*** START OF THE PROJECT GUTENBERG EBOOK 49054 ***
ANATOMY AND EMBALMING
ANATOMY
AND EMBALMING
A Treatise on the Science and Art of Embalming,
the Latest and Most Successful Methods
of Treatment and the General
Anatomy Relating to
This Subject.
BY
ALBERT JOHN NUNNAMAKER, A. B.
AND
CHARLES O. DHONAU
PROFESSORS OF ANATOMY AND SANITARY SCIENCE AT THE
CINCINNATI COLLEGE OF EMBALMING, CINCINNATI, OHIO.
Illustrated
Cincinnati, Ohio.
THE EMBALMING BOOK COMPANY.
1913
Copyright, 1913, by
THE EMBALMING BOOK COMPANY.
Dedicated
to
Those Who Are Advancing
The Standards
of the
Profession
[v]
PREFACE
This book is the result of many years of contact with
embalmers in training and in practice. We have included
in this work a crystallization of essential information
without which, the embalmer must be poorly equipped to
carry out the many duties incident to his calling in a
manner satisfactory to his patrons and to himself.
Having been thrown in contact with the many problems
surrounding the education of the embalmer, the
authors have gained many ideas as to just how to place
the information before the embalmer so that the result
will be reflected in an increased capacity for good work
on the part of the individual embalmer.
In prescribing information for the embalmer in this
manner, we know clearly just what is to be expected from
the application of the sciences herein described, and wish
for the novitiate and practitioner the same enthusiasm for
actual knowledge that has helped us thus far in arranging
the information.
In Part One, we have chronicled, from the word of
historians and men of the present day, a condensed, yet
complete exposition of the funeral customs relating to the
[vi]
care of the dead, giving our readers a better understanding
of present methods by reason of an opportunity to
compare them with those of the past.
In Part Two, we have placed the ground work or
foundation for the securing of the proper education in
embalming. The work on Anatomy, which, if mastered
by the student or practitioner, is by far the greatest lever
in helping him to master his lifework.
In Part Three, we have placed the practical application
of the principles of modern embalming, tempered by the
use of the sciences of pathology, bacteriology, and chemistry
in our own application of the work and in its transcription
to these pages.
In formulating the technical part of the work, we have
been greatly assisted by many authorities among whom
are:—Green, Howell, Thomas, Piersol, Gray, Spalteholz,
Myers, Barnes, Renouard, Clarke, and those authors who
have from time to time contributed articles to the current
embalmers journals. We are deeply indebted to these
men for the results of their work.
We have based the treatments given herein on the
following classification of embalming fluid as expressed in
the percentage strength of formaldehyde gas contained
within the fluid.
| ½ strength | = standard fluid of 5% diluted to 2½% |
| ¾ strength | = standard fluid of 5% diluted to 3¾% |
| Normal strength | = standard fluid 5% |
| 1¼ strength | = standard fluid of 5% raised to 6¼% |
[vii]
As the existence of a calling or profession depends on
a constant assimilation of newly discovered information
counterbalanced by the throwing off of that which has
been found faulty, we commend this book to the embalmer
and hope that it will meet with all the requirements of
the higher education, for which we are constantly battling.
THE AUTHORS.
[xvii]
LIST OF ILLUSTRATIONS
[1]
PART I.
HISTORY OF EMBALMING
[3]
Ancient Embalming
CHAPTER I.
HISTORY OF EMBALMING.
Guanch Embalming.
—The Guanches with the Egyptians
are the only nation among whom embalming had
become national, and there exists in the process and
mode of preservation of both such striking analogy,
that the study of the Guanch mummies is, probably, the
surest means of arriving at some positive notions of their
origin and relationship. The details known of the mode
of embalming among the Guanches will enlighten and
complete the descriptions that ancient authors have left
to us of the Egyptian processes. They were silent on
desiccation in the act of mummification, but it is to be
regarded as a simple omission on their part. This
desiccation was continued during the seventy days
of preparation, and it constituted the principle part of
the process adopted.
The details that I am about to give are extracted
from the work of M. Bory de Saint Vincent on the
fortunate Isles.
“The arts of the Guanches were not numerous, the
most singular without doubt is that of embalming. The
[4]
Guanches preserved the remains of their relations in a
scrupulous manner and spared no pains to guarantee
them from corruption. As a moral duty each individual
prepared for himself the skins of goats, in which his
remains could be enveloped, and which might serve him
for sepulture. These skins were often divested of their
hair, at other times they permitted it to remain, when
they placed indifferently the hair side within or without.
The processes to which they resorted to make perfect
mummies, which they named xaxos, are nearly lost.
With the Guanches, the embalmers were abject beings;
men and women filled this employment respectively,
for their sexes; they were well paid, but their touch
was considered contamination; and all who were occupied
in preparing the xaxos lived retired, solitary, and
out of sight.
There were several kinds of embalming, and several
different employments for those who had charge of it.
When they had need of the services of the embalmers,
they carried the body to them to be preserved, and immediately
retired. If the body belonged to persons
capable of bearing the expenses, they extended it at
first on a stone table, the operator then made an opening
in the lower part of the belly with a sharpened
flint, wrought into the form of a knife and called
tabona; the intestines were withdrawn, which other
operators afterwards washed and cleaned; they also
washed the rest of the body, and particularly the delicate
parts, as the eyes, interior of the mouth, the ears,
and the nails, with fresh water saturated with salt.
[5]
They filled the large cavities with aromatic plants; they
then exposed the body to the hottest sun, or placed it
in stoves, if the sun was not hot enough. During the
exposition they frequently endued the body with an ointment,
composed of goats' grease, powder of odoriferous
plants, pine bark, resin, tar ponce stone, and other absorbing
material.
On the fifteenth day the embalming should be completely
terminated; the mummy should be dry and
light; the relatives send for it and establish the most
magnificent obsequies in their power. They sew up the
body in several folds of skin, which they had prepared
while living, and they bind it with straps.
The kings and the grandees were besides placed in
a case or coffin of a single piece, and hollowed out of
the trunk of a juniper tree, the wood of which was
held as incorruptible.
They then finally carried the xaxos, thus sewed and
encased, to inaccessible grottoes consecrated to this purpose.
Egyptian Embalming.
—The Egyptians embalmed their
dead, and the processes which they employed were sufficiently
perfect to secure them an indefinite preservation.
This is a fact which the pyramids, the cavern, and all
the sepultures of Egypt offer us irrefragible proof. But
what were the causes of the origin of this custom? We
have in answer only hypothesis and conjecture. In the
absence of valid documents, each one explains according
to the bias of his mind, or the nature of his studies, a
usage, the origin of which is lost in the night of time.
One of the ancients informs us that the Egyptians took
[6]
so much pains for the preservation of the body, believing
that the soul inhabited it so long as it subsisted. Cassien,
on the other hand, assures us that they invented this
method because they were unable to bury their dead
during the period of inundation. Herodotus, in his
third book, observes, that embalming had for its object
the securing of bodies from the voracity of animals; they
did not bury them, says he, for fear they would be eaten
by worms, and they did not burn them, because they
considered fire like a wild beast that devours everything
it can seize upon. Filial piety and respect for the dead,
according to Sicculus, were the sentiments which inspired
the Egyptians with the idea of embalming the dead bodies.
De Maillet, in his tenth letter upon Egypt, refers only
to a religious motive as the origin of embalming: The
priests and sages of Egypt taught their fellow citizens
that, after a certain number of ages, which they made
to amount to thirty or forty thousand years, and at which
they fixed the epoch of the grand revolution when the
earth would return to the point at which it commenced
its existence, their souls would return to the same bodies
which they formerly inhabited. But in order to arrive,
after death, to this wished for resurrection, two things
were absolutely necessary; first that the bodies should
be absolutely carefully preserved from corruption, in
order that the souls might re-inhabit them; secondly,
that the penance submitted to during this long period
of years, that the numerous sacrifices founded by the
dead, or those offered to their names by their friends,
or relation, should expiate the crimes they had committed
during the time of their first inhabitation on earth.
[7]
With these conditions exactly observed, these souls
separate from their bodies, should be permitted to re-enter
at the arrival of this grand revolution which they
anticipated—remember all that had passed during their
sojourn, and become immortal like themselves. They had
further the same privilege of communicating this same
happiness to the animals which they had cherished, provided
that their bodies inclosed in the same tomb with
themselves, were equally well preserved. It is in virtue
of this belief that so many birds, cats, and other animals
are found embalmed with almost the same care as the
human bodies with which they have been deposited.
Such was the idea of perfect happiness which they
hoped to enjoy in this new life. Surely superstition alone,
it could scarcely be believed, would induce men to save
from destruction the mortal spoils of individuals whom
they had loved whilst living. We much prefer looking
for the source of this usage in the sentiment which survives
a cherished object snatched from affection by the
hand of death. Since death levels all distinctions—respecting
neither love nor friendship—since the dearest
and most sacred ties are relentlessly broken asunder, it
is the natural attribute of affection, to seek to avoid in
some degree, a painful separation, by preserving the remains
of those they loved and by whom they were beloved.
This according to Saint Vincent. Volney and
Paraset write as follows as to the probable cause of the
origin of the custom: In a numerous population, under
a burning climate, and the soil profoundly drenched during
many months of the year, the rapid putrefaction of
bodies, is a leaven for plague and disease. Stricken by
[8]
these numerous pests, Egypt at an early day, struggled
to obviate them; hence have arisen, on the one hand
a custom of burying their dead at a distance from their
habitations; and on the other an art so ingenious and
simple to prevent putrefaction by embalming. One individual
may be induced to embalm the bodies of his
relatives and friends by motives of superstition; another
from egotism and personal interest; a third from motives
of salubrity or common interest; another is impelled
to perform the sacred duty of preserving the
remains of those who were dear to him by an instinctive
affection. Caylus says that the Egyptians, according to
appearances owe the idea of their mummies, to the dead
bodies which they found buried in the burning sands
which prevail in some parts of Egypt, and which, carried
away by the winds, bury travelers and preserve their
bodies, by consuming the fat and flesh without altering
the skin.
The mourning, embalming and funerals were conducted
as follows: When a man of consideration dies,
all the women of his house, cover the head and even the
face with mud; they leave the deceased in the house,
girdle the middle of their bodies, bare the bosom, strike
the breast, and overrun the city, accompanied by their
relations. On the other side, the men also girdle themselves,
and strike their breasts; after this ceremony they
carry the body to the place where it is to be embalmed.
Certain men according to the law have charge of the
embalming, and make a profession of it. When a body
is brought to them, they show the bearers models of the
dead in wood. The most renowned represents, they say,
[9]
Him whose name I am scrupulous to mention. This
model was probably the figure of some divinity. To be
prepared after this model would cost one talent, (about
nine hundred dollars of our money). They show a second
which is inferior to the first, and which is not so
costly, twenty mina, (or about three hundred dollars in
our money). They also show a third of lower price, the
price of which was considered by Herodotus as a trifle,
which we would infer to mean from fifty to seventy-five
dollars of our money. The exhibition of models on the
part of the embalmers, had reference to the richness of
the work demanded, and to the expense of the chosen
form. They demand after which of the three models
they wish the deceased to be embalmed. After agreeing
about the price, the relatives retire; the embalmers work
alone and proceed as follows, in the most costly embalming.
They first withdraw the brain through the nostrils,
in part with a curved iron instrument, and in part by
means of drugs, which they introduce into the head.
They now make an incision in the flank with a sharp
Ethiopian stone. The body is extended upon the earth,
the scribe traces on the left flank the portion to be cut
out. He who is charged with making the incision cuts
with an Ethiopian stone, as much as the law allows;
which, having done, he runs off with all his might, the
assistants follow, throwing stones after him, loading him
with imprecations, as if they wished to put upon him
this crime. They regard, indeed, with horror, whoever
does violence to a body of the same nature as their own.
They withdraw the intestines through this opening,
[10]
clean them, and pass them through palm wine, place
them in a trunk; and among other things they do for
the deceased, they take this trunk, and calling the sun
to witness, one of the embalmers on the part of the dead,
addresses that luminary in the following words, which
Euphantus has translated: “Sun and ye too, Gods, who
have given life to men, receive me, and grant that I may
live with the eternal Gods: I have persisted all my life
in the worship of those Gods, whom I hold from my
fathers, I have ever honoured the Author of my being,
I have killed no one, I have committed no breach of
trust, I have done no other evil: if I have been guilty of
any other fault during life, it has not been on my own
account, but for these things.” The embalmer in finishing
these words, shows the trunk containing the intestines, and
afterwards casts it into the river. As to the rest of the
body when it is pure they embalm it.
Afterwards they fill the body with pure bruised myrrh,
with cannella and other perfumes, excepting incense, it
is then sown up. When that is done they salt the body
by covering it with natrum for seventy days. The natrum
carries off and dries the oily, lymphatic, and greasy
parts. After the seventy days the body is not permitted
to remain longer in the salt. The seventy days elapsed,
they wash the body and entirely envelope it in linen and
cotton bandages, soaked with gum Arabic. The relatives
now reclaim the body, they have made a wooden case
for the human form, in which they enclose the corpse,
and put it in a chamber destined for this purpose, standing
erect against the wall. Such is the most magnificent
method of embalming the dead.
[11]
Those who wish to avoid the expense, choose this
other method; they fill syringes with an unctious liquor
which they obtain from the cedar, with this they inject the
belly of the corpse without making any incision, and
without withdrawing the intestines; when this liquor
has been introduced into the cavity, they cork it; the
body is then salted for the prescribed time. The last
day they draw off from the body the injected liquor, it
has such strength that it dissolves the ventricles and intestines,
which come away with the liquid. The natrum
destroys the flesh, and there remains of the body only
the skin and the bones. This operation finished, they
return the body without doing anything further to it.
The third kind of embalming is only for the poorer
classes of society, they inject the body with a fluid called
surmata, they put the body in natrum for seventy days,
and they afterwards return it to those who brought it.
As to the ladies of quality, when they are dead, they
are not immediately sent to the embalmers, any more than
such as are beautiful or highly distinguished; they are
reserved for three or four days after death. They take
this precaution lest the embalmers might pollute the
bodies confided to their care.
The relatives now fix the day for the obsequies in
order that the judges, the relations, and the friends of
the dead may be present, and they characterize it by saying
that he is going to pass the lake; afterwards the
judges, to the number of more than forty arriving, place
themselves in the form of a semicircle beyond the lake.
A bateau approaches, carrying those who have charge
of the ceremony, and in which is a sailor whom the
[12]
Egyptians name in their language, Charon. Before
placing in the bateau the coffin containing the body of
the deceased, it is lawful for each one present to accuse
him. If they prove that he has led a sinful life, the
judges condemn him, and he is excluded from the place
of his sepulture, if it appear that he has been unjustly
accused, they punish the accuser with severity. If no
accuser presents himself or if the one who does so is
known to be a calumniator, the relatives, putting aside
the signs of their grief, deliver an eulogism, on the deceased
without mentioning his birth, because they consider
all Egyptians equally noble. They enlarge on the
manner in which he has been schooled and instructed
from his childhood; upon his piety, justice, temperance,
and his other virtues since he attained manhood, and they
pray the Gods of hell to admit him into the dwelling of
the pious. The people applauded and glorified the dead
who were to pass all eternity in the abodes of the happy.
If any one has a monument destined for his sepulture,
his body is there deposited; if he has none, they construct
a room in his house, and place the bier upright
against the most solid part of the wall. They place in
their houses those to whom sepulture has not been
awarded, either on account of crimes, of which they are
accused, or on account of the debts which they may have
contracted; and it happens sometimes in the end that
they obtained honorable sepulture, their children or descendants
becoming rich, pay their debts or absolve them.
The Egyptian embalmers knew how to distinguish
from the other viscera, the liver, the spleen, and the kidneys,
which they did not disturb; they had discovered
[13]
the means of withdrawing the brain from the interior
of the body without destroying the bones of the cranium;
they knew the action of alkalies upon animal matter,
since the time was strictly limited that the body could
remain in contact with these substances; they were not
ignorant of the property of balsams, and resins to protect
the bodies from the larvae of insects and mites;
they were likewise aware of the necessity of enveloping
the dried and embalmed bodies, in order to protect them
from the humidity, which would interfere with their
preservation.
The preceding is a description of ancient Egyptian
embalming as given by Herodotus, and has been the subject
of numerous commentations, discussions and researches.
It is almost a positive fact that Herodotus has
omitted desiccation, and that it naturally took place during
the time consecrated to preparation. From the mummies
examined it is believed now that the body was first
salted for seventy days, then dried, and that it was not
until after this desiccation that the resinous and balsamic
substances were applied. A simple inspection of the
mummies is sufficient to confirm this opinion and besides
what use would have been these resinous matters, with
which the alkali of the natrum would soon form a soapy
mass, which the lotions would have carried off, at least
in great part? It is much more reasonable to suppose
that these balsamic and resinous substances were not
applied to the bodies until after they were withdrawn
from the natrum.
All the ancients agree, in saying that the Egyptians
[14]
made use of the various aromatics to embalm the dead;
that they employed for the rich myrrh, aloes, canella, and
cassia lignea; and for the poor, the cedria, bitumen, and
natrum. The natrum was a mixture of carbonate, sulphate,
and muriate of soda. It was a fixed alkali, which
acted after the manner of quicklime; despoiling the
bodies of their lymphatic, and greasy fluids, leaving only
the fibrous and solid parts. The odoriferous resins and
bitumen not only preserved from destruction, but also
kept at a distance the worms and beetles which devour
dead bodies.
The embalmers, after having washed the bodies with
palm wine, and having filled them with odoriferous resins
or bitumen, they place them in stoves, where by means
of convenient heat these resinous substances united intimately
with the bodies, and these arrive in a very little
time to that state of perfect preservation which we find
them at the present day. This operation of which no
historian has spoken, was, without doubt, the principle
and most important part of their embalming.
[15]
CHAPTER II.
EMBALMING FROM EGYPTIANS DOWN TO
CIVIL WAR.
Here facts are almost entirely wanting and the history
of the art we are studying, can only be followed in the
recitals of historians, to control whose veracity we have
no longer those monuments which Egypt offers us in such
great numbers. Among the Jews, the Greeks, the Romans,
and all modern nations, we see the honors of embalming
accorded to Kings, Princes and men of distinction,
but no tomb that has been opened, has rendered a
single mummy so perfect, as those which we admire among
the Egyptians.
Jews.
—The Jewish people, who, like others, testified
their respect for the dead, never admit the care of
embalming the body as a common usage. Thus Abraham
purchased the field where Sarah was buried; Joseph had
the body of his father magnificently embalmed; Moses
only carried away the bones of Joseph; David praised
the people of Gilead, for having buried with pomp Saul
and his sons, etc. In most of these examples, no mention
is made of embalming; nevertheless, the body of
Jesus Christ was embalmed. It is written that Joseph
of Arimathea, a secret disciple, and Nicodemus, ministered
unto him, after the crucifixion, and that 100 lbs. of myrrh
[16]
and aloes were used. In this action the greatest secrecy
had been observed, for “when the Sabbath was over, very
early on the first day of the next week, came the faithful
women who had loved him, with spices and ointment
they had prepared where with to annoint him, not
knowing that, already, this loving service had been performed
by the hand of pious affection.”
The following is nearly the method used by the Jews:
Each sex took care of its dead; they first of all, close the
mouth and eyes of the exposed person, afterward they
washed the body and then rubbed it with perfumes,
tied it with bands, and then bandaged it in several cloths
of very fine linen or woolen; and finally, they put it into
the sepulture. It is thought that the myrrh and aloes
which they employed had very little virtue to resist
putrefaction, and that the great quantities of aromatics
which they consumed, was rather for pomp, than for
the long preservation of the subject. They took no pains
to dry the body; they did not take away the intestines,
and in spite of all these odoriferous drugs, decomposition
must have soon revealed itself as was testified by
the body of Lazarus when resurrected.
Persians.
—Neither did the Persians possess a very
great knowledge of preservation. Cyrus, King of Persia,
said to his children: “when I have ceased to live, place
my body neither in silver nor in gold, nor in any other
coffin, but return it immediately to the earth, etc.” It
will be perceived that Cyrus, in forbidding that any
care should be taken with his body, does not allude to
embalming, which, of all other means, would have been
[17]
the most efficient in preventing its elements from returning
to the Common Mother.
Babylonians.
—The Babylonians, anointed the bodies
of their dead with honey, after which, they were immersed
in the same substance. It is highly improbable
that this process was successful for long time preservation,
for the preservative power of honey was only equal
to its ability to keep the air from the body.
Scythians.
—The Scythians coated the bodies of their
dead with wax. This process could not have been successful
excepting to retard decomposition through shutting
off all communication between the body and the
air.
Ethiopians.
—The Ethiopians coated the bodies of their
dead with waxy covering called parget. The same comment
given on the Babylonian and Scythian processes
must also be used here.
Romans.
—The disposition of the dead among the Romans
embraced the following treatment: the deceased
was first washed with hot water varied with oil, at intervals,
for seven days; was dressed and embalmed with
the performance of a variety of singular ceremonies.
Cremation was then the means of ultimate disposal of
the dead, the ashes being gathered and placed in urns
and then the urns, in turn, were placed in tombs.
Greeks.
—Homer describes cremation, as an honorable
mode of sepulture practiced in the heroic ages. Later
from their many conquests, the Greeks acquired the art
of embalming patterned after the Arabian and Assyrian-Persian
methods, of which we have no record.
[18]
Norsemen.
—It appears from the sages that a form of
cremation was used by the early Norsemen, who used
to place the viking in his ship and send him “flaming
out to sea.” Later it became the custom to place him,
with all his belongings, in his vessel set on an even keel,
and entomb him beneath a mound of earth.
Hindoos.
—Suttee (from Sati-a virtuous wife), an Indian
custom, involving the burning of widows on the
same funeral pyre as the husband, was the rule until
1829 A. D.
French and Belgians.
—Paleolithic cave dwellers of
France and Belgium buried their dead in natural caves
or crevices, like those in which they lived. Later stone-age
people throughout Europe buried in chambered barrows
or cairns. Bronze age people buried in unchambered
barrows or in cemeteries of stone cists set in the ground
often on a natural eminence, and surrounded by circles
of standing stones. The cist was formed of a double
row of stones covered with rude stone slabs.
Britains.
—Neolithic tribes in Britain buried either in
caves or in chambered tombs, probably representing the
huts of the living. Some of these barrows are very
elaborate and massive; that of West Kennett is said to
be 350 feet long. The dead were buried in the British
tombs as they died, or in a contracted posture, probably
due to their habit of sleeping in this position, and not
at full length on a bed. Many cleft skulls are found in
these tombs, suggesting human sacrifice, which as Caesar
tells us, was prevalent among the Gauls. The bronze age
usages were divided between burying and cremation. In
[19]
burying, the contracted posture was followed. In cremation,
the body was placed in a coffin made of the hollow
trunk of an oak, split in two. In cremation, the ashes
were collected in a funeral urn, twelve to eighteen inches
high and were placed in a chamber. Articles of daily
use were thrown into the fire.
Peruvians.
—The aborigines of the western continent
were familiar with embalming. Prescott's “Conquest of
Peru” tells that the royal “Incas” of Peru, were preserved
by some process which did not give evidence of an
external application. These bodies were then secreted
under mounds of earth and in the interior of the temples.
Prescott presents highly interesting pictures of these
embalmed Peruvian monarchs sitting “natural as life,”
in the chairs of the temples of the sun, at Cusco. They
were clothed as in life, the raven black hair on their
heads was still unchanged, and their hands were crossed
upon their bosoms in the grim dignity of death.
Aztecs.
—The Aztecs, who were highly civilized, and
were one of the most interesting and powerful tribes of
early America, inhabited Mexico. The Aztecs were conquered
by Cortez in 1519. Their history has been traced
back to the twelfth century. The bodies of their dead,
especially of those who could claim royal descent, were
embalmed. It is related in Aztec legends how, after the
deluge, seven persons came forth from the tomb to which
their mummified bodies had been committed, and, in renewed
existence, repeopled the earth.
North American Indians.
—Even our own North American
Indians knew the art of embalming. Mummies remarkably
[20]
well preserved have been found among the
Flat Heads, Dakotas and Chinooks; and the Florida and
Virginia Indians preserved the bodies of their Kings in
the same way. The Kentucky caves have given up some
remarkable specimens of this kind. The bodies of a
woman and child were, in 1899, found in a cave in the
Yosemite valley, and which, on account of its size (six
feet and eight inches), some authorities believe to be a
relic of the lost tribe of the stone age, possibly antedating
the Christian era 3,000 years.
Early Christians.
—For a time the early Christians
embalmed the bodies of their dead, using these forms
with which they were familiar in Palestine. After a time,
however, they gave up the practice. It has been said that
they feared by the continuation of the process to cast
discredit upon the power of God to call together the
scattered dust of the body which had returned to its
native element, and present it, like unto Christ's own
glorious body, on the morning of the resurrection. No
word spoken by Jesus, would indicate that he disapproved
of methods, with which he as a Jew was familiar,
to preserve the body from decay. During the first four
centuries of the Christian era, the catacombs at Rome
were used for burial. These catacombs consist of subterranean
excavations, long horizontal passages with recesses
on either side, arrayed in tiers for the reception of
bodies, closed in by slabs bearing inscriptions and emblems
of the faith.
Later European Embalming.
—After the previous discussion
of the care of the dead affecting prehistoric as
[21]
well as the earliest historic usages, we are brought forward
to the seventeenth century. All embalming processes
of the earlier days having been forgotten during
the dark ages. The slow but sure development of the
medical profession having manifested a dire necessity
for the preservation of anatomical material, this necessity
was first met by Dr. Frederick Ruysch, who occupied the
chair of anatomy at Amsterdam, Holland, during the close
of the seventeenth and early years of the eighteenth century
(1665-1717).
Dr. Ruysch was probably the first to practice a successful
system of arterial injection, in order that his
anatomical specimens might resist the processes of decay.
The reader should understand that embalming as
a convenient process for preserving human dead bodies
for funeral purposes had not been thought of at this time,
and the principal interest in embalming was for its successful
preservation of anatomical specimens. The method
followed by Dr. Ruysch, was first an arterial injection,
then allowing the diffusion of the fluid for some hours,
after which, he proceeded to open the body as in making
a postmortem examination, removing the viscera, cleaning
them and replacing them surrounded with a preservative
solution. Dr. Ruysch died, leaving his secrets
buried with him, and they were lost to science.
Dr. William Hunter, an eminent Scottish physician,
anatomist and physiologist of the eighteenth century
(1718-1783) is given credit by many as being the original
inventor of the injection system, for he published his
plan of injection in minute detail, so that science might
[22]
benefit thereby. The artery usually selected by Dr.
Hunter was the femoral and his solution was composed
of oil of turpentine five pints; Venice turpentine, one
pint; oil of lavender, two fluid ounces; oil of rosemary,
two fluid ounces; and vermillion. This was forced into
the vessel until it reached over the whole body, giving
the skin a general reddish appearance. As in Dr. Ruysch's
method, the body was left untouched for a time, and
was then opened, the viscera being treated and placed
back again. After treating the exterior of the body in
some cases, a coffin was prepared and the body was
placed on a bed of dry plaster of paris in order that
desiccation might set in. The body was then left for
four years and if dryness had not set in by that time,
was placed upon another bed of plaster of paris. Some
of Hunter's specimens are to be seen today in the
museum of the Royal College of Surgeons, London.
Dr. John Hunter, a younger brother of William, was
also very active in experimentation along these lines,
and his work was little less renowned along the same lines.
The Hunterian method was used for years by English
anatomists with little if any alteration.
M. Boudet, attempted to use the Egyptian form of
procedure in embalming, using as preservative agents
corrosive sublimate, tan, salt, asphalt, Peruvian bark,
camphor, cinnamon, and other aromatics. He completely
enveloped the body in bandages, varnish being coated
over the body and cavities and outer bandages.
M. Franchini, injected the common carotid artery
with a solution made up of eight decigrams of arsenious
[23]
acid, combined with a small quantity of cinnabar, dissolved
in nine kilograms of spirits of wine. By this method
bodies could be kept odorless and natural in color for
sixty days, after which desiccation set in.
Jean Nicholas Gannal, and his son Dr. Gannal of Paris,
injected chloride of alumina with success, J. N. Gannal,
had previously, a formula containing arsenic, which the
French Government compelled him to discontinue by
prohibiting the sale of the arsenic. In addition to the
above treatment the body was placed in a lead coffin and
four or five litres of various essences were poured over
the body and the casket was soldered. In this way preservation
was said to be indefinite.
M. Sucquet, injected a solution of chloride of zinc
arterially, and in one body which was taken up after
being buried 14 months achieved remarkable success, the
incident being the result of a contest between M. Gannal,
M. Dupre, and M. Sucquet. This led to the use of the zinc
salts in fluid, not only in Europe but in this country
as well.
M. Falcony, desiccated the body in a mixture which
was composed of saw dust and powdered zinc sulphate.
Bodies so preserved remained flexible for about forty
days, after which they dried up, although still retaining
their natural color.
Franciolli, used arsenic acid, four ounces; carbonate
of potash, two ounces; powdered alum, eight ounces. He
completely eviscerated the body and then injected it in
all directions, afterwards replacing the organs and surrounding
them with liquid preparation composed of corn
[24]
starch, water, alcohol, and corrosive sublimate, which
after hardening, would prevent the sinking of the parts.
Many processes are noted in the various histories of
the art, all using the arterial injection, which by this
time had become universally accepted as the only true
way of reaching the body tissues completely. The reader
has noted absolutely nothing as to embalming being the
most convenient process for funeral purposes. This is
left to the following matter which begins with the embalming
done by Dr. Thomas Holmes during the civil
war (1861-1865 A. D.)
[25]
CHAPTER III.
EMBALMING IN AMERICA AFTER THE
CIVIL WAR.
Dr. Holmes was authorized by the U. S. Government
to prepare the bodies of slain troops, so that they could
be transported to their former homes. The practice of
embalming for funeral purposes received its greatest
impulse during the regime of Dr. Holmes, and it opened
up an era of unprecedented discovery and success in preserving
the dead body.
After Holmes, the man who cared for the dead began
to feel that his was a professional work worthy of the
name. The average undertaker, at the time just after
the civil war, was a cabinet maker, whose chief function
was to make the coffin or casket for the body, take the
casket to the house and place the body in it. Then the
larger undertakers in the larger cities found that they
were compelled to preserve some of the bodies in some
way so that distant relatives could reach the scene before
the funeral. This probably was the result of betterments
in transportation facilities which led people to
travel more. Along with this, travelers frequently died
away from home and had to be shipped. The baggage
men rightfully objected to remaining in the same enclosed
space with an unembalmed body and, altogether,
[26]
a condition arose in which it was necessary to have some
way to preserve the body.
As evolution is always a slow process, we cannot as
we would like to do, chronicle the introduction of chemical
embalming at this time, for refrigeration was the first
thing thought of. The ice box, was the means by which
bodies were kept for several days; the body being covered
and left that way until a few hours before the
funeral. This became so unsatisfactory specially when the
sensibilities of the undertaker became sharpened, that
they immediately looked about for a more convenient
way to handle the situation. Spurred on by this demand,
several concerns came into the market with preservative
solutions with an arsenical base, and which were used
principally for external application and cavity injection.
All kinds of instruments were used with which to introduce
the fluid into the body cavities until Captain
George Billow, of Akron, Ohio, a civil war veteran, and
at present a member of the Ohio State Board of Embalming
examiners, contrived the pen point trocar, which
is still in use among the profession.
With the introduction of the trocar, and the campaigns
of the fluid manufacturers, trade periodicals and traveling
men, cavity embalming became the means of preservation,
until its limitations were learned.
Joseph Henry Clarke, who first traveled for fluid
houses, and who was interested in the anatomy of the
human body, since his connection with the U. S. hospital
service in the Civil war, determined to introduce the
arterial injection as the means of placing the fluid through
[27]
the body. In collaboration with Dr. C. M. Lukens, the
occupant of the chair of Anatomy at the Pulte Medical
College of Cincinnati, Prof. J. H. Clarke opened a school
of embalming naming it the Cincinnati School of Embalming.
This took place during the year 1882. Prof.
Auguste Renouard of Denver, Colorado, came into the
field about the same time. Thus we have the beginning
of the greatest revolution of all times in the care of the
dead human bodies.
After Prof. Clarke and Prof. Renouard, came Prof.
Frank Sullivan, and from time to time the list was
augmented by the addition of others, a few of whom
being Dr. Eliab Meyers, of Springfield, Ohio, Dr. Carl L.
Barnes of Chicago, etc. With the efforts of all these men,
the undertakers were led to use the arteries more and
more until now, at the present time, this form of embalming
is used exclusively through the United States, and
Canada; European countries not having, as yet progressed
as rapidly in that direction. The additions to the work
from the time just previous to the start given to it by
Prof. Clarke, number all the methods which we use today,
including, the injection of any large artery in the
body; the drainage of blood to further the obtaining of a
complete circulation; the various processes by which
discolorations are prevented and cured; the various processes
by which bodies are disinfected; the various processes
by which features are restored and many other of
the vital operations of the present time. The undertaker
having progressed from the cabinet maker, to a man of
professional bearing having a good knowledge of all
[28]
things pertaining to the dead human body, is now a
man in whom the greatest reliance may be placed. Where
previously, he was uneducated and uncultivated in matters
pertaining to the body, he is now an authority to
a great extent.
As a part of this historical contribution, we cannot
overlook the very great advance made in the nature
and composition of the preservative solutions used today.
When formaldehyde was introduced, the high cost of
it prevented its immediate use; but, later on, improved
methods of manufacture brought the cost down to such
a point where it became an essential ingredient in the
fluids. Later when, on medico-legal grounds, arsenic
was prohibited in the fluid (this action paralleling the
action taken by France in the case of J. N. and Dr.
Gannal), formaldehyde was depended upon for the maximum
preservative action. Thus it still remains the base
of most of the modern fluids. Several compounders have
discontinued its use, preferring phenol, creosote, etc., but
these chemicals have not as yet, made much progress
against the formaldehyde.
In the early days, when the fluids were likely to be
inadequate to care for certain conditions, the question
as to which fluid is to be used was the principal care of
the embalmer. Today, when the standard fluids are of the
highest possible efficiency, it is a question of knowledge
and technic on the part of the embalmer; it being a
recognized fact that there is only about 1 chance in 1,000
for a standard fluid to contain inferior elements. In this
way we may state that the burden of obtaining success
[29]
has been shifted from the fluid, to the man using it; and
it is then unnecessary to state that the best preparation
along the line of education for the embalmer is advised,
so that by his knowledge, he may do what he is expected
to do by the people whom he is serving.
[33]
Anatomy
The word anatomy is derived from two Greek words,
meaning, to cut apart, which literally means dissection.
Anatomy is used to indicate the study of the physical
structure of organized bodies.
Anatomy is the science of organization or the science
of organic structure.
Human anatomy is divided into two great divisions,
known as (a) general or descriptive anatomy and (b)
surgical or regional anatomy.
Descriptive anatomy deals with the separate parts
of the human body.
Histology is that part of descriptive anatomy where
the separate parts of the human body are studied by
means of the microscope.
Osteology is that part of descriptive anatomy describing
the number, form, structure and uses of bone.
Myology is that part of descriptive anatomy which
treats of muscles.
Neurology is that part of descriptive anatomy which
treats of nerves.
Syndesmology is that part of descriptive anatomy
which treats of ligaments.
[34]
Angiology is that part of descriptive anatomy which
treats of the blood-vessels and lymphatics.
Surgical or regional anatomy describes the relation
which certain parts,—muscles, nerves, arteries, etc.,—bear
to each other.
[35]
CHAPTER IV.
HISTOLOGY.
Definition.
—Histology is that part of descriptive anatomy
which treats of the intimate structure of the tissues
as seen under the microscope.
Histology as taught in most professional schools constitutes
a one year's course, but for the embalmer this
is not entirely necessary and with the short term of schooling
now existing it is quite impossible, but certain of
the fundamental principles of histology are important.
For this reason a few of the more important tissues have
been discussed, not, however, in great detail, but only
superficially, merely to have the embalmer acquainted
with them.
A Cell.
—A cell is defined as a nucleated mass of protoplasm
endowed with the attributes of life.
Protoplasm is the name applied to the semi-fluid,
granular substance contained within the cell.
The simplest forms of animal life are organisms consisting
of only one cell which are called protozoa.
Cells having similar shape and similar functions are
grouped to form tissues.
Tissues are grouped together to form organs.
[36]
Every cell consists of a cell body and a nucleus. The
cell body consists of a substance known as protoplasm.
The nucleus is the essential part of a typical cell and
is the controlling center of its activity.
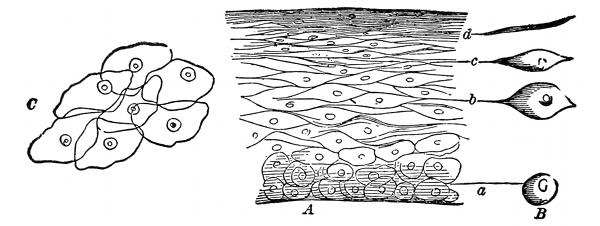
Fig. 1—A, A vertical section of the cuticle; B, the lateral view of the
cells; C, the flat side of scales like (d) magnified
250 diameters.
Cells divide or reproduce themselves by means of
direct or indirect division. In direct division the nucleus
and the cell wall simply divide into two equal divisions
and results in the formation of two new cells. In indirect
division the process is much more complicated,
and several stages must be passed through before there
is a complete division.
The process of fertilization consists in the conjugation
of two sexual cells. The male sexual cell is called the
spermatazoon, and the female sexual cell is called the
ovum.
The nucleus of the ovum in its earlier development
stages is known as the germinal vessicle.
In the living organism many cells are destroyed during
the various physiologic processes and are replaced by new
[37]
ones. When a cell dies, changes take place in the nucleus
which result in its gradual disappearance. This
process is known as chromatolysis.
Tissues.
—A tissue is an aggregate of cells all having
a common function.
Those important tissues with which the embalmer
should be more or less acquainted are the following:
Skin, nails, hair, superficial fascia, deep fascia, lymphatics,
glands, cartilage, bone, teeth, nerves, muscles,
tendons, aponeuroses, ligaments, fat, mucous membranes,
serous membranes, synovial membranes, arteries, veins
and blood.
The Skin.
—The skin or integument (intego, to cover)
is the outside covering of the human body. It is the
first tissue that is cut when
operating upon the body.
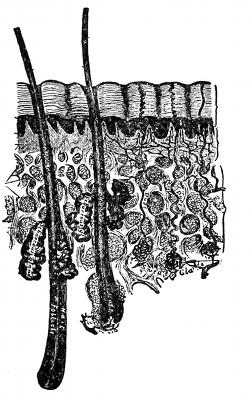
Fig. 2—A cross section of
the skin. (Gray)
The skin is the seat of the
organs of touch. The multitudes
of sensory nerve endings
convey the sensations of temperature,
pressure and pain to
the brain, thus informing the
brain at all times, to keep the
body from harm, and in a
strong and healthful condition.
The skin is also the regulator
of the body temperature, for
connected with the skin are
sweat glands, and sebaceous
glands, each having important
excretory functions.
[38]
The skin is also a protective coat, very elastic, and
varies greatly in thickness. It is thinnest in the eyelids
and thickest over the back of the neck, back of the
shoulders, palms of the hands and the soles of the feet.
The color of the skin depends upon two things, first,
on the pigment, which is found, one of the discriminating
points between the races, named by the color of the skin
as white, black, yellow, etc.; second, the color depends
upon the amount of blood in circulation, the deepest hue
being in the parts exposed to the air, light and the varied
temperatures. Besides these the color of the skin varies
with age, pinkest in the infant and becoming yellow with
old age. It varies with exposure and with climate, the
people living in the north having a much different complexion
than those living in the south under the tropical
sun. The color of the skin also varies with certain diseases,
being extremely pale in anaemia, brown in Addison's
disease, and yellow in jaundice.
The skin can be said to be moveable, although in
places it is attached firmly to the underlying structures,
especially on the scalp, the soles of the feet, and the palms
of the hands.
Upon close examination the skin discloses a multitude
of openings, creases, furrows, depressions, folds and
hairs.
A dimple is a permanent pit or depression due to the
adhesion of the surface to parts beneath.
Structure.—The skin consists of two intimately connected
structures, the one is the true skin, corium, or
dermis and is the deepest layer of the skin; and the other
[39]
is the false skin, cuticle, or epidermis, and is the outermost
layer of the skin.
The true skin, is composed mostly of connective tissues
and elastic fibers. It is the real seat of the sense
of touch, for it is here that the sensory nerves have their
termination. In this layer we also have the termination
of the minute capillaries of the skin.
The false skin, contains no blood vessels or nerves,
and being without these it is practically dead tissue, and
to illustrate this fact one can take a needle and run it
through this outside layer without the least pain or the
drawing of blood.
The false skin is the part which slips off in case of
skin slip. In as much as the minute capillaries end at
the termination of the true skin, when putrefaction and
fermentation begin there is an oozing of water from the
capillaries and the surrounding tissues, between the two
layers of skin, causing a blister to form, and known as
skin slip.
At the lowest part of the false skin is a layer of
germinal cells, from which all the other cells are derived,
and becoming more flattened and horny as they are pushed
farther away from the blood supply; and also a layer
of pigment cells, which give the discriminating color to
the skin.
In the skin are seen numerous sebaceous and sweat
glands.
The sweat glands are the organs by which a large
portion of the aqueous and gaseous materials are excreted
[40]
by the skin. Sweat glands are found in almost every
portion of the skin, and are situated in small pits below
the surface of the skin, surrounded by a quantity of
adipose tissue or fat. They are small, round, reddish
bodies, consisting of a single tubule, convoluted in form,
which extends up through the skin and opens on the surface.
The size of these glands, of course, vary, being
especially large in those regions where the flow of perspiration
is copious as in the axilla.
The sebaceous glands are small, sacculated, glandular
organs, lodged in the substance of the skin. They are
found in most parts of the skin and are usually connected
with the hair follicles. Each gland consists of a
single duct, more or less capacious, which terminates
in a cluster of small secreting pouches or saccules. These
glands secrete an oily fluid, which keeps the skin soft
and also oils the shaft of the hair.
The Nails.
—The nails are a peculiar modification of
the epidermis and have the same cellular structure as that
of the epidermis. The nails are found on the dorsal surface
of the fingers and toes and act as a protection, and
enable one to pick up small objects, or to grasp more
firmly any object. Were it not for the nails it would
be impossible for one to pick up a needle from off the
floor.
Each nail is convex on its outer surface, and its chief
mass which is called the body lies upon the nail bed, or
true skin; the free end projects out over the surface of
the finger, and is that part which is not attached below,
and since it is the continuation of the epidermis, it likewise
[41]
will have no nerve or blood supply and therefore
can be trimmed without pain to the individual.
The root is implanted in a groove in the skin and
is composed of cells which have not become horny. The
root is white in color and is the little half moon which
you can see next to the skin.
The matrix is that part of the true skin beneath the
body and the root of the nail, and is so called, because,
it is that part from which the nail is produced and so
long as the matrix at the root of the nail is uninjured,
the nail will be reproduced after an accident.
After death the nail turns black, due to the infiltration
of blood into the matrix.
Treatment by the Embalmer.—The blackened condition
of the nail due to the infiltration of blood into the
matrix can in many cases be overcome by carefully rubbing
the nail at the time the body is being injected. After
the discoloration is removed the fingers should be kept
elevated so that the blood will not settle there again.
The Hair.
—The hair, like the nails, is a peculiar modification
of the epidermis and consists of practically the
same cellular structure as the epidermis. Hair is found
on nearly every part of the body excepting the palms
of the hands and the soles of the feet, the borders of
the lips, etc. It varies much in length, thickness and in
the different races of mankind. In the eyelids it is short,
on the scalp it is of considerable length. In other parts
as the eye-lashes, the hair of the pubis region, the whiskers
and beard the thickness is remarkable.
A hair consists of the root and the shaft. The root
[42]
of the hair or that part implanted in the skin presents
at its extremity a bulbous enlargement, called the hair
bulb. Into this bulb we find the small arterial capillary
circulating and at its termination the beginning of the
venous capillary. In this way the hair is nourished in
life. We also find a small nerve going to the hair bulb.
The shaft is the remaining part or that part coming out
from the skin.
The hair grows from its roots and as it grows it
pushes itself out from the skin and owes its growth to the
small capillary circulation, carrying pure arterial blood to
each and every hair, and for this reason you can understand
for yourself the erroneous idea of what is termed
the “post-mortem growth of hair.” Only a few weeks
ago one of the students declared that he had actually seen
a subject shaved and the body at the time of the funeral
was placed in a vault to await the arrival of a close relative
who had to come from Europe.
Three weeks later the student, together with the undertaker
and relatives, went to the vault to view the remains.
The body was in a perfect state of preservation,
only for a large growth of beard as the student supposed.
This student had observed rightly, but he did not go
far enough. He did not think of how the hair actually
got its nourishment. The hair owes its life to the circulation
of the blood, just as much as the heart or any
other organ does, and will die and cease to grow just
as soon as the body dies and the circulation is cut off.
What this student saw was only an apparent growth, for
after the body dies the tissues begin to shrink, squeezing
[43]
the blood and fluid substances out of them, thus giving
the hair cylinder a more projected appearance.
The student was very much surprised at his mistake,
but after the explanation he saw that the hair owed its
life to the circulation and that when this circulation was
cut off, the hair must cease to grow.
The chief function of hair is that of protection from
heat or cold and to help shield the brain from the effect
of a blow upon the head.
The hair, next to the teeth and bones, is the least destructible
part of the body.
The Fascia.
—The fascia (fascia, a bandage) is areolar
or aponeurotic tissue of variable thickness and
strength found in all regions of the body and invests or
surrounds the softer and more delicate organs. From
its situation in the body the fascia is divided into two
groups, superficial and deep.
Superficial fascia is found immediately beneath the
skin over almost the entire surface of the body. It connects
the skin with the deep fascia and consists of areolar
tissue.
The superficial fascia varies in thickness in different
parts of the body and some places, especially in the groin
is capable of being subdivided into several different
layers. The first layer of the superficial fascia, which
is just beneath the skin, usually contains a great amount
of fat or adipose tissue. This, in most text books, has
been termed the subcutaneous tissue. The second layer
is comparatively devoid of adipose or fatty tissue and
in this we find the trunks of the subcutaneous vessels and
[44]
nerves, as for example, the radial and ulnar veins in the
arms and the saphenous vein in the leg.
The superficial fascia facilitates the movement of the
skin, serves as a soft medium for the passage of the vessels
and nerves to the skin and retains the warmth of
the body, since the fat contained in its meshes is a had
conductor of heat.
Deep fascia or aponeurotic fascia is a dense inelastic,
unyielding fibrous membrane, forming a sheath for the
muscles and affording them broad surfaces for attachment.
On removal of the superficial fascia, the deep
fascia is usually exposed and can be seen as a dense,
tough membrane, which not only binds down the muscles
to each region, but gives to each a separate sheath as
well as to the blood vessels and nerves.
Thus, on going down into the arm between the biceps
and triceps muscles to raise the brachial artery, you
would first cut through the skin, then the subcutaneous
tissue, the superficial fascia and then you would come
to a membrane investing the artery, vein and nerve.
This membrane is the part of the deep fascia which
covers the vessels, making a distinct sheath for them and
you must go through this sheath before you can hope
to raise the artery.

Fig. 3—Lymphatics of the head and neck.
B, the thoracic duct.
The Lymphatics.
—The lymphatics occur in all parts
of the body, and in many respects resemble the veins,
one of the most striking similarities being that the lymphatics
contain valves just the same as the venous system.
The lymphatic capillaries are arranged in the form of
a net work and resemble closely in structure the blood
[45]
capillaries. These capillaries then unite to form the
lymph vessels and these then convey the lymph to the
subclavian veins. The lymph is a colorless fluid and
contains numerous blood corpuscles known as lymphocytes.
But in those lymphatic vessels, which have their
origin in the walls of the small intestines, the lymph,
especially during digestion, contains a great amount of
fat, so that it has a milky appearance, and for this reason
the lymphatics of this region, have been termed lacteals.
There are two main lymphatic trunks, the one on the left
side is called the thoracic duct. This duct extends from
the lower border of the second lumbar vertebra, through
the entire length of the thorax, and opens into the left
[46]
subclavian vein, close to the point where it is joined to
the left internal jugular. It receives the lymph from the
lower limbs, the pelvic walls and
viscera, the abdominal walls and
viscera; the lower part of the
right half and the whole of the
left half of the thoracic viscera,
the left side of the neck and head
and the left arm.
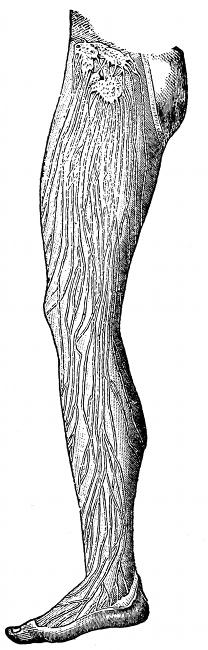
Fig. 4—Lymphatics of
the leg.
The other duct is called the
right lymphatic duct and receives
lymph from the upper part of
the right side of the thoracic wall,
part of the right side of the diaphragm
and the right lobe of the
liver, the whole of the right arm
and neck and right side of the
head. This trunk is very short
and empties its supply of lymph
into the right subclavian vein.
Receptaculum chyli is the expanded
portion of the thoracic
duct just at its beginning. Its
function is to receive the lacteals
which come from the villi of the
intestines.
Lymph glands are the enlargements
of the lymph vessels. They
occur frequently in the lymphatic
system, being most numerous in
[47]
the axillary space, the cervical region (in the neck)
and in Scarpa's triangle.
The lymphatic system aids greatly in warding off such
diseases as blood poisoning, anthrax, etc.
The lacteals are the lymphatics which carry the
chyme from the villi of the intestines and deposit it in
the receptaculum chyli.
Glands.
—The glands of the human body are divided
into three classes called tubular, alveolar and tubulo-alveolar
glands.
Tubular Glands.—In these, the secreting portion consists
of a long or short tubule, which may be relatively
straight or variously twisted, one end of which ends
blindly, while the other end opens on the free surface
or into a duct.
Tubular glands may be simple, or having only a single
tubule; they may be simple branched, having more than
one tubule; or they may be compound branched, thus
resembling the branching of a tree.
Some tubular glands would be the liver, kidneys,
testes, lachrymal glands, serous glands of the mucous
membranes, fundus glands of the stomach, uterine glands,
the majority of the pyloric glands and the majority of
the sweat glands.
Alveolar Glands.—In these, the secreting compartments
have the form of variously shaped vesicles or saccules,
known as alveoli which open on the free surface
or into a duct.
Alveolar glands may be either simple, simple branched,
or compound branched.
[48]
Some alveolar glands would be the sebaceous glands,
pancreas, mammary gland, ovary and thyroid.
Tubulo-alveolar Glands.—In these, there is a combination
of the tubular and the alveolar type. They may
also be simple, simple branched or compound branched.
Some of this type would be certain of the pyloric
glands, certain of the sweat glands, some mucous glands,
the prostate and the lungs.
The most important glands will be discussed under
the tissue or the organ in which they are situated.
Cartilage.
—Cartilage is a transition stage between
connective tissue and bone; when it is boiled it yields
condrin. It is found in various parts of the body, in
the adults being found chiefly in the joints, in the sides
of the thorax, and in various tubes which are not kept
permanently open, such as the air passages, nostrils, ears,
etc. In the foetus, the greater part of the framework is
cartilaginous and as the foetus matures this cartilage
is finally replaced by bone. Cartilage is divided into
hyaline cartilage, elastic cartilage, and fibro cartilage.
Hyaline cartilage is found in the nose, larynx, trachea,
and bronchi.
Elastic cartilage is found in the epiglottis and the
cartilages of the larynx.
Fibro cartilage is found at the point of insertion
of the ligaments, into the body of the bone, such as the
cartilage which helps to hold the femur or long bone
of the thigh into the hip.
Bones.
—Bone results from the calcification of cartilage
or fibrous tissue. It is a highly specialized form of
[49]
connective tissue. There are two varieties of bone;
dense or compact bone and cancellous, loose, or spongy
bone. Compact bone is dense, like ivory, and is always
found on the exterior of bones.
Cancellous bone is found in the interior of bones, and
has a lattice-work appearance.
Bone consists of one-third animal or organic matter
and two-thirds earthy or inorganic matter. These proportions,
however, vary with age. In youth it is nearly
half and half, while in the adult the earthy is greatly
in excess. It also varies with disease. With some defect
of nutrition, the bone is deprived of its normal proportion
of earthy matter, while the animal matter is of
unhealthy quality, and we have as a result, a disease
called rickets, so common in the children of the poor.
The earthy or inorganic matter consists of phosphate,
carbonate, fluoride of calcium, sodium chloride, and
phosphate of magnesium. The animal matter consists of
fat collagen, which when boiled with water is resolved
into gelatin.
To illustrate the two substances, take a bone and place
it in dilute hydrochloric acid. The acid will eat out all
the mineral matter and we have left only the animal
matter. After this operation one can take the bone and
can bend it into any position whatever, which experiment
shows that the animal matter gives elasticity to the bone.
The second experiment would be to put the bone on
a bed of hot coals and burn it. Only the animal matter
will burn and we will have the mineral matter remaining.
[50]
After this operation one will find that the bone is very
brittle and will easily break, which experiment shows
that the mineral matter gives stability and support to
the bone.
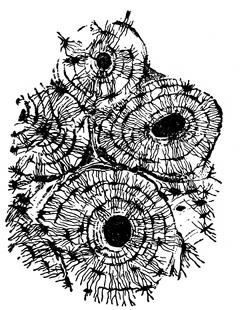
Fig. 5—Cross section of
bone. (Sharpey)
If a cross section is made of any
long bone, such as the humerus,
and this section placed under the
low power of the microscope, the
Haversian canal system can be
discerned. The Haversian canal
system consists of the numerous
small openings or canals through
which the blood vessels ramify in
distributing the nourishment to
the bone. Around each individual
canal are seen smaller spaces arranged
in a circle. These are known
as the lacunae (small lakes). Going from the lacunae
are smaller canals which take on the name canaliculae,
and joining all the lacunae together, making the appearance
of concentric circles, we have the lamellae. The
outside covering of the bone is called the periosteum and
the inside covering is called the endosteum. Most of
the long bones and many of the smaller bones are supplied
by a nutrient artery, which enters the bone near
its center, enters the bone marrow, and divides into
two branches, one going up and the other down in the
marrow. The blood is then distributed through the Haversian
canal system. Veins emerge from the long bones
in three places: 1. One or two large veins accompany
[51]
the nutrient artery. 2. Numerous veins emerge from
the articular extremities. 3. Many small veins arise
in and emerge from the compact substance.
Bones are divided, according to shape, into four
classes: long, short, flat and irregular.
Long Bones.—These bones are usually used as a system
of levers to confer the power of locomotion. A long
bone consists of a shaft and two extremities. The shaft
is a hollow cylinder within which is the medullary canal.
The extremities are somewhat expanded for the purpose
of articulation, and to afford a broad surface for the
attachment of muscles. The long bones are as a rule
curved in two directions to give greater strength to the
bone. Some examples of this class of bone are the
clavicle, radius, ulna, humerus, femur, tibia, fibula, metacarpal,
metatarsal, and the phalanges.
Short Bones.—These bones are placed in that part
of the skeleton where there is need for strength and compactness,
and where the motion of the part is slight and
limited. Some examples of this class of bone are the
bones of the carpus and tarsus (in the hand and the
foot).
Flat Bones.—Flat bones are found where the principle
requirement is either extensive protection, or the
need of a broad surface for the attachment of muscles.
Some of the bones of this class are the occipital, parietal,
frontal, nasal, lachrymal, vomer, scapula, sternum, and
the ribs.
Irregular Bones.—These bones are such as from their
peculiar shape and form can not be grouped under any
[52]
of the preceding heads. Some of the bones of this class
are the vertebrae, sacrum, coccyx, temporal, sphenoid,
ethmoid, etc.
If the surface of a bone is examined, certain articular
and non-articular eminences and depressions will be seen.
Articular Eminences.—Examples of this class are
found in the heads of the humerus and the femur.
Articular Depressions.—Examples of this class are
found in the glenoid cavity of the scapula and the
acetabulum.
Non-articular Eminences.—These are designated according
to their form.
A tuberosity is a broad, rough, and uneven elevation.
A tubercle is a small, rough prominence.
A spine is a sharp, slender, pointed eminence.
A ridge, line, or crest is a narrow, rough elevation,
running some way along the surface.
Non-articular Depressions.—These are of variable
form, and are described as notches, sulci, fossae, grooves,
furrows, fissures, etc. These non-articular eminences and
depressions may serve to increase the extent of surface
for the attachment of ligaments and muscles or may
receive blood vessels, nerves, tendons, ligaments, or portions
of organs.
Canals or foramina are channels or openings in bone
through which pass the nerves and blood vessels.
Teeth.
—In the human body we find two sets of teeth.
One appearing in childhood, and are known as milk teeth,
twenty in number, the permanent teeth replacing these
about the sixth year.
[53]
There are thirty-two permanent teeth, divided into
four incisors, two canines, four bicuspids and six molars.
Teeth are made up of three different substances, which
are known as enamel, dentine and cement.
The enamel is a very hard substance, the hardest in
the body, and may be compared to quartz. The enamel
covers the entire tooth down as far as the gums.
The cement is a continuation of the enamel below the
gums, and is closely adherent to the dentine. The cement
consists of bone tissue, but the lamellae as a rule
do not contain Haversian canals.
The dentine is, next to the enamel, the hardest tissue
of the tooth, and composes the main body of the tooth.
The pulp cavity is found within the center of the tooth,
with the opening toward the jaw bone. The tooth is
nourished by a nutrient artery and vein and nerve which
pass into the pulp of the tooth.
Nerves.
—Nerves are divided into two general classes,
called medullary and non-medullary nerves. The non-medullated
type arise mostly from the sympathetic system,
while the medullated type arise from the brain and
cord. As a rule, the nerves of
the body follow the course of
the arteries, and are generally
found in the same sheath with
the artery and vein.

Fig. 6—Section of a nerve fibre.
(Klein and Noble Smith)
They are easily distinguished from the arteries and
veins by touch and by their color, being very inelastic
and fibrous, hard to the touch, and unlike the artery
or vein, since they have no central opening.
[54]
Muscles.
—Myology is that branch of anatomy which
treats of the muscles. The muscles are formed of bundles
of reddish fibres, endowed with the property of contractility.
In the body we find two kinds of muscular
tissue, called voluntary and involuntary muscle. The
voluntary type is characterized by the
striped appearance which it displays when
seen under the microscope, and for this
reason it is called striped or striated
muscle. It is so named “voluntary” because
it is capable of being put into action
and controlled by the will. The involuntary
muscles do not present any
striped appearance, and consequently are
called unstriped or non-striated, and are
not under the control of the will. An
example of voluntary muscle would be
any muscle of the bony framework as
for example, the biceps or triceps.

Fig. 7—View of
muscle fibers.
An example of involuntary muscle would be those of
the intestines and stomach, the muscles of the bladder
and uterus and the walls of the arteries and veins, etc.
When viewed under the microscope, the muscle is
seen to be composed of many fibrils. The sheath covering
each fibril is called the sarcolemma, and contains
within its boundaries the muscle plasma, or protoplasm,
and a nucleus. Many of the fibrils when grouped together
constitute the entire muscle.
The muscles get their blood supply from the nutrient
artery, which ramifies the tissues, the smallest capillaries
coming in contact with each muscle cell.
[55]
Tendons.
—Tendons are white, glistening, fibrous
cords, varying in length and thickness, sometimes round,
sometimes flattened, of considerable strength, and devoid
of elasticity. It consists principally of a substance
which yields gelatin.
Tendons do not have a direct blood supply.
Aponeuroses.
—Aponeuroses are flattened or ribbon-like
tendons, of a pearly-white color, irridescent, glistening,
and similar in structure to the tendons.
Ligaments.
—Ligaments consist of bands of various
forms, serving to connect the articular extremities of
bones. They are strong bands of smooth, silverwhite
fibrous tissue.
A ligament is pliable and flexible, so as to allow the
most perfect freedom of movement, but at the same
time it is tough and strong, so as not to yield readily under
the severe applied force, and for this reason they
serve as good connecting links for the binding of bones
together.
Poupart's Ligament.—Poupart's ligament extends
from the crest of the ilium to the top of the pubic bone.
This ligament is of utmost importance to the embalmer,
as it serves as a guide to locate the femoral artery. By
placing the thumb on the crest of the ilium and the second
finger on the top of the public bone, then letting
the first finger drop midway between the two, which
would be the center of Poupart's ligament, we have a
point which marks the exit of the artery from the body
and the beginning of the femoral artery.
[56]
Poupart's ligament also forms the base of Scarpa's
triangle. The structure of this triangle will be taken
up later.
Fat.
—Fat is a deposit of an oil in the cells of the tissues,
just beneath the skin, giving roundness and plumpness
to the body, and acting as an excellent non-conductor
for the retention of heat.
So tiny are these cells, that there are over sixty-five
million in a cubic inch of fat. As they are kept moist,
the liquid does not ooze out; but, on drying, it comes to
the surface, and thus a piece of fat feels oily when exposed
to the air. The quantity of fat varies with the
state of nutrition. In corpulent persons, the masses of
fat beneath the skin, in the mesentery, on the surface of
the heart and the great vessels, between the muscles, and
in the neighborhood of the nerves, are considerably increased.
Conversely, in the emaciated we sometimes find
beneath the skin cells which contain only one oil drop.
Many masses of fat which have an important relation
to muscular actions—such as the fat of the orbit or the
cheek, do not disappear in the most emaciated persons.
Even in starvation, the fatty substance of the brain and
spinal cord are retained.
Fat collects as pads in the hollows of the bones,
around the joints and between the muscles, causing them
to glide more easily upon each other. As marrow, it
nourishes the skeleton, and also distributes the shock of
any jar the limb may sustain.
Fat does not gather within the cranium, the lungs
[57]
or the eyelids, where its accumulation would clog the
organs.
Mucous Membranes.
—Mucous membranes line all the
open cavities of the body, or all those cavities which communicate
with the outside.
At the edges of the openings into the body, the skin
seems to stop and give place to a tissue which is redder,
more sensitive, more liable to bleed, and is moistened by
a fluid or mucous, as it is called. Really, however, the
skin does not cease, but passes into a more delicate covering
of the same general structure, and it is to this
that the name mucous membrane is applied.
The entire alimentary canal, the entire respiratory
tract, and the genito-urinary tract, are lined with a mucous
membrane. Mucous membrane secretes a mucous
fluid.
Serous Membranes.
—Serous membranes line the closed
cavities of the body. The pleurae, the pericardium
and the peritoneum are examples of serous membranes.
Serous membranes secrete a serous fluid.
Synovial Membranes.
—Synovial membranes are serous
in character, and consist of loose connective tissue,
containing fat, vessels and nerves, its inner surface being
usually lined with secreting cells. The fluid secreted is
yellowish-white or slightly reddish, resembling very much
the white of an egg. It contains fats, salts, albumen,
extractives from the lymph, and a fluid known as synovia.
The chief function of this fluid is to act as an oil
to lubricate the joints and surfaces in which there is any
friction.
[58]
Synovial membranes are divided into three classes,
known as articular, bursal and vaginal.
Articular synovial membranes are found in every
free movable joint.
Bursal synovial membranes are sacs interposed between
the surfaces which move upon each other, producing
friction, as in the gliding of a tendon or of the
integument over projecting bony surfaces.
Vaginal synovial membranes serve to facilitate the
gliding of a tendon in the bony canal through which it
passes.
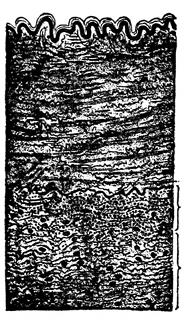
Fig. 8—Section of
artery. (Grunstein)
Arteries.
—The arteries are cylindrical vessels which
serve to convey the blood from both ventricles of the
heart to every part of the body. They are called arteries
from the Greek words which mean
“to contain air,” and they were supposed,
by our ancients, to have this
function until the time of Galen, when
he refuted this opinion and showed that
these vessels, though for the most part
empty after death, actually contained
blood. The distribution of the arteries
may be compared to a tree, the common
trunk of which corresponds to the aorta,
and the smallest twigs corresponding
to the minute capillaries. When
one artery communicates with another
it is said to anastomose, and
this communication is very free between
the larger as between the smaller branches.
[59]
Anastomosis between trunks of equal size is found where
great activity of the circulation is requisite, as at the
base of the brain, where the two vertebrals unite to
form the basilar artery.
In the limbs and arms the anastomoses are more numerous
and of larger size around the joints. The branches
of the artery above, unite with branches, from the vessels
below. These anastomoses are called collateral circulations.
The principal ones of interest to the embalmer
are those of the deep brachial uniting with the
recurrent radial and ulnar arteries, forming the collateral
circulation in the arm; the deep femoral uniting
with the recurrent posterior and anterior tibials, forming
the collateral circulation in the leg; the superficial
and deep mammary arteries, branches of the subclavian
artery uniting with the superficial and deep epigastric
arteries, branches of the external iliac, forming the collateral
circulation over the abdomen and chest, and may
be considered the longest collateral circulation in the
body.
A terminal artery is one which forms no anastomoses;
such vessels are found in the heart, brain, spleen, kidneys,
lungs and mesentery.
Structure.—An artery consists of an internal, a middle
and an external coat.
The inner coat consists of endothelial cells and elastic
fibrous tissue, sometimes arranged longitudinally, but
usually they form a distinct fenestrated membrane (similar
to a doorscreen).
[60]
The middle coat consists mostly of elastic tissue and
white fibrous tissue.
The external coat is called the fibrous coat. It contains
fibrous connective tissue and elastic tissues.
Vasa-Vasorum.—Running in the outer wall of the
artery, we find small capillary vessels, and their function
is that of nourishing the outer wall, for the blood
which passes through the artery does not nourish the
artery from within, but depends on these small capillaries,
called vasa-vasorum, for their nutrition.
The individual sheath, or arterial sheath, the covering
for the artery, is composed of connective tissue, and
at places may adhere very tightly to the artery.
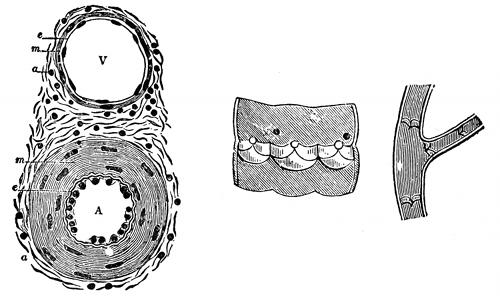
Fig. 9—Valves of the veins.
Fig. 10—Cross section through a small artery
and vein. (Klein and Noble Smith)
Veins.
—The veins are the vessels which carry the
blood from the capillaries back to the right auricle of
the heart, and are found in nearly every tissue of the
body. They commence as venous capillaries, uniting
together into larger and larger veins, until we have the
[61]
great ascending and descending venae cavae. In form the
veins are perfectly cylindrical, like the arteries, but with
this difference, that their walls collapse when empty and
that they contain valves.
Structure.—The vein has about the same structure
as the artery, only that the middle coat is much thinner
and less elastic than the artery, and for this reason it
easily collapses.
Veins are divided into superficial, deep and sinuses.
Superficial veins are found between the layers of the
superficial fascia, just underneath the skin.
Deep veins accompany the arteries, and are usually
enclosed in the same common sheath with the artery.
Sinuses are venous channels, which in their structure
and mode of distribution differ altogether from the veins.
They are found only in the interior of the skull, and consist
of channels formed by a separation of the two layers
of the dura mater.

Fig. 11—Human blood.
Blood.
—The blood of the body is
contained in a practically closed system
of tubes, the blood vessels, within
which it is kept circulating by force
of the heart beat. It is usually spoken
of as the nutritive liquid of the body,
but the functions may be stated explicitly,
although still in quite general
terms, by saying that it carries to the
tissues food stuffs after they have been
properly prepared by the digestive organs; that it transports
to the tissues oxygen, absorbed from the air by the
[62]
lungs; that it carries from the tissues various waste products
formed in the processes of dissimilation; that it is
the medium for the transmission of the internal secretion
of certain glands; that it aids in equalizing the temperature
and water contents of the body.
The total quantity of blood in the body has been determined
approximately for man as one-thirteenth of the
body weight. The specific gravity of human blood in
the adult may vary from 1.041 to 1.067, the average being
about 1.055.
The blood is composed of a liquid part, the plasma,
in which float a vast number of microscopical bodies, the
blood corpuscles, known respectively as the red corpuscles,
the white corpuscles or leucocytes, of which in turn
there are a great many different kinds, and the blood
plates.
Blood plasma, when obtained free from corpuscles, is
perfectly colorless, in thin layers, for example, in microscopical
preparation; when seen in large quantities it
shows a slightly yellowish tint. The red color of the
blood is not due, therefore, to coloration of the blood
plasma, but is caused by the mass of red corpuscles held
in suspension in the liquid. The proportion by bulk of
plasma to corpuscles is usually given roughly as two to
one. The blood plasma is composed of two substances,
blood serum and blood fibrin. You have noticed that
blood, after it has escaped from the vessels, usually clots
or coagulates. The clot, as it forms, gradually shrinks
and squeezes out a clear liquid, to which the name blood
serum has been given. Serum resembles the plasma of
[63]
normal blood in general appearance, but differs from it
in composition. Here it is sufficient to say that blood
serum is the liquid part of the blood after coagulation
has taken place. You can prepare this experiment for
yourself: If shed blood is whipped vigorously with a rod
or some similar object while it is clotting, the essential
part of the clot, namely the fibrin, forms differently from
what it does when the blood is allowed to coagulate
quietly. It is deposited in shreds on the whipper. Blood
that has been treated in this way is known as defibrinated
blood. It consists of blood serum plus the red and
white corpuscles, and as far as appearances go it resembles
exactly the normal blood; it has lost, however, its
power of clotting.
Red blood corpuscles are bi-concave, circular disks,
without nuclei; their average diameter is 7.7 microns (1
micron equals 1-25,000 of an inch); their number, which
is usually reckoned as so many to a cu. millimeter, varies
greatly under different conditions of health and disease.
The average number is given as 5,600,000 per cubic millimeter
for males and 4,500,000 per cubic millimeter for
females.
The number of red corpuscles also varies in individuals
with the constitution, nutrition and manner of life.
It varies with age, being greatest in the fetus and in
the new-born child. It varies with the time of the day,
showing a distinct diminution after meals. In the female
it varies somewhat with menstruation and pregnancy,
being slightly increased in the former and diminished in
the latter condition.
[64]
The red color of the corpuscles is due to the presence
in them of a pigment, known as hemoglobin. Owing to
the minute size of the corpuscles, their color when seen
singly under the microscope is a faint yellowish red, but
when seen in mass they exhibit the well-known blood-red
color, which varies from a scarlet in arterial blood to a
purplish red in venous blood, this variation in color being
dependent upon the amount of oxygen contained in
the blood in combination with the hemoglobin. The
function of the red blood corpuscles is to carry oxygen
from the lungs to the tissues. This function is entirely
dependent upon the presence of hemoglobins, which have
the power of combining easily with the oxygen gas.
White blood corpuscles or leucocytes contain no hemoglobin
or coloring matter. They have a nucleus or center
spot. Their size varies from 5 to 12 microns, and are
less numerous than the red corpuscles, being in this proportion:
one white corpuscle to 500 red corpuscles. The
chief functions of the white corpuscles are: (1) That they
protect the body from pathogenic or disease-producing
bacteria. In explanation of this action it has been suggested
that they may either ingest the bacteria and thus
destroy them directly, or they may form certain substances,
defensive proteids, that destroy the bacteria.
White corpuscles that act by ingesting the bacteria are
spoken of as phagocytes (meaning to eat the cell). (2)
They aid in the absorption of fats from the intestines.
(3) They aid in the absorption of peptones from the intestines.
(4) They take part in the process of blood
coagulation. (5) They help in maintaining the normal
composition of the blood plasma in proteids.
[65]
Blood plates are small circular or elliptical bodies,
nearly homogeneous in structure, variable in size, always
much smaller than the red blood corpuscles. Less is
known of their origin, fate and functions than in the
case of the other blood corpuscles, but there is some considerable
evidence to show that they take part in the
process of coagulation or clotting.
Coagulation of the Blood.—One of the most striking
properties of the blood is its power of clotting, or coagulating,
shortly after it leaves the blood-vessels, or if
any foreign elements come in contact with it. The general
changes in the blood during this process are easily
followed. At first perfectly fluid, in a few minutes it
becomes viscous, and then sets into a soft jelly, which
quickly becomes firmer, so that the vessel containing it
can be inverted without spilling the blood. The clot continues
to grow more impact, and gradually shrinks in
volume, pressing out a greater or smaller amount of
clear, faintly yellow liquid, to which the name blood serum
is given. The essential part of the clot is the fibrin.
Fibrin is an insoluble proteid not found in normal
blood. In shed blood, and under certain conditions while
still in the blood-vessels, this fibrin is formed. In forming,
it shows an exceedingly fine network of delicate
threads that permeate the whole mass of the blood and
gives the clot its jelly-like character. The shrinking of
the threads causes the subsequent contraction of the
clot. If the blood has not been disturbed during the
act of clotting, the red corpuscles are caught in the fine
fibrin mesh-work, and as the clot shrinks these corpuscles
[66]
are held more firmly, only the clear liquid of the blood
being squeezed out, so it is possible to get specimens of
serum containing few or no red blood corpuscles. The
white corpuscles or leucocytes, on the contrary, although
they are also caught at first in the forming meshes of
fibrin, in latter stages of the clotting they readily pass
out into the serum, on account of their power of having
movement. If the blood has been agitated during the
process of clotting, the delicate net work will be broken
in places, and the serum will be more or less bloody—that
is, it will contain numerous red blood corpuscles. If
during the time of clotting the blood is vigorously whipped
with a bundle of fine rods, all the fibrin is deposited
as a stringy mass on the whipper, and the remaining liquid
part consists of serum plus red corpuscles. Blood
that has been whipped in this way is known as defibrinated
blood. It resembles normal blood in appearance,
but is different in composition; it can not clot again. The
way in which fibrin is normally deposited can be easily
demonstrated by taking a drop of blood on a slide and
covering it with a cover slip, allow it to stand several
minutes until coagulation is complete, and view under a
microscope. If the drop is examined, it is possible by
careful focusing, to discover in the spaces between the
masses of corpuscles many examples of delicate fibrin
net work. The physiological value of the clotting of blood
in life is that it stops hemorrhages by closing the openings
of the wounded blood vessels, but the clotting of the
blood after death, is to the embalmer one of the bugbears,
and a real method of preventing it, or of dissolving
[67]
the clot after it has once formed in the blood vessels is
one of those difficult problems which remains as yet unsolved.
Since we have no real method of preventing coagulation
in the blood vessels, let us search out the things
which will hasten or retard this coagulation. Blood
coagulates normally within a few minutes after it is
liberated from the blood vessel, but this process may
be hastened by increasing the amount of foreign substance
with which it comes in contact. Thus the agitation
of the liquid in quantity or the application of a
sponge or handkerchief or the application of heat hastens
the onset of clotting.
Coagulation in drawn blood may be retarded or prevented
altogether by a variety of means, of which the
following are the most important:
(1) By cooling.
(2) By the action of neutral salts.
(3) By the action of oxalate solutions.
(4) By the action of sodium fluoride.
Summary.—To summarize then, the following statements
may be made:
(1) The immediate factor necessary to the clotting
of the blood is the fibrin.
(2) That blood does not clot normally in the blood
vessels before death.
(3) That after death blood remains for a long time
without clotting, provided some outside agent is not
introduced to cause it.
Such an agent may be the blood coming in contact
with the air, or the blood drainage tube. The one point
[68]
then to be emphasized is that when a vein is cut, and the
blood begins to flow, you know that the blood is not in a
coagulated condition. Then work rapidly, put the blood
drainage tube quickly into the vein and draw off as much
blood as you can before it begins to clot at the end of
the tube. The great trouble has been, that the embalmer
does not work with precision. He first raises the vein,
and exposes it on the surface of the incision. He then
raises the artery. He places the drainage tube into the
vein, but shuts it off till he is ready with the artery.
Now, by the time he has placed the arterial tube in the
artery, injected a few bulbs full to see that all is in
working order, and has perhaps attended to a few other
duties, he is amazed to find that the blood will not flow,
that it has clotted. What is the reason? He gave it
time to clot after the drainage tube was inserted.
A better procedure would be not to touch the vein
until every other procedure has been attended to. Then
raise the vein, insert the drainage tube and withdraw
the blood quickly, and at the same time keep injecting
slowly into the arterial system to keep up the needed
pressure to keep the blood flowing.
(4) That when a clot is once formed in a blood vessel,
it is not dissolved by the addition of fluid or any other
solution.
(5) That sometimes when the blood has become
clotted at the end of the drainage tube, it can be loosened
up or be slightly pushed away by attaching the pump
to the drainage tube and injecting a few bulbs of fluid,
which, when it runs out, will again start the flow of
blood.
[69]
CHAPTER V.
OSTEOLOGY.
Definition.
—Osteology is the science of the structure
and functions of bones.
In regard to the treatment of this subject, it is not
our aim to take up all the minute details concerning each
bone, all we desire is to explain the form, uses and location
of some of the principle bones and sets of bones
of the body in so far as they may come to be used as
landmarks for the embalmer.
The Skeleton.
—The entire skeleton in the adult consists
of 200 distinct bones.
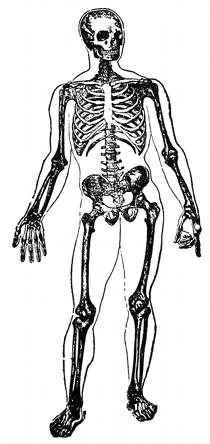
Fig. 12—The Skeleton.
[70]
| Spine— |
| | Cervical | 7 |
| | Dorsal | 12 |
| | Lumbar | 5 |
| | Coccygeal | 1 |
| | Sacral | 1 |
| | | 26 | | 26 |
| Cranium | | | | 8 |
| Face | | | | 14 |
| Hyoid | | | | 1 |
| Sternum | | | | 1 |
| Ribs— |
| | True | 7 | Pair |
| | False | 3 | “ |
| | Floating | 2 | “ |
| | | 12 | “ | 24 |
| Upper Extremities | | | 64 |
| Lower Extremities | | | 62 |
| | | | | 200 |
In the above outline the bones of the ear and the
sesamoid bones are not considered. Different anatomists
make different computations as to the number of bones
in the skeleton. Some authorities add the bones of the
ear, thus making 206 in all. If all the little sesamoid
bones were added, the number could be greatly augmented.
[71]
The Vertebral or Spinal Column. (The Spine).
—The
spine is a flexuous and flexible column formed of a series
of bones called vertebrae. There are twenty-six in number
and may be divided as follows:
| Cervical | 7 | bones |
| Dorsal | 12 | “ |
| Lumbar | 5 | “ |
| Sacral | 1 | “ |
| Coccygeal | 1 | “ |

Fig. 13—The Spine.
The cervical vertebrae are smaller
than those in any other region of the
spine, and may be readily distinguished
as they lie in the neck and extend from
the base of the skull to the dorsal vertebrae,
or the point of attachment of
the first rib to the first dorsal.
The dorsal or thoracic vertebrae are
the next in rotation down the spine and
are intermediate in size between those
in the cervical and those in the lumbar
region, and increase in size from above
downward.
The lumbar vertebrae, the next in
rotation, are the largest of the vertebral
column and can be distinguished
as those lying in the lumbar region or
the small of the back.
The sacrum, meaning sacred, so
called, because it was the part selected
in sacrifices. The sacrum is a large
[72]
triangular bone, situated at the lower part of the vertebral
column, and at the upper and back part of the pelvic
cavity.
The coccyx, so called from having been compared to
a cuckoo's beak. It is usually formed of four small segments
of bones, and gradually diminish in size from above
downward, and blend together so as to form a single
bone.
The spinal column is situated in the median line,
at the posterior part of the trunk. Its average length
is about two feet, two or three inches. The female spine
is about one inch shorter than the male.
The spinal canal in which runs the spinal cord, follows
the different curves of the spine; the opening being
the largest in those regions in which the spine enjoys the
greatest freedom of movement, and the smallest where
motion is more limited.
The Skull.
—The skull is the bony framework of the
head. The cranium is the name applied when we do
not consider the mandible (the lower jaw).
The skull is oval in shape, wider behind than in front,
and is supported on the summit of the vertebral column.
The skull is composed of twenty-two bones and is
divided as the following diagram will show:
[73]

Fig. 14—The Skull.
| | Cranium | Occipital |
| | Two parietal |
| | Frontal |
| Skull | Two temporal |
| Sphenoid |
| Ethmoid |
| |
| | Two inferior turbinate |
| | Two nasal |
| | Two superior maxillary |
| Face | Two lachrymal |
| | Two malar |
| | | Two palate |
| | | Inferior maxillary |
| | | Vomer |
[74]
The Bones of the Cranium.
—Occipital Bone.—The
occipital bone is situated at the back part and base of
the cranium.
Frontal Bone.—The frontal bone is situated at the
anterior part of the cranium, and forms the forehead.
Parietal Bones.—The parietal bones, two in number,
form, by their union, the sides and roof of the cranium.
They are between the frontal and the occipital bones.
Temporal Bones.—The temporal bones, two in number,
are situated at the sides and base of the skull.
Sphenoid Bone.—The sphenoid bone is situated at
the anterior part of the base of the skull articulating with
all the other cranial bones.
Ethmoid Bone.—The ethmoid is an exceedingly light,
spongy bone, which is situated at the anterior part of
the base of the cranium.
The Bones of the Face.
—Nasal Bone.—The nasal
bones, two in number, are placed side by side at the middle
and upper part of the face, forming, by their junction,
“the bridge” of the nose.
Superior Maxillary Bones.—The superior maxillae,
two in number, are the largest bones of the face, excepting
the lower jaw, and form by their junction, the upper
jaw.
Inferior Maxillary Bone.—The inferior maxillary
bone is also called the mandible. This bone is the largest
and strongest bone of the face. In a great many cases
after death this bone drops down, and it becomes one
of the first duties of the embalmer, to place this bone
in the proper position, so that it will set with the gradual
[75]
death stiffening. If the lower jaw has already set, in
proper position, it is best not to break up the rigor, because,
once broken up, it will be hard to set it in proper
condition again without the use of stitches.
The upper and lower jaws are the fundamental bones
for mastication.
Lachrymal Bones.—The lachrymal bones, two in number,
are the smallest and most fragile bones of the face.
They are situated at the front part of the inner wall of
the orbit of the eye.
Malar Bones.—These are the cheek bones. There are
two in number, situated at the upper and outer part of
the face.
Palate Bones.—The palate bones, two in number are
situated at the back part of the nasal fossae. Each bone
assists in the formation of three cavities: the floor and
the outer wall of the nose, the roof of the mouth, and
the floor of the orbit.
Inferior Turbinated Bones.—The inferior turbinated
bones are situated one on each side of the outer wall of
the nasal fossae.
Vomer.—The vomer, a single bone, is situated vertically
at the back part of the nasal fossae, forming part
of the septum of the nose. It is thin and somewhat like
a ploughshare in form.
The Hyoid Bone.
—The hyoid bone is named from its
resemblance to the Greek letter U. It is also called the
lingual bone, because it supports the tongue and gives
attachment to its numerous muscles.
The omo-hyoid muscle, which crosses the carotid
[76]
artery at its middle third, has its insertion with the hyoid
bone.
The Bones of the Thorax.
—The Sternum or Breast
Bone.—The sternum is a flat, narrow bone, situated in the
median line of the front of the chest. The lower end is
called the ensiform process, to which the diaphragm has
its anterior attachment.
The Ribs.—The ribs, which are curved arches of bone,
form the chief part of the thoracic walls. There are
twelve in number on each side, although this number
may vary.
The ribs are divided into seven pairs of true ribs,
three pairs of false ribs, and two pairs of floating ribs, as
the following outline will show:
- Ribs
- 7 true
- 3 false
- 2 floating
- —
- 12 pairs in all.
The true ribs are connected behind to the spine and
in front to the sternum.
The false ribs are connected behind to the spine, but
are called false because they are not attached directly to
the sternum, but indirectly, the cartilages attaching to
the cartilage of the rib next above.
The floating ribs are so named because they are only
attached at one place, which is the spine and are loose
or float in front.
[77]
The Bones of the Upper Extremities.
—The Shoulder
girdle consists of the clavicle and scapula.
The Clavicle.—The clavicle or key bone, so-called because
of its supposed resemblance to the key used by the
Romans, forms the anterior portion of the shoulder girdle.
It is often commonly called the collar bone.
The Scapula.—The scapula comes from a Greek word
meaning “a spade.” It forms the back part of the shoulder
girdle.
The arm is that portion of the upper extremity which
is situated between the shoulder and the elbow.
The Humerus.—This is the largest and strongest
bone of the upper extremity and is found in the arm between
the shoulder and the elbow. It is the only bone
in the arm.
The fore arm is that portion of the upper extremity
which is situated between the elbow and the wrist. The
fore arm has two bones, the ulna and the radius.
The Ulna.—A long thin bone, but larger than the
radius, and situated on the inside of the fore arm.
The Radius.—So-called because it is the rotary bone
of the fore arm. It is situated on the outside of the fore
arm and parallel with the ulna.
The hand is subdivided into the wrist or carpus
bones, the metacarpus or the bones of the palm, and the
phalanges or the bones of the digits. There are twenty-seven
bones in each hand.
The Bones of the Lower Extremities.
—The bones of
the lower extremities consist of the pelvic girdle, the
thigh, the leg and the foot.
[78]
The pelvic girdle consists of three portions, the
ilium, the pubis, and the ischium.
The Ilium.—The ilium is the superior, broad and expanded
portion and forms the prominence of the hip.
The top part is called the crest.
The Ischium.—The ischium is the lowest portion of
the girdle, and is the portion which supports the body
when in a sitting position.
The Pubis.—This bone forms the front of the pelvis,
and supports the external organs of generation.
The thigh is that portion of the lower extremity which
is situated between the pelvis and the knee. It consists
of a single bone called the femur.
The Femur.—The femur is the largest, longest and
strongest bone in the skeleton. It is almost perfectly
cylindrical. It extends from the hip to the knee.
The bones of the leg are three in number and are as
follows: patella, tibia, and fibula.
The Patella.—This bone is often called the knee cap
or the knee pan. It is a flat triangular bone, situated at
the anterior part of the knee joint.
The Tibia.—The tibia is situated at the front and inner
side of the leg, and is next to the femur in strength
and size. It is sometimes called the shin bone.
The Fibula.—The fibula is sometimes called the calf
bone. It is situated at the outer side of the leg, and is a
quite slender bone.
The foot is divided into the tarsus, metatarsus, and
the phalanges. There are seven tarsus bones, five metatarsus
bones, and fourteen phalanges bones, making a total
of twenty-six bones for each foot.
[79]
CHAPTER VI.
ORGANOLOGY.
The body itself is divided into the upper and the
lower extremities and the trunk. The upper extremities
consist of the head and arms. The lower extremities
consist of the legs. The trunk is that part of the body
remaining after the head, arms, and legs have been
severed from the body.
The Cavities.
—The body has three principal cavities:
namely, the cerebro-spinal, the thoracic, and the abdominal.
The Cerebro-Spinal Cavity.
—The cerebro-spinal cavity
is formed by the cranial bones, and the vertebral column.
The cerebro-spinal cavity is divided into the sub-cavities,
called the cranial cavity and the spinal cavity.
In the cranial cavity we find the brain. The brain
is the seat of the mind, and the functions which the
brain performs distinguishes man from the other animals,
as man becomes a conscious, intelligent, responsible being
through the action of the brain. The brain is egg-shaped,
soft and yielding, closely fitting the cranial cavity.
The front and top of the brain is called the cerebrum,
which is the center for intelligence, reason, and will. This
part of the brain is convoluted, and the depth of the
convolutions to a great extent indicates the amount of
intelligence.
[80]
Below the cerebrum and lying in front of the occipital
bone, we find the cerebellum, which is the seat of
memory and the center for the co-ordination of muscle
movements. By co-ordination of muscle movement is
meant that the muscles will do just what we want them
to do, that they will act harmoniously, the one with the
other. The condition of Saint Vitus' Dance would be an
example showing a lack of co-ordination. This part of
the brain is also convoluted.

Fig. 15—Brain and spinal
cord.
Between the cerebrum and the
cerebellum, and connecting the
two, is found the pons Varolii.
The word pons means bridge, and
the word Varolii means to cross
over. It is in this part of the
brain, then, that the nerve fibers
cross over to the opposite side.
A person having a paralytic stroke
on the right side of the body
would indicate that the left side
of the brain had become affected.
Joined to this is the medulla oblongata.
This is the lowest part
of the brain and is the connecting
link between the brain and the
spinal cord. The medulla controls
the circulation, respiration, and
deglutition (swallowing).
Closely adhering to the brain, is a delicate membrane,
sinking into the convolutions, and following the surface
of the brain valleys throughout. This membrane is called
[81]
the pia mater. In it is found the capillaries, which supply
the brain with its nutritive blood in life and with embalming
fluid after death. These capillaries do not penetrate
the substance of the brain, but the process is one
of osmosis, absorption or transfusion. Covering the outer
most part of the brain, and closely adhering to the cranial
bones is a dense, tough, glistening, membrane, called the
dura mater. In the dura mater is found the sinuses of
the brain.
In between the pia mater and the dura mater is a delicate
double membrane forming a closed sack, called the
arachnoid membrane. This sac contains a serous fluid,
which offers great protection to the brain. These same
three membranes also cover the spinal cord, and are
called all together the meninges of the brain and cord.
The brain is composed of white and gray matter. The
gray matter is on the outside, and the white matter is on
the inside.
The spinal cavity is formed by the bones of the vertebral
column. In this spinal cavity is found the spinal
cord. It is cylindrical and usually about seventeen inches
in length, and extends from the medulla oblongata, to
the lower border of the first lumbar vertebra, where it
terminates in a slender filament of gray substance.
There originate from the under surface of the brain
twelve pairs of nerves, as follows:
- 1. Olfactory
- 2. Optic
- 3. Motor Oculi
- 4. Trochlear
- [82]
- 5. Trigeminal
- 6. Abducens
- 7. Facial
- 8. Auditory
- 9. Glosso-pharyngeal
- 10. Pneumogastric
- 11. Spinal accessory
- 12. Hypoglossal
There originate from the cord thirty-one pairs of
nerves, as follows:
| Cervical region | 8 | pairs. |
| Thoracic region | 12 | “ |
| Lumbar region | 5 | “ |
| Sacral region | 5 | “ |
| Coccygeal region | 1 | “ |
| | — | |
| | 31 | “ |
The circulation of the blood through the brain will be
taken up later.
[83]
CHAPTER VII.
ORGANOLOGY.—Continued.
The Thoracic Cavity.
—The thorax, or chest is a bony,
cartilaginous cage. It contains and protects the principle
organs of respiration and circulation.
The thorax is bounded in front by the sternum and
costal cartilages, behind by the twelve dorsal vertebrae
and the posterior parts of the ribs, on the sides by the
ribs, above by the root of the neck and below by the
diaphragm.
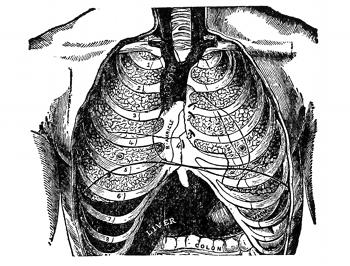
Fig. 16—Front view of the thorax. (Gray)
In the female the thorax differs as follows from the
male: Its general capacity is less, the sternum is shorter,
and the upper ribs are more movable and so allow a
greater enlargement of the upper part of the thorax than
the male.
[84]
The capacity of the cavity of the thorax does not correspond
with its apparent size externally, because, (1)
the space enclosed by the lower ribs is occupied by some
of the abdominal viscera; and (2) the cavity extends
above the first rib into the neck. The size of the cavity
of the thorax is constantly varying during life, with
the movements of the ribs and diaphragm, and with the
degree of distention of the abdominal viscera.
From the collapsed state of the lungs, as seen when
the thorax is opened, in the dead body, it would appear
as if the viscera only partly filled the cavity of the thorax,
but during life there is no vacant space, that which is
seen after death being filled up during life by the expanded
lungs.
Larynx.
—The larynx is the organ of voice, placed at
the upper part of the air passage. It is situated between
the trachea and the base of the tongue, at the upper and
forepart of the neck, where it forms a considerable projection
in the middle line. It is for this reason that
it is of considerable importance to embalmers, for it is
just opposite this projection, on either side of the neck,
that the common carotid divides into the internal and
the external carotid.
On either side of it lie the great blood vessels of the
neck, behind it forms a part of the boundary of the
pharynx, and is covered by the mucous membrane lining
that cavity.
Its vertical extent corresponds to the fourth, fifth,
and sixth cervical vertebrae. It is placed somewhat
higher in the female than in the male.
[85]
The movements of the head affect the position of the
larynx. When the head is drawn back, the larynx is
lifted, and when the chin approaches the chest the larynx
is depressed. During swallowing the larynx moves distinctly;
during singing it moves slightly.
Until puberty there is no marked difference between
the larynx of the male and that of the female. In the
male after puberty all the cartilages increase in size,
and the larynx becomes prominent as the Adam's apple
in the middle line of the neck. In the female after
puberty the increase of size is only slight.
The larynx is broad above, where it presents a triangular
appearance, flattened behind and at the sides.
Below it is narrow and cylindrical.
It is composed of cartilages which are connected
together by ligaments and moved by numerous muscles.
It is lined by a mucous membrane which is continuous
above with the lining of the pharynx and below with
that of the trachea.
The arteries that supply the larynx are the laryngeal
arteries, branches of the superior and inferior thyroid
arteries.
The superior laryngeal vein runs into the superior
thyroid vein and then into the internal jugular vein,
while the inferior laryngeal vein runs into the inferior
thyroid vein and then into the innominate vein.
The Trachea.
—The trachea or windpipe is a cartilaginous
elastic, cylindrical tube, flattened posteriorly. It
extends from the lower part of the larynx, on a level
with the sixth cervical vertebra to opposite the body of
[86]
the fourth dorsal, where it divides into two bronchi, one
for each lung.
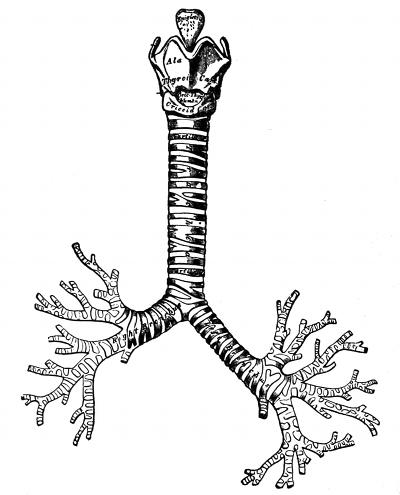
Fig. 17—The cartilages of the larynx; the trachea and
bronchi. (Gray)
The trachea is in the median line of the body. It
measures about four and one-half inches in length. The
diameter is from three quarters to one inch, being always
greater in the male than in the female.
The trachea is composed of imperfect cartilage rings,
not coming quite together in the back.
[87]
The artery that supplies the trachea is the inferior
thyroid artery.
The vein that withdraws the blood is the inferior
thyroid vein.
The Right Bronchus.—The right bronchus is shorter,
and wider than the left bronchus. It is about one inch
in length. It enters the lung opposite the fifth dorsal
vertebra.
The Left Bronchus.—The left bronchus is smaller and
longer than the right. It is two inches in length and
enters the lung at a point opposite the body of the sixth
dorsal vertebra.
Each bronchus divides into smaller divisions called
bronchial tubes.
Each bronchial tube divides into still smaller divisions
called bronchioles.
Each bronchiole ends in the air cell.
The Pleurae.
—Each lung is invested upon its external
surface by an exceedingly delicate serous membrane, the
pleura. This encloses the organ as far as its root, and
is then reflected upon the inner surface of the thorax.
The pulmonary pleura is the portion investing the
surface of the lung, and dipping into the fissures between
its lobes.
The parietal pleura is that which lines the inner
surface of the chest.
The space between these two layers is called the
cavity of the pleurae, (the pleural cavity); and contains
nothing but a very little clear fluid.
In the healthy condition the two layers are in contact
[88]
and there is no real cavity, but after death the lungs
become collapsed and separate from the walls of the
chest. Each pleura is therefore a shut sac, one occupying
the right, and the other the left half of the thorax,
and they are perfectly separated from one another. The
two pleurae do not meet in the middle line of the chest,
excepting for a short distance between the second and
third pieces of the sternum—a space being left between
them, which contains all the viscera of the thorax excepting
the lungs; this is called the mediastinum.
The mediastinum then, is the space between the right
and left pleural sacs.
The arteries of the pleura are derived from the intercostal,
internal mammary, musculo-phrenic, thymic, pericardiac,
bronchial.
The veins correspond to the arteries.
The Lungs.
—The lungs are the essential organs of
respiration. They are two in number, placed one on
each side of the chest, separated from each other by the
heart and the contents of the mediastinum. A healthy
lung hangs free within the pulmonary space. The lung
is suspended by the root. The root of the lung is formed
by the bronchial tubes, pulmonary artery, pulmonary
veins, bronchial arteries, bronchial veins, etc., all of which
are enclosed by the reflections of the pleurae.
The root of the lung may be described as being that
part where all the great blood vessels and the bronchial
tubes, enter the lungs.
In many cases the lung does not hang free, but as a
[89]
result of former pleurisy, the area of the pulmonary
pleura is adherent to the parietal pleura.
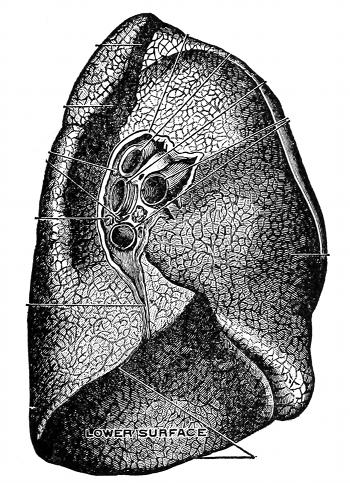
Fig. 18—The root of the left lung. (Toldt)
Each lung is conical in shape, and presents for examination,
an apex, a base, and two surfaces.
The Apex forms a tapering cone which extends into
the root of the neck about an inch and a half to two
inches above the level of the top of the first rib.
The Base is broad and concave and rests upon the
convex surface of the diaphragm, which separates the
[90]
right lung from the upper surface of the right lobe of
the liver and the left lung from the upper surface of the
left lobe of the liver, the stomach, and spleen.
Surfaces.—There are two in number. The external,
costal or thoracic surface is smooth, convex and corresponds
to the form of the cavity of the chest. The inner
or mediastinal surface is concave, and the middle portion,
where all the vessels enter and leave the lung is
called the root.
Lobes.—Each lung is divided up into lobes. The right
lung has three lobes, and the left lung has two lobes.
Weight.—The weight of both lungs together is about
42 ounces, the right lung being a little heavier than the
left. The lungs are heavier in the male than in the female.
The male lungs weigh from 42 to 45 ounces, and
the female lungs weigh from 32 to 35 ounces.
Color.—The color of the lungs at birth is a pinkish
white, in adult life a dark slate color, mottled in patches
and as age advances this mottling assumes a black color.
Substance.—The substance of the lung is of a light
porous, spongy texture. It floats in water, if it has once
been filled with air. It is elastic and for this reason we
always find the lung collapsed after death.
The structure of the lung is such that the blood
brought by the pulmonary artery comes into close relation
with the air in the air-cells which enters from the
bronchioles. The blood gives off carbon dioxide to the
air-cells and the air in the cells furnishes oxygen for the
blood. The process of respiration causes the dark blood
[91]
brought from the heart by the pulmonary arteries to return
to the heart as red blood in the pulmonary veins.
Arteries.—The bronchial arteries supply the lungs
with nutrition.
The pulmonary arteries convey venous blood from
the heart to the lungs to be purified.
Veins.—The bronchial veins carry off the impure
blood from the lungs.
The pulmonary veins convey the blood which has been
purified by the lungs, back to the heart.
—The mediastinum is the space left
in the middle portion of the chest by the non-approximation
of the two pleurae. It extends from the sternum
in front to the spine behind.
Within it are the contents of the thorax, excepting
the lungs. The mediastinum may be divided into two
parts.
The superior mediastinum is that portion of the interpleural
space which lies above the level of the pericardium.
This space contains the arch of the aorta, innominate,
part of the left carotid artery, part of the left
subclavian artery, the upper half of the superior vena
cava, the upper half of the innominate vein, the left
superior intercostal vein, trachea, esophagus, thoracic
duct, remains of the thymus gland, etc.
The inferior mediastinum is divided into three portions:
The anterior mediastinum is that portion in front
of the pericardium. It contains nothing but some loose
areolar tissue.
[92]
The posterior mediastinum is that portion back
of the pericardium. It contains the descending thoracic
aorta, the greater and lesser azygos veins, the esophagus,
the thoracic duct, etc.
The middle mediastinum is that part within the
pericardium or heart sac. It is the largest space of all
the mediastinal spaces. It contains the heart, the ascending
aorta, the lower half of the superior vena cava, the
vena azygos, the bifurcation of the trachea, the pulmonary
artery, etc.
The middle mediastinum is sometimes called the cardiac
cavity, because it contains the heart.
The Pericardium (Heart Sac).
—The pericardium is
a serous sac in which is located the heart and the commencement
of the great blood vessels.
Behind we find the bronchi, esophagus and descending
thoracic aorta. To the sides we find the pleura, the
phrenic nerve and the accompanying vessels. In front
we find the sternum and the remains of the thymus gland.
It is attached above to the great blood vessels and below
to the diaphragm.
The Heart.
—The heart is a hollow, muscular organ
of a conical (cone shaped) form, placed between the
lungs and enclosed in the pericardium.
The heart is placed obliquely in the chest. The base
is directed upward, backward and to the right, and corresponds
to the dorsal vertebrae from the fifth to the
eighth inclusive.
The apex is directed downward, forward and to the
left and corresponds to the space between the cartilages
between the fifth and sixth ribs.
[93]
The exact location of the apex of the heart would be
¾-inch to the inner side, and an inch and one-half below
the left nipple, or about three and one-half inches from
the middle line of the sternum or breast bone.
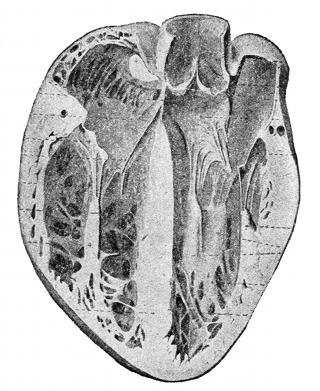
Fig. 19—A cross section of the heart showing valves. (Spalteholz)
The heart is placed behind the sternum, and extends
about three inches to the left of the median line, and
about one and one-half inches to the right, or in other
words, about one-third of the heart lies to the right of
the median line, and two-thirds lies to the left of the
median line.
The heart in the adult measures five inches in length,
three and one-half inches in breadth in its broadest part,
and two and one-half inches in thickness. The weight
[94]
of the male heart varies from ten to twelve ounces, and
that of the female from eight to ten ounces.
The capacity of the ventricles of the heart averages
about three and one-half ounces of blood to each ventricle,
and the auricle a little less than four ounces,
making the total capacity of the heart average about
fifteen ounces.
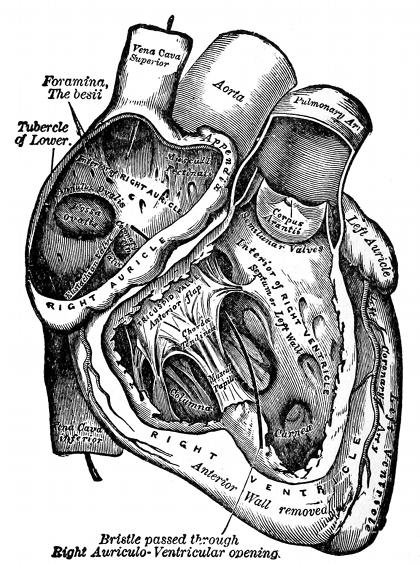
Fig. 20—The right auricle and ventricle laid open. (Gray)
The heart is divided by a muscular septum (separation
[95]
wall) into two lateral halves, which are named respectively
the right or venous side and the left or arterial
side. The septum is called the longitudinal septum.
Each side of the heart is further sub-divided into an
upper and lower compartment, the upper on each side is
called the auricle and the lower the ventricle. The
upper and lower compartments of the heart (auricles
and ventricles) are separated by the auricular-ventricular
septums (meaning a separation between the auricle
and ventricle).
The superior and inferior venae cavae empty into the
right auricle of the heart, also the blood from the coronary
sinus.
In fact, this compartment receives all the venous
or impure blood from all parts of the body, and sends
it through what is known as the tricuspid valve into
the right ventricle or lower compartment. After getting
into the right ventricle, the blood is sent forth into the
lungs by first passing through the pulmonary semi-lunar
valve into the pulmonary artery, which enters the lungs
at the root of the same.
This would then finish the circulation through the
right side of the heart, and after the purification has been
accomplished by the lungs, we find the blood being returned
to the left side of the heart through the four
pulmonary veins. The pulmonary veins extend from the
lungs (two on each side) to the left auricle (upper compartment
of the heart) and deliver the purified blood
to the left or arterial side. The course of the blood from
the left auricle is downward into the left ventricle (or
[96]
lower compartment) through what is known as the bicuspid
or mitral valve.
The blood is then sent out into the body to nourish
all the tissues, by being forced through the aortic semi-lunar
valve into the great aorta artery. The circulation
is then completed by the blood running into the branch
arteries and from them into the smaller branches and
into the capillaries from which the course of the blood
is into the smaller veins and into the larger veins, finally
terminating into the two large trunk veins, the ascending
(or inferior) and descending (or superior) venae cavae.
Of these two large trunk veins the ascending vena cava
is the only one to have a valve at its termination (eustachian).
The functions of this valve are to prevent a
backward flow of blood into the vein from the auricle.
The heart has three walls, the inner wall is called the
endocardium, the middle wall is called the myocardium,
and the outer wall is called the epicardium.
The heart is surrounded by a serous sac called the
pericardium.
The heart receives its blood supply from the coronary
arteries, which are branches of the ascending aorta, just
after it leaves the aortic semi-lunar valve.
The coronary veins bring the venous blood back from
the tissues of the heart and empty into the coronary
sinus, back of the right auricle of the heart.
The veins which originate about the region of the
right auricle, empty directly into the right auricle of
the heart through the valves of Thebesii.
The Alimentary Canal.
—The alimentary canal is a
[97]
muscular membranous tube. It is about thirty feet in
length, and extends from the mouth to the anus. It is
lined throughout by a mucous membrane.
The following outline will show the parts of the alimentary
canal:
Mouth
Pharynx
Oesophagus
Stomach |
| |
| Small Intestines | Duodenum |
| Jejunum |
| Ileum |
| |
| Large Intestines | Caecum |
| Colon |
| Rectum |
The accessory organs to the alimentary canal are the
following:
Teeth, Salivary glands, Liver, Spleen, Pancreas.
The Mouth.
—The mouth is placed at the commencement
of the alimentary canal. It is a nearly oval shaped
cavity.
In this cavity the mastication of the food and the insalivation
of the food takes place.
The Teeth.
—The structure of the teeth has been considered
under the head of tissues.
The Palate.
—The palate forms the roof of the mouth.
It consists of two portions: The hard palate is in front
and the soft palate is in the back.
[98]
The Salivary Glands.
—By the term salivary glands
is usually understood the three chief glands on each side
of the face.
The parotid gland is placed near the ear. The submaxillary
gland is placed below the jaw. The sublingual
gland is placed below the tongue.
These glands secrete the salival juices which are
brought into the mouth by three small ducts, where it
aids in the digestion of the food. The digestive action of
the saliva is limited to the starchy foods. Its action is
to change starches into sugars.
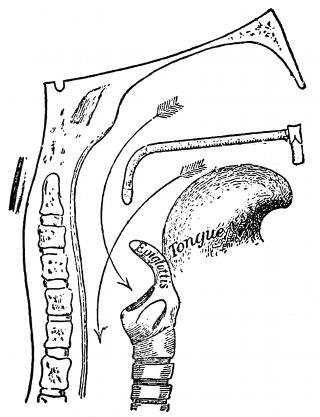
Fig. 21—Passage into trachea and
esophagus; Pharynx.
It also fulfills other important functions. By moistening
the food it enables
us to reduce the material
to a consistency suitable
for swallowing and
for manipulation by the
tongue and other muscles.
The saliva also
serves as a kind of lubricator
that insures the
smooth passage along
oesophageal canal.
The Pharynx.
—The
pharynx is that part of
the alimentary canal,
which is placed behind,
and communicates with
the nose, mouth and
[99]
larynx. It is a muscular, membranous tube which extends
from the back of the mouth and under surface of
the skull to the level of the cricoid cartilage or to a point
between the fifth and sixth cervical vertebrae.
The pharynx is about four and one-half inches in
length.
Seven openings communicate with it, as follows:
Two posterior nares, two eustachian tubes, mouth,
larynx, esophagus.
The Esophagus.
—The esophagus or gullet is a muscular
canal about nine or ten inches in length, extending
from the pharynx to the stomach.
It begins at a point between the fifth and sixth cervical
vertebrae and descends along in front of the spine
through the posterior mediastinal space, passes through
the diaphragm, and entering the abdomen, terminates in
the stomach wall at a point opposite the tenth dorsal
vertebra.
At its commencement it is placed in the median line
and gradually inclines to the left as it passes forward to
the esophageal opening to the diaphragm.
The esophagus is from one-half to an inch in diameter.
Arteries.—The arteries which supply the esophagus
are the esophageal, which are branches from the aorta.
Veins.—The esophageal veins empty into the ascending
vena cava.
The Diaphragm.
—The diaphragm (a partition wall)
is a dense, muscular, fibrous septum, placed obliquely
across the trunk. It separates the thoracic from the abdominal
[100]
cavity, forming the floor of the thoracic and the
roof of the abdominal cavity.
It is attached in front to the ensiform process of the
sternum, on the sides to the inner surface of the cartilages
and bony portions of six or seven inferior ribs, and
behind it is attached to the lumbar vertebrae.
The diaphragm has three openings, as follows: opening
for the esophagus, opening for the aorta, opening for
the ascending vena cava.
The diaphragm is the principal muscle of respiration.
The arteries which supply the diaphragm are the
phrenic arteries.
The phrenic veins receive the blood from the diaphragm.
[101]
CHAPTER VIII.
ORGANOLOGY.—Continued.
The Abdomen.
—The abdomen is the largest cavity in
the body. It is oval in form, the extremities of the oval
being directed upward and downward.
To facilitate description, the abdomen is artificially
divided into two parts:
An upper and larger part, the abdomen proper.
A lower and smaller part, the pelvis.
These two cavities are not separated from each other,
but the limit between them is a line drawn around the
brim of the true pelvis.
The abdomen proper differs from the other great cavities
of the body, in being bounded for the most part by
muscles and fascia.
It varies in capacity and shape according to the condition
of the viscera which it contains and in addition, it
varies in form and extent with age and sex.
Boundaries.—The diaphragm forms the dome over the
abdomen, the cavity of the abdomen extending high into
the bony thorax.
The lower end of the abdomen is limited by the bones
of the pelvis.
In front and at the sides it is bounded by the lower
ribs and abdominal muscles.
[102]
Behind by the vertebral column and muscles.
Regions.—For convenience of description of the viscera,
the abdomen is artificially divided into nine regions.
Thus if two circular lines are drawn around the body,
the one at the extremities of the ninth ribs where they
join the costal cartilages, and the other around the crest
of the ileum, the abdominal cavity is divided into three
zones.

Fig. 22—The regions of the abdomen and their
contents. (Gray)
If two parallel lines are now drawn perpendicular
upward from the center of Poupart's ligament, each of
these zones is subdivided into three parts.
The middle region of the upper zone is called the epigastric;
and the two lateral regions, the right and left
hypochondriac. The central region of the middle zone is
[103]
called the umbilical; and the two lateral regions, the
right and left lumbar regions. The middle region of the
lower zone is called the hypogastric; and the two lateral
regions are called the right and the left inguinal regions.
The viscera contained in each of these are as follows:
| Right Hypochondriac | Epigastric Region | Left Hypochondriac |
| The greater part of the right lobe of the liver, the hepatic flexure of the colon and part of the right kidney. | The greater part of the stomach including both cardiac and pyloric orifices, the left lobe and part of the right lobe of the liver and the gall-bladder, the pancreas, the duodenum, the suprarenal capsules and parts of the kidneys. | The fundus of the stomach, the spleen, the extremity of the pancreas, the splenic flexure of the colon and part of the left kidney and small portion of the left lobe of the liver. |
| Right Lumbar | Umbilical Region | Left Lumbar |
| Ascending colon, part of the right kidney and some convolutions of the small intestines. | The transverse colon, part of the great omentum and mesentery, transverse part of the duodenum and some convolutions of the jejunum and ileum and part of both kidneys. | Descending colon, part of the omentum, part of the left kidney and some convolutions of the small intestines. |
| Right Inguinal or Iliac | Hypogastric Region | Left Inguinal or Iliac |
| The caecum and vermiform appendix and a portion of the ascending colon. | Convolutions of the small intestines, the bladder in children and in adults if distended, and the uterus during pregnancy. | Sigmoid flexure of the colon and a portion of the descending colon. |
The Stomach.
—The stomach is the principal organ of
digestion. It is the most dilated part of the alimentary
canal, and is situated between the termination of the
esophagus and the commencement of the small intestines.
It is placed in part immediately behind the anterior wall
of the abdomen and beneath the diaphragm.
The lesser curvature of the stomach extends between
the cardiac and the pyloric orifices along the right border
of the organ.
[104]
The greater curvature of the stomach is directed
to the left, and is four or five times as long as the lesser
curvature.
The cardia is the point at which the esophagus enters
the stomach wall.
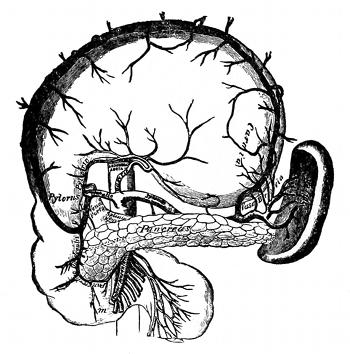
Fig. 23—The coeliac axis and its branches. (Gray)
The cardiac orifice is the opening by which the esophagus
communicates with the stomach. It is sometimes
called the esophageal opening. It is situated on a level
with the body of the tenth and eleventh dorsal vertebrae.
It is to the left of and in front of the aorta. On the anterior
surface of the body the cardiac orifice corresponds
to the articulation of the seventh left costal cartilage to
the sternum.
The pylorus is the point at which the stomach passes
into the duodenum.
[105]
The pyloric orifice is the opening by means of which
the stomach communicates with the duodenum.
This orifice is guarded by the pyloric valve. When
the stomach is empty the pylorus is situated just to the
right of the median line of the body on a level with the
upper border of the first lumbar vertebra. On the anterior
surface of the body its position would be indicated
by a point one inch below the tip of the ensiform process
and a little to the right.
The size of the stomach varies considerable in different
subjects. The distance between the two orifices is
from three to six inches. The weight of the stomach is
about four and one-half ounces.
The capacity of the adult male stomach is from five
to eight pints. The stomach of a new born child holds
about one ounce.
The stomach is held in place by the attachment of the
esophagus to the diaphragm and the fixation of the duodenum
to the front of the vertebral column.
The wall of the stomach consists of four coats: serous,
muscular, areolar, and mucous.
The glands of the stomach are of three kinds: gastric,
pyloric, and cardiac. These glands furnish the digestive
enzymes of the stomach, namely: pepsin, renin, and hydrochloric
acid.
Arteries.—The arteries that supply the stomach are
the gastric, and branches from the splenic and the hepatic.
It must be remembered that when a body is arterially
injected after death, that the fluid only goes to the stomach
walls and there ends in the capillary system. No
[106]
doubt a little of this fluid will soak through into the
inside of the stomach, and tend to preserve the contents
of the stomach, but it must be added that if the stomach
contains a considerable quantity of food and water, that
there will not be enough fluid soak through the stomach
wall to preserve the contents of the stomach and as a
result gases arise which cause distention of the abdomen
and perhaps purging from the mouth and nose. As a rule
then it is safe to say that when we have purging from the
mouth and nose, with a visible distention of the abdominal
cavity, indicating gases in the stomach and the intestines
that fluid has not reached the contents of the stomach and
the fecal matter of the intestines, and therefore it will be
necessary to introduce fluid to these parts, in order to preserve
the contents, and prevent further formation of
gases. The method for doing this will be given under
cavity embalming.
The Small Intestines.
—The small intestine is a convoluted
tube, extending from the pyloric end of the stomach
to the ileo-caecal valve where it terminates in the large intestines.
It fills up the greater part of the abdominal and
the pelvic cavity. It is about twenty feet in length and
gradually diminishes in size from the commencement to
the termination.
The small intestines are surrounded at the top and at
the sides by the large intestines. The small intestines
are held in place by the mesentery, a part of the peritoneum,
which connects or fastens to the spine.
The small intestines are divisible into three portions:
Duodenum, Jejunum, and the Ileum.
[107]
Arteries.—The main arterial supply to the small intestines
is through the superior mesenteric artery.
The superior mesenteric vein withdraws the main part
of the blood from the small intestines.
Duodenum.
—The duodenum has received its name
from being about equal in length to the breadth of twelve
fingers (ten inches).
It is the shortest, widest and the most fixed part of
the small intestines, being closely and firmly attached to
the posterior abdominal wall. It is not covered by the
mesentery. The upper half of the duodenum is in the
epigastric region and the lower half is in the umbilical
region. It is practically in the median line of the body.
The duodenum is shaped like a horseshoe, the opening
being directed toward the left. The arteries supplying
the duodenum are the pyloric and the pancreatic duodenal
branch of the superior mesenteric. The veins correspond
to the arteries.
The pancreatic duct and the bile duct empty into the
duodenum at its middle portion.
Jejunum.
—The jejunum is the second portion of the
small intestines, it derives its name from the latin word
“jejunas,” meaning empty, because it was formerly supposed
to be empty after death.
It is wider, thicker, more vascular and of a deeper
color than the ileum. The jejunum is about eight feet in
length or two-fifths of the length of the small intestines.
The arteries which supply the jejunum are the
branches of the superior mesenteric artery. The veins
are of the same name.
[108]
The jejunum is fastened to the posterior wall of the
abdomen by an extensive fold of the mesentery.
Ileum.
—The ileum is derived from a Greek word meaning
to twist, and is so named on account of its numerous
coils and convolutions. It is the third portion of the
small intestines and is placed below the jejunum. It is
much narrower and thinner than the jejunum, about
twelve feet in length or three-fifths of the length of the
small intestines. It is also attached to the posterior abdominal
wall by means of the mesentery. The arteries
which supply the ileum are the branches of the superior
mesenteric artery. The veins are of the same name.
The villi are minute projections on the mucous membrane
of the small intestines. They are largest and most
numerous in the duodenum and jejunum, and become
fewer and smaller in the ileum. It is in the villi of the
intestines that we find the termination of the mesenteric
arteries, the beginning of the mesenteric veins and the
commencement of the lacteals.
As the food passes down the intestines, having been
previously prepared in the stomach and intestines for
absorption, it comes in very close contact with the villi
of the intestines and it is here that the nutrition from
the food is absorbed through the villi wall into the lacteals,
and hence carried to the receptaculum chylii.
The Large Intestines.
—The large intestine extends
from the termination of the ileum to the anus. It is about
five or more feet in length or about one fifth of the whole
extent of the intestinal canal. It is largest at its commencement
at the caecum, and gradually diminishes in
[109]
size as far as the rectum, where there is a dilatation of
considerable size just above the anus.
The large intestine differs from the small intestine in
its greater size, its more fixed position, its sacculated form.
The large intestine in its course describes an arch,
which surrounds the convolutions of the small intestines.
It commences in the right inguinal region, in a dilated part
of the caecum. It ascends through the right lumbar and
the right hypochondriac regions to the under surface of
the liver, it here takes a bend to the left, the hepatic flexure,
and passes transversely across the abdomen on the
confines of the epigastric and umbilical regions, to the
left hypochondriac region; it then bends again, the splenic
flexure, and descends through the left lumbar region
to the left inguinal region, where it becomes convoluted
and forms the sigmoid flexure; finally it enters the pelvic
cavity and descends along the posterior wall to the anus.
The large intestine is supplied by the branches of the
inferior mesenteric artery, and the veins are of the same
name.
The large intestines are divided into the caecum, colon
and rectum.
Caecum.
—The caecum is the commencement of the
large intestines, it is a large blind pouch situated below
the ileo caecal valve. The ileo caecal valve is the valve
between the exit of the small intestines and the commencement
of the large intestines. The caecum is held
mostly in place by the folds of the peritoneum.
The Vermiform Appendix.—The appendix is found
only in the human, the higher apes, and the wombat,
[110]
although in certain rodents a somewhat similar arrangement
exists. The appendix is a long, narrow, worm
shaped, musculo-membranous tube, which starts from the
inner side of the posterior wall of the caecum, below and
behind the termination of the ileum. It is the seat for
a very common disease called appendicitis. It varies
from one half to nine inches in length, its average being
about three inches. Its diameter is from one eighth to
one quarter of an inch.
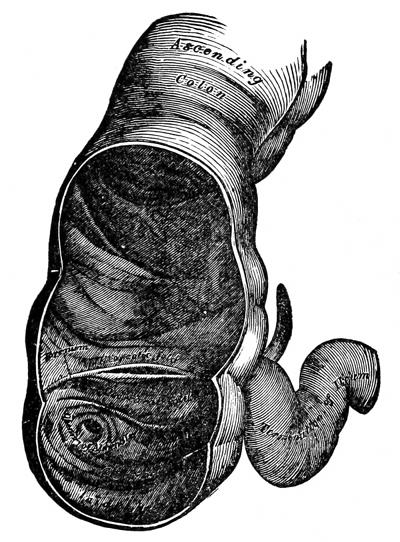
Fig. 24—The caecum and colon laid open to show the ileo-caecal
valve. (Gray)
[111]
The Colon.
—The colon is divided into three parts, the
ascending, transverse and the descending colon.
The ascending colon is smaller than the caecum, with
which it is continuous. It passes upward from its commencement
at a point corresponding to the ileo-caecal
valve, to the under surface of the right lobe of the liver,
on the right of the gall bladder, where it is lodged in a
shallow depression on the liver; here it bends abruptly
inward to the left, forming the hepatic flexure. It is
held to the posterior wall of the abdomen by folds of the
peritoneum.
The transverse colon is the longest part of the small
intestines, passes transversely from the right to the left
across the abdomen, opposite the confines of the epigastric
and umbilical regions, where it curves downward
beneath the lower end of the spleen, forming the splenic
flexure. In its course the transverse colon describes an
arch, the concavity of which is directed backward toward
the vertebral column and a little upward.
This is the most movable part of the colon, only covered
by peritoneum and held to the back wall by the
folds of the peritoneum. The transverse colon is in relation,
by its upper surface with the liver and gall bladder
the great curvature of the stomach, and the lower end
of the spleen; by its under surface with the small intestines;
by its anterior surface with the anterior layers of
the great omentum and the abdominal wall; its posterior
surface on the right is in relation with the duodenum and
on the left it is in contact with the convolutions of the
jejunum and ileum.
[112]
The descending colon passes downward through the
left hypochondriac region and lumbar region along the
outer border of the left kidney. At the lower end of the
left kidney it turns inward where it terminates in the
formation of the sigmoid flexure. The descending colon
is held to the back wall by folds of the peritoneum.
The sigmoid flexure, the narrowest part of the colon,
is situated in the left inguinal region and communicates
with the rectum.
The Rectum.
—The rectum is the terminal part of the
large intestines, and extends from the termination of the
sigmoid flexure to the anus. The adult rectum in male
is from four to six inches in length, and in the female is
from three to five inches in length.
The anus is the terminal opening of the alimentary
canal.
Liver.
—The liver is the largest gland in the body,
and is situated in the upper and right part of the abdominal
cavity, occupying almost the whole of the right
hypochondriac, the greater part of the epigastric, and extending
almost to the middle of the left hypochondriac
region.
In the male it weighs from fifty to sixty ounces, and in
the female, from forty to fifty.
It is relatively much larger in the foetus, being about
one-eighteenth of the body weight in the foetus, and in
the adult, about one-thirty-sixth of the body weight.
Its greatest width is from seven to eight inches, is
about twelve inches long, and in its greatest thickness
about three inches.
[113]
The liver is very soft and is easily lacerated and friable;
its color is a dark reddish brown. To obtain a correct
idea of its shape, you might compare it to a wedge,
the base of which is directed to the right, and thin edge
toward the left.
The liver has five surfaces, superior, inferior, anterior,
posterior and right lateral.
The liver has five lobes, right and left, caudate, quadrate,
and lobus spigelii. It has five ligaments, right and
left lateral or triangular, falciform, coronary and round.
The liver has five fissures, the umbilical, the fissure of the
ductus venosus, the transverse fissure, the fissure for the
gall bladder, the fissure for the vena cava. These fissures
can be represented by the letter H.
L
E
F
T | Fissure of Ductus venosus | BACK
Transverse | Fissure inferior vena cava | R
I
G
H
T |
| Umbilical fissure | FRONT | Fissure for gall bladder |
The liver is movable within certain narrow limits.
It moves with respiration. On inspiration, it moves down
with the diaphragm to a little below the right nipple
line. The ligaments do not give the liver much support
because they lie relaxed, but it does get its main support
from the connective tissue which unites the liver to the
diaphragm, the hepatic veins which join the vena cava
and also by the intra-abdominal pressure resulting from
the tonic contraction of the abdominal muscles.
[114]
Also when the abdominal tension is normal, the intestines
are driven up, and become a bed for the liver.
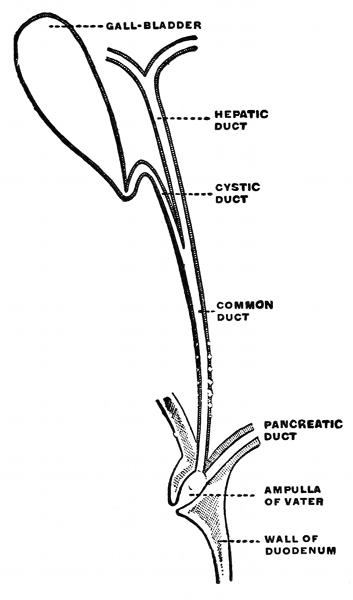
Fig. 25—Excretory
apparatus of the
liver. (Poirier and
Charpy)
The most important function is the secretion of the
bile; it is also the excretor of deleterious matter and impurities.
It also effects important changes of the blood
in its passage through it, for the portal circulation.
The excretory apparatus of the liver consists (a) of the
hepatic duct, (b) the gall
bladder, (c) cystic duct, (d)
the common bile duct.
The hepatic duct is formed
by two main trunks nearly
of equal size which issue
from the liver, one from the
right and one from the left
lobe. The hepatic duct passes
downward and to the
right from one to two inches
where it is joined at an acute
angle with the cystic duct.
The Gall Bladder.
—The
bladder is a reservoir for
the bile. It is a conical
or pear-shaped
sack, lying on the
under surface of the
right lobe of the
liver. It is about
four inches in length,
[115]
one inch in depth and holds from eight to ten drams.
The cystic duct is about an inch and a half in length,
and passes obliquely downward to the left from the neck
of the gall bladder, and joins the hepatic duct.
The common bile duct (ductus communis choledochous)
is the common excretory duct of the liver and the gall
bladder, and is formed by the union of the cystic and
hepatic ducts. It descends to the middle portion of the
duodenum, where it unites with the pancreatic duct, the
two passing obliquely through the wall of the descending
portion of the duodenum. The tissues of the liver are
nourished by the blood from the hepatic arteries.
The Pancreas.
—The pancreas (the sweet bread) is
a gland similar in structure to the salivary glands; is
about seven inches long, of a grayish white color; its
weight varies from two to six ounces. It is situated behind
the stomach, and it secretes the pancreatic juice. It
extends to the right in a part of the epigastric space.
The tail lies above the left kidney, and is in contact with
the lower end of the spleen and in the left hypochondriac
region; the body lies behind the stomach and transverse
colon and in front of the great aorta, portal vein
and inferior vena cava. The arteries nourishing it are
the large and small pancreatic, which are branches of the
splenic artery.
The pancreatic duct is the principal excretory duct
of the pancreas. It extends transversely from the left
to the right through the substance of the pancreas.
After leaving the body of the pancreas, it unites with
the common bile duct of the liver where it empties into the
[116]
duodenum (first section of the small intestines after
leaving the stomach).
The pancreatic duct carries pancreatic juice (a digestive
fluid) from the pancreas to the duodenum.
The Spleen.
—The spleen belongs to that class of bodies
known as ductless glands and has no excretory duct;
is oblong, flattened, soft, very brittle, very vascular, of
a very dark bluish red color; is situated in the left hypochondriac
region behind and to the left of the stomach;
is five inches long, three inches wide and two inches
thick and weighs about seven ounces. The vessels which
nourish it are the splenic artery and splenic vein.
Function. It is supposed to furnish blood corpuscles.
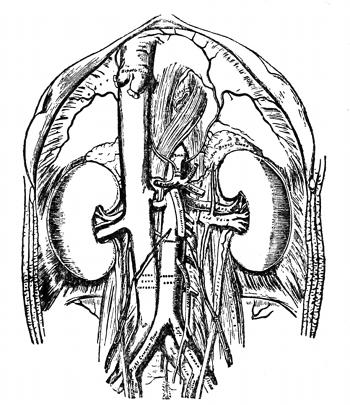
Fig. 26—The abdominal aorta and its branches. (Gray)
The Kidneys.
—The kidneys are large glands, two in
[117]
number and are situated from five to six inches apart or
about three inches on either side of the median line in the
right and left lumbar regions.
The upper extremity of the kidneys lies on the level
of the twelfth dorsal vertebra and the lower extremity
on the level of the third lumbar vertebra. Each kidney
is four and one-half inches in length, two to two and one-half
inches in breadth, a little more than one inch in
thickness.
The weight of the kidney in the adult male is from four
and one-half to six ounces each. In the adult female the
weight would be from four to five and one-half ounces.
Their function is to separate from the blood certain
waste products and an excess of water, the combination
of which we know as urine. The principal products
excreted by the kidneys from the blood along with water
are ammonia and urea. The blood is taken to the kidneys
by the renal arteries and the renal veins carry it back
to the blood circulation.
The urine is then taken from the kidneys by the
ureters and conveyed to the urinary bladder.
The Ureters.
—The ureters are cylindrical tubes about
sixteen inches in length and of diameter of a goose-quill.
The Suprarenal Capsules.
—The suprarenal capsules
belong to that class of bodies known as ductless
glands and are two small flattened bodies of yellowish
color, situated at the back of the abdomen, behind the
peritoneum (the covering for all of the abdominal organs),
and immediately above and in front of the upper end of
[118]
each kidney. The name is derived from the position it
occupies in relation to the kidney, supra meaning above,
and renal pertaining to the kidneys.
The functions are as yet unknown. The suprarenal
arteries furnish nourishment for the suprarenal capsules.
The Pelvic Cavity.
—The pelvic cavity is that portion of
the abdomen situated between the ilium and pubic bones,
or in other words the extreme lowest portion of the abdominal
cavity. The organs located within this cavity
are the bladder in the male and the bladder and the
uterus (womb) in the female.
The Bladder.
—The urinary bladder is a reservoir for
the urine, situated in the pelvic cavity behind the pubic
bone. In life it is supplied with blood by the anterior
branches of the internal iliac arteries accompanied by the
internal iliac veins.
The Uterus.
—The uterus is the organ of gestation, receiving
the fecundated ovum into its cavity, retaining it,
and supporting it during the development of the foetus,
and becoming the principal agent in its expulsion at the
time of parturition (delivery). It is nourished in life by
branches of the internal iliac artery, which is accompanied
by the iliac vein.
The uterus is situated in the pelvic cavity between
the rectum and the bladder, and is held in position by the
lateral and round ligaments on each side. The uterus
is about 3 inches in length, 2 inches in breadth and weighs
[119]
from one to two ounces. It is composed of three coats,
external serous, middle muscular, and internal mucous.
The serous coat, derived from the peritoneum, is thin
and vascular.
The muscular coat is the chief coat, it is dense, firm, of
a grayish color and cuts like cartilage.
The mucous coat is thin, smooth and closely adherent
to the muscular coat. It is highly vascular.
The blood supply to the uterus is the uterine arteries
which are the posterior branches of the internal iliac
arteries, and the ovarian arteries which are branches of
the aorta. These break up in capillaries and form a fine
network plexus in the coats of the uterus.
The veins are of large size and are the uterine which
empty into the internal iliac veins and the ovarian veins.
On the right side the ovarian vein empties into the ascending
vena cava, and on the left side into the renal vein.
Prostate.
—The prostate gland is a pale, firm glandular
body, which surrounds the neck of the bladder in the
male. Its shape and size resembles a horse chestnut. It
weighs from one-half to one ounce and measures one
and one-half inches across and three quarters of an inch
deep. Its structure is inclosed by a firm thin fibrous capsule.
Its substance is of a pale reddish grey color and
is composed of glandular substance and muscular tissue.
The arteries that supply the prostate are derived
from the internal pubic, a branch of the internal iliac.
The veins form a plexus around the gland and communicate
[120]
with veins which empty into the internal iliac
veins. Its function is to secrete an opaque fluid.
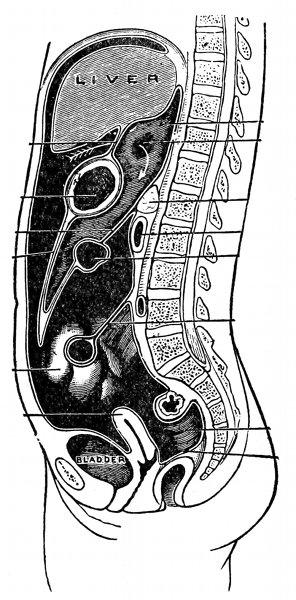
Fig. 27—The Peritoneum. (Gray)
The Peritoneum.
—During life and in the uncut corpse
the peritoneal cavity is air-tight. It is not a real cavity,
as muscular tension and atmospheric pressure permit no
vacant space to form. When the surgeon or embalmer
[121]
opens the abdomen, the peritoneal cavity is at that moment
produced.
The peritoneum is the largest serous membrane in the
body. In the male it is a closed sac, a part of which is
applied against the abdominal sides, while the remainder
is reflected over the contained viscera. In the female
it is not a closed sac, since the free extremities of the
fallopian tubes open directly into the peritoneal cavity.
The parietal peritoneum is that portion applied
against the abdominal sides.
The visceral peritoneum is that portion reflected over
the viscera.
The peritoneum consists of two sacs.
The greater sac lines the greater part of the abdominal
cavity as almost all of the viscera are covered
by it.
The lesser sac is placed behind the stomach. These
two sacs communicate with each other by a narrow orifice
called the Foramen of Winslow.
The peritoneum, as it covers different organs or sets
of organs, receives special names.
The lesser omentum consists of two layers, these
split to envelope the stomach.
The greater omentum consists of four layers. Two
of these layers extend from the stomach and together
with two other layers of the same structure which envelope
the transverse colon, form an apron for the intestines.
[122]
The mesentery consists of two layers which invests
the small intestines. Between the two layers of the mesentery
we find the blood vessels, nerves, lacteals, and
glands, leading to and from the intestines. The mesentery
is fan shaped, and is attached to the second lumbar
vertebra. The length of the mesentery fan is about
eight inches from commencement to termination at intestine.
It extends the whole length of the intestines,
which is about twenty feet.
[123]
CHAPTER IX.
THE VASCULAR SYSTEM.
The Vascular System.
—The vascular system is composed
of the organs immediately concerned in the circulation
throughout the body of the fluids which convey
to the tissues the nutritive substances and oxygen necessary
for their metabolism and carry from them to the
excretory organs the waste products formed during metabolism.
The system is usually regarded as being composed of
two portions, the one consists of organs in which circulate
the red fluid which we term blood, and called the
blood vascular system, while the organs of the other contain
a colorless or white fluid known as lymph or chyle,
and is known as the lymphatic circulation.
| | | Blood vessels | arteries |
| | The blood vascular system | capillaries |
| The vascular system | veins |
| Heart |
| The lymphatic circulation |
The Blood Vascular System.
—A knowledge of the
general features of the circulatory system are essential
to the undertaker and the embalmer as a means of enabling
him not only to perform the ordinary operations and
[124]
duties of his profession intelligently, but to equip him
with the knowledge necessary to meet the exceptional
conditions which sometimes arise.
There is a growing appreciation of the fact, also, that
thoroughness in the practice of embalming is worth striving
after. Many cases of embalming, no doubt, require
a minimum amount of attention, particularly where the
body is to be kept but a short time. Where preservation
for longer periods is required, as for transportation, or
where disease and accident have interfered seriously with
the circulation, a more exact knowledge is evidently desirable.
The blood vascular system comprises the heart, which
is the central organ of the whole system, and all the blood
vessels. This system, with its arteries and veins, permeates
the whole body and becomes divided and subdivided
at its outer portion into vessels constantly decreasing in
size, until those extremely minute vessels, the capillaries,
are reached. All the tissues of the body are very rich in
these, so that all portions of the body are supplied with
blood, which is essential for the nourishment and rebuilding
of the tissues. The large vessels which convey
blood from the heart are termed arteries, while the vessels
which convey the blood back to the heart are termed
veins.
For one to properly embalm the human body, it is
necessary to understand the way the fluid will circulate
through the body, and the only way we can do this is
to study the circulation of the blood as it would occur in
life.
[125]
To facilitate the description of the blood vascular system,
it has been divided into six subdivisions as follows:
- (1) Systemic.
- (2) Pulmonary.
- (3) Coronary.
- (4) Portal.
- (5) Foetal.
- (6) Collateral.
The Systemic Circulation.
—The systemic circulation
is called the greater circulation of the body. The course
of the blood is from the left ventricle of the heart through
the aortic semi-lunar valve to the great aorta and its
branches which end in capillaries in the tissues of the
body then through the veins the terminal trunks of which
end in the right auricle of the heart. So the systemic
circulation is the circulation of the blood from the left
ventricle of the heart to the right auricle of the heart and
this circulation has the important function of carrying
oxygen to the tissues to nourish them, and of carrying
carbonic acid gas back to the heart which is a waste product
of the tissues.
The systemic circulation is divided for the sake of
convenience into the following:
- (1) The arterial system.
- (2) Capillary.
- (3) The venous system.

Fig. 28—The arch of the
aorta and its branches.
(Gray)
The Arterial System.
—The blood leaving the heart
passes from the left ventricle through the aortic semi-lunar
valve, into the ascending aorta. Here the two
[126]
coronary arteries come off which go to supply the muscular
tissues of the heart. The ascending aorta passes
into the arch of the aorta. Here are given off the innominate
artery to the right and the common carotid
and the subclavian to the left.
The innominate is only about
an inch or two in length, and
divides into the right common
carotid and the right subclavian
arteries. On each side the subclavian
passes down beneath
the clavical bone and enters the
axillary space where it is known
as the axillary artery. After
leaving the axillary space, the
artery passes down the arm and
is known as the brachial artery.
About one inch below the bend
of the elbow the artery divides
into two branches, known as the
radial and ulnar. The radial
goes to the thumb side of the
hand, and the ulnar to the little finger side of the hand.
The ulnar artery and a branch of the radial form the palmar
arch, which gives off the branches to the fingers. Coming
off the brachial are the deep brachial arteries and the
anastomotica magna arteries which anastomose and give
collateral circulation to the forearm, by means of the recurrent
radial and ulnar arteries.
The common carotid arteries pass up each side of the
neck to a point opposite the Adam's apple, where they,
[127]
divide into the external carotid, which supplies the muscular
tissue of the face, and the internal carotid artery,
which goes up through the skull and helps to form the
circle of Willis.
The vertebral arteries come off the subclavian arteries
on either side and pass upward, winding through the
foramen of the vertebrae, until finally arriving inside
the cranial cavity, unite to form one artery called the
basilar, which helps to form the circle of Willis.
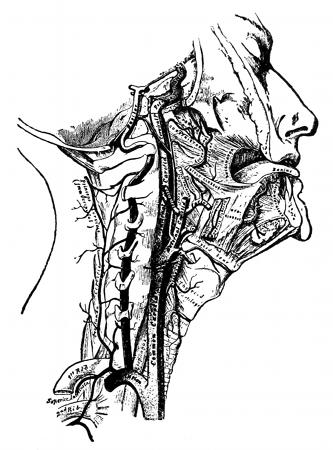
Fig. 29—The internal carotid and vertebral arteries. (Gray)
The circle of Willis is situated at the base of the brain
and gives off to the front the two anterior cerebral arteries,
[128]
to the sides the two middle cerebral arteries, and
to the back the two
posterior cerebral arteries.
The two anterior
cerebral arteries
are connected by the
anterior communicating
branch, and the middle
cerebral artery and the
posterior cerebral arteries
on each side are
connected by the posterior
communicating
branches. The cerebral
arteries terminate in
the piamater as a dense
capillary network, and from there supply the substance
of the brain with nutrition.
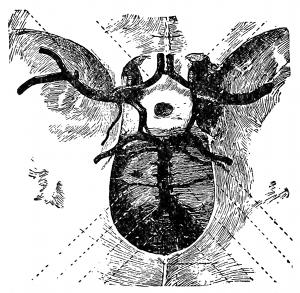
Fig. 30—The circle of Willis.
(Spalteholz)
The external carotid artery supplies the muscular
tissues of the face. The external carotid artery arises
from the common carotid artery at about the level of the
upper border of the thyroid cartilage—a level which corresponds
with the body of the fourth cervicle vertebra.
Thence it is directed upward and slightly backward towards
the angle of the jaw, where it enters the substance
of the parotid gland and continues upward in that structure
to just below the root of the zygoma. Here it gives
rise to a large branch, the internal maxillary, and is then
continued upward over the root of the zygoma upon the
side of the skull, this terminal portion of it being termed
[129]
the superficial temporal artery. The branches of the external
carotid artery from below upward are (1) the
ascending pharyngeal, (2) the superior thyroid, (3) the
lingual, (4) the occipital, (5) the facial or external maxillary,
(6) the posterior auricular, (7) the internal maxillary,
(8) the superficial temporal.

Fig. 31—The arteries of the face
and scalp. (Gray)Fig. 32—The external carotid and
its branches. (Gray)
The arch of the aorta now continues into the thoracic
aorta, so called while it is in the thoracic cavity, and
after it has passed through the diaphragm becomes the
abdominal aorta. At a point opposite the umbilicus or
navel the abdominal aorta divides into the two common
iliac arteries. Each common iliac artery divides into
an internal iliac artery, which supplies the organs of the
pelvic cavity, and an external iliac artery, which passes
[131]
beneath Poupart's ligament. As the artery passes down
the leg it is known as the femoral artery, until it passes
into the popliteal space, where it is called the popliteal
artery. About one inch below the popliteal space the
artery divides into the anterior tibial artery, which runs
on a straight line down the front and outside of the leg
to a point between the big toe and the one next to it,
and the posterior tibial artery which passes down the
back part of the foreleg between the inside ankle and
the heel. The peroneal, a branch of the posterior tibial,
passes down the foreleg between the outside ankle and
the heel. The anterior tibial artery, as it passes through
the instep is known as the large dorsal artery and further
on is known as the small dorsal artery. In the foot
is the plantar arch, formed by branches of the posterior
and anterior tibial arteries, which send out branches to
each toe.
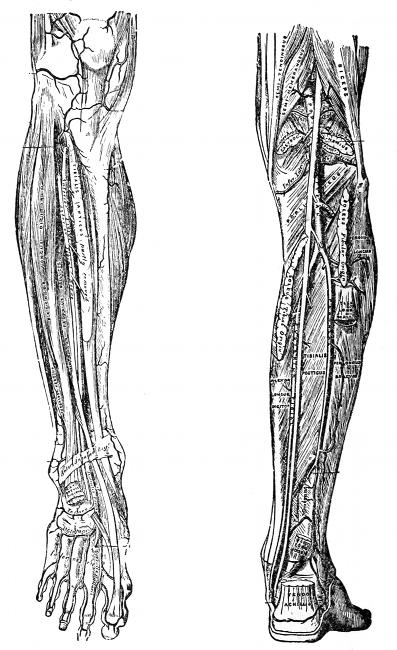
Fig. 33—The anterior tibial
artery. (Gray)Fig. 34—The popliteal, posterior
tibial, and peroneal arteries. (Gray)
Coming off the femoral are the deep femoral and the
anastomotica magna arteries, which anastomose and form
collateral circulation to the foreleg by means of the recurrent
anterior and posterior tibial arteries.
Coming off the subclavian arteries are the superior
and inferior mammary arteries, which pass down over
the chest wall, anastomose and give collateral circulation
to the lower extremities by means of the superior and inferior
epigastric arteries, branches of the external iliac
and femoral arteries.
The thoracic aorta gives off the intercostal arteries,
which supply the ribs, the bronchials which supply the
[132]
lungs, the esophageal which supplies the esophagus, and
the pericardiac which supplies the pericardium.
The abdominal aorta gives off in rotation the coeliac
axis, which as a hub in a wheel gives off three spokes,
the gastric artery to the stomach, the hepatic to the liver,
and the splenic artery to the spleen. The next branch
is the phrenic, which supplies the diaphragm, then the
suprarenal artery, two or more in number coming off
of both the aorta and the renal arteries. The suprarenal
arteries supply the suprarenal capsules. The next
branch is the superior mesenteric artery, which supplies
the small intestines; the next branch is the renal arteries,
which supply the kidneys; the next branch is the spermatic
or the ovarian arteries, which supply the testes in
the male or the ovaries in the female; the inferior mesenteric
artery, which supplies the large intestines. Also
coming off the aorta at regular intervals are the lumbar
arteries, which supply the side walls.
The Capillary Circulation.
—The capillaries are very
minute blood vessels, forming a network between the
terminating arteries and the commencing veins.
They derive their name from the word capillus (hair).
They vary in size from 1-3500 to 1-3000 of an inch, the
largest capillaries being those of the skin. These little
vessels are so thickly distributed throughout most of the
tissues of the body as to make it impossible to insert a
cambric needle in the flesh without pricking scores of
them.
[133]
When we embalm a body the object should be to introduce
a sufficient amount of fluid through the arterial
system so that these tiny capillaries will be filled. These
little vessels are so minute and the walls are so thin that
the fluid is immediately taken up into the tissues. If
every tissue of the body can be supplied with fluid by
means of the capillaries, we would have the ideal, the
body would be perfectly embalmed. Let
us then not only be arterial embalmers,
but, better still, let us be capillary and
tissue embalmers.
Fig. 35—Capillaries
a, cells; b, nuclei.
(Gray)
Capillaries have one wall, which is
the continuation of the inner wall of the
artery, thus making the capillary so thin
that fluid finds its way easily through it
into the surrounding tissues.
Some parts of the body are more vascular
than others and some tissues of the
body, such as the cornea of the eye, the
epidermis, cartilage, the substance of the
brain, etc., are entirely destitute of capillaries.
The combined area of all the capillaries
of the body is many times greater
than the combined area of the trunk
vessels. If this were not so, the high pressure on the
arterial system would break the thin capillary walls and
also the greater area allows the blood to circulate more
slowly which gives time for the liberation of oxygen to
[134]
the tissues and for the absorption of carbon dioxide.
The Venous System.
—The veins, like the arteries, are
tubular vessels, their function being to receive the blood
from the capillaries and convey it to the auricles of the
heart. There are two classes of veins, systemic and
pulmonic.
The systemic veins receive the impure or carbonized
blood from the capillaries and convey it to the right
auricle of the heart.
The pulmonic veins receive the pure oxygenized blood
from the lungs and convey it to the left auricle of the
heart. The pulmonic veins will be taken up and discussed
later under the pulmonary circulation.
Systemic veins are divided into superficial and deep
veins and sinuses.
The superficial veins are found between the layers of
the superficial fascia, just beneath the skin, and communicate
with the deep veins by branches which pierce
the fascia.
The deep veins are found deeper down, between the
muscles, and are surrounded by the deep fascia.
The smaller arteries, such as the radial, brachial, posterior
and anterior tibial, and the peroneal arteries, are
each accompanied by two veins, one on each side of the
artery, which are called venae comites (accompanying
[135]
veins). The larger arteries, such as the common carotid,
the femoral and the iliac, are accompanied by only one
vein.
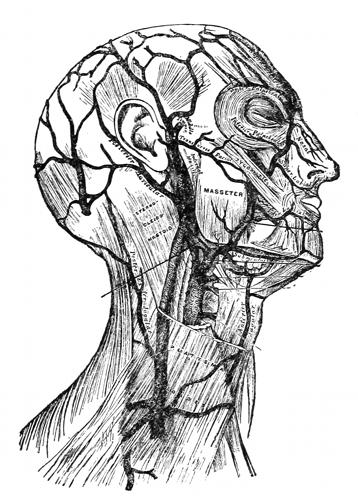
Fig. 36—Superficial veins of the head and neck. (Gray)
Veins arise from the capillaries, or, rather, from the
minute capillary plexus, formed by a massing or blending
of the tiny venules. These small vessels unite to form
larger trunks, and as they continue toward the heart increase
in size until they finally unite to form the ascending
and descending venae cavae.
[136]
The Sinuses.—The cerebral veins are small vessels that
arise from the capillaries of the brain, and terminate in
the sinuses of the dura mater. There are many sinuses
in the cranial cavity, and differ from the vein, in that
the walls are thinner, having only two walls while the
veins have three, and they do not have valves. The outer
walls of the sinuses of the brain are formed by a division
of the dura mater, while the inner wall is the continuation
of the inner wall of the vein.
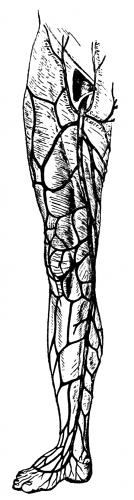
Fig. 37—The internal
long saphenous
vein. (Gray)
They are of little interest to embalmers,
except for the fact that when the brain is
injected by any of the so-called needle
processes, the fluid is quickly conveyed
through these vessels to the tissues of the
brain, and that organ is thoroughly
preserved.
The vessels starting at the foot are the
anterior and posterior tibial veins, which
unite just below the knee to form the
popliteal vein, in the popliteal space.
Another vein starts from the foot and runs
into the popliteal vein called the external
short saphenous. Starting also at the foot
and running into the posterior tibial vein
is the peroneal vein.
The popliteal vein after leaving the
popliteal space is known as the femoral
vein as it passes up the leg, to Poupart's
ligament. Another vein, the internal long
saphenous, starts at the foot, and runs into
[137]
the femoral vein about an inch below Poupart's ligament.
After passing beneath Poupart's
ligament the vessel is called the
external iliac. Coming from the
organs of the pelvic cavity is the
internal iliac, which joins with the
external iliac vein to form the common
iliac vein. The right and left
iliac veins join opposite the umbilicus
to form the ascending vena
cava. The ascending vena cava
passes upward to the right of the
vertebral column through the diaphragm
and enters the right auricle
of the heart by means of the eustachian
valve.
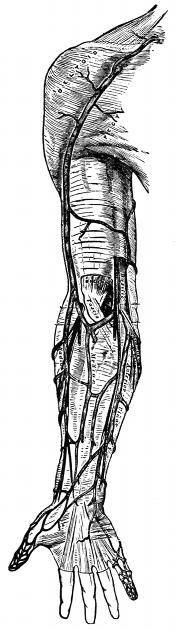
Fig. 38—The superficial
veins of the arm. (Gray)
In the forearm are the radial
veins on the thumb side of the hand,
the ulnar veins on the little finger
side of the hand, and the median
vein just between the radial and
ulnar veins. The median vein
divides into the median cephalic vein
and the median basilic. The median
cephalic vein unites with the radial
vein to form the cephalic vein, which
runs up the back part of the arm
and finally empties into the subclavian
vein. The median basilic
[138]
unites with the ulnar vein to form the basilic, which runs
up the inner part of the arm between the biceps and triceps
muscles. The deep brachial veins or the vena comites,
two in number, which follow the brachial artery, run into
the basilic vein. When the basilic vein arrives at the axillary
space it takes on the name of the axillary vein, and as
the vessel passes beneath the subclavian bone, it becomes
the subclavian vein. The right and left subclavian veins
with the right and left internal jugular veins from each
side of the head form the right and left innominate veins,
which unite to form the descending vena cava, which
runs into the right auricle of the heart.
Starting at the head, the superior longitudinal sinus
begins at the fore part of the brain and runs backward
[139]
between the two hemispheres of the brain and empties into
the wine press or Torcular herophili. The inferior
longitudinal sinus begins at the fore part of the brain,
but rung deeper down in the pia mater between the two
hemispheres of the brain, terminates in the straight
sinus which empties into the wine press. Beginning at
the base of the cerebellum are the two occipital sinuses
which run together and terminate in the wine press.
After all the blood has been gathered together in the
[140]
wine press, it leaves by means of the right and left lateral
sinuses which pass down as far as the jugular foramen.
Beginning at the base of the brain in front are the right
and left cavernosus sinuses, which run into the inferior
petrosal sinuses, which pass down as far as the jugular
foramen, where they join the lateral sinuses to form the
right and left internal jugular vein. The superior petrosal
sinus is between the lateral sinus and the cavernosus
sinus uniting them. Joining the right and left
cavernosus sinuses is the circular sinus and joining
the right and left inferior petrosal sinuses is the transverse
sinus. The right and left internal jugular veins
pass down through the jugular foramens and down the
neck to where they with the right and left subclavian
veins form the right and left innominate veins. The right
and left innominate veins unite to form the descending
vena cava which empties into the right auricle of the
heart.
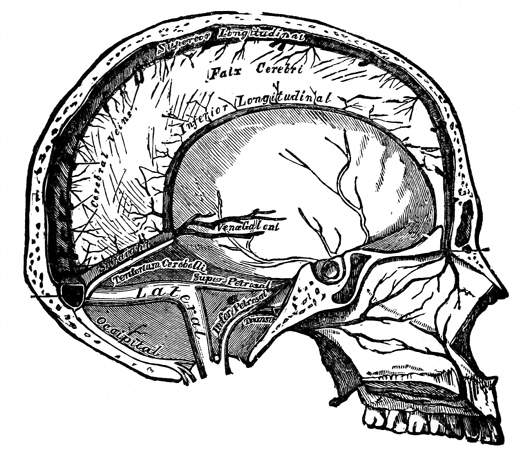
Fig. 39—Vertical section of the
skull, showing the sinuses of the
dura mater. (Gray)
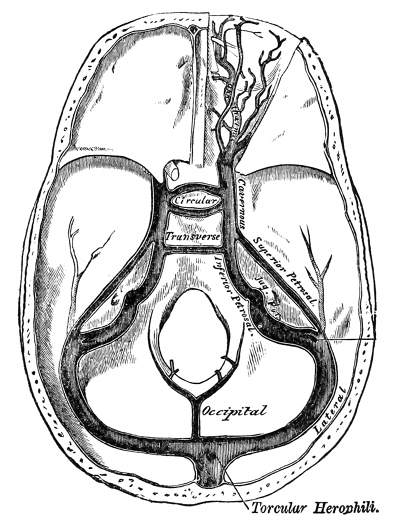
Fig. 40—The sinuses at the base of the skull. (Gray)
Beginning in the tissues of the heart are the coronary
veins, which terminate in the coronary sinus and then
into the right auricle of the heart through the coronary
valves.
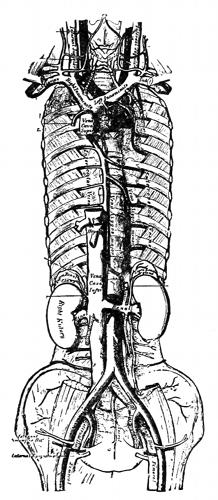
Fig. 41—The azygos system
and venae cavae with
branches. (Gray)
The azygos system consists of the major azygos vein,
which starts at the right external iliac vein and empties
into the descending vena cava; the minor azygos vein
which starts at the left external iliac vein and empties
into the major azygos vein back of the heart; and the
tertiary azygos vein, which starts at the left subclavian
vein and empties into the minor azygos vein. The azygos
veins collect all the blood from the side walls of the
[141]
body and form a perfect collateral circulation between
the superior and inferior caval systems, and thoroughly
equalizes the blood pressure all
over the body. The major azygos
vein receives the following: the
right intercostal veins, excepting
the first; the azygos minor; the
right bronchial vein; the esophageal
vein; the pericardiac; and the
posterior mediastinal veins. The
minor azygos vein receives the following:
the tertiary azygos vein;
the lower five left intercostal
veins; the small left mediastinal
veins; the lower left esophageal
veins. The tertiary azygos receives
the following: the fifth,
sixth and sometimes the seventh
intercostal veins; the lower end of
the lower left superior intercostal
vein; and the left bronchial vein.
The inferior vena cava receives
the following veins: the lumbar
veins; the hepatic veins; the
phrenic veins; the renal veins; the right suprarenal
vein; the right spermatic or ovarian vein. The left
spermatic or ovarian vein and the left suprarenal vein
empty into the left renal vein.
The Pulmonary Circulation.
—This is the circulation
existing between the right ventricle of the heart through
the lungs back to the left auricle of the heart.
[142]
The pulmonary artery takes its origin from the summit
of the right ventricle. It is about two inches in
length, and is directed upward, backward and slightly
towards the left, and beneath the arch of the aorta it
divides into the right and left pulmonary arteries. These
end in a system of capillaries in between the air cells of
the lungs, where carbon dioxide is thrown off and oxygen
taken on.
The pulmonary veins are four in number, two passing
from the root of each lung to the posterior surface of the
left auricle of the heart. Each vein is formed at the root
of the lung by the union of a number of smaller vessels
which take origin ultimately from the capillary net work
formed from the branches of the pulmonary artery, and
to a certain extent from that formed by the bronchial
arteries. Each pulmonary vein is about six inches in
length.
The Coronary Circulation.
—The heart receives its
blood supply through the two coronary arteries which
arise from the aorta immediately above its origin, the
return flow being by the coronary veins which open into
the right auricle of the heart by the coronary sinus. The
branches of the coronary arteries upon the surface of the
heart are, as a rule, all end arteries; that is, arteries which
form no direct anastomosis with their neighbors. Practically
no blood can be carried directly, therefore, by the
left coronary artery into the territory supplied by the
right one, or vice versa.
The coronary sinus is a short venous trunk a little
over an inch in length, which occupies the right half of
[144]
that portion of the auriclo-ventricular groove which lies
between the left auricle and ventricle. At the right end
it opens into the right auricle, its orifice being guarded
by the Thebesian valve.
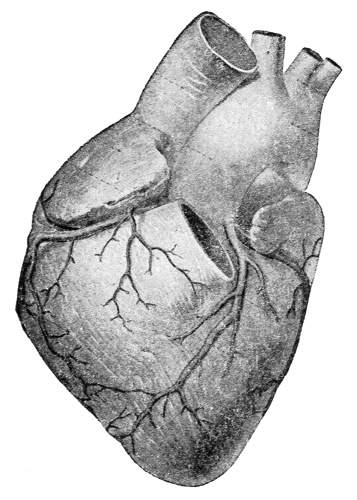
Fig. 42—A front view
of the heart showing
coronary arteries.
(Spalteholz)
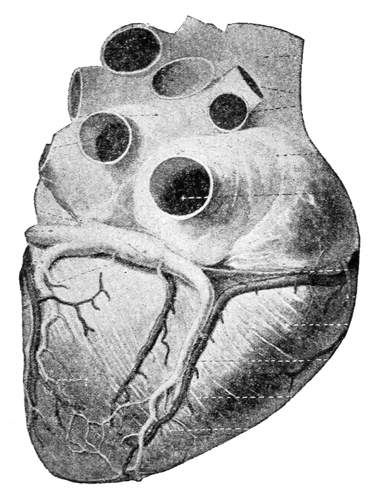
Fig. 43—A back view
of the heart showing the
coronary sinus, and vessels
entering and leaving.
(Spalteholz)
The Portal Circulation.
—This circulation is of little or
no value to the embalmer, as no part of it is directly required
to supply any of the tissues with embalming fluid.
The portal circulation is formed by the superior mesenteric
vein and the splenic vein uniting to form
the portal vein. The inferior mesenteric vein runs into
the splenic vein; the gastric and cystic veins run into the
portal veins. The portal vein ends in capillaries in the
liver, where certain important changes take place, namely,
the taking out of the bile.
The portal vein and its tributaries are unlike the
veins in the general circulation, as there are no valves.
Their function in life is to gather up food or nutrition
for the blood, and to the embalmer is of no special importance,
only to know how this circulation is made up.
The vessels that convey blood to the liver in life and the
fluid in death are discussed under the liver.
After death, about one-fourth of the blood of the body
is to be found in the portal system. This blood can in
no way be removed, and this is one of the reasons why
the embalmer is not able to draw more blood than he
does.
The Foetal Circulation.
—The foetal circulation is that
circulation existing between mother and unborn child.
The placenta constitutes, from the third month of
intra uterine life, the nutritive and respiratory organ of
[145]
the foetus. The placenta consists of a maternal portion
and a foetal portion. The maternal portion is that portion
of the placenta next to the uterine wall of the mother.
In this are intervillus blood spaces, which may be regarded
as derivations from the eroded maternal blood
vessels. In the non-pregnant state the uterus is supplied
with branches from the internal
iliac artery, which end
in capillaries in the wall of the
uterus. In the pregnant state
the numerous branches of the
arteries supplying the uterus
do not end as capillaries, but
pierce the basal plate of the
placenta, where the arterial vessels
lose their muscular coat and
open directly into the intervillus
or intraplacental blood
spaces. Maternal capillaries
are wanting within the placenta,
since they become early replaced
by the intervillus
spaces. The maternal blood is
carried away from these spaces
by wide venous channels, forming
networks from which proceed
the larger venous trunks.
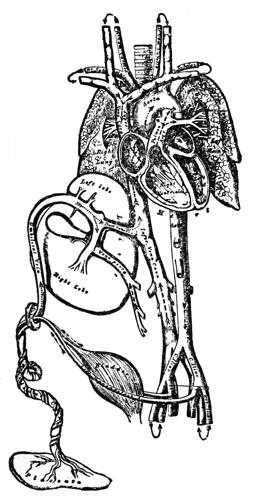
Fig. 44—Plan of the foetal
circulation. (Gray)
The foetal portion of the placenta is that portion next
to the child. Here end the terminal loops of the foetal
blood vessels, the blood being conveyed to and from the
placenta along the umbilical cord, by the umbilical
[146]
arteries and vein. Although coming into close relation,
the blood streams of the mother and of the child never
actually mingle, because of the delicate septum which
intervenes. The delicate septum, however, allows the
free interchange of gases necessary for the respiratory
function as well as the passage of nutritive substances
into the foetal circulation.
The umbilical cord connects the body of the foetus
with the placenta, and conveys the foetal blood to and
from the placenta to the child. This blood is carried by
means of two umbilical arteries and one umbilical vein.
The umbilical vein originates by means of capillaries
in the placenta, traverses the cord and enters the body
of the child at the umbilicus. The umbilical vein now
enters the substance of the liver and passes from that
organ to the ascending vena cava by means of the ductus
venosus. The blood now enters the right auricle of the
heart and the eustachian valve is so placed that this
blood is thrown directly into the left auricle of the heart,
from there into the left ventricle, and out into the aorta
to find itself in the general circulation of the child. The
blood coming from the upper extremities of the child
finds its way into the right auricle of the heart by means
of the descending vena cava, thence into the right ventricle,
and out into the pulmonary artery. This artery
after birth will lead the blood to the lungs, but before
birth, in as much as the lungs are not functioning, the
lungs can not accommodate this amount of blood, so it
passes directly into the arch of the aorta by means of
the ductus arteriosus, and thence into the general circulation.
[147]
The umbilical or hypogastric arteries leave the
internal iliacs, pass one on each side of the bladder to
the umbilicus, and thence down the cord to the placenta,
end there in capillaries, where the blood is now purified,
and nourished for its return flow.
The Collateral Circulation.
—By collateral circulation
is meant the anastomoses of arteries, or veins through a
side branch. There are three great arterial collateral
circulations in the body. One is in the arm, the deep
brachial artery, and the anastomotica magna, coming off
of the brachial artery and anastomosing with the recurrent
radial and ulnar artery. One is in the leg, the deep
femoral artery, and the anastomotica magna coming off
of the femoral artery and anastomosing with the recurrent
anterior and posterior tibial arteries. One over the
front part of the body, the superior and inferior mammary
arteries branches of the subclavian artery and anastomosing
with the superior and inferior epigastric
arteries, branches of the external iliac and femoral arteries.

Fig. 45—Collateral anastomosis of veins
(Poirier and Charpy)
The Lymphatic Circulation.
—The lymphatic system is
a system of vessels which occurs abundantly in almost all
portions of the body and converge and anastomose to
form two or more main trunks, which open into the subclavian
[148]
veins just before they are joined by the internal
jugular. The vessels contain a fluid termed lymph, usually
colorless and containing numerous white blood corpuscles
known as lymphocytes.
In those vessels which have their origin in the wall of
the small intestines, the contained fluid has, especially
during digestion, a more or less milky appearance, owing
to the lymphocytes being loaded with particles of fat
which they have taken up from the intestinal contents.
On this account, these vessels are usually spoken of as
lacteals, although it must be recognized that they are
merely portions of the general lymphatic system.
In certain respects the vessels of the system strongly
resemble the veins. They arise from a capillary network,
their walls have a structure closely resembling that of the
veins, they are abundantly supplied with valves, and it
may be said that the fluid which they contain flows from
the tissues towards the subclavian veins. With these
similarities there are combined marked differences. One
of the most important of these consists in the fact that
the capillaries of the lymphatics are closed and do not
communicate with any other set of vessels as the venous
capillaries do with the arterial; and another important
difference is to be found in the frequent occurrence upon
the lymphatic vessels of characteristic enlargements, the
so-called lymphatic nodes or glands, quite different from
anything occurring in connection with the veins.
Throughout the body spaces of varying size are found,
containing a clear, more or less watery fluid, which are
called lymph spaces. These spaces do not communicate
[149]
with the capillaries of the lymphatics, but are in such
close relationship with them that the fluid easily finds its
way into the lymph capillaries by osmosis, absorption,
lymphocytes going out into these spaces and returning
filled with the lymph fluid.
The lymphatic capillaries, which are arranged in the
form of networks of very different degrees of fineness and
complexity, closely resemble in structure the blood capillaries,
their walls consisting of a single layer of endothelial
cells. They differ from those of the blood vascular
system not only in their ultimate branches being closed,
but also in their general appearance. They are of greater
caliber.
The lymph vessels, which issue from the capillary networks
and convey the lymph ultimately to the subclavian
veins, have the arrangement closely resembling that of
the veins; the larger ones are usually situated alongside
and accompany the course of the blood vessels. Just as
the veins unite to form larger trunks as they pass from
the capillaries toward their termination, so, too, the lymphatics,
but the lymphatics present two peculiarities
which distinguish them from the veins. They do not
anastomose as abundantly as veins and there is not the
same proportional increase in the size of the lymphatic
vessel. The left trunk or thoracic duct is much larger
than the right, beginning in the abdominal region and
traversing the entire length of the thorax to reach its
destination. It receives all the lymph returned from the
lower limbs, the pelvic walls and viscera, the abdominal
walls and viscera, the lower part of the right half and
[150]
the whole of the left half of the thoracic viscera, the left
side of the neck and head, and the left arm. The other
trunk, the right lymphatic duct, is very short and sometimes
wanting. It receives the lymph from the upper
part of the right side of the thoracic wall, from the right
half of the thoracic viscera and the upper surface of the
liver, the right side of the neck and head, and from the
right arm. The structure of the larger lymphatic vessels
is similar to the veins, but, as a rule, their walls are
thinner than those of the veins of corresponding caliber
and their valves are more numerous. The walls of the
most robust trunks, particularly those of the thoracic
duct, consist of three coats. From within outward these
are: (a) the intima, composed of the endothelial lining
and the fibro-subendothelial layer; (b) the media, made
up of involuntary muscle interspersed with fibro-elastic
tissue; and (c) the adventitia, consisting of fibro-elastic
tissue and longitudinal bundles of involuntary muscle.
Lymphatic nodes are scattered along the course of
the lymphatic vessels, found in various regions of the
body as elliptical flattened nodules of varying size. The
embalmer will meet with these in the axillary and inguinal
regions, or when he is raising the axillary or
femoral arteries.
[151]
PART III.
EMBALMING
[153]
Embalming
The central thought of the modern funeral director
in the care of the dead and in all the arrangements of
the funeral is to remove so far as may be all that is necessarily
painful to those who must place out of sight the
body through which the soul of the dear one has expressed
itself, in all the ways that are prompted by
affection. This does not seem to have been the case in
the former days when the methods were in striking contrast
to those of today and were such as would intensify
the suffering of the living. Beginning with the arrangement
of the body in the room made cold by nature in
winter or by the ice box in the summer and ending by
lowering the body into an unlined grave, each detail
seems to have been made with little thought of lessening
the pain caused by those things which necessarily
have to be done. Perhaps the central thought in
the old days was the same as that which was the comfort
offered upon funeral occasions by a former local
pastor which was “death is a horrible thing.” If this
was not the controlling thought, it is certain that many
details of former funeral customs would be considered
[154]
horrible today. Today the aim is to lighten the burden
and to cheer the hearts of those who mourn.
The introduction of embalming in the seventies has
been of untold benefit in improving the environment
of the dead prior to interment. Recollections of the use
of the old ice box, the crude and cumbersome cooler,
the ice water to be cared for and the thought of the
chilled body are not pleasant now, and were far from
pleasant then to those into whose homes death had entered
in hot weather. In winter natural cold was depended
upon, the body being placed in the coldest place
possible. With the best of care the results were uncertain
and far from satisfactory. Modern embalming has
changed all this. Its results are with rare exceptions
certain and satisfactory and the embalmed body may be
dressed and placed in a warm and comfortable room.
[155]
CHAPTER X.
MODES, SIGNS AND TESTS OF DEATH.
Just as surely as we are born, just so surely must
we die, and just as it is the physician's duty to care for
the living body, if possible to keep it in a strong and
healthful condition, so it is the embalmer's duty to care
for the body after death, not so much for the body itself,
but from a sanitary standpoint, namely, to see that the
body is well disinfected and embalmed so that there
will be absolutely no chance for the spread of disease.
Any one who is familiar with hospital work must know
that all do not die in the same way. For some it is the
long lingering disease, chronic in form, which after a
long and tedious course the thread of life is finally
broken, and we hardly know the instant at which the
change was completed. For others, it is the short, acute
attack, which snaps the life away in a very instant,
only after a very short duration. For some it is to die
from accidental causes, while for others it is only the
passing out from the period of old age. For some the
mind may be active and the intellectual faculties useful
up to the last moment, while for others the contrary
is all but too true.
Although there may be many different kinds of
disease infecting the human race, yet we find that death
[156]
ultimately results from the stoppage of any one, or maybe,
all three of the vital organs, namely the heart, brain
or lungs. Anything whatsoever which plays upon the
body, to such an extent, as to affect the functions absolutely,
of either the heart, brain or lungs, will result
in the death of that body. And since these organs are
of such vital importance to us, and since the stoppage
of any one of them will result in death, they have been
termed the vital organs.
Modes of Death.
—There are, then, only three modes
of death: syncope, or the stoppage of the heart; coma,
or the failure of the brain to perform its functions; apnea,
or the stoppage of the lungs.
Syncope.—For the heart to properly perform its
function, namely that of propelling the blood to all parts
of the body, it must first be properly nourished itself.
If for any reason the heart does not get this proper
nourishment, say the coronary arteries should become
clogged, or a fatty infiltration, or a lack of red blood corpuscles,
we would have a condition in the body known as
anemia.
The heart must also have a proper nerve supply from
the brain, and if because of any disease, the vaso-motor
or the vaso-constrictor fibers should become affected,
the heart would cease to contract and expand, and hence
the complete stoppage of the heart. A condition of this
kind is known as asthenia.
But whether it is death by anemia or asthenia, the
state of suspended animation, common to both these forms
is expressed by the single term—syncope.
[157]
Coma.—In cases of apoplexy, where we have the blood
escaping from the ruptured vessels, compressing the brain,
we find death ensuing. Also in accidental cases such
as fracture of the skull, the injury will often cause death.
These are examples of coma, and can be explained in
this way, viz.; the power of the brain becomes inactive
either through the result of an injury or a disease, and
when this inactivity occurs the respiratory apparatus subsides
and the heart deprived of its normal stimulus
through the vaso-motor and constrictor fibers, soon ceases
to beat, and death is the result.
Apnea, Asphyxia.—If for any reason the supply of
oxygen is cut off from the lungs, we will have the body
dying the result of asphyxia or apnea. The most common
forms found of this mode of death are those of hanging,
drowning or coal gas poisoning.
Signs of Impending Death.
—The signs of impending
death are those conditions which exist on the body or
the peculiar features of the body which aid the physician
in ascertaining the exact condition of the body.
These signs assume many different forms and in no two
instances may they be found alike. They of course, are
not positive in themselves, but are sufficient to guide us
in forming an opinion as to the approach of death.
One of the first signs to be noticed is the coldness of
the extremities. In this case the coldness begins at the
extreme tips of the fingers and toes and gradually extends
toward the trunk. This, of course, is due to the
gradual diminishing activity of the heart to propel the
blood to the extremities.
[158]
The brain also fails to receive its proper blood supply
and becomes weakened and we find the mind wandering.
This wandering results in the patient going through
movements representing the playing with flowers, or picking
at the bed clothing. A further result of this weakness
is that the patient may have visions of angels and heaven.
Speech begins to grow thick, and a large lump of
phlegm gathers in the throat.
The hands now feel cold and clammy, and if they
are raised they instantly fall. One cannot detect the act
of respiration, as the movements of the thoracic walls
are so slight as to be scarcely perceptible.
The heart loses its power to propel the blood and
the stoppage of every organ in the body ensues.
The eyes become fixed with a staring look as though
they were not focused on anything directly. The eyes
lose their lustre on account of the lachrymal glands refusing
to secrete.
The vital organs, the heart, brain and lungs come
to a halt, and we find the body passing from life to the
great beyond.
Tests of Actual Death.
—From the large number of
statistics that have been gathered together for our purpose,
we find that the time of greatest mortality is in
the early morning hours between three and six A. M.,
for it is between these hours that the body is in a perfect
state of relaxation, and at the lowest ebb of vitality.
The time of least mortality is between the hours of
eleven and two P. M., as the body is in a relatively high
state of vitality during these hours.
[159]
The tests of actual death can be placed in two classes,
the common tests and the expert tests.
The common tests are those that have long been used
by the inexperienced to ascertain the fact of death. They
are not necessarily conclusive in themselves, but when
all are taken together there can not be much doubt.
(a) The Feather Test.—In this test a feather is
held to the nostrils to observe whether it moves. The
feather being so light, the slightest respiration of the
lung would be apt to move it.
(b) The Mirror Test.—In this test a mirror is held to
the mouth and nostrils. If moisture collects on the mirror
it is evident that respiratory movements are going on.
If there is an absence of moisture we are quite safe in
saying that the patient is dead.
(c) The Bandage Test.—In this test a bandage is
placed around the arm and then twisted very tightly.
If there is the slightest circulation existing in the body
the blood will accumulate back of the bandage in the
venous system and thus demonstrate the fact. There
will also be no swelling or discoloration beyond the
ligature.
(d) By placing the ear to the chest over the heart,
no sounds will be heard.
(e) If the ear is applied over the lungs, no sounds
will be heard.
(f) If a cup of water is placed on the chest there
will be no movement of rays or ripples on the surface.
(g) If the skin is cut, no blood will flow, nor will the
wound close.
[160]
(h) If heat, say for instance a burning match be
applied to the skin it will not blister, or if ammonia is
hypodermically injected under the skin there will be no
redness, but rather the skin will turn to a yellowish
color.
(i) The living hand when held to the light shows
pink through the inner edges of the fingers, but with
the dead hand it shows opaqueness.
(j) When a strong light is brought before the eye
the pupil of the eye will not dilate or contract.
(2) The expert tests are those which a doctor or
coroner might use to ascertain the fact of death. These
tests are made with the stethoscope and the ophthalmoscope.
(a) By the use of the stethoscope the physician can
hear the sounds of the heart and if there is the slightest
sound he can detect it. In the absence of any sound the
body is pronounced dead.
(b) By the use of the ophthalmoscope the physician
is enabled to look into the pupil of the eye and if there
is life he can see the blood circulating through the tiny
capillaries of the retina. If he does not see this capillary
circulation he is quite safe in saying the body is dead.
(c) Another method consists in the hypodermic or
intravenous injection of certain substances, and ascertaining
whether these substances have been dispersed
throughout the body. If they have, then a circulation
exists and life continues, although the pulsation of the
heart may not be detected by auscultation. Among the
[161]
substances recommended for injection are fluorescin,
sodium iodide, lithium iodide and potassium ferro-cyanide.
The injection of the small quantities as used will not
cause death should the patient still be living.
Fluorescin is usually injected, one gramme dissolved
with an equal weight of sodium carbonate in eight cubic
centimeters of water, and the whole quantity injected
hypodermically. If the circulation is persisting, the
skin and the mucous membranes after a very few minutes
assume a greenish color; about twenty minutes after
the injection, the portion of the eye within the iris assumes
a green color from penetration of the fluorescin
into the vitreous and aqueous humors, and in the blood
the fluorescin may be detected by the following method:
One or two threads of cotton are passed under the skin
in the form of a seton, and when saturated with blood are
transferred to a test tube, and boiled with a little water.
As the liquid clears the green color of the fluorescin becomes
evident, if that substance has been absorbed into
the blood.
(d) Another method for the distinction of real from
apparent death consists in picking up a fold of the skin
and compressing it with a pair of artery forceps. If the
skin does not completely settle down, and if the fine
furrows produced by the teeth of the forceps continue
indefinitely, then death has occurred. Whereas, if the
circulation is continuous, the fold and the marks of the
forceps would disappear. Moreover, if death has occurred
the portion of the skin compressed by the forceps
assumes a parchment-like appearance.
[162]
(e) The electrical current affords a means of determining
death. It is now known that the muscles, after
cadaveric rigidity has set in, do not respond to electric
stimuli. The faradic current will cause, when death has
occurred, muscular contractions until a short time before
post-mortem rigidity occurs. The faradic stimulus is lost
first and the galvanic stimulus soon after. We may be
enabled to approximate the time at which death occurred,
for, if we find any response to either the faradic or the
galvanic current, we know at once that post-mortem
rigidity has not yet occurred.
No person should be buried as long as the muscles
contract when stimulated by either the faradic or the
galvanic current. If the electrical test were always applied
before a death certificate was signed, there would
be absolutely no possibility of a person being buried alive
and the public would soon lose the morbid fear of such
an occurrence.
Later and More Positive Signs.
—(a) After a few hours
the blood gradually sinks to the dependent parts of the
body giving a reddish-blue discoloration, known as post-mortem
discoloration, or cadaveric lividity.
(b) The eyes become sunken in the sockets, the eye
balls become flattened, the cornea opaque and the pupil
irregular in shape.
(c) The eyelid loses its elasticity, and the white transparent
color of the conjunctiva is lost, often becoming
black or gray.
(d) Rigor mortis may or may not be present.
[163]
(e) The body gradually cools to the temperature of
the surrounding atmosphere.
(f) On opening an artery it is generally found to
be empty after death.
(g) The latest and most positive sign of all is putrefaction,
and when this is found to be present all other
signs may be ignored.
(h) Skin slip present on the body is only another
manifestation of putrefaction, and also signifies that the
body is dead.
[164]
CHAPTER XI.
PREMATURE BURIAL.
Premature Burial.
—In this enlightened age, with our
knowledge of respiration and the circulation of the blood,
with our complete mastery of the phenomena of death
with scientific tests, it is absolutely impossible to have
such a thing as a premature burial.
Nevertheless from the earliest times the fear of premature
burial has been felt by many, and curious and strange
methods have been adopted to prevent the possibility of
individuals being consigned to their graves before life
was extinct.
Tradition records many cases where, in spite of their
precautions, such unfortunate actions have happened. It
may be that tradition is an uncertain and erring guide.
And yet underlying all tradition, as Dieulafoy said, is a
solid substratum of truth which the thoughtful investigator
must take into consideration. The tale of the
Cologne goldsmith's wife, that survives in the legend of
the neighing horses, may be weird, bizarre, and from a
scientific point of view, demonstratively ludicrous, but
its germ is to be found in the recorded fact that in times
of epidemics, when the dying were huddled away with the
[165]
dead, mistakes did occur, and one or two were rectified
by the resurrection of the “dead.” In cases where burial
took place in commodious family vaults, the changes in
the position of the coffin, produced by atmospheric and
other physical factors and were startlingly disclosed when
the vaults were opened to receive new bodies, doubtless
gave an impetus to the belief in the comparative frequency
of such mistakes. The medical man remembers that on
occasions he has found it difficult, without applying some
of the common and finer tests, to certify death in a
patient dying of a lingering disease, but his knowledge
forbids him believing that such difficulties as he may
have experienced in his own practice can ever have
caused his fellow practitioner to make so grievous a mistake
in a similar case. The public has no such knowledge;
it relies on the exceptional cases and glibly credits the
statement—true enough in a limited sense that there is
no certain proof of death. While it is certainly true that
no single sign can be absolutely relied upon to prove that
life is extinct, all practitioners will agree that several
signs taken in combination and methodically applied are
sufficiently accurate to obviate the possibility of mistake.
Much has been made of the cataleptic condition and the
probability of mistaking it for death, which has formed
the basis of one of Poe's narratives. As a matter of
fact, catalepsy, of such a nature as to be confounded
with tota exitus, is extremely rare—so rare that we
doubt if any practitioner with a large experience of nervous
conditions has met with more than one or two instances.
Further, even in such extremely rare conditions,
[166]
the usual tests are applicable and to the trained medical
man at least clearly prove the nature of the case. The
stethoscope and the mirror held in front of the patient's
mouth are usually sufficient to demonstrate that the patient
is alive and we should want more conclusive evidence
than such as has been brought forward up to the
present, to feel that cataleptic patients have been consigned
to their coffins before life was totally extinct.
Newspaper writers delight in the fictitious and marvelous,
and without any regard whatever to the scientific
phase of the subject, frequent mention of cases of premature
burial is to be found almost daily in the press of
the country. But upon investigating these newspaper
stories, it will be found that they have been either originated
in the fertile brain of some reporter or were
merely published to consume space.
[167]
CHAPTER XII.
THE CHANGES IN THE BODY AFTER DEATH.
Cooling of the Body.
—The internal temperature of the
healthy living being is about 37 degrees centigrade. But
it may be increased several degrees in consequence of disease.
After death the chemical changes upon which the
maintenance of this temperature depends rapidly diminishes,
and the body gradually cools to the temperature of
the surrounding atmosphere. This usually occurs in from
about fifteen to twenty hours, but the time required depends
upon a variety of conditions. Immediately after
death there is, in nearly all cases, a slight elevation of
internal temperature, owing to the fact that the metabolic
changes in the tissues still continue for a time, while
the blood ceases to be cooled by passing through the lungs
and peripheral capillaries. After death from certain diseases
yellow fever, cholera, rheumatic fever, and tetanus,
a considerable elevation of internal temperature has been
repeatedly observed.
The time occupied by the cooling of the body may
be prolonged after sudden death from accidents, acute
diseases, apoplexy, and asphyxia. A number of cases is
reported in which the body retained its heat for several
days without known cause.
[168]
After death from wasting chronic diseases, and in
some cases after severe hemorrhage, the cooling of the
body is very rapid, the internal temperature being reduced
to that of the surrounding air within four or five
hours.
Fat bodies cool less quickly than lean ones, the bodies
of well nourished adults less quickly than those of children
or old persons. The temperature of the surrounding
atmosphere, the degree of protection of the body from
currents of air, of course, modify the progress of cooling;
and the internal organs naturally retain their heat longer
than the surface of the body. The rate at which cooling
occurs is most rapid as a rule, during the hours immediately
following death, notwithstanding the postmortem rise
which may ensue.
Cadaveric Lividity.
—This means the black and blue
discoloration from the effects of the congestion or contusion
of the blood.
After life becomes extinct, and before the blood coagulates,
it changes its position chiefly in two ways: First,
it is driven by their contraction out of the arteries and
into the veins; second, it settles in the veins and the
capillaries of the more dependent parts of the body,
inducing, usually within a few hours after death, a mottling
of the surface with irregular livid patches. These
patches may coalesce, forming a uniform dusky red color
over the back of the trunk, head and extremities, and
sometimes over the ears, face and neck. The same effect
is noticed on the anterior aspect of the body if it has
lain on the face. At points of pressure, from the folds in
[169]
the clothing, and from the weight of the body on the
bed or the cooling board, the red color is absent or less
marked. This to the undertaker and the embalmer is
known as postmortem discoloration. These changes
occur before putrefaction sets in. This cadaveric lividity
should not be mistaken for the antemortem ecchymoses
from which it may usually be distinguished by its position
and extent by the fact that the surface of the skin
is not elevated, and by the fact that on incision no blood
is found free in the interstices of the tissues. Not infrequently
the subcutaneous tissue in the neighborhood
of these postmortem discolorations become infiltrated
with a reddish serum. Very soon after death, particularly
in warm weather, the tissues immediately around the
subcutaneous veins of the neck and the thorax and in
other situations, may become stained a bluish red color
from the decomposition and escape from the vessels
of the coloring matter of the blood. This to the undertaker
and the embalmer is known as postmortem discoloration.
Putrefactive Changes.
—As soon as the body dies, it
becomes as any other inanimate object, subject to putrefaction
and decay.
The tissues of the body undergo various changes
as to consistency of the solids, semi-solids, fluids, and as
to color.
Putrefactive changes are caused by the presence of
putrefactive germs normally present in the tissues or gaining
access to them, which in their effort to satisfy their
[170]
own nutrition, break down those complex molecules of
which the tissues are composed into simpler compounds.
Putrefaction then is organic decomposition or decay
the result of putrefactive bacteria. Putrefaction may also
be defined as the separating of the constituent elements of
the body due to the presence and growth of bacteria.
Although septic changes may take place before the
death of a body, yet the term putrefaction is not applied
until after the death of a body, and denotes those changes
in color, consistence, and smell so clearly perceptible.
Usually in from one to three days, depending upon
circumstances, a greenish discoloration of the skin occurs
at first upon the middle of the abdomen, over which it
gradually spreads, assuming a deeper hue, and often
changing to greenish purple or brown. Greenish patches
may now appear on the different parts of the body,
earliest upon those overlying the internal cavities; this
discoloration is probably produced by the action on the
haemoglobin of gases developed by decomposition.
The eyeballs now become placid and if the eyelids
are not closed the conjunctiva and cornea become brown
and dry. The pressure of gases developed by decomposition
in the internal cavities not infrequently forces a
greater or less quantity of frothy, reddish fluid or mucous
from the mouth and nostrils, distends the abdomen, and,
if excessive, may lead to changes in the position of the
blood in the vessels and even a moderate amount of displacement
of the internal organs.
After five or six days, under ordinary circumstances,
the entire surface is discolored to a green or a brown.
[171]
After this the epidermis becomes loosened through the
formation of gases and separating of fluids beneath, and
the tissues become flaccid.
The abdomen and the thorax may be greatly distended,
and the features distorted and scarcely recognizable
from swelling, and the hair and nails loosened.
On the interior of the body, those soft and less compact
tissues, or those tissues in which there is a great
amount of fluid, are the first to decompose. This may be
noticed by examining the walls of the trachea, esophagus
and the intestines and noting the change in color.
Decomposition of the soft and liquid portions of the
body take place almost immediately after the death of
the body, and then follow in rapid succession the decomposition
of the semi-solids and finally the solids. Beyond
this stage of putrefaction, the consecutive changes can
scarcely be followed with accuracy.
The putrefactive changes can not be said to begin at
the same place in all bodies, as the conditions under which
death occurred will regulate that. The rapidity with which
these changes follow one another depends upon a variety
of conditions such as temperature, moisture, access of air
and the diseases which have preceded or caused death.
Various temperature relations will effect greatly the
more or less rapid decomposition of the body. Bodies
dying in mid-summer are decomposed much more quickly
than those dying in mid-winter.
Moisture added to the temperature relation will hasten
the rapidity of the decomposition as can be noticed in
[172]
those localities with a high temperature but moist climate
that the decomposition takes place very quickly.
In those climates with high temperature, but dry or absence
of moisture, the tendency is to dry up the tissues,
and instead of putrefaction we have mummification as
the result. This last statement then serves to explain
the reason for the high state of preservation in the forms
of mummification as exists in those countries like Egypt
with their extremely hot and dry climates.
Exposure added to the temperature and the moisture
relations adds greatly to the rapidity of the decomposition.
A moist climate with a hot temperature and free
exposure favors rapid decomposition. We notice that
putrefaction progresses much more rapidly in the air than
in the water and in the earth its progress is slower than
in the water. The more exposed a body is then, to the
elements, especially the air, the more rapid will be the
decomposition.
An elevated temperature and the presence of air and
moisture hasten the advent and progress of putrefactive
changes.
Bodies dying in high fever and edematous subjects
are much more quickly decomposed than those dying
with the ordinary wasting away disease.
The bodies of infants usually decompose more rapidly
than those of adults, fat bodies more rapidly than lean
ones.
The infectious diseases, intemperance, and the puerperal
condition promote rapid decomposition as also does
death from suffocation.
[173]
Poisoning from arsenic, alcohol, antimony, sulphuric
acid, strychnine and chloroform may retard the progress
of decay.
It is impossible, then, to say how long a body will
keep without the use of preservatives, as it depends partly
upon temperature, partly upon moisture, partly upon the
amount of exposure and partly upon the conditions existing
in the body before death.
We can easily understand the reason for all this if we
understand the bacteriology relating to the subject.
In the first place, bacteria require for their best and
most rapid growth the proper temperature, moisture and
media relations. By this we mean that the temperature
should be moderately warm, ranging from about forty to
one hundred degrees Fahrenheit, the optimum being about
the body temperature 98.6 degrees Fahrenheit or 37 degrees
on the centigrade scale. With this optimum temperature,
the element of moisture should always be present,
as we find that nothing in nature will germinate
without the necessary moisture. Then the bacteria must
have the proper media, meaning that they must have the
right substance on which to grow. Inasmuch as the
cause of putrefaction is the host of putrefactive bacteria
which abound trying to satisfy their own nutrition, and
since these bacteria require a moderately warm and moist
media on which to grow, it is only natural that putrefaction
and decomposition should occur much more rapidly
in warm moist climates than in dry cold climates.
In regard to exposure we learn that certain putrefactive
bacteria are aerobic in character, i. e., that they
[174]
need a great quantity of oxygen for their growth, and
for this reason a body in water or buried in the earth
does not decompose as rapidly as one exposed to the air.
But although they do not decompose as rapidly yet
we find that they do decompose in time. This is due
to the fact that there is another class of bacteria, called
anaerobic, i. e., which do not need oxygen for their growth.
In the case of the body in water these anaerobic bacteria
exist and develope slowly in the alimentary tract, and
eliminate gases sufficient to bring the body to the surface,
where the aerobic bacteria enter, and putrefaction
progresses much more rapidly.
The starting point of decomposition is usually at the
seat of the disease the subject had before death, but it
soon spreads to all the various tissues of the body.
Putrefaction is always accompanied by a great amount
of odor, which is caused by the generation of gases the
result of bacterial action. The obnoxious gases, offensive
to the smell are sulphureted hydrogen, nitrogen, carbonic
acid and ammonia.
The material actually present when the body is actually
decomposed has been determined as being water, nitrogen,
methane, carbon dioxide, etc.
Treatment by the Embalmer.—Putrefaction always
means that there is present a great amount of putrefactive
bacteria and if you are to arrest this condition
you must resort to the most thorough embalming. By
placing some preservative fluid in the arteries and having
a thorough circulation all the tissues of the body can be
[175]
reached and hence the complete destruction of those
bacteria causing the putrefaction.
If all the tissues are properly bathed with embalming
fluid there need be no further danger of putrefaction;
but what seems sometimes at first a thorough circulation,
proves afterward to be only a partial one. If after several
days the body still shows signs of decomposition it is
best to reinject or if the decomposition only occurs in spots
a simple hypodermic injection will prove adequate.
Skin Slip.
—To properly understand the causes of skin
slip a thorough knowledge of the structure of the skin is
necessary. It would be best then to turn to the chapter
on the tissues of the body and study the minute structure
of the skin.
Skin slip is caused by a putrefactive softening of the
epidermis. There is a watery infiltration from the minute
capillaries and the surrounding tissues between the
dermis and the epidermis, causing the latter to loosen and
if touched to slip and tear away from the dermis or true
skin.
Many embalmers have been led to believe that the
slipping of the skin is due to the use of certain fluids
used in injecting the arterial system. This error should
be corrected, as it is most generally the absence of the
fluid from the part which results in the slipping of the
skin.
Diseases of the heart, liver, kidney and dropsical
conditions predispose to the early skin slip. The immense
amount of water occurring in the minute capillaries of
[176]
the skin prohibits the embalming fluid from reaching
the tissues.
Skin slip then is due to putrefactive changes occurring
in the skin, and if it should occur after embalming, it is
positive proof that the part or parts have not received a
sufficient quantity of a preservative fluid.
Treatment by the Embalmer.—In the average case
you will never see skin slip, because you will be called
comparatively soon after death has occurred and the body
will be embalmed and buried before this later form of
putrefaction will manifest itself. But in some few cases
you will have to keep the body for a greater length of
time, say to await the arrival of some friend living abroad,
or it may be a coroner's case. In cases like this the
body being kept for a period of weeks, will if it is not
perfectly embalmed show signs of skin slip. As has
been stated above, cases that die from diseases causing
dropsical infiltration in the subcutaneous tissues should
also be handled carefully. If you are aware before hand
that you are to keep the body for a great length of time
or that you have a dropsical subject, a little formaldehyde
should be added to the fluid that is injected, about
two or three ounces to each quart of fluid. Zinc compounds
might be added, but formaldehyde is better because
of its great affinity for water.
If skin slip occurs after the body is embalmed it is
best to place a layer of cotton over the part where the
skin slip occurs and saturate the cotton with equal parts
of alcohol, formaldehyde and glycerine.
[177]
In drowned cases where all the skin is slipping it is
best to envelope the whole body with a layer of cotton
saturated with formaldehyde.
Rigor Mortis.
—Rigor mortis is the stiffening condition
which occurs on the body after death.
When the muscle substance dies it becomes rigid, or
goes into a condition of rigor; it passes from a fluid to
a solid state. The rigor that appears in the muscles after
somatic death is designated usually as rigor mortis, since
its occurrence explains the death stiffening in the cadaver.
It is characterized by several features: the muscles become
rigid, they shorten, they develope an acid reaction,
and they lose their irritability to stimuli.
After the death of an individual the muscles enter
into rigor mortis at different times. Usually there is a
certain sequence, the order given being the jaws, neck,
trunk, upper limbs, lower limbs, the rigor, therefore,
taking a downward course. The actual time of the appearance
of the rigidity varies greatly, however; it may
come on within a few minutes or a number of hours may
elapse before it can be detected.
Death after great muscular exertion, as in the case
of hunted animals, or soldiers killed in battle, is usually
followed quickly by muscle rigor. Death after wasting diseases
is also followed by an early rigor, which in this
case is of a more feeble character and shorter duration.
Certain drugs such as veratrum, hydrocyanic acid, caffeine
and chloroform, will hasten the development of
rigor.
[178]
People who die in full habit, meaning that there has
been no muscular exertion or wasting processes before
death, usually have the rigor developing more slowly and
of a longer duration.
After a certain interval, which also varies greatly,
from one to six days, the rigidity passes off, the muscles
become soft and flexible; this phenomenon is known as
the release of the rigor.
The usual explanation that is given of rigor is that it
is due to a coagulation of the fluid substance, the muscle
plasma, of which the fibers are constituted. During life
the fluids exist in a liquid or viscous condition; after
death they coagulate into a solid form.
Rigor mortis is not a sign of death, as there is rigidity
of the muscles following apparent death, as in cases
of asphyxia and trance. If the body is rigid, in a case
in which there is a doubt that death is present the rigidity
may be broken up. If it is a case of trance or that of
the contraction of the muscles following drowning, it is
likely to return, especially in case of trance; but if death
is actually present it will not return.
The chemical changes occurring, the result of rigor
mortis can be briefly stated:
(a) There is a coagulation of the proteid material
of the muscle plasma.
(b) There is an increased acidity, which is doubtless
due to the production of lactic acid.
(c) There is a production of carbon dioxide.
(d) There is a consumption of glycogen.
[179]
Treatment by the Embalmer.—Many times when
called to embalm a subject you will find the body in a state
of rigor. In cases of this kind the rigor mortis should be
broken up. This can be done by taking each of the joints
and gradually bend them a little at a time until they become
perfectly lax. Once a joint is bent the stiffening
disappears and the embalmer can proceed.
Fermentation and the Production of Gas.
—A molecule
is the smallest portion of a compound which can exist
by itself.
An atom is one of the ultimate particles composing a
molecule. A complex molecule is one in which two or
more elements have been combined. Example: water
molecules are formed by two atoms of hydrogen and
one atom of oxygen.
A ferment is a substance causing fermentation in
other matter with which it comes in contact. There are
two kinds of ferment expressed by the names organized
and unorganized.
Unorganized ferments are chemical substances having
the power to produce or assist in the production of fermentation.
Organized ferments are bacteria having the power
to produce fermentation.
Fermentation means the process through which complex
molecules are decomposed and their ingredients disassociated
by the action of ferments. As an example of
fermentation, we can take proteid food substances, the
molecules of which are always of complex form, and
by subjecting them to the action of organized ferments
[180]
(bacteria), decompose them, and separate each gas ingredient,
obtaining therefrom a variety of gases from
what was formerly a substance of perfect chemical union.
Fermentation is present in most of the natural processes
whereby chemical changes are produced in animal and
vegetable matter. Fermentation is taking place all the
time in all the climes excepting possibly the frigid zones.
The organized ferments (bacteria) are subject to the same
temperature limits that govern the reproduction and the
growth of all bacteria.
Fermentation is divided into spirituous fermentation,
digestive fermentation, metabolic fermentation, and putrefactive
fermentation.
Spirituous Fermentation.
—Spirituous fermentation
is that process of fermentation by which forms of yeast
cells, by their growth and reproduction in such complex
substances as grapes, fruit, apple juice, grains, etc., extract
alcohol from these substances and by this process
produce wine, cider, spirits, etc. Many times in the dead
body, spirituous fermentation occurs. Spirituous fermentation
is caused by a vegetable parasite called yeast.
Digestive Fermentation.
—Digestive fermentation is
that process by which digestion and nutrition in the living
body is assisted through the action of ferments called
enzymes, acting on the food substance. This process is
mainly one where each food particle is split up by a
particular ferment or enzyme. After death this process
may continue for a certain length of time and result in
the formation of gas. Digestive fermentation is mostly
chemical.
[181]
Enzymes are unorganized ferments and are cast off
the living body within the living body.
—Metabolic fermentation
is that process by which enzymes in the tissues of the
living body destroy the dead cells, and reduce them to
the following gases: nitrogen (N), carbon-dioxide
(CO2), ammonia (NH3), uric acid, and other materials.
In the living body these gases and other products are
eliminated from the tissues, by the sudoriferous glands
and ducts through perspiration, by the lungs with the
expired air, by the intestines with the feces and by the
kidneys with the urine. In the dead body the enzymes
become active agents in tissue gas production, unless
they are kept in restraint by being brought in contact
with germicidal embalming fluids.
Putrefactive Fermentation.
—Putrefactive fermentation
is the process by which undigested food substances
(principally proteids), under the influence of ferment
bacteria, yield gases. This change rarely takes place in
the small intestines of the living body as the germs are
held in restraint by lactic acid and acetic acid bacteria in
those parts. There is little restraint to their activity in
the large intestines, however, and the intestinal gases
along with putrefactive changes in fecal material are a
natural consequence.
Intestinal fermentation is hastened in the dead body
by the presence of much undigested food and the absence
of any restraining organisms. The gases produced
in the intestines of either the living or dead body by the
action of putrefactive ferment bacteria are: carbon-dioxide
[182]
(CO2), hydrogen (H), nitrogen (N) hydrogen
sulphide (H2S), methane (CH4). The continued fermentation
in the stomach and the intestines causes a
coffee colored material of a frothy character to purge from
the mouth.
When the hollow needle or trocar is used to reach the
scene of ferment activity, the gases mentioned are released
from the effected organs. As these gases are extremely
odorous, they should be passed through a pledget
of cotton saturated with formaldehyde, before being
allowed to pass into the open air. Germicidal fluids
when directed against the bacteria in an intelligent manner
should destroy them and prevent their becoming active
again.
Putrefactive fermentation is divided as follows: abdominal
fermentation, gastric fermentation, and intestinal
fermentation.
Abdominal Fermentation.
—Abdominal fermentation
is putrefactive fermentation as it effects the tissues and
necrotic substances of the abdominal cavity itself (excepting
the digestive organs), caused by the action of zymogenic
bacteria. Perforations of the intestines or appendix,
inflammation of the mesentery or peritoneum, may allow
putrid material to escape into the cavity proper, where
bacterial action will produce noxious gases. You will
recognize a condition of this kind by the following illustration:
As soon as the point of the trocar has penetrated
the peritoneum and the rod has been withdrawn,
there will be an escape of gas. This escape is due to the
internal pressure being greater than the atmosphere pressure.
[183]
This explains the swollen condition of the abdominal
wall and its subsequent relaxation as the gas is allowed
to escape.
Certain diseases predispose to abdominal fermentation
as inflammatory diseases which effect the peritoneal
covering of the organs, and cause a swollen abdominal
wall after death.
Treatment.—In the treatment of these cases it is always
advisable that the operator be familiar with the
location of the disease, so that direct trocar application
can be made to the affected part. The location of the
affected part is not always the same, as it varies with
the location of the particular tissue or organ affected.
In appendicitis, where death has occurred without surgical
attempts to remove the appendix, the operator should
spray the right inguinal space with enough fluid to
neutralize the cause of the gas. Where the cause of
death has been typhoid, the umbilical, hypogastric and
epigastric spaces should be sprayed. Where the cause
of death is puerperal fever, the right and left inguinal
and hypogastric spaces should be sprayed. The gas itself,
will be eliminated from the cavity of the body by
simply inserting the trocar and allowing the gas to escape
until the internal pressure approximates that of the
atmospheric pressure. This though does not prevent the
reformation of gas, as the origin of the gas is the living
and growing fermentative and putrefactive bacteria. To
prevent a recurrence the bacteria must be killed, and
this is done by spraying a germicidal fluid around the
affected part. Abdominal fermentation and gas is much
[184]
easier to treat than gastric or intestinal fermentation.
Gastric Fermentation.
—This is recognized by a frothy
coffee colored purge from the mouth or nose caused by
pressure in the stomach, due to putrefactive bacteria, and
their action on proteid food substances which are present
in the stomach. Where the cause of death has been principally
from inflammatory processes, or where the deceased
has died shortly after eating a full meal, this condition
must be looked forward to. The swollen condition
directly over the stomach is another visible sign of value
in diagnosing the condition.
Treatment.—When the body is placed in your care,
the embalmer should make a careful and thoughtful survey
of the condition of the body and the cause of death.
Any inflammatory disease of the abdominal tissues or a
full meal eaten shortly before death will almost always
predispose to the formation of gas. The treatment would
be to take proper care of the stomach contents.
(a) Insert the trocar at a point two inches to the
left of the median line, half the distance from the ensiform
cartilage and the umbilicus. Direct the trocar
downward and diagonally to the left to a depth of three
to four inches. Remove the trocar rod and allow the gas
to escape into a fluid bottle, containing a small amount of
fluid, so that the gas may be deodorized. Before removing
the trocar, inject not less than one pint of normal
fluid into the stomach, so that the fermentable materials
and the bacteria may be destroyed.
(b) Make an incision in the median line of the
[185]
body, three inches long, from the tip of the ensiform
cartilage downward toward the umbilicus, and proceed as
directed for the direct incision described on page 257.
The treatment for gastric fermentation demands the
specific treatment as directed above. No short treatments
can be depended upon for certain results. Cotton placed
in the mouth only delays the time for the purging to
begin from the mouth. Gastric fermentation can be prevented
in all cases by the use of the specific treatments as
described in (a) and (b).
If in your practice, you receive a body from a shipping
undertaker, which unfortunately was not treated in the
correct manner, and which is purging from the mouth,
arrange to puncture the stomach in the manner described
in treatment (a). This can be done without disturbing
the position of the body in the casket, by opening the
clothes above the stomach. After puncturing the stomach
and allowing the gas to escape, inject not less than one
pint of fluid therein, cleanse the mouth with absorbent
cotton by the use of the lock forceps and a recurrence of
the purge will not be possible.
If in your practice you have overlooked the possibility
of gastric fermentation, and find, either by advice from
the family or from your own observation, that purging is
going on, use either the treatment (a) or (b), neutralize
the fermentable material, cleanse the mouth and no recurrence
will be possible.
Intestinal Fermentation.
—Here we have the fermenting
gases in the intestines and the colons. The pressure
of the gases will bear upon the stomach and there may or
[186]
may not be purging from the mouth depending upon the
fact of presence or non presence of material in the stomach.
The abdomen though will be greatly distended, and
when palpated will give a drummy note.
Treatment.—(a) Insert the trocar through the umbilicus,
and direct the point downward into the right inguinal
region so as to relieve the gases from the caecum,
then inject a small quantity of fluid; then direct the point
of the trocar upward into the left inguinal region so as
to relieve gases from the sigmoid flexure, and inject a
small quantity of fluid; then direct the point of the
trocar upward into the right hypogastric region so as
to relieve gases from the hepatic flexure, and inject
a small quantity of fluid; then direct the point of the
trocar upward into the left hypogastric region so as to
remove gases from the splenic flexure, and inject a small
quantity of fluid; and if at this time it is thought that the
stomach contains gas, relieve it, and inject therein a
small quantity of fluid; now place some fluid directly into
the abdomen around the small intestine and with this
treatment you are assured that your intestinal fermentation
is taken care of.
(b) Intestinal fermentation may also be treated by
the direct incision, as described on page 257.
[187]
CHAPTER XIII.
DISCOLORATIONS.
Discolorations.
—Discolorations should be treated as
a separate and independent subject because they are
causes of great annoyance and embarrassment to the operator,
and their treatment is of utmost importance. Just
think of the possibility of having a body properly injected,
and the preservation complete, and something
along the line of a discoloration coming to the front and
ruin the results of the work. If there is any condition
possible in the dead body that can cause more trouble
to the embalmer than discolorations in general, it has not
as yet been discovered. You have only to realize what the
appearance of a body would be in the casket, if any discolorations
were present on an exposed surface, to know
that too much can not be said on the subject.
Discolorations may not occur in conjunction with
tissue changes, so when they do occur we should look for
the cause of the same before deciding just what the
name of the discoloration is, or what treatment should be
given to eradicate it.
For convenience in study, and for the proper classification
of the various conditions, the subject has been
divided into those discolorations occurring before death,
[188]
and those discolorations which may occur in the body
after death.
Discolorations Occurring before Death.
—Those discolorations
occurring before death and which would remain
on the body after death would be:
- (a) Yellow jaundice,
- (b) Pigmentary atrophy,
- (c) Cancerous spots,
- (d) Gangrene,
- (e) Ecchymosis or ante-mortem staining,
- (f) Wounds, fractures, scars and tattoo marks.
(a)
Yellow Jaundice.
—In the study of the liver you
have heard that the liver secretes a digestive juice called
the bile.
Bile acts as the natural antiseptic of the intestines in
life, and aids with the digestion of fatty food substances
along with other actions. The principal coloring matter
of the bile is a yellow substance called bili-rubin. Biliverdin,
green, is precipitated by alkalies.
The course of this bile in life is from the liver to the
gall bladder, which acts as the reservoir, into the cystic
duct and then into the common bile duct and into the
cavity of the duodenum (first section of the small intestines).
It sometimes happens that there may be an
obstruction of the bile ducts with the result that the bile
is backed up into the gall bladder, and from there into the
liver again, throwing it into the blood vessels of the liver
and out into the tissues of the body along with the blood.
As the blood traverses the entire area of the body, and
[189]
as the yellow coloring matter of the bile acts as a stain,
it is only a matter of course that the tissues will be
stained the characteristic color of the bile.
This stain will be found all over the body from the
outer layer of the skin to the membrane covering the
bone (the periosteum) and will adhere very closely to
the tissues, rendering the removal practically impossible.
Ordinary arterial injection of a body of this character
will have absolutely no effect, no matter what preservative
fluid may be used and regardless of whatever any
one may say, as it stands to reason that when the discoloration
is not located in the blood vessels, that the removal
of same can not be accomplished by flushing the
blood vessels alone.
Of course, the washing of the blood vessels with a
solution will aid the removal of the discoloration, but
it is necessary to employ a strong bleaching solution on
the outer surface of the exposed parts in order to better
the conditions so that the body may be made presentable.
In addition to this treatment, it would be advisable
to color the lights in the room in which the body is to be
shown, so as to make every thing in the room about the
same color of the body, including the persons viewing
the remains. This will have the effect of lessening the
apparent bad color of the body, and will add to your reputation
as an embalmer.
(b)
Pigmentary Atrophy.
—Here is another instance
of the work of bile pigments or coloring matters, in which
not only the yellow, but the green colors are deposited
in the tissue cells. In addition to this, the cells all
[190]
over the body atrophy (contract or reduce in size). The
contraction of the cells may be due to imperfect nutrition
or perhaps anemia or some other action causing great
emaciation of the body.
You will see very readily that the main point of difference
between yellow jaundice and pigmentary atrophy is
in the color, and also in the fact that the cells in yellow
jaundice are in their normal state and in pigmentary
atrophy are in a contracted condition. The treatment
given for yellow jaundice as follows: injecting and washing
the blood vessels with a mild solution and the application
to the affected parts of a strong bleaching solution,
should be given for pigmentary atrophy.
The suggestions as regarding the lights to show the
body under, should also be noted and used in these cases.
(c)
Cancerous Spots.
—What is intended for this
particular discoloration, is not the ordinary cancer that
has eaten through the skin, but that form sometimes
noted in aged persons where the cancer is just about to
come through the skin. In other words, a yellowish
brown color showing in any of the exposed parts of the
skin before death.
As cancer is in fact a rottening or mortification of the
tissues, the injection with a hypodermic outfit of a strong
hardening and bleaching solution will harden and bleach
out the color of the cancer to a great extent, and thus
improve the appearance greatly, the ordinary cosmetic
powders will finish the preparation.
[191]
For the hypodermic injection we would suggest the
following:
| R | Alum, 10 gr. |
| Corrosive sublimate, 5 gr. |
| Zinc chloride, 5 gr. |
| Grain alcohol, 4 fluid oz. |
| Formaldehyde, 2 fluid oz. |
The cancerous spot should not be confounded with
the color of dessication which will resemble it somewhat.
The main point of difference would be that the cancer
would be present before death, and the dessication could
not possibly occur until after the body is embalmed.
This caution is advised on account of the tendency the
solution to be injected hypodermically would have to
make a dried spot worse in color than better.
(d)
Gangrene.
—Gangrene can best be described as
the death of certain areas of tissue of the living body.
The death of the tissue may be brought about by very
many causes; by vascular obstruction and arrest of the
blood supply to a part, or of the outflow from a part; by
enfeebled circulation; temporary stoppage of the circulation
of a part or organ; acute infection; and by burns.
Gangrene with its peculiar color, a dark green, is not
often found on the exposed surfaces of the body, but will
more often be found on the lower extremities and then
only on the bodies of aged persons. For this reason it
will be unnecessary to treat it for the removal of color.
(e)
Ecchymosis, or Antemortem Staining.
—Ecchymosis
is an extravasation of blood into the areolar tissues,
[192]
forming a bruised place caused principally by a blow
from a heavy instrument or missile.
This form of discoloration is mostly seen in accident
cases, where death was due to mechanical causes.
In ecchymosis the blood capillaries being ruptured,
the blood permeates the bruised tissues surrounding the
ruptured vessels and thus gives the characteristic color
of venous blood. There seems to be no positive treatment,
but in some cases it can be remedied to some
degree by a hypodermic injection of a good bleacher,
and then massaging the part with a strong bleaching
solution. Spots of this kind can sometimes be covered
with flesh tints.
It is often important to determine whether violence
has been inflicted on a body before death. In regard to
this point, we must remember, first, that blows and falls
of sufficient violence to fracture bones and rupture the
viscera may leave no marks on the skin, even though
the person has survived for several days; and, second,
that there are postmortem appearances which simulate
antemortem bruises. A severe contusion during life may
present, at first, no mark or only a general redness.
After a short time the injured part becomes swollen and
of a red color, this color may be succeeded by a dark
blue, and this in turn fade into a greenish yellow or
yellow; these later appearances are due to an escape of
blood from the vessels and to a subsequent decomposition
of the hemoglobin. If, therefore, we cut into such
an ecchymosis after death, we find extravasated blood
or the coloring matter of the blood, in the form of pigment
[193]
granules, free in the tissues. Postmortem discolorations,
on the other hand, although their external appearance
may resemble that of antemortem ecchymosis, are
not formed by an extravasation of blood, but by a circumscribed
congestion of the vessels or by an escape of
blood stained serum. If you cut into such discolorations,
therefore, we find no blood outside the vessels. Care
should be taken not to mistake the lesions of hemorrhagic
infection for traumatic ecchymosis.
Blows on the skin of a body which has been dead for
not more than two hours may produce true ecchymosis
with extravasation of blood, such as can be distinguished
with great difficulty or not at all from those formed during
life. If putrefactive changes be present, the difficulty
of distinguishing between antemortem and postmortem
bruises is greatly enhanced.
Hanging and strangulation are attended with the
formation of marks on the neck which are described in
works on forensic medicine. These marks must not be
confounded with the natural creases of the skin of the
neck. Many adults during life have creases of the skin
of the neck, one or more in number, running downward
from the ear under the chin or encircling the neck. After
death these creases may be much more evident than
during life, and may be rendered more decided by the
position of the head, or if the body be frozen. They
usually persist until the skin putrefies.
(f)
Wounds.
—The embalmer should notice the situation,
extent and the direction of a wound, the condition
of the edges, and the surrounding tissues. If it be a
[194]
deep, penetrating wound, its course and extent should
be ascertained by careful dissection rather than by the
use of a probe.
If the edges of a wound be inflamed and suppurating,
or beginning to heal, it must have been inflicted some
time before death. In a wound inflicted a short time
before death the edges are usually everted; there may
be more or less extravasation of blood into the surrounding
tissues, and the vessels contain coagulated blood; but
sometimes none of these changes occur. The chief characteristics
of a wound inflicted after death are absence
of a considerable amount of bleeding, non-retraction of
edges, and the absence of extravasation of blood into the
tissues. But a wound inflicted within two hours after
death may resemble very closely one received during
life. In general, unless a wound is old enough for the
edges to present inflammatory changes, the embalmer
must be very careful in asserting its antemortem or postmortem
character.
(g)
Fractures.
—It may be important to determine
whether a bone was fractured before or after death.
This point can not always be decided. Fractures inflicted
during life are, as a rule, attended with more extravasation
of blood and evidences of reaction in the surrounding
tissues; but fractures produced within a few hours
after death may resemble these very closely. Usually
a greater degree of force is necessary to fracture bones
in the dead than in the living body.
(h)
Scars and Tattoo Marks.
—The presence and
[195]
character of these should be noted. Scars produced by
any considerable loss of substance may become very much
smaller and less conspicuous, but never entirely disappear.
Slight and superficial wounds, however, leave marks which
may not be permanent.
The discoloration produced by tattooing may, although
it rarely does, disappear during life. The embalmer
should not try to remove it.
[196]
CHAPTER XIV.
DISCOLORATIONS.—Continued.
Discolorations Occurring After death.
—Those discolorations
occurring after death would be as follows:
- (a) Desiccation.
- (b) Greenish tinge of putrefaction.
- (c) Chemical action.
- (d) Postmortem discoloration.
- (e) Postmortem staining.
- (f) Capillary or venous congestion.
Desiccation.
—This is a brownish color caused by the
drying of the skin. Various conditions might cause this
color of which a few are considered here:
Natural evaporation, the drying action of formaldehyde,
freezing the skin, feverish conditions of the body
before death, absence of a normal amount of moisture in
the skin of the dead body.
Natural Evaporation.—The passage of moisture from
the skin into a dry atmosphere reduces the normal amount
of moisture in the skin, thereby producing an altered
color. The extent of the moisture reduction governs the
color produced. When evaporation begins, the skin loses
its softness and becomes slightly yellow in color. As
[197]
evaporation continues the skin becomes more hard and
the color changes from yellow to brown. At this time
nothing can be done to restore the original color as in
the absence of the blood circulation, the pigment of the
skin will not take up moisture, nor will moisture penetrate
the skin itself.
Treatment.—The only treatment for a condition of
this kind is necessarily a preventive one. While embalming
a body, the operator should apply either water or
one of the commercial face solutions to the skin of all
the exposed portions of the body. If the condition within
the skin is one in which there is a predisposition toward
dryness, the face solution or the water by being present
on the skin will reduce evaporation from the skin itself;
in this way maintaining the natural degree of moisture.
Should a hard, dry spot appear in the absence of any
preventive treatment, the operator can only coat the spot
with grease paint and thereby hide it.
The Drying Action of Formaldehyde.—Formaldehyde
is derived from methyl spirits, which in itself has
an active affinity for water. The amount of water ordinarily
mixed in formalin in the compounding of a formaldehyde
fluid is not sufficient to satisfy the appetite of
the formaldehyde for more water. When a formaldehyde
fluid comes in contact with moisture laden skin, there
will be a movement of moisture from the skin toward
the formaldehyde fluid, thereby reducing the degree of
moisture in the skin and in that way causing it to become
dry. When the skin becomes dry, it changes in color
the same as in natural evaporation.
[198]
Treatment.—There are three conditions in the skin
met by the operator. The first is where there is a predisposition
toward dryness and this is where the skin
does not contain a normal amount of moisture to begin
with. In old age cases, tubercular, and anemic bodies,
the ordinary embalming fluid should be diluted at least
one half for the first part of the injection, thus reducing
the appetite for moisture on the part of the fluid. In
addition to this, water or a face solution should be used
externally to prevent outward evaporation from further
reducing the moisture in the skin. The fluid exhibits a
tendency to draw water into the pores, thus maintaining
to a large degree, the normal moisture percentage.
The second condition met with is one in which the
skin contains a normal amount of moisture. In this case
it would not be necessary to reduce the strength of the
standard fluid at any time during the injection, but it
is necessary to apply water or a face solution externally
to limit outward evaporation and to provide a source
whereby moisture could be drawn into the pores by the
appetite of the formaldehyde, thus again maintaining
the normal percentage of moisture in the skin.
The third condition is one in which the skin along
with the balance of the body, will contain more than a
normal percentage of moisture. This condition may be
looked for in edematous or dropsical cases. The injection
in these cases should be normal in strength unless
the dropsy is very pronounced, when an overnormal injection
can be given without reducing the moisture percentage
in the skin below the normal point.
[199]
Should the above precautions not be used and the
skin be dried through the appetite of formaldehyde for
water, no treatment can be given which will restore the
moisture to the skin. When moisture is drawn from the
skin and the percentage is below normal, the skin will
shrink and will draw tight against the bones and subcutaneous
tissue. This frequently gives rise to the sharp
nose and to the drawn appearance so common in those
cases. Prevention is the only remedy.
Freezing the Skin.—When the body is subjected to
a temperature of 32 degrees Fahrenheit, the moisture in
the skin freezes, thereby removing it from its usual consideration,
as the element that is responsible for the usual
softness and flexibility of the skin.
In the cold months, bodies are sometimes left in cold
rooms with the windows open. The embalmer did this
in the past, thinking that subjecting the body to the influence
of a cold atmosphere would simplify preservation.
From the standpoint of preservation alone, this theory
is correct, but in accomplishing the above result the
moisture of the skin may be frozen. The resulting color
is light yellow. The texture of the skin is changed from
soft to a slightly hardened condition.
Treatment.—Never allow the room temperature to
approach the freezing point. Should the above treatment
be disregarded, and the yellow color become present, have
the room warmed, and the color will slowly disappear.
Feverish Conditions in the Body Before Death.—Fever
is the name usually given to the rise of temperature
that goes with inflammation. In severe inflammatory
[200]
diseases, the tissues lose much of their moisture
through the arrest of the saturating power of the blood
stream and the disturbance of circulation. The skin contains
a sub-normal amount of moisture when the embalmer
reaches these cases, which may be further reduced by
outward evaporation and the dehydrating power of the
embalming fluid. Small brown spots resembling the
fever blister in the living body may be present around the
mouth.
Treatment.—Use half strength fluid for the first part
of the injection, followed by normal fluid for the second,
third and fourth parts. Apply water or a commercial
skin or face solution while the injection is going on.
Absence of a Normal Amount of Moisture in the
Skin of the Body.—The normal amount of moisture in
the skin has been determined to be an amount equal to
seventy-five per cent. of the weight of the skin. Any
percentage less than seventy-five per cent. is considered
subnormal. This condition can be expected in all fever
cases, in anemics, and in old age.
Treatment.—When the skin appears rather dry, the
injection of fluid should be half strength for the first
and second parts, normal for the third and fourth. The
skin of the exposed parts of the body should be dampened
with an application of water or a commercial face or
skin solution, while the injection is being made.
Greenish Tinge of Putrefaction.
—Putrefaction discolorations
are those which are produced when putrefactive
bacteria become active in the skin or subcutaneous tissue.
This discoloration appears generally about the second
[201]
day, unless preservative fluids have been applied to prevent
it. It first begins in the ileocaecal region or lower
part of the abdomen. The skin covering these parts assumes
a brownish color which shades to yellow, yellowish
green, and finally a green color. This green discoloration
will in a few days spread all over the surface of the body.
Among the putrefactive bacteria is the bacillus fluorescens,
a chromogenic germ, which produces a greenish
color when it becomes active in the tissues. One of the
first external evidences of putrefaction is the production
of a greenish color in the abdominal wall. This, of course,
could not occur when embalming had been done with any
degree of completeness. Should an insufficient circulation
be encountered when embalming a body, the part which
does not receive the fluid, being unprotected, may be affected
by the color producing germ mentioned above. The
most likely to be affected by an insufficient circulation
will be located somewhere in the extremities of the circulation,
that is to say, in the skin. We can place the
affected part more definitely in the skin of the face, particularly
the nose, which has a rather poor circulation.
This condition will not make its presence known until
three or four days after embalming has been done, making
it almost entirely absent in bodies embalmed in ordinary
practice. Should several days elapse between the time
the body died and embalming, allowing the discoloration
to appear, the following treatment would be advisable:
Treatment.—Inject a very small portion of the following
solution just under the skin, using a hypodermic
needle.
[202]
| Alum | 10 | gr. |
| Corrosive Subl. | 10 | gr. |
| Zinc Chloride | 5 | gr. |
| Grain Alcohol | 4 | fl. oz. |
| Formaldehyde | 2 | fl. oz. |
Just a small portion of the above solution is all that
will be necessary, working it under the skin with the
finger tip, so as to avoid destroying the features by swelling
the tissues.
This treatment being a chemical one, it is necessarily
slow in its action of bleaching the green color. Should
haste be necessary, inject a very small quantity of embalming
fluid to arrest the putrefactive process and then
cover the spot with theatrical grease of the proper color
to match the surrounding skin.
Chemical Action.
—Chemical action is any discoloration
of the skin or tissues of the body which may be
caused by the action of opposing chemicals. There is
only one known discoloration occurring in the body after
death as a result of the presence of a chemical in the body,
which, when coming in contact with formaldehyde, produces
a discoloration. This particular discoloration,
greenish in color, is the result of the work of the drug
methylene blue in contact with formaldehyde.
Often, in cases of chronic malaria, or diseases of the
liver, or again as a general antiseptic, methylene blue
will be administered by the attending physician, and you
should learn this fact beforehand, for if methylene blue
has been administered it is advisable not to use a formaldehyde
[203]
fluid. There is a chemical action set up between
the formaldehyde and the methylene blue, which gives
the tissues a greenish color, which is quite objectionable.
In this case you would use some fluid which does
not contain formaldehyde, benzoate of soda, or borax,
or peroxide solution should be used.
Another good formula to use is the following:
Rx
| Carbolic acid | 5 | oz. |
| Borax | 12 | oz. |
| Glycerine | 1 | oz. |
| Water, sufficient to make | 1 | gall |
or
Rx
| Carbolic acid | 5 | oz. |
| Oxalic acid | 12 | oz. |
| Boracic acid | 2 | oz. |
| Water, sufficient to make | 1 | gall |
Postmortem Discoloration.
—This is a general expression,
and refers to any discoloration which might occur
on the body after death.
What is usually meant, though, when this term is
used is the settling of the blood to the dependent parts
of the body after death. If the body is lying on the
back, the blood will naturally gravitate toward the back,
into the azygos system and cause a bluish discoloration,
or the same condition will result, if the body is found
lying on the face and stomach, in which case the discoloration
will be in the face and the anterior chest and
abdominal walls.
[204]
Postmortem Staining.
—This condition is caused by
changes in the blood while in the veins. The blood becomes
more fluid in character and the red blood corpuscles
become granular and give off their oxygen which
escapes through the walls of the veins and carrying
with it the haemoglobin or coloring matter of the blood,
stains the tissues over the superficial veins a purplish
red color. This discoloration only appears on the ventral
surface of the body and along the course of the large
superficial veins. An excellent example of this discoloration
is seen in the drowned subject where almost always
all the superficial veins can be easily traced by this discoloration.
Capillary or Venous Congestion.
—This term includes
those discolorations either caused by gas distension
or by the unskillful injection of fluid into the vascular
system. Gas forming in the abdominal or thoracic cavities
will so press upon the heart as to empty it of its
blood, which will be forced upwards into the large venous
trunks of the head, neck and axilla. All embalmers are
familiar with the flushed face which often appears when
the arterial system has been injected in a too hasty manner.
It causes the veins and capillaries of the face and
neck to become congested the same as that caused by
the formation of gases in the cavities.
[205]
CHAPTER XV.
ARTERIAL EMBALMING.
Making the First Call.
—There are some pertinent
points to consider regarding the procedure at the time
the call is received. Many embalmers have some particular
rules that govern their inquiries at this time. It is
the consensus of opinion among professional men of all
kinds that a rule is a good thing to have to cover any
regular procedure. It matters not so much as to what
the rule is, just so the necessary information can be acquired
in a uniform manner, thus systematizing that part
of the work and enabling the embalmer to properly prepare
for the case at hand before leaving the establishment.
The habit of inquiring about the sex, and age of the
person, as well as the cause of death, should be cultivated.
The importance of knowing the sex of the person lies in
the fact that in some communities different styles of
door badges or decorations are more appropriate for one
sex than for the other. When the ruling decoration is
some form of fresh flowers, this should be ordered before
the embalmer leaves for the house of mourning if possible,
unless the call should be received at night or in the early
hours of the morning, when this item is usually left until
the earliest business hour. The age of the person also
[206]
determines to a great extent the style of decoration which
is to be used.
The cause of death is vitally necessary. In some
cases, the ordinary contents of the embalmer's grip or
hand bag are sufficient for the usual needs. In other
cases, extra material of various kinds are necessary, for
instance, the rubber floor covering for the carpet in dropsical
cases; the sanitary clothes in eruptive contagious
diseases; the fumigating outfit in the same diseases, (providing
this duty is not performed by the health authorities);
and other articles needed only in the treatment
of special cases.
After obtaining the above information, examine your
grip or hand bag to see that you have all the equipment
needed to care for the case in the proper manner. This
saves many cases for those who follow these rules, as they
are enabled to have just what is needed, and prevents
the slighting of a case for which there may be some excuse
if the proper materials are not in the outfit. From
a professional standpoint, it should be necessary for the
embalmer to carry anything he may need, otherwise carelessness
may dictate his procedure and disaster may
result.
An ordinary case can be attended with the following
material[1]:—
[207]
- The couch embalming board.
- The slumber robe, and face cover.
- A rubber or oil cloth cover for the board.
- A suit case grip, or hand bag.
- Concentrated fluid (at least 4 bottles).
- One or two empty 64-oz. bottles (for mixing fluid).
- One bottle for blood drainage.
- One injecting outfit (pump, tubes, etc.)
- One blood drainage outfit.
- One instrument wallet, containing:—
- 2 scalpels, 1 bone separator, 2 aneurism needles, 1 spool linen thread, 1 grooved director, 3 arterial tubes (assorted diameters), 1 bistoury, 1 lock forceps, 1 spring forceps, 1 artery forceps, 1 case needles, 1 6-inch child's trocar, 1 12 or 14-inch trocar, 1 chin rest, 1 hypodermic outfit, 1 roll absorbent cotton, 1 sponge, 1 box face powder, 1 nail file, 1 hair brush, 1 bottle bichloride of mercury tablets, 1 shaving outfit.
For special cases it would be well to have on hand
the following articles:—
- 1 small can plaster of paris.
- 1 tube lip cement.
- 2 rubber bandages.
- 1 can hardening compound.
- 1 bottle Platt's chlorides or any other good deodorant.
- 1 outfit of formalin and permanganate of potash, or any other standard gaseous germicide preparation for fumigating.
- [208]
- 1 small bottle of tincture of iodine as a preventive to infection should you cut yourself.
After the outfit has been found correct for the case
at hand, place everything in the conveyance, and leave
for the house. Upon arriving at the house, enter alone
and meet the member or members of the family who
have been delegated to talk to you. At this time it will
be well to ascertain the position of the body, the wishes
of the family in reference to where the body is to be
placed after embalming and to where the body is to rest
in the casket until the time of the funeral.
If you meet with any objection as to embalming, it will
be well for you to consider the sanitary aspect of the
case in speaking to those interested. In this case the
sanitary aspect should always take precedence over the
preservative aspect, since you can count on the assistance
of the physicians in supporting embalming on that account.
Should your wishes be overruled after you have
presented the facts in the matter, it would be well for
you to place the entire responsibility for the condition
of the body upon the family, since without embalming
you are unable to know the final condition of the body,
and should not be held responsible for it regardless of
what the condition may be in that case.
After this short talk with the family, return to your
conveyance and carry your outfit to the room of death.
Everything that you carry should be properly covered,
as there is nothing quite as indecorous as the display
of an embalming board without a cover. When you have
placed the outfit in the room, call for everything that you
[209]
will need from the family, which will include such things
as a pail, warm water, soap, towels, etc. Do all of this
before touching the body; and after securing all the necessary
items, close the door, and do not open it again
until the work has been completed.
Should unforeseen circumstances cause you to re-open
the door, present yourself with a coat on, and never,
under any circumstances, appear before any one in your
shirt sleeves, as that is another indecorous procedure.
After the preservation has been completed, dust a little
face powder on the face and hands, to remove the moist,
clammy appearance which may have been left on those
parts. Place the undergarments on the body and then
any other garments which may have been given to you
by the family. Cover the body with the slumber robe,
and then call in as many members of the family as may
wish to view the body, asking them to criticize your
work. Before calling in the family it would be well to
put everything out of sight and not have any grips open.
If favorable comment is heard from the family, your
work is done for the time being. If unfavorable comment
is heard, ascertain the cause of the comment and do not
leave the house until the proper appearance has been
secured. If your work has been pleasing to the family,
you can rest assured that the case is a success and that
you have done your work well. When you are satisfied
in your own mind that all is well with the body, make
arrangements for the selection of the casket, and then
retire from the house. If the door decoration has not
[210]
been placed in position before you leave, you will place
it in position yourself.
Some funeral directors set the time for the funeral
during the first call, and some wait until later. The same
for the other arrangements, such as newspaper notices,
minister, singers, church or chapel services, number of
conveyances, etc. Whatever method you choose to use in
your community should be carried out systematically so
that at no time, will anything be left undone to cause
confusion at some inopportune time.
The Position of the Body on the Embalming Board.
—The
position of the body on the embalming board is regulated
by the adjustment of the movable head end of the
board.
After much experience with various classes of bodies,
we find that the adjustment mentioned is a very valuable
aid in securing the best results both as to completeness
of the circulation and amount of blood drained.
In anemic, tubercular, cancer of the stomach and exhaustion
cases, together with other conditions resulting
in emaciation, the head end of the board should be
raised to the height that seems suitable for the position of
the upper part of the body when placed in the casket
during the injection of the first bottle of fluid. When the
first bottle of fluid has been injected, lower the head end
of the board until the entire board is level, and leave
it in that position until you have completed the injection,
when you will again raise the end of the board until the
position of the body is just as it will be in the casket.
When pneumonia and other non-emaciated bodies are
[211]
to be injected, with drainage, use the same procedure
as is stated above for the emaciated bodies.
In dropsical cases, raise the head end of the board only
for the first bottle of the injection; then for the second
bottle, lower the head end to about half of its first height,
and set the foot end of the board on some object that will
raise it five and six inches. In this way you will
have a slight elevation at both ends of the body, and
drainage can better be obtained from the center of the
circulation. When the operation is complete, lower the
foot end again and raise the head end so that the body
occupies the proper position for the casket.
These adjustments are practical methods of overcoming
gravity handicaps in the distribution of the fluid,
and of accelerating the amount of drainage obtainable
by keeping the level of the drainage tube below the
blood level in the body, thus accomplishing a universal
distribution of fluid, and securing a greater quantity of
undiluted blood from the vein.
It is very important to remember when you are through
injecting the body that you are to place the body in the
exact position on the cooling board which you want it to
have in the casket. After a little time the body will become
more or less rigid due to the action of the preservative
fluid used, and will set in the position you have placed
it which condition will be hard to change later.
Selection of an Artery.
—Great care should be taken
in the selection of an artery. Never make a practice of
using the same artery on all cases. Acquaint yourself
with the location of them all, and on different occasions, as
[212]
different conditions arise, use the artery most likely to
give the best results for the condition in hand.
Convenience usually governs the operator as to the
artery he is to use. If blood is to be removed it is
best to raise one of the larger blood vessels, such as the
carotid artery and the internal jugular vein, or the femoral
artery and femoral vein, or the axillary artery and
axillary vein. If it is desired to draw the maximum
amount of blood, the femoral artery and vein should be
selected, as they are more dependent, and control more
of the blood, when the body is placed on an incline. A
drainage tube sufficiently long to reach above Poupart's
ligament as far as the common iliac is all that is necessary
as there are no valves intervening between the bifurcation
of the common iliac and the right auricle. However if
you can, extend the tube up through the ascending vena
cava and eustachian valve into the right auricle. This
will give you a chance to draw blood from the right auricle
and is a much better procedure than tapping the right
auricle with the trocar.
If the body is already dressed and the hands or feet
need to be re-injected, the radial or posterior tibial likely
will be most convenient as their use will not necessitate
the removal or cutting of the clothing.
Oftimes there is but a single window to admit
light and the operator should be so skilled as to be able
to raise the arteries either on the right or left side without
having to turn the cooling board.
In emaciated subjects the linear and anatomical guides
are always plain but in fleshy subjects this is not always
[213]
the case. Look over the subject and see which artery will
be the most convenient to raise. Usually in fleshy subjects
the femoral is hard to raise as there is a great amount
of fat in Scarpa's triangle making the artery lie very
deep, but in these subjects the guide for the brachial is
quite plain, a distinct groove being seen between the
biceps and triceps muscles.
In a short necked subject it is never advisable or convenient
to raise the carotid as there is not much room
to work and the incision is very liable to show. Another
artery will be found much more advantageous in these
subjects.
In accident cases the seat of injury will determine the
artery to be raised, using the one through which you can
give the body the greatest supply of fluid to all parts.
Often it will be necessary to raise several arteries to complete
the injection.
There is no necessity for undue exposure in either
sex, however it is hardly ever advisable to inject the
femoral in the female, as some mischief-maker might
without any real cause influence others in the community
against your methods.
When selecting the brachial and femoral arteries always
raise them at a place below the point where collateral
circulation is given off or in other words raise them in
the middle third. By so doing the fluid will reach, by
means of collateral circulation, the tissues of the arm
and leg below the point of injection.
As far as the injection of fluid is concerned, one artery
is just as good as another. All arteries are parts of the
[214]
same channel branches of the aorta. No valves exist in
any part of their course.
How to Raise an Artery.
—With the scalpel make an incision
an inch long in the average size arm, cutting
through the skin and then through the fat. Reverse the
blade and at each end of the wound cut forward and upward
to make it clean. Take the grooved director and
with the small end puncture the deep fascia, then reverse
ends of the director and force the blunt end up the
wound, underneath this deep fascia, one-fourth to one-half
an inch longer than the wound. Now take the
scalpel with the edge of the blade upward and split the
fascia as far up as the needle extends and cut the tissue
(fascia and fat) up to the skin, being careful not to cut
the skin. Reverse the needle and cut the lower end of
the wound the same way. This will give you an incision
one inch long on top and one and one-half or two
inches at the bottom of the wound, and none of the vessels
will be injured.
With the handle of the aneurism needle separate the
tissues between the muscles, artery, vein and nerve, then
use the hook end of the aneurism needle, pass it under
the artery and raise it to the surface, passing the bone
separator or the forceps with the closed end underneath.
Remove the individual sheath surrounding the artery.
Likewise raise the vein to the surface.
If the artery and vein lie side by side and it is desired
only to raise the artery, hook down between the two,
away from the vein, sliding the hook forward and backward
underneath the artery, then raise to the surface.
[215]
If the artery and vein lie side by side and it is desired
to raise both, pass the hook around the vein first,
as by hooking around the artery toward the vein the
point of the hook will often rupture the vein.
How to tell an Artery from a Vein or a Nerve.
—Raise
the suspected vessels to the surface, placing a bone
separator underneath to form a bridge, which will cause
the blood to recede on every side. If you are in doubt
which is the artery, remove the individual sheath from
each one.
The nerve will appear as a glistening white cord, very
solid to the touch and showing bands of nerve fibres
which can be separated by the aneurism hook. It will
not have any central opening.
The vein will appear as a dark blue color and collapsible
because of the fact that they have thinner walls
than the arteries, lacking the middle circular layer of
fibres. Veins have a central opening. As a rule the vein
contains blood after death, which gives it the dark blue
color but should it not contain blood, it resembles the
artery very closely as to color.
The vein contains valves which can be seen distinctly,
if the blood be pushed the opposite way from which it
runs in life.
The artery is of a creamish white color and non-collapsible
because of the fact that it has heavy walls and
a middle circular layer of fibres. The arteries feel firm
to the touch while the veins are soft and velvety. Arteries
have a central opening and as a rule do not contain blood
[216]
after death. They likewise do not have valves. The artery
is usually more constant than the vein.
Should all these not convince you, raise the one you
think is the artery with the hook, pass the forceps underneath,
spread these and pass the bone separator under
for a bridge and with the scalpel incise the artery about
one-fourth the way. Attach the arterial tube and if there
is blood present, allow it to drain by lowering the arm.
When it has ceased to flow, inject very gently and slowly.
If you get a half-pint of fluid in the body, you may be
assured of its being the artery.
Another way to tell the artery from the vein is to
roll them lightly between the fingers. If it feels like a
thin rubber tube, and does not roll together in a little
bundle, the supposition is that the vessel is an artery.
This however is not certain, as phlebitis, or some other
diseased condition of the veins may result in the thickening
of the walls of those vessels, to such an extent as to
make it impossible to distinguish in this way between
the artery and the vein.
The anatomical and the linear guides for the arteries
and veins, and their relation to the accompanying nerve,
will help also to tell them, one from the other.
How to Cut an Artery for Injection.
—After the artery
has been located it should be freed from the surrounding
tissues and then raised to the surface. After it has been
raised to the surface the bone separator which is to act
as a support while cutting the artery, should be placed
underneath the artery.
[217]
The artery may be cut in several ways as follows—a T
shaped incision may be made. This is a very old method,
one of the first to be used for this purpose. To make this
kind of an incision in the artery, the scalpel is placed
point down about one-fourth the distance from the edge
of the artery, and then by forcibly bearing down on the
scalpel cut the artery crosswise. Rotating the artery the
cut will now be on the upper surface. Now from the
middle of the crosswise cut, extend a longitudinal cut
lengthwise of the artery, for almost one half inch. We
have no comment to make on this kind of an incision,
excepting to say that the method is old and obsolete,
and no longer used, and that a much better method is
now used.
Another method suggested by some authors is the
longitudinal incision. With the belly of the scalpel
cut the artery lengthwise for a distance of a little less
than one half inch. The disadvantage of this kind of a
cut is that the operator does not know when he has cut
to the center of the artery and no more than the center.
If the cut has been made to a distance beyond the center,
then the inside wall on the opposite side will be cut and
if the wall is in the least diseased, the arterial tube when
it is inserted may get between the walls which will mean
that no fluid can be injected.
Another method is to cut the artery crosswise, placing
the point of the knife on the artery about one fourth
the distance from the edge of the artery, bearing down so
that the point will come through to the bone separator
which is beneath, then forcibly bearing down cut outward
[218]
with the belly of the knife. Now rotate the artery and
the cut will be on the front of the artery.
Another better method is the same as the above, but
instead of cutting outward perpendicular to the artery,
cut outward diagonally, then when the artery is rotated
there will be a V—shaped cut. The point of the V
should be made opposite the way the operator is to inject
the fluid. With the aneurism hook, pick up the point
of the V, which will mean that the hook will have to be
inside of the artery, and using the hook as a guide insert
the arterial tube. The only disadvantage of this
method is that the tensil strength of the artery is to a
certain extent weakened, but if the artery is not cut too
deep, this is not a serious disadvantage. The advantage
is that the operator is always certain that he is in the
center of the artery, that if his knife is sharp, that he will
always cut all three walls of the artery at once, and thus
prevent a ruffling up of the inner wall of the artery
should it be diseased.
The Injection of Fluid.
—One very important point to
be taken into consideration when embalming, is the slowness
with which the fluid should be injected.
Upon this one thing will depend very largely the
success you will have with the perfect circulation of the
fluid and cosmetic effects.
Some authorities on the art and science of embalming
have made the claim that it makes no difference how
rapidly a body is injected as the fluid is so widely distributed
through so many branches of the artery that no
harm can come from this source. This is very erroneous
for when the fluid is forced rapidly through the arteries,
[219]
it also flows rapidly through the capillaries into the
veins, thereby enlarging the quantity of fluid in those
vessels and often forcing the blood into the exposed parts
of the body, causing serious discolorations.
The capillaries are sometimes ruptured by the rapid
injection of fluid, causing spots to appear on the face
that would never have been there had the body been injected
more slowly.
A further reason for slow injection is that the disinfecting
fluid is given an opportunity to be absorbed by
the tissues as it passes into the capillaries and not be
forced through those little vessels into the veins, as it is
by the absorption of the fluid that the body is disinfected.
This is especially true when the drainage tube is
being used as the fluid, seeking the course of least resistance,
passes through the artery, into the capillaries,
through those vessels to the veins and out through the
drainage tube.
As it takes but little blood to color a large quantity of
embalming fluid, many embalmers are led to believe that
they are removing large quantities of blood, while in
reality perhaps one-half of the colored liquid which flows
from their drainage tube is the fluid which is being injected.
Many failures have resulted from this error.
Fluid should always be injected into the body very
slowly, and the more slowly it is injected the more perfect
will be the cosmetic effect.
If necessary make a second injection. An embalmer
who makes the proper charge for his services as a professional
can afford to make two injections if necessary.
[220]
He can let it be known that he will not be content with
anything but perfect work, and patrons will not only
cheerfully pay for it, but will have a better opinion of
his professional standing. Thorough drainage and slow
injection are the best safeguards against discoloration.
Dr. Erdman before the Minnesota association suggests
that the amount of fluid that fills the arteries is not enough
to percolate through the capillaries and into the tissues,
and saturate all the parts of the body. He favors the
gravity injection by merely allowing the fluid to flow
naturally into the arteries from an elevated vessel, and
would use no force or pressure in injection. Ideal embalming
would be a series of gravity injections at intervals
of several hours. While the gravity injection
such as the doctor describes will undoubtedly be a sure
method of getting a perfect circulation, and while it is
the process generally pursued in morgue work where the
apparatus is convenient, it is in the majority of cases in
the home impractical.
All bodies to be shipped must be thoroughly arterially
embalmed, that is, to have introduced into the arterial system
sufficient amount of disinfecting fluid to thoroughly
sterilize every particle of matter in the dead body. This
can only be done by introducing into the arteries an
approved disinfecting fluid.[2]
[221]
Approved Disinfectants.
—This is construed by most
states to mean a fluid which is sufficient in strength to
kill all the germs on the surface of the body or on the
interior. An approved disinfectant for the external surface
of a dead body is a solution of 1 : 1000 bichloride
of mercury. An embalming fluid which has the official
approval should contain 5% formaldehyde.
Embalming Fluids.
—At the present time only a few
states have placed restrictions on fluids. These restrictions
are that they contain neither mercury, arsenic,
antimony or any of their compounds. These poisons
when used to inject a body make it almost impossible
to detect from a chemical analysis whether death was
caused by a poison or the poison was from the embalming
fluid. Iowa recommends a fluid the formula consisting
of formaldehyde, glycerine, borax, boracic acid, salt
petre and water.
Wrapping a Body in Cotton.
—In certain diseases,
when a body is to be shipped, the law compels the embalmer
to wrap the body in cotton. This may be the ordinary
cotton purchased from a dry goods store. The
cotton should be cut in strips at least one to one and one-half
feet longer than the body. Two layers are laid side
by side upon a sheet, the body then placed thereon and
the whole wrapped about the body will envelope the body
in a satisfactory manner. This means that the entire
body is to be enveloped, so that the face head or feet
will not be exposed, and the wrapping should never be
removed. Absorbent cotton may be used for this work,
[222]
but it is more expensive and not as good as dry cotton
for this purpose.
[3]The Charge of Embalming.
—This subject is one that
has long been forcing itself upon the thought and attention
of progressive undertakers, principally because
of the many abuses and misunderstandings that have
grown out of the manner in which members of the profession
regard the value of their services and the careless
and indifferent systems used in conducting the business
side of our work.
In order to succeed in a chosen calling one must first
have a liking and a natural adaptation for the work; second,
he must prepare himself by obtaining a thorough
working knowledge of the profession or business he expects
to follow. He must educate himself for the work.
This is fundamental and has been proven many times with
the successes in every profession. It is fair to presume
then that the great majority of men entering this profession
have considered the probabilities of success and have
met the requirements needed to qualify them to follow
this calling and to receive the support of any who through
necessity need their services.
Without going into the non-essentials showing the
rights of individuals holding a license as an embalmer to
practice, we may naturally come to the next question in
this connection, the value of his services and how they
should be charged for. Charge what your work is worth,
[223]
and do not conceal the amount in the price made on the
casket or any other part of the funeral expenses. Make
it a specific charge in every instance for there is a good
and sufficient reason why you should.
An explanation of these reasons may be summed up
as follows: the conscientious effort in qualifying yourself
to meet the needs of your calling and the requirements of
the state, the cost of your training and education in time
and money, the years spent in the hard school of practical
experience and self development.
Next your business equipment and investment, the
care of the case on which you are called, its peculiar requirements
and how it taxes your skill in doing the
work, the risk from infection, the distance you must travel
and the expense of the trip. All of these considerations
enter into the cost and should be the basis on which to
formulate a charge for the work.
Just as the well equipped surgeon of wide experience
and training skillfully performs operations relieving
suffering, saving and prolonging life, naturally allows the
difficulties of the case and the distinctive personal service
rendered to govern him in the amount of the fee,
so in a very similar sense the services of the embalmer
should hold a certain ratio of value to the conditions
under which he works and the ability he employs in its
performance. Therefore let me again urge that you
make it a specific charge showing it a distinctive personal
service.
In the matter of the value of personal services the
question is often raised: “Which is the more important
[224]
part of the work in our profession, directing and managing
the funeral or the embalming and care of the body.”
In answer to this let me say that the care and the embalming
of the body is first importance because the law
says so, because the education of the embalmer is paramount
to other considerations and so regarded by the
national association, because sanitary science demands
it, because without a body properly embalmed and prepared
for burial the funeral is a failure from whatever
standpoint you wish to judge it.
A director may bungle the arrangements and at the
most it is but a matter of annoyance to the family. However,
let him fail to properly fit and prepare the body so
that the relatives can see restored to them the face of
their beloved one, beautified in the last long sleep of
death, and they will never forgive him. They secured
his services first as an embalmer and incidentally as a
director of the funeral, naturally, therefore, the greater
importance of his work centers around his services to
the family in that capacity. Now in all candor, why
should he not make a specific charge for his work? He
is rendering the greater service in caring for the body,
it should be the first item charged for on the funeral bill.
[225]
CHAPTER XVI.
THE ANATOMICAL AND LINEAR GUIDES FOR
SPECIAL ARTERIES.
How to Locate and Inject the Carotid Artery.
—The
carotid artery, is not used much, by the average embalmer
for several reasons. It is usually a hard artery
to raise, partly because the average embalmer does not
know the anatomy of the neck. In subjects having short
and very fleshy necks it is not advisable to use the carotid,
however in subjects where the neck is long and not
fat it is with some a favorite. It is always essential to
know how to raise and inject the carotid for in accident
cases, where the arteries of the lower part of the neck
and thorax are ruptured it becomes necessary to raise
and inject the carotids to get the fluid into the tissues of
the face and brain. In cases of suicide where the arteries
of the neck have been cut it is necessary to know
where the arteries and veins lie so that they may be tied
off. Often the body is so badly mutilated that it is impossible
to raise any other artery excepting the carotid.
Every practitioner should know how to raise and inject
this artery, even though some other artery is the one
generally used.
[226]
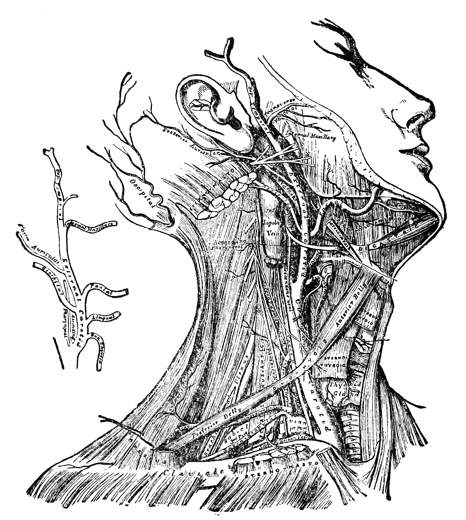
Fig. 46—The arteries of the neck. (Gray)
Linear Guide.—By a linear guide is meant that an
imaginary line is drawn from a point to a point the
same direction the artery runs so that by mentally imagining
this line one can be safe to cut on the line and
be sure that the desired artery will be reached.
The linear guide for the carotid is represented by
a line drawn from the sterno-clavicular junction to a
point between the angle of the jaw and the lobe of the
ear. (Mastoid process).
As the body lies on the cooling-board place one finger
[227]
on the sterno-clavicular junction and the other at a point
between the angle of the jaw and the lobe of the ear,
and by cutting on this imaginary line, the artery will be
reached, providing the artery is normal and if the embalmer
is thoroughly acquainted with the anatomy about
the artery, as is summed up in the anatomical guide.
Anatomical Guide.—By the anatomical guide is meant
the relation which the artery bears to the surrounding
tissues.
The anatomical guide for the carotid artery is that
the artery lies between the sterno-mastoid muscle to the
outside, and the muscles surrounding the trachea (wind
pipe) and the esophagus, to the inside. In the middle
third or sometimes between the middle and upper third
the omohyoid muscle crosses over the artery.
Perpendicular Incision.—The artery is divided for
the sake of description into thirds. By making an incision
on the linear guide in any one of the thirds the
tissues that must be passed through are the following:—skin,
platysma muscle, superficial fascia, deep fascia, common
sheath, and the individual sheath.
The platysma muscle is a broad tissue paper like
muscle, placed immediately beneath the skin and a part
of the superficial fascia, in the cervicle or neck region.
It arises by thin fibrous bands from the fascia covering
the pectoral and deltoid muscles on the thoracic wall,
and passes upward over the clavicle and inserts the
lower jaw. This muscle is so delicate and the fibers so
finely divided that it is hardly perceptible. When the
skin is cut, the platysma muscle will as a rule be cut
[228]
too, and because of its thinness it will rarely be seen or
does it form any hindrance to the raising of the artery.
It is only mentioned here because it forms part of one
of the questions so often asked by the State Board in
their examination: “What tissues would you pass through
in raising the carotid artery?”
Having cut through the skin and platysma muscle, the
superficial fascia is next seen. In this part of the body
it consists of but a single layer and very thin.
The deep fascia lies next and constitutes a complete
investment of the neck. When this is torn or cut through
the sternomastoid muscle comes into view.
The sternomastoid, is a large, thick muscle, which
passes obliquely across the side of the neck, being inclosed
between two layers of deep fascia. It has its origin at
the sternum and clavicle and attaches to the mastoid
process of the temporal bone. By making the perpendicular
incision in the lower third, in as much as the
muscle slightly covers the artery, it can either be cut
or pushed to the outside of the incision. It is best to
push the muscle to the outside with the thumb, and with
the handle of the scalpel, work down deep through the
areolar tissue. The operator will now arrive at the common
sheath, or that part of the deep fascia surrounding
the artery, vein and nerve. The common sheath will be
very tough and a slit must first be cut, then it can be torn
the length of the incision.
The artery will now be seen lying next to the wind pipe
and the internal jugular vein to the outside. In the lower
third the artery will be about one-half inch deep, while
[229]
in the upper third it will be about one to two inches deep,
owing to the amount of fat in this region. In the upper
third, the omohyoid muscle crosses over the artery, which
must be either pushed aside or cut in two.
It is always advisable, to raise this artery in the lower
third, as it is less apt to show in that third.
Loosen the artery well from the surrounding tissues
with the aneurism hook, raise to the surface and place
a bone separator beneath the artery.
Now remove the individual sheath, incise the artery
and insert the arterial tube.
If it is desired to raise the internal jugular vein for
the withdrawal of blood, it is best not to open up the
common sheath, but to raise the artery and the vein both
at the same time. Having raised them to the surface
they can then be separated by the removal of the common
sheath and dropping it back into the incision.
If it is desired only to raise the carotid, the hook
should always be inserted between the artery and the
vein, and directed toward the trachea. If it is directed
around the artery in the other direction there is danger
of rupturing the vein, and thus getting a bloody incision.
The Circular Incision.—In the circular incision as
much of the skin as can be, is pushed above the clavical
bone from off the chest wall. The cut is then made from
one sterno-clavicular junction to the other following the
supra-sternal notch. This method was devised for the
use of the “Y” shaped tube, where both sides of the
face could be injected at the same time. One precaution
however should be noted, which is, that care should be
[230]
taken that not more than the skin, be incised with the
first cut. Just below the incision will be noticed a little
branch vein which runs into the arch connecting the two
external jugular veins. If the first cut is too deep this
branch will be cut, and a flow of blood will result. However
by cutting carefully this little branch can be noticed,
tied off in two places and cut in between, and thus cause
no further trouble. Remembering the linear guide, the
artery can be reached by going down at either end of the
incision. The tissues to go through will be the same as
for the perpendicular incision, and the method of raising
the artery will be the same, only, in the circular incision
usually both carotids are raised, so as to inject both sides
of the face at the same time.
The only advantages derived from the circular incision
is that one can by the use of the “Y” shaped tube
inject both sides of the face at the same time and get
an equal distribution of fluid, and that after the injection
is over, and the incision sewed up, the skin can be pulled
back in place, making the incision appear much below the
clavical, and where it is less liable to show than in the
perpendicular incision.
For embalming female subjects, if the carotid is chosen
as the artery to use, it will be best to use the circular
incision. However for ordinary embalming it will perhaps
be best to choose some other artery, which will be less
apt to show, and not so deep.
We should be so skilled as to never make a mistake,
but the best sometimes do make mistakes. If in raising
another artery, a mistake should occur, the operator
[231]
can raise either above or below the original cut, but with
the carotid, the only advisable incision to make is in the
lower third, and if a mistake is made the last chance is
lost. For this reason then a great amount of care should
be taken.
In injecting the body from the carotid, the arterial
tube should be inserted first toward the heart, and after
the body has received a sufficient amount of fluid, if it
is noticed that the side of the face from which you are
injecting has not received a supply of fluid, then reverse
the tube and inject a few bulbs of fluid upward.
Relation of Artery, Vein and Nerve.—The common
carotid artery lies in relation to the internal jugular
vein and the pneumogastric nerve. The artery lies to the
inside next to the muscles surrounding the trachea (windpipe).
The internal jugular artery lies to the outside of
the artery. Just back of the common carotid artery
and the internal jugular vein and between the two lies
the pneumogastric (vagus) nerve. These all as a rule
lie in the same common sheath of deep fascia.
How to Locate and Inject the Axillary Artery.
—The
axillary in recent years has come to be a much used
artery. It not quite as large as the common carotid, but
as a rule large enough to admit the large size arterial
tube. It has become a favorite with many because it
is quite easy to locate and to raise, and because of its
proximity to the axillary vein, a vein which is large
enough to admit a drainage tube for the withdrawal of
blood. Again the axillary artery is in a secluded place,
being as it is in the axillary space (arm pit). The artery
[232]
does not lie very deep, and is not covered by any muscles
as you operate, there being practically nothing to hinder
the progress of the operation.
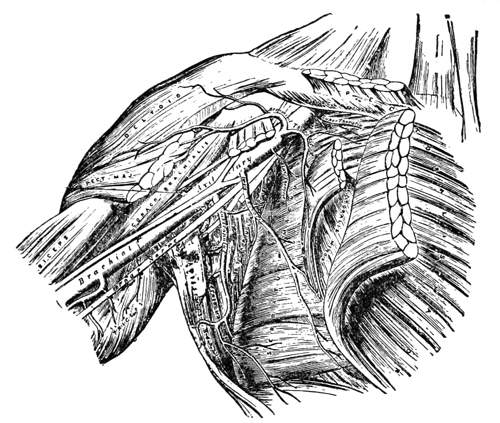
Fig. 47—The axillary and its branches. (Gray)
Then after the operation is completed and the arm
placed back in normal position, the casual observer is not
liable to see the incision, even though the body be only
partially dressed.
Linear Guide.—A line drawn through the center of
the axillary space (arm pit), at the anterior border of
the hair line.
The Axillary Space.—When the arm is maintained in
a horizontal plane, the axilla has the shape of a three-sided
pyramid, the apex of which lies above, below the
[233]
clavicle, and the base of which corresponds to the lower
wall, covered only by skin and fascia.
The axilla is filled with blood vessels, lymph vessels,
lymph glands, nerves, and masses of fat.
To Raise the Artery.—Make an incision on the linear
guide. After the skin is passed through there is a large
quantity of fascia, lymph glands, and lymph vessels,
which must be carefully dissected through, and at the
same time the axillary vein will be discovered. This
vein, for the present, should not be loosened from the
surrounding tissues. Dissect down to the upper side of
the vein, and the common sheath of fascia surrounding
the artery and nerves will be seen. By carefully tearing
this the length of the incision, the brachial plexus of
nerves now is exposed. Now by gently pushing the
nerves apart with the handle of the scalpel, the artery
will be seen. With a hook loosen the artery from the
surrounding tissues and raise to the surface.
If it is desired to draw blood, now proceed to raise
the vein to the surface. Open the vein and insert a drainage
tube, which should be long enough to reach through
the entire length of the axillary and subclavian veins,
because they have valves along their entire course nearly
to the bifurcation of the innominate.
Inject a few ounces of fluid toward the hand as the
axillary is above the point of collateral circulation. Then
reverse the tube and inject toward the heart, until a
sufficient amount of fluid has been injected.
Relation of Artery, Vein and Nerve.—The vein is
quite superficial, just below it and to the upper part of
[234]
the incision is the brachial plexus of nerves, which surrounds
the artery.
How to Locate, Raise, and Inject the Brachial Artery.
—The
brachial artery is located in the upper arm
and extends from the inferior margin of the muscle
pectoralis major, or from the shoulder to the elbow. It
is one of the most popular arteries known to the embalmer,
and is now used, perhaps, more than all others
combined.
The anatomy of this vessel is simple, yet, when we
take into consideration all the numerous anomalies or
irregularities that surround its use to us as embalmers,
we feel the necessity of making the description very thorough
and complete, in order to raise it under all the
various difficulties that attend its use.
The brachial artery has its several branches, the most
prominent of which are the artery profunda brachii (superior
profunda artery) and the artery collateralis ulnaris
superior (inferior profunda artery) and the artery
collateralis inferior (anastomotica magna artery).
For the sake of a more correct description we divide
the artery into thirds, viz: the upper, middle and lower
thirds. The upper third begins at the extreme upper
part of the arm and extends one third of the way to the
elbow, the middle and lower thirds occupy the remainder
of the artery. In the upper third we have the superior
and inferior profunda arteries coming off; their position
is not always the same, and in the extreme lower third
the anastomotica magna artery. These arteries continue
down the outer and inner arm and anastomose with
[235]
the recurrent radial and ulnar arteries, thus furnishing
collateral circulation. Thus if the fluid is injected in
the middle third, toward the heart, these branches that
come off the brachial in the upper third will convey the
fluid down the arm, filling the branches below the point
of injection, which supply the forearm and the hand.
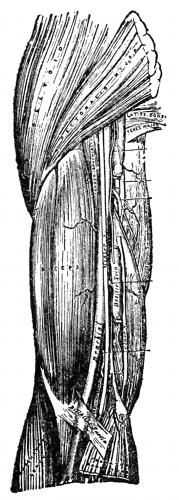
Fig. 48—The brachial
artery. (Gray)
The brachial artery is one continuous vessel, the entire
length of the upper arm, and varies in
size according to the size of the person
and the development of the arm.
It is accompanied by the venae comites
or deep brachial veins, the one to the
inner side of the artery about one-third
to one-half the size of the artery,
the other about one-half its size
lies directly underneath. All are encased
in the same common sheath of
deep fascia that surrounds and holds
them together. Great care, then,
should be taken to separate the
artery from these veins before cutting
the artery for injection.
The artery lies along the inner and
under border of the large muscle on
top of the arm known as the biceps.
The biceps is the muscle used when
lifting a weight. To those whose occupation
is to exercise the muscular
tissue of the body liberally, this
muscle becomes quite large, and generally the artery
is proportionally large.
[236]
Linear Guide.—The course of the brachial artery may
be marked out by drawing a line from the middle of the
axillary space (arm pit) to the center of the elbow, provided
the palm of the hand be turned upward. This
line will be immediately over the artery, which will be
found by cutting through the skin at any point on the
line, and dissecting through the subcutaneous tissue toward
the center of the arm.
The Anatomical Guide.—In the upper third the artery
lies between the biceps and coracobrachialis muscles which
lie above the artery, and the triceps muscle which lies
below the artery. In the upper third the nerve lies close
to the muscle, the artery below and to the inner side toward
the body, and the vein a little farther to the inside.
In the middle third the artery lies between the biceps
which lies above the artery, and the triceps muscle which
lies below the artery. In the middle third the artery
will lie beneath the nerve.
In the lower third the artery lies between the biceps
which lies above the artery, and the triceps which lies
below the artery. In the lower third the artery lies next
to the muscle and the nerve to the inner side next to the
body, and the vein still farther to the inner side.
How to Raise the Artery.—First trace the inner border
of the biceps muscle, feel for the median nerve, which
will always be present. The artery in the middle and lower
thirds will follow the border of the muscle. The palm
of the hand should always be turned upward, and the
linear guide, as stated above, will indicate the exact
position of the artery. Make an incision through the skin,
[237]
on the linear guide, pushing the fatty subcutaneous tissue
to one side, if there be any, and with the handle of
the scalpel, work through the superficial fascia. Reverse
the blade, and at each end of the incision, cut forward
and upward to make it clean. Now with the scalpel
cautiously cut through the deep fascia, and remove this
from the vessels below. This will expose to view the
median nerve, and with the handle of the scalpel, separate
the tissue between the artery and the muscle, and
between the artery and the nerve. Having thus freed
the artery, use the hook end of the aneurism needle and
pass it under the artery toward the muscle, and raise
the artery to the surface. Pass the bone separator or the
forceps with the closed end, underneath, remove the
sheath surrounding the artery and the deep brachial
veins. The natural position will be, the artery on top,
the larger deep brachial vein to the inner side and the
smaller one underneath. It is very necessary to remove
these deep brachial veins, for the reason that if they are
not, in cutting the artery for injection, they will be cut
also, resulting in a flow of venous blood into the incision.
How to Locate, Raise and Inject the Radial Artery.
—The
radial artery is one of the branches of the brachial
artery, and extends from about one half inch below the
bend of the elbow, along the valley of the forearm, to
the thumb part of the hand. It is divided into thirds, viz:
the upper, middle and lower thirds. It is accompanied in
close relation by the radial veins, but in no way do they
interfere with the operation of raising the vessel. The
value of this artery is in the embalming of ladies, where
[238]
the body has been dressed and the sleeve cannot be removed
to use the brachial artery without material inconvenience
and annoyance. It is especially desirable to
those who are just beginning to use the arteries.
The radial artery is somewhat smaller than the ulnar,
but, on account of the depth of the latter and inconvenience
of raising, the radial artery is the one artery in
the forearm which is generally used. It is an excellent
vessel to employ in cases where the friends are opposed
to embalming because of the mutilation of the body, as
they choose to call it. Some object to the use of this artery
on account of the fact that the mutilation is not
easily hidden. The wound can be easily covered by simply
pulling the sleeve down to its normal place. The incision
necessary to be made is so small and it can be closed
so neatly, that no objection on the part of the relatives
need be apprehended.
Before the advent of formaldehyde fluids the radial
artery offered more advantages to the embalmer than
any other artery used for injecting. But at the present
time almost all embalming fluids contain large quantities
of formaldehyde, and when injected into this artery,
which is very small, it is liable to constrict the vessel to
such an extent as to sometimes make it difficult to inject
the fluid.
Moreover, since both the radial and the ulnar arteries
have many branches, a large quantity of fluid is liable
to accumulate in the forearm, hardening it more
than is necessary and giving the hand an undesirable
color.
[239]
The radial artery is very superficially located, and
can be secured without the possibility of error and with
very little mutilation. The expert will, of course, choose
that vessel which he believes will at the time and under
the circumstances best serve his purpose.
The Linear Guide.—Is a line drawn from the center
of the bend of the elbow to the center of the ball of the
thumb.
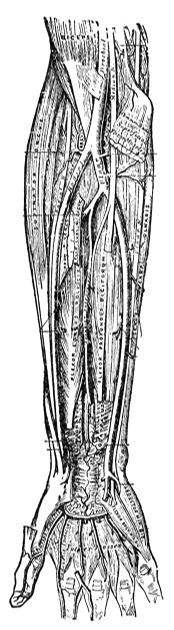
Fig. 49—The radial and
ulnar arteries. (Gray)
The anatomical guide for the radial artery (in the
wrist, where it should be raised) is the brachio-radialis
muscle on the outside of the artery and the flexor carpi
radialis muscle on the inside of the artery.
When about to raise this vessel, the embalmer should
hold the arm at right angles with the body, with the
palm up, and holding the hand of the body, with the
hand, draw the arm tight. In most bodies this will show
plainly the tendons of the muscles between which the
vessel lies, thus affording an excellent guide for the incision.
The arm should never be grasped and the tissues
drawn out of their normal position, as that is very misleading.
The vessel should be raised at a point about
three inches above the wrist joint (the space where you
would feel the pulse beat in life). The operator making
an incision through the skin, superficial fascia, and fat,
about one-half inch in length, will plainly see the artery
lying in its sheath between the two tendons of the muscles.
The cut should now be opened carefully, by placing
the fingers on either side of it, and the fascia dissected
from the artery, when it can easily be raised with the
aneurism hook. There is no other vessel at this point
[240]
that can be mistaken for the radial
artery. Its two venae comites, or
accompanying veins, are usually
attached to the artery and need
not be removed, as they are very
small and can give the embalmer
no trouble.
How to Locate, Raise and Inject
the Ulnar Artery.
—The ulnar is
the larger branch of the brachial
artery. It crosses obliquely the inner
side of the forearm, to the beginning
of its lower half, it then
runs along the ulnar border to
the wrist, crosses the annular ligament
on the radial side of the pisiform
bone (wrist bone), and immediately
beyond this bone into
two branches, the superficial and
deep palmar arch. In its upper
half it is deeply seated, being
covered by all the surface muscles.
It is crossed by the median nerve,
which lies to the inner side for
about an inch. In the lower half
of the forearm the artery runs
more superficially, and is covered
only by the skin and superficial
and deep fascia, but at that, the
ulnar lies a little deeper in the
wrist than the radial. The ulnar
[241]
nerve lies to the inner side in the lower half and the
ulnar artery is accompanied by two ulnar veins, one on
either side, called the venae comites.
The Linear Guide.—Is a line drawn from the center
of the bend of the elbow, to the inside of the pisiform
bone in the wrist.
The Anatomical Guide.—The artery lies in a groove
in the wrist, made by the flexor carpi ulnaris muscle on
the outside, and the flexor digitorum sublimis on the
inside.
To raise the ulnar artery, locate the valley in the
lower third about one to two inches above the pisiform
bone. Make an incision about an inch in length, cutting
first the skin, superficial fascia, layer of fat, which will
vary in thickness. The deep fascia is now reached, which
should be split by means of the fascia needle and bistoury.
Then separate with the handle of the knife or bone separator,
the artery from its connective tissue on either
side. Then with the hook raise it to the surface, and
place the bone separator beneath, remove the hook, and
tear off the individual sheath.
The two ulnar veins will be separated from the artery
by taking away the individual sheath, which should be
allowed to drop back into the incision. Proceed now to
open and inject the artery the same as you would the
radial or the brachial. While this artery may seem just
a little more difficult to raise, still at times it has its place
in arterial embalming.
How to Locate, Raise and Inject the Femoral Artery.
—The
femoral artery is usually objected to, because, situated
[242]
as it is, it requires an undue exposure of the limb,
especially in ladies. For this reason, then, the femoral
artery should never be raised in the female, excepting in
accidental case when it is impossible to raise any other
artery. In the male, however, the femoral with many is
a favorite. The artery should be raised either in the upper
or the middle thirds, but preferably in the former, as by
raising at this point the artery is not very deep in the
tissues as it will be further down, and at the same time
one is able to get collateral circulation to the lower leg
and foot by means of the deep femoral and the recurrent
anterior and posterior tibials.
It is believed quite commonly, that by the injection
of the femoral artery, there is a great danger of flushing
the face. This belief is erroneous. Flushing of the face
will result from the injection of any artery if it is full
of blood and if it is found that the femoral artery contains
blood, and likewise any other artery, this blood
should be removed before injection takes place, and what
little then remains, will not discolor the face, since it
will be greatly diluted.
The internal long saphenous vein is mistaken frequently
for the femoral artery. It is a superficial vein
and is usually found empty after death. It lies a short
distance to the inner side of the femoral artery in Scarpa's
triangle. This vein is taken up frequently, not only by
the younger members of the profession, but by the older
as well, when the guides are not followed closely, and
when this mistake does occur, and fluid is injected
through it, flushing of the face results.
[243]
Next to the common carotid artery the femoral artery
is the largest branch artery used in embalming. The
femoral artery commences immediately behind Poupart's
ligament and is a continuation of the external iliac artery.

Fig. 50—The femoral
artery. (Gray)
It passes down the forepart and
inner side of the thigh, terminates at
the opening in the adductor magnus,
at the junction of the middle with
the lower third of the thigh, where it
becomes the popliteal artery. In
the upper third the artery is contained
in a triangular space called
Scarpa's triangle and in the middle
third of the thigh it is contained in
an aponeurotic canal called Hunter's
canal.
At a point about one and one-half
to two inches below Poupart's ligament,
the femoral artery gives off a
branch to the outer and under side,
known as the deep femoral artery, or
the profunda femoris, which courses
the thigh downward, and connects
with branches coming off the popliteal
and the anterior tibial arteries, thus forming the
collateral circulation to the lower leg and foot.
As the femoral artery leaves the body, it is accompanied
by the femoral vein, which for two inches down,
lies along side the femoral artery to the inner and under
side. At about this juncture, however, it passes underneath
[244]
the artery and continues its course in that position
until it passes below where we have occasion to use the
artery.
The femoral artery can be used all the way from where
it leaves the body at Poupart's ligament until it reaches
Hunter's canal. At Poupart's ligament the artery is very
superficial, being covered only by the skin, superficial
fascia and superficial lymphatic glands, but it gets deeper
further down, being covered not only by the above named
tissues, but also by muscles, making it very difficult to
raise in the middle and lower thirds of the thigh. About
five to seven inches below Poupart's ligament the artery
passes under the adductor magnus muscle, and enters
what is known as Hunter's canal. Because this artery
does get deeper as it courses down the thigh, it is generally
raised in the upper third.
A knowledge of the anatomy of the vessels of the
thigh and leg will be of value in treating accidents when
this member is injured.
Scarpa's triangle is a triangular space, the apex of
which is directed downward, and the sides formed externally
by the sartorius muscle, internally by the inner
border of the adductor longus muscle, and above by
Poupart's ligament. The floor of the space is formed
from without inward by the ilio-psoas pectineus and the
adductor longus muscles. The space is divided into two
nearly equal divisions by the femoral vessels, which extend
from the middle of its base to its apex, the artery
giving off in this situation the superficial and profunda
branches, and the vein receiving the deep femoral and the
[245]
internal saphenous veins. Besides the vessels and nerves
this space contains some fat and lymphatics.
Hunter's canal is the aponeurotic space in the middle
third of the thigh, extending from the apex of Scarpa's
triangle to the femoral opening in the adductor magnus
muscle. Hunter's canal contains the femoral artery and
vein inclosed in their own sheath of areolar tissue, the
vein being behind and on the outer side of the artery,
and the long saphenous nerve lying at first on the outer
side and then in front of the vessels.
Linear Guide.—The guide for the femoral artery is
represented by a line drawn from the center of Poupart's
ligament to the inner side of the knee joint.
Poupart's ligament extends from the crest of the ileum
bone to the top of the pubic bone. To determine the
center of Poupart's ligament for the right leg, get on
the right side of the body and with the left hand, place
the second finger on the top of the pubic bone and the
thumb on the crest of the ileum bone, then let the index
finger drop down between the two which will represent
the commencement of the femoral artery.
Anatomical Guide.—The artery runs through the center
of Scarpa's triangle from the center of its base to
its apex. In the middle third of the thigh the artery
passes beneath the vastus medialis muscle and enters
Hunter's canal.
Relation of the Artery, Vein and Nerve.—The femoral
vein at Poupart's ligament lies close to the inner side
of the artery, separated from it by a thin fibrous partition;
[246]
but two inches down the vein runs behind the artery and
then to its outer side.
There is no nerve in relation to the artery in the upper
third, the anterior crural nerve lies about half an inch
to the outer side of the femoral artery, being separated
from the artery by the ilio-psoas muscle. In the middle
third of the thigh the internal saphenous nerve is situated
on the outer side of the artery, but not usually
in the same sheath with the artery.
To raise the femoral artery in its proper place, is to
measure down from Poupart's ligament from one and
one-half to two inches in the linear guide, and there begin
the incision, making it two inches or less in length.
This will bring the incision below the point where the
collateral branches are given off. Cut through the skin,
then the fat, which will vary in thickness with the subject.
Underneath the fat are several layers of deep fascia,
which must be split the length of the incision.
The femoral artery will then be seen, and underneath
it will be the femoral vein. Both will be in the same
common sheath of fascia, which may be removed with a
hook by gently tearing the sheath loose over the artery.
When the artery has been loosened the length of the
incision, raise it to the surface, placing a bone separator
underneath for a bridge.
If it is desired to remove the blood, the femoral vein
should then be raised.
[247]
CHAPTER XVII.
CAVITY EMBALMING.
Cavity Embalming.
—In shipping a body, cavity embalming
must always be resorted to and consists of introducing
a trocar into the abdominal and thoracic cavities
and injecting sufficient fluid over the contents of
these cavities to thoroughly preserve them.
The scientific work in the embalming of to-day is
being done on the arteries, but cavity embalming should
still hold an important place with those embalmers who
desire to get the best results. Although the arteries have
been injected, yet we find that sometimes the fluid does
not reach the cavities. Any cavity may contain gas or
material for decomposition, such as blood, pus, lymph,
or as in perforation of the intestines, feces in the abdominal
cavity. Besides these we always have the bacteria
of decomposition, called saprophytes, which have
thoroughly invaded the organs and tissues of the body
as soon as sixteen hours after death. Then, if for any
reason the fluid has not reached a certain part, fermentation,
and putrefaction will immediately set in.
The Cerebral Cavity.
—Gases may be generated in the
cerebral cavity soon after death, especially in drowned
[248]
cases, where the gas forming bacteria, the aerogenes capsulati,
are distributed all over the body. These bacteria
work much more rapidly in fresh or shallow water, or
in the summer when the water is warm, than in the
winter when the water is cold, or the body is in salt
water. The gases may penetrate every tissue in the body,
particularly the tissues about the eyes, which gives the
eyes their bulged appearance. The gases that are formed
in the brain and forced out into the tissues surrounding
the eye do not enter the eye ball. In these cases the eye
ball may or may not be pushed out of its socket, depending,
of course, upon the amount of gases that have
been produced.
These gases may be removed by inserting a trocar
inside the head at the inner angle of the eye or in the
nose through the turbinated process of the ethmoid bone.
After the gases have been removed from the inside
of the skull, about one-half pint of strong formaldehyde
fluid should be injected.
Another method of inserting the trocar into the brain
would be to pass it through the foramen magnum. This
can be done by inserting the trocar in the neck a little
below and behind the lobe of the ear, directing the needle
upward and inward toward the opposite eyebrow, when
the needle will enter the subarachnoid space (Barnes
Method).
In cases of hydrocephalus (water on the brain)
where there may be from one to two quarts of water inside
the cranium, the water may be removed by any of the
above processes.
[249]
For ordinary cases we do not feel that it is necessary
to make a cavity injection in the head for the reason
that the circulation there is complete, only in rare instances
do we find an obstruction.
Purging.
—By purging, as the embalmer uses the term,
is meant, the fluid which emerges from the mouth and
nose of the cadaver. If this fluid is a brownish coffee-like
substance, it signifies it is coming from the stomach,
but if it is a bloody frothy mixture it signifies it is coming
from the lungs.
The real cause of purging is the living and growing
saprophytic bacteria, which were normally in the body,
or having gained access later, produce as a result of their
development, gas formations. These gases confined as
they are, press out from the stomach and lungs the contained
fluids of the color mentioned above.
Purging from the stomach may either be due to the
presence of gases in the stomach itself, or in the intestines
or in both. If the gases have formed in the intestines,
they would dilate the canal sufficiently to fill the entire
abdominal cavity, thus pressing the stomach against the
diaphragm with enough force to cause the contents to
escape through the upper end of the alimentary canal.
Purging from the lungs is due to the presence of bacteria
of putrefaction, which begin to develope in the diseased
portions. These cause liquefaction of the lung
substance and the formation of gas. The gas will force
the liquefied matter, of a bloody, frothy color out through
the respiratory tract.
Before embalming of the chest and the abdominal
[250]
cavity is begun the trachea and the esophagus should be
treated in order to prevent purging. There are two
ways of doing this:
The first method consists of placing a ligature about
the trachea and the esophagus, this is done by making an
incision through the skin and tissues over the left edge of
the trachea, one-half inch above the top of the sternum.
Insert the right forefinger, passing it to the right side behind
the trachea and the esophagus to separate the tissues
from them. In doing this great care should be taken
so as not to injure the carotid on the left and the innominate
artery on the right side. Pass the aneurism
hook threaded with narrow tape (this must be very
strong tape) along the inner side of the finger, below
the trachea and the esophagus, to the point of entrance on
the left side. You will have no difficulty now in tying
securely both the above tubes, and there will be no possibility
of purging from either the lungs or the stomach.
The second method of preventing purging from the
lungs and stomach consists in plugging the pharynx
through the mouth, there-by plugging the trachea and
the esophagus. The only disadvantage of this method
is that it can not be done successfully after the body has
been embalmed arterially. And for this reason, after
arterial embalming, the lower jaw will be firmly set and
to use this method, it would mean that the lower jaw must
be pried back in order to gain access through the mouth.
Then it will be found very difficult and in some cases
impossible to set the lower jaw again in its proper position.
If this method is to be used at all, it is advised
[251]
that you do the plugging of the pharynx before the arterial
embalming has been done.
To do this, take your position at the head of subject
on the right side, and open the mouth wide enough to
admit two fingers. Roll several pieces of dry cotton,
the size of an English walnut, and holding the corner of
the mouth back with the left hand, insert a ball of
cotton with the right hand and shove it hard down behind
the tongue (this can best be done with a pair of
clamp forceps). Continue to do this until the pharynx is
well and firmly filled, but avoid bulging out the side of
the cheek. If properly done this plug will prevent an
ordinary amount of purging and dry cotton seems much
better to use for this purpose than absorbent. It must
be borne in mind that simply filling the mouth is of no
use; nothing is plugged by this procedure, as it leaves
the opening into the nose open.
If you had not anticipated purging in the beginning,
and the body has been embalmed arterially it will be
necessary to stop the purging by the first method.
A third method of preventing purging from the lungs
and stomach is in the use of plaster of paris. In this
method the plaster of paris is mixed thinly, then by means
of a paper funnel, pour the liquid into the nose and mouth,
then plug tightly with absorbent cotton as in method two.
It requires only a short time for the plaster of paris to
set and it has been found quite successful. Probably the
only disadvantage of this method is that it is mussy and
because of the rapid drying qualities of the plaster of
paris the operator must work very quickly.
[252]
The Thoracic or Chest Cavity.
—Cavity embalming
must be resorted to frequently in the chest or thoracic
cavity for the reason that in certain diseases, especially
tuberculosis, fluids cannot enter the diseased cavities, as
the capillaries and small vessels are destroyed by the
disease and the ends of the arteries securely plugged.
If this were not so, the patient would have died of hemorrhage
of those arteries, a thing which seldom takes
place.
Again in certain other diseases, especially pneumonia,
the fluid cannot reach the diseased lung, either through
the nutrient arteries or by the respiratory tract, because
of the resistance offered. The nutrient arteries will be
filled with coagulated blood and the bronchi, to a certain
extent, with a bloody mucous.
This being the case, the bacteria of putrefaction will
begin to develop within the diseased portions of the
lungs, and will be the cause of the purging so much
dreaded by the embalmer.
The thoracic cavity may be treated by one of several
methods.
A first method consists in passing a curved trocar
into the trachea just above the sternum and injecting a
strong embalming fluid into the bronchi. In cases of
gangrene of the lung, the sputum has a very offensive
odor, which may be disinfected by this method. But
it must be remembered that the ends of the bronchioles
which enter the diseased parts of lungs will be closed
(from the nature of the disease), so that any fluid injected
[253]
into the bronchi from the trachea will not reach
the diseased part of the lungs. You will thus see that
it is absolutely necessary to use a method in treating the
thoracic cavity, whereby any mass of rotten tissue, which
may be present, may become thoroughly saturated with
the disinfectant.
A second method written about the Robbins, is accomplished
by inserting the trocar on both the right and
left sides at the tops of the lungs, and at the bases. At
the top of the lungs the trocar is introduced two inches
outside the sternum just below the clavicle. The trocar
may then be pushed in any direction, except toward the
sternum, without injury to any of the larger vessels.
The arch of the aorta passes a little to the right of the
sternum and as high as the lower border of the first rib,
then makes a turn to the left and goes directly back to
the left side of the fifth dorsal vertebra. The superior
vena cava lies a little to the right of the arch of the
aorta. The advantage of inserting at this point rather
than above the clavicle is that there are no vessels in the
location in danger of perforation. If the trocar is inserted
above the clavicle on either the right or the left
side there is danger of perforating the subclavian artery
or vein, while if the insertion is made next to the sternum,
the aorta may be perforated, in either case breaking the
circulation. Disease fluids are seldom found at the top
or apexes of the lungs, but in consumption, breaking
down of the lung substance usually begins at this point,
especially in young cases. To insure a perfect embalming
of the lungs, you should inject at the apexes, about
[254]
a half-pint of strong formaldehyde on each side. It
should, however, be remembered that the injection at the
tops of the lungs, as suggested, gives no fluid to the lower
parts of the lungs where it is often most necessary.
It is not an unusual condition to find a whole lobe
rotten and broken down at the base of the lung, and when
such a diseased condition exists the lungs become firmly
attached to the chest walls, and unless fluid is placed
below these adhesions it does not reach the diseased parts.
The intelligent embalmer, will never trust to the fluid
passing from the tops of the lungs to the base, as in almost
all cases the adhesions between the lungs and the
walls absolutely prevent this taking place.
It is necessary first to draw off by aspiration, at the
bases of the lungs, the fluids which have accumulated and
which may be either water, pus or blood. This is done
by inserting a curved trocar of small size, between the
fifth and sixth ribs on the axillary line. The thoracic
cavity extends in the back as low as the last rib and the
twelfth dorsal vertebra and it may be necessary to pass
the trocar down into this part of the cavity in order to
remove the fluids.
As soon as the fluids are removed, inject from a pint
to a quart of strong formaldehyde on either side. By so
doing the gangrenous and decomposed part of the lung
will be put to soak in the embalming fluid, which will insure
perfect disinfection and an absence of bad odors.
Abdominal Cavity.
—Often it will be found necessary
to do cavity work in the abdominal cavity. Gases may
arise causing a distention of the abdominal wall, resulting
[255]
in purging from the mouth and nose. This gas
is the result of putrefaction and fermentation in the alimentary
canal. When one of the principle arteries is
injected, the fluid finds its way to the minute capillaries
of the organs of the abdominal cavity, including the
stomach and the intestines. It must be remembered that
often there is a great amount of undigested food and
fecal matter in the stomach and intestines. The only
way the fluid which is in the minute capillary circulation
of the stomach and intestines, is able to reach the inside
of those organs and come in contact with the undigested
food and the fecal matter is by soaking through the
mucous wall. No doubt a certain quantity of the fluid
does soak through, and when it does, if there is not much
undigested food or fecal matter in these parts, disinfection
will be accomplished and it is in these cases that
we do not have any trouble with distentions of the abdomen.
When however, there is a great amount of undigested
food and fecal matter inside the stomach and
the intestinal tract, it is only obvious that enough fluid
can not possibly soak through to disinfect, and consequently
a host of putrefactive, and fermentative germs
will begin their work, with the formation of gases and
the distended abdomen, and perhaps purging from the
mouth and nose.
To prevent the formation of gas now which has arisen,
a second injection will do no good. More drastic measures
will have to be used. One method that has long been in
vogue is the use of the trocar.
The Trocar Method.—In this method a trocar varying
[256]
in length from six to fourteen inches is used. It may
either pierce the abdominal wall through the umbilicus, or
two inches above and two inches to the left of the umbilicus.
Then after the trocar has entered the abdomen
the secret of removing gases successfully depends very
largely upon the operator having a very correct idea of
the location of all the abdominal organs. It is difficult
to know when the trocar has pierced the interior of the
stomach, or in fact even to make it pierce the stomach
at all for the peritoneum which is a covering for all the
organs of the abdominal cavity contains a serous fluid
which makes the organs slippery, and even the sharp
pointed trocar often does not take hold as it should.
Again it must be remembered that the stomach is a hollow
organ, and for example let us try to pierce a soft
rubber ball, containing air and a small opening, a condition
resembling the stomach, with a trocar, we know
that the one wall, will have to be pushed up against the
other wall, and then placed against something firm,
before the trocar will pass through. Just this condition
happens with the stomach when the trocar tries to pierce
the arterial wall of the stomach there is nothing solid to
bear against and consequently the front wall will be
pushed up against the back wall and then if enough pressure
is now used to push the trocar through, it is very
liable to pass all the way through both walls.
Again it must be remembered that the descending
aorta passes very close behind the stomach and should
the trocar go all the way through the aorta might be
pierced and the circulation in a measure ruined. The one
[257]
main disadvantage of this trocar method is that the operator
is always working blindly, it is always impossible to
tell just how much damage may be done to the internal organs
and the circulation, and again should the operator
desire to place fluid in a certain part—say the inside of
the intestines or the inside of the stomach or the colons,
will the operator have assured knowledge that he has
actually placed the fluid in the part desired. From the
number of experiments that have been carried out in our
anatomical rooms, the proof seems to be in every case that
the fluid has not reached the part it was supposed to reach.
The advantage of this method is the fact that by introducing
the trocar into the abdominal cavity two inches
above and two inches to the left of the navel that after
the abdomen has been treated that the trocar then can
be directed upward into the thoracic cavity and fluid
there distributed to the several parts, but this is seldom
necessary. After the trocar has been removed or better,
just before the trocar is entirely pulled out the operator
should sew a circular stitch about the wound and then
as soon as the trocar is pulled out, pull the stitch closely
together as if it were a draw string, and tie. This will
prevent any further leakage from the part.
The Direct Incision.
—Sometimes before the body is
embalmed or a day or two after the body has been embalmed,
there is a distention of the abdominal wall indicating
gases and there may or may not be purging
from the mouth and nose. From the great number of
cases that have been posted in our anatomical laboratories,
it has been found that the gas that has accumulated
[258]
is as a rule located in either the stomach, the transverse
colon, or the colons in general, but rarely in the
small intestines to the extent that it would do much damage.
By the use of the direct incision, make a cut with
a sharp scalpel, about three inches long in the median
line of the body over the abdomen. Start the cut about
one inch below the ensiform process of the sternum and
cut toward the navel. After a cut has been made three
inches in length on the skin, direct the scalpel downward
so that it enters the abdomen. Place the index and
second finger in the incision thus made pressing the organs
from the abdominal wall, and carefully cut upward
between the two fingers. This will prevent the operator
cutting any of the underlying intestines.
The incision having been made, it is evident now that
the part containing the gas will come up into the incision.
If the stomach contains the gas it will come up, if the
transverse colon contains the gas it will come up, but
that makes no difference, for it is the part with the gas
that the operator is after. Usually the transverse colon
will be the first to come up into the incision, now take
hold of the part with your artery forceps and with a pair
of scissors make a clip through the wall, this will let the
gas escape. Do not let the gas escape into the room
not deodorized, so place over the hand quickly after you
have made the clip, a towel, or absorbent cotton that has
been saturated with formaldehyde, this will both deodorize
and disinfect the gas. Keep hold of the part until all
the gas has escaped, and then pick up the arterial tube
and inject a small quantity of fluid in the colon, and
[259]
then sew up with the circular stitch. Then locate the
stomach, which can easily be found if it contains gas
and treat it in the same way, relieving the gases and then
placing a small amount of fluid inside. Treat the other
several parts of the intestines in the same way if gas be
present and it is remarkable how quickly the abdomen
sinks to its normal level. After this has been done place
hardening compound or common salt in the cavity, and
placing a layer of absorbent cotton in the abdomen under
the incision, sew up neatly.
The one great advantage of this method is that you
can actually see what you are doing, you can see the
part that contains the gas and treat that part particularly,
the operator is not working blindly, but is able to
place the fluid in the part that he desires and is assured
of the fact that it is in the part for his eyes do not deceive
him as the sense of feel and touch sometimes do. By
this method the operator is able to surround the parts of
the abdominal cavity with a hardening compound, and
thus feel sure that his case if it is to be shipped, will
be received in proper condition, at least it will be as
far as the abdomen is concerned, if it is treated under
this method. This method is one sure cure for purging,
for the gases once properly relieved from the stomach
and the contents disinfected, there is no chance for them
to recur. If the stomach is found to be full of liquid as
well as of gas, as is the condition during purging, the
liquid can be taken from the stomach with a drainage tube
or a stomach pump, and lastly every part is deodorized
and disinfected properly.
[260]
A seeming disadvantage might be that a critic might
suggest that you are mutilating the body with your abdominal
incision. Let a fair question be asked. If it were
your sister that was to be embalmed and gases had to be
removed, which would you rather see some operator running
a trocar here and there through the abdomen, relieving
gases and injecting fluid here and there, or, the
use of the neat surgical incision, made as a surgeon would
make it.
Embalming of the Subcutaneous Tissue.
—It is not
always possible to fill the tissues of the body through the
arterial system, the arteries may be full of blood in a
coagulated condition so that it can not be removed, the
walls of the arteries may be diseased, or they may be severed
at many places the result of accidental death, such as
railroad accident, etc. If any of the above conditions be
present or other similar conditions, it will be impossible
to inject the arterial system, or it may be that arterial
injection is only partly possible. In order, in arterial
embalming, to have the tissues embalmed the fluid must
reach the capillaries, and to fill the capillaries it is first
necessary to fill the larger arteries. So if for any reason
it is impossible to reach all or certain tissues by arterial
embalming, it becomes necessary to resort to some other
means.
With these difficulties then in view, the best operation
for filling the tissues, that is the subcutaneous tissue
covering the bony framework of the body, is the direct
injection of fluid into the part by means of (1) the hollow
needle trocar, and (2) the hypodermic needle.
[261]
The hollow needle trocar is to be used for the rough
work, so called. Inserting the trocar into the center of
the popliteal space it can be pushed through the tissues
of the foreleg, and fluid injected; then reversing, push
the trocar through the tissues of the leg proper, and inject
fluid. Inserting the trocar into the center of the
bend of the elbow it can be pushed into the tissues of the
forearm, and fluid injected; then reversing, push the trocar
through the tissues of the arm proper and inject fluid.
Turn the body over so as to trocar the back. Insert the
trocar above the sacrum bone in the middle line of the
back, and push the trocar through the fleshy parts of the
gluteal regions, and inject fluid. Again insert the trocar
in the middle line of the back between the two scapulae
bones, and inject fluid into the region of the shoulders and
the small of the back.
After each puncture, before the trocar is removed a
circular stitch should be thrown around the trocar and
when the trocar is removed draw the puncture shut, the
circular stitch acting as a draw string.
A large amount of fluid may be injected in this manner,
it being possible to inject several gallons into a body
of average size. The fluid transudes through the tissues
very readily filling them up completely, but of course, not
as certainly as if the fluid were injected arterially. It
is an easy matter to inject from two to three gallons of
fluid into the soft tissues on the outside of the skeleton
of a body weighing from 130 to 140 pounds.
This procedure is only to be used if it is impossible to
inject the body by the ordinary arterial embalming. The
[262]
cavity work in the cerebro-spinal, the thoracic, and the
abdominal cavity, should be done first, and then follow
with this subcutaneous tissue outside the bony framework.
This procedure may be used in dropsical cases and
in certain cases, where for some reason the fluid does not
reach a certain part, or where a certain part is not completely
supplied with fluid, by the arterial injection.
The hypodermic needle is to be used for the more
delicate work, such as the hands and the face. Insert the
needle at the wrist and direct it into the palm of the hand,
inject a very small quantity of fluid; then into the back of
the hand and inject a small quantity of fluid.
To reach the tissues of the face insert the needle into
the muscles and tissues of the face from the inside of the
mouth. The region about the temple can be reached
by inserting the needle into the tissues in the hair line,
which will hide the puncture.
With the use of the hypodermic needle fluid can be
placed in contact with all the tissues of the hands and
face, and the cosmetic effect will be almost perfect if the
operator is careful as to the amount he injects, and is
careful to see that, the fluid is equally distributed throughout
the part.
Plugging Orifices of the Body.
—The proper manner
in which to plug the orifices of the body is to use a pledget
of absorbent cotton dipped in your embalming fluid
and forced into all the orifices, following this up with a
pledget of dry absorbent cotton. In this the fluid disinfects
the surface with which it comes in contact and
the dry cotton prevents the outgoing of the germs from
[263]
the body or the passage inward of bacteria. It must be
understood that absorbent cotton filters out germs from
the air, even though air passes through it, they become
entangled in the meshes of the cotton and there remain.
Removal of Urine.
—As a rule, in the last throes of
death, the bladder is emptied, but in some instances this
is not done and then it becomes necessary for the embalmer
to remove the urine. This may be done in two
ways. Use the steel catheter, insert it in the bladder
through the urethra, and draw off the urine, or use the
trocar and insert it through the abdominal wall in the
median line just above the pubic bone, directing the
end of the trocar into the bladder which lies just below
the pubic bone and draw off the urine. It is seldom
necessary to inject the bladder with fluid, as after the
urine has been removed, we find from general experience
that it is well supplied with fluid from the arterial injection.
In the male it is wise to tie a string about the penis
just back of the head, or glans, while in the female it is
best to plug the meatus of the urethra and the vagina
with cotton.
[264]
CHAPTER XVIII.
THE REMOVAL OF BLOOD.
The Removal of Blood.
—In November 1882, Prof.
J. H. Clarke and Dr. C. M. Lukens, while instructing a
class in Philadelphia, in taking up the carotid artery,
the internal jugular vein was injured and a flow of blood
followed much to their dismay. This however turned
out to be one of the greatest events that ever happened
for the embalming profession, as it marked the beginning
of the practice of the removal of blood from the body.
There are some very important reasons why blood
should be removed from the body.
(1) There may be discolorations on the body, especially
the face. This discoloration may be due to
the presence of blood in the minute capillary system and
other vessels which are near the surface skin. This
discoloration may be due to the presence of the bile pigments
in the blood, which would tend to give the body a
yellowish hue. This discoloration may be due to the
breaking up or disintegration of the blood corpuscles
after death, which would tend to give the tissues of the
body a light, pale, yellow color. Or this discoloration
may be due to the presence of chromogenic bacteria, or
[265]
color producing bacteria, in the blood, which might give
to the tissues a characteristic green color.
(2) There may be blood in the arterial system after
death, which certainly will have to be removed or else it
may be pushed into the tissues of the face during the injection
of the fluid and cause a discoloration. Besides if
the arteries are congested with blood, this will have to be
removed to make room for the embalming fluid, so that it
will reach the capillaries and the tissues of the body.
(3) There may be the formation of tissue gas, and
there is no doubt but that the removal of blood will greatly
facilitate in the treatment, for without the blood, the
fluid will have more chance to act on the parts containing
the gas. This gas may be in the blood vessel itself,
and the removal of that blood then will relieve the gas
and the pressure exerted by the gas, which will aid in
the injection of the fluid.
(4) To prevent a hasty decomposition. It may be
that our subject is very heavy and fleshy which will mean
that there is more tissue to be preserved and necessarily
more fluid will have to be used. To make room for this
increased amount of fluid, blood should be removed.
It may be that the body is in a hydropic condition.
The tissues and the blood vessels will be filled with water.
This will mean a hasty decomposition. The watery blood
should be drawn from the blood vessels in order to make
room for more fluid than ordinarily.
It may be that the body has died of a fever, which will
also mean a hasty decomposition. This will mean that
the blood will soon coagulate after death, and therefore
[266]
the sooner it is removed, the better for the general cosmetic
effect.
We do not however believe that blood should be removed
from every subject, in order to get good cosmetic
effect. Rather there are times when blood should not be
removed, the conditions which are as follows:
(1) In the thin emaciated subject where there is no
discoloration. An example of this condition would be
in the tubercular subject, where before death the body has
become very thin and emaciated. We would not remove
blood when the subject is in this condition, for as a rule
the body will take plenty of fluid, the arteries are as a
rule empty after death, and besides we desire to leave
the blood in the body, in order to give the skin of the
face a more filled out healthy cosmetic effect.
(2) In the pale, marble-like, anemic subject. We
would not remove blood in this case, first because it is
not necessary, for there is a lack of blood in the surface
capillaries showing that the arterial system is completely
empty, and there is no congestion of the veins; secondly,
experience teaches us that in these cases, you probably
would not get any blood if you did try to remove it, and
thirdly what little blood is in the surface capillaries is
needed to build up a more healthy cosmetic effect.
There are times when blood should be removed from
the subject after death which are as follows:
(1) Whenever blood is found in the arterial system.
An example of this might be found in those cases of sudden
death, such as drowning, suffocation, electric shock,
or general heart failure. Whenever there has been a
[267]
case of sudden death, the operator may expect to find
blood in the arterial system. The last contraction of the
heart normally would drive all the blood out of the arteries
and arterial capillaries into the venous capillaries
and veins, but this is not accomplished in the cases of
sudden death. Whenever, on incising an artery, you
find blood in the artery, and it runs freely, it indicates
that there is a considerable quantity of blood in the arterial
system. This blood then should be removed, because,
were fluid to be injected into the artery, when it
is full of blood and in this congested condition, all of
this blood would be pushed ahead of the fluid toward the
center of pressure, and from there large quantities would
be pushed back into the tissues of the face, which would
result in a greatly discolored face and a very poor cosmetic
effect. DO NOT FORGET. Always remove blood
when you find it in the arteries. The regular blood
drainage tube should be placed in the artery, and all the
blood removed that is possible, before attempting to inject.
If this blood is not removed, the operator need not
be surprised if he causes a decided blood discoloration of
the face and a bad cosmetic effect. In these cases blood
should be removed from the veins too, for that procedure
will help to make room for what blood does remain in
the arteries and capillaries, so that it can be pushed by
the fluid into the veins rather than the tissues of the face.
(2) When the venous blood vessels are congested with
blood and gas. An example of this might be found in
almost any case. When the operator makes the incision
to disclose the vessels and finds the venous channels
[268]
congested, or when over the body the surface veins show
signs of congestion and distention with gases, then blood
should be removed.
(3) In dropsical cases. Often in these cases the tissues
throughout the body are in a hydropic condition
(filled with water), the arteries as well as the veins are
filled with a watery, bloody colored fluid. It will be
best for the operator to remove all this watery blood
from the arteries, veins, and the tissues also, in order to
get the greatest amount of preservative action from his
fluid.
(4) In heavy, fleshy subjects. Experience teaches
us that these bodies are as a rule difficult to handle from
a cosmetic, as well as from a preservative standpoint.
It seems advisable to draw blood from these subjects
whenever possible, and by so doing bring about a clear
non-discolored cosmetic effect; also the removal of blood
will give more room for a greater supply of fluid, and
thus the tissues will be better preserved.
(5) When the face is discolored. Whenever the
operator takes charge of a body and finds the face discolored,
no matter what the cause of the discoloration
may be, it is a good indication to remove blood from that
body.
By removing blood from the larger venous channels,
the operator will make room for the blood to leave the
face, and in this way better cosmetic effect is assured.
Massage the face toward the internal jugular vein, and
push the discoloring blood from the tissues of the face,
[269]
out into the larger channels, that have been emptied by
the removal of blood.
(6) In fever. Whenever a body dies in a high state
of fever, it indicates a hasty coagulation of the blood, and
a tendency to a discoloration of the face. Whenever the
operator knows that the subject has died of a fever, or
when there has been considerable fever on the body
before death, then blood should be removed.
(7) To make room for fluid. The average embalmer
only injects a gallon to a gallon and a half of fluid into
a body. There are times when the operator desires to
use more fluid. It may be that the body will have to be
shipped a long distance, perhaps to another country or
a distant state. After a certain amount of fluid has been
injected the vessels become filled up and there is a great
resistance established. If the operator disregards this
pressure, and forces still more fluid into the arterial system,
the fine capillary network will be broken, especially
in the lung where the result will be a leakage of fluid
through the mouth and nose from the ruptured air cells
in the lung, or in the tissues of the skin, where the result
will be a leakage into a certain area of tissue later
causing a condition known as leathery skin. To have
prevented this the operator should not have forced the
fluid beyond a certain maximum resistance. He could,
though, have reduced this resistance by removing the
blood from the venous system, and then succeeded in the
further injection of fluid.
There are times when blood ought to be removed from
a subject after death, but for some reason it seems impossible
[270]
to remove any. The reasons may be stated briefly
as follows:
(1) The blood may already be in a coagulated condition,
owing to the fact that the body has died in a
state of high fever.
(2) The blood may be in a coagulated condition
owing to the fact, that the bacteria of decomposition and
putrefaction, have so altered the blood as to make its
removal impossible.
(3) Certain drugs may have been previously given,
or taken during life which would cause a hasty coagulation
of the blood.
(4) The body may still be in a condition of rigor,
and although the operator may have released the rigor
in the joints, still all the tissues are in that condition,
a condition which might prevent the blood from draining
from the veins no matter what method was used.
Arterial blood is removed from the aorta indirectly,
and from the arteries, only when the arterial system contains
blood after death.
Venous blood is removed from the right side of the
heart directly or indirectly, and the veins, only when
it is deemed necessary by the operator.
There are two methods of removing this arterial or
venous blood from the body. These two methods are
aspiration and drainage. Besides these two methods some
modified methods or combinations of the two, are given.
Aspiration consists in actually pumping the blood
from the heart, arteries or veins. In this method, if
blood is to be taken from the heart directly, the trocar
[271]
is used; if the blood is to be taken from the heart indirectly
or from the arteries or the veins one of the drainage
tubes is used. Either the trocar or the drainage
tube is connected by rubber tubing, to the goose neck on
the blood bottle, which in turn is connected by rubber tubing
to the aspirator side of the aspirator and injector pump.
When the air is drawn from the blood bottle, there is a
vacuum formed, which will aspirate or draw the blood
from the heart directly or indirectly from the arteries or
veins. The one great disadvantage of this method is
that if the vacuum is made too great, the artery or vein
will collapse ahead of the drainage tube and thus prevent
the successful aspiration of the blood.
Drainage or gravity consists in opening one of the
principle arteries or veins of the body, inserting a blood
drainage tube into the artery or vein as far as it seems
practical, and then connecting the blood drainage tube
to the blood bottle by means of rubber tubing. The blood
bottle should be placed considerably lower than the body
in order to have the blood drain successfully. If the
femoral artery or vein is used, the body ought to be on a
considerable incline, the head at least one foot higher
than the feet in order to get the maximum amount of
blood.
If the axillary, brachial, or carotid, or their corresponding
veins are used, the body ought to be on a level
or turned to the side of the opening veins.
Simple drainage in itself is not a very successful
method of getting the maximum amount of blood from
the body.
[272]
The process can be modified in three ways which are
as follows:
(1) By placing the blood drainage tube in the vein
and the arterial tube in the corresponding artery. Inject
fluid into the arteries which will tend to push the
blood in turn from the capillaries into the veins, and out
into the drainage tube into the blood bottle. This modified
method has been called by Robbins “Displacement.”
This is a good name and one which should be generally
adopted.
(2) By placing the blood drainage tube in the artery
or vein, preferably the femoral, and connect it by
means of rubber tubing to the blood bottle. The operator
now stands at the head of the subject, he reaches
over, takes hold of each hand of the subject, raises the
arms of the subject to right angles with the subject, then
crosses the arms and with a steady gentle pressure bears
down on the chest of the subject over the heart region.
If the axillary is used the operator is able to manipulate
but one arm, the one opposite. Raise this arm to
right angles with the body then fold down on the chest,
exerting an even steady pressure. By raising the arms
the blood will leave the hands, and each time pressure
is exerted on the chest blood begins to flow from the
artery or the vein, and will continue to flow as long as
the even pressure is exerted.
(3) By the combination of number one and two. The
operator opens the artery, preferably the femoral, inserts
the arterial tube, and injects a pint of fluid to exert
a pressure on the venous system. He then opens the vein,
[273]
inserts the blood drainage tube which is connected with
the blood bottle. With the pump in his right hand (granting
that he is using the aspirator and injector pump), he
stands at the head of the subject and slowly injects the
fluid. If at any time the blood ceases to flow, by taking
hold of the hands, raising both arms at right angles to the
subject, crossing, and while in this position injecting a
few ounces of fluid, then bear down gently on the chest
with a steady pressure. If the blood will not flow by this
method and the operator is using either the axillary or
the femoral, there is hardly any use of trying any other
method. The operator will be able to draw the maximum
amount of blood with this method, if it is at all
possible to draw blood.
Often when the blood stops flowing, there is a blood
clot formation ahead of the drainage tube. By injecting
just a few ounces of fluid or salt water through the tube
into the vein, the clot may be pushed to one side, and
the blood will continue to flow.
Removal of Blood from the Right Auricle of the Heart.
Direct Method.
—Insert the trocar in the third intercostal
space, just to the right edge of the sternum or the breastbone.
The trocar should be inserted obliquely, the point
of the trocar is to pass in the general direction of the
left hip joint, while the open end of the trocar is to point
in the general direction of the right ear. A general knowledge
of the anatomy as far as the location of the heart is
absolutely necessary to master this procedure. The object
is to have the point of the trocar pierce the right
auricle of the heart. When the trocar has pierced the right
[274]
auricle, which the operator will have to judge through
practice, attach rubber tubing to the gooseneck of the
blood bottle and by the use of the aspirator pump, draw
the blood from the heart into the blood bottle. This is
removal of blood by aspiration.
Removal of Blood from the Right Ventricle of the Heart.
Direct Method.
—Insert the long thin twelve or
fourteen inch trocar two inches above and two inches to
the left of the navel and pierce the abdominal wall, pass
the trocar keeping the point close to the abdominal wall,
in the general direction of the right shoulder as far as
the lower border of the third intercostal space, without
fear of breaking any circulation. The right ventricle will
thus be reached from which blood can be aspirated as
in the previous method. Here again a general knowledge
of the anatomy as far as the location of all the organs
in the upper abdominal and thoracic cavity is necessary
to perform a successful operation. This is removal of
blood by aspiration.
Removal of Blood from the Right Auricle of the Heart.
Indirect Method.
—Make the incision for the femoral artery
and vein.
Raise the artery and inject about a pint of fluid in
order to cause a pressure on the venous system. Open
the vein and insert the flexible rubber drainage tube,
known on the market as the Red Seal drainage tube or
the Worsham drainage tube. Push this tube up through
the femoral, external iliac, the ascending vena cava,
through the eustachian valve, and into the right auricle of
the heart.
[275]
In order to determine when the tube is inside the right
auricle, the operator should have laid the tube on the
external surface of the body from the point of entrance
to the point where the right auricle normally should be,
allowing for the bend of the vein in its course. Mark the
tube, then when it has been pushed into the vein to that
point the operator is reasonably sure that the end is in
the right auricle.
In order to make the tube slip easily it should be
greased with a liquid solution of vaseline.
After the tube has reached the right auricle the blood
may be allowed to drain, or it may be aspirated.
Either femoral may be used, but the left femoral is
preferable owing to the fact that, the angle at the bifurcation
of the ascending vena cava is more obtuse.
If the operator desires to remove blood from the
heart, we believe that the indirect method is the better
way. By the use of the direct method to draw blood
from the right auricle by means of the trocar there is
always danger of rupturing the circulation. The aorta
may be accidently pierced. When the trocar is inserted
from below to reach the right ventricle the stomach may
be punctured and the liver and diaphragm will have
to be pierced which, too, may mean an injured circulation.
If any accidental damage has been done, it can
not be remedied. The direct method is a blind procedure
and is always uncertain. On the other hand if the
flexible rubber drainage tube is inserted into the vein it
must follow the channel of that vein. It is more certain
[276]
than the trocar method and there is no danger of rupturing
the circulation.
The basilic or axillary vein may be used to remove
blood from the heart instead of the femoral. These veins
should be used on the left side of the body owing to the
fact that the angle at the junction of the subclavian
and internal jugular veins is not so acute as on the right
side.
Removal of Blood by the Use of the Femoral Vein.
—The
use of the femoral vein is considered by some operators
a very good method. The femoral should be employed
in the upper third. Make the incision in the
center of Scarpa's triangle, just below Poupart's ligament.
The incision should be about two inches in length, the
length of the incision usually depends upon the size and
thickness of the thigh and the depth of the vein in the
tissue. Expose the artery and the vein. The vein at
this point will lie to the inside of and a little below the
femoral artery. Open the artery and inject about a pint
of fluid to cause a pressure on the venous system.
Have all the blood drainage outfit in readiness then
open the vein and quickly insert the drainage tube. Any
of the drainage tubes now commonly sold on the market
are good. For the femoral, though, the flexible rubber
drainage tube seems to be the best, because the femoral
vein dips deep down into the posterior part of the abdomen
after it leaves the Poupart's ligament. The flexible
rubber drainage tube will follow this bend and can
be pushed as far as is desired by the operator, in contrast
[277]
the steel drainage tube could only be pushed into the vein
for a few inches.
Blood ought to drain out into the blood bottle, if it
does not, inject a little more fluid to cause more pressure
on the venous system, and if it will not flow by the
drainage method or any of its modifications try the aspirator.
If blood still will not flow, it may mean that there
is a clot ahead of the drainage tube. Pump some fluid
through the drainage tube into the vein, to see if the
tube is open, then let the fluid drain out which usually
will bring some blood. After you have tried all the
methods, if blood still does not flow, it will indicate that
the blood is either in a coagulated condition, or there
is not very much blood in that particular vein, which
in this case is the femoral. The blood may be more in
the dependent parts of the body.
Removal of Blood from the Axillary Vein.
—The axillary
vein is of large size, and is formed by the junction
of the venae comites or deep brachial veins with the basilic.
The axillary vein begins at the lower part of the
axillary space, increases in size as it ascends by receiving
tributaries corresponding in name with the branches of
the axillary artery and terminates immediately beneath
the clavicle at the outer margin of the first rib where it
becomes the subclavian vein. To remove blood from the
axillary vein, raise the vein to the surface, and insert
the drainage tube. The Eckels-Genung steel drainage
tube will perhaps be the best tube to use. Insert the drain
tube high up in the arm pit, pass through the subclavian,
to beyond the valve located in the subclavian vein outside
[278]
the point at which the internal jugular vein unites
with the subclavian to form the innominate. There being
no more valves the blood should pass out freely. If the
blood does not flow, raise the axillary artery, begin the
injection of fluid which will tend to cause a pressure
through the capillaries on the venous system pressing the
blood back to the right auricle of the heart as in life, and
as there is no obstructed passage the blood should flow
freely from the tube. The vein tube is of metal having a
plunger rod within, and a Y attachment at the upper end.
The blood runs from the Y shaped attachment into a
rubber tube which is connected with the blood bottle. A
flexible arterial tube should be used in the artery, which
will measure eight to ten inches in length and constructed
with a shut-off valve. The tube will reach the innominate
artery close to the arch of the aorta. With these arterial
and drainage tubes the arms can be folded and placed
in position, with the hands over the abdomen and the
tubes will extend out over the upper border of the arm.
This method will enable the operator to inject the body
and have the arms in their natural position. If a short
circuit through the internal mammary vessels occurs, and
this will be evidenced by the premature flow of thin
blood, close the vein tube now and then during the operation,
continuing the injection until the proper results are
obtained.
Removal of Blood from the Basilic Vein.
—To withdraw
blood from the basilic vein the left arm should be
employed, because of a more direct route to the right
auricle. Make the incision in the middle or the upper
[279]
third of the arm. The basilic vein lies in the upper arm
and extends from the elbow to the shoulder, and can be
found a short distance from the brachial artery, either
above or below, but generally below and toward the
body. Its position is not always the same, owing to the
many anomalies that might occur. As a rule the vein is
quite large and prominent and when secured, raise to
the surface freeing it from the surrounding tissues.
Prepare two ligatures, make the incision in the vein
and pass gently the basilic drainage tube upward toward
the heart. Either a steel or rubber tube may be used. If
the flexible rubber tube is used, it will find its way to the
right auricle of the heart, its course is through the basilic,
axillary, sub-clavian, innominate, superior vena cava, to
the right auricle. Either the aspiration or the drainage
methods may be used. If these fail try the displacement
method.
The use of the basilic for the removal of blood is fast
disappearing from general practice. Larger veins can be
used, which will always insure greater success.
The Removal of Blood from the Internal Jugular Vein.
—The
internal jugular vein is the largest tributary vein
in the body, and accompanies the carotid artery. The
operator will cut through the skin at a point from one
half inch above the clavicle or collar bone and in the
valley formed by the sterno-mastoid muscle to the outside
and the muscles of the wind pipe to the inside, cut
upward making the perpendicular incision. Raise both
the artery and the vein according to the usual method.
It seems best to raise the artery and the vein together,
[280]
and by so doing this will tend to give added strength
to the vein which is very large but has quite thin walls.
Direct the hook around the vein first then around the
artery toward the wind pipe or trachea, raise both to
the surface, place on the bone separator, and remove the
sheaths. Use any of the drainage tubes. Insert the vein
drainage tube and the arterial tube, the point of both
tubes being directed toward the heart. The injection
should be made slowly, which will cause the blood to
flow from the vein through the tube and into the blood
bottle.
This vein is not as much used as the axillary or the
femoral for the removal of blood.
It is true that it is very close to the center of circulation
and a gateway for the blood from the face. The
chief disadvantage is that the vein lies quite deep, is very
large and has such thin walls, that it is almost impossible
to raise it without a rupture.
About one-thirteenth of the body's weight is calculated
to be blood. Granting for the sake of argument
that the average body that we would desire to draw blood
from would weigh 208 pounds, then that average body
would contain 16 pounds of blood. One pound of blood
is practically equal to one pint, making the average body
to contain about 16 pints of blood.
After death about one-fourth of the blood of the body
is found in the portal system. The portal system has
capillaries at both ends so that it is impossible to draw
this blood.
[281]
After death about one-fourth of the blood of the body
is found in the tiny capillaries and tissues, blood which
by the ordinary methods used today the embalmer is
unable to draw.
After death about one-fourth of the blood of the
body is found in the azygos system, and points dependent
in the body, which blood, too, it is impossible to draw.
This leaves about one-fourth of the blood of the body,
which we are able to draw. One-fourth of 16 pints, is
4 pints which is the maximum we can draw from the
average body.
The point of this argument is that if from the average
body you have taken from two to four pints of pure
undiluted blood, then you should be satisfied. If the
majority of this blood has been taken from the face you
will get the desired cosmetic effect. The claims by some
that they are able to draw a gallon or more of blood is
in our judgment erroneous, as we feel the blood has been
greatly diluted. We have tested this out many times
with the aid of control solutions and have found that
what the embalmer would ordinarily call thin blood was
composed of from 10 to 30% blood and from 70 to 90%
fluid.
[283]
PART IV.
TREATMENTS
[285]
Infectious Diseases
CHAPTER XIX.
TREATMENT OF SPECIAL DISEASES.
Anthrax.
—Synonyms.—Malignant Pustule; Splenic
Fever, Wool-sorter's Disease; Carbuncle; Charbons.
Definition.—An acute infectious, non-contagious disease,
caused by the bacillus anthracis, and characterized
by the formation of a boil with a circumscribed, infiltrated
base and dark center, and a systemic infection of a severe
type, the toxemia being of the gravest character.
Pathology.—The blood is dark, thick, diffluent, and
rich in the spores of this disease.
Treatment.—Wash the body with 1 : 500 bichloride of
mercury or 5% carbolic acid. Inject the arteries, using
64 ounces of half strength fluid followed by enough
normal fluid to secure preservation. Inject the cavities
with normal fluid. Drain blood from the veins, and disinfect
the blood before disposing of it. Close the openings
of the body. For transportation, govern yourself
according to the provisions of the transportation rules.
[286]
Cerebro-spinal Fever.
—Synonyms.—Spotted fever;
Cerebro-spinal meningitis; Typhus syncopalis; Malignant
purpuric fever.
Definition.—An acute, infectious non-contagious
disease, occurs sporadically, epidemically and endemically
characterized by hyperemia of the brain and spinal cord,
and sometimes attended by a petechial eruption.
Cause.—The meningococcus intracellularis of Weichselbaum.
Pathology.—In those cases that speedily prove fatal,
there are little, if any, changes in the blood or tissues
after death. Where the disease has continued for several
days, however, we find the characteristic suppurative
exudation. The sinuses of the brain contain
blood clots. Sometimes pus is found in the internal ear,
and the chamber of the eye. The liver, spleen and kidneys
are usually slightly engorged and somewhat softened.
There occurs in quite a number of cases a petechial
eruption; the purpuric spots may be quite profuse,
or but one or two may be seen.
Treatment.—As the means of ingress and egress of
the infectious material is not known, it is best that we
give these cases a thorough treatment; which should
include a full arterial injection, drainage from the vein,
injection of the cavities, and full care of the exposed portions
of the body by washing same with a 1 : 500 solution
of bichloride of mercury. The ears should be treated by
packing them with absorbent cotton saturated with the
fluid or with bichloride of mercury solution. The eyes
should be carefully cleansed with a soft cloth or with
[287]
cotton saturated with bichloride of mercury solution.
The arterial injection should consume an amount of fluid
equal to 10 per cent. of the body weight. Give full cavity
injection. Govern yourself by the regulations of
your district for transportation of these cases.
Erysipelas.
—Synonym.—St. Anthony's fire.
Definition.—An infectious, non-contagious disease,
characterized by an acute and specific inflammation of the
skin and subcutaneous tissues, attended by a shining
redness, which spreads rapidly, marked swelling and
pain, and which finally terminates in desquamation.
Cause.—This disease is supposed to be caused by the
streptococcus erysipelatis.
Pathology.—The blood vessels are dilated and distended
with blood, the cell infiltration may extend into
the deeper tissues with suppuration. The cocci are found
in the lymph spaces of the affected area, also in the lymph
vessels. There is a true dermatitis, involving the skin,
subcutaneous, and mucous surfaces.
Treatment.—Operator should wear rubber gloves.
Wash the body externally with 1 : 500 solution of bichloride
of mercury using absorbent cotton in the process. If
crusts have formed bathe the spots with sweet oil, which
will soften them and which will allow you to remove
them; destroying them by burning would be the best
means of disposal. If the face be the part affected, treat
as above and then apply the following solution to the
part with lintine (Moadinger) or by simple saturation:
boric acid, one drachm; glycerine, one ounce; water, three
ounces.
[288]
Inject the first 64 ounces of fluid at half the normal
strength, gradually strengthening the fluid until the tissues
become firm. Drain blood freely from a large vein
and disinfect the drawn blood before disposing of it.
Allow the softening solution mentioned above to remain
on the face until you are ready to place the body in the
casket, when the face can be dried and the usual cosmetic
powders applied. Should the peritoneum or the pleura
be affected, inject the proper cavities with very strong
fluid. For transportation, govern yourself according to
the provisions of your district rules.
Glanders.
—Synonyms.—Farcy.
Definition.—A specific, infectious, non-contagious disease
of the horse, communicable to man by inoculation,
and characterized by the formation of nodules in the mucous
membrane of the nose-glanders; and also beneath the
skin and lymph structures—farcy.
Cause.—In 1882, Loeffler and Schütz discovered the
bacillus mallei which is the exciting cause of this disease.
The infectious material is transmitted directly
from horse to men, usually through an abraded surface,
and occurs most frequently among hostlers, veterinarians,
farmers, and those who come in contact with horses. It
has been communicated from man to man, but this is
rare.
Pathology.—There are found nodules located in the
nose, in which case the disease is called glanders; or beneath
the skin, in which case it is called farcy. These
nodular masses discharge a yellow pus, which will infect
any abraded surface.
[289]
Treatment.—Disinfect the oral and nasal openings,
and wash the body with a good germicide. Give a thorough
arterial injection, using half strength fluid in the
first bottle and normal thereafter. Drain blood from a
large vein, disinfecting the blood before disposing of it.
Give a complete cavity injection. Close openings. For
transportation, govern yourself according to the provisions
of the transportation rules.
Hydrophobia.
—Synonyms.—Rabies.
Definition.—A specific infectious, non-contagious disease
peculiar to animals, especially the dog, and communicable
to man by inoculation, generally by a bite. It is
characterized in many by melancholia; great fear of
water; violent spasms of the pharynx and larynx, rendering
deglutition and respiration very difficult; great prostration,
a stage of paralysis, which generally terminates
in death.
Cause.—The specific cause has not been determined,
though bacteriologists agree that it is of microbic origin.
Pathology.—The blood vessels of the cerebrospinal system
are congested.
Treatment.—Wash the body with 1 : 500 solution of
bichloride of mercury, or 5% carbolic acid. Inject half
strength fluid into a large artery for the first part, followed
by enough normal fluid to secure preservation.
Drain blood from the veins and disinfect the blood before
disposing of it. If circulation to face and head is impaired
through the cerebral congestion, open the common carotids
and inject upward, draining from the internal jugular
[290]
vein. Give thorough cavity injection. Close all
openings of the body. For transportation, govern yourself
according to the transportation rules.
Relapsing Fever.
—Synonyms.—Typhus recurrens; Bilious
fever; Famine fever; Hunger pest; Spirillum fever.
Definition.—An acute, infectious and non-contagious
disease, characterized by a series of exacerbations and remissions,
each lasting from five to seven days, and prevailing
epidemically.
Cause.—The spirillum of Obermeier.
Pathology.—There is no characteristic change in the
solids of the body. There is sometimes icteric discoloration
during the disease and the tissues are stained after
death. The liver, kidneys and spleen are somewhat enlarged.
The heart becomes soft. The body retains its
heat a long time after death and the blood coagulates
slowly if at all.
Treatment.—Arterial injection with half strength
fluid, followed, in the second and third parts, with normal
fluid. Drainage of blood. Spray fluid over abdominal
viscera, through the usual puncture.
For transportation of bodies dead of this disease,
govern yourself according to the provisions of the transportation
rules.
Syphilis.
—Synonyms.—Pox; mal-venereal; lues venereal.
Definition.—A specific infectious, non-contagious disease,
weeks or months are occupied in its development;
[291]
contracted by inoculation which is known as acquired
syphilis, or hereditary, which is congenital syphilis, and
is characterized by three distinct stages; primary, secondary,
tertiary.
History.—”In all probability syphilis is as old as the
human race; for we can readily believe that illicit intercourse
was practiced in the cities of the ancient world
when the morals of the people were more lax than those
of today. Our knowledge of the disease, however, dates
from the fifteenth century. Breaking out among the
troops of Charles VIII, King of France, it rapidly spread
over Europe. From then to the present day our knowledge
of the disease has grown, till today we are able to
classify and separate the various lesions resulting from
illicit and promiscuous intercourse. All forms of venereal
disease were included under the name of syphilis till
Ricord, in 1831, demonstrated that gonorrhea and syphilis
were two distinct diseases.”
Etiology.—Predisposing causes are injuries or abrasions
of the mucous surfaces of exposed parts, for the
disease can originate in only one way, by inoculation.
Modes of Infection.—There are three modes of infection;
illicit intercourse, heredity and accidental. Of
these the embalmer need only consider the accidental
form of infection.
Pathology.—The initial lesion is the chancre, the secondary
lesions are ulceration of the mucous surfaces and
cutaneous eruptions, and the tertiary lesions are inflammatory
products known as gummata, and are found upon
[292]
the bones and periosteum, or in the skin, muscles, liver,
kidneys, lung, heart, brain; in fact in any of the viscera
of the body.
Treatment.—Wash body thoroughly with 5% carbolic
acid or 1 : 500 solution of bichloride of mercury.
Work with rubber gloves. Inject half strength fluid for
the first 64 ounces of fluid and follow that with normal
fluid until disinfection and preservation are assured.
Give the body a complete cavity injection with normal
fluid. Drain blood from a large vein, and disinfect the
blood before disposing of it. Close all openings of the
body with absorbent cotton saturated with normal fluid.
Bandage any large sores and saturate the bandage with
normal fluid. When purpura (characterized by a blue
spot on the face) exists, the discoloration cannot be removed.
If anything is to be done at all for the discoloration,
it must be of the nature of a covering for the spot,
such as paint or other cosmetics. For transportation of
the body, govern yourself according to the transportation
rules.
Tetanus.
—Synonyms.—Lockjaw; Trismus.
Definition.—An acute infectious, non-contagious disease,
characterized by painful spasmodic contraction of
the voluntary muscles, most frequently those of the jaw,
face, and neck; less frequently those of the trunk, the
extensors of the spine and limbs.
Cause.—The cause is recognized as the bacillus tetanus.
Pathology.—The infection usually enters by way of
a wound, especially of the hands and feet, and a punctured
[293]
wound rather than an incised one. The post-mortem
lesions are not constant.
Treatment.—The body should receive a complete arterial
injection using half strength fluid for the first part
of the injection, followed by sufficient normal fluid to
secure preservation and disinfection. Blood should be
drained from the veins and should be disinfected before
being disposed of. Wash the wound with 1 : 500 solution
of bichloride of mercury and bandage it to avoid infection
from it. Inject the cavities of the body. Close the
openings. For transportation, govern yourself according
to the provisions of the transportation rules.
Actinomycosis.
—Synonyms.—Big Jaw; Lumpy Jaw.
Definition.—A specific infectious, non-contagious disease
of domestic animals, particularly cattle, communicable
to man, and caused by the ray-fungus.
Pathology.—Infection takes place, as a rule, through
the mouth, through a cut or abrasion of the skin
and rarely through the respiratory tract. The fungus produces
a tumor, with a rapid proliferation of the neighboring
connective tissue. The disease is not limited to
any organ as the name lumpy jaw would imply; we may
have actinomycosis of the lung, digestive tract, and of
the skin.
Treatment.—Disinfect the outside of the body by
washing with a good germicide. Care should be exercised
against inoculation through an abrasion of the skin.
Give the body a thorough arterial injection, draining
blood, and disinfecting the blood before disposing of it.
[294]
Close all openings. For transportation, govern yourself
according to the provisions of the transportation laws.
Dengue.
—Synonyms.—Break-bone fever; dandy fever;
broken-wing fever.
Definition.—An acute, specific, infectious, non-contagious
fever, occurring epidemically in tropical and subtropical
climates and characterized by two severe paroxysms
of fever, separated by an intermission, great
muscular pain, and usually attended by an eruption.
Cause.—The nature of the infection or contagion
is not known. That it is infectious is shown by the rapidity
with which it spreads when once it invades a section. In
1885, within a few weeks, sixteen thousand, in Austin,
Texas, were stricken. Neither age, sex, race, nor position
exert an influence in staying the disease.
Pathology.—As few cases prove fatal, but little opportunity
has ever been given to study its pathological character.
There has been found infiltration of the tissues
about the joints. It is rare for a case to end fatally, only
few succumbing to its influence. For this reason the
embalmer will not have many of these cases to treat.
Treatment.—As this rarely comes excepting in the
epidemic form, that form will be treated on. The body
should be washed with a good germicide, and all openings
should be closed with absorbent cotton. The body should
then receive a very heavy arterial injection, with drainage
of blood, and cavity injection. As is the case in epidemics,
the body should be buried as soon as possible. While the
mortality is light, yet the most strenuous treatment should
[295]
be given to assist in the campaign of the health authorities
against the disease and its spread. When more is known
about the characteristics of the disease, it is likely that a
more definite treatment can be advised.
Malarial Fever.
—Synonyms.—Ague; Chills and fever;
Intermittent fever; Swamp fever; Marsh fever; Paludal
fever.
Definition.—A specific, infectious, although non-contagious
disease, caused by the hematozoa of Lavaran, and
consisting of two distinct parts; first, a succession of
exacerbations and intermissions, or a series of short fevers
separated by short intervals of health; second, a continued
fever made up of exacerbations and remissions, there
being but one cold stage.
Cause.—The hematozoa of Lavaran.
Pathology.—There is a destruction of the red blood
corpuscles, due to the action of the parasite. There is
an increase of pigment, in the spleen, liver, kidneys, bone
marrow, skin, and in fact, in all the tissues, due to the
conversion of hemoglobin into pigment granules. The
spleen is enlarged as are also the liver and the kidneys.
The skin presents a jaundiced appearance in chronic
malarial fever.
Treatment.—Arterial injection of 64 oz. 1% solution
of borax or oxalic acid followed by 64 oz. of half strength
fluid and then a sufficient quantity of normal fluid to
complete preservation. Drainage of blood and solution
to wash stain from capillaries. Application of full
strength peroxide hydrogen to face, and massage during
injection.
[296]
For transportation of bodies dead of this disease,
govern yourself according to the provisions of the transportation
rules.
Yellow Fever.
—Synonyms.—Typhus ichteroides; Febris
flava; Black vomit; Yellow jack.
Definition.—An acute, infectious, though non-contagious
disease of the tropics or sub-tropics, characterized
by a high grade of fever, lasting from two to seven days,
tenderness over the epigastrium (stomach), vomiting of
black, broken down blood, and yellow discoloration of
the skin.
Cause.—Not known, although it is definitely known
that the infection is spread through the bite of a species
of mosquito, the stegomyia fasciata.
Pathology.—The skin and the mucous membranes
show a varying degree of jaundice, from a light yellow
to a dark brownish or orange color; the color deepening
over the course of the blood vessels. The stomach contains
more or less of broken down blood, the so-called
black vomit. The blood is dark and broken down.
Treatment.—Arterial injection of 64 oz., of half
strength fluid followed by sufficient normal fluid to assure
disinfection and preservation. Drainage of contents from
vein and massage of face with full strength hydrogen
peroxide in an attempt to clear the complexion. Full
abdominal cavity treatment, and close orifices of the body.
For transportation of bodies dead of this disease,
govern yourself according to the provisions of the transportation
rules.
[297]
Diphtheria.
—Synonyms.—Diphtheritis; angina maligna;
membranous croup.
Definition.—An acute infectious, contagious disease
characterized by a grayish-white, fibrinous exudate, usually
located on the tonsils or the neighboring tissues.
Cause.—This is the bacillus diphtheriae, although some
still hold that the specific cause has not as yet been
determined.
Pathology.—In the severe forms the deeper connective
tissues are involved, and there may be extensive destruction
of tissue, including the blood-vessels. There is more
or less discoloration of the tissues from extravasation
of the coloring matter. The kidneys and spleen may be
enlarged. The blood is more or less broken down, the
fibrin is deficient.
Treatment.—Disinfect the oral and nasal cavities
with the embalming fluid. Wash the body externally
with 1 : 500 solution of bichloride of mercury. Inject an
amount of fluid equaling 10% of the body weight into
the arteries, and give cavity injection. Drain blood and
inject additional fluid to make up for that which will be
lost in drainage. In young persons the strength of the
fluid for the first 64 ounces of the injection should be
cut to half of the normal strength. Close all openings of
the body with absorbent cotton. Dress the body and then
place it in the casket, drawing the glass slide and closing
it, after which, it should not be re-opened. Abide by
the regulations of your district concerning the amount
of time to elapse between the time of death and of burial
in these cases. For transportation govern yourself according
to the provisions of your district rules.
[298]
Tuberculosis.
—Definition.—An infectious, slightly
contagious disease, characterized by the formation of
small nodules, tubercles, varying from the size of a millet-seed
to that of a mustard-seed or even larger.
Cause.—Tubercle bacillus of Koch.
Pathology.—Any organ of the body may be the seat
of the disease. In the adult the lungs are the most frequently
affected, while in children the lymph glands,
joints, and intestines are favorable seats for the disease.
Probably the only form that will give the embalmer any
trouble is tuberculosis of the lungs. Here either from the
poison, developed by the bacilli, or from some other
source, necrosis of the cells occurs, forming a cheesy condition
known as caseation. At a later period this breaks
down, forming an abscess, the cavity being filled with a
purulent material. At other times there is a calcareous
deposit, and the tubercular mass is said to undergo calcification.
Treatment.—In pulmonary tuberculosis, give the body
a complete arterial injection using half strength fluid
for the first part of the injection, followed by three-fourths
strength for the latter part. Hohenschuh prefers
to drain blood from all cases; the authors prefer to drain
blood in tuberculosis, only when it is necessary as a means
of preventing discolorations, and that would be in case
the blood vessels contained much blood. Massage the
face carefully with one of the commercial solutions, or,
with water which of course has no bleaching action. For
transportation, govern yourself according to the provisions
of the transportation rules.
[299]
Typhoid Fever.
—Synonyms.—Typhus abdominalis;
Typhus nervosus; Ileo-typhus and Autumnal fever, are the
most common terms, although Murchison's list includes
forty others.
Definition.—An acute, infectious and slightly contagious
disease, derived from a specific cause and characterized
by inflammation and generally sloughing of
Peyer's glands, swelling of the mesentery, engorgement
of the spleen and a rose colored eruption.
Cause.—A specific germ called the bacillus of Eberth
or the bacillus typhosus.
Pathology.—The lesions resulting from this disease
may be divided into two parts. First, the lesions of the
intestinal canal, Peyer's patches, the solitary glands of
the ileum and caecum, and more rarely of the colon and
the rectum, and changes in the spleen. Secondly, those
lesions resulting from sepsis occurring during the long
period of fever, and affecting the tissues and organs at
large. The first effect of the poison or bacilli is to cause
hyperemia (swelling) of the lymphatics, the capillaries
become engorged and cell infiltration takes place in the
solitary glands of the intestines. Frequently the infiltration
is so excessive that the capillaries become engorged
and entirely choked with the infiltration. Ulcers form,
which are shallow or deep, according to the amount of
necrosis (sloughing), and when very deep, perforation
of the bowel may follow, although this condition is rare.
The spleen is nearly always involved, congestion takes
place, followed by softening. The liver becomes hyperemic,
swollen and soft, and often shows abscess formation.
[300]
There is granular degeneration in the kidney, ulceration
of the larynx and sometimes congestion of the lung. The
heart muscles too often become weakened the result of
the poison.
Treatment.—If death occurs early in the disease, the
body will not be greatly emaciated, and the following
treatment may be followed in detail:
If intense abdominal fermentation exists, relieve the
accumulated gas with trocar, aspirate as much serous
matter as possible from the pelvic cavity, introduce a
strong fluid into the cavity, taking care to have as much
of this fluid reach the cavities of the intestines as possible.
Open one of the arteries commonly used in one of the
drainage processes and inject 64 ounces of half strength
fluid, draining blood from the vein simultaneously with
the injection. Then inject a sufficient quantity of normal
fluid to complete preservation. Close all openings of
the body with absorbent cotton. Massage the face with
water or a commercial solution during the injection.
If death occurs late in the disease, the abdomen may
require a stronger treatment such as we would give in
acute peritonitis. The trocar may not prove efficient in
reaching the affected parts and in such a case we would
make a 4 inch incision along the median line and between
the umbilicus and the pubic arch, exposing the ileum and
caecum, which should be incised, their contents removed,
and then all replaced in the cavity thoroughly surrounded
with hardening compound. After this the wound should
be closed with stitches. After preservation has been completed
in either this form of the disease or the one mentioned
[301]
above, dust on a good quality of face powder to remove
the moist appearance from the skin. When a body
dead of this disease is to be transported, consult the
state or local transportation rules in addition to these
treatments.
Leprosy.
—Definition.—A chronic, infectious, contagious
disease, which usually terminates fatally.
Cause.—The bacillus leprae. There are tuberculous
growths in the skin, which push outward, form nodular
masses, between which are seen areas of ulceration and
cicatrization, which in the face, distort the features.
These tubercular masses discharge a thick purulent material.
The destruction of tissue proceeds gradually,
years being occupied in destroying a patient. The deep,
ulcerative process may amputate fingers and toes in its
progressive march.
Treatment.—The body is rarely presentable for sometime
before death, and this should not be a consideration
in our treatment. If an arterial injection is possible, give
it, using normal fluid for the injection. Work with rubber
gloves. Give a complete cavity injection. Wrap the
body in absorbent cotton and then in a sheet. For transportation,
govern yourself according to the provisions
of the transportation rules.
Influenza.
—Synonyms.—Epidemic catarrhal fever; la
grippe.
Definition.—An acute, infectious disease, the contagion
of which is questionable occurring pandemically.
Cause.—The bacillus influenza.
[302]
Pathology.—There is no characteristic lesion in the
uncomplicated case. When death occurs it is usually from
complication.
Treatment.—Disinfect the oral and nasal cavities with
embalming fluid. Inject as much fluid as you can into
the arteries and cavities. The usual 10% of the body
weight must be given for transportation. If blood vessels
are filled with blood, drain from a large vein, and add
more fluid to your injection, to make up for the loss of
blood to the blood bottle. Close all openings with absorbent
cotton. For transportation, govern yourself according
to the provisions of your district rules.
Cholera.
—Synonyms.—Cholera Algida; Cholera Asiatica;
Cholera maligna.
Definition.—Cholera is an acute, specific, infectious
slightly contagious disease, occurring epidemically and
endemically, and characterized by severe vomiting and
copious watery stools, violent cramping of the muscles
and collapse.
Cause.—The exciting cause is now generally recognized
as the comma bacillus of Koch, or spirillum cholerae.
Pathology.—The tissues after death are shrunken and
drawn, and the extremities are inclined to be mottled; in
some cases there is a postmortem rise of temperature.
Rigor mortis sets in very early. Spasmodic contractions
sometimes occur for some moments after death; hence
the eyes and jaws have been seen to move after life was
extinct. Owing to this marked contraction, the limbs
have been distorted and the partial turning of the body
[303]
is thus accounted for, and is not, as many have supposed,
the result of being buried alive. The tissues are dry,
having been drained of these fluids before death,
hence some time elapses before decomposition begins after
death. The chief visceral lesion is that of the intestinal
canal. The intestines contain a more or less quantity
of rice-water, fluid rich in the comma bacillus. The blood
is very dark, but slightly coagulable and robbed of its
salts and fluids.
Treatment.—Arterial and cavity embalming, closing
all orifices of the body. Any discharges from the bowels
should be disinfected before being disposed of. In epidemics,
cosmetic effect is a non-essential and in that case
the most thorough treatment must be given without regard
to appearances.
For transportation of bodies dead of this disease,
govern yourself according to the provisions of the transportation
rules.
Bubonic Plague.
—Synonyms.—The Pest; Black
Death; Plague of Egypt.
Definition.—A specific, infectious, contagious disease,
running a rapid course, and characterized by inflammation
of the glands (buboes), carbuncles, ecchymoses, and
petechiae upon the surface. It is endemic on the eastern
coast of the Mediterranean Sea and the Oriental
countries adjacent. Epidemics occur when it spreads
to other parts of the world, traveling along the great
thoroughfares of travel and commerce.
Cause.—To Kitasato belongs the honor of discovering
the specific cause, the bacillus pestis. On entering the
[304]
body, either by inoculation or by way of the digestive
or respiratory tracts, it multiplies with great rapidity.
It is found in the blood, in the internal organs, in the
intestinal canal, lymphatic glands and in great numbers
in the suppurating buboes.
Pathology.—Rigor mortis occurs early, and often there
is elevation of temperature immediately after death.
Petechiae, ecchymoses, and carbuncles are generally
found upon the skin. The lymphatic system is generally
affected, the lymph glands of the groin and axilla showing
evidence of inflammation.
Treatment.—Wash the body thoroughly with a good
germicide, close all openings, first however, disinfect the
oral and nasal openings. Nothing should be done for the
ecchymotic spots, the cosmetic effect in these cases being
secondary to disinfection. The arteries should receive a
heavy injection of normal fluid, blood being drained from
the veins. The blood should be disinfected before being
disposed of. The cavities should receive a heavy injection
of normal fluid. For transportation of these cases, govern
yourself according to the provisions of the transportation
rules.
Scarlet Fever.
—Synonyms.—Scarlatina; scarlet rash.
Definition.—An acute, contagious disease, characterized
by a bright scarlet colored eruption, diffused over
the entire body, terminating by desquamation of the skin.
Cause.—Not definitely known, although thought by
Klein and Gordon to be the streptococcus scarlatinae.
Pathology.—The blood is dark, diffluent, and does not
coagulate readily, owing to a defect in the fibrin. The
[305]
eruption disappears after death, except in those malignant
cases where the eruption failed to appear during
life, and appears upon the death of the patient.
Treatment.—First protect yourself by wearing a
bandage of surgical gauze over your mouth and nose, then
enter the room of death and wash the body thoroughly
with a 1 : 500 solution of bichloride of mercury. Inject
an amount of fluid equaling 10% of the body weight into
the arteries and inject into the cavities. Drain blood
through one of the drainage processes, and add an amount
of fluid to the arterial injection equal to that which is
lost to the blood bottle. Close all openings with absorbent
cotton, dress the body, and then place it in the casket,
drawing the glass slide and closing it, after which, it
should not be reopened. Abide by the regulations of
your district concerning the amount of time to elapse
between the time of death and of burial in these cases.
For intra-state and inter-state transportation, govern
yourself according to the provisions of your district rules.
Variola.
—Synonyms.—Small-pox; German Blattern;
French, La Petite Verole.
Definition.—A specific, infectious, highly contagious
febrile disease, characterized by a dermatitis, in which the
eruption passes from the papule to vesicle, and this in
turn into pustule, finally dessicating.
Cause.—The true nature of the virus is not known,
and although certain microorganisms have been described
which are found in the pock, there is no proof that they
are responsible for producing the poison. All that is
[306]
positively known is, that it is developed in the system
and reproduced in the pustule.
Pathology.—The most marked change occurs in the
skin, where an eruption takes place, finally with the
formation of scabs or crusts. The blood does not reveal
any microscopic changes, although darkened in color.
Treatment.—No one but an immune should handle
these cases, and he should first wash the body with a
1 : 500 solution of bichloride of mercury. After this has
been done, inject an amount of fluid equal to 10 per cent.
of the body weight, distributing same by arterial injection.
If blood is drained, and it is proper to do so, add
fluid to the injection to make up the loss into the blood
bottle. Give full cavity injection. Bodies dead of this
disease should be buried within a reasonably short length
of time, so that the apartments may be rendered safe
by fumigation, and under no circumstances should a
public funeral be held. After the body has been placed
in the casket, the slide, preferably of glass, should be
closed and should not be reopened under any circumstances.
Govern yourself by the regulations of your district
for transportation of these cases.
Measles.
—Synonyms.—Morbilli; rubeola.
Definition.—An acute, infectious, contagious fever,
characterized by a general papular eruption.
Cause.—The efforts to isolate a specific germ which
will produce the disease has thus far failed, though many
organisms have been found in the secretions.
Pathology.—There is a lack of coagulability of the
blood, which is dark in color. The internal organs are
[307]
congested and softened. The lesion of the skin consists
of an acute hyperemia with exudation in the vascular
papillae of the corium, the sebaceous and sweat glands.
Treatment.—Bodies rarely die from this cause; the
usual immediate cause of death is exhaustion. An injection
of half strength fluid for the first part of the injection
followed by normal fluid for the balance of the injection,
with full cavity injection, closing the orifices is
all that is necessary. For transportation, govern yourself
according to the provisions of the transportation
rules.
Parotitis.
—Synonyms.—Mumps, epidemic parotitis.
Definition.—An acute, infectious, and contagious disease,
characterized by an inflammation of one or both of
the parotid glands.
Cause.—The specific cause is a contagion generated
during the course of the disease, the exact nature of
which is not known, although thought by some to be the
tetrad of mumps.
Pathology.—The parotid glands become swollen and
hard. Death very seldom occurs from this disease.
Treatment.—Disinfect the oral cavity with embalming
fluid. The swelling cannot be reduced, so that the next
concern to the embalmer will be to preserve the body.
This should be done by injecting 64 ounces of half
strength fluid, followed by enough normal fluid to secure
preservation. If blood vessels contain much blood, drain
from a large vein, and then inject additional fluid to
make up for that lost by drainage. Close all openings
[308]
with absorbent cotton. Abide by the regulations of your
state governing the transportation of these cases.
Pertussis.
—Synonyms.—Whooping-cough; tussis convulsiva.
Definition.—A specific infectious, contagious disease
occurring epidemically, and characterized by a peculiar,
spasmodic cough, ending in a whoop.
Cause.—The cause of whooping-cough has always been
a matter of conjecture.
Pathology.—In the uncomplicated form there is no
lesion which can be said to be characteristic. There might
in complications be hemorrhage from the lung.
Treatment.—Disinfect the oral and nasal cavities
with embalming fluid. Inject 64 ounces of half strength
fluid followed by enough normal fluid to secure preservation.
If blood vessels contain much blood, drain from
a large vein, and then inject additional fluid to make up
for that lost by drainage. Close all openings with absorbent
cotton. Discourage public funerals in these cases.
For intra-state or inter-state transportation of these
cases, govern yourself according to the provisions of your
district rules.
Typhus Fever.
—Synonyms.—Famine fever; Ship
fever; Jail fever; Hospital fever; and Putrid fever.
Definition.—An acute, infectious, very contagious,
endemic, and also epidemic disease, characterized by a
high grade of fever and a peculiar rash.
Cause.—Not known.
Pathology.—The blood is dark and diffluent the result
of the intense fever and rapid work of the poison.
[309]
The liver is somewhat enlarged and softened, as are also
the kidneys and spleen. There is an extravasation into
the pericardium which gives it an ecchymotic appearance.
There is also a slight engorgement and infiltration of the
capillaries. The muscular tissues are of a dark red color.
The skin shows a characteristic rash and ecchymotic
spots are found on the more dependent parts of the body
after death.
Treatment.—Slow arterial injection and drainage of
blood. On account of rash, apply bichloride of mercury
1 : 500. In the presence of fermentation, give the abdomen
a special treatment.
For transportation of bodies dead of this disease,
govern yourself according to the provisions of the transportation
rules.
Varicella.
—Synonym.—Chicken-pox.
Definition.—An acute, specific, and infectious disease,
characterized by an eruption that rapidly passes through
the stage of papule, vesicle, and pustule, and terminates
by dessication.
Cause.—This is not known. All attempts to isolate
the microorganisms or the contagium, whatever that may
be, have failed.
Pathology.—The only pathological lesion is the eruption
that appears on the skin.
Treatment.—These cases should be thoroughly
washed with 1 : 500 solution of bichloride of mercury,
after which a thorough arterial and cavity injection
should be given, consuming for this purpose an amount
[310]
of fluid equal to 10 per cent. of the body weight in the
arteries. Blood should be drained from the veins, and an
amount of fluid equal to what is lost to the blood bottle
should be injected in addition to the 10 per cent. mentioned
above. After the body is placed in the casket,
close the slide which should be of glass, and do not reopen
again. Public funerals of these cases should be
discouraged, to avoid the indiscriminate transfer of the
disease.
Septicemia.
—Definition.—A morbid process commonly
known as blood poisoning, in which there is an invasion
of the blood by bacteria or their toxins.
Cause.—Any bacteria or its toxin.
Pathology.—The blood is found to be dark, diffluent,
and rich in bacteria. The liver and spleen are soft,
dark in color, and show swelling. The lymphatics are
also swollen.
Treatment.—The operator should approach these
cases with unbroken skin on his hands, or if that be impossible,
with rubber gloves, as the disease is disseminated
through abrasions. Take up a large artery and vein,
inject half strength fluid for the first bottle and normal
fluid thereafter in the arteries, and drain from the veins.
Disinfect the blood obtained from the vein before disposing
of it. Give the body a complete cavity injection.
Massage the face to stimulate capillary circulation while
the arterial injection is being made. For transportation,
govern yourself according to your district transportation
rules.
[311]
Pyemia.
—Definition.—An infectious disease due to
the absorption of animal poisons, principally pyogenic
organisms, and characterized by the formation, in the
various tissues and organs, of multiple metastatic abscesses.
Cause.—One of the forms or a combination of pyogenic
micrococci are held to be responsible, for this condition.
The streptococcus and the staphylococcus are the forms
most common, though it is not uncommon to find the
micrococcus lanciolatus, the gonococcus, the bacillus coli
communis, bacillus typhosis, bacillus pyocyaneus, and
many others.
Pathology.—The body does not undergo putrefaction
as rapidly as in septicemia. The first effects of the morbid
changes are found in the veins, which result in
thrombi. These thrombi are found in the various organs
and tissues of the body.
Treatment.—Use the precautions observed in the
treatment for septicemia. Give the body a complete arterial
injection using half strength fluid for the first bottle
of the injection. Drain as much blood from the veins
as possible. Thrombi may complicate the drainage, and
if none can be obtained from several of the larger veins,
tap the heart as a last resort. Disinfect the blood before
disposing of it. Streptococcus infection of the embalmer
from abrasions of the skin is very dangerous and every
possible precaution should be carefully taken. Give the
body a complete cavity injection. For transportation,
govern yourself according to the provisions of the transportation
rules.
[312]
CHAPTER XX.
TREATMENT OF SPECIAL DISEASES.—Continued.
DISEASES OF THE RESPIRATORY SYSTEM.
Gangrene of the Lung.
—Definition.—A putrefactive
necrosis of the lung.
Cause.—Many putrefactive bacteria thrive in the necrotic
soil, but whether they are the cause or the result
is not known.
Pathology.—When the gangrene is due to the plugging
of one of the large branches of the pulmonary artery,
a large part of the lung becomes dark, greenish brown,
or a black fetid mass, softening rapidly in the center,
forming an irregular cavity, containing a foul-smelling
disgusting, greenish fluid.
Treatment.—Give complete arterial injection. Inject
the pleural sac on the affected side through the first intercostal
space or through the apex of the cavity. Spray
fluid into the mouth and nose and close them with absorbent
cotton. For shipment of these cases govern yourself
according to the transportation rules.
Pulmonary Hemorrhage.
—Synonyms.—Hemoptysis;
[313]
Broncho-pulmonary hemorrhage; Bronchorrhagia; Pneumorrhagia.
Definition.—An expectoration of blood, due to hemorrhage
from the mucous membrane of the bronchi, trachea,
or larynx and from erosion or rupture of capillaries
in lung cavities.
Cause.—The hemorrhage may result from congestion
of the lungs, due either to pulmonary lesions or from
cardiac derangements. It may accompany malignant affections,
infectious fevers, scurvy, cancer of the lung, gangrene,
and abscess of the lung.
Pathology.—There is, in most cases rupture of the
capillaries of the bronchial mucous membranes. If tubercular
cavities are formed, a ruptured aneurism is sometimes
seen, or large blood vessel eroded by ulceration. If
pulmonary apoplexy has existed, the parenchyma may
be lacerated.
Treatment.—Some operators wait until fluid passes
from the mouth before taking steps to stop the hemorrhage
due to the injection of fluid. We prefer to use
plaster of paris and cotton, making a paste of them and
forcing the paste down upon the epiglottis to prevent the
waste of fluid from that source. When the cause of death
is known, this operation must be done before the injection
is begun or the throat will have to be dried out
before the plaster of paris will set properly. Another
treatment to prevent the leakage of fluid would be to tie
off the trachea just above the upper border of the sternum.
The body is usually emaciated and should be injected
arterially with comparatively mild fluid, in order to avoid
[314]
drying or dessication of the features. Whenever fermentation
exists in the abdomen, the cavity should be injected;
otherwise it is not usually necessary. The amount
of fluid for the injection should be based on the amount
that will be taken by the vessels of a body the size of the
one being injected. For transportation of these cases the
provisions of the transportation rules should be your
guide.
Pulmonary Abscess.
—Synonyms.—Abscess of the
lungs; Suppurative pneumonitis.
Definition.—A collection of pus in the lung, accompanied
by degeneration of tissue.
Pathology.—The abscess may involve one or more lobules,
or engage almost the entire lobe, or the abscesses
may be scattered throughout the whole lung.
Treatment.—Should hemorrhage occur, treat this case
the same as for pulmonary hemorrhage. If no hemorrhage
occurs, give the body a complete injection with
a mild fluid and inject the pleural sacs from the first
intercostal space or the apex of the cavity. For transportation,
govern yourself according to the provisions of
the transportation laws.
Pneumonia.
—This disease is divided into different subdivisions
as follows: Lobar Pneumonia, broncho-pneumonia,
and chronic interstitial pneumonia.
(A) Lobar Pneumonia.—Synonyms.—Croupous or
Fibrinous Pneumonia; Pneumonitis; Inflammation of the
lungs; and Winter fever.
Definition.—This is an acute infectious disease characterized
by an inflammation of the lung tissue in which
[315]
there is, first, congestion and engorgement, second, exudation
or consolidation; and third, resolution or suppuration.
Pathology.—The right lung is more frequently affected
than the left, and one lobe, or one entire lung, rather
than both lungs at the same time.
Treatment.—Should suppuration occur, turn the body
on its side, press on the sternum and cause the suppurative
matter to leave the windpipe by purging it into the folds
of a towel which should be placed at the mouth. Spray
the mouth with fluid and close the oral and nasal cavities
with absorbent cotton.
Give the body a thorough arterial and cavity injection,
paying especial attention to the pleural sacs, which
should be injected independently from the first intercostal
space on each side or from the apex of the cavity.
Drain blood and disinfect the contents of the blood bottle
before disposing of same. For transportation, govern
yourself according to the provisions of the transportation
laws.
(B) Broncho-Pneumonia—Synonyms.—Capillary
Bronchitis; Lobular Pneumonia; Catarrhal Pneumonia.
Definition.—An inflammation of the terminal bronchi,
air vesicles, and interstitial tissue of a few or many of the
lobules.
Pathology.—The interstitial tissue between the air
cells and the capillaries are greatly weakened. In most
cases the lung will float when placed in water, though
the small mahogany-colored nodules found distributed
throughout the lung when excised sink in water.
[316]
Treatment.—The nature of the disease is such that
preservation is comparatively simple, the disease affecting
the extremities of the respiratory system. Arterial injection
together with special attention to the pleural sacs
will suffice for the cases. For transportation, govern
yourself according to the provisions of the transportation
rules.
(C) Chronic Interstitial Pneumonia.—Synonyms.—Cirrhosis
of the lungs; Fibroid Pneumonia.
Definition.—A chronic inflammation of the lungs, in
which the normal air cells are replaced by fibrous or
connective tissue, followed by induration and atrophy of
the lung.
Pathology.—The disease is nearly always confined to
one lung, though, in very rare cases, both lungs may be
involved, while localized areas are the rule. The affected
lung becomes atrophied and in extreme cases, may be no
larger than the closed hand. As a result of the shrinkage
of the lung tissue, the heart undergoes hypertrophy.
When tuberculosis exists, cavities of varying size and
number are found, and the interstitial tissue between the
capillaries and the air cells is very much weakened.
Treatment.—Should this disease be followed by a rupture
of the capillaries during the injection, thereby causing
a hemorrhage from the oral and nasal openings, treat
it as you would a case of pulmonary hemorrhage. Otherwise
give the body a thorough arterial and cavity injection
with special attention to the pleural sacs. For transportation,
govern yourself according to the provisions of
the transportation laws.
[317]
Hydrothorax.
—Synonyms.—Thoracic dropsy; Dropsy
of the chest; Dropsy of the pleura.
Definition.—A collection of serous fluid within the
pleural cavity without inflammation.
Pathology.—Hydrothorax, unless due to cardiac affections,
is usually bilateral. The quantity of fluid varies,
and is generally greater on one side than on the other.
The fluid is free, and of a low specific gravity, alkaline
in character, clear, and of an amber color.
Treatment.—To prevent the formation of blisters on
the posterior surface of the thorax, aspirate the serous
fluid from the pleural sacs, introducing the trocar through
the apex of the cavity, and extending it into the cavity
until it has almost reached the diaphragm. This must
be done with both the right and left sacs. Give the body
a complete injection, using normal fluid throughout the
entire injection. Inject the pleural sacs after the serous
fluid has been withdrawn. For prevention of post-operative
dangers such as bursting blisters, etc., line the casket
with rubber for a distance of 3 inches above the
bottom. For transportation of these cases, govern yourself
according to the provisions of the transportation
laws.
[318]
CHAPTER XXI.
TREATMENT OF SPECIAL DISEASES.—Continued.
DISEASES OF THE CIRCULATORY SYSTEM.
Pericarditis.
—Definition.—An acute inflammation of
the pericardium and the serous covering of the heart.
Treatment.—Give the body a thorough injection of
half strength fluid followed by normal fluid. Drain from
the veins. Inject the abdominal cavity. For transportation
of these cases, govern yourself according to the provisions
of the transportation rules.
Hydropericardium.
—Synonym.—Dropsy of the pericardium.
Definition.—Hydropericardium is a non-inflammatory
condition of the pericardium, attended by an accumulation
of sero-albuminous fluid.
Pathology.—Hydropericardium is not a disease of itself,
but it is always secondary. The accumulated fluid
is usually clear, of an amber color, though it may become
turbid by the presence of fibrin or red blood corpuscles.
The fluid is alkaline in reaction.
Treatment.—As this disease is always secondary to
another, the treatment will also be secondary and all that
[319]
can be said is that the heart sac should be relieved of its
accumulated serous fluid, after the body has received the
treatment necessary for the immediate cause of death.
Transportation will also be covered by the disease causing
death.
Hemopericardium.
—Definition.—Hemopericardium is
an infiltration of blood into the pericardium. It is the
result of a rupture of an aneurism of the aorta or coronary
arteries, or in rare cases from rupture of the heart. It
may also arise from injuries such as bullet wounds, fracture
of the ribs, sternum, etc.
Treatment.—This condition is usually secondary to
another such as gun shot wound, aneurism of the aorta,
etc., so that the treatment must be given under the heading
of the immediate cause of death. For transportation
requirements also refer to the immediate cause of death
and the transportation rules.
Pneumo-Pericardium.
—Definition.—Pneumo-pericardium
is an accumulation of air in the pericardium. Although
this is a rare disease, it does occasionally occur,
either through diseased processes, such as cancerous or
tubercular ulceration or through injuries; thus a ruptured
pulmonary cavity might result in this condition, or the
perforation of the esophagus, by malignant processes
would give rise to this lesion. Sometimes pus in the
pericardium will generate gas.
Treatment.—As the accumulation of air or gas is
secondary to some other process of disease, the immediate
cause of death will carry with it the proper treatment.
[320]
The gas itself should be removed by piercing the pericardium
with a small needle or trocar, after which a small
quantity of fluid should be injected.
Endocarditis.
—Definition.—Endocarditis is an inflammation
of the lining membrane of the heart, and is generally
confined to the valves, though other parts may be
affected.
Pathology.—The morbid changes are, first, a reddened
and injected appearance of the endothelium, which soon
becomes opaque and swollen from congestion of the small
blood vessels. This swelling or thickening of the membrane
furnishes a favorable resting place for deposits of
fibrin, and we have small, beady deposits from the size
of a pin point to that of a pea, or even larger. These
small, beady excrescences may become detached, and floating
off in the general current, give rise to embolism in
distant parts.
Treatment.—An embolism means the obstruction of a
blood vessel by some foreign material. If in the injection
of fluid, there is an obstruction in one of the blood vessels,
leading to one of the organs, you will never be any
the wiser, but if the obstruction is in one of the vessels
supplying a certain area of skin, the condition will show
up sooner or later, when that certain part will have to be
treated hypodermically. Slow arterial injection with
drainage of blood should be given and when symptoms
of fermentation are present, include special attention to
the abdominal cavity.
[321]
Aortic Incompetency.
—Synonyms.—Aortic Insufficiency;
Aortic Regurgitation.
Definition.—Inability of the aortic valves to properly
close an abnormally large aortic opening, or a change in
the segments whereby they are shortened by curling of
the leaflets, or by calcification.
Treatment.—Bodies dead of this disease will be found
with very much blood, and the elimination of the blood by
drainage should be the first consideration along with the
injection of fluid. The fluid should be diluted one-half
for the first part of the injection, and sufficient fluid used
to reach all parts of the circulatory system. It will be
well to add fluid equal to the amount of blood and fluid
taken from the vein to your normal injection in a body
the size of the one to be operated on. A complete cavity
injection should be given. For transportation, govern
yourself according to the provisions of the transportation
rules.
Aortic Stenosis.
—Definition.—Aortic stenosis is an obstruction
of the aortic orifice, due to changes in the segments
of the semilunar valves, or arterio-sclerosis, or
atheromatous deposits.
Treatment.—Give same treatment advised for aortic
incompetency, with special care in the injection. Sclerotic
conditions may complicate the injection, and in that
case as many arteries should be injected as possible together
with full blood drainage.
Mitral Incompetency.
—Synonyms.—Mitral Regurgitation;
Mitral Insufficiency.
[322]
Definition.—This condition is an incomplete or imperfect
closure of the auriculo-ventricular opening, permitting
the regurgitation of blood during the contraction
of the left ventricle, and due to an abnormal condition
of the leaflets or an enlarged opening.
Treatment.—Give same treatment as advised for
aortic incompetency, with special care to remove as much
blood as possible, which, with massaging the face downward,
should relieve any blood discolorations.
Mitral Stenosis.
—Definition.—Mitral stenosis is a constriction
of the left auriculo-ventricular orifice, usually
due to valvular endocarditis.
Treatment.—Give this body the same treatment as
advised for aortic incompetency, with special care indicated
in mitral incompetency.
Tricuspid Incompetency.
—Synonym.—Tricuspid Regurgitation.
Definition.—This condition is an imperfect closure of
the tricuspid valves, due to dilation of the right ventricle
or to disease of the valves.
Treatment.—Drain as much blood as possible from
this case. Massage the face downward, and inject the
maximum amount of fluid; diluting the first bottle to
half strength. In obstinate cases of blood discoloration,
open the common carotid arteries and internal jugular
veins, inject upward in the arteries and drain from the
veins, so as to wash out the vessels of the face. For
facial injection use nothing stronger than half strength
fluid. Give thorough cavity injection. For transportation,
[323]
govern yourself according to the provisions of the
transportation rules.
Tricuspid Stenosis.
—Definition.—Tricuspid stenosis is
an obstruction of the tricuspid opening, usually congenital,
though it may be acquired.
Treatment.—Treat the same as for tricuspid incompetency.
Pulmonary Incompetency.
—Synonym.—Pulmonary
Insufficiency.
Definition.—Pulmonary incompetency is an imperfect
closure of the pulmonary orifice of the right ventricle due
to changes in the pulmonary valves.
Treatment.—Treat the same as for tricuspid incompetency.
Pulmonary Stenosis.
—Definition.—Pulmonary stenosis
is an obstruction of the pulmonary opening of the right
ventricle, due to congenital defects or to endocarditis.
Treatment.—Treat the same as for tricuspid incompetency.
Cardiac Thrombosis.
—Definition.—Cardiac thrombosis
is the formation of blood clots in the cavities of the heart.
Pathology.—The blood clots are found most frequently
in the right side of the heart. They vary in size, from
that of a pin head to that of a hen's egg. When degeneration
takes place, softening follows, and sometimes particles
become dislodged and float off to set up thrombi
in other viscera.
Treatment.—Remove the maximum amount of blood
by drainage along with the injection of fluid. The fluid
[324]
in this case should be not more than half strength for
the first part of the injection, to be followed by enough
normal fluid to secure preservation. If thrombi have
lodged in any of the larger arteries, the circulation to
the part reached by the branches of the artery will be
affected. This can be overcome by injecting an artery
close to the part which is not receiving the fluid. Massage
the face downward to assist capillary circulation.
Give a complete cavity injection. For transportation,
govern yourself according to the provisions of the transportation
rules.
Hypertrophy of the Heart.
—Definition.—Hypertrophy
of the heart is an enlargement of the organ, due to an
increase in the volume of its muscular fibers, and usually
also to dilatation of its cavities.
Treatment.—Secure full drainage from the veins.
Drainage will be stimulated by an injection of half
strength fluid for the first part of the injection and a
massage of the face. Follow the first part of the injection
with enough normal fluid to secure preservation.
Give a complete cavity injection. For transportation,
govern yourself according to the provisions of the transportation
rules.
Cardiac Dilatation.
—Definition.—Cardiac dilatation
is an increase in the size of the cavities of the heart,
due either to thickening or thinning of the walls.
Treatment.—Treat the same as for hypertrophy of the
heart.
Cardiac Atrophy.
—Definition.—Cardiac atrophy is a
[325]
decrease in the size, strength, weight, and activity of the
heart.
Treatment.—Remove blood by drainage, and inject
half strength fluid for the first part of the injection.
The amount of fluid need not be as great as in the acute
disease of the heart. Massage the face downward. Give
cavity injection. For transportation, govern yourself
according to the provisions of the transportation rules.
Arterio-Sclerosis.
—Synonyms.—Endarteritis; Atheroma;
Arterial Sclerosis.
Definition.—Arterio-sclerosis is an inflammatory and
degenerative condition of the arterial system, primarily
of the intima, although later degenerative changes may
involve the whole structure. Calcarine deposits are quite
common.
Pathology.—As a result of proliferation, infiltrated
areas begin in the middle and outer coats. These nodules
vary in size from that of a small shot to that of a large
coin. As they increase in size, the intima loses its smoothness
and becomes thickened and rough. As these changes
progress, the middle and outer coats are weakened. Calcification
may also occur in the wall.
In the diffuse form the change in the coats of the
vessels extends throughout the greater part of the arterial
system, and in some cases invades the capillaries and
veins.
In the senile arterio-sclerosis calcareous deposits occur,
which render the vessels rigid. Where these tissue-changes
involve the capillaries, there may be complete obliteration
of their lumen in some places.
[326]
Treatment.—In some cases the artery appears to be
closed at a point ahead of the tube and will resist the
injection of fluid. Usually, however, the injection can
be made without resistance. Blood should be drained
from these cases so as to allow as full capillary penetration
as possible. When no arterial injection can be
made, open the internal jugular and several other large
veins, drain blood from them and then inject fluid while
the tube is within the vessel. If necessary add a complete
hypodermic injection to all parts of the body excepting
the face. Give the cavities full treatment. For transportation,
govern yourself according to the transportation
rules.
Fatty Degeneration of the Arteries.
—In the fatty degeneration
of arteries the process consists in the gradual
replacement of certain parts of the muscular cells by fat
droplets. The fat makes its appearance as minute droplets
or granules in the cells. These granules, which are
characterized by their dark color, gradually increase in
number and ultimately the whole of that part of the cell
may be transformed. During the process the granules
coalesce, and in this manner form distinct drops of fat.
As the process proceeds the cell is increased in size and
becomes more globular in shape. The cell wall is destroyed
and the cell may thus be converted into a mass
of granular fat. Ultimately the matter between the granules
of fat liquify. The corpuscles break up and the fat
becomes distributed in the surrounding tissues. The immediate
effect of this fatty degeneration is to produce
more or less softening of the fatty part, which will impair
[327]
or destroy its function. In the case of the artery, the
internal, middle and external coats may be affected, but
the external is the one usually first attacked. The inner
layer or endothelium, and the connective tissue cells in
the deeper layers of the inner coat may become affected in
various parts of the vessel. The process may involve a
great portion of the inner coat, even the whole thickness
of the intima may be destroyed. The walls of the artery
may be entirely solidified, the canal being closed completely
with a soft, yellowish substance as a result of the
disease. The artery might appear to be a solid mass when
the dissecting knife is passed through. We have seen
the anterior and posterior tibial, the popliteal, radial,
ulnar, the aorta arteries, and especially the arch of the
aorta thus affected. Calcification may be present at many
places. These cases are frequently met with in old age.
A body of this kind, where there is fatty degeneration
of the arteries, is sometimes hard to embalm. The walls
of the artery will be very much weakened, and too much
pressure must not be made on them while injecting fluid.
Inject the fluid so that it will take several hours to fill
the tissues. The pressure should be gentle and regular
when the aspirator and injector pump is used. If this
precaution is taken often the whole body can be embalmed
without a rupture of the arterial system, the fluid reaching
all the extremities by means of collateral circulation.
If the embalmer should be so unfortunate as to rupture
the circulation then he will have to resort to cavity
embalming, and the subcutaneous tissues will have to be
embalmed by the hollow needle trocar.
[328]
Aneurism.
—Definition.—An aneurism is a circumscribed
dilatation of an artery, formed by the giving away
of one or more of its coats. A false aneurism is where
there is a rupture of the coats, and the blood is found in
the adjacent tissues.
Treatment.—Drain blood from a large vein. Inject
half strength fluid for the first part of the injection, followed
by enough normal fluid to secure preservation.
The aneurism itself, will not affect the circulation of
fluid to any great extent. Massage the face downward.
Give a complete cavity injection. For transportation,
govern yourself according to the transportation rules.
[329]
CHAPTER XXII.
TREATMENT OF SPECIAL DISEASES.—Continued.
DISEASES OF THE DIGESTIVE SYSTEM.
Jaundice.
—Synonym.—Icterus.
Definition.—Jaundice is a symptom rather than a disease,
and is found in the various affections of the liver.
It is characterized by a deposit of bilirubin in the various
structures and fluids of the body, which gives them a
yellow or jaundiced hue.
Etiology.—Most pathologists agree that all the forms
of jaundice can only come from obstruction. The obstruction
is due to inflammation tumefaction of the duodenum
or bile-ducts; to foreign bodies, such as gall stones
or parasites, within the ducts; tumors within the duct
or by pressure from without, such as tumors, gravid
uterus, or fecal matter; or to stricture or obliteration
of the duct.
Catarrhal Jaundice.
—Definition.—Catarrhal inflammation
of the lining membrane of the biliary ducts, and the
duodenum, and attended with discoloration of the skin
and tissues from the consequent retention and absorption
of the bile.
[330]
Pathology.—That portion of the duct lying in the
intestines is more frequently and seriously affected, though
the inflammation may extend to the cystic and even the
hepatic duct. The membrane lining the ducts is swollen
and inflamed. The liver is usually congested, slightly enlarged,
and of a deep yellow color. The gall bladder is
usually distended with bile. The ducts are occluded by
the swollen mucosa and plugs of inspissated mucous.
Discoloration of the skin and conjunctiva occurs.
The yellow tinge begins in the eyes, forehead, and neck,
gradually extending over the body, the color being the
deepest in the wrinkles and folds of the skin. The color
is generally of a lemon hue, becoming darker and assuming
a bronze or greenish tint as the hepatic lesion assumes
a graver character.
Infantile Jaundice.
—Etiology.—It is not known positively
what causes give rise to temporary jaundice in the
new-born. Some say it is due to a reduction of blood
pressure in the hepatic capillaries, while others say it
is due to a stasis in the smaller bile ducts, which are compressed
by the distended radicles of the portal vein. The
severe form may be due to congenital closure or absence
of the common or hepatic duct, to hepatic syphilis of
congenital form, or to septic infection due to phlebitis
of the umbilical vein.
In the child the skin becomes a yellowish hue of
various shades. In the severe form the hue increases
in intensity, the skin assuming a bronze or yellowish-green
color. The abdomen becomes full and tumid, owing
[331]
to the congestion of the liver and spleen. When due to
syphilis, there is usually skin eruption.
Malignant Jaundice.
—Synonyms.—Acute Yellow Atrophy
of the Liver.
Definition.—A grave form of jaundice characterized
by neurosis of the hepatic cells and atrophy of the liver.
Pathology.—The liver shows marked atrophy, being
not more than two-thirds or one-half of the normal size,
is thin, flabby. On making a section a yellow or a reddish
yellow surface is presented. The hepatic cells are found
in every stage of necrosis. Most of the organs are bile
stained, as well as the skin, and hemorrhages are frequent.
Treatment for Jaundice.—Since the conditions are
similar and since the conditions after death are identical
in reference to pigmentation, we will consider the treatment
of infantile, malignant, and catarrhal jaundice under
one head.
The pigmentation of the skin, no matter how small,
is the condition which presents itself most forcefully, and
is the most annoying to the embalmer. Much study has
been given to the subject, but with little success. It is
claimed by some that certain fluids will bleach and bring
out the natural color.
A small amount of bile is sufficient to tint the surface
of the body. Bile is composed of salts, fats, organic
matter, acids, and also coloring matter, called the bile
pigments. Bilirubin is the principal coloring matter, and
when dissolved in alkali, forms, when coming in contact
with the air and also in the dead body, a green precipitate
known as biliverdin. The bile pigments in the blood are
[332]
carried with the serum from the capillaries to the tissues,
being deposited in the internal coat or deep layer of the
epidermis as well as the papillary of the dermis. The
amount deposited regulates the extent of the pigmentation.
One of the most beneficial things to do, where pigmentation
is present is to wash out the arterial system,
draw blood from the veins, massage the exposed parts.
Inject a diluted fluid at first, follow with a fluid of full
strength, until complete disinfection and permeation of
the tissues has taken place. Keep up constant massaging
during the whole course of injection. This may bring
fair results, with the addition of face tints and showing
the body under artificial light.
Strong solutions of formaldehyde when used at first
are deleterious, causing the skin to become green. This
greenness is more pronounced when chemicals such as
methylene blue have been administered by the attending
physician before death. Bilirubin is a red yellow color, and
alkalies precipitate the bilirubin and form biliverdin.
Biliverdin is a greenish color.
All fluids contain alkalies, and are mostly alkali in
reaction, and this may account for the greenish color of
the skin after the injection of fluid. Acids do not precipitate
the biliverdin and there is a tendency to dissolve
it and keep it in solution.
Moadinger suggests that a weak solution of some
acid be injected into the arterial system before the injection
of embalming fluid. He prefers a two per cent.
solution of oxalic acid.
Dhonau prefers the use of a one or two per cent. solution
[333]
of borax, to be injected into the arterial system,
followed by half strength fluid, and this followed by full
strength fluid. Dhonau also applies full strength peroxide
of hydrogen to the skin while massaging the face.
Eckels prefers the use of a fluid containing a peroxide.
If methylene blue has been administered by the attending
physician and you have learned this fact before
hand, it is then not advisable to use a formaldehyde fluid.
There is a chemical action set up between the methylene
blue and the formaldehyde which will give to the tissues
a greenish color which is quite objectionable. In this
case you would inject some fluid which does not contain
formaldehyde. A benzoate of soda or borax, or peroxide
solution would do.
A good formula to use, when you know methylene blue
has been used by the attending physician is:
| Rx | Carbolic acid | 5 | oz. |
| Borax | 12 | oz. |
| Glycerine | 1 | oz. |
| Water, qs. | 1 | gal. |
For transportation, govern yourself according to the
transportation rules.
Cirrhosis of the Liver.
—Synonyms.—Interstitial Hepatitis;
Sclerosis of the Liver; Nutmeg Liver; Hobnailed
Liver.
Definition.—A chronic disease of the liver, characterized
by an increased connective tissue, a reduction in
the size of the organ, and a degeneration of the parenchymatous
constituents.
[334]
Etiology.—In a great majority of cases the disease
is due to alcohol, syphilis, highly spiced and very rich
foods. Cirrhosis may result from chronic obstruction of
the bile ducts, due to gall stones, or tuberculosis. Cirrhosis
frequently occurs between the ages of thirty and
sixty years, though it may be found in the extremes of
life. Men are more liable to contract the disease, owing
to greater dissipations.
Pathology.—The liver is increased in size by the increase
of connective tissue, and hyperaemic. On the surface
it exhibits a knobbed appearance (hobnailed liver)
and these knobs present through the capsule a yellowish
appearance. The granulations vary in size from a pinhead
to a pea. As a rule there is a little jaundice, as
there is a decrease in the production of bile, instead the
skin takes on an earthy, sallow tint. There is generally
ascites, swelling of the feet and legs, which increases
until the abdomen and the lower extremities become
of an enormous size. The nutrition of the body
suffers, the skin is dry and harsh. The blood is altered
in quantity, and coagulates quickly. Ecchymotic spots
appear on the skin, about the face and nose.
Treatment.—There are probably not many other cases
of death, which need greater skill and intelligence in
their treatment than does cirrhosis. The condition that
presents itself is a distended abdomen with gas and liquid.
The limbs are also distended and the upper part of the
body is wasted away and is greatly discolored as death
was caused by asphyxia.
Place the body on the board, open the femoral vein,
[335]
and insert your drainage tube. It is better to use this
vein as it is larger, and there is more control of the removal
of blood, and we would advise in this case the use
of the flexible rubber drainage tube, which can be pushed
up in the vein till it reaches the right auricle of the heart
if you wish. Drain all the blood possible. Use the trocar
method, see page 255, or the direct incision, see page
257, to remove the gases and ascitic fluid from the abdomen.
Use the bandage method, see page 339 to remove
the water from the tissue of the extremities.
Raise the femoral artery and inject slowly a diluted
fluid and massage the face gently toward the jugular vein,
using some recognized face bleacher. Then follow with
an injection of fluid of full strength until you are sure
the fluid has permeated every tissue of the body. Do not
be afraid to use plenty of fluid. Inject the cavities.
For transportation, govern yourself according to the
transportation rules.
Carcinoma of the Liver.
—Definition.—A cancerous
growth in the liver.
Pathology.—Jaundice is present in most cases and
where the portal circulation is seriously compressed, ascites
developes. The liver is greatly enlarged, and the
surface is nodular.
Treatment.—As in all chronic affections of the liver,
where the skin takes on a yellowish or bronze hue, due
to pigmentation, it is almost impossible to bring about
the desired cosmetic effects. The pigment is not only in
the blood vessel but also in the tissues of the skin.
[336]
We would advise the washing out of the tissues, by
the use of the oxalic or borax solution, injecting the
axillary artery and draining from the femoral artery or
raising both the carotid arteries, injecting upward on
one side and draining from the other.
For transportation, govern yourself according to the
transportation rules.
Appendicitis.
—An inflammation, acute or chronic, of
the appendix.
Pathology.—The pathology will depend to a great
extent upon the degree of the inflammation. Ulceration
may take place or there may be perforation.
Treatment.—If, after an operation, reopen the incision
made by the surgeon, relieve the gas pressure on
the intestines by incising them; surround the intestines
with hardening compound; then inject an artery, using
half strength fluid for the first 64 oz., followed by enough
normal fluid to secure preservation. Drain the blood
during the injection by one of the drainage processes.
If no operation has been made, insert a trocar into the
caecum to relieve the gas pressure, then inject normal
fluid into the same place, using sufficient fluid to neutralize
the process of putrefactive fermentation. The trocar
can be first inserted in the usual place passing it to the
caecum, or through the abdominal wall directly over the
caecum. The arterial injection and drainage should be
made as is mentioned above. For transportation, govern
yourself according to the transportation rules.
Peritonitis.
—An acute or chronic inflammation of the
peritoneum either local or general.
[337]
Pathology.—There is nearly always present more or
less fluid in the abdominal cavity.
Treatment.—Drain blood from a large vein, and inject
half strength fluid for the first part of the injection, following
this with enough normal fluid to preserve the tissues
of the body. After the arterial injection and drainage
have been completed, pierce the abdominal cavity in
the usual place and draw off all the fluid that you can
reach, paying especial attention to the lower part of the
cavity. Then inject normal or supernormal fluid into
the cavity to neutralize the process of putrefactive fermentation.
Pierce the colons and inject fluid into them
as well. If fermentation resists this treatment, make a
small incision along the median line and above the umbilicus,
examine the stomach and intestines, incising them
if they contain the gas. After eliminating the gas, inject
fluid directly into them, or, surround the organs of the
cavity with good hardening compound; sew up the incision
and the body should not deteriorate in any way.
For transportation, govern yourself according to the
transportation rules.
Dropsy.
—Definition.—Dropsy is the accumulation of
serous fluid in a cavity or in the tissues.
Dropsy of the abdomen is called ascites.
Dropsy of the chest is called hydrothorax.
Dropsy of the peritoneum is called hydroperitoneum
or ascites. General dropsy of the cellular tissues is called
anasarca.
Ascites.
—Synonyms.—Dropsy of the Peritoneum; Abdominal
Dropsy.
[338]
Definition.—An accumulation of serous fluid in the
peritoneal cavity.
Etiology.—Any obstruction of the portal circulation
is a possible cause of ascites, the most frequent being
cirrhosis of the liver. Pressure from tumors or neighboring
organs may also give rise to it. Peritonitis and
valvular diseases of the heart are also responsible for
ascites, and chronic pulmonary affections may impair the
portal circulation to the extent of producing it.
Pathology.—The quality and character of the fluid
show great variation, from a few pints to several gallons,
and from a straw or lemon tint to a brownish or greenish
hue. It may be blood stained, and occasionally clean and
transparent. It is usually watery in character.
Treatment.—Use the trocar method. Insert the trocar
through the umbilicus and draw off all the ascitic fluid
from the abdomen, then surround the organs with a quantity
of fluid sufficient to preserve them. Or if you desire,
use the direct incision and after the ascitic fluid has
been drawn off, surround the organs with a hardening
compound.
The body in general should be preserved through an
arterial injection of normal fluid for the first 64 ounces,
then one and one-quarter strength for all subsequent
bottles. This, if attended by copious drainage from a
large vein, will preserve all portions of the body excepting
possibly the epidermis of the posterior abdominal wall,
which, by gravitation of the ascitic fluid, will become
separated from the derma, producing skin slip, and causing
the formation of blisters.
[339]
Previously to placing the body on the embalming
board for treatment, a rubber cover should be placed
over the board so that drippings of all kinds can be made
to flow into a bucket at the lower end of the embalming
board. When the above mentioned blisters are cut and
their contents disposed of by gravitation into the bucket,
a strong solution of formaldehyde should be applied to
the affected skin to harden it and to prevent any further
progress toward decomposition.
In ascitic cases the casket should be lined with rubber
or oil cloth to a point three or four inches above the
bottom. In addition to this precaution, the use of sawdust
is favored so that any unlooked for breaking of
blisters may not be attended by a flow of the ascitic
liquid from the casket. Many embalmers do not protect
themselves against contingencies of this kind and are
frequently criticized by the friends and family of the
deceased.
Anasarca.
—Definition.—Anasarca is a general dropsy
of the cellular tissues.
Treatment.—Bandage Method.—Bandage the extremities
of the body, commencing at the toes and finger
tips, bandaging upward to the hip and shoulder, using
a rubber bandage. Relieve the water as you go along,
then rebandage, and by the third application you will
have removed most of the water from the extremities. Do
not leave the bandage on while injecting.
Bandage Method.—Bandage the lower limbs, commencing
with the thighs. Bandage as tight as possible
down to the toes and make an incision in the heel, from
[340]
which drainage of the serous fluid can be secured. In
this method no laps are left between the bandaging so
that the serous fluid can be forced toward the opening
at the heel. (This method is said to be reliable, although
we have had but little experience with it.)
Any accumulation of ascitic fluid in the cavities should
be removed by aspiration with the trocar, as described
in the treatment of ascites and hydrothorax. The
rubber cover for the embalming board as described in
the treatment for ascites, should not be omitted.
After the water has been eliminated as far as possible,
the arterial injection should be made, using 64 ounces of
normal strength fluid, followed by enough one-fourth
strength fluid to secure preservation. Copious drainage
will help to clear the blood vessels and allow a better
distribution of the fluid, thereby assuring good preservation
of all parts excepting the epidermis, which is practically
closed off to the fluid by the accumulation of water
in the subcutaneous tissue.
In these cases the skin should receive a good application
of strong formaldehyde fluid before and after the
principle operation, so as to strengthen it against the
putrefactive tendencies of the rete mucosum.
These cases should be watched closely between the
time of embalming and the funeral, as the most thorough
preparation is sometimes unequal to the task of preserving
the entire body in such a way as to prevent the
formation of blisters.
For transportation of all dropsical conditions, govern
yourself according to the provisions of the transportation
rules.
[341]
CHAPTER XXIII.
TREATMENT OF ACCIDENT CASES.
Under this head are treated those deaths which are
the result of accident.
Specific Treatment of Accidents.
—Broken Neck, Hanging,
Strangulation.—The mode of death may possibly
cause a separation or dividing of the blood vessels of the
neck. If this is the case there will remain in the head
and face a large amount of blood, which would soon become
coagulated, causing a dark bluish turning black
discoloration. The treatment then must be to get this
blood from the face, so would recommend the common
carotid for injection of fluid and the internal jugular vein
for the removal of blood.
Raise both the artery and the vein to the surface, and
insert the arterial tube in the artery toward the face, and
inject a small quantity of fluid in order to cause a pressure
on the venous system, then open the vein, insert the
drainage tube and begin to remove the blood, and as the
blood drains from the drainage tube inject slowly into
the artery. This will help to push the blood out of the
capillary system and into the blood bottle and thus clear
up the face of its discoloration.
[342]
In these cases the raising of only one common carotid
would hardly suffice, and it would be far better to
operate on both carotids to get the best results. For
this reason then the circular incision would be the best
operation, and perhaps the use of the Y shaped drainage
tube. With the Y shaped drainage tube both sides of
the face could be injected at the same time, and the blood
could be removed from both internal jugular veins, and
the operator could not help but get good results. The
removal of blood from the internal jugulars in this direct
way will relieve the pressure in the capillaries and
smaller veins and induce a better circulation to all the
immediate tissues.
Body Severed.
—For these cases one should have a
very good idea of the general arterial and venous circulations
of the body, for many of the smaller as well as the
larger vessels will be cut, necessitating one to tie them
off.
If the body is severed below the diaphragm remove
and cleanse all the loose and injured organs and tissues,
place them in a bucket or pan and cover with fluid.
Ligate all the injured arteries and veins in the upper and
lower parts.
Inject the lower extremities from inside the abdominal
cavity using the common iliac artery, observing the presence
of the remaining united arteries and veins, which
you can now see, for fluid will leak from them. The lock
forceps will enable you to pick them up and with the
aneurism needle dissect around the end of the vessel
and tie each one tight.
[343]
Treat the upper extremity in the same way injecting
either from the inside or the outside, according as the
severity of the accident may lead you to decide. Inject
from the inside upward through the aorta, or from the
outside either through the radial, brachial, axillary or
carotid.
The trunk may now be sewed together, beginning at
the middle of the back. Sew each side up leaving the
top open to receive the organs and the tissues which were
removed. After these are placed more or less in position
sprinkle hardening compound throughout the cavity.
Now sew up the front and then place a strong bandage
around the body.
The Arm Severed.
—Clean off the parts, and inject the
severed part through the radial towards the hand and
by means of collateral circulation through palmar arch,
the upper part will be embalmed and the arteries that
have been severed disclosed, when they can be tied off.
If there is a great leakage through the stub end, and all
the arteries can not be tied off, plaster of paris may be
put on the stub and then a strong and tight bandage
drawn around.
The remaining body can then be injected through
the opposite carotid, brachial or femoral, and when the
leakages begin to occur at the stub end of the arm they
can be found and tied off or if the leakage is too great
plaster of paris may be used and a tight bandage placed
about the stub end.
After both the arm and the body have been injected
the arm can now be sewed on in its natural position,
[344]
plaster of paris put around and a strong bandage placed
around or a splint may be used on both sides.
The Leg Severed.
—Clean off the parts, and inject the
severed part through the large dorsal toward the foot
and by means of collateral circulation through the plantar
arch, the upper part will be embalmed and the arteries
that have been severed disclosed, when they can be
tied off. If there is a great leakage through the stub end,
and all the arteries can not be tied off, plaster of paris
may be put on the stub and then a strong and tight bandage
drawn around.
The remaining body can then be injected through the
carotid, brachial, axillary, or the opposite femoral and
when the leakages begin at the stub end of the leg they
can be found and tied off, or if the leakage is too great
plaster of paris may be used and a tight bandage placed
about the stub end.
After both the leg and the body have been injected,
the leg can be sewed on in its natural position, plaster
of paris put around and a strong bandage placed around,
or a splint may be used on both sides.
The Head Severed.
—Clean off the parts, and inject the
head through the stub end of the carotid artery, and
by means of collateral circulation through the circle of
Willis, the fluid will leak through the other severed vessels
and disclose them, so that they can be tied off. If
one side of the face should take more fluid than the other
side by this method the other carotid can be injected
so as to equalize. It would perhaps be impossible to
[345]
tie off all the tiny vessels that are severed so plaster
of paris may be used to cover the stub end.
To inject the body, the four principle arteries to be
tied are the two common carotids and the two vertebrals,
besides numerous veins and small vessels. If it is impossible
to tie all the severed vessels plaster of paris may
be used, and then by injecting either through the brachial,
axillary or femoral a thorough injection may be obtained.
The stub end of the carotid might also be used for injection,
but would not advise it as in most cases we find
that it would be hard to get especially if the head were cut
off close to the shoulders.
When both the head and the body have been injected,
bring the two parts together by using a splint in the
vertebral column, and having plastered well together
sew the skin. Demi-surgery can be practiced to the fullest
extent in this case, with great cosmetic effect.
The Head Crushed.
—Remove all the coagulated blood
and the injured parts of the brain. Cleanse the cavity
thoroughly and remould with plaster of paris. Inject
the best you can through one or both of the carotid arteries,
and complete the injection hypodermically. Inject
the rest of the body in the regular way, through one of the
carotids raised for the injection of the head. With the
practice and use of demi-surgery, all the bruised and torn
fragments may be blended together, and the cosmetic
effect made almost perfect.
—Remove all the coagulated blood
by washing, and place all the parts together as nearly
natural as possible. Now inject any of the principle arteries
[346]
used in embalming, watching carefully the flow of
fluid and blood. As soon as you see a leakage stop injecting
long enough to tie it up, and when all the visible
leakages have been thus treated, wrap the whole of the
injured part with a bandage saturated with a plaster
of paris solution. After this becomes dry and set complete
the injection.
The Chest Crushed.
—Open up the cavity and remove
all the injured organs and tissues, which you will place
in a vessel containing formaldehyde fluid. With a soft
sponge remove all the coagulated blood from the cavity.
Now tie up all the visible arteries and start the injection
from the inside, using first the innominate to inject the
right arm and the right side of the face then the left common
carotid to inject the left side of the face and the
left subclavian to inject the left arm. It must be remembered
though that while one artery is being injected
the others should be tied off lest by collateral
circulation you would get leakages. The thoracic aorta
might be used but it will be found more difficult because
of the leakages which would occur through the intercostal
arteries. These leakages would not occur nearly as
much by the raising of the branches off the arch of the
aorta, namely the innominate, the left common carotid
and the left subclavian. Any leakage can be stopped by
means of the lock forceps and then tied.
The lower part of the body, if it is not injured, can
be injected now through the abdominal aorta, but if
there has been any damage done below the diaphragm, it
[347]
would probably be best to further open up the cavity and
inject each lower extremity through the common iliacs.
Now replace all the organs and surround them with
hardening compound, and sew up the cavity incisions,
with great care and neatness. It would be well to practice
demi-surgery here, so that you would become more
proficient in the art, and thus be able to do more efficient
work on the exposed parts, should the occasion ever demand
it.
Gun-shot in the Abdomen.
—When death occurs it is
generally due to severing or dividing of an artery or decomposition
resulting from the injury done the intestines.
The operator should open the body cavity, from the end
of the sternum bone to the pubic bone, and cleanse the
cavity of all the coagulated blood and other putrid matter.
Locate and tie up the injured vessels. The injection can
then be started from one of the principle arteries which
will aid in locating the other injured vessels. Puncture
the stomach and inject inside, so as to prevent the formation
of gas, and after the body has been injected place
hardening compound inside the body cavity and sew up
carefully and neatly.
Burns and Scalds.
—A burn is an injury to the body
produced by the application of a flame or of a substance
heated above a certain temperature.
A scald is an injury produced by the application of
a liquid heated above a certain temperature.
Injuries resulting from corrosive liquids such as
sulphuric acid, nitric acid, caustic potash, carbolic acid,
[348]
etc., are properly termed burns. A heated solid such as
iron may produce a burn of great intensity from the
blistering of the skin to the charring of the underlying
tissues. Metals heated above 212 degrees Fahrenheit will
produce redness, vesication and coagulation of the blood.
Molten metals cause burns or scalds very similar to those
produced by heated solids. Boiling oil produces severe
burns. If a part is severely scalded with boiling water,
the skin may appear sodden, blistered, and of an ash
grey color, but never produces blackening or charring of
the cuticle. Phosphorous burns are usually very severe
and of great depth, while the area of skin destroyed is
usually small. Gunpowder burns caused by explosions
are often of great superficial extent, extensive scorching
and numerous carbon particles are commonly found imbedded
in the true skin. Petroleum burns are generally
severe, as usually all or nearly all the body is scorched
and blackened. Burns from flame, extensive scorching
with burnt hair is a usual feature in a flame burn.
Burns from explosions of fire damp in coal mines are frequently
of great extent and present the appearance of
great scorching, and very often a quantity of coal dust
will be found imbedded in the true skin. There are six
degrees of burns as follows: (a) Simple hyperemia of
the skin, (b) dermatitis, with vesicles or bullae, (c) necrosis
of the superficial layer of the skin, (d) complete
necrosis of the skin, (e) necrosis of the skin, superficial
fascia and muscles, and (f) complete carbonization of
the part.
Treatment.—The embalmer does not treat these cases
[349]
according to the cause as much as to what is left of the
part after burning has been accomplished. After observing
the part to note whether the condition can be bettered
by a replacement of tissue by artificial means and finding
such to be the case, I would use a form of paste commonly
used for filling in cuts and restoring the features
and with this paste thoroughly cover the burned part.
If the affected part covers the entire face or most of it,
an entire new surface will have to be built up with the
paste. If the burning of the skin has left particles of
epidermis adhering to the derma, I would use sweet oil
and bath the entire face with it, thus softening the skin
and allowing the removal of the small particles. Any
small desiccated spots should be covered with the paste.
After carefully blending the paste with the skin so as
to produce a smooth even complexion, which can best be
done by the use of a brush to smooth it with, apply a good
quality of face powder (flesh color) to the part. If the
color is too striking, or too white, destroy the contrast
with carmine rouge. This form of operation is commonly
known as demi-surgery. We find that the face powder
is best applied with a pad made of surgical gauze especially
when applied with a patting movement. This
gives a good imitation of the pores of the skin, and if
any further smoothing is necessary the brush can be used
again. The principal result wanted is a good imitation
of the natural parts. If the operator will use the utmost
care to give the parts gentle, fine touches here and there,
a most artistic effect will be produced. If the eye brows
have been destroyed, imitate them with charcoal, carbon,
or dark theatrical paint. A good make-up outfit is indispensable
[350]
for an embalmer handling many railroad cases
during the year, and as such can be had at any dealer in
theatrical supplies, we advise the securing of a few
varieties of pastes, and some good face powder together
with carmine rouge.
If the face is damp or moist, the theatrical paste
above mentioned will not adhere properly, and in that
case alcohol applied to the skin will cause it to dry. One
of the most important considerations in these cases, is
the placing of the body in the casket. The body should
be placed as low as possible, the silk slide should be
closed and a view of the body only secured through it,
the light in the room should be tempered so that no striking
rays of light serve to distort any portion of the features.
Wonderful work has been accomplished by the
authors and by others in rescuing cases of this kind from
non-presentability to presentability, but in all cases, the
ingenuity of the operator is taxed to the utmost, and the
case never looks just right until the last touch is applied.
With the above information, you have only the rudiments
of the work. Your success or failure will depend upon
how hard you try to make good in each individual case,
and your success in matching colors, which can only be
acquired with much patience.
Give burned bodies a very thorough arterial injection,
using half strength fluid for the first part of the injection.
The cavities should also receive a good injection of normal
fluid. The peculiar odor present about a burned body
can be lessened by the use of false deodorizers such as
flowers, perfume, etc.
[351]
CHAPTER XXIV.
TREATMENT OF POSTED CASES.
Cranial Evisceration.
—By this term is meant the complete
removal of the brain. To do so the scalp is cut
from ear to ear, the front part is pulled forward over
the nose and the back part over the occipital bone. A
skull clamp is placed in position and with a saw take
away the calvarium. When the calvarium or skull cap
has been removed the brain is in full view and can be
easily removed by cutting the arteries at the circle of
Willis and the ligaments at the base of the skull.
Thoracic Autopsy.
—By this term is meant the complete
removal of all the organs of the thoracic or chest
cavity. To do so the skin is cut on either side from the
sterno-clavicular junction to a point where the ninth
rib joins to its costal cartilage. The ribs are cut on either
side at the costochondral articulation, which will permit
the entire front chest wall to be taken away. The
heart and lungs are now in full view and can be easily
removed.
Abdominal Post.
—By this term is meant the complete
removal of all the organs of the abdominal cavity. To do
so the skin and muscles are cut on either side from a
[352]
point where the ninth rib joins its costal cartilage vertically
downward to about an inch above Poupart's ligament
and from there to the top of the pubic bone. When
the anterior abdominal wall has been removed all the
organs will be in full view and can easily be removed.
Posted Cases.
—By this term is meant those cases
on which an autopsy has been held and all the internal
organs of the body have been removed. Here all the
internal circulation has been destroyed.
Treatment.—Place the body on the cooling board
and undo all the stitches made by the physician in sewing
up the body after the post-mortem. Remove all the
organs, that have been previously removed by the physician,
and place same in a bucket or other container.
Clean out thoroughly all the blood from the cranial,
thoracic and abdominal cavities. Now try to tie off the
arteries in the cranial cavity which will be the vertebrals
or the basilar and the common carotids. If these
have been cut too short to be tied, then mix up some
plaster of paris and cover them securely so that there
will be no leakage. While the plaster of paris is setting
raise the common iliac artery, which you will find at
the back of the abdomen just over the ilio-psoas muscle,
represented by a line drawn from the body of the fourth
dorsal vertebra to the center of Poupart's ligament.
Inject the right and left common iliac arteries downward
which will take care of the lower extremities. Here the
only artery you need to tie off is the deep epigastric
artery which is a branch of the external iliac just a short
distance above Poupart's ligament and which takes a
[353]
course upward over the abdominal muscles finally to
anastomose with the deep mammary artery.
By the time you have injected the lower extremities,
the plaster of paris will be set. Work from the inside of
the thoracic cavity, and tie off the innominate, left common
carotid and the left subclavian arteries, and when
this has been accomplished inject each one separately.
Here the only leakage you will have will be through the
mammary or intercostal arteries which you will tie off
as the leakage occurs.
Now turn the body over and hypodermic the back,
then turn body over again. Fill the cranial cavity with
sawdust, place the skull cap in position and sew up the
scalp. Wash all the organs and place them back in the
cavities in their proper positions or as nearly so as possible
and as you do so fill in with hardening compound. Sew
up the abdomen and wash the body with a disinfecting
solution and apply outward cosmetics.
[354]
CHAPTER XXV.
TREATMENT OF MISCELLANEOUS CASES.
Alcoholism.
—Definition.—An intoxication, acute or
chronic, due to the injection of a sufficient quantity of
alcohol to produce muscular inco-ordination, mental disturbances,
and finally narcosis.
Pathology.—Where death is the result of acute alcoholism,
the mucous membrane of the gastro-intestinal
canal is engorged, injected, and dark red in color, and
covered with a sticky, mucoid exudate. The brain and
the kidneys show the same characteristic changes. In
chronic alcoholism, changes of a more permanent character
take place, depending somewhat upon the quantity,
quality and kind of alcoholics consumed, and the length
of time used. While all the bodily tissues are more or less
impaired, the brain, kidneys, and digestive system suffer
most. There may be connective tissue changes, fatty degeneration,
sclerosed kidneys, liver or arteries, and a
more or less dilatation of the stomach.
Treatment.—In acute alcoholism, the blood should
be drained from a large vein, while fluid is being injected
into a large artery. After draining a sufficient amount of
blood from the body, the vein tube should be shut off
[355]
and the arterial injection should continue until the capillaries
have been filled to their utmost capacity. This
strong treatment is advised on account of the early tendencies
toward putrefaction, which is sometimes in an
advanced state shortly after death. The cavities should
receive a thorough treatment with normal or supernormal
fluid. Myers advises the re-injection of the cavity in 6
or 8 hours after removing the fluid remaining in the
cavity from the first injection. As a preventive treatment,
this last is a wise precaution. While the cavity
treatment is being given the stomach should be entered
by the trocar, relieved of its contents and injected, thus
preventing post-operative purging.
In chronic alcoholism, the greatest circulation difficulties
will be encountered. The capillaries will not receive
the fluid, the putrefactive processes causing the formation
of tissue gas early in the case, which, when
coupled to many natural impediments to the circulation
in cases of this kind, virtually nullifies the circulation for
fluid distribution. Inject as many arteries as possible,
and if necessary the veins also. Use the hollow needle
or trocar and give the unexposed portions of the body a
heavy hypodermic injection. The fluid used in this case
should be not less than normal in strength and in most
cases should be at least ¼ over normal. Give the cavities
a very heavy injection, paying special attention to the
food passages. This is one of the cases coming to the attention
of the embalmer where every emphasis must be
laid upon the injection of a sufficient amount of fluid,
through as many channels as possible. Do not count the
cost of the fluid in this case, if you value the securing of
[356]
satisfactory results. Cosmetic effect will be enhanced by
injection of the carotids upward with drainage from the
internal jugular veins. Finish the case with the use of
good face powder, unless a discoloration is present, when
this should be obliterated with one of the improved
methods mentioned in the chapter on discolorations.
Morphinism.
—Definition.—A chronic intoxication due
to the habitual use of opium, or some of its alkaloids,
especially morphine.
Pathology.—There are no characteristic tissue
changes, other than that due to indigestion and malnutrition.
At death the patient is anemic, the skin dry,
sallow and inelastic, the heart and blood vessels show
the effects of poor nutrition, and the tissues generally
present a starved appearance. The blood disintegrates,
causing a discoloration of a brownish color, one or two
days after death.
Treatment.—Drain blood from these cases using half
strength fluid for the first part of the injection. The more
blood obtained, the less the danger of discoloration will
be. Give the body a thorough cavity injection in addition
to the arterial injection. If your treatment does not
eliminate the blood as a factor, the discoloration will
occur and then it cannot possibly be removed. In this
case the use of cosmetics, if in the hands of a patient
operator, will overcome the color.
Plumbism.
—Synonyms.—Lead-poisoning.
Definition.—A chronic intoxication due to absorption
of lead.
[357]
Pathology.—The muscles are atrophied and pale in
color. Arteriosclerosis of the cerebral blood vessels is
found. There may be softening of the brain and hemorrhage.
Treatment.—Drain blood from the veins while injecting
fluid in the arteries. The fluid should be used half
strength for the first bottle of the injection. Massage
the face downward to help eliminate any discoloration
of blood origin from cerebral hemorrhage. Give the body
a thorough injection both as to arteries and cavities. If
the face is unduly pale from this treatment, carmine
rouge, judiciously applied will lessen the paleness.
Arsenicism.
—Definition.—A chronic intoxication
caused by the continued absorption of arsenic.
Treatment.—Same as for plumbism.
Mercurialism.
—Definition.—A chronic mercurial poisoning,
caused, either by ingestion of the drug, or by inhalation
and absorption of the mineral in the industrial
pursuits.
Pathology.—There is an acute inflammation of the
mouth, stomach, and intestines. The kidneys are inflamed
and the liver is degenerated.
Treatment.—Drain blood from a large vein while the
injection is going on. The first bottle of fluid for the injection
should be half strength. The cavities should be
injected, as intense inflammation takes place in the alimentary
tract.
Heat-Stroke.
—Synonyms.—Sunstroke.
Definition.—Heat-stroke is the result of exposure to
[358]
intense heat, either from the direct rays of the sun, or the
radiation of blasts or furnaces, or to an overheated atmosphere.
Pathology.—Owing to the excessive heat of the body,
putrefactive changes occur very early. If a post-mortem
examination is made very soon after death, the left heart
will be found contracted, while the right heart will be
engorged, and the venous trunks filled with dark semi-fluid
blood. There is also venous engorgement of the
brain, spinal cord, and lungs. Ecchymoses and extravasations
of blood are found in the skin and mucous membranes.
Treatment.—Drain blood from a large vein during the
injection. The first two bottles of the injection should be
of half strength fluid. The face should be massaged to
assist in the securing of capillary circulation and in the
elimination of the blood discoloration. The body should
be treated as soon as possible after death, as putrefaction
begins early. The cavities should have a very thorough
treatment, eliminating the gases and injecting normal
fluid therein. Should ecchymosis occur, obliterate the
color by an application of cosmetics.
Obesity.
—Definition.—An excessive accumulation of
fat, impairing the bodily functions, or rendering one uncomfortable.
Treatment.—Drain blood from these cases, injecting
the first bottle of fluid half strength followed by normal
fluid for the balance of the injection. Massage the face
downward during the injection. Inject the cavities, with
special attention to the stomach and intestines. For
[359]
transportation of these cases, govern yourself according
to the provisions of the transportation laws.
Elephantiasis.
—Definition.—A chronic disease caused
by inflammation and obstruction of lymphatics and
marked by great thickening of the skin.
Treatment.—Drain blood from these cases and inject
normal fluid sufficient enough in quantity to secure preservation.
For long time preservation, supplement the foregoing
treatment by a special injection into the thickened
extremity, either through an artery leading directly to
the part or by trocar or hollow needle inserted under
the skin. Give the body a thorough cavity treatment,
using normal fluid throughout. For transportation,
govern yourself according to the provisions of the transportation
laws.
Drowned Cases.
—Treatment.—Inject fluid into the
lungs by inserting a child's trocar into the windpipe at
the upper border of the sternum, making the injection
sufficient in strength and amount to fill the lungs. If this
is not done, a bloody purging will take place several
hours after death. Tap the stomach through the epigastric
region, aspirate the contents and inject strong fluid
before removing the instrument. Drain blood from the
body during the injection, which should be quite heavy
and of normal fluid. The last bottle should be made 1¼
strength or ¼ over normal.
Floater.
—Definition.—A body that has been floating
on the water.
Treatment.—The body is distended with gases in the
cavities, tissues and capillaries, putrefaction is in an advanced
[360]
state, and a vile odor will be present. If body is
to be shipped, aspirate all the gas possible from the tissues
with the hollow needle, injecting strong fluid in the
same openings. Open the body from the base of the neck
to the pubic bone, relieve the gases in the alimentary
tract and lungs, and fill cavity thoroughly with hardening
compound, after which it should be sewed up. Inject
as many arteries as possible with very strong fluid. Dress
the body and place it in a metallic casket. Pour the contents
of two pound bottles of Platt's chlorides on the
underclothing to assist in deodorizing the body. Do not
open the casket after it is once sealed.
If the body is not to be shipped, it will be advisable
to deodorize it as much as possible and bury it without
delay.
Mother and Unborn Child.
—Mother and Foetus in
Utero.—Treatment.—Before pregnancy has reached the
three months stage, the child will receive fluid directly
from the circulation connected with the mother.
After the three months stage, the circulation, by direct
flow, is stopped and fluid could only reach the foetus by
absorption from the placenta. This is naturally insufficient
to preserve the child, which by this time is immersed
in the liquor amnii (water of the womb) and
which is subject to early putrefaction in that situation.
The trocar should be directed to the uterus or womb
from a point on the median line, half way from the umbilicus
to the pubic arch, care being taken to reach the
water which surrounds the foetus. Withdraw the water,
and inject as much strong fluid as possible so that the
[361]
foetus will be surrounded with fluid, and in that way
preserved. If the trocar enters the body of the child, this
will not occur, so the instrument should be carefully manipulated
to reach the space between the child and the
uterine wall. The mother should receive a very heavy
arterial and cavity injection, with full drainage of blood.
The vulva should be closed with absorbent cotton. The
face should be massaged thoroughly toward the heart.
Senility.
—Synonyms.—Old age.
Definition.—A state of decline in an aged person
characterized by progressive atrophy of all the tissues and
organs.
Pathology.—Excessive shrinking and obliteration
takes place among the capillaries. The skin becomes
diminished in thickness. When this occurs, it is easily
seen why in old age there will follow, after the injection
of fluid into the arterial system, greenish, brownish, and
soft spots, in the different parts of the body, especially
notable in the face, neck and hands. The products of degeneration
may accumulate in the tissues and cause them
to be thicker than they are in health, as is seen in the
vessels, the walls of which are much thicker than normal.
The blood contains fewer corpuscles and solid constituents,
is more watery, and coagulates more readily; also the
total quantity is less. The pericardium, endocardium, and
the capsules of the liver and spleen are opaque and
toughened. Degeneration of the cardiac substance may
lead to a state of asthenia, which generally produces
death. Dilatation of the orifices of the heart may be the
prominent lesion, or they may be contracted by atheroma,
[362]
or by thickening of the vales or rings. The lungs are
changed more or less, increasing the bronchial secretions,
which during life have been attended by severe paroxysms
of coughing.
Treatment.—Inject half strength fluid for the first
bottle, following that with ¾ strength for the second
and normal for the third and all thereafter if more be
necessary. Blood may be drained from the vein if the
operator thinks it advisable. The commercial face solution
or water should be used on the face while massaging
in order that the skin may be kept moist and to prevent
dessication from the action of the fluid. The cavity should
be injected as a matter of precaution.
Gangrene.
—Synonyms.—Senile gangrene; mortification.
Definition.—Putrefactive fermentation of dead tissue,
from various causes.
Treatment.—The extremities are affected in senile
gangrene. They should be wrapped with absorbent cotton
which should then be saturated with fluid. The body
itself should receive the same treatment accorded in
the paragraph on senility.
[363]
INDEX
(References are to pages.)
A.
- Abdomen, 101, 254
- Abdominal cavity, 101, 254
- Abdominal fermentation, 182
- Abdominal post, 351
- Absence of normal moisture in skin, 200
- Alimentary canal, 96
- Anatomical guides, 225
- Anatomy, 33
- Angiology, 34
- Antemortem staining, 191
- Anus, 112
- Apnea, 157
- Aponeuroses, 55
- Appendix, 109
- Arterial system, 125
- Arteries, structure of, 58
- Artery, differentiated from nerve, 215
- Artery, differentiated from vein, 215
- Artery, how to cut for injection, 216
- Artery, how to raise, 214
- Artery, selection of, 211
- Ascending color, 111
- Asphyxia, 157
- Axillary artery, location, 231
- Aztecs embalming, 19
- Azygos system, 125
B.
- Babylonian embalming, 17
- Bandage test, 159
- Belgian embalming, 18
- Bladder, urinary, 118
- Blood, 61
- Blood coagulation, 65
- Blood corpuscles, 63, 64
- Blood plasma, 62
- Blood, removal of, 264
- Blood vascular system, 123
- Bones, 48, 69
- Bones of face, 74
- Bones of lower extremity, 77
- Bones of pelvic girdle, 78
- Bones of thorax, 76
- Bones of upper extremity, 77
- Boudet, 22
- Brachial artery, location, 234
- Britain embalming, 18
- Bronchus, 87
C.
- Cadaveric lividity, 168
- Caecum, 109
- Cancerous spots, 190
- Capillary circulation, 132
- Capillary congestion, 204
- Cardia, 104
- Carotid artery, location, 225
- Cartilage, 48
- Cavities, 79
- Cavity embalming, 247
- Cell, 35
- Cerebro-spinal cavity, 79, 247
- Charge of embalming, 222
- Chemical action, 202
- Christian embalming, 20
- Circle of Willis, 127
- Clavicle bone, 77
- Coagulation of blood, 65
- Collateral circulation, 147
- Colon, 111
- Coma, 157
- Cooling of the body, 167
- Coronary circulation, 142
- Cranial cavity, 79, 247
- Cranial evisceration, 351
- Cranial nerves, 81
- Cranium, 94
D.
- Descending colon, 112
- Descriptive anatomy, 33
- Diaphragm, 99
- Desiccation, 196
- Digestive fermentation, 180
- Direct incision, 257
- Discolorations, 187
- Discolorations after death, 196
- Discolorations before death, 188
- Disinfectants, 221
- Drying action of formaldehyde, 197
- Duodenum, 107
[364]
E.
- Ecchymosis, 191
- Egyptian embalming, 5
- Embalming, 153
- Embalming, abdominal cavity, 254
- Embalming, Aztec, 19
- Embalming, Babylonian, 17
- Embalming, Belgian, 18
- Embalming, Britain, 18
- Embalming, cavity, 247
- Embalming, cerebral cavity, 247
- Embalming, charge, 222
- Embalming, chest cavity, 252
- Embalming, crania cavity, 247
- Embalming, early Christians, 20
- Embalming, Egyptian, 5
- Embalming, Ethiopian, 17
- Embalming, French, 18
- Embalming, Greek, 17
- Embalming, Guanch, 3
- Embalming, Hindoo, 18
- Embalming, Indian, 19
- Embalming, Jewish, 15
- Embalming, later European, 20
- Embalming, Norsemen, 18
- Embalming, Persian, 16
- Embalming, Peruvian, 19
- Embalming, Roman, 17
- Embalming, Scythian, 17
- Embalming, subcutaneous tissue, 260
- Embalming, thoracic cavity, 252
- Epigastric region, 103
- Esophagus, 99, 250
- Ethiopian embalming, 17
- Ethmoid bone, 74
- European embalming, 20
F.
- Face bones, 74
- Falcony, 23
- Fascia, 43
- Fat, 56
- Feather test, 159
- Femur bone, 78
- Fermentation, 179
- Fermentation, abdominal, 182
- Fermentation, digestive, 180
- Fermentation, gastric, 184
- Fermentation, intestinal, 185
- Fermentation, metabolic, 181
- Fermentation, putrefactive, 181
- Fermentation, spirituous, 180
- Feverish condition, 199
- Fibula bone, 78
- First call, 205
- Fluid, injection of, 218
- Foetal circulation, 144
- Foramen of Winslow, 121
- Fractures, 194
- Franchini, 22
- Franciolli, 23
- Freezing of the skin, 199
- French embalming, 18
- Frontal bone, 74
G.
- Gall bladder, 114
- Gangrene, 191
- Gannal, 23
- Gas formation, 179
- Gastric fermentation, 184
- Glands, 47
- Greek embalming, 17
- Greenish tinge of putrefaction, 200
- Guanch embalming, 3
- Guides, anatomical, 225
- Guides, linear, 225
H.
- Hair, 41
- Heart, 92
- Heart sac, 92
- Hindoo embalming, 18
- Histology, 33, 35
- Holmes, 25
- Humerus bone, 77
- Hunter, 21
- Hyoid bone, 75
- Hypochondriac region, 103
- Hypogastric region, 103
I.
- Ileum, 108
- Ilium bone, 78
- Indian embalming, 19
- Inferior maxillary bone, 74
- Inferior turbinate bone, 75
- Inguinal region, 103
- Injection of fluid, 218
- Intestinal fermentation, 185
- Intestines, large, 108
- Intestines, 106
- Ischium bone, 78
J.
- Jejunum, 107
- Jewish embalming, 15
K.
L.
- Lachrymal bone, 75
- Large intestines, 108
- Larynx, 84
- Leucocytes, 64
- Ligaments, 55
- Linear guides, 225
- Liver, 112
- [365]
- Lumbar region, 103
- Lungs, 88
- Lymphatic circulation, 123, 147
- Lymphatics, 44
M.
- Malar bone, 75
- Mediastinum, 91
- Membranes, 57
- Mesentery, 122
- Metabolic, fermentation, 181
- Mirror test, 159
- Modes of death, 155, 156
- Mouth, 97
- Mucous membranes, 57
- Muscles, 54
- Myology, 33
N.
- Nails, 40
- Natural evaporation, 196
- Nerves, 53, 81, 82
- Neurology, 33
- Norse embalming, 18
- North American Indian embalming, 19
O.
- Omentum, 121
- Omohyoid muscle, 75
- Osteology, 33, 69
P.
- Palate, 97
- Palate bone, 75
- Pancreas, 115
- Parietal bone, 74
- Patella, 78
- Pelvic cavity, 118
- Pericardium, 92
- Peritoneum, 120
- Persian embalming, 16
- Peruvian embalming, 19
- Pharynx, 98
- Pigmentary atrophy, 189
- Pleura, 87
- Plugging orifices, 262
- Portal circulation, 144
- Position of body on embalming board, 210
- Positive signs of death, 162
- Postmortem discoloration, 203
- Postmortem staining, 204
- Poupart's ligament, 55, 56
- Premature burial, 164
- Prostate, 119
- Protoplasm, 35
- Pubic bone, 78
- Pulmonary circulation, 134, 141
- Purging, 249
- Putrefactive changes, 160
- Putrefactive fermentation, 181
- Pylorus, 104
R.
- Radial artery, location, 237
- Radius bone, 77
- Raising an artery, 214
- Receptaculum chylii, 46
- Rectum, 112
- Regional anatomy, 34
- Removal of blood, 264
- Removal of urine, 263
- Ribs, 76
- Rigor mortis, 177
- Roman embalming, 17
- Ruysch, 21
S.
- Salivary glands, 98
- Sarcolemma, 54
- Scapula bone, 77
- Scars, 194
- Scythian embalming, 17
- Selection of artery, 211
- Serous membranes, 57
- Signs of death, 155, 157
- Sinuses, 136
- Skeleton, 69
- Skin, 37
- Skin slip, 175
- Skull, 72
- Small intestines, 106
- Sphenoid bone, 74
- Spinal cavity, 81
- Spinal nerves, 82
- Spine, 71
- Spirituous fermentation, 180
- Spleen, 116
- Stomach, 103
- Sucquet, 23
- Superior maxillary bone, 74
- Suprarenal capsule, 117
- Surgical anatomy, 34
- Syndesmology, 33
- Synovial membranes, 57
- Systemic circulation, 125
- Systemic system, 134
T.
- Tattoo marks, 194
- Teeth, 52, 97
- Temporal bone, 74
- Tendons, 55
- Tests of death, 155, 158
- Thoracic autopsy, 351
- Thoracic cavity, 83, 252
- Thoracic duct, 45
- Tibia bone, 78
- Tissue, 37
- Trachea, 85, 250
- Transverse colon, 111
- Treatment of accidents, 341
- Arm severed, 343
- Body severed, 342
- [366]
- Broken neck, 341
- Burns, 347
- Chest crushed, 346
- Foot crushed, 345
- Gun shot in abdomen, 347
- Hanging, 341
- Head crushed, 345
- Head severed, 344
- Leg severed, 344
- Scalds, 347
- Strangulation, 341
- Treatment of diseases, 285
- Actinomycosis, 293
- Ague, 295
- Alcoholism, 354
- Anasarca, 339
- Aneurism, 328
- Anthrax, 285
- Aortic incompetency, 321
- Aortic insufficiency, 321
- Aortic regurgitation, 321
- Aortic stenosis, 321
- Appendicitis, 336
- Arsenicism, 357
- Arterio sclerosis, 325
- Ascites, 337
- Black death, 303
- Black vomit, 296
- Bubonic plague, 303
- Carbuncle, 285
- Carcinoma of liver, 333
- Cardiac atrophy, 324
- Cardiac dilatation, 324
- Cardiac thrombosis, 323
- Cerebro spinal fever, 286
- Cerebro spinal meningitis, 286
- Charbons, 285
- Chicken-pox, 309
- Chills and fever, 295
- Cholera, 302
- Cirrhosis of liver, 333
- Dengue, 294
- Diphtheria, 297
- Dropsy, 337
- Elephantiasis, 359
- Drowned cases, 359
- Endoarteritis, 325
- Endocarditis, 320
- Erysipelas, 287
- Famine fever, 308
- Farcy, 288
- Fatty degeneration of arteries, 326
- Floater, 359
- Gangrene, 362
- Gangrene of lungs, 312
- Glanders, 288
- Heat stroke, 357
- Hemopericardium, 319
- Hospital fever, 308
- Hydropericardium, 318
- Hydrophobia, 289
- Hydrothorax, 317
- Hypertrophy of heart, 324
- Influenza, 301
- Jail fever, 308
- Jaundice, 329
- Leprosy, 301
- Lockjaw, 292
- Lumpy jaw, 293
- Malaria, 295
- Malignant pustule, 285
- Marsh fever, 295
- Measles, 306
- Mercurialism, 357
- Mitral incompetency, 321
- Mitral insufficiency, 321
- Mitral regurgitation, 321
- Mitral stenosis, 322
- Morphinism, 356
- Mother and unborn child, 360
- Mumps, 307
- Obesity, 358
- Parotitis, 307
- Pericarditis, 318
- Peritonitis, 336
- Pertussis, 308
- Plumbism, 356
- Pneumonia, 314
- Pneumopericardium, 319
- Pulmonary abscess, 314
- Pulmonary hemorrhage, 312
- Pulmonary incompetency, 323
- Pulmonary insufficiency, 323
- Pulmonary stenosis, 323
- Putrid fever, 308
- Pyemia, 311
- Rabies, 289
- Relapsing fever, 290
- Rubeola, 306
- St. Anthony's fire, 287
- Scarlatina, 304
- Scarlet fever, 304
- Scarlet rash, 304
- Senility, 361
- Septicemia, 310
- Ship fever, 308
- Small-pox, 305
- Splenic fever, 285
- Spotted fever, 286
- Swamp fever, 295
- Syphilis, 290
- Tetanus, 292
- Tricuspid incompetency, 322
- Tricuspid regurgitation, 322
- Tuberculosis, 298
- Typhoid fever, 299
- Typhus fever, 308
- Varicella, 309
- Variola, 305
- Whooping cough, 308
- Wool-sorter's disease, 285
- Yellow fever, 296
- [367]
- Treatment of posted cases, 351
- Abdominal post, 351
- Cranial evisceration, 351
- Posted cases, 352
- Thoracic autopsy, 351
- Trocar method, 255
U.
- Ulna bone, 77
- Ulnar artery, location, 240
- Umbilical region, 103
- Ureter, 117
- Urinary bladder, 118
- Urine, removal of, 263
- Uterus, 118
V.
- Vasa-vasorum, 60
- Vascular system, 123
- Veins, structure of, 60, 61
- Venous circulation, 134
- Venous congestion, 204
- Vermiform appendix, 109
- Vertebral column, 71
- Vomer, 75
W.
- Winslow, Foramen of, 121
- Wounds, 193
Y.
Transcriber's Note
Original spelling, hyphenation and punctuation, even where inconsistent,
have been preserved. Minor typographical errors have been corrected
without note.
Figure 10 (p. 60), which was printed upside down in the original, has been restored to proper alignment.
Cover created by Transcriber and placed into the Public Domain.
*** END OF THE PROJECT GUTENBERG EBOOK 49054 ***