There are three parts to this book, each starting with page 1.
Footnotes have been moved to the end of each part.
Variant spelling and inconsistent hyphenation are retained, a few palpable printing errors have been corrected.
To make some tables easier to read on small screens some words have been repeated, for example each occurence of the word “idem” in the key of the plan of the Lariboisière Hospital has been replaced by the words it represents.
The key for the plan of the Lariboisière Hospital was originally handwritten. No changes have been made to this for missing or irregular use of accents or cedillas.
The tables of numbers of nurses near the end of the book were originally printed in landscape, with some sideways printing. The columns and rows have been swapped to make these tables easier to read on small screens.
SUBSIDIARY NOTES
AS TO THE
INTRODUCTION OF FEMALE NURSING
INTO
MILITARY HOSPITALS
IN PEACE AND IN WAR.
Presented by request to the Secretary of State for War.
LONDON:
PRINTED BY HARRISON AND SONS, ST. MARTIN’S LANE, W.C.
1858.
| PAGES | ||
|---|---|---|
| Digest | v–x | |
| Thoughts submitted by Order, concerning— | ||
| I. | Hospital Nurses | 1–9 |
| II. | Nurses in Civil Hospitals | 9–14 |
| III. | Nurses in Her Majesty’s Hospitals | 15–19 |
| Systems of Female Nursing in the War Hospitals of the different Nations engaged in the Crimean War | 19–26 | |
| Note in regard to the Russian Nurses employed in the War Hospitals of the Crimea | 26–28 | |
| Subsidiary Notes as to the Introduction of Female Nursing into Military Hospitals in Peace and in War | 1–63 | |
| Addenda with regard to Female Nursing in a Military Hospital on the Pavilion or Lariboisière Plan | 63–90 | |
| Addenda as to Mixed Nursing, by Nurses and Orderlies, in Military Hospitals, on the Double Pavilion or Vincennes Plan | 91–117 | |
| Additional Hints as to Ventilation, Hospital Floors, and Cautions in Ward-building suggested by the Lariboisière Hospital | 118–127 | |
| Note on Contagion and Infection | 128–132 | |
| [iv]Note on Observations by the Principal Medical Officer of the Army in the East | 132, 133 | |
| Thoughts submitted as to an Eventual Nurses’ Provident Fund | 1–19 | |
| Note as to the Number of Women employed as Nurses in Great Britain | 20, 21 | |
| Note as to Teaching Nursing | 22, 23 | |
| PAGES | ||
|---|---|---|
| THOUGHTS SUBMITTED BY ORDER | 1–28 | |
| CONCERNING | ||
| I. | Hospital Nurses. | |
| II. | Nurses in Civil Hospitals. | |
| III. | Nurses in Her Majesty’s Hospitals. | |
| I. | Hospital Nurses | 1–9 |
| Twenty Observations on how to improve Hospital Nursing. | ||
| II. | Nurses in Civil Hospitals | 9–14 |
| Twenty-three Heads for Regulations as to Nursing in Civil Hospitals. | ||
| III. | Nurses in Her Majesty’s Hospitals | 15–19 |
| Twenty-two suggestions in the event of the introduction of Female Nursing into Military Hospitals. | ||
| Various systems of Female Nursing during the Crimean War in the Military Hospitals | 19–28 | |
| Of the French and Sardinians | 19–22 | |
| Russians | 22, 23, 26–28 | |
| English | 23 | |
| Proposed Duties of Female Nurses in Military General Hospitals | 23, 24 | |
| The Hospital Serjeant, or Ward Master will not be superseded—he will still have too much to do for any one man properly to perform, and part of his duties must be given to another officer | 24–26 | |
| Note in regard to the Russian Nurses employed in the War-Hospitals of the Crimea | 26–28 | |
| SUBSIDIARY NOTES AS TO THE INTRODUCTION OF FEMALE NURSING INTO MILITARY HOSPITALS IN PEACE AND IN WAR | 1–133 | |
| I. | Five Conditions essential to this service | 1–3 |
| II. | Our Nurses were of four kinds | 3 |
| Absolute subordination to the Medical Officer as to Medical Orders essential and practised by us | 4 | |
| III. | 1. Qualified subordination essential of Superintendent-General to Director-General and Principal Medical Officer | 4–6 |
| 2. Also of Matron and Nurses to Principal Medical Officer and Staff-Surgeons | 6, 7 | |
| 3. Female service can only be introduced gradually, and introduction regulated by Director-General | 7–9 | |
| IV. | 1. Shall Roman Catholic Sisters be introduced? | 9, 10 |
| 2. Or Anglican Sisters? | 10 | |
| 3. Power of Police in Civil Hospitals | 11 | |
| Power of Police in Military Hospitals | 12–15 | |
| 4. Pay and Rations of Nurses | 15–20 | |
| On the whole it would seem best, where practicable, to board the Nurses, not to “ration” them, nor to let them “find themselves.” Community of cooking implies economy of nourishment | 17–20 | |
| 5. Washing to be “put out” | 20, 21 | |
| 6. Cleaning their own Rooms | 21–23 | |
| 7. Nurses to keep keys of closet in Wards | 23 | |
| 8. Pay, dress, and duties of Matrons | 24–28 | |
| More properly named Superintendents | 27 | |
| Lady Volunteers had better begin by being Nurses, not Superintendents ex-officio | 28 | |
| 9. Sundry Regulations as to Nurses | 29–31 | |
| 10. Have the Patients’ Diets sent hot, and ready divided, from kitchen | 31 | |
| 11. What Ward duties the Nurses should do themselves | 31 | |
| And why | 32, 33 | |
| Patients should not be made quasi Orderlies | 34 | |
| Visitors in Military Hospitals | 35 | |
| 12. Regulation-Number of Orderlies—depends on the size of wards whether sufficient | 35–41 | |
| What is the regulation-attendance in Naval Hospitals | 37 | |
| What in Civil Hospitals | 38 | |
| Comparative Cost of Nursing in larger and smaller wards | 39–41 | |
| 13. Hospital floors [vii] | 42–51 | |
| Sanitary necessities | 42 | |
| Trial of Hospital floors, oiled and polished with “laque” as in Berlin Hospitals, recommended on sanitary grounds and for ease of cleaning | 43–51 | |
| 14. Ventilation of Wards | 51–52 | |
| 15. Special Wards, whether desirable or not | 53–54 | |
| 16. Opinion as to Superintendent-General paying Nurses’ wages, and as to Governor’s jurisdiction over Nurses | 54–56 | |
| 17. Wages and Pensions of Nurses | 56–60 | |
| Three rules in raising Wages | 56 | |
| Five general principles as to Wages and Pensions | 58 | |
| Six applications of the foregoing principles | 58, 59 | |
| Seven heads for Regulations as to Nurses’ Wages and Pensions | 59, 60 | |
| 18. Proportion of Nurses to Patients | 61, 62 | |
| 19. Precautions in sending Nurses on Foreign Service | 62 | |
| Hospital Laundries | 63 | |
| Addenda, with regard to Female Nursing in a Military Hospital on the Pavilion, or Lariboisière Plan | 63–90 | |
| I. | Four conditions to be considered in adopting the Pavilion Plan | 63 |
| 1. Economy of attendance | 64 | |
| 2. Facility of supervision | 65 | |
| 3. Desirableness of doubling the Pavilion, in a Military Hospital, in order to give to each Nurse but one floor to serve | 65 | |
| 4. Nurse to sleep near her Ward | 66 | |
| Importance of lighting by gas | 67 | |
| II. | 1. One Nurse must serve the whole Pavilion, in a Military Hospital, if single Pavilions be adopted | 68 |
| 2. Nurses’ day in such a Pavilion | 68, 69 | |
| 3. What the responsibility of Nurses is for | ||
| discipline of Ward or Pavilion | 70, 71 | |
| 4. Importance of Lifts | 71 | |
| III. | 1. “Casualty” Cases should be in a completely appointed set of Wards, apart | 72 |
| And why | 73 | |
| 2. Restraint or non-restraint in Violent Cases | 74 | |
| IV. | Simplicity of Construction essential to Discipline[viii] | 75 |
| Polished impervious Walls. | ||
| Covered Exercising Place. | ||
| Reserve Wards | 76 | |
| V. | Nurses’ Meals to be sent them Cooked | 76 |
| VI. | Arrangements for a Pavilion and its Wards | 77–90 |
| 2. Where should Wardmaster sleep? | 77 | |
| 3. And Orderlies sleep? | 77 | |
| 4. And dine? | 78 | |
| 7, 8, Scullery to each Ward, and what to be done in it | 79 | |
| Poultice-making | 79 | |
| 9. Presses in Ward | 80, 81 | |
| 10. Nurses’ Room | 82 | |
| Lavatory, Water-Closet, Sink | 83 | |
| Baths | 84 | |
| 11. Summary of arrangements | 85 | |
| Scullery Appurtenances | 86 | |
| 12. Nurses’ Sleeping Quarters | 86 | |
| Ward for Sick Nurses | 87 | |
| 13. Classification of Patients | 88 | |
| 14. Nurses to be called by their Wards | 88 | |
| 15. Foul Linen | 88 | |
| 16. Washing Bandages | 89 | |
| 17. Splints, &c., where to be kept | 89 | |
| Cotton Lint never to be used | 89 | |
| 18. Classification of Nurses | 90 | |
| Superintendent’s Store Room | 90 | |
| Addenda as to Mixed Nursing by Nurses and Orderlies in Military Hospitals on the Double Pavilion Plan | 91–117 | |
| I. | Orderlies’ Duties | 91–108 |
| Proportion of Nurses, Ward Masters, and Orderlies to Sick | 91–93 | |
| Wine to be always administered by Nurse | 93 | |
| Orderlies—their Duties vary according to appurtenances of Ward | 94 | |
| If Hot and Cold Water are laid on, and there are Lifts, one Orderly’s Service saved to each 30 Sick | 94, 95 | |
| Night-Duty of Orderlies | 95–108 | |
| Scheme of Night-Service for three Orderlies watching by turns | 96, 97 | |
| [ix]Exercise for Orderlies | 97 | |
| Night Refreshment for Orderlies | 98, 99 | |
| Where are the Night Orderlies to sleep? | 100 | |
| Comparative Merits of different Systems of Night Nursing in Home and in Foreign Hospitals | 101–3 | |
| An Assistant Ward Master should go round the Wards at Night | 104 | |
| Extraordinary System of Night-Nursing in the Army at present | 105–8 | |
| II. | Twelve Sundries in organizing a Military Hospital | 108–114 |
| 1. Nurses’ Room | 108 | |
| 2. Medical Officer’s Room | 108 | |
| 3. Water-Closets | 109 | |
| 4. Warm and Cold Water Supply | 109 | |
| 5. Corridors | 109 | |
| 6. Lobby | 110 | |
| 7. Material of Ward Utensils | 110 | |
| 8. Reserve Wards | 111–112 | |
| Necessity of Annual Cleansing of the whole of a Hospital | ||
| 9. Occasional Revision of Rules | 113 | |
| 10. Defect in German Organization of Nursing | 113 | |
| 11. Nurses’ Exercise | 113 | |
| 12. Number of Ward Masters | 114 | |
| III. | Regulations | 114–117 |
| 1. Deprivation of Visitors salutary in certain Wards | 114–16 | |
| 2. Numbering Patients saves time | 117 | |
| 3. Prohibition of Swearing | 117 | |
| Conclusion | 117 | |
| Additional Hints as to Pavilion Hospitals suggested by the Construction of the Lariboisière Hospital at Paris | 118–127 | |
| I. | Ventilation | 118–120 |
| Artificial Ventilation never freshens a Ward | ||
| II. | Oiled Boards versus Parquets | 120–124 |
| Cleaning polished and oiled Boards much less laborious, and freshens the Ward much more than the frottage of Parquets. | ||
| Mode of Cleaning them at Berlin | 122–124 | |
| III. | [x]Ten Cautions in Building Hospital Pavilions | 124–127 |
| Size of Wards. Our own Regimental Hospitals extraordinary for their many holes and corners | 125 | |
| Casualty Wards | 126 | |
| “Contagion” and “Infection” Defined | 128–132 | |
| Idea of “Contagion” invented by Men to excuse themselves for the neglect of all Sanitary arrangements | 128 | |
| In the ordinary sense of the word, no such thing as “Contagion” | 129 | |
| Nor as inevitable “Infection” | 130 | |
| “Infection” and Incapable Management, or Bad Construction, convertible terms | 131 | |
| “Epidemics” do not spread—they develop themselves in Constitutions made ripe for them by Sanitary neglects | 131 | |
| Note on certain “Observations” by Sir John Hall | 132, 133 | |
| Thoughts Submitted as to an Eventual Nurses’ Provident Fund | 1–19 | |
| Actual Wages and Prospects of Nurses | 1–3 | |
| Some further Provision desirable | 4–6 | |
| Of what Nature? | 6–15 | |
| With regard to Kind? | 6–8 | |
| With regard to Persons? | 8 | |
| With regard to Objects? | 9–15 | |
| Material Objects? | 9–12 | |
| Children, in the case of Nurses, a Temptation to Petty Dishonesty and taking Bribes | 11, 12 | |
| Sanitary Objects? | 13 | |
| Moral Objects? | 13–15 | |
| Hospitals not places for Penitents | 14, 15 | |
| Rules to be followed in giving Assistance | 15–17 | |
| Prospects of Eventual Support | 18, 19 | |
| Note as to the Number of Women employed as Nurses in Great Britain | 20, 21 | |
| Tables of Ages, &c. | 21 | |
| Note as to Teaching Nursing—Institution at Madras | 22, 23 | |
PRIVATE AND CONFIDENTIAL.
1. It would appear desirable to consider that definite objects are to be attained; and that the road leading to them is to a large extent to be found out—therefore to consider all plans and rules, for some time to come, as in a great measure tentative and experimental.
2. The main object I conceive to be, to improve hospitals, by improving hospital-nursing; and to do this by improving, or contributing towards the improvement, of the class of hospital-nurses, whether nurses or head-nurses.
3. This I propose doing, not by founding a Religious Order; but by training, systematizing, and morally improving as far as may be permitted, that section of the large class of women supporting themselves by labour, who take to hospital-nursing for a livelihood,—by inducing, in the long run, some such women to contemplate usefulness,[2] and the service of God in the relief of man, as well as maintenance, and by incorporating with both these classes a certain proportion of gentlewomen who may think fit to adopt this occupation without pay, but under the same rules, and on the same strict footing of duty performed under definite superiors. These two latter elements, if efficient (if not, they would be mischievous rather than useless), I consider would elevate and leaven the mass.
4. It may or may not be desirable to incorporate into the work, either temporarily or permanently, members of Religious Orders, whether English or Roman Catholic, or both, who may, with the consent of their Superiors, enter hospitals nursed under the above system, upon the definite understanding of entire obedience to secular authorities in secular matters, and of abstinence from proselytism.
5. Great and undoubted advantages as to character, decorum, order, absence of scandal, protection against calumny, together with, generally speaking, security for some amount of religious fear, love, and self-sacrifice, are found in the system of female Religious Orders.
6. On the other hand, the majority of women in all European countries are, by God’s providence, compelled to work for their bread, and are without vocation for Orders.
In England the channels of female labour are few, narrow, and over-crowded. In London and in all large towns, there are accordingly a large number of women who avowedly live by their shame; a larger number who occupy a hideous border-land, working by day and sinning by night; and a large number, whether larger or smaller than the latter class is a doubtful problem, who preserve their chastity, and struggle through their lives as they [3]can, on precarious work and insufficient wages. Vicious propensities are in many cases the cause, remediless by the efforts of others, of the two first classes: want of work, insufficient wages, the absence of protection and restraint, are the cause in many more.
Perhaps the work most needed now is rather to aim at alleviating the misery, and lessening the opportunities and the temptations to gross sin, of the many; than at promoting the spiritual elevation of the few, always supposing that this latter object is best effected in an Order.
At any rate, to promote the honest employment, the decent maintenance and provision, to protect and to restrain, to elevate in purifying, so far as may be permitted, a number, more or less, of poor and virtuous women, is a definite and large object of useful aim, whether success be granted to it or not.
The Orders remain for the reception of those women who either are or believe themselves drawn to enter them, or who experience their need of them.
7. The care of the sick is the main object of hospitals. The care of their souls is the great province of the clergy of hospitals. The care of their bodies is the duty of the nurses. Possibly this duty might be better fulfilled by religious nurses than by Sisters of any Order; because the careful, skilful, and frequent performance of certain coarse, servile, personal offices is of momentous consequence in many forms of severe illness and severe injury, and prudery, a thing which appears incidental, though not necessarily so, to Female Orders, is adverse to or incompatible with this.
8. Grave and peculiar difficulties attend the incorporation of members of Orders, especially of Roman Catholic Orders, into the work. And, both with reference to the Queen’s hospitals, and still more to the civil hospitals, I [4]humbly submit that much thought, and some consultation with a few impartial and judicious men, should precede the experiment of their introduction. This appears to me one of the most important questions for decision. Should it be decided in favor of their introduction, I trust it may be resolved to do so only tentatively and experimentally.
I confess that, subject to correction or modification from further experience or information, my belief, the result of much anxious thought and actual experience, is, that their introduction is certain to effect far more harm in some ways than it can effect good in others; that a great part of the advantages of the system of Orders is lost when their members are partially incorporated in a secular, and therefore, as they consider, an inferior system; and that their incorporation, especially as regards the Roman Catholic Sisters, will be a constant source of confusion, of weakness, of disunion, and of mischief.
Saint Vincent de Paule well knew mankind, when he imposed, amongst other things, the rule on the Sisters of his Order never to join in any work of charity with the Sisters of any other Order. This rule was mentioned to me on an occasion which gave it weight, by the Superior of the Sisters of Charity of one of the two Sardinian Hospitals on the Heights of Balaklava, in the spring of 1856, and by the Mère Générale at Paris, October 1854, when she was solicited by me, with the assent and sanction, both of the English and of the French Governments, to grant some of her Sisters to us at Scutari.
9. As regards ladies, not members of Orders, peculiar difficulties attend their admission: yet their eventual admixture to a certain extent in the work is an important feature of it. Obedience, discipline, self-control, work understood as work, hospital service as implying [5]masters, civil and medical, and a mistress, what service means, and abnegation of self, are things not always easy to be learnt, understood, and faithfully acted upon, by ladies. Yet they cannot fail in efficiency of service or propriety of conduct—propriety is a large word—without damaging the work, and degrading their element. Their dismissal (like that of Sisters) must always be more troublesome, if not more difficult than that of the other nurses.
It might be better not to invite this element; to let it come if it will learn, understand, and do what has to be learnt, understood, and done: if not, it is better away.
It appears to me, but I may be quite mistaken, that, in the beginning, many such persons will offer themselves, but few persevere; that in time a sufficient number will form an important element of the work; more is not desirable.
It seems to me important that ladies, as such, should have no separate status; but should be merged among the head-nurses, by whatever name these are called. Thus efficiency would be promoted, sundry things would be checked, and the leaven would circulate.
There are many women, daughters and widows of the middle classes, who would become valuable acquisitions to the work, but whose circumstances would compel them to find their maintenance in it. These persons would be far more useful, less troublesome, would blend better and more truly with women of the higher orders, who were in the work, and would influence better and more easily the other nurses, as head-nurses, than as ladies. Whether or not the better judgment of others agrees with mine, my meaning will be understood.
In truth the only lady in a hospital should be the chief of the women, whether called Matron or Superintendent. [6]The efficiency of her office requires that she should rank as a lady and an officer of the hospital. At the same time, I think it important that every Matron and Superintendent, (unless during war-service, when the rough-and-ready life and work required will probably be best undergone by women of a higher class) should be a person of the middle classes, and if she requires and receives a salary, so much the better. She will thus disarm one source of opposition and jealousy, and enough will remain, inseparable from her office.
The quasi-spiritual dignity of Sisters of Mercy is a thing sui generis. But the real and faithful discharge of the duties of the wards of a General Hospital, whether with reference to superiors, companions, or patients, is incompatible with the status, as such, of ladies. The real dignity of a gentlewoman is a very high and unassailable thing, which silently encompasses her from her birth to her grave. Therefore, I can conceive no woman who knows, either from information or from experience, what hospital duties are, not feeling as strongly as I do, that either the assertion or the reception of the status as such of a lady, is against every rule and feeling of common sense, of the propriety of things, and of her own dignity.
10. The question of the mode of Religion is an all-important one, and the choice of a mode bears far more directly upon this work than may, at first sight, appear. To give up the common ground of membership of the National Church is to give up a great source of strength.
St. John’s House, if it steers clear of the rock of prudery, undoubtedly possesses great advantages over a system of hospital nursing by promiscuous instruments. Not because it includes a Sisterhood, a system, in which I, for one, humbly but entirely disbelieve; but because the [7]laborious, servile, anxious, trying drudgery of real hospital work (and to be anything but a nuisance it must ever remain a very humble and very laborious drudgery), requires, like every duty, if it is to be done aright, the fear and love of God. And in practice, apart from theory, no real union can ever be formed between sects. The work now proposed, however, must essentially forbear to avail itself of the bond of union of the National Church.
11. None but women of unblemished character should be suffered to enter the work, and any departure from chastity should be visited with instant final dismission. All applications on behalf of late inmates of penitentiaries, reformatories, of all kinds and descriptions, should be refused. The first offence of dishonesty, and, at the very furthest, the third offence of drunkenness, should ensure irreversible dismissal. No nurse dismissed, from whatever cause, should be suffered to return.
12. It is very important, if possible, to make provision for the disabled age of deserving nurses. It does not seem to me, I speak very diffidently, desirable to concentrate them in one or more large buildings. I believe half the inmates of half the alms-houses, &c., are not on speaking terms with each other. John Bull is of a peculiar idiosyncrasy: nowhere are there such homes as in England, but life in community does not seem congenial here. A pension and the option of ending their days in solitary quiet, or with some friend or relation, would probably be the most comfortable arrangement for nurses.
13. Many women are valuable as nurses, who are yet unfit for promotion to head-nurses. It appears to me that it would be very desirable to have an intermediate recompense: say, after ten years’ good service, to raise nurses’ wages; after a second ten years, to raise them further.
14. There should be an age for the reception and for [8]the retirement both of nurses and head-nurses. I think no head-nurse should be under thirty.
15. Simplicity of rules, placing the nurses, in some respects, absolutely under the Medical man, and, in others, absolutely under the Female Superintendent, is very important; also, at the outset, to have a clear and recorded definition of these respective limits.
16. Economy is very important, with regard to the eventual extension of the work.
17. In the event of the nurses not being trained in Her Majesty’s service, advantage, it seems to me, would attend their beginning in a great established hospital; unless indeed it should be judged best to select and train a staff of nurses first in a smaller and quieter one. Yet much that would be unpleasant in the larger place would probably be beneficial. The restraint, control, contact with the masters, work, and order of things of a great and settled place, would materially help with reference to the nurses.
18. Common sense will assuredly make the fixed resolve; both to fulfil one’s duty, and to keep within it. It is as essential to do the latter as the former, and often more difficult, especially for women; most especially for hospital-nurses.
19. It appears to me most important to be free, once and for ever, from the injurious, untrue, and derogatory appendage of public patronage: what is called support in these days always ends in patronage. This work, truly understood, never has been, never will be, never can be, a popular work; for many reasons, one of which is that the public, of all orders, never can know anything of the real nature of hospital-work. With the best intentions, it will therefore make perpetual and impeding mistakes in “supporting” or patronizing it. Its support and patronage [9]are equally injurious in different ways as regards our masters the medical men, ourselves the nurses, and people who are neither medical men nor nurses.
20. I end as I began. Let nothing be done rashly. Let us not be fettered with many rules at first. Let us take time to see how things work; what is found to answer best; how the work proceeds; how far it pleases God to accept and bless it. Let us be prepared, as I know well we must be, for disappointments of every sort and kind. What can any of us do in anything, what are any of us meant to do in anything, but our duty, leaving the event to God? His Will be done in earth, as it is in Heaven.
1. The isolation of each head-nurse and her nurses appears to me very important. The head-nurse should be within reach and view of her ward both day and night. Associating the nurses in large dormitories tends to corrupt the good, and make the bad worse. Small airy rooms contiguous to the ward are best. The ward should have but one entrance, and the head-nurse’s room should be close to it, so that neither nurse nor patient can leave, nor any one enter the ward, without her knowledge.
2. All the nurses should rank and be paid alike, with progressive increase of wages after each ten years’ good service, or a slow annual rise, which is better.
3. The night-nurses should be on duty 12 hours, with instant dismissal if found asleep; 8 hours should be allowed for sleep, and 4 hours for daily exercise, private occupation, or recreation. If they have no time to themselves for their mending, making, &c., they do it at night, sometimes[10] innocently, sometimes to the injury of the patients. I would not however prohibit occupation at night; as sometimes the ward-duty is slight; and doing something is far better and more awakening than doing nothing. This is one of the matters the head-nurse should constantly look to. I do not fancy, but at present am not positive about, cleaning or scrubbing at night. The night-nurse should have a reversible lamp, or something that without disturbing the patient, gives her light, brighter than the dim fire or gas-light properly maintained in the wards at night. She should have a room to herself.
4. The day-nurses should have eight hours’ sleep, and if it be possible, 4 hours daily for exercise, private occupation or recreation. They may have one room.
5. All provisions, &c., &c., should be as much as possible brought into the wards, or to the ward-doors, by lifts. Nothing should be fetched by the nurses. This would save much time; would enable the nurses to do more work, and yet have more leisure; and above all, would obviate the great demoralization consequent on the nurses, patients, and men-servants congregating in numbers several times daily.
6. The patients should be made as useful as possible, consistently with their capacities, inside the ward; but should be permitted to fetch nothing to it.
7. I strongly incline to have the scrubbing done in each ward, by a nurse assigned for that purpose, and for general attendance when the scrubbing is done. There should be hours for the scrubbing, before and after which it should not be done. This whole matter is one on which I am not positive at present.
8. At present, I incline to something of the following scale. Two wards, single are best, but it might be one double ward, with 40 beds, served by 1 head-nurse and 3[11] nurses. The head-nurse to superintend all things, and to do the dressings not done by the surgeons and dressers, assisted mainly by one nurse, whom she thus instructs in nursing. Another nurse to do the scrubbing, and mainly the cleaning, and when these are over to mind the ward during the remaining hours in turn or in conjunction with the first nurse. The third to be night-nurse. In the morning, before dressing begins, and before the night-nurse goes off duty, all three nurses to clean the ward, make the beds, wash the helpless patients, &c.
9. Hours of morning and evening poulticing and dressing to be fixed.
10. Hours of administration of medicine, always except at night given by head-nurse, to be fixed.
11. Hours of exercise of head-nurse and nurses to be fixed, and arranged with reference to the ward-duties. A fixed occasional holiday given in turn to the nurses is good. An annual longer holiday for them and for the head-nurses is good; a fortnight is, I think, a good limit. The holidays cause inconvenience, no doubt, but on the whole do, I think, far more good than harm. The holidays should be distributed in rotation during a fixed time of year, and comprehended in two or three months, or four at the very outside; and no woman declining her holiday at the proper time should be allowed it at any other.
12. No head-nurse or nurse should be out of the hospital before or after the limit of her daily exercise time, two hours, without written permission of the Matron. The Matron, I think, should put the cause and amount of the extension in writing, and report the same to the Treasurer or Chief Officer, at the next general meeting, whenever it is called, of the Officers of the Hospital. She will find this a great protection against petitions. There is not a doubt that the fewer extraordinary absences, the better.
13. Were it possible to have a small garden (in college gardens much effect and much refreshment is produced by a green sward, a few trees, some shrubs, a fountain, and some seats), in this, at strictly separated hours, the men-patients, the women patients, the head-nurses and nurses, the men-servants, if they choose, which perhaps is not likely, could walk or sit down. This arrangement would little interfere with its enjoyment by the dignitaries and their children, who require it quite as much, and would be found in its results practically and not poetically useful. Hospitals are, and perhaps must be, in or near crowded thoroughfares. Streets are miserable places to walk in during great part of the year. Nurses want and unconsciously crave for fresh air, and often half-an-hour is better than more, given them close to their work—and away from the streets, it would be often a great preservative.
14. I should, however, be very cautious as to introducing music or anything of that sort. Hospitals are not tea-gardens, nor homes, nor meant to be either. Great quiet and some severity of discipline are necessary, and ought to be exacted.
15. I think the head-nurses should wear a regulation dress, and the nurses another; if we adopt the honest word livery, in use in the hospitals, it will perhaps do no harm. Caps, dresses, aprons, should be prescribed: whether or not out-of-door dress should be prescribed is to be considered apart. Each should have three dresses yearly. Better, I think, avoid washing stuffs; they require endless change to look decent. Head-nurses and nurses might wear the same dress, and some difference in the cap would be quite distinction enough.
16. I incline towards giving the head-nurses £50 a-year, one or two rooms (one room with an alcove and curtain would be best), fuel and light. The nurses[13] lodging; the night-nurse a room to herself, the others together; entire board, fuel, light, and good wages to be decided upon.
17. The nurses’ rooms should be supplied with plain comfortable furniture. In the large Hospitals the head-nurse furnishes her own room or rooms, which doubtless promotes her comfort and her care of the furniture, both desirable things; yet the tendency of many to accumulate decorations, which take time to clean, &c., is a drawback. I should be inclined, as an experiment, to try the furnishing plan, or at least to have some scale as to furniture allowed. A bed, arm-chair, and sofa; a chest of drawers, wash-hand table or shelf; book-case or shelves; a little table, and a larger one, a couple of chairs, a footstool, and a cupboard with broad shelves, are the utmost that can be required.
18. A difficult and important point to settle is the amount of liberty allowed as to receiving visits. It is desirable on all accounts to make head-nurses and nurses feel comfortable, and, as it were, at home: it is also better they should not be unnecessarily out; also London distances are great, and even omnibus-fare is a consideration; also it is important to remember that these women are apt to feel and say: “We are not in a nunnery,” nor should they be. Still upon the whole, considering the nuisance of ordinary visitors, and the greater nuisance of extraordinary (e. g., visitors to some head-nurses, kind friends come to see how we are getting on, &c., &c., &c.), I think if it were possible to make the rule that no visitors are allowed, it would be a great gain. I am not sure, at present, whether it is possible or not—still less whether it is possible to keep such a rule, if made. But, at all events, nurses and head-nurses should only be permitted to receive visitors on certain days and hours of the[14] week; and those hours and days should be strictly kept to. In Military Hospitals a still more rigid rule will be necessary.
19. No discharged patients, however previously well-conducted, should be allowed to visit the wards.
20. Apart from raising the wages of good nurses after every ten years’ service, I think it would well answer to establish a graduated scale of pensions, for both head-nurses and nurses; beginning with a small pension after ten years’ good service, increasing every five years afterwards. Many women are quickly worn out in this life; and it is equally undesirable to turn faithful worn-out servants adrift without any provision, or to retain them in duties for which they are become unfit. It is a question whether there should not be a compulsory stoppage from wages, in order to entitle the nurses to pension under conditions.
21. Have no occasional wards, or wards for accidental and peculiar patients.
22. Every ward, or set of wards, should be under a head-nurse. Discipline is always defective under other arrangements.
23. This turns greatly upon a previous question. Every endeavour should be used to bring the women under the influence of religion, God’s instrument for saving, strengthening, and comforting souls. So far as this work depends on rule, system, and superintendence, great things may be done at any rate—so far as moral influence is concerned, it can only be hoped for in the channels appointed by Him who turneth all hearts whithersoever He will.
1. If their introduction is eventually commanded by the Queen’s Government, it will be advisable to consider that their service admits of two distinct kinds.
2. “Their chief duties” may be “taking charge of the linen and superintending the issue of extras.”
They will thus contribute materially to the comfort and well-being of the sick; the real difficulties which undoubtedly beset the introduction of women into ward service will be avoided; and, an important consideration, not lightly to be discarded, their exclusion from the ward service will materially diminish the opposition of adverse masters, some of whom are also unscrupulous masters.
3. On the other hand, I suppose, the experience of every woman, admitted to ward service in hospitals where women were not before, is that many lives are actually saved by such admission, which would otherwise, humanly speaking, be lost. In time of war some ciphers may be safely added to the many. Any other great emergency, I suppose, but do not speak from experience, would give the same result.
That the experience of many surgeons is identical, their conduct has proved; no other testimony, under present circumstances, can rationally be expected from them.
4. It is often right to begin with the smaller and less-opposed good, and to introduce gradually, and, as it pleases God, the remainder. It may be our duty to do this, as to this matter.
5. Practically, it is of little avail to superintend, ever so carefully, the issue of extras to the sick, unless there is permission and opportunity to pour the nourishment, perhaps in continual drops, down the throat of reluctant agony, or delirium, or stupor. And it is of little avail to have this permission, unless there be also that of raising[16] the decent covering under which cholera, erysipelas, or the oppression of long recumbency, or the discharging wound, or the recent operation lie, and seeing to matters within. It is a further question, whether the painful cleansing of painful wounds, and the important minor dressings, as poulticing, which things, generally speaking, never have been done, and never will be done by surgeons, are best left to nurses, orderlies, or the patients themselves.
6. At the same time, nothing is more pernicious than to under-rate the objections of opponents. There is no doubt that the admission of women to ward service is beset with difficulties. These Naval and Military Hospitals are, and must ever be, peculiar Hospitals, essentially different in important details from the Civil Hospitals.
Sisters of Mercy, as regards the ward service, are decorous and kind, and sometimes inefficient and prudish. Nurses are careful, efficient, often decorous, and always kind, sometimes drunken, sometimes unchaste.
Misconduct of women is far more pernicious in a Military or Naval Hospital than in any other, as regards the result of things—the crime is, of course, equally crime everywhere.
7. It appears to me desirable to simplify and condense, as much as possible, female service in these Hospitals. Let there be as few women, and these few as efficient and as respectable as can be. Let all that can really be done by men be so done.
8. Head-nurses are alone, I think, desirable to be employed; I mean persons of the character, responsibility, and efficiency, of head-nurses in other Hospitals.
9. The patients should be distinctly classed, though, of course, this is not the Female Superintendent’s business.
There are many pros and cons to the formation of convalescent wards.
It is a question whether convalescent or chronic patients require female nurses at all.
Of such chronic cases, probably 100 would be efficiently served by one nurse, having orderlies under her. Of acute cases, probably, one nurse should take charge of not more than fifty, possibly not more than forty.
10. The nurses should be strong, active women, of not less than thirty, nor, I think, more than sixty years of age, of unblemished character, and should be irreversibly dismissed for the first offence of unchastity, drunkenness, or dishonesty, or proved impropriety of any kind.
11. Their wages, I think, the same as those of head-nurses in Civil Hospitals—certainly, not more.
12. Their pension on the same graduated scale.
13. Their rules should be simple, very definite, should leave them at the absolute disposal of the surgeon as to ward matters, and at the absolute disposal of the Female Superintendent in all other matters. Their dress should be uniform.
14. Their duties should be strictly defined, and be consistent with the Code of Army Hospital Regulations, the revision of which has been announced.
15. Give them plenty to do, and great responsibility—two effectual means of steadying women.
16. The nurse’s lodging in view of her ward renders her far more efficient; but this requires some special arrangement. It would not do to have the chance of the nurse’s being suddenly taken ill, with only patients and orderlies within immediate reach. Were the nurses’ rooms so arranged that two or more were on one floor (as is the case in all Hospitals), and so arranged as to be entirely separate, and yet, when so desired, easily accessible to each[18] other, which might easily be contrived, this would probably answer all purposes.
17. Their food should be sent them cooked with some slight variety. With the plainest intentions nature often revolts from the perpetual joint of excellent meat in Hospital air and life. The occasional “potage,” fish, &c., of other systems, are in fact, a refreshing and palatable change. If, however, avoiding names that shock and frighten, some slight change of diet could be contrived, the effect would be good. This is practical and not at all romantic, though it may look the latter.
18. Could the honest opinions be had of a few good Military and Surgical Authorities before beginning, it would be good.
19. The Female Superintendent-General’s own powers and responsibilities must be absolutely fixed, and so as not to clash with those of the Officer (should such an Officer be appointed, as has been elsewhere recommended), who shall superintend the Hospital attendants.
20. Confidential reports must be so modified, as far as women are concerned, that the humble boon granted to pickpockets, of being informed of accusations laid to their charge, must be extended to Her Majesty’s nurses.
21. In framing the system and the Superintendent’s own office, let it be attempted to secure the permanent efficient working, please God, in ordinary hands. To aim at the best conceivable may lead to failure. Genius works with ordinary materials, but never constructs an edifice which it alone can inhabit.
22. “In quietness and in confidence shall be your strength.” Quietness has been from the beginning of its publicity the one thing wanting in this work. I know the fuss, which from its beginning surrounded it, was abhorrent to us and was the act of others: but the work, which is all[19] we care for, has throughout suffered from it. It is equally injurious and impeding as regards surgeons, nurses, and people, who are neither. External help in this coarse, repulsive, servile, noble work, for it is all these things, is truly the reed which pierced the hand that leant upon it. One hospital, naval, military, or civil, nursed well, and gradually training a few nurses, would do more good to the cause than an endless amount of meetings, testimonials, pounds, and speeches, to say nothing of newspaper puffings, which to-morrow might turn into revilings. This never will, never can be a popular work. Few good ones are, for few are without the stern fructifying element of moral restraint and influence; and though the streams of this are many, its source is one. Hearts are not touched without Religion. Religion was not given us from above in impressions and generalities, but in habits of thought and action, in love of God and of mankind, carried into action.
A very short comparison will here be made between the methods of Female Nursing in the Military Hospitals of
as exemplified in the last War.
To do this, a sketch must be partly repeated, which has been already given, of the organic difference between the Hospital Service of each nation.
The essential characteristic of the French is, the importance given in the field to the Divisional Hospital Service over the Regimental.
The Regimental Medical Service treats only those ephemeral cases which are to be exempted from duty for a day or two. Cases of wounds or disease likely to last for a term of weeks are sent to the Divisional Ambulance[20] in the field; those, where disease may possibly last for months, to the General Hospitals at the base of operations.
The Medical Service of the Sardinians closely resembles the above in its formation. In the late War, their General Ambulances were at Balaklava; their General Hospitals at Jeni Koi on the Bosphorus. They had no Divisional or Regimental Hospitals.
In our Army, as is well known, the Regiment establishes its Regimental Hospital wherever it goes. Theoretically, it is exclusively a Regimental system of Hospitals; however much, practically, it breaks down.
The Russian system can scarcely bear a comparison with ours; because their Regiments are Divisions. They had a regular system of transporting the sick and wounded upon the North side of Sebastopol, then upon Mackenzie’s Heights, then upon Bakschi-Serai, and lastly upon Simpheropol.
The adaptation of Female Nursing to the different systems in the
has now to be noticed.
The Sardinians had Sisters of Charity, both in the General Ambulances in the Crimea, and in the General Hospitals on the Bosphorus.
The principal duties of these admirable women appear to have been the care of the linen and small stores, and the cooking, much of which they did with their own hands, for sick officers and men. These duties were admirably performed. They appeared, besides, to have a certain charge in the wards, the power of giving “douceurs,” the administration of extras, the seeing to the cleanliness of[21] beds and patients, and something more precise with regard to sick Officers; but their duties seemed to be somewhat undefined in their relation to the Infirmiers. Whether the Sœur or the Infirmier Major were in charge, to see the duties about the patient properly executed, was rather a problem.
This was still more the case in the French Hospitals, where the “Sœur” in the wards appeared more of a “consolatrice” and an administratrix of extras: although, out of the wards, her admirable housekeeping, both in the kitchen and the linen-store, was predominant.
The French “Sœurs” were not admitted to the Divisional Ambulances in the front: it was whispered, because of the corruption of the French Intendance, upon whom they tacitly exercised a very inconvenient “surveillance.” They served in all the General Hospitals at Constantinople; and to their admirable services, M. Baudens, Inspecteur-Général en Crimée, has rendered an “éclatant témoignage” in his “Mission Médicale en Orient,” published in the numbers of the “Revue des Deux Mondes,” of February 15, April 1, and June 1, 1857.
In these French Hospitals of Constantinople, the “Sœurs” appeared to do all the cooking for the sick Officers and that of the extras for the men.
I do not think that, in either French or Sardinian Hospitals, the care of bed-sores and such like, which can only be done by women, was sufficiently given to the “Sœurs.”
I have heard complaints made of this kind both by Officers and men; and “Sœurs,” both French and Sardinian, have been to me to look at the way in which we treated bed-sores, and to borrow air-pillows and water-beds.
There is such a difference however in different Hospitals,[22] in time of war and of peace, &c., that I would not be understood to mean that any of these remarks apply absolutely or generally, but only to Hospitals I have seen.
It may be as well to mention that, talking of “French” and “Sardinian” Sisters, they all come from one “Maison Mère,” that of the “Filles de la Charité de S. Vincent de Paule,” at Paris. There is a “Maison Succursale,” at Turin. But all are of the same Order, and under the same head.
Let me mention Sœur Cordero, the excellent Superioress of all the Sisters employed in the Sardinian Hospitals of the war, with the warmest affection and respect. She was a woman of high rank, of the most captivating manners, but of the utmost simplicity of character, and of unfailing devotion to right and to God.
It remains to mention the Russian system, which, as regards the organization of the duties of the “Sisters,” appeared to me by far the best I have known. I am at a loss to conceive what is meant by the following sentence in the Report by two of our Army Medical Officers on the “Russian Medical Department,” presented to the House of Commons. Speaking of the Sisters of Mercy, who are generally widows of officers, it is said “their chief duties appeared to be in taking charge of the linen and superintending the issue of extras.” This is founded on error of observation—as the Russian system seems to be the only perfectly organized system of female attendance in Military Hospitals, which was developed in the Crimean War. In it, the Sister has charge of all that relates to the bed-side of the patient; she receives the orders from the Medical Officer, attends him in his rounds; he confers with her afterwards; she even reports the “felchers” or dressers, as also the orderlies, as far as regards their [23]discharge of duties at the bed-side of the patient. The orderlies are, of course, under the control of a Non-commissioned Officer, in all that pertains to discipline, clothing, meals, &c. The “felchers” are under a superior “felcher,” and under the Medical Officers.
There are female nurses, wives and widows of soldiers, under the “Sisters,” who are generally, as has been stated, widows of Officers.
This appears the nearest approach to good organization I have met with.
But again I say there may be much difference among the Russian Military Hospitals. I would not be considered as laying down an absolute experience.
It has been said elsewhere what was the system or no system pursued in the English Military Hospitals, as to Female Nursing. It was a new thing, and no General Order or Warrant was ever issued as to the duties of the nurses. Many duties clearly devolved upon the Female Superintendent-General, as she was afterwards called in “General Orders,” which never should devolve upon her again.
But it may be now clearly enunciated what the duties of Female Nurses should be, and many reasons will subsequently be given why there never will be discipline in Military Hospitals till they are as follow:
Women only of the character, efficiency, and responsibility of Head Nurses in other Hospitals should be admitted into Military ones. They should have charge and be responsible for all that pertains to the bed-side of the patient; for his cleanliness, and that of his linen, bed, and utensils; for all the minor dressings, not performed by Surgeons or Dressers; for the administration of medicines, and of the meals; for the obedience of the patient and orderlies to the orders of the Medical Officer. They [24]should receive the orders of the latter, and always attend him in his visits.
Till the above is done by women, the same want of discipline, now to be observed in Military Hospitals, and often already noticed, will continue,—such is my firm belief, the result of much experience.
There will be abundance left for the Ward Master or Serjeant to do in taking Military charge of the Hospital and its inhabitants, in being Office Clerk, &c., i. e., keeping the Admission books, making States, Returns, Accounts, and other documents, without his being Head-Nurse, without his superintending the Orderlies at the bed-side, his administering medicines, &c., which can only be satisfactorily done by a woman. And, when done by her, there will still be ample work for two men, where one does now the work of three.
The first should do the Military part, the second should compound, take charge of Medical and Surgical stores, of Returns and Accounts connected with these; and, where there is no Purveyor, of Purveyor’s and Barrack stores, provisions, cooking, washing, diets, and extras, including Returns and Accounts connected with these.
As it is, there is one Hospital Serjeant, who is Ward-Master, Serjeant, Steward, Clerk, Dispenser, Purveyor’s Clerk, and Head-Nurse—a kind of “Maître Jacques,” as in Molière’s “Avare.”
One man cannot do all these things.
A Female should be the Head-Nurse—a Serjeant should be the Serjeant and Clerk—a Ward-Master the Steward, Dispenser, Ward-Master, and Purveyor’s Clerk.
And here I must deplore the confusion unavoidable in these definitions of proposed duties, while we have no separate system for Regimental and General Hospitals.
What Dr. Menzies declared, in his evidence as to the [25]General Hospitals at Scutari, is strictly true, and one great cause of our failure at Scutari:—“I have followed the general rules for Regimental Hospitals, so far as I could.”
While Regimental Hospitals are what they are, females never can be admitted there. On the other hand, if General Hospitals be established, one happy consequence will be that the cooking and washing will be taken out of the hands of the Hospital Serjeant, and regularly organized, it is hoped under a Captain-Superintendent of Orderlies. All Purveyor’s and Barrack stores, that is, Hospital stores and furniture will, it is hoped, fall under the charge of a Steward; Medical and Surgical stores under that of an Apothecary.
It will only remain to place a female Head-Nurse in charge of all that concerns the bed-side of a patient, and the duties of the Orderlies about the bed-side, and a Ward-Master in charge of everything else belonging to the Orderlies and Patients.
But, if it should be determined to retain everywhere the old Regimental system, it is only just to add this very strong testimony and appeal in favour of the old Hospital Sergeant, who indeed deserves it:—
“I may take this opportunity of stating my conviction that, from the very arduous, constant, and responsible duties of the Hospital Sergeant, and his influence for good or ill among the non-commissioned officers and men of the regiment, it is particularly required for the good of the service that he should be put at least on the same footing in rank and pay as a first-class staff sergeant. He ought to pass an examination by a Board of Medical Officers as to his fitness for compounding medicines on the same footing as a druggist in England. My Hospital Sergeant, who has been eight years a sergeant, three of which as Hospital Sergeant, receives at present 1s. 10d. pay per diem, and an allowance of 4d. per diem as Hospital Orderly; at the same [26]time that there are sergeants in the ranks of the regiment four years junior to him as a non-commissioned officer who are receiving 2s. 10d. pay per diem.
“My experience leads me to consider that the regimental bandsmen are not, as a body, likely to be sufficiently strong or able men for the duty of carrying the wounded to be consigned to them.
“(Signed) Thomas Longmore,
“Surgeon 19th Regiment.”
The Russian nurses, in the opinion of their Master, the famous surgeon, Pirogoff, did other things besides what the Army Medical Director-General told the House of Commons they did. But it is to be observed—
In the first place, that much allowance is to be made for the confusion incident to Scotch and Russian surgeons talking French together, and going over many subjects in a very short time.
And in the second, that very likely some extra confusion arose in the minds of our Army Medical Officers from the fact of two entirely different sets of women having served in the Russian War Hospitals, viz.:
(1.) The Sisters of the Elevation of the Cross.
(2.) The “Frauen des Barmherzigen Wittwen Instituts,” (mentioned in a very cold manner in pages 4, 26, and implicitly, 27, of Professor Pirogoff’s pamphlet, “Die Gemeinschaft der Schwestern zur Kreuz-erhöhung. Berlin: 1856”); who are those spoken of at pp. 22, 23, above.
The Widows were so instituted, about forty years or more ago, by Mary of Wirtemberg, during so many years the venerated Empress-Mother. It is quite possible that in the war-pressure their services proved rather nondescript, they being neither sisters nor nurses, strictly speaking; or perhaps the sole reason why Professor Pirogoff has not one good word for them is, that they were not under his orders.
The Sisters of the Elevation of the Cross were a body of secular women, with a few Sisters of Mercy, formed by the Grand Duchess Helena, and placed by her under the orders of the famous civilian Surgeon Pirogoff, to whom the supreme surgical command in Sevastopol was virtually given. Several things are incidentally mentioned concerning them in his pamphlet, quite inconsistent with the constitution of an ordinary religious order.
One or two things in the pamphlet are incongruous enough to English ideas:—the narrative given, however simply and succinctly, of the performances of the sisters by name, the publication of the Professor’s evident disagreement with the first “Oberin,” or Superior, who served ten months, (the second, whom he so highly praises, had only served two when he wrote); the improvement, by which the Sisters’ concerns were “sat upon” by the Comité of Oberin, Chaplain, Doctor, and elder Sisters, &c., &c.
But the division of Professor Pirogoff’s war-nurses into three categories is a pregnant hint for future service, please God we yield it. These three categories consisted of (1) the “Verband-Schwestern,” or those who assisted the Surgeon in the dressings, and the “Feld-scherer” (Dresser) in preparing them. (2) The “Apothekerinnen,” or those who were in charge of all medical appliances for immediate use, and who superintended the “Feld-scherer” (Dresser) in the administration of medicines. (3) The [28]“Wirthinnen,” who looked after the diets, clean linen, &c., of the patients, and the order of the hospital. Each “category” was responsible for carrying out the orders of the medical officers. To every Hospital-Baracke (hut) was attached one sister of each of the above descriptions.
In ordinary service the less nurses know of each other’s wards the better—in war service it is essential that as few women should serve as many sick as possible; and it is impossible to attempt assigning to each nurse the entire supervision of a ward. I think the categories, modified, of course, and adapted to the Queen’s service, might be most useful.
Another point usefully proved by Professor Pirogoff’s pamphlet is the extreme importance, if it be possible, of placing the nurses clearly under the orders of the Principal Medical Officer, though a further point is, if possible, to be secured, viz., that of the Principal Medical Officer being favourable to their service. As women they should be entirely under the control of their female superior, yet the Principal Medical Officer should have a certain clear amount of power in ordering that Superior as to their employment at particular stations and on particular services.
The Transport Abtheilung of the Russian sisters seems to have been an admirable, though very unpretending service. We might take a useful hint from it. Three Sisters accompanied the more numerous[1] convoys of Sick Transport from Simpheropol to Perekop, and provided the sick with tea, sugar, clean linen, medical and surgical appliances, &c., on the way.
[1] According to Professor Pirogoff sick were almost daily sent from Simpheropol to Perekop. They could not, therefore, be always accompanied by Sisters.
It is, perhaps, advisable first to speak of some of those difficulties met with in the War Hospitals of the East, in order that such may be prevented for others who may in future be Superintendents-General of Nurses in Military Hospitals whether in peace or in war.
No one ought to undertake a matter of duty of this kind without first obtaining the consent of the War Office to five conditions.
1. That every month, each of her sub-Superintendents shall furnish her with an abstract of the requisitions made by her on the Purveyor, whether for Nurses’ consumption, or for that of Patients, and that she furnish the War Office with an abstract of these. It is then the part of the Purveyor to disprove her accounts, instead of its being, as before, her part to disprove his.
2. That it be made a point of honour, not of grace, with the War Department, to submit to her any Report, confidential[2] or otherwise, made concerning the Female Nursing Staff; a condition, without which it would be impossible to have respectable women in the Military Service.
3. That the powers of the Superintendent-General shall be [2]strictly defined, and put in “General Orders” in the first place, and not in the last, in order that there may not be the useless and endless correspondence which there was in the first Superintendent-General’s case (and for what?).
4. That the Superintendent-General have the power of communicating directly with the War Department; and that her Money-Accounts be sent in by her directly to that Department.
5. That it be made a point of honour that the Medical Officers communicate to the Superintendent-General, or Local Superintendent, any complaint they may have against the Nurses for disobedience.
In March 1856 the following appeared in “General Orders.” Had it but been seventeen months earlier how much it might have saved![3] The definition of the Superintendent-General’s powers and duties, therein contained, is all that is wanted to prevent irregularities disastrous to the Service.
General Orders.
March 1856.
“It is notified, by order of the Secretary of State for War, that Miss Nightingale is recognized by Her Majesty’s Government as the General Superintendent of the Female Nursing Establishment of the Military Hospitals of the Army. No lady, sister, or nurse is to be transmitted from one Hospital to another, or into any Hospital, without previous consultation with her. Her instructions, however, require her to have the approval of the Principal Medical Officer, in her exercise of the responsibility thus vested in her.
“The Principal Medical Officer will communicate with Miss Nightingale upon all subjects connected with the Female Nursing Establishment, and will give his directions through that lady.”
1. Our Nurses were of four sorts.
The Nuns were received not as Nuns, but as Nurses.
Their (so called) training told sometimes against us; sometimes for us. The same with the “Sisters” (Anglican).
The Ladies were useful, exactly in proportion as they approached the professional, and not the dilettante, mode of thought.
A larger proportion of paid Nurses than of Ladies did well, and this under circumstances of peculiar temptation. Paid Nurses are always the most useful.
2. There should always be a proportion of Nurses in Army Hospitals
The proportion of Roman Catholic “Sœurs,” in French Military Hospitals, is as small as this would be; they undertake even less duty than this: in Military Hospitals they do much less than in Civil Hospitals.
Women in Military Hospitals should all be contracted servants, whether Nuns, Ladies, or professional Nurses.
There should be a retiring pension to each woman.
3. Miss Nightingale took service on the ground of being under the Principal Medical Officer, and, consequently, of not [4]interfering with him.
There was no imperium in imperio in her case.
This exists in the case of the French “Sœurs de Charité,” and existed in individual instances among the “Sisters” under Miss Nightingale; i. e., they gave articles of diet, &c., as from Sisters, not in obedience to Medical orders. This was immediately put a stop to by her. That the Medical Officer is sole master of diets, is an axiom of medicine, and of common sense.
This involved our only answering the Extra Diet Rolls in our kitchens; not originating either in quantity or quality.
Afterwards, although frequent were the insinuations that we transgressed the above maxim, no evidence of the fact was ever obtained, except the following, which is given verbatim and literatim, as “put into Court” by a First Class Staff-Surgeon, in charge of one of the divisions of the Barrack Hospital, Scutari. He alleged “that the Nurses were in the habit of giving diets without leave;” and when pressed for the facts, produced the annexed statement in “W. J. Northcott’s” handwriting.
“2447. Pte. John M‘Cormick, L. T. Corps, age twenty, 11 Company, admitted into 6 Ward, F. Corridor. Admitted with Febris C. C., April 30th, 1856. On or about the 10th of May I was confined in the Garrison Cells, Scutari, for allowing food and drink to be brought to this Patient, by one of Miss Nightingale’s Nurses; and at the time it was brought I were on duty at the Victoria Barracks, Scutari, three-quarters of a mile from the Hospital, and never saw the Nurse, food, or drink that was administerd to the above-named Patient, and I never saw the docter that ordered me to be confind. I was confind by order of 1st Class Staff-Surgeon Prendergast. About two and a half hours after I were aquanted with the case.
“(Signed) 173. W. J. Northcott,
“A.W.M., M S.C.”
1. In defining the office and duties of the Superintendent-General of Nurses, her direct communication with, and qualified subordination to, the Director-General of the Army Medical Department, and, abroad and in war, with and to the Principal Medical Officer of the district, or equivalent, must be very exactly defined. If the formation and government of a body of[5] women to serve in the Hospitals of the Army Medical Department, and in these alone, is contemplated, the less the Director-General and the Superintendent-General have to do with each other, in matters of detail, the better, and the less chance of collision. For very weighty moral and practical reasons, the sole government of the women must belong to the Superintendent-General, and to the Matrons, whom she delegates, and who are themselves responsible and amenable to her. But it will never work to introduce female service into the Army Hospitals, and to leave the Director-General of the Army Medical Department, which, like everything else in the Army, is and must be a hierarchy, no other power in connection with it, than to write and encourage confidential reports against it. There ought to be a definition of the Superintendent-General’s position as regards him, and also, as regards the Principal Medical Officer of the district, abroad and in war. It is useless, and would be dangerous to evade this; it ought to be deliberately settled, and distinctly stated. In the “General Orders” of March 1856, the Superintendent-General’s complete power over the women, and qualified subordination to the Principal Medical Officer, are well and definitively expressed.
It is impossible to appoint the work of the Nurses without the concurrence of the Director-General. It does not do to put a woman into a great ward, or several smaller wards, of men, with several orderlies, without clearly defining her position there. To put her under the orderlies would be to make her being there at all much worse than useless; but she cannot have assigned to her the responsibility of the ward or wards, and consequently, authority over both orderlies and patients, herself being responsible to the Surgeon and Matron, without the concurrence of the Chief of the Army Medical Department.
Nor, without such concurrence, can the duties of the Nurses be assigned. At this moment there are extant two sets of Regulations—the old Army Hospital Regulations, and those of 1855 made for the late Medical Staff Corps. In these Regulations, both the former and the latter, every duty a Nurse can discharge is assigned to different men. The responsibility of the ward, the administration of diets and medicines, the application of poultices, fomentations, leeches, [6]enemas, and minor dressings, are all in so many words assigned as the duties of Assistant-Surgeons, of Hospital-Serjeants, and Orderlies; and of Assistant-Surgeons, of Ward-Masters and Orderlies of the Medical Staff Corps. The Regulations in general are being revised;—so much the better. But the new body of Orderlies, announced in the “Gazette” as the Hospital Corps, will, of course, receive rules from the Director-General; and if these things are not settled with him, there will be contradictory rules in operation, which will most materially thwart the working of the Female Service.
We have ourselves experienced this, as to the administration of medicines, which one Principal Medical Officer took away from the Nurses, saying that it was the duty of the Assistant-Surgeons, in which he was borne out by an existing Regulation. And it would really seem as if this were the intention of the said Regulation, for it is there laid down that the medicines are to be administered twice-a-day, as if this were a property of medicine.
The existence of these Regulations proved also a great stumbling-block in the Castle Hospital, after the war-pressure was over.
Unless the Director-General, and in war and abroad, the Principal Medical Officer, are brought into regular communication with the Superintendent-General of Nurses, by the Rules, they will, at every inspection of Hospitals, revert to the procedure of giving orders and making alterations, which in fact amount to reprimands on the Superintendent-General, and on her Matrons, through the medium of some Clerk or Orderly. There should be, therefore, a distinct channel of communication laid down between the Director-General, and in war and abroad, the Principal Medical Officer and the Superintendent-General of Nurses.
2. Also, and in the same way, there should be distinct rules for direct communication between the Principal Medical Officer of each Hospital, and the Matron, and between the Staff (or equivalent) Surgeons of the Hospital, and the Matron; if not also between these latter and the Nurses.
The constitution of a General Hospital is about to be organized in England. In the large War Hospitals there was the Principal Medical Officer, a Staff-Surgeon in charge o[7]f each Division, then the Assistant-Surgeon, who answered to what, as is now proposed, is called the Prescribing Medical Officer of the Wards. As regards the Matrons and Nurses, it must not be proposed to ignore all but these Prescribing Medical Officers. Certainly, it would never do to give the Superior Surgeons of the Hospital no say as to the nursing. In 999 cases out of 1,000, the Superior and older Surgeon is the one who understands and cares much the most about the men, and who, therefore, in the long run, would more appreciate and be fairer to Matrons and Nurses who did their duty by them. The Superior and older Surgeons too, in general, have far more correct ideas of the importance of discipline in a ward, and of the ways of maintaining it, than the Assistant-Surgeons. Moreover, as far as one can judge on a mysterious subject, generally speaking, the older and Superior Surgeon is the honester man. He must be brought into direct communication with the Matron; this will effect good, and prevent mischief. So also let the Staff-Surgeon of the Division, or equivalent, be placed in direct communication with the Nurses of the wards of his Division; this will effect good and prevent mischief. If the Nurse is to trust to receiving the orders of the Staff-Surgeon, through the medium of the Assistant-Surgeon, she will often find herself in a false position.
3. Now, as to the introduction of Nurses into all General Hospitals—this gets rid of many difficulties, but at a fearful cost.
For years to come, the difficulty will be not to extend the work, but to serve such Hospitals as must be undertaken, with respectable and efficient women. The material has, in a great degree, to be created; abundance of applications will be received—the prospect of a pension alone will do that—but the real choice will be very limited. In these Military Hospitals each Nurse must be a Head Nurse, and a trustworthy woman. Many a woman who will make a respectable and efficient Assistant-Nurse under the eye of a vigilant Head-Nurse, will not do at all when put in a military ward or wards, herself the only woman, and Head-Nurse over the Orderlies. As a body, the mass of Assistant-Nurses are too low in moral principle, and too flighty in manner, to make any use of here. Supposing all the Head-Nurses of the great Civil Hospitals[5] offered themselves, [8]there are perhaps not many who could be recommended for a Military Hospital. Some, who are very highly to be thought of, would never bear transplanting into the res dura et servitii novitas of the Army Hospitals. The class from which the Head-Nurses are mainly drawn, tradesmen’s and servants’ widows, &c., will volunteer in numbers, but, in the majority of cases, intending only to lead the idle life of many a London Head-Nurse—“mental, not manual labour”—“Superintendence”—i. e., standing by while the Orderlies do her work and their own. The material has to be created. The rarest powers can do nothing effective in this, in 3, 6, or 12 months. To lay a solid foundation will take the patient, anxious labour of years. To begin with one Hospital would have great advantages. Netley, if it is proceeded with, might be the one, though, in most respects, a Hospital in an ordinary vulgar seaport would be far preferable. Then let the work gradually be extended. It is much more to be feared that the line will be taken of forcing prematurely than of opposing its extension. If it is attempted to occupy all the General Hospitals at once, how is the gratuitous repetition to be avoided of the inevitable misfortune of Scutari, viz., that of beginning on a large scale, with a number of strangers? It certainly should be left to the Director-General to regulate the introduction of Nurses into the General Hospitals—and there is far more reason to fear that he, if unfavourable to the change, will hurry, than obstruct such introduction; indeed it might be better to settle that matter[9] beforehand with the Secretary of State, letting the Director-General be apprised of it, viz., that time is required to effect the gradual introduction of the Female Service with which the Superintendent-General has been charged.
To sum up. A rule must be introduced by which the Director-General is brought into communication with the Superintendent-General, and her qualified subordination to him distinctly expressed. Let the Principal Medical Officer in war also communicate directly with the Superintendent-General or the person performing her functions in the War-Hospitals, and her qualified subordination to him be distinctly expressed. The same with each Principal Medical Officer of a Hospital, and the Matron of that Hospital. No alteration in these Regulations can, of course, be made without the consent of the Secretary of State. In case the Director-General and Superintendent-General finally differ as to any new arrangements, the matter should be referred to the Secretary of State.
The Superintendent-General should issue special regulations for nurses, after conference with the Director-General, and under the sanction of the Secretary of State; also, local regulations for the Matrons with the consent of the Principal Medical Officer and sanction of the Governor of any General Hospital.
If the Matron differ with the Principal Medical Officer, the decision should rest with the Governor of the Hospital.
As to some miscellaneous considerations, of no small importance—
1. It is necessary for a Superintendent-General to have counted the cost, and to be prepared or not prepared to include Roman Catholic Sisters among the Nurses. This will deprive her of some valuable women; of one (speaking for the present time,) who is invaluable; of many decorous, not very useful women. The question is perhaps settled by the fact, that where you have the Roman Catholic Sister, you cannot be secure from the Roman Catholic Direction, with all its many strings, and machinery of opposition. Abroad the cause of the Roman Catholic Church is often the cause of religion; and the Romish Priest serves both zealously at the same time, and with [10]a pure heart. In England, and in matters of England, the first aim of the Direction is too often to damage what is not Roman, and the second to promote what is Christian. Upon the whole I must think Roman-Catholic Sisters are better out of, than in, the Army Hospitals. It would be right to think well over how far they could be entirely dispensed with, in the event of having soon to undertake a War Service.
In the event of a decision being made to dispense altogether with Roman Sisters, it would be as well to be prepared (though we never can speculate on the tactics of the Roman faction, and after what occurred during the Crimean war, it may think it better to take things quietly) for a battle, (not confined to the Army Medical Department,) for the production of an Inspector-General’s letter assigning “reasons” for preferring Nuns to secular Nurses, and for the delivery of sundry opinions of similar purport, ranging from that line to the one taken in the paper emanating from the Army Medical Department, extolling the Russian Nurses, “who were all Sisters of Mercy, and mostly widows of officers.”
2. The nature of the Service and Rules would, unless in war service, perhaps exclude English “Sisters” from the Nurses. They supplied us with some valuable women in the last war, and their Lady-Superior behaved ever generously, loyally, and well towards us.
The principle and detail of most sisterhoods render them unsuited for admixture with the secular element; and the comfortable belief into which the good women (of both branches) practically, if not theoretically, settle, that secular women are too bad to be mended or influenced, unfortunately makes their usefulness among Nurses nearly null. It would never do to unsettle any of the Sisters; but if it so happened that any voluntarily offered to serve as bonâ fide Nurses, some valuable individuals might thus be acquired; but this should not at all be pressed.
It would certainly remove a difficulty in declining Roman Catholic Sisters, if the rule should be to decline also English Catholic Sisters, forming the Staff entirely of secular women.
3. In Civil Hospitals there are three distinct elements of government. First, the Civil Authority; the chief being the Treasurer, or the equivalent civilian, whose subordinate is called [11]diversely Steward, Superintendent, House Governor; second, the Physicians and Surgeons (duly represented, in case of holidays or illness, by the Assistant Physicians or Surgeons), Apothecary and House Surgeon; and third, the chief of the Nurses—the Matron.
It requires of course temper, discretion, forbearance, and fortunate circumstances which do not always happen, for these authorities not to spend a portion of their time in quarrelling with each other; but the ruts are old and deep, and the wheels move on, though they often stick. The Civil Authority is a very important element, especially when the chief is a man of judgment and firmness, who keeps himself paramount over all, and does not delegate all to his subordinate the Steward. The Steward and the Matron generally find their duties disposed to clash.
In some Hospitals the rules are inexplicit in assigning power to the Matron over all the women. But this apart. The Steward represents and wields the police of the Hospital. He progresses through the wards, he perceives, or the Head Nurse reports to him, something disorderly. He rectifies it (or not, as the case and the man may be). She thus, over and above her relation to the Matron, has to appeal to, and to account to, the Steward.
This power of police and discipline, wielded by the Civil Authority of the Hospital, is of immense moment in regulating the good order of the Hospital; it acts in sundry important ways which need not be particularized.
Now, in the case of Military Hospitals, there is one important simplification of the business, which need not be enlarged upon. All the patients are men. But there are two things which do not simplify the machinery of the Military Hospital. The attendants, in the plan proposed, are not (and cannot be) all Nurses, under the Matron; nor all Orderlies, under an Officer; there are Nurses under a Matron, and Orderlies under some Officer; and there is no Civil element. The Doctors both prescribe, and hitherto have governed. An Officer orders flogging, &c.; but the Doctors practically both prescribe, and hitherto have governed. And a Military Hospital must, and should ever remain, essentially different from a Civil Hospital; both different in discipline and detail, and altogether a rougher and [12]ruder place. It should never for a moment be forgotten that the soldier is a very peculiar individual, old and stern as is his trade. A regiment, if one thinks into it, is a curious thing. The Hospital which receives these men when ill and wounded, whether regimental or general, is, and ought to be, a place essentially different in many things from the great Civil Hospital. The moral standard of the patients of the Military Hospital, their readiness to obey, their good feeling to each other, are strikingly higher than in the Civil Hospital; but the soldier is what, amidst all his faults, he has been made by the habit and spirit of discipline, which has become an instinct and a second nature, and which ennobles his own. Relax discipline, and in proportion as you do so, there remains of the soldier a being with as much or more of the brute than the man.
Discipline then being the pivot upon which the good order of all military things, Military Hospitals included, turns, it follows, that if you set down a few women (they should not be many) in a great Military Hospital, unless they can become effectually incorporated into the general spirit of discipline of the place, they will only injure themselves and the whole.
As women, the more entirely they are under the government of the Matron, herself under the government of the Superintendent-General, the better. As Ward Nurses, the more entirely they are under the orders of their Surgeons, the better; but they have not only to obey the Surgeons, they have to enforce the Surgeons’ orders among the patients, and both for so doing, and for the cleanliness, &c., of the ward, they have to give orders to the Orderlies.
In the case where a rule will work, by which, if the Nurse has to complain of an Orderly, she reports the same to the Matron, who lays the complaint before the chief of the Orderlies (whatever may be fixed upon as his name); well and good; but a more direct procedure will also be found necessary.
Every firm and discreet woman (none other is fit for a male ward, least of all for a military ward), will avoid collisions, reports, and violent outbreaks in the ward as much as possible. But still, every now and then these things will happen, and though by all means to be avoided if possible, when they do [13]come, they clear the ward-atmosphere like a storm, provided the discipline be strict. Every now and then—and every experienced Head Nurse will tell the same story—some disobedience, slovenliness, truculence, or sly impudence, will arise in the ward, and she will find she cannot put it down alone. If she remain helplessly deprecating or scolding the men, her position becomes at once an unseemly and a dangerous one, as that of all contemned authority is. In such a case, in the Civil Hospital, the Head Nurse goes straight, according to the nature of the case, to the House Surgeon or to the Steward, unless the visiting hour be at hand, and she judges it best to refer to the Surgeon. Discretion is again here required, as in everything in Hospitals; but between the Surgeon and the Steward, a firm, discreet Head Nurse will generally get the ringleader expelled, and two or three others, named or unnamed, warned of a similar fate. After this sort of explosion, the ward is quiet and orderly for months. The thing is seldom done, but the patients know it can be done at any time, and that it will be done, in such or such a contingency.
Now the soldier cannot be turned out of Hospital, and he knows he cannot. It becomes the more important not to suffer an hour’s relaxation of discipline there. If, therefore, such an outbreak, either on the part of patients or orderlies, should happen in a Military Hospital, the Nurse ought to be able to summon at once the proper authority and afterwards to report the whole to the Matron, but first to bring direct the proper authority into the ward. Whether it be the Captain of Orderlies or the Orderly Medical Officer, or, as in case of emergencies, is generally preferable, the Staff-Surgeon himself, she ought to have power at once to bring the proper authority into the ward, to put down confusion and restore discipline at once, and then afterwards to report to the Matron what has passed.
It must never be forgotten, that in every Regiment we must calculate upon there being two or three thorough scoundrels, five or six men who are not far off from being so, and an indeterminate number whom discipline saves from ranking after them. One year with another, characters no doubt as vile as the worst that disgrace our gaols pass through the General Hospitals.
Another thing to be remembered is, that whatever classification may be carried out, we may be certain beforehand that numbers of patients from a vile cause will be in the ordinary surgical wards of every General Hospital in time of peace. Very severe cases of this sort give heavy work, and little trouble. They suffer much generally, alike from disease and treatment; are frightened, if not ashamed, about themselves; and are generally extra-submissive and quiet. These cases, however, generally would belong to the separated wards; which latter contain usually a large admixture of patients who suffer comparatively little, and who require to be dealt with with unswerving firmness. For reasons somewhat too technical to write, it is to be hoped, upon the whole, that female service will not be, at first, at all events, extended to these wards. The disgusting and comparatively painless secondary condition will, I fear, find its way into the ordinary surgical wards, as it does into the equivalent wards of every Civil Hospital.
All these things would increase the mistake of laying any bar between the Staff Surgeon and the Nurse. In all matters of discipline, generally speaking, the Staff Surgeon will give much more support than the Assistant Surgeon.
A short definite rule should therefore be made, saying whom the Nurse is to summon in the event of disorderliness in the ward.
One thing more. There is nothing more dangerous than to undervalue the objections of opponents. Let us give them their full weight, and while firmly holding our course, and trusting to God to guide it, draw useful cautions from the objections which we quietly and steadily confront.
In the great Military Hospitals, of Roman-Catholic countries, intelligent, well-behaved, Army Surgeons, while explaining everything with thorough business-like precision, if spoken to of the Paris Army Hospitals, before the recently introduced Sœurs de St. Vincent served there, and asked what they think upon the whole of the service of women in Army Hospitals—after a little hesitation, and being urged to speak plainly, will generally say that they prefer in Civil Hospitals the service of Sœurs to those of hired nurses—but they deprecate either Sisters or any women in Military Hospitals. 1. [15]Because the presence of women, however virtuous and guarded, would excite passions and produce unfavourable results in many cases. 2. Because they were unnecessary, the Orderlies being efficient, faithful, kind, and sufficient.
Of the second reason one can judge nothing by a walk through a hospital, as it does not always follow that what the master says is enough is so—though this is one of the mysteries it is good to know and not good to reveal. Of the first there is no doubt. The question remains, striking the balance of good and evil—Do chaste, guarded, and efficient nurses on the whole contribute more to the economy of human life, the order, cleanliness, and decency of a Military Hospital than they do harm? Possibly the former effects are usual and general; the latter exceptional and rare: after all, most soldiers are men and not beasts. But it is well and necessary to bear in mind both the existence of this danger, and the exaggerated fears many Army Surgeons conscientiously as well as unconscientiously have of it.
I therefore very earnestly hope that the work will not be encumbered, at first at all events, with the charge of the venereal wards. And it is most important, for the favourable result of the anxious and difficult experiment about to be made, of permanently introducing female service into Army Hospitals, that we should be quite clear of the convalescent patients, and should only attend patients severely ill or severely injured.
4. Pay and Rations.—In the great Civil Hospitals the Head-Nurses have, on an average, 50l. a-year, no board, an allowance of fuel and light, and the use of one or two, generally unfurnished, rooms. The Assistant-Nurses, on an average, receive about 12s. a-week, [£31 per annum] no board, lodging, with the use of some furniture, sometimes an allowance of fuel and light, apart from the use of both in the wards.
Both Guy’s and St. Bartholomew’s Hospitals now give partial board to the Assistant-Nurses, and St. Thomas’s is about to adopt the same plan.
St. Mary’s Hospital gives board to both Head and Assistant-Nurses.
In the last war Her Majesty’s Nurses received, on an [16]average, 18s. a-week, lodging and board, fuel, light, and partial clothing—18s. a-week is 46l. 16s. yearly. Incorporated into a permanent Service, and with a pension, they ought not to receive the latter amount until after approved years of Service.
It is certainly a different thing to undertake service in a Hospital in Smithfield or the Borough, and to undertake to go, at a moment’s notice, to any part of the world. But the Army Service involves this; and the pension it involves makes a reasonable equivalent for the additional wear and tear of climate, travel, &c. Going abroad is a regular part of the Service undertaken.
Any artificial inducements should be avoided; at the same time their condition should be made a comfortable one. Wages, say 20l., rising to 50l. a-year, rations, an allowance of fuel and light, and a small furnished room, would be enough, and not too much. To this should be added a fixed annual gift of a few strong articles of regulation dress;[6] avoiding multiplicity, and securing the things being all good of their kind. In the last war they had too many things, and some were rubbish. They ought to be well able to supply themselves with linen, shoes, &c., whether at home or when ordered abroad. The articles to be given annually should be three strong dark gowns, six strong aprons, six caps, six collars, one bonnet—and let the things be good—biennially or triennially, one summer and one winter cloak. In India, &c., this might be modified. Their room should be furnished, because, in removing to and fro, it is better to release them from the cares and the pretences of furniture; also, because, instead of many gimcracks, you can thus furnish their rooms with a few comfortable, strong, plain things, presenting a certain military simplicity, which ought to pervade a Military Hospital.
Their wages abroad should not be increased. Whether they serve at home or abroad concerns the Superintendent-General alone, and is no merit or title for additional advantages on their part.
If the principle of rations is considered preferable by the War Department, it is important to give no extra trouble that can be helped. If not, it is to be considered whether or not it would be well to get rid of the rations, in the three kingdoms at all events, for these reasons:
(1.) These women are Head-Nurses. They will think themselves more comfortable “finding themselves” than managing on the substantial and somewhat unvarying provisions of the rations. Some take coffee rather than tea; some tea rather than coffee; many would rather pay for white sugar than not pay for brown. Considering the nature of nursing-work, when faithfully done, it is better they should enjoy and be refreshed by simple meals to their taste than by unpalatable larger portions; especially if the former can be done at no additional cost or trouble to the Queen.
(2.) You thus relieve the Superintendent and Matrons of all communication with the department of the Purveyor-General; of all the mistakes, accidental or otherwise, which might occur; of all complaints of quantity or quality of provisions; of amenities such as those experienced at Balaclava General Hospital, &c., &c., &c.
Of five London Hospitals, the three endowed Hospitals pay all their Head-Nurses in money, and give no board. (This is strictly correct, although, to avoid a long unimportant detail, I have simplified things in this paragraph, and in the two concerning the pay of Head-Nurses and Nurses.) The London Hospital gives its Head-Nurses wages, and a fixed quarterly payment vice the rations of bread, meat, and vegetables, to which they are by the rules entitled. This change was made not very long ago, to end the frequent complaints of quantity, quality, and price, made, perhaps with foundation, by the Nurses. The Westminster Hospital paid its Head-Nurses partly in money, partly in rations of cooked provisions, and there were repeated and general complaints of the quality, quantity, and cooking of the provisions issued to them.
It is therefore to be considered whether the simpler and better plan be not to give the Nurses a fixed money payment, and let them “find themselves,” unless the War Department object to rations not being issued in part payment.
Abroad in many cases, in war in all cases, rations would be desirable. A fixed calculation as to expense should be made.
Experience and consideration will probably give rise to the following conclusion—except in war and in retired stations abroad, not to have Rations; still less to let the Nurses “find themselves,” for the following reasons:—(1.) It is important that the Nurses should not have this excuse for being absent from their duties—“that they have been to get provisions.” (When absent, it should be in pursuit of health and exercise.) (2.) If the Nurse is to cook for herself, greater accommodation will be required than the one room recommended, otherwise the necessary cleanliness cannot be observed. To commute the Rations for mess-money, to put this mess-money in charge of the Matron, wherever there is a market; wherever there is none, to let her “draw” for such provisions on her own indent, as she thinks best, upon the Purveyor, appears to me the safest course. For with regard to this question of dieting the Nurses it should never be forgotten that, in all cases (how much more in those where great physical fatigue and mental anxiety are involved) that principle is the best, if such can be established, which settles diet with a view to producing the highest physical efficiency. Variety and mode of cooking are two essential elements in this. And there can be no doubt that, if a Matron will take the trouble to consult the tastes of her Nurses, together with the above conditions, a better diet might be laid down than could be secured by leaving them solely to their unassisted vagaries and ignorance of what is really the best diet. Community of cooking also implies economy. Also the Nurse ought not to be permitted to starve herself, to save money. Her time is too valuable to allow of her cooking her own dinner; but she should always prepare her own breakfast and tea, when and of what she prefers herself, if she feels inclined to do so.
Where, however, the system of rations must be adopted, three ways remain of working it:—
(1.) Let each Nurse receive, and cook her own rations.
(2.) Let the rations be delivered en masse to the Matron, who has them cooked, sending her proportion to each Nurse.
(3.) Let the Matron, requiring a small payment to cover expenses, arrange that each Nurse can receive her dinner cooked as she wishes it. There is something of this sort at the London Hospital; where the Nurses (and Assistant Nurses) have the right of sending their joint to be boiled or baked in one of the kitchen stoves.
Of these different ways, the first would be liked best by the women—a thing to be considered, in subordination, and as a help to their respectability and their efficiency—still it is, for some reasons stated above, objectionable. However, in this, as in far more important things, it is essential to consider everything as tentative and experimental for some years to come. Do not be fettered by too many rules at first: try different things, and see which answers best.
With regard to rations, it is as well to explain that there were two ways of drawing them for the nurses during the war. In some of the Crimean Hospitals, it was arranged that the same ration should be drawn for a Nurse as that appointed by Regulation for a Medical Staff Orderly. This answered, as may be supposed, exceedingly ill. There was considerably more of some articles, such as bread and meat, than the women could eat; and the surplus had to be wasted or returned to the Purveyor—a serious complication. Of some articles, such as tea and sugar, there was as much too little; and these had to be drawn as extras, except such as the Superintendent-General found it easier and more simple, as she generally did, to provide herself.
The other method was for the Local Superintendent to draw daily on the Purveyor for such articles as she judged necessary; and by thus drawing en masse, a considerable saving was, of course, effected for the Queen, the tastes and health of women were consulted, and there was no complication of accounts.
Where rations are to be drawn at all the latter method should be always followed; and as the former might be understood by the word “rations,” it would be better to call them by some other name, as it must be obvious that such a method could never answer for women.
The experiment which I should wish to try, by which greater variety could be secured, but which could only be practised where there was a market at hand, would be for a commutation to be made of rations for money. Each nurse to supply her quota of “mess money,” the “mess money” to be all[20] expended on the “mess,” and the Matron to manage the “mess” day by day, and arrange for the cooking to be done in common. If each nurse’s dinner is to be cooked separately, it necessarily entails great waste of nourishment. The Nurses would not like this so well as “finding themselves,” but it would ensure them a far better diet.[7]
It would be a question whether the Queen should pay the Superintendent-General so much for each Nurse’s wages, and so much for board, the latter to be retained by the Superintendent-General, or whether the Superintendent-General or each Matron, with the Superintendent-General’s consent, should arrange with the Nurses. This is important, as which ever way it is settled, there must not be disputes between Matron, Nurses, or still less Superintendent-General, as to what amount of wages is to be allotted to the board, or what savings can be effected in the coals, &c.
On the whole it would seem best for the Nurse’s pay to be so much in money for herself, and so much in money for food into the Superintendent-General’s hands. But the question of how much is a serious business.
5. Washing.—Except in war-emergencies, this must not be suffered to be done by the Nurses, they must be compelled to put it out. I would not trouble the Authorities about this; the Nurses can afford it, and the more things are simplified the better. In out-of-the-way districts, the Matron might arrange with a laundress, the Nurses making a fair payment. In war-emergencies, if possible, provide a strong washerwoman, but this would have to be settled each case on its merits. Except in emergencies they must not wash; it takes up far too much time; it takes up strength which is wanted for other things; and washing and drying either in wards or nurses’ rooms is unhealthy and objectionable. There must be a rule [21]as to this: some worthy souls would scrub at every rag, rather than pay a few pence weekly. The Nurse ought, however, to be compelled to have certain changes of linen weekly, which some will not, if they pay for it themselves.
6. Cleaning their own rooms.—I well foresee sundry difficulties in the little rooms at the entrance of their wards, where I hope it will be managed to quarter the Nurses. But there is no other way of fairly and really working a ward; and I trust this plan will receive a fair trial. For efficiency, also for comfort, it is most objectionable to make the Nurse sleep at a distance from the patients. This is one of the points on which theories, and the practical working of things, are very divergent. It is an excellent thing when the Head-Nurse’s room opens into the ward and when part of the upper part is of glass, with a thick curtain, so that she can see into the ward, without being seen. Let each Head-Nurse have a small room, with a window opening into external air, with a curtain making an alcove, behind which there should be a small iron bedstead, with good bedding, and a washing table; and in the foreground a table, a small one for meals, a chest of drawers, and a comfortable arm-chair, two chairs, and I should add a sofa. Each room should have a few shelves on the wall, and a large cupboard or small closet with broad shelves, and space at the bottom to stow away the Nurse’s box. Simplification and avoiding all trouble which can be spared to the Departments are very important. I would not therefore insist upon a little kitchen for the Nurses, nor upon a very capital arrangement in some of the Sisters’ rooms in Guy’s Hospital, where, behind a decent little door in the sitting-room, there is a sink, with water laid on, a little safe for meat, &c., at top, and a complete little apparatus of the very few utensils required for cooking one woman’s meals; so that a Nurse can cook and wash-up, in her own room, without carrying things out of it. This is much better than a kitchen, if the Nurse is to cook her own meals; but, as above stated, I would rather she did not. One room, with a curtain making an alcove, is much better than two. The Queen is saved fuel; the Nurse is saved cleaning two rooms; and if fuel is only issued for one, she sleeps in a warm room, instead of one where there never is a fire, and where her things get damp and spoiled. Often, where Head-nurses have two rooms, one is built without a fire-place. Condense [22]and simplify all things—one great object is to form a body of useful hard-working women, of simple self-helping habits. Two Nurses’ rooms should be together, but separate. Sudden illness might occur, and the two women should be at each other’s summons. The Quartermaster-General must grant a cabinet between the two: this is must, not may. The Superintendent-General must see to this herself, at first at all events: there is a singular obtuseness in the small officials, by whom these things are managed: if not overlooked, they will be sure to put the construction in a particularly awkward, exposed place. These things do enter into an Englishwoman’s daily comfort or misery—it is worth arranging them decently in the first instance.
Now as to the cleaning of these rooms. Head Nurses generally are far too much disposed to make servants of their nurses; put orderlies for nurses, and this objectionable tendency would be a hundred-fold more objectionable. The Matron must make it an absolute rule, that the only thing an orderly does for a nurse is to carry her box in and out on the two grand occasions of her entering and leaving the Hospital. The one thing which in a Civil Hospital, an Assistant Nurse should be allowed to do for the Head Nurse, is the cleaning her fire-place, a thing done in a few minutes, and with satisfaction, by women who have done it all their lives; but a dirty tedious messing business to those who have not. But never mind: the orderly must never enter the Nurse’s room: she must do it, and learn to do it. The prosaic little business of black-lead, ashes, and mess lying on the threshold of the work will do good rather than harm. And even black-lead is unnecessary, as a varnish now obtainable looks better. The orderly must never enter the Nurse’s room—a sine quâ non. The Nurses should have, at their choice, a carpet, not nailed down, or none. In either case the room will require scrubbing, once a week if no carpet, (which is best and cleanest in Hospital life), seldomer, if carpet. Now the Nurses should not be required to scrub their own rooms—it is useless waste of strength—it makes their hands coarse and hard, and less able to attend to the delicate manipulation which they may be called upon to execute—and with all the nursing proper which ought to fall upon them, and not upon the orderlies, their time can be better occupied than in cleaning [23]their own rooms. Also, while trying to keep clear, on the one hand, of the tribe of “fine ladies,” it will be possible, on the other, if such menial offices are to be performed, to fall into the opposite mistake and to fail in obtaining the class of women desirable to fill such important trusts. Let the Matron consent to a charwoman, soldier’s wife, or some one person named and defined, and found, to be paid by the Head Nurse, to come for the two hours, which, at furthest, this business will take. It would be well worth while for the Matron to look out and provide two or three strong women to do this, by fixed rotation—each Nurse making a fair payment—and to ascertain that they are in and out of the Hospital by a particular hour, so as to prevent these external persons doing other things than scrubbing. But do not trouble the Departments as to this—the more things are simplified, and the fewer expenses are in connection with the Nurses, by far the better.
Take the trouble to see that a tidy useful fire-place is in each Nurse’s one room. Some fire-places will consume thrice the fuel of one which can do ten times more work. A compact useful little fire-place, to burn as little fuel, and do as much business (in a very small way) as possible, is a thing of daily use, economy, and comfort.
The nurse should not do anything of her own in the ward, or the ward or orderlies’ scullery, if there is such a place. This is a matter requiring some decision.
7. Let there be in each ward a closet, or, better still, a dresser,[8] with broad shelves, and a large table with large drawers, of which closet or dresser, and drawers, the nurse has the sole keys. Let the articles of linen which are kept in the ward be there; also the bandages, lint, old linen, oilsilk, ointments, &c., &c., which should always be, some at hand, some in reserve; also the wine and brandy ordered for the men. Let the nurse never be allowed to deposit Hospital property in her room, which, if there is no place for it, she must do, and it is much better she should not.
8. With regard to the Matrons, though as Locke says of tutors, there are all kinds of persons to be found, it is certain the right persons are not always found; and these officers will take time to find, at the outset especially. Let them be (if it be possible) of the middle class; if it be possible, middle aged, active women, widows of officers or army surgeons. A vast deal of struggle is ever going on in professional life; a vast deal of silent, decorous misery ever follows on the premature deaths, the compelled early retirements, the sundry chances and changes which ever abound in the army of England. So far as it goes, and cæteris paribus, it would be right, just, and expedient to give a preference for these matronships to widows of officers and army surgeons. Try to secure thorough principle, sense, activity, and steady discreet ways; never mind a little vulgarity of manner; that the different orders should have their indefinable perpetual distinctions of manner as of other things, is perhaps for a long time to come in the essence of things. Two or three women of the stamp of the Matrons of a few of our Civil Hospitals would be very valuable. If the Matron do not get tired of what, unless one keeps one’s secret thoughts fixed on the meaning and the end of all things, is coarse, thankless, up-hill work enough—she will in the course of years accomplish great good. But she must have principle, sense, heart, and a firm cheerful mind. She must be not under thirty and, if possible, not over forty, on appointment. Should her being without children be made a sine quâ non? Children—poor little things—are wanted nowhere in the way of business, but do not be too strict about this: they are sometimes pledges to other things than fortune—thoughts, anxieties, and labours for them, concentrate and steady a mother’s heart—there will be fewer adventurers. Maternal nurses must upon the whole be discouraged, because upon the whole the disadvantages seem to overweigh the advantages.[9] But the Matron’s office and duties are different; she is not fixed to a great ward of patients; and her having children should not be a bar, especially if they[25] did not live with her. Young and grown-up daughters are much in a Matron’s way; sons matter much less.
The greatest Civil Hospital gives its Matron 200l. and a house, the other great Hospitals, 150l., and a house. The London Hospital gives 150l., and a couple of good well-furnished rooms, and a servant. A house is an impediment to a Matron’s duty. She is seen arriving in the wards, and she is more or less hindered in entering them. From her rooms she issues and re-issues, unexpectedly, and much more efficiently. 200l. and quarters is not at all too much.
The Matron must be responsible for the storing, mending, and distribution of the linen, and for returning to the laundry any linen not properly washed or dried. Linen ought never to be dried in the wards, a process both inconvenient and unwholesome. The Matron ought to have a steady, respectable woman, certainly not below the rank and pay of a nurse, to be responsible to, and under her, for the linen, otherwise the proper care of the linen will take up far too much of her time. This is important. If, however, a Nurse should be thus set aside for the Laundry, she must not be allowed to enter the wards; otherwise she will unconsciously become a gossip and mischief-maker. I would term her “Linen Nurse,” not Assistant. The Matron should also have a steady, properly paid servant. A Matron of the proper sort has quite other things to do at a leisure moment, than to keep her wardrobe in order. She must have a servant; but it seems to be advisable to simplify things, and condense payments as much as possible; and I would rather consider this in the salary, and let the Matron find and pay her own servant. Try to have the servant’s room near the Matron’s. These minutiæ, once provided for, enter much into the daily working and comfort of things.
The dress of the Matrons is a difficult thing to settle. Sometimes a Matron is afflicted with a taste for either gorgeous or elegant apparel, which the Nurses are invariably proud of, admire and humbly emulate. This sort of thing would be really out of [26]place in a Military Hospital, and would moreover sadly discompose the Nurses with their plain caps and gowns. How would it be to allow the Matrons the choice between a Regulation dress and a plain black or brown silk gown?
It will take much thought to decide whether the Matrons should all be paid alike, or whether climate and size of Hospital enter into this. On the one hand they undertake a service, of which almost the first regulation very properly is, that they undertake to go to all parts of the world as soon as sent; on the other hand, certainly some climates wear health and life much quicker than at home.
The Matrons out of the three kingdoms have increased responsibility, and can do more mischief, if incompetent or untrustworthy.
If the Matron has increased pay abroad, it would not do not to augment that of the Nurses. This is an important matter; and as it is on all accounts necessary that Matrons and Nurses should on their engagement thoroughly understand the nature of the service they undertake and, of course, a serious part of the service is that it involves sudden and long removals, it would be necessary to define upon what terms they go abroad. Yet it never would do, for reasons which will readily be perceived, to make the foreign stations objects of desire to Matrons and Nurses. These stations will always be so far the most anxious, that they will always be the most removed from the Superintendent-General’s inspection and immediate rectification of anything that goes wrong. They will also be, in various ways, the most trying to Nurses. The rules once settled, every Matron and Nurse refusing to go abroad when ordered, ought at once to be discharged, and to forfeit all re-admittance into the service and all pensions. On the whole, I think the Matrons should all be paid alike. But inasmuch as foreign service necessitates more wear and tear to the constitution, one year should count as equal to two years of service for pension, in case of disability. The same should be made applicable to the Nurses. As the advantage is distant, it would, in a great measure, do away with any desire for foreign service.
Volunteering for foreign or war-serv[27]ice must be the exception—careful selection the rule. The “adventurers” will be generally ready to volunteer, and it would be too much to hope that we shall always, perhaps ever, be entirely free from that tribe; the most we can hope is soon to discover and get rid of them. Foreign stations will never do for an untried Matron or Nurse. At the same time it is most desirable not to change the Executive officers of any Hospital more than can be avoided.
But let there not be too many rules at first; see how things work, and take one step at a time.
The selection of exclusively middle-class Matrons seems to be important.[10] Their order will disarm one source of opposition and jealousy; plenty more will remain, inseparable from the work; but it is good to get this out of the way.
The name of Matron is the same as in Civil Hospitals. In many respects the office and duties are different: e. g., the Matron in Military Hospitals must exercise a far more constant supervision in the wards. But this will require great discretion on her part. It is the practice of most Civil Hospitals for the Matron never to enter the wards till the Nurse’s dressings are over. It would be advantageous to modify this. But, at the same time, the Matron must understand Hospital Nursing, or she may make very serious mistakes in either reprimanding or directing the Nurse as to technical matters. She must be a person who knows herself what she has to see that others know; or she will get herself, with or without the Nurse, into very injurious errors. There is much in a name; and, in some respects, that of Superintendent would better denote her office, as regards the Nurses, would add to her authority, which is desirable, and would point her out as acting under the Superintendent-General.
Incorporate among the Nurses whatever women of the higher orders may be admitted into the Service at first. If inefficient and unfit they are far better altogether eliminated. If thoroughly efficient as Ward Nurses, if thoroughly obedient and respectful to the Matron, if they have sense and heart to gradually leaven, not coldly withdraw from occasional companionship with the other Nurses, they will, in the course of [28]time, effect quietly a great deal of good.
There should be some Rule of this kind—
Any Matron or Nurse who may receive permission to serve Her Majesty without pay shall be, in all respects, bound by and amenable to the Regulations on pain of dismissal from the service, without permission of re-entering it.
If this cannot be done, money can easily be returned in one shape or other; but it would have a good moral effect on the Nurses to allow of the admixture of unpaid Nurses, provided they are strictly bound by the same Regulations, and distinguished by no sort of peculiar designation.
The Surgeons will dislike these unpaid Nurses; but, in the long run a firm, discreet woman, who is an efficient Nurse, can get on with any Surgeon who has his sick at heart. The Matron also will not at all like them, at first, but will find that she can rely upon them and that they quietly and effectually help her with the other Nurses: and, if she has her heart in her work, she will end by being just, though, perhaps, always a little extra strict with and jealous of them. The other Nurses will have, at the first, a strong little touch of republicanism towards them, which will gradually wear off, and, with God’s help, a higher and truer moral tone, and a simpler and more useful kind of habits among them will prevail, than would otherwise be the case. As for the patients, with all their faults, trust them—trust the English soldier, and the peasantry from which he springs. What these poor fellows are we know, and need not discuss. They are worth suffering a good deal for; please God in the long run good will be done. If only we can keep clear of the false, pernicious, and derogatory system of puffery and fuss which others, for their own purposes, and from vague, silly good-feeling have wound around this work—a work essentially unpopular the moment we come to details! We have learnt what reality is and what its presence or absence in this business imports. As for the many and great other difficulties of the work, they must be appreciated, they need not be dreaded. The purpose is a good and noble one, and God grant it success! All we have to do is, to do our utmost, and leave the event to Him.
9. As for the Nurses the material must be formed. If a few respectable soldiers’ widows, including, and all the better, non-commissioned officers’ widows, could be found, cæteris paribus, a preference should be given to widows of the Service.
Except in emergencies Nurses should not be taken under thirty, or above forty[11] years of age. These women are Head Nurses. Most of the Civil Hospitals take no Head Nurse after forty.
One caution in engaging Nurses is perhaps not sufficiently attended to. Certificates, without personal inquiry and answers to distinct questions, are not worth the paper on which they are written.
As to engaging any Nurses out of the great Hospitals, for sundry reasons, this should be done as little as may be.
Let us begin, for the sake of God and this His work, with few women. Extension is easy—to occupy too much ground at first would be, I do in my conscience believe, an irretrievable mistake.
No unnecessary Nurses should be suffered in Hospital; and no Nurse in charge of wards should be required to do needlework for the Hospital. There should be no superfluous hands; and the less a Nurse enters another’s ward the better.
In case of suspension of a Nurse for misconduct, temporary assistance must, however, be obtained; and this might be either appointing another Nurse, to do, for the time, such duty in the suspended ward as she could do in addition to her own, or putting in a temporary substitute.
All such dislocation of the Service, necessary and useful for emergencies and holidays, should, nevertheless, be made to take place as seldom as may be.
No Nurse, during her suspension, should be allowed to enter any ward of the hospital.
Any Nurse asking or accepting a present, whether in money or in kind, from any patient, or friend of any patient, whether during his illness or after his death, recovery, or depar[30]ture, must be at once suspended from duty, her pay immediately cease, and the Superintendent-General be apprised of it, who, if satisfied of the truth of the charge, should immediately dismiss her.
Two hours daily for exercise or recreation should be allotted to the Nurses, during which two hours they are to be considered relieved of the responsibility of their wards. But I would not be too absolute in requiring them to go out: sometimes to lie down or sit still for an hour or two will do more good than a walk. Give them two hours for optional exercise. Head-Nurses cannot have more of fixed leisure. They must get time for private occupation as they can: very often not at all; and no Nurse fit for her place will, of course, in emergent states of her ward, leave it. Also the Matron must not worry herself or them, if an anxious Nurse sits up part of a night or a whole night with bad cases.
To a certain degree the Matron will find it better to allow a little liberty and choice, in the matter of times and hours, (always excepting after proper hours, i. e., after dark) to the Nurses, who are Head-Nurses, than to attempt making them mere machines. An uniform system, as far as possible, and a little range to each, will answer best. But do not hurry the uniform system too much; take time: this is very important.
The Nurse should, every morning, at an hour to be fixed by the Chaplain or Matron, read aloud in the ward, the Confession, the Lord’s Prayer, the Collect for the Week, the Collect for Grace, and the Benediction; and every evening, at an hour to be fixed by the Chaplain or Matron, she should read aloud in the ward the Confession, the Lord’s Prayer, the Thanksgiving, the Collect for Aid, and the Benediction.[12] This would Christianize things, instead of heathenizing them; and I believe not a soldier would dream that his conscience was injured by it. The Roman Catholics and Presbyterians might be allowed quite to refrain, if they chose, which they would not. It would be necessary for the Chaplain-General to approve of and direct in this, and best to wait a year or two before beginning it.
The prayers should be very short, the whole not more than five or six minutes each time, and the Nurse should read them, the men joining at the proper times.
In some Civil Hospitals the prayers are far too long and are gabbled over by some patient, perhaps the worst character and the best scholar in the ward, or are stumbled through by some little boy, upon whom the others cast the distasteful office, with circumstances of irreverence, partly unintentional and partly shocking. At St. Bartholomew’s Hospital the very short morning and the very short evening prayers are printed clearly on each side of a card, which is affixed to each bed; and each morning and evening the Head-Nurse reads them aloud: the difference is very great.
10. The Colney-Hatch Lunatic Asylum has a diet system worth inquiring into; nothing is fetched by the Nurse, the Medical Officer writes the diets on a large slate which is ready for him outside the ward.
The great advantage of this seems to be, that the Nurse’s time is set free from a good deal of arithmetic and some writing; also that each man’s portion is served him hot from the kitchen, not cut up laboriously by the Nurse. In most Hospitals the Nurse cuts and divides the diets; in the London Hospital she moreover weighs them. All this takes a great deal of time. If the patients can get the divided portions hot from the kitchen, it is far preferable.
At St. George’s Hospital the portions are sent hot and divided from the kitchen.
11. It should be distinctly settled by whom poulticing, fomenting, and all minor dressings, applying leeches and blisters, and giving enemas,[13] are to be done.
It would be advisable to consider whether the Nurse ought not to instruct the Orderlies in some things. This, if it did not clash with Orderlies’ Rules, would make these men, especially those ordered for foreign service, much more useful than they are now, without such teaching.
It will, however, be essential that there should be no clashing between the Nurses’ Regulations and those already or to be issued to the Orderlies. And for this, among other reasons, it is essential to establish a direct channel of communication between the Director-General and Superintendent-General of Nurses.
I think, upon the whole and with reference to preventing, as far as rules can do it, the obstruction of the Nurse’s duty, by adverse or inexperienced Medical Officers giving orders to Ward or Assistant Ward-Master, Orderlies, or patients, instead of to her, that it is better to charge him to give the Nurse his orders as to the sick.
All the above-mentioned things should be done by the Nurse, i. e., by her habitually and as a rule; occasionally letting an orderly do them, under her own eye, in order that he may learn, as well by doing them sometimes himself as by often seeing her.
The reasons why all these things must be clearly settled beforehand are these:—
I. Adverse Medical Officers will make all use of counter-regulations.
II. Medical Officers who give fair play will find it impossible to settle the matter, if, on ordering, e. g., leeches, the Orderly shows Rule so and so by which he does it, and the Nurse Rule so and so by which she does it. The existence of the old regulations and the arrival of the new ones, about the Medical Staff Orderlies, were made great use of against our work, by some of the Medical Officers, after the heavy pressure of the war was over. So, at Scutari, a Principal Medical Officer took away and would not restore the practice of the nurses giving medicines, in which he was borne out by an existing rule. Contradictory rules are miserable things.
Unless the Matron’s authority is supported by the Principal [33]Medical Officer the Patients always suffer. The Nurse is the only proper person to be responsible for the directions of the Medical Officers being carried out in a General Hospital.
III. It will enable the Matron to stop all nonsensical prudery, on the part of the nurses, and to require that they should do what they undertake to do, and not pass off to an Orderly, still less to a patient, the duties they should discharge themselves.
As a general rule there is a good deal of this false modesty on the part of Nurses, especially of Head Nurses. In individual cases it is a serious thing to shake even false ideas of decorum: in laying down general Rules it is the more important to lay down as duties what are such. Suppose an application of what the French call “la petite chirurgie” ordered. The Head Nurse “never dreams of doing such things.” The Nurse, following her superior’s false shame of duty, transfers the business to an ignorant patient. In some cases great harm has arisen thereby to the Patient. In other cases, but not the majority, after such an order given, the Head Nurse goes quietly to the bed, draws the curtain round it, and makes the application herself—saying “she always did that herself, as it was a business requiring care, as the patient was often disposed to resist, and as she was thus certain that it was properly and effectively done.” I have always admired and respected such women; but they are not the majority. Very often patients are allowed or left to do things for themselves, which they cannot do properly, or when they ought not to be trusted to inflict the pain on themselves which doing things properly often causes.
The practice of allowing some particular patient to become a sort of half orderly in the ward, letting him always attend some particular case, or give general help in severe cases, is most reprehensible. It is never allowed, whether in Civil or in Military Hospitals, without very bad consequences to the discipline of the ward. Where extra help, in lifting, &c., is required, let the Nurse require the most convalescent of the patients to help, but let her carefully refrain from selecting any patient or allowing any patient to put himself forward, as a regular help or quasi-Orderly. As an almost invariable rule it will be found that the less patients do for each other the better for themselves, and for the discipline and the good feeling of [34]the ward. Let them be made useful in the wards, as far as possible, in such lighter cleaning, &c., as a patient can properly do (here, again, discretion is required, or a lazy Orderly will lay undue burdens on a willing patient); but the less they do for each other undoubtedly the better for all parties. I would not, however, expressly exempt the patients from being made useful in nursing the sick. A lazy or ill-conditioned patient might make it a handle to refuse to do or grumble at doing things which he ought to do, such as (a thing frequently required) giving and emptying a bed-pan to an ordinary patient who cannot leave his bed, while the Nurse and Orderlies are doing other things in the ward; assisting to move a helpless patient, if all the Orderlies are not at hand; sometimes watching or attending for an hour or so a critical case, &c., &c., &c. What the Superintendent-General and all Superintendents must be especially vigilant against is selecting any particular patient or allowing a willing patient constantly or often to do these things, and to become a quasi-Orderly to the ward or to any patient in it.
Assistant-Surgeons, partly from inexperience and partly from spite, sometimes make this sort of quasi-Orderly of a patient. The Nurse should have the power of respectfully saying, in such a case, “The Regulations order me to do so and so, sir: I beg you to let me do my duty.”
It is an important and should be, if possible, an invariable rule that no discharged patient is ever to enter any ward. Soldiers are, in many respects, on a different footing, as to each other, from Civil patients. The above provision is perhaps rendered thereby (not the less, but) the more important for the good order of the ward. Still this, desirable in (and the rule in several) Civil Hospitals, might be considered by Military as well as Medical Officers to interfere too much with the feeling of comradeship which, in its measure, is so essential a part of the soldier’s very peculiar condition. The following rules however might, at all events, be carried out. Some of them are actually in the “Hospital Regulations.”
As quietness is indispensable in Hospitals, every duty should be performed with the least possible noise, more especially at night. Every patient must be in bed by 8 o’clock in winter, and 9 in summer; and no conversation must be permitted after [35]that time. Patients should be made useful in the wards, as far as possible; but should fetch nothing into them. And no discharged patient should be permitted to enter any ward, except in the fixed visiting hours. The Governor, where there is a Governor, or the Principal Medical Officer, will fix the visiting hours; which shall not be more than two hours during each of three days of the week. [Take proper advice as to whether this maximum is too short. It is fully enough for Civil Hospitals, but Military Hospitals are in sundry respects essentially different.]
In the discipline of all Military Hospitals, besides the prohibition of all swearing and foul language included in the Articles of War, is included the non-admission, or if by oversight admitted among visitors, the immediate expulsion of all disorderly persons. (Query—whether not to specify prostitutes.)
I very much wish that Hospital Sentries in General Hospitals might keep out all visitors, except in the fixed visiting hours. And I very much wish that a stringent rule were made as to female visitors, both in Regimental and in General Hospitals. Proper Military as well as Medical advice should be taken on this point. It might not do to exclude them altogether; and, if soldiers’ wives come, it might be better to admit also all respectable-looking women, for it would be useless attempting defining as to sisters, aunts, friends, &c., &c.; though, except in the case of dying patients, all women, except their wives and mothers, are better away. I do not know what amount of strictness in practice is shown in enforcing the Regulations in English Army Hospitals; but if, at present, equivocal women, as well as ascertained prostitutes, are not excluded (which very possibly they are) they should be. At the same time, a sentry may often be honestly puzzled as to equivocal or non-equivocal appearance, in these days of over-dressing. And some mistake, made by a stupid or brutal sentry, might lead to endangering the rule. This whole matter must be referred to men.
12. With regard to the question of the “Regulation” number of Orderlies, viz., 1 to every 10 patients, it is to be observed,—
(1.) A ward of 40 patients might be efficiently served (but it would be hard work) with
With no number under 40 of patients to a ward, can the Regulation proportion of 1 attendant to 10 patients be adhered to.
(2.) With a ward of 20 patients (cut, scheme, and arrange the hours and duties as you will), you cannot efficiently serve it with less than
And the other ward of this Head Nurse ought to be on the same floor.
N. B.—The same number would quite as efficiently serve a ward of 25 or even 30 patients.
(3.) The Army system of 1 Orderly to 10 patients, with a number not exceeding 10 patients to a ward, is upset as immediately by one bad case among the 10, as by 9 to the 10.
For, is the same Orderly to be on duty for the 24 hours?
The difficulty is practically got over by the Army, with a permission that any “bad case” may select any one he likes of his comrades (out of the Depôt) to be “told off,” to attend upon him.
This extraordinary regulation is equivalent to (and affords little other practical result, than) granting opportunity for any quantity of spirits, and illicit food, to be smuggled into Hospital, and it is clear that it would be totally inadmissible in a General Hospital, where the whole system of nursing would be under the most stringent discipline and supervision.
(4.) The introduction of Female Nurses into Military Hospitals is not intended to supply the place of Orderlies, but to perform a class of duties which never has been performed at all in the Army. Few other Hospital duties of those generally called such have been hitherto fulfilled, in Military Hospitals, except
(5.) In all Naval Hospitals, the Regulation number of attendants is 1 to every 7 patients, or 2 attendants for each ward containing more than 7 patients and up to 14. These [37]Attendants or Nurses, in sailor’s language, have charge of the linen, bedding, and ward furniture, under the Ward Matron, and they are responsible for the proper care of the sick, and the due administration of the medicine, wine, and other medical comforts. They are on duty all day and watch at night in their turn, which is regulated by the Medical Officer in charge of the ward, in this or similar fashion:—a group of three contiguous wards is allotted during the night to two nurses, one begins her duty at 9 and ends at 1 o’clock, when she is relieved by another, who watches till 6. She patrols the three wards, resting in that one where there may be a case requiring more than ordinary attention. If there should be a case of fever, delirium, or other sharp seizure, extra Nurses, both men and women, are assigned to the charge of that special case, according to the urgency of its wants. The great majority of Naval patients are either convalescent, or suffering from trivial complaints, which do not impair their activity. They can therefore take care of themselves, and assist the Nurse during the day in cleaning the wards, &c.—and we know what good housemaids seamen make. The Nurses are paid one shilling a night for night watching. They have under the most severe circumstances two-and-a-half nights in bed for half a night out of bed.
At Haslar Naval Hospital the system of Orderlies, as understood from the Principal Medical Officer, is as follows:—12 Orderlies are on a floor, to look after, say, 90 patients. These are divided for night duty into three divisions of 4 each; of these 4—
The Head-Quarter room or ward is the one which has the most severe cases; this ward, then, the Watcher at night sits in, and makes the rounds of the others every now and then to see if anything is required. This system will of course be modified, according to the nature of the cases in Hospital. The other attendants do not sleep in the wards. The Nurses are male or female according to the discretion of the Principal Medical Officer.
In Civil Hospitals the number is as great of attendants to patients, and is mainly determined by the size of the ward:
E.g., in one Hospital, where there are quadruple war[38]ds of 44 patients, 11 in each compartment, though the average number of patients is 48, the number of attendants is 7.
In exceptional cases extra Night-Nurses, sometimes extra Day-Nurses serve particular patients. The labour, both of cleaning and of night-nursing, is much increased by the wards being four, separated by a large lobby.
In another of the large London Hospitals, where there are to each ward,
| Patients. | Attendants. | |||
|---|---|---|---|---|
| 22 24 | ⎫ ⎬ ⎭ | there are | ⎧ ⎨ ⎩ | 1 Sister. 2 Nurses. |
| 30 | there are | ⎧ ⎪ ⎨ ⎪ ⎩ | 1 Sister. 2 Nurses. 1 Scrubber. | |
| 34 | there are | ⎧ ⎨ ⎩ | 1 Sister. 3 Nurses. | |
| 40 | there are | ⎧ ⎪ ⎨ ⎪ ⎩ | 1 Sister. 3 Nurses. 1 Helper. | |
In the Lariboisière Hospital at Paris, where the wards hold 32 beds, 1 Sister, 1 Nurse, and 2 Orderlies on the Men’s side, 1 Sister, 2 Nurses, and 1 Orderly on the Female side, serve the ward efficiently.
(6.) One woman does the work of more than a man in a Hospital, speaking of the duties discharged by Under Nurses in Civil Hospitals; for men are not accustomed to these duties in England, as women are from their childhood.
From this it is by no means to be inferred that women of the class of Under Nurses in Civil Hospitals should be employed in Military Hospitals, which unquestionably they should not. But it is to be inferred that the work will not be done efficiently, with a smaller number of men than would be employed of women.
(7.) The question of attendance has scarcely been intelligently considered in the Army at all. And hardly any practical answer has yet been given to such questions as the above.
I conceive it to be practically impossible to serve 4 wards, as proposed at Netley, viz., of 9 beds each, with
For, as has been said, one bad case in each ward, makes this economy as unmanageable as nine.
(8.) A ward in a Military Hospital now may often be little else than a barrack-room, with an Inspection by a Medical Officer twice a day. It is designed to make it by the new Regulations into a place where the sick must be and always will be suitably attended. But this cannot be done by such a scheme as—
| 1 Female Head Nurse | ⎫ ⎬ ⎭ | to | ⎧ ⎨ ⎩ | 50 Patients, in (say) |
| 6 Orderlies | 6 Netley Wards; |
though this attendance would be more than sufficient for 50 cases in one ward; but such a ward is considered in a sanitary sense too large. Two wards of 30 beds each on the same floor would be efficiently served by such a Staff, however; and there would be no sanitary objection.
(9.) The Regulation number of one Orderly to ten patients therefore requires modifying. Practically it is broken every day and in the extraordinary manner above mentioned, which gives the most critical cases to be attended by the rawest hands.
(10.) The question of Hospital floors will be fully discussed farther on. An Orderly should be trained to be the frotteur to each ward. He should also be the porter to fetch and carry every thing to and from the ward.
(11.) The plan of Netley, with its wards for 9 sick, is by far the costliest for administration, as the following facts will prove:
I. It is proposed to provide the Hospital with Orderlies and Nurses to conduct the nursing in wards of 9 sick, as mentioned.
II. On sanitary grounds wards may safely be large enough to accommodate 25 to 30 sick.
We may therefore choose the larger wards, being guided only by the cost of the nursing.
III. A ward of 9 sick would require 1 day and 1 night Orderly, and a-third of a Nurse (that is, a Nurse could superintend three such wards.)
A ward of 30 sick would require 2 day and 1 night Orderlies and 1 Nurse = 4 persons in all.
Or if two such wards were on one floor, 1 Nurse could serve both.
IV. We cannot count the cost of Orderlies and Nurses, including lodging, rations, wages, at less than £50 a year, which when capitalized at 3 per cent. (33 years’ purchase), would amount to £1,650 for each.
V. A ward of 9 sick would cost in nursing £1,650 × 2⅓ = £3,850, or £427 15s. 6d. per bed.
VI. A ward of 30 sick would cost for nursing, in perpetuity,
£1,650 × 4 = £6,600 = £220 per bed.
[One Nurse to each ward is here allowed.]
VII. The cost of the two plans relatively for a Hospital of 1,000 sick would stand thus:
| Wards with 9 beds | = | £427,775 | |
| Wards with 30 beds | = | 220,000 | |
| Capitalized difference of cost in favour of large wards |
} | £207,775 | |
| Netley has cost already Land | = | £30,000 |
| Works | 89,000 | |
| £119,000 | ||
It hence appears that, if works and site were both sacrificed, and fresh land purchased, and wards for 30 sick built on it, the country would actually save the difference between the two sums of = £88,775.
Suppose the sanitary requirement of 25 sick to a ward, which is the best number, be combined with the greatest economy of administration, the cost would stand thus:
| For each ward of 25 sick, 3 Orderlies, at £1,650 | = | £4,950 |
| If two such are built in line, close to each other, with the Nurse’s room between them, one Nurse could superintend both wards, or half a Nurse to a ward. The cost would be for the ward | 825 | |
| 5,775 | ||
| Or cost for each bed 5775 / 25 | = | £231 |
The comparative cost of wards with 9 beds and 25 beds, would stand thus for 1000 sick:
| Wards with 9 beds | £427,775 | |
| Wards with 25 beds | 231,000 | |
| Saving | £196,775 | |
| Deduct cost of Netley, already incurred | 119,000 | |
| Saving from abandoning Netley | = | £77,775 |
The cost of the administration per 1000 beds at Netley and Aldershot would stand as follows:
| Netley | £427,775 | |
| Aldershot, pavilions, with 3 superimposed wards and 25 sick in each, would require 3 Orderlies and 1 Nurse[14] to each ward, and would cost £264 per bed in perpetuity, or per 1000 sick | 264,000 | |
| Difference of cost in favour of Aldershot | £163,775 | |
Some abatement would have to be made, as regards the cost of Netley, as there are a few wards with 16 or 18 sick.
If we take money at 4 per cent., the calculation will be as follows:
| Small wards, 2 Orderlies and a third of a Nurse, at £50 per annum; money at 4 per cent., per 1000 sick | £324,000 | |
| Wards of 30. 3 Orderlies and a Nurse, money at 4 per cent., per 1000 sick | 166,000 | |
| Extra cost of small wards | 158,000 | |
| Cost of Netley | 119,000 | |
| Saving in giving it up | £39,000 | |
13. Floors.—In building a new Hospital or laying a new floor we shall hope to see, by degrees, everywhere introduced the only safe Hospital floor. In the expense the difference between oak and the best white deal ought never to be considered. The staircases and passages should always be of stone. When once an oak floor is well done with bees’-wax it is no longer an absorbing surface. There cannot be a doubt that the frequent washing of the floors, in London Hospitals, is one main cause of Erysipelas and Hospital Gangrene.
But, with regard to deal flooring,—
(1.) The best way with a pine floor already laid is to close the joints, plane the surface quite smooth, and then saturate the wood with beeswax and turpentine, either at once, or after the wood has been saturated with “drying” linseed oil well rubbed in.
(2.) Enough beeswax should be used to fill up the grain of the wood, and rubbing with a brush will then smooth the surface. It will be polished somewhat, but not slippery. The amount of polish depends on the brushing.
(3.) The surface should be kept clean by using a brush with a cloth tied over it, and if offensive liquids are spilt, they should be immediately removed, the surface washed with soap and water, and immediately dried.
(4.) List slippers, which ought to be part of Hospital furniture, effectually obviate risk of slipping. It would hardly be possible, however, to make deal floors as slippery as oak parquet, because the surface (except of very fine deal, such as is used for musical instruments) never takes so high a polish.
(5.) Dry rubbing, which is done with sand, or with sandstone, is not well adapted for ordinary sick wards, on account of the dust; unless it be very carefully done. The rationale of it is to remove a certain amount of the surface of the floor. It answers very well on board ship. A certain amount of surface cleaning may be done by rubbing with a hard short brush; it is, however, defective. The wood becomes in time saturated with organic matter, and only wants moisture to give off noxious effluvia.
(6.) Scrubbing is absolutely objectionable, for this reason. In any schoolroom, reading-room, institute, which is much inhabited, a smell, while the floor is being scrubbed, is very perceptible, quite different from that of soap and water. It is the exhalation from the organic matter which has entered the[43] floor from the feet and breath of the inhabitants. How much more dangerous this in Hospital Wards need hardly be said.
There is at Bethanien Hospital, at Berlin, a very admirable flooring, which would be worth trying in England. The floors throughout are wood, prepared in the following manner:—The floor is first oiled with linseed oil, and then rubbed over with a peculiar “laque” varnish, the technical process of which will be found in the note,[15] and polished, so as to resemble French polish. Every three years or so the rooms and wards are successively emptied for a fortnight, when a new flooring is laid, re-oiled, varnished with the laque varnish, and thoroughly dried. Every day the floors are wet-rubbed by means of a piece of sacking or coarse webbing at the end of a long, hard broom, the performer stands for the performance, also while immediately afterwards, having wrung the sacking completely dry, she goes over the ground again with the dry sacking. One, or, in case of the weekly extra wet-rubbing, two dry rubbings, dry the floor completely in a few minutes from the cessation of the wet-rubbing, never more than ten minutes. Three or four times a year the ward floors are thoroughly wetted with water thrown on, and the floors scrubbed with a long brush. Nei[44]ther soap, soda, &c., is used.
The great advantages of this are:—
(1.) That it purifies the air exceedingly and freshens the wards.
(2.) That it reduces the daily accumulation of dust to a minimum.
(3.) That it dries completely within ten minutes from being wet-rubbed.
(4.) That a woman, standing, can thoroughly clean a ward with some hours less time, and greatly less fatigue, than scrubbing.
(5.) That wet scrubbing is sometimes and ought to be always forbidden and dry rubbing substituted, on the score of the unhealthiness of scrubbing.
(6.) That it would relieve us of all external scrubbers in the Nurses’ own rooms. Each Nurse would sweep, wet-brush and dry-brush her bed-room and day-room herself, daily, would once-a-week give a little extra wash, and would wash the wooden skirting which runs along the bottom of the walls. As the bed-room must be tiny and the day-room small (it would be better if we could keep to one room, which would take a quarter of an hour daily, and the grand weekly purification not more than one hour, even to a slow performer) a short time daily and a moderate time weekly will do it.
One disadvantage of this very simple, very efficient, and excellent flooring is, that it shows scratches. Furniture must always be lifted, not dragged. In a Military Hospital where men are always at hand, this would matter less as to the wards, and the Nurses could help each other once a week in their bed-rooms, and manage alone in their day-rooms.
There are four other examples of this flooring in Berlin Hospitals.
(1.) Bethesda Siechenhaus, a small old house, about to be rebuilt and enlarged, in a suburb of Berlin, where three Deaconesses, with a man and woman servant, take excellent care of about forty infirm old women and imbecile children. These patients, of the class to be found in the infirmary wards of our workhouses, move about little, and have few visitors, so that the flooring, which is the same as at Bethanien, is less used.
(2.) St. Hedwig’s Hospital, where 250 male and female medical and surgical patients are nursed by Roman Catholic Sisters of St. Charles Borromæus (head quarters at Nancy), with female servants and male nurses. The house is new; the flooring the same as at Bethanien. The Superior, an intelligent German, speaks much of its excellence for hospital purposes; it is being introduced, though as yet very partially, into France.
(3.) The great Charité Hospital, the town-hospital for 1,200 patients, spite its French name. It consists of two buildings; the old one, used in winter; and a splendid new one, into which all the patients, except the lunatics and the small-pox and the venereal cases, are moved for the six summer months. The flooring throughout is of the same wood (deal) as at Bethanien, but has much more laque. The more laque is used, the brighter the floor shines, but the sooner it requires re-oiling and laque varnishing. The Charité floors are re-oiled with laque every year; they are cleaned in the same way as at Bethanien, only with more dry rubbing. On bad days, when the numerous students have passed through, the ward floors occasionally require to be cleaned; but, in general, even on these occasions, it is enough to sweep them, and to clean the next morning as usual.
(4.) The principal Military Hospital, the Garnison Lazareth in the Hirsch Allée, for 800 patients, usually not filled. The flooring is the same as at Bethanien, except that no laque is used. It is oiled generally, not always, yearly.
The Ober Inspector, a Landwehr civilian, who is supreme over the Hospital, and an Ober-Stabs-Arzt, both speak very strongly as to the superiority of this flooring over all others for Hospital use, and in particular over flooring which requires scrubbing. It has only been introduced of late years. They consider it equal to any amount of hospital wear and tear. The military patients, like those of the Charité, Bethanien, and St. Hedwig’s, wear hospital slippers, with soles thick enough to admit of their walking in the garden, when fine; when not fine, they are not allowed to go out. This flooring would not stand the constant tread of nailed shoes. But often, on bad days as on fine ones, great numbers of soldiers come to visit their sick comrades, and leave[46] the floor very dirty; generally it is enough to sweep the floor after the visitors are gone, and to clean it as usual next morning; sometimes it is necessary to clean it the same afternoon.
The flooring is cheap. Somewhat more expense attends laying it down than the ordinary boards, and a certain expense attends the re-oiling, but the constant outlay for soap and soda is entirely saved, except a little soda in the grand annual purification, with hot water, in addition to the daily one with cold; the time and labour attending scrubbing is saved, and above all the great gain to the sick arising from its use is secured.
The strong, decided way in which the old grey-headed Army Surgeon, and the middle-aged business-looking Civilian, spoke of the merits of this flooring, and of its capacities, was exceedingly satisfactory.
(5.) Two years ago the greater part of the boards in the Kaiserswerth Institution, which are of deal, were oiled, both on sanitary grounds, and to rid the Sisters of the drain on time and strength in scrubbing. They are considered far preferable to the old ones, and to answer in every respect. Yet the Kaiserswerth floorings would not answer the English requirement of extreme cleanliness. They are substantially clean, but, like those of the Military Hospital of Berlin, it takes examination to ascertain that they are so, and from the same cause—there is no “laque.” Also the colour is not at all so agreeable as the Bethanien colour. These oiled boards last a year only. A moderate amount of laque is required to add to their durability.
The sum of the information, condensed as much as possible, on this subject is;—
I. The boards, which are always of deal, can be prepared in three ways:
(I.) Laquering, only suitable for reception rooms, or when by some chance a ward is wanted to be got ready in a hurry; it takes less time; after two or three days, the room or ward can be used, and it shines brighter, but it lasts a much shorter time than the other procedures, as it stands less the incessant treading incident to all ward floors; it is also more expensive. Let us consider it wholly unsuitable for wards.
(II.) Oiled boards, with more or less laque.
The Charité boards have a great deal of laque.
The Bethanien and St. Hedwig’s boards much less.
(III.) Oiled boards without any laque—
As in the Military Hospital.
II. Much laque makes the floors shine brighter; requires more time to clean them; and earlier re-preparation than where less laque is used.
The Charité boards would be unmeaningly splendid for an English Hospital, and quite out of place in a Military one; besides entailing some unnecessary annual expense, and some daily finicking care.
III. A small quantity of laque, as at Bethanien, gives an amount of polish to the floors, which enables the eye at once to ascertain whether they are clean or not; considerably improves the appearance of the floor; and, according to all high authority, adds both to the durability of the floor, and the healthiness of the Hospital. It renders the whole flooring less subject to cracks, to dirt and dust getting into holes and corners; and, above all, by filling up the grain of the floor, it prevents the saturation, by organic matter, which otherwise takes place and which scrubbing only makes more mischievous.
IV. Where no laque is used, the absence of all polish on the dark-brown floors makes examination necessary, to see whether they are thoroughly clean or not. This flooring would never satisfy the eye or the mind of an English Inspector-General or Surgeon. But the main objection to the absence of laque certainly consists in the sanitary one above stated.
V. All the various authorities agree in estimating very highly the superiority of this flooring to flooring requiring scrubbing. They all agree in their reasons for this preference, viz.:—
(I.) The dampness which remains in a ward more or less time after it has been scrubbed, is completely avoided.
(II.) The tendency to miasma is greatly counteracted, both by getting rid of the damp, which encourages and spreads the exhalation of the organic saturations; and by making the floor impervious, preventing dirt, and with dirt miasma, finding its way into holes, chinks, and corners of the floor.
(III.) The mode of cleaning this flooring, w[48]hile it avoids damp, daily purifies the ward air.
(IV.) The floor, and its mode of cleaning, get rid more than by any other way of dust, and of the miasma dust often conveys.
(V.) The time, labour, and expense of scrubbing are saved.
(VI.) The Berlin authorities consider that these oiled boards, with a small quantity of laque, are, on the whole, decidedly cheaper than the common boards; that the boards last rather longer; and that the avoidance of scrubbing saves more than the extra preparation and its renewal cost, apart from the sanitary gain.
VI. Against these advantages, the following disadvantages are to be placed:
(I.) This flooring shows where most used, instead of the uniform appearance of the white scrubbed boards.
(II.) Scratches show, and remain upon it; so all furniture must be lifted, not dragged over it.
(III.) The tread sounds a little more, little, but more, than on white boards.
(IV.) It would not stand the constant tread of nailed shoes; and patients of a ward so floored, ought to wear slippers with moderately thick soles. (The German Doctors consider the use of slippers preferable to that of shoes, by the patients, as keeping a ward much quieter, cleaner, and disturbing the severe cases less.)
(V.) Carpets could not be nailed on it, as the floor should be daily cleaned. Several Hospital authorities whose rooms are thus floored, have large pieces of carpet round the furniture most used, bed, tables, sofas, &c.; these are daily taken up and dusted while the floor is being cleaned. To many English minds, the sight and feel of a carpet is essential to the idea or feeling of comfort; and it might be sound policy, in the event of a trial being made of this flooring, to leave the Officers, Military and Medical (I do not mean patients), in possession of scrubbed rooms and carpets. The Superintendent might have one or two pieces of carpet for her rooms; and the Nurses should dispense with carpet.
Both in the new part of the Charité and at Bethanien, long broad corridors run along the back of the wards which open into them. The corridors are floored like the wards. In those of the Charité a piece of long carpet is laid in the midst of the corridors, where patients walk not a little. At Bethanien, a[49] long piece of matting is laid in the midst of the corridors, where the patients walk freely. Carpet of either kind is not considered to benefit the floors, but to diminish the noise. In the wards of Guy’s Hospital, for the same reason, a long piece of matting is laid along the middle of the floors.
VII. This flooring is unsuited for stairs, though so used in some Hospitals, as, in case of fire, oiled wood would burn rather quicker than common wood. Hospital stairs should be of stone.
VIII. It is also unsuitable for kitchens, wash-houses, water-closets, and sinks. The floor round a stove or fire-place in a ward or room should be protected by a strong plate of lead or tin.
It might also be as well to floor operation-rooms with flooring, admitting of scrubbing, because these oiled boards do not well stand sand or bran, and our Surgeons might be discomposed at missing one or other of these things. Sand or bran mixed with blood would make a mess, the traces of which would show a little on this flooring. For the rest, it is particularly easy to wipe blood off it. After each operation, one or two minutes, a wet cloth of the kind here mentioned, and a broom, remove the blood that has fallen, and leave a clean floor; or if there has been a very great mess, five minutes, a wet cloth to lap up the blood, &c., another wet cloth, a pail, and a broom, do all: after the operations are over, a few minutes’ whole or partial cleaning, as the case may be, make all tidy again. Still, many English Surgeons expect to have sand or bran thrown on the floor before, or just after the first blood has fallen, and might object to standing some minutes on the bloody floor, which spoils boots, &c. Red floorcloth, of sufficient size, round the operating-table, might answer every purpose.
IX. On laying down the oiled boards for the first time, six weeks should pass after the oiling and laquering before the ward is inhabited.
X. After subsequent re-preparation of the floors, the longer the wards are left vacant the more the floor both hardens and shines; but for practical purposes the interval of a fortnight is enough.
XI.[50] The flooring, so prepared, or re-prepared, ought, on an average, to last about three years. In case of any extra miasma, it is often desirable to hasten the re-preparation, and to have it done after two years’ use. To do it annually is, unless in some emergency, quite unnecessary.
Although the process cannot be said to be by any means perfect, on account of the deficient durability of the surface, it would be well worth while to try it in England, and, if it answers and if it were improved, the sick would gain much, and the Hospital staff would gain much—the latter much more even in Civil, than in Military Hospitals.
But it would be incurring a great responsibility to have the whole of a large new Hospital floored in this way, because,
I. An English climate has made, and makes, so many things which are good and suitable abroad, unsuitable and sometimes pernicious for England.
II. Our coal-fires, whether assisting or assisted by our atmosphere, certainly give us an amount of soot and dirt unknown abroad. At Berlin, all fire-places are stoves, where sometimes coal, sometimes coal and wood are burnt.
This flooring might not stand well either the damp climate, or the smoky atmosphere and amount of flying soot of England: but it would be well worth trying; as also trying to improve it.
By all accounts, a great deal depends upon the manner in which these boards are prepared; a little more or a little less, whether of oil or laque, makes a great and lasting difference. It would never answer to make an English carpenter or painter do this from written or printed directions.
If we obtain a trial of this floor—the best course would be, to let an English carpenter prepare a number of boards and skirtings, of due size, suitable for the new flooring of some few wards in one of Her Majesty’s hospitals, which requires new flooring; then to desire either the proper tradesman, or the Queen’s Minister at Berlin, to order the house-painter, Schonby, No. 5, Michael Kirchplatz, Berlin, to send an experienced, trustworthy foreman, with the proper tools and materials, and for this man, with a complement of English workmen, to prepare the boards.
The mode of cleaning is extremely simple, though of course there is a knack to be learnt; and, like everything else, it can be done well, indifferently, or ill. Any English man or wo[51]man accustomed to cleaning would understand the thing in one morning, and would, if he or she opened instead of shutting the mind to the outlandish thing, be proficient in it in a week. All these things sound abstruse on paper, and are far more simple and more easily learnt by seeing done than by reading. The foreman ought to give one or two lessons to one or two Orderlies, or Nurses, as the case may be.
14. Ventilation.—The amount of fresh air required for ventilation has been hitherto very much underrated, because it has been assumed that the quantity of carbonic acid produced during respiration was the chief noxious gas to be carried off. The total amount of this gas produced by an adult in 24 hours is about 40,000 cubic inches, which in a Barrack room of 16 men would give 370 cubic feet per diem. Allowing 8 hours for the night occupation of such a room, when the doors and windows may be supposed to be shut, the product of carbonic acid would be 123 cubic feet, or about 15½ cubic feet per hour. This large quantity if not speedily carried away would undoubtedly be injurious to health; but there are other gaseous poisons produced with the carbonic acid which have still greater power to injure. Every adult exhales by the lungs and skin 48 ounces or 3 pints of water in 24 hours. Sixteen men in a Barrack-room would therefore exhale in 8 hours 16 pints of water and 15½ cubic feet of carbonic acid in the atmosphere of the room. With the watery vapour there is also exhaled a large quantity of organic matter ready to enter into the putrefactive condition. This is especially the case during the hours of sleep. And as it is a law that all excretions are injurious to health if reintroduced into the system it is easy to understand how the breathing of damp foul air of this kind, and the consequent reintroduction of excrementitious matter into the blood through the functions of respiration will tend to produce disease.
This will be still more the case in sick wards overcrowded with sick, the exhalations from whom are always highly morbid and dangerous, as they are nature’s method of eliminating noxious matter from the body, in order that it may recover health.
A much larger mass of air is required to dilute and carry away these emanations than is generally supposed. And the whole art of ventilation resolves itself into applying in[52] any specific case the best method of renewing the air sufficiently, without producing draughts or occasioning great varieties in temperature.
When the question of ventilation first assumed a practical shape in this country, it was supposed that 600 cubic feet of air per hour were sufficient for a healthy adult, in a room where a number of people are congregated together. Subsequent experience however has shown that this is by no means enough. As much as 1,000 cubic feet have been found insufficient to keep the air free from closeness and smell; and it is highly probable that the actual quantity required will ultimately be found to be at least 1,500 cubic feet per hour per man. In sick wards we have more positive experience as to the quantity of air required to keep them sweet and healthy. It has been found in certain Parisian Hospitals, in which the ventilating arrangements were deficient, that pyœmia and Hospital gangrene had appeared among the sick in consequence. These diseases disappeared on the introduction of ventilating arrangements, whereby 2,000 cubic feet of fresh air per bed per hour were supplied to the wards. Notwithstanding this large quantity, however, the ward atmosphere was found not to possess sufficient freshness or purity: and the quantity of air had to be increased in subsequent ventilating arrangements. As much as 4,000 to 5,000 cubic feet per bed per hour have been supplied in certain Hospitals. At the rate of 4,000 cubic feet, the ward atmosphere is found perfectly fresh.
At one of our largest London Hospitals it will be perceived that above the one door of each ward is a large ventilator, ordered to be open day and night—that beyond this ventilator, which opens into the landing-place, is a large window which opens into the external air; and thus admits fresh air into the ward at night, diminishing the foul night atmosphere. This night ventilation system is good; but it requires careful watching, as chilly patients, Nurses, and sometimes Sisters, are very apt to give, after they conclude the rounds are over for the night, a sly pull at the rope and to shut the window, and thus imbibe the foul air directly generated, in quiet.
15. Special Wards.—It may be laid down as an axiom in the management of sick affected with certain zymotic diseases, such as fevers, cholera, dysentery, &c., that they should be distributed over a wide superficial area, and have a large allowance of cubic space. Agglomeration of such cases in small ill-ventilated wards is quite sufficient of itself to occasion a high proportionate mortality among the sick. In mild climates and seasons very little protection is necessary from the change of temperature; so that the sick from epidemic diseases can be camped out and exposed to the full influence of the atmosphere, not only without danger, but often with great benefit. It is only when the temperature is low and variable, and the season inclement, that danger is likely to accrue from this exposure. And hence the necessity of inquiring how we can best combine the requisite elevation of temperature and the most suitable amount of cubic space and ventilation for the treatment of these diseases in Hospitals.
Medical Men generally are satisfied that these ends cannot be safely arrived at by agglomerating sick in fever wards in Hospitals. And hence has arisen a practice, which experience appears to have approved, of intermingling a small number of fever cases in wards containing a certain number of sick from other diseases. The practice appears to be not only perfectly safe, but advantageous for the sick. It is known, however, that if the proportion of fever cases exceeds a certain number, the other cases in the ward are apt to become affected with fever. It would appear as if, so far as the fever is concerned, the cubic space occupied by other diseases was to a certain extent available for the use of the fever cases. But the proportion of such cases, that can be advantageously placed among the general sick of any ward, will depend upon the size of the ward, the means of ventilation, the number of cubic feet per patient, the position of the windows, the exposure of the building, and other similar circumstances.
Again, it is doubtful whether the preservation of an uniform temperature in any Hospital, even in one set apart for chest complaints, is beneficial for the sick, or whether it be beneficial to agglomerate consumptive cases, without very special precautions, under the same roof. Without discussing the validity of the opinions held in Southern Europe as to the contagious nature of consumption, it may be very fairly doubted[54] whether a number of cases placed under a common roof, and breathing a common atmosphere, would not yield a higher rate of mortality than the same cases would do if distributed through the wards of a well-ventilated Hospital, among other diseases.
The subject is worthy of examination. At all events the phenomena observed in this disease in the warmer climates of Europe have led to the popular belief above stated; and it would appear to point to a higher rate of mortality as a not unlikely result of the establishment of special Hospitals or wards for consumptive diseases, unless extraordinary care were taken to ventilate them properly, and to imitate the natural variations of temperature which appear to be necessary for recovery.
16. All salaries and wages of Matrons and Nurses should be paid, on the Superintendent-General’s order, from the Hospital chest, to the Matron, who should pay the wages and other expenses of the Nurses, and account for all monies received by her on such orders. All outfits and travelling expenses, in cases of transfer, &c., should be provided on the order of the Superintendent-General.
There would be considerable difficulty in the way of making all payments at a distance to Nurses, direct from the Superintendent-General, otherwise than by orders on the Hospital chest or Treasury. But there can be no doubt that the Nurses ought to be paid by the Matron and by no one else. The service of Nurses in Hospital is a peculiar service, and if not successfully conducted by influence never can be by coercive discipline. It would be a great mistake, therefore, to throw away any means of influence which we can command, and the “eye of the maid-servant is to the hand of her mistress” now as it was 2,000 years ago. The fact of paying and being paid helps greatly to establish the proper mutual relations between the superior and the subordinate. The Matron would draw from the Hospital Treasury, on the orders of the Superintendent-General, and would account to her. As a matter of discipline, it would make no material difference whether the orders of the Superintendent-General, in favour of the Matron, for the pay of the Nurses, are cashed by the Hospital Treasurer or by a banker, always supposing that the Tr[55]easurer is bound to honour those orders, as any other banker would.
The Matron, in any Hospital out of Great Britain and Ireland, should be able, with the concurrence of the Governor of the Hospital, to dismiss and send home any Nurse; or the Governor himself, on his own responsibility, may direct the Matron to do so, under appeal, however, in either case, to the Superintendent-General, who shall decide, after the arrival of the Nurse, whether she is to be dismissed or whether she may be placed in another Hospital.
It should be secured, not left to chance, that the Matron be immediately made acquainted with any complaint of the Medical Officers against a Nurse.
The Matron should be able to draw from the Purveyor, on her own indent, with the sanction of the Governor of the Hospital, such rations and extras as she may consider necessary for the Nursing establishment, and make the arrangements for cooking. In the United Kingdom the Matron should be able to make arrangements, subject to the approval of the Superintendent-General, for commuting rations for mess-money, not pay.
The Governor is responsible for the sufficiency of all supplies and none ought to be expended, without his sanction. This might be indispensable, if there were danger that supplies might run short.
Upon both these latter points, supposing the Governor of a General Hospital to exist, he must have power to maintain the discipline of the Hospital, in all its Departments, as a General commanding a division has, in regard to every regiment composing it. But he ought to exercise it only through the Matron, as commanding a corps. He must also have power to require the exclusion from the Hospital of any Nurse whose conduct he may find to be inconsistent with maintenance of discipline, and this power he would enforce, on his own responsibility, by directing the Matron to remove the offending Nurse from the Hospital. The conduct of the Nurse would become the subject of investigation afterwards, in terms of the established regulations. But practically such a case could hardly occur, unless by the fault of the Matron, who would, of her own accord, desire to remove a Nurse, on being satisfied that such a measure was necessary or expedient. It would be[56] proper, too, both for her own justification and for the maintenance of the Governor’s supremacy in the Hospital, that the Matron should obtain his concurrence in the removal of a Nurse from the Hospital. The proceedings, in all such cases, would, of course, be reported by the Matron to the Superintendent-General.
Whether the Governor has the power of removing the Matron, who clearly and properly ranks among the officers under him, should be settled and not left to be disputed about in a distant station. At all events, if he has this power over her, it must be guarded, as extending only to suspension from office, in cases of alleged flagrant neglect or misconduct, till the whole matter can be remitted and decided on by the Superintendent-General.
17. Generally, as to the question of wages and pensions, a regulation that Nurses shall have a small annual increase of wages is better than one giving an increase after five or three years.
Efficiency does not go by starts and springs, like grasshoppers, but makes “a small annual increase,” like the wages proposed.
Nay, I appeal to everyone with experience in these matters whether the greatest improvement is not made the first year, the second year a little less, and so on the third and fourth, till, when the fifth year comes, if improvement has not been made by that time, it never will be.
For trust-worthiness is the true efficiency of a Nurse. And it may safely be said that, if by the end of the first year she has not improved in trust-worthiness, she had better go; and if she have not almost reached her culminating point by the fifth year, she certainly will not improve afterwards.
The reasonable principle I believe to be, 1, to begin improving the wages at as early a period as possible; 2, to let them increase till the Nurse reaches her maximum of efficiency; and, 3, after that to make no more increase.
Because the object is to induce the young and efficient women to stay, not the old ones. They will stay long enough, because the old ones nobody else will take.
The rate of pension ought, on the other hand, to increase with the number of years’ service, and continue increasing till the end. The principle of pensioning is different from that of wages. After the woman has reached her maximum of efficiency, which certainly will be not later than forty-five, probably not later than forty years of age, the inducement to stay should be the improvement of pension. This compensates for any apparent injustice in the first principle towards an old servant.
No other system appears to be founded on common sense; and it is one generally acknowledged in the Civil Service, where salaries are made to rise as soon as possible. Military Hospitals must not be made training schools for Nurses; else it would be better to admit them much younger than at the age of thirty years.
If a Nurse cannot enter the Service till after she is thirty, the majority will no doubt be some years above thirty when they enter, say an average of thirty-five; and five years appear a very long probation for a person at that age before increase of wages begins. In most cases, in Civil Departments, there is only one year of such probation before increase begins, though the persons are much younger when they enter. A maximum might be fixed, beyond which the wages should not rise, and when the increase of pension would be sufficient inducement to remain. Very few Nurses can be expected to continue really efficient till sixty years of age; but it is often difficult to say that a person is disabled, though she may have become less active and efficient. If there is no retiring allowance there will be great reluctance to dismiss her, and it might, in that case, be cruel. The better plan would be to promise a small pension after ten or twelve years’ service, on a scale so graduated thereafter as to offer an inducement to remain, at the same time that it would afford facility for enforcing retirement without injustice. This would be economy. The “Nursing Sisters” grant £20 after twelve years’ service.
After a time there may probably be difficulty in dismissing persons who have done good service for ten years, but have declined in efficiency, unless there is a retiring allowance. They may be reluctant to retire; and, if so, it would be a[58]lmost impossible to dismiss them, without some kind of provision. This is a difficulty which is encountered in every employment in which there is no such provision. Persons who can hardly be said to be disabled but who have become less efficient are retained, because, if dismissed, they have no means of livelihood.
I have consulted the best authorities upon these points; and I find the following general principles admitted:—
General Principles as to Wages and Pensions.
(1.) At whatever age a Nurse enters the Service she shall begin with the same salary.
(2.) The annual rate of increase shall be the same for all ages of entrance.
(3.) The maximum salary shall not exceed £ .
(4.) The pension for service shall not begin until ten years of completed service.
(5.) The amount of pension shall be a certain percentage on the salary during the year preceding that on which she is pensioned.
Applications of the foregoing Principles.
(1.) That the wages of Nurses shall rise annually, for a definite number of years, attaining their maximum, on an average, at the age forty-five, when the Nurses are found to be most efficient.
(2.) That, after five years’ service, the Nurse shall, in the case of ABSOLUTE DISABILITY, become entitled to a pension during the period of her disability.
(3.) The pension will be on a scale graduated on the wages. It will be twenty per cent. of the annual wages in the year of service, 5–6, and the rate to be granted will rise progressively two per cent. per annum, until the rate on the wages becomes seventy per cent.
(4.) All Nurses will be placed on the Retired List at the age of sixty.[16]
(5.) Those Nurses who are pensioned at an earlier age, for disability, will, if called upon, be liable to serve when that disability ceases, or to forfeit their pension. They must therefore bring an annual medical certificate of disability to the Superintendent-General, in order to receive their pension.
(6.) Nurses who are partially disabled will only be entitled to a certain proportion of the pension allowed in the scale, to be determined, on representation made by the Superintendent-General.
Example.
| Age. | Completed Years of Service. | Wages. | Pension. | |
|---|---|---|---|---|
| 30 | 0 | £20? | Gratuity | |
| 31 | 1 | 22 | Gratuity | |
| 32 | 2 | 24 | Gratuity | |
| 33 | 3 | 26 | Gratuity | |
| 34 | 4 | 28 | Gratuity | |
| 35 | 5 | 30 × ·2 = | £6 | |
| 40 | 10 | 40 × ·3 | 12 | |
| 45 | 15 | 50 × ·4 | 20 | |
| 50 | 20 | 50 × ·5 | 25 | |
| 55 | 25 | 50 × ·6 | 30 | |
| 60 | 30 | 50 × ·7 | 35 | |
These principles, if admitted, would suggest the following heads for regulations as to Nurses’ wages and pensions:—
(1.) At whatever age a Nurse enters the service, the amount of wages paid to her during her first year of service, will be £20.
(2.) There will be an annual rate of increase of wages equal to 10 per cent, of the first year’s wages, until the yearly wages amount to £50, beyond which there will be no further increase.
(3.) A pension will be awarded for service to any Nurse, who may retire, on account of age, at the expiry of ten full years’ service, but in case of disability, a Nurse shall receive a pension after five years’ service, or a gratuity, according to circumst[60]ances, if discharged for disability, before she has completed five years of service.
(4.) Rate of Pension. The pension will be on a scale graduated on the wages. It will be 30 per cent. of the wages received by the Nurse in her tenth year of service, and the pension granted to Nurses who have served more than ten years, will rise at the rate of 2 per cent. of the wages for every additional year of service, until the pension amounts to 70 per cent. of the wages received during the year preceding its grant, beyond which no higher pension will be granted, except in cases of special devotedness to the public service, when an addition to the regulated rate of any pension may be granted on special recommendation, made by the Superintendent-General of Nurses, setting forth the nature of the service for which such augmented pension is to be granted.[17] But no such pension shall exceed the amount of £50.
(5.) Any Nurse pensioned for disability, may be called on for service in the event of such disability ceasing before the age of sixty, in which case her wages will be the same as they would have been, had she not been disabled.
(6.) Every Nurse who has completed her sixtieth year, must retire from the service on her rate of pension.
(7.) Any Nurse, temporarily or permanently disabled in the service, who has served more than five and under ten years, will be entitled to a lower rate of pension, according to the circumstances of each case, as represented by the Superintendent-General.
18. Nurses should be selected and appointed by the Superintendent-General of Nurses for each General Hospital, in a proportion not exceeding one nurse for every twenty-five[61] cases.
There is nothing so fatal to discipline as to require by regulations what it is known and admitted cannot be performed. Such rules are made to be broken. Therefore, is it not better, instead of fixing a number to fix a limit, and say “not exceeding one to every 25 or 30 patients,” leaving it to the Superintendent-General to economize Nurses, and not appoint the full number permitted, unless when really necessary? In one case she might consider one nurse for fifty or even sixty sufficient; in another, one for every twenty-five might be few enough. Why tie up her hands against economy as well as against extravagance?
At the same time it is necessary to state—
(1.) That, by all accounts, at home and abroad, in the English and in foreign armies, the proportion of severe cases is very considerably less, in time of peace, in a Military Hospital than in a Civil one, especially in the surgical wards.
(2.) That the Nurse’s time, being relieved of the waste incurred by fetching and waiting for things, the cleaning of the ward being done by Orderlies, and, an important item, the Ward-Master being responsible for the serving the patients’ food, twenty-five sick are not enough, on an average, to occupy, properly, her time.
(3.) That idleness, always pernicious, is never more so than to Hospital-Nurses.
(4.) That petting the patients, by way of filling up time, would be, of the two, more pernicious than idleness.
(5.) That it is most important, apart from these reasons, to train and accustom these Nurses to serve efficiently large numbers of patients, so as to make them useful in war-service, where every woman who can be spared is better away; and where a small efficient staff would, please God, do excellent service.
(6.) That it is not in human nature, taking its average, supposing the Regulations lay down that the proportion is not to exceed 25, for many Nurses not to murmur at having more; whereas they ought from the first to understand, that the service is a very laborious one, and that none but women able and willing to undergo and render laborious service, ought to enter it, or be suffered to remain in it.
(7.) Care must be taken therefore that in fixing this minimum, no use may be made of it dangerous to the service, either in the Hospital work itself, or in provoking adverse criticisms upon these Regulations in quite different places. Twenty-five cases are not generally enough.
19. It would be expedient to take the advice of an able and honest man of business as to whether the Superintendent-General should, on engaging a Matron or Nurse, have her signature to a bond or not. On the one hand, we know what bonds are to loose consciences, and if the promulgation of the Regulations give undoubted power to the Superintendent-General and to her Matrons on foreign stations, I should prefer having no bond. But this is for a man of business to answer. It is important to remember that the power of instant dismissal for misconduct, and of sending the Nurse home must be retained, which renders the service different from ordinary female service. A discharged governess or servant, if she insisted on remaining at her own expense at the foreign station, could not be sent home forcibly by her late mistress; now it is essential that an offending Nurse be forthwith passed on board the first returning ship. Also performances similar to those of one or two of the women in the War-Hospitals who, on hearing of good situations, misbehaved in order to be discharged, ought to be effectually prevented. A lawyer must advise, first, if it can be; secondly, how it can be done. The Superintendent-General, on sending abroad Nurses, ought to have some security either that they remain there and do their duty, or that they be sent home for her judgment if they fail in duty. To have them either going abroad as Nurses by way of securing a free passage, and then looking out for lucrative situations, or accepting the offers which might, and, occasionally, undoubtedly would, be made to them, would be most injurious to the Service. Can it be prevented by any stronger measure than the instant forfeiture of all claim to the eventual pension? If so, it should. Could this power be extended to the washerwomen who would probably be sent with the Nurses ordered to War or out-of-the-way foreign stations? Perhaps it will simplify things not to include them in the Regulations.
The persons provided by the Officer, whoever he may be, to attend to the hospital linen under the orders of the Matron, will be pretty sure to give the Matron trouble. But it is much better to begin very modestly, and to avoid alarming the Attendance Department; and so to be content with the people provided in the linen store, and not at all to invade the regions of the kitchen. By degrees, please God the work prospers, it may be extended. I fear a laundry of men, except in war-service, will be a costly and inefficient concern. Yet a laundry of women, exempt from the control of the Matron, would be probably the worse evil of the two. And it is both right and expedient to move very slowly, and to begin with the nursing service alone. Ultimately, if we invade both laundry and kitchen, I should still wish, in both, to have as few women as possible. The fewer women are about an Army Hospital the better.
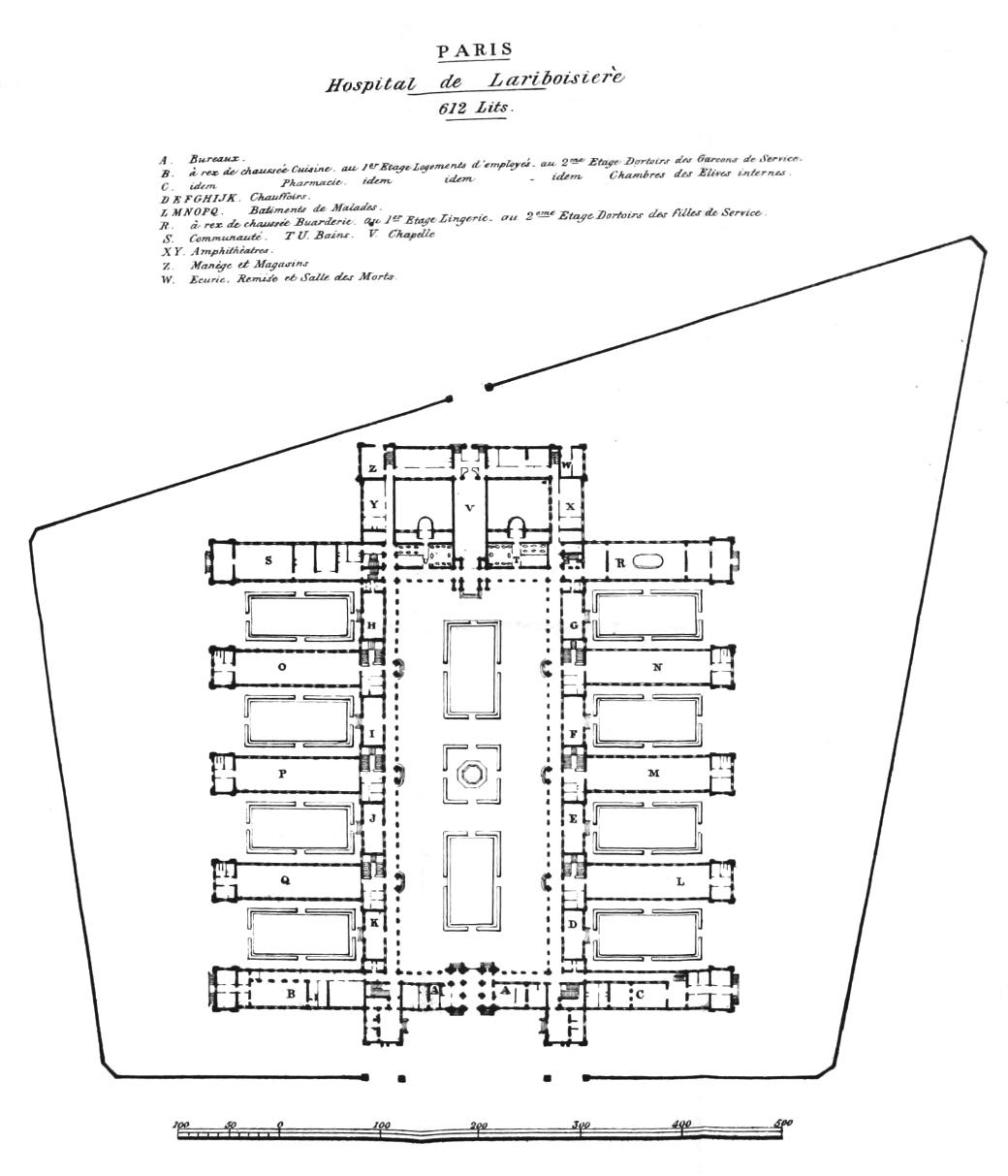
PARIS
612 Lits.
A. Bureaux.
B. à rez de chaussée Cuisine. au 1ᵉʳ Etage Logements d’employés —au 2ᵐᵉ Etage Dortoirs des Garcons de Service.
C. à rez de chaussée Pharmacie. au 1ᵉʳ Etage Logements d’employés —au 2ᵐᵉ Etage Chambres des Elèves internes.
D E F G H I J K. Chauffoirs.
L M N O P Q. Batiments de Malades.
R. à rez de chaussée Buanderie. au 1ᵉʳ Etage Lingerie. au 2ᵉᵐᵉ Etage Dortoirs des filles de Service.
S. Communauté.
T U. Bains.
V. Chapelle
X Y. Amphithèatres.
Z. Manège et Magasins
W. Ecurie. Remise et Salle des Morts.
1. In considering the Pavilion Plan to be in future received as the sanitary necessity for Hospital construction, we must look upon it as susceptible of many modifications.
And, particularly in adapting it for a Military Hospital, we must ask by what modification can it be made, 1. Most economical as to attendance, a greater amount of which is rendered necessary than by other plans of construction.
2. Easy as to supervision; and, of course, a Hospital spread over the extent of space now proved to be essential by sanitary knowledge, whether built on the Pavilion plan or not, must multiply the amount of supervision over that required in the concentrated over-crowding of the old Hospital system (over-crowding not with regard to cubic space in the wards, but to the superficial area on the ground).
3. Economical as to the number of sick to be accommodated on the same floor, so as to save unnecessary waste of time and strength on the stairs to both Ward-Masters and Nurses. Each Nurse should have, in time of peace, not less than from 50–60 patients under her charge.
4. Efficient as to convenient ac[64]commodation for Nurses and Ward-Masters, near to the wards of which they are in charge.
1. The Pavilion Plan, while it is incontestably superior, on sanitary grounds, to any other, while it perhaps may be made equally economical, with regard to building, is more expensive than the older crowded and badly-constructed Hospitals, not only as to ground, but because each separate entrance, staircase, set of appurtenances, represents an additional cost of materials, and of hands to keep them clean and in order. Human life is, however, a more expensive article than any other. If human beings, and especially sick human beings, are to be spread over as much space as possible, which is now known to be an essential to health and more especially to recovery, this must be done under any system and can be best done under the Pavilion system. It of course necessarily entails a greater amount and cost of attendance and of supervision. Pure air and light are the prime necessities of a hospital. These are best secured by the Pavilion Plan, and therefore it is the cheapest in the end. As to the hands, there never ought, never will, never can, be a superfluity of hands in a well-regulated Hospital. The duty of the hands consists of two parts—to keep the Hospital clean; to attend the sick. I had rather not enumerate the instances where I have seen that, often from the most various causes, one result arises—that more time and care is given to floors, stairs, &c., &c., &c., than to the sick. Extreme cleanliness is of vital importance; this should be combined with extreme simplicity of detail, and with providing for considerable numbers at once. You can effectually clean a large ward in much less time than two small ones; a long stair than two short ones, &c. Extreme, not finicking, cleanliness, thorough ventilation, for which an ample supply of opposite windows will certainly in the long run prove infinitely the best plan, and careful nursing, are probably the main conditions, humanly speaking, of a large proportion of cures—subsidiary to the medical or surgical treatment.
Sanitary necessities are never to be rejected, on account of the trouble they give or of the means of cleanliness which they render necessary. Because the saving of life, not the saving of trouble, is the object of all sanitary appliances, Hospitals among the number. And the saving of life is the only real economy. If you have saved “hands” and trouble, and lost life, you have been extravagant. The object is not to banish appliance[65]s which will cost trouble in keeping them clean, but to discover those appliances which can be kept clean, at least cost of labour. And this is perfectly possible.
2. The Vincennes modification of the Pavilion plan has been adopted, among other reasons, for the greater facility of supervision it affords. The Military Superior, the Surgeon, the Matron, can at any instant pop in upon any ward of a Hospital which has one roof. Each pavilion may, unless the matter be specially considered with a view to providing this effectual supervision, perceive the approach of any inspector. The system of scouts, watch, alarm, is well understood in many hundred wards, whose patients would be puzzled to give the things names. Military patients will know both things and names. Remember that Ward-Masters, Orderlies, and Nurses require inspection as well as patients. Whatever system of Hospital construction is adopted should provide for easy supervision, at unexpected times.
3. The more we see of different systems, the more we see the great mistake of giving a Nurse too little to do.
Twenty-four ordinary sick or surgical cases are too few for a Head Nurse.
In a Military Hospital, the proportion of heavy cases is in ordinary times considerably below the average proportion of such cases in a Civil Hospital, open, as the latter is, to accidents, and to the cases of dangerous disease always more or less rife in low and crowded neighbourhoods.
Upon an average, a third or a fourth of the cases in the ordinary surgical wards of a Military Hospital will be ulcers from causes honest and dishonest. What these men will require is rest (the cleanliness which is often so irksome a novelty to the corresponding Civilian patient is routine to the soldier), and very simple treatment.
It is most important, if possible, to form a staff of active, laborious, useful women, who, if ordered on war-service, can at once cope with numbers, and serve efficiently a considerable number of heavy cases.
Relieved of all cleaning, and relieved of the great loss of time incurred by fetching, waiting, &c., &c., none of these Nurses, who are, in fact, Head Nurses, should serve less than forty men. And, as I before submitted, I had rather she ser[66]ved fifty or sixty than forty.
Give them twenty-four patients, and either they will become idle, finicking women, or they will take to petting the patients, a thing to be sedulously avoided everywhere, most of all in Military Hospitals.
4. The more we see of different systems, the more apparent becomes the importance of the Head Nurse (all these are Head Nurses) sleeping close to the ward:—
As regards the efficiency of her service:—
As regards the saving her own time, strength, and securing her a modicum of comfort in a work where, if she does her duty, she will never have a superfluity of comfort. Time, strength, and this modicum of comfort, enter much into a Nurse’s health—and health is essential both for efficiency and economy.
Where the Nurse sleeps at a distance from her ward, her efficiency, both as to superintendence and work, especially at night, in dangerous cases, is seriously impaired.
If she sleeps at a distance from her ward, her comfort, also, such as it is, is destroyed. Whatever a Nurse does for herself, she must do by fits and starts. A really efficient Head Nurse is never able to make anything for herself, though she often would far rather save the money it costs to “put it out.” The most simple mendings, even the feat of stowing away the laundress’ supply of a Saturday evening, become, when a ward is heavy, or when there are two or three of those cases of urgent danger, so many of which, by God’s blessing, the assiduous care of these women saves, year by year, in our Hospitals, a procedure done in several acts. The misery of dividing her small effects (the smaller the better) between a day-room and a distant sleeping-room, the unseemliness and inconvenience of carrying things backwards and forwards, cannot be described.
If it be possible, the Nurses must sleep adjoining their wards; and it will not do to give each only 24 patients.
It would be considerably better, if feasible, to have two Nurses in contiguous rooms; but in the Pavilion Plan this would involve bringing one Nurse away from her ward; and rather than this, the next best, though inferior plan is to put one Nurse immediately above and below the other, with a [67]distinct bell which she can in a moment ring from her bed into the other Nurse’s room, to summon her if needed.
Some years ago gas was laid on in the Sisters’ rooms in Guy’s Hospital. In the other Hospitals there is an allowance of candle to each Sister. The disadvantages of gas are its alleged unhealthiness and its certainly being disagreeable to some eyes. Its advantage is its cheapness. Liberty to buy a candle and not use the gas is allowed at Guy’s. As it will be a very important thing to conduct the Nursing Service as economically as possible, and as there must not be any wretched false economy as to essential matters, which in the end always proves waste, it will be well to save as much as can be in matters not essential. It would be worth while to ascertain the average amount of saving which the substitution of gas for an allowance of candle has effected at Guy’s. Gas is used in the wards of St. Bartholomew’s, St. Thomas’s, and Guy’s, day and night. It appears, when ventilation is properly attended to, to answer well, and to do no harm. At night the gas is lowered so as to leave the ward just light enough to see all that is done in it: if bleeding, &c. occurs, it can in an instant be raised, and the ward lighted up. London Hospital burns gas in the evening, and throughout the passages at night; but when the night watch begins at nine, the wards are dark, except the Nurse’s candle. A spare candle, un-lighted, is always at hand.
It is very important for the order of a ward that the attendant in charge, and also any inspector suddenly entering, should see at once all that is going on in the ward. Where there are dangerous cases, this is of great moment; and where there are not, it is equally necessary for the police of the ward. A candle or a rushlight give insufficient light. Properly lowered, gas at night does not disturb the patients. After a night or two, those who are accustomed to sleep in the dark get used to it. If the Nurse sleeps adjoining the ward, there must be sufficient light in the ward at night. If the gas-fittings are properly tight and if every gas-burner has a ventilator, so that the products of combustion are effectually conveyed away, for each gas-jet consumes as much air as eleven men, it would be greatly preferable that there should be a low gas light in the wards at night.
II.—1. Suppose the Lariboisière plan retained, as proposed at Aldershot, for a Military Hospital, with wards of twenty-four beds each—then, with fear and trembling, but with the firm conviction that it is better for human nature, most of all, for nursing human nature, to have somewhat too much than a great deal too little to do, I respectfully recommend that one Nurse serve the three wards of each Pavilion.
One woman cannot sleep alone in the Pavilion. The Nurses must sleep together near the Matron’s quarters. If the Nurses sleep away from the wards there should be some way by which a Nurse can at once be summoned, in case of any urgency in her ward, and it would be well to consider this in the distribution of quarters. Either the Matron should lock the Nurses’ quarters at night, and any summons should be brought to her and by her referred to the Nurse; or the summons should go straight to the Nurse’s door. There are difficulties both ways, even supposing these summons should be unfrequent. The Nurse of each Pavilion should inhabit the room on the ground-floor ward, where the heaviest surgical cases will be probably placed, whence she can better command the movements of the Pavilion, and attend the entrance of the Surgeon.
2. Her day might be something like this (in time, perhaps, God will bless us with some Army Chaplain who will get up early and give us a very short service morning and evening):—
She should be effective, and enter the Pavilion about 6 A.M., go through the wards, read prayers in one by turns at the appointed hour, and give out the linen wanted. (Six is the nominal hour when the Head Nurses of one great London Hospital enter on their duty.) Here must be no nominal hours, all must be real, though not overstrained. Then the dressings, &c., attendance on Surgeons, &c. With 72 patients on different floors, she must train the Orderlies to do the lighter dressings (by training I mean real teaching, not leaving the Orderly to find them out himself); she must see all the wounds of all her wards which she does not dress herself at least every other day (which she can do by seeing some in the morning and some in the evening), and she must dress the heavy cases of all the wards herself. All this, with method, and not losing time by fetching and waiting, an efficien[69]t Head Nurse can do.
She must be responsible for the linen of the wards; but this must be simplified as much as can be, so as to secure responsibility, yet relieve the Nurse of unnecessary time spent over it.
The Nurse should be relieved of all writing and counting, on the score of loss of time incurred. It will not do to charge a Nurse, with seventy-two patients on three different floors, with serving each man his portion of diet; the diets of two wards would get cold while she was serving the first. It will be better to make the Ward-Master of Pavilion wards responsible for the serving the diets. There must, of course, be a card at each bed, or some other record, showing the diet the man is ordered. The Nurse must know at a moment’s glance what each patient is ordered.
The largest London wards are the two male accident wards in the London Hospital. Each Head Nurse has charge of five wards of 12 beds, separated (and in some respects impeded) by two lobbies. Very often there are fifteen beds in each ward (not by over crowding), and these Head Nurses are often to be seen in charge of seventy-five patients each, including many serious, and some urgent cases. The two lobbies, the small wards, and the duty of some daily writing and arithmetic in settling the diets, with some daily loss of time in fetching and waiting for medicine, render a Head-Nurse’s service, as regards “manual” labour, less efficient than it might be; even where she is most efficient.
Relieve the Nurses as much as possible of all writing and arithmetic. If it could be possible to relieve them altogether of the “settling” the diets, so much, by a great deal, the better. In the Lariboisière system, with one Nurse to each Pavilion, it is utterly impossible to prevent the Nurse losing daily time and strength on the stairs. But, relieved of writing, of arithmetic, of losing time by “settling” and fetching, such women as it will be our aim to procure can get through the duty of seventy-two patients, although with the serious drawback of their being in separate wards and on separate floors.
If, however, the Pavilion plan were so modified as to have two pavilions end to end, with an intervening staircase, so spacious and well ventilated as to cut off the ventilation of the two wards on the same plane, then all the conditions as to[70] health, and facility of nursing and supervision, would be much more easily obtained. Of this more hereafter.
3. As to the Nurse’s responsibility for the good order of the three wards in a pavilion, supposing the three wards are served by one Nurse, there must always be a clear difference between this responsibility in the Head Nurse of a Civil and a Military Hospital. The Civil Head Nurse, whose assistants are all Nurses, who with herself are under the Matron, is charged with, and responsible for, the good order of the ward, and it becomes her duty, the moment she finds herself unable to do this alone, at once to call in the Steward, or equivalent Officer, in whose hands is the police of the Hospital.
The Military Head-Nurse’s Assistants are Orderlies, i. e. men and soldiers, who, with the patients, are under military discipline. Of this military discipline, the military power from the Commandant down to the Non-Commissioned Officers acting as Ward-Masters, &c., is in charge; the duty of the Military Nurse is, I apprehend, in case of any insubordination which she cannot put down at once, to call in the Ward-Master or equivalent, before calling in the superior Military or the Surgical Officer; it being, however, well understood on all sides, that she has the right of direct appeal to the superior Military or the Surgical Officer, if the Ward-Master does not do his duty, or in the event of a grave irregularity, if he is not at hand, besides its being her duty to report such to the Matron, if the case admits of being deferred till that can be done. It is impossible to settle details until the regulations as to the new Hospital Corps are fixed; and whatever regulations, whether for Nurses or for Orderlies are made, some difficulty, and much discretion will be inevitable and necessary in working them. But it is necessary to bear in mind that whereas in the Civil Hospital the Head Nurse, under the control of, and responsible to, the Officers, including the Matron of the Hospital, is solely in charge of both the nursing and the discipline of her ward, both as to patients and as to Assistant Nurses; in the Military Hospital, she is in charge of the nursing, and the Ward-Master of the discipline, both of patients and Orderlies. To be in charge of the nursing, implies to have power to enforce discipline, but this i[71]s rather, in ordinary cases, to call in the military power, beginning from the lowest or Ward-Master’s grade and reporting this to the Matron, than to invoke herself the military superiors. Therefore it would be well worth while trying how far it would answer to serve the three wards by one Nurse, who, in each ward where she successively is, is bound, on perceiving any irregularity, to call in the Ward-Master, and, in contingencies, to appeal directly to the Surgeon and the Captain of Orderlies, and to make the discipline of the three wards the charge of the Ward-Master, who is bound to go through the wards when the Nurse is not in them. The Ward-Master, in order to fulfil his charge, must enter all the wards, while the Nurse is in one of them; so that the patients of one ward, who may know that they are safe from the Nurse for half an hour or more, as she is in another ward, know that they are not safe from the Ward-Master.
In a military Hospital we must bear in mind that it is essential that the discipline over patients and orderlies should be exercised by men, and that the Ward-Masters must be the lowest and immediate deposits of this power of discipline.
All these things must be settled with the concurrence of the Director-General.
It is a great comfort that the Hospital staff returns to soldiers. We shall get on infinitely better with them than we could have done with the late Medical Staff Corps, though, after all, in the long run, we should manage with them too. If only God helps us with the sort of women required, thoroughly efficient Nurses, laborious active women, discreet as well as well-conducted, and aware (a little) of the sort of work and place, they are in!—let us trust this to Him, when the time comes, and depend upon it, to give each Nurse plenty to do will become one great means of forming such women—provided, which must be strenuously kept in view, they are made to do it.
4. It is very important to have the system of lifts throughout the Hospital, although here, as throughout, the plan of Pavilions renders them much more requisite, and makes them work less efficiently than the block plan. Lifts, to carry meals and medicine, linen, coals, &c., &c., to and from the first and second floor wards, are very preferable to the Orderlies carryin[72]g them up and down. One sort of load ought certainly not to be brought up and down by lifts, but to be carried up and down by men, viz., coffins and the dead. Using the lift for this purpose (as is done in one Civil Hospital) is on all and every account thoroughly objectionable.
The system of lifts is the more important, because although there is no objection to the washing of tea cups, drinking cups, and medicine vessels at the sink in the scullery, it is certainly neither necessary nor safe to wash the dinner dishes close to the sick wards. By a little arrangement, the whole of these could be removed by lifts to a scullery beside the kitchen, and there cleansed and set aside for next day’s use.
III.—1. Sanitary necessities can never be interfered with. The concentrating offensive and noisy cases together, while entirely separating them from each other, in a completely appointed set of wards, is a far more efficient working thing than appending a small ward to each ward.
St. Thomas’s (a very admirable Hospital in very many things) has a casualty ward (for such cases) for men and one, adjoining but separate, for women, under the charge of one Sister. Baths are in the wards.
Guy’s had the same provision with, however, the drawback that there was not a Sister in charge, but a Nurse over other Nurses, with higher pay, but not a Sister or Head Nurse. However excellent such a Nurse may be, every ward must be under the same regular government as is general in the Hospital, if discipline and order are not to suffer. Every ward or set of wards should be under a completely appointed staff.
St. Bartholomew’s had a set of casualty wards, including two of about ten beds each, several small wards of two and one bed each, including two with gratings and other melancholy necessary appliances to prevent extremely violent delirious patients from becoming suicides. These wards were often partially empty, never quite so. They were long served like the casualty wards of Guy’s; but some years ago they were placed under the charge of the Sister of the male operation ward immediately above, who received in consequence a small annual increase of wages.
London Hospital sent its [73]noisome, offensive, and extra-infectious cases to its other wards—small wards for one patient each, and, like Guy’s, not under the regular management of a regular Head Nurse.
It most certainly appears that the plan of concentrating these cases together, but with (as at St. Bartholomew’s) small wards where extra-violent patients can be put separately, the whole under one staff of Nurses, is far the best working plan.
And for this reason. Occasionally, a very offensive case requires little nursing beyond the fixed daily dressings, and can lie quietly enough in his bed or ward. But noisy cases almost always, and offensive cases generally, require close watching. Now the moment we have a patient in a little room at the end of the ward, it is our duty to go in and out and see after him, and supposing him to be a violent, delirious case, he is, unless under strong restraint, unsafe alone; and even then the restraint requires looking to. In very many cases the frequent inspection of Nurse and Orderlies would not be enough, and the man ought to have a watcher.
We can never send one of the Orderlies of the ward, wanted for its regular duty, to sit down in one of these little rooms; and we can never keep a fixed extra Orderly idling about, unless the little ward is inhabited. We must then fall back upon extra Orderlies, put in when the case wants close watching—of course not otherwise.
At night, also, the watching which suffices for the ward will often not suffice for the extra case—and he must have a watcher apart.
The plan of extra Orderlies or extra Nurses is a very bad one, to be avoided as much and as long as possible; it very seriously interferes with the discipline of wards.
Recollect that each offensive or extra-infectious case, put into the little ward, ought to represent a great amount of separation and care, which it will be difficult to secure. His mug, utensils of all descriptions, bandages, &c., ought to be washed separately from those of the patients of the large ward. Is this easily secured?
In the two Borough Hospitals they at once remove a case of erysipelas or gangrene, occurring in any ward, erysipelas from venereal wards included, into the casualty ward. In the two other great Hospitals it is only when the erysipelas or gangre[74]ne becomes severe that the removal is made. Now at once to remove these cases from the ordinary wards is very advantageous.
St. Bartholomew’s larger wards for male and female casualty cases, two small wards for two patients each, and two grated wards for one each, are very efficient. The wards are all contiguous, and, as has been said, under the charge of a remarkably efficient Sister, who has charge also of the male operation ward immediately above. The little casualty wards, of course, add to the work, and greatly to the anxiety of watching; but certainly violent delirium tremens’ cases, alone and in a secure ward which can be darkened, appear often to quiet much sooner than where several of these wretches lie shouting to and at each other. Delirium tremens will never be a thing unknown in a Military Hospital.
One such case in the little ward adjoining the Pavilion Ward would be a heavy infliction on the severe cases in the latter; the noise would be heard throughout it. And unless the ward were properly secured, or unless the man were under strong restraint—and then that would require constant looking to—he would not be safe a moment alone; while the Orderly was emptying slops or bringing in his dinner, something might occur.
2. Restraint is again a thing which must be left to our masters, and to them solely—but an ugly, sorrowful, little truth may here be told. Restraining and non-restraining processes, and their results may be seen, both where, in the same Hospital, one or more of the Surgeons orders restraint never to be used to his patients, however violent, and others order it to be used in violent cases: and where the rule of the Hospital is to restrain violent cases, removing the restraint so soon as the paroxysm is over, or as soon as amelioration renders the sudden return of paroxysms less likely. I am not speaking of lunatic asylums, but of delirium, particularly delirium tremens, in hospitals. Lunatics occasionally enter the Civil Hospitals, but, of course, as soon as that supreme earthly misery is ascertained, they are removed to the proper refuge. It is my humble opinion and firm belief that mechanical restraint excites a patient much less, and quiets him much sooner, than the prolonged struggle with his attendant’s arms and hands, whi[75]ch must otherwise be resorted to.
The coercion apparatus ought also to be good, not cheap, and always in perfect order. The least thing out of order either causes pain, which when it can be avoided is cruel, or it endangers the efficiency of the whole. The strength and cunning of these patients resembles those of madmen, which for the time being they are.
Restraint renders the usual complement of ward servants able to manage many cases. Non-restraint means that some person must stand or sit by or upon the patient’s bed, and hold and struggle with him often for hours—also that generally this person must be a stranger to the ward. Extra attendants are most injurious to discipline. Could there be a set of casualty or equivalent wards, with its own Head-Nurse, the sick would gain much.
But if necessary to adopt the little ward with every ward—in that case the Nurse must manage the three additional patients—twenty-four or twenty-five are, indeed, too few.
IV. In all Hospitals, let the construction be as simple as it can be. Let its splendour be its lofty airy wards, with plenty of windows; water in all due abundance on each floor; an ample, not excessive, supply of linen, polished impervious walls and ceilings, well-laid and bees-waxed oak floors, and a thorough not excessive, supply of good apparatus of the various necessary kinds. But every unneeded closet, scullery, sink, lobby, represents both a place which must be cleaned, and which must take hands and time to clean, and a hiding or skulking place for patients or servants disposed to do wrong; and of such no Hospital will ever be free. And every cornice, every brass lock or handle, which could be replaced by a plain china or ebony one; every decoration, or flourish, or ledge, on doors, windows, tables, beds, presses, &c., represents either a collection of dust or a great waste of hands, time, and strength in unnecessary cleaning and dusting. These are not crotchets, but the result of close observation of the practical working of these matters. Every five minutes wasted upon cleaning what had better not have been there to be cleaned, is something taken from and lost by the sick. Let the appurtenances of the wards be simple and complete, but as plain and as undecorated as it[76] is possible to be.
Polished impervious walls and ceilings are of the first consequence in Hospitals. It is perhaps hardly necessary to state that, if Parian cement be used, it must not and need not be of the kind lining the wards and corridors at Guy’s Hospital, which is as rough as the roughest plaster, of a dark and dirty colour, and which nothing could improve but being lime-washed twice a-year; it should be polished like that used at the Lariboisière Hospital at Paris, and of a pure white.
In building a new Hospital, some covered arcade or some place where the patients might take exercise in wet weather, and where inspection could be exercised over them, without fuss, is worth contriving. In St. Thomas’s, the patients walk under the covered arcades of the court.
Both in Bethanien and in the Charité Hospitals at Berlin there are reserve wards,—or rather in the Charité there is a reserve Hospital, into which most of the sick are moved for six months in the year, to change the air alternately of all the wards, which during the time receive a thorough cleaning. Great stress is laid at Berlin on thus providing, when building a new Hospital, a certain reserve space, which obviates the necessity of less efficient and far more costly steps afterwards.
V. Let us, by all means, consider as settled, that the Nurses’ food is sent them cooked. Possibly, in the long run, the undoubted advantages of this plan will be found to be over-balanced by its disadvantages; but let us begin by trying it. I submit that their dinners, and possibly suppers, should alone be sent them cooked, and that each Nurse should receive a fixed weekly quantity of groceries, and a daily or two days’ allowance of bread.
For packing up the Nurse’s meals sent her from the kitchen, a Vienna custom might be useful. Each Nurse to have a long, strong, straw basket, properly named or numbered. Some contain five dishes and covers, but two or three would here be sufficient for every purpose, including an occasional slice of pudding. The dishes strong tin, with a tin cover, and if the Nurse prefers eating her dinner out of it rather than the dignity of plates, and the trouble of washing them up, the Matron should let her take hers her own way. If taken by hand, two baskets of this sort can be carried with ease.[77] But if the Matron, as a general procedure, sends each Nurse a hot little dinner, of a good well-cooked portion of meat and vegetables, one such dish and cover will do for one Nurse, and three, five, or six can be accommodated out of the same basket, or one large basket, carried by two men, would serve all the Nurses round. The dishes should, in either case, be numbered or named, not the Nurse’s name, but the ward.
A dish and cover of strong, coarse earthenware is used in the Vienna Hospital, as a grander edition of dinner, &c. The tin ones keep warm without fire for a long time. If the meal arrives when the Nurse cannot eat it, put by on the hob, or some provision for warming in the scullery, it will keep warm and good till she can eat it.
VI. Supposing that we serve each Pavilion by one Nurse, I submit that—
1. The Nurse’s day-room should be on the ground floor.
2. The Ward-Master should sleep in his room on the second or highest floor; should the Nurses sleep in the Pavilion, the Ward-Master should still sleep in it.
In the event of the Pavilions being arranged end to end, as already suggested, the difficulty in regard to Nurses’ and Ward-Masters’ rooms would be materially diminished.
3. I think, but am not sure, that the Orderlies had better sleep away from their wards, but I would leave this to be settled by the Doctors. In cases of sudden outbursts of danger, delirium, or drunkenness, from the results of concealed spirits, and of the Surgeon being sent for, it is useful to have, at once, other than the Night Orderly at hand. And a part of what has been said as to the importance of the Head Nurse sleeping near her ward, applies to the Orderlies. Yet there are important reasons why the Orderlies should not be or feel too much at home in their wards; and if the authorities are disposed to try the plan of lodging the Orderlies together, away from their wards, they are probably right, though I should not be surprised if, after a fair trial, it were found better to revert to the having them near the ward. The Pavilion Plan, which, on the one hand, gives all concerned more liberty of doing wrong than the block plan, and which, on the other,[78] renders it more difficult to call in help, whether of supervisor or of Orderlies, if help is suddenly wanted in the night, makes it the more desirable to let the authorities take quite their own way, as to this.
4. I think the Orderlies had better have their cooked meals sent them into the wards. Of course, they can only eat together in detachments; but in many cases, the absence of even one of the Orderlies would be very inconvenient. Perhaps just as the bell rings to summon to the common meal, something is going on which requires all the ward service; the man either goes late to a cold dinner, or goes away just when he is wanted. If his dinner is brought to him in one of these emergencies, it is put by to keep warm till it is over. Regularity as to meals, as far as possible, should be strictly attended to; and is, in all well-regulated wards: and it is well, where, as in some Hospitals, there is a fixed hour for meals; but it would seem better that the meals should come to the ward servants than the ward servants go to their meals.
5. In the case of Civil Hospitals served by women, it is very important that each Head-Nurse, and each set of Assistant-Nurses, should sleep, eat, and live in the ward and its appertaining rooms, and not assemble together more than can be avoided. With Orderlies the case is partly different. Still I would not unnecessarily bring them all together, any more than allow them to be too much at home in their wards.
6. If the Orderlies do not sleep in the Pavilion they should not have a day-room.
7. To each ward should be attached a scullery, small, but not too small, which only muddles things and work, well provided with cold, and, if possible, with warm water; and it should be law that no patient enters the scullery unless sent there by the Nurse to help in washing up, &c.; and, as a rule, they ought not to be sent there. Make them useful in the ward; keep the scullery for the Nurse and Orderlies.
8. From this scullery let the Nurse get the water she requires—Orderlies ditto.
Let the Orderlies eat their meals in it, if they do not eat them away from the ward. The food of the Orderlies is generally different from that of most of the patients, and it[79] answers better for them to eat their meals not under the noses of the patients. In emergencies, of no rare occurrence, the Orderly must watch a patient and eat his dinner at the same time, and so must the Nurse; but, as a rule, it is undoubtedly better that ward-servants should not eat under the observation of the patients.
In the scullery all the cleaning must take place, which is not done in the lavatory.
In the scullery extras are to be warmed, drinks ditto, hot-bricks heated, water-bottles filled, &c., &c., &c., and none of these things are to be done at the ward-fire.
On the other hand, there is no way so good of making poultices, a thing humble but important, as for the Nurse to stand at a small table in front of the ward-fire, to make the poultices there, spread them, and forthwith apply them.
Sometimes in a large ward, where the Surgeon orders them extensively, a large iron pot is filled with poultice, and then quickly spread and applied. Sometimes the pot is filled and the poultices spread in the scullery or kitchen, to avoid the mess in the ward. When a number of poultices are thus spread away from the sight of the patients, even by very clever Nurses, some arrive too large, or too small, or too broad, or too narrow; and either the poultice has to be returned, or, as of course usually takes place, to be put on the wound it does not fit.
I would not trust any Nurse, including myself, to make a number of poultices of the right size, unless within sight of the patients. Rather than do this it is better to make the poultice-pot (wood does not hold heat, this must be of iron), in the scullery, to take it into the ward, and there spread and apply the poultices.
But a large iron pot of linseed poultice seldom contains the article nearly so well made, as when made in smaller consecutive quantities in a wooden bowl. The bowl does not keep warm above a certain time. Where the poultice is made in a mass, even by very clever Nurses, it never is so well made as when the Nurse makes the poultices in the wooden bowl. These must be forthwith spread, applied, and the bowl re-filled, if more are wanted.
This is another reason why the person who washes the wound should also make the poultice, as also why the Orderlies should clean the ward, why the Nurse should as far as possible be relieved of all “mental labour,” and why kept as much as possible to “manual labour.” All severe wounds she should wash and dress herself, and many a wound becomes severe, when the patient is allowed to fiddle over it himself. Some wounds will not bear being left uncovered, and of course in some cases the Nurse will wash the wound, and immediately afterwards apply the poultice. In general, the Surgeon will consider the wounds take no harm from being washed all round, and then poulticed all round. This requires not to be over-hurried, and not to lose a moment’s time. A careful Nurse will never apply a poultice without having first seen the wound: carelessness, haste, idleness, over-work, and prudery, each and all produce very sorry results as to this.
I think, therefore, poultices should be made in the ward, and immediately after the table cleared away, and the slight mess also. In some Hospitals they place a straw carpet just round the table, and also carry it to any bed which requires an extra mess in dressing or cleaning.
9. A regular store closet is hardly desirable. A good arrangement is this:—
At the end of the ward, nearest the Nurse’s room, or the ward-door, a large press for linen.
By it or opposite it another press, for stimulants, dangerous medicines, stock medicines, such as castor oil and one or two others which are always to be at hand, though not ordered for any particular case, stock lotions (as few as possible), lint, old soft linen, stronger but not coarse ditto for pads, &c., cotton wool, tow, oilskin, splints and pads, &c., &c. Of all these things, the Nurse should always have a certain reserve on hand.
It will be well worth while to see that these presses are made commodiously for their purpose. The linen press should have broad deep shelves, and the different kinds of things should be sorted apart; the other press should have broad deep shelves for the heavier things, and separate shelves for the bottles; the stimulants by themselves in one row, the stock medicines[81] in another, unless these and the stock laudanum were together, but they are better apart, and the dangerous things upon the topmost shelf; another row for sweet oil, mustard, stock lotions, &c., another row for ointments. Each bottle and pot to be distinctly labelled in whatever is reckoned the most lasting manner; opinions differ as to labels and letters cut in the glass. The latter are boring by night, if something is suddenly wanted, and it is just then that mistakes are to be guarded against. A strong clear PRINTED label, securely fastened to the bottle, is preferable, to be renewed when necessary, as Orderlies’ thumbs even while holding a bottle, if the Nurse’s hands are on the bed, wear labels out. There is a great saving of time and of chance of mistakes effected by clearly printing the directions for the administration of medicine, “once,” “twice a day,” “every three hours,” &c., and affixing them to each medicine bottle.
Of both these presses the Nurse should have the key or keys. One key might do for both, but it may be best to have two keys.
It is a very good plan where the shape of all medicine bottles and of those for liniments is distinctly different; and where, e. g., square bottles are used for poisons, or blue bottles for poisons, and square for lotions.
A small narrow shelf over each patient’s bed, or over his locker, solely for his medicines and wine. When these are on the locker it is less convenient. Where the medicines are not dangerous, it is better to have them thus at each bed, than concentrated away from the beds. Dangerous medicines should never be left at a patient’s bed.
The two presses will answer all demands. As, however, it does not do not to have a supply of everything that may be wanted always in readiness, a stand or table in the ward should have upon it a small supply of whatever may be suddenly wanted—a little lint, linen, tow, and two or three vessels. The supply of lint, &c., to be small enough for the Nurse to keep account of it, and for the patients to know that account is kept of it.
In constant daily use in the surgical wards of the great Vienna Hospital is a thing called in Teutonic style “Apparat.” The Nurse carries it round for herself, when preparing a[82]nd dressing the patients, and carries it after the Surgeon when he makes his rounds. The system of both dressing and washing is in some respects so different from the English one, that the fittings would vary.
This concentration of what is wanted for dressing and washing wounds, and for attending the Surgeon in his inspection of them, and of what is at once wanted on any bleeding, fit, &c., is very useful; all the more from its being in a compact portable form, which can be thus successively carried to each bed. An English carpenter would make a lighter and handier thing. Brass basins, which are there used, are not desirable. Of course, one must be most especially anxious not to introduce any novelty, particularly any foreign novelty, faster than can be avoided, and we may consider it better either to leave the general system unaltered of rushing on some emergency to the dressing table drawer, or closet, and thence bringing successively the things wanted, or at all events not to extend concentration further than the excellent plan, so far as it goes, of the London Hospital, where each Head Nurse attends the Surgeons with a large basket in her hand, containing most of the dressings required, spunges, and one or two little matters also usefully at hand. The apparat has the advantage of carrying with itself the basins used for washing. In the Military Hospital of Vienna a tray attends each Surgeon, without basins.
10. It is important to have the Nurse’s room opening at once into the ward, and, upon the whole, I should incline to its having but one door, although it may be thought better there should be a second, so that she can leave her room without being seen to do so by the patients. Also, by all means, let the scullery be opposite the Nurse’s room, and not between the ward and the room. As an invariable Hospital rule, rather more than elsewhere in Military Hospitals, publicity may be considered to be a very great police, and a still greater protection. It is far better that twenty-four patients should see the Nurse’s door than one or none; and that her room should open full upon the ward than into an intervening scullery.
In contem[83]plating a Military Hospital, we contemplate a place through which, one year with another, all characters, including a few of the vilest, pass. These are not theoretical matters. The more repulsive the subject, the more prevention is better than cure. Guard against too many closets, sinks, &c., &c., &c.
At the end of the ward there should be a lavatory, with a row, or two opposite rows, of white earthenware basins fixed in a stand, with outlet tubes and plugs: each basin should have a hot and cold water-pipe: and there should be not less than one to each four beds. There should also be in the lavatory a hot and cold water-pipe, from which a portable bath can be filled.
At the furthest end of the ward should be a water-closet, with not less than one soil-pan to each eight beds: and white earthen or porcelain urinals in the same proportion. In the London Civil Hospitals water-closets are now in general use throughout the wards, but not in all of the great Hospitals. In all the Civil Hospitals, it is usual that the patients’ water-closets have no inside bolt or lock, and that there is only accommodation for one inside. In some London Civil Hospitals the male patients, able to take exercise, are expected to make use of urinals out of doors. These matters one, two, or three experienced army surgeons had better pronounce upon; other things are to be considered than the recommendations of architect, plumber, or even sanitarian.
There is in a Berlin Hospital a very useful piece of prosaic apparatus—adjoining the water-closet, a sink, with a high, large, deep, round, pierced basin of stone, above a large hole, into which the contents of a bed-pan can be at once emptied, and from which the bed-pan is at once effectually cleansed. Adjoining this is a sink into which all other slops are emptied. In mentioning this pierced basin or sink solely for emptying and cleansing bed-pans, &c., which is used at the Bethanien Hospital at Berlin, and is far better than emptying the said vessels into the often-occupied water-closet, and then cleansing them in an awkward fashion between the water-closet and the sink, it is necessary to add that the cock ought to extend far enough over the sink for the bed-pan, &c., to be thoroughly cleansed by a stream of water falling directly into it. The Nurse stands at the sink, empties the pail, &c., in it, without fear of splashing, and rinses [84]and fills it, without stirring from the place. Now this absence of splashing water and of moving about from sink to pump, or cock, saves mess and time. The oblong sink, usual in England, has by no means the same advantages.
(The partition containing the sink would be an appropriate receptacle for the bed-pans to hang by hooks or nails on the wall pending their use.)
In Civil Hospitals, two baths, in an airy closet at the end of the ward, to be locked at all times when not in actual use, are a very great advantage. Bringing a bath into a ward, which in many urgent cases must be done when the baths are distant, is a messing discomfort. Still it had better be left to surgeons to say whether, in Military Hospitals, it would not be preferable to have, in each ward, only a portable bath, on wheels, covered with india-rubber, to be brought into the ward for any urgent case; and to take all the men able to walk, or safely to be carried, to the Hospital baths. Of these, some trustworthy, or intended and supposed to be trustworthy, man, who ought to rank as a non-commissioned officer, should have charge. An intelligent and respectable-looking man, a serjeant, has charge of the baths in the Garrison Hospital at Vienna.
In a great London Civil Hospital, St. Thomas’s, it is the very admirable practice for each patient (of course with necessary exceptions) to be bathed on his or her admission. The Sisters are responsible for examining each woman in the bath, which is within the female wards, and for at once reporting before suffering them to go to bed, any case of suspected pregnancy, syphilis, or contagious disease. A man does the same for the men, who are bathed apart from the wards. This arrangement is an excellent one. On the other hand, severe cases, just able to be carried to baths, get no good by going through the air, and being jolted up and down stairs.
In planning a Military Hospital, in which the service of women is to be introduced, it is important to obtain the advice of experienced Army Surgeons as to the arrangement of appurtenances of the wards to be used by the patients alone. Endeavour to prevent the system of holes and corners. It is best that the Nurse’s door should command the view of those who come in or out of the lavatory, and in or out of the wa[85]ter-closet. This whole section is both ugly and important.
11. To sum up. I think it would work the best to have no store-closet, only two well-appointed presses, by which a certain amount of cleaning is saved, and a corner avoided.
Could two cupboards or presses in the wall be arranged for the ward linen and the ward stores, it would be preferable to presses placed against the walls. Take care, however, that the wall is sufficiently thick, so that the presses are not damp, and if this cannot be provided against, keep to presses separate from the wall.
Believe that all this is neither theory nor fidget—but practice.
The furthest end of the ward should contain a lavatory, a water-closet, and the pierced basin for emptying and cleaning bed-pans is a very useful thing. At the other end of the ward, the Nurse’s little room, her door opening full upon the ward. If the upper half were of glass, with a curtain before it, allowing the Nurse to see the ward without being seen, it would be all the more useful. At St. Thomas’s, a window opens into the ward, the Sister drawing a blind when she chooses, and a door opens into the passage, just within the ward doors, opposite the scullery, so that the Sister enters the scullery, in which there is a water-closet, for the accommodation of herself and Nurses, without traversing her ward. Whether door or window, the Nurse should see at once all that is going on in her ward. I prefer a door; yet, if there is to be a ward for one, it may be best and most central to have the Nurse’s window on the large ward, and her door open on the passage. Opposite the Nurse’s room should be a scullery, not too small. The scullery should be well provided with cold, and, if possible, warm water.
If a supply of hot water can be obtained by turning a cock, this is best. Provision should be made in the ward scullery for keeping poultices warm which is every now and then wanted. It is not right to wash eating-vessels and poultice pans, &c., in the same sink; and this should be considered in arranging the scullery. If each ward washes its own bandages, which it ought not to do, the second sink will come in usefully for this. It is worth while, in enforcing extreme simplicity, to prevent jumbling together eating-vessels and things for[86] wounds and sores. Sinks are infinitely most handy when made deep, somewhat in the shape of broad round basins, with hole at bottom; it saves much splashing and mess; the cock to overhang full the middle of the sink. The Wall against the sink should have some protection.
Such a scullery, with complete efficient simple apparatus for its various purposes, places for washing up and cleaning, and for ward purposes and cookery, so that the Nurse can warm the drinks, prepare fomentations, &c., without jostling the Orderlies, who are washing up or cleaning, will be a very great comfort, simplification, and promoter of order, cleanliness, efficiency, and work. At one corner a decent little table for Orderlies’ meals, above it their separate safes for their bread, cold rations, &c., &c.; each to have and keep his key; each to have his locker.
Each floor and ward will require a scullery. It is far better for each ward to contain its own appointments—and all the other stores to be together, apart. On the second floor might be the Ward-Master’s room; vice the Nurse’s room.
12. Nurses’ quarters, if we are driven to their not sleeping near their wards, should be adjoining the Matron’s two rooms, and separate water-closet, in a part of the Hospital as central as can be managed without trespassing on our betters. I would simplify these quarters as much as possible—either a series of very small rooms, or one great space partitioned off each into a little cell, with a window, bed, washing table, chest of drawers, and a very small wardrobe, with space to hang up three or four gowns, deep enough for another row for shawl, &c., at top a shelf for bonnet and caps, at bottom a deep drawer for boots and shoes. These things will be a convenient riddance to the chest of drawers, and comfort to the women. In each cell very strong hooks to hang up and air a little gowns taken off at night, and one or two chairs. The nurses must wash their hands, &c., in the rooms off their wards, and I think it must be understood as a rule that they leave their quarters in the morning and return to them at night. Optional carpet.
Each cell to be numbered either with number or with name of Pavilion. Opposite this space a small lumber room, wherein each nurse may deposit her box, thereby hindering dissemination of bugs. Opposite also a running open cupboard, with partitio[87]ns numbered or named as rooms, containing each Nurse’s broom, dustpan, &c., each with a key.
Also pump, sink, water closet.
When furnishing begins, it will be well worth while to see that all articles of furniture, whether for wards or Nurse’s quarters, admit of being easily swept and scrubbed underneath, and swept and dusted at top. Chests of drawers, &c., with too narrow space between bottom and ground, harbour dust, or sadly waste a few precious minutes in the most busy part of every day. As few high pieces of furniture as possible, to gather dust and be out of easy reach; as few as possible of cumbrous articles difficult to move from the wall, to sweep and dust behind, &c.
There ought to be, near the Superintendent’s quarters, one or two small rooms, where, necessity occurring, sick Nurses might be lodged. We cannot hope always to escape having sick Nurses; and there would be serious objection in a Military Hospital, where only one Nurse sleeps on each floor, to having the Nurse ill in her room for more than 2 or 3 days at the outside. Or there might be one good-sized airy room, with two or three dark washable curtains dividing it into little dormitories, so that one Nurse, whom the Superintendent must engage and watch, could attend them all. And as Her Majesty’s Nurses must have allowed them such decent comfort as can be, but no fastidiousness, I think the cubicles in one room would be best. Not to be called so, however, by any means, as it would sound Latin and “Puseyitical.” The Nurse’s ward to be locked and key kept by Superintendent, except when tenanted. I should hope three beds would answer thoroughly, as well as that the ward would be empty eleven months out of the twelve.
Considering the awkwardness of illness among Nurses, when it did occur in a Military Hospital, it would be worth while that, adjoining the little ward, there should be a little room for any one infectious case which might occur; e. g., supposing one Nurse ill in the ward with bronchitis, it would not do to put another with small-pox into the ward,—at least it would be very impolitic. The ward should have a water-closet and a little sink of its own, and a little cell, but with window and fireplace, for the attending Nurse to lie down in. When not used, once a month’s, or week’s at the most, cleaning by a cha[88]rwoman would be enough. It should be always clean and ready for use. In the Civil Hospitals, few years pass without sundry Head-Nurses and Nurses dying, not a few Nurses being warded, and sundry Head-Nurses ill in their rooms. The peculiarity of Military Hospitals makes this little preparation for what is certain every now and then to occur seem desirable and economical; to hire lodgings in the neighbouring town would be in all ways a worse plan.
13. Endeavour, if possible, to obtain a classification of the severe and non-severe cases, and let the Nurses be only appointed to the wards of severe cases. The convalescent cases to be successively removed to the convalescent pavilions, whether they bear or not that name. No convalescent ward in any of the floors of the Pavilions to be served by Nurses.
14. It will be found excellent in many respects not to allow the Nurses’ names to be used in the ward of the Hospital, or among each other, so far as the Matron takes cognizance of. In the great London Hospitals the name of a Nurse is never heard, except occasionally to each other as a solace, partly very natural, partly harmless vanity. She is Sister or Nurse of such and such a ward. In hasty parlance she is distinguished from the others by the name of the ward only. In it she is always addressed as Sister or Nurse.
Thus a Sister of St. Thomas’s Hospital, whose services in the War Hospitals of the East I can never forget, was always at St. Thomas’s spoken of out of her ward as Sister of George, or, more commonly, Sister George; and spoken to quickly or called to in a hurry as George.
All this, the only course of all the great and, I believe, of the smaller London Hospitals, works excellently, in many ways.
15. Arrangements should be made that foul linen remains for the least possible time out of the laundry. As regards the laundry deposits, the best plan is that of the London Hospital, where each ward has a bin of its own marked accordingly. To similar bins all the foul linen should be, at least, daily carried, unless it is judged best to receive and wash all the linen in a heap, returning numbers only to each ward. The former plan is preferable. In any case the linen of the “foul wards” should be received and washed apart. During the time, which ought[89] to be as short as possible, between dirty linen leaving the patients and reaching the bin or bins, a large box in the scullery is making the best of a bad business—the presence of foul Hospital linen always is that—and is preferable to a closet.
16. Washing bandages, a very important thing. Shall a washerwoman be told off for that particular purpose? or shall the Orderlies of each ward do it alla meglio? The former is the better plan; if not adopted, the Nurse must see well to the matter.
17. It would depend upon what sort of work is usually going on in the Surgical Wards of a Military Hospital in peace whether it will be worth either a press with glass front, in which splints, pads, &c., &c., are excellently arranged, as at St. Bartholomew’s; or the pad-basket and splint-rack, which are also excellent, provided in London Hospital. The splint-rack, enabling the Surgeon at once to see and choose of all shapes and sizes, is perhaps only suited for an accident ward, and would be out of place in a military ward in peace. It may be better to have these stores entirely in some dispenser’s or store-keeper’s jurisdiction, and to let the Nurse confine herself to padding, &c., any splint sent by the Surgeon into the ward. Let our masters take exactly their own way about this.
Bandages, lint, &c., &c., &c. should perhaps rest entirely with the Dispenser, otherwise it would be useful in the greater Hospitals, to have under the Matron a Nurse charged with preparing them and giving them out, writing in a book the date, amount of each, and the ward they are given to. In a small Hospital the Matron could do this herself.
While speaking of lint, it seems a duty to state that, in some of the Military Hospitals, in certain County and even London Hospitals, and also in Workhouses, and in the practice of private Surgeons, a preparation of cotton has been recently substituted in the dressing of wounds for charpie or Surgeons’ lint, properly so called. So miserable an economy at the expense of the sick is not adopted in several, at least, of the London endowed Hospitals, probably in none. For all purposes for which lint is necessary cotton fibre should be totally disused, in the army and everywhere else. It is irritating and injurious to wounds. It increases human suffering; it delays patients in Hospital, and, in doing so, of course, increases the cost which such a[90] substitution has been intended to reduce. Nurses should be particularly careful never to use this material, which is easily distinguished, even by the touch. Any Surgeon may tell the best of it from lint by submitting it to microscopic examination, and on doing so he will readily discover that characteristic of cotton fibre which renders it so ill adapted for surgical dressings. It does not absorb the discharges from wounds, as linen lint does. The fibre is ragged instead of being smooth, and it is apt to become matted together, and to adhere to the surface and edges.
18. It is essential to have as few women as can efficiently do their work. Supposing the Hospital were for one thousand patients, not taking into account that some wards would probably be foul wards, where I earnestly hope female service will not be, at present at all events, introduced, and that some wards would be for slight or convalescent cases, where I hope it never will be—supposing each Nurse served seventy-five patients, supposing one Nurse, at the very least, was told off for the linen, fourteen or fifteen Nurses would serve the Hospital. I conclude the Matron to have no cognizance of the laundry.
The Superintendent[18] will require a store room, or at least a store closet, and hers should be well appointed. It would depend upon the other arrangements of the quarters, whether the world in general, when sent for to fetch what it wanted, enter from the same side as the door of the Superintendent’s bed-room, or from the other side. And it would depend upon the nature and amount of stores of which she had charge, in the larger Military Hospitals, whether or not she should have a Nurse told off for this also. Economy is essential; but useless fiddling over every duster or scrubbing-flannel given out, &c., &c., &c., sadly hinders the Matron’s time from more important things.
Housekeepers must be avoided, and every woman must have a distinct and sufficient share of work, and each be distinctly and equally under the Matron. Still it would be ad[91]vantageous if we could from the first include in the staff of Nurses for the larger Hospitals, one or two places which could be filled by efficient persons who yet were unfitted for the ward work, which calling will be, and ought to be, laborious and wearing enough. Many a woman would never do to look after a Pavilion and seventy-five men; who yet, in charge of linen or stores, would be most valuable, and influence most beneficially the Nurses, whom yet she might be unfit to govern. The system of the Sœurs de St. Vincent, who, in theory and fact, subject entirely to the will of the Superiors in general practice, are yet selected and trained for spécialités, who remain long in these spécialités, which spécialités include such requiring more or less of physical strength, seems to be one giving many useful hints for us.
I. After much anxious thought, re-consideration of all things, and pondering, I submit—
1. That three Orderlies will efficiently serve a ward of from 28 to 30 patients, including night-duty.
2. That each of two wards of 30 each, should there be two such under the same Head Nurse, on the same flat, ought to be entirely separate in all other respects.
3. That if night-duty be required, each such ward should have an Orderly on night-duty.
4. That each such ward should have a scullery.
With regard to these questions, I further submit—
1. Economy of hands, combined with efficiency of service, is an urgent thing in all Hospitals; most of all in Military Hospitals,
On the score of expense;
On that of efficiency of inspection;
From the nature of Military Hospitals, where the aim should be throughout to combine great simplicity with thorough efficiency;
From the importance of training the staff, male and female, of Military Hospitals, for service in War Hospitals, where every man or woman who can be spared is better away.
2. Yet economy of hands, carried too far, becomes, like all other such economies, penny wise and pound foolish.
3. Without doubt, large wards can be efficiently served by fewer hands than small or moderate wards. But, as sanitary considerations limit the size of wards to from 24 to 30 patients, let us make this the basis of all calculation.
4. The more it is considered, the more essential it appears, to train Nurses, from the first, to do efficiently a great deal of work. A small staff of respectable, laborious, and thoroughly efficient women seems the thing to be aimed at; whether considering Military Hospitals by themselves, or as a training-school for Hospital war-service.
5. It would be better to give each Nurse one great ward; but wards above a certain size are inadmissible for sanitary reasons.
6. The care of 24 to 30 patients is not sufficient duty, by a great deal, for a Nurse.
7. Therefore, upon the whole, and as decidedly the lesser of two evils, I recommend assigning to each Nurse two wards.
8. It is less difficult, and less objectionable, that she should have charge of two wards on one floor, than of two wards on two floors.
9. As regards the Nurse, I recommend therefore, upon the whole, to give each Nurse the charge of two wards of 30 men each; the wards to be on the same floor; but, except as being under the same Head Nurse, entirely separate.
10. It is important to repeat that the Nurse (who is Head Nurse), will be set free of two things, which consume much of a Civil Head Nurse’s time.
(1). “Settling the diets,” and fetching, besides waiting for, portions of those diets (e. g. wine) and medicine.
(2). Distribution of Diets.—It is quite possible that, in no long time, it may be found desirable to assign this duty to the Nurse. But it would be better to try to have it efficiently, which implies honestly, discharged by the Ward-Master. It will relieve the Nurse daily of considerable time; and it[93] charges the Ward-Master with a definite duty which he can perform. The more he has defined duties, the less he will be inclined to fidget and disturb the Nurse. He is pretty certain to do this; but definite duties will diminish the tendency.
I should avoid giving the Ward-Masters too few wards. Otherwise they will make themselves insufferable obstructions, one way or another, to the Nurses. I should say that each Ward-Master, in charge of a Pavilion of six wards of 30 each, besides the small wards for one, would not have at all too much to do. Where there are no Nurses, the Ward-Master should have Assistant Ward-Masters in their place.
N.B. Wine might be treated as medicine, and, as such, delivered by the Nurse. Wine and medicine are usually, in the Civil Hospitals, given from the Apothecary’s shop at the same time. Or it might be considered desirable to leave this duty to the Ward-Master. In either case, it will never do to serve a bad case at once with all his wine, and either to let him stupify himself by swallowing it at once to make sure that he has it; or to set it by his bed-side for the flies to spoil it, or for a dishonest comrade, or here and there an Orderly, to drink it. The Nurse should receive, whether directly or from the Ward-Master, the wine of such patients, and should administer it in successive small fresh portions. The intelligent administration of wine ordered to bad cases is one of those momentous minutiæ by which, I do believe, and believe more and more, many lives are, by God’s blessing, annually saved in English Hospitals which would be lost elsewhere. Of course the only Regulation about wine should be to specify whether the Ward-Master or the Nurse should administer it.
11. Relieved of the loss of time incurred by fetching and waiting, and relieved at starting, at all events, and we will hope permanently, of the time consumed in distributing the diets, I certainly consider that a Nurse of the class of which, please God, Her Majesty’s must all be, (strong, laborious, active, and conscientious women,) can efficiently serve two wards of 30 men each.
Orderlies.
12. I should prefer wards of 30 each to wards of 25 each.
13. In forming rules for the proportion of Orderlies to sick, it is important to consider that the duty varies extremely according to the appurtenances of the ward.
14. I consider extreme plainness and simplicity to be proper and indispensable to a Military Hospital. Let us take for granted (and may it prove correct to do so), that in none of Her Majesty’s Hospitals Orderlies’ time will be wasted in cleaning any ornamental things, whether unnecessary furniture, flourishes, or cornices, &c., &c., on necessary furniture; supernumerary shelves, nooks and corners, &c., &c. Once provided, all these things must be carefully and constantly cleaned, or they become receptacles of dust and breeders of fleas; and to clean them involves enormous waste of time. A few minutes daily wasted on each of many things, make an enormous sum.
15. But it is very true economy to supply, if possible—which in old buildings it often is not—every ward of every hospital with a constant supply of water, (taking care that it is not wasted by mischievous or childish patients); and to give every ward of every Hospital the use, under proper control, of a lift by which, at fixed hours, food, medicine, linen and fuel are brought into the wards.
Believe that this is not theory, but the result of practical observation, much extended.
16. Now, these two things—supply of water (if hot and cold so much the better, and supply of water imports, of course, the appliance for getting rid of it, and of the contents of bed-pans, &c., &c., by one or more sinks) and the use of lifts can be applied to a new Hospital; can possibly, not certainly, be applied to some of the old Hospitals within the Kingdom,—can certainly not be applied to many of the Army Hospitals abroad.
17. Upon an average, these two things make the difference of one Orderly’s duty to a ward of 30 men.
18. And a ward of 30 men, so supplied, would be efficiently served by half a nurse and three Orderlies, including night-duty.
19. Without these two things (it is a mere comparative question as to loss of time and absence of thorough cleanliness, whether the water is brought from a pump in the court,[95] or a stream some hundred yards off, above or below), and many, if not most, Army Hospitals abroad, must always remain without these two things, I consider that one Orderly to every seven patients will not be too much; while it is certain that, other things being equal, the ward with the appliances and the three Orderlies will be better served than the ward without the appliances and with the four Orderlies. Where there is no Nurse, one Orderly for 7 patients will always be advisable.
In these memoranda as to Orderlies’ work, &c., no notice whatever has been taken of the possible abolition of scrubbing, because it does not do to count unhatched chickens. If, however, that formidable weekly business could be got rid of, as well as the bi-weekly or daily washings of bed-head-floors, &c. the labour of the Orderlies would be, without underrating that required for keeping oiled floors cleaned, very materially lightened.
Night-duty of Orderlies.
20. Convalescent wards, which will be of great use in many ways, will be of use here. With them Nurses will have nothing to do. It is possible enough that, in course of time, the Medical Officers will desire to have Nurses there, and that it may be useful to place there elderly, still efficient Nurses; but let this come or not as it will, and let us keep quite clear of them, at all events, till the Nursing-service be tried and established in Army Hospitals. In these wards, night-duty will probably be quite unnecessary, though in that case either an Orderly or Assistant Ward-Master ought to sleep at hand; and night-duty is a service which must be spared wherever it can be spared, and rendered as efficient as possible wherever it is really wanted.
I have before submitted that in Paris, Vienna and Berlin, the average of severe cases in Army Hospitals, in time of peace, is very considerably lower than in Civil Hospitals.
This quite as much applies to English Army Hospitals. Whether the ordinary wards would require night-duty I do not know. If they often did, I should prefer having a regular night-duty in them. If they seldom required it, I would not have it.
21. In Civil Hospitals, served by women, I should undoubtedly prefer assigning the night-duty to one Assistant Nurse.
22. But Orderlies are in sundry respects different, and, upon the whole, I recommend not to have night Orderlies, but to let each Orderly in turn do the night-duty.
23. It is important to remember—the more so as it is often forgotten—that to lay more upon human nature than its Maker has made it to bear, is to do a foolish, let alone a wicked thing. Upon an average, all men and women can dispense with, or abridge sleep for more or less time. Upon an average, all men and women, after a laborious day, require a good night, in the long run. When they do not have it, either health, efficiency, or sobriety, or all go.
Believe, again, that this is not theory, but the result of practical observation, much extended.
A strong soldier is no exception to the general rule. In the long run, if made to do night-duty after a laborious day, he will either go to sleep, or drink to keep awake, or he will get knocked up before his time. And this it is part of his business to be in time of war; therefore, in peace-service, it is economical to let him last his time. It is then sound economy to give watchers sufficient sleep.
24. Supposing regular night duty required, in a ward of 30 men, supplied as above, and served by half a Nurse and three Orderlies, it might be worked thus: the Principal Medical Officer would decide whether the same Orderly should do the night duty for a week, or the three on successive nights: probably the latter. The Orderly might come on night duty at 9 P.M., and remain on duty until 9 A.M., thus taking his share in the heavy morning work of cleaning the ward, &c. In all well-ordered Hospitals it is required that this should be done by 10 A.M., in some by 9 A.M. Earlier is undesirable in the English latitude (in other climates it is different), unless either the patients are to be disturbed earlier than English Surgeons consider right; or the ward, &c. cleaning is hurried through. A large ward, got into thorough order by 9 A.M., is in very good time. Of course it may happen occasionally to be got ready somewhat earlier, but this refers to the average.
Scheme for Three Orderlies A. B. C. Serving Ward X.
Monday, 3 P.M. A goes to bed, after taking his share of the morning work, eating his dinner, and helping to clear away ward dinner, &c. 9 P.M. A comes on night duty, after 5 hours’ sleep, and allowing 1 hour for undressing, dressing, and eating his supper.
Tuesday, 9 A.M. A goes off duty, having watched until 6 A.M., having breakfasted, having taken his share of the morning work, and leaving the ward clean. Let him have the option of one or two hours’ fresh air, either now, or before 3 P.M.; let him sleep full three hours; let him have his hot portion of dinner taken to him at the usual hour, unless all the Orderlies on night duty are served together at a different hour; and let him, 3 P.M., return on duty, washed and shaved. B goes to bed, &c.; 9 P.M. B comes on night duty.
Wednesday, 9 A.M. B goes off duty; 3 P.M., C goes to bed, &c.; 9 P.M., C comes on night duty, &c.
I have reckoned 12 hours for the Orderly to be off duty. It is better for him to have eight than seven hours’ sleep, and one or two hours’ fresh air are more healthy, and make a man last longer than going to and from his bed and his ward. An English soldier comes on duty clean, washed, and shaved, a once national peculiarity it is highly desirable he at all events should retain—at any rate that of thorough cleanliness—the shaving is unfortunately now not certain; for this and for his meals, some little time must be given. I think you will get more, and get it longer, out of the man by giving him 12 hours on night duty and 12 hours off. Still it will not do to interfere too much with analogies, and the proper authorities must decide whether this is too much.
25. Again, leaving the question for decision to the proper authorities, I had rather each Orderly had one hour or two hours for exercise each afternoon or each alternate afternoon, care of course being taken that he did not exercise himself in some tap. He should report himself to the Nurse, or to the Ward-Master, or Assistant Ward-Master on going and on his return. So should the Night-Orderly when coming on and going off duty. Also in many emergencies of no very unfrequent occurrence at home, and constantly abroad, the Orderly must dispense with recreation time. But as a rule, it is certain that fresh air is necessary to preserve health in Hospital duty. Doctors of a[98]ll kinds know and act on this as regards themselves.
The waste of time and strength, at present too often incurred by the endless fetching, heavy carrying, &c., of many Hospitals is in a considerable degree counteracted by its forcing the Nurses into other than ward air; the air of a Hospital Court is better than that of the best ventilated wards as it is, not as it might be. The same applies, in its degree, to Orderlies. But it is better, and far more economical, to avoid the fetching and carrying as much as possible; to keep the ward attendants in the ward to their duty under the supervision of the chief and responsible ward-servant; and to give each in turn a short daily recreation, if possible.
26. Now comes a thing I am very anxious about concerning night duty, the more anxious because it is important, and because I am afraid it is an innovation. I have watched the night duty with particularly anxious interest, in each Hospital I have entered, feeling at once its importance and its difficulties, and of the following principle I am thoroughly certain.
The Orderly doing night duty should either be allowed refreshment during the night, or the recurrence of this night refreshment should be considered in allotting the rations.
In none of the Civil Hospitals, so far as I know, is night refreshment given. The Nurses usually on board wages, apportion, when they can, some from their food. In one Hospital there exists a rule that no Night Nurse is to take refreshment during her watch, the intention being to keep her more vigilantly to her duty. This is one instance among many of the serious and cruel mistakes which men of business or benevolence, or both, make, when legislating on matters which they do not understand. It is, fortunately for the fine Hospital where it is the rule, practically disregarded; the Head Nurses knowing well that a Nurse watching and fasting in a ward from 9 to 9, or even from 9 till the breakfast hour of 6, would either soon be unfit for duty, or put drams in her pocket, or doze through the night.
A strong soldier, required to watch in a ward and fast from 9 P.M. till 9 A.M., or 6 A.M., or shortly before, would stand the trial quite as ill as a Nurse. There is an admirable rule at two foreign Hospitals where I have served. Sisters watch in some wards, Men Nurses in others; and each watcher receives[99] from the house, on going on night duty, a bottle of beer, a can with about six or eight cups of coffee, milk and sugar in proportion, and three slices of bread and butter. The Sister’s bottle of beer is about one pint; the Man-Nurse’s double; his coffee can is also a good deal larger. The rule of allowing sufficient for three solid refreshments (which of course can if desired be made by the watcher two or three) during the night, is an excellent one.
I think it would be very sound economy to allow each Orderly on night duty, a proportion of beer or porter, of coffee or tea, and of bread and butter, or bread and cheese, to take at his own time during his watch, besides his supper before going on duty, and his breakfast just before 6, (both Nurse and Orderlies ought to have breakfasted by 6, and to begin the day duty at 6, and I wish it began by opening the windows and repeating the short prayers for 5 or 6 reverent minutes). Of course it may be considered preferable to reckon this night-ration in the Orderly’s rations. Or suppose the bread and beer or porter to be reckoned in the rations, and a can of coffee given him for the night watch. Settle details as is best, and of course analogies must be considered; but in truth hospital watching is a very peculiar business; important, unobtrusive, most peculiarly trying, and the bright side of very few Hospitals. Each watcher should undoubtedly have refreshment for the night.
The Nurse should have her groceries in the lump, and refresh herself as she likes out of them. Her watching, if she does her duty, will be, when she has bad cases, severe enough; but I would not provide her with extra refreshment; as the watching is not prescribed and regular duty.
There should be as little extra watching on the part of Orderlies as is possible; when it is indispensable the extra watcher should have the same night-ration. I submit my strong impressions on the subject of this night refreshment now, because, small as it may seem, it very largely enters into the working of a night watch.
I have suggested the division of the Night Orderly’s sleep, because, if A. comes on duty at 6 A.M., and is sent to bed at noon or 1 to get ready for his night watch at 9 P.M., he is scarcely fit for a long sleep, and supposing the patients dine at noon (an excellent hour) he has not, or scarcely, taken his[100] share of the clearing away which, got over in time, enables the other Orderlies, one or both, to have a short recreation in the afternoon. Also if sent to bed at one he has not eight hours’ sleep, as out of that he has to undress, dress, and sup. Also he has to remain on duty from 9 P.M. to 9 P.M. next night, which is much too long as a rule. If he does not go to bed before his watch, and goes off duty at 9 A.M. next morning, whatever time may be then allowed him for sleep, he cannot, as a rule, be depended upon for performing his watch duty efficiently.
27. If the Ward Orderlies watch by turns, it should be arranged that the men who sleep before and after the watch can do so quietly. This is by no means always attended to, as to Nurses in Civil Hospitals. Upon the whole, I cannot think it would answer to have always the same watchers, as regards Orderlies. The other Orderlies, supposing them lodged apart from the wards, will certainly go seldom enough to their quarters during day, except during their exercise time. It may be thought essential to retain soldiers under very primitive notions as to quarters. So though in a dormitory of women, I think little cells, parted either with a partition or a curtain, the whole thoroughly airy, are in all respects preferable to unparted rooms, it may be, by some, thought better that the Orderlies shall sleep in large airy wards, not parted by curtains or partitions. I know, however, one high Military authority, at least; who considers the same reasons apply to men as to women in this. Soldiers are generally able to go to sleep whenever ordered. Indeed their general capacity of doing whatever they are bid is one of their many fine points. The Orderlies’ wards must be under some sort of inspection, and noise must not be suffered in them. Non-Commissioned Officers, either Ward or Assistant Ward-Masters, or some special functionary (but such I would not multiply) must sleep near, and have general charge of the order and quiet of such wards. I conclude that one or more Assistant Ward-Masters, at all events, must watch, and as they must sleep by day, this will fit in well enough.
I should avoid putting the Orderlies in a too much out of the way part of the Hospital; they should know themselves liable to inspecting visits any time. I am not sure that Ward or Assistant Ward-Masters would not be much better guardians of the Orderlies’ wards than any special functionary. Drink [101]is the vice of these men, noble fellows as, as a body, they are, and I should avoid quartering any man too comfortably and solely in one particular post. Cases have been where the duenna of the Nurses’ dormitory was herself a determined, disguised drunkard, and reported others accordingly as she was bribed or not with drink for herself.
The whole question of Orderlies sleeping near or away from their wards should be well considered by the proper authority, two or three experienced Army-Surgeons. Upon the whole, I think it would be well to try the quartering them separately: there is much to be said on both sides as usual.
28. In several foreign Hospitals a certain number of Night Watchers, both Sisters, and Men-Nurses, are told off for night-duty for four weeks, during which they are exempted from all labour by day, and receive better food than the usual diet. They also receive good night-refreshment.
In one Hospital the following is the arrangement. The wards usually contain from 10 to 13 beds, and there are many small wards for three, two, or one, bad cases or operation cases. All the wards open upon a corridor. The Sisters do not watch in the men’s wards.
| A Sister watches in the female medical wards | 5 Watchers | |
| A Sister watches in the female surgical wards | ||
| A Sister watches in the children’s wards and girls’ ward | ||
| A Man-Nurse watches in the male medical wards | ||
| A Man-Nurse watches in the male surgical wards and boys’ ward |
An operation-case, or an extra bad or anxious case, or a case requiring special attendance and put in a single ward, has an Extra-Watcher. Often there are no Extra-Watchers: sometimes there are several at once. The Extra-Watcher is either a Sister or a Man-Nurse, taken from among the other Sisters or Men-Nurses, who, after his or her day’s duty, does the extra watch.
As regards all English hospitals, civil or military, the advantages of this system are these:—
1. It severs certain persons for night-duty, who have full time for sleep and refreshment in the air during day, and who are allowed to do no other work.
2. It secures these persons good[102] food and refreshment at night.
3. These persons know their sick, and, being told on coming on duty, of any change, &c., are as much at home in their posts by night as others are by day.
4. When it is found that a Sister cannot sleep by day, and, therefore, that her health breaks, she is not allowed to finish the four weeks and become ill, but is put to another duty and another Sister appointed to the watch.
(Many a strong Nurse cannot sleep at day.)
5. The persons so appointed get into the way of it, if they stand it at all, and the system is found a great relief to the whole house and a great gain to the sick, in the place of another system of dividing the night between two Sisters and two Men-Nurses, who each watch half of the watch.
Per contrà.
I. The great London hospitals are places very far from perfect: some things may, please God, be, with time, patience, and extreme quietness, very much improved; but some things will never be perfect and never can be. But they are places where I do believe, and so far as I know, the sick are cared for in a way that is done nowhere else. The proportion of heavy cases in every London ward, cannot, I think, be met except by having a watcher in each. An English physician or surgeon would not consider that his cases could otherwise receive the attendance and the watching, the observation of possible change and prevention of possible mischief, which they ought to receive.
It is right to bear in mind,—
1. That small wards multiply exceedingly the demand for Watchers: four wards, of 10 patients each, taking the average of patients as in London, would not be attended, according to the English notion, by one Watcher; 40 patients in one ward would be fully attended by one Watcher. The London Hospital has two Night-Nurses for its quadruple wards. An extra Night-Nurse has frequently to be put on, on account of the difficulty the subdivision of the ward gives to the watching.
2. That the average of severe cases in each ward of London hospitals is very considerably more than the proportionate average of severe cases in each ward of the foreign hospitals in question. In all foreign hospitals with which I am acquainted the proportion of accidents is comparatively small [103]to those of the London hospitals. The docks, the manufactures, the crowded and dangerous works, &c., &c., with us, account for this.
3. That, striking the balance for and against, it is necessary that each London ward should be watched by a Nurse; at the same time, that without doubt a certain number of troublesome, ill-conditioned patients (no ward of any Hospital is without such) sleep soundly and let their neighbours sleep soundly when the Watcher only looks into the ward at frequent intervals, who would, if the Watcher sate in the ward the whole night, make it their business to require attendance from the Watcher during the whole night, or at least much oftener than by the other plan.
II. The second flaw of the above system, as it applies to London Hospitals, is, that it renders Extra-Watchers so often indispensable.
The employment of Extra Watchers can never be wholly prevented, but it should be the endeavour of every Hospital to employ such as seldom as can possibly be. Extra watching is most injurious to the health of all ward-servants, and to the sobriety, and therefore morality, of many paid ward servants.
This is a very important reason, I humbly consider, for avoiding as much as possible small wards.
I do consider small wards very objectionable in working a Hospital.
But it is right to remember that we have been told of England, of Austria and of Prussia that the proportion of severe cases in Military Hospitals in time of peace is considerably smaller than in Civil Hospitals. Night watching is not done in the Military Hospitals either of Vienna or Berlin. Orderlies, or an Orderly, sleep in each ward, and watching is only done to bad cases.
How far English Army Surgeons consider night watching desirable in the Army Hospitals I will presently tell.
I should think the convalescent wards, among many important advantages, would receive a number of patients who require no night watching. An Orderly ought to be at hand here, but not watching.
If night duty[104] is considered requisite in the ordinary wards, I do not see how the English standard of things could be met, excepting by having one Watcher in each ward where there is regular night watching.
I think, however, that the foreign system of night watching above detailed might give very useful hints for women in war service, and for emergencies of cholera, &c., &c., in home service; and with regard to supervision in the latter.
I think, with submission to the proper authorities (the two or three experienced Army Surgeons I have so often adverted to) feeling strongly that awkward mistakes might occur in several of these matters without them, as civilians and women cannot and ought not to trust their own judgments respecting such, that in a large Military Hospital, an Assistant Ward-Master ought to go round the wards at night. Not with any idea of his rendering assistance to the Watchers over bad cases. The Nurses must do their duty of Head-Nurses, and see to this themselves. Perambulation through a large Hospital at night in point of fact excludes the possibility of doing anything in any one ward, unless in some exceptional occurrence which only proves the rule. The object is the important one of seeing that the Orderlies are awake, sober, alert, and at their duty, and that the patients are quiet and in bed. The Nurse would hear any noise, but there is such a thing as quiet drinking, as well as noisy drinking.
In St. George’s there is a Night-Matron, chief over the Night-Nurses, who goes through the Hospital every hour during the night-watch.
I have heard this spoken of by experienced Authorities of other Hospitals with approbation and envy, and some idea was entertained of introducing it into another great Hospital. In Civil Hospitals, I think, but I do not know, that the benefits of this Night-Matron may be perhaps more imaginary than real. The Head-Nurses at St. George’s sleep away from their wards; a great mistake, I humbly consider.
But Military Hospitals are entirely different in sundry essential respects. I think a non-commissioned officer, Assistant Ward-Master for instance, ought to make his rounds every night. When once such a service takes place, every hour is better than three or four times a night. He must be “up to” sundry things—taking the wards in uncertain rotation, sometimes returning suddenly on his steps, &c., &c., &c.
It will be worth securing, if possible (this parenthesis will be understood), that the Nurse’s water-closet should be within her room, if not, as close to it as may be.
29. The following extraordinary system of Night Nursing is that which prevails in the Army at present:
The “nursing is managed” either by means of patients “told off in watches” through the night for the purpose of attending to other patients, or by means of soldiers sent in from the ranks to attend specially upon each bad case; or by Orderlies “arranging it among themselves,” without any exemption meanwhile from day duty.
Upon each and all of these systems or no-systems it is hardly necessary to make any comment. It is difficult to tell which is the worst.
In the principal, indeed the only General Hospital in England, “Nursing is managed by comrade-patients told off in three watches of two hours each for the night.” [sic.]
“Orderlies are likewise warned and often sit up for the purpose.”
These passages are given verbatim et literatim, because they are so remarkable.
And it is necessary to add that these patients being the relapses among the “Invalids” are nearly the worst cases we have.
Were it the report of a Head-Nurse in a Civil Hospital to her Resident Medical Officer, it would undoubtedly cost her her place. One scarcely knows whether to pity more the sick patient or the orderly patient. One scarcely knows how to estimate the amount of medical comforts intended to be consumed by the sick patient which will actually be consumed by the sitting-up patient, and necessarily so. And the expedient which turns over the man who is too ill to be left at all to the care of men who ought to be recovering themselves, but who are pulled out of their beds for two hours to nurse (for the first time perhaps in their lives,) and a very “serious” case too, is to say the least of it a singular one.
At Woolwich Artillery Hospital the cases which require constant attention are about 2 per cent. There are now 545 patients in Hospital, and 11 cases consequently, each requiring one Orderly to itself. The Orderlies, according to Regulation, are 55, so that one-fifth part of the Orderly service is requir[106]ed for these cases. Yet there is no system or arrangement for such. The Orderlies arrange (or do not arrange) among themselves to do the reliefs day and night. Of the 11 cases at this time in Woolwich Hospital with 11 Orderlies sitting up with them, it so happens, as I am informed, that only one would require, if such were together in wards where regular night nursing was established, an attendant specially to itself.
It is needless to enlarge upon the cruelty of the above practice. The one serious case is disturbed in the day by the goings to and fro, the noise and bustle of the light cases—while these are disturbed at night by the sitting-up necessary for the one bad case, which may be besides, and too often is, a noisy or offensive one. The bad economy is as obvious. It often happens that 11 cases who might all, if in one ward, be attended and as efficiently attended, by one Night Orderly, require each an Orderly to itself in as many different wards.
In the “Garrison Hospital” at Chatham, “when any case assumes such a character as to require more than the usual care and watching, a Requisition is immediately sent to the Commanding Officer of the Corps to which the man belongs for a steady well-conducted soldier and who generally is the man’s own comrade” [so much the worse] “to nurse him, and to attend upon him throughout his illness, but who is relieved by another as often as the Medical Officer in charge of the case considers necessary.”
The following is the average number of sick in Army General Hospitals in time of peace at home, for whom night-nursing is considered necessary by the Medical Officers. But it is important to add that this number would be probably estimated as very much higher if proper means of night-nursing were at their disposal.
Of constantly sick mean proportion per cent. requiring night nursing:
| General Hospital, Fort Pitt Medical Division | 5 |
| General Hospital, Fort Pitt Surgical Division | 1 |
| Garrison Hospital | 2 |
These cases are usually scattered through the wards.
It is but fair to add that the best Medical Officers[107] themselves desire another system, or rather are aware that there is at present no system at all, and would gladly accept one. “With means for good night-nursing,” they say, “arrangements in accordance might be introduced. At present we like to have a case requiring much attendance amongst cases that require little, in order that the patients or comrades may assist.”
What are the consequences of such “assistance” to the cases in question has already been fully stated throughout these notes.
“With respect to the use of [the inmates as] servants, they require the strictest superintendence on the part of the * * officers. The employment of [the inmates] in offices of trust is inexpedient, inasmuch as it tends to impair the discipline of the house. In offices of mere labour, which can be performed under trustworthy superintendence, [the inmates] may be useful. Where responsibility is involved, paid servants should be engaged.”
The above is one of the regulations of what?—not of a Charitable Institution but of the Poor Law; and the house of which it treats so tenderly and wisely is—a Workhouse![19] If paupers are to be thus cared for, how should it be with our soldiers? If any “office” can be called one “of trust,” surely it is that of carrying out the orders of the Medical man in a critical case, a case of life or death! Can any “responsibility” be “involved,” greater than this? Yet these are just the cases left to the “Comrade Patients.” For ordinary cases the ordinary attendance is given; for serious cases, the untrained and unskilled attendance. Yet, if the Hospitals are not for these serious cases, what are they for? For these alone, however, is no systematic provision made. One would think that every bad case took the Hospital by surprise. Imagine the orders of the Medical Officers carried out by nurses (?) changed “every two hours,” and who are, in fact, sleepy patients!
The system of Military nursing and management, as described by Army Medical Officers themselves in the above quotations, and which is, we are expressly told, to be re-enacted at the Royal Victoria Netley Hospital, is precisely the one which led, as[108] a matter of course, to the calamities, as far as nursing was concerned, in the Hospitals in the East, and which will lead to them again so long as it is continued. Even in the case of invalids, who may not require such careful attendance as sick, the system of nursing by comrades is most objectionable; and if the attendance at Netley can only be carried out on such a plan, it is doubtful whether Netley should be used even for an Invalid Hospital.
The question has been asked the Netley Committee, By whom are your Invalids to be nursed, when sick? And it has been answered, that they are to nurse each other!
It is essential that between every two wards, in a hospital where the blocks are built end to end, there should be, as at the new Military Hospital of Vincennes, a lobby with a thorough supply of pure fresh air.
If it were possible, where the Head Nurse, or rather in a Military Hospital the Nurse, has charge of two such wards on the same floor, to let her have a long, narrow room, with screened windows, opening into both wards, the door opening into the passage in the midst, it is worth contriving.
2. The Medical Officer’s room should be on the ground floor at the entrance and apart from everything else.
The servant or whoever cleans the room, should not be a Ward-Orderly, (ward-attendance cannot be kept too entirely separate from all other concerns).
3. The ward water-closet should have a pane of glass at top, so that a faint gas-light in the lavatory at night can light sufficiently the closet, and the (bed-pan) sink.
The water-closet should be constructed, as is done often in those of English railway stations, so that each visitor involuntarily, on rising or on opening the door, purifies the concern.
Besides the ward water-closet, there should be general water-closets, and urinals separate from the wards, for the use, during the day, of those patients who can leave the[109] wards.
The latrines at the Lariboisière Hospital are a good example, both for what should be avoided in construction, and what should be imitated in position.
The sort of latrine used there would never do for England.
The men able to go out are expected to use by day an urinal in a corner of the little garden belonging to each pavilion.
At night no sick men are allowed to leave the ward on that or any other pretence; they must use the latrines.
The latrines are at the furthest end of the ward. Opposite the one door is a partially glazed door, beyond this is a large window, grated in network as well as with panes and frame. On one side opens a space where the men, able to get up, are expected to wash, and which, moreover, contains two latrines, each separated by a partition and secured by a door. The same arrangement prevails on the female side.
The rule of having the water-closet on the furthest side of the ward, removing all pretence of leaving the ward by night, is excellent.
4. The importance, immense addition of efficiency, and ultimate economy of carrying warm and cold water into every ward, and the necessity of intending and contriving this in the first construction of a Hospital,—subsequent additions and alterations being generally less effectual, and always more expensive—cannot too frequently be repeated.
5. Corridors as proposed at Netley are useful and objectionable. They lie between one side of the wards and air. They make oversight of the patients more difficult; and when a number of patients are walking up and down them, the serious cases in the wards are disturbed. On the other hand, it is desirable to have some place of exercise and yet shelter for patients, capable of being heated and of being overlooked. There ought to be no accumulation of patients at the same time suffered.
With regard, however, to corridors inside the building, if there are none it is all the better for the sick; that each ward should have two rows of large windows opening direct into the outer air is indispensable, as has often been said already.
6. Provided this double range of windows be secured, double wards of thirty on the same floor would cause no disadvantage to the sick.
But, if such be determined on, let especial care be taken to separate the two, not by a showy hall, but by a lobby and an ample staircase, extending from top to bottom of the building, and communicating freely with the open air at the roof, as well as by the stair-windows: admitting a thorough current of external air, so that, of a morning especially, the two wards do not mutually send the close air into each other.
The lobby should not be turned into a vestibule. Thorough air is all that is wanted. Patients should not be suffered to remain in it.
7. The material of the different utensils required for ward service should be settled. In the use of glass or earthenware for all eating, drinking, and washing vessels there is great superiority as to cleanliness, and the saving of time and labour in cleaning these materials, to those of tin or other metal. Still two things have to be weighed against these great advantages. First, if these vessels are cleaned by Ward-Orderlies, the amount of breakage would be much greater in proportion than as done by Nurses, and it is imperative to have as few women as possible in the service of Military Hospitals. Secondly, it is very important to avoid even the appearance, especially at first, of anything like introducing luxury into Army Hospitals; and I can quite understand this appearing like luxury.
The material of one description of ward-vessels should in particular be left to the Surgeons. In sending to distant foreign or war-stations, urinals of tin have one material advantage over those of glass or china, that they do not break so easily; but, as to home-service, these tin urinals cannot, by any amount of cleaning, be freed from an unclean smell. In Vienna General Hospital, where economy is exceedingly attended to, all the urinals are of glass, as the superior cleanliness is considered well worth the additional expense. A damaged or broken glass or earthenware urinal is dangerous; and if there is difficulty in obtaining the immediate issue of a new for a damaged one, it is better to have tin.
In Vienna General Hospitals the patients’ eating vessels were formerly of tin; but were some time ago furnished of earthenware, for the same reasons as those given above; [111]also because the hot tin vessels were found awkward to the patients. (I do not think much of this latter reason; in hospitals, there is little fear of food reaching the patients too hot). In Vienna and Berlin Military Hospitals the eating vessels are all of tin.
8. In building a large new Hospital, the question of whether or not reserve wards, or Pavilions, should be provided is an important question, to be referred to the proper Authorities. In one German Hospital is a Sommer-Lazareth, or separate Hospital, which most of the sick occupy during the six summer months. This is considered the best plan; but so expensive that well-considered arrangements in designing the building may render its adoption unnecessary. In another German Hospital is a group of wards on each of two floors, into which the male and female patients, especially the surgical cases, are successively moved; both in order that during this time the other wards may be thoroughly cleaned; also to change the air; also in case of some sudden epidemic, &c.
In every Hospital a thorough cleaning of the wards is essential. In three of the great London Hospitals this is done every year, in one every three years. Nuisance as it is, for the time being, it is such a complete purification of places which want purifying, that having it done every year is preferable to every three years. For the same reasons bare white walls, whitewashed every year, and oftener if there has been some sudden outburst of any zymotic disease or Hospital gangrene are preferable to all colour. But polished impervious cement is, it is needless to repeat, the only really safe Hospital wall. When the cleaning time of a great London Hospital draws near, the number of patients is gradually reduced, and none but urgent cases taken in. The cleaning usually begins with the topmost ward of one part of the building, or of several parts of the building at once. The patients are usually moved to the ward immediately beneath. The ward goes through a complete purification, also reparation of whatever wants repair. All its furniture ditto; the bedsteads in particular. Afterwards windows and doors are left wide open for two or three days, and nights so far as feasible. In about a week from its commencement the cleaning is over; the patients moved back; and the ward or wards so cleaned recommence their usual taking-in—and so [112]on. The cleaning of a great London Hospital usually takes two full months; and a great nuisance it is for the time, but the place benefits by it the whole remaining ten. It is excellent economy to have plenty of hands, so as to have the cleaning part, in distinction to the airing part, done as quickly as thorough cleaning admits of. It is very bad economy to put too much of this great extra cleaning upon the Nurses. This would of course not apply to a Military Hospital, where it is important the Orderlies should become as thoroughly qualified as may be for foreign and war service. It is necessary that whatever exterior help is called in, should be closely overlooked; contractors and contractors’ servants being seldom overmuch troubled with conscience.
Now it might be exceedingly worth while to have one or more reserve Pavilions, with a view to this annual cleaning.
If the flooring of polished oiled boards should be found to answer (that it should receive a fair trial is very desirable, as it might result in a material benefit to our Hospitals), it would be doubly useful, when, every third year or so, the oiling and polishing required renewal, to leave the newly-oiled wards empty for a fortnight. An additional week or two would additionally harden and improve the flooring; but a fortnight would suffice.
It might also be right to have reserve wards for what must occur every now and then in a Military Hospital, an influx of patients beyond the usual number, or an outbreak of cholera, or some malignant epidemic, which it might be desirable to isolate from the other patients.
It may now be confidently expected that, under the new régime, the progress in improvement of Military Hospitals will proceed rapidly; that it will be quietly done is almost as certain—real improvement and noisy philanthropy being fearfully inconsistent with each other, especially in that momentous machine called the Army of England, which is no safe plaything.
Dr. Helm, the Director of the Vienna General Hospital, in a little pamphlet published some time ago, insists on the importance, in designing a new Hospital, of providing Reserve wards, especially with a view to dangerous epidemics. They should admit, he urges, of easy and complete isolation from all[113] the remaining parts of the building.
9. Dr. Esse, Director of the Charité, at Berlin, in a practical and systematic, but pedantic and pudding-headed, little book on Hospitals, published in 1857, strongly urges the importance of occasionally revising and altering the rules of Hospital Officers and servants, and all the Charité instructions end with this proviso of alteration. It is one of our many unavoidable difficulties that it is necessary to begin our work under definite rules, while it is also necessary to consider the service, for some years to come, as tentative and experimental. It is well to bear in mind what cannot be expressed.
10. In admiring much, very much about the German Hospitals, it becomes necessary not to omit a warning. A number of women, all equal among themselves, with no female Superior or Superiors whatever, under the sole control of men, in an ascending scale from the Abtheilungs-Inspectoren or Oberkrankenpfleger, through Doctors of sundry ranks, to the Director himself, such is the system followed, as in the great Charité Hospital at Berlin, so in the great General Hospital at Vienna; and this cardinal mistake leads to many others.
11. It is desirable that the Rules should give daily exercise to the Nurses, or rather that the Rules should give them the right of daily exercise; that the Superintendent should encourage and exhort them to take fresh air daily when feasible, leaving them sometimes to take a little quiet in their rooms. But in war service, and sundry foreign stations in time of peace, not merely exigencies of service (which at home will and ought often enough to curtail or abrogate exercise time), but various other reasons might render it very undesirable to give the Nurses right to two hours’ daily exercise. It must be impressed upon all Superintendents, that it is essential in the long run to the health of Nurses to have fresh air; but in many foreign stations it might be far better for the Superintendent to take, or rather send, them out for one vice two hours, &c.
In war and foreign service, the exercise time must be at the discretion of the Superintendent.
There may be awkwardness enough on sundry home stations in allowing each Nurse two hours at her own discretion outside of the Hospital every day. Still it is right to look things in the face. The Rules do not contemplate a Sisterhood, but a [114]staff of secular women, bound by strict rules in all that concerns the duty they undertake, left to themselves as to sundry things which in Sisterhoods are ruled. (How and by what measures in process of time strong and quiet religious influence may be brought to bear upon this staff, is the question of vital importance as to the whole; without it, I doubt whether the service of women would, in the long run, answer in Military Hospitals, which are and must remain very peculiar places; with it, it might please God to suffer good service to be done Him). Nurses trusted to do their duty in wards must be trusted to walk out alone if they choose, and I would not attempt to restrict it, though the Superintendent must see to this, so far as she can without doing or encouraging spy-work, a thing which has many advantages, and is often done in various, very various ways, but which in the long run brings no blessing, and pro tanto, degrades all who are concerned with it.
12. In Vienna Military Hospital each set of five or six wards, with 30 or 40 patients, sometimes 20, in each, had a Sergeant and a Corporal over the Orderlies. (Berlin Military Hospital is served by Civil male Nurses).
I think a Ward-Master would be enough for each Pavilion of six wards of 30 patients each, in three stories, each couple of wards being in charge of a Nurse, and each ward served by three Orderlies.
1. Proper military and medical advice should be taken as to whether it would be advisable to draw a distinction between the venereal and the other patients.
In the Vienna Military Hospital they are locked up by themselves in particular wards, but are allowed to see their comrades at visiting hours.
In the Berlin Military Hospital they are locked up in wards, and allowed to receive no visits whatever, excepting, of course, from the Chaplain and the proper Military and Medical Officers; and in the case of dying patients from their nearest friends.
Nor are [115]they allowed exercise in the grounds.
This excellent regulation makes them heartily tired of the venereal wards, and even this is a very salutary thing.
In the Vienna and Berlin Civil Hospitals, the venereal patients of both sexes are also placed in locked wards, and allowed no visitors. Nor are they allowed exercise in the grounds or garden.
In the two Paris Venereal Hospitals no visitors are allowed.
Now, as the more disagreeable the subject, the more necessary it is to be explicit upon it when entered upon, this wholesome discipline exists in a very faint degree in our great Civil Hospitals,—a thing not to be lost sight of in introducing any change in the Army Hospitals.
The three greatest London Hospitals have venereal wards. The female patients never leave the ward. The male patients take exercise in the court. In one case the rule is, that this should be at different hours from the other patients; the rule is not strictly adhered to.
The exercise question should, in Military Hospitals, be left entirely to the Surgeons; they may fairly consider it enters into the question of treatment, which is different from the Continental treatment. The enforcement of different hours of exercise from those of the other patients is good, as is every brand which can, quietly and effectually, affix disgrace to these wards.
Deprivation of visitors, if it could be done, would be very salutary. In the great London Civil Hospitals, men and women visit the male venereal wards; women alone the female wards (and melancholy things are the visiting hours there; here and there a heart-broken mother, abundance of prostitutes, and no lack of procuresses. A firm and vigilant Head Nurse will sometimes refuse admitting one of the two latter sorts to some patient, whom she knows they are endeavouring to make sure of again; but as the rules admit female visitors, and she is by rights only entitled to eject a visitor whose behaviour is disorderly in the ward, the Head Nurse can only do this in point of fact by straining the rules, and cannot do it often). The female visitors of the male venereal wards are usually, on the average, much less disreputable than those to the equivalent female wards; and are generally wives, mothers, and sisters, seldom prostitutes. There can be no doubt, however,[116] that it would be much better if the patients of neither male nor female foul wards were allowed visitors, unless in the comparatively very rare cases of extreme danger; it would, in that case, be necessary that the Hospital should supply them with linen, and either supply them with groceries or forbid their receiving them from without.
In various essential respects the patients of a Military Hospital are different from those of a Civil Hospital. Were it possible to prevent all female visitors to the wards, except in dangerous cases, this would be best. If the existing rules or practice do not compel the sentries to refuse entrance to all disorderly women, however orderly their behaviour, such a rule, at any rate, should be enforced. And if all visitors, male and female, including, of course, soldiers, could be refused admittance to the venereal wards, always excepting cases of great danger, it would be very desirable. At all events, it would be very desirable to have all female visitors, without exception, excluded from these wards. These things are, I do consider, very important. But I would not press them, if refused.
Let the female service obtain, please God (I do not write these words pro formâ,—if possible, I feel every day more intensely how solely it is to Him we must trust in this difficult work,—the more so that, if possible, I feel every day more intensely the importance of, if He grants it success, improving secular Hospital nursing, leaving the English Sisterhoods, which will always have great advantages, and, I believe, great disadvantages, with reference to Hospital nursing, to take their share in this great field, which has plenty of room for both), let, I say, the female service obtain a firm footing in the Army Hospitals, and with it, and by cautious degrees, sundry ameliorations will creep in insensibly as to decorum among other things. Those solemn beautiful words I have always felt so full of meaning to us, “In quietness and in confidence shall be your strength.”
2. Military as well as Medical advice should also be taken upon the following point:
In most, not all, the great London Hospitals the patients, whose names are on their bed-tickets, are called by the numbers 1, 2, 3, &c., suspended over each bed; sometimes a[117] patient’s name is never heard in the ward.
Now, very possibly, this would not at all do in a Military Hospital, and, if so, there is not another word to be said about it.
Otherwise, very few things so effectually save time, as the numbering plan. (In Civil Hospitals it is also excellent in other ways, of much less consequence in a Military Hospital, which will never, I conclude, be afflicted with “gentlemen,” Mr. So-and-So, and Master So-and-So, which latter inscription is frequently to be read on the letters of little boys in Hospitals, whose friends, on visiting days, also enquire for them by that title). But few things, I repeat, so effectually save time as numbering instead of naming the patients (names, of course, to be on bed-tickets). If, however, the officers consider it “unsoldierly,” give it up at once.
3. The regulations lately in force contained in plain strong language prohibition of swearing and indecent language in Hospitals; they are quoted from the Articles of War. It would be well to retain this in any new Regulations; and the retention of this Rule is not the less important when women are put in charge of Military wards, since, though it is not their business to maintain discipline, it is their duty to call in those whose duty it is when discipline is infringed. And it is important that this prohibition of swearing and foul language should not be looked upon as an individual or collective crotchet, or female innovation, but remain the rule of the Service. Such language would never be used in the Nurse’s presence unless by her own fault. But it should be unheard in the ward, whether she is in it or not. The old definite words should be transcribed.
I do not like writing any part of the above, not because it can, in any sense, be said to strain the necessary principle of reserve, save for strictly business purposes, as to all which is, strictly speaking, Hospital business, but because of the extreme caution necessary as to this sort of topics. Still life is so uncertain that the possible introduction of permanent Female Service into Army Hospitals has determined me on writing what I had rather not have written.
The question of ventilation is so all-important, so much doubt still seems to exist as to the comparative merits of natural and artificial ventilation, so much has been said in favour of the latter, because it is seen adopted in the finest hospital in the world, the Lariboisière, that I have added a few practical remarks upon this system. The conclusion is, that even at the Lariboisière, without opening the windows occasionally, and especially in the morning, real freshness is never obtained in the wards, and that, therefore, if there must be artificial ventilation, that is the best which allows the most of the windows being opened.
On the men’s side, Thomas’ system, or that of injecting air at given points, by means of two high-pressure steam engines, each working a large fan, is adopted. On the female side, Duvoir’s system affords ventilation by extracting air at given points. In both, a number of shafts and openings provide for the exit of the air.
Persons at the Lariboisière Hospital, who ought to be good judges, including foremost the Director, an experienced and able administrator, consider the ventilation on the male side the most expensive and the best, both for day and night, being the coolest in summer and the warmest in winter. In winter two great advantages are assigned to this side: first, the heating being provided by the Hospital, the wards are warmable at pleasure; whereas that of the female side is provided by the contractor at a fixed degree of heat, which, in extra cold weather, is augmented: from 15° to 18° C are the usual limits of the winter temperature on the female side, while that on the male side is usually several degrees higher. Secondly, the system of heating on the male side permits the windows to be opened: while on the female side objections are often made to opening the windows in winter, which it is alleged interferes with the heating.
Per contrà. How difficult it is to learn any facts by hearsay we know. Other persons who ought to be good judges think the male side apt to be too warm in winter, especially at night, and consider the temperature on the female [119]side quite sufficient.
Both sides are ventilated both by the windows and by the machinery by day in summer. Both sides are ventilated, each by its own different machinery, by night in summer, except that, exceptionally on hot summer nights, a window is opened two or three times in the night, or five minutes every hour.
Both sides are considered to be ventilated in winter mainly by the machinery by day; and both sides are entirely ventilated in winter by the machinery by night.
As far as can be made out from conflicting accounts, (conflicting from the very simple reason that one person will consider a ward, or drawing room, for that matter, airy which another will consider close; one, pleasantly warm, another too hot or too cold), it is practically found impossible to freshen the ward of a morning without opening some windows, and to keep it fresh during the day without now and then doing the same; and it is easier to open the windows on the male side in winter than on the female side.
The ventilation on both sides is considered to work with equal efficiency during the whole of the day.
Of the eighteen wards, the ventilation on entering the wards at five a.m., when the ward nightwatch has generally not opened a single window, is certainly surprisingly good; i.e. the air is surprisingly little bad. But neither here, any more than anywhere else, are the wards effectually freshened, until the windows are, of course with proper caution, opened.
In both these particulars, no difference is to be observed between the male and female side.
In repeating that the Director, and other persons who ought to be good judges, consider the machinery of the male side the most expensive and the best, I add these things:
First. Since this machinery was erected, so far as concerns the steam engine, it is said that equally efficient and much less expensive engines have been erected in other Hospitals, among others, Necker and Beaujon. In both Hospitals, the plans of Duvoir and Van Heecke are in use, one on either side. But certainly, the system of outlets at Beaujon for the foul air is by no means so good as at the Lariboisière.
Secondly. If an accident happened to the machi[120]nery of the male side, which is in communication with the steam engine, the results might be very serious. Twice a stove has burst on that side, happily without damaging anything else than furniture near it; had patients been near it, they must have been hurt or killed: and an accident on a large scale might blow up not a small part of the Hospital.
More or less danger is inseparable from powerful steam machinery, or powerful machinery of any kind: the question is one of degree.
Thirdly. Both sides of the Hospital have one thing in common. Except the sculleries of the 3 ground floor wards on the male side, which have each a stove or fire place, the kitchens or sculleries attached to all the other wards are warmed by hot water. Undoubtedly this saves much mess, much cleaning of stoves &c., and much bringing of fuel and consequent dirt. But the absence of fire is always a loss to the service of a ward. Sundry things, some one or other, often all of which are constantly wanted in a large ward, e.g. warming broth or drink, cooking for an extra bad case, warming poultices, warming (not airing) linen for ditto, &c., &c., &c., are much more slowly done by water than fire heat, and it is a question, variously answered, whether some of these things are as well done by the slow water method, as by the quick fire heat. Occasionally the hot water is not forthcoming, a nuisance alike to the ward attendants of the ward whose scullery is thus heated, and to those of the wards supplied with stoves, which have then to do, in driblets, considerable extra duty.
During the hot months the smell of the latrines is very little perceptible in the wards, generally not at all: but the test of this, as of the ventilation, is in winter, when the large window close to the latrines is generally closed, and the smell is very offensive.
1. They have in common the superiority over common floorings—that they are not scrubbed, and the damp thus arising is avoided.
2. As re[121]gards labour, so far as Civil Hospitals are concerned, where the ward service is done by women, parquets would be more laborious than scrubbing; a large ward, to be kept in a proper state, requires a certain amount of frottage (the peculiar polishing of parquets) every day; and this frottage is held to be unfit, from the fatigue it causes and the strength it requires, to be done by women, and is always done by men. Certainly Ward Nurses could never be required to frotter; it is altogether a man’s business.
3. As regards labour, so far as Military or Naval Hospitals are concerned, where men preponderate in the ward service, it is my impression (for of course I cannot pretend any certainty as to this), that sailors who are proverbially handy (a different quality from either laboriousness or endurance, though they have these too) would, with instruction and painstaking, accomplish in time frottage; that civilians would under the same conditions; that soldier orderlies (infinitely, I humbly think, the best material for the staple of military ward service), would generally make bad frotteurs.
4. As regards labour, cleaning oiled boards, though a laborious business, is much less so than either scrubbing or frottéing; and is fully within the power of average strong women: none other should nurse. (What subdivision of cleaning the ward, and of nursing properly so-called, might both improve the work done and relieve the Nurses, is another thing; my impression remains, that it is better to consider these things to a certain extent as distinct duties, discharged by women ranking alike; and that in a ward of forty, served by a Head Nurse and three Nurses, to charge one with the main ward cleaning, is better economy of strength and time than to divide it among the three).
5. As regards labour, any Orderly giving his mind to it for a day at the shortest, or a week at the longest, ought to learn thoroughly how to clean polished oiled boards well, always supposing him to be properly taught a very simple thing, which, like everything else, can be done well, ill, or indifferently.
6. Apart from the question of labour augmented or spared, the advantages of oiled and polished boards I believe to be these:—
(1.) Prevention of dust.
(2.) More easy purification[122] of the air of the ward in the morning.
The air of every ward becomes more or less impure during the night, and the floor and furniture more or less dusty. Making the beds in the morning adds to the dust the night has accumulated.
The dust is more thoroughly destroyed by the cleaning necessary to oiled and polished boards of the Bethanien variety, than by any other cleaning I have seen. It is fairly destroyed; whereas both parquets and boards generally retain a little.
Also, the water, with which the oiled boards after being swept are cleaned, freshens the ward and purifies it of the closeness remaining of the night air, in a very speedy and remarkable manner, which is even more evident as well as more useful in winter than in summer—as in winter it is not possible to admit as much air from the windows as in summer, especially when it is most wanted, in the cold, close, early mornings.
The advantages of oiled and polished boards as counteracting the spread of miasma, which is strongly dwelt on at Berlin by competent authorities, I have not alluded to, as probably parquets are considered equal in these respects to them.
Stains, mess, and dirt falling on polished oiled boards are much more easily cleaned than on parquets.
1. Take a common hair broom, a broom with a hard brush, a cloth of coarse flax, and one or two pails of cold water.
2. Sweep the floor and skirtings with the hair broom.
3. Dip the cloth in a pail, wring it gently between the hands, so as to have the whole equally wet, not running. Throw it on the ground, reverse the hard broom, and placing the reversed handle upon the cloth, clean the floor close to the skirtings, not the skirtings themselves, and the corners. When the cloth becomes dry, rinse it and re-wet it in the same pail.
4. Then wet the cloth somewhat more, wringing it as before, throw it on the floor at the end furthest from the door, and placing the brush of the hard broom upon it, brush, firmly and quickly, each board in the direction that the boarding[123] runs, about as far as the arms can reach, standing, not kneeling. A small ward can be at once brushed wet, a large one must be divided into parts, and each part be successively brushed wet and brushed dry. When the cloth becomes dry, rinse it and re-wet it.
5. To brush dry, rinse and well wring the cloth, brush as before. The firmer you can press, the better and quicker the floor will be dried. When the cloth becomes wet, rinse it and wring it as before.
6. Change the water when dirty. More or less water must be used, according as the floor is trod by dirty boots and shoes.
7. Aim at drying the floor by one dry brushing; if not, it must be dry brushed a second time. Once should suffice.
8. Ten minutes, at the furthest, after the dry rubbing is over, the floor ought to be thoroughly dry. When it is quite dry, sweep quickly over it with the hair broom.
9. On putting by the cleaning materials, rinse well the cloth in clean water.
1. Brush the skirtings with a small hard brush, and wipe them dry with a rag, as the cloth would be too large, and wet the walls.
2. Use more water to clean the floor, which will probably require two dry brushings.
3. Clean the brooms and pails.
1. Throw warm, not hot, water on the floor, and brush firmly and quickly, wet and dry. A very little soda in each pailful will be an improvement. More than very little will injure the flooring.
[A new cloth, which it is economical to cut from a great piece which makes into some or many dozens, should be steeped for a night in a pail once filled with boiling water, an[124]d in the morning rinsed and wrung several times in clean cold water, then used at once. Two or three new cloths can be steeped in the same pail.]
1. Wherever practicable build the hospital on arches; but, for the sake of discipline, they should be locked up.
2. If practicable, let the laundry, if served by women, be removed from sight of the place where the patients take exercise, and of the ward windows.
3. In a Civil Hospital it is objectionable to give the female patients right to take exercise in corridors which the officers and servants have constantly to traverse to go to and from the wards. In a Military Hospital it is of little comparative disadvantage that the patients should do this, although,
4. In building a hospital it might be well worth while to contrive that the covered space, essential to give the patients power of taking exercise, should be used solely for that purpose.
5. In Germany, the general opinion is in favour of small wards, twenty beds are considered the desirable maximum; twelve, per se, better than twenty.
Ditto in Belgium, under the same restriction, although, in practice, there are wards containing larger numbers.
In the old Hospitals at Paris, the number of patients is too large. The Charité has long great wards of 100 and 120 patients. At St. Louis (which is mostly for cutaneous, not venereal, diseases, where the patients usually are long under treatment and able to go about, and where there is little acute illness,) wards of eighty and seventy beds are the rule, smaller wards the exception. This may be considered an exceptional class of patients. The Charité, somewhat densely pressed upon by neighbourhood, is also not considered a favourably circumstanced Hospital as to air.
Putting aside for a moment the sanitary question, which we have fully discussed elsewhere, and which appears to be decided in favour of wards of from twenty to thirty patients, we will look upon the question of administration. The[125] moment we consider that a great public Hospital has to provide efficient attendance for all the sick it receives, that it must be economical of attendance, both because the expense of attendance, as well as the other requirements of the sick, commands all practicable economy; and because efficient attendance in sufficient numbers is difficult to obtain; it becomes evident that it is far better for the sick to have larger wards, efficiently served by as few attendants as is compatible with efficiency.
This, which is the fair statement of the case, strikes those who have watched the working of the system of small wards in North Germany as more true than ever.
Such persons consider that the size and numbers of the wards at the Lariboisière Hospital, viz., thirty-four beds, including the two in the little ward, are good: that preserving the existing considerable space between the beds, and supposing the same ratio of conditions as to windows, &c., and the small ward for two at the end, wards of forty or fifty would be equally healthy for the sick, but that the number fifty should not be surpassed.
Assuming, however, that thirty patients in a ward, or thirty-two, are the maximum number, sanitary and administrative necessities being conciliated, let us see what we do in our Military Hospitals at home.
In most of our Regimental Hospitals the number of wards and of holes and corners, in comparison with the number of sick, is quite extraordinary.
In a hospital for a battalion 500 or 600 strong, we shall find eight or ten wards of small size, a small kitchen, everything, in fact, on a small scale, just as if a large French Hospital had suddenly collapsed.
How much more sensible would it not be to have one or, at most, two large wards for thirty sick each, with a small casualty ward and an itch ward!
How much less expensive such a structure would be in erecting and administering, and how much more easy would be the discipline and oversight, not to mention the greater facility of ventilation!
6. There is not[126]hing at the Lariboisière Hospital answering to casualty wards. Besides the eighteen wards of thirty-four each, the Hospital contains two little (and inconveniently placed), wards of ten beds each, which, when medical cases overflow, are made medical wards; and which are closed when the ordinary wards suffice. But of casualty wards, for offensive, or noisy cases, there are none, and the double-bedded little ward at the end of each large ward is intended to answer this purpose; also, but subsidiary to this, to allow now and then a patient of the better class to have the comparative privacy.
This latter consideration does not apply to a Military Hospital. As to allowing Non-Commissioned Officers for instance to be in the little wards, discipline would, I think, very soon suffer.
But if casualty wards are provided for extra offensive, and noisy cases, it seems to me that any Hospital would be much better without these small wards attached to each larger one.
Apart from the purposes which the casualty wards answer, they are a nuisance. If convalescent patients are put into them, they are comparatively removed from inspection, and often play tricks there. Patients requiring much attention can seldom be put there, however their condition otherwise fits them for the little ward, because the ward attendants, and especially the Sister (as in secularly served Hospitals the Head Nurse), find it impossible to serve the inmates of the little ward properly, if there are also many serious cases in the large ward.
I submit therefore that the small ward is only an incubus, if casualty wards are provided. One thing is certain: a patient requiring much attendance, put into a little ward, ought to have an extra attendant to himself, by day and by night; otherwise, either he is more or less neglected, or he unduly monopolises the service of the ward attendants.
It remains a question for far others than women to settle, whether offensive and delirious cases are under more favourable conditions of cure when scattered in little wards, than when assembled in a large, or in several small wards. On this subject, I can only add my confirmed belief that a large airy ward, provided with a few small wards, and with complete ward attendance, is a much better place for the care and[127] attendance of such cases, than small wards attached to the ordinary wards.
7. Avoid many holes and corners. I could not recommend a dining room for patients attached to each ward, or floor, or pavilion. If there is any dining room, let all the convalescent patients of the wards not being convalescent wards, dine together in a room apart from the wards, and let the rest dine each at his bed side. If not, let each patient dine at his bed side.
At the Lariboisière Hospital, each ward has a vestiary, a doubtful arrangement. The nature of a Military Hospital renders it proper to have but one vestiary under charge of some man.
8. If possible, let all foul linen be delivered daily, twice perhaps better than once daily, into the laundry, so as to remain the shortest possible time in the neighbourhood of the ward; otherwise, do what you will, foul Hospital linen will fairly, to say the ugly truth—stink, and its temporary receptacle will stink also. I would not make this temporary receptacle a room. A large chest in the scullery, a region under constant purification by fire and air, would be, as already hinted, p. 88, the least bad place for an accumulation inevitable to all Hospitals, but which should accumulate for as little time as possible.
9. Provide from the first room for storing and issuing dried clean linen, as well as laundry room.
10. In badly-planned Hospitals artificial ventilation is an excellent auxiliary for expelling the foul air, engendered in the ward, especially at night; but windows only can be relied upon for introducing good air. Let Hospitals, therefore, be so constructed as to admit of opening one or more windows as much as possible all the year round, with as little chance of draught as may be to individual patients, which can be done by providing double windows, opening above and below, or by some similar expedient.
There are no words in regard to which there is more misconception, or more nonsense talked and written, than the two words “contagion” and “infection;” and as the word “infectious” has been used in these Notes, it is necessary to say what it does mean, and what it does not mean. The word “contagion” appears to have been first used by certain classical writers to signify the spread of scab among sheep; and it would have been well for humanity if the word had been restricted to this very primitive bucolic signification. It was not till centuries after Virgil’s death that the common sense of men had descended so low as to introduce it into the Medical vocabulary. This took place at a period when, from the neglect of sanitary arrangements, pestilence attacked whole masses of people, and when no one appears to have considered that nature had any laws for her guidance whatever. It was not until human intelligence had descended to this depth that men seem to have bethought themselves of Virgil’s term as affording them an adequate explanation for pestilence, and sufficient reason for not exerting themselves to prevent its recurrence. So it has continued ever since. The little word used in all innocence by the poet for poetic purposes has become the ground-work of every manner of false observation, false reasoning, neglect of sanitary laws, lazarettos, quarantine, and continually-threatened interruption to the commercial intercourse of mankind. No single word has ever done so much harm to the human race, or given such a proof of what a mighty thing a word is!
One would have thought that, after the sanitary experience of the last fifteen years, the word “contagion” would have disappeared from our language; but, even in the last document issued by the expiring Board of Health, written by their Medical Officer, Mr. Simon, and based on erroneous statistical evidence (Papers relating to the Sanitary state of the People of England, 1858), it is stated that “a further—practically speaking, unavoidable—cause of premature death in every civilized country is the risk of its current contagions.” [The italics are not mine.] And this refers to small pox, hooping cough, measels, and scarlatina, the mortality from which we are to presume, is [129]“unavoidable.”
If this be Board of Health doctrine, it is certainly not sanitary doctrine. It would have astonished the Health of Towns Commission, and the first Board of Health.
“Contagion,” as its etymology implies, means the communication of disease from person to person by contact. It is often confused with “infection;” but it has quite a different meaning. Contagion presupposes the existence of certain germs, like the sporules of fungi, which can be bottled up and conveyed any distance, attached to clothing, merchandize, especially to woollen stuffs, for which it is supposed to have a particular affection, and to feathers, which of all articles it especially loves, so much so that, according to Quarantine laws, a live goose may be safely introduced from a plague country; but, if it happens to be eaten on the voyage, its feathers cannot be introduced without danger to the entire community. The absurdities connected with the doctrine are numberless. Suffice it to say that in the ordinary sense of the term there is no such thing as “contagion.” There are two or three diseases in which there is a specific virus which can be seen, tasted, smelt, and analysed, and which, in certain constitutions, propagates the original disease by inoculation, such as small-pox, cow-pox, and syphilis, but these are not “contagions” in the sense supposed.
With regard to the mysterious, imponderable, indivisible nonentities, which make up our “current contagions,” they may safely be dismissed into the limbo of extinct superstitions.
The word “contagion” therefore is altogether objectionable.
The word “infection” expresses a fact, without involving a hypothesis.
It is most necessary, however, that the meaning should be guarded; for, just as there is no such thing as “contagion,” there is no such thing as inevitable “infection.” Infection acts through the air. Poison the air breathed by individuals and we have infection. Shut up 150 healthy people in a Black Hole of Calcutta, and in twenty-four hours you have an infection produced, so powerful that it will in that time have destroyed nearly the whole of the inmates. Sick people are more susceptible than healthy people; and if you shut up sick people together, without a sufficient space and sufficient fresh air, you will have not only fever, but erysipelas, pyæmia, a[130]nd the usual tribe of Hospital-generated epidemic diseases produced.
Again, if we have a Fever Hospital with over-crowded badly-ventilated wards, or with the air stagnant in them, we are quite certain to have the air become so infected as to poison the blood not only of the sick, so as to augment their mortality, but also of the medical attendants and nurses, so that they shall also become subjects of fever.
It will be seen at a glance that, in every such case and in every such example, the infection is not inevitable, but the simple result of gross carelessness and ignorance. In certain Hospitals it has been the custom to set apart wards for what are called “infectious” diseases; but, in reality, there ought to be no diseases considered such. It follows from what has been stated that, with proper sanitary precautions, diseases reputed to be peculiarly “infectious” may be treated in wards among other sick without any danger; just in the same way as, with proper sanitary precautions, a number of healthy people may be congregated together without becoming subject to the horrors of the Black Hole of Calcutta.
It is in the highest degree probable that we should never have heard of “infectious” wards, if the other wards of a Hospital had been supplied with sufficient space and air for the sick; and in too many cases it is to be feared that the presumed “infectious” cases are huddled away into small, ill-lighted, ill-ventilated rooms, a kind of Lazaretto, in fact, where, if they die, they have at least been kept from doing harm to the other sick in Hospital!
It is high time that common sense should deal with the question; for there does not seem to be much hope for a deliverance from these superstitions from any other quarter.
The “infectious” wards in Military Hospitals correspond, in some sense, to the “casualty” wards in Civil Hospitals, into which accidents, noisy, and erysipelatous cases are transferred, when necessary. The advantages of a separate set of wards for this class of cases have been already insisted upon in these Notes; not certainly because the cases are inevitably “infectious,” but because the segregation of such facilitates greatly administration and nursing, while it removes offensive and noisy patients out of the Hospital wards, whose inmates they would annoy. The question of infection or non-infection[131] has nothing to do with the arrangement. No stronger condemnation of any Hospital or ward could be pronounced than the simple fact that any disease has attacked other patients than those first affected by it. “Infection” and incapable management, or bad construction, are, in Hospitals, convertible terms.
It may be useful to mention what the meaning is of the words “epidemic,” “endemic,” “sporadic,” and “zymotic.”
When a large number of people are attacked simultaneously with the same form of disease it is said to be epidemic. When a small number, as, e. g., the inhabitants of a single court or alley, are so attacked, it is said to be endemic. When scattered cases of the same disease happen, one here, one there, over a large surface, the disease is said to be sporadic. The term zymotic, which includes all diseases of the preceding categories and some others, implies the existence of certain changes in the constitution or in the blood, rendering persons so affected liable to the diseases in question.
It is a vulgar error to suppose that epidemics are occasioned by the spread of disease, from person to person, by infection or contagion; for it is an ascertained fact that, before any people is attacked epidemically, the disease attacks individuals in a milder form, one at a time, at distant intervals, for weeks or months before the epidemic appears. Before an epidemic of cholera, these cases consist generally of diarrhœa of more or less intensity, followed by a rapidly fatal case or two, very much resembling cholera. Even plague itself, as in the recent epidemic at Bengazi, begins with cases which cannot be distinguished from ordinary typhus-fever, the succeeding cases getting more and more intense, until the epidemic seizure takes place. Experience appears to show that without this antecedent preparatory stage, affecting more or less the entire population of a town or district, the occurrence of an epidemic is impossible—the epidemic being, in fact, the last or, so to speak, the retributive stage of a succession of antecedent phenomena extending over months or years, and all traceable to the culpable neglect of natural laws. It is simply worse than folly, after the penalty has been incurred, to cry out “contagion,” and call for the establishment of sanitary cordons and quarantine, instead of relying on measur[132]es of hygiène. Epidemics are lessons to be profited by: they teach, not that “current contagions” are “inevitable” but that, unless nature’s laws be studied and obeyed, she will infallibly step in and vindicate them, sooner or later.
In the words of the Registrar-General, which are as applicable to Armies as to States, “Sanitary measures and not quarantines are the real safe-guards of nations.”
I have just seen a paper by Sir John Hall, entitled “Observations on the Difficulties experienced by the Medical Department of the Army during the late War in Turkey.” In this somewhat singular document, which appears to be a defence of Sir John Hall’s own conduct, there are certain statements made about the female nursing establishment in the East which require a word of comment.
It will be observed that throughout the paper, the weapon which Sir John Hall uses against all civil interference in repairing the sufferings which proceeded from the defects of his own department is simply detraction.
As for Civil Commissions, they were useless, as for Civil Hospitals, they were costly, and their officers lived magnificently and were extravagantly paid. As for the nurses, they were benevolent, pious, well-intentioned persons, but what could they do? How could one woman nurse eighty sick? The medical men thought they could not.
Why had Miss Nightingale stores of port wine placed at her disposal, which she could give to the French Hospitals, while he, the principal Medical Officer of the Army, had no such stores at his disposal?
Sir John Hall must have already discovered that this old weapon is no longer of use in defending his position.
It would have been more to the purpose had he produced his requisitions for food, clothing, comforts, &c., and shown how they were refused or not complied with. At the very time I gave over part of our own private stores of port wine, &c., to the French Hospitals (for part only of what was given were Government stores at all), Sir John Hall might have obtained,[133] out of the large wine store at Balaklava, any amount of wine he required, by merely asking for it. The simple statement of this fact would have been a better answer to M. Baudens[20] than assuming that I could obtain from Government stores and wine for the French Hospitals which he could not obtain for his own.
As to his statement about the Nurses, it simply shows ignorance of the whole matter. Nobody ever contemplated giving to a Nurse the entire charge of a number of sick in a Military General Hospital. It is no part of good Hospital nursing to do so. With proper Orderlies, a Nurse can very well attend to sixty or seventy sick. We were prevented, indeed, by the authorities, and by circumstances, from organizing a proper system of nursing, and were obliged to do all the good possible in the best possible way. But Sir John Hall’s method of estimating the efficiency of nursing, by dividing the number of sick by the number of Nurses, is simply absurd.
[2] As little reference as possible, no reference at all, if it can be avoided, should be made, on our part, to the Confidential Report, which, in 1855, was presented against the War-Nurses. The less scandal about women is reverted to the better—a truth all slanderers have always appreciated: “Calomniez, calomniez toujours: il en reste toujours quelque chose.” It would be far preferable if Nurses could enter the Army Hospitals quietly, and let by-gones be by-gones (the useful experience always excepted, which has been gained).
[3] The work was done under many difficulties, some inevitable, some which should have been spared. Things happened among us deeply to be regretted. Rebellion among some ladies and some nuns, and drunkenness among some nurses unhappily disgraced our body; minor faults justified pro tanto the common opinion that the vanity, the gossip, and the insubordination (which none more despise than those who trade upon them) of women make them unfit for, and mischievous in the Service, however materially useful they may be in it. Of all this, the material consequences might have been spared by some such “General Order” as the above, which, at least, prevents others from taking advantage and making capital of such faults.
[4] The Extra Diet Kitchens must, it is necessary to state, be under a separate roof from the General Kitchens, as long as the present system (or no-system) of cooking exists. But the sooner it is altered the better. There should be one kitchen only. But the Nurse should always superintend the administering of the Diets. She is unquestionably the proper person, also, to administer the medicines, &c. The Orderlies, to be of any use, must act under the direction of the Head-Nurse and not independently. It would seem hardly necessary to enunciate such a self-evident proposition.
[5] To all references which may here be made to Civil Hospitals I should wish to say, by way of preface:—
1. That I have always believed and I believe it more and more every day I live, that what is wrong in hospitals is to be patiently, laboriously, and, above all, quietly mended by efforts made from within them, if it pleases God to grant that blessing upon them without which all human efforts are vain, and not by accusations, investigations, and noise from without.
2. Also I have always believed, since I knew Hospitals at all, and I believe it more and more every day I live, that, with all their faults and shortcomings, which are easily learnt and more easily declaimed against, our great English hospitals are places in which more is done for the relief and cure of human misery, or, rather, of that large branch of it arising from disease, than in any other places in the world. Also that their faults are not essential to them, but that they may, by God’s blessing on the patient endeavours of many years, be very much modified.
[6] In their regulation dress they should always appear, except when they go on holidays.
But let the Queen pay for the transport of one box and one bag only, for each Nurse on duty; and if she takes more let her pay for it herself.
[7] I would allow each Nurse 1½ pint of porter or ale per diem, or, instead of the half-pint of porter, 1 oz. of brandy or a wineglass-full of wine, as she likes best. Most Nurses crave, and rightly, for a luncheon about 9 or 10 A.M., and drink some beer then. I would let them take their own time as to when they drink their day’s allowance. But, while trying to suit each Nurse’s varying tastes (and in Hospital duty the taste does vary) each Nurse must keep to one thing, say for a week or month.
[8] Better than a closet is a moveable dresser, only table-height, under which cleaning can be carried on.
There should be no projections in a ward or recess, which are only lodgments for flue and dust. The walls of a ward should be even, polished, impervious.
[9] With regard to children we might look forward to a time when a school might be formed for the children, if any, of such of Her Majesty’s Nurses as are widows. This would be an additional bond to the Service for the mothers. The children, of course, are not to be admitted into Hospital; and strict rules must be made (and kept to) as to when the mother should visit them. I do not anticipate that it would be possible ever to have married women in the Service. And it is hardly necessary to add, that no women but of unblemished character can ever be admitted.
[10] Should a woman, however, out of the higher orders, be found as efficient as one of the middle classes, as Matron, this should be no reason for excluding her.
[11] If it be desired to include some War-Nurses after 40 it would be better for the Superintendent-General, with the sanction of the Secretary of State, to take, at first starting, a few past the age, than, on their account, to alter the age. It stands to reason that, on the formation of the Staff, approved Nurses of the War-Service should be included in it, for the sake of the Service.
[12] It is better to omit the Belief. Singularly enough it is the one thing objected to by Dissenters and Roman Catholics.
[13] If the Surgeons are for the men doing it, I would not overpress this point. But, in the case of weak patients, it requires extra care, and it would be much better to leave it as the duty of the Nurse. At all events it will not answer to leave the enema and its administrator unspecified. The Medical Staff Regulations assign it to the Ward-Masters. It is a simple thing enough, but one by the careless or ignorant administration of which many a man (and woman) has been injured for life; and either the Ward-Master, the Assistant Ward-Master, or the Nurse should be responsible for it. I should prefer, as above stated, charging the Nurse with it; but if objected to by the Surgeons, I should at once let them assign it to whichever Non-commissioned Officer they chose.
[14] One Nurse might possibly be able to serve the whole Pavilion. The highest estimate is here taken.
[15] The floors are of deal; the length and breadth of the boards depending on circumstances. Wood skirtings run round the walls, following the recesses of the window and doors, 2½ in. in height and 1½ in. in thickness. The skirtings should have no indents in them, which form convenient lodgments for dust and take time to clean. A little rim must run round the top of the skirting, edging the wall. The skirting should thence descend, unindented, upon the floor. The boards are coloured and prepared, as follows: A new floor is rubbed over two or three times, with warm linseed-oil varnish, having some fine yellow-ochre, powdered, in it; then a coat of “laque-lustre,” a species of French polish, is laid over it, the result being a reddish-yellow colour, in which the grain and veining of the wood is shown. If, after being used some time, it begins to look worn, it is rubbed over with oil and a new coat of polish laid on it; but, as this takes a long time to dry, it is usual to fill up the worst parts with thin oil-colour, and then to take the yellow polish and lay it on, in two successive coats, leaving it to dry, if possible, for twenty-four hours, as it wears the better the firmer and drier it is. For old boards, that have been much used, considerably more laque-lustre is required than for new ones.
After laying on the laque-lustre it is desirable that the floor should not be trodden upon for six weeks, and it is also well occasionally, say about once a week, to polish it, which conduces much to make it serviceable.
[16] And this should be adhered to, the rare though extant cases of efficiency for Hospital nursing, past this age, notwithstanding.
[17] Great caution must be used in acting upon this. The Superintendent-General, or the Superintendents who are responsible to her, order the service of each Nurse. How far is it just to consider extra dangerous duties or stations meritorious in the Nurse who does or suffers from them? Others might have done the same, if so ordered. Others might have wished for such an order. Or a strong efficient Nurse who, in other respects, gives anxiety, may render extra useful service on an emergency, and suffer for it in health: and yet, during her whole service, have given more anxiety and less satisfaction than others who did not, perhaps had not the opportunity to, distinguish themselves by any extra useful service.
[18] The “Superintendent” and “Matron” are here used throughout as synonymous terms; because “Matron” is the shorter and more familiar name; although, for reasons before given, “Superintendent” would be the better word for Military Hospitals.
[19] If it be said that the Workhouse sick are ill-nursed, it is in proportion as this rule is broken, not as it is kept, that they are so.
[20] To M. Baudens, whose recent death is so much to be lamented, I cannot here but add a tribute of admiration for his wise and enlightened sanitary views, during the year of his superintendence over the Medical Department of the French army in the East, and of gratitude for his ready and magnanimous acceptance of our stores, when the French sick were really in want of them, after these had been refused by other French authorities.
LONDON:
PRINTED BY HARRISON AND SONS,
ST. MARTIN’S LANE, W.C.
PRIVATE AND CONFIDENTIAL.
I. Wages and Prospects of Nurses.
II. Desirability of some further Provision.
III. Of what Nature?
IV. Suggestions as to the Rules to be followed.
V. Prospects of Eventual Support.
1. The nurses of the great London hospitals are divided into two classes: head-nurses or sisters, and nurses or assistant-nurses. These latter are, generally, subdivided into day and night-nurses.
2. The head-nurses, on an average, receive about £50 a-year and no board, or lower wages and partial board; the use of one or two rooms, generally unfurnished, and an allowance of fuel and light. Sometimes uniform outer-clothing is included. Sometimes two pints of beer daily are added to the above.
3. The day-nurses, on an average, receive about 12s. a-week and no board, or lower wages and partial board; lodging, with the use of some furniture; sometimes an allowance of fuel and light apart from the use of both in the wards. Sometimes uniform outer-clothing is added to the above; sometimes they have also an allowance of one pint of beer daily.
4. The night-nurses, on an average, receive about 10s. a-week and no board; lodging, with the use of some furniture; sometimes an allowance of fuel and light apart from the use of both in the wards. Sometimes they live in their own lodgings, near the hospital, receiving the same wages.
5. I am informed that St. Bartholomew’s Hospital has no fixed scale of pensions, nor is the term of service defined. But pensions have been granted to worn-out sisters of from £15 to £25; as also pensions of smaller amount to some worn-out nurses.
6. St. Thomas’s Hospital, in like manner, has given, without any fixed rule, pensions to worn-out sisters, of from £30 to £50. A gift in money has been granted on the retirement of a sister; and the same has been done in the case of nurses who may have received injuries in the discharge of their duties; and in a very few instances of long and faithful service they have been pensioned.
7. Guy’s Hospital for a long time generously provided for its superannuated sisters, but the plan in practice being found very objectionable, was a few years since given up, and the authorities established a Superannuation Fund for the Servants of the Hospital.
It is compulsory on sisters, optional to nurses, to belong to it. Each subscriber receives a book containing printed rules, with tables of rates of ages, payments, and pensions, and also blank leaves. The subscriber selects the amount of pension for which she wishes to subscribe. At each quarterly payment of wages, a proportion is paid into[3] the fund; entered in the subscriber’s book, and properly attested; the hospital makes a payment of equal amount into the fund on the subscriber’s account. If the subscriber die before attaining the age when the pension begins, the amount paid by the subscriber is disposable by will, and in case of intestacy reverts to the next of kin. The pensions, one-half of which are thus purchased by the subscriber, and one-half presented by the hospital, vary, if I remember rightly, from £15 to £50. In February 1857, no nurse subscribed; to which three remarks apply:—first, that every good work takes time to grow; secondly, that not a few of the sisters, having looked forward to benefiting by the old system of superannuation, rather grudged their own payments than sought to induce their nurses to subscribe; thirdly, that many of the nurses were really unable to make the payment.
8. The non-endowed hospitals, I believe, but write from very imperfect information, grant few pensions. Sometimes they grant a gift of £25 or less to a retiring head-nurse. Sometimes they employ a head-nurse, become too old for her work, as an extra and inferior nurse. Sometimes they grant a worn-out head-nurse an asylum in the incurable ward of the hospital. I believe the pensions to old nurses are still fewer than the few to head-nurses. Definite information could easily be procured. Their funds do not permit such a diversion from their main and primary object, for which they are often, as it is, inadequate.
9. Of the wages and prospects of eventual provision of the nurses of the county hospitals I know nothing; but understand that the former are lower than, and the latter as entirely blank as those of the nurses of the non-endowed London hospitals.
1. It may be safely taken for granted as a rule, with few exceptions, that a thorough hospital nurse can seldom turn herself to any other business. Her life and work are altogether peculiar; she acquires a knowledge and habits which incapacitate her from all ordinary occupations, grows into fitness for them, and out of fitness for all others.
2. No less so, that the time during which a hospital nurse can work and lay by, is short, compared with the average duration of other kinds of service. Apart from all excess of their own, their work and its concomitants wear out hospital nurses fast. In every large hospital you will see many women of 40, whom you would suppose 60, and strength often decays as prematurely as appearance. Well-ventilated bed-rooms, more sleep, and better food, would be materially in their favour; but the work can never be other than one which wears out most constitutions fast.
3. In the London hospitals there are some women of excellent character and of great efficiency; many the reverse, in one or both respects; many between the two classes, who generally end by ranking in the second.
4. To augment the number of the first class, to reduce the number of the second, to induce the intermediate eventually to rank with the first, and not with the second, is the desire of every hospital.
5. It is most important, in all things, in none more than in hospital matters, to moderate expectations, not to hope too much from any measure, or set of measures, and to keep well in view the stern prosaic realities of things. The hospitals of great towns are not asylums where a few or many selected patients can be received and petted; but great receptacles of all sick comers. Their foundations lie down and deep in the human sin and misery for which they in part provide, and the traces of their purpose an[5]d nature must ever remain impressed upon them. They are also schools for the practical education of a great profession, important to mankind and dangerous to its members.
Hospital nurses are not women attempting or following “counsels of perfection,” (whatever incorporation of other elements may be eventually effected), but some of those many women whom God has ordained to earn their bread by toil, (and in the large towns of England honest ways of earning that bread are for women but too scarce and too overcrowded), and upon whom He has laid the same condition as on all the souls He has made, to keep the commandments to enter into life. A very mixed class they must ever remain: to improve the class, by God’s blessing, would be to effect a great benefit both to the hospitals and to these immortal souls.
6. Among several things which might be done or tried, with the view, if it please God to prosper the endeavour, of eventually improving the class of hospital nurses, the establishment of some definite prospect of eventual provision, dependent upon good character, appears very important.
7. It would tend to augment the number of steady respectable women, who are anxious to keep a good moral and require a good business character, whose aim it is to do their duty, to give satisfaction to their superiors, to keep their places in the same hospital, and eventually to end their days out of the workhouse.
8. It would tend to diminish the number of ill-conducted women, who wander from hospital to hospital; whose wages go in drink or finery, or both; who would be disgusted at the idea of regularly laying by for their future support, and who would resent strict investigation into character.
9. It would tend to induce the intermediate class of women, who hesitate between good and bad companions, to incline to the former, and to break off from the latter, by the favourable result of provident and economical habits on their actual conduct; and by the effect which the prospect of a decent support in their age, dependent upon these habits, would produce.
1. With regard to kind.
There are three kinds of possible assistance.
First. Granting free pensions to efficient and well-conducted sisters and nurses, under fixed regulations.
Second. Providing sisters and nurses with a secure channel of investing their savings; giving them thus the important assistance of saving their time, trouble, and expense, in obtaining information as to such secure investment.
Third. Combining, with the second, a certain proportion of pecuniary aid.
As to the first. It would be wise economy if the endowed hospitals, who alone could do it, were to grant such pensions; but whether they are likely to do more than they do now I am quite ignorant.
Whether our labours in this field should take the direction of the second or third, is one of the most difficult questions with reference to a thing which is rife with difficulties. Towards solving it, I submit that it would be expedient to employ an able and honest man of business to procure—
I. The rules, working, and results so far of the Servants’ Provident Society.
II. Of several of the various partly self-supporting and partly assisted provident societies of the different trades’ and city unions.
III. Of some dozen benefit societies in large towns.
IV. Of Guy’s Hospital Superannuation Fund.
V. To take the practical opinion of two experienced actuaries.
VI. Also of the Treasurer and Matron of St. Bartholomew’s;
My impression is that it is not possible, in the majority of cases, for either head-nurses or nurses to purchase annuities out of their savings.
I. Their work wears them out comparatively soon.
II. During its continuance they require to live well i. e., to have a sufficiency of good plain food.
III. They are obliged to put out and pay for either the whole or nearly the whole of their washing, making, and mending (and most properly obliged).
Thus apart altogether from the consideration that many nurses are widows with families, and many others burdened with helpless or infirm relations, and that, in many of these cases, the smallest saving out of their wages is impossible, I doubt whether it can be reasonably expected that, as a class, hospital nurses should lay by out of their unassisted savings a provision for their age.[21]
2. With regard to persons.
Shall the Fund be open exclusively to nurses belonging to the proposed Institution under Miss Nightingale?
Shall the Fund be extended to private and monthly nurses, including midwives, as well as to hospital-nurses?
I submit that we should consult, on these points, the authorities of the principal hospitals and a few men of experience in business besides. (Philanthropists by trade are, as is well known, the worst possible authorities on subjects of this kind.)
My impression is that the Fund should certainly be extended to the three kingdoms. Whether it should be extended to the empire would depend entirely, in my judgment, upon the check and scrutiny it would be possible to exert, on accounts, monies, and certificates, in distant parts. Upon this men of business should advise.
I think the Fund might eventually be open to private nurses, midwives, and monthly nurses.[22]
I think it perhaps might be open to the St. John’s House nurses and to those of any institution which does not provide its servants with a pension. The Nursing Sisters’ Society, I believe, have recently decided on granting their sisters £20 a-year, after twelve years’ service, a wise, generous, and, if properly worked, economical measure. We must avoid the very appearance of disfavour to other nursing institutions.
3. With regard to objects.
Shall the objects be
Or shall they be restricted either to the first only or the first and second? Here, again, I submit that we should consult hospital authorities and a few men of business and of experience, as to the feasibility, often a distinct thing from desirability, of these things.
Upon the whole, and weighing many opposite difficulties, my impression is strongly in favour of attempting to combine the three.
The benefit and provident societies embrace many objects: annuities, payments on illness, payments at burial, provision for children’s apprenticeships, provision for children at death, and other things.
I. It appears to me that the main if not the only object of the Fund should be to provide annuities.
II. It would be a question whether or not to arrange for payments during illness.[23] Every now and then ward air gets down the throat of almost every nurse, and every few years or so there is an illness. In many cases a nurse’s pay stops either when or soon after she becomes a patient. Some check upon malingering, a thing well[10] known where the name is not, is essential to every hospital. Of course it presses heaviest upon those who do not require it. After an illness, before returning into the wards, the best thing is a short thorough change of air. Often a severe illness is, and oftener still would be prevented by a week’s change of air, when the peculiar hospital-languor, so well known in hospitals, and so indescribable outside of them, first fairly sets in. The means of change of air, either before or after illness, are often deficient. Still, useful as some such provision would be, in many cases every year, it appears to me so subordinate to the great object of furnishing these women with some provision on their superannuation, that if it in the least impeded or rendered the latter less secure, I should unhesitatingly give it up.
III. With burial payments I think the Fund should have nothing to do.
IV. As to payments for children, whether on apprenticeship or at death:—Upon the whole, after much anxious thought, I think it undesirable to encourage mothers, as such. This is one of the many points, as to hospitals, where theories and experience differ much from each other.
A very large proportion of nurses are mothers, often widows, with large families, whom they support and put to service out of their wages, too often eked out by improper means, i. e., bribes and petty dishonesty. Many of these women are moral, sober, industrious, and doubly anxious to retain their places, on account of their children; still there are serious embarrassments in employing them. The wages of hospital nurses are not and never can be enough to supply a proper support for children, in addition to the support the mothers ought themselves to have. Consequently when children are in whole or in part lodged, fed,[11] clothed, “educated,” and put to service out of the £50 a-year of the head-nurse, or out of the 12s. a-week of the nurse, the mother either stints herself of proper food, proper strong drink (we deal with practice not with theory), proper warm clothing, for the children’s sake, or she supplies the deficiency by improper means. If the nurse cannot afford to live well and abstains from dishonesty, one of two things infallibly happens—either she takes to drink, as the fallacious support of an exhausted frame, or her strength fails and she breaks down, after a few months’, sometimes a few years’ struggle. When once she has taken to drink, one of two things invariably follows (dishonesty may be presumed to ensue upon, though it often does not precede habits of drink); she is or becomes unguarded, and is soon found out, and sinks into the miserable second and far too numerous class of characterless hospital nurses, unless drink shortly finishes her; or, in the other case, she is cautious and guarded—she then becomes sly, dishonest, and thoroughly venal; she extorts gifts and takes bribes from her patients and their friends—and the friends of hospital patients, like others, are of various kinds; she commits constant acts of petty but often most dangerous dishonesty, possibly remaining an efficient and clever nurse, sometimes a favourite nurse; and, so far as regards the crime which has taken the name of immorality, a moral woman. A certain proportion of nurses are all the above, excepting drink; for though, almost without exception, every nurse who drinks takes bribes, some take bribes and do not drink.
Of course widows and unmarried women who are not mothers do the above things; but there cannot be a doubt of the additional and terrible temptation [12]to women burdened with children, to make money in various ways out of their patients. Even in the most favourable cases (and it is to be feared they are few) where the real good principle of the mother restrains her from venality, there are still serious objections. The time when a nurse can go out must necessarily be comparatively very limited. The time that is enough for the moderate demands of friendship or acquaintance is miserably insufficient for the natural yearnings of the mother, especially if the children are young and helpless. The consequence is that, either openly or by stealth, she goes to them or has them brought to her at unallowed times; or, if the rules of the hospital are lax as to visitors, the children are perpetually with her: and let it be remembered, that the head-nurse’s room or rooms are usually at the entrance of the ward, that being infinitely the best place. It is difficult to say whether such a practice is most objectionable as regards the children, or the patients, or the hospital; and whether it is most objectionable when the children are young, or adolescent, or grown up. It is objectionable in all and every one of these cases. And no less objectionable is it in the case of the assistant-nurse, who where the rules are lax will receive her children either in the ward or in the nurses’ kitchen; or where they are strict, will have the children come about the hospital and will meet them on the sly.
These things enter immensely, minute as they seem, into the discipline of wards and of the hospital; and discipline means a great deal.
A good many nurses enter hospital service who are quite unfit for it. Often consumptive and ruptured women, those suffering from piles or prolapsus, &c., present themselves, are admitted, struggle on for a time, and break down with or without taking to drink. Undoubtedly, none but strong healthy women should enter hospital service; the work will wear them out quite soon enough, and some of the above complaints are particularly liable to follow the work.
Here again men of business must advise: the fund ought to have some efficient though not infallible security as to the average good health on joining of its members. Life Insurance rules as to this would be to the point.
Believe me, all these things are important.
The most difficult part of a difficult thing, only perhaps it is at the same time the most important.
I. I think that every nurse, before joining the Fund, should produce a certificate from her matron, stating her to be a respectable woman. In plain words, for the word respectable is certainly capable of most wondrous extension, the certificate should state her to be, in the matron’s belief, and to the best of her knowledge, a chaste woman, and should specify whether she be spinster, wife, or widow. In either of the latter cases, the marriage certificate, and in the last that of the husband’s death, should accompany the matron’s.
The matron’s certificate should, I consider, also state her to be sober; and it would be a question whether it should not also state her to have served for not less than a year in the hospital. The vagabond class are a terrible drag upon the whole order; and some of these might, from the novelty of the thing, be disposed to join it at first.
II. An important question would be: Should the matron’s certificate be renewed every year, and should the continuance of the nurse’s membership depend on its production? Men of business must advise as to this: I am quite unversed as to the details of Provident Societies.
So far as regards the contributor’s own money, the contract once entered into, must certainly be open to no further question; unless there has been fraud in the preliminary statement on which it was based. With regard to any assistance that may be given the question is different.
III. The preliminary certificate I do consider very important, and the subsequent ones, if they can be required.
Until the hospitals are swept of the many mothers who are not wives, now unhappily to be found in them, no real good can be done. Hospitals are not, and never can be, places for “penitents;” and they are about the most dangerous places where sham penitents can be.
This is precisely what so many people of very different kinds cannot or will not see; some from ignorance, some from knowledge, some from the vague, silly, kind feeling which does such mischief when exerted on practical matters.
Suffer me to submit, without wearying patience by urging proof,—
i. That real penitents are wrongly placed in hospital service, because their admission breaks down the standard which respectable women who are hospital nurses feel (quite as keenly as their superiors do in their own concerns) ought at once to restrain and to protect those engaged in this very peculiar, very trying, and very exposed work and life. (I have invariably observed that real penitents are extra-prudish, and comparatively inefficient, in their hospital duty. It will at once be perceived how inevitable this result is.)
ii. That sincere but unconfirmed penitents, in addition to the above, are most dangerously and improperly placed in a situation, to them, of very peculiar trial.
iii. That sham penitents, who unhappily abound, are dangerous everywhere, extra-dangerous in hospitals, whether to superiors, companions, or patients.
iv. That although the class must ever be a very mixed one, it is most important to have a standard. Let it be necessary for every nurse to enter hospital with a good character, and to leave it on losing it. Deception, hypocrisy, and successful guilt will be found in hospitals, as elsewhere; but the class must be raised, and therefore improved, by requiring the condition of good character; though guilt may occasionally mask itself behind it.
v. That although, for various and very differing reasons, the certificates will be not unseldom untrustworthy, still the same reasoning will apply. Upon the whole the tendency will be, by requiring the condition of good character, to improve a class which, containing, as it does, many well-conducted women, is sadly degraded and contaminated by many vile ones.
vi. I do not overlook the fact that honest certificates, especially if annually renewed, might give the matrons some perplexity, from reasons which need not be enlarged upon. Still, it seems to me, it would be well worth trying.
Lastly. With regard to rules to be followed in giving assistance of whatever kind.
It seems to me most important that we should obtain the opinions both of hospital authorities and of a few able men of business, before laying down rules. The whole matter is so essentially mixed up with the tangible point of securing that the savings of these poor women should avail them in their age, that it is urgent to have sound practical advice as to letting nothing else imperil this. Security seems the cardinal point of the whole, and that is a question for men of business to answer.
The following suggestions toward obtaining it are offered.
1. Security of invested savings to be the first and main thing to be secured. Every other object should be subordinate to this.
2. If we decide upon aiding their savings, let the security of this aid be the main point. Invest all donations, annual or not; unless, should any hospitals contribute annually, it might be fairly considered that those contributions should be annually used.
3. The aim should be to enable all hospital nurses, of good character, to provide annuities for themselves, whether with or without assistance. I think assistance will be necessary.
4. Also to enable private and monthly nurses, and midwives, to do the same, but without requiring the certificate of character, which, not to be a mockery, ought to be an effectual one; and these persons are not under a fixed superior.
5. The pensions should, if it be possible, range from £13 or £15 a-year to £50 a-year: say £13, £20, £30, £40, £50.
6. Each hospital nurse to produce, before being allowed to join the Fund, a certificate from her matron of chastity, general good conduct, and a statement as to her being unmarried, married, or a widow, also of her having served in one hospital not less than a year. Also her marriage certificate, if a wife, and, if a widow, that and the certificate of her husband’s death. In the event of her marriage or re-marriage afterwards, the marriage-certificate to be[17] produced, and her altered name and the fact of her marriage duly recorded in the Fund-book. (All this is important: aliases and fictitious marriages are sadly common, in this class).
7. If possible the certificate to be produced once a-year, and, on its failure, the contributor to cease to have a title to assistance. Assistance in the form of an addition to the annuity may be made contingent; the annuity which the premiums provide must be absolute: most of the vices tend to shorten life, that is, to diminish the number of annual payments, so that the fund would not be likely to incur losses through them.
8. Private and monthly nurses, and midwives, to produce, before being allowed to join the Fund, a certificate from the Clergyman of the parish, stating his belief that the subscriber is a respectable woman, unmarried, married, or a widow; and in the latter cases, marriage and death certificates. On any after-marriage or re-marriage, certificate to be produced and altered name registered, on pain of expulsion from the Fund. I should not attempt an annual certificate for this migratory and “independent” class.
9. Each nurse, before being allowed to join the Fund, to undergo whatever examination is undergone by women before they are allowed to effect Life Insurances, as to her being, at the date of joining, a healthy woman. (Physicians ought to advise here as to inserting provisions technical enough to be effective).
10. Payments to be made weekly, monthly, quarterly, or annually, as shall be advised. Amounts to run from 6d. or 1s. a week upwards. For the plan to work, it ought to allow small payments on an ascending scale.
Many will only be able to make very small payments.
Few will be able to make other than small payments.
11. Payments made by a subscriber dying before attaining pension to be devisable by will, and in case of intestacy, divided among next of kin.
12. All possible safe curtailment of office expenses.
13. Treasurers, or equivalent civil chiefs, of all hospitals that subscribe, to be on the committee or council, or by whatever name the equivalent may be termed.
1. I believe that many head-nurses would thoroughly appreciate and thankfully avail themselves of such a Fund.
2. I think that many nurses would do the same, and, in time, many more. Many cannot contribute to it; many will not.
3. What aid the hospitals might be disposed to give I do not know. I rather think none at first. If the thing works and works well, I think they would probably contribute. But it must never be forgotten that, excepting the endowed hospitals (the financial position of St. George’s I do not know) the London hospitals find their income scarcely sufficient, often not sufficient, to meet their expenditure. They cannot be expected, nor would they perhaps be justified, to curtail the number of the sick they relieve, in order to provide for the superannuated nurses of those sick. It is true, however, that it might enable them to get better nurses, which is surely economy.
4. I do not think that much lasting public interest is likely to attend the Fund. The interest the public has, for the last few years, taken in hospitals has been fictitious and almost mischievous. The public can never really know what hospitals are, nor is it feasible or desirable that it should. What eventual good may be done in them[19] must be done quietly and with great patience. What good may be done among the nurses must be done by infusing, if it may be, a higher and truer spirit of duty, by increased discipline and protection, and by ameliorating, in some material points, among which the aim contemplated by the Fund ranks very high, a condition which, to the end of time, must remain severe, rough, dangerous, and in all senses trying. In the details of all these things, most especially in all that concerns discipline, which involves protection, the public, with the best intentions, will only be an obstacle, and John Bull is sadly prone to pull up anything he plants or anything he waters, to see how it grows.
I think anything like appeals to or solicited support from the public might, in various ways, seriously embarrass the Superintendent of a very difficult and a very important though, at the same time, a very humble branch of Her Majesty’s Service. I should be very anxious to avoid this: it would be perpetuating the evils of publicity, and sacrificing the greater good for the lesser.
5. In conclusion I again submit that it would be desirable to ascertain from the hospital authorities above mentioned, and if possible from three or four able and honest men accustomed to business, their opinion as to the scope and details of this plan. In matters of spirit and of discipline we should probably rely on other judgment; but these are matters of business; and in which, without binding ourselves to follow, it seems most important to obtain and to weigh, the opinions of men long conversant with business.
January 23, 1858.
To show the importance of an Institute for Nurses, it must be stated that 25,466 were returned, at the census of 1851, as nurses by profession, exclusive of 39,139 nurses in domestic service,[24] and 2,882 midwives. The numbers of different ages are shown in table A, and in table B their distribution over Great Britain.
To increase the efficiency of this class, and to make as many of them as possible the disciples of the true doctrines of health, would be a great national work.
| NURSES. |
Nurse (not Domestic Servant) |
Nurse (Domestic Servant) |
|---|---|---|
| All Ages. | 25,466 | 39,139 |
| Under 5 Years. | ... | ... |
| 05 — | ... | 508 |
| 10 — | ... | 7259 |
| 15 — | ... | 10,355 |
| 20 — | 624 | 6537 |
| 25 — | 817 | 4174 |
| 30 — | 1118 | 2495 |
| 35 — | 1359 | 1681 |
| 40 — | 2223 | 1468 |
| 45 — | 2748 | 1206 |
| 50 — | 3982 | 1196 |
| 55 — | 3456 | 833 |
| 60 — | 3825 | 712 |
| 65 — | 2542 | 369 |
| 70 — | 1568 | 204 |
| 75 — | 746 | 101 |
| 80 — | 311 | 25 |
| 85 and Upwards | 147 | 16 |
|
Nurse (not Domestic Servant) |
Nurse (Domestic Servant) |
|
|---|---|---|
| Great Britain and Islands in the British Seas. | 25,466 | 21,017 |
| England and Wales. | 23,751 | 18,945 |
| Scotland. | 1543 | 1922 |
| Islands in the British Seas. | 172 | 150 |
|
1st Division. London. |
7807 | 5061 |
|
2nd Division. South Eastern. |
2878 | 2514 |
|
3rd Division. South Midland. |
2286 | 1252 |
|
4th Division. Eastern Counties. |
2408 | 959 |
|
5th Division. South Western Counties. |
3055 | 1737 |
|
6th Division. West Midland Counties. |
1225 | 2283 |
|
7th Division. North Midland Counties. |
1303 | 957 |
|
8th Division. North Western Counties. |
970 | 2135 |
|
9th Division. Yorkshire. |
1074 | 1023 |
|
10th Division. Northern Counties. |
402 | 410 |
|
11th Division. Monmouth and Wales. |
343 | 614 |
There is, at Madras, an Institution called the Military Female Orphan Asylum, which trains 200 orphan girls, daughters of European soldiers. They enter in infancy, and, as they attain a proper age, they are married to soldiers or others. There is always an abundance of applicants for them, and every endeavour is made to train them to be useful soldiers’ wives. Dr. MacPherson, the excellent Principal Medical Officer of the Turkish Contingent, when at Kertch, who is now in charge of this Asylum, was the person, I believe, who introduced amongst the senior girls, a system of training, to enable them to officiate as nurses, an all-important element in their education. Below is a syllabus of the theoretical branches taught, a practical knowledge being acquired in the Hospital attached to the Institution. It would be well if all women underwent a similar training.
A general knowledge of the human body, its various organs, and their uses.
To be made acquainted with every subject relating to health, viz.: Food—Exercise—Clothing—Cleanliness—Ventilation, &c.
Administration of Medicines, Application of Leeches, Lotions, Fomentations, &c. Cleanliness, Darkening of the Apartment, Quietness, &c. Cooking for the Sick. Diet for Infants.
To be taught how to act in emergencies, viz.: in cases of Fainting—Hysterics—Convulsions of Children—Burns—Stings of Insects—Wounds, &c.; and the simplest mode of treating the diseases most commonly met with in India, viz.:
How to prepare Poultices, Fomentations, and Lotions.
How to dress Wounds, Sores, and Blisters.
How to apply Bandages.
[21] If the sisters and nurses, as a rule, were fed as well as lodged at all the Hospitals, &c., the class of women would, in a very short time, be entirely changed; this kind of employment would not then, with the reduced money payment, be so much an object of desire to widows with families, particularly if compelled to subscribe to a pension fund, which should be compulsory.
[22] At first it would be unwise to attempt too much. If extended to Her Majesty’s dominions or private nurses, it would be almost impossible to control abuses.
[23] Every institution ought to provide for its nurses during illness, but in fact it is not done.
[24] A curious fact will be shown by Table A, viz., that 18,122 out of 39,139, or nearly one-half of all the Nurses, in domestic service, are between 5 and 20 years of age.