity is found to exist, the consequences if she becomes pregnant, must be laid before her. If, after being told this, she will marry, or has already done so, the means of avoiding conception should be placed at her disposal, so that she may not be made, of necessity, a helpless victim. These means need not be described here, though I have no hesitation in referring to them. When I know that the life, or life-long health, of a female, depends on her not becoming pregnant, I consider it my duty to put such means at her disposal, if she desires it. In many instances I have known females suffer, several times, the most frightful tortures, merely to bring into the world the mangled fragments of a dismembered child, with the greatest risk to their own lives; and in others I have known them in constant dread of becoming pregnant, because they were conscious it would be their death warrant. In such cases I leave it to humanity, and common sense, as to whether such information should be withheld? I could not reconcile it with my notions of duty to withhold it.
In case pregnancy has occurred before the deformity is discovered, and it is then found that a full grown child cannot be born, premature delivery must be brought on; or, in other words, the Uterus must be made to expel the child before the full term, while it is yet small enough to pass through the Pelvis. This operation is of course only allowable when needed to preserve life, or to escape great suffering and danger. It must always be decided[285] upon by the medical man, and performed by him, so that a description of it is uncalled for here. In Europe it is quite common, and nothing has tended so much to do away with those disgusting and horrid operations, on mother and child, which were formerly absolutely necessary in cases of deformity. If it is found at the first delivery of a female, or before, that she cannot bear a living child at full term, artificial delivery is accomplished at seven or eight months, thus avoiding all the danger to the mother, and frequently preserving the child. In the case of the dwarf before referred to, when she became pregnant the second time, M. Dubois brought on premature delivery, and the child was born alive, with but little difficulty. According to statistics it appears that, when artificial premature delivery has been induced, in one hundred and sixty-one cases only eight mothers have died, and all but forty-six of the infants were born alive. Of the whole number of children seventy-three continued to live; and of the eight mothers five died from other causes, leaving but three whose death resulted from the operation. Now when the fearful number of deaths from instruments, and other operations, necessary at full term, is recollected, the advantage of this practice will be evident. In the Cesarian operation for instance, which is often the only remaining resort, but one female out of six recovers.
The delivery should be postponed as long as possible, so as to give the best chance for the child living. This must of course be decided upon after the size of the pelvis is ascertained. Seven months is the earliest time at which the fœtus is viable, and it is much better left till eight, if the size of the parts will allow of its birth then. In case they are so[286] small that it cannot be born even at seven months, we have our choice, as M. Chailly remarks, between the dreadful Cesarian operation at full term, and producing early miscarriage.
M. Dubois seems to recommend premature delivery in nearly all cases, if the smallest diameter is under three inches; because, as he remarks, spontaneous delivery at full term is then a very rare exception, and the danger and suffering to the mother is so great. He also recommends it when there are tumors, and even when the female is afflicted with any acute disease. Of course it is always necessary, before operating, to be sure that the child is alive.
I knew a lady myself who had given birth, at full term, to seven children, all of which were torn from her with instruments, dead, owing to the smallness of the pelvis. When pregnant with the eighth, premature delivery was brought on, at my suggestion, at about seven months and a half. The fœtus was born with comparative ease, and lived. But for this operation she probably would never have been blessed with a living child at all. Since then she has avoided conception.
Tumors of various kinds are met with, both in the bones of the pelvis and attached to the soft parts. They frequently offer the most serious impediments to delivery, and baffle the skill of the most experienced obstetricians. In fact they differ so much in their structure, their size, and their situation, that but few general directions can be given as to their management. In every case where one exists pregnancy[287] should never occur, if possible to be prevented, before it is removed; for though it may cause no inconvenience at other times, yet during delivery it may necessitate very serious operations, or even cause death. Some of these tumors are mere vesicles, or bags, filled with fluid, and may be punctured and their contents let out, so as to make them less. Others are more or less solid but moveable, and may often be supported above the upper strait till after the child is born. When they are so large as to block up the passage, and are either fixed or cannot be carried up into the Womb, there is often no other choice than to either cut them out or open the child's head; the practice being determined by the circumstances of the case. In some instances the bladder itself, distended with urine, has impeded delivery, and been mistaken for a tumor; and in other instances stones in the bladder have caused the same error.
A specimen of one of these tumors is represented in Plate XLVII, and one of a Polypus in Plate XLVIII.
PLATE XLVII.
This represents an Ovarian Tumor, which has descended before the head of the child, and completely blocked up the passage. The delivery, it will be seen, is utterly impossible in such a case, unless the Tumor can either be pushed away, or reduced in size.
PLATE XLVIII.
This Plate represents a case which occurred in the practice of Dr. Ramsbotham, and which terminated favorably. The polypus had a very long neck, and was forced out of the external opening by the child, which was then born with ease. I once saw a case myself, in which the labor was completely arrested by a large hard tumor about the middle of the Vagina; it could not be moved, and delivery was evidently impossible while it remained. In consultation it was decided to cut it out, as there seemed but little circulation of blood in it, and its situation was favorable for the operation. This was accordingly done with but little trouble, and the child was born without difficulty in about twenty minutes after. The mother perfectly recovered.
Sometimes tumors exist externally, on the lips, or in the Vulva, but as they seldom offer much obstruction, and are easily detected and managed, but little need be said about them. They should always however be attended to, if discovered, before labor comes on, or better still before pregnancy.
In some instances the veins around the Vulva become much enlarged, and resemble tumors, and sometimes even impede delivery. It is usual then to open them, and let out the blood, but not till the head is sufficiently low to press upon it and prevent dangerous bleeding.
The Vagina may be partly closed by its sides growing together, or it may be united by bands and membranes stretching across; and these obstructions may be sufficient to impede or prevent delivery. Most usually they give way, and are gradually broken down by the pressure of the child's head; but if they prove too strong, after waiting a reasonable time, they must be cut through. Cases have even been known in which the hymen has been found perfect at delivery, and even offered considerable resistance, so as to necessitate its being cut through before the child could be born. In such cases this membrane is unusually strong, and conception occurs without its being broken.
When the perineum or Vulva remains rigid and hard, so that the opening cannot be enlarged sufficiently[296] for the child to pass, it may also be necessary to operate with the knife. But this should never be done till after every means of relaxation has been tried, and the head has been kept back as long as prudent. It is however, always better to open a passage than to let one be torn, because it may be made in the most favorable place. When the perineum is allowed to be torn, the most serious consequences often ensue, and the patient is made a miserable sufferer for life. The Vagina and Rectum may be torn into one, or the power of retaining the contents of the intestine, or bladder, may be for ever lost. When an incision is made none of these evils follow; the wound speedily heals, and in a little time no trace of it can be seen. It has even been necessary to cut the neck of the Womb, when it would not open, to prevent the organ from being ruptured; and this has been done with perfect safety. A celebrated practitioner in this city had to perform such an operation very recently, on a female who had injured herself, and made the mouth of the Womb grow together, by violent attempts to produce abortion. The delivery took place with comparative ease, and no unpleasant results whatever followed, either to the mother or the child.
This means the escape of a portion of the cord before the child itself. It is most frequent in the irregular presentations, as they do not so fully close up the mouth of the Womb, and it is most likely to occur at the commencement of labor, though not impossible at a later stage. Very often the cord descends when the membranes break, being carried down by the rush of the waters; and sometimes it is already in the sack, or bag, before the rupture takes place. This accident is comparatively frequent, being found to occur as often as once in about three hundred cases.
The causes which produce procidentia of the cord, are most likely these:—A large quantity of liquor amnii, and its sudden discharge,—Unnatural presentations,—Deformities of the superior strait of the Pelvis,—A very long cord,—and rupturing the membranes too early. But it may also happen from other causes with which we are unacquainted.
There is seldom much difficulty in detecting this accident, because if the membranes are broken it protrudes into the Vagina, and if they remain whole it can be felt within the sack, and its pulsation will[298] be quite distinct. Sometimes, it is true, it may be so firmly compressed, between the fœtus and the walls of the pelvis, that its pulsation may be very indistinct, or even totally suspended for a time; but this only necessitates a little extra care.
Procidentia of the cord may be very serious for the child; in fact, it is a frequent cause of its death. The reason of this will be evident when the functions of the cord are borne in mind. The circulation in it is as necessary for the life of the child before birth, as breathing is after, and when protruded first it can seldom escape being so pressed upon as to stop its circulation, and hence the danger. To the mother it makes no difference whatever, unless it be told and alarm her; or unless violent efforts are made to correct it. She had therefore better not know if it occurs.
If assistance is not rendered in this accident the consequences are almost always fatal to the child, though in some instances the cord has remained hanging from the Vulva several inches, for an hour or more, and still the infant has been saved.
If the fallen cord is detected before the membranes are broken, it may frequently be put back into the Womb without much difficulty. The accoucheur must wait till the mouth of the Womb is fully dilated, and then watch his opportunity, in an interval between two contractions, to push the cord upwards, between the fœtus and the uterine walls. If he succeeds in this, as is usually the case, he must then break the membranes during the next pain, and this will bring the presenting part at once into the upper strait, and so block up the passage. To effect this manœuvre it is requisite to introduce two or three fingers, and sometimes even the whole hand. It[299] must never be attempted till the mouth is fully dilated, otherwise the membranes may be ruptured too soon, and the delivery be delayed, thus increasing the danger.
After the rupture of the membranes the replacing of the cord becomes a much more difficult matter, and frequently cannot be effected at all; particularly if the head be descended far down. Every effort however must be made, and if unsuccessful the delivery should be hastened as much as possible. In many such cases the forceps are applied, and the child brought away at once, because every moment's delay increases the risk to its life.
Several different kinds of instruments have been invented to return the cord, but they are seldom at hand when needed, and none of them are so good as the hand itself.
If the return of the cord cannot be effected, and the progress of the labor will allow of it, the hand is introduced and the child turned, unless the position of the head will allow of the advantageous application of the forceps, in which case they are mostly resorted to. The only general rule is, to terminate the labor as speedily as possible, consistent with the welfare of the mother. In spite of all that can be done the pulsation is often found to cease, and when the child is born it is either quite dead or breathes but a few times.
A very frequent indication that the fœtus suffers from compression of the cord, is a greenish color of the water discharged, owing to the discharge of Meconium from the child's bowels. This is brought about, most probably, by its straining, and its efforts to relieve itself.
The cord is sometimes too short, and this may operate very unfavorably in many ways. It may keep the fœtus up in the Womb, and prevent it from descending to the bottom of the Vagina,—it may cause the placenta to be torn away too soon, and so lead to serious flooding,—it may pull down and invert the Womb,—or it may make the labor very tedious, and cause the death of the child.
Unfortunately there are but few signs of this accident, even after the rupture of the membranes, and none at all before, that can be depended upon. If the head has descended properly, and the parts be fully relaxed, but still the expulsion is delayed from no obvious cause, it may reasonably be supposed that shortness of the cord exists; and if so there is very soon given a proof of it by a discharge of blood. This is owing either to the breaking of the cord, or to the separation of the placenta, and is frequently the first intimation the assistant has of the accident. All that can be then done is, to conclude the delivery as soon as possible, and in the best way that circumstances will allow.
In some cases the cord is not too short absolutely, but is made so by being twined round the body or limbs of the child, which are often cut off by it. M. Tasil saw a case where the cord round the neck had nearly severed the head; and Montgomery gives several instances in which the limbs had been amputated in this way. Two of these are represented below:—
PLATE XLIX.
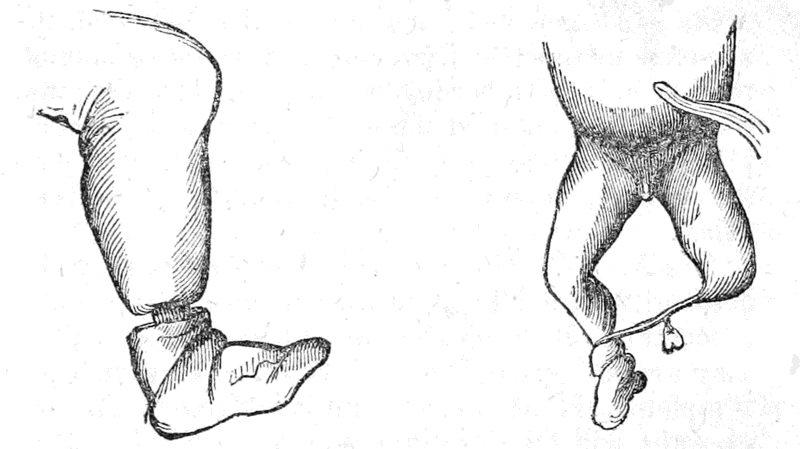
Limbs cut off by the Cord.
Occasionally the cord can be slipped over the head, or limbs, when wound round them, and the strain upon it be thus removed. If this cannot be done however, and the danger increases, relief may be obtained by cutting the cord, particularly if it be absolutely short. But this must not be done till everything indicates that the labor will probably soon terminate; and the end connected with the child must be carefully held, or tied.
One Arm.—The descent of one arm along with the head may cause some delay and difficulty, but Nature nearly always overcomes the impediment. It is seldom that the arm can be reduced, and therefore but little can be done at first; if the delivery be evidently arrested by it the accoucheur must at last assist in the most feasible manner. Sometimes even it is necessary for him to apply the forceps.
The Two Arms.—Even this difficulty is often[302] overcome spontaneously, though much more rarely than the former one. As soon as it is detected, the accoucheur must endeavor to return one or both of the limbs, if the labor has not proceeded too far; and if he cannot succeed the delivery must be accomplished as soon as possible, either by turning or with the forceps, unless there be reasonable ground for delay.
The Feet.—Either one or both of the feet may also descend with the head, at first, though they usually recede and allow the head to be born alone. When they are so impacted as to prevent the delivery being completed, the accoucheur must interfere. In most cases he will find it quite easy to push the feet above the head, and allow that to descend alone; but if this is not possible he must introduce one hand, grasp the feet with it, and pull them down, while the other pushes the head up. This will turn the child, and if it be in no immediate danger, and the mother is not suffering, the rest may be left to nature; but if the contrary is the case, the delivery must be finished as speedily as possible. When the head is very low down it may be necessary to use the forceps, but great care must be observed not to grasp the feet along with the head when using them.
A Foot and Arm.—The proceeding is the same as with the foot alone. If the limbs cannot be returned the head and arm must be pushed up, while the foot is brought down.
In most cases where there are two or more children the delivery is easier than with one, because they are generally small, and the first one so prepares the[303] way that the rest are born without difficulty. It is also a fact that twins are nearly always born before full term, and consequently are not quite grown.
The expulsion of the second fœtus usually takes place, immediately after the first, though sometimes the Womb stops contracting, and it is not born for half an hour or more, and it may even remain for hours or days. It is a question whether, in such a case, the second delivery should be left for Nature to finish, or whether the accoucheur should terminate it sooner artificially. The most general practice is to wait only about half an hour, and then, if the Womb is still inert, use friction, or other necessary means, to excite it, and accomplish the second delivery as soon as possible. If there be more than two the proceeding is still the same.
Some difficulties may arise however with twins, which it is necessary to be prepared for. Thus the two heads may come together, and mutually impede each other. In this case the one which moves the easiest must be pushed up till the other is descended sufficiently low. One head may also descend with one or two feet; in which case, if the feet cannot be returned, the head must be pushed up, and they must be brought down. The force exerted however, must not be very great at first, because one may belong to each of the children, and much injury may be done; a little gentle traction will soon detect this however, with ordinary care. If two arms, or one arm and a foot descend, the same care is also required, before pulling upon them, to ascertain that they are not parts of the two children. Sometimes when the head of one twin descends along with the feet of the other they may, if small, descend together. But if this is impossible, and interference is needed, we must first[304] try to push up the head; and if this cannot be done, it must be drawn upon, not the feet; because if the feet were drawn down the two children would soon occupy the passage together, body and head, and would perhaps become firmly wedged. In nearly every case one of the twins presents by the head and the other by the feet, as formerly shown.
Fœtus too large.—It is very rarely the case that the Fœtus is so large as not to pass easily through a well-formed Pelvis, though such cases have been known. The mode of proceeding is of course precisely the same as if the pelvis were too small. If no means will succeed in abstracting the Fœtus whole, it must be made less; but Nature should be first allowed full time to act with all her force.
Hydrocephalus.—This consists of an accumulation of water in the head of the child, and is usually termed watery head. The bones of the cranium will sometimes be widely separated by it, and the head be made so large that it cannot possibly be born till made less. The causes which produce this disease before birth are unknown.
In cases of hydrocephalus the head does not descend into the straits, owing to its size, and is felt to be full and firm, during a pain, but soft and yielding during the intervals, especially at the fontanelles and sutures, which are also very large. The bones are usually very wide asunder, or even totally separated, as if floating in the fluid.
In some cases, when the quantity of fluid is but small, the delivery may terminate spontaneously;[305] the head lengthening, from being so soft, and thus adapting itself to the size and form of the strait. Most frequently however, assistance is rendered in such cases, either by the forceps, which will sometimes succeed, or by puncturing the head, and letting out the fluid. This operation has been performed and the child saved, though such an occurrence can never be reasonably anticipated. Such instances however, show that great care should be taken not to injure the brain, as that would destroy the small chance there is.
Dropsy may also occur in the chest, or abdomen of the child, causing similar difficulty with dropsy of the head. If the natural or artificial expulsion of the child cannot be effected without, the part must be carefully punctured, and the fluid evacuated.
Tumors on the Fœtus.—Sometimes various kinds of tumors form on the child's body, but they are rarely so large as to prevent delivery, though they may delay it. If they should be too large however, it will be necessary to remove them, as in the case of tumors in the Pelvis.
Occasionally the bones of the head will be so hard, and so closely united, that they will not overlap, in which case the labor may be very difficult, unless the head is small, or the pelvis very large. If after waiting a reasonable time, there be no prospect of the labor terminating naturally, and the female is exhausted, it must be terminated artificially, as if it were a case of deformed pelvis. It is seldom however, that the head does not eventually give way.
Presentations of the Face.—These are usually more difficult, and longer, than those of the head. They will nearly always however, terminate spontaneously, or with ordinary assistance; but, if they should not, artificial delivery must be practised, either by turning, if the case be not too far advanced, or with the forceps. Some of the most celebrated authors recommend that all these cases should be treated like cases of natural labor. Dr. Merriman says that in some very favorable instances turning may be practised with safety and advantage; but Dr. Lee says, "My firm belief is, that the child, even under such favorable circumstances, would have a far better chance to be born alive if the labor were left wholly to Nature; or, if the natural powers were inadequate, to be extracted with the forceps." In such cases there is often too little patience, and too much interference.
The forehead inclined against the Pubes.—In this position the labor may be long delayed, and difficult, and most practitioners endeavor to turn the head round, if they cannot bring down the feet, or else apply the forceps at once. Dr. Lee however remarks, and very properly, "From all that I have seen of these cases, I am disposed to believe that it is best to leave them to the natural efforts, and to avoid all interference, all attempts to change the position, while the pains continue regular, and the head advances, however slowly." If the labor does not progress at all, or the female becomes exhausted, of course artificial delivery is necessary.
Several varieties of head and face presentations may also retard labor considerably, but Nature nearly always overcomes the difficulty; or if she cannot do so mere ordinary assistance is required.
It has already been remarked, in another place, that breech presentations mostly terminate spontaneously, and that but few of them require interference. In some of them even, when the pelvis is large, or the fœtus small, the delivery is effected quite rapidly. Still such presentation occasionally causes delay and difficulty, and necessitate more or less assistance.
As soon as the mouth of the Womb is opened sufficiently, unless the labor is rapidly progressing without it, one of the fingers may be introduced and hooked over the groin, and a little gentle force exerted upon it. This will assist very much, and will often be all sufficient. If the pelvis is too small, or the fœtus too large, and the delivery is evidently arrested, the breech must be pushed up, if possible, and the feet be brought down, as in turning. The remarks of Dr. Lee on this presentation are so plain and practical, and marked with such good sense, that I think a better explanation of what should be done in such cases-could hardly be given, I will therefore quote his remarks in full:—
"Having ascertained that the nates present, whatever the position of the fœtus may be, whether the abdomen look backward or forward, we cannot alter it with safety, and no change can be required to be made till the nates and lower extremities are expelled. The os uteri dilates slowly in most cases[308] of nates presentation, but we cannot employ any means with advantage to accelerate the delivery, and in most cases, if we do not interfere, but wait patiently, they are gradually pressed lower and lower into the pelvis, and at last escape from the vagina without any assistance. If the os uteri and vagina are imperfectly dilated, and the nates are drawn down or pass rapidly through the pelvis, the child is often lost. The membranes should not be ruptured, and the expulsion of the nates should be left entirely to the natural efforts, unless the labor is protracted and exhaustion takes place. Except supporting the perineum, nothing is required in a great proportion of these cases before the nates and lower extremities have been expelled, when it becomes necessary to ascertain precisely the relative position of the child to the pelvis, to rectify this if it is unfavorable, and artificially extract the superior extremities and head, to prevent the fatal compression of the umbilical cord. If we find, after the expulsion of the nates and lower extremities, that the toes are directed forward, or that the child is in the position represented in the second figure, with its abdomen applied to the anterior part of the uterus, and that its back lies along the spine of the mother, we should wrap the nates and sides in a soft napkin, and turn the child very gently round during a pain, observing to which side the feet are inclined to turn, till its abdomen is to the spine of the mother, and the toes are directed backward to the hollow of the sacrum, or to the side of the pelvis. In many cases the nates turn round in the passage spontaneously, so that it is not required artificially to alter the position. It is necessary always to recollect that it is possible to turn the body of the child round without turning the face round into[309] the hollow of the sacrum, and that the chin may be over the symphysis pubis when the front of the chest and abdomen are turned backward. After the lower extremities and body of the child have been expelled, and placed in the most favorable position for the extraction of the superior extremities and head, it is necessary to proceed without loss of time to draw these through the pelvis, that the child may not be destroyed by compression of the umbilical cord. As pressure upon the cord for a very short time will in some cases kill the child, it is proper to watch closely the pulsations of its arteries. Draw the body of the child forward as far as the arm-pits, and place it over the palm of your right hand and fore-arm, and gently draw the body towards the left thigh of the mother; then pass the fore and middle fingers of your left hand along the back part of the left arm of the child to the elbow-joint, and press down the arm with your lingers along the thorax of the child, and extract it. Then transfer the body of the child and left arm to your left hand and fore-arm for support, and with the fore and middle fingers of your right hand disengage and bring down, in the same way, the right arm of the child; then pass the fore and middle fingers of your left hand into the mouth of the child, or rather over the lower and upper jaw, and at the same time place the fore and middle fingers of your right hand over the back part of the neck and occiput, and with the fingers of the two hands thus applied extract the head, in the line of the axis of the pelvis. The perineum is very rigid in some cases of nates presentation, where it is the first child, and it will be torn if the head is extracted hastily, and not drawn forward to the symphysis pubis. When you feel the pulsations of the cord beginning to cease, you may[310] be tempted to employ greater extracting force than the neck of the child and perineum can bear, and both may be destroyed. The only method of obviating this is to press back the edge of the perineum, that the air may gain admission into the mouth of the child, and the respiration go on, when the circulation in the cord has been arrested, until the perineum is sufficiently dilated to slide back over the face, and allow the head to pass. I have seen from twenty minutes to half an hour elapse in some cases, after the cord had ceased to pulsate, before the perineum would allow the head to escape, during which time the respiration was regularly performed. This is not a new practice; it has been alluded to by some of the older accoucheurs, and some others; and the advantages to be derived from it were fully pointed out some years ago by Dr. Bigelow, in a paper published in the American Journal of the Medical Sciences, 'On the means of affording Respiration to Children in Reversed Presentations.' The object of Dr. Bigelow in this paper is to show that in many cases the life of the child may be saved by forming a communication between the mouth and atmosphere previous to the delivery of the head. If the head be low down, the fingers alone can give the necessary assistance; but if it is high in the pelvis, and is reached with difficulty, the assistance of a tube may be necessary. He recommends a flat tube, which is to be guarded, and kept within the fingers of the inserted hand.
"Where the pelvis of the mother is small or distorted, and the child large and unfavorably situated, the efforts of nature may be insufficient to expel the child, either alive or dead. The nates may become so firmly impacted in the pelvis, that they cannot[311] advance without artificial assistance. A finger should be passed up to one of the groins, and when a pain comes on a considerable extracting force may be exerted with it, without injuring the child; or a soft handkerchief may be passed between the thigh and abdomen, and the nates drawn down; but this cannot be done unless they have descended low into the cavity of the pelvis. Where these means fail, and it is impossible to extract the child alive, the blunt hook or crotchet must be employed. In cases of nates presentation, where the pelvis is distorted, after the extraction of the trunk and extremities, it is necessary to perforate the back part of the head, and complete the delivery with the crotchet. In presentations of the feet and knees the treatment does not essentially differ from that required in presentations of the nates."
These are the most dangerous of all the presentations, and most frequently require assistance; in fact the delivery can seldom be terminated naturally when the shoulder presents.
Sometimes the child will pass doubled up, as formerly explained, but this must not be too confidently expected. Dr. Lee says—
"It is now a general rule, established in all countries where midwifery is understood, that in cases of preternatural labor, where the shoulder and superior extremities of the child present, the operation of turning ought to be performed. But the hand must not be forced into the uterus, if the orifice is rigid and undilatable; it should be dilated nearly to the[312] size of half-a-dollar piece or more, or the margin ought to be very thin, soft, and yielding, if it is expanded to a smaller extent than this when turning is attempted. If the os uteri will not admit the extremities of the fingers and thumb in a conical form to be introduced without much force, if it is thick, hard, and unyielding, some delay is necessary, that the parts may relax, death being almost always the consequence of thrusting the hand with violence through the orifice of the uterus in a rigid and undilatable condition, whether the membranes be ruptured or not. But as soon as it will admit of the safe introduction of the hand, where you have ascertained that an arm presents, no time should be lost in completing the delivery, otherwise the membranes may give way, the liquor amnii be evacuated, and a case of little difficulty and danger be suddenly converted into one equally hazardous to the mother and child. In all cases of labor, where the first stage is far advanced without the nature of the presentation being positively determined, or a superior extremity is felt through the membranes, the patient should be kept in the horizontal position, that they may not be ruptured; and you should remain in constant attendance upon the patient, and be prepared to interfere the instant the necessity arises."
Speaking of the operation of turning in these cases he remarks as follows:—
"In some favorable cases of shoulder and arm presentation, the uterus is widely dilated before the membranes are ruptured and the liquor amnii discharged; and no difficulty is experienced in passing the hand into the uterus, laying hold of the feet, and[313] extracting the child by the operation of turning. If the uterus is not contracting strongly and at short intervals, little resistance is offered to the introduction of the hand, and the delivery may be speedily accomplished with safety both to the mother and child. But if the membranes have burst, the liquor amnii escaped, and the uterus has been contracting firmly upon the child many hours before the operation of turning is attempted, the child is often destroyed by the pressure, and the coats of the uterus exposed to great danger from contusion and laceration in passing up the hand and bringing down the feet. The shoulder and thorax become so strongly impacted in the pelvis, that great force is required to introduce the hand to grasp the feet, and much exertion necessary before the position can be changed.
"In other cases of shoulder and arm presentation, the membranes burst and the liquor amnii escapes at the commencement of labor, and the os uteri is rigid and undilated, so that the hand cannot be passed into the uterus after the labor has continued many hours. The difficulty and danger of these cases is greatly increased when the uterus is contracting with violence, and the pelvis is distorted, or a disproportion exists between the child and pelvis from any other cause. The greater number of women, if abandoned to the efforts of nature under these circumstances—the uterus having no power to alter the position of the fœtus—would ultimately die undelivered, from exhaustion or rupture of the uterus and vagina."
Fortunately these cases are very rare, and when assistance is rendered early, the difficulty is readily overcome. This is a strong reason why all women especially should know what to do, because a little timely help may save much suffering, or even life.
This is always a troublesome, and frequently a fatal accident. It should be always watched for, and attended to as early as possible—a few minutes frequently determining the recovery or death of the patient.
The chief causes of flooding are, the too early or violent, separation of the placenta; insertion of the placenta over the mouth or on the neck of the womb; laceration of the womb or vagina; the bursting of a swelled vein; rupture of one or more of the blood vessels of the uterus; and breaking of the cord.
Probably the most frequent of these causes are the premature or violent separation of the cord, and the bursting of the blood vessels. The insertion of the placenta over the mouth of the womb, instead of on the fundus, occurs very seldom, but when it does severe flooding is nearly certain to follow, because the placenta has then to be torn, by the expansion of the parts, at the very commencement of the labor, and probably continues to pour out blood for a long time before the child is delivered, and it can be expelled. In fact this occurrence, unless the labor terminates very speedily, is nearly always fatal to the mother, and frequently to the child also. In most cases there is more or less hemorrhage from this cause during gestation, particularly after the sixth month, when the neck of the uterus begins to[316] enlarge more than the placenta, and consequently tears away from it. Abortion frequently results also, if the flooding be not stopped. Madame Boivin tells us that in twenty thousand three hundred and fifty-seven deliveries there were but eight cases in which the placenta grew over the mouth of the womb; which is equal to one case in every two thousand five hundred and fifty-four. Dr. Churchill has collected the accounts of one hundred and seventy-four cases of this kind, and he finds that out of these forty-eight terminated fatally; or nearly one out of every three.
The rupture of the blood vessels may occur when they are too much engorged with blood, or when their coats are weakened and corroded by disease. Shortness of the cord may also produce a rupture of the vessels, by the strain it causes on them and on the membranes.
In many cases the flooding comes on suddenly, without any warning whatever, though most usually it is preceded by a sensation of weight, heat, and fluttering in the pelvis, pains in the thighs and back, flushed face, headache, and dizziness. The pulse also becomes irregular, the hands and feet grow cold, and the ears often ring, or buzz. The only certain sign that the hemorrhage has really commenced is the appearance of the blood itself, and this often occurs, as previously remarked, without any premonitory sign whatever.
The danger from hemorrhage during labor is greatest when it commences the earliest, because it has then the longest to last. From any of the causes mentioned it is evident that it must continue till delivery is accomplished, and therefore if it appears at the commencement of the labor it may cause the[317] death of both mother and child, before the labor can be terminated. The danger is greatest however to the child, unless the flow be very profuse indeed, and then it is equally so to both. After delivery the danger is of course only to the mother; and the rapidity with which it may compromise her life is in some cases fearful. Dr. Lee thus speaks of such cases.
"But one of the most dangerous varieties of uterine hemorrhage is that which follows the expulsion of the placenta, or its removal from the uterus by art. Sometimes the blood escapes in great quantities from the uterus immediately after the removal of the placenta, and the pulse ceases at the wrist, and consciousness is entirely lost in a few seconds. There is no symptom before labor has commenced, or during its progress, to warn you of what is about to take place. The child has been safely delivered, the placenta has come away in a short time, and while you are perhaps congratulating yourself on the happy termination of the labor the blood begins to trickle over the bed upon the floor, or the patient suddenly complains of great faintness. In such cases there may be either a want of uterine contraction, or the contractions may not be permanent, but be followed by relaxation and the effusion of a large quantity of blood, which may either appear externally, or remain to become coagulated, and distend the uterus. For several hours after delivery, in some cases, this alternate relaxation and contraction goes on, to the great hazard of the patient, and if her condition be not clearly ascertained, and the proper remedies be employed, death may unexpectedly take place."
In regard to the treatment, he gives such excellent and practical rules, that I cannot do better than quote them.
"By far the most important remedies in these cases of uterine hemorrhage are constant and powerful pressure over the fundus uteri, the application of cold around the pelvis, and the free administration of wine, brandy, and other stimulants: ergot is indicated, but it most frequently produces no effect. The pressure and cold are always within our reach, however sudden the attack may be. The hypogastrium should be strongly compressed with the binder, and a pad of folded napkins placed under it, and in addition the hand should be firmly applied over the fundus uteri. I do not know who it was that first employed compression of the fundus uteri in cases of flooding after the birth of the child; but it has been often recommended, and there are few practitioners in this country who are not fully aware of the importance of the binder and pad, in exciting permanent and regular uterine contractions. Dr. M'Keevor states, that in 1815 it was recommended by Dr. Labatt in his lectures, and for a number of years before this Dr. Labatt was accustomed to recommend a thick firm pad, or compress over the pubes, previous to the application of the ordinary binder, where, in former labors, uterine hemorrhage had taken place. Dr. M'Keevor states, that of 6665 women delivered during the years 1819 and 1820, only 25 were attacked with hemorrhage after the birth of the child. Of these, 15 occurred before the expulsion of the placenta, ten afterwards, and in all the results was favorable. He saw only two fatal cases during the time he was in the Dublin Lying-in[319] Hospital, and he attributes this small mortality partly to the process of parturition being left entirely to the unassisted gradual efforts of the uterus; partly to the patient having been kept cool and quiet, free from all sources of disturbance and irritation; but, above all, to the careful application of the binder immediately after delivery, by which means the expulsion of the placenta, and permanent contractions of the uterus, are most effectually secured, and whenever any tendency to hemorrhage did occur before the removal of the placenta, the first point invariably attended to was to tighten the binder, and in the event of this not succeeding, a thick firm compress, made by folding a couple of large coarse napkins into a square form, was placed over the region of the uterus, and the binder again adjusted. In the great majority of instances, these, with the admission of cool air, checked the discharge; if not sufficient, additional pressure was made with the hands.
"At the same time that you efficiently compress the fundus uteri with the binder and pad, cold should be vigorously applied to excite the contractions of the uterus. The best mode of doing this is to plunge a large napkin in a pitcher of cold water, and dash it suddenly against the external parts, the nates and thighs; and this should be repeated till the uterus contracts, and the violence of the hemorrhage is controlled. I am satisfied that this is the most efficacious method of applying cold to excite uterine contractions; it is far less formidable than pouring water from a height over the naked abdomen, but it is not less efficacious, and it possesses these decided advantages over the other method, that while the application is made to the external parts, nates, and[320] thighs, the pressure of the binder and pad is not withdrawn from the hypogastrium, the position of the patient is not changed from the side to the back, the bed is not inundated with water, and the application can be repeated as often, and continued as long, as the urgency of the symptoms may require. The abdomen may be exposed once, and cold water poured over it from a height, and the uterus made to contract, and the flow of blood be arrested for a time, but relaxation of the uterus may follow after a short interval, and the hemorrhage be renewed again with equal violence as at first; but we cannot with propriety expose the abdomen a second time, and empty over it from a height the contents of a great decanter or kettle. Besides, by adopting this practice, we sacrifice the whole of the effects derived from pressure on the fundus uteri. The application of a napkin soaked in vinegar and water to the parts is often sufficient, along with the binder, to restrain the hemorrhage where it is not very profuse.
"I have very seldom introduced a plug of any kind into the vagina in these cases, but when there has been a draining of blood from the uterus, after the practice now described has been employed, a large soft sponge passed into the vagina, and pressed up against the os uteri, has appeared in some cases to promote the coagulation of the blood. The sponge, however, cannot be employed with safety after the expulsion of the child and placenta, unless the uterus be firmly compressed above the brim of the pelvis to prevent its becoming distended with blood. More frequently I have had recourse with good effect, to the introduction of several pieces of smooth ice into the upper part of the vagina, and allowing them to remain there, in contact with the os uteri, and be[321] dissolved, or pieces of ice have been inclosed in a bladder and laid over the pubes.
"Other means besides those now described have been recommended in cases of flooding after the expulsion of the placenta. It has been proposed to inject cold water into the cavity of the uterus by means of the stomach pump, and favorable reports have been given of the practice. The effect, I think, would be similar to directing forcibly a stream of cold water against a stump soon after amputation; the coagula in the cavity of the uterus and in the orifices of the vessels would be all washed away: nevertheless, it might perhaps be advantageous in some desperate cases. Port wine and water, as cold as possible, Dr. Collins says, injected into the rectum, has been of service. Some of the earlier writers on midwifery, and many in the present century, have strongly recommended the introduction of the hand within the uterus for the purpose of removing the coagula accumulated within the cavity, and to excite the uterus to contract. But it is not necessary to pass the hand into the uterus for the removal of coagula, because if the binder has been properly applied, and strong pressure made over the fundus uteri, clots cannot accumulate within the uterus, and if they have been permitted to collect in consequence of neglect, then expulsion will immediately follow the use of proper compression of the hypogastrium, without the introduction of the hand. Nor do I consider it necessary, to excite uterine contractions, that the hand should ever be introduced into the cavity of the uterus after the removal of the placenta. I am fully convinced, from repeated observation, that this practice, which is so common as to be almost universal in this country at[322] the present time, is often not only ineffectual for the purpose, in the worst cases of flooding, but that it is often followed by the most pernicious effects; the coagula which nature has formed have been displaced by the hand, and the uterus has not been excited by the stimulus of it to secure a permanent contraction. In the greater number of fatal cases of uterine hemorrhage after the expulsion of the placenta, which have come under my observation, the hand had been introduced into the cavity, and the closed fist had been pressed for a longer or shorter time round and round against the lining membrane, to make the uterus contract. I do not recollect a single fatal case, where the unfortunate result could be fairly attributed to the want of the introduction of the hand into the cavity of the uterus, and the friction of the knuckles against the lining membrane. I have repeatedly passed the hand into the uterus to produce contraction, but it has refused to obey the stimulus of the hand; it has remained like a soft flaccid bag, more like a piece of intestine than uterus, and the blood has continued to pour down the arm, until the hand has been withdrawn, and more efficient remedies employed. Leroux was well aware that the stimulus of the hand would not in all cases excite the uterus to contract, for he observes, "where the os uteri is contracted, the means indicated by Levret are very efficacious, and remove the hemorrhage as if by a charm. But it is not so in complete inertia of the uterus; often it is widely dilated, and offers no resistance to the introduction of the hand. The introduction even of the whole hand excites little sensation, and the woman will promptly perish from hemorrhage if other means more active and certain are not employed to prevent it." The tampon[323] or plug is the remedy Leroux recommends in cases of flooding after delivery, and he affirms that it will often succeed in stopping the flow of blood when all other means fail. Dr. Dewees observes, that he has not found it necessary to introduce the hand for the purpose of stopping an hemorrhage after the expulsion of the placenta, during the last five-and-thirty years, as he regarded the practice as always frightful, and oftentimes unnecessary and pernicious. But it is difficult to subvert an established mode of practice, however unsound, and probably some of you, without much reflection, because you have heard this recommended, will pass up the hand into the cavity of the uterus after the expulsion of the placenta, on the very first occasion that you have an opportunity of doing so, remove all the coagula, and rub the inner surface with the fist till you are tired, without effect. I have seen cases repeatedly where this has been diligently performed by those who had neglected to apply the pad and binder, and all the other means now described. If you pass the hand at all within the parts, which I strongly suspect you will do, let me entreat you to carry it no farther than the os uteri, which you may, with much less risk and with greater effect, press and rub with the fingers and irritate than the inner surface of the body and fundus of the uterus.
"Mauriceau recommends that women who are subject to flooding after delivery should be bled twice or thrice from the arm during pregnancy, and once, or oftener, after labor has commenced. There are cases of uterine hemorrhage after the delivery of the child and expulsion of the placenta unconnected altogether with the plethora, or an excited state of the heart and arteries, and where bleeding[324] and low diet do not prevent the accident. Rupturing the membranes at the very commencement of labor is by far the best remedy, the only thing indeed upon which any dependance can be placed.
"After attacks of uterine hemorrhage, the patient should not be raised from the horizontal position for several hours, and the strength should be supported by wine, beef-tea, and light nourishment. Brandy in gruel sometimes agrees when wine is rejected. A good large dose of the liquor opii sedativus often produces the most decided benefit after the hemorrhage has ceased; there are few cases before this in which opium does good, though it is constantly given in all the varieties of flooding, even when the great object is to excite uterine action. Where recovery is to take place after uterine hemorrhage, says Dr. M. Hall, the pallor of the countenance, the disposition to syncope, the coldness of the extremities, the feeble state of the pulse, and uninterrupted respiration, pass gradually away. Where the case is to terminate fatally, the symptoms gradually assume a more alarming aspect, the countenance becomes pale and sunk, the respiration stertorous, and the pulse cannot be felt at the wrist. There is great restlessness, and before death one or more fits of convulsions sometimes occur. Where recovery takes place, in some women it is astonishing how little permanent inconvenience is felt from the great loss of blood which they have sustained. In the course of ten days or a fortnight the effects have entirely disappeared; and this is the most common result. In some women, a violent determination of blood takes place to the brain, marked by heat, strong pulsations of the carotid and temporal arteries, intolerance of light, and all the symptoms of inflammation of the[325] brain or its membranes. A strong febrile attack is also sometimes experienced, without an increased determination of blood to any particular organ. These affections of the brain and nervous system are aggravated by depletion. The patient should be kept in a cool, dark room, and mild cathartics, anodynes, and antispasmodics, occasionally given. Where there is much headache and throbbing, a few leeches should be applied to the temples, and a cold lotion to the scalp."
These remarks of Dr. Lee, as to bleeding frequently making the after symptoms worse, should be carefully borne in mind. There is no doubt but that too copious, or too frequent bleeding, during pregnancy or labor, disposes the female to many serious dangers afterwards. I have known some suffer constant headache, dizziness, and loss of memory, for weeks after from it; and others have even been made light headed.
To the above remedies I would only append one other, which has, on many occasions succeeded, when all others have failed, namely Galvanism. This has, at the last moment, when the female was sinking, brought on uterine contractions, stopped the flooding, and saved her life. The application is very simple; one pole being placed on the back, immediately between the hips, and the other over the uterus. Or one of the poles may be coated with wax, all but the end, and introduced into the vagina, so that the unwaxed part may touch the mouth of the womb, while the other is placed over the fundus, or on the back, as found most efficient. The power should be sufficiently strong to produce contraction, and the application must be continued till the contraction[326] remains after the pole is withdrawn. No medical man should give any female up who is flooding, no matter how severely, till he has tried Galvanism. In my "Neuropathy" and "Practical Facts" will be found many cases, with such plain directions that any one could follow them and apply it.
The presentation of the placenta, or its growth over the mouth of the womb, is the most serious cause of flooding, and generally makes any attempt to check it of no avail, except delivery. The discharge however nearly always occurs before the full period, and either causes miscarriage or necessitates premature delivery. Dr. Lee remarks:
"In the greater number of cases of placental presentation the discharge of blood takes place spontaneously in the seventh and eighth months of pregnancy, and cannot be referred either to bodily exertion, external violence, nor to any unusual determination to the uterine organs, or congestion of their vessels. The hemorrhage generally comes on suddenly, when the woman is in a state of rest, and the blood continues to flow until faintness or even syncope takes place. It often ceases entirely, and the patient resumes her usual occupations, and has no dread of another attack. But after an interval of several days, and sometimes not before two or three weeks, the flooding is renewed, and perhaps with increased violence, or a constant profuse discharge takes place, and a decided effect is produced upon the constitution,—the pulse becomes rapid and feeble, and the countenance pale. Similar attacks return at longer or shorter intervals, and if delivery be not accomplished by art, sooner or later death takes place. The first attack of flooding seldom proves fatal, but[327] it sometimes does so; for in the second case related in the table, which occurred in the British Lying-in Hospital, the life of the patient was at once extinguished by a single gush of blood from the uterus. I examined the body after death. The centre of the placenta was over the centre of the os uteri.
"When flooding takes place to an alarming extent in the seventh or eighth months of gestation, you ought first to ascertain, by a careful internal examination, whether or not the placenta be situated at the os uteri. It is impossible, from the manner in which the discharge of blood takes place, to be certain of the fact; for there are some cases of hemorrhage from detachment of the placenta from the upper part of the uterus, where the flooding occurs spontaneously, and to as great an extent as in cases where the placenta presents. In some cases I have been induced, from the symptoms, to believe that the placenta was at the os uteri when it was not. As the treatment and the successful or fatal result of the case will, in a great measure, depend on the correctness of the diagnosis, the examination should be conducted with so much care and circumspection as to leave no room for doubt on the subject. An ordinary examination, with the fore and middle fingers, is generally sufficient to enable us to ascertain the true state of the case, but where the os uteri is very high up, and directed backwards, it becomes requisite to introduce the whole hand within the vagina. The finger should then be passed gently through the os uteri, and, if the placenta adheres to the cervix, it will be distinguished from coagulated blood, the only substance with which it can be confounded, by its firmer, fibrous, vascular structure, and, above all, by its adhering at one part to the uterus, and being[328] separated at another. If you will take the trouble to pass the finger carefully and repeatedly over the uterine surface of a recently expelled placenta, you will never, in actual practice, mistake a placenta at the os uteri for a clot of blood, however firm. In all cases it is requisite to proceed at once to determine by an examination, so carefully conducted as to render a mistake impossible, whether or not the placenta presents—even though the hemorrhage should be slightly renewed by the displacement of the coagula; you cannot be too early acquainted with the precise condition of the patient. You ought, at the same time, to ascertain whether the placenta adheres partially or completely to the cervix uteri, and whether the os uteri is in a condition to admit of the operation of turning being performed.
"The operation of turning, which is required in all cases of complete placental presentation, is not necessary in the greater number of cases in which the edge of the placenta passing into the membranes can be distinctly felt through the os uteri. Sometimes there is profuse and dangerous hemorrhage where the placenta does not adhere all round to the neck of the uterus, but only partially. If the os uteri is not much dilated or dilatable, the best practice in these cases is to rupture the membranes, to excite the uterus to contract vigorously, by the binder, ergot, and all other means, and to leave the case to nature: by adopting this treatment the operation of turning may be avoided with advantage in the greater number of cases of partial placental presentation. But, if the hemorrhage is profuse, has returned at different intervals, and a great quantity has been lost, and the constitution is really affected, it is the safest practice at once, if the orifice of the[329] uterus is in a condition to allow the hand to pass without difficulty, to deliver by turning the child.
"Where the placental presentation is complete, the operation of turning should be performed, in all cases, as soon as the orifice of the uterus is so much dilated or dilatable as to allow the hand to be introduced without the employment of much force. It is seldom safe to attempt to deliver by turning before the os uteri is so far dilated that you can easily introduce the points of the four fingers and thumb within it: however soft and relaxed it may be, until dilatation has commenced, and proceeded so far, I am convinced there are very few cases in which the operation of turning will be required, or completed without the risk of inflicting some injury on the os uteri. This is a point of the greatest practical importance, but I do not know in what manner to communicate to you, in words, a more clear and definite idea of the grounds upon which you ought to proceed.
"In every case, before attempting to turn, make a most careful examination of the os uteri, and endeavor, from the degree of dilatation, and the thinness and softness of the orifice, to form a correct judgment upon this point, before interfering, for the hemorrhage will be renewed if the attempt is unsuccessful, and the patient will be placed in a worse condition than she was before. When you have resolved to turn, let the patient lie on the left side, with the pelvis close to the edge of the bed, and introduce the right hand into the vagina as before described, and then pass the fingers and hand gently and slowly in a conical form through the os uteri, giving it time to dilate, and onward into the cavity between the detached portion of the placenta and the[330] uterus: then force the fingers through the membranes, grasp both feet, and bring them down into the vagina, and slowly extract the child as in the cases of nates presentation, and do not afterwards be in a hurry to remove the placenta, unless it is wholly detached and lying in the upper part of the vagina. This operation is easily and speedily performed when the os uteri is widely dilated and dilatable. It is, however, a great exaggeration of the facility with which turning may be accomplished in these cases, to represent it as a very simple process—like putting the hand into the coat-pocket and pulling out your handkerchief. At the best it is a dangerous operation, and you can never tell with certainty whether or not the patient will recover after its performance, however easily it may have been effected.
"But there is not unfrequently most profuse and alarming flooding from complete placental presentation, where the os uteri is so thick, rigid, and undilatable, that it is impossible to introduce the hand into the uterus without producing certain mischief. In thirteen out of thirty-six recorded cases the os uteri was rigid and undilatable. The tampon or plug has no power to restrain the hemorrhage in such cases, nor do I know of any other means—either cold, quietness, or opium—which effectually have, and it is sometimes absolutely necessary under such circumstances to deliver by turning, before the hand can possibly be introduced into the uterus without producing fatal contusion or laceration of the part. I have found in several of these cases, however, that the delivery may be safely accomplished by merely passing the hand into the vagina, and afterwards the fore and middle fingers between the[331] uterus and detached portion of the placenta, grasping with them the feet, which are generally situated near the os uteri, and drawing down the inferior extremities into the vagina, and delivering. I know that the inferior extremities may often be brought down in this way where it is impossible to pass the whole hand through the os uteri."
The same state of things may however result from other causes, and a very different mode of proceeding may then be needed, as the doctor very clearly shows.
"Flooding may take place in the latter months of pregnancy, and during labor, where the placenta does not adhere to the neck of the uterus, but to the body or the fundus, and is detached by some external or internal cause. The separation of the placenta from the upper part of the uterus may be produced by violence, as blows, falls, pressure over the hypogastrium, and shocks of various kinds; but it arises much more frequently from internal causes, of which morbid states of the placenta, and twisting of the umbilical cord once or oftener round the neck of the child, are the most common and obvious. This variety of hemorrhage, though usually termed accidental, can rarely, however, be referred to accident. Sometimes the flooding occurs to a great extent without any assignable cause; a large portion of the whole of the placenta, when in a healthy condition, being suddenly detached from the uterus, when the patient has been exposed to no external accident, or injury of any kind, and when no symptoms of increased determination of blood to the uterus have preceded the attack. When this happens a large[332] quantity of blood is poured out between the placenta and uterus, a small portion of which only at the time usually escapes from the vagina, to indicate what is going on within the uterus. There may be a great internal hemorrhage, accompanied with the ordinary constitutional effects resulting from loss of blood—as faintness, sickness, or vomiting, coldness of the extremities, rapid feeble pulse, hurried breathing; when there is little or no discharge from the vagina to excite alarm, or to point out the source of danger, when it is extreme. It is from the general symptoms of exhaustion, and by the disagreeable sense of uneasiness, weight, or distension of the uterus, experienced, and not from the quantity of blood which appears externally in these cases, that we are led to discover the true state of the patient—to suspect that internal hemorrhage is going on. But much more frequently only a small portion of the placenta is at first detached, and the greater part of the blood which is extravasated between it and the uterus separates the membranes, and descends by its weight to the orifice, and escapes through the vagina. In all cases, however, of uterine hemorrhage in the latter months, the danger cannot be so accurately estimated by the quantity of blood which appears externally, as by the general symptoms. The portion of placenta which is detached, never re-unites to the uterus, but when expelled it is usually seen covered with a dark coagulum adhering to the uterine surface.
"When the blood escapes in small quantity, and there are no labor pains present, and no disposition in the os uteri to dilate, and the constitutional powers are not impaired, an attempt should be made to prevent a return of the discharge, and the occurrence[333] of labor pains. For this purpose, if the pulse is full and frequent, some blood may be taken from the arm, and the patient should be kept in the horizontal position, surrounded by cool air, cold applications made over the hypogastrium, and acetate of lead and opium, mineral acids, and other remedies that diminish the force of the circulation and promote the coagulation of the blood, should be taken internally. The plug is here totally inadmissible; it can only convert an external into an internal hemorrhage. But where the flooding occurs at first profusely, and is renewed even in a moderate degree, in spite of our efforts to check it, the continuance of pregnancy to the full period cannot be expected; it will be of no avail to bleed and administer internal remedies, except for the purpose of checking the discharge, and thus averting the immediate danger until the uterus is emptied of its contents.
"The operation of turning, which is required in all cases of complete placental presentation, is rarely necessary in uterine hemorrhage where the membranes are felt at the orifice. In a great proportion of these cases, where, on making an examination, you can feel the smooth membranes extending across the neck of the uterus, the flooding will be arrested, and the labor safely completed, if the membranes are ruptured, the liquor amnii discharged, and contractions of the uterus excited by gentle dilatation of the orifice, and other appropriate means. The only cases in which this treatment fails are those in which it has not been had recourse to sufficiently early, or where the whole or a large portion of the placenta has been suddenly separated from the uterus, and a great internal hemorrhage has taken place. The uterus will not contract effectually in these cases[334] after the membranes have been ruptured; the pains, instead of becoming stronger, become more and more feeble, return at longer intervals, and during these the blood flows more profusely, and death would take place before delivery, if the child were not extracted by the forceps, crotchet, or by the operation of turning. In all cases, then, of uterine hemorrhage in the latter months of pregnancy, and in the first stage of labor, where the placenta does not present, and the quantity of blood discharged is so great as to render delivery necessary, where it appears improbable that the pregnancy can go on longer with safety, or to the end of the ninth month, rupture of the membrane with the nail of the forefinger of the right hand, evacuate the liquor amnii by holding up the head of the child, dilate very gently the os uteri with the fore and middle fingers expanded, and occasionally make pressure with the fingers around the whole orifice; apply the binder, give ergot and stimulants, and the uterus will, in all probability, contract upon its contents, and expel them without further trouble. If the hemorrhage should, however, continue after the employment of these means, delivery must be accomplished by the forceps, craniotomy, or by turning, according to the peculiarities of the case. In women who are liable to attacks of flooding after the expulsion of the child or placenta, rupture the membranes at the commencement of labor, even before the os uteri is much dilated, if the presentation is natural, and you will often succeed in entirely preventing hemorrhage."
The recommendation to bleed may be with good reason objected to, at least in the great majority of such cases; and I cannot but think that a timely[335] and persevering use of the ordinary remedies, namely, keeping quiet, using acid drinks, and cold fomentations to the abdomen, would do away with any necessity for it at all. I question very much if ever bleeding really prevented abortion from flooding, and I cannot but think that it has often brought it on sooner. Nevertheless, if all other means fail to arrest the discharge, and there are no decided objections to the contrary, it might be cautiously tried; though the policy of taking more blood from a person who is already losing too much, is not very evident.
I have often known the most severe flooding stopped, merely by the female lying on her back, drinking plentifully of lemonade, and applying cold wet cloths over the abdomen. A small dose of laudanum occasionally is also useful; and complete rest and tranquillity of mind is as indispensable as rest of the body. Many females flood and miscarry merely from worrying and fretting themselves, and from passion, or strong excitement, particularly of a certain kind. This in short must be carefully avoided, and the patient must live strictly as if a widow.
This accident is likely to occur in subsequent pregnancies, at nearly the same time, and should therefore be guarded against by a careful avoidance of all excitement, or violent bodily exertion, during the whole time. Keeping the bowels gently open, and practising a regular diet, are also requisite. A good supporting bandage is also of frequent service. For much more valuable information on this subject however, I refer to my work on "The Diseases of Women," in which it is fully treated.
Convulsions are to be looked upon as very serious indications of derangement, during either pregnancy or labor, and are frequently followed by fatal results to both mother and child. They may be of several different kinds, epileptic, hysteric, or cataleptic, though the epileptic form is most common. They often occur during pregnancy, but not usually before the seventh month, though occasionally met with much earlier. According to observations it appears that there is not above one case of convulsions in six hundred deliveries.
The principal cause of this disease appears to be the strong sympathy between the womb and other organs, owing to which they are continually disturbed by the changes it undergoes. Certain temperaments also dispose to it, particularly the lymphatic, and also dropsy, rickets, and other diseases. Strong moral impressions may also have a predisposing effect, such as sudden frights, joy or anger, and also acute pain, or the dread of it.
In most cases, and particularly during pregnancy, the convulsions are preceded, and indicated, by severe headache, and spasm at the stomach, with dimness of sight, bright sparks before the eyes, buzzing in the ears, and partial difficulty in speaking. Occasionally however the fit comes on quite suddenly, without any warning whatever.
There are few exhibitions of suffering more frightful than one of these attacks, and none that call for[337] more prompt and decided action. In general females are perfectly helpless when one is attacked in this way, and instead of being able and disposed to render proper assistance, they either run away alarmed, or fall into hysterics themselves. It is however of the utmost consequence that the sufferer should be attended to instantly, and therefore every female should know what to do in such an emergency, at least till better aid can arrive.
At the first commencement of convulsions the features become gradually fixed, the eyes are expanded and distorted, the breath is drawn with difficulty, and all consciousness appears to cease. The body then begins to twitch, the mouth opens, usually on one side, the tongue protrudes, the head turns on one side, and the blood rushes to it and the face in great quantities. In a short time the jaws close again with great force, and the tongue is bitten if proper care has not been taken to prevent it. At last the eyes began to twinkle, the mouth moves as if the patient were muttering, and the nostrils expand; the arms are thrust straight down by the sides of the body, with the hands firmly closed; the legs are stiffened straight out, and the body is bent back like a bow. In short every muscle is affected with spasms, which are sometimes fearfully violent, and may endure for a considerable time. When they subside, the fit gradually terminates and passes off. During the whole time the breathing is difficult, the mouth froths very much, and the heart palpitates quickly, but irregularly. When the spasm is over the patient falls into a perfect stupor, during which she remains unconscious, but with all the limbs soft and moveable, except the fingers, which appear to grasp. The jaws generally remain closed, and so do the[338] eyes, but they may be easily opened, and will sometimes remain open; the breathing becomes powerful and loud, and the pulse beats with rapidity. At last slight motions are observed, and consciousness gradually returns, but the memory is generally gone for some time. This state of stupor usually lasts from ten minutes to half an hour, but has been known to continue for many hours, or even a whole day. The spasm seldom continues more than from one to ten minutes, though it has lasted for an hour or more.
These convulsions might be mistaken for ordinary hysteria by those not acquainted with the difference. In hysteria however the female moves about and struggles more; she also cries out, and retains both sensibility and consciousness, so perfectly even sometimes that she requests those around to hold her, which is never the case in convulsions.
During the stupor it might be supposed, by any one not aware of the previous fit, that the patient was suffering from apoplexy, or intoxication, the appearance being so similar to that exhibited in those states. This shows the necessity for careful inquiries as to what has previously occurred.
During pregnancy convulsions generally cause abortion, either by bringing on uterine contractions or by causing the death of the child. Some few patients have suffered from them however, and yet gone their full time, but this must never be expected. A gradual extinction of the vital spark, during the stupor is the ordinary termination, though sudden death is not unfrequent, during the fit. Gradual recovery is occasionally witnessed, but seldom without partial loss of memory, or some other affliction. Madame Lachapelle says that one-half of the[339] females attacked with convulsions die, and of their children many more.
There is no doubt but that the tendency to this fearful affliction may be very much lessened in many females, by proper attention to diet and regimen. Those who are of a full habit, and disposed to headache, and rush of blood to the head, should live low, and carefully avoid everything of a heating or stimulating character, and also every kind of excitement or agitation. The bowels should be kept free, and the skin well rubbed and kept warm, and the head cool.
Treatment.—While the patient is in the fit, care must be taken that she does not fall off the bed, or bite her tongue, to prevent which the jaws must be kept apart, by putting something between, as a piece of soft wood, or the handle of a spoon covered with cloth, or even a knotted napkin. The face should be sprinkled with cold water, and the whole body well chafed, particularly the hands and feet, which should also be made warm as soon as possible. As soon as the spasm is over it is customary to bleed, either at the arm, or by leeches to the temples and behind the ears. Mustard poultices should also be applied to the feet, and inside the thighs, and an enema should be given of warm water and a table-spoonful of salt. Ice, or cold water, should be applied to the head constantly, and if possible the body should be immersed in a hot bath, which will, in many instances, bring the patient round immediately without any other treatment. The bladder should be also looked to, as well as the bowels, and if necessary the catheter should be used. As soon as she can swallow a few drops of laudanum may be given, or a little ether, but not a full dose by any means.
The propriety of bleeding, even in these cases, is denied by many, and I am almost inclined to think myself, that a prompt and persevering use of the other remedies mentioned, would be fully as successful without it. At all events, the fearful mortality in spite of it proves that it has not much power, and may well raise a doubt of its utility.
Convulsions however are so fearful and violent, that few practitioners can resist the temptation to bleed, because it seems so well calculated to give prompt relief; and besides it has popular prejudice in its favor. Some authors however assert that it makes the danger greater of paralysis, and loss of memory, afterwards.
When convulsions occur during pregnancy they seldom cease entirely till the uterus is emptied of its contents. It is therefore necessary to bring on labor, and terminate it as soon as possible, after the parts are in a proper condition. When they occur during labor it must also be finished in the shortest time possible, to afford the best chance of saving the child, and also because no treatment will prevent the attack while the patient remains undelivered. All means of bringing on dilatation of the mouth of the womb, mentioned in the article on Rigidity, may be resorted to, excepting Ergot, which should never be used in these cases.
M. Chailly tells us, that in thirteen cases of convulsions nine were first pregnancies, and seven of the females were dropsical. Only one was attacked during pregnancy, ten while in labor, and two after. Only two died, and ten of the children.
It is worthy of remark that where pregnant females have had convulsions, apparently from living too high, the children have also had them after delivery.
Rupture of the womb arises from various causes, but most usually from powerful contractions when the pelvis is small, or the fœtus large, or when it presents unfavorably. It not unfrequently results also from force being used, particularly with instruments. In fact there is no doubt but that numerous females die from this accident, brought on by the violence, haste, and want of skill of their attendants. Few injuries are more serious, or more beyond the reach of any remedy than this, though it is sometimes suffered with impunity.
The symptoms of rupture of the womb are strongly marked, and fearfully evident. When it occurs, which is most usually during a powerful contraction, the female shrieks, and instantly complains of an agonizing pain over the seat of the rupture; her face grows deadly pale, her pulse falls, and she faints. In general death is almost instantaneous, though sometimes life may be preserved for an hour or two, but very seldom. There have even been cases of recovery, but they are very few, and regarded almost as miracles.
In most cases, directly the rupture happens the fœtus escapes through the rent into the abdomen, and most of the fluid with it; but sometimes it still remains in the womb, and then if the liquor amnii is discharged there may little or nothing pass through the opening, and the danger will be much lessened[342] in consequence. In all cases the only proceeding which offers any chance of recovery is, to deliver as soon as possible, because when the fœtus is expelled the uterus begins to contract, so as to close the wound, and when that is effected, if but little fluid has passed into the cavity of the abdomen, all may yet go well. It may frequently happen, when the hand is passed into the womb, to turn and deliver, that nothing can be found, the fœtus having passed through the opening into the abdominal cavity, in which case the hand must be passed through the opening also, and the fœtus be brought back if possible. If however the rent is too much closed, or the child cannot be reached, the Cesarean operation is the only resort.
M. P. Dubois tells us of a case of this kind which occurred in his own practice. The female had only been in labor about an hour when she uttered a piercing cry, and sank as if suddenly mortally wounded. The head of the child, which was previously at the mouth of the womb, could not be felt, and on introducing his hand M. Dubois found its feet were passed through the opening into the mother's abdomen; he brought them back however, and effected delivery by turning with comparative ease. Strange to say this woman was discharged cured, in fifteen days after, though the uterus was so torn that the intestines had forced themselves through the opening into its cavity, and M. D. put them back with his hand, which also passed clear into the peritoneal cavity. In all cases, after the delivery is effected, the womb should be again explored, so that if any parts have come through they may be returned before the opening closes, which it may do very soon.
Cases are even mentioned where the child passed clear out of the womb into the abdominal cavity, and[343] remained there till absorbed, or escaped through a fistulous opening many years after; while the wound healed up, and otherwise the patient perfectly recovered. Recovery however, in any way, is a rare occurrence.
Some females seem more disposed to this accident than others; possibly from a peculiar tenderness in the substance of the womb. All are however liable to it, and this liability should beget a proper caution in all manipulations, and forbid uncalled for violence in any way.
Rupture of the vagina is much less serious than rupture of the womb, unless it occurs at the upper part, when it may give rise to similar symptoms and results. At the lower part the danger is much less, though still sufficient to excite apprehension.
The treatment is the same as in the former case. Delivery must be effected as soon as possible, and the patient kept still and cool to avoid inflammation.
It is generally thought that the greater part of these accidents result from improper treatment, and particularly from using instruments.
OPERATIONS WITH THE HAND AND WITH INSTRUMENTS.
The use of instruments in effecting delivery is a last resort to save life, and ought to be intrusted only to persons of skill; it may therefore be thought unnecessary to treat of them in the present work, and indeed I should not have done so but for the purpose of satisfying the natural curiosity of females themselves. The greater part of the dread they now experience where instruments are needed, arises from ignorance of their nature and mode of action. At the present time nearly all the instruments used, in competent hands, are comparatively safe and harmless, and if females generally understood how they operated, much less fear would be excited by their use. Years ago, when cutting and tearing instruments were employed, in nearly every case of difficulty, the lamentable results which followed fully justified the fears experienced, but at the present day such things are seldom seen, except in medical museums, the same purpose being much better effected by simpler and more harmless apparatus. I wish therefore simply to give a brief explanation of the structure, and mode of action, of the instruments now chiefly employed, and to show the extent of their application and the results which have followed from it.
The forceps are intended to take hold of the fœtus, and assist us to draw it into the world when the natural[346] forces are inadequate, and no hold can be obtained by the hands. They were first invented about the year 1650, by an English surgeon named Chamberlin, who made a secret of his invention and realized a large fortune from it. Since that time they have been modified in various ways, by different practitioners, but still remain essentially the same as when first used.
The most usual form, and probably the best, is that represented below:
PLATE L.
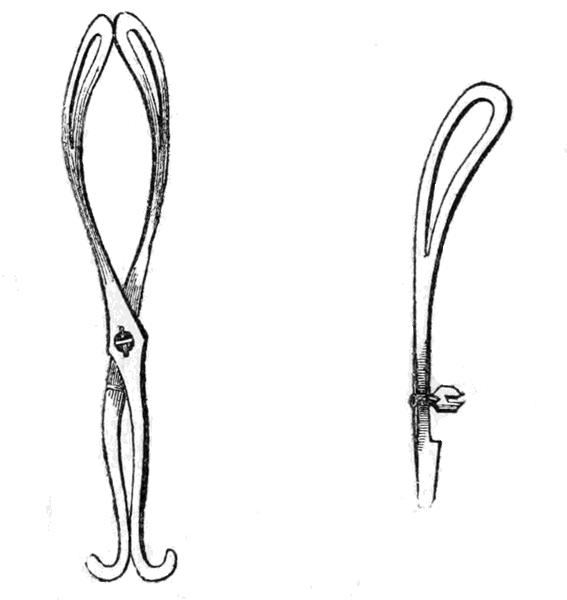
It consists of two blades articulated by a button, or screw joint, so that they can be easily separated and again adjusted,—Fig. 1. Each blade is cut out in the middle, and curved, as seen in Fig. 2.
The only part to which the forceps are intended to be applied is the head, to the dimensions and form of which they are specially adapted. Some practitioners have used them on the breech, but the practice is not generally sanctioned, because they seldom retain their hold on this part and are nearly sure to seriously injure the child when so applied. With properly constructed forceps, rightly applied to the head, there is but little danger either to the mother or the child; but in the hands of an unskillful or careless person the consequences of their use may be deplorable to both.
It is scarcely necessary to remark that the forceps are neither cutting nor crushing instruments, but are simply intended to lay hold, like the hand itself, and enable us to draw down the head, or change its position. Most usually they are made long and curved, as shown in the above plate, but sometimes they are made much shorter and straight. They may be used upon the head when it is either at the upper or the lower straits, or while it is in the passage; but on no account should they be applied till the parts are fully dilated, and everything indicates that the child can pass. Thus they should never be used when the head is too large, or the pelvis too small, nor when there are tumors in the way. In short no attempt should be made with them to force the fœtus through a passage which will not admit it by reasonable efforts. M. Dubois says they should never be used when the pelvic diameter is less than three inches, because with such dimensions the child is nearly certain to be crushed to death, and the mother can scarcely escape serious bruises and lacerations. In like manner, if they are thrust into the womb before the mouth of it is naturally dilated they are sure to tear and injure it.
It is not necessary here to give directions for using the forceps in every variety of presentation and position, but simply to show the mode of applying them as they are most frequently required. The two blades are adjusted separately, one to each side of the head, and then locked together, so that the head is firmly inclosed between them, but not crushed. Dr. Denman gives perhaps the best and simplest directions on this point, and I therefore quote from his work.
"The first part of the operation consists in passing the forefinger of the right hand behind the ossa pubis and the head of the child to the ear; then taking the part of the forceps to be first introduced by the handle in the left hand, the point of the blade is to be slowly conducted between the head of the child and the finger till the instrument touches the ear: there can be no difficulty or hazard in carrying the instrument thus far, because it will be guided, and in some measure shielded, by the finger. But the further introduction must be made with a slow semi-rotatory motion, keeping the point of the blade not rigidly, yet closely, to the head of the child, by raising the handle toward the pubes. In this manner the blade must be carried gently along the head till the lock reaches the external parts near the anterior angle of the pudendum. The point of the blade, while introducing, sometimes hitches upon the ear of the child, and it then requires a little elevation. But when it has passed the ear, and is beyond the guidance of the finger, should there be any check to the introduction either of this or the other blade, it should be withdrawn a little, to give us an opportunity of discovering the cause of the obstacle, which we must[349] never strive to overcome by violence, though we must proceed with firmness. When the first blade is properly introduced, it must be held steadily in its place by pressing the handle towards the pubes, and it will be a guide in the introduction and application of the second blade. Let the second blade be introduced in this manner. Keep the blade first introduced in its place with the two lesser fingers of the left hand, and carry the fore-finger of the same hand between the perineum and head of the child as high as you can reach. Then take the second blade of the forceps by the handle in the right hand, and, conveying the point between the finger placed within the perineum and the head of the child, conduct the instrument, with the precautions before mentioned, so far that the lock shall touch the interior part of the perineum, or even press it a little backwards. In order to fix the two blades thus introduced, that which was placed towards the pubes must be slowly withdrawn, and carried so far backwards that it can be locked with the second blade retained in its first position; and care must be taken that nothing be entangled in the lock, by passing the finger round it. When the forceps are locked, it will be convenient to tie the handles together with sufficient firmness to prevent them from sliding or changing their position when they are not held in the hand, but not in such a manner as to increase the compression upon the head of the child. Should the blades of the forceps be introduced so as not to be opposite each other, they could not be locked; or if, when applied, the handles should come close together, or be at a great distance from each other, they would probably slip, or there would be a failure of some kind in the operation, as the bulk of the head would not be included,[350] or they would be fixed on some improper part of the head; though allowance is to be made for the difference in the size of the heads of children. But if a case be proper for the forceps, if they be well applied, and we were to act slowly with them, there would not be much risk of failure or disappointment. The difficulty of applying the forceps is most frequently occasioned by attempting to apply them too soon, or by passing them in a wrong direction, or by entangling the soft parts of the mother between the instrument and the head of the child, against all which accidents we are to be on our guard.
"When the forceps are first locked, they are placed backwards, with the lock close to, or just within, the internal surface of the perineum; and they can have no support backwards, except the little which is afforded by the soft parts. The first action with them should therefore be made by bringing the handles, grasped firmly in one or both hands, to prevent the instrument from playing upon the head of the child, slowly towards the pubes till they come to a full rest. Having waited a short interval with them in that situation, the handles must be carried back in the same slow but steady manner to the perineum, exerting, as they are carried in the different situations, a certain degree of extracting force; and after waiting another interval, they are again to be carried towards the pubes, according to the direction of the handles. Throughout the operation, especially the first part, the action of that blade of the forceps originally applied towards the pubes must be stronger and more extensive than the action with the other blade, this having no fulcrum to support it, and chiefly answering the purpose of regulating the action of the other blade. If there were any labor[351] pains when the operation was begun, or should they come on in the course of it, the forceps should only be acted with during the continuance of the pains; the intention being, not only to supply the want or insufficiency of the pains, but to follow them, and imitate also the manner in which they return. By a few repetitions of this alternate action and rest before described, we shall soon be sensible of the descent of the head; and it will be proper to examine very frequently, to know the progress made, that we may not use more force than needful, nor go on with more haste than may be expedient or safe. In every case we ought to proceed slowly and circumspectly, not forgetting that a small degree of force, continued for a long time, will in general be equivalent to a greater force hastily exerted, and with infinitely less detriment to the mother or child. But after some time, should we not perceive the head to descend, the force hitherto used must be gradually increased, till it be sufficient to overcome the obstacles to the delivery of the patient. It was before observed, as the head of the child descended, that the face would be accordingly turned towards the hollow of the sacrum, without any aim or assistance on our part. Of course the position of the handles of the forceps, and the direction in which we ought to act with them, should alter; for they becoming first more diagonal or oblique with respect to the pelvis, and then more and more lateral, every change in their position will require a differently directed action, because the handles should ever be antagonists to each other. In proportion also to the descent of the head the handles of the forceps should approach nearer to the pubes; so that, in the beginning of the operation, though we acted in the direction of the cavity of the[352] pelvis, towards the conclusion we should act in that of the vagina. When we feel that we have the command of the head, by its being cleared of the pelvis, and the external parts begin to be distended, we ought to act yet more slowly, especially in the case of a first child, or there would be great danger of a laceration of the soft parts; and this can only be prevented by acting very deliberately in the direction of the vagina—by giving the parts time to distend—by duly supporting the perineum, which is the part chiefly in danger, with the palm of the hand—by soothing and moderating the hurry and efforts of the patient—and, in some cases, by absolutely resisting for a certain time the passage of the head through the external parts."
PLATE LI.
The head being drawn through a narrow Pelvis by the Forceps.
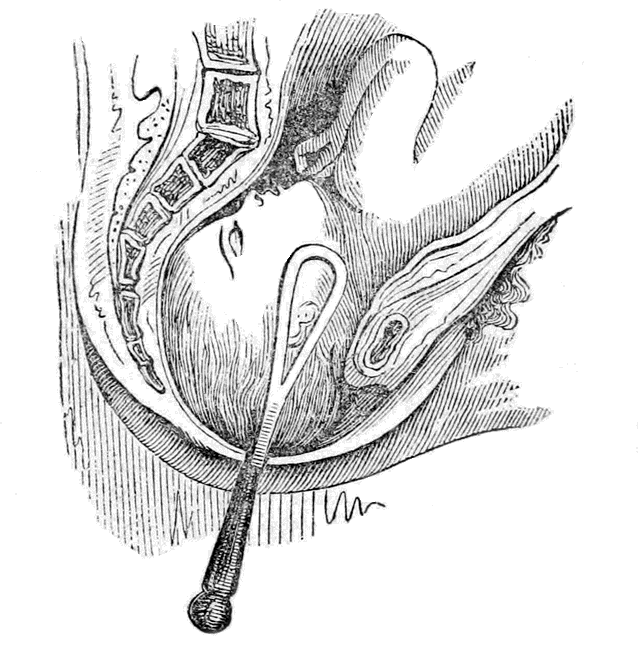
The manner in which the forceps draw the head is well shown in the above plate, and also the compression of the head itself, which is seen to be squeezed almost to a point at its presenting part. This compression, however, is not likely to do serious injury, unless it be excessive. The child may be convulsed a little from it, but usually recovers, and suffers nothing afterwards.
It is merely necessary to remark, in conclusion, that the forceps should never be used till it is manifestly impossible for the child to be born without them; and it should be remembered that nature alone frequently effects delivery under the most unfavorable circumstances, by giving her time. We should wait therefore as long as the safety of the mother will allow, but never delay a moment when that safety is compromised.
The accidents which have followed from the use of the forceps are numerous and terrible, and I could give a most horrifying account of them if it were necessary. It must be recollected however, that these accidents have chiefly followed from want of skill in managing the instrument, or from its being used under improper circumstances. It is true that there is always more or less of pain and injury to be dreaded from the forceps, even in the most favorable cases, and with the most competent operators, but this is no argument against their employment altogether. In every case where they are really called for, the female would, most probably, die undelivered, or have to be cut open, so that it is simply a choice of evils, of which the forceps are the least.
The cases in which the forceps are absolutely necessary however, are VERY RARE, much more so in fact than many people suppose. Patience, and the persevering use of ordinary assistance, would probably succeed alone in half the cases where they are now employed.
In Murphy's lectures on difficult Labors, he gives us some valuable statistics on this subject. He tells us that in seventy-five thousand nine hundred and eleven labors, the forceps were used only one hundred and thirty-eight times, or once in every five hundred[355] and fifty labors. In these one hundred and thirty-eight cases thirty-five of the children died, and ten of the mothers. Dr. Murphy however, thinks that the general results, to both mother and child, would be equally favorable if the forceps were not used at all, and he gives the tables of Dr. Collins to support his opinions. From these tables it really appears that, when all the difficult labors were left entirely to nature, the number of deaths was just about the same as when the forceps are used, in fact rather less, while the accidents, and subsequent evils, were not nearly so great. Dr. M. therefore thinks that the forceps should never be used, except in a few cases where everything is quite favorable to the passage of the fœtus; and the uterus cannot be made, in a reasonable time, to contract and expel it; and also when immediate delivery is needed to save the mother's life, as in flooding. In cases of mere ordinary difficulty or delay, he decries their use entirely; and he evidently thinks that when the labor is fit to be terminated by the forceps, nature can and will terminate it herself if left alone. There is no doubt but that they are now used a great deal too much, either from a desire to operate, or from want of patience; and I have no hesitation in expressing my opinion that more have been killed than saved by them.
Respecting other instruments, such as the Crotchet, the Vectis, and the Cephalotribe, or crushing forceps, it is not necessary to say anything here, as their use, when imperatively needed, must necessarily be confined to the surgeon; and fortunately may now be dispensed with altogether. The recently introduced[356] practice of bringing on premature labor, in all cases of deformity or smallness of the pelvis, entirely obviates the necessity for any of these dreadful resorts, if the difficulty be known in time, which it is sure to be when a sufficient degree of knowledge is disseminated.
The Cesarian operation, or cutting open the womb externally; and Cephalotomy, or the opening of the child's head, may also be dismissed with the same observations. They can always be avoided, if the real condition of the patient is known in time; and if from neglect nothing else can be done, they must always be performed by a skillful surgeon.
This is one of the most useful operations that the accoucheur can perform, in many cases, and has the advantage of being altogether accomplished by the hand. Its object is to change the presentation, when unfavorable, and to facilitate delivery. Most usually the hand is introduced into the uterus, and the feet are brought down. This is called pelvic version; but sometimes the head is brought to the mouth of the womb, particularly in shoulder presentations, and this is called cephalic version.
Cephalic Version.—This can seldom be performed, and not often attempted with safety. In some cases however, when it is ascertained that the shoulder presents, and before the membranes are broken, an effort may be made to remove it and bring the head in its place. To do this the position of the head must be ascertained externally, and one hand placed upon it; then with the two forefingers of the other raise up the shoulder from within, as in ballotment, and endeavor to push the head into its place. If the child be very moveable this may sometimes be done, and will be highly advantageous; but most frequently the substitution cannot be accomplished, and the attempt ruptures the membranes, after which it is still more difficult, and even becomes dangerous. Even if the head be brought down there is always danger of its becoming displaced, and the shoulder[358] again presented, owing to the tendency which any presentation has to be reproduced. To prevent this the hand should be firmly pressed on the fœtus, externally, as soon as the head is brought down, to fix it; and the membranes should be ruptured so that it may begin to descend, after which there is no danger of a change.
Cephalic version can be so seldom performed however, and is so difficult, and sometimes dangerous, that it is seldom or never attempted; more particularly as pelvic version can always be substituted, and is more easy and safe. It is true that presentations of the head are the most favorable, providing they occur before the rupture of the membranes, but after that event they may not be so favorable as those of the lower extremities, and certainly are not so easy or safe to induce.
Pelvic Version.—Turning to bring down the feet is performed for various reasons, and under many different circumstances. As a general principle we may say that it is done either to change the presentation, when unfavorable, or to terminate the labor when it is lingering, or when it is desirable to have it over as quickly as possible. The feet may be drawn through the mouth of the Womb when it is but little opened, and when they have once passed, the limbs and body soon follow, and the head seldom remains long behind. The fœtus may in fact be compared to a wedge, of which the feet are the point, and if they enter the passage the rest part is gradually driven after by the uterine contractions.
The chief contingencies which call for the operation of turning are, a protracted labor, a presentation of the placenta, causing hemorrhage, and a wrong presentation, particularly one of the shoulder.
The operation of turning is very clearly explained by Dr. Lee, and I know from experience that his directions can be safely relied upon. It very frequently happens however, that there will be some peculiar circumstances in a case, which will necessitate more or less change in the manner of proceeding, so that the practitioner must after all be guided, to a great extent, by the requirements and conditions then existing. Dr. Lee's directions therefore, must merely be considered as general ones, to be modified as occasion may require:—
"When the operation of turning is required before the membranes are ruptured, and when the orifice of the uterus is widely dilated, and there are long intervals between the pains, it is accompanied with little difficulty and danger. Having explained to the patient and her relatives the nature of the case, let her lie on the left side near the edge of the bed, with the knees drawn up to the abdomen. Sit down by the side of the bed, and quietly take off your coat; lay bare your right arm by turning up the shirt above the elbow, and cover the back of the hand and the whole forearm with cold cream, lard, or a solution of soap. Introduce one finger after another into the vagina, and slowly and effectually dilate its orifice. The hand, in a conical form, and in a state of half supination, must then be pressed steadily forward with a semi-rotatory motion against the perineum and sides of the passage, till it clears the orifice of the vagina. This should always be done very slowly and gently, as it is accompanied with great pain. Let the hand remain some time in the orifice of the vagina, that it may be fully dilated, and offer no resistance in the[360] subsequent steps of the operation of turning. When the hand has dilated the vagina sufficiently, in the absence of pain gently insinuate the points of the fingers and thumb into the os uteri in a conical form; and if it is not sufficiently open to allow the hand to pass, you must proceed next to use artificial dilatation here also, very gently and slowly, always stopping as soon as a pain comes on, but not withdrawing the fingers altogether at the time from the os uteri. Having succeeded in dilating the part without rupturing the membranes, slide the hand up between the membranes and the anterior part of the uterus into the cavity, and grasp the feet when the membranes give way. Most frequently the membranes burst as the hand is entering the uterus, before it reaches the feet, and the liquor amnii rushes out and is lost, if it is not prevented by pressing the hand forward firmly into the orifice. Never be contented with one foot when it is possible to grasp both; and this can always be done when the liquor amnii has not escaped, and the uterus is not closely contracted round the body of the child. Seize both feet and legs, and when there is no pain, draw them down into the vagina; and as the nates descend through the os uteri, the shoulder and arm will gradually recede or be retracted, and will offer no obstacle to the remaining part of the operation, which should be completed as if the nates and inferior extremities had originally presented, and which has already been very fully described. In actual practice, except in twin cases, the membranes have been ruptured and the liquor amnii is gone, in a great proportion of cases—in about ten to one—long before we are called upon to deliver by turning, and the operation is then a much more serious affair. Sometimes, when the[361] os uteri is half dilated, there is an interval of freedom from pain for several hours after the rupture of the membranes, and partial escape of the liquor amnii. Here it is advisable to turn without delay; and the hand can be passed up into the uterus and the feet brought down with little more difficulty than if the membranes had not been ruptured."
The operation of turning is however beset with many difficulties, and unless the conditions for it are very favorable, and the operator skillful, it may cause greater mischief than it is intended to remedy. The probability is, as in the case of other operations, that it would seldom or never be needed if proper means were used in time, and perseveringly; and it is yet a question whether the prospect, for both mother and child, would not be more favorable if the delivery was always left to nature, in those cases where version is now attempted. Dr. Collins says, "As to turning, the risk to the mother is, in the majority of cases, so great as to forbid its employment, nor do I think the practitioner justified by the circumstances in so greatly hazarding his patient's life."
THE DISEASES OF WOMEN DURING PREGNANCY, AND IN CHILD-BED.
Women are liable during pregnancy, and after childbirth, to most of the diseases which afflict them at other times, and also to many derangements peculiar to those periods. As a general rule either of those conditions somewhat modifies the disease, and also necessitates certain differences in its treatment. My former work on the Diseases of Women having treated on all those affections common to every other period, I shall in this confine myself chiefly to those peculiar to the two conditions referred to; giving their causes, symptoms, and treatment, with practical hints for their prevention.
THE DISEASES OF PREGNANCY.
The diseases which are found during pregnancy are of two kinds; the first kind called Sympathetic, or nervous, consist of various derangements of different parts of the system, produced chiefly by nervous sympathy with the Womb. The second kind, called Idiopathic, are real primary derangements of the Generative Organs themselves, or of those intimately connected with them. Each of these kinds will be treated of separately.
Nausea, or sickness, with or without vomiting, is one of the most frequent and troublesome accompaniments of pregnancy. It is so general, in fact, as to be looked upon as one of the earliest and most reliable signs of that state. It is undoubtedly caused, in the earlier stages, simply by the intimate sympathy which exists between the stomach and womb, and which causes one of those organs to be temporarily deranged whenever the other is in any unusual condition. In the latter months it is also produced by the enlarged womb pressing on the lower part of the stomach, as it rises in the abdomen. In many diseases of the womb, particularly in enlargements, and tumors, the stomach will become deranged in precisely the same manner as during pregnancy, and the patient is frequently deceived thereby as to her real condition.
In most cases the sickness does not begin till about the second month, and it seldom lasts beyond the third or fourth. There are some however, with whom it commences almost immediately after fecundation, and others with whom it lasts till the very commencement of labor. I have even known persons who always experienced the nausea at the very moment of conception, and who were thus aware when [367]that event took place. With some persons the trouble occurs only during certain parts of the day, most usually in the morning, while with others it comes on irregularly, or even endures constantly. In most cases it is not very severe, and causes but little distress; occasionally however, it is very serious, and may even lead to fatal results, in spite of all that can be done. Abortion is frequently brought on by it; and so are faintings, and spitting of blood. Many women however, will vomit with violence, during almost the whole period, without either accident or evil effect. The treatment must vary according to the cause of the derangement, its violence, and the effect it produces. In regard to diet but little can be said that will be found generally applicable. Mild and light food is generally recommended, but is not always the best, for some females can only keep on their stomachs the most indigestible articles. Perhaps nothing more can be said, with propriety, than that the patient should take whatever she can retain, particularly if she has become weak from want of nourishment, which is often the case. Some females can only keep down a little broth, or tea, or sweetened water, while others find solid food the best, or fruits. I have known many able to take Gum Arabic, either solid or dissolved in water, and retain it, when nothing else could be borne. This is nourishing, and may often keep up the strength till the sickness abates.
There are many remedies that will sometimes relieve, though frequently they are of no use whatever. A little wine or brandy, or orange flower water;—a few drops of laudanum, or ether, or essence of peppermint, may be tried. One or two ipecac, or cayenne, or camphor lozenges, will sometimes be efficacious, and so will a little Port wine and Peruvian bark, or[368] a seidlitz powder, or even common soda water. A tea-spoonful of powdered charcoal succeeds occasionally, or some very strong bitters, or a cordial, such as a wine-glassful of curacoa. A plaster of opium may also be placed over the stomach, or one of meal wet with laudanum. A mustard poultice over the stomach, will frequently relieve when everything else fails;—sometimes it is more effective however, when placed on the spine, opposite the stomach. As a general rule the bowels should be kept free, either with injections or with mild purgatives, as castor oil, or manna. Regular bathing will often act as a complete preventive or cure, and the vomiting may be frequently stopped by simply dashing cold water over the stomach. Some practitioners recommend emetics, and bleeding if the patient be of a full plethoric habit. Leeches and cups have also been used over the stomach, and sometimes with good effect. Ether and chloroform have also been inhaled, and have operated favorably in a few instances. Plentiful draughts of cold water, or swallowing bits of ice will likewise afford relief to some.
In several instances the vomiting has been so violent, and the patient has suffered so much, and become so exhausted from want of nourishment, that it has been absolutely necessary, after all other means have failed, to cause miscarriage, as the only means of saving the patient's life.
Whenever the trouble can be borne, Patience is the grand specific. The sufferer must recollect that it will surely cease with delivery, and most probably before.
Some pregnant females will secrete an immense amount of saliva for weeks and months in succession, as if they had been salivated. I have never known a case in which this discharge caused any evil, even when very great, though it is often troublesome. It would probably not be judicious to stop it, even if we could do so, as long as it does no harm, though it may be advisable at times to moderate it. The only treatment proper to effect this is, to keep the bowels free and the body well bathed, and to gargle the mouth with mint or balm teas, or canella water, or a little syrup of poppies.
This discharge, like the vomiting, arises from the sympathetic action of the uterus, and it generally ceases about the fourth month, though with some it will last the whole time.
This is also a very general trouble during pregnancy, and sometimes a very severe one. Like several other sympathetic affections it is very irregular as to its first appearance and duration, some suffering from it most of the time, almost without intermission, while others only have it at intervals, and but slightly.
It sometimes depends upon unsound teeth, but is frequently experienced without any such cause, and is then a true neuralgia. When it arises from a bad tooth, the pain is usually confined more or less to the neighborhood of the tooth, but when it is neuralgic it extends over the greater part or the whole of the jaw and face, and darts about from one part to[370] another. In true toothache there is also usually more or less inflammation and swelling, while in the most agonizing neuralgia nothing of the kind can be seen.
The treatment must be regulated by circumstances. If the pain appears to be kept up by an unsound tooth, it should by all means be extracted, unless the patient be so exceedingly nervous and irritable that abortion is to be feared, in which case the pain must be alleviated as well as it can be, though there is almost as much danger in leaving the tooth in such cases as in extracting it. A few leeches to the gums will sometimes relieve, or a mustard poultice to the cheek, or a blister behind the ear. The stomach or bowels being out of order may also keep up the irritation, and regulating them may materially assist in giving relief. Some persons are relieved by lotions of camphor, or laudanum, and others by washes of cayenne tea, or alum water. In the neuralgic form, when no particular tooth can be found in fault, the treatment must be more general than local. The Carbonate of Iron Pills, which can be purchased at the druggists ready made, have frequently an excellent effect; from two to four may be taken at a dose, twice a day, the bowels being kept open, if necessary, by a little tincture of rhubarb. If the pain comes at regular intervals, or intermits, it may frequently be stopped by quinine. Two of the ordinary quinine pills may be taken every five hours, for two or three days. If the head feels oppressed by their use, the dose must be lessened to one. M. Guillemeau recommends the following to be tried if other means fail, and I have known it to be of decided benefit. Take the whites of two eggs, and two ounces of common black pepper, in powder, and beat them well together.[371] Spread this on some tow or cotton, and lay it on the cheek. It may be kept on till it causes considerable irritation, and sometimes may be used on both sides.
Some females have been relieved by bathing the face in cold water, or keeping ice in the mouth, and others by hot fomentations. It has also been recommended to fill the mouth with cold water, and bathe the cheek with hot at the same time!
Occasionally an abscess, or gum boil will form, and when there seems a tendency to that it may be promoted by keeping a roasted fig in between the cheek and gum, over the part where the abscess points; when full, it should be lanced, as the discharge usually gives relief.
This pain is however very obstinate sometimes, and defies all treatment, but is seldom of such long duration when so severe.
The powerful sympathetic action of the womb on the stomach produces not only nausea and vomiting, but various derangements of the appetite and taste also. All of these require notice, and some need attention.
Anorexia.—This means a complete distaste, or even disgust, for food, sometimes of particular articles only, and sometimes for those of every kind. It seldom lasts beyond the fourth month, but occasionally during the whole period. It is remarkable how some females will be affected in this way, and how little they will eat, for several months together. This however is scarcely ever of any consequence, for the system does not seem to suffer in the slightest[372] degree; on the contrary, the mother will remain quite stout, and the child be born fully developed, though the quantity of food taken has apparently been scarcely sufficient to sustain life.
In many cases there is even a decided benefit from this state of things, particularly in those who are of a too full habit.
As long as the loss of appetite is merely of a sympathetic or nervous character it is not necessary nor advisable to resort to any special treatment. But when it arises from indigestion, or a foul stomach, it is necessary to attend to it. A mild emetic of ipecac or warm mustard and water, may be given, or a dose of Epsom Salts. This state will be recognized by a furred tongue, unpleasant breath, and uneasiness at the pit of the stomach; while in the purely nervous anorexia nothing of the kind is observed. Sometimes it may arise merely from debility of the stomach, and in that case a few of the Carbonate of Iron Pills will be of use. In general the patient is benefited rather than injured by this voluntary fasting.
Boulimia.—This state is the reverse of the former, meaning a ravenous appetite. Some females exhibit it in a most extraordinary degree, and will eat to excess of anything that comes in their way. Many injure themselves in this manner, by causing indigestion, flatulence, heartburn, vomiting, and even inflammation of the stomach. It is of no use reasoning with them, for the appetite is so strong that they will eat let them suffer ever so much.
All that can be done in such cases is, to drink freely of various nourishing liquids, such as soup, broth, rice milk, or chocolate; and by eating jelly, arrow-root, and eggs. These contain much nourishment in a small space, and satisfy the hunger without[373] overloading the stomach. The appetite may also be deadened considerably by eating figs, dates, sugar, or chocolate; and by drinking soda water.
Capricious Appetite.—Sometimes a female is found to have an inordinate desire for some one particular article of diet, which she will eat to excess, but will not touch anything else; this is called malacia. Others will have a craving for some article not proper for food;—this is called Pica. They will devour chalk, cinders, earth, wood, flies, spiders, charcoal, and various other things, sometimes of the most disgusting kind, though ordinarily they may be quite fastidious in their diet. This unnatural desire is also frequently seen in hysteria and chlorosis, and in several uterine diseases.
It does not appear that a moderate indulgence of these unusual tastes is at all injurious, unless the article wished for be of a decidedly hurtful character. On the contrary, it is reasonably conjectured, by many physiologists, that they arise from a real want in the system of the very substances longed for. For instance, there may not be in the mother's blood sufficient lime to form the bones of the child, and this deficiency is intimated by her desire for chalk or plaster; nature having no other mode of making her wants known, or of causing them to be supplied. As a general rule, so long as the indulgence is not obviously improper, it should be allowed to a reasonable extent, both to gratify the patient and to answer to what are probably the demands of nature.
It is seldom that interference is needed in these cases, except when there is danger of the patient doing herself harm; we may then try to alter the condition of the stomach, and so change the taste.[374] A gentle emetic will sometimes do this, or a saline purgative. If these fail use a few of the Carbonate of Iron Pills, or some good strong bitters, or teas, drunk freely, such as Cammomile, Boneset or Centaury.
This disease is more frequently called water brash and sometimes heart burn. It is characterized by the raising of a hot acrid fluid into the throat, causing a sensation of burning from the stomach upward, even to the mouth. It is a very frequent attendant upon many forms of dyspepsia, and is generally experienced more or less by most pregnant females, arising either from improper diet or from mere sympathetic derangement. If it arises only from errors of diet, a reform in that particular is all that is needed, but if it is merely sympathetic nothing can be done beyond palliating it, to give temporary relief. For this purpose the patient must take a spoonful of lime water, in half a tumbler of milk two or three times a day, or some carbonate of soda, or magnesia, with a few drops of laudanum if there be any pain. In those cases which resist such remedies a little of the compound iron mixture may be of service, such as can be obtained at the druggists. A nourishing diet should also be observed, and plenty of exercise should be taken in the open air.
Difficulty of swallowing, which is meant by this term, is a more troublesome and alarming affection, frequently attendant on pregnancy. There is however nothing dangerous in it, except that it frightens[375] the patient. Some will gasp and be unable to swallow, or even speak, for a considerable time, and will think they have something in the throat. It is however entirely a nervous symptom, arising from uterine irritation, and seldom lasts beyond the third or fourth month. A little cordial, wine, or brandy, will frequently relieve it, or some spirits of camphor rubbed on the neck. M. Colombat d'l'Isere recommends the following ointment, to be rubbed on the neck. Extract of Belladonna forty-seven grains,—Extract of Strammonium fifteen grains,—white wax one ounce,—oil of lemons twelve drops.—These must be warmed and well rubbed together. A dash of cold water on the throat and chest will often succeed better than anything else.
This is commonly termed cramp at the stomach, or nervous colic. It consists of a severe kind of cramp, with dragging and cutting sensations in the stomach, as if it were being tied in knots and cut to pieces. Sometimes the attack will only last for a few minutes, and then totally pass away, at other times it will remain for half an hour or more, and cause the most intense suffering. The patient will be drawn together, or doubled up, with her hands placed on her stomach, and will groan and exhibit in her features the greatest agony; sometimes even, she will faint away with it.
This affection may, like the others, be merely nervous, and then it is attended by nothing but the pain. It may also arise from real inflammation of the stomach, and then it is attended by fever, excessive soreness and tenderness of the stomach when[376] touched, and by a hot, dry mouth. In the nervous spasm the pain is frequently relieved by pressure, but when inflammation exists the pressure increases it.
Some females always have these attacks whenever the stomach is empty, and they pass away immediately anything is taken to eat or drink. With others they are often brought on by overloading the stomach, or by eating some improper articles.
To relieve the spasm, one of the best things is a tea-spoonful of Compound Spirits of Lavender, taken without water. This nearly always gives relief in ten minutes at most; but if necessary a second spoonful may be taken in a quarter of an hour. A little brandy, or peppermint, or curacoa cordial will also succeed in many instances, or simply drinking freely of any hot tea, or swallowing half a tea-spoonful of common pepper. A mustard plaster put on hot over the stomach will scarcely ever fail, even without anything being taken internally. M. Colombat gives the following recipe as one which he has found efficacious, and it is certainly a pleasant one. Orange and Linden Flower waters each two ounces; Syrup of Ether and of Valerian each one ounce; Syrup of Poppy heads half an ounce. Of this mixture a tea-spoonful may be given every quarter of an hour till the pain abates.
To prevent the return of the attack, the patient must carefully avoid everything that disagrees with the stomach, or creates wind; she must keep the bowels free, and accustom herself to regular bathing or rubbing the body. If the stomach appear weak, which is often the case, some Boneset tea, or Port wine and bark, or a few of the Carbonate of Iron Pills may be advantageous. If there be acid on the stomach, use the means recommended for heartburn.
This is a very common trouble with pregnant females, and one that may lead to many others. Very frequently it arises merely from the pressure of the expanded uterus upon the large intestine, but it may also arise from a simple want of power, the uterine action having apparently weakened the force of all the neighboring organs. It is advisable to correct it as soon as possible, let it arise how it may, as it is very apt to cause various derangements of the stomach and intestines, and even inflammation of the womb itself. As a general rule, not more than three days should elapse without the bowels being moved, though some will remain a week or more without any apparent inconvenience; but there is always danger in such delay.
Many females do themselves much harm by taking what they call opening medicines, the action of which is often more injurious than the constipation itself. All drastic purgatives, such as aloes, gamboge, colocynth, and jalap should be carefully avoided, as they not only make the costiveness worse after their action is over, but they also frequently produce inflammation, and even abortion, by the violent straining they cause. The best medicines, when they are really needed, are manna, seidlitz powders, or castor oil. Enemas are better however, as a general rule, such as those of thin starch, or molasses and water, to which may be added a little castor oil. The grand aim should be, in all such cases, to stimulate the bowels to an increased action without medicines, by a properly regulated diet! Salads may be eaten when they do not cause derangement of the stomach, and ripe or stewed fruits, particularly figs, dates and[378] prunes. Soups are also good, except they contain rice, or vermicelli, or maccaroni. Bran bread should be eaten regularly, and not white. The only meats should be veal or poultry. As a drink lemonade is excellent, with a little cream of tartar, or tamarind tea, or barley water sweetened with honey. With some patients a cup of coffee, or a glass of beer will always relieve the bowels, especially if a glass of water is also drank after it. I have known persons neglect the bowels so long that they have become completely impacted, by the hard fæces, and could be relieved only by instruments. It is very important to attend to this affection in time, and to persevere with the means of permanent relief regularly.
It is frequently the case that pregnant females, instead of being constipated are afflicted with severe diarrhœa. This may arise from inflammation, and is then attended by fever, and extreme tenderness and soreness of the bowels. Most usually however it is entirely nervous, and arises from the sympathetic irritation of the womb. There is then no tenderness or soreness, no fever, no derangements of the appetite, nor in fact any other symptom of any consequence. If it remains long unchecked blood will be discharged, from the extreme irritation of the intestines, and it is then called dysentery. This is nearly always accompanied by fever and general irritation. Sometimes there will be a constant and painful desire felt to move the bowels, but with little power to do so, and at the same time a burning heat and unpleasant sensation at the fundus. This is called tenesmus, and the straining from it has frequently produced abortion.
If the diarrhœa is not excessive, and the female does not lose her appetite, or strength, it is better let alone, particularly if she be of a full habit, and disposed to fever. If thought desirable to check it a little, this may usually be done by a change in the diet. Rice milk, sago, tapioca, and arrow-root may be taken, white bread may be used, and not much fluid drunk. If such means are insufficient an injection may be thrown up the rectum in the morning, of thin starch, with a tea-spoonful of laudanum. The abdomen may also be well fomented, and a dose of Tincture of Rhubarb taken occasionally. If the tenesmus is very troublesome, an injection of tepid water may be used, and the female should sit occasionally over the steam of hot water: in extremely painful cases a few leeches may be used round the fundament, and a hot flaxseed poultice placed over the abdomen. A warm bath is also an excellent remedy with many. When the diarrhœa still continues notwithstanding the above remedies, resort should be had to tonics and opiates. The patient should take Port wine and Peruvian bark, or some Gentian wine, and use injections of Starch and Laudanum regularly. Cammomile tea may also be freely drunk, and an opium pill may be taken at night. Above all, the patient must endeavor to avoid all mental agitation. When dysentery sets in, every effort should be made to subdue it as early as possible. Half a pint of rice milk, with ten or fifteen drops of laudanum may be taken two or three times a day, and an injection may also be used night and morning of flaxseed, with fifteen or twenty drops of laudanum. M. Colombat recommends the following recipe as seldom failing to cure. Take the whites of six eggs and beat them up in a quart of water;[380] then use one-third as a drink, and the rest as an injection. A neat spoonful should be drunk every ten minutes, and an injection used every two hours, but not more than one small syringeful at a time. A tea-spoonful of syrup of poppies, with some loaf sugar, may also be added to every spoonful that is drunk. Eggs, jellies, and rich soups, with meat and wine, if there be no inflammation, may be taken regularly, in addition to the articles already mentioned.
There are but few pregnant females who do not complain more or less of difficulty of breathing, and this difficulty may arise from different causes. In the earlier months it is caused by sympathetic irritation only, the same as difficulty of swallowing. In the latter months it is caused by the enlarged womb filling up the abdomen so much that the lungs in the chest are pressed upon and have not sufficient room to play freely. It may also be caused by a plethoric or too full habit, the lungs then being in reality congested.
The temporary difficulty of breathing which is felt in the early months, from nervous sympathy, needs scarcely any kind of treatment, as it passes off naturally in a short time. In severe attacks the same remedies may be used as for difficulty of swallowing before referred to.
That which arises in the latter months, from pressure of the womb, can frequently be relieved only by the patient remaining as long as possible in certain favorable positions. I have known many who could never sleep except when propped nearly upright, by means of pillows and cushions, as immediately they[381] assumed the recumbent position the upward pressure became so great they were nearly suffocated. In such cases the patient should be careful never to eat or drink to excess, nor take anything likely to produce wind, because the least increase in the size of the abdomen adds to the difficulty. The bowels should also be kept free, and nothing tight or heavy in the way of clothing should be worn.
This difficulty is most frequently seen in those who have contracted chests, and in those who have been accustomed to wear corsets and tight dresses. A deformed pelvis may also give rise to it by forcing the womb above its usual position. Many females both create and increase this difficulty by binding themselves tighter than usual during pregnancy, under the mistaken idea that it enables them to support their burden so much easier.
When the dyspnœa arises from a full habit the patient must live low, keep the body regularly bathed and rubbed, and the bowels freely open by an occasional seidlitz powder, or dose of Epsom Salts. If the difficulty becomes at any time suddenly great and alarming, the feet should be placed immediately in hot water, while the patient is upright; a mustard plaster should also be put upon the chest, and an opening injection of starch and Castor Oil administered as soon as possible. The usual practice in such cases is to bleed from the arm, to the extent of eight or ten ounces, and in case no other means give relief, this may be tried.
Like the previous affection cough is most usually produced during pregnancy by sympathetic irritation.[382] It may arise, however from a partial congestion, or inflammation of the lungs or bronchial tubes, produced by a too great determination of blood to them. In the merely nervous cough, there is no expectoration, nor any soreness or pain in the chest, and it will frequently disappear for several days together. No particular attention need be bestowed upon this cough, unless it become so violent as to threaten abortion. In that case a pill, containing one grain of opium, may be taken, or from ten to fifteen drops of laudanum, whenever the attack is severe. Barley water, or gum arabic water, may also be freely drunk, with a large spoonful of Syrup of Poppies added to each pint. A small dose of Hive Syrup, or Paregoric, will also be found sometimes better than anything else. An enema of Starch and Laudanum, as formerly described, will also relieve, in some cases, better than anything taken by the mouth. The body should be kept warm, particularly the feet, and a mustard poultice may be placed over the chest, if the straining at any time becomes too great. Some patients experience relief from an assafœtida pill, or a little musk, and others from a small dram of cordial, or wine.
If there be expectoration, with fever, and tenderness in the chest, or sharp pains when a long breath is drawn, there is reason to fear inflammation of the lungs, or bronchitis. In this case all the above means, except the wine and stimulants, may also be used only more freely, and the mustard poultice must be kept on till it makes a blister. The patient must live low, her feet must be frequently bathed in hot water, and her bowels regularly opened either with saline purgatives or enemas. All that is requisite is to keep the inflammation from extending till[383] after delivery, when it usually subsides without any further trouble. As soon as the womb is emptied, its pressure upon the abdominal aorta ceases, and the blood can then flow freely to the lower extremities, and thus the lungs become relieved and the inflammation goes down.
This is also a frequent accompaniment of pregnancy, and one that is likely to cause alarm sometimes, from its violence. Unless dependant upon organic disease of the heart however, it is in general only a nervous affection, and passes away with delivery. We may always reasonably suppose it to be nervous when it occurs only during pregnancy, and particularly if it is irregular in its frequency and violence. I have known females who were always attacked with it about the same period, and who could therefore always tell when it was coming on, and sometimes even how long it would last. It will sometimes come on during sleep, and so forcibly as to waken the patient instantly. At other times while awake, it will commence so suddenly that she will sink down as if struck by a powerful blow.
The only directions that can be given for alleviating it are, to keep as quiet as possible, use the bath regularly, avoid constipation, and live rather low, particularly if the patient be of a full habit. Exercise should also be taken regularly in the open air, but not of a violent kind. She should also sleep with the head on a high pillow, and never eat late suppers, nor take any food that disagrees with the stomach.
All kinds of stimulants, such as wine, coffee and[384] spices, should be abstained from, and all powerful emotions carefully guarded against. During an attack a few drops of Laudanum, or an Opium pill may be taken, and the feet placed in hot water. An Assafœtida pill is sometimes good, or a little Ether. Bleeding is generally practised in extreme cases, but there is often considerable danger in it.
A too full habit is often the exciting cause of the palpitation, as may be seen by the patient being always liable on the slightest exertion to flushed face, dimness of sight, ringing in the ears, swelling of the limbs, and puffiness of the gums, sometimes to such an extent that the mouth will taste of blood. Such persons should carefully observe a moderate unstimulating and simple diet, and never allow the bowels to remain constipated more than a single day. They should also rub and wash the skin well, and study calmness and quiet.
In this condition, which is just the reverse of the former, the heart suspends its action altogether; the breathing ceases, all power of motion and feeling is lost, the face turns ghastly pale, the eyes close, and the individual seems as if actually dead. It seldom lasts however more than five minutes, when the pulse gradually begins to beat, the color returns, and the individual slowly recovers. Some females are liable to such attacks once a month, others once a week, others every few days, and some at irregular periods. They are generally preceded by a dull pain at the pit of the stomach, fullness in the head, yawning, and loss of sight, or ringing in the ears.
The causes that predispose to this fainting are not[385] very well understood, though there is no doubt but it is mainly dependant upon uterine disturbances. In some females it is brought on by the sudden motions of the fœtus, or by their remaining too long in one posture. In others it is produced by straining from constipation, or by sudden fright or anger. In very nervous persons it not unfrequently arises from unpleasant sights, smells, and sounds. In fact it is caused in them much the same as a common hysterical fit, such as is described in my Diseases of Woman. A full habit, and over feeding, or drinking stimulating liquors may also bring it on, and so on the contrary may a state of weakness and exhaustion.
This accident is more alarming than dangerous, except to the child, which may lose its life if the fainting lasts too long.
To recover a person from one of these fainting fits, she should be laid upon her back on a level place, and every part of her dress should be carefully loosed. Some strong odor should then be applied to the nostrils, such as hartshorn, vinegar, burnt feathers, or smelling salts. The body should be well rubbed over the heart and lungs, either with the hand or with a soft, dry napkin. Cold water may also be dashed on the face, and the hands may be well chafed. If the fit still endures, a mustard plaster may be placed on each arm, or the whole body may be placed in a warm bath, if convenient. Care should also be taken to admit the fresh air freely. As soon as she begins to show signs of consciousness, a little wine or brandy may be placed in the mouth, and the body may be elevated a little.
To guard against such attacks, the same precautions as to diet and mode of life must be observed as were directed in the article on palpitation of the[386] heart; and, as this accident is most frequent in those of a hysterical habit, they should carefully follow the advice given in the article Hysteria, in my Diseases of Woman.
Each of these distressing affections, both of which are very common during pregnancy, may arise either from nervous excitement or from a full habit and determination of blood to the head. Nervous headache is generally met with in the earlier months of pregnancy, and is characterized by being frequently periodical, and often confined to particular spots. It also commences suddenly, from some excitement or depression of mind, and leaves little or no distress when it is gone. The headache, which arises from a too full habit, commences with flushing of the face, heaviness in the eyes, dull pain in the forehead, and a sense of uneasiness, with disposition to sleep or dose. It seldom comes on much till the latter months of gestation. Headache may arise also accidentally, from derangement of the stomach, but this cause is easily ascertained by the furred tongue, loss of appetite, and bitter taste in the mouth; it is also felt most acutely in the back of the head, down by the neck, and passes away immediately the stomach is corrected by an emetic, or by fasting.
Nervous headache during pregnancy often defies all our attempts to alleviate it, though we sometimes succeed in doing so. The best general remedies are warm baths, and, if the bowels are constipated, enemas of starch and castor oil daily. To these may be added occasional small doses of Laudanum, or an Opium pill, or two grains of Camphor. Smelling odors, such as Camphor, Cologne, or Hartshorn, will[387] relieve some, but will make others worse; so that its utility can only be determined by experience. When a severe attack comes on, the patient should put her feet in warm water, or use a warm bath, take a few drops of Laudanum, or a little Musk, or Valerian, and then try to go to sleep. To guard against the attack, she must never overload the stomach, nor take anything indigestible; and never think too much nor allow herself to become excited or depressed.
When the trouble is caused by a too full habit, she must observe the directions given in the articles on palpitation of the heart, and Syncope. The diet must be mild and not too nutritious, the bowels must be regularly moved every day, chiefly by Epsom Salts and Seidlitz Powders, and regular gentle exercise must be taken in the open air.
In the latter months it is especially important to attend to a severe headache immediately, particularly when the pain is seated at the top of the head, because it is very likely, if unchecked, to terminate in convulsions. The means above recommended must be carefully and perseveringly applied; the feet must be kept warm, the bowels freely opened, and the head kept cool by wet clothes, or cold lotions, or ice. It is the general practice in all such cases, if the pain does not abate soon, and the pulse be full and quick, to bleed freely at the arm, and the most eminent physicians of the Allopathic school assure us, that the life of the patient frequently depends upon its being done promptly. I have no doubt, however, but that relief can be generally obtained by the simple means described, if they are used early and perseveringly.
There are few affections that cause more real distress during pregnancy than this. Many females will be utterly unable to sleep for many days and nights together, and others can only obtain a few minutes broken and unrefreshing sleep at distant intervals. There is danger, when this state becomes highly aggravated, that it may lead to delirium, or that the want of rest may wear away the strength to such a degree, that the patient will sink from mere exhaustion. There are some females, however, who will remain without sleep, or at most take but very little, for a long time, without suffering any inconvenience.
This affection is essentially a nervous one, and the only means likely to relieve it are those that have a tendency to soothe and calm the nerves. If the patient be surrounded by any irritating circumstances they should be at once removed, or she herself removed from them. Particular attention must be paid to the diet, so that no derangement of the stomach or bowels be kept up, and a regular system of out-door exercise must be practised. A warm bath just before going to bed, with a good rubbing of the skin, will frequently act like magic in procuring rest. As a general rule narcotic drugs should not be used, but in extreme cases they may be resorted to sparingly. A single Opium pill, or a few drops of Laudanum may be taken after the bath. If the patient be thin and delicate, she should eat meat, eggs, and milk, and take a little wine, if it causes no unpleasant symptoms. Indeed a glass of wine will frequently act better than Laudanum, and so will ale with some, and coffee with others. If the[389] patient be of a full habit these things will be improper, and may injure. She should then be kept quiet, and fed sparingly. Music has a powerful effect in many of these cases:—a slow, solemn air, played while the patient is reclining after her bath, seldom fails in inducing sleep.
These disorders are quite common during pregnancy, particularly in the latter months. Some females will be utterly unable to distinguish any odors, even the most powerful; others completely lose their taste, and others again become deaf or blind. When they are caused only by the sympathetic action of the womb, such deprivations are seldom of long duration, though they may recur at frequent intervals. In some cases they remain a considerable time, and great fear is felt that they may become permanent, but there is little danger of such a result. I knew a lady who suddenly lost her sight when about two months gone, and who remained totally blind till about three hours after her delivery, when her sight returned in a moment as perfect as before. The same thing has frequently been observed of the other senses. In some cases the vision will not be lost but perverted, and the patient will then see everything double, or larger or smaller than natural, or always of a wrong color. In like manner some will hear imaginary conversations, or will fancy everybody is shouting, or perhaps only whispering, though they are all the time speaking in their natural voice.
These perversions, when thus produced, need occasion no alarm, and seldom require attention, unless[390] accompanied by other urgent symptoms. They may arise however, from a fullness of blood in the head, in which case they are accompanied by a flushed face and drowsiness, and are preceded by bright sparks flashing before the eyes, or by ringing in the ears.
The treatment of all these affections should be the same as that recommended for most of the previous derangements, particularly for Headache, Syncope, and Palpitation of the Heart. If there be nervous excitement merely, it must be calmed in the same way as recommended in the articles referred to, and also in the last one on sleeplessness. If the female be of a full habit, and there is evidently a pressure of blood on the brain and nerves of the special senses, the same means should be adopted to reduce the system, and draw the blood to the extremities, that have already been described.
In such cases these sudden deprivations of sight and hearing sometimes indicate the commencement of Convulsions, or Apoplexy, particularly if they occur during labor, when every means should be resorted to instantly to relieve the pressure on the brain. If no simpler means succeed in a reasonable time, it is the general custom to bleed freely from the arm, and there is no question but this frequently removes the difficulty at once, whatever objections may be made to the practice. It is also proper to say that many eminent practitioners, who are not advocates of the lancet in general, strenuously urge that it should be used immediately if the sight or hearing suddenly disappear in this way at any time. And I certainly have myself known these accidents sometimes followed by a fit of Apoplexy, or Convulsions, and even death. Such was the case with[391] a friend of one of my patients. She found one day, quite suddenly, that she could only see half of any thing she looked at, and at times it even disappeared altogether. Nothing was done for her, and in about five hours after the first attack she fell speechless and died before they could lift her upon the bed. It will therefore be a necessary precaution, in all pregnant females of a full habit, to attend rigidly to the advice that has been given, because simple means, used in time, and regularly, may prevent the necessity of stronger ones altogether. In purely nervous cases of this kind no apprehension whatever need be felt, and no such practice as bleeding is required.
The sympathetic irritation of the uterus, in some females produces extraordinary phenomena of this kind, from simple desire to the most furious craving, and from mere caprice to actual insanity. There is no doubt but that many of these unusual desires, or longings as they are called, are either produced or much aggravated by the imagination of the patient, and frequently would never be experienced at all, if the idea was not suggested by other people having had the same. Custom and imitation are very powerful in such cases, particularly when the nervous sensibility is much exalted. Still the most singular aberrations of this kind will often arise without any such adventitious aid, and the fact should be borne in mind, so that these temporary vagaries may be regarded with proper charity and forbearance.
Some females will entirely change in their dispositions at these times, the most amiable and mild becoming[392] positively ill-natured and malicious;—the gentle will turn headstrong, the haughty and proud will become humble, and the gay will become melancholy, or the sad will madly seek every kind of gaiety. Such things however should never be remembered, nor be brought up against them afterwards, for truly at such times they know not what they do!
Women have been known while in this state, to become thievish, or to have an irresistible propensity to burn or kill. Some have even been known to exhibit great talents for music or poetry, though ordinarily without any capacity for such things. Some will suddenly exhibit a most extraordinary intellect, while others will become quite silly. A medical writer tells us an instance of one female who always had an excellent sound judgment while pregnant, but no memory, while in her ordinary state she had a poor judgment but a most extraordinary good memory. The celebrated Baudelocque gives an account of another who could scarcely eat anything but what she stole, while going to market; and another writer mentions a lady who longed till she was almost delirious to bite a piece out of a baker's shoulder, who worked opposite her window. There is even an account of one who longed to eat some of her husband, whom she dearly loved, and who actually killed him to satisfy her appetite, and then salted pieces of the body to keep for future use. A writer named Vives also tells us of a female whose husband paid a large sum of money for her to be allowed to bite a young man's neck, it being evident that she would be nearly certain to miscarry unless so gratified. In the year 1816, at Mons, in France, an unfortunate woman in this condition was seized with an irresistible impulse[393] to destroy her children, and actually drowned three of them, and herself afterwards. She had previously sent a poisoned cake also to one at school, but fortunately it was not eaten.
Generally speaking all these things pass away with delivery, if not before, unless it be actual insanity, which sometimes remains. All that can be done is to attend strictly to the general health, keep the skin, bowels, and stomach, in good action, and remove all depressing or irritating circumstances. If there be a propensity to anything decidedly injurious or dangerous, the patient must be strictly watched, but without its being perceived or known by her, for fear of exciting suspicion in those who would be disposed to be cunningly secret or revengeful. Proper diet, regular bathing, and out-door exercise often correct many of these things.
These three terms mean spitting of blood, vomiting of blood, and bleeding from the nose, all of which frequently occur during pregnancy.
Spitting of blood is most usually observed in nervous women, and in those of a full habit. It is caused partly by sympathetic irritation, and partly by the womb pressing upwards against the diaphragm and lessening the size of the chest, which deranges the circulation in the lungs, and causes rupture of their blood vessels. The premonitory symptoms are pains round the waist, cold extremities, creeping of the skin, and a sensation of anxiety or depression round the heart. The attack begins by difficulty of breathing, heat in the chest, and dry cough, followed by spitting up more or less bloody frothy mucus; all[394] which symptoms are much increased by violent exercise, or a hot atmosphere. In ordinary cases a mere spitting of blood need occasion no great alarm, unless attended by symptoms of inflammation, or unless the patient has had cough, and other indications of pulmonary derangement before conception.
In hæmatemesis the blood is vomited from the stomach, and is in black clots, frequently mixed with the food, or bile, while that which comes from the lungs in spitting on the contrary is bright red, and quite fresh. In vomiting of blood also, there is seldom any cough or exertion of any kind.
The treatment of spitting of blood must be nearly the same as for many other derangements already described. When there is a full habit, the patient must live low, keep the bowels free, and the skin in good order, and avoid all agitation of mind or over exertion of body. An Opium pill occasionally will be useful, or a few drops of laudanum. The cough must be combatted in the way recommended in my previous article on Cough. Lemonade or tamarind tea, with some Syrup of Poppies added, may be freely drunk, or some of the black currant root tea. The treatment of Hæmatemesis is precisely the same. Occasionally however the blood will pass into the intestines and occasion colic, and then it must be removed by administering an enema of starch and castor oil, or a little manna may be taken.
Epistaxis, or bleeding from the nose, is much more frequent than either of the preceding, but is seldom of much consequence. In many cases in fact it is highly beneficial, as it relieves the head from pressure, and thus obviates many inconveniences. If it continue too long, or becomes excessive, it may generally be arrested by putting cold wet[395] cloths between the eyes, and on the cheeks, while the head is kept elevated. The feet and hands should be kept warm, and the air breathed should be as cold as possible. In extreme cases, the nostrils may be plugged with bits of sponge, or cotton, or some powdered alum may be snuffed up them. The best plan is to raise the hands above the head and put something very cold, as a lump of ice for instance, or a piece of cold iron, between the shoulders; this seldom fails.
Very often in pregnant women the veins in different parts, but particularly of the thighs and legs will swell out in knots, either singly or in bunches, sometimes like strings of beads, or like the links of a chain. These are called Varices, and occasionally they attain a large size, and extend to various other portions of the body, as the external lips, vagina, and mouth of the womb. Some women in fact have them over nearly the whole body. They are caused by the pressure of the womb on the large abdominal veins, preventing the return of the blood and disturbing the balance of circulation between the veins and arteries. In the majority of cases, unless very large, they cause but little inconvenience, and may be let alone, but sometimes they cause pain, or become so full that there is danger of their bursting, and then it is necessary to interfere.
The first thing to be done is to relieve the abdominal veins from the pressure of the womb, and this may be done by the patient keeping more or less the horizontal position, and carefully avoiding all violent exertion. The swelling is always worse during the latter part of the day, particularly if the woman has[396] been much on her feet, she should therefore apply a cloth roller round the limbs before she rises in the morning. If this be carefully put on, just tight enough not to interfere with the motion of the limbs, nor totally obstruct the circulation, it will prevent the varices to a great extent, if not altogether. Brisk friction with the hand will disperse the swelling in many persons, or warm fomentations, but sometimes cold bathing answers better. It is advisable always to disperse them as soon as possible, for if they remain too long that part of the vein becomes permanently weakened by being overstretched, and will be always liable to swell again from any slight cause. It is particularly advisable in these cases to avoid constipation, and also to keep the skin in good action by bathing and frictions.
If at any time one of these varices should burst, it need occasion no alarm, unless it be seated on a large vein, and the bleeding becomes profuse. To stop it, bind on firmly over the rent any firm cold body, as a flat stone, or a large silver coin, passing the bandage several times round. In slight cases a simple cold compress will be sufficient, or a little powdered alum, or some vinegar and water. In short any of the usual remedies for stopping bleeding from wounds. The female must be quite still till it is stopped, and must be careful when she begins to move about again, because it is liable to break out afresh. Those of a very full habit must live low, and avoid all stimulants, so as not to increase the quantity of blood in the body more than is necessary. It is advisable to remove the varices, as much as possible, before labor comes on, particularly if they are situated on the lips, or in the vagina, because they may burst during delivery and cause considerable[397] inconvenience, or even danger. It is rare that these swellings continue after delivery, but if they should do so, the same treatment must be persisted in as before.
These are troublesome annoyances at any time, but particularly during pregnancy, and unfortunately they are very common at that time. They are, no doubt, chiefly caused in the same way as varicose veins, that is by the enlarged womb preventing the proper flow of the blood in the small veins, and so causing them to swell, and form tumors. They may in fact be called varices, as truly so as those on the limbs. In many persons however they are undoubtedly brought on merely by Constipation, which will undoubtedly either cause them or make them much worse when otherwise produced. In general they become worse as the pregnancy advances, because the womb becomes larger and the bowels are more apt to be confined.
As long as they only cause inconvenience, without any particular distress or urgent symptom, they may be let alone, or be slightly treated in the way of palliation, till after delivery, when they will disappear. Occasionally however, they grow to a large size, so as to hinder the passage of the bowels, and prevent the patient from sitting down or walking. They may then cause inflammation, and bring on falling of the intestine, or abortion, by the straining which they necessitate when the bowels are moved. And even if these extreme results do not follow, there may be serious derangements of the general health, indicated by difficulty of breathing, sleeplessness, headache, and fever. In short there are few of the derangements[398] incident to pregnancy so annoying as this, and unfortunately, from its nature, the sufferer dislikes to speak of it and seek the necessary assistance. Many prefer undergoing the most excruciating agony for months, rather than complain, which shows the necessity for females knowing how to treat themselves, when possible.
The bleeding which sometimes takes place from Piles is more often beneficial than otherwise, unless it becomes excessive, from rupture of a large vessel, in which case, if the wound is external, it may be treated the same as the ruptured varicose vein; if it be internal, the remedies must be injected with a syringe, or a large roll of lint or cotton may be soaked in alum water and passed up the rectum. Frequently bathing the thighs and perineum with cold water will be sufficient.
To relieve the pain and swelling, the female should sit over the steam of hot water, and use the warm bath. If the piles are external, they should be bathed with hot milk and Laudanum, or rubbed with any soothing ointment, particularly the Cucumber Ointment, mentioned in my Diseases of Woman, or with Stramonium Ointment. If they are internal the milk and Laudanum should be injected if possible, or some thin starch and Laudanum, and a stiff roll of cloth may be smeared with the ointment and introduced. In general, ointments or other greasy matters are not so good as the milk or starch. In conjunction with this, the bowels must be kept free, either with enemas or castor oil, or by using a seidlitz powder in the morning. This is indispensable, for if constipation exists, no applications can render much service. The patient must also avoid fatigue, and not remain too long upon her feet, nor sit long, particularly[399] on a hard seat, and if she be of a full habit she must live low, to avoid making too much blood. It is also important, at all times, to avoid using drastic purgatives, such as Aloes, Colocynth, or Gamboge, as they always make piles much worse, or even cause them.
This affection also appears, like the preceding, to arise from obstructed circulation, but instead of the blood accumulating it is merely the serum, or watery portion of it. The swellings are generally whitish, and spread about, and a small pit remains in them when pressed with the finger. They are found on various parts of the lower limbs, and on the groin or abdomen, and also upon the external lips, in which place they are often exceedingly troublesome. As a general rule these swellings are of small account, and as they disappear with delivery, but little attention need be bestowed upon them. Sometimes, however, they become very extensive, and so engorged that they inflame and are extremely painful. They have even been known to mortify, and cause considerable sloughing, particularly when chafed and afterwards wet with the urine. In these extreme cases there may be serious disturbance of the general health, from the constant irritation, and from the patient being unable to walk about. I have often known the limbs and vulva covered with patches of Erysipelas from this cause. Sometimes the swellings even become so large that they interfere with the process of delivery.
The treatment of this affection consists in rest, particularly lying down, saline purgatives, regular, and frequent washing the parts with cold milk and[400] Laudanum, or with a solution of Borax, half an ounce to a pint of water, to be used cold and with a tea-spoonful of Laudanum added to it. Simple cold water is frequently quite sufficient. In general all kinds of ointments are injurious, but if other means fail to give relief, the Cucumber Ointment may be tried. The wash should always be used after urinating, and the parts must not be rubbed, but lightly dried with a piece of soft linen. Fullers earth is often an excellent application when there is chafing.
If the patient be of a full habit, she must carefully diet herself, and bathe regularly. If she be thin and weak, a generous diet will be advisable, with meat and even a little wine.
This consists in a discharge of water, more or less profuse, from the vagina, at various periods during pregnancy. Some females will only discharge a small quantity, at intervals, others will have a constant dropping, and others again will pour out an immense quantity, sometimes several pints, or even quarts, in the course of a few days. In general this water is quite limpid and colorless, but sometimes it contains much mucus, and at other times it is tinged with blood. It does not appear that this discharge leads to any evil result, even when excessive, and I only refer to it to relieve anxiety. The origin of this water is not yet ascertained, but it is generally thought to be secreted between the membranes and the womb, and to be quite distinct from the liquor amnii.
Occasionally the external lips will be covered with[401] pustules during pregnancy, and frequent discharges of mucus will occur from the vagina. They are both however caused by the unusual action of the uterine system, and merely require frequent bathing of the parts with milk and Laudanum, and regular action of the bowels. The most important thing to remark in connection with them is that they have often been mistaken, even by medical men, for the effects of syphilitic disease, and much distress has resulted from such mistakes.
Several derangements of the urinary organs are liable to occur during pregnancy, partly from sympathetic irritation, and partly from mere pressure. Some of these may be partially relieved, others have to be borne as patiently as they can be till delivery removes them.
The swollen womb often presses on the neck of the bladder, and hinders the passage of the urine, or even obstructs it sometimes altogether, and thus causes straining, burning heat, and great distension of the bladder. In some instances this passes off as the pregnancy advances, owing to the womb rising higher in the abdomen, but in other cases it remains more or less, during the whole term. It is particularly important, in such cases, that the female should not let the difficulty remain too long unremedied, for if the bladder be very full it may become utterly impossible to empty it by natural effort. Sometimes the difficulty is much lessened by lying on the back a short time before attempting to urinate, or by raising up the abdomen with the hand at the time. Many females can urinate with tolerable comfort while lying on the back or abdomen, and others are much[402] relieved by constantly wearing a bandage. Constipation always makes this difficulty worse, and sometimes even causes it, by keeping the rectum full and thus increasing the pressure. In all such cases it will be readily seen, that forcing medicines are not only useless, but liable to cause injury. The change of position, rest, and supporting the abdomen are the means to be relied upon. If these fail, and the urine accumulates, the catheter must be used. A warm bath, or fomentation with warm water and Laudanum, will assist, and sometimes relieve alone. To ease the burning and distress the patient must drink freely of gum water, or barley tea, with a little Syrup of Poppies.
There is one manœuvre which, if practised aright, will nearly always allow the female to urinate with ease, and fortunately she can practise it herself. It consists in introducing two of the fingers into the vagina, and raising up the womb, as if practising the ballotment. This removes the pressure from the bladder, and the urine then escapes by natural effort. A few trials will soon enable any one to do this, particularly if they notice well the form and position of the parts, as shown in the plates of this work. A lady who heard me mention this in one of my Lectures, afterwards stated that the knowledge of it enabled her to dispense altogether with the catheter, which she was previously necessitated to use during most of her pregnancy.
When there is merely a nervous irritation causing the difficulty, the warm bath, or fomentation with warm water and Laudanum will be sufficient, or a little Belladonna Ointment may be rubbed over the meatus urinarius, while some starch and Laudanum is injected carefully into the vagina.
These arise from the womb pressing on the nerves of the sacrum, and are therefore not under the control of medicine. All that can be done is to change the position of the body as much as possible, from lying down to standing up, and by turning from one side to another. Brisk rubbing with the hand will also assist in giving relief. The cramps however usually disappear after delivery, and must therefore be borne as patiently as possible till that takes place.
Having treated this affection fully in my Diseases of Woman, I cannot do better than extract the article from that work on the subject.
"This disease, though not so immediately dangerous as some others, is perhaps the most distressing that can be met with.
"It consists in an intolerable and incessant itching of the parts, which nothing seems to allay. Sometimes it is so bad that the female is almost tormented to death; she cannot see company, or walk out, and often shuts herself up alone in her agony. Many have fainted from it, and some have even become delirious. I have seen patients whose hands it was necessary to tie, to prevent them tearing themselves to pieces.
"The causes of pruritus appear to be most of those that produce simple inflammation, which it very frequently accompanies or precedes. Pregnant females are very liable to it, and in some it will continue, in spite of all that can be done, till after delivery, when[404] it usually disappears. I have known it produce abortion. Some females always have it at the menstrual period, and others during nursing. Occasionally there is a little eruption attending it, but not always, though the parts are generally swollen and red. Parasites are sometimes the exciting cause, and should always be destroyed immediately.
"The treatment consists in first attending strictly to the diet, which must be light and unirritating, and to the regular action of the bowels and womb; and in using the cooling washes and lotions before mentioned. If the itching still continues, use either of the following washes to the parts:—Sub. carbonate of potash three drachms, water four ounces; put a tea-spoonful of this into a quart of warm water, and use it three times a day.—A tea-spoonful of Eau de Cologne to a pint of warm water.—Sulphate of Zinc, half a tea-spoonful to a quart of warm water. Both these may be used many times in the day.—Borax half an ounce, Sulphate of Morphia six grains; pure water half a pint. This last seldom fails of giving relief. It should be applied three or four times a day, with a piece of soft linen, the parts being first washed with warm soap and water. A tea-spoonful of laudanum will sometimes answer as well as the six grains of Sulphate of Morphia.
"Caustic has been employed, and blisters to the inside of the thighs, but such violent remedies are seldom either necessary or serviceable. I have known the parts to be deeply scarified with the lancet, and even burnt with a red hot iron, without at all alleviating the pruritus.
"In young persons it seems to be often produced by constipation, worms, and gravel; but it most probably depends, essentially, on some impurity, or[405] irritating quality, in the blood, or in the natural secretions of the parts, which should therefore never be allowed to remain long unwashed.
"Sitting in cold water, and the application of ice to the parts, has given relief. I have also effected many cures, almost instantaneously, by means of a small Galvanic plate, so constructed as to be worn just within the vulva.
"All remedies must of course be applied with caution during pregnancy; and it must be recollected that sometimes the disease will continue, more or less, till after delivery, though the distress from it may be much alleviated."
Flooding is one of the most dangerous accidents that occur during pregnancy, its consequences being often of the most serious character. The causes that lead to flooding are very numerous, some of them predisposing to it, and others immediately exciting it. Among these may be mentioned a too full habit, violent exertion, falls, coughing, vomiting, straining from costiveness or violent purgatives, forcing medicines, criminal attempts at abortion, overwalking, blows on the abdomen, too much dancing, or running up stairs, strong mental emotions, fright, or anger, and certain excesses. The immediate cause is the separation of the membrane in which the fœtus is inclosed from the walls of the womb. Flooding may however result from the placenta growing over the mouth of the womb, and being torn as that opens—usually about the sixth or seventh month.—(See the article Flooding during Labor.)
In most cases flooding is preceded by dull pain in the loins and groins, and a sensation of weight and dragging. Similar sensations however are often produced by other causes, which makes it difficult to predicate, with any degree of certainty, whether the patient is about to flood or not. The very first appearance of blood from the vagina must therefore[407] be watched for carefully, as that removes all doubt, and warns us to be prompt with the proper remedies. Sometimes a female will flood internally, the blood being retained by the passage being closed or plugged up by clots, or by its passing behind the membranes, or under the centre of the placenta. These internal or concealed hemorrhages are very dangerous, as the patient may lose much blood before her condition is suspected. It is therefore necessary to bear this in mind, and carefully use every means to ascertain whether such an accident has occurred or not. In general the indications are pretty plain, the patient suffering from deep seated and distressing pains in the back and groins, with great weakness in the limbs, faintness, weak pulse, dimness of sight, ringing in the ears, coldness of the hands and feet, swelling of the abdomen, and finally fainting, particularly if the retained blood suddenly escapes, which it usually does.
In the early months there is more danger to the child from flooding than there is to the mother, because it is nearly certain to lead to abortion. In the latter months, on the contrary, the mother runs the greatest risk, as the child may then live if it be expelled, while the mother may sink and die from excessive loss of blood. There are many females of a very full habit, who suffer but little from hemorrhage, unless it be excessive, indeed some seem to be benefitted by it, and are thus relieved from headache and convulsions. It should, however, be carefully watched, and its effects duly noted.
The treatment of flooding must depend materially upon its severity, and the time when it occurs. In the early months, when the discharge is slight, and when it causes little distress, simple means will answer.[408] The patient must lie on her back, on a hard mattress, with the pelvis raised, by means of a pillow, higher than the rest of the body. The air must be kept fresh and cool around her; she must keep herself quiet in body and mind, live rather low, and drink freely of cooling drinks, such as soda water, lemonade, tamarind tea, or ice water. [The fullest directions for making and using all these drinks will be found in my "Diseases of Woman."]
If the flooding does not stop with these simple means, external applications must be made, of cold, wet cloths, or even ice, over the abdomen, and inside the thighs. Finally, if further treatment is still needed, cold astringent injections may be carefully thrown into the vagina. Cold water is perhaps as good as anything for this purpose, and I have frequently known a most severe flooding checked immediately by injecting cold water into the vagina and rectum, and applying cold wet cloths over the abdomen, and inside the thighs. Some astringent drink may also assist, such as a little syrup of comfrey, or extract of Rhatany, and particularly a tea made of the root of the black currant, as recommended in my "Diseases of Woman."—[A handful of the root may be boiled in two quarts of water, for twenty minutes; it should be sweetened to taste and drunk freely. The common blackberry, or the dew berry, is also excellent, though not so good as the black currant.]—If the patient be nervous and irritable, or suffer much from pain, an opium pill may be taken, or from ten to twenty drops of laudanum.
The general practice in these cases is to bleed freely and give opium! And as this practice certainly does succeed in many extreme cases, I should certainly recommend, if the simpler means fail, to[409] resort to it at once. I dislike bleeding very much, in any cases, and here it seems particularly inappropriate; I should therefore say try almost anything and everything first, but never obstinately refuse to do it if nothing else succeeds.
In some cases a plug or tampon is used, to fill up the vagina. It may be made of a roll of cloth, cotton, or a piece of sponge. This practice, however, is useless in the latter months of pregnancy, and very often fails even at other times. When it succeeds it causes the blood to coagulate, and thus closes up the mouths of the vessels. Quite as often, however, it only keeps it in, and makes it accumulate in the womb till it all rushes away at once; still it may be tried.
If the hemorrhages should occur so frequently, or be so excessive, in spite of all treatment, as to endanger the safety of the patient, there is no other resource left to save her life but to produce abortion, because the presence of the fœtus and its appendages is evidently then the irritating cause which keeps up the discharge, and it cannot be expected to stop till the womb is emptied.
When the fœtus is prematurely expelled before it can survive, it is called an Abortion, but if its expulsion take place so late that it can live, it is called Miscarriage. Both these are serious accidents. In abortion the child is lost, as a matter of course, but in miscarriage it may live, after the seventh month. The danger to the mother is considerable from both, though greatest probably from abortion. It is probable that many very early miscarriages take place[410] unperceived, the female suffering but little from the accident, and the embryo being too small to be seen, unless carefully looked for.
The most frequent periods for such accidents are found to be six months, five months, and three months; and what is very singular, a much greater number of male children are aborted than females, the proportion being about sixteen to eleven.
These accidents are so intimately connected with flooding, that many writers always treat of them together, considering the flooding merely as the most frequent cause and symptom of miscarriage or abortion. In speaking therefore of the immediate causes of premature expulsion of the fœtus, we place hemorrhage first, and the causes before enumerated which produce that as being its most frequent remote ones.
A full habit, with tendency to local congestion, seems to predispose a female very much to miscarriage; every one so constituted should carefully avoid luxurious living and an inactive life. Violent bodily exertion, falls, or blows, or strong mental excitement are most usually the immediate causes, though with some it will come on spontaneously without any such exciting agencies. Some females will miscarry many times in succession, and always so near the same period, that they can tell to a day or two when it will happen. It seems to become a habit of the womb with them to contract at that particular time, and the only way to break through the habit is for them to avoid becoming pregnant for some considerable time, say two or three years after, they may then go the full time, but will seldom do so if they conceive immediately after having miscarried. In some persons miscarriage is caused by[411] a too eager gratification of certain desires; but in others it may arise from the opposite cause.
There is a disease of the womb also by no means unfrequent, though but little understood, which undoubtedly causes much miscarriage, and that is Rheumatism of the Womb! This mostly exists before the pregnancy however, and should be then treated according to the plan laid down in my "Diseases of Woman."
Miscarriage also arises in many females from a rigid state of the muscular fibres of the womb, which not relaxing sufficiently to allow that organ to expand become irritated by the pressure they experience, and begin to contract. This contraction of the womb of course soon leads to the expulsion of its contents, the same as in real labor. Women with their first children are more liable to miscarriage than others on this account, the womb not having become habituated as it were to the necessary relaxation.
And this is the reason also why some females, after suffering from this accident many times in succession at last escape it. In general they miscarry early the first time, from the womb not relaxing sufficiently, but go a little longer the next time, and longer still the next, and so on till they reach the full period. The fibres of the womb have gradually become accustomed to relax, and have borne the irritation longer and longer each pregnancy, till at last they have forborne to contract till the proper time. I knew one female who miscarried twenty-one times in succession, getting gradually nearer to the full period each time, till at last she reached nine months, and was rewarded with a living child.
Sometimes the accident may be produced by a uterine tumor, by a great quantity of water in the[412] womb, or even by there being more than one child, because in either of these cases there is required more room than ordinary; and of course from the greater expansion required, the liability is increased. Various womb diseases may also be mentioned as causes, or adhesions of its walls or ligaments to the walls of the abdomen, and also a diseased state of the placenta. The pressure of corsets and tight dresses also not unfrequently lead to the same result. Some general diseases undoubtedly often cause miscarriage, such as measles, jaundice, scarlet fever, consumption, and probably many others, particularly those in which the quality of the blood is much altered, or the nervous power much exalted or depressed. Convulsions have already been mentioned as being frequent causes of miscarriage, and all strong mental or moral impressions. Indeed these last causes operate more than is suspected, and make it necessary for a pregnant female to be kept as calm in her mind as it is possible for her to be. I have even known one to miscarry from a fright in a dream.
It is also a fact, though not generally known, that there are certain diseases of the father that may produce miscarriage, and unfortunately they are of that kind that often remain for a long time in the system without much external manifestation, so that many persons think they are perfectly free from them even while they are working such mischief.
The death of the child also is sure to produce miscarriage, and this may result from various causes, such as external injuries and violence, or from remaining too long in the warm bath and thereby causing congestion of blood in the womb. Small pox and syphilis in the mother may also cause the death of the child,[413] though not always. Many having been born at full term with these diseases upon them.
In general the fœtus is expelled very soon after it dies, but occasionally it is retained for a considerable time, and may not pass away till it is completely decayed. It has even been known to become almost fluid, and several months elapse before it was entirely expelled. Most women know when it dies, by its seeming to fall down to the bottom of the abdomen, like a dull weight, and also by its feeling very cold. Very often, however, there is no indication of its death whatever. M. Chailly mentions a case where the embryo died, probably when about fifteen days old, but the placenta continued to grow, and the lady was delivered when about six months and a half gone of the dead embryo, only about a quarter of an inch in length, though the after-birth was nearly large enough for one of the usual size. In this case it had died but not decayed, and remained in the womb six months and a half. In cases of twins also, one will sometimes die at an early period, but remain till the other is born at full term.
The growth of the placenta over the mouth of the womb, and shortness of the chord, have already been referred to as causes both of flooding and miscarriage; and to these may be added monstrous or deformed fœtuses, which rarely reach the full term.
It is probable that there are many constitutional and individual peculiarities predisposing to miscarriage, with which we are not much acquainted, and which may account for the constant occurrence of that accident in many females, notwithstanding all we can do. A scrofulous taint is with good reason supposed to be one of these, and it is probable that the disease of the placenta, and its consequent separation from the womb, before referred to, is mostly[414] caused by a taint of this kind. In many instances, where a female has miscarried from no apparent cause, if the placenta be carefully examined it will be found dotted here and there with diseased spots, sometimes like scrofulous sores! It is advisable always to ascertain this, and to carefully examine the fœtus and its appendages. In all cases the advice I gave to keep from being pregnant for some time, will be found most likely to succeed in averting the accident, both because it gives the womb time to regain its strength and break through its habit, and also because it gives us time to operate upon the constitutional taint, if there be reason to suppose it exists.
It is a curious fact, but one often observed, that living in certain localities even predisposes to miscarriage. There is a certain district in France where the females are so liable to it, that all who can do so leave the place when they become pregnant, and thus escape the greater risk. Miscarriage also becomes epidemic at certain times, and prevails like contagious diseases; several instances of this are recorded in history.
Bleeding is also supposed to be a cause of abortion, and probably it may lead to it in certain states of the system, but by no means so certainly as many suppose. Instances have been known of pregnant females being bled from ten to twenty times without any evil result, even though carried so far as to make them faint. Mauriceau tells us of one who was bled ninety times, and yet was delivered of a healthy living child at full term. In like manner many other ordinary causes of abortion will often fail entirely of their usual effects. Thus Mauriceau informs us that a female seven months gone fell upon the hard pavement from a three story window and broke her arm,[415] but yet did not miscarry. Madame Lachapelle also tells us of a young pregnant woman who threw herself down stairs purposely, from fear that she should have to submit to the Cesarean operation, she having a deformed pelvis. The fall caused her death soon after, but did not make her miscarry. Certain powerful medicines are also taken by some, a very small quantity of which, in most cases, produces abortion immediately, but without effecting what they desire, though it sometimes poisons themselves.
Indeed the power which the womb sometimes exhibits to retain its contents in spite of the most violent disturbing agencies, is truly astonishing. Cases have been known even where the womb itself has been severely wounded, and yet miscarriage did not take place; as in the case of a poor country-woman whom I heard of, who accidentally fell upon a sharp wooden stake, and run it far into the body, injuring the womb in a terrible manner, but strange to say, though far advanced in pregnancy, she recovered and went safely through her full time. I have often known women begin to flood and suffer from dreadful pain, with other common symptoms of abortion, as early as the second month, and yet they went safely the full time, though these signs continued the whole time. In some cases the waters have even been partially discharged, and yet abortion did not result. M. Velpeau tells us of an instance where the bag of waters broke, in a female six months gone, and one arm of the child even came down into the vagina, and yet the arm returned, the discharge ceased, and she went her full term.
The progress of a miscarriage varies according to the time at which it occurs, and the causes from which it arises. When it results from any violence[416] or accident, it usually takes place in a short time, and is preceded by abundant flooding, which comes on immediately. The discharge of blood however, is lesser the nearer we approach the full term, so that a female six months gone is not in nearly so much danger from flooding as one only two or three months gone. The reason is this, in the early months nearly the whole of the fœtal membranes are attached to the womb, so that in case of their being separated, it bleeds from nearly all its internal surface, but in the latter months the only point of attachment is the placenta. In the latter months also the womb contracts vigorously, and so closes its vessels, but in the early months its contractions are comparatively feeble. In those cases also, where the child has been dead a considerable time before its expulsion, there is seldom much flooding, the connection between it and the mother having been more or less destroyed by decay of the parts. The same result mostly follows a miscarriage from internal disease, particularly of the placenta. Indeed in some of these cases, the blood-vessels connecting the fœtus with the mother have been so completely destroyed, that no blood whatever could escape from them.
In regard to the probable consequences of premature delivery, it has already been remarked that it is more dangerous in the early months than the latter. It may also be added that it is much more dangerous, at any time, when caused by violence of any kind, or by forcing medicines, than when it occurs naturally. The danger is much increased if it occurs during fever, or any eruptive disease, or if the patient be suffering from diarrhœa or convulsions. As a general rule we may say, in all cases, that miscarriage or abortion is always more dangerous to[417] mother and child than natural labor, both in its present and in its future consequences. During an attack of jaundice an abortion may terminate fatally in a few hours; and very frequently the trouble with the after treatment is very great and long-continued.
The treatment in an accident of this kind must vary according as we are required to prevent it, or to remedy the evils that follow when it has occurred.
If an abortion be threatened from any cause, the same general practice must be adopted as recommended for flooding, the indications being the same. I believe myself that in most cases, except from accidental violence or internal disease, miscarriage may be averted. I knew a lady who had miscarried many times, always at the same period, who avoided it at last by simply preventing constipation from the first commencement of pregnancy, and by using an enema every evening of warm starch and water, pretty thick, with about thirty drops of laudanum. This was administered by means of a common injection pipe, just before going to bed, and continued till after she had quickened, and repeated occasionally after that, if she felt any premonitory symptoms of uterine disturbance. If the patient be of a full habit, she should also, from the very beginning, live low, keep the bowels free, and the skin in good action, and take gentle regular exercise in the open air.
When all the means used are found of no avail, and it becomes evident that the fœtus must be expelled, every endeavor should be used to assist nature in its removal as early and as safely as possible. For this purpose the same treatment, as far as practicable, must be pursued as in a real labor. If the hand can be conveniently introduced, without undue force, it may be so, to remove clots, or to take hold[418] of any part of the fœtus which may present, and assist in its extraction. In the early months considerable help may be given, sometimes by introducing the finger into the mouth of the womb, with a little extract of Belladonna, to promote its relaxation, but no force must be exerted in doing so. If any part of the after-birth can be laid hold of it should be withdrawn, but no extraordinary effort must be used to reach it. Frequently it happens that a portion of the after-birth remains in spite of all attempts to take it away, and there is a possibility that it may produce inflammation of the womb, but no very serious apprehensions need be felt of such a result, providing the patient is properly attended to in other respects. The retained portion gradually decays, and passes away, merely occasioning inconvenience and being very offensive. The danger from leaving it except at a very late period, is generally thought to be less than that from using any forcible means to remove it.
The best means for correcting the offensive discharge are cleansing and antiseptic injections. Warm soap suds are very good, or a decoction of Peruvian bark in water. Strong coffee is also excellent, or a weak solution of chloride of lime. The bowels must be kept free, and the skin carefully cleansed and well rubbed. On all occasions when the hand can be introduced with moderate and safe efforts it should be so, and the after-birth removed.
In conclusion it should be remarked, that the tendency to miscarry, like many female diseases, is undoubtedly owing, in great part, to the general debility and weakness which characterizes so many women at the present day, and which is brought on chiefly by neglect of their physical education when girls, and by their artificial mode of life afterwards.
This is undoubtedly the most serious of all those maladies that so often follow labor. It appears from medical records that puerperal fever has been known from very remote times, and that it has frequently become epidemic, or has spread from one to another, like the Cholera. In hospitals this has often been observed, and also in cities, sometimes almost every female delivered in the place having been attacked while it prevailed. There is also no doubt but that it is contagious, or capable of being transmitted from one person to another, like small pox. Numerous instances have been known where nurses and physicians have conveyed it to all whom they attended, during a long period after having been with a single case. One physician, after attending a case of puerperal fever, lost nine patients successively from the same disease, before he suspected the cause, and an old nurse assured me, that when she was a young woman, she was the unfortunate means of conveying it to two females whom she visited, by merely having been in the room a short time with one who was suffering from it. It is therefore highly important that all persons who may happen to be with a female so affected should not attend another case of childbirth for some time, and particularly that they should not wear any portion of the same clothing they had then on, and that they[421] should bathe the whole body several times. If a case occurs in a hospital or other public institution, the female must be carefully isolated from all the others, and none of her attendants must be permitted on any account, to visit other puerperal patients, till after a sufficient time has elapsed, and every precaution has been taken.
The causes that produce this terrible disorder are not very well understood; some of them probably predispose to it before delivery, or even before pregnancy, while others are connected with labor and its consequences. Among the former may be mentioned, improper diet, an inactive life, anxiety of mind, bad air, a damp situation, a full habit, or great weakness, the frequent use of stimulants, and certain excesses! The principal causes operating immediately are difficult labors, violent treatment, the use of instruments, tearing away the placenta too soon, retention of the lochia, cold, rising from the bed too soon, depression or excitement of the mind, over exertion in talking to and seeing company, and neglect of cleanliness. The most frequent cause probably is cold or damp, which checks the lochia and the perspiration, and leads directly to inflammation. It is on this account that the complaint is nearly always worse in winter than in summer, and prevails most in low damp situations, and in badly ventilated apartments, or in those insufficiently warmed. In most warm countries, and in those of an equable temperature, where the females remain much in the open air, and use regular exercise, puerperal fever appears to be but little known.
The nature of this complaint appears to be a severe and sudden inflammation, commencing either in the womb or some of the neighboring parts, which, if not arrested, rapidly extends to all the organs of the pelvis[422] and abdomen, and hastens to a fatal termination with fearful speed. The precise seat, and place of commencement, of the inflammation, varies in different cases, but this makes little difference either in the symptoms, consequences, or treatment of the disease, and it is of but little use to give a separate name to all these various forms. Uterine Phlebitis, Metro Peritonitis, Puerperal Metritis, and Puerperal Peritonitis, are all essentially the same complaint, and identical with what is called Puerperal, or Childbed fever.
The disease generally appears from the second to the fifth day after delivery, but may be delayed as late as the fifteenth or twentieth day, or commences as early as two or three hours after; and has even been known to show itself before labor came on.
It usually begins with headache, general debility, uneasy feelings, creeping of the flesh, and chills: then follow tremblings, numbness of the limbs, cold feet and hands, with a burning heat in the body. The abdomen gradually gets tender, so that it cannot bear the slightest pressure, sharp pains are felt in various parts of it, and the patient continually complains of twisting and burning within. She prefers to lie on her back, with the head raised and the knees drawn up, so as to relax the abdominal muscles. Very soon she complains of great thirst, and cries out repeatedly from the sharpness of the pain; the headache increases, and the breathing becomes laborious. Hiccough generally occurs at an early stage, and is usually accompanied or followed by vomiting and diarrhœa, but sometimes by obstinate constipation. The abdomen continues to swell, and becomes still more tender, the face is pale, bathed with cold perspiration, and indicates in every line the anxiety and[423] suffering under which the patient labors. The features seem to be drawn upwards, and all together, or pinched up, and indeed the whole body seems to shrink. In general the lochial discharge either stops altogether or lessens very much, the breasts remain empty or nearly so, and the pulse is weak and irregular. In some few cases however, the lochia continues to flow, or even increases, and the breasts remain full up to the time of death. The urine is high colored and thick, and causes smarting and burning as it passes away. The tongue furs and becomes pointed, and pale colored. The eyes often seem much engorged, and the white part become yellow, as indeed the skin does over the whole body, owing to derangement of the bile, and alteration in the character of the blood. In most cases the mind retains its faculties nearly till dissolution, but there is frequently a vague sense of uneasiness and fear, with great depression of spirits and weeping. Some even feel assured, from the beginning, that they will never recover, and occasionally become delirious.
The duration of this disorder varies considerably, though in most cases it carries off the sufferer in a short time, frequently even in two or three days. It may however last five, ten, or twelve days, and has been known to do so fourteen.
The manner in which it terminates is also different in different cases. The fluid resulting from the inflammation may either be absorbed, or suppuration may ensue, and the matter be discharged, either from one of the natural passages or from an artificial opening; or it may not be discharged at all. Sometimes gangrene or mortification ensues, and sometimes the inflammation partly subsides and becomes chronic. When it terminates by resolution, which[424] is the most favorable mode, the patient begins to improve about the fourth or fifth day; the pains become less acute, the swelling and tenderness become less, and the milk, lochia, and other secretions that were suppressed begin to reappear. The patient is also able to lie either on the back or sides, and soon feels conscious herself that she is improving. But even when a turn for the better has decidedly taken place, too much confidence should not be prematurely felt, nor should there be any relaxation of attention, for the slightest causes may bring back all the symptoms with more than their former severity. When suppuration ensues, which is most commonly the case, a mass of fluid forms in the womb or abdomen, and is plainly indicated, either by its moving about or by a portion escaping from the body. In this case also the pain and tenderness decreases, and the abdomen seems less hard, but the pulse becomes weaker, a sense of weight is felt about the womb, the extremities become cold, chills come on, and gradually the powers of the system seem to fail till complete exhaustion ensues. When gangrene or mortification ensues, the termination is nearly the same, but more rapid, and all the above symptoms are more marked. When it passes into the chronic form, there is but little permanent abatement in the severity of the symptoms for some time; they partially lessen at intervals, but return again, sometimes with renewed vigor, and it remains long a matter of doubt whether the disease has really passed the critical period or not. Recovery takes place occasionally in this form of the disease, but more frequently the patient becomes daily weaker and more emaciated, diarrhœa and slow fever set in, the vital powers steadily sink, and at last death ensues. This fatal termination[425] may however be delayed for an indefinite period, and may ultimately result from Consumption or Dropsy, both of which frequently follow chronic puerperal fever.
In regard to the probable termination of this disease, but little hope can be entertained that it will be favorable. Nor are there many indications that can be relied upon with certainty, as to what course it is likely to take. In general it is favorable when the swelling subsides, and the pains abate in severity, and particularly if the milk and lochia begin to be secreted again. The indications are also good in proportion as the symptoms are mild, and when there is no great sympathetic disturbance of other parts of the system. It is regarded as unfavorable when the pain and tenderness extends over a large portion of the abdomen, and when the attack commences very suddenly. The danger is also considered greater in proportion as the disease begins nearer to delivery; and when its first symptoms exhibit themselves before labor it is always considered mortal. It is likewise more dangerous with twins than with a single birth, and with first children than afterwards. It is seldom possible however to come to any probable conclusion till between the fifth and tenth day, and even then it is in general a matter of great uncertainty.
The best treatment of this fearful disease is one of the greatest problems in medical science. So many different plans have been adopted, and with such various success, that the history of past cases affords but little reliable data to guide us in future ones. In general the most powerful antiphlogistic measures, or those thought most likely to reduce the inflammation at once, are immediately resorted to,[426] such as bleeding, purgatives, and cold bathing. Bleeding is in particular the great agent depended upon, either from the arm, or by cups and leeches to the abdomen and vulva. Dr. Gordon, of Aberdeen in Scotland, who once met with a regular epidemic of puerperal fever in that city, assures us that nothing else succeeded in arresting the disorder but copious and frequent bleeding, at the very commencement. He carried it so far as to take twenty-four ounces at once, and he says that when he did so the patient was nearly sure to recover, but that at first, when he only abstracted about twelve ounces, she was as nearly sure to die. In about fifty cases to which he was called in time, he only lost five, and taking the average of all he attended the recoveries were about two-thirds of the whole number, which is above the usual proportion.
It appears however, from the experience of the most eminent practitioners, that the bleeding must commence early; that the first abstraction should not be omitted beyond twenty-four hours after the first symptoms of the disease, and should be as much earlier as possible. With very few exceptions they also think Gordon's standard of twenty-four ounces not too much. Indeed it is generally admitted that if the blood be not drawn at first and in large portions, it had better not be drawn at all. There may be of course many peculiar circumstances that will make bleeding improper, which nothing but experience and observation will teach a practitioner, but the number of such cases is thought to be small. The use of leeches meets with but few advocates, and certainly they seem to have had but partial success, compared with the lancet. Dr. Collins of Dublin depended chiefly upon leeches and Calomel, but he[427] tells us that in eighty-eight cases fifty-six died when so treated, while in fifteen that were freely bled from the arm only eight died. In short it appears that the bleeding must be carried far enough, at the very beginning of the disease, to cut it short at once, or it will be of no avail, it being of little or no use merely to check it! In conjunction with the bleeding it is also usual to give enemas of starch and castor oil, or something similar, and to bathe the extremities in hot water.
I know that this practice of bleeding meets with strong opposition from many physicians, and that it is objected to by patients generally. I myself am as much opposed to it as any one reasonably can be, and I am well aware of the numerous evils which follow it, but still it cannot be denied that Dr. Gordon's plan has cured a greater number of cases of puerperal fever than any other yet tried. It is true that many of those thus cured may have afterwards died of dropsy, convulsions, typhus and other diseases produced by the bleeding, but then the risk they run of dying from these was less than that from the puerperal fever, and in a choice of evils we ought to choose the least. It should also be remembered that some eminent practitioners assert, if this plan be adopted promptly and fully, it will always cure, or at least with very few exceptions.
Several other modes of treatment have also been adopted to dispense with bleeding, some of which have been much more successful than others, though none so much so as we could desire. Thus some practitioners resort immediately to hot fomentations and sweating medicines, or a hot bath if convenient, together with brisk purgatives, and injections. Some depend upon Calomel in large doses, with leeches to[428] the groins and vulva. Others again use cold fomentations, and cold injections both to the rectum and to the vagina. Others again use blisters over the abdomen, in conjunction with purgative enemas and moderate bleeding; but this mode seems to do but little good. Another plan is to give about six grains of ipecac, and to repeat the dose several times, at intervals of an hour or less, in conjunction with purgatives and warm fomentations. Turpentine has also been used internally and by enema, but seems to have accomplished little good. Perhaps the most frequent plan after bleeding, is to rub one or two drachms of Mercurial Ointment well on the skin, over the abdomen, every two or three hours, sometimes for several days regularly; eight or ten grains of Calomel being also given daily, at the same time. This brings on salivation, and in many cases the symptoms begin to abate in severity as soon as that commences. I am not aware however, that this treatment is any more successful than bleeding, nor do I think the consequences afterwards, in a case of recovery, are any less to be dreaded. It is difficult in fact to say what plan can be best recommended, even in the majority of cases, and certainly no one yet tried is applicable to all, on account of the peculiarities and varying circumstances of each. If the practitioner or patient is not decidedly opposed to the bleeding plan, that has undoubtedly the best recommendation, from former success. Next to that perhaps comes the mercurial treatment, which usually meets with as much opposition as the bleeding, but which certainly has been frequently found efficacious. The other plans have met with but little favor, though possibly they might sometimes succeed when the rest fail.
If I were asked what I should advise for those who would not submit to the use either of the lancet or mercury, I should say, commence with a strong dose of Epsom Salts, or Jalap, and repeat it in about five hours after its full operation. Also apply warm fomentations to the abdomen, or put upon it a flannel bag full of hops soaked in vinegar, as hot as it can be borne, and put mustard poultices on the feet, and inside of the thighs. The hands must also be kept as warm as possible, and the head cool. The diet should be very spare, and contain nothing heating or stimulating, and cooling drinks, such as ice water, or cold lemonade, should be drunk freely. The purgative should be repeated at least every day, for two or three days, or more if the symptoms are not modified, and the mustard poultices may be regularly used to various parts of the limbs, for the same length of time. In conjunction with these means the breasts should also be kept warm, to promote the flow of the milk, and injections of starch and castor oil should be thrown up the rectum daily. The object being, as far as possible, to keep the surface of the body warm, and to cool the internal fever, at the same time that all the natural secretions are excited as much as possible to remove any morbid matter that may be formed. It should also be mentioned that the urine sometimes stops, or at least becomes very scanty and thick, in which case a little sweet nitre may be given, or if necessary the catheter must be used. Some bitter tea, as boneset or chammomile, should also be taken occasionally, and a James's Fever Powder with it once or twice a day, to promote perspiration; or if there be severe pains, a dose of Dover's Powders may be used instead.
If the disease passes the acute stage and becomes[430] chronic, the same means must be pursued, and with strict regularity, or there will be danger of its again becoming acute. In all cases send for the most experienced practitioner as early as possible, and whatever his plan may be, if his past success proves it to be tolerably successful, submit to it, whether it be bleeding, salivation, or anything else. If there be no one at hand on whom dependence can be placed, follow the plan I have laid down as nearly as circumstances will allow, but practise it fully without delay, and till a change takes place. Those persons who make light of this disease, and pretend to say that this or that simple treatment is all-sufficient, either deceive themselves or wish to impose upon others. There are few affections more serious, as will be evident when it is borne in mind that, on an average, two females die out of every three attacked by it. To avoid all liability to it as far as possible, attend well to the general health during pregnancy, have everything comfortable, clean, and wholesome, during labor, and be careful to avoid cold, damp, and all kinds of mental and bodily excitement afterwards. The assistant also, whoever it may be, must be as careful and as gentle as possible, so as to avoid all violence or undue force, and not to hurry nature. A want of attention to such simple details has, undoubtedly, brought on many attacks of this fearful disease that otherwise would never have been experienced.
The functions of the breasts are liable, from many causes, to become deranged, and such derangements may lead to serious results, both to the mother and the child. It is a common opinion that females who[431] nurse are not so liable to suffer in this way as those who do not, but experience proves this opinion to be untrue; nevertheless, as it is the duty of mothers to nourish their own offspring, it should be a subject of careful study to relieve them of this liability as far as possible, or to assist them when necessary.
Galacterrhœa. This means an overflow, or excessive secretion of the milk, which sometimes takes place, particularly in those who do not nurse. At the commencement of the milk fever, Galacterrhœa needs but little attention, but if it continue to the second or third day, proper remedies should be applied to correct it. These consist in complete rest, both of body and mind, cooling drinks, and spare diet. If these do not correct it soon, a flaxseed poultice should be placed on each breast, and the patient should be made to perspire, either by warm teas and clothing, or by means of steaming. The bowels should also be freely opened with castor oil, or a seidlitz powder, and it will often benefit very much to give warm water freely to drink, with ten grains of nitrate of potash (saltpetre) to the pint.
In those that nurse it is very seldom the case that the secretion of milk is too profuse, unless the child has been kept too long from the breast. As a general rule it should be put to nurse in a few hours after birth, even if there be no milk, because its suction will materially help to bring on the flow. It frequently happens, when the child is kept away till the milk comes, that the breasts have swelled so that the nipple is buried and cannot be laid hold of well by the mouth, in consequence of which the child does not get nourishment enough, and the breasts not being well emptied become engorged, and their functions deranged. All this may be avoided by[432] putting it too early. Sometimes however notwithstanding every precaution, the flow of milk is excessively great, and constitutes a real disease, which may cause great weakness and debility. In such cases it will generally be found that the diet is too stimulating or too rich, or that the bowels have been too inactive, and the first step towards an improvement must consist in correcting these faults. The skin should also be kept active by frequent bathing and good friction, and the quantity of nourishment taken should not be greater than the mere healthy support of the body requires. In particular no stimulating liquors should be used.
Agalaxy.—This complaint is the reverse of the former, as it consists in a deficient secretion of milk. The causes of this deficiency are various; sometimes it arises from a constitutional inertness of the breasts, sometimes from insufficient nourishment, and sometimes from profuse discharges in other parts. All excesses also tend to decrease the quantity of the milk, particularly those of a certain kind; and it is seldom so abundant or lasting either in extreme youth or advanced age. The appearance of the menses in like manner generally causes the flow to become less, and it ceases naturally in some much earlier than in others. Sometimes there is a deformity in the child's mouth, which prevents its sucking properly, and the milk may stop for want of being completely drawn. The breasts also may be diseased, or the nipple not sufficiently prominent, and the same difficulty be thus produced in another way.
In treating agalaxy, therefore, the first thing is to ascertain if there be no deformity or disease in either mother or child, which prevents proper nursing. If there be nothing of the kind, it must next be ascertained[433] whether the mother has any excessive secretion elsewhere, such as diarrhœa, great flow of urine, or heavy sweats; if she have, these must be corrected. It must next be seen if she takes sufficient nourishment, and of a proper kind for her stomach and bowels. Sometimes a little spiced wine is excellent, or some porter, with white meats, and arrow-root milk. If she be of a full habit, however, and makes much blood, the contrary course must be pursued, and the diet be made low and unstimulating, while the bowels are kept free and the skin in good action.
In many cases when the nipple is small, it may be much enlarged by titillation, just before the child is put to it, after which the suction will increase it still more.
If the female be advanced in life, or very weak, or if she becomes pregnant, it may be better to procure a nurse than to attempt to stimulate the flow at all. The appearance of the menses need not occasion a suspension of nursing, unless it evidently deranges the secretion of the milk, or affects the health of the mother; in either of which cases the child should be weaned at once.
Engorgement of the Breasts.—The breasts are liable to become swollen, or engorged, from colds, blows, hard nursing from the child, over feeding, and from soreness or excoriations preventing them being fully emptied. This state may occur at any time, but is most frequent a few days after delivery. In general there is no danger from it, unless it be very bad or continues too long; it may then inflame and discharge, or become permanently hardened. To prevent such accidents the breasts should always be sufficiently emptied, either by the child or by artificial[434] means, and every precaution should be used against cold or violence. Constipation must also be guarded against, and the diet and drink must be carefully observed, so that it be not too feeding, or too stimulating. Warm fomentations or poultices may also be used when the breasts are painful, and a Dover's Powder may be given at night, after bathing the feet in warm water, to promote perspiration.
Inflammation of the Breasts.—This is only a more advanced stage of the previous malady, produced by the same causes, and by want of timely attention. Like simple swelling, it may arise at any time during nursing, but is more frequent a few days after delivery. As soon as the inflammation commences the breasts become red, swollen, and excessively tender, particularly at one point, which soon begins to project like a nipple, if the disease is not stopped, and at last bursts and discharges the contained pus. Sometimes the inflammation is comparatively superficial, and extends only over a small portion of the surface, but at other times it goes deep and spreads wide. In proportion to its extent is the severity of the symptoms, which are those of inflammation in general, such as headache, thirst, fever, general uneasiness, and cutting pains in the part affected.
As soon as the abscess is formed and can be plainly discovered, it is usual to open it immediately, because the longer it remains the more extensive it becomes, and the larger portion of the breast becomes diseased. It is necessary however to be certain, before making an opening, that it is really an abscess on which we are going to operate, for sometimes a healthy part of the breast feels very much like one, and a mistake may easily be made; in fact such a mistake has often been made, and by men of experience[435] too. In the early stage of the inflammation every effort should be used to prevent an abscess from forming, by the use of purgatives, sweating medicines, low diet, cooling drinks, and warm fomentations over the whole chest. Some females practice cold fomentations over the breasts, and with good success, in the commencement of the inflammation, but it may increase the difficulty with others, and, so far as I have seen, is no more generally useful than the other method. The warm bath all over the body is also very serviceable in a number of cases.
It usually happens however, in spite of every precaution, that matter will form, and its discharge become necessary. As soon as this is evident, it should be promoted as much as possible, by hot fomentations and poultices, till the head of the abscess is sufficiently distinct for it to be safely opened. While the swelling is going on the pain is often very severe, and it should be eased as much as possible, by using laudanum in the fomentations, or by putting on an opium plaster. After an abscess has opened and discharged, it should be kept open for some time, by little pledgets of lint, to prevent its closing up too soon, otherwise a portion of the matter may be shut in by the wound healing over it, and another abscess will form. Warm poultices and lotions should also be used afterwards, to promote the discharge as much as possible, but they should not be used after it has evidently begun to cease naturally. In short every means pointed out should be used energetically in the first stage, to prevent the gathering, but if it takes place in spite of them, then it should be hastened and discharged as early as possible, to prevent its extending. After this, when it has evidently all escaped, the wound may be suffered to heal, and the[436] patient must be enjoined to be very careful in future, for the same accident will be very liable to reappear.
Sometimes these abscesses become very extensive, and remain for a long time. I have known ten or twelve on one breast, and I have known them to continue open for many months. When this is the case it is much to be deplored, as it is very likely indeed to destroy the breast, and may even lead to more serious results. Attention therefore cannot be bestowed upon them too early or too unremittingly, particularly if the female be scrofulous, or of a very full habit. Sometimes the inflammation attacks both breasts, and at other times only one, in which case every effort should be exerted to prevent its extending to the other. In many persons the same side is always affected, and becomes a scape-goat as it were for the other.
When the means used succeed in scattering the swelling, its dispersion is usually followed by some critical discharge, such as diarrhœa, or a great flow of urine, or even by profuse perspiration, which shows how nature operates in removing the diseased matter, and cautions us not rashly to check such discharges.
It is a very serious matter for the swelling to indurate or harden, as it sometimes will, without either scattering or dispersing, as it is then constantly liable to become worse again, besides destroying the structure of the gland. Every means should therefore be used to prevent this, by promoting its dispersion or discharge, in the way already pointed out. It is also very good in these cases to bathe frequently with alum water, or decoction of white oak bark, or even to rub on some of the Ointment of Hydriodate of Potassa, diluted with an equal weight of fresh lard. A piece as large as a hickory nut may be well rubbed[437] on twice a day, for three or four days, but it should be stopped immediately the swelling begins to subside, and not used again unless it still remains or again increases. In many cases pretty frequent friction, with the hand anointed with a little oil, will be all sufficient, especially if a hot fomentation be used afterwards.
Excoriations, or Cracks in the Breasts.—The annoyance from this cause is sometimes very great, the pain which is experienced when the child begins to nurse being so acute that it is impossible for the mother to allow it to remain. Frequently I have known it compel weaning much earlier than was desirable, and sometimes it has even been so bad, that the dress could scarcely be borne against the breasts. The precise cause of this liability to crack is not known, nor do we know of any certain means to prevent it. In many cases however I have known it prevented, to a great extent, by having the nipple gently sucked, very frequently, for six weeks or two months before childbirth. This hardens it, and if a wash of borax water be also used, after each time, it will be gradually prepared for its proper use. Our means of curing this troublesome affection are very limited, and frequently everything fails that is tried. The mucilage of Quince seed, prepared by bruising and boiling them in a small quantity of water, rubbed over the sores with a soft feather, immediately after nursing, often does much good. The mucilage from the tender tops of young sassafras sometimes succeeds better than that from the Quince, and a bruised leaf from the large horse-shoe Geranium, laid on like a poultice, is sometimes better than either. A good lotion may also be made with a quarter of an ounce of borax, and a tea-spoonful[438] of laudanum, to half a pint of warm water, to be used frequently during the day. Some females use a wash made of saleratus, with considerable benefit, and others find relief from one made of nut galls, or white oak bark. Most of these means however are well known, and many others also, which, like them, sometimes succeed and often fail. The artificial nipple, or shield, should be tried if none of these means succeed, and frequently it will enable the mother to allow the child to nurse, though it may not altogether prevent the pain.
It not unfrequently happens that the child's mouth may be diseased, particularly with apthæ, or thrush, and this may possibly keep up the excoriations; in like manner the state of the breasts may also influence the mouth, and therefore the condition of each should be well ascertained when anything is the matter with either.
This is often observed in childbed, and sometimes even comes on during labor. It is usually attributed to cold, and no doubt it often does arise from cold, but more frequently it is owing to sympathetic derangement, and from violent attempts to swallow during and after the pains. Many females in fact cry out at those times, that something has broken in the throat, and they fear they are going to suffocate. As a general rule the swelling gradually subsides in a short time, without any special treatment, but sometimes it increases and inflames, and an abscess forms which may become very troublesome, and even dangerous. To prevent this it should be frequently treated with warm fomentations and poultices, till the inflammation subsides, and then with[439] the same washes recommended for indurated or hardened breast, in the preceding section of this chapter. If the swelling becomes hard, and remains indolent, the ointment of hydriodate of potassa may also be prepared and used, as there recommended.
This is a painful tumefaction or swelling of one or both of the limbs, which comes on from the fifth to the fifteenth day after delivery. It generally commences with slight pain, or stiffness, or cramp, becoming more painful as it proceeds; but, sometimes, shooting, cutting pains, of great violence, are felt suddenly, at the very commencement. The swelling, also, sometimes comes on gradually, but, at other times, rapidly. In most cases the patient complains of a sudden pain in the groin and thigh, which is preceded by a chill followed by fever, and then the limb begins to enlarge. Most frequently the lower part swells first, and then it extends upward, sometimes, even to the hip. The skin, on the swollen part, looks white, shining and tight, as if ready to break; it is also extremely painful, so that pressure upon it can scarcely be borne. It looks in fact like a thin bag of skin filled with milk, and hence the name milk leg, from an idea that it was really filled with milk, which had, by some means, reached there from the breast. This idea is erroneous, in the sense it is usually taken; the milk does not flow into the leg as many imagine, nor is anything like it to be found there, except a peculiar thin, white matter, when it breaks. Still, however, a sudden stoppage of the milk may cause such a swelling, like a sudden stoppage of any other secretion, but in no other way.[440] It is, probably, most frequently produced by sudden cold, which checks that profuse perspiration into which females gradually fall immediately after delivery, and so drives the perspirable matter within, and causes inflammation and suppuration. A difficult or prolonged labor may also lead to it, by preventing, for a long time, the proper circulation of the blood through the large veins of the pelvis, and so engorging those below. Or the veins may become paralyzed, as it were, by the pressure they have sustained, and so become, for a time, unable to transmit the blood. In fact, both the veins and lymphatics become engorged, as if tied above the limb, and exhibit knots and bundles, like bunches of grapes.
Sometimes the fever will occur some days first, and the female cannot tell what it is owing to, till the swelling comes on; and even this may take place so gradually, and with so little pain, that the limb may be very large before it is observed. I have known females complain of a slight fever only, on going to sleep at night, and wake up in the morning with a confirmed case of milk leg; and I have known others start with a sudden pain in the groin, or hip, and be affected in the same way, in less than two hours.
The disease usually lasts from a month to seven or eight weeks, and terminates, either by a gradual resolution, or scattering, of the fluids, or by suppuration and discharge. When suppuration ensues, there will, sometimes, form one or more very large abscesses, which it may be difficult to heal, and which may lead to serious results, either from their extent, or from the constitutional irritation they produce.
The treatment, at first, consists in warm fomentations, such as those of poppy-heads, or hops, with cooling drinks, purgatives, low unstimulating diet, and[441] occasional doses of James's Fever Powder, to promote perspiration. This is intended to disperse the swelling, and, in general, it does so. If, however, the abscess forms and breaks, in spite of all the means used, it must be treated the same as abscess in the breast, previously described. In ordinary practice, it is the general custom to bleed at the commencement of the disease, or to apply leeches to the groin. This sometimes does good, but frequently is of no service at all, even if it does not make matters worse. I would, however, make the same remarks on bleeding here, as I did in regard to its use in puerperal fever, to which milk leg has a resemblance, in some respects.
Another practice is to use tight bandages, the same as for varicose veins, but I think the plan is not, in general, a successful one, though it may be occasionally. Plunging the limb in cold water, or keeping it wrapped in cold wet cloths, has succeeded much more frequently, and is, with some, a favorite remedy. Stramonium leaves boiled in vinegar, and laid on hot, will also effect a cure sometimes; and so will bathing with hot lye or alcohol. A large poultice of hops, soaked in hot vinegar, has also been found useful.
The bladder, from its position, is very apt to be inconveniently pressed during the passage of the child, and to be temporarily affected for a short time after, in consequence. Sometimes, the neck of the bladder will be paralyzed, and the urine cannot be discharged. In this case, fomentations of warm milk and laudanum must be used, or a[442] warm hip bath, if there be no danger of flooding, and the bowels must be freely opened. If this does not relieve, the catheter must be used, and always before the bladder is too full. To avoid its becoming so, the attendant should inquire of the female, during the first day, if she has urinated, or feels any inclination that way, so that he may know in time if the difficulty exists. In general, this paralysis passes off in the course of a day, but may endure longer sometimes; in which case the patient herself should speak of it. Cases have been known where the bladder has become so full as to burst through inattention to this matter. The contrary difficulty is occasionally observed, and the urine cannot be retained, but it flows away as fast as it is secreted. It is very seldom, however, that this state remains more than a single day and, more frequently only a few hours. A dash of cold water on the pubes, and against the meatus urinarius, has often corrected it at once, and so has a single purgative dose. If it remain after the first two days without amendment, it is customary to put a small blister on the abdomen, which usually relieves in a short time.
USE OF CHLOROFORM IN MIDWIFERY.
AN ENQUIRY INTO THE UTILITY AND PROPRIETY OF PREVENTING THE PAIN AND SUFFERING WHICH USUALLY ATTENDS CHILDBIRTH, WITH AN ACCOUNT OF THE MEANS TO BE EMPLOYED FOR THAT PURPOSE.
In the preface to this work I remarked that a great part, and, perhaps, nearly the whole, of the suffering and danger to which parturient females are exposed, arises, undoubtedly, from their bad physical education and mode of life; and that, in a more rational state of existence, it was probable that both would be so slight as to excite no apprehension. This improved state of things is much to be desired, and should, of course, be striven for by all friends of humanity. But, in the mean time, it is proper to consider whether there are any means by which those now living can be relieved in their hours of distress. The agony which many females endure at this time is so great that there are few circumstances under which relief is more needed, or would be more acceptable; and I, for one, cannot subscribe to the doctrine that such relief would be improper, unless it prove to be injurious. There are some persons, I know, who say that this suffering has been ordained for woman, and that it ought to be endured. This notion, I think, needs no refutation, it being just as unreasonable as to say that the sick should be allowed to suffer and die without assistance, because their condition has been ordained. There are others, and men of science, too, who think that the pains of childbirth are necessary to its safe accomplishment, and that they are also valuable in a moral point of view. This opinion will be examined by and by, and the facts on which it is founded, carefully analyzed; but it is first necessary to state the means of[445] prevention usually employed, and to note their mode of action, and effects.
Some years ago, a celebrated physiologist, who supposed that the chief cause of pain and difficulty in labor was the size and hardness of the child's bones, advanced the theory that if these bones were less developed, and softer, the pain and difficulty would be materially lessened, if not entirely removed. He proposed, therefore, since the hardness of the bones is caused by the deposition of lime in them, which is derived, of course, from the blood of the mother, that she should avoid taking anything to eat or drink, during pregnancy, that contained lime. This, he supposed, would keep the bones of the child soft till after birth, and so allow them to give way and crush together during delivery, and thus prevent the suffering and difficulty usually experienced. It was also thought that the bones of the mother would be partially softened at the same time, and give way a little, so as to facilitate the process still more.
I am not aware, however, that this theory has ever succeeded in practice, either in the human species or in the lower animals, though frequently tried. Nature will work on her own plan, and will develop the bones of the fœtus, while in the womb, to a certain extent, providing she has the means to do so; and if these are withheld, she is very likely to suspend its development altogether, rather than send it forth imperfect. I have known cases where everything was withheld, for the whole period, that contained a particle of lime, and yet the child's bones were as hard at birth as in any other case; the material being, probably, taken from the bones of the mother, which might be thus weakened, and made liable to displacement, without any good result whatever. It is also a question whether such a course, supposing it to succeed, might not be dangerous in another way, by causing an imperfection in the child which its future growth could not overcome. I have known some cases where this practice appeared to have caused abortion from imperfect development, and several others in which there was too much reason to fear that the[446] child was injured, though safely born. As this is, therefore, at best, a very uncertain and ineffective process, and is also, probably, dangerous to the mother or child, or both, it does not appear to me worthy of further attention, and I merely allude to it in order to make the present sketch of such means complete.
The other means are such as do not interfere, in any way, with the natural processes, but merely prevent sensation or feeling at the time of delivery. Mesmerism has been recommended, and, in some few instances, tried, for this purpose, but its success has either been so small, or its action so uncertain, that no dependance can be placed upon it, notwithstanding many persons assert its power. Opium and other powerful drugs have also been given, but so much of them is required, at that time, to produce a sufficient effect, that their use becomes dangerous. Other substances, in the form of vapour, or gas, have also been used, the effects of which only last for a short time, and are not, generally speaking, at all dangerous. Among them may be mentioned nitrous oxide, or laughing gas, carbonic acid, sulphuric ether, and chloric ether, all of which were first employed in severe surgical operations.
The success of these agents, especially ether and chloroform, in preventing pain, is undoubted; nor do they appear to have any other effect, nor to prevent any necessary effort or process of nature, except in a few cases which will be mentioned further on. Many hundred operations of the most severe kind, such as cutting off limbs, removing tumors, stones, and so forth, have been performed while the patients were under the influence of these agents, and without causing them the slightest pain; in fact, many remain, during the whole process, in a pleasant dream, and cannot be persuaded, when they wake, that the dreaded operation is over. The same thing has also been observed in hundreds of cases of midwifery, both in natural labor and when instruments have been used. In numerous instances the female has been put to sleep, and safely delivered, without knowing or feeling anything whatever, during the whole time;[447] the first intimation that she had become a mother, being the cheering cry of her newborn babe. In some instances, the state of insensibility has been continued for a long time, and during its continuance, the most hazardous operations have been safely performed.
So far as can be safely judged, from the limited time during which such means have been used, it appears that there is no danger whatever, from their employment, except when improperly administered, and in certain peculiar conditions of the system; which causes of danger will, of course, be removed by competent experience and knowledge. It is highly encouraging however, to note, though ether and chloroform have both been used so extensively and indiscriminately, both by those who understood their nature and those who did not, that the cases in which they are proved to have done injury, are not more than two or three; and in all those that I have heard of, some obvious impropriety had been committed in their use. It should be borne in mind, however, that even if the danger from them was considerable, we might still be justified in their use. It is well known that, in numerous cases, the fear of suffering, beforehand, and its severity while being endured, produce the most serious, and even fatal results. Many a patient has passed safely through the ordinary effects of a painful operation, and yet sunk from the mere effects of fear and physical suffering. Instances have even been known in which a fear of this kind has caused death, and frequently it has given a shock from which the patient never fully recovered. There is also, frequently, great danger from the violent efforts and struggles of a person in pain, and many necessary operations are even prevented altogether by them; this is often observed in difficult labors. When insensibility is produced, however, all these causes of difficulty and danger are removed; the patient's fears are quieted, suffering is entirely prevented, and there is no struggling to prevent the necessary assistance. Supposing, therefore, that the ill effects of these agents were more certain and greater in amount than has yet appeared, it would still be a question whether[448] the evil they really prevent is not greater than that which they possibly may cause.
In regard to the two agents now chiefly used, ether and chloroform, there is no difference in their mode of action, but the chloroform appears to be more speedy, certain, and efficacious, and is, therefore, the most valuable, but proportionably more dangerous when improperly administered. There are numerous instruments or inhalers, for administering these vapors, most of which are both costly and complicated, and all of which may be easily dispensed with. A very good plan is to take a large sponge and dip it in hot water, then squeeze out the water and pour on the ether or chloroform, and hold it over the mouth and nose. In two or three minutes consciousness and feeling will both be gone, and the patient will sink into a calm sleep which will last sometimes ten or fifteen minutes, and may be kept up as long as desired, by putting the sponge to the mouth for a few minutes whenever there are signs of waking. When it is left off the patient gradually comes round as if waking from ordinary sleep, and frequently speaks of having been in a dream, sometimes of a very pleasant character, but never knows what has taken place. No ill effects follow, but sometimes there is a little drowsiness or stiffness of the limbs, which soon passes off. A pocket handkerchief soaked in the fluid, and held over the mouth and nose will answer equally well; but whatever is used, it must not be pressed close, because a portion of air ought to enter with the vapor to prevent suffocation; and it should also be removed immediately the effect is produced. When it is borne in mind how much these requisites have been neglected, and how impure the ether or chloroform has often been, it is wonderful that more accidents have not occurred; and the fact that so few have happened under such a state of things, and with our little experience, goes far to prove that there is little or no danger at all in competent hands, with pure materials. The accounts circulated in the papers of "death from ether," and "fatal effects of chloroform," have mostly been gross exaggerations, and frequently[449] false altogether. In most of the cases where death has followed from the use of these agents, it has been proved to arise from other causes, and would have happened if they had not been used. In one or two cases, however, of surgical operations, the ether itself appears to have caused death by producing suffocation, or congestion of the lungs; but, even in these, it has been shown that it was used in an improper manner. Thus a young woman in Newcastle in England, inhaled ether to have a diseased toe-nail cut off, and died. It appears, however, that there was an evident disposition in her to congestion or rushes of blood, and therefore she was not a fit subject, and besides, the ether was poured on a thick table cloth, which, of course, prevented the entrance of air along with the vapor, and thus suffocated. I believe there is not a single case on record of injury resulting when due precautions have been used, and I have not heard of one at all in midwifery practice.
Ether having been the first article used, I shall first give an account of its effects, and then proceed to chloroform, explaining the mode of administration, and other incidental matters, as I proceed. The best article on ether which I have met with, is a review in the British and Foreign Medical Review for April, 1847, of some pamphlets on the subject, from which I shall make an extract.
In the state of perfect etherization we believe all sensation is abolished; in a less perfect state an obscure perception of external objects remains, while the sense of pain is extinct. The psychical state is various. Generally speaking, the sense of external impressions becomes at first confused, then dull, then false, with optical spectra or auditory illusions, general mental confusion, and then a state of dreaming or utter oblivion. In the majority of cases the mind is busy in dreaming, the dreams being generally of an active kind, often agreeable, sometimes the reverse, occasionally most singular; and, frequently, a great deal is transacted in the few short moments of this singular trance. Many of the patients who have undergone the most dreadful operations, such as amputation of one or both thighs or arms, extraction of the stone, excision[450] of bones, extirpation of the mamma, have readily detailed to us, and most with wondering thankfulness, the dreams with which, and with which alone, they were occupied during the operations. The character of the dreams seemed to be influenced, as in ordinary cases, by various causes, immediate or remote, present or past, relating to events or flowing from temperament.
A good many seemed to fancy themselves on the railway amid its whirl and noise and smoke; some young men were hunting, others riding on coaches; the boys were happy at their sports in the open fields, or the filthy lane; the worn Londoner was in his old haunts carousing with his fellows; and our merry friend, Paddy, of the London Hospital, was again at his fair, wielding his shelala in defence of his friends. Others, of milder mood, and especially some of the women patients from the country, felt themselves suddenly transported from the great city and the crowded hospital-ward to their old quiet home in the distant village, happy once more with their mothers and brothers and sisters. As with the dying gladiator of the poet, the thoughts of these poor people—
"Were with the heart, and that was far away."
Some seemed transported to a less definite but still happy region, which they vaguely indicated by saying they were in heaven; while others had still odder and warmer visions, which need not be particularized.
For the purpose of obtaining information on all the points of this most interesting subject, we personally questioned all the patients in the London hospitals, who, at the period of our visits, still remained in the wards after the ether-operations. They were in all fifty-four, and the great majority had been the subjects of capital operations. They were unanimous in their expressions of delight and gratitude at having been relieved from their diseases without suffering. In listening to their reports, it was not always easy to remain unmoved under the influence of the conceptions thereby communicated, of the astonishing contrast between the actual physical condition of the mangled body in its apparent tortures on the operating table of a crowded theatre, and the really happy mental state of the patient at the time.
This perfect freedom from pain is proved by every case wherein the vapor has been efficiently administered,[451] although there are frequently the same cries uttered, and the same motions practised as when pain is experienced which proves that nothing is prevented but the mere feeling, which it can be of no use whatever for any one to suffer from.
Chloroform has been more recently introduced than ether, but has nevertheless been used quite as much, or probably more, and, in general, with still more success. It was first described, I believe, by Professor Simpson of Edinburgh, at a sitting of the medical society of that city, in November, 1847, and several cases were narrated, two of which I quote.
I have employed it in obstetric practice with entire success. The lady to whom it was first exhibited during parturition, had been previously delivered in the country by perforation of the head of the infant, after a labor of three days' duration. In this, her second confinement, pains supervened a fortnight before the full time. Three hours and a half after they commenced, ere the dilatation of the os uteri was completed, I placed her under the influence of the chloroform, by moistening with half a teaspoonful of the liquid, a pocket-handkerchief, rolled up in a funnel shape, and with the broad or open end of the funnel placed over her mouth and nostrils. In consequence of the operation of the fluid it was once more renewed in about ten or twelve minutes. The child was expelled in twenty-five minutes after the inhalation was begun. The mother subsequently remained longer soporose than commonly happens after ether. The crying of the child did not, as usual, rouse her; and some minutes elapsed after the placenta was expelled, and after the child was removed by the nurse into another room, before the patient awoke. She then turned round and observed to me that she had "enjoyed a very comfortable sleep, and, indeed, required it as she was so tired, but would now be more able for the work before her." I evaded entering into conversation with her, believing, as I have already stated, that the most complete possible quietude forms one of the principal secrets for the successful employment of either ether or chloroform. In a little time, she again remarked, that she was afraid her "sleep had stopped the pains." Shortly afterwards her infant was brought in by the nurse from the adjoining room, and it was a matter of no small[452] difficulty to convince the astonished mother that the labor was entirely over, and that the child presented to her was really her "own living baby."
Perhaps I may be excused for adding, that since publishing on the subject of ether inhalation in midwifery, seven or eight months ago, and then for the first time directing the attention of the profession to its great use and importance in natural and morbid parturition, I have employed it, with few and rare exceptions, in every case of labor that I have attended, and with the most delightful results. And I have no doubt whatever, that some years hence the practice will be general. Obstetricians may oppose it, but I believe our patients themselves will force the use of it upon the profession. I have never had the pleasure of watching over a series of better and more rapid recoveries, nor once witnessed any disagreeable result follow to either mother or child, whilst I have often seen an immense amount of maternal pain and agony saved by its employment. And I most conscientiously believe that the proud mission of the physician is distinctly twofold—namely, to alleviate human suffering, as well as preserve human life.
In another part of the same publication Professor Simpson has another list of cases, all equally favorable. In some of these the labors were protracted many hours, and in others, operations with instruments were performed, of the most terrible character, such as would, under ordinary circumstances, have been attended with the most horrible suffering. As this article gives an instance of nearly every kind of delivery under the influence of chloroform, and contains also some admirable reflections upon its employment, I quote it in order to make the present account complete.
Case 2.—Seen with Mr. Carmichael; a second labor; she began the chloroform inhalation before the dilatation of the os uteri was entirely completed; the child was expelled in fifty minutes afterwards. I kept her under the chloroform for a quarter of an hour, till the placenta was removed, the binder applied, and the body and bed-clothes were arranged and adjusted. On awaking she declared that she had been sleeping refreshingly; she was quite unaware that the child was born, till she suddenly heard it crying at its first toilet in the[453] next room. An hour afterwards she declared she felt perfectly unfatigued, and not as if she had borne a child at all. In her first or preceding confinement she had been in severe labor for twenty hours, followed by flooding. No hæmorrhage on the present occasion.
Case 3.—Patient unmarried; a first labor; twins; the first child presented by the pelvis, the second with the hand and head. The chloroform was exhibited when the os uteri was nearly fully dilated; the passages speedily became greatly relaxed, (as has happened in other cases placed under its full influence,) and in a few pains the first child was born, assisted by traction. I broke the membranes of the second, pushed up the hand, and secured the more complete presentation of the head; three pains expelled the child. The mother was then bound up, her clothes were changed, and she was lifted into another bed; during all this time she slept soundly on, and for a full hour afterwards, the chloroform acting in this as in other cases of its prolonged employment, as a soporific. The patient recollected nothing from the time of the first inhalations, and was greatly distressed when not one but two living children were brought in by the nurse to her. Dr. Christison, who was anxious to observe the effect of the chloroform upon the uterus, went along with me to this patient.
Case 4.—Primipara; of full habit; when the first examination was made, the passages were rigid, and the os uteri difficult to reach. Between six and seven hours after labor began, the patient, who was complaining much, was apathized with the chloroform. In about two hours afterwards, the os uteri was fully dilated, and in four hours and a half after the inhalation was begun, a large child was expelled. The placenta was removed, and the patient bound up and dressed before she was allowed to awake. This patient required an unusual quantity of chloroform, and Dr. Williamson, who remained beside her, states to me, in his notes of the case, "the handkerchief was moistened often, in order to keep up the soporific effect. On one occasion I allowed her to emerge from this state for a short time, but on the accession of the first pain, she called out so loudly for the chloroform that it was necessary to pacify her by giving her some immediately. In all, four ounces of chloroform were used." Like the others, she was quite unconscious of what had gone on during her soporised state, and awoke altogether unaware that her child was born.
Case 6.—Second labor. The patient—a person of a small form and delicate constitution—bore her first child prematurely at the seventh month. After being six hours in labor, the os uteri was fully expanded, and the head well down in the pelvic cavity. For two hours subsequently it remained fixed in nearly the same position, and scarcely, if at all, advanced, although the pains were very distressing, and the patient becoming faint and exhausted. She entertained some mistaken religious feelings against ether or chloroform, which had made her object to the earlier use of the latter; but I now placed her under its influence. She lay, as usual, like a person soundly asleep under it, and I was now able, without any suffering on her part, to increase the intensity and force of each recurring pain, by exciting the uterus and abdominal muscles through pressure on the lower part of the vagina and perinæum. The child was expelled in about fifteen minutes after the inhalation was commenced. In a few minutes she awoke to ask if it was really possible that her child had been born, and was overjoyed to be told that it was so. I have the conviction, that in this case the forceps would in all probability have been ultimately required, provided I had not been able to have interfered in the way mentioned. I might, it is true, have followed the same proceeding, though the patient was not in an anæsthetic state; but I could not have done so without inflicting great agony upon her.
Case 7.—A third labor; the patient had been twice before confined of dead premature children; once of twins, under the care of Mr. Stone, of London; the second time of a single child under my charge. The liquor amnii began to escape about one o'clock, A.M., but without pains for some time. I saw her between three and four o'clock, with the pains commencing and the os uteri beginning to dilate. In two hours afterwards, the third stage was well advanced, and the pains becoming very severe, she had the chloroform exhibited to her, and slept soundly under its influence. In twenty minutes the child was born and cried very loudly without rousing the mother. In about twelve or fifteen minutes more she awoke as the application of the binder was going on, and immediately demanded if her child was really born alive, as she thought she had some recollection of hearing the nurse say so. She was rejoiced beyond measure on her son being brought in and presented to her.
Case 9.—In the Maternity Hospital; first child. Labor[455] began at 10 P.M., (Nov. 21st.) I was desired to see her at six A.M., (22nd.) The os uteri was well dilated, but it was evident that the pelvic canal was contracted throughout, and the head was passing with unusual difficulty through the brim. The patient was complaining much of her sufferings. It was evident that it would be a very tedious, and probably, at last, an instrumental case, and one therefore calculated to test the length of time during which chloroform might be used. She began to inhale it at a quarter past six, A.M., and was kept under its influence till a quarter past seven, P.M.,—the date of her delivery—thirteen hours in all. From the time it was begun till the time delivery was completed, her cries and complaints ceased, and she slept on soundly throughout the day. The bladder required to be emptied several times with the catheter. The head passed the os uteri at ten A.M., and during the day, gradually descended through the pelvis. At seven P.M., I at last deemed it proper to deliver her by the forceps; the head, which was now elongated and œdematous, having by that time rested for some hours against the contracted pelvic outlet, with little or no evidence of advancement; the bones of the fœtal cranium overlapping each other, and the fœtal heart becoming less strong and distinct in its pulsations. A warm bath, irritation of the chest, &c., were necessary to excite full and perfect respiration in the infant. Whilst we were all busied with the infant, the mother lost some blood, but the placenta was immediately removed, and the uterus contracted perfectly. On afterwards measuring the quantity of blood lost, it was calculated to amount to fifteen or eighteen ounces. The mother's clothes were changed, she was bound up, and removed to a dry bed before she awoke. She had at first no idea that the child was born, and was in no respect conscious of being delivered. In fact, she had been "sleeping," according to her own account, from the time she had begun the inhalation, and thought she remembered or dreamed that she heard Dr. Williamson, the house-surgeon, speak near her once or twice. Dr. Beilby, Dr. Ziegler, &c., saw the case with me. Three days afterwards I found the mother and child perfectly well. She continued to recover so rapidly, that she insisted on leaving the hospital on the tenth day after delivery.
A sufficient number of such accounts as these could[456] be collected to fill a large volume; but these are quite sufficient for our purpose.
In regard to the objections to using chloroform or ether, in midwifery, it will be thought by most persons, and with good reason, too, that the safety and success which has attended their use, is itself a sufficient answer to all objections.
It was at first thought, by some physicians, that the expulsive force of the womb was lessened when the pain was prevented; but this is not the case; on the contrary, it has been, in many cases, much increased. It was also thought by others that there was more danger from flooding, and convulsions, than in ordinary cases; but this is also equally at variance with truth, for it appears, beyond doubt, after a careful examination of all the cases recorded, that there is much less danger, particularly from convulsions, than when the patient is allowed to be tortured and terrified by feeling pain. Dr. Simpson remarks in another part of the article above quoted:—
The question which I have been repeatedly asked is this—Will we ever be "justified" in using the vapor of ether to assuage the pains of natural labor? Now, if experience betimes goes fully to prove to us the safety with which ether may, under proper precautions and management, be employed in the course of parturition, then, looking to the facts of the case, and considering the actual amount of pain usually endured, I believe that the question will require to be quite changed in its character. For, instead of determining, in relation to it, whether we shall be "justified" in using this agent under the circumstances named, it will become, on the other hand, necessary to determine whether, on any grounds, moral or medical, a professional man could deem himself "justified" in withholding and not using any such safe means, (as we at present presuppose this to be,) provided he had the power, by it, of assuaging the pains and anguish of the last stage of natural labor, and thus counteracting what Velpeau describes as "those piercing cries, that agitation so lively, those excessive efforts, those inexpressible agonies, and those pains apparently[457] intolerable," which accompany the termination of natural parturition in the human mother.
Since the latter end of January I have employed etherization with few and rare exceptions, in every case of labor which has been under my care. And the results, as I already stated in The Lancet, have been, indeed, most happy and gratifying. I never had the pleasure of watching over a series of more perfect or more rapid recoveries; nor have I once witnessed any disagreeable result to either mother or child. I do not remember a single patient to have taken it who has not afterwards declared her sincere gratitude for its employment, and her indubitable determination to have recourse again to similar means under similar circumstances. Most have subsequently set out, like zealous missionaries, to persuade other friends to avail themselves of the same measure in the hour of suffering. And a number of my most esteemed professional brethren in Edinburgh have adopted it with success and results equal to my own. At the same time, I most sincerely believe that we are, all of us, called upon to employ it, by every principle of true humanity, as well as by every principle of true religion. Medical men may oppose, for a time, the superinduction of anæsthesia in parturition, but they will oppose it in vain; for certainly our patients themselves and their friends will force the use of it upon the profession. The whole question is, I believe, even now, one merely of time. It is not—Shall the practice come to be generally adopted? but—When shall it be generally adopted? And, for my part, I more than doubt if any man (rejecting willingly its benefits) is really justified, on any grounds, moral or medical, in deliberately desiring and asking his patients to shriek and writhe in their agonies for a few months, or a few years longer, in order that, by doing so, they may defer, forsooth, to his professional apathy, or pander to his professional caprices and prejudices.
Another objection has also been advanced against the employment of ether or chloroform, the force of which must be estimated by every one for themselves. It is well known that many, if not most of the lower animals during labor, or immediately afterward, experience certain feelings and desires stronger than at any other time; and it is supposed that such would be the case, as[458] a general rule, with human beings, if it were not for the pain which overpowers everything else. This supposition has, in fact, been partly verified in a few cases; several females having confessed, after recovering from a painless labor under the influence of ether, that their dreams during the sleep were of a peculiar warm character! How far this may be generally the case, of course, we have no means of ascertaining, nor do I consider it to be practically of any consequence to know, because it can in no way interfere with the safe progress and termination of the labor, which alone is what we are properly concerned in. I have merely thought it proper to state the fact as being a singular one, and to make my readers acquainted with it. Physicians are well aware that the peculiar feelings referred to are frequently produced by various causes which act on the nervous system, such as mesmerism, and even by strong devotional excitement. I have known females with strong moral impressions who always carefully avoided both the above causes, from having discovered their liability to produce such effects; in fact, this has been one objection raised to allowing mesmerists to operate upon young persons, and several cases of moral failing having been attributed to this cause. It is not at all improbable, therefore, that such results may occasionally occur during labor, though we are not at all justified in assuming that they will in any particular case. How far this may be considered an objection to the employment of such means, must be however, as I before remarked, decided by all persons for themselves, and for themselves only! It is not a medical question at all.
Notices of Dr. Hollick's Lectures.
Dr. Hollick and Physiology.—The second of a series of Lectures, by this gentleman, on human physiology, and the all important truths connected with our physical constitution, was attended by a full house, in National Hall, last evening. The time was well spent, and so appeared to think the audience. On the delivery of the first of these Lectures on Tuesday evening, the speaker in a comprehensive and well-digested exordium, placed himself and the subject right with the public. His manner, language and style, did the first; his sound logic, his argument, his candor and research, accomplished the second. Apart from the interesting and apposite details of the wonders of reproduction, the illustrations of the immutable wisdom of nature, which teem in the animal and vegetable worlds—which
"Glows in each stem, and blossoms in each tree;
Lives through all life, extends through all extent,
Spreads undivided, operates unspent."
Apart from all this, Dr. Hollick's Lecture was excellent as a defence of truth, a vindication of the right of free and unshackled inquiry, and as a convincing refutation of that silly, but far too prevalent opinion that there are truths of which it is better to remain in a state of ignorance. Had nothing else been imparted in the forcible and well defined exordium of Dr. Hollick than this judicious demolition of that fallacious, silly, but injurious twaddle which would forbid research to pass in advance of the old landmarks prescribed by custom, ignorance, or a spurious morality—even that would well deserve the public patronage. Truths, well set forth, will make an impression, whether their investigation be fashionable or not. There is an affinity between the capacity to learn, and the truths to be learned, which always results, when a fitting opportunity is presented, in a free inquiry, and the gentleman who is bringing, in a judicious and elevated manner, a knowledge of those fundamental principles of our corporeal existence which are abused because unknown, will accomplish more good than half a dozen teachers of higher pretensions, and lower ability. It was gratifying to observe the decorum—the sense of respect for both speaker and subject, that was observed throughout the evening, which evidently shows that those who go there are actuated by higher motives than mere curiosity; by desires more ennobling than a passing gratification; in a word, it was clear that those who composed Dr. H.'s hearers, were men who know and dare to think, and who will profit by these most useful discourses.—New York Herald, Aug. 7, 1844.
The Origin of Life.—We attended Dr. Hollick's Lecture at the Masonic Hall, on Monday evening, and if we were to say we were delighted, we should but feebly express the gratification we experienced. It was, in fact, a whole series of anatomical lectures crowded into one, and that one so divested of technicalities, and rendered so concise, so intelligible to the most illiterate mind, and withal couched in such delicate as well as perspicuous language, that the most fastidious could find no fault, nor the idlest curiosity go away uninformed. The[460] human figure—a French model, made, we believe, of papier mache—is beautifully constructed, and every trifling organ is not only an accurate counterpart of nature, but can be taken apart, opened, examined, &c., with an ease that renders the study as perfect as an actual dissection, without the desagremens that attend a scrutiny of the real subject. We advise all who love knowledge, and particularly a knowledge of their physical organization, to attend these lectures.—Phila. Spirit of the Times, Dec. 4, 1844.
At a Meeting of the Class attendant upon Dr. Hollick's Select Lectures on the Physiology and Philosophy of the "Origin of Life" in Plants and Animals, held at the Lecture Room of the Museum, Wednesday evening, December 1, 1844, George G. West, Esq., was called to the Chair, and Samuel W. Black appointed Secretary.
Resolved, That we have listened with unfeigned pleasure and interest to the Course of Lectures delivered by Dr. Hollick, and now brought to a close, and that we deem it an act of justice to him and the community, to express our entire confidence in his character, ability, and the manner of illustrating his subject, which, to use the words of a daily journal, "is couched in such delicate as well as perspicuous language, that the most fastidious could find no fault, nor the idlest curiosity go away unimproved."
Resolved, That a committee of three be appointed to tender to Dr. H. the thanks of the Class for his courtesy to the members in affording them every facility for obtaining information upon the subject of his Lectures, and that he be requested to repeat the Course at the earliest period consistent with his other engagements.
Published in all the Philadelphia daily papers of December 14, 1844, and signed by one hundred and forty of the most respectable and influential inhabitants.
(See similar Resolutions, with over two hundred names attached, in the Philadelphia daily papers of March, 9, 1844; also of March 16; and on several other occasions.)
From the Philadelphia Daily Papers, Feb. 21, 1845.
At a meeting of the Ladies composing Dr. Hollick's Class, held on Wednesday afternoon, February 19th, in the Lecture Room of the Museum, the following Resolutions were unanimously adopted, and ordered to be published in one or more of the city papers:
Resolved, That we have listened with great pleasure and interest to Dr. Hollick's Lectures, and are happy to add our testimony to the many already recorded in behalf of such Lectures: and regarding Dr. Hollick as a benefactor of his race, and especially of our sex, we cordially wish for him abundant success, and ample reward in the consciousness of doing good.
Resolved, That we will exert ourselves to induce our female friends and acquaintances to avail themselves of the great and rare privilege of obtaining the valuable instruction imparted in these Lectures in so chaste and dignified a manner.
Signed on behalf of the meeting by
(See also similar Resolutions, with numerous names, on Feb. 27, 1846, March 20, 1846, and on April 10, 1846, with over three hundred names attached.)
Dr. Hollick's Lectures.—These Lectures continue to attract much attention, and are commended by all who hear them. During the past week Dr. H. has given a private Lecture and exhibition of his models to many of our prominent Senators and public men, all of whom expressed themselves highly gratified, and desirous that another class should be formed to accommodate their friends who had not attended.—National Intelligencer, Jan. 30, 1846.
Dr. Hollick is a gentleman of no less knowledge in his profession than eloquence in his means of imparting it, and he is certainly deserving of great credit and support for his exertions in a new field of such universal importance. We commend these Lectures with the fullest confidence to the attention of our citizens.—N. Y. Sun, Aug. 6, 1845.
"LETTERS FROM NEW YORK, NO. 11."
" * * * * There have been several courses of Lectures on Anatomy, this winter, adapted to popular comprehension. I rejoice at this; for it has long been a cherished wish with me that a general knowledge of the structure of our bodies, and the laws which govern it, should extend from the scientific few into the common education of the people. I know of nothing so well calculated to diminish vice and vulgarity as universal and rational information on these subjects. But the impure state of society has so perverted nature, and blinded common sense, that intelligent women, though eagerly studying the structure of the Earth, the attraction of the Planets, and the reproduction of Plants, seem ashamed to know anything of the structure of the human Body, and of those Physiological facts most intimately connected with their deepest and purest emotions, and the holiest experience of their lives. I am often tempted to say, as Sir C. Grandison did to the Prude—'Wottest thou not how much in-delicacy there is in thy delicacy?'
"The only Lectures I happened to attend were those of Dr. Hollick, which interested and edified me much. They were plain, familiar conversations, uttered and listened to with great modesty of language, and propriety of demeanor. The Manikin, or Artificial Anatomy, by which he illustrated his subject, is a most wonderful machine invented by a French Physician. It is made of papier mache, and represents the human body with admirable perfection, in the shape, coloring, and arrangement, even to the minutest fibres. By the removal of wires it can be dissected completely, so as to show the locality and functions of the various Organs, the interior of the Heart, Lungs, &c.
"Until I examined this curious piece of mechanism, I had very faint and imperfect ideas of the miraculous machinery of the house we live in. I found it highly suggestive of many things to my mind." * * *
L. M. C.
[Extract from a Letter in the "Boston Courier" of Monday, June 3d, 1844, by Mrs. L. M. Child.]
Dr. Hollick's Lectures.—We cordially say to those who love a scientific treat not to fail to attend. More instruction is contained in those three Lectures, than can be mastered by a twelve month's reading.—Baltimore Clipper, March 30, 1847.
WRITING DESK AND GOLD PEN PRESENTED TO DR. H. BY ONE OF HIS LADY CLASSES.

Dr. Hollick—Dear Sir: The members of your class, desiring the gratification of offering you some testimonial of their personal regard, and grateful appreciation of the benefits which you are conferring upon them and their sex generally, respectfully request your acceptance of the accompanying writing desk.
Were it necessary, we might repeat our assurances that your services to humanity will be, by us, long and gratefully remembered. The women of this generation have reason to rejoice that, by your efforts, a new and extensive field of information has been opened to them, whence they may derive treasures of knowledge, of immense importance to themselves and their posterity, hitherto concealed within professional enclosures.
Wishing you health and happiness, we beg leave to subscribe ourselves,
Truly your Friends,
Signed on behalf of the class by,
M. G.
Philadelphia March 20, 1845.
NOTICES OF BOOKS.
From the New York Herald.
Outlines of Anatomy and Physiology, with a Dissecting Plate or the Human Organization, by Frederick Hollick, M. D. We regard this as one of the most valuable works issued in a long time. It is a complete general treatise on anatomy and physiology, and the dissected plate answers the purpose of a model of the human frame. Dr. Hollick is entitled to great credit for his laudable desire to disseminate a knowledge of subjects that are of such vital consequence to all, but which hitherto has been monopolized by the medical profession. We commend it to all as a work of great merit and usefulness.
From the Patriot, Baltimore, March 24th, 1847.
Outlines of Anatomy, &c.—Dr. F. Hollick, whose history as the great simplifier of the human anatomy, so well known throughout the country, and whose public Lectures have won for him so high a reputation, has just published a work which he designates "Outlines of Anatomy and Physiology for Popular Use." This book contains a very curiously and ingeniously arranged plate, which opens by pieces, so that the different parts of the organs of the human system may be seen in all their variety, all of which are fully explained in English. The second part of this invaluable work gives a general description of these organs and parts of the system, under the division of bones, muscles, arteries, veins, &c., &c. This work should fall into the hands of every family.
From the New York Argus, January 9, 1847.
Neuropathy.—This is a new name, but a good one, being the title of a work by Dr. F. Hollick, whose excellent Lectures on various subjects will be remembered by many of our citizens. In this work is explained the action of Galvanism, Electricity and Magnetism; Homœopathy and Allopathy are contrasted in theory and practice; Mesmerism is discussed, and other subjects "too numerous to mention," treated in a manner at once novel and instructive. Dr. Hollick has also published a work on "Anatomy and Physiology for Popular Use," illustrated with a new dissected plate of the human organization, of most ingenious construction. Of this work we shall have more to say anon. It is no ordinary production.
From the New York Sunday Times and Messenger, Jan. 10, 1847.
"Outlines of Anatomy and Physiology, for popular use," illustrated by a new dissected plate of the human organization, and by separate views. The work is designed either to convey a general knowledge of these subjects in itself, or as a key for explaining larger and more complete works. These Outlines should be in the hands of every body; and Dr. Hollick, or any one else, is a public benefactor who furthers the publication of such able, interesting, and truly important works.
From the Pennsylvanian, (Philadelphia,) Jan. 26, 1847.
The following in regard to two works from the pen of Dr. Hollick, of this city, we copy from the Washington Union, of the 20th instant:—
Outlines of Anatomy and Physiology for popular use. By Frederick Hollick, M. D., Lecturer on Anatomy, Physiology, &c.—We regard this as an eminently useful publication. It gives in a form far more condensed and intelligible than we have before seen, a very comprehensive view of the human organization. The dissected plate of the human anatomy, which forms an interesting feature of the work, is to us at least a novelty. The explanations are drawn up with great simplicity, and cannot be misunderstood by the general reader, while they, with the illustrations, will often serve to render more clear and precise the views of scientific and professional students.
From the Sunday Mercury, New York.
Dr. Hollick's Last Work—The Diseases of Woman, their Causes and Cure familiarly explained, with Practical Hints for their prevention, &c.—We regard this as an invaluable production, the most useful, in many respects, which has yet emanated from this distinguished author and practitioner. It is just the kind of work which has ever been wanted, and is just suitable to the excellent purpose for which it was intended; this it accomplishes most fully, and its extensive circulation must be productive of vast practical benefit. It is works of this nature and CHARACTER which really do good; which exhibit plain facts in a plain manner, and record in language simple and intelligible, knowledge of the most vital importance to the health and consequent happiness of every daughter, sister, wife, and mother in the land. The work is dedicated to the Ladies of America, and we congratulate them upon the possession of a friend at once so able, so sincere and valuable as Dr. Hollick. Burgess, Stringer & Co., of this city, are the publishers.
The New York Sun says of this Book:
"Burgess & Stringer have just issued a most invaluable work, being a treatise upon the diseases of women, by the celebrated Dr. Hollick. We have thoroughly examined the work, and can say without hesitation, that it should be in the hands of every mother who cares for the health of her daughters, and every woman who values physical and mental well-being. Dr. Hollick and his publishers have done a public benefit by issuing such a book."
From the New York Sunday Times.
Dr. Hollick's great work, The Diseases of Woman, which will be found advertised in another column, is truly a valuable production, and well sustains the author's well-earned reputation. It is a complete practical treatise on female diseases, scientific enough for a medical man, and yet so plain that every body can understand it, and so delicately written that even the most fastidious cannot object to a single passage. Much of the matter it contains is quite new in this country, even to medical men, and of the greatest interest and importance. The anatomical plates are superb, and the whole book is excellently got up. Every adult female in the land should read this book; the information it gives would prevent an incalculable amount of disease and suffering, if possessed in time; or it will teach the best way to cure it when unfortunately established.
WORKS PUBLISHED BY DR. HOLLICK.
OUTLINES OF
ANATOMY AND PHYSIOLOGY,
BY FREDERICK HOLLICK, M. D.
This is the most complete, and at the same time most simple work ever issued on the subject. It is illustrated in a novel manner, by a large colored Plate of the Human Organization, which dissects by means of separate layers, from the surface of the Abdomen down to the Spine, showing all the Organs in their proper places, all connected together, and many of them in sections! the whole being colored to life. This plate is on an entire new plan, nothing of the kind having ever before been invented; it is almost as complete as a model, and is invaluable for private study, for teachers, and for Medical students. The explanations are familiar, and divested of technicalities: and it is still further illustrated by separate wood-cuts throughout the work, and a beautifully engraved portrait on Steel of the author. One volume, quarto, bound, price One Dollar. Third Edition.
NEUROPATHY;
OR,
THE TRUE PRINCIPLES OF THE ART
OF
HEALING THE SICK.
BY FREDERICK HOLLICK, M. D.
Being a complete practical treatise on the use of GALVANISM, ELECTRICITY, and MAGNETISM, in the cure of disease, and a comparison between their powers, and those of Drugs or Medicines.
These two works are published by T. B. PETERSON, No. 98 Chestnut-st., Philadelphia, and for sale by Booksellers and News Agents generally throughout the United States.
THE ORIGIN OF LIFE.
A complete popular Treatise on the Philosophy and Physiology of Reproduction, in Plants and Animals, with a detailed description of human generation. Illustrated by colored plates of the male and female systems. New being at every stage, &c. Published by Nafis & Cornish, 268 Pearl street, New York. Price $1. Thirtieth Edition, with additional Plates and various improvements.
N. B.—This is the only popular and yet strictly scientific work on the Generative Functions ever yet published.
THE
DISEASES OF WOMAN,
THEIR CAUSES AND CURE
FAMILIARLY EXPLAINED;
With Practical Hints for their prevention and for the preservation of Female Health. By F. Hollick, M. D. Especially designed for every Female's Private Use. Burgess, Stringer & Co., corner of Broadway and Ann streets, New York, and for Sale by all Booksellers. Second Edition. Price $1—300 pages, beautifully bound, and illustrated with numerous splendid Anatomical Plates. By remitting $1 in a letter to T. W. Strong, 98 Nassau-st., N. York, it will be forwarded to any part of the Country.
The above works, along with the present one, constitute a complete practical and popular Library of Anatomy, Medicine and Physiology. They have all been purposely designed for the instruction of non-professional readers, but at the same time are so scientifically correct, and so complete, that they would serve as text books for Medical students. The favor they have already met with, and the extensive circulation they have attained, is proof that they both meet the wants of the public and enjoy its approbation.
From the Boston Mail, March 7, 1848.
Dr. Hollick's Separate Lectures to Ladies and Gentlemen on Physiology.—The importance of adult persons, of both sexes, understanding themselves, and their natural relations, must be obvious to every thinking mind. The present ignorance on these matters is, undoubtedly, the chief cause of the vices and sufferings which so extensively prevail, and our only hope of a beneficial change must be founded on a proper system of public instruction. This instruction is difficult to impart we admit, and there are but few men qualified for imparting it. We have no hesitation, however, in saying that Dr. H. is one of these men. He knows how to preserve in his subject all that intense interest which it intrinsically possesses, and yet to divest it of everything in the slightest degree obnoxious to censure, or even distrust. He has a happy faculty of making every thing easy to be understood, and yet avoiding the slightest approach to undue familiarity. All who attend, express themselves both surprised and delighted, and unhesitatingly recommend his Lectures wherever they go. Many of the most eminent Ladies in our city were among his auditors last week, and were unreserved in their expressions of approbation, both for the Lecture itself, and for the becoming modesty and true refinement that characterised its delivery. The present series, which commence to-day, has been anxiously expected, and will no doubt be numerously attended by both sexes, but particularly by the Ladies, many of whom were unable to gain admission last week.
THE GOLD MEDAL PRESENTED TO DR. HOLLICK, BY THE LADIES OF PHILADELPHIA.
TO GIVE LIGHT TO THEM THAT SIT IN DARKNESS
Presented to FREDERICK HOLLICK M.D. by the Ladies who attended his Lectures on Physiological Science, delivered at Philadelphia, March, 1846, as an expression of their approbation of the knowledge therein conveyed, and as a testimonial of personal regard.
IMPORTANT NOTICE TO LADIES!
THE PATENT ELASTIC AND MEDICATED PESSARY;
FOR THE RELIEF AND PERMANENT CURE OF
PROLAPSUS UTERI, OR FALLING OF THE WOMB;
Prolapsus Vagina, Rupture of the Bladder or Intestine into the Vagina; Retroversion, or Anteversion of the Womb; and also, in many cases, of Leucorrhœa, or Fluor Albus; invented by Dr. Hollick, and first described in his "Diseases of Woman."
This Instrument is certain to cure all the above named diseases, where a cure is possible. It can be worn with perfect ease by young or old, summer or winter, night or day, without the slightest inconvenience. It is made of a soft elastic material, which never corrodes, and which gives way to the slightest motions of the body. It can never become displaced, nor fail to effectually support the parts, and is so light that it only weighs one ounce.
This is the only Instrument of the kind ever invented, and certainly the only one that can cure Falling of the Womb; or be worn with ease, to relieve it, when incurable. Dr. Hollick is the only person who keeps it, as he has no Agent any where, at present.
N. B.—The article is Patented: but, besides this, no imitations, however similar, can be depended upon, because the Original is impregnated, in a peculiar manner, known only to the Inventor, with a substance which imparts its Medicinal Power, and without which it would be comparatively inefficacious.
All the old fashioned Trusses, Supporters, Pessaries, &c., are entirely superseded by this Instrument, which can only be obtained from Dr. Hollick, New York, who will also give the necessary directions as to its use and application. It may be sent any distance. Price—Five Dollars.
ADVERTISEMENT.
Dr. Hollick is daily receiving numerous Letters from all parts of the country, the answering of which has hitherto been a great tax on his time, already sufficiently occupied; he is therefore compelled to announce, that in future he cannot attend to any which merely request advice, unless they contain the customary fee of Five Dollars. Address, Dr. Hollick, New York.
Transcriber's Notes
Page 39 states, "In Plate VII. the line marked † crosses the upper strait, or brim of the Pelvis," but there is no † in the original image.
On page 341, Chapter XXIII was incorrectly labeled Chapter XXII. That has been corrected here.
Minor punctuation errors were corrected on pages vi, 4, 13, 19, 90, 141, 151, 200, 202, 206, 215, 258, 271, 301, 313, 323, 346, 457, 460, 464.
Inconsistencies in hyphenation and capitalization have been retained. Original spellings have been retained except in the cases of these apparent typographical errors:
Page 29, "situate" changed to "situated." (This is the part situated between...)
Page 53, "tha" changed to "that." (Thus some authors asserted that...)
Page 56, "barenness" changed to "barrenness." (...or, in other words, which produce barrenness...)
Page 64, "Tincœ" changed to "Tincæ." (The Os Tincæ, or mouth of the Womb.)
Page 116, "is" changed to "in" in two instances. (...Womb in a first pregnancy, and in a female...)
Page 138, "expeeted" changed to "expected." (...or before the expected period...)
Page 156, "foetal" changed to "fœtal." (...and covered with the fœtal membranes...)
Page 183, "rotale" changed to "rotate." (...the head is compelled to turn, or rotate...)
Page 203, "cephalio" changed to "cephalo." (...it is called the right cephalo iliac position...)
Page 238, "langour" changed to "languor." (...falls into a quiet and pleasing langour...)
Page 240, "signs" changed to "sign." (...and if there is no sign of its coming...)
Page 243, "subseqnent" changed to "subsequent." (...being done in their subsequent labors.)
Page 247, "asphyxated" changed to "asphyxiated." (...are most likely to become asphyxiated...)
Page 253, "capble" changed to "capable." (...she thinks herself stronger, and more capable...)
Page 255, "presentatious" changed to "presentations." (...very unfavorable presentations of the fœtus...)
Page 257, "unforseen" changed to "unforeseen." (...alarmed when unforeseen difficulties occur...)
Page 281, "developement" changed to "development." (The development of the head cannot be ascertained...)
Page 307, "cause" changed to "causes." (Still such presentation occasionally causes...)
Page 311, "presentatations" changed to "presentations." (...most dangerous of all the presentations...)
Page 313, "and" changed to "any." (...child and pelvis from any other cause.)
Page 323, "recommeuds" changed to "recommends." (Mauriceau recommends that women...)
Page 333, "continuanee" changed to "continuance." (...the continuance of pregnancy to the full period...)
Page 333, "inadmissable" changed to "inadmissible." (The plug is here totally inadmissible...)
Page 341, "honr" changed to "hour." (...may be preserved for an hour or two...)
Page 341, "amni" changed to "amnii." (...and then if the liquor amnii...)
Page 349, "introdueed" changed to "introduced." (When the first blade is properly introduced...)
Page 371, "distate" changed to "distaste." (This means a complete distaste...)
Page 380, "meat" changed to "neat." (A neat spoonful should be drunk...)
Page 385, "weaknes" changed to "weakness." (...a state of weakness and exhaustion.)
Page 385, "chlid" changed to "child." (...than dangerous, except to the child...)
Page 395, "unles" changed to "unless." (...unless very large, they cause...)
Page 397, "truely" changed to "truly." (...as truly so as those on the limbs...)
Page 408, "mattrass" changed to "mattress." (...lie on her back, on a hard mattress...)
Page 409, "accummulate" changed to "accumulate." (...and makes it accumulate in the womb...)
Page 413, "ocurrence" changed to "occurrence." (...which may account for the constant occurrence...)
Page 418, "ccnclusion" changed to "conclusion." (In conclusion it should be remarked...)
Page 422, "temblings" changed to "tremblings." (...then follow tremblings, numbness of the limbs...)
Page 426, "spmptoms" changed to "symptoms." (...after the first symptoms of the disease...)
Page 436, "two" changed to "too." (...or too unremittingly, particularly...)
Page 441, "oocasional" changed to "occasional." (...occasional doses of James's Fever Powder...)
Page 441, "James' fever powders" changed to "James's Fever Powder." (...occasional doses of James's Fever Powder...)
Page 445, "recommened" changed to "recommended." (Mesmerism has been recommended...)
Page 445, "develope" changed to "develop." (...will develop the bones of the fœtus...)
Page 450, "crowed" changed to "crowded." (...on the operating table of a crowded theatre...)
Page 452, "minmtes" changed to "minutes." (...the child was expelled in fifty minutes afterwards.)
Page 455, "throngh" changed to "through." (...with unusual difficulty through the brim.)
Page 457, "humau" changed to "human." (...natural parturition in the human mother.)
Page 459, "coporeal" changed to "corporeal." (...principles of our corporeal existence...)
Page 460, "1840" changed to "1846." (March 20, 1846)
Page 464, "Peansylvanian" changed to "Pennsylvanian." (From the Pennsylvanian, (Philadelphia,) Jan. 26, 1847.)
On page 240, an extra "an" was removed from the phrase "...to wait more than an hour..."
On page 456, the word "of" was missing from the phrase "...after a careful examination of all the cases recorded..."
On page 457, an extra "of" was removed from the phrase "the superinduction of anæsthesia."
End of the Project Gutenberg EBook of The Matron's Manual of Midwifery, and
the Diseases of Women During Pregnanc, by Frederick Hollick
*** END OF THIS PROJECT GUTENBERG EBOOK MATRON'S MANUAL OF MIDWIFERY ***
***** This file should be named 47836-h.htm or 47836-h.zip *****
This and all associated files of various formats will be found in:
http://www.gutenberg.org/4/7/8/3/47836/
Produced by Cindy Horton, Sarah Jensen and the Online
Distributed Proofreading Team at http://www.pgdp.net (This
file was produced from images generously made available
by The Internet Archive/American Libraries.)
Updated editions will replace the previous one--the old editions will
be renamed.
Creating the works from print editions not protected by U.S. copyright
law means that no one owns a United States copyright in these works,
so the Foundation (and you!) can copy and distribute it in the United
States without permission and without paying copyright
royalties. Special rules, set forth in the General Terms of Use part
of this license, apply to copying and distributing Project
Gutenberg-tm electronic works to protect the PROJECT GUTENBERG-tm
concept and trademark. Project Gutenberg is a registered trademark,
and may not be used if you charge for the eBooks, unless you receive
specific permission. If you do not charge anything for copies of this
eBook, complying with the rules is very easy. You may use this eBook
for nearly any purpose such as creation of derivative works, reports,
performances and research. They may be modified and printed and given
away--you may do practically ANYTHING in the United States with eBooks
not protected by U.S. copyright law. Redistribution is subject to the
trademark license, especially commercial redistribution.
START: FULL LICENSE
THE FULL PROJECT GUTENBERG LICENSE
PLEASE READ THIS BEFORE YOU DISTRIBUTE OR USE THIS WORK
To protect the Project Gutenberg-tm mission of promoting the free
distribution of electronic works, by using or distributing this work
(or any other work associated in any way with the phrase "Project
Gutenberg"), you agree to comply with all the terms of the Full
Project Gutenberg-tm License available with this file or online at
www.gutenberg.org/license.
Section 1. General Terms of Use and Redistributing Project
Gutenberg-tm electronic works
1.A. By reading or using any part of this Project Gutenberg-tm
electronic work, you indicate that you have read, understand, agree to
and accept all the terms of this license and intellectual property
(trademark/copyright) agreement. If you do not agree to abide by all
the terms of this agreement, you must cease using and return or
destroy all copies of Project Gutenberg-tm electronic works in your
possession. If you paid a fee for obtaining a copy of or access to a
Project Gutenberg-tm electronic work and you do not agree to be bound
by the terms of this agreement, you may obtain a refund from the
person or entity to whom you paid the fee as set forth in paragraph
1.E.8.
1.B. "Project Gutenberg" is a registered trademark. It may only be
used on or associated in any way with an electronic work by people who
agree to be bound by the terms of this agreement. There are a few
things that you can do with most Project Gutenberg-tm electronic works
even without complying with the full terms of this agreement. See
paragraph 1.C below. There are a lot of things you can do with Project
Gutenberg-tm electronic works if you follow the terms of this
agreement and help preserve free future access to Project Gutenberg-tm
electronic works. See paragraph 1.E below.
1.C. The Project Gutenberg Literary Archive Foundation ("the
Foundation" or PGLAF), owns a compilation copyright in the collection
of Project Gutenberg-tm electronic works. Nearly all the individual
works in the collection are in the public domain in the United
States. If an individual work is unprotected by copyright law in the
United States and you are located in the United States, we do not
claim a right to prevent you from copying, distributing, performing,
displaying or creating derivative works based on the work as long as
all references to Project Gutenberg are removed. Of course, we hope
that you will support the Project Gutenberg-tm mission of promoting
free access to electronic works by freely sharing Project Gutenberg-tm
works in compliance with the terms of this agreement for keeping the
Project Gutenberg-tm name associated with the work. You can easily
comply with the terms of this agreement by keeping this work in the
same format with its attached full Project Gutenberg-tm License when
you share it without charge with others.
1.D. The copyright laws of the place where you are located also govern
what you can do with this work. Copyright laws in most countries are
in a constant state of change. If you are outside the United States,
check the laws of your country in addition to the terms of this
agreement before downloading, copying, displaying, performing,
distributing or creating derivative works based on this work or any
other Project Gutenberg-tm work. The Foundation makes no
representations concerning the copyright status of any work in any
country outside the United States.
1.E. Unless you have removed all references to Project Gutenberg:
1.E.1. The following sentence, with active links to, or other
immediate access to, the full Project Gutenberg-tm License must appear
prominently whenever any copy of a Project Gutenberg-tm work (any work
on which the phrase "Project Gutenberg" appears, or with which the
phrase "Project Gutenberg" is associated) is accessed, displayed,
performed, viewed, copied or distributed:
This eBook is for the use of anyone anywhere in the United States and
most other parts of the world at no cost and with almost no
restrictions whatsoever. You may copy it, give it away or re-use it
under the terms of the Project Gutenberg License included with this
eBook or online at www.gutenberg.org. If you are not located in the
United States, you'll have to check the laws of the country where you
are located before using this ebook.
1.E.2. If an individual Project Gutenberg-tm electronic work is
derived from texts not protected by U.S. copyright law (does not
contain a notice indicating that it is posted with permission of the
copyright holder), the work can be copied and distributed to anyone in
the United States without paying any fees or charges. If you are
redistributing or providing access to a work with the phrase "Project
Gutenberg" associated with or appearing on the work, you must comply
either with the requirements of paragraphs 1.E.1 through 1.E.7 or
obtain permission for the use of the work and the Project Gutenberg-tm
trademark as set forth in paragraphs 1.E.8 or 1.E.9.
1.E.3. If an individual Project Gutenberg-tm electronic work is posted
with the permission of the copyright holder, your use and distribution
must comply with both paragraphs 1.E.1 through 1.E.7 and any
additional terms imposed by the copyright holder. Additional terms
will be linked to the Project Gutenberg-tm License for all works
posted with the permission of the copyright holder found at the
beginning of this work.
1.E.4. Do not unlink or detach or remove the full Project Gutenberg-tm
License terms from this work, or any files containing a part of this
work or any other work associated with Project Gutenberg-tm.
1.E.5. Do not copy, display, perform, distribute or redistribute this
electronic work, or any part of this electronic work, without
prominently displaying the sentence set forth in paragraph 1.E.1 with
active links or immediate access to the full terms of the Project
Gutenberg-tm License.
1.E.6. You may convert to and distribute this work in any binary,
compressed, marked up, nonproprietary or proprietary form, including
any word processing or hypertext form. However, if you provide access
to or distribute copies of a Project Gutenberg-tm work in a format
other than "Plain Vanilla ASCII" or other format used in the official
version posted on the official Project Gutenberg-tm web site
(www.gutenberg.org), you must, at no additional cost, fee or expense
to the user, provide a copy, a means of exporting a copy, or a means
of obtaining a copy upon request, of the work in its original "Plain
Vanilla ASCII" or other form. Any alternate format must include the
full Project Gutenberg-tm License as specified in paragraph 1.E.1.
1.E.7. Do not charge a fee for access to, viewing, displaying,
performing, copying or distributing any Project Gutenberg-tm works
unless you comply with paragraph 1.E.8 or 1.E.9.
1.E.8. You may charge a reasonable fee for copies of or providing
access to or distributing Project Gutenberg-tm electronic works
provided that
* You pay a royalty fee of 20% of the gross profits you derive from
the use of Project Gutenberg-tm works calculated using the method
you already use to calculate your applicable taxes. The fee is owed
to the owner of the Project Gutenberg-tm trademark, but he has
agreed to donate royalties under this paragraph to the Project
Gutenberg Literary Archive Foundation. Royalty payments must be paid
within 60 days following each date on which you prepare (or are
legally required to prepare) your periodic tax returns. Royalty
payments should be clearly marked as such and sent to the Project
Gutenberg Literary Archive Foundation at the address specified in
Section 4, "Information about donations to the Project Gutenberg
Literary Archive Foundation."
* You provide a full refund of any money paid by a user who notifies
you in writing (or by e-mail) within 30 days of receipt that s/he
does not agree to the terms of the full Project Gutenberg-tm
License. You must require such a user to return or destroy all
copies of the works possessed in a physical medium and discontinue
all use of and all access to other copies of Project Gutenberg-tm
works.
* You provide, in accordance with paragraph 1.F.3, a full refund of
any money paid for a work or a replacement copy, if a defect in the
electronic work is discovered and reported to you within 90 days of
receipt of the work.
* You comply with all other terms of this agreement for free
distribution of Project Gutenberg-tm works.
1.E.9. If you wish to charge a fee or distribute a Project
Gutenberg-tm electronic work or group of works on different terms than
are set forth in this agreement, you must obtain permission in writing
from both the Project Gutenberg Literary Archive Foundation and The
Project Gutenberg Trademark LLC, the owner of the Project Gutenberg-tm
trademark. Contact the Foundation as set forth in Section 3 below.
1.F.
1.F.1. Project Gutenberg volunteers and employees expend considerable
effort to identify, do copyright research on, transcribe and proofread
works not protected by U.S. copyright law in creating the Project
Gutenberg-tm collection. Despite these efforts, Project Gutenberg-tm
electronic works, and the medium on which they may be stored, may
contain "Defects," such as, but not limited to, incomplete, inaccurate
or corrupt data, transcription errors, a copyright or other
intellectual property infringement, a defective or damaged disk or
other medium, a computer virus, or computer codes that damage or
cannot be read by your equipment.
1.F.2. LIMITED WARRANTY, DISCLAIMER OF DAMAGES - Except for the "Right
of Replacement or Refund" described in paragraph 1.F.3, the Project
Gutenberg Literary Archive Foundation, the owner of the Project
Gutenberg-tm trademark, and any other party distributing a Project
Gutenberg-tm electronic work under this agreement, disclaim all
liability to you for damages, costs and expenses, including legal
fees. YOU AGREE THAT YOU HAVE NO REMEDIES FOR NEGLIGENCE, STRICT
LIABILITY, BREACH OF WARRANTY OR BREACH OF CONTRACT EXCEPT THOSE
PROVIDED IN PARAGRAPH 1.F.3. YOU AGREE THAT THE FOUNDATION, THE
TRADEMARK OWNER, AND ANY DISTRIBUTOR UNDER THIS AGREEMENT WILL NOT BE
LIABLE TO YOU FOR ACTUAL, DIRECT, INDIRECT, CONSEQUENTIAL, PUNITIVE OR
INCIDENTAL DAMAGES EVEN IF YOU GIVE NOTICE OF THE POSSIBILITY OF SUCH
DAMAGE.
1.F.3. LIMITED RIGHT OF REPLACEMENT OR REFUND - If you discover a
defect in this electronic work within 90 days of receiving it, you can
receive a refund of the money (if any) you paid for it by sending a
written explanation to the person you received the work from. If you
received the work on a physical medium, you must return the medium
with your written explanation. The person or entity that provided you
with the defective work may elect to provide a replacement copy in
lieu of a refund. If you received the work electronically, the person
or entity providing it to you may choose to give you a second
opportunity to receive the work electronically in lieu of a refund. If
the second copy is also defective, you may demand a refund in writing
without further opportunities to fix the problem.
1.F.4. Except for the limited right of replacement or refund set forth
in paragraph 1.F.3, this work is provided to you 'AS-IS', WITH NO
OTHER WARRANTIES OF ANY KIND, EXPRESS OR IMPLIED, INCLUDING BUT NOT
LIMITED TO WARRANTIES OF MERCHANTABILITY OR FITNESS FOR ANY PURPOSE.
1.F.5. Some states do not allow disclaimers of certain implied
warranties or the exclusion or limitation of certain types of
damages. If any disclaimer or limitation set forth in this agreement
violates the law of the state applicable to this agreement, the
agreement shall be interpreted to make the maximum disclaimer or
limitation permitted by the applicable state law. The invalidity or
unenforceability of any provision of this agreement shall not void the
remaining provisions.
1.F.6. INDEMNITY - You agree to indemnify and hold the Foundation, the
trademark owner, any agent or employee of the Foundation, anyone
providing copies of Project Gutenberg-tm electronic works in
accordance with this agreement, and any volunteers associated with the
production, promotion and distribution of Project Gutenberg-tm
electronic works, harmless from all liability, costs and expenses,
including legal fees, that arise directly or indirectly from any of
the following which you do or cause to occur: (a) distribution of this
or any Project Gutenberg-tm work, (b) alteration, modification, or
additions or deletions to any Project Gutenberg-tm work, and (c) any
Defect you cause.
Section 2. Information about the Mission of Project Gutenberg-tm
Project Gutenberg-tm is synonymous with the free distribution of
electronic works in formats readable by the widest variety of
computers including obsolete, old, middle-aged and new computers. It
exists because of the efforts of hundreds of volunteers and donations
from people in all walks of life.
Volunteers and financial support to provide volunteers with the
assistance they need are critical to reaching Project Gutenberg-tm's
goals and ensuring that the Project Gutenberg-tm collection will
remain freely available for generations to come. In 2001, the Project
Gutenberg Literary Archive Foundation was created to provide a secure
and permanent future for Project Gutenberg-tm and future
generations. To learn more about the Project Gutenberg Literary
Archive Foundation and how your efforts and donations can help, see
Sections 3 and 4 and the Foundation information page at
www.gutenberg.org
Section 3. Information about the Project Gutenberg Literary Archive Foundation
The Project Gutenberg Literary Archive Foundation is a non profit
501(c)(3) educational corporation organized under the laws of the
state of Mississippi and granted tax exempt status by the Internal
Revenue Service. The Foundation's EIN or federal tax identification
number is 64-6221541. Contributions to the Project Gutenberg Literary
Archive Foundation are tax deductible to the full extent permitted by
U.S. federal laws and your state's laws.
The Foundation's principal office is in Fairbanks, Alaska, with the
mailing address: PO Box 750175, Fairbanks, AK 99775, but its
volunteers and employees are scattered throughout numerous
locations. Its business office is located at 809 North 1500 West, Salt
Lake City, UT 84116, (801) 596-1887. Email contact links and up to
date contact information can be found at the Foundation's web site and
official page at www.gutenberg.org/contact
For additional contact information:
Dr. Gregory B. Newby
Chief Executive and Director
gbnewby@pglaf.org
Section 4. Information about Donations to the Project Gutenberg
Literary Archive Foundation
Project Gutenberg-tm depends upon and cannot survive without wide
spread public support and donations to carry out its mission of
increasing the number of public domain and licensed works that can be
freely distributed in machine readable form accessible by the widest
array of equipment including outdated equipment. Many small donations
($1 to $5,000) are particularly important to maintaining tax exempt
status with the IRS.
The Foundation is committed to complying with the laws regulating
charities and charitable donations in all 50 states of the United
States. Compliance requirements are not uniform and it takes a
considerable effort, much paperwork and many fees to meet and keep up
with these requirements. We do not solicit donations in locations
where we have not received written confirmation of compliance. To SEND
DONATIONS or determine the status of compliance for any particular
state visit www.gutenberg.org/donate
While we cannot and do not solicit contributions from states where we
have not met the solicitation requirements, we know of no prohibition
against accepting unsolicited donations from donors in such states who
approach us with offers to donate.
International donations are gratefully accepted, but we cannot make
any statements concerning tax treatment of donations received from
outside the United States. U.S. laws alone swamp our small staff.
Please check the Project Gutenberg Web pages for current donation
methods and addresses. Donations are accepted in a number of other
ways including checks, online payments and credit card donations. To
donate, please visit: www.gutenberg.org/donate
Section 5. General Information About Project Gutenberg-tm electronic works.
Professor Michael S. Hart was the originator of the Project
Gutenberg-tm concept of a library of electronic works that could be
freely shared with anyone. For forty years, he produced and
distributed Project Gutenberg-tm eBooks with only a loose network of
volunteer support.
Project Gutenberg-tm eBooks are often created from several printed
editions, all of which are confirmed as not protected by copyright in
the U.S. unless a copyright notice is included. Thus, we do not
necessarily keep eBooks in compliance with any particular paper
edition.
Most people start at our Web site which has the main PG search
facility: www.gutenberg.org
This Web site includes information about Project Gutenberg-tm,
including how to make donations to the Project Gutenberg Literary
Archive Foundation, how to help produce our new eBooks, and how to
subscribe to our email newsletter to hear about new eBooks.