*** START OF THE PROJECT GUTENBERG EBOOK 62429 ***
Transcriber’s Note:
The cover image was created by the transcriber and is placed in the public domain.
EPIDEMIC RESPIRATORY DISEASE
The Pneumonias and Other Infections of the Respiratory Tract Accompanying Influenza and Measles
BY
EUGENE L. OPIE, M.D.
COLONEL, M. R. C., U. S. ARMY; PROFESSOR OF PATHOLOGY, WASHINGTON UNIVERSITY SCHOOL OF MEDICINE
FRANCIS G. BLAKE, M.D.
MAJOR, M. R. C., U. S. ARMY; ASSOCIATE MEMBER OF THE ROCKEFELLER INSTITUTE FOR MEDICAL RESEARCH
JAMES C. SMALL, M.D.
FORMERLY FIRST LIEUTENANT, M. C., U. S. ARMY; BACTERIOLOGIST, PHILADELPHIA GENERAL HOSPITAL
THOMAS M. RIVERS, M.D.
FORMERLY FIRST LIEUTENANT, M. C., U. S. ARMY; ASSOCIATE IN BACTERIOLOGY, JOHNS HOPKINS UNIVERSITY
ILLUSTRATED
ST. LOUIS
C. V. MOSBY COMPANY
1921
Copyright, 1921, By C. V. Mosby Company
Press of
C. V. Mosby Company
St. Louis, U. S. A.
11
INTRODUCTION
Death from lobar pneumonia, bronchopneumonia and
measles, fatal with few exceptions in consequence of complicating
pneumonia, constituted in 1916 approximately one-sixth
(16.8 per cent) of the mortality in the army,[1] whereas
in 1917 the same diseases were responsible for nearly two-thirds
(61.7 per cent) of all deaths. During the first half
of 1918 the incidence of pneumonia steadily increased and
in some army camps there were extensive outbreaks of unusually
severe pneumonia.
In July, 1918, the Surgeon General assigned a group of
medical officers to the study of the pneumonias prevalent
in the army and stationed them at Camp Funston, Kansas.
At the base hospital of this camp all cases of pneumonia occurring
among troops assembled in the camp were studied,
but during the month of August there were few cases of
pneumonia and these were of mild type.
Pneumonia which occurred at Camp Funston during August
was almost wholly limited to recently recruited colored
troops from southern states (Louisiana, Mississippi).
There was a low rate of mortality, and few complications.
This pneumonia exhibited a noteworthy difference in etiology
from that usually seen in civil life, for it was associated
with a high incidence of those types of pneumococci which
occur in the mouths of healthy men, namely, Pneumococcus
atypical II,[2] Type III, and the group of microorganisms
represented by Type IV. Pneumococcus Type I was encountered
in only a few instances and Type II was not found,
although these two microorganisms are responsible for
two-thirds of the lobar pneumonia which occurs in civil
life.
12During the investigation at Camp Funston the Commission
had the courteous cooperation of Major Willard Stone,
Director of Medical Service, and received much valuable
assistance from Lieutenant A. McGlory, Registrar of the
Base Hospital.
A review of the accurately compiled records of the base
hospital was made in order to obtain a history of the pneumonias
and other respiratory diseases which had occurred
throughout the existence of the camp, established in September,
1917. It soon became evident that a disease recognized
as influenza had been prevalent throughout this period
and its incidence had shown a close parallel with that
of acute bronchitis. At the same time there had been much
pneumonia and a high death rate from this disease. The
chart[3] which was constructed showed that the disease which
had been designated influenza assumed epidemic proportions
in March, 1918. Any doubt that may have been entertained
concerning the nature of the disease is dispelled
by the characters of this epidemic which, beginning at the
end of February, reached its height on March 12 and rapidly
subsided; 1,127 men with influenza entered the base
hospital between March 4 and March 29 and many more
were treated in the infirmaries of the camp. In April there
was a second wave of influenza and in May a third, each in
large part limited to newly drafted men brought into the
camp shortly before these outbreaks. Corresponding to
the epidemic of influenza there was a great increase of
pneumonia, reaching a maximum about one week after the
height of the incidence of influenza; subsequently the
incidence of pneumonia increased after each one of the secondary
waves of influenza. Pneumonia following measles
occurred throughout the history of the camp; in November
and December, 1917, there was a severe outbreak of pneumonia
following measles and the mortality was high. Our
13conclusions in regard to the pneumonias which occurred
during the history of Camp Funston were as follows:
1. Pneumonia of a relatively stationary camp population,
such as that which occurred among white troops during
the period of our investigation, was in considerable
part caused by Pneumococcus Types I and II and resembled
the pneumonia of civil life.
2. Pneumonia of newly drafted colored troops from
southern states during the period of our investigation was
caused in great part by pneumococci of those types which
occur in the mouths of healthy men, namely, Types IV, III
and atypical II.
3. Pneumonia caused by influenza occurred after the epidemic
of influenza which we have described. The report
states: “With the information available it is not possible to
draw a sharp line between (1) the pneumonia of the stable
camp population, (2) the pneumonia of the newly drafted
southern troops, and (3) the pneumonia following influenza.
It is possible that influenza, in greater or less degree,
also acts as a predisposing factor in the production of the
first and second varieties.”
4. Pneumonia with measles was a frequent and unusually
fatal type of the disease. The most important causes
of pneumonia during the history of the camp were influenza
and measles.
Evidence is not lacking that influenza occurred in epidemic
form in other widely separated camps in the United
States during the spring of 1918. Vaughan and Palmer[4]
state that a disease strongly resembling influenza became
prevalent in the Oglethorpe camps about March 18, 1918,
and continued three weeks; during this time the number
sent to hospital or to quarters with this disease was 1,468
in a total strength of 28,586. Pneumonia does not appear
to have followed this epidemic.
14Miller and Lusk[5] found the ordinary type of pneumonia
prevalent at Camp Dodge, Iowa, until March 18
to 20, 1918, when abruptly the streptococcus type predominated
and there was a great increase in the rate of mortality.
A mild tracheitis, they state, was widespread in the
camp during March.
In March, 1918, one member of our commission saw an
outbreak of influenza at Fort Sam Houston which was identical
in its clinical characters with the disease which appeared
as a pandemic in the fall of 1918.
The report of the Surgeon General[6] for 1919 shows that
there was a sharp increase of the incidence of influenza in
the army during March, reaching a maximum in April.
The rate of influenza for 1,000 troops fell to its original
level through May and June and finally rose to a great
height in September and October.
Influenza in epidemic form made its appearance in the
army camps of the United States during March, 1918. The
symptomatology of the disease associated with its peculiar
epidemiology as seen at Camp Funston make its recognition
unquestionable. The disease had doubtless been present
in this camp since its establishment in September, 1917,
but did not assume epidemic proportions until the spring
of 1919.
Pneumonia followed the epidemics of influenza which occurred
in the spring of 1918 and exhibited characters similar
to those of the pneumonias which followed the pandemic
of September and October, 1918. In both instances
the height of the outbreak of pneumonia has been one week
after the maximum incidence of influenza.
Influenza became epidemic in Spain about the middle of
May and in other countries received the name “Spanish
influenza” which is not more applicable than the designation
“Russian influenza” often applied to the disease during
the pandemic of 1889–90.
15The studies of MacNeal[7] have shown that the first epidemic
of influenza in the American Expeditionary Force in
France occurred about April 15, 1918, at a rest camp near
Bordeaux, reached its height on April 22 and ceased May
5. The disease was of a mild character with few complications.
Localized epidemics were reported from various
camps and hospitals during May and June, when the disease,
MacNeal states, had become widespread in all sections
of the American Expeditionary Force in France and in the
French and British armies as well. Influenza had become
epidemic in the Italian navy in the first two weeks of May.
The belief that the disease was introduced from America,
the author thinks, is “probably completely disproved by
the fact that the epidemic was subsequently introduced into
America in August and September and found there a
most fertile soil for its spread.” This view is disproved
by the demonstration that influenza had appeared as scattered
epidemics in the army camps in March, 1918. There
is little reason to doubt that influenza in the American Expeditionary
Force was brought from America.
At the end of August our commission was transferred
from Camp Funston to Camp Pike, where throughout the
history of the encampment pneumonia had been so prevalent
that it had given the camp the rank of third in death
rate from lobar pneumonia and fourth in death rate from
bronchopneumonia among 32 camps established in this
country. We arrived at Camp Pike September 5 and were
stationed at the base hospital. Our work was facilitated
by the hearty cooperation of the commanding officer, Major
Morton R. Gibbons, who neglected no opportunity to promote
the investigation. Our work was cordially aided by
Major Carl R. Comstock, Director of the Medical Service,
and by Major Henry H. Lissner, who later occupied this position.
Work in the laboratory of the hospital received the
valuable cooperation of Major Allen J. Smith, Director of
16the Laboratory, who placed at our disposal every facility
available. Lieutenant James R. Davis, who was for a time
in charge of the laboratory, effectively assisted the work.
The commission consisted of the following officers: E.
L. Opie, Colonel, M. R. C.; Allen W. Freeman, Major, M. C.;
Francis G. Blake, Major, M. R. C., James C. Small, Lieutenant,
M. C. and Thomas M. Rivers, Lieutenant, M. C.
Major Freeman acted as epidemiologist and will publish
a report upon the epidemiology of influenza and pneumonia
at Camp Pike. On October 11 the laboratory car “Lister”
in charge of Lieutenant Warren H. Butz was assigned to
the commission. Lieutenant Harry D. Bailey was attached
to the commission on October 14 and later assisted in its
work. Valuable technical assistance was given by Sergeant
Charles Behre, by Wm. E. Hoy, detailed from the
Army Medical Museum, and by Thomas Payne.
Study of the pathology of the lesions concerned was completed
in the Pathological Laboratory of Washington University
School of Medicine.
The existence of an epidemic of influenza at Camp Pike
was recognized on September 23, when 214 cases of influenza
were admitted to the base hospital. Preceding this
date and beginning September 1 there had been a gradual
increase of the number of patients admitted with the diagnosis
of acute bronchitis. It is noteworthy that the demonstration
of B. influenzæ had been regarded as essential
for a diagnosis of influenza and since this microorganism
had not been found, instances of acute inflammation of the
respiratory passages with the symptoms of influenza were
classified under a variety of names.
After September 23 influenza was recognized by its
symptoms. The number of cases increased with great rapidity
and on September 27 reached over 1,000 per day; this
number was approximately maintained during one week
and after October 3 the epidemic gradually subsided.
Among 52,551 men in the camp, including those who arrived
17during October, 12,393 were attacked by influenza; of
these 1,499 suffered with pneumonia and 466 died. The
height of the outbreak of pneumonia followed approximately
one week after that of influenza. The statistics from
September 20 to October 14 collected by Major Freeman
show that pneumonia following influenza, like the pneumonia
at Camp Funston during the interepidemic period,
has a conspicuous tendency to select men who have been in
the camp less than one month, designated in Table I as new
recruits:
| Table I |
|---|
| |
|
POPULATION |
INFLUENZA |
PNEUMONIA |
| No. |
Per cent. |
No. |
Per cent. |
| Men in camp more than one month |
27,782 |
4,462 |
15.6 |
493 |
1.7 |
| New recruits |
23,769 |
7,263 |
30.6 |
1006 |
4.2 |
| Total |
51,551 |
11,725 |
22.7 |
1499 |
2.9 |
New recruits were nearly two and a half times as susceptible
to pneumonia as men who had been in camp more
than one month. This statement does not take into consideration
differences in the environment and mode of living
of the new men.
In view of the existing uncertainty concerning the bacteriology
of influenza and its associated pneumonias, the commission
has availed itself of the opportunity afforded by
the epidemic of influenza to determine what bacteria were
present in the nasopharynx and sputum in these diseases.
The examinations have been necessarily limited to a small
proportion of the immense number of patients admitted to
the hospital with influenza and pneumonia. Autopsies on
those who have died with pneumonia have offered a more
direct means of determining the relation of bacteria to inflammation
of the bronchi and lungs. An attempt has been
made to classify the pneumonias following influenza and to
determine their relation to the complex bacterial flora of
the injured respiratory passages. These studies have
shown very early the threatening prevalence of streptococcus
18pneumonia, and appropriate measures have been
taken to combat the spread of this infection. No better illustration
could be furnished to demonstrate the value of
routine performance of autopsies as a means for the recognition
of obscure epidemic disease.
In view of the wide difference of opinion concerning the
pathology of influenzal pneumonia special study has been
given to the lesions of the disease, because the epidemic has
furnished the unique opportunity of examining all instances
of pneumonia accurately referable to an epidemic
of influenza attacking a large but definitely defined group
of individuals (50,000 troops). In a civil hospital there is
often great difficulty in deciding, even in the presence of an
epidemic, if death from pneumonia is the result of influenza,
but at Camp Pike the relation of the heightened death
rate to the epidemic has excluded all save a trivial error in
determining the relation of fatal pneumonia to influenza.
At the direction of Col. F. F. Russell, who has promoted
the work of the commission by unfailing aid, a special
study has been made of the relation of hemolytic streptococcus
to the complications of measles.
During the later period of the investigation at Camp Pike
experiments were performed on monkeys to determine the
pathogenicity of B. influenzæ and of microorganism isolated
from the pneumonias following influenza. Typical lobar
pneumonia was produced in monkeys by intratracheal injection
of pneumococci. These experiments are described
in an appendix.
The Surgeon General has approved the publication of this
report but the authors alone are responsible for the views
expressed.
Eugene L. Opie.
Washington University
School of Medicine
19
CONTENTS
| CHAPTER I |
|
|
PAGE |
| The Etiology of Influenza. (By Francis G. Blake, M.D.; Thomas M. Rivers, M.D.; James C. Small, M.D.) |
25 |
| |
| |
Discussion, 43; Conclusions, 49. |
|
| |
| |
| CHAPTER II |
| |
| Clinical Features and Bacteriology of Influenza and Its Associated Purulent Bronchitis and Pneumonia. (By Francis G. Blake, M.D., and Thomas M. Rivers, M.D.) |
51 |
| |
| |
Influenza, 52; Purulent Bronchitis, 56; Pneumonia, 59; Hemolytic Streptococcus Pneumonia Following Influenza, 70; Bacillus Influenzæ Pneumonia Following Influenza, 72; Summary, 73; Discussion, 76. |
|
| |
| |
| CHAPTER III |
| |
| Secondary Infection in the Ward Treatment of Influenza and Pneumonia. (By Eugene L. Opie, M.D.; Francis G. Blake, M.D.; James C. Small, M.D.; and Thomas M. Rivers, M.D.) |
83 |
| |
| |
Secondary Infection with S. Hemolyticus in Pneumonia, 84; Secondary Infection with Pneumococcus in Pneumonia, 91; Secondary Contact Infection in Influenza, 95; Methods for the Prevention of Secondary Contact Infection in Influenza and Pneumonia, 98; Summary, 106. |
|
| |
| |
| CHAPTER IV |
| |
| The Pathology and Bacteriology of Pneumonia Following Influenza. (By E. L. Opie, M.D.; F. G. Blake, M.D.; and T. M. Rivers, M.D.) |
107 |
| |
| |
Bronchitis, 142; Lobar Pneumonia, 154; Bronchopneumonia, 162; Peribronchial Hemorrhage and Pneumonia, 189; Suppurative Pneumonia with Necrosis and Abscess Formation, 199; Interstitial Suppurative Pneumonia, 209; Suppurative Pneumonia with Multiple Clustered Abscesses Caused by Staphylococci, 225; Empyema, Pericarditis and Peritonitis, 232; Bronchiectasis, 239; Unresolved Bronchopneumonia, 261. |
|
| |
| |
| 20CHAPTER V |
| |
| Secondary Infection in the Ward Treatment of Measles. (By James C. Small, M.D.) |
282 |
| |
| |
Hemolytic Streptococci with Measles at Camp Pike, 297; Complications of Measles, 303; The Dissemination of Hemolytic Streptococci in Wards, 315; Carriers of Hemolytic Streptococci, 321. |
|
| |
| |
| CHAPTER VI |
| |
| The Pathology and Bacteriology of Pneumonia Following Measles. (By Eugene L. Opie, M.D.; Francis G. Blake, M.D.; James C. Small, M.D.; and Thomas M. Rivers, M.D.) |
334 |
| |
| |
Changes in Bronchi, 336; Lobar Pneumonia, 337; Bronchopneumonia, 340; Suppurative Pneumonia, 347; Pneumonia Associated with Acute Infectious Diseases other than Influenza and Measles, 353. |
|
| |
| |
| CHAPTER VII |
| |
| Summary of the Investigation and Conclusions Reached. (By Eugene L. Opie, M.D.) |
359 |
| |
| |
Lobar Pneumonia, 362; Bronchopneumonia, 363; Streptococcus Pneumonia, 365; Staphylococcus Pneumonia, 366; Empyema, 366; Bronchiectasis, 367; Unresolved Bronchopneumonia, 368; B. Influenzæ, 369; Pneumococcus, 372; S. Hemolyticus, 374; Nonhemolytic Streptococci, 376; Staphylococci, 377; Pneumonia of Measles, 378; The Transmission of Streptococcus Pneumonia, 381; Transmission of Pneumococcus Pneumonia, 383; Prevention of the Transmission of Pneumonia, 383. |
|
| |
| |
| APPENDIX |
| |
| Experimental Inoculation of Monkeys with Bacillus Influenzæ and Microorganisms Isolated from the Pneumonias of Influenza. (By Eugene L. Opie, M.D.; Allen W. Freeman, M.D.; Francis G. Blake, M.D.; James C. Small, M.D.; and Thomas M. Rivers, M.D.) |
387 |
| |
| |
Inoculation of the Nose and Pharynx with B. Influenzæ, 389; Introduction of Bacillus Influenzæ into the Trachea, 391; Introduction of B. Influenzæ and S. Hemolyticus into the Trachea, 392; Introduction of B. Influenzæ and of Pneumococcus or of Pneumococcus Alone into the Trachea, 393. |
|
21
ILLUSTRATIONS
| CHARTS |
|
PAGE |
| 1. |
The onset of cases of pneumonia shown by autopsy to be uncomplicated by secondary infection with hemolytic streptococcus and of cases of streptococcus pneumonia |
141 |
| |
| 2. |
The date of onset of cases in which autopsy demonstrated lobar pneumonia |
161 |
| |
| 3. |
Shows the relation of the epidemic of measles to that of influenza at Camp Pike, and the relations of the pneumonia following measles to both measles and influenza |
293 |
| |
| 4. |
Shows the time interval between the onset of measles and the onset of the subsequent pneumonia in the 56 cases of pneumonia following measles at Camp Pike |
306 |
| |
| 5. |
Shows the time relation between the identification of hemolytic streptococci in the throats and the development of otitis media in 27 cases shown to be due to hemolytic streptococci |
314 |
| |
| |
| FIG. |
|
|
| 1. |
Acute bronchitis showing engorgement of blood vessels of mucosa and elevation of epithelium by serum and blood |
146 |
| |
| 2. |
Acute bronchopneumonia with nodules of peribronchiolar consolidation and purulent bronchitis |
167 |
| |
| 3. |
Acute bronchopneumonia with peribronchiolar consolidation |
169 |
| |
| 4. |
Acute bronchopneumonia with peribronchiolar consolidation |
170 |
| |
| 5. |
Bronchopneumonia with hemorrhagic peribronchiolar consolidation |
174 |
| |
| 6. |
Acute bronchopneumonia with confluent gray lobular consolidation in lower part of upper lobe and hemorrhagic peribronchiolar pneumonia in lower lobe; purulent bronchitis |
180 |
| |
| 7. |
Bronchopneumonia with purulent bronchitis and peribronchial hemorrhage |
190 |
| |
| 8. |
Streptococcus pneumonia with massive necrosis |
201 |
| |
| 9. |
Abscess below pleura with perforation caused by hemolytic streptococci |
202 |
| |
| 10. |
Interstitial suppurative pneumonia; interstitial septa are the site of suppuration and lymphatics are distended with purulent fluid; empyema |
211 |
| |
| 11. |
Suppurative interstitial pneumonia |
212 |
| |
| 12. |
Suppurative interstitial pneumonia |
216 |
| |
| 13. |
Suppurative interstitial pneumonia showing a dilated lymphatic |
217 |
| |
| 2214. |
Endophlebitis occurring in association with suppurative pneumonia |
219 |
| |
| 15. |
Abscesses in two clusters caused by S. aureus in upper part of right upper lobe |
227 |
| |
| 16. |
Abscesses in cluster caused by S. aureus at apex of right lobe |
228 |
| |
| 17. |
Acute bronchiectasis showing fissures penetrating into bronchial wall and at one place entering alveolar tissue |
246 |
| |
| 18. |
Acute bronchiectasis showing fissures in the bronchial wall extending into neighboring alveoli which in zone about are filled with fibrin |
247 |
| |
| 19. |
Acute bronchiectasis; the bronchial wall indicated by engorged mucosa shows a varying degree of destruction, fissures extending into and through the bronchial wall |
248 |
| |
| 20. |
Acute bronchiectasis with destruction of bronchial wall exposing alveoli filled with fibrin |
249 |
| |
| 21. |
Bronchiectasis with fissures extending through the bronchial wall into alveolar tissue which is site of fibrinous pneumonia |
251 |
| |
| 22. |
Regeneration of epithelium over fissures which have been formed in the wall of a bronchus |
252 |
| |
| 23. |
Squamous epithelium growing over the defect in the bronchial wall |
253 |
| |
| 24. |
Acute bronchiectasis with fissures extending through bronchial wall which is marked by great engorgement of blood vessels |
255 |
| |
| 25. |
Advanced bronchiectasis throughout lower left lobe |
258 |
| |
| 26. |
Unresolved bronchopneumonia with tubercle-like nodules of peribronchiolar consolidation best seen in lower lobe; bronchiectasis |
268 |
| |
| 27. |
Unresolved pneumonia with peribronchial formation of fibrous tissue; bronchiectasis |
270 |
| |
| 28. |
Unresolved pneumonia with bronchiectasis showing new formation of fibrous tissue about a greatly dilated bronchus of which the epithelial lining has been lost |
271 |
| |
| 29. |
Lobar pneumonia following measles |
338 |
| |
| 30. |
Unresolved bronchopneumonia with measles showing new formation of fibrous tissue about a bronchus and in immediately adjacent alveolar walls |
342 |
| |
| 31. |
Unresolved bronchopneumonia with measles showing a nodule of chronic fibrous pneumonia surrounding a respiratory bronchiole |
343 |
| |
| 32. |
Unresolved bronchopneumonia with measles showing chronic pneumonia about a respiratory bronchiole and alveolar duct |
344 |
| |
| 33. |
Experimental lobar pneumonia in the stage of gray hepatization produced by injection of Pneumococcus III into the trachea of a monkey |
395 |
25
EPIDEMIC RESPIRATORY DISEASE
THE PNEUMONIAS AND OTHER INFECTIONS OF THE RESPIRATORY TRACT ACCOMPANYING INFLUENZA AND MEASLES
CHAPTER I
THE ETIOLOGY OF INFLUENZA
Francis G. Blake, M.D.; Thomas M. Rivers, M.D.; James C. Small, M.D.
The bacteriologic investigation which will be described
was made at Camp Pike, Arkansas, during the period of
the influenza epidemic from September 6 to December 5,
1918. The data presented are limited to observations made
during life in uncomplicated cases of influenza and to control
studies in normal individuals, and in cases of measles.
Bacteriologic studies made at autopsy will be described
in a subsequent part of this report.
Because of the wide variations in opinion concerning the
relationship of various bacteria to influenza that have
arisen during the progress of the recent pandemic, a brief
review of the salient features of the earlier literature seems
advisable. In 1892 Pfeiffer[8] found a small, Gram-negative,
hemophilic bacillus in all cases of influenza, often in almost
pure culture, both during life and at autopsy. He stated
that the organism was found only in cases of influenza or
in those convalescent from the disease. Similar bacilli occasionally
found in other conditions he classified as pseudoinfluenza
bacilli. He furthermore showed that freshly isolated
cultures were pathogenic for monkeys, producing a
disease not unlike influenza, though lacking in what he considered
26the characteristic lung lesions. He therefore felt
justified in claiming that this bacillus, which he designated
B. influenzæ, was the cause of epidemic influenza. Pfeiffer’s
work, though hailed by many as unassailable, has
failed to stand the test of time in two respects. It has been
definitely shown, by Wollstein[9] in particular, that there is
no justification for recognizing a group of pseudoinfluenza
bacilli, organisms so classified by Pfeiffer being indistinguishable
from B. influenzæ. Furthermore, numerous investigations
have demonstrated that B. influenzæ may frequently
be found in a variety of diseases affecting the respiratory
tract and in a small proportion of normal individuals.
Kretz[10] found it 47 times in 950 examinations, usually
associated with disease of the respiratory tract. Süsswein,[11]
Liebscher,[12] Jehle,[13] Wollstein,[9] Davis[14] and many
others have demonstrated its presence in cases of measles.
Lord[15] isolated B. influenzæ in 30 per cent of 186 sputums
from patients with acute and chronic infection of the respiratory
tract. Boggs[16] found it in frequent association
with chronic bronchiectasis. Wollstein[9][17] showed that it
was often present in the respiratory diseases of infants,
and was not an infrequent cause of meningitis. Rosenthal[18]
found that one in six of normal individuals harbors influenza
bacilli and therefore considered it purely a saprophyte,
a position, of course, thoroughly untenable in the
face of indisputable evidence that it may be highly pathogenic.
The widely accepted statement that B. influenzæ is
nonpathogenic for animals has apparently served in considerable
degree to shake belief in its etiologic relationship
to epidemic influenza. It would appear, however, that this
opinion is not founded upon fact. Reference is again made
27to the work of Wollstein[19], who has shown that virulent
strains of B. influenzæ, when freshly isolated from the human
host, are highly pathogenic for rabbits and monkeys
and that nearly all strains are more or less pathogenic for
mice and guinea-pigs.
None of these modifications of Pfeiffer’s original work,
however, would seem to constitute any valid reason for
abandoning the conception of the etiologic importance of
B. influenzæ. On the contrary, they are quite in harmony
with well-established facts concerning other bacteria which
cause infections of the respiratory tract. Such bacteria are
frequently found in normal individuals leading a saprophytic
existence, are often associated with other disease
conditions, and tend to show marked variations in virulence.
Since the outbreak of scattered epidemics of influenza
beginning in 1915–16, which finally culminated in the pandemic
of 1918–19, a vast amount of literature on the subject
has appeared. No attempt has been made thoroughly to
analyze this, because much of it is not available, much of
it abounds in contradictions which it is difficult to harmonize
at the present time, and much of it has been written on
the basis of insufficient data gathered under the handicap
of war conditions by men without sufficient time to undertake
special investigation, or it is feared, in many instances,
not sufficiently qualified by previous bacteriologic training.
The sum and substance of opinion in 1918 would seem to
be best summarized by quoting from the published report
compiled by the British Medical Research Commission:[20]
“Although Pfeiffer may yet furnish reasons why the verdict
should not be pronounced, there is already sufficient
material to shake the orthodox conception out of its high
altar. Two facts stand out prominently: the generally acknowledged,
or by some reluctantly admitted, absence of
B. influenzæ from organs on postmortem examinations, and
28the universally recorded findings of diplostreptococci, singly
or in association with the Pfeiffer bacillus.” Comment
on this opinion will be made in the general discussion at
the end of this paper.
In undertaking a study of the bacteriology of influenza,
it seemed essential to bear in mind certain clinical features
of the disease which will be discussed in greater detail in a
subsequent paper. It suffices to say for our present purpose
that it is felt that influenza in itself should be regarded
as a self-limited disease of short duration (two to five days
in most instances), the most prominent local manifestation
of which is a rapidly progressing attack upon the mucous
membranes of the respiratory tract. Among the cases observed
during the epidemic at Camp Pike uncomplicated
influenza never proved fatal and death invariably was associated
with a complicating pneumonia. In a large majority
of cases pneumococci, S. hemolyticus, or less frequently
other bacteria in addition to B. influenzæ were associated
with the pneumonia. It is felt, therefore, that in
any attempt to determine the primary cause of influenza
bacteriologic studies made during life in early uncomplicated
cases of the disease are of primary importance and
that the bacteriology of the sputum of patients with complicating
pneumonia and the bacteriology of autopsies can
only properly be used as valuable supplements to data so
obtained.
Since cultures from the respiratory tract must often of
necessity contain many bacteria which play no part in the
production of influenza, it is essential to have a working
knowledge of the bacteria that may be encountered by the
methods employed. It is also important that such knowledge
as may have been gained in interepidemic periods be
amplified by study of the bacterial flora present at various
periods throughout the course of an epidemic, both in normal
individuals and in other disease conditions. These
points have been borne in mind throughout the present
29study and such observations have formed an essential part
of the work.
Methods.—In an investigation of this nature the culture
methods employed should be suitably directed to determine
primarily what bacteria are present and in what relative
proportion they exist. The use of culture or animal inoculation
methods that are highly selective in character, enhancing
the growth of certain bacteria and retarding or inhibiting
the growth of others, are of great additional value,
but can only properly be used secondarily in order to augment
the results obtained by nonselective culture methods.
As the most suitable medium for the purpose in hand plain
meat infusion agar, titrating 0.1+ to 0.3+ to phenolphthalein,
to which 5 per cent of sterile defibrinated horse blood
was added, was used. Since growth on freshly poured
plates is greatly superior to that on plates that have been
stored, the agar was melted as needed, the blood being
added when the medium had cooled to approximately 45°
C. Cultures from the nose and throat were made by swabbing
the mucous membranes with a sterile applicator,
touching the applicator to a small area on the surface of a
blood agar plate, and spreading the inoculum over the surface
of the medium with a platinum needle, insuring as
wide a separation as possible. Direct cultures of selected
and washed specimens of sputum were made when possible.
In many instances, of course, it was impossible to get
sufficiently satisfactory specimens to permit of washing,
especially when cultures were made very early in the disease.
To supplement direct culture of the sputum the
mouse inoculation method as employed for the determination
of pneumococcus types was used. This is, of course,
a highly selective method, of particular value in the detection
of pneumococcus and B. influenzæ when they are present
in relatively small numbers as compared with other
bacteria. Plates were examined after twenty to twenty-four
30hours’ incubation and again at the end of thirty-six
to forty-eight hours when necessary.
In the present study, attention has been centered upon
B. influenzæ, S. hemolyticus, and the various immunologic
types of pneumococci, other organisms encountered having
played no significant part in the cases studied except in rare
instances. B. influenzæ was identified by its morphologic,
staining and cultural characteristics and conformed to the
classical description given by Pfeiffer. S. hemolyticus was
identified by its morphologic, staining, and cultural characteristics
on blood agar, supplemented by a confirmatory
hemolytic test with washed sheep corpuscles, and bile solubility
test. Pneumococci were identified by morphologic,
staining and cultural characteristics, bile solubility test, and
agglutination with specific antipneumococcus immune sera.
Note was made in most instances of the presence of other
organisms, such as members of the Gram-negative diplococcus,
staphylococcus, diphtheroid and streptococcus viridans
groups, but no attempt was made further to isolate or identify
them.
Bacillus Influenzæ in Cases of Influenza.—On October 10,
1918, at the height of the epidemic at Camp Pike, search for
B. influenzæ was made in a group of 23 consecutive cases of
uncomplicated influenza from one to six days after the onset
of the disease. From each individual simultaneous cultures
on blood agar plates were made (a) from the nose,
(b) from the throat, and (c) from the sputum, and the sputum
from each case was injected into the peritoneal cavity
of a white mouse. A similar study of 5 consecutive cases
was made on November 19. The results are presented in
Table II.
By means of multiple cultures taken simultaneously from
different portions of the respiratory tract no difficulty was
encountered in demonstrating B. influenzæ in all these cases
of uncomplicated influenza. Not only was B. influenzæ
found in all cases, but often in very large numbers predominating
31over all other bacteria on at least one of the plates
from each patient, and in occasional instances occurring in
nearly pure culture. One culture made about two hours
after onset of the initial coryza is of interest. There was
at the time a profuse serous nasal discharge. One drop of
this allowed to fall on the surface of a blood agar plate
gave a practically pure culture of B. influenzæ.
| Table II |
|---|
| |
| Presence of B. Influenzæ in 28 Cases of Influenza |
|---|
| |
| NO. |
DAY OF DISEASE |
NOSE |
THROAT |
SPUTUM CULTURE |
SPUTUM PASSED THROUGH MOUSE |
| 1 |
1 |
+ |
+ |
+ |
+ |
| 2 |
4 |
− |
+ |
+ |
+ |
| 3 |
5 |
− |
− |
+ |
− |
| 4 |
4 |
− |
− |
+ |
+ |
| 5 |
3 |
− |
− |
+ |
+ |
| 6 |
4 |
− |
+ |
+ |
c |
| 7 |
2 |
− |
+ |
− |
c |
| 8 |
4 |
+ |
+ |
+ |
− |
| 9 |
5 |
− |
+ |
+ |
+ |
| 10 |
2 |
+ |
− |
− |
− |
| 11 |
2 |
− |
+ |
c |
+ |
| 12 |
3 |
c |
+ |
+ |
+ |
| 13 |
3 |
− |
− |
− |
+ |
| 14 |
2 |
− |
− |
+ |
+ |
| 15 |
3 |
c |
− |
− |
+ |
| 16 |
1 |
− |
+ |
+ |
+ |
| 17 |
3 |
− |
+ |
− |
+ |
| 18 |
4 |
+ |
+ |
c |
+ |
| 19 |
6 |
− |
− |
+ |
+ |
| 20 |
1 |
− |
+ |
+ |
+ |
| 21 |
2 |
− |
+ |
− |
+ |
| 22 |
4 |
+ |
− |
+ |
+ |
| 23 |
3 |
c |
− |
− |
+ |
| 24 |
2 |
+ |
− |
− |
− |
| 25 |
1 |
− |
− |
+ |
+ |
| 26 |
5 |
− |
− |
+ |
+ |
| 27 |
? |
− |
+ |
− |
+ |
| 28 |
1 |
− |
− |
+ |
+ |
| |
|
6 |
14 |
17 |
22 |
| |
| c indicates that the plate was contaminated. |
During the latter part of November and in early December
a small secondary wave of influenza occurred at Camp
Pike. In a series of 48 consecutive cases, B. influenzæ was
readily found in all by means of combined throat cultures
32and mouse inoculation of the sputum, 33 times (68.7 per
cent) in the throat cultures, 39 times (81.3 per cent) in the
sputum. These cases were cultured on admission to the
receiving ward of the hospital within twenty-four to forty-eight
hours after onset and were all early cases of influenza
without complications at the time the cultures were made.
In 90 more consecutive cases in this series 62 or 68.9 per
cent showed B. influenzæ in a single throat culture taken
on admission.
A summary of all cultures made in cases of uncomplicated
influenza is presented in Table III.
| Table III |
|---|
| |
| Presence of B. Influenzæ in Cases of Influenza |
|---|
| |
| METHOD |
NUMBER OF CASES CULTURED |
B. INFLUENZÆ FOUND |
| NUMBER |
PER CENT |
| Nose culture |
28 |
6 |
21.4 |
| Throat culture |
166 |
109 |
65.7 |
| Sputum culture |
28 |
17 |
60.7 |
| Sputum (mouse passage) |
76 |
61 |
80.3 |
| Combined nose, throat and sputum cultures and sputum inoculation |
28 |
28 |
100 |
| Combined throat cultures and sputum inoculation |
48 |
48 |
100 |
Of any single method used the intraperitoneal inoculation
of a white mouse with a specimen of the patient’s sputum
proved the most efficient in demonstrating the presence
of B. influenzæ. No single method served to demonstrate
B. influenzæ in all cases, but by simultaneous cultures from
the nose, throat, and deeper air passages no difficulty was
met in showing that B. influenzæ was invariably present,
usually in abundance somewhere in the respiratory tract
during the acute stage of the disease. This result is not
out of harmony with the rapidly progressive character of
the attack upon the mucous membranes of the respiratory
tract in influenza.
Of interest in this connection are certain observations
which suggest that the presence of B. influenzæ in predominant
33numbers at least is in many cases coincident with the
acute stage of influenza and that the organisms show a tendency
rapidly to diminish in abundance with the progress
of the disease to recovery. In 82 cases of influenza cultured
on the day of admission to the hospital, B. influenzæ was
present in 52 (63.4 per cent) of the throat cultures. Repeated
throat cultures in this group of cases from the
fourth to the eighth day after admission when the temperature
had fallen to normal, showed that B. influenzæ was
still present in demonstrable numbers in the throat of only
25 cases or 30.5 per cent. Not only was there a material
reduction in the number of patients in whom B. influenzæ
could be demonstrated by the throat culture method, but
the contrast in the predominance of B. influenzæ on the
plates made early in the disease with those made during
convalescence was often very striking. It is only fair to
say, however, that some cases continued to carry B. influenzæ
in their throats in large numbers throughout the period
of observation.
Presence of Pneumococcus in Cases of Influenza.—It
seemed of some importance to determine the prevalence of
pneumococcus in cases of influenza, not because of any possibility
that pneumococci might bear an etiologic relationship
to the disease, but more by way of comparison with the
prevalence of B. influenzæ, since both organisms are found
in the mouths of normal individuals and are also frequently
found together in the pneumonias that complicate influenza.
The results obtained in cases of influenza early in the
disease before the development of either a purulent bronchitis
or of pneumonia are presented. The presence of
pneumococcus was determined by the intraperitoneal inoculation
of white mice with the saliva or sputum.
Twenty-four cases examined on September 27 and 28
gave the results shown in Table IV. These patients had
been in the hospital from two to five days at the time the
determinations were made.
| 34 |
| Table IV |
|---|
| |
| Pneumococcus in Cases of Influenza |
|---|
| |
|
NUMBER |
PER CENT |
| Pneumococcus, Type I |
0 |
0 |
| Pneumococcus, Type II |
0 |
0 |
| Pneumococcus, Atypical II |
0 |
0 |
| Pneumococcus, Type III |
2 |
8.3 |
| Pneumococcus, Group IV |
15 |
62.5 |
| No pneumococci found |
7 |
29.2 |
From November 27 to December 1, the pneumococci present
in 47 consecutive cases of influenza were determined.
In this group specimens of sputum were collected shortly
after admission of the patients to the receiving ward of the
hospital. The results are shown in Table V.
| Table V |
|---|
| |
| Pneumococci in Cases of Influenza |
|---|
| |
|
NUMBER |
PER CENT |
| Pneumococcus, Type I |
0 |
0 |
| Pneumococcus, Type II |
0 |
0 |
| Pneumococcus, Atypical II |
2 |
4.3 |
| Pneumococcus, Type III |
0 |
0 |
| Pneumococcus, Group IV |
25 |
53.2 |
| No pneumococci found |
20 |
42.5 |
The results obtained show that pneumococci found in
early uncomplicated cases of influenza, both early and late
in the course of the epidemic, differ in no respect from
those found in the mouths of normal individuals at any
time.
Similar studies of the prevalence of S. hemolyticus as
determined by throat cultures in early cases of influenza
are shown in Table VI.
The only point of interest in these observations is the increased
prevalence of S. hemolyticus in cases examined late
in the epidemic of influenza as compared with that found
early in the epidemic. The significance of this will be discussed
in other parts of this report.
| 35 |
| Table VI |
|---|
| |
| S. Hemolyticus in Cases of Influenza |
|---|
| |
| DATE |
NUMBER OF CASES CULTURED |
S. HEMOLYTICUS FOUND |
S. HEMOLYTICUS NOT FOUND |
PER CENT POSITIVE FOR S. HEMOLYTICUS |
| Sept. 25–26 |
100 |
6 |
94 |
6 |
| Nov. 27–Dec. 5 |
138 |
39 |
99 |
28.3 |
Presence of Bacillus Influenzæ in Normal Men.—For
comparison with the results obtained in cases of influenza
a fairly extensive study of the prevalence of B. influenzæ
in normal individuals has been made at various times prior
to and throughout the course of the epidemic. This was
deemed of special importance, since it was obvious that the
results obtained by previous workers during interepidemic
periods would not in all probability coincide with those obtained
in the presence of a widespread epidemic of influenza
where the opportunity for the dissemination of B. influenzæ
was almost unlimited.
From the results obtained in the multiple cultures in
cases of influenza it is obvious that only like methods can
be compared. The results obtained in normal individuals
have, therefore, been tabulated in groups dependent upon
the culture method employed. These groups have been
subdivided according to the time and the place of the study,
such explanatory notes as seem necessary being added.
(See Tables VII-IX.)
The most striking feature of the figures presented in
Table VII is the wide variation in the incidence of B. influenzæ
in different groups varying all the way from 11.1 to
68 per cent. Analysis of these differences brings out certain
points of great interest. It is apparent that the percentage
of cases carrying B. influenzæ depended in large
part upon the prevalence of respiratory diseases in the
group from which the data were obtained. In the studies
made at Camp Funston prior to the fall outbreak of influenza
in epidemic proportions, it is noteworthy that “bronchitis”
and pneumonia were prevalent throughout the summer
in those groups showing a relatively high incidence of
B. influenzæ. At the time these studies were made the presence of influenza in these organizations was not recognized,
but in view of knowledge gained throughout the course of
the epidemic at Camp Pike, it seems not improbable that
influenza in mild form was present throughout the summer
in certain organizations at Camp Funston. This would
seem more likely in view of the fact that this commission
has clearly demonstrated that a considerable epidemic of
influenza swept through Camp Funston in March, 1918, and
was followed by recurring smaller epidemics in April and
May.[21] In contrast with these groups showing a high incidence
of B. influenzæ is that of the 210th Engineers, an organization
entirely free from respiratory diseases during
the period of our study.
| 36 |
| Table VII |
|---|
| |
| Incidence of B. Influenzæ in Normal Men as Determined by Intraperitoneal Inoculation of White Mice With Saliva or Sputum |
|---|
| |
| DATE |
PLACE |
ORGANIZATION |
NUMBER EXAMINED |
B. INFLUENZÆ PRESENT |
PER CENT POSITIVE FOR B. INFLUENZÆ |
REMARKS |
| 1918 |
|
|
|
|
|
|
| Aug. 13 |
Camp Funston, Kans. Detention Camp, No. 2 |
22 Prov. Colored Co. 164th Depot Brigade |
25 |
6 |
24 |
Bronchitis and pneumonia were prevalent in this organization of recently drafted negroes during July and August, 1918 |
| Aug. 18 |
Camp Funston, Kans. Detention Camp, No. 2 |
Co. D. 3rd Dev. Bn. |
25 |
11 |
44 |
Recently drafted southern negroes not fit for full military duty. Bronchitis and pneumonia were prevalent in this organization during July and August, 1918 |
| Aug. 20 |
Camp Funston, Kan. |
70th Inf. |
25 |
11 |
44 |
25 men presenting themselves at sick call for various complaints; not strictly normal; respiratory diseases not prevalent |
| Aug. 22 |
Ft. Riley, Kan. |
Quarters 4 M M.O.T.C. |
32 |
16 |
50 |
Recently drafted white men of 4 to 8 weeks’ service. Pneumonia fairly prevalent in this organization |
| Aug. 26 |
Camp Funston, Kan. |
210th Eng. |
27 |
3 |
11.1 |
About one mile distant from Camp Funston proper. No sickness in this organization |
| Nov. 12 |
Hot Springs, Ark. |
Drafted men assembled to entrain for camp |
50 |
11 |
22 |
50 men selected from isolated farm communities; 12 gave a history of “influenza” within the preceding 8 weeks |
| Nov. 25 |
Camp Pike, Ark. |
Miscellaneous |
26 |
13 |
50 |
12 of this group had influenza during the epidemic |
| Dec. 10 |
Camp Pike, Ark. |
Miscellaneous |
25 |
17 |
68 |
12 of this group had influenza during the epidemic |
| |
Summary: |
Normals |
235 |
88 |
37.4 |
|
| |
|
Cases of influenza (for comparison) |
76 |
61 |
80.3 |
|
37On November 12 search was made for B. influenzæ in 50
normal drafted men who had assembled at Hot Springs,
Ark., on that date preparatory to entraining for Camp
Pike. These men were all from isolated farming communities
where influenza was only moderately prevalent and
where there was little opportunity for the wide dissemination
of B. influenzæ such as occurs when large bodies of
men are assembled in camps. Twelve of the 50 gave a history
of influenza within the preceding eight weeks. The
cultures were made by the same methods as those used at
Camp Pike, the laboratory car “Lister” being taken to
Hot Springs for that purpose. The incidence of B. influenzæ
was only 22 per cent. In striking contrast with this
figure are the figures of 50 and 68 per cent obtained in the
last two groups studied at Camp Pike after the epidemic
had swept through the camp: 24 of the 51 men in these
groups had influenza during the epidemic.
It is of interest to record that the incidence of pneumococcus
in these cases was approximately the same in all
groups and bore no relation to the prevalence of influenza,
bronchitis, or pneumonia.
| 38 |
| Table VIII |
|---|
| |
| Incidence of B. Influenzæ in Normal Men as Determined by Throat Cultures on Blood Agar Plates |
|---|
| |
| DATE |
PLACE |
ORGANIZATION |
NUMBER EXAMINED |
B. INFLUENZÆ PRESENT |
PER CENT POSITIVE FOR B. INFLUENZÆ |
REMARKS |
| Sept. 14–Oct. 5 |
Camp Pike, Ark. |
Med. Detachment, Base Hos.; personnel on measles wards |
82 |
14 |
17.1 |
82 throat cultures in 42 individuals |
| Nov. 5–9 |
Camp Pike, Ark. |
Miscellaneous |
296 |
71 |
23.9 |
Number among this group who had had influenza not recorded |
| Nov. 12 |
Hot Springs, Ark. |
Drafted men assembled to entrain for camp |
64 |
0 |
0 |
Men, in large part from isolated farm communities; 13 gave a history of “influenza” within the preceding 8 weeks |
| Nov. 25 |
Camp Pike |
Miscellaneous |
26 |
13 |
50 |
12 of this group had influenza during the epidemic |
| Dec. 10 |
Camp Pike |
Miscellaneous |
25 |
13 |
52 |
12 of this group had influenza during the epidemic |
| |
Summary |
Normals |
493 |
111 |
22.5 |
|
| |
|
Cases of influenza (for comparison) |
166 |
109 |
65.7 |
|
The results obtained by throat culture are quite similar
to those obtained by the mouse inoculation method. The
entire absence of B. influenzæ in the group of 64 throat cultures
made in the draft men assembled at Hot Springs as
compared with the relatively high incidence in the last two
groups examined at Camp Pike is very striking.
In consideration of the figures presented in Table IX
it is important to remember that the group of 50 men from
Hot Springs were all from isolated farm communities, had
not previously been assembled and had not been in continuous
contact with a widespread epidemic of influenza. On
the other hand, the two groups of normal men at Camp
Pike were studied immediately after the epidemic had
swept through the camp and had been constantly in contact
with epidemic influenza for a period of three months, 24 of
the 51 actually having had the disease during this period.
The fact that in the group of men from Hot Springs, B.
influenzæ was found only by the mouse inoculation method
is noteworthy, since it indicates that the organism was present
in relatively small numbers and could be detected only
by a highly selective method.
39
| Table IX |
|---|
| |
| Incidence of B. Influenzæ in Normal Men Contrasted With That in Early Cases of Influenza as Determined by Multiple Cultures from Nose, Throat, and Sputum |
|---|
| |
| DATE |
PLACE |
GROUP |
NUMBER EXAMINED |
PER CENT SHOWING B. INFLUENZÆ |
| NOSE |
THROAT |
SPUTUM DIRECT CULTURE |
SPUTUM MOUSE INOCULATION |
BY MULTIPLE CULTURES |
| Nov. 12 |
Hot Springs, Ark. |
Normal draft men assembled to entrain for camp |
50 |
0 |
0 |
0 |
22 |
22 |
| |
|
|
|
(4 cultures only) |
(31 cultures only) |
|
|
|
| Nov. 25 |
Camp Pike |
Normal men; 12 had influenza during the epidemic |
26 |
38.6 |
50 |
34.6 |
50 |
80.8 |
| Dec. 10 |
Camp Pike |
Normal men; 12 had influenza during the epidemic |
25 |
48 |
52 |
24 |
68 |
88 |
| Oct. 10 and Nov. 19 |
Camp Pike |
Patients with influenza in Base Hos. |
28 |
21.4 |
50 |
60.7 |
78.6 |
100 |
Summary of the results obtained in normal men shows
that the incidence of B. influenzæ in normal individuals
from isolated communities or in groups free from respiratory
diseases prior to the occurrence of the fall epidemic
40was relatively low, namely, 10 to 20 per cent; that in observations
made before the fall epidemic in groups in which
“bronchitis” and pneumonia were fairly prevalent, B. influenzæ
was found much more frequently, namely, in 25 to
50 per cent of the cases; and that in groups studied at intervals
during the epidemic the incidence of B. influenzæ
rapidly rose, reaching 85 per cent at the end of the epidemic.
In contrast with this, B. influenzæ was found in 100
per cent of cases of influenza without reference to the time
at which they occurred during the epidemic. It is obvious
that the high percentage of normal men carrying B. influenzæ
found at the end of the epidemic can depend only on
the wide dissemination of B. influenzæ that must occur during
epidemic times.
Bacillus Influenzæ in Measles.—Since the presence of B.
influenzæ in other diseases than influenza has been advanced
as an argument against its causal relationship to
influenza, an extensive study of the incidence of B. influenzæ
in the throats of measles patients was made during the period
of the epidemic of influenza at Camp Pike from September
10 to October 20. In all a total of 830 throat cultures
in 487 cases of measles were made, many cases being
cultured repeatedly at weekly intervals. The results have
been condensed as far as possible and are presented in
Tables X, XI, XII.
| Table X |
|---|
| |
| Incidence of B. Influenzæ in 400 Consecutive Cases of Measles as Determined by Throat Culture at Time of Admission to the Base Hospital |
|---|
| |
| DATE |
NUMBER OF CASES |
B. INFLUENZA FOUND |
| NUMBER |
PER CENT |
| Sept. 16–Oct. 4 |
100 |
27 |
27 |
| Oct. 4–Oct. 10 |
100 |
32 |
32 |
| Oct. 10–Oct. 15 |
100 |
32 |
32 |
| Oct. 15–Oct. 19 |
100 |
48 |
48 |
The prevalence of B. influenzæ in cases of measles during
the period of the influenza epidemic corresponded very
closely with that found in normal individuals under similar
circumstances. The increasing proportion of cases carrying
B. influenzæ as the epidemic of influenza advanced is
further evidence of the wide dissemination of the organism
during the epidemic.
| 41 |
| Table XI |
|---|
| |
| Incidence of B. Influenzæ in 830 Throat Cultures in 487 Cases of Measles; Cultures Repeated at Weekly Intervals |
|---|
| |
| DATE |
NUMBER OF CASES |
B. INFLUENZA FOUND |
| NUMBER |
PER CENT |
| Sept. 10–15 |
47 |
15 |
31.9 |
| Sept. 16–29 |
106 |
33 |
31.1 |
| Sept. 30–Oct. 6 |
122 |
38 |
31.1 |
| Oct. 7–13 |
235 |
96 |
40.8 |
| Oct. 14–20 |
320 |
157 |
49.1 |
| Total |
830 |
339 |
40.8 |
| Table XII |
|---|
| |
| Total Number of B. Influenzæ Carriers Among 223 Cases of Measles as Determined by Repeated Throat Cultures at Weekly Intervals after Admission to Hospital |
|---|
| |
| TIMES CULTURED |
NUMBER OF CASES |
NUMBER OF CULTURES |
B. INFLUENZÆ FOUND |
TOTAL CARRIERS IN ONE OR MORE CULTURES |
| NUMBER |
PER CENT |
NUMBER |
PER CENT |
| 2 |
129 |
1st |
37 |
28.7 |
82 |
63.6 |
| |
|
2nd |
63 |
48.8 |
|
|
| 3 |
69 |
1st |
20 |
28.9 |
52 |
75.4 |
| |
|
2nd |
31 |
44.9 |
|
|
| |
|
3rd |
33 |
47.8 |
|
|
| 4 |
25 |
1st |
6 |
24 |
21 |
84.0 |
| |
|
2nd |
10 |
40 |
|
|
| |
|
3rd |
13 |
52 |
|
|
| |
|
4th |
14 |
56 |
|
|
It is evident from the figures presented in Table XII that
a large percentage of the measles cases studied were at one
time or another carriers of B. influenzæ. In consideration
of this fact, it must be borne in mind that all these cases
were cultured during the period when the influenza epidemic
was at its height and that many of these cases had influenza
while in the hospital for measles. No data are
available as to the exact number, since a definite diagnosis
of influenza could hardly be made during the acute stage of
measles. It is probable that approximately 25 per cent
42developed influenza, since that was the incidence of influenza
in the total population of Camp Pike. The consistent
increase in the percentage of influenza carriers clearly
demonstrates that this was due to wide dissemination of
B. influenzæ with the progress of the epidemic. Another
point of exceeding interest is that the percentage of measles
cases carrying B. influenzæ in the throat was lowest during
the acute stage of the disease and increased during convalescence.
This is in direct contrast with the results found
in cases of influenza where the number of cases carrying B.
influenzæ in the throat was highest during the acute stage
and rapidly diminished in uncomplicated cases with the onset
of convalescence.
Summary.—Multiple cultures made simultaneously from
the nose, throat and lower respiratory tract showed that
B. influenzæ was invariably present in all cases of influenza
from the onset of the disease. Not only was B. influenzæ
present in all cases, but it was frequently present in predominant
numbers, sometimes in nearly pure culture. In
the majority of cases that went on to rapid recovery without
the development of an extensive bronchitis or complicating
pneumonia, the predominance of B. influenzæ over
other organisms rapidly diminished coincident with onset
of convalescence. Many cases, however, continued to carry
B. influenzæ in large numbers in the throat throughout convalescence.
No data on the possible duration of the carrier
state have been obtained. By the culture methods employed
no other organism has been found that would suggest
any etiologic relationship to the disease. The two
organisms most frequently associated with B. influenzæ in
postinfluenzal pneumonias, pneumococcus and S. hemolyticus,
have not differed in their incidence in early uncomplicated
cases of influenza from that found in normal individuals.
The incidence of B. influenzæ in normal men, in different
groups studied, has varied between 11.1 and 88 per cent.
43This wide variation has depended upon the prevalence of
respiratory diseases, more particularly influenza, in the
groups studied and the opportunity thereby offered for the
wide dissemination of B. influenza. With the progress of
the epidemic, the number of normal men carrying B. influenzæ
has steadily increased until it reached its maximum
at the end of the epidemic.
The incidence of B. influenzæ in cases of measles studied
during the epidemic of influenza has been relatively high
though never equaling that found in cases of influenza. As
in normal men, the incidence in cases of measles has steadily
increased during the period of the epidemic. Repeated
throat cultures at weekly intervals in cases of measles have
shown that approximately 80 per cent became temporary
carriers of B. influenzæ at one time or another during the
period of the epidemic. Many of these cases had influenza
during the time that they were in the hospital. The carrier
state in cases of measles was found to bear no relation to
the acute stage of the disease since the number of carriers
at the time of admission to the hospital was considerably
lower than that found during convalescence as determined
by repeated cultures in the same cases.
Discussion
The bacteriologic studies in cases of influenza described
in this report fully support Pfeiffer’s claim that B. influenzæ
is invariably present in the disease. It is particularly
important to note that these results were obtained in early
uncomplicated cases of influenza and are not dependent
upon cultures made from cases complicated by pneumonia
or obtained at autopsy. In view of this fact the tendency
so apparent in much of the recent literature to relegate B.
influenzæ to a place of secondary or minor importance in
the disease seems hardly justifiable. It would seem that
this tendency is largely dependent upon three factors: first,
the failure of many to find B. influenzæ either during life or
44at autopsy in any considerable proportion of cases; second,
the frequent failure to draw a clear distinction between influenza
itself and the pneumonia to which it predisposes
with a consequent overemphasis upon autopsy bacteriology
where a considerable variety of secondary organisms have
attracted particular attention; and third, an incorrect interpretation
of the undoubtedly large number of B. influenzæ
carriers found among normal individuals and those
with other diseases during the period of the epidemic and
to less extent in interepidemic times.
Since the majority of workers who are thoroughly familiar
with the technic of cultivating B. influenzæ have encountered
little difficulty in finding it in a large majority
of cases, it is felt that the considerable number of negative
reports that have appeared can depend only upon the unfamiliarity
of those who have failed to find it with the
proper bacteriologic methods. This is quite apparent in
many of the reports that have been published, and is not
surprising in the face of the excessive demand for well-trained
bacteriologists occasioned by the war.
One important feature in the successful isolation of B.
influenzæ from all cases that has been brought out in the
course of the work here reported, is the necessity of making
simultaneous cultures from all portions of the respiratory
tract, since by no single culture method was it found possible
to find the organism in all cases. It has been pointed
out that one of the most characteristic local phenomena of
the disease is the rapidly progressing attack upon the mucous
membranes of the respiratory tract. It seems quite
possible that B. influenzæ in predominant numbers at least
may be found in many cases only at the crest of the wave,
if we may speak of it as such. By way of analogy is the
well-recognized fact that the successful isolation of streptococcus
from cases of erysipelas often depends upon taking
cultures from the margin of the advancing lesion. While
definite proof is lacking for this opinion, it would seem to
45receive some support from the observation that B. influenzæ
rapidly disappears from the throat with the onset of
convalescence in a considerable proportion of cases. It is
felt that these observations, establishing the predominance
of B. influenzæ in the early acute stages of the disease, are
of considerable significance, especially when exactly the reverse
condition was found in studying the incidence of the
organism in cases of measles.
In consideration of the primary cause of influenza, attention
has often been focused upon the many different bacteria
found in autopsy cultures. The most prominent of these
are the ill-defined diplostreptococci of the European writers,
the various immunologic types of pneumococci, and S.
hemolyticus. Other microorganisms less frequently found
are staphylococci, M. catarrhalis, nonhemolytic streptococci,
and B. mucosus capsulatus. It is not within the scope
of this paper to discuss their relation to the various types
of pneumonia found at autopsy, but their very multiplicity
would seem sufficient prima facie evidence that they bear
no etiologic relationship to influenza and must be regarded
only as secondary invaders. If any further support for this
opinion were necessary, it may be found in the studies upon
the incidence of pneumococcus and S. hemolyticus in early
cases of influenza described in this report. Both were found
to occur in the same proportions in which they may be
found in normal individuals at any time.
Although Pfeiffer maintained that B. influenzæ was
found only in true epidemic influenza, the incorrectness of
this contention has been thoroughly established by many
reliable investigators and it has been shown beyond question
that influenza bacilli may always be found in a small
proportion of normal individuals and are not infrequently
found in other respiratory diseases.
The fairly extensive study that has been made of the incidence
of B. influenzæ in normal men and in cases of measles
has clearly demonstrated that the proportion of carriers
46found in any group depends upon the prevalence of
influenza in the group studied and that with the progress
of the epidemic the percentage of carriers has steadily increased.
When one considers that the opportunity for the
dissemination of B. influenzæ by contact infection is almost
unlimited during an epidemic of the proportions of that
which has swept over the country, this is not at all surprising.
That such a large number of normal individuals became
carriers of B. influenzæ during the epidemic would
seem to be sufficient evidence that actual dissemination does
occur and to controvert the theory that in actual cases of
influenza, conditions are established in the respiratory tract
whereby B. influenzæ, always present in small numbers, is
enabled to “grow out” and become the predominant organism.
From a consideration of all the observations made
as to the incidence of B. influenzæ in various conditions it
would appear that the carrier condition is quite analogous
to that found with many other bacteria, and may be divided
into three groups: (a) acute carriers, those having influenza,
(b) contact carriers, those who during epidemic times
become temporary carriers of the organism without contracting
the disease, and (c) chronic carriers, the relatively
small number of normal individuals or those with chronic
respiratory conditions who carry B. influenzæ over long
periods of time. From the facts at hand this would seem to
be the most probable explanation of the conditions found.
It is certainly true that the established presence of pneumococcus,
B. diphtheriæ, meningococcus and many other
organisms in a varying proportion of normal individuals is
not regarded as sufficient evidence to exclude them as the
etiologic agents of the diseases which they cause.
It is quite obvious that if B. influenzæ is to be regarded
as the cause of epidemic influenza, it must change quite
rapidly under certain circumstances from a relatively saprophytic
organism to a relatively virulent pathogenic organism,
and conversely return to its avirulent state following
47the passage of an epidemic. Animal experimentation
has taught us that virulence is acquired by the rapid passage
of an organism from host to host. That an opportunity
for the rapid transference of B. influenzæ from man
to man was provided by the assembling of large groups of
individuals relatively susceptible to respiratory diseases
in our camps and cantonments is by no means impossible.
It has been clearly shown by Vaughn and Palmer[22] that
men from rural districts are very susceptible to respiratory
diseases and that the camps in which such men were assembled
suffered most heavily in this respect during the
winter of 1917–18. This Commission has clearly demonstrated
that an epidemic of influenza swept through Camp
Funston[21] in the spring of 1918 and that a similar epidemic
occurred at Camp Pike. Accumulating evidence will undoubtedly
show that like epidemics existed in many of our
southern camps (Vaughn and Palmer,[22] Soper[23]). It is of
considerable interest that B. influenzæ was found in almost
one-half of the cases of bronchopneumonia studied by Cole
and MacCallum[24] at Fort Sam Houston in February and
March, 1918. This relation is especially noteworthy, since
an epidemic of influenza was seen by one of us (Blake)
among the troops at Kelly Field and Fort Sam Houston
during these months. That similar conditions existed in
European armies as early as 1916–17 is suggested by the
reports of Hammond, Rolland, and Shore[25] and of Abrahams,
Hallows, Eyre, and French[26] on epidemics of “purulent
bronchitis” with bronchopneumonia in the British
army. B. influenzæ was found abundantly in these cases.
Theoretically, under the conditions outlined above, ideal
opportunities have been provided for B. influenzæ to build
up sufficient virulence to enable it to produce the pandemic
of 1918–19. While it is thoroughly recognized that these
48considerations are in the main hypothetical, it is felt that
they are by no means beyond the bounds of possibility, and
for that reason are offered as suggestions worthy of further
investigation.
It is, of course, perfectly possible on the basis of the observations
presented still to regard B. influenzæ as a secondary
invader which makes its appearance in all cases of
influenza simultaneously with the onset of clinical symptoms.
Final proof of its causal relationship to the disease
must depend upon the production of influenza by experimental
inoculation. Results hitherto obtained in attempts
to produce the disease experimentally have been contradictory.
Pfeiffer[8] claimed to have produced a disease in
monkeys in some respects resembling influenza by the intratracheal
injection of freshly isolated cultures of B. influenzæ.
Wollstein,[19] in studies upon the pathogenicity of
various strains, has shown that B. influenzæ is generally
pathogenic for mice and guinea-pigs without respect to
source or virulence for man. Pathogenicity for rabbits
and monkeys, on the other hand, was possessed only by
strains that were highly virulent for man. She furthermore
pointed out that for successful animal experimentation,
it is imperative that inoculations be carried out immediately
after the isolation of the bacilli because they rapidly
lose virulence by subculture on artificial media. It is
felt that failure to appreciate these facts has been responsible
for the often repeated statement that B. influenzæ is
not pathogenic for animals.
In a series of animal experiments carried out by this commission
recorded in an appendix to this report, sixteen-hour
cultures of B. influenzæ freshly isolated from early
cases of influenza were demonstrated to be pathogenic for
monkeys, both by inoculation of the nasal and pharyngeal
mucosa and by intratracheal injection. Monkeys so inoculated
developed coryza, epistaxis, tracheitis, bronchitis, and
extreme prostration. Experiments with forty-eight-hour
49cultures of strains preserved by subculture during from ten
to fifteen days failed to demonstrate pathogenicity for monkeys.
Proof that these monkeys had influenza can depend
only upon the demonstration that they suffered with a disease
having the clinical character and pathologic lesions of
influenza.
The reported failure to produce influenza in man by direct
inoculation with freshly isolated cultures of B. influenzæ
in experiments conducted on volunteers by the United
States Public Health Service[27] at Gallops Island, Boston,
is interesting, but would seem to lack definite significance
since attempts to transmit the disease from man to man by
direct contact also failed. Since all the subjects of these
experiments had been previously exposed to influenza during
the epidemic, 30 per cent actually having contracted the
disease, it would seem probable that the remaining 70 per
cent were only very slightly if at all susceptible. It is noteworthy
that the attack rate of influenza in most army
groups was approximately 20 to 30 per cent during the epidemic,
the remaining 70 to 80 per cent failing to contract
the disease though equally exposed. No other explanation
presents itself except that influenza is no longer transmissible
when clinical symptoms have appeared.
Conclusions
1. Consideration of all the evidence available makes it
seem highly probable that B. influenzæ is the specific etiologic
agent of epidemic influenza, because (a) it is always
present in early uncomplicated cases of influenza; (b) it is
predominantly so during the acute stage of the disease in
cases going on to rapid recovery without development of
complications; (c) its presence in varying numbers in normal
individuals and in other diseases of the respiratory
tract is not valid evidence against its etiologic relationship
to influenza, but on the contrary is quite in harmony with
50what should be expected from our knowledge of other bacteria
known to be the etiologic agents of various respiratory
diseases; (d) its rapidly increasing prevalence in normal
individuals simultaneously with the progress of the
epidemic indicates that actual dissemination of B. influenzæ
readily occurs and is very widespread during pandemic
times; (e) cultures of B. influenzæ freshly isolated from
early acute cases of influenza are pathogenic for animals,
and may produce in monkeys a disease closely resembling
influenza.
2. Final proof of the exact relationship of B. influenzæ
to influenza must depend upon (a) more definite knowledge
of the immunology both of the organism and of the disease,
and (b) knowledge of the pathologic lesions of influenza
and the production of these lesions in animals by inoculation
with B. influenzæ.
51
CHAPTER II
CLINICAL FEATURES AND BACTERIOLOGY OF INFLUENZA AND ITS ASSOCIATED PURULENT BRONCHITIS AND PNEUMONIA
Francis G. Blake, M.D., and Thomas M. Rivers, M.D.
The material presented in this section of the report consists
of clinical and bacteriologic observations made during
the course of an investigation of influenza and its associated
bronchitis and pneumonia at Camp Pike, Ark., between
September 6 and December 15, 1918, comprising part
of a correlated study of the epidemiology, bacteriology,
pathology, and clinical features of these diseases. The bacteriologic
studies are in the main limited to those made during
life, those made at necropsy being reported in another
section of this report.
Methods.—All cases upon which the clinical and bacteriologic
data presented are based, were examined by the
authors and our own clinical histories and physical examinations
were recorded. This was considered of special importance,
since in studying a group of diseases in which
secondary infection of the respiratory tract might supervene
at any time, it was essential to determine as far as
possible the exact clinical condition of the patient at the
time when bacteriologic examinations were made. The bacteriologic
methods employed were the direct culture of
nose and throat swabbings and of selected and washed
specimens of sputum on the surface of 5 per cent defibrinated
horse blood agar plates, the intraperitoneal inoculation
of white mice with specimens of sputum according to
the method described by Blake[28] for the determination of
52pneumococcus types, and in some cases the method of
Avery.[29] B. influenzæ pneumococci and hemolytic streptococci
were identified by the methods described elsewhere.
Note was made in most instances of the presence of other
organisms such as members of the Gram-negative diplococcus
group, staphylococci, diphtheroids, and members of
the streptococcus viridans group, but no attempt was made
to further isolate or identify them since they played no significant
part in the cases studied except in rare instances.
Influenza
The fall epidemic of influenza at Camp Pike began about
September 1, 1918, and reached epidemic proportions on
September 23 when 214 cases were admitted to the base
hospital. The epidemic was at its height from September
27 to October 3, during which period there were in the
neighborhood of 1,000 new cases daily. From this date until
October 31 the number of new cases occurring daily
steadily decreased and by the latter date the epidemic was
over. Scattered cases continued to occur, however, throughout
November, and during the last week of this month and
the first week of December a second epidemic wave of relatively
mild character occurred. From September 1 to October
31 the total number of cases of influenza reporting sick
was 12,393. During the same period there were 1,499 cases
of pneumonia with 466 deaths.
Influenza as observed at Camp Pike differed in no essential
respects from that occurring elsewhere. In brief,
it presented itself as a highly contagious, self-limited infectious
disease of relatively short duration in most instances,
the principal manifestations of which were sudden onset
with high fever, profound prostration, severe aching pains
in back and extremities, conjunctival injection, flushing of
the face, neck, and upper thorax often amounting to a true
erythema, and a rapidly progressing attack upon the mucous
53membranes of the respiratory tract as manifested by
coryza, pharyngitis, tracheitis and bronchitis with a
marked tendency to hemorrhage; in itself it is rarely serious,
but in reality serious because of the large number of
individuals attacked and temporarily incapacitated and because
it predisposed to widespread and highly fatal secondary
infection of the lungs.
Clinical Features.—A clinical study of 100 consecutive
cases of influenza admitted during the height of the epidemic
was made.
The onset was sudden, in most instances being initiated
with marked sensations of chilliness in 82 cases. Although
a severe chill was probably relatively uncommon, 44 of these
patients considered the symptom of sufficient severity to
describe it as such. This was accompanied by extreme general
malaise with severe aching pains throughout the whole
body. Intense backache was complained of in 40 cases,
headache in 54 cases. A varying degree of prostration,
sometimes leading to complete collapse, was almost universal;
5 patients complained of extreme asthenia and 2
of marked dizziness. At time of admission to the hospital
the face, neck and upper chest exhibited a uniform erythematous
flush, never macular in appearance. The conjunctivæ
were deeply injected, but lacrimation was not noticeable
and a true exudative conjunctivitis was not encountered.
Onset was accompanied by a sharp elevation of temperature
ranging from 100° F. to 106° F., in most cases being
between 102° F. and 105° F., at the time of admission.
No constant type of temperature curve was maintained.
Excluding the 15 cases in this group that developed pneumonia,
the temperature was well sustained throughout the
course of the disease in 46, irregular in 33, and definitely
remittent in 6. The duration of the fever varied between
one and seven days, the temperature having returned to
normal in all but 19 of the 85 cases by the end of four days.
The duration of fever was one day in 18 cases, two days in
5412, three days in 19, four days in 17, five days in 10, six
days in 4, and seven days in 5. Of the 4 cases with fever
for six days, 2 had a fairly extensive bronchitis, 1 a laryngitis.
Of the 5 cases with fever of seven days’ duration, 3
had signs of an extensive bronchitis, 2 of only a mild bronchitis.
The pulse was relatively slow in rate as compared with
the degree of temperature elevation, running between 90
and 100 beats per minute in the large majority of cases.
At the height of the disease it was full and easily compressed.
No irregularities were noticed. With recovery
it fell promptly to normal. The respiratory rate showed
only moderate elevation, being between 20 and 26 in most
cases. In a few instances a rate as high as 32 was recorded
at time of admission to the hospital, but this promptly fell
with rest in bed. A respiratory rate rising above 26 after
the third or fourth day of the disease nearly always indicated
a beginning pneumonia. With recovery the rate
promptly fell to normal. Cyanosis did not occur in the
absence of pneumonia.
Aside from the manifestations of a profound toxemia,
influenza was preeminently characterized by symptoms of
respiratory tract infection. The appearance of respiratory
symptoms occurred at varying intervals after the onset of
the disease, being well developed by the end of twenty-four
hours in most cases. A progressive attack upon the mucous
membranes of the respiratory tract was universal, beginning
with coryza and pharyngitis and progressing to
tracheitis or vice versa. Further extension of the infection
to the bronchi, however, was by no means universal, 49
cases in the group studied recovering without developing
evidence of bronchitis. Sore throat was rarely complained
of, and laryngitis, possibly due to secondary infection, occurred
only once. The progress of the infection was marked
subjectively by sensations of irritation, stinging, and a feeling
of tightness. A profuse, thin, mucoid exudate appeared;
55the pharyngeal walls and the soft palate showed a characteristic
deep red granular appearance. The onset of tracheitis
began with a sense of burning and tightness beneath
the sternum accompanied by a harassing cough, at first nonproductive,
later with the outpouring of an exudate becoming
productive. The sputum varied in character between a
scanty, thin, mucoid sputum and a profuse, frankly purulent
sputum in cases subsequently developing an extensive
bronchitis. Hemorrhage from the mucous membranes was
common. Epistaxis occurred in 12 per cent of the cases
and was often profuse. The sputum contained fresh blood
in varying amounts in 24 per cent of the cases; 51 per cent
of the cases developed signs of bronchitis. In 15 of these
the bronchitis was mild, probably limited to the larger
bronchi, physical examination showing only inconstant sibilant
and musical râles. The sputum in these cases was
neither profuse nor frankly purulent; 36 cases developed a
fairly extensive purulent bronchitis as manifested by more
or less diffusely scattered moist râles and by moderately
copious mucopurulent or frankly purulent sputum. This
bronchitis was not accompanied by an increase in the respiratory
rate or by cyanosis unless pneumonia subsequently
developed.
Gastrointestinal symptoms were insignificant: 8 patients
complained of nausea early in the disease and 6 of them
vomited. Diarrhea occurred in only 1 case, constipation
being the rule. The spleen was palpable in 21 cases, but
this is of doubtful significance, since nearly all the patients
came from malarial regions. Jaundice was not noted.
Aside from the profound depression, sometimes amounting
to stupor, mental symptoms were not noted except in 1
case which showed a mild delirium.
Influenza, although per se a self-limited disease of short
duration, frequently leads to the development of serious
complications, the most important of which are pneumonia
and purulent bronchitis with a varying degree of bronchiectasis.
56In the group of 100 cases of influenza studied, purulent
bronchitis developed in 36 instances, pneumonia in
15; in 3 cases there was lobar pneumonia, in 12 bronchopneumonia.
Further discussion of these complications is
reserved for the sections dealing with them in detail. Other
complications were relatively rare. Otitis media occurred
in one case and frontal sinusitis in one. No fatalities were
observed among cases of uncomplicated influenza, the
deaths that occurred being invariably associated with a
secondary pneumonia due in nearly all instances to secondary
infection with pneumococci or hemolytic streptococci.
Purulent Bronchitis
It has been stated that a considerable number of cases
of influenza developed a more or less extensive purulent
bronchitis. This term is used as descriptive of a group of
cases showing clinically evidence of a diffuse bronchitis as
manifested by numerous medium and fine moist râles scattered
throughout the chest and evidence of a definitely purulent
inflammatory reaction as indicated by the expectoration
of fairly copious amounts of mucopurulent or frankly
purulent sputum. This condition is regarded as quite distinct,
on the one hand, from the common type of mucoid
bronchitis frequently associated with “common colds” and
a fairly common feature of uncomplicated cases of influenza,
in which physical examination of the chest reveals
only transient sibilant and musical râles without evidence
of extension to finer bronchi, and, on the other hand, from
bronchopneumonia.
Bacteriology.—Thirteen cases of purulent bronchitis following
influenza in none of which was there any evidence of
pneumonia at the time cultures of the sputum were made
nor later were subjected to careful bacteriologic study.
Specimens of bronchial sputum were collected in sterile
Petri dishes and selected portions thoroughly washed to
remove surface contaminations before bacteriologic examinations
57were made. The results are shown in Table
XIII.
| Table XIII |
|---|
| |
| Bacteriology of the Sputum in Cases of Purulent Bronchitis Following Influenza |
|---|
| |
| CASE |
STAINED FILM OF SPUTUM |
DIRECT CULTURE ON BLOOD AGAR PLATE |
MOUSE INOCULATION |
| |
|
|
|
| GJ |
B. influenzæ + + + |
B. influenzæ + + + + |
B. influenzæ |
| |
Gram + diplococci + |
Pneumococcus + |
Pneumococcus
(type undetermined) |
| WAL |
B. influenzæ + + |
B. influenzæ + + + |
|
| |
Gram + diplococci + + |
Pneumococcus IV + + |
|
| TH |
B. influenzæ + + + |
B. influenzæ + + + + |
|
| |
Gram + diplococci + + + |
Pneumococcus IV + + |
|
| LH |
B. influenzæ + |
B. influenzæ + + |
|
| |
Gram + diplococci + |
Pneumococcus IV + + |
|
| FBD |
Gram + diplococci + + + + |
Pneumococcus IV + + + |
Pneumococcus IV |
| |
|
B. influenzæ + |
B. influenzæ |
| Wa |
B. influenzæ + + |
B. influenzæ + + |
|
| |
Gram + diplococci + + |
Pneumococcus IV + + |
|
| Sh |
B. influenzæ + + + |
B. influenzæ + + |
|
| |
Gram + diplococci + + |
Pneumococcus IV + + + |
|
| Wal |
Gram + diplostrep + + + |
S. viridans + + |
|
| |
B. influenzæ + |
B. influenzæ + + |
|
| CLF |
B. influenzæ + + + + + |
|
B. influenzæ |
| |
Gram + diplococci + |
|
Pneumococcus IV |
| NCC |
B. influenzæ + + |
B. influenzæ + + + |
B. influenzæ |
| |
Gram − micrococcus + |
M. catarrhalis + + |
M. catarrhalis |
| |
Gram + diplostrep. + |
S. viridans + + |
|
| JCM |
B. influenzæ + + + |
B. influenzæ + + + + |
B. influenzæ |
| |
Gram + streptococcus + |
S. hemolyticus + |
S. hemolyticus |
| |
Gram − micrococcus + |
M. catarrhalis + |
Pneumococcus IV |
| |
Gram + diplococcus + |
|
|
| Bl |
B. influenzæ + |
|
B. influenzæ |
| |
Gram + diplococcus + |
|
Pneumococcus IIa |
| Bu |
B. influenzæ + + + + |
B. influenzæ + + + |
B. influenzæ |
| |
Gram + diplococcus + + + + |
Pneumococcus IV + + + |
Pneumococcus IV |
From the data presented in Table XIII it is evident that
a mixed infection existed in all cases. The results obtained
by stained sputum films and by direct culture on blood agar
plates are of special significance. B. influenzæ was present
in all cases, being the predominant organism in 6 cases,
abundantly present in others, and few in number in 2.
Of other organisms the pneumococcus was most frequently
found, occurring in 11 of the 13 cases, in all but 2 instances
being present in considerable numbers. S. viridans was encountered
twice, once in association with a Gram-negative
58micrococcus resembling M. catarrhalis culturally. S. hemolyticus
was found once, together with M. catarrhalis and
a few pneumococci, Type IV, coming through in the mouse
only and of doubtful significance. The stained sputum
films and direct cultures always showed these organisms
present in sufficient abundance to indicate that they were
present in the bronchial sputum and were not merely contaminants
from the buccal mucosa.
It seems quite probable from these results that purulent
bronchitis following influenza is, in most cases at least, due
to mixed infection of the bronchi and should be looked upon
as a complication of influenza. Whether the condition may
be caused by infection with B. influenzæ alone is difficult
to say. No evidence that it may be caused by B. influenzæ
alone was obtained in the cases studied. It is not intended
to enter here into a discussion as to whether B. influenzæ
should be regarded as a secondary invader or not; the other
organisms encountered certainly are. It would seem most
probable that purulent bronchitis is caused by the mixed
infection of B. influenzæ and various other organisms, commonly
the pneumococcus, but that the condition is initiated
by the invasion of the bronchi by these other organisms in
the presence of a preceding infection with B. influenzæ.
Clinical Features.—Purulent bronchitis following influenza
began insidiously without any prominent symptoms
to mark its onset. About the third or fourth day of influenza,
when recovery from the primary disease might be
looked for, the patient would begin to cough more frequently,
raising increasing amounts of mucopurulent
sputum. This sputum was yellowish green in color, copious
in amount, and often somewhat nummular in character,
sometimes streaked with blood. These symptoms were accompanied
by the appearance of coarse, medium and fine
moist râles more or less diffusely scattered throughout
the chest and usually most numerous over the lower lobes.
The percussion note, breath and voice sounds, and vocal
59and tactile fremitus remained normal. There was no
increase in the respiratory rate or pulse rate, and cyanosis
did not develop in the absence of a beginning pneumonia.
Many such cases, of course, developed bronchopneumonia;
in this event areas showing diminished resonance,
suppressed breath sounds, and fine crepitant râles
with the “close to the ear” quality would appear, the respiratory
rate would become increased and cyanosis would
become evident. In those cases of purulent bronchitis
not developing pneumonia, a moderate elevation of temperature,
rarely above 101° F., and irregular in character
usually occurred and persisted for a few days or a week.
Many cases maintained a persistent cough, raising considerable
amounts of sputum throughout the period of their
convalescence in the hospital, which was often considerably
prolonged when this complication of influenza occurred.
Although no clinical data are available on such cases over
a prolonged period of observation, it seems probable that
some of them, at least, had developed some degree of bronchiectasis.
This would seem all the more probable, since
many cases of pneumonia following influenza showed at
autopsy extensive purulent bronchitis with well-developed
bronchiectasis. Bronchiectasis will be discussed in greater
detail in another section of this report. It is this group
of cases with more or less permanent damage to the bronchial
tree that makes this type of bronchitis following influenza
a serious complication of the disease.
Pneumonia
The opportunity presented for a correlated study of the
clinical features, bacteriology, and pathology of pneumonia
following influenza throughout the period of the epidemic
at Camp Pike from September 6, 1918, to December 15,
1918, made it evident that this pneumonia could be regarded
as an entity in only one respect, namely, that influenza was
the predisposing cause. Clinically, bacteriologically, and
60pathologically it presented a very diversified picture ranging
all the way from pneumococcus lobar pneumonia to
hemolytic streptococcus interstitial and suppurative pneumonia
with the picture modified to a varying extent by the
preceding or concomitant influenzal infection.
One hundred and eleven consecutive cases in which careful
clinical and bacteriologic studies were made form the
basis of the material presented. Of these cases, 38 came to
necropsy so that ample opportunity was presented to correlate
the clinical and bacteriologic studies made during
life with the pathology and bacteriology at necropsy. It
has seemed advisable to group the cases primarily on an
etiologic basis with secondary division according to clinical
features in so far as this can be done. Bacteriologic studies
showed that at the time of onset these pneumonias were
either pneumococcus pneumonias or mixed pneumococcus
and influenza bacillus pneumonias in nearly all instances.
Certain of these cases later became complicated by a superimposed
hemolytic streptococcus or a staphylococcus infection.
In a few instances hemolytic streptococcus
pneumonia directly followed influenza without an intervening
pneumococcus infection. B. influenzæ was present in
varying numbers in nearly all cases. In only 2 instances
however, was it found unassociated with pneumococci or
hemolytic streptococci, once alone and once with S. viridans.
Clinically the cases fell into four main groups: (1) Lobar
pneumonia; (2) lobar pneumonia with purulent bronchitis;
(3) bronchopneumonia (pneumococcus); (4) bronchopneumonia
(streptococcus). It should be borne in mind, however,
that the picture was a complex one and that correct
clinical interpretation was not always possible, since
many cases did not conform sharply to any one type and
superimposed infections during the course of the disease
often modified the picture.
Pneumococcus Pneumonia Following Influenza.—Bacteriologic
examination of selected and washed specimens of
61sputum coughed from the lungs at time of onset of pneumonia
showed the various immunologic types of pneumococcus
to be present in 105 cases. The incidence of the
different types is shown in Table XIV.
| Table XIV |
|---|
| |
| Types of Pneumococcus in 105 Cases of Pneumococcus Pneumonia Following Influenza |
|---|
| |
|
LOBAR PNEUMONIA |
BRONCHOPNEUMONIA |
TOTAL |
PER CENT |
| Pneumococcus, Type I |
8 |
0 |
8 |
7.6 |
| Pneumococcus, Type II |
3 |
1 |
4 |
3.8 |
| Pneumococcus, II atyp. |
12 |
7 |
9 |
18.1 |
| Pneumococcus, Type III |
3 |
3 |
6 |
5.7 |
| Pneumococcus, Group IV |
32 |
36 |
68 |
64.8 |
The most noteworthy feature of the figures in Table XIV
is the high proportion of pneumonias due to types of pneumococci
found in the mouths of normal individuals, 93 cases
or 88.6 per cent, being caused by Pneumococcus Types II
atypical, III, and IV. This is in harmony with the results
generally reported and is in all probability due to the fact
that in patients with influenza pneumococci, which under
normal conditions would fail to cause pneumonia, readily
gain access to the respiratory tract and produce the disease.
It is also of interest that with one exception the highly
parasitic pneumococci of Types I and II were associated
with pneumonias clinically lobar in type.
Superimposed infection of the lungs with other types of
pneumococci than those primarily responsible for the development
of pneumonia occurred not infrequently in this
group of cases either during the course of the disease or
shortly after recovery from the first attack of pneumonia.
Pneumococcus Type II infection was superimposed upon
or shortly followed pneumonia caused by Group IV pneumococci
in 4 instances, by Pneumococcus II atypical in 1
instance. In 1 case pneumonia due to Pneumococcus II
atypical occurred three days after recovery from a Pneumococcus
Type I pneumonia, in another case Pneumococcus
62Type III infection was superimposed upon a pneumonia originally
due to a pneumococcus of Group IV. These cases
are presented in detail in another section of this report,
and in several instances were shown to be directly due to
contact infection from patients in neighboring beds.
In a similar manner, superimposed infection with S.
hemolyticus at some time during the course of the pneumonia
occurred in 13 cases in this group, with fatal result
in all but one. Streptococcus infection occurred in pneumonia
due to Pneumococcus II atypical once, to Pneumococcus
Type III once, and to pneumococci of Group IV
eleven times. Nine of these cases were free from hemolytic
streptococci at the time of onset of the pneumonia,
4 showed a very few colonies of hemolytic streptococci in
the first sputum culture made.
B. influenzæ was found in the sputum coughed from the
deeper air passages in the majority of cases, being present
in 80, or 76.2 per cent, of the 105 cases. In the 58 cases
of lobar pneumonia it was found 41 times, or 70.7 per cent,
in the 47 cases of bronchopneumonia 39 times, or 82.9 per
cent. The abundance of B. influenzæ in the sputum varied
greatly in different cases. Microscopic examination of
stained sputum films and direct culture of the sputum on
blood agar plates showed that in general it was more abundant
in the mucopurulent sputum from cases of bronchopneumonia
than in the mucoid rusty sputum from cases
of lobar pneumonia. This was by no means an invariable
rule, however, since in the former the bacilli were sometimes
very few in number, in the latter quite abundant.
Whether B. influenzæ shared in the production of the actual
pneumonia in these cases is difficult to decide and cannot
be stated on the basis of the bacteriologic and clinical observations
which have been made.
Clinical Features.—One of the most striking aspects of
pneumococcus pneumonia following influenza was the
diversity of clinical pictures presented. These varied all
63the way from the classical picture of lobar pneumonia to
that of bronchopneumonia of all grades of severity from
the rapidly fatal coalescing type to that of very mild character
with very slight signs of consolidation. For this
reason it is questioned whether there is any real justification
for speaking of a typical influenzal pneumonia, an
opinion that seems well supported by the diversified picture
found at the necropsy table.
For purposes of presentation, pneumococcus pneumonia
following influenza may be divided into three clinical
groups: (1) Lobar pneumonia; (2) lobar pneumonia with
purulent bronchitis; (3) bronchopneumonia. No accurate
data are available as to the relative frequency with which
these three types occurred at Camp Pike. In the group of
105 cases studied there were 58 cases of lobar pneumonia, 11
of which had purulent bronchitis, and 47 cases of bronchopneumonia.
The majority of these cases, however, occurred
during the early days of the epidemic of influenza
and probably show a considerably higher proportion of
lobar pneumonias than actually occurred in the total number
of pneumonias throughout the epidemic. This is indicated
by the fact that of 100 consecutive cases of influenza
selected for observation at the height of the epidemic, 3 developed
clinical evidence of lobar pneumonia and 12 of
bronchopneumonia.
(1) Lobar pneumonia presenting the typical clinical picture
with sudden onset, tenacious rusty sputum, sustained
temperature, and physical signs of complete consolidation
of one or more lobes occurred in 47 cases; 36 cases in this
group definitely followed influenza. In 11 cases no certain
clinical evidence of a preceding influenza was obtained, and
it is probable that some of these represent cases of pneumonia
occurring independently of the epidemic of influenza.
The onset of pneumonia in this group of cases occurred
from four to nine days after the onset of influenza and with
few exceptions was ushered in by a chill and pain in the
64chest. In several instances the patient had apparently recovered
from influenza as evidenced by fall of temperature
to normal. After twenty-four to seventy-two hours of normal
temperature the patient would have a chill and develop
lobar pneumonia. In the majority of cases, however, lobar
pneumonia developed while the patient was still sick with
influenza. The course of the disease, symptomatology
and physical signs were quite characteristic of lobar pneumonia
and require no special comment. Recovery by crisis
occurred in 21 cases, by lysis in 8. Pneumococcus empyema
developed in 3 cases, fibrinopurulent pericarditis in 3 and
all but 1 of these 6 cases terminating fatally.
In Table XV 5 fatal cases of lobar pneumonia, which
illustrate some of the unusual features of the disease when
it follows influenza, have been summarized. The first 2
cases represent examples of recurring attacks of pneumonia
which developed shortly after recovery from the
first attack, in both instances being due to types of pneumococci
different from those causing the first attack. The
third case represents an example of superimposed infection
of the lungs with hemolytic streptococci and staphylococci
during the course of a pneumonia due to Pneumococcus IV
and disappearance of the latter organism from the tissues
so that it was not found at time of necropsy. The last
2 cases are examples of fulminating rapidly fatal cases of
lobar pneumonia associated with mixed infections of pneumococci
and hemolytic streptococci, the streptococci probably
being secondary in both cases. Cases like the few
examples cited above, which occurred not infrequently
throughout the epidemic of influenza, serve to illustrate
the difficulties which may be met in attempting to correlate
the clinical, bacteriologic and pathologic features of
pneumonia following influenza unless careful bacteriologic
examinations are made both during life and at the necropsy
table in the same group of cases.
65
| Table XV |
|---|
| |
| Cases of Lobar Pneumonia Following Influenza |
|---|
| |
| CASE |
ONSET OF INFLUENZA |
ONSET OF PNEUMONIA |
SPUTUM EXAMINATION |
COURSE OF PNEUMONIA |
NECROPSY |
| DATE |
BACTERIOLOGY |
DIAGNOSIS |
BACTERIOLOGY |
| Pul |
Sept. 7 |
Sept. 9 1st attack bronchopn. |
Sept. 10 |
Pn. IV ++++
B. inf. +++ |
Recovery by crisis on Sept. 14. On Sept. 21 developed lobar pneumonia. Died Sept. 30 |
Lobar pneumonia. Gray hepatization L.L, L.U, R.L. |
H.B. Pn. II
Br. Pn. II ++++
B. inf. +++
R.L. Pn. II + + |
| Lew |
Sept. 16 |
Sept. 20 chill |
Sept. 22 |
Pn. I +++
B. inf. + |
Lobar pn., recovery by crisis Sept. 29. Developed 2nd attack lobar pn. on Oct. 2. Died Oct. 8 |
Lobar pneumonia. Gray hepatization R.U. Fibrinopurulent pleurisy |
H.B. Pn. II atyp.
Br. B. inf. ++++
Pn. IIa +++
S. hem. +
Staph. +
R.U. Pn. IIa ++++ |
| Col |
Sept. 20 |
Sept. 24 |
Sept. 27 |
Pn. IV ++ |
Severe lobar pneumonia. Died on Sept. 30 |
Lobar pneumonia. Red hepatization all lobes. Serofibrinous pl., rt. 125 c.c. |
H.B. S. hem.
Br. S. hem. ++++
Staph. +
L.L. S. hem. ++++
Staph. + |
| Gar |
Sept. 23 |
Sept. 28 |
Sept. 30 |
Pn. IV ++
S. hem. +
B. inf. + |
Fulminating rapidly fatal lobar pneumonia. Died Sept. 30 |
Lobar pneumonia. Engorgement and red hepatization L.U., R.U. |
H.B. S. hem.
Br. S. hem. ++++
B. inf. +++
L.U. S. hem. ++++ |
| Hol |
Sept. 25 |
Sept. 30 |
Sept. 30 |
Pn. III ++
B. inf. ++ |
Fulminating rapidly fatal lobar pneumonia. Died Oct. 1. |
Lobar pneumonia. Engorgement all lobes |
H.B. sterile
Br. B. inf. ++++
Pn. III ++
S. hem. +
R.L. Pn. III ++++
B. inf. ++
S. hem. + |
| L.L. R.L., etc., indicates lobes involved. H. B. = Heart’s blood. Br. = bronchus. |
66(2) There were 11 cases of lobar pneumonia with purulent
bronchitis in the group studied. Clinically, they
closely resembled the cases in the preceding group except
in so far as the picture was modified by the presence of the
purulent bronchitis. All directly followed influenza. The
sputum, instead of being rusty and tenacious, was profuse
and mucopurulent, usually streaked with blood. Stained
films and direct culture on blood agar plates showed pneumococci
in abundance and B. influenzæ in varying numbers,
in only two instances the predominant organism. The
physical signs were those of lobar pneumonia with, in addition,
those of a diffuse bronchitis as manifested by medium
and coarse moist râles throughout both chests. Five cases
recovered by crisis; 6 terminated fatally and in all of them
the clinical diagnosis of lobar pneumonia with purulent
bronchitis was confirmed at necropsy.
(3) Forty-seven cases in the group studied presented the
clinical picture of bronchopneumonia. The onset of pneumonia
in these cases was in most instances insidious and
appeared to occur as a continuation of the preceding influenza.
The temperature, instead of falling to normal
after from three to four days, remained elevated or rose
higher, the respiratory rate began to rise, a moderate cyanosis
appeared, the cough increased, and the sputum
became more profuse, usually being mucopurulent and
blood streaked, sometimes mucoid with fresh blood. The
pulse showed little change at first, being only moderately
accelerated. Pleural pain, so characteristic of the onset of
lobar pneumonia, was rarely complained of, but a certain
amount of substernal pain was common, probably due to
the severe tracheobronchitis. Physical examination at this
time revealed small areas showing relative dullness, diminished
or nearly absent breath sounds, and fine crepitant
râles. These areas usually appeared first posteriorly over
the lower lobes.
67The subsequent course of the disease showed the widest
variation from mild cases with limited pulmonary involvement
going on to prompt recovery in four or five days with
defervescence by lysis or crisis to those presenting the picture
of a rapidly progressive and coalescing pneumonia
with fatal outcome. In the milder cases the diagnosis of
pneumonia depended in considerable part upon the general
symptoms of continued fever, increased respiratory rate,
and slight cyanosis. Definite pulmonary signs were always
present if carefully looked for, though sometimes not outspoken.
Areas of bronchial breathing and bronchophony
often appeared late, sometimes not until the patient was
apparently recovering. In the severe cases cyanosis became
intense and an extreme toxemia dominated the picture.
In certain of these cases there was an intense pulmonary
edema. The respiratory rate showed wide variation,
the breathing in some cases being rapid and gasping,
in others comparatively quiet. Progressive involvement
of the lungs occurred with the development of marked dullness,
loud bronchial breathing and bronchophony. Abundant
medium and coarse moist râles were heard throughout
the chest, probably due in considerable part to the extensive
bronchitis almost universally present. An active delirium
was not uncommon. Signs of pleural involvement,
even in the most severe and extensive cases, rarely occurred,
except in those cases in which a hemolytic streptococcus
infection supervened.
Of the 47 cases in this group, 29 recovered; 14 by crisis,
15 by lysis. The average duration of illness from the onset
of influenza until recovery from the pneumonia was ten
days, the majority of these cases being relatively mild in
character with pneumonia of three to six days’ duration.
Empyema with ultimate recovery occurred in 1 of these
cases, Pneumococcus Type II being the causative organism.
There were 18 fatal cases in the group. Nine of these
are summarized in Table XVI as illustrative of the frequently
68complex character of bronchopneumonia following
influenza and because of the interest attaching to the bacteriologic
examinations made during life and at necropsy.
Case 70 is a typical instance of the rapidly progressive
type of confluent lobular pneumonia with extensive purulent
bronchitis, intense cyanosis, and appearance of suffocation,
with which pneumococci, in this case Pneumococcus
IV, and B. influenzæ are commonly associated. Case 59
is illustrative of the small group of bronchopneumonias
following influenza which die, often unexpectedly, after a
long drawn out course, in this instance three weeks after
onset. Examination of the sputum at the time the pneumonia
began, showed Pneumococcus Type IV and B. influenzæ.
At necropsy there was a lobular pneumonia with
clustered small abscesses, probably due to a superimposed
infection with S. aureus. There was a well-developed bronchiectasis
in the left lower lobe. Cultures taken at autopsy
showed a sterile heart’s blood, which is not infrequently
the case in cases of pneumococcus lobular pneumonia after
influenza. Cultures from the consolidated portions of the
lung showed no growth, the pneumococcus having disappeared
as might be expected from the duration of the case.
B. influenzæ together with staphylococci were found in the
bronchi. In Cases 50 and 56 a second attack of pneumonia
caused by a different type of pneumococcus from that responsible
for the first attack occurred, the second attack in
both instances being due to contact infection with Pneumococcus
Type II from a patient in a neighboring bed suffering
with Pneumococcus Type II pneumonia. Both cases
showed at necropsy the type of confluent lobular pneumonia
so commonly found in pneumococcus pneumonias following
influenza. Case 107 illustrates well the extent to which
mixed infections may occur, especially when cases are
treated in crowded hospital wards. The sputum at time
of onset showed Pneumococcus IV in abundance and a few
staphylococci. At necropsy there was a confluent lobular
pneumonia with clustered abscesses, purulent bronchitis,
and bronchiectasis in the left lower lobe. The heart’s
blood was sterile, the lungs showed Pneumococcus Type III
and staphylococci. B. influenzæ was not found, but through
oversight, no cultures were taken from the bronchi. Cases
92, 99, 102, and 104 are all examples of superimposed hemolytic
streptococcus infection occurring in the presence of a
Pneumococcus Type IV pneumonia, with the picture of interstitial
suppuration, abscess formation, and empyema
due to S. hemolyticus on the background of a pneumococcus
lobular pneumonia found at necropsy. All showed abundant
pneumococci and B. influenzæ in the sputum and were
free from hemolytic streptococci at time of onset of pneumonia,
except Case 92 which showed 2 colonies of S. hemolyticus
in the first sputum culture made. At time of death
the pneumococci had disappeared in all cases and were replaced
by hemolytic streptococci.
69
| Table XVI |
|---|
| |
| Cases of Bronchopneumonia Following Influenza |
|---|
| |
| CASE |
ONSET OF INFLUENZA |
ONSET OF PNEUMONIA |
SPUTUM EXAMINATION |
COURSE OF PNEUMONIA |
NECROPSY |
| DATE |
BACTERIOLOGY |
DIAGNOSIS |
BACTERIOLOGY |
| 70 |
Sept. 18 |
Sept. 21 |
Sept. 22 |
B. inf. ++++
Pn. IV ++ |
Diffuse bronchitis with rapidly progressive confluent bronchopneumonia. Died Sept. 24 |
Nodular and diffuse confluent lobular pneumonia. Purulent bronchitis. Bronchiectasis |
H.B. sterile
Br. B. inf. ++++
Pn. IV ++
Lun. B.inf. +++
Pn. IV +++ |
| 59 |
Sept. 13 |
Sept. 18 |
Sept. 19 |
Pn. IV +++
B. inf. + |
Bronchopneumonia with long drawn out course. Died Oct. 4 |
Lobular pneumonia, with clustered abscesses. Bronchiectasis |
H.B. sterile
Br. B.inf. +++
Staph. ++
R.L. no growth. |
| 50 |
Sept. 14 |
Sept. 17 |
Sept. 18 |
Pn. IV +++ |
Mild bronchopneumonia improving on Sept. 24. On Sept. 26 became suddenly worse and died on Sept. 30 |
Nodular and confluent lobular pneumonia. Purulent bronchitis |
H.B. sterile
Br. B.inf. +++
Staph +
R.L. Pn. II +++
B.inf. +
L.U. Pn. II +++ |
| 56 |
Sept. 10 |
Sept. 17 |
Sept. 18 |
Pn. IIa +++ |
Bronchopneumonia with recovery by crisis on Sept. 19. Developed a second attack of pneumonia and died Sept. 29 |
Confluent lobular pneumonia |
H.B. Pn. II
Br. Pn. II +++
B.inf. ++
L.L. Pn. II +++
B.inf. +
|
| 107 |
Sept. 27 |
Sept. 29 |
Oct. 1 |
Pn. IV +++
B. inf. +
Staph. + |
Diffuse bronchitis and severe bronchopneumonia. Died Oct. 5 |
Confluent lobular pneumonia with clustered abscesses. Pur. bronchitis and bronchiectasis |
H.B. sterile
R.L. Pn. III ++
Staph. ++
L.L. Staph. ++ |
| 92 |
Sept. 23 |
Sept. 28 |
Oct. 1 |
B. inf. +++++
Pn. IV +++
S. hem. 2 col. |
Severe bronchopneumonia with empyema. Died Oct. 5 |
Lobular pneumonia. Empyema. Purulent bronchitis |
H.B. S.hem.
Br. B.inf. +++
S.hem. +++
R.L. S.hem. +++
B.inf. ++ Emp. S.hem. |
| 99 |
Sept. 24 |
Sept. 29 |
Oct. 1 |
B. inf. ++++
Pn. IV ++
S. vir. + |
Diffuse purulent bronchitis with bronchopneumonia. Died Oct. 7 |
Bronchopneumonia. Purulent bronchitis |
H.B. S.hem.
Br. B.inf. +++ Lun. S.hem. +++
S.hem. ++ B. inf. + |
| 102 |
Sept. 24 |
Sept. 28 |
Oct. 1 |
Pn. IIa +++
B. inf. ++ |
Severe bronchopneumonia with empyema. Died Oct. 4 |
Lobular pneumonia with interstitial suppuration. Pur. bronchitis. Empyema |
H.B. S.hem.
Br. B.inf. +++
S.hem. +++
R.L. S.hem. +++ |
| 104 |
Sept. 26 |
Oct. 1 |
Oct. 1 |
B. inf. ++++
Pn. IV +++ |
Diffuse purulent bronchitis with severe bronchopneumonia. Developed streptococcus empyema. Died Oct. 11 |
Nodular bronchopneumonia with interstitial suppuration. Pur. bronchitis and bronchiectasis. Empyema. |
H.B. S.hem.
R.L. S.hem. ++++
Emp S.hem. |
70The cases cited in the preceding paragraph are illustrative
examples from a series of over 250 necropsies which
are described in another section of this report. They serve
to indicate clearly the extent to which mixed and superimposed
infections of the lungs may occur in pneumonia
following influenza and leave little doubt that a considerable
proportion of the deaths from influenzal pneumonia are
due to this circumstance.
Hemolytic Streptococcus Pneumonia Following Influenza
But 4 cases of hemolytic streptococcus pneumonia directly
following influenza without an intervening pneumococcus
infection of the lungs occurred in the group of cases
studied clinically. Superimposed infection with S. hemolyticus,
however, occurred not infrequently during the
course of pneumococcus pneumonia following influenza, as
has been stated above. This occurred 3 times in lobar
pneumonia and 10 times in bronchopneumonia, with fatal
outcome in all but 1 case.
71Bacteriology.—Bacteriologic examination of the sputum
in the 4 cases of streptococcus pneumonia directly following
influenza showed S. hemolyticus present in abundance.
B. influenzæ was also present in large numbers in 3 cases,
but was not found in the fourth. In 1 case a Gram-negative
micrococcus resembling M. catarrhalis was also present
in large numbers in the sputum. Pneumococci were
not found either by direct culture on blood agar plates or
by inoculation of the sputum intraperitoneally in white
mice.
In the 13 cases of superimposed hemolytic streptococcus
infection occurring during the course of pneumococcus
pneumonia, bacteriologic examination of the sputum by direct
culture and by mouse inoculation shortly after onset
of the pneumonia showed Pneumococci (atypical II once,
Type III once, Group IV eleven times) B. influenzæ
present in large numbers, and no hemolytic streptococci except
in 4 instances in which a very few organisms were present.
Subsequent invasion of the lower respiratory tract by
S. hemolyticus was shown to occur by means of cultures of
empyema fluids or by cultures made at necropsy.
Clinical Features.—The 4 cases of hemolytic streptococcus
pneumonia following influenza that occurred in this
series resembled in all respects the secondary streptococcus
pneumonias of the winter and spring of 1918 and presented
no features requiring special comment. The onset resembled
that of pneumococcus bronchopneumonia, the
disease appearing to develop as a continuation of the preceding
influenza. The sputum was profuse and mucopurulent
in 3 cases, mucoid and bloody in the other. Two
cases ran a severe and rapid course with the development
of empyema early in the disease and fatal outcome. The
other 2 cases ran only moderately severe courses without
developing empyema and recovered by lysis in twenty and
fifteen days, respectively, after the onset of influenza.
Clinical differentiation between streptococcus and pneumococcus
72bronchopneumonia following influenza did not seem
possible without bacteriologic examination of the sputum
except in those cases of the streptococcus group which developed
an extensive pleural effusion early in the disease.
The advent of superimposed hemolytic streptococcus infection
of the lower respiratory tract during the course of
pneumococcus pneumonia following influenza presented no
clinical features that made diagnosis certain without bacteriologic
examination. The sudden occurrence of a pleural
exudate during the course of the disease seemed of particular
significance, especially since empyema in the bronchopneumonias
following influenza was exceedingly rare
in the absence of hemolytic streptococcus infection. Other
suggestive symptoms were a chill during the course of the
disease, a sudden turn for the worse in cases apparently
doing well, or the development of a cherry red cyanosis.
None of these features, however, was sufficiently constant
or distinctive of streptococcus invasion to be depended upon
and when they occurred, were merely indications for further
bacteriologic examination.
Bacillus Influenzæ Pneumonia Following Influenza
Bacteriologic evidence that cases of pneumonia following
influenza might be due to B. influenzæ alone was very
meager in the group of cases studied clinically at Camp
Pike; in fact, no convincing evidence was obtained that
such cases occurred. In one case B. influenzæ alone was
found in the sputum coughed from the deeper air passages,
and in another case B. influenzæ with a few colonies of S.
viridans was found. Both were cases of bronchopneumonia,
mild in character, and recovered promptly. They
presented no clinical features by which they could be distinguished
from cases of pneumococcus bronchopneumonia.
It has been previously stated that B. influenzæ was found
in all early uncomplicated cases of influenza somewhere
in the respiratory tract; that it was present together with
73other organisms, notably pneumococcus in the sputum from
cases of purulent bronchitis following influenza; and that
it was found in the sputum coughed from the lung in approximately
80 per cent of cases of pneumonia complicating
influenza. In 35 cases it was very abundant, often
being the predominating organism. In all these cases,
however, pneumococci or hemolytic streptococci were also
present in considerable numbers at the time of onset of the
pneumonia. It is impossible to say merely from the clinical
and bacteriologic data under consideration what part
B. influenzæ played in the development of the actual pneumonia
in these cases. Discussion of this subject is therefore
reserved for the section of this report dealing with the
pathology and bacteriology of pneumonia following influenza.
Summary
Influenza as observed at Camp Pike presented itself
as a highly contagious infectious disease, the principal
clinical manifestations of which were, sudden onset with
high fever, profound prostration with severe aching pains
in the head, back and extremities, erythema of the face,
neck and upper chest with injection of the conjunctivæ,
and a rapidly progressive attack upon the mucous membranes
of the respiratory tract as evidenced by coryza,
pharyngitis, tracheitis and bronchitis with their accompanying
symptoms. In the majority of cases it ran a short
self-limited course, rarely of more than four days’ duration,
and was never fatal in the absence of a complicating
pneumonia.
Bacteriologic examination in early uncomplicated cases
of the disease showed the B. influenzæ of Pfeiffer to be
present in all cases, often in predominating numbers. It
was found more abundantly present during the acute stage
of the disease than during convalescence in uncomplicated
cases. No other organisms of significance were encountered
by the methods employed.
74Purulent bronchitis of varying extent developed in approximately
35 per cent of the cases and often prolonged
the course of the illness to a considerable extent. Bacteriologic
studies showed that it was invariably associated
with a mixed infection of the bronchi with B. influenzæ and
other bacteria, in most instances the pneumococcus, and indicated
that it should be regarded as a complication rather
than as an essential part of influenza. Its clinical features
consisted of a mild febrile reaction, frequent cough with
the raising of considerable amounts of purulent sputum,
and the physical signs of a more or less diffuse bronchitis.
It led to a varying degree of bronchiectasis in at least some
instances.
Pneumonia complicating influenza presented a very diversified
picture and appeared to have only one constant
character, namely, that influenza was the predisposing
cause. It may be best classified on an etiologic basis since
the clinical features to some extent and the pathology to a
much greater extent depended upon the infecting bacteria
in a given case.
Bacteriologic examination showed that a very large proportion
of the cases was due to infection with the different
immunologic types of pneumococci or to a mixed infection
with B. influenzæ and pneumococci. The types of pneumococci
commonly found in normal mouths, namely, II atypical,
III, and IV, comprised approximately 88 per cent of
these, the highly parasitic Pneumococci Types I and II,
but 12 per cent. A small number of cases were due to
hemolytic streptococci or to mixed infection with B. influenzæ
and S. hemolyticus. No certain evidence was obtained
that pneumonia was due to B. influenzæ alone. This organism
was present in varying numbers, however, in
approximately 80 per cent of the sputums examined, and
it seems fairly certain that it must have played at least
a part in the development of the pneumonia in many of
the cases in which it was found. Superimposed infections
75with other types of pneumococci than those primarily responsible
for the development of pneumonia, with hemolytic
streptococci and with Staphylococcus aureus occurred
frequently in cases of pneumococcus or mixed pneumococcus
and B. influenzæ pneumonia and undoubtedly contributed to
a considerable extent in increasing the number of deaths.
Three clinical types of pneumococcus pneumonia following
influenza occurred: lobar pneumonia, lobar pneumonia
with purulent bronchitis, and bronchopneumonia. Lobar
pneumonia was usually sudden in onset and ran the characteristic
course of the primary disease. Lobar pneumonia
with purulent bronchitis similarly ran the characteristic
course of the primary disease but presented the unusual
picture of lobar pneumonia with mucopurulent rather than
rusty, tenacious sputum and numerous moist râles throughout
the unconsolidated portions of the lungs. The cases
of bronchopneumonia ran a very variable course from mild
cases of a few days’ duration and meager signs of consolidation
to rapidly progressive cases with signs of extensive
pulmonary involvement. Purulent bronchitis was very
frequently associated with bronchopneumonia.
Hemolytic streptococcus pneumonia following influenza
presented the clinical picture of bronchopneumonia and was
not readily distinguished on clinical grounds from pneumococcus
bronchopneumonia except in those cases which
developed a pleural exudate early in the disease. The advent
of tertiary infection of the lower respiratory tract with
hemolytic streptococci in cases of secondary pneumococcus
pneumonia presented no symptoms sufficiently constant or
certain to make clinical diagnosis easy. The development
of empyema in pneumococcus bronchopneumonia usually
meant streptococcus infection.
Pure B. influenzæ pneumonia, if such cases existed, presented
no diagnostic features by which it could be distinguished
from pneumococcus bronchopneumonia following
influenza. It was impossible to determine on clinical and
76bacteriologic grounds alone what part the prevalent influenza
bacilli played in the causation of the actual pneumonia.
Discussion
That wide variations in the conception of influenza have
arisen during the recent pandemic, even a hasty review of
the literature makes clear. In its essence this divergence
of opinion seems to depend upon whether pneumonia is
considered an essential part of influenza or a complication
due either to the primary cause of influenza or to
secondary infection. One extreme is expressed by Dunn[30]
who says “the so-called complication is the disease,” the
other by Fantus[31] who finds influenza a relatively mild
disease with pneumonia a relatively infrequent and largely
preventable complication.
A similar divergence of opinion prevails with respect to
the bacteriology of influenza. There is fairly general
agreement that the members of the pneumococcus and
streptococcus groups and to a less extent other organisms
are responsible for a large proportion of the secondary
pneumonias, and but few observers hold that they possess
any etiologic relationship to influenza. No such uniformity
of opinion exists, however, with respect to the relation
of B. influenzæ to influenza and to the complicating pneumonia.
By some it is considered the primary cause of
influenza, by others it is regarded as a secondary invader
responsible for a certain proportion of the secondary
pneumonias, and by still others it is not considered to bear
any relation either to influenza or its complications.
A limited number of references to the extensive literature
of the recent pandemic will amply serve to illustrate
the various points of view that have developed.
Keegan[32] regards pneumonia as a complication and considers
that B. influenzæ, the probable cause of influenza, is
77the primary cause of the pneumonia which may or may not
be still further complicated by pneumococcus or streptococcus
infection as a terminal event. Christian[33] states that
epidemic influenza causes a clinically demonstrable bronchitis
and bronchopneumonia in the larger proportion of
cases, and lays particular emphasis upon the fact that it
is quite incorrect to consider fatalities in the epidemic as
due to influenza uncomplicated by bronchopneumonia.
Blanton and Irons[34] speak of influenza as an “antecedent
respiratory infection” of undetermined etiology, and believe
that pneumonia when it occurs is due to autogenous
infection by a variety of secondary invaders, principally
of the pneumococcus and streptococcus groups. Hall,
Stone, and Simpson[35] regard pneumonia strictly as a complication
and quite distinct from influenza itself. Synnott
and Clark[36] believe that the infection is characterized by a
progressive intense exudative inflammation of the respiratory
tract often terminating in an aspiration pneumonia
with a variety of conditions found at autopsy and a multiplicity
of secondary organisms responsible for the fatal
termination. B. influenzæ was usually found but always
with other organisms. Friedlander and his collaborators[37]
speak of a fulminating fatal type of influenza with acute
inflammatory pulmonary edema, but regard true bronchopneumonia
as secondary, due to infection with pneumococcus
or S. hemolyticus. B. influenzæ was not found more
frequently than under normal conditions. Brem[38] and his
collaborators present a clear cut clinical picture both of
influenza and the secondary pneumonia to which it predisposes,
regarding the latter as definitely due to secondary
infection with pneumococcus, streptococcus or B. influenzæ,
the virus of influenza being unknown. Ely[39] and his collaborators
78make no distinction between influenza and pneumonia,
and apparently consider the epidemic due to a hemolytic
streptococcus of indefinite and inconstant characters.
The Camp Lewis Pneumonia Unit[40] states “the process
[influenza], whether mild or severe, is etiologically and
pathologically the same; * * *.” B. influenzæ was not
found. In a report of The American Public Health Association[41]
it is stated that deaths resulting from influenza
are commonly due to pneumonias resulting from an invasion
of the lungs by one or more forms of streptococci,
by one or more forms of pneumococci, or by the so-called
influenza bacillus. This invasion is apparently secondary
to the initial attack. Wolbach[42] found B. influenzæ in a
high proportion of cases, not infrequently in pure culture
in the lung, and believes that there is a true influenzal pneumonia
whether B. influenzæ is the cause of the primary disease
or not. Spooner, Scott and Heath[43] isolated B. influenzæ
in a high percentage of cases and consider it
reasonable to suppose that it was the prime factor in the
epidemic. Kinsella[44] found B. influenzæ infrequently and
regards it as a secondary invader. MacCallum[45] regards
B. influenzæ as a secondary invader and believes that it is
responsible for a form of purulent bronchitis and bronchopneumonia
following certain cases of influenza. Pritchett
and Stillman[46] found B. influenzæ in 93 per cent of cases of
influenza and bronchopneumonia. Hirsch and McKinney[47]
state that B. influenzæ played no rôle in the epidemic at
Camp Grant and apparently consider it due to a specially
virulent pneumococcus.
No further references to the extensive literature of the
recent pandemic seem necessary, since those cited above
serve to illustrate the various points of view that exist.
79A similar diversity of opinion may be found in the reports
from foreign sources.
It would appear that much of the divergence of opinion
that has been formed has depended to a considerable extent
upon the conditions under which cases have been observed.
This is clearly brought out by contrasting the
experience of Fantus[39] dealing with private cases in civilian
practice, where pneumonia was relatively uncommon, with
that of others dealing only with cases in large hospitals,
where those admitted have been in large part selected seriously
ill patients with a high incidence of pneumonia, the
milder cases comprising from 60 to 90 per cent of those
attacked by influenza never reaching the hospital. Variations
in opinion with respect to the bacteriology of the
epidemic, especially in regard to B. influenzæ, would appear
to be due for the most part to differences in bacteriologic
technic, in some degree to differences in interpretation.
Accumulating evidence can leave little doubt that B. influenzæ
was at least extraordinarily and universally prevalent
throughout the period of the epidemic and thereafter,
and that earlier reports of failure to find it were due to the
use of methods unsuitable for its detection and isolation.
The opportunity afforded the commission at Camp Pike
to devote their full time to a systematic and correlated
group study of the epidemic simultaneously from many
aspects throughout its whole course made it apparent that
influenza per se is in the large majority of instances, in
spite of the initial picture of profound prostration, a relatively
mild disease which tends to rapid spontaneous recovery.
This opinion is supported by the fact that the
disease during the first waves of the epidemic in this country,
which it is now recognized occurred pretty generally
in the army camps during the spring of 1918, was so mild
that it attracted only passing attention, since the disease
at that time was not sufficiently virulent to predispose to
any alarming amount of pneumonia. With the return of
80the epidemic in the late summer and early fall, however,
the disease had attained such a high degree of virulence
that it predisposed to an appalling amount of severe and
often rapidly fatal pneumonia, which often detracted attention
from the real nature of the preceding disease.
Yet even during the fall epidemic from 60 to 90 per cent
of the cases of influenza proceeded to rapid recovery without
developing complications. On this ground alone it
would seem only logical to regard pneumonia strictly as a
complication of influenza rather than as an essential part
of the disease, irrespective of whether the pneumonia may
be caused by the primary cause of influenza or not. The
complexity of the clinical features, the bacteriology and
pathology of the pneumonias following influenza lend further
support to this opinion.
It seems better, therefore, to consider influenza first as
a disease by itself and subsequently to take up the question
of pneumonia and the relation of influenza to it.
The most striking clinical features of influenza are its
epidemic character, its involvement of the respiratory
tract, its extremely prostrating effect, and the often surprising
rapidity with which the individual cures himself.
These features strongly suggest that the etiologic agent of
the disease is an organism subject to rapid changes in virulence;
that it is confined to the respiratory tract where it
produces a superficial inflammatory reaction giving rise to
the characteristic symptoms of coryza, pharyngitis and
tracheitis; that it elaborates a poison, possibly a true toxin,
readily absorbed by the lymphatics, the effect of which is
manifested in the profound prostration, severe aching
pains, erythema, and leucopenia; and that it may either
disappear promptly from the respiratory mucous membrane
at time of recovery or may persist, leading a relatively
saprophytic existence for an indefinite period of
time, being no longer harmful to the individual, at least
more than locally, because of an acquired immunity. Furthermore,
81in our opinion, the very brief incubation period
suggests that the disease is bacterial in origin, rather than
that it is analogous to the exanthemata, the majority of
which present a comparatively long, fairly constant, incubation
period.
B. influenzæ has characteristics in accord with the clinical
features of influenza. It is an organism of very labile virulence;
it is always present in our experience on the mucous
membranes of the respiratory tract in early uncomplicated
cases of influenza, often in overwhelming numbers; in only
very exceptional instances, in adults at least, does it invade
the body producing a general infection, as the numerous
reports of negative blood cultures testify; recent investigations
by Parker[48] and others indicate that it is capable of
producing a toxin quickly fatal for rabbits; it is predominantly
present in the respiratory tract during the active
stage of the disease and disappears in a considerable proportion
of cases at time of recovery, while in others, more
particularly those that develop an extensive secondary
bronchitis and bronchiectasis it may persist for an indefinite
period of time.
It is, of course, fully appreciated that the foregoing is
in the main merely argumentative reasoning and it is put
forth only to suggest that B. influenzæ merits a much closer
scrutiny with respect to its etiologic relationship to influenza
than the trend of present opinion has awarded it.
Although there remains some difference of opinion as to
the relation of influenza to pneumonia, the majority of observers
concur in regarding pneumonia as a complication
and this would seem to be the only logical interpretation of
the facts available. The same may be said with respect to
purulent bronchitis and bronchiectasis. It is of considerable
significance in this connection that pneumonia following
influenza presents no uniform clinical picture, no uniform
bacteriology and no uniform pathology. Whether the
82predisposition of patients with influenza to contract pneumonia
is preponderantly due to lowering of general resistance
to infection by the extremely prostrating effect of the
disease and the inhibition of leucocytic defense, or to a destruction
of local resistance against bacterial invasion by
reason of profound injury to the bronchial mucosa, or to a
combination of both factors, is difficult to say. It seems
most probable that both are concerned. At any rate it
seems clear that in the presence of influenza a considerable
variety of organisms which under ordinary conditions do
not find lodgement in the lungs are able to gain access to
the lower respiratory tract and produce pneumonia.
83
CHAPTER III
SECONDARY INFECTION IN THE WARD TREATMENT OF INFLUENZA AND PNEUMONIA
Eugene L. Opie, M.D.; Francis G. Blake, M.D.; James C. Small, M.D.; and Thomas M. Rivers, M.D.
One of the most pressing problems that presented itself
in the care of influenza and pneumonia patients in the army
cantonments during the recent epidemic was the danger of
secondary contact infection because of the overcrowding of
the base hospitals, nearly all of which were taxed far beyond
the limits of their capacity. That this danger was
very real was fully demonstrated by certain studies in ward
infection that this commission was able to make at Camp
Pike[49]. It is the purpose of the present section of the report
to present these studies and to discuss the means
whereby this danger may be most successfully met.
It is perhaps well, first to define exactly what is meant
by secondary contact infection in influenza and pneumonia.
In our experience at Camp Pike it was found that a very
large percentage of the pneumonias following influenza
were accompanied by secondary infection with pneumococcus,
some few being caused by hemolytic streptococcus.
The types of pneumococcus encountered were almost entirely
those that are found normally in the mouths of
healthy men, approximately 85 per cent being Types II
atypical, III, and IV. It has been generally accepted that
infection with these types of pneumococci is usually autogenous—that
is, that under the proper conditions of lowered
resistance an individual becomes infected with the
pneumococcus that he carries in his own mouth. Many observations
84made during the course of the present work
have suggested that this is probably not so in many instances
and that the influenza patient may not be so much
in danger from the pneumococcus that he normally carries
in his own mouth as he is from that carried by his neighbor,
in other words, he is in danger from contact infection. The
same considerations hold true with respect to hemolytic
streptococcus infection. Secondary contact infection in
cases of already existing pneumonia following influenza
were found to occur frequently. These were for the most
part caused by hemolytic streptococcus infection superimposed
upon a pneumococcus pneumonia. Many instances
of double pneumococcus infection, however, either coincident
with or following one another were encountered.
Secondary Infection with S. Hemolyticus in Pneumonia
Pneumonia caused by streptococci was repeatedly observed[50]
during the pandemic of influenza which occurred in
1889–90. With clearer recognition of the characters which
distinguish varieties of streptococci several observers have
shown that secondary infection with hemolytic streptococci
may occur during the course of pneumonia and though definite
evidence has been lacking have suggested that it may
be acquired within hospital wards. That a similar secondary
infection with S. hemolyticus in pneumococcus pneumonias
following influenza occurred not infrequently at
Camp Pike during the epidemic was shown by bacteriologic
studies made during life and at autopsy in a considerable
series of cases. During the early days of the epidemic of
influenza, secondary streptococcus infection was almost
entirely limited to certain wards which were opened for
the care of the rapidly increasing number of patients
with pneumonia. During this period these wards were
overcrowded, organization was incomplete, and the opportunities
for transfer of infection from patient to patient
85were almost unlimited. The spread of streptococcus
contagion and its fatal effect may be clearly brought out
by comparison of these wards with wards that had long
been organized for the care of patients with pneumonia.
Ward 3 had been in use for the care of patients with
pneumonia for some time prior to the outbreak of influenza.
It was provided with sheet cubicles and conducted by medical
officers, nurses and enlisted men accustomed to the care
of patients with pneumonia, ordinary precautions being
taken against transfer of infection from one patient to another.
The data in Table XVII show the average number
of patients in the ward, the number of new cases of pneumonia
admitted, and the number of deaths among patients
admitted during the corresponding period, for three periods
of ten days each from September 6 to October 5. The
types of infection in fatal cases as determined by cultures
taken at autopsy are also shown.
| Table XVII |
|---|
| |
| Pneumonia in Ward 3 |
|---|
| |
|
AVERAGE NUMBER OF PATIENTS IN WARD |
NUMBER OF PATIENTS ADMITTED |
TOTAL DEATHS AMONG PATIENTS ADMITTED DURING THE CORRESPONDING PERIOD |
CULTURES AT AUTOPSY |
| NUMBER |
PER CENT |
PNEUMOCOCCUS |
S. HEMOLYTICUS |
UNDETERMINED (NO AUTOPSY) |
| Sept. 6–15 |
18.6 |
11 |
3 |
27.2 |
3 |
0 |
0 |
| Sept. 16–25 |
46.1 |
52 |
16 |
30.7 |
13 |
1 |
2 |
| Sept. 26–Oct. 5 |
58.6 |
23 |
8 |
34.7 |
5 |
1 |
2 |
During the period from September 6 to 15, just prior to
the outbreak of influenza in epidemic proportions, the ward
had an average population of 18.6 patients. The total
number of new patients admitted was 11, of whom 3 died,
a mortality of 27.2 per cent. All these cases were pneumococcus
pneumonias as determined by bacteriologic examination
of the sputum at time of admission. The 3 fatal
cases showed pneumococcus infection at autopsy. During
the second period, from September 16 to 25, with the outbreak
86of the epidemic of influenza, the ward rapidly filled
with new cases of pneumonia, attaining an average population
of 46.1 patients. Of the 52 new cases admitted 16
died, a mortality of 30.7 per cent. Again all the cases admitted
during this period in which bacteriologic examination
of the sputum was made, were found to be pneumococcus
pneumonias with one exception. This case, admitted
on September 21 and dying two days later, had a hemolytic
streptococcus pneumonia. Fortunately, though quite by accident,
he was placed in a bed at one end of the porch and
no transmission of streptococcus infection to other cases
in the ward took place. At autopsy 13 cases showed pneumococcus
infection; the foregoing case, hemolytic streptococcus.
During the third period from September 26 to
October 5 the ward became even more crowded, having an
average of 58.6 patients; 23 new cases were admitted, 8 of
whom died, a mortality of 34.7 per cent. Autopsy showed
that 5 of these were pneumococcus pneumonias and 1 was
caused by hemolytic streptococcus infection. It is noteworthy
that the death rate from pneumonia gradually increased
as the ward became more and more crowded. This
may possibly be attributed in part to the increasing severity
of the pneumonia during the early days of the influenza
epidemic. That it was in part directly due to secondary
contact infection with pneumococcus will be shown when
the transmission of pneumococcus infection is discussed.
In spite of the overcrowding of the ward the introduction
of 2 cases of streptococcus pneumonia did not cause an outbreak
of streptococcus infection. Whether this was due
to precautions taken against the transfer of infection or
was merely a matter of good luck is difficult to say, in view
of the fact that a considerable amount of transfer of pneumococcus
infection from one patient to another did occur.
Ward 8 had long been used for the care of colored patients
with pneumonia. As in Ward 3 cubicles were in use
87and ordinary precautions against the transfer of infection
were used. The data are presented in Table XVIII.
| Table XVIII |
|---|
| |
| Pneumonia in Ward 8 |
|---|
| |
|
AVERAGE NUMBER OF PATIENTS IN WARD |
NUMBER OF PATIENTS ADMITTED |
TOTAL DEATHS AMONG PATIENTS ADMITTED DURING THE CORRESPONDING PERIOD |
CULTURES AT AUTOPSY |
| NUMBER |
PER CENT |
PNEUMOCOCCUS |
S. HEMOLYTICUS |
UNDETERMINED (NO AUTOPSY) |
| Sept. |
|
|
|
|
|
|
|
| 6–20 |
25.5 |
18 |
2 |
11.1 |
2 |
0 |
0 |
| Sept. 21–Oct. 5 |
46.1 |
59 |
20 |
33.9 |
10 |
1 |
9 |
During the period from September 6 to 20, prior to the
outbreak of influenza in epidemic proportions among the
colored troops, the ward had an average population of 25.5
patients; 18 new cases of pneumonia were admitted during
this period, all of whom were pneumococcus pneumonias
as determined by bacteriologic examination of the sputum
at time of admission to the ward. Only 2 died, a mortality
of 11.1 per cent, autopsy cultures showing pneumococcus
in both cases. All these patients were treated on the porch
of the ward while they were acutely sick. During the second
period from September 21 to October 5, when the influenza
epidemic was at its height, the ward rapidly filled
with active cases of pneumonia and became distinctly
crowded. It contained an average of 46.1 patients, but
had actually reached a population of 64 patients at the end
of the period. Of the 59 new cases admitted, 20 died, a
mortality of 33.9 per cent, 10 with pneumococcus pneumonia,
one with hemolytic streptococcus pneumonia. In
9 there was no autopsy. The conditions in Ward 8 were
quite analogous to those in Ward 3. In spite of the overcrowding
during the second period no outbreak of secondary
infection with S. hemolyticus occurred, but secondary
pneumococcus infection did occur as will be shown below.
88In contrast with these two wards are Wards 1 and 2 in
which widespread secondary contact infection with S.
hemolyticus took place. Ward 2 was opened September
26, at the beginning of the period when 20 new wards for
pneumonia were organized. From September 26 to October
1 the cubicle system was not in use, the ward was
crowded, organization was imperfect, and few precautions
were taken to prevent transfer of infection from one patient
to another. On October 2 the cubicle system was
installed and precautions against transfer of infection were
instituted. The data are shown in Table XIX.
| Table XIX |
|---|
| |
| Pneumonia in Ward 2 |
|---|
| |
|
AVERAGE NUMBER OF PATIENTS IN WARD |
NUMBER OF PATIENTS ADMITTED |
TOTAL DEATHS AMONG PATIENTS ADMITTED DURING THE CORRESPONDING PERIOD |
CULTURES AT AUTOPSY |
| NUMBER |
PER CENT |
PNEUMOCOCCUS |
S. HEMOLYTICUS |
UNDETERMINED (NO AUTOPSY) |
| Sept. 26 |
10 |
10 |
40 |
27 |
67.5 |
0 |
23 |
4 |
| Sept. 27 |
27 |
17 |
| Sept. 28 |
40 |
13 |
| Sept. 29 |
51 |
12 |
17 |
6 |
35.3 |
2 |
2 |
2 |
| Sept. 30 |
49 |
1 |
| Oct. 1 |
43 |
4 |
| Oct. 2 |
47 |
6 |
10 |
4 |
40.0 |
2 |
1 |
1 |
| Oct. 3 |
42 |
0 |
| Oct. 4 |
41 |
4 |
During the first three days 40 patients with pneumonia
were admitted to the ward. Of these 40 patients, 27 died,
a mortality of 67.5 per cent. Cultures at autopsy showed
that 23 of these died with hemolytic streptococcus infection,
none of pneumococcus infection. In four there was no autopsy.
To appreciate the full significance of these figures
it must be emphasized that these patients at time of admission
to the ward in no way differed from those admitted
to Ward 3 during the corresponding period and were not
in any sense selected cases. The type of infection in 9 of
these patients had been determined by bacteriologic examination
89of the sputum just prior to or immediately after admission
to the ward before opportunity for secondary contact
infection in this ward had occurred. All 9 were shown
to have pneumococcus pneumonia free from hemolytic streptococci
at that time. All 9 died, 7 with secondary streptococcus
infection as shown by cultures taken at autopsy, 1
with a secondarily acquired Pneumococcus Type III infection—sputum
showed a Pneumococcus Type IV on admission—and
in 1 there was no autopsy. In view of the fact
that bacteriologic examination of the sputum in cases of
pneumonia following influenza had shown that the large
majority of them were due to pneumococcus infection, it is
probable that most of the other cases of pneumonia admitted
to this ward were pneumococcus pneumonias at time
of admission, and that they acquired the streptococcus infection
after admission.
During the next three days 17 new patients were admitted,
of whom 6 died, a mortality of 35.3 per cent. Cultures
at autopsy showed pneumococcus infection in 2, streptococcus
in 2. It is noteworthy that the porch was first put
into use on September 29. Of the 12 patients admitted on
this date, 8 were treated throughout the acute stage of their
illness on the porch. Of these 8 patients but one died, of
a Pneumococcus Type IV infection and none became infected
with S. hemolyticus. From October 4 to October 6,
10 patients were admitted, of whom 4 died. Cultures at
autopsy showed pneumococcus infection in 2, hemolytic
streptococcus in 1.
The widespread prevalence of hemolytic streptococcus
infection in this ward as compared with its almost entire
absence in Wards 3 and 8 is very striking. Cultures made
during life and at autopsy have shewn clearly that it was
due to rapid spread of contagion throughout the ward.
The almost unlimited opportunities for transfer of infection
from patient to patient, during the first six days the ward
was in use, undoubtedly greatly facilitated this spread.
90From the data available it is impossible to state exactly
when and by which patients hemolytic streptococcus infection
was introduced into the ward, but it must have been
very early since the death rate was very high from the beginning,
and the first 23 cases coming to autopsy died with
streptococcus infection.
Ward 1 was opened on September 24. From that date
until October 2 no cubicles were in use and few precautions
were taken against transfer of infection. On October 2
cubicles were installed and ordinary precautions to prevent
transfer of infection were instituted. On October 6 the
ward was closed to further admissions. The data presented
in Table XX are divided into two periods, because
on September 29 and 30, 4 patients with streptococcus pneumonia
were admitted to the ward.
| Table XX |
|---|
| |
| Pneumonia in Ward 1 |
|---|
| |
|
AVERAGE NUMBER OF PATIENTS IN WARD |
NUMBER OF PATIENTS ADMITTED |
TOTAL DEATHS AMONG PATIENTS ADMITTED DURING THE CORRESPONDING PERIOD |
CULTURES AT AUTOPSY |
| NUMBER |
PER CENT |
PNEUMOCOCCUS |
S. HEMOLYTICUS |
UNDETERMINED (NO AUTOPSY) |
| Sept. 24–29 |
35.8 |
34 |
11 |
32.3 |
5 |
3 |
3 |
| Sept. 30–Oct. 5 |
55.3 |
40 |
24 |
60.0 |
6 |
14 |
4 |
During the first period from September 24 to 29 the ward
contained an average of 35.8 patients, being only moderately
crowded; 34 cases of pneumonia were admitted, of
whom 11 died, a mortality of 32.3 per cent. It is noteworthy
that deaths among this group which occurred prior
to September 30 were due to pneumococcus infection with
one exception, a patient entering the ward on September 26
and dying the following day. Of the other 2 patients in
this group who died with hemolytic streptococcus pneumonia,
1 was admitted to the ward on September 25, was
91shown to be free from S. hemolyticus on September 30, and
died on October 12 with a secondarily acquired streptococcus
pneumonia and empyema; the other was admitted on
September 29 with streptococcus pneumonia and died the
following day.
During the second period from September 30 to October
5 the ward contained an average of 55.3 patients, being
very overcrowded; 40 new cases of pneumonia were admitted
of whom 24 died, a mortality of 60 per cent. Cultures
taken at autopsy showed that 6 died of pneumococcus
pneumonia, 14 with hemolytic streptococcus infection. As
in Ward 2, patients admitted to this ward were in no way
selected and were probably, as experience has shown, in
large part pneumococcus pneumonias at time of admission.
The widespread dissemination of hemolytic streptococcus
and its fatal effect following the introduction of the organism
on September 29 and 30 is only too evident.
| Table XXI |
|---|
| |
| Secondary Infection with Pneumococcus Type II |
|---|
| |
| NAME |
BED OCCUPIED |
ADMITTED |
PNEUMOCOCCUSIN SPUTUM ON ADMISSION |
SECONDARY INFECTION |
| DATE |
PNEUMOCOCCUS AT AUTOPSY |
| Pvt. Wolfe |
No. 6 |
Sept. 17 |
IV |
Sept. 23 |
II[51] |
| Pvt. Pullam |
No. 5 |
Sept. 9 |
IV |
Sept. 24 |
II |
| Pvt. Swain |
No. 3 |
Sept. 16 |
II |
|
|
92
Secondary Infection with Pneumococcus in Pneumonia
The foregoing studies have shown that hemolytic streptococcus
infection may spread by contagion throughout an
entire ward with great rapidity. Other observations have
demonstrated that pneumococcus infection may be transmitted
in the same way. Only three instances of this nature
will be cited. The first occurred in Ward 3 (Table XXI).
Between September 6 and 16 no cases of pneumonia caused
by Pneumococcus Type II had been admitted to the ward.
On September 16 Pvt. Swain was admitted to the ward and
placed in Bed 3. Bacteriologic examination of his sputum
showed that his pneumonia was caused by Pneumococcus
Type II. At this time Pvt. Pullam, who had been admitted
to the ward on September 9 with a pneumococcus
Type IV pneumonia, occupied Bed 5 separated from Bed 3
by one intervening bed. He had had his crisis on September
14 and was doing well, his temperature being normal.
On September 24 he developed a second attack of pneumonia
and died on September 30. Cultures at autopsy
showed Pneumococcus Type II in heart’s blood and lung,
Pneumococcus Type II and B. influenzæ in the right bronchus.
Pvt. Wolfe was admitted to the ward with bronchopneumonia
on September 17 and placed in Bed 6 next to
Pvt. Pullam. Pneumococcus Type IV and B. influenzæ
were found in his sputum. His temperature had fallen to
normal by lysis on September 21 and he was doing well.
On September 23 his temperature suddenly rose and he
developed a second attack of pneumonia. Pneumococcus
Type II was isolated by blood culture on this date. He
recovered. In both instances Pneumococcus Type II was
acquired after the admission of a patient with a Pneumococcus
Type II pneumonia, the opportunity for contact infection
having been favored by the association of these
patients in adjoining beds.
| 93 |
| Table XXII |
|---|
| |
| Secondary Infection with Pneumococcus Type II |
|---|
| |
| NAME |
BED OCCUPIED |
ADMITTED |
PNEUMOCOCCUS IN SPUTUM ON ADMISSION |
SECONDARY INFECTION |
| DATE |
PNEUMOCOCCUS AT AUTOPSY |
| Pvt. Smith |
No. 26 |
Sept. 18 |
II |
|
II |
| Pvt. Thompson |
No. 28 |
Sept. 17 |
Atyp. II |
Sept. 21 |
II |
| Pvt. Linehan |
No. 30 |
Sept. 16 |
IV |
Sept. 26 |
II |
The second instance is almost identical and occurred on
the opposite side of Ward 3 at about the same time (Table
XXII). Pvt. Linehan was admitted on September 16 and
placed in Bed 30. Pneumococcus Type IV was found in
his sputum. Pvt. Thompson was admitted the following
day with a Pneumococcus II atypical pneumonia and placed
in Bed 28. The next day Pvt. Smith was admitted and
placed in Bed 26. Pneumococcus Type II was found in
his sputum. On September 19 Pvt. Thompson recovered
by crisis and was doing well. On September 21 he had a
chill, his temperature rose to 104.4° F. and he developed a
second attack of pneumonia. He died on September 29;
cultures at autopsy showing Pneumococcus Type II in
heart’s blood and left pleural cavity, Pneumococcus Type
II and B. influenzæ in bronchus and lung. Pvt. Linehan
had begun to improve on September 24 and his temperature
was falling by lysis. On September 26 he became worse,
developed signs of pericarditis and died on September 30.
Cultures from lungs and bronchus at autopsy showed Pneumococcus
Type II and B. influenzæ. In both instances the
fatal secondary infection with Pneumococcus Type II was
undoubtedly acquired from Pvt. Smith in the nearby bed.
The third instance occurred in Ward 8 (Table XXIII).
Pvts. Lewis and Scott were admitted on September 21 and
were placed in adjoining beds, 50 and 51. Lewis showed
Pneumococcus Type I in his sputum, Scott Pneumococcus
II atypical. The following day Pvts. Pighee, Jones, and
Columbus were admitted and given Beds 48, 49 and 53 respectively.
All showed Pneumococcus II atypical in the
sputum. Pvt. Lewis with Pneumococcus Type I pneumonia
recovered by crisis on September 29. His temperature
remained normal until October 2 when it suddenly
rose to 104.2° F. He developed a second attack of pneumonia
and died on October 8. Cultures at autopsy from
heart’s blood and lung showed Pneumococcus II atypical,
from the bronchus Pneumococcus II atypical and B. influenzæ. It is, of course, impossible to say from which one
of his neighbors Pvt. Lewis acquired his second pneumococcus
infection.
| 94 |
| Table XXIII |
|---|
| |
| Secondary Infection with Pneumococcus II Atypical |
|---|
| |
| NAME |
BED OCCUPIED |
ADMITTED |
PNEUMOCOCCUS IN SPUTUM ON ADMISSION |
SECONDARY INFECTION |
| DATE |
PNEUMOCOCCUS AT AUTOPSY |
| Pvt. Pighee |
No. 48 |
Sept. 22 |
Atyp. II |
|
|
| Pvt. Jones |
No. 49 |
Sept. 22 |
Atyp. II |
|
|
| Pvt. Lewis |
No. 50 |
Sept. 21 |
I |
Oct. 2 |
Atyp. II |
| Pvt. Scott |
No. 51 |
Sept. 21 |
Atyp. II |
|
|
| Pvt. Columbus |
No. 53 |
Sept. 22 |
Atyp. II |
|
|
It is noteworthy that these instances of secondary contact
infection with pneumococci occurred in wards where
every precaution was supposedly taken to prevent transfer
of infection from one patient to another. It is true
however that the wards were greatly overcrowded at the
time. Many other instances of secondary pneumococcus
infection in cases of pneumonia following influenza were
encountered in which it was impossible to trace the source
of infection, many combinations of different types of pneumococcus
being found. There were two instances in which
Pneumococcus Type IV was found in the sputum by inoculation
of white mice shortly after onset of pneumonia,
whereas secondary infection with other types was found
at autopsy, one with Pneumococcus Type II, one with Pneumococcus
Type III. In 2 cases by inoculation of white mice,
two types of pneumococcus were found simultaneously in
the sputum coughed from the lung, in one Pneumococcus
Types III and IV, in the other Pneumococcus Types
I and IV. There were 5 cases in which two types of pneumococcus
were found in cultures at autopsy as shown in
Table XXIV. Combined pneumococcus infections of this
nature are almost never encountered in pneumonia occurring under normal conditions in the absence of epidemic influenza.
| 95 |
| Table XXIV |
|---|
| |
| Mixed Pneumococcus Infections in Pneumonia |
|---|
| |
| NAME |
CULTURES AT AUTOPSY |
| HEART’S BLOOD |
BRONCHUS |
LUNGS |
| Pvt. Gal. |
|
Pn. Type III |
Pn. Type III |
| |
|
B. influenzæ |
Pn. Type IV |
| |
|
Staphylococcus |
B. influenzæ |
| Pvt. Sug. |
Pn. Type III |
Pn. Type III |
Pn. Type III |
| |
|
Pn. Type IV |
Pn. Type IV |
| |
|
B. influenzæ |
B. influenzæ |
| |
|
Staphylococcus |
|
| Pvt. Hig. |
S. hemolyticus |
|
Pn. Type II |
| |
|
|
Pn. Type IV |
| |
|
|
S. hemolyticus |
| |
|
|
Staph. aureus |
| Pvt. Can. |
Pn. Type I |
|
Pn. Type III |
| |
|
|
S. hemolyticus |
| Pvt. Fer. |
Sterile |
Pn. Type IV |
Pn. Type I |
| |
|
B. influenzæ |
Pn. Type IV |
| |
|
Staphylococcus |
B. influenzæ |
The foregoing data show that infection with one type of
pneumococcus may readily be superimposed upon or closely
follow infection with another type. Cases have been cited
in which it was clearly demonstrated that this was due to
contact infection. It is furthermore evident that pneumonia
caused by one type of pneumococcus affords no reliable
immunity against pneumonia caused by another type.
The same conditions that favored the spread of hemolytic
streptococcus infection also favored the transfer of pneumococcus
infection from patient to patient.
Secondary Contact Infection in Influenza
The material so far presented has dealt with contact infection
in cases of pneumonia following influenza. That a
similar contact infection in cases of influenza treated in
crowded hospital wards is responsible in considerable degree
for the development of pneumonia in cases of influenza
seems quite probable. It has already been stated that
this pneumonia was found in large part to be caused by
96infection with types of pneumococcus that are found in the
mouths of normal individuals. It has been fairly definitely
established by Stillman[52] that lobar pneumonia caused by
pneumococcus Types I and II is in all probability due to
contact infection, and definite instances of such infection
by Pneumococcus Type II have been reported above. In
a recent communication Stillman[53] has furthermore shown
that of the various groups of Pneumococcus II atypical
those most frequently associated with pneumonia are
rarely found in normal mouths, while those infrequently
associated with pneumonia are more commonly found.
Whether similar considerations will hold true for pneumococci
of Group IV can only be determined by further
investigation. It has been stated that certain observations
made during the course of this work have suggested that
cases of pneumonia which complicate influenza may be due
to contact rather than to autogenous infection. The data
available are far too limited to establish this fact and it
would require a very extensive study to furnish conclusive
evidence.
Certain general observations have suggested this point
of view. It is well recognized that the incidence of pneumonia
in patients with influenza has been much higher
where overcrowding has existed. It would seem probable
that this has been in large part due to the greater opportunity
for the dissemination of organisms capable of producing
pneumonia and the consequently increased opportunity
for secondary contact infection among patients
treated under such conditions. The not infrequent occurrence
of influenzal pneumonia due to combined infections
of the different types of pneumococci, hemolytic streptococci,
staphylococci, and other bacteria, instances of which
have been cited, is in harmony with this view, especially
since pneumonia under ordinary conditions is rarely found
to be associated with mixed infections of this nature. It
97is true that healthy individuals occasionally carry more
than one type of pneumococcus simultaneously in the
mouth, though this is very infrequent, and autogenous infection
occurring in such individuals might account in
some instances for the mixed pneumococcus infections encountered.
By way of analogy it has been clearly shown
in other studies by the Commission on the relation of hemolytic
streptococcus carriers to the complications of measles,
that secondary infection of the respiratory tract with
S. hemolyticus is in very large part due to contact infection,
the chronic carrier rarely developing complications
due to this organism.
To obtain further light on this question the type of pneumococcus
present in the mouths of 46 consecutive cases of
early uncomplicated influenza was determined by the mouse
inoculation method at time of admission to the receiving
ward of the hospital before the patients had been associated,
with the purpose of determining if cases among this
group which subsequently developed pneumonia might be
shown to have acquired a pneumococcus which they did not
carry at time of admission. This group of patients was
treated in a special ward set apart for the purpose. The
patients were assigned to beds in rotation and confined in
bed until thoroughly convalescent. Beds were well separated
and cubicles, masks and gowns were in use. Cultures
were made from the ward personnel. By these procedures
an accurate record was kept of all sources of pneumococcus
infection. The types of pneumococcus found in the mouths
of these patients at time of admission are shown in Table
XXV.
| 98 |
| Table XXV |
|---|
| |
| Types of Pneumococci in the Mouths of Influenza Patients |
|---|
| |
| PNEUMOCOCCUS |
NUMBER |
PER CENT |
| Pneumococcus, Type I |
0 |
0 |
| Pneumococcus, Type II |
0 |
0 |
| Pneumococcus, II atypical |
1 |
2.2 |
| Pneumococcus, Type III |
0 |
0 |
| Pneumococcus, Group IV |
25 |
54.3 |
| No pneumococci found |
20 |
43.5 |
Only 1 patient in this group developed pneumonia. At
time of admission he had no pneumococcus in his mouth as
determined by inoculation of a white mouse with his sputum.
Examination of the sputum by the same method at
time of onset of pneumonia three days after admission
showed Pneumococcus Type III. The only ascertainable
source of infection in this case was one of the ward attendants
who carried Pneumococcus Type III in his throat in
sufficiently large numbers to be demonstrable by direct culture
and who frequently came in contact with the patient.
In this instance the development of pneumonia was probably
due to contact infection. An extensive study of this
nature would be necessary to determine in what proportion
of cases pneumonia following influenza is caused by secondary
contact infection and in what proportion to autogenous
infection. It is at least evident that contact infection with a
type of pneumococcus found in the mouth of normal individuals
may occur in influenza and be responsible for the
development of pneumonia. Therefore every precaution
should be taken to prevent it.
Methods for the Prevention of Secondary Contact Infection in Influenza and Pneumonia
The methods at present in vogue for preventing the
spread of contagion in wards devoted to the care of patients
with influenza and pneumonia may be briefly enumerated:
The separation of patients by means of sheet or screen
cubicles, the wearing of masks and gowns by the ward personnel
and to some extent by convalescent patients who are
up and about the ward, and in some hospitals the separation
of streptococcus carriers from noncarriers as determined
by throat culture at time of admission. That these
methods are of some value in preventing spread of infection
cannot be denied, and it is probable that they are fairly
99effective under ordinary conditions when conscientiously
carried out. That they inevitably break down in the presence
of an overwhelming epidemic when hospital wards
become overcrowded is only too evident. Under such conditions
the sheets hung between the beds are constantly being
displaced and are slight proof against a patient’s curiosity
as to the identity and condition of the man in the adjoining
bed; masks cannot be worn by patients seriously
ill with pneumonia, during the very time when they are
most dangerous and in greatest danger and those worn by
the ward personnel are very rarely sufficiently well made
to prevent spread of contagion by droplet infection as the
studies of Haller and Colwell[54] and Doust and Lyon[55] have
shown; the separation of streptococcus carriers from noncarriers
as at present carried out cannot keep pace with the
ever increasing influx of patients nor with the rapidity of
the spread of the hemolytic streptococcus, in part because
of the time required to make the bacteriologic diagnosis, in
part because the amount of work involved cannot be accomplished
by the laboratory personnel available. That this is
so will be shown in data presented below. Not only do
these methods break down in the face of an epidemic, but
they often provide a false sense of security.
In searching for a solution of the problem it is essential
to have the following considerations clearly in mind. Every
patient with influenza must be considered a potential
source of pneumococcus or hemolytic streptococcus infection
for his neighbor until he is proved otherwise by bacteriologic
examination. Every person engaged in the care
of patients with respiratory diseases must also be regarded
as a potential source of danger. Pneumonia cannot be regarded
as one disease but must be looked upon as a group
of different diseases, with more or less similar physical
signs and symptoms, it is true, but caused by a considerable
variety of bacteria, infection with any one of which not
100only provides no protection against infection with another,
but may even render the individual more susceptible to
secondary infection. Therefore, every patient with pneumonia
must be regarded as an actual source of danger to
his neighbor, at least until it is established that he has the
same type of infection. All these considerations are especially
true in the presence of influenza, for it has become
evident that many organisms readily gain access to the
lung and produce pneumonia in patients with influenza
which under ordinary circumstances fail to cause disease
of the respiratory organs.
Since secondary infection in respiratory disease is undoubtedly
spread in large part by droplet and contact infection,
the prevention of secondary infection must depend
upon the elimination of these methods of transmission.
Three solutions present themselves: (1) Ward treatment
with absolute elimination of overcrowding and much wider
separation of patients than has hitherto been deemed necessary;
(2) segregation of patients according to type of
bacterial infection; (3) effective individual isolation of
every patient.
It has been clearly shown that treatment of influenza and
pneumonia in overcrowded wards even with the use of such
precautions to prevent transfer of infection as cubicles,
masking of attendants and patients, etc., is attended by serious
danger of contact infection and that such infection
will almost inevitably occur. This is not at all surprising
when it is remembered that we are treating in the same
ward, in the case of pneumonia, a group of what are in reality
entirely different diseases, all of which may be transmitted
from one patient to another, and in the case of influenza
a group of individuals who carry a variety of
potentially pathogenic bacteria. No one would expect to
treat cases of scarlet fever, measles, and diphtheria together
in a hospital ward without having contact infection
result. Among patients ill with influenza and postinfluenzal
101pneumonia, certainly streptococcus pneumonia and
to some extent pneumococcus pneumonia may be transmitted
quite as readily as any of these diseases. In view of
these considerations it must be apparent if ward treatment
of these diseases is to be continued without respect to type
of bacterial infection, not only that overcrowding is absolutely
contraindicated but also that much wider separation
of patients than has hitherto been regarded as necessary
is imperative. Furthermore, beds should be separated by
permanent cubicles that cannot readily be displaced. Patients
should be confined to their cubicles until thoroughly
convalescent and when up and about should not be allowed
to enter cubicles occupied by patients still sick. Medical
officers, nurses and attendants who come into contact with
the patients should use the same rigid precautions that are
used in the care of patients with typhoid or erysipelas or
meningitis with the additional use of means to prevent
droplet infection of the patients, always bearing in mind
that the respiratory tract in patients with influenza or
postinfluenzal pneumonia is as susceptible to secondary
infection as the postpartum uterus or an open surgical
wound. In other words, the most rigid aseptic technic
should be maintained. The recognition of a case of streptococcus
pneumonia in a ward should be an indication for
immediate quarantine of the ward until it has been shown
by bacteriologic examination that there is no longer danger
of spread of streptococcus contagion. This is done in the
case of meningitis or diphtheria, neither of which diseases
is comparable with streptococcus pneumonia in rapidity
of spread or in resulting fatality.
Segregation of patients in wards according to type of
bacterial infection while theoretically an improvement over
the indiscriminate mixing of patients with many different
types of infection presents many practical difficulties which
make it impossible to carry out in the presence of an overwhelming
epidemic. It is quite obvious that grouping of
102influenzal patients on the basis of the types of pneumococci
that they carry in their mouths is impossible since the great
majority of mouth pneumococci belong to Group IV and
comprise a heterologous immunologic group. The separation
of influenza patients who carry S. hemolyticus from
those who do not would appear to offer a more hopeful field.
Since we cannot make an immediate distinction between
streptococcus carriers and noncarriers by inspection of the
patient, this procedure requires the taking of throat cultures
at time of admission to the hospital, the holding of
patients for eighteen to twenty-four hours in receiving
wards until the bacteriologic diagnosis has been made, and
their subsequent distribution to streptococcus and nonstreptococcus
wards. This is feasible when the admission
rate is low and the number of streptococcus carriers found
at time of admission is small. In the presence of an influenza
epidemic it immediately becomes impossible to carry
out in base hospitals as now constituted, since the demand
for beds under such conditions at once converts a large
part of the hospital into a group of receiving wards with
little room remaining for subsequent separation of patients.
The amount of bacteriologic work involved at once becomes
prohibitive and the time required to make the bacteriologic
diagnosis defeats its purpose since it allows the
spread of hemolytic streptococcus to occur in the receiving
wards during the interval.
The foregoing statements are based on results obtained
in an attempt to separate streptococcus carriers from noncarriers
in a limited group of cases of influenza at Camp
Pike, the investigation being conducted during a secondary
wave of influenza between November 27 and December 5. A
special group of five wards consisting of one receiving
ward and four distributing wards were set aside for the
study. Cubicles, masks and gowns were in use and the
wards were not crowded. The personnel on these wards did
not carry S. hemolyticus in their throats. Patients entering
103the receiving ward were assigned to beds in rotation.
Throat cultures were made on blood agar plates at time of
admission. The plates were examined promptly the next
morning, the diagnosis of S. hemolyticus being made by the
characteristic hemolytic colonies and microscopic examination
of stained smears. By this method a report reached
the receiving ward at 9:30 a.m. and patients were promptly
evacuated to the streptococcus and nonstreptococcus wards,
where they were again assigned to beds in rotation, remaining
confined in bed until convalescent. Confirmation
of all strains of hemolytic streptococcus was subsequently
carried out by isolation in pure culture, bile solubility test,
and hemolytic test with washed sheep corpuscles. All cases
free from hemolytic streptococci at time of admission who
were sent to the “clean” wards were recultured daily
throughout the period of study, those acquiring a hemolytic
streptococcus being transferred to a streptococcus
ward as soon as the bacteriologic diagnosis was made.
The results are shown in Table XXVI.
| Table XXVI |
|---|
| |
| S. Hemolyticus in Cases of Influenza |
|---|
| |
| DATE |
PATIENTS ADMITTED TO RECEIVING WARD |
THROAT CULTURES ON ADMISSION. S. HEMOLYTICUS: |
“CLEAN” CASES ACQUIRING S. HEMOLYTICUS IN THE HOSPITAL |
| + |
− |
WHILE IN REC. WARD |
WHILE IN “CLEAN” WARD |
TOTAL |
| Nov. 27 |
12 |
4 |
8 |
0 |
2 |
2 |
| Nov. 28 |
8 |
2 |
6 |
0 |
1 |
1 |
| Nov. 29 |
17[56] |
8 |
9 |
1 |
2 |
3 |
| Nov. 30 |
11 |
2 |
9 |
3 |
0 |
3 |
| Dec. 1 |
10 |
5 |
5 |
0 |
0 |
0 |
| Dec. 2 |
37 |
16 |
21 |
1 |
1 |
2 |
| Dec. 3 |
21 |
8 |
13 |
0 |
2 |
2 |
| Dec. 4 |
32[56] |
11 |
21 |
4 |
2 |
6 |
| Dec. 5 |
17 |
10 |
7 |
5 |
0 |
5 |
| Totals |
165 |
66 |
99 |
14 |
10 |
24 |
One hundred and sixty-five cases were admitted to the
receiving ward during the period of study as cases of influenza.
104Of these, 137 had influenza; 4 of those with influenza
had pneumonia at time of admission, 23 had acute follicular
tonsillitis, 3 epidemic cerebrospinal meningitis, 1 scarlet
fever, and 1 Vincent’s angina. Sixty-six cases (40 per cent)
showed hemolytic streptococcus in the throat at time of
admission and were sent to the streptococcus wards; 99
cases (60 per cent) were negative for hemolytic streptococcus
on admission, and of these 91 were sent to the “clean”
influenza wards. Twenty-four of these clean cases subsequently
became positive for S. hemolyticus. It is especially
noteworthy that 14 of them acquired a hemolytic streptococcus
during the short period that they were held in the
receiving ward awaiting the report of the culture taken at
time of admission, the first culture taken shortly after admission
to the “clean” wards being positive. This result
was undoubtedly due to the fact that these cases were unavoidably
associated in the receiving ward with many carriers
of hemolytic streptococcus. It is evident that cases
which were supposedly free from streptococci but which in
reality had picked up the organism in the receiving ward
were constantly being sent to the “clean” wards. It is
furthermore evident that if the precaution had not been
taken of reculturing all clean cases on day of admission
to the “clean” wards and daily thereafter these wards
would soon have become saturated with hemolytic streptococci.
Even under these conditions, 10 cases, after varying
periods in the “clean” wards, acquired the organism in
their throats. When it is stated that it required the full
time of two men under very special conditions to carry out
this work in a very limited number of cases and that it
failed to keep “clean” wards free from hemolytic streptococci,
it is only too apparent that the efficient separation of
carriers from noncarriers in the presence of an epidemic of
influenza is an impossible task.
The segregation of pneumococcus pneumonias following
influenza according to type of infection is obviously impossible,
105since they are caused by an almost unlimited variety
of immunologic types as far as present knowledge goes.
Even the efficient separation of streptococcus pneumonias
from pneumococcus pneumonias would require a considerable
team of workers and the closest cooperation between
laboratory and ward staffs, so that no case of pneumonia
would be sent to a pneumonia ward until the bacteriologic
diagnosis had been made. In our experience this is
rarely considered feasible even under ordinary conditions,
and in the presence of an epidemic is nearly impossible because
of the volume of work involved and the delay necessitated
by bacteriologic methods. It is, nevertheless, absolutely
essential if highly fatal ward epidemics of streptococcus
pneumonia are to be prevented.
In view of the considerations discussed above, it is believed
that the clear and most fundamental indication for
the management of epidemic respiratory diseases in the
army is to scatter patients as widely as possible instead of
following the time-honored custom of concentrating them.
In brief, abandon open ward treatment and adopt effective
individual isolation of every case, maintaining as strict a
quarantine as is demanded in other highly contagious and
infectious diseases. The adoption of a strict aseptic technic
in the handling of these patients is an evident corollary.
Only by this means can the serious and highly fatal secondary
hospital infections, which occur in influenza and pneumonia
when these diseases are present in epidemic form,
be prevented.
The prevention of secondary infection, prior to admission
to the hospital, is another and more difficult problem.
That opportunity for secondary contact infection in cases
of influenza before patients reach the hospital is great
seems unquestionable, since many cases have already developed
these infections at time of admission. During the
epidemic patients were crowded in regimental infirmaries,
in ambulances, and in the receiving office of the hospital
106with every opportunity for droplet infection present. No
study has been made of this question, but it seems reasonable
that the same methods of prevention should apply,
namely, effective separation of patients.
It is not within the scope of this paper to discuss details
of method, but anything that is possible becomes feasible
as soon as sufficient evidence can be brought to bear that
it is a necessity. In the present instance it would seem that
any means that can be used to reduce materially the terrific
toll taken by respiratory diseases is an absolute necessity.
Summary
1. Secondary contact infection with pneumococci not infrequently
occurs in patients with pneumonia following influenza
when they are treated in hospital wards.
2. Secondary contact infection with S. hemolyticus readily
occurs in patients with pneumonia and may spread
rapidly throughout an entire ward with highly fatal results.
3. Secondary contact infection may be responsible for
the development of pneumonia in patients with influenza.
4. Ward treatment of these diseases is fraught with serious
danger which is greatly increased by overcrowding,
by imperfect separation of patients by cubicles, and by
imperfect aseptic technic of medical officers, nurses, and
attendants.
5. It is probable that secondary contact infection can be
effectively prevented only by individual isolation and strict
quarantine of every patient.
107
CHAPTER IV
THE PATHOLOGY AND BACTERIOLOGY OF PNEUMONIA FOLLOWING INFLUENZA
E. L. Opie, M.D.; F. G. Blake, M.D.; and T.M. Rivers, M.D.
Many observers have described isolated phases of the
recent epidemic and of past epidemics of influenza. Few
have had an opportunity to follow the pathology of influenza
from the onset of an epidemic through a period of several
months and to observe the succession of acute and
chronic changes which occur in the lungs. Our commission
arrived on September 5, 1918, at Camp Pike two weeks before
the outbreak of influenza. The commission had previously
made a careful study of the clinical course, the bacteriology
and to a limited extent the pathology of pneumonia
occurring at Camp Funston where there was little
if any influenza. Study of the records preserved at the
base hospital at Camp Funston had convinced us that this
camp had passed through an epidemic of influenza during
the spring of 1918, this epidemic being followed by
a very severe outbreak of pneumonia. Our investigation
at Camp Funston had brought to our attention those
phases of pneumonia which with the facilities of a base
hospital laboratory could be most profitably studied with a
view to determining the causation, the epidemiology and
the prevention of the pneumonias prevalent in the American
army.
Study of pneumonia after death offers the only opportunity
of determining the relation of pulmonary lesions
to the considerable variety of microorganism associated
with them. Clinical diagnosis furnishes no certain criterion
for distinguishing lobar and bronchopneumonia; suppurative
108pneumonia is rarely recognizable during life.
The relation of pneumococci, streptococci, staphylococci or
B. influenzæ to one or other type of pneumonia can be determined
with accuracy only after death; for the demonstration
of one or more of these microorganisms in material
obtained from the upper respiratory passages in life,
though of value, furnishes us no definite evidence that the
organism which has been identified has entered the lung
and passed from the bronchi to produce pneumonia.
Study of autopsies following examination of the sputum
during life has shown that an individual primarily attacked
by influenza may suffer with a succession of pneumonias,
one microorganism having prepared the way for another.
The complexity of the subject is much increased by the
truth that pyogenic microorganisms, like the tubercle
bacilli, are capable of producing a considerable variety of
pulmonary lesions.
Examination of the lungs of a large number of individuals
who have died as the result of pneumonia following influenza
has disclosed a succession of acute and chronic diseases.
Immediately succeeding the height of the epidemic
of influenza, death occurred with acute lobar pneumonia
or with diffusely distributed hemorrhagic bronchopneumonia
caused in the majority of instances by Pneumococcus
IV in association with B. influenzæ. Superimposed infection
with hemolytic streptococci increased in frequency and
in individuals who had occupied certain wards was almost
invariable. At a later period, from one to two months following
the maximum incidence of influenza chronic lesions,
namely, bronchiectasis, unresolved pneumonia, and chronic
empyema were common and often occurred as the result
of influenza which had had its onset at the height of the epidemic.
When influenza attacked the encampment, about 50,000
troops were quartered in it, and for a considerable period
no more troops were brought into the camp and none left
109it. All cases of pneumonia occurring among these troops
were brought to the base hospital so that the autopsies
which were studied were representative of all the pneumonias
following influenza in this limited group of men.
It is noteworthy that autopsy disclosed no instance of fatal
influenza unaccompanied by pneumonia.
Pneumonia of Influenza.—Knowledge concerning the bacteriology
of the pneumonia of influenza dates from the
study of the epidemic of 1889–90. The frequency with
which Diplococcus lanceolatus occurred in association with
influenzal pneumonia was well recognized, although several
observers, notably Finkler[57] and Ribbert,[58] found Streptococcus
pyogenes so often that they attributed the pneumonia
of influenza to this microorganism.
During a subsidiary outbreak of influenza occurring in
1891–92 Pfeiffer[59] discovered the microorganism which he
believed was the cause of the disease. Pneumonia, he believed,
was caused by the invasion of this microorganism
into the lung, and the pneumonia of influenza, if death occurred
at the height of the disease, was characterized not
only by the presence of the bacillus of influenza, but was
recognizable by its anatomic peculiarities. He described
lobular patches of consolidation which were separated from
one another by air containing tissue or were confluent, so
that, although the lobular character was still recognizable,
whole lobes might be affected. The consolidated tissue
was dark red and within each lobular area were small, yellowish
gray spots varying in size from that of a pinhead to
a pea. In the mucus of the larynx and trachea were numerous
microorganisms, including diplococci and streptococci,
among which influenza bacilli were predominant; in
the larger bronchi, bacteria other than influenza bacilli
were less abundant, whereas in the finer bronchi filled with
110purulent fluid and in the lung tissue influenza bacilli had
undivided sway. Pfeiffer stated that the changes described
were found when death occurred at the height of
the disease, whereas other pulmonary lesions might be
sequelæ of this typical influenzal pneumonia.
Observations upon the pathology of influenzal pneumonia
made during the epidemic of 1889–92 have been collected
in the monograph of Leichtenstern[60] published in 1896. He
combats the opinion held by some observers that pneumonia
with influenza is always catarrhal and cites many writers
to prove that lobar pneumonia not infrequently accompanies
the disease. Indeed, some have found “croupous”
pneumonia more often than “catarrhal.” Krannhals[61]
at Riga found typical fibrinous pneumonia in 53 instances,
doubtful forms in 22 and bronchopneumonia in 37. Cruickshank[62]
in England found croupous forms predominant.
Among 43 autopsies performed upon individuals dead with
influenza Birch-Hirschfeld[63] found 11 instances of croupous
lobar pneumonia, 8 instances of croupous lobular pneumonia
and 24 instances of catarrhal pneumonia. Leichtenstern
thinks that the atypical symptomatology of lobar
pneumonia with influenza—for example, the purulent character
of the sputum—has led many physicians to believe
that lobar pneumonia rarely occurs. It is equally true that
many instances of confluent lobular pneumonia are mistaken
for lobar.
There appears to be no comprehensive description of the
pneumonias of influenza based upon the epidemics of 1889–92.
Descriptions dating from this period are much obscured
by attempts to separate croupous or fibrinous from
catarrhal pneumonias. Croupous lobular pneumonia has
been recognized, for example, by Birch-Hirschfeld. Leichtenstern
describes a form of pneumonia which he regards as
111neither lobar nor lobular although it implicates whole
lobes; the consolidated tissue is homogeneous and varies
in color from fleshy red to bluish red; it is tough and elastic
in consistency. The author thinks that it is an error to
regard this lesion as a confluent lobular pneumonia.
Kuskow[64], who has discussed the pathology of influenza
in considerable detail, has seldom seen lobar pneumonia but
has almost invariably found, even when there is lobar distribution
of the lesion, lobular patches of consolidation involving
groups of lobules, single lobules or only parts of
lobules; the lung tissue has been hyperemic and in places
edematous.
Opinions concerning the pathology and bacteriology of
the pneumonias of influenza, published since the recent
epidemic, have varied almost as much as those just cited.
Few observers have had the opportunity of making a considerable
number of observations under conditions which
determine the relation of the pulmonary lesions to the primary
disease.
Keegan[65] has found with influenza a massive and confluent
bronchopneumonia, frequently resembling lobar pneumonia
but distinguishable particularly in its early stages
when the cut section of the consolidated lung has a finely
granular character and each bronchiole stands out as a
grayish area with intervening dark red alveolar tissue.
Symmers[66] states that the pneumonia of influenza is a
confluent lobular exudative and hemorrhagic pneumonia
which bears a close resemblance to the pneumonic variety
of bubonic plague.
Our commission[67] published a preliminary report on
pneumonia following influenza observed at Camp Pike.
The occurrence of purulent bronchitis, distention of lungs,
112peribronchial hemorrhage and bronchiectasis were described.
B. influenzæ was isolated from the bronchi in approximately
85 per cent of instances of influenzal pneumonia
but from the consolidated lung in less than half this
number of autopsies. Lobar pneumonia was present in a
large proportion of autopsies but was less frequent than
bronchopneumonia. Bronchopneumonic consolidation is in
part red, lobular and confluent, in part nodular; pneumococci
have a predominant part in the production of these
lesions. Three types of suppurative pneumonia are described:
(a) Abscess caused by hemolytic streptococci
usually in contact with the pleura and accompanied by empyema;
(b) Suppuration of interstitial tissue of the lung
caused by hemolytic streptococci and accompanied by empyema;
(c) multiple foci of suppuration clustered about a
bronchus of medium size and caused by staphylococci. We
have expressed the opinion that B. influenzæ descends into
the bronchi; pneumococci, usually Type IV, may enter the
lung and produce either lobar or bronchopneumonia.
Hemolytic streptococci may descend and infect the pneumonic
lung causing death often before suppuration has occurred.
Epidemics of such superimposed streptococcus
pneumonia in wards of the hospital were described.
LeCount[68] says: “The pneumonia of influenza is commonly
referred to as bronchopneumonia. It may be so designated,
but it differs from other bronchopneumonias in its
predilection for the periphery of the lungs and in the extent
to which the inflammation is hemorrhagic.”
MacCallum[69] states that the following types of pneumonia
following influenza may be recognized. 1. Pneumococcus
pneumonia. The lobular character of the consolidation is
in these cases well marked, although it tends to lose its
definiteness through the confluence of adjacent areas. The
cut surface of the lung shows in the more acute cases a
113peculiar lobular or confluent consolidation which corresponds
well with what is commonly written of the stage
of engorgement in the description of lobar pneumonia.
Later stages in the pneumonia show within these areas
patches of rough gray consolidated tissue from which definite
plugs of exudate project. 2. Staphylococcal pneumonia.
3. Streptococcal pneumonia. There is lobular pneumonia,
the interlobular septa are edematous and, microscopically,
bronchi and alveoli are loaded with streptococci.
Whole areas of lung, though retaining their form, are entirely
necrotic. Lymphatics are distended with exudate
containing streptococci in great numbers, but in none of
these cases is interstitial bronchopneumonia found. 4.
Pneumonia produced by B. influenzæ of Pfeiffer. The lung
is studded with palpable shot-like grayish yellow nodules;
the bronchi exude thick yellow pus, which contains influenza
bacilli. Microscopically, the walls of the bronchi
are found to be thickened by mononuclear infiltration and
new formation of connective tissue. The walls of the alveoli
are thickened and indurated and the alveoli often contain
fibrin in process of organization. Absence of conspicuous
changes in lymphatics, absence of intense pleural infection
and relatively scant numbers of polynuclear leucocytes
in the exudate within the alveoli and bronchial walls
are, MacCallum states, all that distinguish this pulmonary
change from the interstitial bronchopneumonia caused by
the hemolytic streptococcus and described by him in
previous papers.
Lyon[70] designates the pulmonary lesion following influenza,
hemorrhagic pneumonitis, the lung tissue containing
serous fluid loaded with red blood corpuscles; in
many instances there was such scant consolidation that the
process could not be regarded as a true pneumonia. In 35
instances the lesion was lobular in distribution and in 16
114instances was sufficiently extensive to be designated lobar,
but it was not typical lobar pneumonia, and, often associated
with lobular patches of consolidation, appeared to be
a confluent lobular pneumonia.
Goodpasture and Burnett[71] say: “The difficulties of analyzing
the pulmonary lesions in any group of influenza
pneumonias as they have appeared in this epidemic, are
very apparent to anyone who has had an opportunity to observe
the bacteriology and pathology of this accompaniment
of the disease.” There is an acute outflow of the
fluid elements of the blood and of hemorrhage into the lung
tissue filling the alveoli in lobular areas and not infrequently
in an entire lobe. By a special method of staining
these authors have studied the distribution of Gram-negative
bacilli with the morphology of B. influenzæ. The fact
that in certain very early cases demonstrable bacteria of
any kind are scarce or not found at all, has lead them to
believe “notwithstanding the demonstration of influenza
bacilli in pure culture in the lung in all but one instance,
that at this stage organisms are comparatively few within
the alveoli, and the primary injury is due to a very potent
toxic agent elaborated in and disseminated through the
larger air passages. In the later stages or from the beginning,
if the injury be slight, the infection focalizes about
the bronchi or their terminations, so that the bronchial and
lobular distribution becomes very conspicuous.” Typical
lobar pneumonia with “croupous” exudate within the alveoli
occurs in cases complicated by secondary pneumococcus
infection.
Wolbach[72] has found that two types of pneumonia are
characteristic of influenza. In cases in which death has
occurred within a few days after onset of pulmonary signs,
the lung tissue is dark red and “meaty in consistency” and
contains abundant blood-tinged serous fluid which drips
115from the cut surface. The other type of lesion is found in
patients who have lived for ten days or more after onset
of the disease; there is extensive bronchitis, bronchopneumonia,
discrete or confluent, and peribronchitis. The lungs
are voluminous and the smaller bronchi are distended.
Microscopically, there is peribronchitis with extensive infiltration
of the interlobular septa and organization in alveoli
and bronchioles. This lesion is that designated by
MacCallum as “interstitial bronchopneumonia.” Wolbach
thinks that the two types of lesion represent different
stages of the same process. He regards as distinctive of
the pneumonias of influenza the presence of hyalin fibrin
lining distended air spaces. With the two types of lesion
which have been described, B. influenzæ was the only organism
which could be cultivated, and the author associates
these distinctive conditions with that microorganism.
Streptococcus Pneumonia.—Finkler emphasized the importance
of streptococcus pneumonia as a complication of
influenza. In 1888 he described instances of acute primary
streptococcus pneumonia observed in 1887 and 1889. This
form of pneumonia, Finkler thought, occurred in Bonn in
epidemic form before the influenza epidemic of 1889–90
and, he states, exhibited an astonishing similarity to the
pneumonia of influenza. He thought that later there was
in Bonn a mixed infection of influenza and primary streptococcus
pneumonia. In one type of streptococcus pneumonia,
described by Finkler, there was lobular consolidation
which in multiple patches produced “pseudolobar” consolidation;
the consolidated lung was smooth and red, and
similar to spleen, rather than hepatized. In another group
of instances the lesion merited the name “erysipelas of
the lung.” The lesion was an acute interstitial pneumonia
in some places, a cellular or occasionally fibrinous pneumonia
with involvement of the interstitial tissue in other
places. There was edematous swelling and accumulation of
leucocytes in the interstices between the alveoli and about
116the blood vessels and bronchi. Finkler stated that the similarity
to erysipelas might suggest that the lymphatics contain
streptococci, but this relation did not exist although
large lymphatic channels were occasionally filled with coagulum.
He asserted that the disease was contagious and
cited cases which he believed had their origin in hospital
wards.
The widespread occurrence of streptococcus pneumonia
in the army camps in this country attracted attention during
the first months of 1918. Cummings, Spruit and
Lynch[73] at Fort Sam Houston, Texas, recognized the prevalence
of streptococcus pneumonia, both as a complication
of measles and in association with lobar pneumonia, and
showed that the microorganism concerned was a hemolytic
streptococcus. In 7 autopsies upon individuals with lobar
pneumonia, they found pneumococcus alone in 2 instances
and pneumococcus and hemolytic streptococcus or hemolytic
streptococcus alone in 5 instances. Hemolytic streptococcus
was found in all of 24 instances of bronchopneumonia,
three-fourths of which followed measles. They recommend
the bacteriologic examination of the throat of
patients with measles and the segregation of those who
harbor hemolytic streptococci.
Cole and MacCallum[74] have published almost simultaneously,
with that just cited, a report upon the pneumonia
which has occurred at Fort Sam Houston and have shown
the importance of hemolytic streptococci in its causation.
They have found two varieties of pneumonia, namely, acute
lobar pneumonia which does not differ essentially from
that which occurs elsewhere and bronchopneumonia which
in most cases has followed measles and is caused by S. hemolyticus.
They think this infection is usually acquired in
the hospital. They believe that the pulmonary lesions are
characteristic. In this publication and elsewhere MacCallum
117has designated the lesion “interstitial bronchopneumonia.”
The epidemic of streptococcus pneumonia and empyema
occurring at Camp Dodge, Iowa, from March 20 to May 10
is described by Miller and Lusk[75]. During this period there
were 400 cases of pneumonia, whereas from September 20,
1917, to March 20 there had been only 276 instances of lobar
pneumonia. The type of pneumonia changed, there was
more severe intoxication and empyema became very frequent;
in 85 of 95 exudates streptococci were found. The
outbreak of pneumonia bore no relation to measles. The
authors state that a mild tracheitis was prevalent in the
cantonment during March, and whenever a large group of
soldiers congregated coughing was noticeable.
MacCallum[76] studied the pneumonia at Camp Dodge during
May and found 17 instances of the lesion which he had
designated interstitial bronchopneumonia; of these, 9 followed
measles, although in the earlier part of the epidemic
there appear to have been, he states, few such cases. Cultures
made at autopsy, except in a few fatal cases of uncomplicated
lobar pneumonia caused by the pneumococcus,
showed the hemolytic streptococcus in every situation
throughout the respiratory tract and pleura.
The pneumonia which occurred at Camp Funston is of
special interest to our commission because we were for a
time stationed at this camp and had the opportunity of
following in the excellent records of the hospital the history
of the occurrence of pneumonia during the year following
the establishment of the camp in September, 1917. Stone,
Phillips and Bliss[77] have described the outbreak of pneumonia
which occurred in March, 1918. At this time there
was, the authors state, severe pneumonia with frequent
empyemas due to hemolytic streptococci. This condition
118which did not follow measles was responsible for the
greatly increased death rate in March; 9 deaths occurred
in February, 45 in March, 25 in April and 14 in May. They
found during March 26 instances of multiple pulmonary
abscess. In 29 autopsies they found a pleural lesion which
they designate “subcostosternal pus pockets”; it occurs
only in association with empyema caused by hemolytic
streptococci.
Our commission[78] has shown that an epidemic of influenza,
well characterized by its epidemiology and symptoms,
preceded and accompanied the outbreak of pneumonia
just described. Between March 4 and 29 1,127 men
from Camp Funston, which then contained 29,000 men, were
sent to the base hospital with influenza and many more
were treated in the infirmaries of the camp; on March 11
107 patients with influenza were admitted to the hospital.
The greatest incidence of pneumonia in the history of the
encampment up to this time occurred between March 9 and
29, immediately following the outbreak of influenza, the
maximum incidence of pneumonia occurring five days after
the maximum for influenza.
The foregoing observations are cited to prove that streptococcus
pneumonia, which occurred during the spring of
1918 at Camp Funston and doubtless at other camps, had
its origin in influenza and did not differ in character from
that which occurred on a much larger scale in the fall of
1918.
Table of Autopsies.—In order to present as briefly as
possible the data upon which the present study has been
based, autopsies have been assembled in tabular form in
the order of their performance (Table XXVII). During the
early period of the epidemic autopsies were performed on
all who died with pneumonia, but later, with increase in the
number of deaths, this became impossible and autopsies
were performed on all those who died in certain wards.
119Comparison of charts representing incidence of influenza
and of deaths from pneumonia furnishes evidence that fatal
pneumonia during the period of investigation was with
few exceptions referable to influenza. During two weeks,
namely, from September 1 to 14, before the presence of the
epidemic was evident, there were only 2 fatal cases of
pneumonia. In most instances the relation of pneumonia
to influenza is established by a definite history of influenza
having its onset during the epidemic. Bronchopneumonia
usually develops gradually as a sequence of influenza in
which purulent bronchitis has occurred. Lobar pneumonia
may develop in cases of influenza complicated by purulent
bronchitis. In some instances there is apparent recovery
from influenza indicated by return of temperature to normal;
after from one to three days of normal temperature
there is typical lobar pneumonia with rusty sputum. In
many instances of pneumonia having their onset at the
height of the epidemic of influenza, the history indicates
that pneumonia was present immediately after the onset
of symptoms, so that the onset resembled that of pneumonia
rather than of influenza.
Cases of pneumonia following measles have been excluded
from the table in order that they may be studied
separately and compared with the pneumonias of influenza.
It is noteworthy that the lesions of pneumonia following
measles have shown a very close resemblance to the pneumonias
of influenza, with regard both to pathologic characters
and to bacteriology.
Five instances of pneumonia following typhoid fever
(Autopsies 245 and 329), scarlet fever (Autopsy 311) or
mumps (Autopsies 403 and 417) have been excluded from
the table. These secondary pneumonias are grouped as
an appendix to the section on pneumonia following measles.
It is not improbable that individuals with the diseases
named are just as susceptible as others to influenza.
Included in the table is an instance (Autopsy 487) in which
a definite attack of influenza preceded scarlet fever.
120
| Table XXVII |
|---|
| |
| NO. OF AUTOPSY |
RACE |
LENGTH OF MILITARY SERVICE |
DURATION OF ILLNESS |
DURATION OF PNEUMONIA |
CLINICAL DIAGNOSIS |
PURULENT BRONCHITIS |
LOBAR PNEUMONIA |
PERIBRONCHIOLAR CONSOLIDATION |
HEMORRHAGIC PERIBRONCHIOLAR CONSOLIDATION |
LOBULAR CONSOLIDATION |
PERIBRONCHIAL CONSOLIDATION |
ABSCESS |
INTERSTITIAL SUPPURATIVE PNEUMONIA |
MULTIPLE ABSCESSES IN CLUSTERS |
EMPYEMA |
BRONCHIECTASIS |
UNRESOLVED BRONCHOPNEUMONIA |
ORGANIZING BRONCHITIS |
BACTERIA IN SPUTUM |
BACTERIA IN BRONCHUS |
BACTERIA IN LUNG |
BACTERIA IN BLOOD OF HEART |
| 229 |
W |
1m |
12+ |
12+ |
L |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. I. B. inf. |
|
|
0 |
| 231 |
W |
2m |
13 |
4 |
B |
P |
|
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
| 232 |
W |
14d |
9 |
6? |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. IIa. B. inf. |
|
Pn. IIa. |
Pn. IIa. |
| 233 |
C |
11m |
5 |
2 |
L |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
Pn. IIa. |
|
|
Pn. |
| 236 |
W |
3w |
8 |
7+ |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. |
|
B. inf. Staph. |
0 |
| 237 |
W |
10d |
8 |
2 |
L |
|
|
|
+ |
+ |
|
N |
|
|
E |
|
|
|
St. h. |
|
|
St. h. |
| 238 |
W |
2d |
8 |
5 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. |
|
|
Pn. IV |
| 239 |
W |
11d |
9 |
5 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. II. |
|
Pn. II. B. inf. |
Pn. II. |
| 240 |
W |
13d |
8 |
4 |
L |
|
+ |
M |
|
+ |
|
|
|
|
|
|
|
|
Pn. IV. |
B. inf. |
|
Pn. IV. |
| 241 |
W |
14d |
5 |
5 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. |
|
|
Pn. IV. |
| 242 |
C |
14d |
7 |
4 |
L |
P |
|
|
+ |
+ |
|
|
|
|
|
|
|
|
Pn. IIa. B. inf. |
|
|
Pn. IIa. |
| 243 |
W |
15d |
5 |
5 |
L |
|
+ |
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 244 |
C |
1m |
6 |
3 |
B |
P |
|
M |
+ |
+ |
|
|
|
|
|
+ |
|
|
|
Pn. IV. B. inf. |
Pn. IV. B. inf. |
0 |
| 121246 |
C |
2m |
6 |
3 |
L |
P |
+ |
M |
|
|
|
|
|
|
|
|
|
|
Pn. IIa. B. inf. |
|
|
0 |
| 247 |
W |
10d |
10 |
5 |
L |
P |
|
M |
+ |
+ |
|
|
|
|
|
|
|
|
Pn. IV. B. inf. |
|
|
Pn. IV. |
| 248 |
W |
1m |
4 |
2+ |
I |
|
|
|
|
|
|
+ |
|
|
E |
|
|
|
|
St. h. |
St. h. |
St. h. |
| 249 |
W |
15d |
12 |
6+ |
L |
|
|
M |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. III. |
| 250 |
W |
14d |
11 |
7 |
L |
|
|
M |
|
+ |
|
|
|
|
E |
|
|
|
Pn. IIa. B. inf. |
|
|
Pn. IIa. |
| 251 |
W |
25d |
7 |
1 |
B |
P |
|
|
+ |
+ |
|
+ |
+ |
|
|
|
|
|
|
|
St. h. |
St. h. |
| 252 |
W |
21d |
14 |
12 |
B |
P |
|
M |
|
+ |
|
|
|
|
|
|
|
|
|
Pn. II. B. inf. St. v. |
Pn. II. B. inf. |
0 |
| 253 |
W |
12d |
19 |
12+ |
B |
|
|
M |
|
+ |
+ |
|
|
|
E |
|
|
|
Pn. Ia. |
Pn. II. B. inf. Staph. |
Pn. II. B. inf. |
Pn. II. |
| 254 |
W |
21d |
7 |
6+ |
B |
P |
+ |
M |
|
+ |
|
|
|
|
|
|
|
|
|
Pn. I. B. inf. |
Pn. I. Staph |
0 |
| 255 |
W |
12d |
5 |
4? |
B |
P |
|
M |
+ |
+ |
|
+ |
|
|
E |
|
|
|
|
St. h. Pn. IIa. Staph. |
St. h. |
St. h. |
| 256 |
W |
17d |
8 |
4 |
B |
P |
+ |
M |
|
|
|
|
|
|
|
|
|
|
|
Pn. Staph. |
Pn. IIa. |
Pn. IIa. |
| 257 |
C |
21d |
10 |
7+ |
L |
P |
|
|
|
+ |
|
|
|
|
|
|
|
|
|
B. inf. Staph |
|
Pn. I. |
| 258 |
W |
1m |
6 |
2+ |
B |
|
|
M |
|
+ |
|
+ |
|
|
E |
|
|
|
|
|
St. h. Pn. IV. B. inf. |
St. h. |
| 259 |
W |
3m |
4 |
1 |
B |
|
|
|
|
+ |
|
+ |
+ |
|
|
|
|
|
|
|
St. h. Pn. III. Staph. |
St. h. |
| 260 |
W |
1m |
2 |
1 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| 261 |
W |
2m |
7 |
5+ |
B |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
B. inf. Pn. IV. |
|
0 |
| 262 |
W |
12d |
5 |
4? |
B |
|
|
|
|
+ |
|
+ |
|
|
E |
|
|
|
|
St. h. B. inf. |
St. h. |
St. h. |
| 263 |
W |
21d |
7 |
5 |
L |
P |
|
|
|
+ |
|
+ |
|
|
E |
|
|
|
|
|
St. h. B. inf. Staph. |
St. h. Staph. |
| 264 |
W |
21d |
10 |
7 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. Staph. |
St. h. Staph. |
St. h. |
St. h. |
| 265 |
W |
14d |
7 |
6+ |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
St. h. Staph. inf. |
Pn. IV. B. inf. |
St. h. |
| 122266 |
W |
1m |
7 |
2 |
L |
|
|
|
+ |
+ |
|
|
|
|
|
|
|
|
St. h. |
St. h. B. inf. |
St. h. |
St. h. |
| 267 |
W |
2m |
22 |
10 |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
Pn. II. B. inf. |
Pn. II. |
Pn. II. |
| 268 |
W |
2m |
6 |
4? |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. III. B. |
Pn. III. B. inf. St. h. |
Pn. III. B. inf. St. h. |
0 |
| 269 |
W |
25d |
8 |
2 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. B. |
Pn. IV. Staph. |
Pn. IV. |
0 |
| 270 |
W |
17d |
18 |
3 |
L |
|
|
|
|
+ |
h |
|
|
|
|
|
|
|
|
St. h. B. inf. Staph. |
St. h. Staph. |
St. h. |
| 271 |
W |
2d |
12 |
5 |
L |
P |
|
|
|
+ |
|
|
|
|
|
|
|
|
|
St. h. Pn. IV. B. inf. |
St. h. |
St. h. |
| 272 |
W |
3m |
7 |
2 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
St. h. |
| 273 |
W |
1m |
8 |
4+ |
L |
|
+ |
+ |
|
|
|
N |
|
|
E |
|
|
|
|
St. h. B. inf. Staph. |
St. h. Pn. IV. Staph. |
St. h. |
| 274 |
W |
2w |
9 |
5 |
B |
|
|
|
|
+ |
|
N |
|
|
|
|
|
|
Pn. IV. |
St. h. Staph. |
St. h. |
St. h. |
| 275 |
W |
4m |
9 |
4 |
L |
|
|
M |
+ |
+ |
|
N |
|
|
|
|
|
|
|
St. h. B. inf. Staph. |
St. h. B. inf. Staph. |
St. h. Pn. IV. |
| 123276 |
W |
1m |
6 |
4+ |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
St. h. Staph B. inf. |
St. h. Pn. IV. B. inf. |
St. h. |
| 277 |
W |
21d |
10 |
3 |
L |
|
|
|
|
|
|
+ |
|
|
|
|
|
|
|
St. h. Staph |
St. h. Staph |
St. h. |
| 278 |
W |
2m |
16 |
6+ |
L |
|
|
|
|
|
|
+ |
|
|
E |
|
|
|
|
St. h. B. inf. |
St. h. |
St. h. |
| 279 |
W |
|
|
|
L |
|
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. IV |
Pn. IV. |
| 280 |
W |
21d |
8 |
8 |
L |
|
|
|
+ |
+ |
|
|
|
+ |
|
|
|
|
|
St. h. B. inf. Staph. |
St. h. |
St. h. |
| 281 |
W |
21d |
9 |
5 |
L |
|
|
|
+ |
+ |
h |
|
|
|
|
|
|
|
|
|
St. h. B. inf. |
St. h. |
| 282 |
W |
1m |
10 |
? |
B |
|
|
|
|
+ |
|
+ |
|
|
E |
|
|
|
Pn. IV. B. inf. |
St. h. B. inf. Pn. II Staph. |
St. h. Pn. II. |
St. h. Pn. II. |
| 283 |
W |
7d |
19 |
8 |
B |
P |
|
+ |
+ |
+ |
M |
|
|
|
|
+ |
|
|
|
B. inf. Pn. IV. Staph. |
Staph. B. inf. |
Pn. IV. |
| 284 |
W |
21d |
11 |
? |
B |
P |
|
|
+ |
|
|
+ |
|
|
E |
|
|
|
|
St. h. B. inf. Staph. |
St. h. |
St. h. |
| 285 |
W |
|
11 |
9? |
B |
P |
|
M |
|
|
|
|
+ |
|
E |
|
|
|
Pn. IIa. B. inf. |
St. h. B. inf. |
St. h. |
St. h. |
| 286 |
W |
20d |
9 |
4+ |
L |
P |
|
M |
|
|
|
|
|
+ |
|
|
|
|
|
Pn. IV. B. inf. Staph. |
0 |
Pn. IV. |
| 287 |
W |
3m |
12 |
4 |
L |
P |
+ |
+ |
|
|
|
|
|
|
|
+ |
|
|
|
Pn. IV. B. inf. Staph. |
Pn. IV. B inf. Staph. |
Pn. IV. |
| 288 |
W |
1m |
10 |
5 |
B |
P |
|
M |
|
+ |
h |
+ |
|
|
E |
+ |
|
|
St. h. B. inf. |
St. h. B. inf. |
St. h. |
St. h. |
| 289 |
W |
19d |
12 |
7 |
B |
P |
|
M |
|
+ |
M |
|
|
|
|
+ |
|
|
|
Pn. IV. B. inf. Staph. |
Pn. IV. |
Pn. IV. |
| 290 |
W |
1m |
3+ |
3+ |
B |
|
|
|
|
|
|
+ |
|
|
|
|
|
|
|
St. h. B. inf. |
St. h. |
St. h. |
| 291 |
W |
2w |
18 |
11 |
B |
P |
|
+ |
|
+ |
M |
|
|
|
|
+ |
|
|
Pn. IV. B. inf. |
B. inf. Staph. |
0 |
0 |
| 292 |
W |
3m |
5 |
5 |
L |
|
|
|
|
|
|
+ |
|
|
E |
|
|
|
|
|
St. h. B. inf. |
St. h. |
| 293 |
W |
2m |
3+ |
3+ |
L |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. III. B. inf. |
Pn. III. B. inf. |
Pn. III. |
| 295 |
W |
1m |
12 |
5 |
L |
P |
|
|
|
|
|
+ |
+ |
|
E |
+ |
|
|
Pn. IV. St. h. |
St. h. B. inf. |
|
St. h. |
| 124296 |
W |
16d |
18 |
3 |
L |
P |
|
+ |
|
|
|
+ |
|
|
E |
+ |
|
|
|
St. h. B. inf. |
St. h. B. inf. |
St. h. |
| 297 |
W |
1m |
5 |
? |
I |
P |
|
|
|
+ |
|
|
|
|
|
|
|
|
|
B. inf. Pn. IV. St. h. |
Pn. IV. B. inf. |
0 |
| 298 |
C |
21d |
13 |
10 |
B |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IIa. B. inf. |
Pn. IIa. |
|
| 299 |
W |
28d |
9 |
3 |
L |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
B. inf. Pn. IV. Staph. St. h. |
|
|
| 300 |
C |
22d |
16 |
12+ |
L |
P |
+ |
M |
|
|
h |
|
|
|
|
|
|
|
Pn. IIa. B. inf. |
Pn. IIa. B. inf. |
Pn. IIa. |
|
| 301 |
W |
1m |
7 |
5 |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. Staph. St. h. |
Pn. IV. |
|
| 302 |
C |
5d |
6 |
3+ |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. |
Pn. IV. |
|
| 303 |
W |
1m |
7 |
3+ |
L |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
|
Staph. Pn. IV. B. inf. |
Pn. IV. B. inf. |
|
| 304 |
W |
4m |
10 |
2? |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
St. h. B. inf. |
St. h. B. inf. |
|
| 125305 |
W |
5m |
3+ |
3+ |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
B. inf. St. h. Pn. IV. Staph. |
B. inf. St. h Pn. IV. Staph. |
|
| 306 |
W |
1y |
6+ |
3 |
B |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
|
B. inf. Pn. IV. Staph. |
0 |
0 |
| 308 |
W |
1m |
6 |
6 |
L |
|
+ |
|
|
+ |
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. St. h. Staph. |
St. h. |
Pn. IV. |
| 309 |
W |
1m |
4 |
2? |
L |
|
|
|
|
|
|
+ |
|
|
E |
|
|
|
|
|
St. h. |
St. h. |
| 310 |
W |
21d |
? |
3? |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. III. B. inf. Staph. |
Pn. III. Pn. IV. B. inf. |
|
| 312 |
W |
1m |
17 |
7 |
L |
P |
|
M |
|
+ |
h |
N |
|
|
|
+ |
|
|
Pn. IV. B. inf. St. h. |
St. h. B. inf. Staph. |
St. h. B. inf. |
St. |
| 313 |
W |
1y |
5 |
2 |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
St. h. B. inf. Staph. |
St. h. |
St. h. |
| 314 |
W |
1m |
3+ |
3+ |
L |
P |
|
|
|
+ |
|
|
|
|
|
+ |
|
|
|
Pn. IV. B. inf. Staph. |
Pn. IV. |
Pn. IV. |
| 315 |
W |
1m |
9 |
2 |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. Staph. |
Pn. IV. |
| 316 |
W |
1m |
11 |
4 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
B. inf. |
Pn. III. B. inf. |
Pn. III. |
| 317 |
W |
13d |
9 |
2 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. |
Pn. IV. |
|
| 318 |
W |
2m |
8 |
3 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. |
Pn. IV. B. inf. |
|
| 319 |
W |
1m |
4+ |
4+ |
B |
P |
|
|
|
+ |
|
|
|
|
|
|
|
|
|
St. h. Staph. |
St. h. B. inf. Staph. |
St. h. |
| 320 |
C |
5m |
1+ |
1+ |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IIa. |
Pn. IIa. |
Pn. IIa. |
| 321 |
W |
28d |
4+ |
4+ |
L |
|
+ |
|
|
|
|
|
|
|
E |
|
|
|
|
B. inf. |
Pn. IV. B. inf. |
Pn. IV. |
| 322 |
W |
10d |
8 |
6 |
L |
P |
|
|
|
+ |
|
|
|
+ |
|
+ |
|
|
Pn. IV. |
|
Pn. III. Staph. aur. |
0 |
| 323 |
W |
2m |
12 |
4 |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. Staph. |
|
0 |
| 126324 |
W |
22d |
9 |
6 |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. I. B. inf. |
0 |
Pn. I. |
| 325 |
W |
1m |
8 |
8 |
B |
P |
|
M |
|
|
|
N |
+ |
|
|
+ |
|
|
|
St. h. B. inf. Staph. |
St. h. |
St. h. |
| 326 |
W |
1m |
5+ |
2 |
B |
P |
|
|
|
+ |
h |
|
|
|
|
|
|
|
|
St. h. B. inf. Staph. |
St. h. B. inf. |
St. h. |
| 327 |
W |
1m |
4 |
? |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| 328 |
W |
5m |
13 |
3+ |
L |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. III. Pn. IV. B. inf. Staph. |
Pn. III. Pn. IV. B. inf. |
Pn. III. |
| 330 |
W |
1m |
10 |
3 |
L |
|
|
M |
|
|
|
N |
+ |
|
E |
|
|
|
|
|
Pn. IV. |
Pn. IV. |
| 331 |
W |
1m |
12 |
11+ |
B |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 332 |
W |
1m |
17 |
3 |
L |
P |
+ |
M |
|
|
h |
|
|
|
|
|
|
|
|
|
|
0 |
| 333 |
W |
19d |
15 |
7 |
L |
P |
|
M |
|
+ |
|
|
|
+ |
|
+ |
|
|
|
Staph. aur. B. inf. St. h. |
Staph. aur. Pn. IIa. St. h. |
Pn. IIa. |
| 334 |
W |
14d |
16 |
5 |
B |
|
|
M |
|
|
|
N |
+ |
|
E |
|
|
|
|
|
St. h. Staph |
St. h. |
| 127335 |
W |
1m |
7 |
? |
? |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
|
|
St. v. B. inf. Staph. Pn. IV. |
Pn. IV. |
| 336 |
W |
2m |
12 |
6 |
B |
P |
|
M |
|
+ |
|
|
|
|
|
+ |
|
|
|
|
|
0 |
| 337 |
W |
1m |
9 |
2? |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 338 |
W |
1m |
7 |
5+ |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 339 |
W |
2m |
9 |
6? |
L |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 340 |
W |
35d |
8 |
3 |
L |
P |
|
|
+ |
+ |
|
|
|
|
|
|
|
|
|
|
|
0 |
| 341 |
W |
3m |
6 |
4+ |
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| 342 |
W |
2m |
9 |
3? |
L |
P |
|
|
+ |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
| 343 |
W |
1m |
11 |
1? |
L |
|
+ |
|
|
|
|
|
|
|
E |
|
|
|
|
|
Pn. IV. |
Pn. IV. |
| 344 |
W |
4m |
13 |
6 |
L |
|
|
|
|
+ |
|
+ |
|
|
E |
|
|
|
|
|
|
St. h. |
| 345 |
W |
1d |
? |
7 |
L |
P |
|
+ |
+ |
|
|
+ |
|
|
E |
|
|
|
|
|
Pn. III. St. h Staph. |
|
| 346 |
W |
26d |
16 |
10 |
B |
P |
+ |
M |
+ |
|
|
N |
|
|
|
|
|
|
B. inf. Pn. IV. |
St. h. B. inf. |
St. h. B. inf. |
St. h. |
| 347 |
C |
3d |
10 |
3 |
L |
P |
|
|
|
+ |
h |
|
|
|
|
|
|
|
|
|
|
St. h. |
| 348 |
C |
4d |
8 |
8 |
B |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IIa. |
| 349 |
W |
2d |
12 |
6 |
L |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. III St. h |
Pn. I. |
| 350 |
W |
2m |
6 |
2? |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
St. h. |
| 351 |
C |
4m |
4 |
3+ |
L |
P |
|
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
| 352 |
C |
2m |
8 |
4 |
L |
P |
+ |
|
+ |
+ |
|
|
|
|
|
+ |
|
|
|
|
|
Pn. IIa. |
| 353 |
C |
6m |
18 |
18 |
L |
P |
+ |
|
|
|
|
|
|
|
E |
|
|
|
Pn. I. B. inf. |
B. inf. Pn. |
Pn. IIa. |
Pn. IIa. |
| 354 |
W |
15d |
2+ |
2 |
L |
P |
|
M |
|
|
h |
+ |
|
|
E |
|
|
|
|
St. h. B. inf. Staph. |
St. h. |
St. h. |
| 355 |
W |
21d |
7 |
7 |
B |
P |
|
|
+ |
|
|
+ |
|
|
E |
|
|
|
|
St. h. B. inf. Pn. IV. Staph. |
St. h. B. inf. Staph. |
0 |
| 356 |
C |
5d |
8 |
4 |
L |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 357 |
W |
1m |
10 |
6+ |
L |
|
+ |
|
+ |
+ |
|
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. |
Pn. IV. |
| 358 |
W |
1m |
15 |
6? |
L |
|
+ |
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
Pn. IIa. |
| 128359 |
W |
1m |
7+ |
? |
L |
|
|
M |
|
|
h |
|
|
|
|
+ |
|
|
|
|
|
Pn. IV. |
| 360 |
W |
36d |
10 |
3 |
L |
P |
+ |
+ |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
0 |
| 361 |
W |
3m |
8 |
2 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 362 |
W |
4m |
15 |
13+ |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
St. h. |
| 363 |
W |
3m |
8 |
1+ |
L |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 364 |
W |
6d |
9 |
5+ |
B |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
St. h. |
| 365 |
W |
2m |
11 |
2 |
B |
|
+ |
|
+ |
+ |
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
Pn. IV. |
| 366 |
W |
6d |
8 |
1+ |
B |
|
+ |
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 367 |
W |
22d |
15 |
8+ |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 368 |
C |
4d |
15 |
11+ |
L |
P |
+ |
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. I. |
| 369 |
W |
68d |
7+ |
4 |
B |
P |
|
|
+ |
+ |
|
N |
+ |
|
E |
|
|
|
St. h. |
|
St. h. |
St. h. |
| 370 |
W |
17d |
17 |
14 |
L |
P |
|
+ |
|
+ |
|
|
|
+ |
|
|
+ |
+ |
[No. St. h.] |
Staph. aur. Pn. IV. B. inf. |
Staph. aur |
0 |
| 372 |
W |
1m |
17 |
5 |
L |
P |
|
|
+ |
+ |
Mh |
|
|
|
|
+ |
|
|
|
|
|
|
| 373 |
W |
4d |
11 |
1? |
B |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
St. h. |
| 374 |
C |
4d |
10 |
5 |
L |
P |
+ |
|
|
|
+ |
|
|
|
|
+ |
|
|
|
|
|
Pn. IV. |
| 375 |
C |
4d |
12 |
6 |
L |
P |
|
+ |
|
+ |
|
|
|
|
|
+ |
|
|
|
|
|
0 |
| 129376 |
W |
1m |
10 |
7+ |
B |
P |
|
|
+ |
+ |
M |
+ |
|
|
E |
+ |
|
|
[No. St h.] |
St. h. B. inf. Staph. aur. |
St. h. |
St. h. |
| 377 |
W |
1m |
7 |
4? |
B |
P |
+ |
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 378 |
W |
1m |
28 |
7 |
B |
P |
|
+ |
|
|
|
+ |
|
|
E |
+ |
|
|
|
St. h. B. inf. Pn. IIa. |
St. h. B. inf. Pn. IIa. |
Pn. IIa. |
| 379 |
W |
11m |
7 |
1 |
B |
|
+ |
|
|
|
|
|
+ |
|
E |
|
|
|
|
B. inf. + |
? |
Pn. IIa. |
| 380 |
W |
3m |
11 |
? |
B |
P |
|
+ |
|
+ |
|
+ |
|
|
|
|
|
|
|
|
Pn. III. |
Pn. III. |
| 381 |
W |
21d |
13 |
9? |
L |
P |
|
|
|
+ |
|
+ |
|
|
E |
+ |
|
|
|
|
St. h. Pn. II. Pn. IV. Staph. aur. |
St. h. |
| 382 |
W |
1m |
9 |
6+ |
L |
P |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| 383 |
W |
2m |
9 |
2 |
L |
|
|
|
|
+ |
|
+ |
|
|
|
|
|
|
|
|
B. inf. Pn. III. St. h. |
Pn. III. |
| 384 |
W |
1m |
13 |
5 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 385a |
W |
3w |
12 |
6? |
B |
P |
|
|
|
+ |
|
+ |
|
|
E |
|
|
|
|
|
St. h. |
St. h. |
| 385b |
W |
2m |
11 |
4 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 385c |
W |
24d |
17 |
10 |
B |
P |
|
M |
+ |
+ |
|
|
+ |
|
|
+ |
|
|
|
|
St. h. B. inf. |
St. h. |
| 386 |
W |
1m |
? |
5 |
L |
P |
|
|
+ |
+ |
|
|
|
|
|
|
|
|
|
|
Pn. III. B. inf. Staph. aur. |
Pn. III. |
| 387 |
W |
3w |
19 |
9 |
B |
P |
|
|
+ |
+ |
+ |
+ |
|
|
E |
+ |
|
|
|
St. h. B. inf. Staph. aur. Pn. |
Staph. alb Pn. II. B. inf. |
St. h. |
| 388 |
W |
3m |
11 |
7 |
L |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 389 |
W |
1m |
15 |
15 |
L |
P |
|
|
+ |
|
|
|
+ |
|
E |
+ |
|
|
|
|
St. h. |
St. h. |
| 391 |
W |
25d |
13 |
13 |
L |
P |
+ |
+ |
|
+ |
h |
|
|
|
|
+ |
|
|
|
|
Pn. IV. |
Pn. IV. |
| 392 |
W |
1m |
12 |
8+ |
L |
P |
+ |
M |
|
|
+ |
|
|
|
|
|
|
|
|
|
|
Pn. II. |
| 393 |
W |
1m |
20 |
4 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 394 |
W |
21d |
? |
? |
L |
P |
|
|
+ |
+ |
h |
|
|
|
|
+ |
|
|
|
|
|
St. h. |
| 395a |
W |
1m |
19 |
11? |
L |
P |
|
M |
|
+ |
|
+ |
|
|
E |
|
+ |
|
|
|
St. h. B. inf. |
St. h. |
| 395b |
W |
3m |
12 |
3? |
B |
P |
|
|
|
+ |
h |
|
|
|
E |
|
|
|
|
|
Pn. IIa. |
Pn. IIa. |
| 396 |
W |
2m |
7 |
1+ |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
| 130397 |
W |
21d |
22 |
14 |
B |
P |
|
M |
|
+ |
|
|
+ |
|
E |
|
|
|
|
|
St. h. B. inf. |
St. h. |
| 398 |
W |
1m |
16 |
6? |
B |
P |
|
+ |
|
|
M |
|
|
|
|
+ |
+ |
|
|
|
|
0 |
| 399 |
W |
1m |
18 |
4 |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IIa. |
| 400 |
W |
1m |
15 |
11+ |
L |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. |
| 401 |
W |
1m |
13+ |
9 |
B |
P |
+ |
M |
|
|
h |
|
|
|
|
+ |
|
|
|
|
|
Pn. IV. |
| 402 |
W |
1m |
14 |
8 |
B |
P |
|
M |
|
+ |
+ |
|
|
|
E |
+ |
+ |
+ |
|
|
|
Pn. IV. St. h. |
| 404 |
|
|
|
|
B |
P |
|
+ |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
| 405 |
W |
21d |
13 |
11+ |
B |
|
+ |
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. |
| 406 |
C |
2d |
18 |
15? |
L |
P |
+ |
|
|
|
|
+ |
|
|
E |
|
|
|
|
|
|
Pn. IV. |
| 408 |
C |
1m |
13 |
? |
L |
P |
|
|
+ |
+ |
|
|
|
|
|
|
|
|
|
|
|
0 |
| 409 |
C |
6d |
12 |
9+ |
L |
P |
|
|
+ |
+ |
M |
|
|
|
|
|
|
|
|
|
|
0 |
| 410 |
W |
35d |
13+ |
13+ |
L |
P |
|
+ |
|
+ |
M |
+ |
|
|
E |
+ |
|
|
|
|
St. h. B. inf. Staph. aur. |
|
| 411 |
W |
3m |
16 |
2 |
B |
P |
+ |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
Pn. IIa. B. inf. |
Pn. IIa. |
| 412 |
W |
1m |
15 |
13? |
L |
|
+ |
|
|
|
M |
|
|
|
|
+ |
|
|
|
Pn. II. B. inf. |
|
Pn. II. |
| 131413 |
C |
2m |
13 |
8+ |
L |
P |
|
|
+ |
+ |
|
|
|
|
|
|
|
|
|
|
Pn. III. B. inf. |
Pn. III. |
| 414 |
C |
7d |
18 |
4 |
L |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IIa. B. inf. |
Pn. IIa. |
| 415 |
C |
16d |
8 |
6+ |
L |
P |
+ |
|
|
+ |
|
|
+ |
|
|
|
|
|
|
|
St. h. |
0 |
| 416 |
C |
7d |
14 |
6? |
L |
P |
|
|
|
|
|
+ |
|
|
|
|
|
|
|
Pn. IV. |
Pn. IV. |
Pn. IV. |
| 418 |
W |
2m |
19 |
4 |
B |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
|
|
Pn. IIa. St. v. B. inf. |
Pn. IIa. |
| 419 |
W |
4m |
20 |
? |
L |
P |
|
+ |
|
+ |
M |
|
|
|
|
+ |
|
|
|
Pn. II. B. inf. |
Pn. II. B. inf. |
0 |
| 420 |
W |
1m |
11 |
3 |
B |
P |
|
|
+ |
|
M |
|
+ |
|
E |
|
+ |
+ |
|
|
St. h. B. inf. Staph. aur. |
St. h. |
| 421 |
W |
21d |
19 |
15? |
B |
P |
|
|
|
+ |
M |
|
|
|
|
+ |
+ |
+ |
|
|
Pn. IV. St. h. |
St. h. |
| 422 |
W |
3m |
11+ |
11+ |
B |
P |
+ |
|
+ |
|
M |
|
|
|
|
+ |
+ |
|
|
|
Pn. IIa. B. inf. |
0 |
| 423 |
W |
1m |
16 |
12? |
B |
P |
|
+ |
|
|
M |
|
|
|
E |
+ |
+ |
|
|
|
St. h. B. inf. |
St. h. |
| 424 |
W |
5y |
14 |
6 |
L |
P |
|
|
|
+ |
+ |
|
|
|
|
|
|
|
|
|
Pn. IV. |
|
| 425 |
W |
1m |
29 |
14 |
B |
P |
|
+ |
|
+ |
M |
|
|
+ |
|
+ |
+ |
|
|
|
St. h. B. inf. Staph. alb. |
St. h. |
| 426 |
W |
4m |
20 |
13 |
? |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IIa. B. inf. |
Pn. IIa. |
| 427 |
W |
1m |
16 |
? |
L |
P |
|
|
+ |
+ |
|
|
|
|
|
|
|
|
|
|
St. h. |
St. h. |
| 428 |
W |
3w |
25 |
21 |
L |
P |
|
M |
|
+ |
|
|
+ |
|
E |
|
+ |
|
|
St. h. B. inf. |
St. h. B. inf. |
St. h. |
| 429 |
C |
2m |
7+ |
5 |
L |
P |
|
+ |
|
+ |
|
|
|
|
|
+ |
|
|
|
|
B. inf. Staph. alb |
0 |
| 430 |
W |
2m |
16+ |
7 |
L |
P |
+ |
|
+ |
|
|
N |
|
|
|
|
|
|
|
|
St. h. B. inf. Staph. aur. |
St. h. |
| 431 |
W |
21d |
23 |
18 |
L |
P |
|
+ |
|
+ |
|
|
|
|
|
+ |
+ |
|
|
|
0 |
0 |
| 432 |
W |
42d |
19 |
12+? |
L |
P |
+ |
|
|
|
|
|
|
|
E |
|
|
|
|
|
B. inf. Pn. IIa. |
Pn. IIa. |
| 433 |
W |
1m |
19 |
17 |
B |
P |
|
M |
+ |
|
M |
|
+ |
|
E |
|
+ |
|
|
|
St. h. B. inf. Staph. aur. |
0 |
| 132434 |
W |
4m |
14+ |
10 |
L |
|
|
|
|
+ |
|
|
+ |
|
E |
|
|
|
|
St. h. B. inf. Staph. aur. |
St. h. Staph. aur. |
St. h. |
| 435 |
W |
1m |
16+ |
2? |
B |
|
|
|
+ |
|
|
|
|
|
|
|
|
|
|
St. h. B. inf. |
B. inf. + |
St. h. |
| 436 |
C |
11m |
5 |
3+? |
B |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IIa. B. inf. Staph. aur. |
Pn. IIa. |
Pn. IIa. |
| 437 |
C |
5m |
11 |
7? |
L |
P |
+ |
|
|
|
|
|
|
|
|
+ |
|
|
|
|
|
0 |
| 440 |
W |
1m |
19 |
12? |
L |
P |
|
+ |
+ |
+ |
M |
|
|
|
|
+ |
+ |
|
|
B. inf. Staph. aur. |
B. inf. Staph. aur. |
0 |
| 445 |
W |
1m |
27 |
16? |
|
P |
|
M |
|
|
h |
|
|
|
|
+ |
|
+ |
|
Staph. aur. |
Staph. aur. Pn. IV. |
St. h. |
| 446 |
W |
8d |
13 |
? |
|
P |
|
|
+ |
+ |
|
|
|
|
|
|
|
|
|
|
0 |
|
| 447 |
W |
8d |
10 |
2 |
B |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
|
Staph. aur. |
B. coli. Staph. aur. |
0 |
| 448 |
W |
70d |
17 |
14+ |
L |
P |
|
+ |
|
+ |
Mh |
|
|
|
|
+ |
|
|
|
0 |
0 |
0 |
| 449 |
W |
2m |
27 |
13+ |
B |
P |
|
+ |
+ |
|
|
+ |
|
|
E |
+ |
+ |
|
|
St. h. B. coli. |
St. h. B. coli. |
St. h. |
| 452 |
W |
4m |
14 |
9 |
B |
P |
|
M |
|
|
|
|
+ |
|
E |
|
|
|
|
St. h. B. inf. |
St. h. B. inf. |
St. h. |
| 133451 |
C |
2m |
7 |
3+ |
B |
|
+ |
|
|
|
|
|
|
|
E |
|
|
|
|
B. coli. Staph. St. v. |
Pn. IIa. B. inf. |
Pn. IIa. |
| 455 |
C |
|
26 |
22+ |
B |
|
|
|
+ |
|
|
+ |
|
|
E |
|
|
|
|
St. h. B. inf. |
St. h. |
St. h. |
| 456 |
W |
1m |
23+ |
20+ |
L |
P |
|
|
+ |
|
|
|
|
|
E |
|
|
|
|
B. coli. |
|
St. h. |
| 457 |
W |
17m |
17+ |
17+ |
B |
|
|
+ |
+ |
+ |
|
|
|
|
|
|
+ |
+ |
|
Pn. IV. B. inf. |
|
|
| 458 |
W |
11m |
10 |
8+? |
L |
|
|
|
+ |
+ |
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. St. v. |
|
0 |
| 459 |
C |
10d |
6 |
3 |
B |
P |
|
|
+ |
+ |
|
|
|
|
|
|
|
|
|
Staph. aur. Pn. IV. |
|
0 |
| 460 |
W |
1m |
17 |
17 |
L |
P |
|
+ |
|
+ |
M |
+ |
|
|
E |
+ |
|
|
|
St. h. B. inf. Staph. |
St. h. B. inf. |
St. h. |
| 461 |
C |
5d |
14 |
8+ |
L |
P |
+ |
M |
+ |
|
|
|
|
|
|
|
|
|
|
Staph. aur. Pn. I. St. h. |
|
Pn. I. |
| 462 |
C |
5d |
15+ |
12 |
B |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
0 |
| 463 |
W |
3m |
20 |
12 |
B |
P |
|
+ |
|
+ |
Mh |
|
|
|
|
+ |
+ |
|
|
B. inf. Staph. |
B. inf. Staph. |
0 |
| 464 |
C |
21d |
24 |
17? |
L |
P |
|
|
|
+ |
|
|
|
|
|
|
|
|
|
B. inf. Pn. I. Staph. |
B. inf. Pn. I. |
0 |
| 465 |
W |
1m |
24+ |
11 |
LB |
P |
|
M |
|
|
|
+ |
|
|
E |
+ |
|
|
|
St. h. B. inf. Staph. St. v. |
St. h. |
St. h. |
| 466 |
W |
2d |
13 |
3 |
B |
|
+ |
|
|
+ |
|
|
|
|
|
|
|
|
|
Pn. IIa. |
Pn. IIa. |
Pn. IIa. |
| 467 |
W |
3m |
30 |
25? |
B |
P |
|
|
+ |
+ |
|
+ |
|
|
E |
+ |
|
|
|
St. h. B. inf. |
0 |
St. h. |
| 468 |
W |
1m |
22+ |
6 |
L |
P |
+ |
|
|
+ |
|
|
|
|
|
+ |
|
|
|
Staph. aur. B. inf. St. v. |
B. inf. St. v. |
0 |
| 469 |
W |
1m |
25 |
12 |
B |
P |
|
+ |
|
+ |
|
|
|
|
|
|
+ |
|
|
|
|
|
| 471 |
C |
|
6+? |
4 |
L |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. Staph. aur. |
Pn. I. Pn. IV. B. inf. |
0 |
| 472 |
W |
1m |
37 |
21 |
B |
P |
|
+ |
+ |
+ |
|
+ |
|
|
E |
+ |
+ |
|
|
B. coli. |
St. h. B. coli. |
St. h. |
| 134473 |
W |
2w |
28+ |
24 |
B |
P |
|
+ |
|
+ |
|
|
|
|
E |
+ |
+ |
+ |
|
B. inf. St. v. Staph. M. cat. |
St. v. |
Pn. III. |
| 474 |
W |
1m |
36 |
31+ |
L |
|
|
|
|
|
|
+ |
+ |
|
E |
|
|
|
|
St. v. B. inf. M. cat. |
St. h. |
St. h. B. inf. |
| 476 |
W |
7d |
6 |
2 |
B |
P |
|
M |
|
+ |
|
|
|
|
|
|
|
|
|
|
|
0 |
| 477 |
W |
5d |
9 |
5 |
B |
|
|
|
+ |
+ |
|
N |
|
|
|
|
|
|
|
St. h. B. coli. |
St. h. B. coli. |
St. h. |
| 478 |
W |
2m |
9 |
3 |
L |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
|
|
St. h. |
St. h. |
| 479 |
C |
8d |
29 |
15 |
L |
P |
+ |
M |
|
|
|
N |
|
|
|
|
|
|
|
B. inf. St. h. Staph. M. cat. |
St. h. Staph. aur. |
St. h. |
| 480 |
W |
4m |
31+ |
29 |
B |
|
|
|
|
+ |
|
+ |
|
|
E |
|
|
|
|
Staph. aur. St. v. |
Staph. aur. B. inf. St. v. |
B. coli. St. |
| 482 |
W |
2m |
11 |
5+ |
B |
P |
|
+ |
+ |
+ |
M |
|
|
|
|
+ |
|
|
|
B. inf. Pn. IV. St. h. |
B. inf. Pn. IV. |
0 |
| 485 |
W |
3d |
9+ |
3+ |
B |
P |
|
M |
|
|
|
|
+ |
|
E |
|
|
|
|
St. h. B. inf. Staph. aur. B. coli. |
St. h. |
St. h. |
| 135487 |
W |
21d |
55 |
40 |
B |
P |
|
+ |
|
|
|
+ |
|
|
E |
+ |
+ |
|
|
B. inf. St. h. |
B. inf. |
St. h. |
| 488 |
W |
4d |
16 |
8 |
L |
P |
|
M |
|
|
|
+ |
|
|
E |
+ |
|
|
|
St. h. Pn. IIa. |
St. h. |
St. h. |
| 489 |
C |
8d |
11 |
4 |
B |
P |
+ |
|
+ |
|
M |
|
|
|
|
+ |
|
|
|
B. inf. Pn. IV. |
Pn. IV. B. inf. |
0 |
| 494 |
W |
2m |
11 |
3 |
L |
|
|
|
|
+ |
h |
+ |
|
|
E |
|
|
|
|
St. h. B. inf. |
St. h. B. inf. |
St. h. |
| 498 |
W |
1y |
6 |
1? |
L |
|
|
|
|
+ |
|
N |
|
|
|
|
|
|
|
St. v. |
St. v. Staph. aur. Staph. alb. |
St. v. |
| 499 |
W |
5m |
36 |
5 |
B |
P |
|
M |
|
|
|
|
|
|
E |
|
|
+ |
|
St. h. B. inf. |
0 |
St. h. |
| 504 |
W |
3m |
6 |
3 |
L |
|
|
M |
|
|
|
|
+ |
|
E |
|
|
|
|
St. h. B. inf. Staph. |
St. h. |
St. h. |
| 506 |
W |
8m |
7+ |
2? |
B |
|
|
|
|
+ |
|
|
|
|
|
|
|
|
|
Pn. IV. B. inf. Staph. aur. M. cat. |
Pn. IV. Staph. aur. |
Pn. IV. |
136In successive columns the table gives the autopsy number,
race, and length of military service. These factors
have had an important influence upon the incidence of influenza
and pneumonia and have been discussed in a preliminary
report.[79] The duration of illness (4th column of
table), counted from the date of onset of symptoms of
influenza or in some instances, when the earliest symptoms
were those of pneumonia, from onset of pneumonia, can
usually be determined accurately. The duration of pneumonia
(5th column of table) is much more uncertain, because
its determination dates from the first recognition of
the physical signs of pneumonia.
Clinical Diagnosis.—The clinical diagnosis recorded
upon the clinical history of the patient is given in column 6.
Many clinicians have been impressed with the difficulty
of determining during life the type of pneumonia associated
with influenza. The occurrence of purulent bronchitis,
the frequent coexistence of lobar and bronchopneumonia
and an atypical onset often make the recognition of lobar
pneumonia more difficult than usual. The diffuse consolidation
of confluent lobular pneumonia increases the difficulty
of recognizing bronchopneumonia. In the table (column
6) lobar pneumonia is indicated by L., bronchopneumonia
by B. Among 227 autopsies the clinical diagnosis
agreed with the condition found at autopsy in 109 instances
(48 per cent); in 35 instances (15.4 per cent) both lobar and
bronchopneumonia were found at autopsy and a diagnosis
of one or other was made during life. In 83 instances
(36.6 per cent) the diagnosis made during life was incorrect.
Cases admitted to the base hospital at Camp Pike
were as carefully studied as the conditions in a base hospital
during an epidemic permitted and diagnosis of pneumonia
was doubtless as accurate as in other base hospitals.
137Statistics from military and other hospitals based upon
clinical diagnosis of the pneumonias of influenza are probably
subject to an error of at least 1 in 3 cases, and conclusions
based upon them are almost valueless.
The inaccuracy of clinical diagnosis of the pneumonia
of influenza is further illustrated by a consideration of
lobar pneumonia. This diagnosis on the one hand was
made 136 times and was correct 67 times and incorrect 69
times; on the other hand, lobar pneumonia was found at
autopsy 98 times and had been diagnosed in only 67 of
these cases (68.4 per cent).
Classification of the Pulmonary Lesions of Influenza.—
Influenzal pneumonia exhibits the following noteworthy
characters:
1. Acute bronchitis with injury or destruction of lining
epithelium and accumulation of inflammatory exudate
within the lumen.
2. Hemorrhagic pneumonia with accumulation of blood
within the alveoli and within and about the bronchi.
3. Susceptibility of bronchi and pulmonary tissue to secondary
pyogenic infection with necrosis and suppuration.
4. Bronchiectasis.
5. Tendency to the occurrence of chronic pneumonia following
failure of pneumonia to undergo resolution.
All these changes are doubtless referable to the severity
of the primary injury to the lower air passages.
In the presence of destructive changes in the bronchi
many bacterial species, including B. influenzæ, pneumococci
of various types, streptococci (notably hemolytic streptococci)
and staphylococci may invade the lungs and produce
acute inflammation. The anatomic characters of the pneumonic
lesions following influenza are equally varied.
In order to obtain insight into the pathogenesis of these
lesions, it is desirable to imitate the historical development
of knowledge concerning the characters and causes of disease,
namely, first to define accurately the lesions concerned
138and later to determine with what microorganisms these
lesions are associated. The difficulties of this undertaking
are increased by the multiplicity of the microorganisms
concerned and by the well-known truth that the same microorganism,
e. g., the tubercle bacillus, may produce
widely different anatomic lesions.
In the table of autopsies the following lesions are listed:
Column 7. Purulent bronchitis.—“P” indicates that the small bronchi
contain mucopurulent fluid.
Column 8. Lobar pneumonia.—The occurrence of the lesion is indicated
by the plus sign (+).
Column 9. Peribronchiolar consolidation.—The presence of nodular
patches of consolidation about respiratory bronchioles is indicated by the
plus sign (+) when the lesion has been recognized at the time of autopsy.
When the lesion has been first recognized by microscopic examination the
letter “M” is used.
Column 10. Hemorrhagic peribronchiolar consolidation.—The occurrence
of this lesion which represents the preceding on a background of
hemorrhage is indicated by the plus sign (+).
Column 11. Lobular consolidation.—The presence of the lesion is indicated
by the plus sign (+).
Column 12. Peribronchial consolidation.—Peribronchial pneumonia
recognized at the time of autopsy is indicated by the plus sign (+). Peribronchial
pneumonia recognized microscopically is indicated by “M.” The
presence of peribronchial hemorrhage without consolidation is indicated by
“h.”
Column 13. Abscess formation with pneumonia.—Suppuration with abscess
formation almost invariably just below the pleura is indicated by the
plus sign (+). Necrosis of lung tissue recognized microscopically and unaccompanied
by suppuration is indicated by “N.”
Column 14. Suppurative interstitial pneumonia.—This lesion invariably
associated with suppurative lymphangitis is indicated by the plus sign
(+).
Column 15. Multiple abscess in clusters.—Abscesses in clusters about a
bronchus of medium size are indicated by the plus sign (+).
Column 16. Empyema.—The presence of the lesion is indicated by “E.”
Column 17. Bronchiectasis.—“B” indicates the lesion.
Column 18. Unresolved bronchopneumonia.—Presence of the lesion is
indicated by the plus sign (+).
Column 19. Organizing bronchitis and bronchiolitis.—“O” indicates
the lesion.
The lesions of columns 7 to 12 are acute inflammatory
processes, columns 9 to 12 represent different types
139of bronchopneumonia. Columns 13 to 15 represent suppurative
lesions. Columns 17 to 19 represent chronic
lesions. A survey of the table shows the predominance
of acute lesions in the early period of the study and the
gradual increase of chronic lesions.
The last four columns of the table of autopsies give the
bacteriology of the sputum during life and the bacteria
found in the bronchi, in the lungs, and in the blood of the
heart after death.
Mortality of Pneumonia Following Influenza.—From
September 6 to December 15, 250 autopsies were performed
on patients who had died with pneumonia at the base hospital
at Camp Pike, and with few exceptions bacteriologic
cultures were made from them. Although it was not possible
to perform autopsies on all who died, those which were
performed afford a fair index of all deaths, for throughout
the epidemic of influenza and its outbreak of pneumonia
approximately one half of all who died were examined after
death. The relation of autopsies to deaths is shown by a
comparison by weeks of the number of deaths and number
of autopsies during the months of September and October.
| WEEK |
DEATHS |
AUTOPSIES |
| Sept. 1–7 |
1 |
1 |
| Sept. 8–14 |
1 |
1 |
| Sept. 15–21 |
4 |
3 |
| Sept. 22–28 |
15 |
14 |
| Sept. 29–Oct. 5 |
121 |
67 |
| Oct. 6–12 |
191 |
78 |
| Oct. 13–19 |
78 |
43 |
| Oct. 20–27 |
22 |
15 |
| Oct. 28–31 |
8 |
6 |
| |
|
|
| |
441 |
228 |
For most of these autopsies there is a record of the
date of onset of the illness, namely, influenza, which finally
resulted in pneumonia and death. Comparison of the number
of cases of influenza which developed on any day with
the number of fatal cases which had their onset on the same
140day will determine the mortality of influenza at different
periods of the epidemic. Chart 1 shows the number of
cases of influenza which had their onset on each day from
September 1 to October 31 and the number of fatal cases
with autopsy which had their origin on corresponding days.
The comparison by weeks between autopsies and total
number of deaths shows that the autopsies represent with
considerable accuracy the deaths. If there is any error it
occurs at the height of the outbreak of pneumonia from
September 29th to October 5th and not at its beginning,
or end. The chart shows that the highest mortality occurred
among cases of influenza which had their origin at the
beginning of the epidemic from September 21 to October 1,
whereas after October 1, though the maximum number of
cases of influenza occurred on October 3, very few developed
fatal pneumonia.
Mortality from Pneumococcus and Streptococcus Pneumonias.—By
referring fatal cases of streptococcus pneumonia
back to their date of origin it is possible to determine
what proportion of the cases of influenza, which developed
on any day, died with infection by hemolytic streptococcus.
The accompanying chart (Chart 1) shows that infection
with hemolytic streptococci has been very frequent at the
beginning of the epidemic of influenza (shown by area with
double hatch in chart) that is, from September 20 to 30
and subsequently has gradually diminished so that few
cases have had their onset in the second half of the epidemic
from September 30 to October 15.
Pneumococcus pneumonia uncomplicated by streptococcus
infection (shown by area with single hatch in chart)
pursued a course which more closely conformed to the curve
representing influenza. The cases of influenza which resulted
fatally bore a fairly constant ratio to the total number
of cases of influenza from the onset of the epidemic
until October 1, but subsequently few cases of influenza developed
fatal pneumococcus pneumonia.
141These charts arranged with reference to the onset of fatal
pneumonias dissociate very clearly the outbreak of streptococcus
pneumonia, which reached its height at the beginning
of the influenza epidemic, from the uncomplicated
pneumococcus pneumonia which reached its maximum at
the midpart of the influenza epidemic and then abruptly
abated.

Chart 1—Showing the relation of (a) onset of cases of pneumonia shown by autopsy to be uncomplicated by secondary infection with hemolytic streptococcus, indicated by upper continuous line with single hatch, and of (b) onset of fatal cases of streptococcus pneumonia, indicated by the lower continuous line with double hatch, to (c) the occurrence of influenza, indicated by the broken line. The onset of each case of fatal pneumonia is represented by a single square.
Our study of ward infection in pneumonia furnishes an
explanation of the outbreak of fatal streptococcus pneumonia
coincident with the initial stage of the influenza epidemic.
This outbreak is a true epidemic of streptococcus
infection superimposed, in many instances at least, upon
preexisting pneumococcus pneumonia, but in some instances,
142doubtless, a primary streptococcus pneumonia,
following the bronchitis of influenza. In the absence of
secondary streptococcus infection a very large proportion
of these individuals would have recovered. This epidemic
of streptococcus pneumonia, it has been shown, was the result
of unfavorable conditions produced by great overcrowding
of the hospital and in the early part of the epidemic
by inadequate separation of those with streptococcus
infection from those with none. With control of these conditions,
streptococcus pneumonia rapidly diminished.
Greater susceptibility to pneumococcus pneumonia in the
early than in the late period of the epidemic is perhaps
explained by differences in the severity of influenza; the
more susceptible individuals were attacked by influenza
in the early period, whereas the less susceptible did not
acquire the disease until they had been exposed to an immensely
increased number of infected individuals. A better
explanation is furnished by the greater opportunity at
the beginning of the epidemic for the transmission of microorganisms
causing pneumonia, for at this time patients
with influenza were crowded together and methods to prevent
the transmission of infection were little used.
Bronchitis
Clinical study has shown that purulent bronchitis (see
Fig. 2) occurs in about one-third of the cases of influenza.
In a large proportion of cases of bronchitis there is no clinical
evidence of pneumonia. The bronchial lesions found in
association with the pneumonia of influenza are an index of
the ability of the agent, which causes influenza, to injure the
bronchi.
In those who have died with pneumonia following influenza
the large bronchi (with cartilage) are intensely injected,
so that the mucosa has a deep red color which
on cross section contrasts very sharply with the pearly
white of the cartilage. Superficial injury to the bronchi is
143not infrequently evident in the larger bronchial branches;
superficial loss of epithelium is indicated by erosion of the
surface, whereas somewhat deeper destructive changes are
occasionally evident. Microscopic examination accurately
determines the degree of destructive change.
Purulent bronchitis was noted in 134 autopsies (55.6 per
cent of autopsies). From the small bronchi, in many instances,
purulent fluid welled up upon the cut surface of
the lung, whereas in other instances tenacious mucopurulent
fluid could be squeezed from small, cut bronchi by pressure
upon lung tissue. The consistency of the material
within the bronchi varied greatly, ranging from a viscid
and tenacious mucus of creamy, yellow color to a thin, turbid,
gray fluid. The coexistence of local inflammatory or
of general edema of the lungs modifies the character of the
material found in the bronchi at autopsy; with edema the
purulent exudate is in some instances diluted so that a thin
cloudy fluid flows from the small bronchi. In the presence
of advanced edema of the lungs the bronchi rarely if ever
contain purulent exudate. The underlying changes in the
bronchi are more significant than the character of the exudate
found at autopsy. Nevertheless, the group of cases
in which the diagnosis of purulent bronchitis has been
made, because small and medium sized bronchi have contained
purulent or mucopurulent exudate, represents instances
of readily recognizable bronchitis of considerable
severity.
With few exceptions, purulent bronchitis was diffusely
distributed in the lungs; occasionally it was observed in
one lung alone, and in several instances was limited to the
bronchi at the base of a lung, usually of the left lung.
In a considerable proportion of instances of purulent
bronchitis abnormal distention of the lungs was noted. On
removal from the chest the lungs fail to collapse and retain
the size and shape of the thorax. Even after section is
made through the organ, parts of the lung fail to collapse
144and have a resistant cushion-like consistency. This condition
is present where the lung tissue is air containing and
dry, and occurs when very small bronchi contain tenacious
mucous exudate which becomes apparent upon the cut surface
after the sectioned lung is squeezed. Microscopic examination
shows that the alveolar ducts and infundibula
are distended with air, though the respiratory bronchioles
contain inflammatory exudate. Complete obstruction of
the bronchi is followed by absorption of air from the tributary
pulmonary tissue with atelectasis. It is not improbable
that partial obstruction, permitting the penetration of
air with inspiration, produces distention of air containing
tissue.
It is furthermore probable that cyanosis, which is a conspicuous
feature of many instances of pneumonia following
influenza, is referable, in part at least, to obstruction of the
bronchi by mucopurulent exudate.
The term pneumonia will refer to those inflammatory
changes in the lung which are found within the alveoli; it
will include inflammatory changes in the alveoli surrounding
the respiratory bronchioles, in the alveolar ducts and
infundibula and in their tributary alveoli. Bronchitis will
be described by defining the changes which occur (a) in the
small bronchi with no cartilage or mucous glands, and (b)
in the large bronchi including the primary branches of the
trachea.
For convenience of description those bronchi may be
designated small, which have no cartilaginous plates in
their wall. Larger bronchi have cartilage and mucous
glands, the latter situated in considerable part outside the
cartilaginous plates. These bronchi, of which the largest
are the right and left bronchi formed by bifurcation of the
trachea, diminish with repeated branching to a caliber of
about 1 mm. Small bronchi are lined by columnar ciliated
epithelium; their wall consists of very vascular connective
145tissue containing a layer of smooth muscle and their caliber
varies approximately from 1 to 0.5 mm. It is convenient
to designate as respiratory bronchioles[80] the terminal
ramifications of the bronchi; they are lined by a
single layer of columnar ciliated cells passing over into
cuboidal nonciliated epithelium and are beset with small
air sacs lined by flat cells or epithelial plates similar to those
of the alveoli elsewhere. Not infrequently these alveoli occur
along only one side of the bronchiole, the remainder of
the circumference being covered by a continuous layer of
cubical epithelium. The respiratory bronchiole by branching
along its course or at its end is continued into several
alveolar ducts which unlike the respiratory bronchioles
have no cubical or columnar epithelium but are closely beset
by alveoli lined by flat epithelial plates. The alveolar
duct is recognized by the absence of cubical epithelium and
the presence of bundles of smooth muscle which occur in
the wall. The infundibula or alveolar sacs arise as
branches from the alveolar ducts and like them are beset
with alveoli, but smooth muscle does not occur in their
walls. The base of the infundibulum is wider than its orifice,
which Miller states is surrounded by a sphincter-like
bundle of smooth muscle.
Changes in the main bronchi and their primary branches
are usually less severe than those in bronchi of smaller
size. The epithelium is often intact, the superficial cells
being columnar and ciliated, but not infrequently desquamation
of superficial cells has occurred and the lower
layers alone remain. Occasionally (Autopsy 471) there is
necrosis of epithelium with which, although the architecture
of cells is preserved, nuclei have disappeared. Accumulation
of blood or serum may separate epithelium from
the underlying basement membrane (Fig. 1). Complete
loss of epithelium occurs, usually in small patches.
146Polynuclear leucocytes are numerous upon the surface
of the epithelium and are sometimes fixed in process of
migration through epithelium and basement membrane.
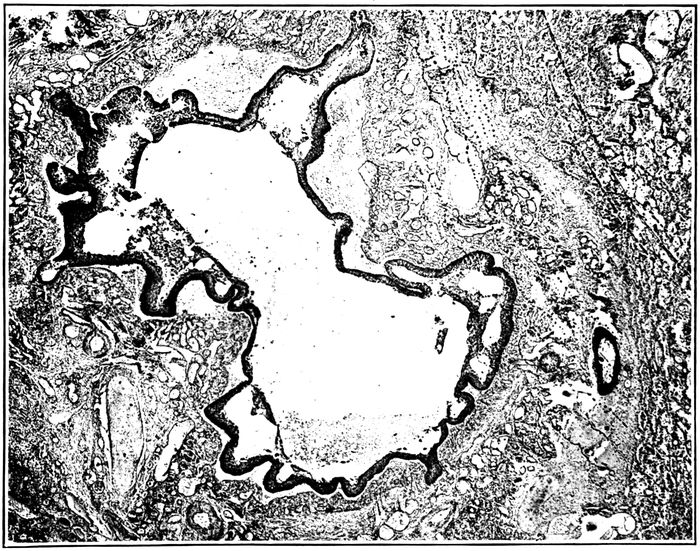
Fig. 1.—Acute bronchitis showing engorgement of blood vessels of mucosa and elevation of epithelium by serum and blood. Autopsy 352.
The blood vessels of the mucosa are engorged. There
is sometimes edema or hemorrhage, and in the superficial
part of the mucosa polynuclear leucocytes are often fairly
abundant. When superficial epithelium has been lost, polynuclears
are numerous immediately below the surface of
the exposed tissue. Fibrin is often present upon the denuded
surface and extends for a short distance into the
tissue below. In the deeper part of the mucosa, about the
muscularis and especially about and between the acini of
the mucous glands, the tissue is infiltrated with lymphoid
and plasma cells.
Changes in the mucous glands are invariably present.
These changes are distention of ducts and acini with mucous,
147degenerative changes occasionally ending in necrosis
of cells, disappearance of acini, dense infiltration of interstitial
tissue with lymphoid and plasma cells and finally
proliferation of this interstitial tissue. The duct of a mucous
gland, dilated and filled with mucus, may be surrounded
by lymphoid and plasma cells in great number.
Acini, similarly dilated, contain mucus and are composed of
cubical cells which have discharged their mucous content.
In some instances (e. g., Autopsy 257) the cells of the acini
have undergone necrosis; the cytoplasm stains homogeneously
and the nuclei have disappeared. Where necrosis
has occurred, polynuclear leucocytes may penetrate into
the dead cells. In association with degenerative changes
in the acini there is abundant infiltration of the interstitial
tissue within and about the glands with lymphoid and
plasma cells. When the acini have disappeared there is
proliferation of fibroblasts and new formation of fibrous
tissue, and mucous glands are found in which a few
atrophied acini are separated by newly formed fibrous
tissue.
With the bronchitis of influenza the small bronchi (with
no cartilage or mucous glands) show every stage of transition
from early acute inflammation characterized by accumulation
of polynuclear leucocytes within the lumen, engorgement
of blood vessels, and infiltration of the wall with
polynuclear leucocytes, through various stages of destructive
changes to complete disappearance of the bronchial
wall and formation of an abscess cavity at the site of the
bronchus. In the early stages of acute bronchitis, hemorrhage
is frequently associated with the lesion. Blood may
be abundant within the lumen of the bronchus, and in the
mucosa red blood corpuscles often infiltrate the tissue
around greatly distended blood vessels, or accumulating
below the epithelium, separate it from its basement membrane.
Hemorrhage is not limited to the wall of the bronchus,
but frequently occurs into the alveoli in a zone encircling
the bronchus.
148With acute bronchitis there may be desquamation of
epithelial cells with partial or complete loss of epithelial
lining. In the smallest bronchi the single layer of columnar
cells may be separated in places from the underlying
tissue, so that intact rows of cells are found within the
lumen. In somewhat larger bronchi, lined by epithelium
in multiple layers, superficial columnar ciliated cells may
be lost. In some instances superficial epithelial cells appear
to have lost their cohesion and are separated by narrow
spaces; in these instances, polynuclear leucocytes are
often numerous between epithelial cells. Epithelium is occasionally
separated from its basement membrane by small
accumulations of serum or blood. Occasionally necrosis
of epithelial cells with disappearance of nuclei is seen and
is doubtless caused by the action of bacteria; the affected
cells may be raised from the underlying tissue by accumulated
serum (Autopsy 253). The changes which have
been described bring about partial or complete loss of
the ciliated lining of the bronchial tube.
The severity of changes in the bronchial wall is in direct
relation to the extent of destruction of the lining epithelium:
when the epithelium remains intact polynuclear
leucocytes may be found in considerable number immediately
below it, but as the lesion progresses, cells in great
part mononuclear, namely, lymphoid and plasma cells, accumulate
in large number throughout the wall of the bronchus.
There is often abundant cellular infiltration within
and about the bundles of the muscular coat. The changes
assume the character of chronic inflammation.
When the lining epithelium of the bronchus is lost, fibrin
tends to accumulate over the surface of the defect, to which
it is firmly attached. It remains separated by a conspicuous
space from adjacent intact epithelium over which it
may project. This superficial network of fibrin merges
with a similar network, extending to a variable depth within
the tissue. What may well be described as coagulative
149necrosis has often occurred, and structures, such as white
fibrous bundles or wall of blood vessels, are marked out
by hyaline material which merges with fibrin. When the
walls of the blood vessels which are invariably engorged
are involved, the lumen is plugged by a fibrinous thrombus.
Little patches of fibrin adherent to the inner surface of
the bronchus may occur in spots where epithelium has been
lost; with uniform loss of epithelium the entire circumference
may be lined with fibrin forming a circular zone
occasionally quite uniform in thickness.
Accumulations of polynuclear leucocytes doubtless bring
about conditions which cause solution of fibrin or prevent
its formation (when disintegration of leucocytes sets free
leucoprotease in abundance). The activity of the infecting
microorganisms, usually hemolytic streptococci or staphylococci,
may cause complete necrosis of a part or all of the
bronchial wall. The cavity which is formed may penetrate
into lung tissue that has previously undergone pneumonic
consolidation.
Further changes caused by the bronchitis of influenza
will be considered under peribronchial hemorrhage and
edema, peribronchial pneumonia and bronchiogenic abscess.
Purulent bronchitis is almost invariably associated
with dilatation of the bronchi, the affected bronchi being
distended with pus. With increasing dilatation bronchiectasis
becomes evident upon gross examination of the tissue,
and is much more advanced in the small bronchi than in
the larger cartilaginous passages. This subject will be
further considered under bronchiectasis.
In association with the acute bronchitis of influenza the
epithelium of bronchi not infrequently looses its superficial
columnar ciliated cells and assumes some of the characters
of a squamous epithelium being covered by polygonal or
flat cells (Figs. 17 and 18). The condition is often described
a “squamous metaplasia,” although it doubtless
represents a stage of regeneration following injury rather
150than a true metaplasia. The basal cells of the epithelium
have a cubical or columnar form; above them the cells become
polygonal and as the surface is approached, cells are
flat and even scale-like. The nuclei of these superficial
cells are often lost. There is no close resemblance to the
squamous epithelium of the skin, for intercellular bridges
are not seen.
This change may occur within six days after onset of
influenza, though in most instances the duration of illness
has been two weeks or more. It may affect either large
or small bronchi, but it is more frequently found in the
latter. Whenever ciliated columnar cells are lost, superficial
cells tend to become flat. Epithelium on one side of a
bronchus may have a squamous character, whereas that
elsewhere is columnar and ciliated. The flat epithelium may
undergo thickening so that it is 0.1 mm. or more in thickness.
It is noteworthy that regenerating epithelium growing
over a denuded surface has the squamous character
which has been described (Plate XIV, Fig. 22).
Bacteriology of the Bronchitis of Influenza.—With the
pneumonia of influenza, bronchitis is invariably present.
Cultures have been made from the right or left main bronchus
or from the very small bronchi which contained purulent
exudate. A routine method of making the culture has
been adopted. The right main bronchus, exposed by drawing
the right lung out of the chest and toward the midline,
was widely seared with a hot knife; the bronchus was partially
cut across through the seared surface with a heated
knife and a platinum needle inserted into the lumen. The
bacteria obtained named in the approximate order of their
relative frequency have been: B. influenzæ, pneumococci,
hemolytic streptococci, staphylococci (aureus and albus),
B. coli, S. viridans, M. catarrhalis, and diphthoid bacilli
which have not been identified. Mixed infections occurred
in most instances. The following list arranged by grouping
151bacteria in the order cited above, shows how varied have
been the combinations which occur:
| B. influenzæ |
3 |
| Pneumococci |
5 |
| S. hemolyticus |
3 |
| Staphylococci |
3 |
| B. coli |
3 |
| S. viridans |
1 |
| B. influenzæ, pneumococci |
17 |
| B. influenzæ, S. hemolyticus |
18 |
| B. influenzæ, staphylococci |
4 |
| Pneumococci, S. hemolyticus |
1 |
| Pneumococci, staphylococci |
3 |
| S. hemolyticus, staphylococci |
4 |
| S. hemolyticus, B. coli |
2 |
| Staphylococci, S. viridans |
1 |
| B. influenzæ, pneumococci, S. hemolyticus |
6 |
| B. influenzæ, pneumococci, staphylococci |
15 |
| B. influenzæ, pneumococci, S. viridans |
2 |
| B. influenzæ, S. hemolyticus, staphylococci |
16 |
| B. influenzæ, S. hemolyticus, M. catarrhalis |
1 |
| B. influenzæ, staphylococci, S. viridans |
1 |
| Pneumococci, S. hemolyticus, staphylococci |
3 |
| Staphylococci, B. coli, S. viridans |
1 |
| B. influenzæ, pneumococci, S. hemolyticus, staphylococci |
7 |
| B. influenzæ, pneumococci, staphylococci, M. catarrhalis |
1 |
| B. influenzæ, S. hemolyticus, staphylococci, B. coli |
1 |
| B. influenzæ, S. hemolyticus, staphylococci, S. viridans |
1 |
| B. influenzæ, S. hemolyticus, staphylococci, M. catarrhalis |
1 |
| B. influenzæ, staphylococci, S. viridans, M. catarrhalis |
1 |
B. influenzæ has been present in the bronchi in 79.3 per
cent of instances of pneumonia referable to influenza. Combinations
which have been found most frequently are B.
influenzæ and pneumococci (17 instances), B. influenzæ and
hemolytic streptococci (18 instances), or the same combinations
with staphylococci, namely, B. influenzæ, pneumococci
and staphylococci (15 instances), and B. influenzæ, hemolytic
streptococci and staphylococci (16 instances). There
is little doubt that B. influenzæ was not identified in some
instances in which it was present; when other microorganisms
are very numerous its inconspicuous colonies may be
overgrown even though the presence of pneumococci, streptococci
152or staphylococci tends to increase the size of its colonies.
Moreover, it is not improbable that the microorganism
may disappear from the bronchi. Comparison with
observations made upon influenza suggests that multiple
methods of examination might have demonstrated a much
higher incidence of B. influenzæ. Throat cultures alone
made during life demonstrated the presence of B. influenzæ
in only 65.7 per cent of patients with acute influenza,
whereas when cultures were made from the nose, throat
and sputum, and a mouse was inoculated with sputum from
each patient, B. influenzæ was found in every instance.
After the acute stage of the disease had passed, the number
of microorganisms diminished, and in many instances
B. influenzæ disappeared from the upper air passages. In
some of our autopsies B. influenzæ doubtless present during
life has similarly disappeared before death due to
pneumonia caused by pneumococci or streptococci. In view
of these considerations it is not improbable that B. influenzæ
demonstrated by a single culture in 80 per cent of
instances has been constantly present.
Table XXVIII represents the incidence of pneumococci,
hemolytic streptococci, staphylococci, and B. influenzæ in
the bronchi, lungs and blood of those individuals with pneumonia
in whom bacteriologic examination has been made at
autopsy. The number of cultures made from the bronchi,
lungs or blood of the heart is given in the second column
of the table and in other columns are given the incidence in
number and percentage of the microorganisms which have
been mentioned.
| Table XXVIII |
|---|
| |
|
NO. OF CULTURES |
PNEUMOCOCCI |
HEMOLYTIC STREPTOCOCCI |
STAPHYLOCOCCI |
B. INFLUENZÆ |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
121 |
56 |
46.3 |
58 |
47.9 |
61 |
50.4 |
96 |
79.3 |
| Lung |
153 |
68 |
44.4 |
77 |
50.3 |
37 |
24.2 |
70 |
45.7 |
| Blood |
218 |
87 |
39.9 |
85 |
39.0 |
1 |
0.5 |
1 |
0.5 |
153Cultures from the bronchus represent the bacteriology
of the bronchitis of influenza. Infection of the lung following
influenza doubtless occurs by way of the bronchi,
so that the bacteria which cause pneumonia are present in
the bronchi before they enter the lung tissue. The figures
in Table XXVIII, similar to those previously cited, show
the high incidence of B. influenzæ, and the occurrence of
pneumococci, hemolytic streptococci and staphylococci each
present in approximately half of all autopsies.
The figures in Table XXVIII are an index of the capacity
of the microorganisms which enter the bronchi to invade
the lungs and finally the blood. Pneumococci were present
in the bronchi in 46.3 per cent of instances, in the lungs
in only slightly less, and in approximately 40 per cent of
autopsies they had penetrated into the blood. Hemolytic
streptococci enter the bronchi with the same frequency and
exhibit an equal ability to penetrate into the lungs and
blood. Staphylococci enter the bronchi in half of these individuals,
but penetrate into the lungs in only a fourth of
the instances. They have entered the blood only once (Autopsy
263) in this instance in association with hemolytic
streptococci. B. influenzæ has been present in the bronchi
in approximately 80 per cent of autopsies. It is noteworthy
that it has been found in the lung in little more than
half this percentage of instances and has entered the blood
only once (Autopsy 474), in this instance in association with
hemolytic streptococci.
In a limited number of autopsies there was purulent
bronchitis recognized by the presence of mucopurulent exudate
in small bronchi. It has been stated that this group
of cases is not sharply separable from other instances of
bronchitis, because in some cases death has occurred before
a purulent exudate has accumulated or in other instances
a purulent exudate has been displaced by edema. Table
XXIX shows the bacteriology of instances of purulent
bronchitis:
154
| Table XXIX |
|---|
| |
|
NO. OF CULTURES |
PNEUMOCOCCI |
HEMOLYTIC STREPTOCOCCI |
STAPHYLOCOCCI |
B. INFLUENZÆ |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
66 |
33 |
50.0 |
32 |
48.5 |
36 |
54.5 |
53 |
80.3 |
The percentages of various bacteria with purulent bronchitis
do not differ essentially from those obtained from
all autopsies with pneumonia. B. influenzæ is found in approximately
80 per cent of autopsies. In 16 instances cultures
were made from the purulent fluid contained in a
small bronchus and the incidence of B. influenzæ (namely,
81.4 per cent) has not differed from that in the main bronchus.
In 7 of 8 instances in which cultures were made, both
from the right main bronchus and from the purulent fluid
in a small bronchus, B. influenzæ was found in one or other
in all but one autopsy (87.5 per cent); in this instance (Autopsy
472) respiratory disease began thirty-seven days before
death and cultures from large and small bronchi at
autopsy were overgrown by B. coli. Since observations
upon influenza made during life have shown that B. influenzæ
is constantly demonstrable when multiple methods are
employed for its detection, the figures just cited give support
to the suggestion that B. influenzæ is constantly present
in the bronchi with the bronchitis of influenza.
Lobar Pneumonia
The frequency with which the confluent lobular consolidation
of bronchopneumonia involving whole lobes or
parts of lobes follows influenza has emphasized the desirability
of distinguishing carefully between lobar and confluent
lobular pneumonia. The pulmonary lesion has been
designated lobar pneumonia when it exhibited the well-known
characters of this lesion, namely, firm consolidation
of large parts of lobes, coarse granulation of the cut surface,
155fibrinous plugs in the bronchi and, on microscopic examination,
homogeneous consolidation and fibrinous plugs
within the alveoli. With confluent lobular consolidation of
bronchopneumonia the consolidated area is in most cases
obviously limited by lobule boundaries, and well-defined
lobules of consolidation occur elsewhere in the lungs.
Lobar pneumonia occurred in 98 among 241 instances of
pneumonia following influenza, namely, in 40.7 per cent of
autopsies.
The difficulty of separating lobar and bronchopneumonia
following influenza has been increased by the frequent combination
of the two lesions in the same individual. There
were 34 instances in which lobar and bronchopneumonia
occurred together. The anatomic diagnosis of lobar pneumonia
was made only when lobes or parts of lobes were
firmly consolidated and exhibited the characters of the lesion
enumerated above; in several instances, in which there
was some doubt concerning the nature of the lesion, microscopic
examination was decisive. The associated bronchopneumonic
lesions represented all the types which have
been associated with influenza. In the group of 34 cases of
coexisting lobar and bronchopneumonia, lobular consolidation
occurred 10 times, peribronchiolar consolidation 14
times (recognized in all but 4 instances by microscopic examination),
hemorrhagic peribronchiolar consolidation 9
times, peribronchial pneumonia 4 times. The intimate relation
of these lesions to changes in the bronchi is well
shown by the frequent presence of purulent bronchitis.
The associated lesions of the bronchi in these cases were as
follows: purulent bronchitis in 23 instances; peribronchial
hemorrhage in 6; bronchiectasis in 11. The frequency of
purulent bronchitis and other bronchial lesions in association
with coexisting lobar and bronchopneumonia is in
sharp contrast with the occurrence of these lesions in association
with lobar pneumonia alone; with 69 instances of
156lobar pneumonia alone purulent bronchitis occurred 17
times and bronchiectasis once.
Lobar pneumonia following influenza passes through the
usual stages of red and gray hepatization. Red hepatization
was found 16 times, combined red and gray hepatization
28 times, and gray hepatization 20 times. The average
duration of pneumonia with red hepatization was 3.7 days,
with combined red and gray hepatization 5.1 days and with
gray hepatization 7.5 days. These figures, it will be shown
later, have some importance in relation to the stage at
which hemolytic streptococcus infects lungs the site of
lobar pneumonia.
Bacteriology of Lobar Pneumonia.—Table XXX is compiled
with the purpose of determining the bacteriology
of the bronchi, lungs and heart’s blood in autopsies
performed on individuals with lobar pneumonia. In some
instances bacteriologic examination of one or other of these
organs was omitted; the percentage incidence is an index
of the presence of pneumococci, hemolytic streptococci,
staphylococci or B. influenzæ in the bronchi, lungs or
heart’s blood and measures the invasive power of these microorganisms
during the course of lobar pneumonia following
influenza.
| Table XXX |
|---|
| |
|
NO. OF CULTURES |
PNEUMOCOCCI |
HEMOLYTIC STREPTOCOCCI |
STAPHYLOCOCCI |
B. INFLUENZÆ |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
44 |
56.9 |
14 |
31.8 |
22 |
37 |
84.1 |
96 |
79.3 |
| Lung |
53 |
77.3 |
13 |
24.5 |
8 |
26 |
49.1 |
70 |
45.7 |
| Blood |
87 |
65.5 |
11 |
12.6 |
|
|
|
1 |
0.5 |
Pneumococci, the recognized cause of lobar pneumonia,
were found in the lungs in 73.3 per cent of autopsies; failure
to find the microorganism in all instances is doubtless
the result of its disappearance from the lung, which, it is
well known, occurs not infrequently particularly during
157the later stages of the disease. In 65.5 per cent of instances
of fatal lobar pneumonia pneumococci have entered the
heart’s blood.
Hemolytic streptococci unlike pneumococci were found
more frequently in the bronchi than in the lungs; this microorganism
which exhibits little tendency to disappear,
once it has established itself within the body, found entrance
into the bronchi in 31.8 per cent of instances of lobar
pneumonia and in 24.5 per cent entered the lungs. Its invasive
power is further illustrated by its penetration into the
heart’s blood approximately in half this proportion of autopsies.
Staphylococci enter the bronchi in many instances (50
per cent), but relatively seldom (15.1 per cent) invade the
lung and rarely if ever penetrate into the blood.
The high incidence, namely, 84.1 per cent, of B. influenzæ
in the bronchi is particularly noteworthy; it exceeds that
of pneumococci, the well-recognized cause of lobar pneumonia,
within the lung. It is found much less frequently
within consolidated lung tissue and shows no tendency to
invade the heart’s blood. B. influenzæ finds the most favorable
conditions for its multiplication within the bronchi.
In view of the frequent occurrence of coexisting lobar
and bronchopneumonia it has appeared desirable to determine
how far the existence of obvious bronchopneumonia
modifies the bacteriology of lobar pneumonia. In Table
XXXI the incidence of pneumococci, hemolytic streptococci,
staphylococci and B. influenzæ after death with lobar pneumonia
on the one hand is compared with their incidence
after combined lobar and bronchopneumonia on the other.
Pneumococci are found in the lung more frequently with
lobar than with combined lobar and bronchopneumonia.
The incidence of hemolytic streptococci and of staphylococci
in the lung is on the contrary higher when bronchopneumonia
is associated with lobar pneumonia. It is not
improbable that these microorganisms have a part in the
production of associated bronchopneumonia. The frequency
with which microorganisms invade the blood is almost
identical in the two groups.
158
| Table XXXI |
|---|
| |
| With Lobar Pneumonia Alone |
|---|
| |
|
NO. OF CULTURES |
PNEUMOCOCCI |
HEMOLYTIC STREPTOCOCCI |
STAPHYLOCOCCI |
B. INFLUENZÆ |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
30 |
20 |
66.6 |
9 |
30 |
15 |
50 |
26 |
86.7 |
| Lung |
34 |
29 |
85.2 |
7 |
20.6 |
3 |
8.8 |
18 |
52.9 |
| Blood |
54 |
36 |
66.7 |
7 |
13 |
|
|
|
|
| |
| |
| With Combined Lobar and Bronchopneumonia |
|---|
| |
|
NO. OF CULTURES |
PNEUMOCOCCI |
HEMOLYTIC STREPTOCOCCI |
STAPHYLOCOCCI |
B. INFLUENZÆ |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
14 |
9 |
64.3 |
5 |
34.3 |
7 |
50 |
11 |
78.6 |
| Lung |
19 |
12 |
63.2 |
6 |
31.6 |
5 |
26.3 |
8 |
42.1 |
| Blood |
33 |
21 |
63.1 |
4 |
12.1 |
|
|
|
|
The relative frequency with which different types of
pneumococci produce lobar pneumonia under the conditions
existing when Camp Pike was attacked by an epidemic of
influenza is indicated by Table XXXII in which instances
of lobar pneumonia alone and of combined lobar
and bronchopneumonia are listed separately.
Pneumococcus I and II, which are found approximately
in two-thirds of instances of lobar pneumonia occurring in
cities, have an insignificant part in the production of these
lesions. Pneumococcus IV and atypical Pneumococcus II,
which are commonly found in the mouth, are the predominant
cause of these lesions, and with Pneumococcus III,
also an inhabitant of the mouths of normal individuals,
have been the cause of two-thirds of all instances of lobar
pneumonia observed in this camp.
159
| Table XXXII |
|---|
| |
| With Lobar Pneumonia |
|---|
|
NO. OF CULTURES |
PNEUMOCOCCUS I |
PNEUMOCOCCUS II |
PNEUMOCOCCUS II (Atyp.) |
PNEUMOCOCCUS III |
PNEUMOCOCCUS IV |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
30 |
1 |
3.3 |
1 |
3.3 |
4 |
13.3 |
4 |
13.3 |
10 |
33.3 |
| Lung |
34 |
1 |
2.9 |
2 |
5.9 |
9 |
26.5 |
6 |
17.6 |
11 |
32.4 |
| Blood |
54 |
2 |
3.7 |
2 |
3.7 |
12 |
22.2 |
3 |
5.6 |
17 |
31.5 |
| |
| With Combined Lobar and Bronchopneumonia |
|---|
|
NO. OF CULTURES |
PNEUMOCOCCUS I |
PNEUMOCOCCUS II |
PNEUMOCOCCUS II (Atyp.) |
PNEUMOCOCCUS III |
PNEUMOCOCCUS IV |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
14 |
2 |
14.3 |
1 |
7.1 |
3 |
21.4 |
|
|
3 |
21.4 |
| Lung |
19 |
1 |
5.3 |
|
|
5 |
26.3 |
|
|
6 |
31.6 |
| Blood |
33 |
2 |
6.1 |
3 |
9.1 |
4 |
12.1 |
|
|
12 |
36.4 |
There is no noteworthy difference in the occurrence of
these types of pneumococci among instances of lobar pneumonia,
on the one hand, and of combined lobar and bronchopneumonia,
on the other. Different types exhibit no noteworthy
differences in their ability to penetrate into lungs
and blood.
Hemolytic Streptococcus with Lobar Pneumonia.—There
can be no doubt that the concurrent infection with
microorganisms other than pneumococcus modifies the
progress of lobar pneumonia. With lobar pneumonia alone
hemolytic streptococci have entered the bronchi in 30 per
cent of instances and have penetrated into the lungs in 20.6
per cent; with associated lobar and bronchopneumonia the
same microorganism has entered the bronchi in 34.3 per
cent of instances and invaded the lung in 31.6 per cent.
Hemolytic streptococci are the only microorganisms other
than pneumococci which, in association with lobar pneumonia,
160have found their way from the lungs to the blood
stream; more than one-third of all instances of lobar pneumonia
in which hemolytic streptococci find entrance into
the bronchi die with streptococcus septicemia.
Separation of instances of lobar pneumonia into groups
on the basis of the occurrence of red or gray hepatization
shows that infection with hemolytic streptococcus is more
likely to occur during the early stages of the disease. The
average duration of lobar pneumonia with red hepatization
has been 3.7 days, with red and gray hepatization, 5.1 days,
and with gray hepatization, 7.5 days. Infection with hemolytic
streptococcus has occurred in association with red or
gray hepatization as shown in Table XXXIII.
| Table XXXIII |
|---|
| |
|
NO. OF AUTOPSIES |
NO. WITH HEMOLYTIC STREPTOCOCCUS |
PER CENT WITH HEMOLYTIC STREPTOCOCCUS |
| Lobar pneumonia with red hepatization |
16 |
6 |
37.5 |
| Lobar pneumonia with red and gray hepatization |
28 |
6 |
21.4 |
| Lobar pneumonia with gray hepatization |
20 |
1 |
5.0 |
Notwithstanding the longer duration of the disease and
consequent prolongation of exposure to infection, lobar
pneumonia, which has reached the stage of gray hepatization,
has shown the smallest incidence of infection with
hemolytic streptococci. In the stage of gray hepatization
there is diminished susceptibility to secondary infection
with this microorganism.
Characteristic histologic changes have been found in the
lungs of those who have died with lobar pneumonia followed
by invasion of lungs and blood by hemolytic streptococci
(e. g., Autopsies 273, 430), but with no evidence of
suppuration found at autopsy. Within the pneumonic
lung occur patches of necrosis implicating both exuded
cells and alveolar walls; in some places nuclei have
disappeared; elsewhere nuclear fragments are abundant.
161In these patches of necrosis Gram-positive streptococci in
short chains occur in immense number. In some instances
(e. g., Autopsies 273, 346, 479) interlobular septa are very
edematous and often contain a network of fibrin; lymphatics
are dilated and contain polynuclear leucocytes in abundance.
Streptococci are found within these lymphatics.
The histologic changes which have been described represent
the earliest stages of abscess formation and interstitial
suppuration, lesions almost invariably caused by hemolytic
streptococci.
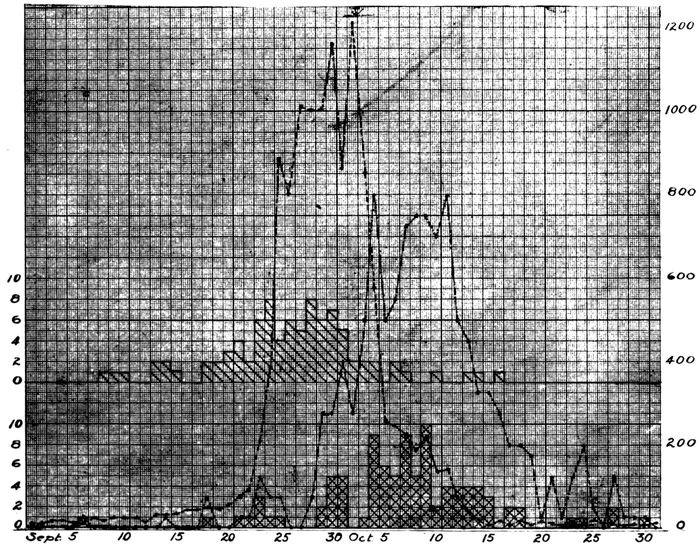
Chart 2.—Showing the relation of (a) date of onset of cases in which autopsy demonstrated lobar pneumonia, indicated by upper continuous line with single hatch, and of (b) date of death of these cases, indicated by lower continuous line with double hatch to (c) the occurrence of influenza, indicated by the broken line, and to (d) the total number of fatal cases of pneumonia, indicated by the broken dotted line. Each case of fatal pneumonia is indicated by one division of the scale as numbered on the left of the chart; cases of influenza are indicated by the numbers on the right of the chart.
Relation of Lobar Pneumonia to Influenza.—Some writers
have suggested that lobar pneumonia, heretofore observed
during the course of epidemics of influenza, is an
162independent disease with no relation to influenza, both diseases
being referable perhaps to similar meteorologic or
other conditions. Chart 2, which shows by weeks from
September 1 to October 31 the relation of deaths from lobar
pneumonia (indicated by double hatch) to deaths from all
forms of pneumonia, disproves this suggestion. The two
curves follow parallel courses; that representing lobar
pneumonia reaches a maximum approximately one week
after the outbreak of influenza had reached its height. Lobar
pneumonia, like other forms of pneumonia, was secondary
to influenza. When a chart is plotted to represent the
dates of onset of fatal cases of lobar pneumonia (indicated
by single hatch in Chart 2), it becomes evident that the
greatest number of these cases of pneumonia had their onset
at the beginning of the influenza epidemic, approximately
one week before it reached its height. Fatal lobar
pneumonia developed less frequently in the latter part of
the epidemic; to obtain an explanation of this relation it is
necessary to chart separately cases of lobar pneumonia with
secondary streptococcus infection, for we have already
learned that streptococcus infection was the predominant
cause of death in the early period of the influenza epidemic.
Exclusion of these instances of secondary streptococcus infection
makes no noteworthy change in the character of the
chart. Fatal lobar pneumonia, like all forms of fatal
pneumonia (p. 140), was more frequent in the first half
than in the second half of the epidemic. This difference
is referable either to greater virulence of the virus of
influenza or to the greater susceptibility of those first selected
by the disease or, as more probable, to conditions
such as crowding together of patients with influenza, favoring
the transmission of microorganisms which cause pneumonia.
Bronchopneumonia
For the purpose of the present study it is convenient to
group together instances of bronchopneumonia which have
163been unaccompanied, on the one hand, by lobar pneumonia
(p. 155) or, on the other hand, by suppuration, which with
few exceptions is caused by hemolytic streptococci or by
staphylococci. A group of cases in which lobar and bronchopneumonia
have occurred in the same individual have
already been considered. In many instances, bronchopneumonia
is accompanied by abscess formation or by some
other form of suppuration; these lesions will be discussed
elsewhere.
Bronchopneumonia unaccompanied by lobar pneumonia
or by suppuration occurred in 80 autopsies.
Pneumonic consolidation distributed with relation to the
bronchi exhibits considerable variety, and an attempt to
define a type of bronchopneumonia characteristic of influenza
would be futile. Nevertheless, the bronchopneumonia
of influenza has in many instances distinctive characters.
Lesions of bronchopneumonia which are frequently
found in the autopsies under consideration may be conveniently
designated by descriptive terms, indicative of
their location in the lung tissue. These lesions, of which
two or more often occur in the same lung, are:
1. Peribronchiolar consolidation with which the inflammatory
exudate is limited to the alveoli in the immediate
neighborhood of the bronchioles.
2. Hemorrhagic peribronchiolar consolidation in which
gray patches of peribronchiolar pneumonia occur upon a
deep red background produced by hemorrhage into alveoli.
Pfeiffer believed that this lesion was characteristic of influenza.
3. Lobular consolidation with which consolidation is limited
to lobules or groups of lobules.
4. Peribronchial pneumonia with which small bronchi are
encircled by pneumonic consolidation.
Each one of these lesions will be discussed separately.
Following is a list of the bacteria which have been isolated
from the consolidated lung of individuals with bronchopneumonia
164unaccompanied by lobar pneumonia or by
suppuration:
| B. influenzæ |
1 |
| Pneumococci |
5 |
| S. hemolyticus |
5 |
| S. viridans |
1 |
| B. influenzæ, pneumococci |
9 |
| B. influenzæ, S. hemolyticus |
4 |
| B. influenzæ, staphylococci |
4 |
| Pneumococci, S. hemolyticus |
1 |
| Pneumococci, staphylococci |
2 |
| S. hemolyticus, staphylococci |
1 |
| S. hemolyticus, B. coli |
1 |
| Staphylococci, S. viridans |
1 |
| Staphylococci, B. coli |
1 |
| B. influenzæ, pneumococci, staphylococci |
1 |
| B. influenzæ, pneumococci, S. viridans |
1 |
| B. influenzæ, S. hemolyticus, staphylococci |
2 |
| B. influenzæ, pneumococci, staphylococci, S. viridans |
1 |
| No microorganisms found |
6 |
| |
|
| |
47 |
The similarity of this list to that representing the bacteriology
of bronchitis is evident; there is the same multiplicity
of microorganisms and the frequent occurrence of
mixed infections. B. influenzæ is much less frequently
found in the lung. The relative pathogenicity of the large
group of microorganisms enumerated above is better indicated
by the following list which shows what microorganisms
have penetrated into the blood in autopsies performed
on individuals with bronchopneumonia:
| Pneumococci |
20 |
| S. hemolyticus |
23 |
| S. viridans |
1 |
| Pneumococci, S. hemolyticus |
2 |
| No bacteria found |
25 |
| |
|
| Total |
71 |
Table XXXIV shows the percentage incidence of pneumococcus,
hemolytic streptococcus, staphylococcus and
165B. influenzæ in the bronchi, lungs and blood and is inserted
for comparison with the similar table (Table XXX)
showing the incidence of these bacteria in lobar pneumonia.
| Table XXXIV |
|---|
| |
|
NO. OF CULTURES |
PNEUMOCOCCI |
HEMOLYTIC STREPTOCOCCI |
STAPHYLOCOCCI |
B. INFLUENZÆ |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
37 |
19 |
48.6 |
13 |
35.1 |
22 |
59.5 |
28 |
75.7 |
| Lung |
47 |
20 |
42.6 |
14 |
29.8 |
13 |
27.7 |
23 |
48.9 |
| Blood |
70 |
22 |
31.4 |
24 |
34.3 |
|
|
|
|
Table XXXIV shows that pneumococci have a less important
part in the production of broncho than of lobar pneumonia;
with lobar pneumonia this microorganism was found
in the lungs in 77.3 per cent of instances and in the blood, in
65.5 per cent, whereas with bronchopneumonia it was found
in the lungs in 42.6 per cent and in the blood in 31.4 per cent.
Hemolytic streptococci (in lungs and blood) and staphylococci
(in lungs), on the contrary, were more common with
bronchopneumonia, and doubtless have a part in the production
of the lesion. Streptococcus viridans, B. coli and
M. catarrhalis, which are not infrequently found in the
bronchi (p. 151), occasionally enter the lungs with bronchopneumonia
but are rarely found with lobar pneumonia.
B. influenzæ has been found in less than 80 per cent of
instances in the bronchi and in about half of the lungs,
maintaining an incidence approximately the same as that
with lobar pneumonia.
Table XXXV shows the types of pneumococci found in
association with bronchopneumonia and is inserted for
comparison with the similar table (Table XXXII) showing
types of pneumococci with lobar pneumonia.
With broncho as with lobar pneumonia pneumococci commonly
found in the mouth, namely, atypical II, and Types
III and IV, have a more important part in production of the
lesion than the so-called fixed types, I and II. Atypical
Pneumococcus II has been less frequently encountered with
broncho than with lobar pneumonia.
166
| Table XXXV |
|---|
| |
|
NO. OF CULTURES |
PNEUMOCOCCUS I |
PNEUMOCOCCUS II |
PNEUMOCOCCUS II (Atyp.) |
PNEUMOCOCCUS III |
PNEUMOCOCCUS IV |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
37 |
1 |
2.7 |
3 |
8.1 |
|
|
|
|
14 |
37.8 |
| Lung |
47 |
2 |
4.3 |
2 |
4.3 |
2 |
4.3 |
2 |
4.3 |
12 |
25.2 |
| Blood |
70 |
1 |
1.4 |
1 |
1.4 |
5 |
7.1 |
4 |
5.7 |
11 |
15.9 |
Peribronchiolar Consolidation.—In many instances of
bronchopneumonia, usually in association with lobular or
confluent consolidation, small firm nodules of consolidation
are clustered about the bronchioles (Fig. 2). These nodular
foci of consolidation are usually 1.5 to 2 mm. in diameter,
being sometimes slightly smaller or slightly larger.
They are usually gray and occasionally surrounded by a
red halo; sometimes they are yellowish gray. They are
clustered about the smallest bronchial tubes to form groups
which are from 0.5 to 1 cm. across. A group of nodular
foci of consolidation occupies the central part of a lobule of
lung tissue. When pneumonia has been of short duration
these foci are fairly soft and not sharply defined, and in
many instances this form of bronchopneumonia is first recognized
by microscopic examination. When the disease has
lasted from ten days to two weeks, the consolidated nodules
are very firm and sharply circumscribed, closely resembling
tubercles. When they have assumed this character,
microscopic examination shows that chronic changes indicated
by new formation of interstitial tissue have occurred.
The lesion may be designated peribronchiolar consolidation.
It has occurred usually in association with other types
of pneumonic lesion in 61 instances, being recognized at
autopsy in 18 and by microscopic examination in 43.
167
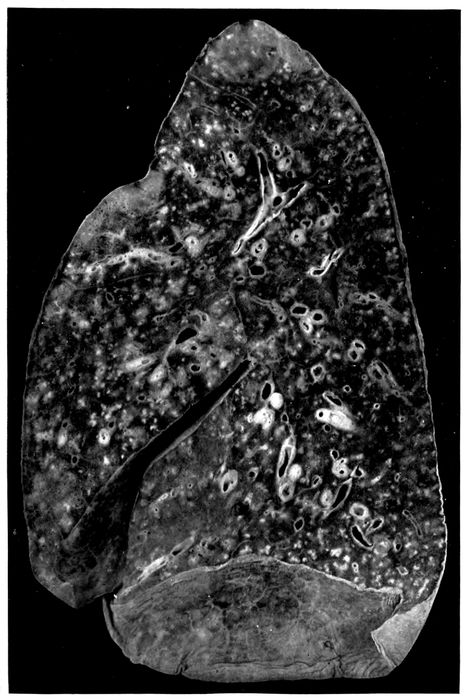
Fig. 2.—Acute bronchopneumonia with nodules of peribronchiolar consolidation and purulent bronchitis. Autopsy 429.
168In association with this lesion there are almost invariably
severe lesions of the bronchi. Purulent bronchitis was
noted in 47 of the 61 instances, in which this nodular bronchopneumonia
was found at autopsy. An index of the severity
of the bronchial injury is the frequency with which
bronchiectasis has occurred; dilatation of small bronchi
was observed in 24 instances. In 10 instances the bronchi
were encircled by conspicuous zones of hemorrhage.
In association with this peribronchiolar lesion the lung is
often voluminous and fails to collapse on removal from the
chest. Pressure upon the lung squeezes from the smallest
bronchi, both in the neighborhood of the nodular consolidation
and elsewhere, a droplet of viscid, semifluid mucopurulent
material. The presence of this tenacious material
throughout the small bronchi doubtless explains the failure
of the lung tissue to collapse. Interstitial emphysema has
been present in some of these lungs.
A red zone of hemorrhage has occasionally been observed
about the foci of peribronchiolar pneumonia. A further
stage in the same process is represented by hemorrhage
into all of the alveoli separating these patches of consolidation.
This hemorrhagic lesion, which will be described in
more detail later, has been found repeatedly in the same
lung with peribronchiolar pneumonia, being present in 8
among the 61 autopsies cited. Lobular bronchopneumonia
accompanied the peribronchiolar lesion 27 times and lobar
pneumonia accompanied it 20 times.
When an abscess caused by hemolytic streptococcus is
associated with peribronchiolar pneumonia, empyema is
present, but otherwise pleurisy is absent or limited to a
scant fibrinous exudate.
169
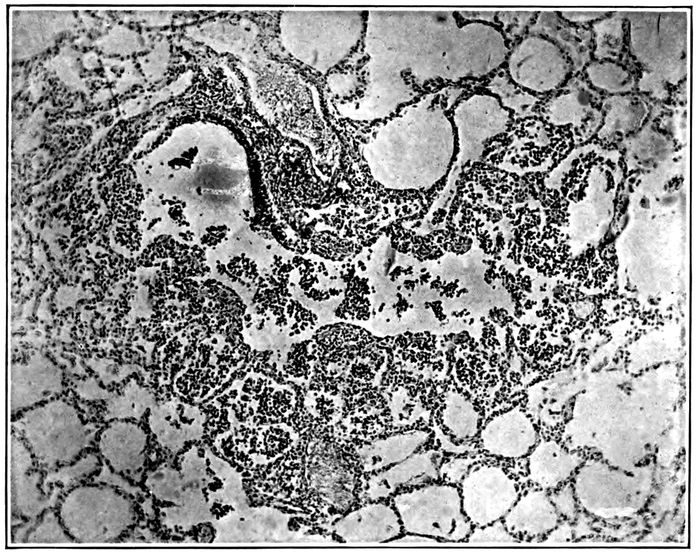
Fig. 3.—Acute bronchopneumonia with peribronchiolar consolidation; a respiratory bronchiole partially lined by columnar epithelium passes into alveolar duct and the adjacent alveoli are filled by polynuclear leucocytes. Autopsy 333.
Histologic examination demonstrates very clearly the relation
of this lesion to the bronchioles (Fig. 3). These
passages are filled and distended with an inflammatory exudate
consisting almost entirely of polynuclear leucocytes.
The respiratory bronchioles are beset with alveoli often
limited to one side of the tubule and these alveoli are filled
with leucocytes. The alveolar ducts, distinguishable from
the bronchioles by the absence of columnar or cubical epithelium
and by possession of smooth muscle, are similarly
filled with leucocytes; the numerous alveoli which form the
walls of the alveolar ducts are distended by an inflammatory
exudate. In sections which pass through an alveolar
duct and one or more of its infundibula, the further extension
of the lesion may be determined (Fig. 4). The infundibulum
in proximity with the alveolar duct contains polynuclear
leucocytes and the same cells are seen in the alveoli
which here form its wall, but the intensity of the inflammatory
reaction diminishes toward the periphery, so that the
distal part of the infundibulum, which is much distended
170and in consequence more readily definable than usual, is
free from inflammatory exudate.
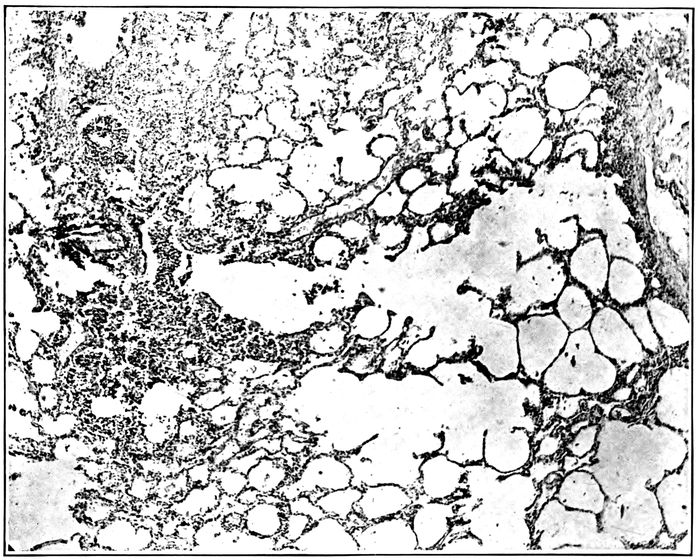
Fig. 4.—Acute bronchopneumonia with peribronchiolar consolidation; a respiratory bronchiole is in continuity with an alveolar duct and two distended infundibula; alveoli about bronchiole, alveolar duct and proximal part of infundibula contain polynuclear leucocytes, the distal part of the infundibula showing no evidence of inflammation. Autopsy 333.
Occasionally there is irregularly distributed hemorrhage
and perhaps some edema in the alveoli immediately adjacent
to those which form the peribronchiolar focus of inflammation.
In such instances small bronchi, that is, air
passages, lined by columnar epithelium and devoid of tributary
alveoli, may be surrounded by a zone of hemorrhage;
immediately surrounding the bronchus, the wall of which
shows intense inflammation, alveoli, in a zone of which the
radius represents several alveoli, are filled with blood. This
hemorrhagic zone is continued from the bronchus over the
focus of inflammation which surrounds the bronchiole.
171Another variation in the character of the lesion is doubtless
referable to variation in the severity of primary bronchial
injury. Alveoli immediately surrounding small bronchi
are filled with dense plugs of fibrin. The alveoli which
besot the walls of the bronchioles contain fibrin, but the
alveolar duct and its tributary alveoli are filled with polynuclear
leucocytes.
The bacteria which have been cultivated from the lung in
autopsies with peribronchiolar pneumonia are as follows:
| Pneumococcus |
5 |
| S. hemolyticus |
8 |
| B. influenzæ, pneumococcus |
5 |
| B influenzæ, S. hemolyticus |
7 |
| B. influenzæ, staphylococcus |
1 |
| Pneumococcus, staphylococcus |
2 |
| S. hemolyticus, staphylococcus |
2 |
| B. influenzæ, pneumococcus, S. hemolyticus |
2 |
| B. influenzæ, pneumococcus, staphylococcus |
1 |
| B. influenzæ, S. hemolyticus, staphylococcus |
2 |
| Pneumococcus, S. hemolyticus, staphylococcus |
3 |
| No organism |
3 |
| |
|
| Total |
41 |
The following list which shows the bacteria found in the
blood is an index to the pathogenicity of pneumococci and
hemolytic streptococci:
| Pneumococcus |
22 |
| S. hemolyticus |
20 |
| Pneumococcus, S. hemolyticus |
1 |
| No organism |
14 |
| |
|
| Total |
57 |
The percentage incidence of pneumococcus, hemolytic
streptococcus, staphylococcus and B. influenzæ in bronchus,
lung and blood, given in Table XXXVI, is inserted to
indicate with what readiness each one of these microorganisms
passes from the bronchus through the lung into the
circulating blood.
| 172 |
| Table XXXVI |
|---|
| |
|
PNEUMOCOCCUS |
HEMOLYTIC STREPTOCOCCUS |
STAPHYLOCOCCUS |
B. INFLUENZA |
| Bronchus |
39.4% |
57.7% |
60.6% |
84.8% |
| Lung |
43.9% |
61.0% |
21.9% |
43.9% |
| Blood |
40.3% |
36.8% |
0. % |
0. % |
B. influenzæ is present in the bronchi in a very large proportion
(84.8 per cent) of those in whom this type of bronchopneumonia
has been found at autopsy; it is much less
frequently recovered from the lungs. Staphylococci, in
part S. albus and in part S. aureus, are less frequently
found in the bronchi and are recovered from the lungs in a
relatively small proportion of autopsies. The percentage
incidence of pneumococci and streptococci in lungs and
blood demonstrates the pathogenicity of these microorganisms,
for whereas pneumococci and hemolytic streptococci
are found in the consolidated lungs in 43.9 and 61.0 per
cent of instances of the lesion respectively, they make their
way into the blood in 40.3 and 36.8 per cent of instances.
Coexisting infection with pneumococci and hemolytic
streptococci has been not uncommon e. g., Autopsy 275 in
which both were in the blood; in 2 instances (Autopsies 333
and 378) in which pneumococci were obtained from the
blood, hemolytic streptococci were found in the lungs and
bronchi; in 3 instances (Autopsies 258, 273 and 445) in
which hemolytic streptococci were present in the blood,
pneumococci were obtained from the lungs.
In the group of autopsies under consideration, examination
of the sputum was made during life and after onset of
pneumonia in 11 instances. The microorganisms found in
the sputum and at autopsy were as follows:
|
|
SPUTUM |
IN BLOOD, LUNGS OR BRONCHUS AT AUTOPSY |
| Autopsy |
240 |
Pneum. IV |
Pneum. IV |
| |
246 |
Pneum. atyp. II, B. inf. |
|
| |
247 |
Pneum. IV, B. inf. |
Pneum. IV |
| |
250 |
Pneum. atyp. II, B. inf. |
Pneum. atyp. II |
| |
253 |
Pneum. atyp. II |
Pneum. II |
| |
285 |
Pneum. atyp. II, B. Inf. |
S. hem., B. inf. |
| |
288 |
S. hem., B. inf. |
S. hem., B. inf. |
| 173 |
291 |
Pneum. IV, B. inf. |
Staph., B. inf. |
| |
300 |
Pneum. atyp. II, B. inf. |
Pneum. atyp. II, B. inf. |
| |
312 |
Pneum. IV, S. hem., B. inf. |
S. hem., B. inf. |
| |
346 |
Pneum. IV, B. inf. |
S. hem., B. inf. |
In 2 instances (Autopsies 285 and 346) among this small
group of cases, pneumococci but no hemolytic streptococci
were found in the sputum several days before death,
whereas death occurred as the result of secondary invasion
with hemolytic streptococci and no pneumococci were found
at autopsy. It is probable that this sequence of events is
not uncommon. B. influenzæ finds its way into the bronchi
and pneumococci follow it; pneumonia limited to peribronchiolar
alveoli may occur in consequence of this invasion.
Later hemolytic streptococci may follow the same path and
cause death with bacteremia.
Hemorrhagic Peribronchiolar Consolidation.—Peribronchiolar
pneumonia accompanied by diffuse accumulation
of blood within the alveoli is one of the most frequent complications
of influenza. The lung tissue is laxly consolidated,
and on section there is a homogeneous dull deep red
background upon which are seen small gray spots (1.5 to 2
mm. in diameter) grouped in clusters about the smallest
bronchi (Fig. 5). Wide areas of lung tissue are implicated
and the lesion is more common in the dependent parts of
the lung than elsewhere. In common with other forms of
bronchopneumonia the lesion is in most instances associated
with changes in the bronchi; in 55 instances of hemorrhagic
bronchiolar pneumonia purulent bronchitis was
found in 43 instances; it is noteworthy that purulent bronchitis
often is not evident in the presence of pulmonary
edema and edema is not infrequent with this pneumonic
lesion.
Microscopic examination demonstrates the presence of
acute bronchitis; the lumina of the small bronchi contain
polynuclear leucocytes and red blood corpuscles. Accumulation
of blood may separate the epithelium from the basement
174membrane. The mucosa immediately below the epithelium
contains polynuclear leucocytes in fair abundance
and the blood vessels of the bronchial wall are much engorged.
Respiratory bronchioles are distended with polynuclear
leucocytes and red blood corpuscles. In a zone
about each bronchiole, in areas corresponding to the small
gray spots seen upon the cut surface of the lung, the alveoli
are filled with polynuclear leucocytes. In the lung tissue
intervening between these spots of leucocytic pneumonia
the alveoli are distended with red blood corpuscles.
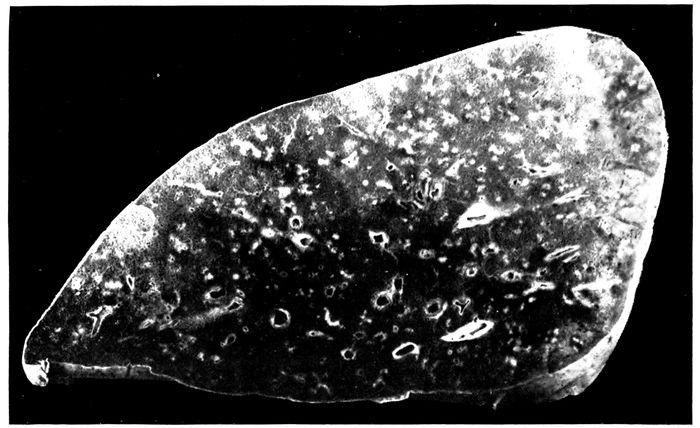
Fig. 5.—Bronchopneumonia with hemorrhagic peribronchiolar consolidation.
In favorable sections it is occasionally possible to follow
the bronchiole and alveolar duct, both filled with leucocytes,
into an infundibulum. The proximal part of the infundibulum
contains polynuclear leucocytes, whereas the
distal part and its tributary alveoli are filled with serum
and red blood corpuscles.
When the lesion has persisted for a short time there is
evidence of beginning migration of polynuclear leucocytes
from the blood vessels into the alveoli which are filled with
175blood. The alveolar walls contain numerous polynuclear
leucocytes and leucocytes which have entered the intraalveolar
blood are numerous in contact with the wall but occur
in scant number in the center of the alveolar lumen.
Alveolar epithelium in contact with the blood in the lumen
is usually swollen and often uniformly nucleated.
The inflammatory process is evidently transmitted from
the bronchioles and to a less degree from the small bronchi
to the adjacent alveoli. Polynuclear leucocytes fill the lumen
of the bronchiole and the alveoli immediately adjacent;
at the periphery of the focus of pneumonia, the alveoli
may contain fibrin. In such instances small bronchi
(lined by a continuous layer of columnar epithelial cells)
may be surrounded by alveoli containing fibrin.
In sections from one part of the lung, the alveoli between
the peribronchiolar foci of pneumonia may be uniformly
filled with red blood corpuscles, whereas in sections from
another part pneumonic foci may be surrounded by a zone
of intraalveolar hemorrhage or of hemorrhage and edema
outside of which some air-containing tissue occurs. There
are transitions between this halo of intraalveolar hemorrhage
and edema surrounding each bronchiolar focus and
complete hemorrhagic infiltration of all intervening alveoli.
Large mononuclear cells are occasionally fairly numerous
within the alveoli containing blood. These cells act as
phagocytes ingesting red corpuscles, so that at times they
are filled with corpuscles. Disintegration of red corpuscles
occurs and brown pigment remains within the cell. It is
not uncommon to find numerous mononuclear pigment containing
cells which resemble those found with chronic passive
congestion of the lungs.
Lungs, the site of hemorrhagic peribronchiolar pneumonia,
may undergo chronic changes which will be described
elsewhere.
The lesion which has been designated hemorrhagic peribronchiolar
pneumonia is that which Pfeiffer regarded as
176the characteristic type of influenzal pneumonia. In the
small bronchi containing pus and in lung tissue, Pfeiffer
states, influenza bacilli are predominant and present in astonishing
number in smear preparations. The demonstration
of B. influenzæ by cultures from pneumonic lung is
mentioned by him but its association with other microorganisms
in such cultures is not discussed.
Microorganisms which we have isolated from the lungs
of individuals with hemorrhagic peribronchiolar pneumonia
are as follows:
| B. influenzæ |
1 |
| Pneumococcus |
2 |
| S. hemolyticus |
10 |
| B. influenzæ, pneumococcus |
7 |
| B. influenzæ, S. hemolyticus |
3 |
| B. influenzæ, staphylococcus |
2 |
| S. hemolyticus, B. coli |
3 |
| B. influenzæ, pneumococcus, staphylococcus |
2 |
| B. influenzæ, S. hemolyticus, staphylococcus |
5 |
| Pneumococcus, S. hemolyticus, staphylococcus |
1 |
| No organisms |
2 |
| |
|
| Total |
38 |
With this type of pneumonia B. influenzæ has not been
isolated in pure culture; B. influenzæ alone is recorded only
once (Autopsy 435), but in this instance the culture has
been so obscured by contamination that the occurrence of
pneumococci or streptococci cannot be excluded; S. hemolyticus
has doubtless been present in this lung, for it has
been found in the heart’s blood, in the bronchus, and in the
peritoneal exudate of the same individual.
The incidence of pneumococci and hemolytic streptococci
in this list does not differ materially from that with peribronchiolar
pneumonia unaccompanied by extensive intraalveolar
hemorrhage, though hemolytic streptococci are
somewhat more frequent with the hemorrhagic lesion. The
following table shows the frequency with which pneumococci
and hemolytic streptococci have penetrated into the
blood:
| 177 |
| Pneumococcus |
11 |
| S. hemolyticus |
24 |
| Pneumococcus, S. hemolyticus |
1 |
| No organism |
12 |
| |
|
| Total |
48 |
Table XXXVII showing the percentage incidence of
pneumococci, hemolytic streptococci, staphylococci and B.
influenzæ further emphasizes the similarity between the
bacteriology of peribronchiolar pneumonia (Table XXXVI)
and the closely related hemorrhagic lesion:
| Table XXXVII |
|---|
| |
|
PNEUMOCOCCUS |
HEMOLYTIC STREPTOCOCCUS |
STAPHYLOCOCCUS |
B. INFLUENZÆ |
| Bronchus |
44.0% |
64.0% |
44.0% |
72.0% |
| Lung |
31.6% |
57.9% |
26.8% |
52.6% |
| Blood of heart |
25.0% |
52.1% |
0% |
0% |
Pneumococci have been found in the lungs (31.6 per
cent) and blood (25 per cent), somewhat less frequently
than with peribronchiolar pneumonia (43.9 and 40.3 per
cent respectively), and hemolytic streptococci have been
found in the blood more frequently (52.1 per cent) than
with the latter (36.8 per cent) but otherwise the bacteriology
of the two lesions corresponds closely. The low incidence
of B. influenzæ in the bronchi (72 per cent) with hemorrhagic
peribronchiolar pneumonia is perhaps incorrect
as the result of the relatively small number of bacteriologic
examinations (namely, 25), but the incidence of the same
microorganism in the lung has been higher (52.6 per cent)
than with nonhemorrhagic peribronchiolar lesion (43.9 per
cent).
In some instances infection with hemolytic streptococci
has occurred after the onset of pneumonia. The following
list compares the results of bacteriologic examination of
the sputum made after the onset of pneumonia with that of
blood, lungs or bronchus after death:
| 178 |
|
|
SPUTUM |
IN BLOOD, LUNGS OR BRONCHUS AT AUTOPSY |
| Autopsy |
237 |
S. hem. |
S. hem. |
| |
242 |
Pneum. atyp. II, B. inf. |
Pneum. atyp. II |
| |
247 |
Pneum. IV, B. inf. |
Pneum. IV |
| |
266 |
S. hem. |
S. hem., B. inf. |
| |
346 |
Pneum. IV, B. inf. |
S. hem., B. inf. |
| |
376 |
(No. S. hem.) |
S. hem., staph., B. inf. |
Instances of secondary infection with hemolytic streptococcus
occur in the list, namely, Autopsies 346 and 376.
From the foregoing studies of the bacteriology of peribronchiolar
and hemorrhagic peribronchiolar pneumonia
the following conclusions may be drawn: (a) B. influenzæ
is found in most instances of these lesions in the bronchi
and in about half of all instances in the lungs, but does not
occur unaccompanied by other microorganisms. (b) In a
considerable number of autopsies pneumococcus is the only
microorganism that accompanies B. influenzæ; from the
lungs it penetrates into the blood from which it is obtained
in pure culture. (c) In a considerable number of instances
S. hemolyticus accompanies B. influenzæ, and in some of
these instances (representing a large proportion of the relatively
small number of cases examined during life), examination
of the sputum has demonstrated that infection has
been secondary to a pneumonia with which no hemolytic
streptococci have been found in the sputum.
Lobular Consolidation.—Consolidation of scattered lobules
or groups of lobules has occurred in nearly all instances,
namely, 71 of 80 autopsies with bronchopneumonia
unaccompanied by lobar pneumonia or by suppuration.
When death follows shortly after the onset of pneumonia,
patches of consolidation have a dull deep red color; blood-tinged
fluid escapes from the cut surface which is almost
homogeneous or finely granular. The consolidated tissue
seen through the pleura, which is raised above the general
level, has a bluish red color. Isolated lobules or groups of
lobules which have undergone consolidation may be scattered
throughout the lungs, but not infrequently there is
confluent consolidation of the greater part of lobes, of
179whole lobes or of almost an entire lung. Such lungs are
very heavy and may weigh 1,400 or 1,500 grams; bloody
serous fluid exudes from the cut surface. The lesion resembles
the red hepatization of lobar pneumonia, but confluent
patches of pneumonia are usually well defined by lobule
boundaries. The tissue is soft and the granulation of lobar
pneumonia is absent. In many instances the lobular or confluent
areas of consolidation are reddish gray; in some instances
consolidated tissue is in places red and elsewhere
gray, and in a smaller group of autopsies there is gray
consolidation only (Fig. 6). Red lobular consolidation is
often seen in those who have died within the first four days
following the onset of pneumonia, but is almost equally frequent
after from five to ten days; the average duration of
pneumonia in these cases was 5.5 days. Combined red and
gray consolidation was more frequently found when pneumonia
had lasted more than five days, the average duration
of pneumonia being 7.3 days. The greater number of instances
of gray consolidation were found after seven days
of pneumonia, the average duration of the disease being
10.0 days. These figures are cited to show that lobular,
like lobar, consolidation passes gradually from a stage of
red to gray hepatization, but the change occurs more slowly
and is often long delayed.
Lobular pneumonia, which occurred 71 times among 80
cases classified as bronchopneumonia, may be regarded as
an almost constant lesion of the disease. It is found not
only in association with other lesions of bronchopneumonia,
but with lobar pneumonia of influenza as well.
The bacteriology of this lesion shows no deviation from
that of the slightly larger group of bronchopneumonia
(p. 163). All types of pneumococcus have been found in
association with the lesion, Pneumococcus I in 2 instances,
Pneumococcus II in 1 instance; atypical Pneumococcus II
and Pneumococcus IV have been found much more frequently.
Pneumococci have been found in more than a
third of these autopsies (42.9 per cent in the lungs, 33.3 per
cent in the blood); hemolytic streptococci in less than one-third
(28.5 per cent in the lungs, 30.2 per cent in the blood).
180
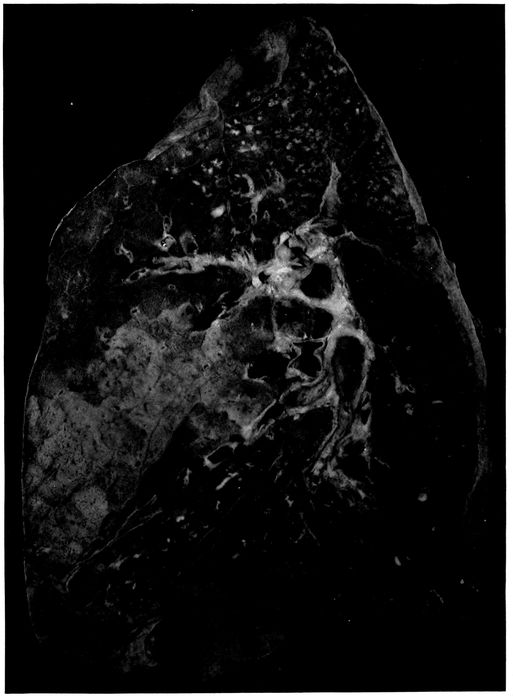
Fig. 6.—Acute bronchopneumonia with confluent gray lobular consolidation in lower part of upper lobe and hemorrhagic peribronchiolar pneumonia in lower lobe; purulent bronchitis.
181The following list shows the bacteriology of a small
group of autopsies in which the sputum was examined after
onset of pneumonia:
|
|
SPUTUM |
BLOOD, LUNGS OR BRONCHUS AT AUTOPSY |
| Autopsy |
233 |
Pneum. atyp. II |
Pneum. |
| |
237 |
S. hem. |
S. hem. |
| |
242 |
Pneum. atyp. II, B. inf. |
Pneum. atyp. II |
| |
250 |
Pneum. atyp. II, B. inf. |
Pneum. atyp. II |
| |
253 |
Pneum. atyp. II |
Pneum. atyp. II, staph., B. inf. |
| |
266 |
S. hem. |
S. hem., B. inf. |
| |
274 |
Pneum. IV |
S. hem. |
| |
291 |
Pneum. IV, B. inf. |
Staph., B. inf. |
| |
312 |
Pneum. IV, S. hem., B. inf. |
S. hem., staph., B. inf. |
In one instance of streptococcus pneumonia (Autopsy
274) infection with streptococci occurred subsequent to the
examination of the sputum made five days before death;
pneumococcus was found in the washed sputum.
With lobar pneumonia there was evidence that superimposed
infection occurred more frequently during the stage
of red than of gray hepatization. With the lobular consolidation
of bronchopneumonia this relation has not been
found. Among 27 instances of red lobular consolidation,
hemolytic streptococcus has occurred 6 times, namely in
22.2 per cent; among 26 instances of red and gray consolidation,
8 times, namely, in 30.7 per cent; among 13 instances
of gray consolidation, 5 times, namely, in 38.5 per
cent. Infection with hemolytic streptococci is more frequent
when the lesion has persisted to the stage of gray
hepatization. This difference between lobar and bronchopneumonia
is probably dependent in part at least upon the
more severe and persistent lesions of the bronchi with
bronchopneumonia.
The histology of consolidation which is definitely limited
to secondary lobules or groups of lobules varies considerably.
When death occurs in the early stage of the lesion,
182consolidated patches are deep red and somewhat edematous,
so that bloody serous fluid escapes from the cut surface
of the lung and red blood corpuscles are present in the
alveoli in great abundance together with polynuclear leucocytes,
fibrin and serum in varying quantity. It is not
uncommon to find evidence that the lesion has had its origin
in the bronchioles and extended from them to other
parts of the lobule. Polynuclear leucocytes may be relatively
abundant within and immediately about the bronchioles
and alveolar ducts, whereas the intervening alveoli and
infundibula are filled with red blood corpuscles among
which are polynuclear leucocytes and perhaps some fibrin.
It may be evident that bronchiolar pneumonia with hemorrhage
into intervening alveoli is in process of transformation
into a more diffuse leucocytic pneumonia, for polynuclear
leucocytes are making their way from the alveolar
wall into the blood-filled lumen and, as the result of the
presence of blood, remain for a time close to the lining of
the alveolus.
When the consolidated lobules have assumed a gray or
reddish gray color, polynuclear leucocytes are more abundant
and often almost homogeneously pack every alveolus
within the boundaries of the lobule. In some instances
there is fibrin partially obscured by the presence of leucocytes
in great number.
Although fibrin is less abundant with bronchopneumonia
than with lobar pneumonia, nevertheless in a considerable
proportion of instances it is a very conspicuous element
of the inflammatory exudate within the bronchioles, alveolar
ducts and alveoli. It is unusual to find the alveolar
ducts and alveoli uniformly plugged with fibrin containing
leucocytes; there is a variegated distribution of exudate
which has little resemblance to that of lobar pneumonia.
Occasionally (Autopsies 242 and 247) polynuclear leucocytes
fill the bronchioles, alveolar ducts and infundibula,
whereas the surrounding tributary alveoli contain fibrin
183and polynuclear leucocytes in moderate number; red blood
corpuscles may be present in sufficient number to give a
homogeneously red color to the lobular consolidation.
In association with lobular pneumonia, fibrin within the
lung tissue undergoes certain changes which outline very
sharply the alveolar ducts and the other structures usually
ill defined in preparations of the lung. A remarkable appearance
is produced by the deposit of hyalin fibrin upon
the surface of the alveolar ducts and infundibula. This
lesion has been described by LeCount.
Within the alveolar tissue of the lung, spaces are seen
lined by a layer of fibrin which stains homogeneously and
very brightly with eosin. They are recognized as alveolar
ducts by the presence of scattered bundles of smooth
muscle in their wall. The layer of hyaline fibrin overlying
the surface of the alveolar duct usually forms a continuous
lining and covers over the orifices of the alveoli which surround
the alveolar duct. These ducts are rendered still
more conspicuous by the character of their contents which
exhibits a sharp contrast with that of the surrounding
alveoli. The alveoli duct occasionally contains a bubble of
air, but more frequently it is filled with serum in which red
blood corpuscles are sometimes numerous. There is within
the lumen scant fibrin and very few cells, among which polynuclear
leucocytes are predominant. In the surrounding
alveoli on the contrary leucocytes and fibrin are abundant.
A similar change is found in the infundibula very clearly
defined by their conical form, which is especially well outlined
below the pleura or in contact with interlobular septa.
The infundibulum is outlined by hyaline fibrin which passes
over the orifices of the tributary alveoli and separates the
serous contents of the infundibulum from the cellular fibrinous
contents of the alveoli about.
The lesion which has been described is often associated
with acute bronchitis and bronchiolitis, and the alveoli immediately
about the respiratory bronchioles may be filled
184with polynuclear leucocytes. It is very common to find
large bubbles of air sharply defined within the purulent
contents of the bronchiole. In some lobules the alveolar
ducts, infundibula and alveoli intervening between
these foci of leucocytic pneumonia are almost uniformly
filled with fibrin and polynuclear leucocytes, but in other
places the formation of complete layers of hyaline fibrin
is in process. Bubbles of air are often seen within the alveolar
ducts, and about them is an irregular layer of fibrin
formed by the penetration of air into a channel previously
filled with a loose network of fibrin containing serum in its
meshes. The fibrin compressed against the walls of alveolar
duct and infundibulum remains as a compact layer separating
these structures from the alveoli which project
from their walls. The bubble of air is doubtless later absorbed
and replaced by serum, so that many alveolar ducts
are filled with serum almost wholly free from cells, whereas
alveoli outside the fibrinous membrane contain a network
of fibrin with leucocytes in greater or less abundance.
In association with this fibrinous pneumonia, which has
been described, hyaline thrombosis of the capillaries is not
uncommon. This hyalin material within the capillaries
gives reactions of fibrin, and in sections stained by the
Gram-Weigert method for demonstration of fibrin, these
thrombosed vessels have the appearance of capillaries irregularly
injected with a blue material.
The interstitial tissue surrounding consolidated lobules
is often edematous; the lymphatics are distended with
serum and contain a moderate number of lymphocytes and
polynuclear leucocytes.
Among the lungs which have been studied histologically,
pneumococcus has been almost invariably associated with
the lobular lesions which have just been described, whether
hemorrhagic, leucocytic or fibrinous; the histologic changes
accompanying infection of the lung with streptococcus will
be described later. Pneumococcus has been cultivated from
the consolidated lung and is found in section of the lung.
B. influenzæ is found in cultures made from the bronchi.
Table XXXVIII includes those instances in which the
histology of the consolidated lung accords with the description
given above.
| 185 |
| Table XXXVIII |
|---|
| |
| NO. OF AUTOPSY |
CHARACTER OF LOBULAR CONSOLIDATION |
PREDOMINANT TYPE OF INFLAMMATORY EXUDATE |
CULTURE FROM HEART’S BLOOD |
CULTURE FROM LUNG |
CULTURE FROM BRONCHUS |
| 242 |
Red |
Fibrinous |
Pneum. atyp. II |
|
|
| 244 |
Red |
Leucocytic and hemorrhagic |
|
Pneum. IV B. inf. |
Pneum. IV, B. inf. |
| 247 |
Red and gray |
Fibrinous |
Pneum. IV |
|
|
| 249 |
Red and gray |
Fibrinous |
Pneum. III |
|
|
| 252 |
Red and gray |
Fibrinous |
|
Pneum. II B. inf. |
Pneum. II, B. inf., S. vir. |
| 257 |
Red and gray |
Leucocytic |
Pneum. I |
|
B. inf., staph. |
| 303 |
Red |
Fibrinous |
|
Pneum. IV B. inf. |
Pneum. IV, B. inf., staph. |
| 314 |
? |
Fibrinous |
Pneum. IV |
Pneum. IV |
Pneum. IV, B. inf., staph. |
| 336 |
Red |
Fibrinous |
|
|
|
| 395 |
Red and gray |
Leucocytic |
Pneum. atyp. II |
Pneum. atyp. II |
|
| 464 |
Red |
Leucocytic and hemorrhagic |
|
Pneum. I B. inf. |
Pneum. I, B. inf., staph. |
| 476 |
Red |
Leucocytic and hemorrhagic |
|
|
|
| 498 |
Red and gray |
Fibrinous |
|
S. aur. |
|
| 506 |
Red |
Fibrinous |
Pneum. IV |
Pneum. IV S. aur. |
Pneum. IV, B. inf., S. aur., M. catarrh |
186Pneumococcus was found in all but 2 instances, and in
one of these (Autopsy 336) the only culture was from the
heart’s blood and in the other (Autopsy 498) cultures were
unsatisfactory because proper media were not obtainable.
Pneumococci of Types I, II, II atypical, III and IV are represented
in the list. B. influenzæ has been found in a considerable
number of instances in which cultures have been
made from the lung and in every instance in which cultures
have been made from the bronchi. Staphylococci are often
found in the bronchi, but in most instances they do not
penetrate into the lung.
Another group of cases of lobular pneumonia are important
because in association with necrosis of lung tissue
recognized by the microscope hemolytic streptococci have
been found in the lungs. In such instances serum is abundant
and polynuclear leucocytes are relatively scant
though their distribution varies considerably; in some
places leucocytes are fairly abundant though elsewhere almost
absent, but this distribution bears no obvious relation
to the bronchioles. In some instances (Autopsies 274 and
487) red blood corpuscles are numerous but in others (Autopsies
275 and 312) they are inconspicuous. The characteristic
feature of the lesion is the occurrence of patches
of necrosis within which the nuclei both of exudate and of
alveolar walls have partially or completely disappeared.
In these areas of necrosis short chains of streptococci are
found in immense number whereas in living tissue they are
present in moderate number. There has been a relatively
inactive inflammatory reaction, great proliferation of
streptococci and necrosis of invaded tissue. The bacteriology
of instances of lobular pneumonia with necrosis is
shown in Table XXXIX.
| 187 |
| Table XXXIX |
|---|
| |
| NO. OF AUTOPSY |
CHARACTER OF LOBULAR CONSOLIDATION |
PREDOMINANT TYPE OF INFLAMMATORY EXUDATE |
CULTURE FROM HEART’S BLOOD |
CULTURE FROM LUNG |
CULTURE FROM BRONCHUS |
| 274 |
Red |
Leucocytic and hemorrhagic |
S. hem. |
S. hem. |
S. hem., staph. |
| 275 |
Red and gray |
Leucocytic |
Pneum. IV S. hem. |
S. hem., B. inf., staph. |
S. hem., B. inf., staph. |
| 312 |
Red and gray |
Leucocytic |
S. hem. |
S. hem., B. inf. |
S. hem., B. inf., staph. |
| 478 |
Red |
Leucocytic and hemorrhagic |
S. hem. |
S. hem. |
|
188Lobular pneumonia, in some of these instances at least,
has been caused primarily by pneumococci; necrosis has
been the result of secondary invasion by streptococci. In
Autopsy 275 Pneumococcus IV has been obtained from the
blood, but in the presence of streptococci has presumably
disappeared from the lung and bronchus. In the case represented
by Autopsy 274, Pneumococcus IV has been found
in the sputum five days before death at the onset of pneumonia,
but at this time no hemolytic streptococci have been
found. In the case represented by Autopsy 312, Pneumococcus
IV, B. influenzæ and a few colonies of hemolytic
streptococci have been obtained from the sputum two days
after recognition of pneumonia and five days before death.
The hemorrhagic and edematous consolidation of the
early pulmonary lesions of influenzal pneumonia is their
most distinctive feature. Red confluent lobular pneumonia
is frequently found in those who have died within the first
week following the onset of influenza. The lungs are voluminous
and heavy and may weigh as much as 1,500 grams;
the pleura which overlies the consolidated area is blue or
plum colored and usually shows scant if any evidence of
pleurisy. Scattered patches of consolidation are accurately
limited to lobules, but in addition there are large
areas often involving the greater part of the lobes and not
infrequently situated in the lowermost part of the lower
lobes. This confluent consolidation may be obviously limited
by lobule boundaries. The consolidated tissue is deep
red and laxly consolidated; red serous fluid escapes from
the cut surface. The lesion not infrequently occurs in association
with hemorrhagic peribronchiolar pneumonia.
The histology of this confluent lesion has been studied
in Autopsies 242, 244, 303, 336, 464, 474 and 506. The histology
varies, because, in some instances, leucocytes, in
other instances, fibrin, is abundant, but the presence of red
blood corpuscles in large number within the alveoli gives
a red color to the consolidated tissue. In these cases pneumococci,
189associated in the lungs or in the bronchi with B.
influenzæ, have been the cause of pneumonia. In two autopsies
studied histologically (Autopsies 274 and 478) there
was red lobular and confluent pneumonia and the blood and
lungs contain hemolytic streptococci demonstrated by cultures;
microscopic examination showed the presence of a
widespread necrosis of the lung tissue.
In the group of autopsies in Table XL there was red confluent
lobular pneumonia. These autopsies are separated
from those just cited because there was no histologic examination
of the tissue.
| Table XL |
|---|
| |
| NO. OF AUTOPSY |
BACTERIOLOGY OF HEART’S BLOOD |
BACTERIOLOGY OF LUNGS |
BACTERIOLOGY OF BRONCHUS |
| 289 |
Pneum. IV |
Pneum. IV |
Pneum. IV, B. inf., staph. |
| 297 |
|
Pneum. IV, B. inf. |
Pneum. IV, B. inf., S. hem. (a few) |
| 306 |
|
|
|
| 339 |
Pneum. IV |
|
|
| 364 |
S. hem. |
|
|
| 418 |
Pneum. atyp. II |
Pneum. atyp. II, B. inf., S. vir. |
|
| 424 |
|
Pneum. IV. |
|
This group of autopsies confirms the view that the red
confluent lobular pneumonia is caused by pneumococci in
association with B. influenzæ. Hemolytic streptococci may
invade secondarily. In Autopsy 297 a few hemolytic streptococci
were found in the bronchus but apparently had not
entered the lungs. In the absence of histologic examination
it is not possible to determine if the invasion of hemolytic
streptococcus (in Autopsy 364) has caused necrosis of
the pneumonic tissue.
190
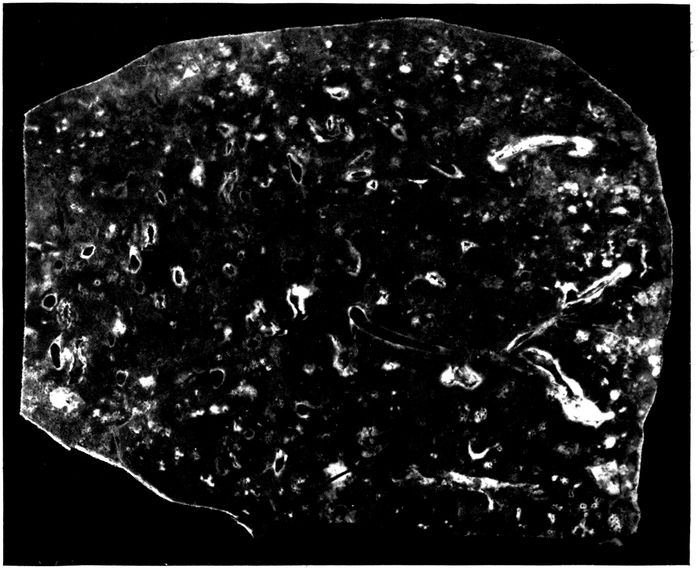
Fig. 7.—Bronchopneumonia with purulent bronchitis and peribronchial hemorrhage.
Peribronchial Hemorrhage and Pneumonia
In a considerable number of instances, namely, in 19 autopsies,
hemorrhage about the small bronchi has been recognizable
upon gross examination of the lung. A conspicuous
zone of hemorrhage 2 or 3 mm. in thickness surrounds
small (with no cartilage) often dilated bronchi and on longitudinal
section may be tracted for a considerable distance
along the bronchus (Fig. 7). In many additional instances
peribronchial hemorrhage has been found by microscopic
examination. In some instances the peribronchial zone of
hemorrhage is firmer than the tissue elsewhere and it is
occasionally difficult to determine whether the lesion is
hemorrhage or pneumonia. In 7 instances frank red consolidation
of peribronchial tissue was recognized at autopsy;
this lesion will be considered later under peribronchial
pneumonia. Hemorrhage about bronchi, like other
evidences of severe injury to bronchi following influenza,
is more frequently found in the lowermost parts of the
lungs than elsewhere. It is invariably associated with
severe bronchitis; the bronchi have contained purulent
191fluid in 15 of 19 instances of peribronchial hemorrhage and
in 10 instances the lesion has been associated with dilatation
of the bronchi.
Microscopic examination furnishes further evidence of
the severity of the bronchial changes which have brought
about hemorrhage into the surrounding alveoli. The lumen
of the bronchus contains blood and leucocytes; the epithelium
is sometimes raised in places from the underlying
basement membrane by blood; blood vessels of the bronchial
wall are engorged, and there is hemorrhage into the
tissue of the bronchus. More frequently the bronchial epithelium
is completely lost and the denuded surface is often
covered by a layer of fibrin intimately adherent to the inflamed
mucosa. Transitions between simple hemorrhage
and pneumonia are found, polynuclear leucocytes being
mingled with red blood corpuscles. In several instances
the alveoli in immediate contact with the bronchial wall
have contained fibrin, whereas those in the surrounding
zone have contained blood.
Bacteria found in the bronchi in 10 instances of peribronchial
hemorrhage have been as follows:
| Staphylococci |
1 |
| B. influenzæ, pneumococci |
1 |
| B. influenzæ, S. hemolyticus |
2 |
| B. influenzæ, pneumococci, staphylococci |
1 |
| B. influenzæ, S. hemolyticus, staphylococci |
4 |
| No organism found |
1 |
The high incidence of B. influenzæ and the frequent association
of B. influenzæ and hemolytic streptococci are
noteworthy. The instance in which no organisms were
found is probably due to a defect in media and should perhaps
be excluded from the list.
The percentage incidence of pneumococci, hemolytic
streptococci, staphylococci and B. influenzæ in the bronchus,
lungs and blood of the heart is an index of the facility with
which these microorganisms penetrate internal organs
when the bronchi are the site of this hemorrhagic lesion.
192
| Table XLI |
|---|
| |
|
NO. OF CULTURES |
PNEUMOCOCCI |
HEMOLYTIC STREPTOCOCCI |
STAPHYLOCOCCI |
B. INFLUENZÆ |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
10 |
2 |
20.0 |
6 |
60.0 |
6 |
60.0 |
8 |
80.0 |
| Lung |
13 |
4 |
30.8 |
7 |
53.8 |
3 |
23.1 |
5 |
38.5 |
| Blood |
17 |
4 |
23.5 |
9 |
52.9 |
|
|
|
|
When these figures are compared with those for all forms
of bronchitis no very noteworthy differences are found;
the incidence of pneumococci here is less and that of hemolytic
streptococci greater. In association with the severe
changes present in the bronchi, hemolytic streptococci
which enter the lungs almost invariably find their way into
the blood.
In 6 instances there has been frank pneumonic consolidation
limited to a zone encircling small and medium-sized
bronchi which have often been obviously dilated. On cross
section these patches of pneumonia are circular, from 1 to
2 cm. in diameter and each contains a bronchus at its center.
When the bronchus is cut longitudinally it is evident that
pneumonic consolidation forms a cylindrical sheath about
the tube. The consolidation varies in color from red to
grayish red. In one instance (Autopsy 253) the consolidated
tissue has formed a gray zone in contact with the
bronchus and is red in a peripheral zone; microscopic examination
shows that the alveoli about the bronchus contain
fibrin, whereas those at a greater distance contain red
blood corpuscles. In this instance, the associated pneumonia
in another part of the lung has been somewhat
anomalous and has had characters both of lobar and bronchopneumonia,
for scattered in the left lung there have been
patches of firm consolidation not more than 2 cm. across.
The smaller of these patches are deep red, but the larger
are coarsely granular and gray in the center. The patchy
193character of the lesion has suggested bronchopneumonia,
but the coarse granulation on section and the presence of
fibrinous plugs within the small bronchi have presented a
close resemblance to lobar pneumonia. This autopsy is
one of the few instances in which Pneumococcus II has been
found, Pneumococcus II being present in blood and lungs,
B. influenzæ, in lungs and bronchi. In 2 additional instances
(Autopsies 374 and 392) peribronchial pneumonia,
recognizable at autopsy, has been associated with consolidation
having the characters of lobar pneumonia. In one
instance, Autopsy 374, the right lung has contained two
patches of firm, mottled red and pinkish red coarsely granular
consolidation each about 6 cm. across, one situated in
the upper lobe and the other in the lower lobe. Elsewhere
in the lung, in definite relation to dilated bronchi, occur
patches of firm, red, coarsely granular consolidation from
1 to 1.5 cm. in diameter when cut transversely. The bronchus
in the center has contained purulent fluid. In the opposite
lung similar consolidation has been limited to zones
about dilated bronchi which contain purulent fluid. Pneumococcus
IV has been obtained from the blood of the heart.
The peribronchial pneumonia which has been described
occurs in association with evidence of profound injury to
the bronchial wall. In 5 of 6 instances purulent bronchitis
has been found at autopsy; in half of these instances bronchiectasis
has been noted. The epithelium of the bronchus
has been found separated from the underlying tissue by serous
exudate, blood and leucocytes; epithelial cells undergo
necrosis and disappear, the denuded surface being covered
by fibrin. Necrosis extends a varying depth into the wall
of the bronchus; blood vessels are engorged, and there is
in some instances hemorrhage throughout the wall of the
bronchus.
The character of the exudate in the alveoli surrounding
the bronchus differs considerably in different instances.
In some instances (Autopsies 374 and 392) red blood corpuscles
194are predominant in the alveoli in contact with the
bronchial wall, whereas in a peripheral zone polynuclear
leucocytes are more abundant. In other instances (Autopsies
253 and 402) alveoli next the bronchial wall contain
abundant fibrin and these are surrounded by a zone in
which the alveoli are filled with blood.
Peribronchial pneumonia is the result of the direct extension
of the inflammatory process through the wall of the
bronchus; it occurs when the epithelium of the bronchus is
destroyed and the underlying tissues are injured, but
may be present in a wide encircling zone even when
the lesion has not penetrated the bronchial wall. The distribution
of the pneumonia demonstrates very clearly that
the inflammatory process does not reach the affected peribronchial
alveoli by way of the bronchioles tributary to the
bronchus.
The bacteriology of these instances of peribronchial
pneumonia is noteworthy. (Table XLII.)
| Table XLII |
|---|
| |
| AUTOPSY |
BLOOD |
LUNG |
BRONCHUS |
| 253 |
Pneum. II |
Pneum. II, B. inf. |
Staph., B. inf. |
| 374 |
Pneum. IV |
|
|
| 387 |
Pneum. II, S. hem. |
Pneum. II, staph., B. inf. |
Pneum. II, S. hem., staph., B. inf. |
| 392 |
Pneum. II |
|
|
| 402 |
Pneum. IV, S. hem. |
|
|
| 424 |
? |
Pneum. IV |
|
Pneumococcus has been found in every instance either in
the lungs or blood. Pneumococcus II, which has been uncommon
with the pneumonia following influenza at Camp
Pike and has occurred only ten times in more than 200
autopsies, has been present in one-half of these cases. The
constant association of the lesion with pneumococcus is
particularly significant when a comparison is made between
the incidence of pneumococcus with peribronchial hemorrhage,
on the one hand, and peribronchial pneumonia on the
other; pneumococcus has been present in less than a third
195of the instances of hemorrhage but in all instances of pneumonia.
In addition to the instances in which gross peribronchial
consolidation has been noted at autopsy, microscopic examination
has demonstrated the presence of fibrinous pneumonia
surrounding bronchi in a considerable number of
autopsies. In a zone encircling small bronchi (with no
cartilage) alveoli are filled by plugs of dense fibrin (Fig.
20) containing in variable number polynuclear leucocytes
and mononuclear cells. The width of the zone is often
equal or greater than the diameter of the bronchus. Alveoli
outside the zone of fibrinous inflammation may contain
red blood corpuscles or serum, and desquamated epithelial
cells are often abundant.
Of 21 instances of peribronchial fibrinous pneumonia 20
were associated with purulent bronchitis. Further evidence
of the relation of the lesion to profound injury to
the bronchi is its association with bronchiectasis in 17 instances.
Peribronchial fibrinous pneumonia, like other lesions encircling
the small bronchi, bears a direct relation to the
severity of microscopic changes in the bronchus. The epithelium
of the bronchus is either partially or completely
lost. Occasionally epithelium is raised by hemorrhage or
leucocytes from the underlying tissue but more frequently
it is wholly lost and the surface is covered by a layer of
fibrin. In the early stages of the lesion, polynuclear leucocytes
may be numerous throughout the bronchial wall, indicating
that the inflammatory irritant within the lumen is
affecting the entire wall and extending its influence to the
surrounding pulmonary tissue. Later lymphoid and plasma
cells are more abundant than polynuclear leucocytes.
Coagulative necrosis and disintegration of the bronchial
wall, proceeding from the inner surface outward, may extend
more or less deeply, and fibrinous inflammation of
adjacent alveoli is often more extensive about that segment
196of the bronchus which shows the greatest change. In some
instances segments of the bronchial wall or even the entire
wall has disappeared, so that alveoli containing fibrin form
part of the wall of the cavity thus formed. When bronchiectasis
has occurred, there are often fissures from the
lumen through the entire wall extending into the surrounding
lung tissue: here fibrinous pneumonia is particularly
conspicuous, occurring in a zone about the edges of the
defect. This deposition of fibrin within the alveoli adjacent
to the injury doubtless has a part in limiting the distribution
of bacterial infection. Nevertheless breaks in the
continuity of the bronchial wall are not essential to the
production of the lesion and the irritant, which is responsible
for the lesion, may penetrate through the bronchial
wall to surrounding alveoli and from alveoli to other alveoli
immediately adjacent.
With this peribronchial pneumonia the smallest bronchi
are distended with pus and their walls are infiltrated with
polynuclear leucocytes, lymphoid and plasma cells. In a
broad zone encircling the bronchus the alveoli are filled
with plugs of fibrin. Bronchioles are similarly distended
with polynuclear leucocytes; the alveoli which occur upon
the wall of the bronchiole are often limited to one side of
the wall and are filled with fibrin. This fibrin occasionally
projects into the lumen of the bronchiole and forms a continuous
layer in contact with the wall on the same side.
The alveolar duct and infundibulum are distended with
polynuclear leucocytes. The alveoli upon the wall of the
alveolar duct and upon the proximal part of the infundibulum
are filled with fibrin. The bronchus, bronchiole,
alveolar duct and part of the infundibulum are thus surrounded
by a continuous zone of alveoli containing fibrin.
The alveoli about the distal part of the infundibulum may
be filled with polynuclear leucocytes. Lung tissue between
adjacent zones of fibrinous pneumonia may contain serum
and desquamated epithelial cells.
197Organization of peribronchial fibrin was found in 10
of the 22 autopsies in which peribronchial fibrinous pneumonia
had been found. Fibroblasts have invaded the fibrin
and newly formed capillaries have penetrated into it. In
some instances the interalveolar septa are thickened and
infiltrated with lymphoid and plasma cells, and in 7 instances
there was chronic pneumonia with thickening and
mononuclear infiltration of the interstitial tissue about the
bronchi and blood vessels, and elsewhere. The duration
of the fatal illness in 12 instances with no organization was
usually from ten days to two weeks, though in 3 instances
there was no organization although the respiratory disease
had lasted from seventeen to nineteen days (average duration
with no organization, 13.5 days). The duration of
illness in 10 instances with organization of fibrin was
slightly less than three weeks (average 18.9 days). These
figures do not accurately represent the duration of pneumonia
which usually develops after a period of several days
following onset of influenza.
This group of instances of peribronchial fibrinous pneumonia
has offered an opportunity to study the bacteriology
of pneumonia with organization and to determine if it presents
any unusual characters. The bacteriology of autopsies
with peribronchial fibrinous pneumonia with no organization
is shown in Table XLIII:
| Table XLIII |
|---|
| |
| AUTOPSY |
BLOOD |
LUNG |
BRONCHUS |
| 289 |
Pneum. IV |
Pneum. IV |
Pneum. IV, B. inf., staph. |
| 372 |
|
|
|
| 376 |
S. hem. |
S. hem. |
S. hem., B. inf., S. aur. |
| 409 |
0 |
|
|
| 410 |
|
S. hem., B. inf. S. aur. |
|
| 412 |
Pneum. II |
|
Pneum. II, B. inf. |
| 420 |
S. hem. |
S. hem., B. inf. S. aur. |
|
| 423 |
S. hem. |
S. hem., B. inf. |
|
| 440 |
0 |
B. inf., S. aur. |
B. inf., S. aur. |
| 448 |
0 |
0 |
0 |
| 482 |
0 |
B. inf., Pneum. IV |
B. inf., Pneum. IV, S. hem. |
| 489 |
0 |
Pneum. IV, B. inf. |
Pneum. IV, B. inf. |
198The bacteriology of instances of peribronchial fibrinous
pneumonia with organization of the intraalveolar fibrin is
shown in Table XLIV:
| Table XLIV |
|---|
| |
| AUTOPSY |
BLOOD |
LUNG |
BRONCHUS |
| 283 |
Pneum. IV |
Staph., B. inf. |
B. inf., Pneum. IV, staph. |
| 291 |
0 |
0 |
B. inf., staph. |
| 398 |
0 |
|
|
| 419 |
0 |
Pneum. II, B. inf. |
Pneum. II, B. inf. |
| 421 |
S. hem. |
Pneum. IV, S. hem. |
|
| 422 |
0 |
Pneum. II atyp., B. inf. |
|
| 425 |
S. hem. |
S. hem., B. inf., S. alb. |
|
| 433 |
0 |
S. hem., B. inf., S. aur. |
|
| 460 |
S. hem. |
S. hem., B. inf. |
S. hem., B. inf., staph. |
| 463 |
0 |
B. inf., staph. |
B. inf., staph., Pneum. IV |
B. influenzæ has been present in the bronchi in every instance
save one in which cultures have been made, and it
is probable that in this exceptional instance cultures have
remained sterile because the media employed have been defective.
The incidence of B. influenzæ in the lung has been
unusually high both with and without organization (66.7
per cent with no organization; 77.8 per cent with organization).
Streptococci and staphylococci have been found
in a considerable proportion of all instances of peribronchial
fibrinous pneumonia, but there has been no notable
preponderance of these microorganisms when organization
has occurred. Organization has been present in instances
in which pneumonia is referable to pneumococcus
associated with B. influenzæ and unaccompanied by either
streptococci or staphylococci (Autopsies 419 and 422).
Wadsworth[81] found no organization after inoculation of the
lungs of dogs with pneumococcus or with staphylococcus
alone, but produced organization when he inoculated animals
with both microorganisms.
Injury to bronchi produced in part at least by B. influenzæ
exposes the bronchi and lung tissue to repeated
infection with a variety of microorganisms; absorption of
199fibrin and regeneration of alveolar epithelium are prevented,
resolution fails to occur and organization of fibrin
follows.
Suppurative Pneumonia With Necrosis and Abscess Formation
Three varieties of suppurative pneumonia have occurred
in association with influenza.
A. Necrosis and suppuration with formation of one or
several abscesses usually below the pleura and almost invariably
caused by hemolytic streptococci.
B. Interstitial suppurative pneumonia caused by hemolytic
streptococcus.
C. Multiple abscesses in clusters caused by staphylococci.
Suppurative pneumonia with necrosis and abscess formation
will be discussed in this section. Pulmonary abscesses
which occurred in 43 autopsies may be included in
this group; in 4 of these autopsies abscess and interstitial
suppurative pneumonia occurred in the same individual.
These abscesses were much more frequently situated in the
lower than in the upper lobes and more often in the right
than in the left lung. In most instances there was one or
several abscesses situated below the pleura of one lobe;
occasionally abscesses occurred in two lobes of the same
lung or in both lungs. The distribution was as follows:
Abscess in only one lung occurred in right upper lobe in
6 autopsies; middle lobe, 3; lower lobe, 15; left upper lobe,
2; lower lobe, 16. Abscesses occurred in both right and
left lower lobes, twice. The usual situation was at the
lower and posterior part of the lower lobe at or near the
basal edge, less frequently below the posterior border or
upon the basal surface of the lobe. These abscesses in
almost every instance were found immediately below the
pleural surface, so that they appeared upon the pleura
as opaque yellow spots usually surrounded by narrow
zones of hemorrhage. In one instance (Autopsy 376) the
200abscess cavity was separated from the pleural cavity by
remains of the pleura which was as thin as tissue paper and
in other instances perforation had occurred (Fig. 9). In
Autopsy 480 the abscess cavity which had perforated the
pleura was in free communication with a bronchus of medium
size.
In most instances of suppurative pneumonia there have
been associated lesions of bronchopneumonia which have
been peribronchiolar, hemorrhagic or lobular and have exhibited
no unusual characters. The abscess or abscesses
are situated within an area of pneumonic consolidation
which is not limited by lobule boundaries and has not the
characters of bronchopneumonic consolidation. In some
instances this consolidation is limited to a zone immediately
about the abscess, but often it involves the greater part of
a lobe. The tissue is laxly consolidated and flabby; on section
it has a dull, conspicuously cloudy appearance and is
grayish red, pinkish gray or gray; it is homogeneous or
very finely granular. Turbid gray fluid, which sometimes
resembles thin pus, oozes from the cut surface.
Widespread necrosis of tissue is not infrequently a conspicuous
feature of this pyogenic pneumonia (Fig. 8).
Upon a cloudy gray background of consolidation are numerous
opaque yellowish gray or yellow patches, occasionally
2 or 3 cm. across, giving a mottled character to the
cut surface. Upon the pleura these necrotic patches appear
as dull opaque yellow spots. They may be surrounded
by a zone of hemorrhage. The opaque material
is at first firm but may undergo softening, becoming semisolid
and finally purulent. Necrotic patches may be scattered
throughout a lobe, but fully formed abscesses are with
few exceptions immediately below the pleura (Fig. 9).
201
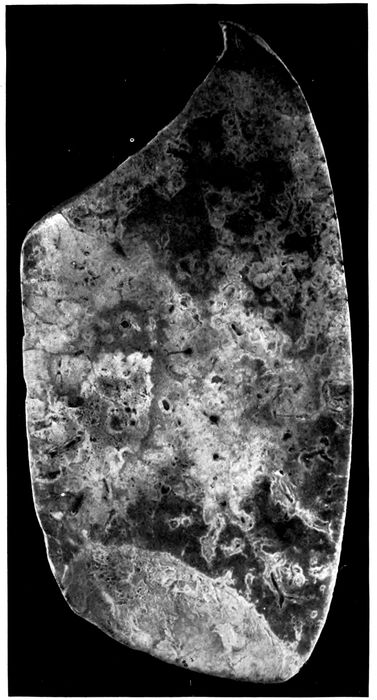
Fig. 8.—Streptococcus pneumonia with massive necrosis. Autopsy 354.
202

Fig. 9.—Abscess below pleura with perforation caused by hemolytic streptococci. Healing suppurative interstitial pneumonia indicated by yellowish gray lines marking interlobular septa at base of lower lobe. Autopsy 474; right lung. (See left lung, Fig. 10.)
203The duration of illness in cases of pneumonia with abscess
varied from a week or less (11 instances) to more
than four weeks. The duration of the greater number of
cases (17 instances) was between one and two weeks. In
one instance onset occurred with symptoms of influenza,
pneumonia was recognized two days later, and death occurred
only four days after the onset of illness. When the
duration of the illness was less than a week the symptoms
of onset were in some instances those of pneumonia.
Table XLV shows the incidence of pneumococcus, S. hemolyticus,
staphylococcus and B. influenzæ in instances of
suppurative pneumonia with abscess formation, 4 instances
of abscess with interstitial suppurative pneumonia being
excluded:
| Table XLV |
|---|
| |
|
NO. OF CULTURES |
PNEUMOCOCCI |
HEMOLYTIC STREPTOCOCCI |
STAPHYLOCOCCI |
B. INFLUENZÆ |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
24 |
5 |
20.8 |
22 |
91.6 |
12 |
50.0 |
18 |
75.0 |
| Lung |
36 |
9 |
25.0 |
30 |
83.3 |
14 |
35.6 |
8 |
22.2 |
| Blood |
37 |
6 |
16.2 |
31 |
83.8 |
|
|
|
|
In over 80 per cent of instances of pulmonary abscess
hemolytic streptococcus has been found in blood, lungs and
bronchus and, when cultures have been made, in the inflamed
pleural cavity as well. Streptococci have been
found in immense number in sections from the necrotic
lung tissue and the abscesses which have been formed. It
is evident that hemolytic streptococci have caused suppurative
pneumonia and death, being found in the blood of the
heart just as frequently as in the lungs (83 per cent). The
relative unimportance of pneumococci is indicated by their
low incidence in the blood (16.2 per cent) when compared
with that of lobar pneumonia (65.5 per cent) or of bronchopneumonia
(31.4 per cent). B. influenzæ has been found
in three-fourths of these autopsies in the bronchus, but its
incidence in the lungs has been much smaller.
In 3 instances of suppurative pneumonia with abscess
formation no hemolytic streptococci were found; they are
as follows:
204Autopsy 380.—Bronchopneumonia with gray and red lobular consolidation
in right upper and lower lobes; peribronchiolar nodules of consolidation
in left lower lobe; abscess, 1.5 cm. across, below the pleura of the
posterior border of the left lower lobe near its base; fibrinopurulent pleurisy
(300 c.c.) on right side; serous pleurisy (200 c.c.) on left. Pneumococcus
III was found in cultures from the blood of the heart from the right
lung and with B. influenzæ from the right pleural cavity. No culture was
made from the left lung which contained the abscess. In sections of the
abscess gram-positive streptococci in chains of 4 to 8 cocci were numerous.
Autopsy 406.—Acute lobar pneumonia with red hepatization of greater
part of right lung; patch of consolidation in lower lobe of left lung containing
an abscess cavity 2.5 x 1.5 cm.; localized seropurulent pleurisy
(375 c.c.) on left side. Pneumococcus IV was obtained from the blood of
the heart; a culture from the lung was contaminated. Tissue from the
abscess was not saved for histologic examination.
Autopsy 416.—Suppurative pneumonia with necrosis and abscess formation
in right lower lobe; fibrinous pleurisy on right side. Pneumococcus
IV was obtained from the blood, right lung and right main bronchus. No
streptococci were found in sections from the abscess in the right lung.
The foregoing observations demonstrate that suppurative
pneumonia with abscess formation following influenza
is with few exceptions caused by S. hemolyticus.
The autopsies (Table XLVI) in which pneumococci have
been found in association with hemolytic streptococci in the
blood or lungs indicate that pneumococci have had a part
in the production of fatal pneumonia.
| Table XLVI |
|---|
| |
| AUTOPSY |
CULTURE FROM BLOOD |
CULTURE FROM LUNGS |
CULTURE FROM BRONCHUS |
| 258 |
S. hem. |
S. hem., Pneum. IV B. inf. |
|
| 282 |
S. hem., Pneum. II |
S. hem., Pneum. II |
S. hem., B. inf. Pneum. II, staph. |
| 345 |
|
S. hem., Pneum. II, staph. |
|
| 378 |
Pneum. atyp. II |
S. hem., Pneum. atyp. II |
S. hem., B. inf., Pneum. atyp. II |
| 381 |
S. hem. |
S. hem., Pneum. II Pneum. IV, staph. |
|
| 383 |
Pneum. III |
S. hem., Pneum. III B. inf. |
|
| 387 |
S. hem. |
Pneum. II, staph., B. inf. |
S. hem., pneum., staph., B. inf. |
These autopsies, notably those in which pneumococci
have been found in the blood, suggest that infection with
205pneumococci has preceded suppurative pneumonia caused
by hemolytic streptococci. In a small number of instances
the sputum was examined in life after onset of pneumonia.
| Table XLVII |
|---|
| |
| AUTOPSY |
SPUTUM |
CULTURES FROM BLOOD, LUNGS AND BRONCHUS |
| 282 |
Pneum. IV. B. inf. |
S. hem., Pneum. II, staph., B. inf. |
| 288 |
S. hem., B. inf. |
S. hem., B. inf. |
| 376 |
(No S. hem., Oct. 8) |
S. hem., staph., B. inf. (Oct. 11) |
In 2 of these 3 cases infection with hemolytic streptococcus
occurred subsequent to the onset of pneumonia.
Several observations help to explain the occurrence of
abscess in association with the pneumonia of influenza.
The fissures which will be described in association with
bronchiectasis represent traumatic ruptures of the bronchial
wall consequent upon weakening by necrosis and over
distention. They expose the injured bronchial wall and
the alveolar tissue adjacent to it to infection by the microorganisms
contained within the lumen of the inflamed
bronchus. Occasionally a favorable microscopic section
demonstrates the relation of pulmonary necrosis and consequent
suppuration to injuries of the bronchial wall.
Peribronchial fibrinous pneumonia occurs about the bronchi
of which the epithelial lining has been destroyed, and
when a fissure penetrates the bronchial wall fibrinous pneumonia
is almost invariably found in a zone about the tear;
it doubtless tends to limit the extension of the process.
Occasionally, wide areas of necrosis occur within consolidated
tissue near the site of the fissure (Autopsy 312 with
S. hemolyticus and B. influenzæ, p. 254). Accumulation of
polynuclear leucocytes between living and dead tissue may
form a line of demarcation (Autopsy 387); finally, fairly
large, irregularly formed, abscess cavities are found.
Necrosis and beginning suppuration in contact with the
lumen of the bronchus will be described in association with
bronchiectasis (Autopsies 312, Fig. 24, and 423, p. 256). In
206the following autopsies upon individuals who have died
with pulmonary abscesses, favorable microscopic sections
have demonstrated abscess formation in contact with lesions
which have penetrated the walls of small bronchi. They
help to explain the pathogenesis of abscess in association
with influenza.
Autopsy 376.—H. M., white, aged twenty-four, a fireman, resident of
Oklahoma, had been in military service one month. Onset of illness occurred
October 1, ten days before his death; he was admitted to the base
hospital on the fourth day of his illness with the diagnosis of bronchopneumonia.
Anatomic Diagnosis.—Acute bronchopneumonia with patches of lobular
and confluent lobular consolidation in both lungs and hemorrhagic peribronchiolar
consolidation in right upper lobe; abscess in right upper lobe
below pleura; fibrinopurulent pleurisy on right side; purulent bronchitis;
bronchiectasis at base of left lobe.
An irregular abscess, 2 x 1 cm., filled with creamy purulent fluid is
separated from the interlobular surface of the right upper lobe by a thin
membrane representing the pleura. The right pleural cavity contains 200
c.c. of turbid yellow fluid in which is soft fibrin. The bronchi contain
purulent fluid in great abundance. The bronchi at the base of the left
lower lobe are widely dilated, so that many small bronchi with no cartilage
in their wall measure from 3 to 5 mm. in diameter.
Cultures show the presence of hemolytic streptococci in the blood of
the heart and in three plates from the lung; B. influenzæ and S. aureus
were found in the left bronchus.
The bronchi have wholly or partially lost their epithelium and there
is deep erosion of the walls. Cavities containing polynuclear leucocytes
occur within the alveolar tissue; in some instances pus containing cavities
are surrounded by alveolar tissue, but in other places it is evident,
that they have had their origin in bronchi. In a short segment of the
circumference the wall of the preexisting bronchus is preserved and
consists of squamous epithelium, vascular connective tissue and smooth
muscle. The remainder of the bronchus has disappeared and a cavity is
produced. The very irregular wall of the cavity is formed by partially
destroyed alveoli filled with fibrin and leucocytes.
Autopsy 387.—C. M., white, aged twenty-one, laborer, resident of Mississippi,
had been in military service twenty-one days. Illness began on
September 22, nineteen days before death, and the patient was admitted
to the hospital on the same day with a diagnosis of bronchitis; a diagnosis
of bronchopneumonia was made on October 2, nine days before death.
The leucocytes on October 3 numbered 8000 (small mononuclear, 36 per
cent; large mononuclear, 5 per cent; polynuclear, 59 per cent).
207Anatomic Diagnosis.—Acute bronchopneumonia with consolidation in
right upper lobe and hemorrhagic peribronchiolar consolidation in left lower
lobe; abscess below pleura in left lower lobe; purulent pleurisy on both
sides; edema of mediastinum; purulent bronchitis; bronchiectasis.
There is advanced bronchiectasis, and bronchi with no visible cartilage
are dilated to from 4 to 8 mm. in diameter; they contain purulent fluid
which wells up from the cut surface. About dilated bronchi there is in
places dull red or grayish red consolidation forming an encircling zone.
Situated below the pleural surface within an area of consolidation at the
posterior border of the left lower lobe there is a spot 3 cm. across where
the tissue is yellow and has in places undergone purulent softening. Several
smaller abscesses occur nearby.
Cultures from the blood of the heart and from the edematous mediastinum
contain hemolytic streptococci. From the abscess are grown S.
albus, Pneumococcus II and B. influenzæ. The purulent contents of a small
bronchus contains S. hemolyticus, B. influenzæ, S. aureus and a few pneumococci.
Microscopic examination shows that the epithelium of dilated bronchi
has disappeared and the denuded surface is covered by fibrin and polynuclear
leucocytes; fissures extend from the lumen through the bronchial wall into
the surrounding alveolar tissue. A zone of fibrinous pneumonia surrounds
these bronchi and fissures in the bronchial wall penetrate into this zone.
One dilated bronchus 2.4 mm. in diameter with no cartilage in its wall
has vascular connective tissue covered by epithelium on one side, whereas
the remainder of the circumference is formed by exposed alveoli filled with
fibrin, the bronchial wall having disappeared. A section through a part
of the abscess which has been mentioned shows a very irregularly formed
cavity approximately 1 x 0.7 cm. Remains of bronchial wall, consisting
of very vascular tissue covered by flat epithelium in several layers, indicate
the origin of the cavity. Between these remnants of bronchi deep pockets
extend into the pulmonary tissue which in the margin of the cavity is the
site of fibrinous pneumonia. In one place, in contact with the cavity, a
wide area of consolidated tissue has undergone necrosis and both alveolar
walls and their contents have lost their nuclei. Leucocytes which are
accumulating at the margin of the necrotic patch form a line of demarcation
between living and dead tissue.
Abscess may be the result of the profound changes which
occur in the bronchi as the result of influenza. Necrosis
caused by bacteria within the bronchi weakens and in
places destroys the wall. Bacteria penetrate into the surrounding
tissue and hemolytic streptococci (or staphylococci)
may produce localized abscesses. These abscesses
are usually situated near the pleural surface of the lung, because
destructive changes causing rupture of the bronchial
208wall occur more frequently in the smaller peripheral bronchi
than in the larger bronchi containing cartilage. Abscesses
occur more frequently at the bases of the lungs,
because the most severe changes in the bronchi occur in
the dependent part. (See “Bronchiectasis,” p. 240.)
Healing of Abscess.—The following autopsy is of interest
in relation to the treatment of pulmonary abscess and associated
empyema.
Autopsy 467.—P. C., white, aged twenty-five, a farmer from Missouri,
had been in military service three months. Illness began September 27,
thirty days before death, and the patient was admitted the day following
onset with headache, backache and cough. Pneumonia with consolidation
in the right lower lobe was recognized on the sixth day of illness. On the
ninth day 500 c.c. of fluid were withdrawn from the right pleural cavity;
there were cyanosis and dyspnea. On the eleventh day 700 c.c. of fluid
were withdrawn. On the twelfth day thoracotomy was performed and 100
c.c. of greenish fluid were removed. The patient’s condition improved for
a time, but on the twenty-sixth day 1,000 c.c. of straw colored fluid were
aspirated from the left pleural cavity and on the twenty-eighth day the
same amount of seropurulent fluid was withdrawn.
Anatomic Diagnosis.—Healing abscess of right lower lobe communicating
with the pleural cavity; acute purulent pleurisy with closed thoracotomy
wound on the right side; purulent pleurisy on the left side; acute bronchopneumonia
with lobular consolidation in the left lung; purulent bronchitis;
bronchiectasis with formation of spherical bronchiectatic cavities; acute
splenic tumor.
At the base of the right chest is a closed thoracotomy wound 2 cm.
in length; the right pleural cavity contains 200 c.c. of thick creamy pus
and the cavity is lined by a thick tough membrane. The left pleural cavity
contains 800 c.c. of white purulent fluid thinner than that on the right
side. The right lung is compressed into the posterior and inner part of
the chest. The upper lobe is pink and air containing; the posterior and
lower part of the lower lobe is red and atelectatic, and fibrous septa are
more conspicuous than elsewhere. The pleura of the external surface near
the basal edge, in an area 2 cm. across, is depressed and yellowish gray in
color. In the center of this area is a small opening communicating with
a pocket 0.5 cm. across within the substance of the lung.
In the lower lobe beneath the interlobular surface are two spherical
bronchiectatic cavities, each about 1.5 cm. across, with smooth lining in
continuity with two branches of the same bronchus of medium size.
Bacteriologic examination showed the presence of S. hemolyticus in the
blood of the heart. No growth was obtained from the left lung; the left
pleural cavity contained hemolytic streptococci and S. aureus, the latter in
209small number. S. hemolyticus and B. influenzæ were grown from the left
main bronchus.
A microscopic section through the abscess and its communication with
the pleura shows that its cavity contains polynuclear leucocytes and the
wall is formed by granulation tissue covered by fibrin. Some alveoli outside
the abscess contain compact balls of fibrin containing a few fibroblasts;
this fibrin stains deeply with hematoxylin as if it contained calcium. The
surface of the lung is covered by fibrin in process of organization.
In the foregoing instance a pulmonary abscess on the
right side has ruptured into the pleura and, completely
separated from the adjacent lung by a wall of newly formed
tissue, is in process of healing. It shows that these pulmonary
abscesses below the pleura may heal provided
drainage is established by rupture into the pleural cavity
and subsequent evacuation of pleural exudate. It is noteworthy
that in this instance empyema extended from the
right to the left pleural cavity, both S. hemolyticus and S.
aureus were found at autopsy. The thoracotomy wound
on the right side was closed at autopsy.
Interstitial Suppurative Pneumonia
A second type of suppurative pneumonia is characterized
by acute inflammation of interstitial tissue between the secondary
lobules of the lung and by acute lymphangitis; suppuration
involves the interstitial septa and the walls of the
lymphatics. The lesion is designated by Kaufmann,[82]
Beitzke[83] and others acute interstitial pneumonia. Pneumonia
dissecans in which solution of interstitial tissue isolates
sections of lung tissue is said to be a consequence of
the lesion. Many text books of pathology, overlooking
the occurrence of this lesion, limit the consideration of interstitial
pneumonia to chronic processes in which the interlobular
and interalveolar fibrous tissue is increased.
Acute inflammation and edema of the interlobular septa
of the lung with no suppuration is often found with both
lobar and bronchopneumonia and is occasionally so far advanced
210that it can be recognized on gross examination of
the lungs. In a small area interlobular septa are conspicuous
as yellowish lines of edematous appearance which may
be 1 to 1.5 mm. in thickness and sometimes form a network
with rectangular or polygonal meshes. The gelatinous appearance
of the edematous fibrous tissue does not suggest
suppuration. Microscopic examination shows that the
tissue is distended by edema and contains fibrin and polynuclear
leucocytes; the lymphatics are distended and contain
a network of fibrin within which leucocytes are numerous.
Inflammatory edema of the interstitial tissue has
been recognized at autopsy four times in association with
bronchopneumonia (Autopsy 253 with Pneumococcus II;
Autopsy 335, with Pneumococcus IV and S. viridans; Autopsy
477 with S. hemolyticus and Autopsy 498 with S.
viridans); twice with lobar pneumonia (Autopsy 343 with
Pneumococcus IV and Autopsy 353 with atypical Pneumococcus
II); twice with combined lobar and broncopneumonia
(Autopsy 273 with S. hemolyticus and Pneumococcus
IV and Autopsy 357 with Pneumococcus IV). Edema of
interstitial septa was recognized at autopsy in the immediate
neighborhood of an abscess three times (Autopsies
277 and 278 with hemolytic streptococci and Autopsy 282
with hemolytic streptococci and Pneumococcus II). In
these instances of inflammation and edema the lymphatics
are found distended by fibrinous thrombi, and it is probable
that occlusion of lymphatics determines the occurrence of
inflammatory edema within the surrounding tissue. Inflammation
has not proceeded to suppuration.
With interstitial suppurative pneumonia, interlobular
connective tissue is marked by conspicuous yellow lines,
1 to 3 or even 5 mm. in thickness, forming a network with
polygonal meshes which represent secondary lobules (Figs.
10 and 11). The distended septa not infrequently have
bead-like enlargements at intervals and from the cut surface
it is often possible to scrape away creamy yellow pus.
These lines of suppuration invariably extend up to the
pleura and are often broadest immediately below it. Adjacent
septa which have not undergone suppuration are much
thickened and have the yellowish gray appearance produced
by edema.
211
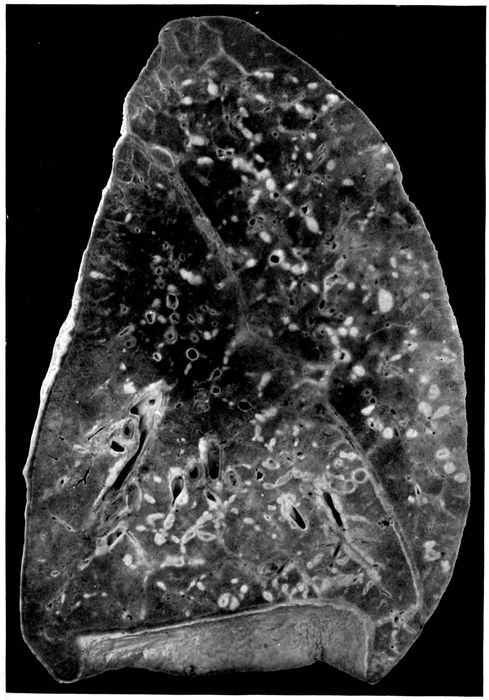
Fig. 10.—Interstitial suppurative pneumonia; interstitial septa are the site of suppuration and lymphatics are distended with purulent fluid; empyema. Autopsy 474, left lung. (See right lung) Fig. 9.
212

Fig 11.—Suppurative interstitial pneumonia; the left lower lobe is the site of almost uniform consolidation and here interstitial septa and their lymphatics are distended with pus. There is more extensive interstitial suppuration in the upper lobe where consolidation is absent. The cloudy appearance of the consolidated lung is well shown. Autopsy 452.
213Suppurative interstitial pneumonia frequently occurs in
association with bronchopneumonic consolidation which
may be peribronchiolar, hemorrhagic or lobular, but there
is in addition consolidation of the pulmonary tissue between
the inflamed septa which may affect part of a lobe, an entire
lobe, or parts of several lobes; it does not exhibit the
characters of confluent lobular pneumonia.
In approximately half of the cases consolidation, associated
with interstitial suppuration, has been lobar in distribution
(Fig. 11). The tissue is laxly consolidated, finely
granular, and has a cloudy red or gray appearance. The
coarsely granular surface of lobar pneumonia is absent.
The affected lung may weigh 1,500 or 1,650 grams. Occasionally,
interstitial septa of air containing lung tissue
is the site of suppurative inflammation or edema. In
Autopsy 452 the lower lobe, save a small part at the base,
is laxly consolidated; interstitial septa in the consolidated
area are yellow, 1.5 to 2 mm. in thickness, beaded and exude
purulent fluid on pressure. In the adjacent part of
the upper lobe there is a patch of consolidation, and a network
of yellow thickened septa extends from it far into the
surrounding air containing tissue. The weight of the right
lung is 635 grams; of the left, 1,650 grams.
The distribution of interstitial suppuration in 21 instances,
including 4 in which the lesion has occurred in the
same lungs with abscess formation, has been as follows:
right upper lobe, 9 instances; middle lobe, 4; lower lobe, 5;
left upper lobe, 7; left lower lobe, 6. In 6 of these autopsies
more than one lobe of the same lung has been affected
by the lesion; in 2 autopsies parts of both lungs have been
affected. Localized abscess of the lung is more common in
214the lower than in the upper lobes, but suppuration of the
interstitial tissue is more often found in the upper lobes.
The duration of illness with interstitial suppurative
pneumonia has varied from six days to five weeks. In over
half of the cases death has occurred during the second week
of illness.
The bacteriology of these cases is shown in Table
XLVIII.
| Table XLVIII |
|---|
| |
|
NO. OF CULTURES |
PNEUMOCOCCI |
HEMOLYTIC STREPTOCOCCI |
STAPHYLOCOCCI |
B. INFLUENZÆ |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
10 |
|
|
9 |
90.0 |
5 |
50.0 |
10 |
100.0 |
| Lung |
20 |
1 |
5.0 |
17 |
85.0 |
5 |
25.0 |
7 |
35.0 |
| Blood |
21 |
2 |
9.5 |
17 |
81.0 |
|
|
|
|
S. hemolyticus has been almost invariably present in
lungs, heart’s blood and bronchi. In 16 of 21 autopsies
hemolytic streptococci have been obtained from the blood
in pure cultures, in one instance associated with pneumococcus.
With associated empyema, pericarditis or peritonitis,
the same microorganism has been found in the
pleural cavities, pericardium or peritoneum. Furthermore,
microscopic examination has demonstrated the presence
of chains of streptococci in the affected interlobular
tissue and in much greater abundance in the distended
lymphatics.
Nevertheless in 2 instances no streptococci have been
found. These cases are as follows:
Autopsy 330.—Illness began with symptoms of influenza ten days before
death; signs of pneumonia were recognized three days before death. There
is firm, gray red consolidation of the entire left upper lobe; the interlobular
septa are here indicated by yellow lines of obvious suppuration and thick puslike
fluid exudes from the cut surface of the consolidated tissue. The upper
half of the left lower lobe has undergone gray hepatization, but here there
is no distention of the interlobular septa. There is fibrinopurulent pleurisy
on the left side with accumulation of 400 c.c. of fluid. Pneumococcus IV is
215obtained from the blood of the heart and from the lung. In the suppurating
tissue diplococci which stain by Gram’s method are present in large number;
there are a few short chains.
Autopsy 379.—Illness began seven days before death with influenza;
signs of pneumonia were first recognized the day before death. The middle
lobe of the right lung is firmly consolidated; on section there is mottling of
deep red and pinkish red and the cut surface is coarsely granular. The interstitial
septa are distended by fluid and are grayish yellow. There is fibrinopurulent
pleurisy on the right side with accumulation of 600 c.c. of fluid.
Pneumococcus atypical II is obtained from the blood of the heart. A large
bacillus unstained by Gram’s method is obtained from the right lung and from
the right main bronchus. In the bronchus are a few influenza bacilli. In the
suppurating and necrotic tissue of the interstitial septa are found diplococci
and chains of 4 to 6 cocci in great number; a few large Gram-negative bacilli
are found.
In both these autopsies consolidation had the characters
of lobar pneumonia, and pneumococci were obtained from
the blood of the heart. It is possible that streptococci failed
to grow or while present elsewhere were absent at the spot
where cultures were made.
It is noteworthy that B. influenzæ was found in the bronchi
in every instance (10) in which cultures were made,
but was obtained much less frequently from the lung. In
one instance (Autopsy 474) this microorganism was found
in the blood in association with hemolytic streptococci.
There was suppurative interstitial pneumonia in the left
lung and abscess in the right lower lobe with rupture into
the cavity and empyema. Hemolytic streptococci and B.
influenzæ were found in the bronchus, right pleural cavity
and blood of the heart.
In 4 instances (Autopsies 251, 259, 295 and 474) interstitial
suppurative pneumonia has been associated with
abscess formation. In one instance (Autopsy 251) the
right middle lobe has been the site of interstitial suppuration
and abscess formation; in another (Autopsy 295) the
left lower lobe has been the site of both lesions, but in the
other 2 instances suppurative interstitial pneumonia and
abscess formation have occurred in opposite lungs. In all
2164 autopsies hemolytic streptococci have been found in the
blood of the heart and in lungs or bronchi.
Empyema has been present in all but 3 of 21 instances of
interstitial suppurative pneumonia.
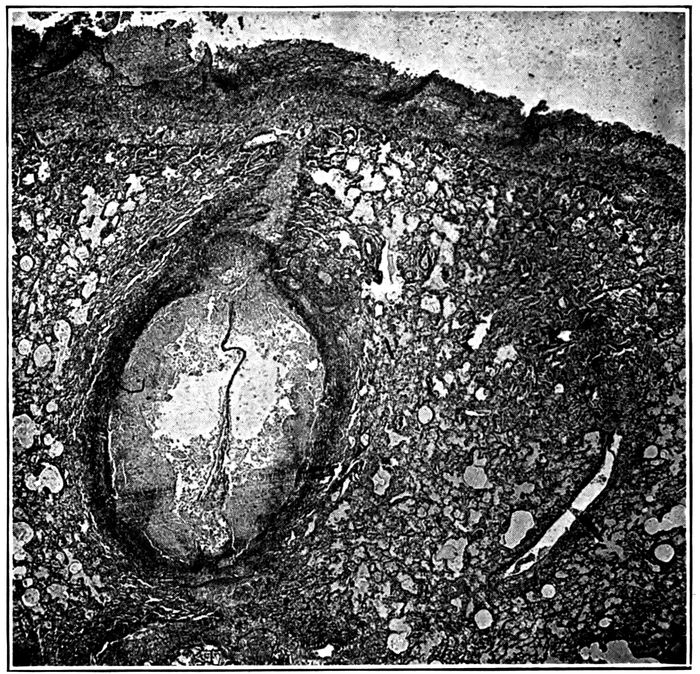
Fig. 12.—Suppurative interstitial pneumonia, showing an immensely dilated lymphatic containing purulent exudate, a short distance below the pleura. Autopsy 474.
Histologic examination of lungs with interstitial suppuration
shows that the interlobular septa are distended by
serum and contain a conspicuous network of fibrin. Polynuclear
leucocytes are present in varying number, and at
times densely infiltrate the distended tissue; it is not uncommon
to find a zone of densely crowded polynuclear leucocytes
along each edge of the septum, whereas the central
part contains comparatively few. Occasionally, there is
hemorrhage into the distended connective tissue.
217Within the distended septa occur greatly dilated lymphatics
filled with polynuclear leucocytes (Figs. 12 and 13).
Thrombosis of the distended lymphatics has usually occurred,
and a conspicuous network of fibrin in which are
polynuclear leucocytes plugs the lumen. Streptococci in
chains of variable length are found in the inflamed interstitial
tissue, but are present in far greater number within
the distended lymphatics.
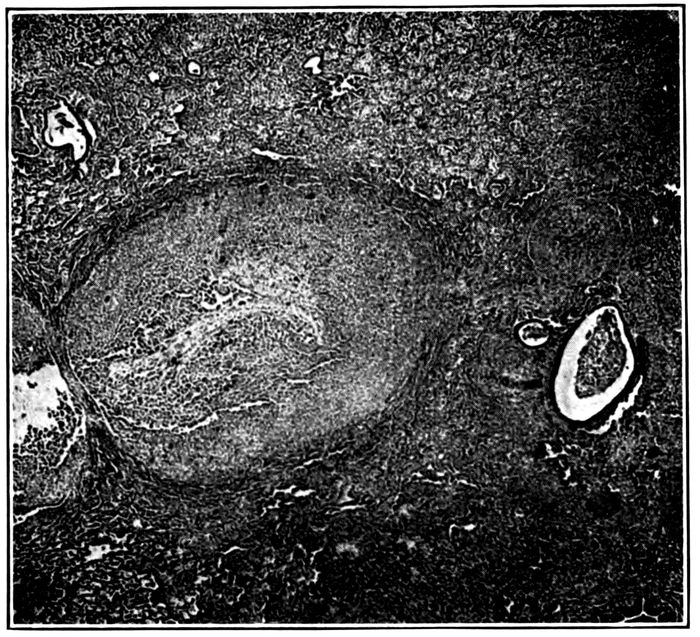
Fig. 13.—Suppurative interstitial pneumonia showing a dilated lymphatic. Autopsy 428.
Necrosis of the cells which fill the lymphatics occurs in
spots, usually in the center of the thrombus, and occasionally
affects the entire contents of the lymphatic; polynuclear
leucocytes have lost their nuclei or in some the nucleus
has undergone fragmentation. In these spots the network
of fibrin has disappeared. Not infrequently the wall
of the lymphatic in a small sector or throughout the circumference
218has undergone necrosis, and spots of necrosis
may occur in the interlobular septa distended by inflammatory
exudate. Wherever necrosis has occurred, chains
of streptococci are present in immense number.
Accumulation of polynuclear leucocytes, necrosis of these
cells, solution of fibrin at first in the centers of the lymphatic
thrombus and later throughout, occasionally with
necrosis of the wall of the vessel, result in the formation
of an abscess at the site of the distended lymphatic. These
lymphatics, dilated by purulent fluid, may have a diameter
from 2 to 3 mm. and may cause considerable compression
and collapse of immediately adjacent alveoli. Lymphangitis,
distention of lymphatics, thrombosis and finally suppuration
may occur in the lymphatic vessels encircling the
blood vessels and in those situated in the adventitia of the
bronchi of medium size.
The alveoli adjacent to the distended septa are filled by
inflammatory products; edema is almost invariably present
and the alveoli may contain serum and desquamated
epithelial cells; fibrin is often present, but more frequently
polynuclear leucocytes are predominant. Not infrequently,
abscess formation, recognized microscopically, has occurred
in contact with septa most often immediately below
the pleura. Polynuclear leucocytes are present in immense
number and alveolar septa have disappeared; occasionally,
with abscess formation there is more or less widespread
necrosis of tissue, cells both of the exudate and of the alveolar
walls having lost their nuclei.
Lymphatics in many places are distended and plugged
by fibrinous thrombi, whereas elsewhere softening of the
thrombus has been brought about by suppuration. Suppuration,
both within the lymphatic and in adjacent alveoli,
appears to be secondary to lymphatic obstruction. In
some instances the lymphatic appears to have undergone
distention after the thrombus has formed, for between the
219thrombus and the wall of the lymphatic a channel is occasionally
found containing uncoagulated lymph.

Fig. 14.—Endophlebitis occurring in association with suppurative pneumonia; the intima contains lymphoid cells in great number; at one spot there is a small thrombus adherent to the intima. Autopsy 325.
Acute endophlebitis has been repeatedly observed in association
with interstitial suppurative pneumonia (Fig.
14). The lesion usually occurs in veins situated within the
septa which are the site of intensely acute inflammation
associated with necrosis. The wall of the vein appears to
be so injured by the surrounding changes that polynuclear
leucocytes and small mononuclear cells accumulate below
the endothelium. Throughout the circumference of the
veins, often 0.5 to 1 mm. in diameter, the endothelium is
separated from the underlying media by polynuclear leucocytes
which form a conspicuous zone encircling the lumen.
Some cells of lymphoid type are usually present
among the polynuclear leucocytes. Polynuclear leucocytes
220are often adherent to the endothelial lining of the vessel
and are not infrequently fixed in the process of passing
through the endothelium. The lesion may be more severe
(Autopsy 325), so that the endothelium has disappeared,
and upon the exposed surface fibrin is deposited; within
this fibrin polynuclear leucocytes are numerous and nuclear
fragmentation has occurred. The middle coat of the
vessel usually contains few cells; some polynuclear leucocytes
within it may be stretched out as if in process of wandering
through the wall.
In other instances the accumulation of cells below the
endothelium is almost wholly mononuclear. Cells of the
type of lymphocytes occur, but more abundant are slightly
larger cells with more abundant cytoplasm. These cells
may form a thick zone below the intima throughout the entire
circumference of the lesion. It seems probable that
these cells, like the polynuclear leucocytes, are derived from
circulating blood within the lumen of the vessel, for small
cells of the type of lymphocytes are not infrequently found
adherent to the lumen and occasionally one is fixed in
process of passing through the endothelium.
This endophlebitis appears to be the result of changes
outside the vessel; there is usually necrosis of the adjacent
tissue and the production of the lesion is favored by lymph
stasis; as the result of injury to the vessel wall, polynuclear
leucocytes in response to chemotaxis, or with milder irritation,
mononuclear cells, wander through the endothelium
and accumulate below it perhaps on account of the greater
impermeability of the middle coat to the passage of cells.
The lesion described does not occur exclusively with interstitial
suppurative pneumonia caused by hemolytic
streptococci, but has been found in association with abscess
formation (Autopsies 354 and 383) caused by hemolytic
streptococci or (Autopsy 322) caused by staphylococci.
In 1 instance it has been found with lobar pneumonia (Autopsy
320) caused by atypical Pneumococcus II and in 2
221instances with combined lobar and bronchopneumonia
(Autopsy 357 with Pneumococcus IV; Autopsy 392 with
Pneumococcus II). In these 3 instances there has been interstitial
inflammation, edema and lymphangitis without
suppuration.
Interstitial suppurative pneumonia of long standing may
occasionally be accompanied by chronic changes which
bring about thickening of the interlobular tissue. In the
following autopsy acute suppurative inflammation in the
left lung has been associated with conspicuous thickening
of interlobular septa in the right lung.
Autopsy 474.—I. H., white, aged twenty-one, was a native of Oklahoma
and had been in military service one month. His illness began with influenza
thirty-six days before death; he was admitted to the base hospital thirty-one
days before his death with signs of pneumonic consolidation of the right
lower lobe. Evidence of fluid in the right pleural cavity was obtained two
weeks before death, and from 100 to 700 c.c. of thick purulent fluid were aspirated
on five occasions. Hemolytic streptococci were found in the aspirated
fluid.
Anatomic Diagnosis.—Interstitial suppurative pneumonia in left lung;
abscess of right lower lobe with rupture into pleural cavity; thickening of
interlobular septa of right lower lobe; double purulent pleurisy with thoracotomy
on right side; serofibrinous pericarditis.
The right pleural cavity contains 85 c.c. of thick purulent
fluid; the right lung (Fig. 9) is collapsed and pushed to the
median line, being bound by firm adhesions to the pericardium.
Over the external and basal surfaces is a localized
cavity walled off by adhesions. An abscess cavity in the
lower part of the lower lobe communicates through a perforation
in the basal surface of the lung with the pleural
cavity and is in free communication with a small bronchus.
About the abscess the lung is red and laxly consolidated,
but elsewhere air containing; throughout the lower half of
the lower lobe, the interlobular septa are marked by conspicuous
yellowish gray lines about 1 mm. in thickness.
Between these thickened septa the lung tissue contains air.
The lung weighs 600 grams. The left lung (Fig. 10) is voluminous
and heavy, weighing 1,320 grams. The surface is
222everywhere covered by thickened pleura and fibrin, the
pleural cavity containing 150 c.c. of thick purulent fluid.
The lung is consolidated varying in color from a fleshy red
to yellowish gray. The surface is very conspicuously
marked by yellow lines 2 or 3 mm. thick, corresponding to
the interlobular septa which have undergone suppuration.
The septa have bead-like swellings along their course, and
when pus escapes from the cut surface small cavities remain
at the site of these swellings.
Bacteriologic examination has shown hemolytic streptococci
in the blood, left lung, right and left pleural cavities,
and right bronchus. B. influenzæ has been found in the
bronchus, in the right pleura and in the heart’s blood. A
few colonies of S. aureus have been found on the plate
from the right pleural cavity (site of thoracotomy).
Microscopic examination of the right lower lobe shows
that the interstitial septa are much thickened by young
fibrous tissue infiltrated with lymphoid and a few plasma
cells. Large mononuclear cells with granular cytoplasm are
very numerous. A lymphatic is much distended and contains
a few polynuclear leucocytes and many lymphoid and
large mononuclear cells. There is no suppuration. Sections
from the right lung show suppurative lymphangitis
with suppurative inflammation of interstitial tissue.
The right lung is the site of a healing lesion of the interstitial
tissue which has developed simultaneously with
acute interstitial suppurative pneumonia in the left lung.
Both lesions are doubtless caused by S. hemolyticus. This
healing lesion exhibits little similarity to the interstitial
bronchopneumonia described by several observers with
both measles and influenza.
The following autopsy furnishes further evidence that
interstitial suppurative pneumonia exhibits a tendency to
heal. Proliferation of endothelial cells lining the inflamed
lymphatics gives rise to phagocytic cells which aid in removing
the accumulated leucocytes.
223Autopsy 397.—N. P., white, aged twenty-one, farmer, a native of Oklahoma,
had been in military service twenty-one days. Illness began twenty-two
days before death, the patient being admitted on the day following onset
with influenza, pharyngitis and bronchitis. A diagnosis of lobar pneumonia
was made fourteen days before death. The left pleural cavity was aspirated
twelve days later and 800 c.c. of thick yellow pus were withdrawn. Hemolytic
streptococci were found in the sputum five days before death.
Anatomic Diagnosis.—Interstitial suppurative pneumonia in left upper
lobe; acute bronchopneumonia with lobular consolidation in right upper lobe;
localized purulent pleurisy on left side with compression and atelectasis of
left lung; compensatory emphysema of right lung; purulent bronchitis; beginning
serofibrinous pericarditis; chronic passive congestion of liver, spleen
and kidneys.
The right lung is very voluminous, free from coal pigment and bright
pink save over lobular patches of consolidation which have a bluish red color;
the bronchi contain mucopurulent material. The anterior surface of the left
lung is bound to the chest wall by firm adhesions, but over the external and
posterior surfaces of the lung there is a localized cavity containing 1,100 c.c.
of turbid fluid. The left lung is collapsed and airless with deep fleshy red
color. In the upper lobe there are scattered patches of consolidation 1.5 to
2.5 cm. across where the tissue is grayish red and coarsely granular. In the
adjacent tissue interstitial septa are thickened to 1 or 2 mm. and are conspicuous
as gray bands. Along their course occur bead-like swellings from
which purulent fluid can be scraped. These septa at one point reach the
anterior surface of the lung where the pleural cavity is in large part obliterated
by adhesions; here there is an encapsulated pocket 4 x 1.5 cm. containing
thick creamy pus.
Bacteriologic examination of the blood shows the presence of hemolytic
streptococci; cultures from the lungs contain hemolytic streptococci and B.
influenzæ.
Microscopic examination shows that interlobular septa are thickened and
infiltrated with plasma cells in large number. Leucocytes in the center of
much dilated lymphatics have undergone necrosis and have lost their nuclear
stain. About the periphery of the lumen and evidently derived from the
swollen endothelial cells which surround it, are numerous large mononuclear
cells. They act as phagocytes and ingest polynuclear leucocytes. Multinucleated
giant cells, derived from these cells, occur. In several places thrombosed
lymphatics in process of organization occur; the lumen is filled with
compact fibrin which is invaded by fibroblasts and newly formed capillaries.
The process just described is analogous to that which occurs
whenever an unopened abscess heals; mononuclear
cells accumulate and act as phagocytes ingesting polynuclear
leucocytes.
224The following instance of streptococcus empyema is noteworthy
because no suppurative pneumonia has been found
in association with it. Nevertheless the character of the
changes present in the lung indicate that the organ has
been the site of an interlobular inflammation which has
healed.
Autopsy 499.—J. H. M., white, aged twenty-four, a farmer from Arkansas,
had been in military service five months. Onset of illness began two
weeks before his admission to the hospital on November 15 with cough, fever,
headache and malaise; on admission there was acute bronchitis. Thirteen
days after admission the patient developed parotitis (mumps?); five days
later and five days before death pleurisy was recognized on the right side
and pneumonia was suspected. Death occurred thirty-six days after onset.
The temperature on admission was 103.2° F. and remained elevated during
one week falling by lysis; from this time until the pleurisy was recognized
it was normal and later it remained approximately 103° F.
Anatomic Diagnosis.—Fibrinopurulent pleurisy on right side; fibrinous
pleurisy on left side; fibrinopurulent pericarditis; chronic interstitial (interlobular)
pneumonia in process of healing; purulent bronchitis; acute splenic
tumor; parenchymatous degeneration of kidneys.
The right pleural cavity contains 1,650 c.c. of grayish yellow fluid containing
an abundant sediment of softened fibrin. Part of this fluid, more
opaque than the remainder is confined in a localized pocket between the inner
surface of the lung and the pericardium. The apex and anterior surface
of the right upper lobe, over an area about 7 cm. across, is held by fibrinous
adhesions to the chest wall; when this adhesion is broken a pocket is exposed
6.5 x 2.5 cm. containing fibrin and fluid. The pericardial cavity is distended
by 350 c.c. of turbid yellow seropurulent fluid. The pericardial surfaces are
covered by shaggy, tough gray fibrin.
The right lung is collapsed; the lower and posterior part of the upper
lobe is deep red and atelectatic. Throughout the upper lobe the interlobular
septa are thickened, often 1 mm. across and very conspicuous; in the lower
and anterior tip of the lobe is an area where tissue is firm grayish red and
heavier than water. The lower and posterior half of the right lower lobe
is firm and airless, and the tissue is reddish gray or gray and in places finely
granular on section; interlobular septa are conspicuous. Although the lung
is cut into thin sections, no abscesses are found. Bronchi throughout the lung
contain mucopurulent fluid.
The left lung over its lower half is covered by a thin layer of fibrin. The
tissue is crepitant throughout and moderately edematous. Bronchi contain
mucopurulent fluid.
Hemolytic streptococci in pure culture are obtained from the blood of
the heart, right pleural cavity and pericardium. No growth is obtained
on a plate inoculated with material from the right lower lobe. The right
bronchus contains hemolytic streptococci and B. influenzæ.
225The pleural surface of the right lung is covered by a thick layer of fibrin
which has undergone advanced organization. Fibrous septa within the lung
are much thickened by the presence of newly formed fibrous tissue; the interstices
of the tissue are distended and contain fibrin into which fibroblasts
and new blood vessels have penetrated. Some lymphatics are plugged with
fibrin and contain polynuclear leucocytes, lymphoid and large mononuclear
cells. In several places organization of these thrombi is beginning. About
the blood vessels are thrombosed lymphatics in which polynuclear leucocytes
and mononuclear cells are equally abundant. Alveoli immediately adjacent
to blood vessels and to fibrous septa often contain fibrin, and alveoli elsewhere
contain desquamated cells in abundance.
In association with hemolytic streptococci in the blood,
pleura and pericardium, there has been inflammation of the
interlobular septa of the lungs with acute lymphangitis;
there has been no suppuration and the lesion is in process
of healing with new formation of fibrous tissue. It is evident
that this lesion, as well as pleurisy with advanced organization,
preceded the exacerbation of the patient’s illness
which occurred five days before death. The advanced
chronic changes found at autopsy indicate that the pulmonary
and pleural lesions had their origin during the
illness which was present at the time of admission to the
hospital. Interstitial pneumonia caused by hemolytic
streptococci was of mild character and did not produce
suppuration within the lung; nevertheless, hemolytic streptococci
which reached the pleura caused empyema.
Suppurative Pneumonia with Multiple Clustered Abscesses Caused by Staphylococci
In the preliminary report of this commission published
in The Journal of the American Medical Association, loc.
cit., pg. 111, we described suppurative pneumonia with multiple
abscesses caused by staphylococci and cited 4 instances
of the lesion which followed influenza. Chickering and
Park[84] published in a subsequent number of the same journal
226an account of staphylococcus pneumonia, a lesion which has
heretofore attracted very little attention.
In a small group of cases abscesses in the lungs have had
characters which serve to distinguish them from the abscesses
previously described. Small, sharply circumscribed
yellow nodules, which in their centers have undergone suppurative
softening, form a cluster upon a red, airless background
(Figs. 15 and 16). One or more of these groups
several centimeters across, occur in the lungs. It is usually
evident that the abscesses are clustered about a medium-sized
bronchus, but occasionally with increase in the size
of the small cavities the lung tissue assumes a honey-combed
appearance.
These clustered abscesses occur in association with bronchopneumonia
and have been in all instances associated
with purulent bronchitis. The mucosa of the small bronchi
may be destroyed so that the surface is eroded. These
small clustered abscesses are seen as conspicuous yellow
spots immediately below the pleura, but there has been no
associated empyema. In 2 instances these abscesses were
accompanied by fibrinous pleurisy, but in the remaining autopsies
the pleura has been normal. The infrequency of
empyema is in contrast with its almost invariable presence
when a streptococcus abscess is found below the pleura.
Autopsy 280.—Onset of illness with malaise, headache, cough and fever
was on September 24, eight days before death. At autopsy there were hemorrhagic
peribronchiolar and lobular bronchopneumonia, clustered foci of suppuration
in right lung, purulent bronchitis and fibrinous pleurisy. Hemolytic
streptococci were obtained from the consolidated lung and from a
bronchus. A culture from the right lung was contaminated. In the bronchus
were found B. influenzæ and a few staphylococci. Microscopic examination
of the abscesses shows that they contain Gram-staining cocci grouped into
staphylococcus-like colonies.
Autopsy 286.—Duration of illness, which began September 25 with
symptoms of influenza, was nine days. At autopsy there were lobular and
confluent patches of bronchopneumonia, clustered abscesses in the right lung
below the pleura, purulent bronchitis, and serofibrinous pleurisy localized
in the neighborhood of the abscesses. Pneumococcus IV was obtained from
the blood of the heart, and Pneumococcus IV, staphylococci and B. influenzæ
from the right main bronchus; growth failed to occur on plates from right
and left lungs. Microscopic examination shows the presence of clumps of
cocci with staphylococcus grouping in the centers of the small abscesses.
Section through one abscess shows its continuity with the wall of a bronchus;
along one side of the abscess is epithelium composed of flattened epithelial
cells in multiple layers continuous with that of the bronchus; the remainder
of the abscess wall is formed by disintegrated lung tissue.
227
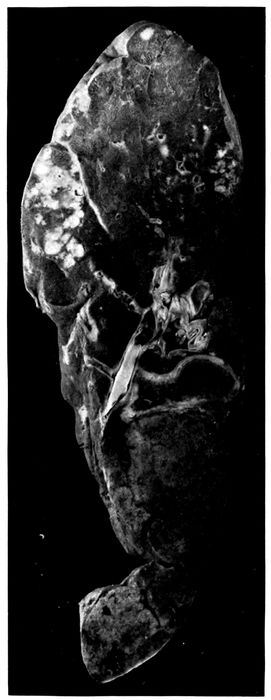
Fig. 15.—Abscesses in two clusters caused by S. aureus in upper part of right upper lobe; confluent lobular consolidation in lower part of lobe. Autopsy 333.
228

Fig. 16.—Abscesses in cluster caused by S. aureus at apex of right upper lobe. Autopsy 322.
Autopsy 322.—The patient was admitted with influenza eight days before
death; signs of pneumonia appeared two days later, and on the following
day Pneumococcus IV was obtained from the sputum. At autopsy
there were bronchopneumonia with lobar consolidation, abscesses clustered
about a bronchus in the right upper lobe and purulent bronchitis. The
blood was sterile; S. aureus was obtained from the consolidated part of
the left lung; S. aureus and Pneumococcus III from the abscesses of the right
lung. Microscopic examination of sections of abscesses showed the presence
of Gram-staining cocci in staphylococcus-like colonies, surrounded by
necrotic material and polynuclear leucocytes; Gram-negative bacilli resembling
B. influenzæ were seen. (See Fig. 16.)
229Autopsy 333.—The onset of influenza was fifteen days before death; a
diagnosis of pneumonia was made seven days before death. At autopsy there
were confluent bronchopneumonia, clustered abscesses in the right lung and
purulent bronchitis (no pleurisy). The blood contained Pneumococcus II
atypical. S. aureus and Pneumococcus II atypical were obtained from the
abscesses; S. hemolyticus, from the consolidated left lung; S. aureus, B. influenzæ
and a few hemolytic streptococci, from the bronchus. (See Fig. 15.)
Autopsy 370.—The patient was admitted seventeen days before death
and signs of pneumonia were noted three days after admission. At autopsy
there were lobular and confluent bronchopneumonia and small abscesses clustered
about bronchi and situated within the gray consolidated lung; purulent
bronchitis and patches of atelectasis, with distention of the lungs, so that they
failed to collapse on removal. No growth was obtained from the heart’s
blood; S. aureus in pure culture was obtained from the abscesses of the right
lung; S. aureus, Pneumococcus IV and B. influenzæ were obtained from a
small bronchus on the left side.
Autopsy 425.—Illness began with influenza twenty-nine days before
death; a diagnosis of pneumonia was made fourteen days before death. At
autopsy there were chronic bronchopneumonia with tubercle-like nodules of
consolidation with some large patches of consolidation, multiple small abscesses
giving a honey-combed appearance to part of the right middle lobe,
purulent bronchitis and bronchiectasis. S. hemolyticus was grown from the
heart’s blood; S. hemolyticus, B. influenzæ and S. albus from the lung. Sections
of an abscess contain clumps of cocci. An abscess cavity has along one
side remains of a bronchial wall covered by squamous epithelium; a dilated
bronchus, cut longitudinally, terminates in this irregular abscess cavity.
Table XLIX shows the incidence of pneumococci,
hemolytic streptococci, staphylococci and B. influenzæ in
the foregoing autopsies with abscesses clustered about
bronchi:
| Table XLIX |
|---|
| |
|
NO. OF CULTURES |
PNEUMOCOCCI |
HEMOLYTIC STREPTOCOCCI |
STAPHYLOCOCCI |
B. INFLUENZÆ |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
4 |
2 |
50.0 |
2 |
50.0 |
4 |
100.0 |
4 |
100. |
| Lung |
6 |
2 |
33.3 |
3 |
50.0 |
4 |
66.7 |
2 |
33.3 |
| Blood |
6 |
2 |
33.3 |
2 |
33.3 |
|
|
|
|
Staphylococcus shows in the lung the same tendency to
produce localized abscesses which it exhibits in other tissues
of the body; it invades the lung by way of the bronchi,
230but shows no ability to invade lymphatics, and in the cases
we have examined rarely enters the pleura or the blood.
In all of these cases B. influenzæ has been found in the bronchi
and perhaps precedes the staphylococcus as an invader
of the lower respiratory passages. Pneumococci atypical
II, Types III and IV have been found in over half of these
cases. The significance of this organism is emphasized by
the 2 cases in which it has been found in the heart’s blood
at autopsy. It appears not improbable that S. aureus has
invaded the lung already the site of bronchopneumonia
caused by pneumococci.
Notwithstanding the small number of autopsies, the figures
in Table XLIX, showing the incidence of pneumococci,
streptococci, staphylococci and B. influenzæ, are cited so
that they may be compared with the corresponding figures
for the usual type of streptococcus abscess (p. 203). The
incidence of hemolytic streptococci is relatively low,
whereas that of staphylococci approximates 100 per cent.
S. aureus was present in great number in the lung of Autopsies
322 and 333 and in pure culture in the abscess of
Autopsy 370. Microscopic examination of sections from
the abscesses which have been described, demonstrated the
presence of Gram-staining cocci in characteristic staphylococcus-like
clumps within the exudate of the abscesses; scattered
chains of streptococci were not found. In those instances
(Autopsies 280 and 286) in which cultures failed to
demonstrate staphylococci, microscopic examination demonstrated
staphylococcus-like clumps of bacteria within the
abscess cavity. Cultures were usually made from the consolidated
lung near the abscess where the pleural surface
could be seared, rather than from the pus, so that in some
instances the microorganism has doubtless escaped detection
although present.
In association with the multiple abscesses which have
been described, injury to the bronchi and bronchopneumonia
have been invariably present. Purulent bronchitis
231has been present in all instances of this lesion; in 2 instances
there has been dilatation of the bronchi, and in 1
instance in which the onset of influenza was twenty-nine
days before death, there has been advanced bronchiectasis.
Microscopic examination shows that the epithelium of the
bronchi is partially or completely destroyed and that destruction
of the underlying tissue, with acute suppurative
inflammation, penetrates to a greater or less depth into the
wall. When the epithelium of the bronchus is wholly
destroyed and the lumen is filled and distended with polynuclear
leucocytes, a cross section of the tube has the appearance
of a small abscess; but more careful examination
often shows that the engorged mucosa is still intact.
Occasionally, a network of fibrin forms a layer covering the
denuded mucosa. Disintegration of the superficial tissue
may extend to the muscularis or through it, and may penetrate
the wall of the bronchus. The tissue in contact with
the exposed surface contains many polynuclear leucocytes
and blood vessels plugged with fibrinous thrombi, but
deeper in the tissue lymphoid and plasma cells are more
numerous. In 2 instances (Autopsies 286 and 425) favorable
sections have demonstrated that the wall of an abscess
on one side consists of the remains of a bronchus, covered
by epithelium composed of squamous cells, Whereas the
remainder of the wall, here very irregular, is formed by
partially destroyed alveoli plugged with fibrin. The suppurative
process has penetrated the wall of the bronchus
on one side and extended into the surrounding alveolar
tissue. In other instances, abscess cavities occur within
the alveolar tissue of the lung and their relationship to
bronchi is not evident. In the mass of polynuclear leucocytes
which fill the abscess cavity, are clumps of staphylococci
in great abundance, usually forming characteristic
colonies which are conspicuous with the low power of the
microscope.
232
Empyema, Pericarditis and Peritonitis
No sharp line can be drawn between nonpurulent and
purulent pleurisy. A diagnosis of empyema has been
made when the fluid in the chest has become opaque and
fibrin has undergone softening or solution. The lesion
has been designated seropurulent when there has been
abundant thin, opaque, gray fluid. Pleurisy has been
designated fibrinopurulent when the cavity has contained
opaque fluid and ragged soft white or yellowish fibrin adherent
to the chest wall; this fibrin is evidently in process
of disintegration and there may be numerous shreds and
flakes of fibrin which subside to the bottom of the fluid.
The amount of fluid in the cavity may occasionally exceed
1,700 c.c.; that in both pleural cavities may exceed 2,500 c.c.
The lesion has been designated purulent when fibrin has
almost wholly disappeared and the cavity contains thick
yellowish white fluid. In 4 of 5 instances in which thoracotomy
had been performed, empyema has assumed this
otherwise uncommon type.
Some inflammation of the pleura is almost constantly
found in association with all forms of pneumonia, but in
many instances is so slight that it has no noteworthy significance.
Table L shows the incidence of various types of
pleurisy.
| Table L |
|---|
| |
|
LOBAR PNEUMONIA |
BRONCHOPNEUMONIA |
SUPPURATIVE PNEUMONIA WITH ABSCESS |
INTERSTITIAL SUPPURATIVE PNEUMONIA |
| No. |
% |
No. |
% |
No. |
% |
No. |
% |
| No pleurisy noted |
30 |
46.9 |
44 |
55 |
1 |
2.6 |
1 |
5.9 |
| Serous pleurisy |
5 |
7.8 |
9 |
11.2 |
|
|
|
|
| Fibrinous pleurisy |
10 |
15.6 |
5 |
6.2 |
1 |
2.6 |
|
|
| Serofibrinous pleurisy |
12 |
18.2 |
14 |
17.5 |
3 |
7.7 |
|
|
| Seropurulent pleurisy |
|
|
|
|
9 |
23.1 |
1 |
5.9 |
| Fibrinopurulent pleurisy |
7 |
10.9 |
5 |
6.2 |
17 |
43.6 |
12 |
70.6 |
| Purulent pleurisy |
|
|
3 |
3.7 |
8 |
20.5 |
3 |
17.6 |
| Total |
64 |
|
80 |
|
39 |
|
17 |
|
233Empyema has occurred, on the one hand, in 12.4 per cent
of instances of lobar pneumonia and in 9.9 per cent of instances
of bronchopneumonia alone. It has occurred, on
the other hand, in 87.2 per cent of instances of suppurative
pneumonia with abscess formation and in 94.1 per cent
instances of interstitial suppurative pneumonia. These
suppurative lesions are caused by hemolytic streptococci,
and when cultures are made from the pleural exudate this
microorganism is isolated.
Of 16 instances in which empyema has occurred in association
with lobar pneumonia or bronchopneumonia unaccompanied
by suppuration in 6 there has been infection
with hemolytic streptococci. Empyema has occurred in
the absence of hemolytic streptococci only 10 times.
Empyema Caused by Hemolytic Streptococci.—When
necrosis preceding abscess formation has occurred in the
lung, streptococci are found in immense numbers in the
dead tissue. The pleura overlying the abscess undergoes
necrosis and occasionally streptococci are particularly numerous
upon the pleural surface of the necrotic tissue. In
Autopsy 376 a membrane thin as tissue paper, representing
the pleura, separated an abscess containing thick pus from
the pleural cavity which was the site of empyema. The
abscess may rupture into the pleural cavity and at the same
time may be in free communication with a bronchus (Autopsy
480). In one (Autopsy 467) instance an abscess
which had ruptured into the pleural cavity had completely
discharged its contents and was in process of healing,
newly formed fibrous tissue being abundant in its wall.
With few exceptions empyema has accompanied subpleural
abscess caused by hemolytic streptococci, being
found on the side corresponding to the abscess. Among
39 instances of pulmonary abscess, empyema has been
limited to the side of the abscess in 23; it has been present
on the opposite side as well in 10 instances. In 2 instances
there have been abscesses in both lungs; in one (Autopsy
234385 A) there has been double empyema, and in the other
(Autopsy 487) empyema only on the left side. In one instance
abscess has been recognized by microscopic examination
and its location is not recorded. In 5 instances of
abscess formation there has been no empyema. In Autopsy
383 there has been no pleurisy noted; in Autopsy 416 there
has been fibrinous pleurisy and in Autopsies 277, 290 and
380, serofibrinous pleurisy.
Empyema has been almost invariably found in association
with interstitial suppurative pneumonia. This lesion
extends by way of the lymphatics up to the pleural surface
and is often more conspicuous just below the pleura than
elsewhere. Empyema has been absent in only 3 of 21 examples
of the lesion and in one of these there has been
serous effusion. In 12 instances interstitial suppuration
has occurred only on one side and empyema has been limited
to this side; in 5 instances with interstitial suppuration
on one side there has been empyema on both sides;
in 2 instances with interstitial suppuration in both lungs
there has been double empyema.
The amount of fluid in the pleural cavity has varied from
less than 100 to 1,500 c.c. The fluid has occasionally been
seropurulent or yellow, thick and purulent, but in most
instances the exudate is best described as fibrinopurulent.
There is yellow or yellowish gray purulent fluid containing
flakes of soft ragged fibrin.
The foregoing study has shown, on the one hand, that
empyema is a frequent complication of streptococcus pneumonia
and, on the other hand, that empyema following influenza
with relatively few exceptions is caused by hemolytic
streptococci. Empyema caused by this microorganism
exhibits in some instances characters not seen with
other varieties of pleural inflammation. The tissue between
sternum and pericardium is often edematous and the
adjacent fat has a firm brawny consistence. In some instances
the exudate contains blood, and hemolysis has occurred
235so that the fluid has a diffuse red color. The occurrence
of multiple pocketed collections of purulent fluid
within the pleural cavity is peculiar to streptococcus empyema.
These pockets have been found 6 times in association
with abscess and 5 times with interstitial suppurative pneumonia.
In the presence of an exudate within the pleural
cavity, some part of the lung, usually the anterior surface
behind the sternum and costal cartilages, is glued by fibrinous
adhesions to the parietal pleura. Here occur pockets
containing thin purulent fluid and softened fibrin or thicker
creamy pus walled off by fibrin about the edges of the
pocket. At the site of the lesion the lung, after it is separated
from the chest wall, is marked by a shallow depression
surrounded by the fibrin which has walled in the
pocket. The little cavity thus formed, varying much in
size, is usually oval, the long diameter being from 1 to 3 cm.
These pleural pockets may occur over the external surface
of the lung (Autopsies 452, 455, and 472) or between
the internal surface and pericardium (Autopsy 452). Occasionally
with partial fibrinous adhesion between the pleural
surfaces there are both scattered pockets containing
purulent fluid and a larger encapsulated collection of fluid;
in Autopsy 455 the pleural surfaces were adherent and
there was 100 c.c. of purulent fluid encapsulated in a space
over the external surface of the lung, 12 × 8 cm. In Autopsy
452 the lower part of the pleural cavity was encapsulated
and contained 650 c.c. of fluid. This tendency of empyema
caused by S. hemolyticus to form encapsulated pockets is
doubtless of considerable importance in the treatment of
the condition.
Stone, Bliss and Phillips[85] have described these encapsulated
pockets as “subcostosternal pus pockets” and have
maintained that they are formed about the sternal lymphatic
nodes. We have found them so widely scattered
that this relation seems improbable.
236Pneumococcus Empyema.—Empyema occurred in association
with pneumonia referable to pneumococci 10 times,
once with Pneumococcus II; 6 times with Pneumococcus
atypical II; once with Pneumococcus III and twice with
Pneumococcus IV. The lesion was seropurulent once;
fibrinopurulent 8 times and purulent once. Fibrin in several
instances was somewhat voluminous. In the following
instance voluminous masses of fibrin had an important influence
upon the attempted treatment.
Autopsy 473.—A. D. P., white, aged twenty-one, a student from Missouri,
had been in military service two weeks. He was admitted to the
hospital with influenza twenty-eight days before his death, and four days
after admission there were signs of pneumonia. Paracentesis was performed
on the right side on the eleventh day after admission; 4 c.c. of
cloudy fluid which contained Pneumococcus III were obtained at this time
and later in the day 800 c.c. were withdrawn. On the thirteenth day attempted
withdrawal of fluid from both pleural cavities failed. On the
eighteenth day aspiration of the right pleural cavity yielded only 30 c.c.
of fluid. On the nineteenth day 400 c.c. of purulent fluid were withdrawn
from the right pleural cavity. On the twenty-fifth day there was cyanosis
and delirium. Shortly before death aspiration of the right pleural cavity
was attempted, but only 4 c.c. of fluid were obtained.
Anatomic Diagnosis.—Chronic bronchopneumonia with lobular and peribronchiolar
consolidation in left lung; fibrinopurulent pleurisy on both
sides; purulent bronchitis and bronchiectasis.
On removal of the sternum, encysted purulent pleurisy is found between
the inner surface of the right lung and the pericardium; there is
here 450 c.c. of very thick creamy, greenish yellow pus entirely separated
from the remainder of pleural cavity. The external part of the cavity
contains 1,450 c.c. of fluid and voluminous masses of firm fibrin which
placed in a measuring cylinder occupy 450 c.c. The left pleural cavity contains
400 c.c. of seropurulent fluid in which there is abundant sediment
of fibrinous particles.
The right lung is compressed; the bronchi exude purulent fluid. The
left lung is voluminous; in the upper and lower lobes there are small yellowish
gray nodules of consolidation, grouped in clusters, and gray patches
of lobular consolidation occur. Bronchi are dilated and filled with purulent
fluid.
Bacteriologic examination shows the presence of Pneumococcus III obtained
in pure culture from the blood of the heart and from the right
pleural cavity. S. viridans is grown from the left lung; a plate from the
right bronchus contained B. influenzæ, S. viridans and a few colonies of
staphylococcus and M. catarrhalis.
237The foregoing case is particularly noteworthy because
aspiration failed repeatedly to yield more than a few cubic
centimeters of fluid, doubtless because the voluminous
masses of fibrin present in the cavity prevented escape of
fluid. Aspiration was attempted shortly before death, but
only 4 c. c. of fluid were obtained; nevertheless, at autopsy
the right pleural cavity contained 2,350 c.c. of exudate. Another
factor of much importance in relation to treatment
is the encapsulation of 450 c.c. of purulent fluid between the
inner surface of the right lung and the pericardium. It is
possible that free drainage might have emptied the main
cavity and perhaps even freed the encapsulated fluid.
Pericarditis.—Among 241 autopsies on individuals with
pneumonia following influenza, pericarditis occurred 23
times; these lesions were classified as follows: Serous pericarditis,
1; serofibrinous pericarditis, 9; seropurulent pericarditis,
1; fibrinopurulent pericarditis, 10; purulent pericarditis,
2.
It is noteworthy that in 12 of 23 instances of pericarditis
the lesion was associated with S. hemolyticus infection of
the lung and whenever in these instances cultures were
made (Autopsies 434, 485, 499 and 504) hemolytic streptococci
were obtained from the pericardial exudate in pure
culture.
The tendency of interstitial suppurative pneumonia to
produce pericarditis is especially evident. Among 21 instances
of interstitial suppurative pneumonia pericarditis
occurred 6 times (28.6 per cent); among 39 instances of suppurative
pneumonia with abscess formation, pericarditis
occurred twice (5.1 per cent); whereas among all other
autopsies, namely, 181, the lesion occurred 15 times (8.3 per
cent).
Pericarditis occurred in association with pneumonia referable
to Pneumococcus I, once, (Pneumococcus I isolated
from the pericardium); to Pneumococcus II, once; to atypical
Pneumococcus II, 5 times (twice isolated from the pericardium);
238and to Pneumococcus IV, twice (once isolated
from the pericardium).
Peritonitis.—Purulent peritonitis occurred only twice,
in both instances in association with pneumonia caused by
hemolytic streptococci. Purulent peritonitis was part of
a general serositis involving both pleural cavities, pericardium
and peritoneum in 2 noteworthy instances:
Autopsy 465.—J. K., white, aged twenty-two, farmer from Oklahoma,
had been in military service one month. He was admitted to the hospital
with influenza, sore throat and bronchitis twenty-four days before his
death. Signs of pneumonia were recognized thirteen days later and at the
same time there was otitis media on the right side. Empyema and pericarditis
were found three days before death and two days later 1000 c.c.
of cloudy fluid were withdrawn from the chest.
Anatomic Diagnosis.—Suppurative pneumonia with consolidation and
abscess in right lower lobe below pleura; purulent pleurisy on right, seropurulent
pleurisy on left side; beginning serofibrinous pericarditis; fibrinopurulent
peritonitis; purulent bronchitis.
The body is emaciated. The right pleural cavity contains 350 c.c. of
thick, creamy yellow pus in which are flakes of fibrin; the right lung
is collapsed and lies at the back and inner side of the cavity. The left
pleural cavity contains 500 c.c. of turbid, yellow, seropurulent fluid in which
is soft fibrin. The lower lobe of the right lung is consolidated throughout,
flabby, gray red and finely granular on section. Below the pleura of the
posterior border is a wedge-shaped cavity with its base 1.5 cm. across, in
contact with the pleural surface. About the cavity consolidated tissue has
an opaque, yellow color. Bronchi in both lungs contain mucopurulent fluid.
The pericardial cavity contains 20 c.c. of turbid fluid; the left auricular
appendage is bound by a thin layer of fibrin to the parietal pericardium.
The peritoneal cavity contains 100 c.c. of thick, creamy, yellow, purulent
fluid. Between the diaphragm and liver is a layer of fibrin, in places 1.5
cm. in thickness; fibrin is present upon the peritoneum overlying the kidneys
and base of mesentery.
Bacteriologic examination shows the presence of hemolytic streptococci,
obtained in pure culture from the blood of the heart, right pleural cavity
and peritoneum. From the right bronchus are grown S. hemolyticus, B.
influenzæ and a few colonies of S. viridans and staphylococcus.
Autopsy 504.—G. R. C., white, aged twenty-eight, farmer from Alabama,
had been in military service three months. Onset of illness occurred six
days before death, and two days later he entered the hospital with fever
(103.4° F.), pains in the abdomen and vomiting. Consolidation at the bases
of the lung was recognized on the day following admission and on the day
before death 900 c.c. of greenish brown fluid were aspirated from the left
pleural cavity.
239Anatomic Diagnosis.—Interstitial suppurative pneumonia with consolidation
in left lower lobe; purulent pleurisy on both sides; purulent pericarditis;
purulent peritonitis; parenchymatous degeneration of kidneys;
acute splenic tumor.
The body is that of a large well-nourished man. The left pleural cavity
contains 975 c.c. of creamy, yellow fluid; right pleural cavity contains 425
c.c. of purulent fluid thinner than that on the left side. The left lung
is collapsed; the posterior and lower half of the lower lobe is consolidated,
flabby, deep red and fleshy in appearance. The interstitial septa are yellow,
thickened with bead-like enlargements and contains creamy purulent
fluid which flows away and leaves small cavities. This interstitial suppuration
is more advanced below the outer surface of the lobe than elsewhere.
The pericardial cavity contains 25 c.c. of creamy, yellow, purulent,
fluid; the epicardium is dull, covered in a few places by a small amount
of fibrin and below it are ecchymoses.
The peritoneal cavity contains 100 c.c. of thick, yellow pus; the peritoneal
surfaces are injected and between the liver and diaphragm is
fibrin.
Bacteriologic examination shows the presence of S. hemolyticus in pure
culture from the blood of the heart, the lower lobe of the left lung, pericardium
and peritoneum. The right main bronchus contains the same
microorganism, B. influenzæ and a few staphylococci.
General serositis has been caused by hemolytic streptococci
which in one instance have entered the pleura from
a subpleural abscess, and in the other from the suppurating
interstitial tissue of the lung. In one of these cases the
patient entered the hospital with symptoms suggestive of
acute peritonitis.
Bronchiectasis
Acute dilatation of the bronchi is a common result of
the bronchitis of influenza, and its frequent occurrence is
an index of the severity of the changes in the bronchial
wall. In some instances the smaller bronchi in well-localized
areas are uniformly dilated; in other instances, large
cavities, several centimeters in diameter, are formed and
all transitions between the two extremes occur.
The occurrence of bronchiectasis following influenza is
mentioned by Leichtenstern[86]. He states that evidence of
240bronchiectasis can persist for weeks or months and nevertheless
end with complete restitution of the lungs to normal.
Lord[87] has described instances of bronchiectasis occurring
in association with infection by B. influenzæ and Boggs[88]
has recorded similar observations.
We have had abundant opportunity to observe early
stages in the production of bronchiectasis and to study the
much discussed pathogenesis of the condition.
The following figures show the predilection of bronchiectasis
for the left lung and for the lower lobes: Bronchiectasis
occurred 30 times in the left lung alone, 9 times in
the right lung alone and 13 times in both lungs, the total
being 52. Among 30 instances in which the lesion occurred
only in the left lung, in 24 it was limited to the lower lobe,
and in 15 of these 24 instances to the base of the lower lobe.
Among 9 instances in which dilatation of bronchi occurred
only in the right lung, it was limited to the lower lobe in
4 instances and to the base of the lower lobe in 2 of these
4 instances.
When the lesion is limited to the base of the lower lobes
small bronchi with no recognizable cartilage in their wall
are dilated to a diameter of from 3 to 6 cm. and are distended
with thick mucopurulent fluid. The tenacious character
of the bronchial contents and the action of gravity
doubtless have a part in the production of the dilatation.
In several instances dilatation of the bronchi was limited
to the basal parts of both upper and lower lobes.
When bronchiectasis occurs throughout a whole lung,
usually the left, or in both lungs, the lesion is more advanced
and conspicuous (Fig. 26). There is diffuse dilatation
of small and medium-sized bronchi. Dilated bronchi
with deeply injected mucosa and filled with yellow mucopurulent
fluid, are seen throughout the sectioned lung. A
bronchus cut longitudinally may have a nearly uniform
241diameter of from 5 to 9 mm. for a distance of 5 or 6 cm.,
maintaining this diameter to within 1 cm. of the pleural
surface, where normally only small bronchi occur.
More advanced bronchiectasis is represented by the occurrence
of spherical bronchiectatic cavities, having a
diameter from 1 to 2.5 cm. In some instances there have
been two or three of these cavities but occasionally there
may be many. Cylindrical dilatation of the bronchi usually
occurs widely distributed in the lungs. In Autopsy
440 a small bronchus, cut longitudinally, was dilated to a
diameter of 5 mm. for a distance of 5 cm. and terminated
in a spherical cavity 2 cm. in diameter; there was another
smaller spherical cavity nearby and dilated bronchi occurred
elsewhere. In Autopsy 467, in the upper part of
the lower lobe, two spherical cavities 1 and 1.5 cm. in diameter
communicated with a bronchus of medium size.
Autopsies with bronchiectasis are listed in the order of
the duration of illness to show the parallel increase in the
severity of the lesion (Table LI). In 2 instances (Autopsies
244 and 314) bronchiectatic cavities surrounded by firm
fibrous tissue have evidently existed before the onset of the
fatal illness, which has lasted in one instance approximately
four and in the other six days; these autopsies have been
omitted from the table.
The table shows that bronchiectasis observed within
twelve days after onset of illness with symptoms of influenza
is moderately advanced and almost invariably limited
to the left lower lobe and usually to the base of the lobe.
Advanced dilatation, indicated by the formation of spherical
or cylindrical cavities, occurs with increasing frequency
as the duration of the respiratory disease increases.
Bronchiectasis has been almost invariably associated
with purulent bronchitis. The dilated bronchi contain mucopurulent
material and throughout the lungs the same condition
is usually widespread. Among 137 instances of purulent
bronchitis bronchiectasis consequent upon influenza
has been present in 50.
| 242 |
| Table LI |
|---|
| |
| NO. OF AUTOPSY |
DURATION OF ILLNESS IN DAYS |
TYPE OF PNEUMONIA |
LOCATION OF BRONCHIECTASIS |
CHARACTER OF BRONCHIECTASIS |
BACTERIA IN BRONCHUS |
| 394 |
5 ? |
Broncho |
Rt. base |
Dilatation |
|
| 359 |
7 + |
Lobar and broncho |
Lt. lower lobe |
Dilatation |
|
| 322 |
8 |
Abscess (staph.) |
Lt. base |
Dilatation |
|
| 325 |
8 |
Interst. suppuration |
Lt. base |
Dilatation |
S. hem., B. inf., staph. |
| 352 |
8 |
Lobar and broncho |
Lt. lower lobe |
Advanced dilatation |
|
| 429 |
8 ? |
Broncho |
Rt. base |
Dilatation |
|
| 288 |
10 |
Abscess |
Lt. base |
Dilatation |
S. hem., B. inf. |
| 374 |
10 |
Lobar and broncho |
Rt. and lt. lungs |
Advanced dilatation |
|
| 376 |
10 |
Abscess |
Lt. base |
Dilatation |
S. hem. |
| 437 |
11 |
Lobar |
Rt. lower lobe |
Advanced dilatation |
|
| 482 |
11 |
Broncho |
Lt. base |
Dilatation |
B. inf., Pneum. IV, S. hem. |
| 489 |
11 |
Lobar and broncho |
Lt. lung |
Dilatation |
B. inf., Pneum. IV. |
| 287 |
12 |
Lobar and broncho |
Lt. lower lobe |
Advanced dilatation |
Pneum. IV., B. inf., staph. |
| 289 |
12 |
Broncho |
Lt. lower lobe |
Advanced |
Pneum. IV., B. inf. staph. |
| 295 |
12 |
Interst. sup. and abscess |
Rt. lung |
Advanced dilatation |
S. hem., B. inf. |
| 336 |
12 |
Broncho |
Lt. base |
Dilatation |
|
| 375 |
12 |
Broncho |
Rt. and lt. bases |
Dilatation |
|
| 422 |
12 ? |
Lobar and broncho |
Lt. base |
Dilatation |
|
| 381 |
13 |
Abscess |
Lt. base |
Spherical |
|
| 391 |
13 |
Lobar and broncho |
Lt. lung |
Dilatation |
|
| 401 |
14 ? |
Lobar and broncho |
Rt. and lt. lungs |
Spherical |
|
| 402 |
14 |
Chronic broncho |
Rt. lower lobe |
Dilatation |
|
| 410 |
14 ? |
Abscess |
Rt. upper lobe |
Dilatation |
|
| 333 |
15 |
Abscess (staph.) |
Lt. upper lobe |
Dilatation |
S aur., B. inf. S. hem. |
| 389 |
15 |
Interst. suppuration |
Lt. lung |
Advanced dilation |
|
| 412 |
15 |
Lobar and broncho |
Lt. lower lobe |
Cylindrical |
|
| 398 |
16 |
Broncho |
Rt. and lt. lungs |
Advanced dilatation |
|
| 423 |
16 |
Broncho |
Lt. base |
Dilation |
|
| 243488 |
16 |
Abscess |
Lt. lower lobe |
Dilatation |
S. hem., Pneum. atyp. II. |
| 312 |
17 |
Broncho |
Rt. and lt. lungs |
Dilatation |
S. hem., B. inf. staph. |
| 372 |
17 |
Broncho |
Rt. lung |
Dilatation |
|
| 385 C |
17 |
Interst. suppuration |
Lt. base |
Dilatation |
|
| 448 |
17 |
Broncho |
Lt. lung |
Dilatation |
|
| 460 |
17 |
Abscess |
Lt. lower lobe |
Spherical |
S. hem., B. inf., staph. |
| 291 |
18 |
Broncho |
Lt. base |
Advanced dilatation |
B. inf., staph. |
| 296 |
18 |
Abscess |
Lt. base |
Dilatation |
S. hem., B. inf., |
| 387 |
19 |
Abscess |
Rt. and lt. lungs |
Advanced dilatation |
S. hem., B. inf., S. aur. Pneum. II. |
| 421 |
19 |
Chronic broncho |
Rt. lung |
Advanced dilatation |
|
| 440 |
19 |
Chronic broncho |
Rt. and lt. lungs |
Spherical |
B. inf., S. aur. |
| 419 |
20 |
Broncho |
Rt. lung |
Dilatation |
Pneum. II, B. inf. |
| 463 |
20 |
Chronic broncho |
Rt. and lt. lungs |
Spherical |
B. inf., staph., Pneum. IV |
| 431 |
23 |
Chronic broncho |
Lt. base |
Dilatation |
|
| 468 |
23 ? |
Lobar and broncho |
Lt. lung |
Dilatation |
S. aur., B. inf., S. vir. |
| 465 |
25 ? |
Broncho |
Lt. base |
Dilatation |
S. hem., B. inf., staph., S. vir. |
| 445 |
27 |
Broncho |
Lt. lower lobe |
Spherical |
S. aur. |
| 449 |
27 |
Abscess |
Rt. and lt. lungs |
Spherical |
S. hem., B. coli. |
| 378 |
28 |
Abscess |
Lt. base |
Cylindrical |
S. hem., B. inf., Pneum. atyp. II. |
| 473 |
28 |
Chronic broncho |
Lt. lung |
Advanced dilatation |
B. inf., S. vir., staph., M. catarr. |
| 425 |
29 |
Abscess (staph.) |
Rt. and lt. lungs |
Cylindrical |
|
| 467 |
30 |
Abscess |
Rt. lower lobe |
Spherical |
S. hem., B. inf. |
| 472 |
37 |
Chronic broncho |
Rt. and lt. lungs |
Advanced dilatation |
B. coli |
| 487 |
55 |
Abscess |
Rt. and lt. lungs |
Cylindrical |
B. inf. S. hem. |
244The bacteriology of autopsies with bronchiectasis is
shown in Table LII.
| Table LII |
|---|
| |
|
NO. EXAMINED |
PNEUMOCOCCUS |
S. HEMOLYTICUS |
STAPHYLOCOCCUS |
B. INFLUENZÆ |
| NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
NO. POSITIVE |
PER CENT POSITIVE |
| Bronchus |
29 |
9 |
31.0 |
15 |
51.7 |
16 |
55.2 |
23 |
79.3 |
| Lung |
37 |
16 |
43.2 |
18 |
48.6 |
10 |
27.0 |
19 |
51.4 |
| Blood |
50 |
12 |
24.0 |
22 |
44.0 |
|
|
|
|
Comparison of the percentage incidence of the organisms
which have to be found associated with bronchiectasis and
with purulent bronchitis unaccompanied by bronchiectasis
shows that there is no noteworthy difference in the occurrence
of pneumococci, hemolytic streptococci or B. influenzæ
within the bronchi. When allowance is made for the
difficulty of demonstrating B. influenzæ in the presence of
a large number of other microorganisms, it is not improbable
that this organism has been constantly present in the
purulent contents of the bronchi with purulent bronchitis,
with and without bronchiectasis. Pneumococci, streptococci
and staphylococci are each present in the bronchi in
about one-half of the instances of bronchiectasis and mixed
infections are very common, S. viridans, B. coli and M.
catarrhalis being occasionally found in the bronchi. The
table shows that pneumococci, streptococci and staphylococci
show no greater tendency to enter the lungs and
blood when bronchiectasis and purulent bronchitis coexist
than with purulent bronchitis alone.
Moderate dilatation of the small bronchi at the base of
the left lung was found in several instances eight days
after onset of symptoms referable to the respiratory passages.
Advanced, diffuse dilatation of the bronchi was
seldom seen before the lapse of two weeks, and bronchiectasis
with formation of spherical or cylindrical cavities
245was found with few exceptions three weeks after onset of
the fatal illness. Long continued, purulent bronchitis does
not necessarily produce dilatation of the bronchi. It is
noteworthy that the average duration of the fatal illness
in 137 instances of pneumonia and purulent bronchitis with
no bronchiectasis was 12.5 days, whereas the average duration
of 49 instances of pneumonia with purulent bronchitis
and bronchiectasis was only 16.5 days.
Bronchiectasis is almost invariably associated with purulent
bronchitis in which tenacious mucopurulent fluid accumulates
in the bronchi. It begins at the bases of the
lower lobes and is usually more advanced here than elsewhere.
Mechanical distention of the small bronchi by
viscid fluid, expelled with difficulty, brings about their dilatation
and gravity appears to have a part in accentuating
the process. Histologic examination of the changes
accompanying bronchitis show that lesions which penetrate
into the muscular layer and presumably weaken the bronchial
wall are not uncommon and partial or complete destruction
of the wall may result. To what extent infiltration
of the muscular wall by polynuclear leucocytes or by
lymphoid and plasma cells is accompanied by changes which
weaken the wall may be questioned. When the epithelial
lining of the bronchus is destroyed coagulative necrosis of
the underlying tissue occurs and may extend a variable
distance into the bronchial wall, not infrequently penetrating
into or entirely through the muscular layer. These
changes furnish an explanation of the occurrence of bronchiectasis
following influenza.
246
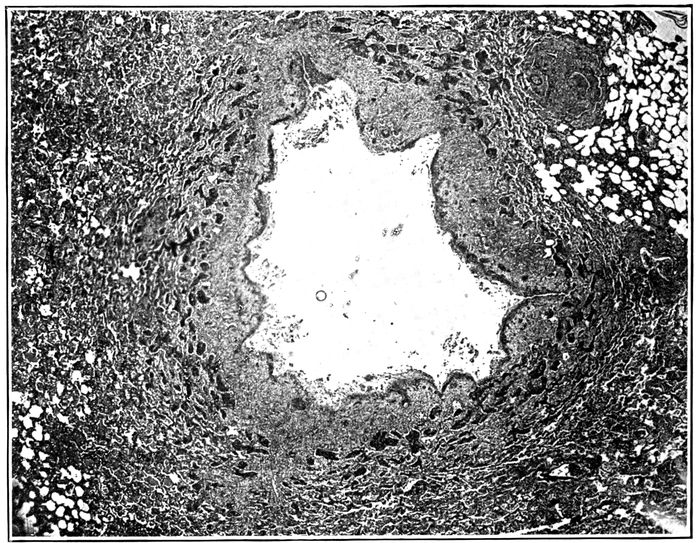
Fig. 17.—Acute bronchiectasis showing fissures penetrating into bronchial wall and at one place entering surrounding alveolar tissue; the surrounding alveoli are filled with fibrin. Autopsy 425.
Acute bronchiectasis may be found following influenza
after the illness has lasted eight or ten days. There is no
increase of fibrous tissue. Small bronchi with no cartilage,
which in normal lungs have a diameter approximating 1
mm., are dilated to 3 mm. or more. The surface epithelium
is wholly or partially lost. Necrosis occurs in places and
extends deep into the tissue, destroying muscle and often
penetrating the entire thickness of the wall which in these
small bronchi consists in large part of fibrous tissue containing
greatly engorged blood vessels. In this necrotic
material nuclei are absent and the tissue containing fibrin
stains deeply with eosin. In it occur fissures or tears which
extend from the lumen a variable distance, very frequently
penetrating the entire thickness of the wall and entering
adjacent alveoli (Figs. 17 and 19). Alveoli thus exposed
almost invariably contain plugs of dense fibrin. Where
these rents have occurred, adjacent edges of the bronchial
wall, held together by underlying lung tissue, have separated
from one another, so that the circumference of the
bronchus has been increased (Fig. 18). These breaks in
the continuity of the wall may occur in several places, so
that a fourth or a third of the circumference may be formed
247by exposed alveolar tissue which has become the site of
fibrinous pneumonia (Fig. 20). During life, though the inflamed
bronchus is filled by mucopurulent exudate, distention
of loose alveolar tissue, uniting the interrupted bronchial
wall, is doubtless greater than it appears in the lung
fixed by hardening fluids.
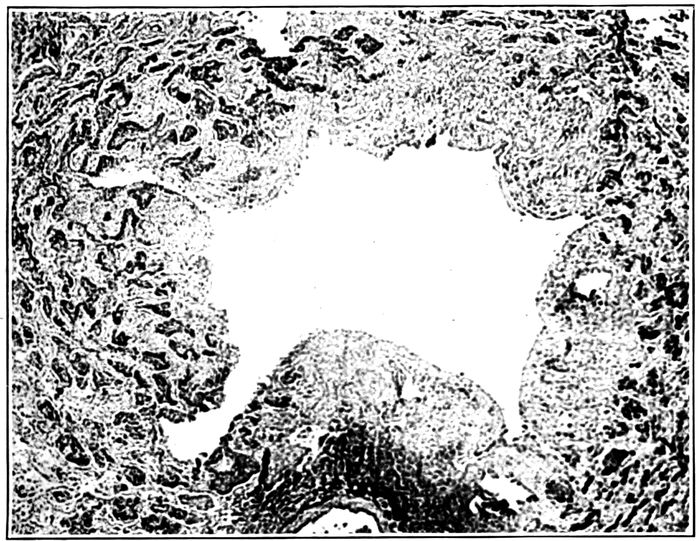
Fig. 18.—Acute bronchiectasis showing fissures in the bronchial wall extending into neighboring alveoli which in zone about are filled with fibrin; one fissure has separated widely; peribronchial fibrinous pneumonia (fibrin is black). Autopsy 425.
Recently dilated bronchi have an irregularly stellate lumen
as the result of clefts penetrating at intervals into or
through the bronchial wall (Fig. 26). Longitudinal fissures
mark the lining of these dilated bronchial tubes.
When the fatal illness has lasted more than two weeks,
abundant new formation of fibrous tissue occurs in a zone
surrounding the dilated bronchus. Adjacent alveolar walls
are thickened by young fibrous tissue. Alveoli, much diminished
in size, are filled by hyaline fibrin into which fibroblasts
248and newly formed blood vessels have penetrated.
These changes are limited to a wide zone in immediate contact
with the dilated bronchus, whereas at a greater distance
alveolar walls have undergone no thickening and
alveoli contain no fibrin.
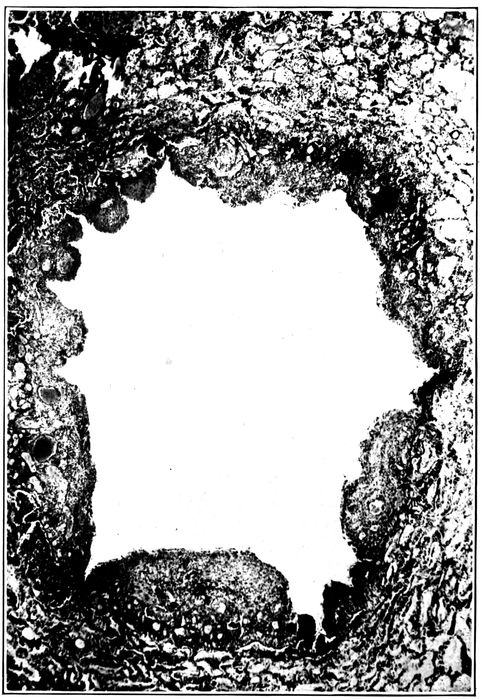
Fig. 19.—Acute bronchiectasis; the bronchial wall indicated by engorged mucosa shows a varying degree of destruction, fissures extending into and through the bronchial wall. Autopsy 352.
249

Fig. 20.—Acute bronchiectasis; with destruction of bronchial wall exposing alveoli filled with fibrin; peribronchial fibrinous pneumonia is seen about several bronchi present in the section; Gram Weigert fibrin stain. Autopsy 425.
This stage is well represented by Autopsy 421 after an
illness of nineteen days. Bronchiectatic cavities, from 3
to 6 mm. in diameter, are numerous in sections of the lung;
their lumina are irregular in outline and often irregularly
stellate. Microscopic examination shows the presence of
250clefts which interrupt the bronchial wall at intervals
throughout its entire circumference. The original wall is
well indicated by the very richly vascularized connective
tissue containing scattered muscle bundles and is infiltrated
with lymphoid and plasma cells in great number.
Where fissures have occurred the adjacent edges of the interrupted
wall have separated from one another, leaving
a wide interval where underlying alveolar tissue is exposed.
Two changes tend eventually to render the fissures inconspicuous,
namely, regeneration of epithelium and new formation
of fibrous tissue. Exposed alveoli filled with fibrin
are in process of organization and epithelium which has assumed
a squamous type has grown down over the exposed
surfaces of the interrupted bronchial wall. It has begun to
cover or in some instances has completely covered the surface
of rents entering alveoli plugged with fibrin (Fig. 21).
In the periphery of the bronchus alveolar walls are thickened
and infiltrated with lymphoid and plasma cells. The
same changes affect bronchi containing cartilage which is
undergoing atrophy.
The reinforcement of the fissured bronchial wall by new
formation of fibrous tissue, by thickening of the interalveolar
walls and by organization of fibrin within the alveoli is
well shown after four weeks (Autopsy 425; Fig. 28).
There are spherical bronchiectatic cavities more than a centimeter
in diameter surrounded by a dense fibrous wall in
which are atrophied alveoli lined by epithelium of cubical
form. Occasionally, the fibrous wall is interrupted and alveoli,
plugged with organizing fibrin, are in immediate contact
with the lumen. When these plugs of fibrin which are
slowly absorbed disappear, evidence of preexisting rents in
the bronchial wall are lost, and there are in this lung bronchiectatic
cavities of which the wall is a continuous circle
of dense fibrous tissue.
251

Fig. 21.—Bronchiectasis with fissures extending through the bronchial wall into alveolar tissue which is the site of fibrinous pneumonia; epithelium has grown down into these fissures and has covered the exposed surfaces. Autopsy 463.
252

Fig. 22.—Regeneration of epithelium over fissures which have been formed in the wall of a bronchus; the epithelium in the neighborhood of and within the fissure is squamous.
Epithelium lining the dilated bronchi is at times completely
destroyed (Fig. 28), but more frequently it persists
in part. That which remains has almost constantly the
character of squamous epithelium (Figs. 22 and 23). The
lowermost cells are cubical; those above them are polygonal,
tending to become flatter as the surface is approached;
upon the surface are cells often much flattened
and occasionally they have lost their nuclei and stain deeply
with eosin as the result of superficial necrosis. The change
should not be regarded as metaplasia, for the epithelium
assumes this squamous type when the superficial columnar
cells have been lost. Actual necrosis of superficial ciliated
columnar cells is occasionally seen (Autopsy 352); injured
cells have separated from one another and desquamated
253into the lumen of the bronchus. The epithelium which remains
after the superficial cells are lost consists of cells
which become flatter from base to surface, but the intercellular
bridges characteristic of the epithelium of the skin
are not found. When epithelium is in process of regeneration,
a layer gradually diminishing in thickness extends
over the denuded surface, the advancing edge being formed
by very flat cells in a single layer. The epithelium growing
into fissures which have penetrated the bronchial wall
may completely cover the exposed alveolar tissue. The
newly formed epithelium may follow a fissure into an alveolus
which has been opened and come into contact with the
fibrin which fills the alveolus.
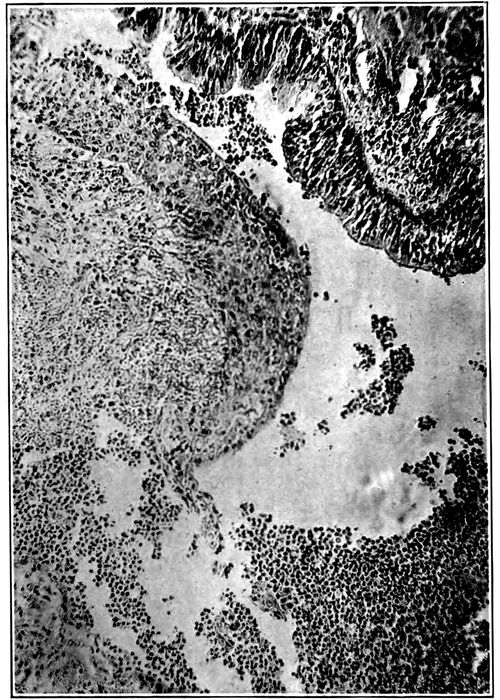
Fig. 23.—Squamous epithelium growing over the defect in the bronchial wall shown in Fig. 22 more highly magnified; squamous epithelium is present above and columnar epithelium below.
254Bronchiectasis usually affects the small bronchi with no
cartilage. It is not uncommon to find greatly dilated bronchi
with no cartilage in close proximity to cartilage containing
bronchi of smaller caliber. In one instance (Autopsy
421) a bronchus of medium size with cartilage measured
3 mm. in diameter, whereas two bronchi with no cartilage
were dilated to 4 and 6 mm., respectively. Nevertheless,
larger bronchi are occasionally the site of superficial
loss of epithelium, necrosis extending into the bronchial
wall, formation of fissures and stretching of the wall at the
spot which is weakened. In association with these changes
atrophy of the cartilage may occur (Autopsies 421, 425,
440, 463). Plates of cartilage in process of atrophy are
readily recognized by their irregularly indented outline
and often by their small size. The fibrous tissue surrounding
the cartilage is the site of chronic inflammation and is
densely infiltrated with lymphoid and plasma cells among
which polynuclear leucocytes are scant. Nevertheless,
polynuclear leucocytes are abundant in immediate contact
with the cartilage and appear to have an important part in
the solution of its matrix, for about them occur indentations
of the edge. Leucocytes penetrate into the cartilage.
The necrosis and tears which occur in the wall of the
bronchus are not always limited to the bronchus, but may
extend deeply into the surrounding tissue. In Autopsies
312 (Fig. 21) and 423 wide areas of necrosis have penetrated
deeply into the tissue about the bronchi.
Autopsy 312.—Illness began with influenza on September 26, seventeen
days before death; a diagnosis of lobar pneumonia with consolidation of
255the right lower lobe was made ten days after onset and Pneumococcus IV,
B. influenzæ and S. hemolyticus were found in the sputum. At autopsy
there was bronchopneumonia with red and gray lobular and confluent
lobular patches of consolidation and right and left serofibrinous pleurisy;
there was purulent bronchitis; no abscesses were seen. Small bronchi
throughout both lungs were dilated and often surrounded by a zone of hemorrhage.
Hemolytic streptococci were found in the heart’s blood, in the pleural
exudate, consolidated lung and bronchus; B. influenzæ was found in the
lung and in a small bronchus, and staphylococci in the contents of a small
bronchus.
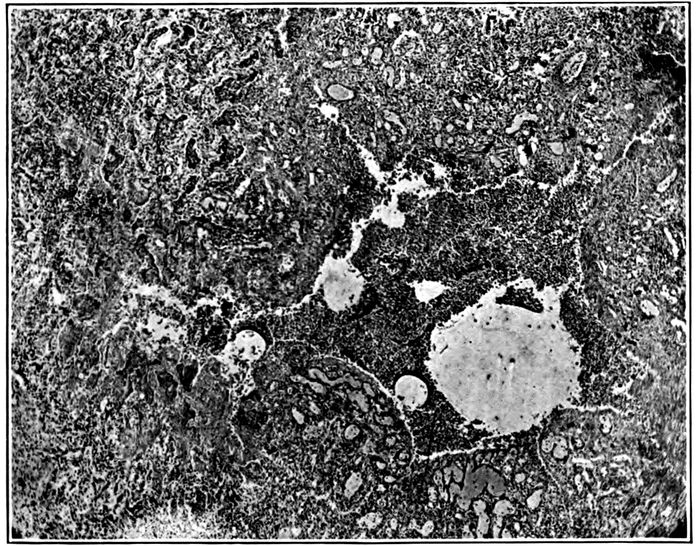
Fig. 24.—Acute bronchiectasis with fissures extending through bronchial wall which is marked by great engorgement of blood vessels; at one point a fissure has penetrated deep into the alveolar tissue and formed a small cavity containing purulent exudate and surrounded by fibrinous pneumonia. Autopsy 312.
Bronchi which are the site of acute inflammation have lost their epithelium
wholly or in part, and deep fissures penetrate the entire thickness
of the bronchial wall, extending into the surrounding lung tissue which is
the site of fibrinous pneumonia. In some instances plugs of fibrin within
the alveoli are bisected by these tears. There is some superficial necrosis
along the edge of each fissure, in several places extending outward from
defects in the walls of small bronchi dilated to approximately 1.5 mm.
There are wide patches of necrosis affecting both alveolar walls and contents
256of alveoli and extending 2 mm. into the lung tissue. When a fissure
has penetrated from the lumen of the bronchus into necrotic tissue
(Fig. 21), polynuclear leucocytes have accumulated within the necrotic
tissue, disintegration of tissue occurs, and a small cavity communicating
with the bronchus is formed.
Autopsy 423.—C. H., white, aged twenty-five, resident of Oklahoma,
had been in military service one month. Death occurred sixteen days after
onset of influenza.
Anatomical Diagnosis.—Chronic bronchopneumonia with peribronchiolar
consolidation throughout right lung and in left lower lobe; right purulent
pleurisy; purulent bronchitis; bronchiectasis at base of left lung.
The right lung weighs 1,260 grams; in the upper lobe are yellowish
gray nodules having the appearance of tubercles clustered about small
bronchi; in places similar nodules occur upon a background of pinkish
gray consolidation occupying the greater part of the lower lobe. Bronchi
contain purulent fluid. The left lung weighs 760 grams; it is edematous
and small, yellowish gray nodules of consolidation in the lower lobe
are clustered about terminal bronchi. Bronchi at the base of the lower
lobe are dilated.
Bacteriologic examination shows the presence of hemolytic streptococci
in the blood of the heart; hemolytic streptococci and B. influenzæ in the
lung.
Microscopic examination shows that the walls of the bronchi are infiltrated
with lymphoid and plasma cells; these cells are very numerous
in peribronchiolar patches of consolidation. A small bronchus 1 mm. in
diameter has squamous epithelium along one side; on the opposite side, the
wall is completely absent and there is superficial necrosis of exposed alveoli
filled with fibrin. A deep fissure passes from the bronchus into the
consolidated tissue; its edges are necrotic and it is filled with polynuclear
leucocytes. A small cavity in contact with the bronchus has been formed.
In another part of the lung a distended bronchus has lost its epithelium
on one side, and here alveoli filled with fibrin form the wall of the bronchus
which is filled with leucocytes. Extending outward from the eroded wall
is a focus of necrosis where both alveolar walls and contained exudate
have lost their nuclei.
The necrosis which has had its origin in the bronchi is
soon followed by accumulation of polynuclear leucocytes,
softening and disintegration of tissue. Discharge of the
disintegrated tissue through the bronchi results in the formation
of a small cavity continuous with the bronchus.
These changes are well illustrated by the bronchiogenic
abscesses which have been described elsewhere (Autopsies
376, p. 206, and 387, p. 206). When disintegrated tissue
257is discharged by way of the bronchi no accumulation of pus
occurs, but cavities will be formed, in part by dilation of
bronchi, in part by erosion of the adjacent lung tissue. Histologic
examination shows that these changes have produced
the advanced bronchiectasis found in Autopsy 445
(Fig. 25).
Autopsy 445.—W. F., white, aged twenty-three, from Mississippi, had been
in military service one month. His illness began September 22, twenty-seven
days before death, with severe coryza, weakness, nausea and vomiting;
great pain in bones, cough and sore throat. He was admitted to the
base hospital one week later with diagnosis of influenza and bronchitis.
On October 3, sixteen days before death, signs of consolidation were found
on the left side over the back and a diagnosis of lobar pneumonia was
made. On October 18 there was severe headache, pupils were dilated, and
there was rigidity of neck; lumbar puncture was made and pneumococci
were found in the fluid obtained. Death occurred on the following day.
Anatomic Diagnosis.—Bronchiectasis with unresolved pneumonia limited
to the left lower lobe; acute bronchopneumonia with peribronchiolar consolidation
in right lung; purulent bronchitis, peribronchial hemorrhage
and organizing bronchiolitis in right lung; adherent pleura on left side;
purulent meningitis.
The left upper lobe is crepitant throughout. The outer and posterior
two-thirds of the left lower lobe is riddled with cavities often rounded
and varying in diameter from 0.5 to 3 cm. but not infrequently irregular
in shape and in communication with adjacent cavities (Fig. 25). In places
cavities pass in a tortuous course from pleura to the midpart of lung.
The lining of these cavities is usually smooth, but in places is covered
by gray necrotic material. Communication between the cavities and medium-sized
bronchi is occasionally found. The lung tissue between the
cavities is in part grayish red and consolidated, in part pink and air containing.
The right lung is edematous throughout; the bronchi in the lower
part of the right lung contain purulent fluid and are in places surrounded
by zones of hemorrhage.
The spleen is very large (14 × 11 × 5 cm.) and firm.
The spinal fluid is cloudy and blood vessels over the lumbar enlargement
and lower thoracic region are congested; in the upper thoracic region the
cord is covered by purulent exudate.
Bacteriologic examination demonstrates the presence of hemolytic streptococci
in the blood of the heart; plates from the left lung contain a few
colonies of S. aureus and Pneumococcus IV; plates from the right main
bronchus contain S. aureus and a large bacillus which does not stain by
Gram’s method. Three plates from the spinal meninges contain Pneumococcus
IV.
258
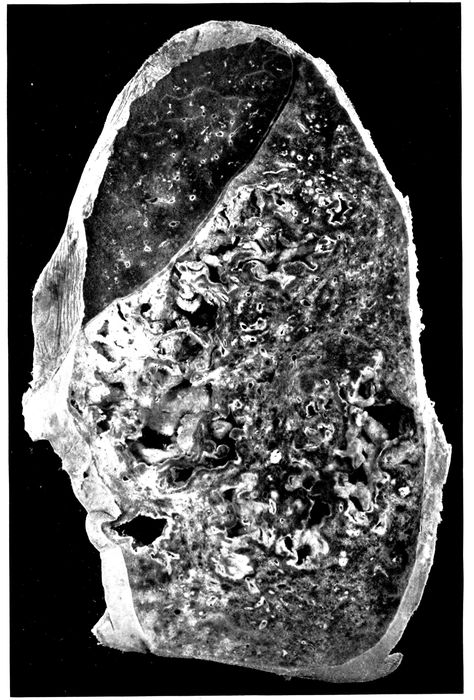
Fig. 25.—Advanced bronchiectasis throughout lower left lobe. Autopsy 445.
259Microscopic examination shows that the cavities which have been described
are lined by very vascular connective tissue containing many cells;
there is no epithelial lining and the surface is in places covered by fibrin.
On the surface polynuclear leucocytes are numerous, but immediately below,
large mononuclear cells occur and frequently contain one or several
ingested polynuclear leucocytes. None of the structures peculiar to the
bronchi can be identified in the wall of these cavities, and in many places
it is evident that lung tissue has undergone destruction, for in places the
lining of vascular connective tissue is interrupted and an extension of the
cavity penetrating into the lung substance is surrounded by alveoli filled with
fibrin; in contact with the cavity there is some necrosis.
The cavities communicate with the bronchi and are
lined in part by vascular connective tissue which may in
part represent preexisting bronchial walls, but no epithelium
is present and the relation to the bronchi cannot be established
with certainty. These cavities have extended by
necrosis which has broken the vascular connective tissue of
their wall and penetrated into adjacent lung tissue. Death
has been the result of purulent meningitis caused by pneumococcus,
and the histologic changes in the walls of the
cavities suggest that the activity of the inflammatory reaction
here is subsiding, for large mononuclear cells are numerous
and are ingesting polynuclear leucocytes. The
changes described would, if continued, result in the formation
of cavities lined by fibrous tissue and resembling many
of those formed as the result of dilatation of the bronchi.
A study of the progress of the changes which result in
the formation of bronchiectatic cavities has shown how the
inflammatory irritant within the bronchus destroys the epithelium
of the bronchus, penetrates into the deeper tissues
and produces fissures which extend through the entire
thickness of the bronchial wall at one or usually several
places. These longitudinal fissures, which at first often
give a stellate outline in cross section to the cavity of the
affected bronchus, permit the separation of the edges of the
fissure, so that an increase in the circumference occurs.
The base of the fissure is formed by surrounding alveolar
tissue and its edges are the site of necrosis. Tears may
extend into the surrounding alveolar tissue, thus permitting
further stretching of the bronchial wall. The consequences
260of rupture of the small bronchi into the adjacent
alveoli are to some extent overcome by the inflammatory
reaction which plugs the adjacent alveoli with fibrin.
Compression of the lungs by forced expiration, even
though the glottis were closed as in coughing, would not
dilate the bronchi, because pressure outside and within the
bronchi would be equally elevated (Thornton and Pratt[89]).
The pressure within the bronchi does not differ greatly
from atmospheric pressure, whereas the negative pressure
within the pleural cavity may vary from approximately
6 mm. of mercury during quiet inspiration to 30 mm. with
forced inspiration. Excess of pressure upon the inner surface
of the bronchial walls will vary with coughing and
other respiratory efforts, between these limits depending
upon the readiness with which pressure is equalized within
and without the bronchi by penetration of air into the alveoli.
The presence of viscid mucopurulent fluid within bronchioles
will obstruct these tubules and retard the entrance
of air into alveoli.
Weakening of the bronchial wall by the changes which
have been described will cause lasting dilatation of the
bronchi. Whatever increases pressure within the bronchi
will increase the tendency to dilatation; the bronchi being
filled with mucopurulent exudate dilatation usually appears
first at the bases of the lung, since gravity increases
intrabronchial pressure here. New formation of fibrous
tissue within the wall of the bronchus, thickening of adjacent
alveolar walls, and organization of fibrin reinforce the
weakened bronchial wall and limit the dilatation which follows
injury to the wall. Regeneration of epithelium covering
the dilated tube will further obscure the early
changes which have made dilatation possible. The changes
which weaken the bronchial wall permit dilatation at a
time when there is no new formation of fibrous tissue.
When the bronchial lesion has persisted several weeks,
261chronic pneumonia is associated with it. It has been suggested
that the contraction of newly formed fibrous tissue
within the substance of the lung might cause bronchi to be
enlarged by traction upon their walls. Newly formed connective
tissue is most abundant in the wall of the bronchiectatic
cavity, and here contraction would tend to diminish
the size of the cavity.
Unresolved Bronchopneumonia
Chronic bronchopneumonia is characterized by changes
similar to those associated with chronic inflammation in
other parts of the body, namely, by thickening of the interstitial
tissue of the lung, by accumulation of mononuclear
cells, by proliferation of fibrous tissue and by organization
of exuded fibrin. In a few instances these changes have begun
at the end of two weeks after onset of influenza, but
they have been little advanced until three weeks has
elapsed; advanced chronic inflammation has occurred after
from four to eight weeks. Chronic inflammation primarily
affects those structures which are most severely injured by
the acute lesion and is most conspicuous in immediate proximity
to the small bronchi and bronchioles; the perivascular
and interlobular connective tissue are secondarily
involved. Corresponding to each of the lesions of the alveolar
tissue which have been found with bronchopneumonia,
namely, peribronchiolar, hemorrhagic peribronchiolar, lobular
and peribronchial consolidation, there is a chronic lesion
which develops when pneumonia has failed to resolve.
The term interstitial bronchopneumonia has been used
by MacCallum to designate a lesion which he has found in
association with measles at Fort Sam Houston. This name
he states does not describe accurately the early stage of the
lesion, for its interstitial character is not evident at first. In
his monograph on “Epidemic Pneumonia in the Army
Camp,” published in 1919, MacCallum describes and pictures
262instances of the lesion which we have designated interstitial
suppurative pneumonia and classifies them as interstitial
bronchopneumonia. We have shown that this lesion,
which is the result of infection of the lymphatics with
S. hemolyticus, bears no necessary relation to the lesion
which is characterized in its early stage by peribronchiolar
pneumonia and in its later stages by chronic inflammation
with mononuclear infiltration and proliferation of the peribronchial,
perivascular and interalveolar tissue. At Fort
Sam Houston, nearly every patient with measles was infected
with hemolytic streptococci; we observed, following
influenza, similar prevalence of hemolytic streptococci in
certain wards in the base hospital at Camp Pike. Among the
cases at Fort Sam Houston there were doubtless instances
both of interstitial suppurative pneumonia caused by hemolytic
streptococcus and of chronic bronchopneumonia not
referable to this microorganism.
Studying pneumonia following influenza at Camp Lee,
Va., and later at Camp Dix, N. J., during the fall of 1918,
MacCallum reached the conclusion that “interstitial bronchopneumonia”
following influenza was caused by B. influenzæ
of Pfeiffer. This lesion attributed to B. influenzæ
differed from that previously referred to hemolytic streptococcus
in the following characters: the lymphatic channels
in the bronchial walls and widened interlobular septa
are inconspicuous and none are found distended with exudate;
there is no intense infection of the pleura, and polynuclear
leucocytes are inconspicuous in the alveolar exudate
and in the walls of the bronchi. It seems probable
these differences are explained by the absence of hemolytic
streptococci which tend to invade lymphatics and produce
severe inflammatory changes in the pleura.
Chronic Bronchitis.—The earliest changes in the bronchial
wall with bronchitis of influenza are hyperemia, leucocytic
infiltration and hemorrhage, and they may occur
even though the lining epithelium remains intact. Epithelium
263frequently undergoes partial or complete destruction,
and with this severe injury the influence of the inflammatory
irritant may extend directly through the wall of the
bronchus, for in some instances there is hemorrhage into
all the alveoli in a zone encircling the bronchus. Since these
alveoli have only indirect communication with the affected
bronchus through alveolar tissue not involved in the inflammatory
process, it is evident that the surrounding
hemorrhage is secondary to the lesion of the bronchus.
Fibrinous inflammation in other instances, similarly localized
in a zone of alveoli encircling a bronchus, is doubtless
the result of direct extension of the inflammatory process
through the bronchial wall. After the disease has existed
during two or three weeks inflammation is still active immediately
below the inner surface of the bronchus; here
polynuclear leucocytes are numerous whereas in the deeper
parts of the mucosa and about the muscularis leucocytes are
scant but lymphoid and plasma cells are very numerous.
The severity of the inflammatory reaction may be judged
by the abundance and extent of this cellular reaction and is
in close relation to the intensity of the changes affecting
the mucous membrane of the bronchus. Infiltration of the
entire bronchial wall with lymphoid and plasma cells is
almost invariable when the primary injury to the bronchus
has destroyed the epithelial lining, and this infiltration is
not limited to the bronchial wall but extends outward into
the contiguous alveolar septa which are thickened by it.
The sheath of the pulmonary artery which accompanies the
bronchus exhibits a similar change, and the alveolar septa,
as a fringe about it, are thickened and infiltrated with mononuclear
cells. Interlobular septa continuous with the bronchus
often show some infiltration.
A later phase in this series of changes is represented by
new formation of fibrous tissue. The bronchial walls and
interalveolar septa are thickened by proliferating fibrous
tissue, young fibroblasts and newly formed collagen fibrils
264being abundant (Fig. 28; also Fig. 30). This increase of
fibrous tissue is especially noteworthy immediately surrounding
the walls of the small bronchi, which are often
considerably dilated, and about the smaller of those bronchi
which have cartilage; with thickening of alveolar walls
immediately adjacent to the bronchus every stage in the
obliteration of the alveoli may be found. Their walls are
thickened and their lumina are diminished in size and often
flattened in a direction concentric with the bronchus. Such
atrophied alveoli lined by cubical epithelial cells occurring
within the thickened peribronchial fibrous tissue give evidence
that this tissue has replaced alveoli. Alveoli surrounding
and within the new fibrous tissue are frequently
filled with fibrin, and organization indicated by
penetration of fibroblasts and capillaries into the fibrin
may be far advanced. There is some increase of perivascular
and interlobular tissue. The bronchiectasis which is
almost invariably found with unresolved bronchopneumonia
has been described. Squamous transformation of epithelium
(page 251) is frequently found in association with
the chronic bronchitis of unresolved pneumonia.
Organizing Bronchitis and Bronchiolitis.—When the
bronchial epithelium is destroyed, fibrin is deposited upon
the denuded surface and may partly or completely fill the
lumen of the bronchial tube. The plug of fibrin is adherent
to the underlying tissue wherever epithelium is lost but is
separated from the bronchial wall by a well-defined space
where epithelial lining is still intact. Fibroblasts promptly
migrate from the wall of the bronchiole into this fibrin, and
fibroblasts, fixed during ameboid movement, are irregularly
elongated in a direction toward the fibrin.
Organization of fibrin occurs within the smallest bronchi
(diameter 0.3 to 0.5 mm.) or within respiratory bronchioles.
It has been found in 8 autopsies. In one instance it has
been present eleven days after the onset of influenza, but
usually it is seen three or four weeks after onset of symptoms
265of respiratory disease. In the early stages of the
lesion a plug of fibrin within the lumen of the bronchus or
bronchiole is invaded by fibroblasts, plasma cells and newly
formed capillaries. These capillaries have their origin in
the wall of the tube and enter the fibrin at points where
in consequence of loss of epithelium fibrin is continuous
with the connective tissue. When the bronchiole is cut
longitudinally, partially or completely organized fibrin may
be found adherent at several places with intact epithelium,
sometimes beautifully ciliated, between the sites of attachment.
The fibrin is finally replaced completely and the
lumen of the bronchiole contains a mass of organized
fibrous tissue in which young fibroblasts and plasma cells
are numerous.
The lesion has been associated with chronic bronchopneumonia
in 6 of 8 instances. In Autopsy 445, p. 257, organizing
bronchitis and bronchiolitis occurred in the right lung
unassociated with other chronic lesion, although there was
advanced bronchiectasis with fibrous induration in the
left lung. In Autopsy 499 (p. 224) organizing bronchiolitis
occurred in association with chronic changes which appear
to have followed interstitial suppurative pneumonia caused
by S. hemolyticus. Other severe lesions of the bronchi
have accompanied organizing bronchitis and bronchiolitis.
Purulent bronchitis has been present in 7 of 8 instances;
bronchiectasis in 5 of 8 instances.
The bacteriology of autopsies with organizing bronchitis
and bronchiolitis is shown in Table LIII.
The bacteriology of these cases presents no constant
feature. Invasion of the blood by S. hemolyticus has been
present in a large proportion of cultures, namely, in 5 of 7
(71.4 per cent). In one of the 2 instances in which hemolytic
streptococci have been found, neither in the blood nor
lungs, Pneumococcus III has been found in the blood and S.
viridans in the lungs and bronchus; in the other, S. aureus
has been found in the lung and bronchus. Staphylococci
have been found frequently in the bronchi (60 per cent)
and in the lungs (50 per cent). B. influenzæ has been present
in the bronchi in the usual proportion of instances
(80 per cent). The lesion has occurred in the presence of
B. influenzæ combined with streptococci or staphylococci.
| 266 |
| Table LIII |
|---|
| |
| AUTOPSY |
DURATION OF ILLNESS |
BLOOD |
LUNGS |
BRONCHUS |
| 420 |
11 days |
S. hem. |
S. hem., B. inf., S. aur. |
|
| 402 |
14 days |
Pneum. IV, S.hem. |
|
|
| 370 |
17 days |
|
S. aur. |
S. aur., Pneum. IV, B. inf. |
| 457 |
17+ days |
|
|
Pneum. IV, B. inf. |
| 421 |
19 days |
S. hem. |
Pneum. IV, S. hem. |
|
| 445 |
27 days |
S. hem. |
Pneum. IV, S. aur. |
S. aur. |
| 473 |
28+ days |
Pneum. III |
S. vir. |
B. inf., S. vir., staph., M. catarr. |
| 499 |
36 days |
S. hem. |
|
S. hem. B. inf. |
Thrombosis of lymphatics in the wall of bronchi adjacent
to blood vessels and in interlobular septa occurs, and occasionally
organization of the fibrinous plug within the lymphatic
is in progress (Autopsies 283, 425 and 463). Fibroblasts
and capillaries penetrate from the wall of the lymphatic
into a mass of hyaline fibrin which fills the lumen.
Unresolved Bronchopneumonia.—The most common type
of pneumonic lesion following influenza is characterized by
acute inflammation of the alveoli immediately adjacent to
the bronchioles and the lesion is associated in many instances
with hemorrhage or edema. If this lesion persists
unresolved during several weeks, evidences of chronic inflammation
are found. Peribronchial, perivascular and interlobular
connective tissue is thickened and richly infiltrated
with lymphoid and plasma cells, large mononuclear
cells and many young fibroblasts. Interalveolar septa adjacent
to the walls of bronchi and between alveoli surrounding
inflamed bronchioles are implicated in the process.
267Interstitial changes characterize the lesion only in its late
stage. It appears undesirable to give the name “interstitial
pneumonia” to the early stage of a lesion which begins and
in most instances terminates as an acute relatively superficial
inflammation of the bronchi, bronchioles and peribronchiolar
alveoli.
Chronic bronchopneumonia is often overlooked at autopsy
because newly formed connective tissue is not present
in sufficient quantity to attract attention (Fig. 26). When
the lesion is advanced conspicuous gray white patches of
fibrous tissue may be seen about the bronchi (Autopsy 487;
Fig. 27) and interlobular septa may be obviously thickened
(Autopsy 472). The most distinctive feature of the lungs
is the presence of small, firm, gray or yellowish gray nodules
of consolidation which resemble miliary tubercles.
They represent the peribronchiolar patches of bronchopneumonia
present during the acute stage and have
assumed the well-defined outline and firm consistence of
tubercles because polynuclear leucocytes and red blood corpuscles
have in large part disappeared, interstitial tissue
is increased, and exudate is in process of organization.
These nodules are grouped in clusters about the small
bronchi.
With unresolved bronchopneumonia the lungs are very
voluminous and fail to collapse after they are removed from
the chest and in some instances even after incision. The
air containing tissue is usually dry. In our autopsies the
lungs have been pink in color and often free from coal pigment,
because those suffering with pneumonia have been in
considerable part men from rural districts. Thick mucopurulent
material exudes from the small bronchi which
have been cut across; purulent bronchitis has been present
in 20 of 21 instances of chronic bronchopneumonia. Bronchiectasis
has been present in 13 instances; dilatation is
often advanced, so that throughout the lungs are found
bronchi with no cartilage distended to a diameter of 0.5 cm.
In addition to the firm peribronchiolar tubercle-like nodules
of consolidation there are scattered patches of gray
lobular or confluent lobular consolidation. Yellowish nodules,
grouped about bronchi and resembling those found
elsewhere in air containing tissue, are occasionally seen
scattered upon the cut surface of a patch of gray, confluent
lobular consolidation (Autopsies 421, 423, 431).
268
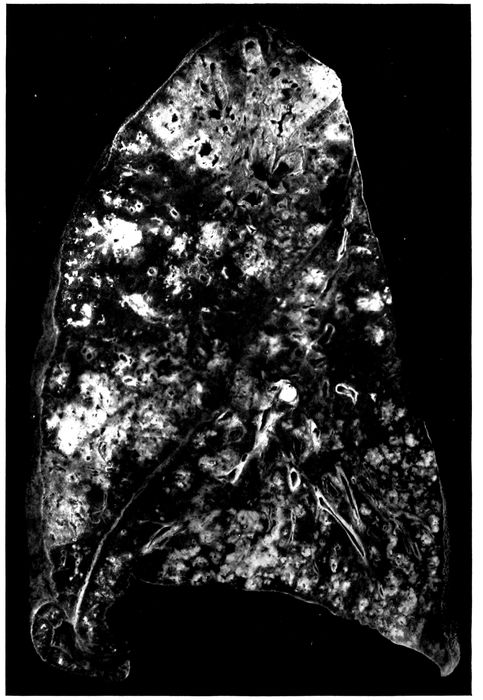
Fig. 26.—Unresolved bronchopneumonia with tubercle-like nodules of peribronchiolar consolidation best seen in lower lobe; bronchiectasis. Autopsy 425.
269Microscopic examination demonstrates the presence of
those changes which have been described in association
with chronic bronchitis and bronchiectasis. There is abundant
new formation of fibrous tissue about the bronchi of
small and medium size, thickening of adjacent interalveolar
walls and incorporation of alveoli into the thickened bronchial
wall (Figs. 27, 28, 30, and 31). In half of the instances
of chronic bronchopneumonia there has been peribronchial
fibrinous pneumonia, and organization of fibrin
within the alveoli is usually well advanced. In one instance
(Autopsy 487; Figs. 27 and 28) after an illness of fifty-five
days this process has resulted in the formation of conspicuous
patches of firm, grayish white fibrous tissue surrounding
dilated bronchi. Organization of fibrinous exudate
within the lung has not been limited to the alveoli but has
occurred in the bronchioles as well. Organizing bronchiolitis
has been present in 5 instances (Autopsies 370, 402,
457 and 473).
Increase of fibrous tissue occurs about the blood vessels
and in the septa between the lobules, which are infiltrated
with mononuclear wandering cells and fibroblasts. Dilatation
and thrombosis of the lymphatic vessels have occurred
in both situations, and in 3 instances (Autopsies
283, 425 and 463) organization of these fibrinous thrombi
has occurred.
270

Fig. 27.—Unresolved pneumonia with peribronchial formation of fibrous tissue; bronchiectasis. Autopsy 487.
271
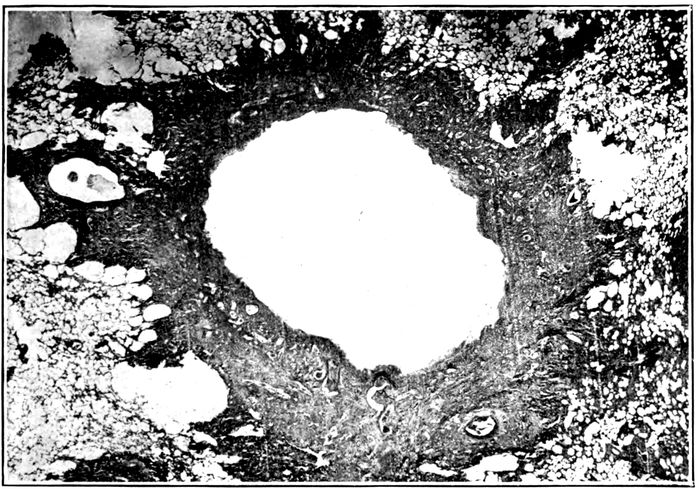
Fig. 28.—Unresolved pneumonia with bronchiectasis showing new formation of fibrous tissue about a greatly dilated bronchus of which the epithelial lining has been lost. Autopsy 487.
Thickening, cellular infiltration and fibrosis of the bronchial
walls with interstitial inflammation and fibrosis of immediately
adjacent alveolar septa are found about the
ramifications of the bronchial tree and may be followed
to the smallest bronchi. When the respiratory bronchioles
are reached it will be found that the alveoli which stud their
walls are implicated in the change. The fibrin which they
contain is infiltrated with lymphoid and plasma cells, and
with progress of the lesion is invaded by fibroblasts and
capillaries. Infiltration and fibroid thickening extends
from the bronchiolar wall to the alveolar septa continuous
with it (Fig. 31 with measles). Similar changes occur about
the alveolar ducts, and about the orifices of the tributary
infundibula (Fig. 32), peribronchiolar foci of acute inflammation
having assumed the characters of a chronic inflammatory
process. Fibrin within the alveoli contains round
cells and fibroblasts. With thickening of alveolar walls the
alveolar lumina may be much diminished in size and often
persist as spaces lined by cubical cells. Polynuclear leucocytes
are usually numerous within the alveolar duct and
272in a few alveoli immediately adjacent to it, but elsewhere
throughout the focus of inflammation round cells are predominant.
The changes which have been described correspond
with the transformation of ill-defined, gray or reddish
gray spots of consolidation grouped about the terminal
bronchi into firm sharply defined grayish white nodules
having the consistence and appearance of miliary tubercles.
One of the most constant characters of pneumonia following
influenza is its hemorrhagic character. In the
earlier stages of pneumonia phagocytosis of red blood corpuscles
by large mononuclear cells is frequently seen. In
association with the chronic changes which have been described,
large mononuclear cells filled with brown pigment,
doubtless formed from red corpuscles, are often found
within the alveoli. These pigment containing cells are similar
to those commonly associated with chronic passive congestion
of the lungs.
In one instance (Autopsy 457) hemorrhagic peribronchiolar
pneumonia has been found in process of organization.
The bronchioles and alveoli adjacent to them contain
polynuclear leucocytes, but intervening alveoli almost uniformly
contain blood and are the site of new formation of
connective tissue. Interalveolar septa are thickened and
alveoli which are lined by cubical epithelium are often diminished
in size. In many places fibroblasts have penetrated
in considerable number into the blood within the alveoli
and occasionally newly formed capillaries are found
within them.
Lobular patches of pneumonia are often found in process
of organization (Autopsies 370, 421, 423, 433, 463, 472 and
473). Microscopic examination shows that whole lobules
well defined by thickened septa are the site of chronic interalveolar
inflammation and intraalveolar organization of
exudate, whereas adjacent lobules are air containing and
relatively normal. In the earlier stages of the process
fibrin present within the alveoli is invaded by fibroblasts,
273mononuclear wandering cells and blood vessels but in the
later stages fibrin has disappeared; the lumina of the alveoli
are occupied by cellular fibrous tissue and in places the
thickened alveolar walls and intraalveolar fibrous tissue
have been fused to form wide patches of new tissue.
With chronic bronchopneumonia confluent lobular consolidation
occasionally has a gray ground upon which are
scattered small yellow spots clustered about the small
bronchi (Autopsies 421, 423 and 431). Microscopic examination
has shown that the yellowish spots correspond to
dilated bronchioles filled with purulent exudate and surrounded
with alveoli containing many polynuclear leucocytes.
In the interstitial tissue about the bronchiole and
between adjacent alveoli plasma cells are often present in
great number. Between these spots of subacute bronchiolar
inflammation lung tissue is the site of interalveolar proliferation
of fibrous tissue and intraalveolar organization of
exudate.
In all instances of chronic bronchopneumonia there has
been peribronchial pneumonia in a zone encircling small
bronchi with no cartilage and the smallest of the bronchi
which have cartilage in their wall; thickening of interalveolar
septa, organization of peribronchial fibrinous pneumonia
and partial disappearance of alveoli have been described.
In the following autopsy peribronchial fibroid
pneumonia has been so advanced that conspicuous patches
of gray white tissue surrounding bronchi have replaced in
some parts of the lung a considerable part of the lung substance.
Autopsy 487.—W. C., white, aged twenty-seven years, a farmer from
Mississippi had been in military service twenty-one days. Illness began
on September 17, fifty-five days before death, with chill, fever, cough, backache,
pain in the chest and coryza. The patient was admitted two weeks
after onset with the diagnosis of influenza. Eight days later his sputum
was blood tinged and there were signs of bronchopneumonia. One month
after admission the patient developed a rash and a diagnosis of scarlet
fever was made.
274Anatomic Diagnosis.—Chronic bronchopneumonia with peribronchial
fibroid induration; bronchiectasis; purulent bronchitis; abscesses at the
bases of both lungs; seropurulent pleurisy on the left side.
The body is much emaciated. The left pleural cavity contains 650
c.c. of opaque, dull yellow, thin, purulent fluid. The surface of the left
lung is covered in spots by white partially organized fibrin.
On section of the right lung (Fig. 27) the tissue is found in great part
air containing but there are numerous firm, gray patches, irregular in shape
and from 1 to 2 cm. across. In these spots the tissue is tough and resembles
fibrous tissue; within them are much dilated bronchi. In the central part
of the upper lobe is a group of cavities with smooth wall, the largest of
these cavities being 12 mm. in diameter; immediately adjacent are dilated
bronchi. Between and surrounding these cavities is gray tissue, like
that described above. Below the outer surface of the upper lobe is an
extensive area 7 cm. from above downward, thickly studded with bronchiectatic
cavities, in the walls of which there is tough fibrous tissue.
In the middle lobe are several dilated bronchi, the largest of which is 7 mm.
in diameter, and elsewhere occur dilated bronchi with thickened walls. At
the base of the lung below the pleura are two abscesses, which are yellow in
the center and surrounded by hemorrhagic tissue. At the posterior part of
the lower lobe there are numerous firm, nodular, yellowish spots grouped in
clusters upon a background of red, air containing tissue. The bronchi
throughout the lung contain mucopurulent fluid.
In the left lung patches of fibrous tissue are more numerous than on the
right side and are irregular in shape, from 1 to 2 cm. across and most abundant
in the center of the upper lobe. This fibrous tissue is in great part gray
but in places it has a yellowish tinge. The bronchi everywhere are moderately
dilated. At the base of the lung below the pleura is an abscess.
The other organs show no noteworthy change.
Bacteriologic Examination.—The fluid in the left pleura and right main
bronchus contain S. hemolyticus. B. influenzæ is found in the right lung and
right main bronchus.
Microscopic examination shows that the patches of dense fibrous tissue
seen at autopsy almost invariably surround dilated bronchi with no cartilage
in their walls (Fig. 28) and with a diameter of from 1 to 2 or more millimeters.
These bronchi have lost their epithelial lining; they contain polynuclear
leucocytes, and their wall in contact with the lumen is infiltrated to
a varying distance with the same cells. Their inner surface is very irregular,
and superficial necrosis occurs. The limits of the preexisting bronchial wall
is no longer recognizable in the dense surrounding fibrous tissue richly infiltrated
with lymphoid and plasma cells. In contact with the bronchus, often
in a wide zone, all traces of alveoli have been destroyed, but further outward
alveoli are represented by spaces lined by cubical epithelium. At the periphery
of the zone of fibroid induration alveolar walls are much thickened
and richly infiltrated with mononuclear wandering cells; the lumina of the
alveoli contain plugs of organized fibrous tissue often covered by flat or cubical
epithelium. In the surrounding tissue a few small bronchi are lined by columnar
275epithelium; there is scant new formation of fibrous tissue but the
alveolar walls are thickened and infiltrated with cells. Epithelium of the
larger bronchi with cartilage in their walls is usually intact and there is about
them little peribronchial inflammation.
Advanced induration about the bronchioles represents a
late stage of chronic peribronchiolar pneumonia. A bronchiole
cut transversely is found in the center of a focus of
induration situated within relatively normal air containing
lung tissue. Next the bronchiole which in some instances
has wholly or partly lost its epithelium there is very cellular
fibrous tissue; further from the bronchiole alveoli are
much diminished in size, lined by flat or cubical epithelium
and separated by thick cellular walls. Plugs of cellular
fibrous tissue sometimes fill the alveolar duct. In favorable
sections, cut in a plane which shows the alveolar duct opening
out into infundibula, it is found that newly formed fibrous
tissue surrounds the alveolar duct and extends into
the walls of its tributary alveoli; alveoli may be obliterated
by this fibrous tissue. Induration of alveolar walls is evident
along the proximal part of the infundibula which are
readily demonstrable because they are much dilated. (See
Fig. 32.) The distal parts of the infundibula are surrounded
by alveoli with delicate walls.
One bronchus retains along one side part of its epithelium
which has assumed a squamous form. In other places
the wall has undergone necrosis which at one spot extends
deeply into the surrounding tissue. Necrotic tissue in another
part of the circumference is infiltrated with polynuclear
leucocytes and separated from the surrounding tissue
by a space filled with leucocytes. An abscess communicating
with the bronchus is thus formed.
The foregoing instance is an example of the chronic fibroid
pneumonias with bronchiectasis which occur as sequelæ
of the epidemic of influenza. It is not improbable
that a considerable number of those who suffer with chronic
bronchitis and bronchiectasis following influenza have less
extensive lesions similar to those which have been described.
276Bacteriology of Unresolved Bronchopneumonia.—Bacteria
found in the bronchi in 10 instances of chronic bronchopneumonia
have been as follows:
| Bacteria in Bronchi with Chronic Bronchopneumonia |
|---|
| |
| B. coli |
1 |
| B. influenzæ and pneumococcus |
1 |
| B. influenzæ and S. hemolyticus |
2 |
| B. influenzæ and staphylococcus |
1 |
| S. hemolyticus and B. coli |
1 |
| B. influenzæ, pneumococcus and staphylococcus |
3 |
| B. influenzæ, S. viridans and M. catarrhalis |
1 |
Bacteria found in the lungs in 17 instances of chronic
bronchopneumonia were as follows:
| Bacteria in Lungs with Chronic Bronchopneumonia |
|---|
| |
| B. influenzæ |
1 |
| Staphylococcus |
1 |
| S. viridans |
1 |
| B. influenzæ and pneumococcus |
1 |
| B. influenzæ and S. hemolyticus |
3 |
| B. influenzæ and staphylococcus |
3 |
| Pneumococcus and S. hemolyticus |
1 |
| S. hemolyticus and B. coli |
2 |
| B. influenzæ, S. hemolyticus and staphylococcus |
3 |
| No organism found |
1 |
A noteworthy feature of these lists is the multiplicity of
microorganism found, namely, B. influenzæ, S. hemolyticus,
pneumococcus, staphylococcus, S. viridans, B. coli, and M.
catarrhalis. More than one microorganism is usually
found in both bronchus and lung. In the one instance
(Autopsy 472) in which B. coli alone has been found in the
bronchus, B. coli and S. hemolyticus have been found in the
lung and hemolytic streptococcus in the blood; it is evident
that B. coli alone has not been responsible for the lesion.
In one instance (Autopsy 487) B. influenzæ alone has been
found in the lung but hemolytic streptococci have been
found in the bronchus, pleura and blood of heart; with
S. aureus alone in the lung (Autopsy 370), S. aureus, Pneumococcus
IV and B. influenzæ have been found in the bronchus.
With S. viridans alone in the lung (Autopsy 473),
277Pneumococcus III has been found in the pleura and in the
blood of the heart and has doubtless had an important part
in the production of pneumonia; S. viridans, M. catarrhalis
and B. influenzæ have been found in the bronchus in this instance.
No single microorganism is associated with the lesions
but combinations of B. influenzæ with hemolytic streptococci
or staphylococci are common (over 50 per cent). In
Autopsy 422 B. influenzæ and Pneumococcus atypical II
have been present in the lungs. Among 10 instances in
which cultures have been obtained from the bronchus B.
influenzæ is found 8 times, and in the 2 instances in which
it has not been identified B. coli has been present. B. influenzæ
has seldom been found (Table XXVII) in the presence
of B. coli, and it is not improbable that B. coli outgrows
and obscures the presence of B. influenzæ.
Table LIV shows the per cent incidence of pneumococci,
hemolytic streptococci, staphylococci and B. influenzæ
in the bronchus, lung and heart’s blood with chronic
bronchopneumonia and serves as an index of the readiness
with which each of these microorganisms passes from bronchus
to lung and from lung to the blood in this disease.
| Table LIV |
|---|
| |
|
PNEUMOCOCCUS
PER CENT POSITIVE |
HEMOLYTIC STREPTOCOCCUS
PER CENT POSITIVE |
STAPHYLOCOCCUS
PER CENT POSITIVE |
B. INFLUENZÆ
PER CENT POSITIVE |
| Bronchus |
40.0 |
30.0 |
50.0 |
80.0 |
| Lung |
12.5 |
56.2 |
37.5 |
68.7 |
| Blood |
16.6 |
55.6 |
0 |
0 |
Comparison of Table LIV with the analogous figures
for acute bronchopneumonia shows little noteworthy difference.
Pneumococci are less frequently found in the
lung (12.5 per cent) and in the blood (16.6 per cent) with
chronic bronchopneumonia than with acute bronchopneumonia
(lung 43.9 per cent; blood, 40.3 per cent). Hemolytic
streptococci and staphylococci are not more frequently
278found with unresolved than with acute bronchopneumonia
and failure to resolve cannot be referred to either or to both
microorganisms, for bronchopneumonia not infrequently remains
unresolved in their absence. B. influenzæ is present
in the bronchi in at least 80 per cent of instances and perhaps
in all; it is usually combined both in the lungs and in
the bronchi with one of the pyogenic cocci.
The severity of the injury to the walls of bronchi resulting
in continued infection with a variety of bacteria,
appears to be the factor determining failure of resolution
and the persistence of bronchopneumonia.
The Relation of Unresolved Bronchopneumonia to Interstitial
Suppurative Pneumonia Caused by Hemolytic Streptococci.—Hemolytic
streptococci have been present in a
considerable proportion of those who have had unresolved
bronchopneumonia and its occurrence in the bronchi, lung
and blood of the heart indicates that it has had an important
part in causing death. Unresolved bronchopneumonia,
following measles, designated by MacCallum “interstitial
bronchopneumonia” in a series of autopsies at Fort
Sam Houston in the spring of 1918, was constantly associated
with hemolytic streptococci. Among the lesions described
as interstitial bronchopneumonia was at least one
which was evidently what we have designated interstitial
suppurative pneumonia. Lymphangitis was not infrequently
found with “interstitial bronchopneumonia” following
measles. At Camp Lee and Camp Dix, following
the epidemic of influenza, MacCallum found “interstitial
bronchopneumonia” with no hemolytic streptococci and
noted that lymphatics in the interstitial septa were inconspicuous
and that none was found distended with exudate;
empyema was not present.
We have shown that interstitial suppurative pneumonia
is an acute lesion caused by hemolytic streptococci. Unresolved
bronchopneumonia is accompanied by chronic pneumonia
and has no necessary relation to this microorganism.
279In a foregoing section we have described instances of interstitial
suppurative pneumonia unaccompanied by chronic
changes, and in the present section we have described instances
of unresolved bronchopneumonia with no infection
by hemolytic streptococci. We have pointed out that the
incidence of streptococcus infection with unresolved bronchopneumonia
does not materially differ from that with
acute bronchopneumonia even though the greater duration
of the disease gives more opportunity for infection. In
some of the autopsies made by MacCallum at Fort Sam
Houston, lesions of streptococcus infection doubtless coexisted
with unresolved bronchopneumonia.
In the 3 autopsies described below, interstitial suppurative
pneumonia with empyema caused by hemolytic streptococcus
occurs in association with unresolved bronchopneumonia.
Autopsy 420.—J. E. S., white, aged thirty-two years, born in England
and resident of Los Angeles, Cal., had been in military service one month.
Onset of illness began on October 3, eleven days before his death. He was
admitted to the hospital on the following day with the diagnosis of influenza
and acute bronchitis. Pneumonia believed to be lobar was recognized eight
days after admission.
Anatomic Diagnosis.—Unresolved bronchopneumonia with hemorrhagic
peribronchiolar consolidation in right lung; interstitial suppurative pneumonia
with consolidation in left upper lobe; fibrinopurulent pleurisy; purulent bronchitis.
The left pleural cavity contains 200 c.c. of turbid yellow fluid in which
are flakes of fibrin. In the inner and upper part of the left upper lobe there
is an area of consolidation where the tissue has a cloudy, pinkish gray color
and is finely granular on section. Here the interstitial septa are distended by
edema, so that they are in places 0.5 c.c. across; in some spots they have a
bright yellow color. In the posterior parts of the middle and lower lobes
there is flabby consolidation where the tissue has a cloudy, red color with
scattered ill-defined yellow spots.
Bacteriologic examination shows the presence of hemolytic streptococci
in the blood of the heart; hemolytic streptococci with B. influenzæ and S.
aureus in the left lung and S. hemolyticus with S. aureus in the right lung.
Microscopic examination shows that bronchi, bronchioles, alveolar ducts
and the greater part of the infundibula are filled with polynuclear leucocytes,
whereas the alveoli surrounding these structures contain fibrin. The walls
of the small bronchi are thickened and contain mononuclear cells; the adjacent
280alveolar walls are similarly infiltrated and thickened and the fibrin within
them is undergoing organization, being invaded by plasma cells, fibroblasts
and newly formed blood vessels. In some sections interstitial septa are distended
by edema and contain fibrin in abundance; in places the tissue contains
polynuclear leucocytes closely packed together. There are lymphatics greatly
distended by polynuclear leucocytes with some fibrin, lymphocytes and red
blood corpuscles.
Autopsy 428.—D. B., white, aged twenty-five, a farmer from Oklahoma,
had been in military service three weeks. Onset of illness was on September
21, twenty-five days before death, with fever, cough and mucopurulent expectoration.
The patient was admitted with the diagnosis of acute bilateral
bronchitis. Four days later bronchopneumonia was recognized, and subsequently
there was otitis media and empyema; 600 c.c. of thin, purulent fluid
were aspirated from the right chest three days before death.
Anatomic Diagnosis.—Unresolved bronchopneumonia; suppuration of interstitial
tissue of upper right and lower left lobes; purulent bronchitis;
fibrinopurulent pleurisy; thoracotomy wound at the base of the right chest;
collapse of both lungs; serofibrinous pericarditis.
The left pleural cavity contains 550 c.c. of turbid seropurulent fluid in
which are numerous flakes of soft fibrin. The right pleural cavity contains
150 c.c. of similar fluid. The mediastinum is edematous. The pericardial
cavity contains 50 c.c. of yellow fluid.
The right lung is moderately collapsed. In the upper and lower lobes are
small patches of red, lobular consolidation. The upper third of the upper
lobe is laxly consolidated and near its inner surface the interstitial septa are
thickened to from 1 to 1.5 mm. in width, and at intervals occur bead-like
swellings from which creamy purulent fluid exudes upon the cut surface. In
the left lung small patches of gray consolidation occur throughout the lower
lobe and here the interstitial septa are thickened, beaded and contain purulent
fluid.
Bacteriologic examination shows that the blood contains S. hemolyticus;
from the right lung and from the right main bronchus hemolytic streptococci
and B. influenzæ are grown.
Microscopic examination shows that the epithelium of the bronchi has
undergone hypertrophy; the wall is infiltrated with lymphoid and plasma
cells and thickened by new formation of fibrous tissue; there is similar thickening
of adjacent alveolar septa and alveoli, often lined by cubical cells, are
diminished in size. Connective tissue about the blood vessels and the interstitial
septa are thickened and infiltrated with mononuclear cells. In parts
of the lung the interstitial septa are edematous and contain polynuclear leucocytes,
in some places in great number. Lymphatics are greatly dilated and
filled with polynuclear leucocytes which in the center of some lymphatics have
undergone necrosis. In one place a small abscess is in contact with a distended
lymphatic. Lymphatics contain Gram-staining cocci in pairs and short
chains, present in immense number where necrosis has occurred.
Autopsy 433.—B. J., white, aged twenty-seven, from Arkansas, has been
in military service one month. Onset of illness was on September 28, nineteen
281days before death, with cough and expectoration. Pneumonic consolidation
was recognized two days later and 20 c.c. of cloudy fluid were aspirated
from the left chest on the same day. Hemolytic streptococci were found
in a culture from the throat nine days before death.
Anatomic Diagnosis.—Unresolved bronchopneumonia with peribronchiolar
and confluent lobular consolidation; interstitial suppuration of the right lower
lobe; purulent bronchitis; fibrinopurulent pleurisy.
The right pleural cavity contains 700 c.c. of yellowish gray purulent fluid
containing flakes of fibrin. The left pleural cavity contains seropurulent
fluid localized over the external part of the lung.
The right lung is voluminous and free from consolidation save at the lower
and posterior part of the lower lobe where the tissue is deep red and studded
with firmer spots of yellow color clustered about the bronchi. In places
the interstitial septa are thickened and yellow. Surrounding some of the
bronchi near the apex of the left lung are red patches of consolidation.
Culture from heart’s blood remained sterile. S. hemolyticus was grown
from right pleural cavity, and S. hemolyticus and B. influenzæ were grown
from the right lung. Culture from the left lung contained S. aureus and
contaminating microorganisms.
Microscopic examination shows the presence of peribronchiolar patches of
pneumonia in which there are few polynuclear leucocytes and many lymphoid
and plasma cells; the alveolar walls are thickened and infiltrated with mononuclear
cells. In some sections the tissue is wholly consolidated and the site
of advanced organizing pneumonia. Interlobular septa and connective tissue
about blood vessels are thickened and cellular. Small bronchi have lost their
epithelial lining, their walls are thickened and there is peribronchial organizing
pneumonia. In some sections the lymphatics are immensely dilated and
distended with polynuclear leucocytes. There is necrosis of the walls of the
lymphatics and of the polynuclear leucocytes within the lumen.
In the discussion of acute bronchopneumonia it has been
shown that S. hemolyticus is not infrequently a secondary
invader of a pneumonic lesion perhaps caused by pneumococci.
With progress of the disease hemolytic streptococci
persist. In the autopsies with unresolved pneumonia
just described, hemolytic streptococci have found their
way into the lymphatics and produced suppurative lymphangitis
with inflammation of the interstitial septa of the
lung.
282
CHAPTER V
SECONDARY INFECTION IN THE WARD TREATMENT OF MEASLES
A study of 979 cases of measles was made in the base
hospitals of Camps Funston and Pike from July to December,
1918, with the purpose of establishing any existing relation
between the prevalence of the hemolytic streptococci
and the incidence of the graver complications of measles,
especially the pneumonia following measles. The greater
number of these cases occurred at Camp Pike coincidently
with the influenza epidemic, so that the picture is modified
during this period by a summation of the after effects of
the two diseases.
The work undertaken includes:
(a) Routine throat cultures on admission of all patients
with measles.
(b) Separation and treatment in separate wards of the
patients harboring hemolytic streptococci and those free
from such streptococci.
(c) Investigation of the bacteriology of all cases under
treatment, by weekly throat cultures during the period in
the hospital.
(d) Bacteriologic study of the complications of measles
during life and at autopsy.
(e) Study of the throat bacteriology of men on duty in
the camp, to establish the prevalence of hemolytic streptococci
and of B. influenzæ in normal individuals.
The work is further divided into that done at Camp
Funston during the latter part of July and throughout
August, and that done at Camp Pike during September,
October, November and December, 1918.
283Studies at Camp Funston.—The work done at Camp
Funston is limited strictly to the identification of hemolytic
streptococci in the throats of all patients with measles
coming into the base hospital at Ft. Riley and to the same
study of a group of normal men on duty. During the
period of study hemolytic streptococci were identified by
throat culture in about 1 in 5 of all the normal men examined.
Two instances of otitis media represent the only
complications developing in the 112 cases of measles. Cultures
from both patients showed staphylococci. The entire
absence of streptococcus complications appears the more
surprising in view of the fact that the prevalence of hemolytic
streptococci among patients under treatment in the
ward was for a time as great as that among the normal
men. No special hospital management was instituted on
the basis of the findings in throat culture. S. hemolyticus
carriers remained in the wards and were treated alongside
the “clean” cases. The sheet cubicle system was used for
bed patients. Face masks were not worn. Convalescent
patients were not segregated, and they assisted in the care
of the bed patients and in the ward kitchen. After the
initial throat culture on admission, the throats were
gargled with argyrol and afterwards sprayed with the same
solution three times a day. This solution was also employed
to relieve the discomfort caused by the conjunctivitis
during the acute stage of the disease.
Throat Culture and Identification of Hemolytic Streptococci.—In
general the methods for the isolation and
identification of hemolytic streptococci as adopted by the
Medical Department of the Army were used. All organisms
were isolated in pure culture, grown in broth, examined
microscopically and subjected to tests for hemolysis,
(a 5 per cent suspension of sheep corpuscles being employed),
and for bile solubility.
Beef infusion broth and beef infusion agar constituted
the two basic media used. They were prepared so that the
284finished product titrated about 0.3 per cent acid to phenolphthalein.
Broth tubes were carried to the bedside. In swabbing,
the attempt was made to produce gagging. This causes
the tonsils to protrude from behind the anterior pharyngeal
pillars and places a slight tension on the capsule which
tends to squeeze material from the crypts. The surfaces
of the tonsils thus protruding toward the midline were
brushed quickly with a small cotton swab which was lastly
touched to the posterior pharyngeal wall and withdrawn so
as to avoid touching any other parts. The swab was immediately
introduced into a tube of broth, twirled freely
under the surface of the liquid and discarded. The material
thus washed into the broth was carried to the laboratory
and kept in the ice box until plating, which was accomplished
with as little delay as possible.
Tubes of melted agar containing 12 c.c. cooled below
45° C., after receiving 0.6 c.c. of sterile defibrinated horse
blood, were inoculated with a loopful of this broth. Thorough
mixing and pouring into Petri dishes (10 cm. diameter)
followed. After cooling, a second loopful was
streaked over the surface of one half of the plate. Deep
and superficial planting were thus effected on the same
plate.
This method was found to be very useful. It can be used
with advantage provided one is not called upon to make
a great number of cultures when its time consuming factor
is a great inconvenience. Another disadvantage is the difficulty
of picking single colonies for subculture. In spite
of the most careful selection and fishing of a deep colony,
subcultures are less likely to be pure than when surface
colonies are chosen. By careful regulation of the amount
of agar in the tubes, the addition of a measured amount
of blood to each enabled one to pour standard blood agar
plates. Uniform thorough mixing of the blood is essential
so that the plate may present the desired “silky” rather
285than a “curdled” appearance when viewed by transmitted
light.
The plates were incubated eighteen to twenty-four hours
when subcultures in broth were made from the hemolytic
colonies. After growing these for a similar period the
additional tests were carried out as indicated above.
Hemolytic Streptococci with Measles.—The incidence of
hemolytic streptococci in the throats of patients with
measles admitted to the base hospital at Ft. Riley was
found to be remarkably small.
| Table LV |
|---|
| |
| Hemolytic Streptococci with Measles in all Patients Admitted to the Wards at Camp Funston |
|---|
| |
|
DAYS IN HOSPITAL |
APPROXIMATE DAY OF DISEASE |
NO. OF PATIENTS CULTURED |
NO. WITH HEMOLYTIC STREPTOCOCCI |
PER CENT WITH HEMOLYTIC STREPTOCOCCI |
| First Culture |
0 to 1 |
1 to 8 |
112 |
3 |
2.67 |
| Second Culture |
3 to 10 |
4 to 16 |
86 |
11 |
12.79 |
| Third Culture |
8 to 23 |
12 to 26 |
58 |
14 |
24.14 |
| |
| The first culture represents the findings on admission, in a series of 112 cases; 86 patients being cultured twice; 58 patients three times. |
Of the 112 cases examined on admission only 3, or 2.67
per cent were found to carry hemolytic streptococci. Those
patients who were recultured after from three to ten days
in the hospital showed an incidence of 12.8 per cent. A
third culture including patients from eight to twenty-three
days in the hospital, showed an incidence of 24.1 per cent.
Hemolytic Streptococci in the Throats of Normal Men.—A
total of 274 throat cultures from normal men on duty at
Camp Funston (Table LVI) shows that 21.9 per cent carried
hemolytic streptococci at a time when there were few
upper respiratory infections in the camp. A small group
of men resident in the hospital shows a slightly higher
prevalence of hemolytic streptococci (29.3 per cent).
The figures in Table LVI are in sharp contrast with
those for measles patients on admission to the hospital.
| 286 |
| Table LVI |
|---|
| |
| Incidence of Hemolytic Streptococci, Camp Funston. |
|---|
| |
|
NUMBER EXAMINED |
HEMOLYTIC STREPTOCOCCI PRESENT |
PER CENT WITH HEMOLYTIC STREPTOCOCCI |
| (a) White Men: |
|
|
|
| 70th Infantry |
24 |
4 |
16.7 |
| 210th Engineers, Co. C |
26 |
6 |
23.1 |
| 164th Depot Brigade, Co. 15 |
50 |
10 |
20.0 |
| 164th Depot Brigade, Co. 18 |
51 |
13 |
25.5 |
| 164th Depot Brigade, Co. 28 |
50 |
13 |
26.0 |
| Total |
201 |
46 |
22.9 |
| |
|
|
|
| (b) Colored Men, Detention Camp No. 2: |
|
|
|
| 164th Depot Brigade, Prov. Co. 22 |
25 |
6 |
24.0 |
| 3d Development Battalion, Co. A |
24 |
3 |
12.5 |
| 3d Development Battalion, Co. D |
24 |
5 |
20.8 |
| Total |
73 |
14 |
19.2 |
| |
|
|
|
| (c) Men resident in the hospital: |
|
|
|
| Laboratory workers |
10 |
3 |
30.0 |
| Patients in surgical ward |
14 |
4 |
28.6 |
| Total |
24 |
7 |
29.3 |
Two organizations from which normal men were chosen
for examination furnished a considerable number of cases
of measles and offer data (Table LVII, A and B) for further
comparison.
| Table LVII |
|---|
| |
| A. Hemolytic Streptococci with Measles in 164th Depot Brigade, Company 28. |
|---|
| |
|
DAYS IN HOSPITAL |
NO. OF PATIENTS CULTURED |
NO. WITH HEMOLYTIC STREPTOCOCCI |
PER CENT WITH HEMOLYTIC STREPTOCOCCI |
| First Culture |
0 to 1 |
23 |
0 |
0 |
| Second Culture |
3 to 9 |
23 |
4[90] |
17.4 |
| Third Culture |
10 to 21 |
21 |
4 |
19.05 |
| Normal men of Co. 28 |
|
50 |
13 |
26.00 |
| |
| B. Hemolytic Streptococci with Measles in Seventieth Infantry |
|---|
| |
| First Culture |
0 to 1 |
38 |
0 |
0 |
| Second Culture |
5 to 9 |
25 |
1 |
4.0 |
| Third Culture |
8 to 17 |
12 |
2 |
16.7 |
| Normal men on duty with 70th Infantry |
|
24 |
4 |
16.7 |
287No one of the 61 cases of measles from the two organizations
was found to be positive on admission to the hospital.
Yet among normal men in one of these organizations
the incidence of hemolytic streptococci was 26 per cent
and in the other, 16.7 per cent. In both organizations the
incidence among normal individuals compares closely with
that of the patients after a period in the measles wards
of the hospital.
Discussion.—Three features of the data collected at
Camp Funston are noteworthy. First, the small percentage
of S. hemolyticus carriers among the men admitted to
the hospital with measles as compared with the percentage
found in normal men in the camp. Second, the increase
in the number of S. hemolyticus carriers among patients
during their stay in the hospital, the increase continuing
until it approaches that of the normal men on the outside.
Third, the prevalence of hemolytic streptococci in normal
throats.
In comparing men arriving at the hospital acutely ill
with measles with normal men in the organization from
which they came, only one variable can be found on which
to base the differences observed in the two groups. This
is the advent of the acute disease. The figures seem to suggest
a temporary disappearance of hemolytic streptococci
from the throats of patients acutely ill with measles, at
least, to such an extent that the same cultural methods fail
to identify the organisms.
The increase in the S. hemolyticus carriers among patients
with measles after a period in the hospital might
depend upon two factors: First, the exposure to contact
infections in the hospital ward, depending on the length
of time in the ward as well as on the character of the ward
management; second, the passing of the acute stage of
measles with a return of the bacterial flora of the throat to
the condition existing before the onset of the acute disease.
The first appears the more probable. The second has only
288the support of the observation that the streptococci were
absent from the throat during the acute stage of measles
or were much less frequently found in patients with measles
than in normal men and later their incidence approached
that in normal individuals. The rather high incidence of
hemolytic streptococci in normal men at Camp Funston may
have been due to the very recent assembling of the 10th
Division which now occupied the camp. It is probable that
the housing of large numbers of men in barracks is attended
by the same contact dissemination of mouth organisms
that occurs in hospital wards.
Measles at Camp Pike.—All cases of measles coming into
the base hospital at Camp Pike between September 15 and
December 15, 1918, a total of 867 cases, are included in the
report. Upon the arrival of the commission at Camp Pike
early in September, a plan for the separation of cases carrying
hemolytic streptococci and those free from these organisms
was put into operation. The preliminary arrangements
included the allotment of suitable wards for treatment
of the different classes of cases; a throat culture survey
of all patients with measles under treatment at the
time; their separation in accordance with the results of
bacteriologic examination, and the transfer of each group
of patients to its designated ward. By September 15 these
preliminary arrangements had been completed. Cases of
measles admitted on this date and afterwards were held in
an observation ward pending the report upon a throat culture
before they were transferred to the treatment wards.
Beginning September 15 the following system of handling
measles cases was maintained in the wards of the base
hospital.
All patients were received in an observation ward where
they remained until the results of a throat culture for hemolytic
streptococci could be reported back to the ward.
Cases reported positive or negative were immediately transferred
to their respective treatment wards. All patients in
289the treatment wards were cultured at intervals of one week
and cases found positive were transferred from the “clean”
treatment wards to a treatment ward for cases carrying
hemolytic streptococci. The ward personnel attending patients
in the “clean” treatment wards was examined by
throat cultures from time to time with the purpose of eliminating
S. hemolyticus carriers. Patients segregated in the
streptococcus wards remained there, if uncomplicated,
throughout their hospital treatment even though subsequent
repeated throat cultures showed that the carrier condition
had disappeared. Two wards were provided to care
for the pneumonia following measles. One received only
patients whose throat cultures were negative for hemolytic
streptococci; the other, those positive. It is essential that
the throat culture on which this differentiation is made be
taken as soon as the complication is reported and that
transfer be made promptly on receipt of the report of the
culture. To facilitate this transfer, cases of pneumonia
complicating measles were reported to the laboratory as
soon as diagnosed and cultures were taken at once. The
case remained in the measles ward during twenty-four
hours, isolated as well as possible, awaiting report of culture
before transfer. Within the positive ward for measles
pneumonias, distinction was made between streptococcus
pneumonias and nonstreptococcus pneumonias harboring
hemolytic streptococci in their throats. The two classes of
cases were treated in separate sections of the ward.
Ear complications were seen and treated by medical officers
from the otological service. These patients remained
in the measles wards while in the acute stage of measles,
but later were transferred to the service of otology whenever
further surgical treatment became necessary.
Within the individual wards for treatment of measles
and measles pneumonias, precautions for minimizing the
dangers of contact infections were carried out as well as
possible. Throughout the study we had the hearty cooperation
290of the base hospital authorities and earnest, well-directed
effort to perfect ward management on the part of
the ward surgeons and their staffs. Difficulties encountered
during the emergency created by the sudden explosion
of the influenza epidemic, in spite of the best efforts of all,
did much to disrupt the plan which had been instituted for
the control and study of the complications of measles.
Scarcely had wards been designated and all measles patients
on hand differentially allotted to them, when the influenza
epidemic appeared and quickly filled the hospital
beyond its capacity. Measles wards were taken over for
the care of influenza patients. Measles patients, of which
there were not a great number at the time, were necessarily
crowded together, so that compartments of wards instead
of separate wards had to be used in maintaining our separation
of the two groups of patients. While the base hospital
was yet filled with patients with influenza and influenza
pneumonia, admission of patients with measles increased,
so that one ward after another was reclaimed for
the care of this disease. During this period the measles
wards were at times overcrowded and the strictest ward
technic could not be practiced. Again new wards were,
on occasions, partly filled by admission and transfer before
they were properly equipped to receive patients. This disorganization
was directly due to the necessity of treating
a rapidly increasing number of measles patients before the
hospital was cleared of patients with influenza and pneumonia.
After this emergency, the system of ward management
was rapidly readjusted, and admissions were limited to the
normal capacities of the wards.
The cubicle system was used in all wards. Bed patients
were not required to wear masks, but the mask was strictly
enforced upon all patients leaving the cubicle. All attendants
were required to wear gowns, caps and masks while
in the wards. An attempt was made to prevent the congregating
of convalescents. Guards were posted at the latrine
291doors to limit admission to the capacity of the latrine. Borrowing
and lending of any materials between patients were
strictly forbidden. Paper sputum cups were provided,
kept clean and covered. In the measles pneumonia wards
hand disinfectant solutions were provided for use by attendants
when they passed from one patient to another.
The ward floors were scrubbed at intervals with lysol in
water. Dry sweeping of the wards in the morning is regrettable.
Bacteriologic Methods Used in the Study.—The methods
used for the identification of hemolytic streptococci here
were essentially the same as those used at Camp Funston
and described above, the one exception being the use of
surface cultures on blood agar instead of the combined surface
and deep culture. Blood agar plates containing 5 per
cent defibrinated horse blood were poured and used while
fresh. The throat swabs were carried to the laboratory in
sterile test tubes. The plates were inoculated by touching
the swab lightly to the surface of the agar plate at two
places, one near either extremity of a given diameter of
the plate. On touching the swab to the agar, the swab
stick was rolled between the fingers so as to turn it through
one revolution and thereby bring all points of the circumference
of the cotton swab in contact with the agar surface.
The material thus inoculated on the plates was spread by
means of a platinum wire slightly turned over at the end in
“hockey stick” fashion. The wire was passed back and
forth several times over the point of inoculation and then
multiple streaks and cross streaks were made over the agar
surface. The initial contact of the wire with the point of inoculation
was not repeated. The cross streaking serves to
spread and distribute this material evenly over the surface.
Well seeded plates by this multiple streak method are the
rule and the uniform distribution of well separated colonies
over the surface makes it very easy to pick pure cultures,
and renders plate reading easy.
292Very early in the course of our study of throat cultures
at Camp Pike, the great frequency of abundant growths of
B. influenzæ was observed. Consequently, the throat cultures
of all measles patients examined from September 15
to October 20 were studied for the identification of B.
influenzæ. In all cases identification was based on the cultural,
staining and morphologic characteristics. Tests for
growth on hemoglobin free media were not made as a
routine.
Relation of Measles and Pneumonia Following Measles
to the Influenza Epidemic.—The influenza epidemic at
Camp Pike was recognized on September 23 because of an
alarming increase of hospital admissions. It ran its brief
course, and ten days later, October 3, the decline began.
The first four days of October rank highest in admissions
of patients with pneumonia following influenza. The onset
of 20 scattered cases of measles occurred before September
25, and later the number slowly increased reaching its
height about the middle of October; after this time a gradual
decline began, and continued during about three weeks
before the preepidemic level was reached. During this
period of six weeks following September 25, 709 cases of
measles occurred.
| Table LVIII |
|---|
| |
| Onset of Measles and of Pneumonia Following Measles by Weeks from September 11 to December 11, 1918 |
|---|
| |
| DATES |
MEASLES |
PNEUMONIA FOLLOWING MEASLES |
| Sept. 11 to 17 |
18 |
0 |
| Sept. 18 to 24 |
20 |
0 |
| Sept. 25 to Oct. 1 |
74 |
0 |
| Oct. 2 to 8 |
143 |
13 |
| Oct. 9 to 15 |
178 |
9 |
| Oct. 16 to 22 |
158 |
16 |
| Oct. 28 to 29 |
100 |
6 |
| Oct. 30 to Nov. 5 |
56 |
3 |
| Nov. 6 to 12 |
38 |
4 |
| Nov. 13 to 19 |
23 |
1 |
| Nov. 20 to 26 |
29 |
1 |
| Nov. 27 to Dec. 3 |
22 |
1 |
| Dec. 4 to 10 |
8 |
1 |
| Dec. 11 |
0 |
1 |
293Pneumonia following measles began to appear on October
5, and within the week following 16 cases occurred. An
equal number of cases appeared each week during about
three weeks and fewer scattered cases occurred throughout
November and December. Table LVIII shows date of onset
of measles and measles pneumonia cases.
Chart 3 presents the occurrence of measles and of the
pneumonia following measles by weeks of onset compared
with that of epidemic influenza.
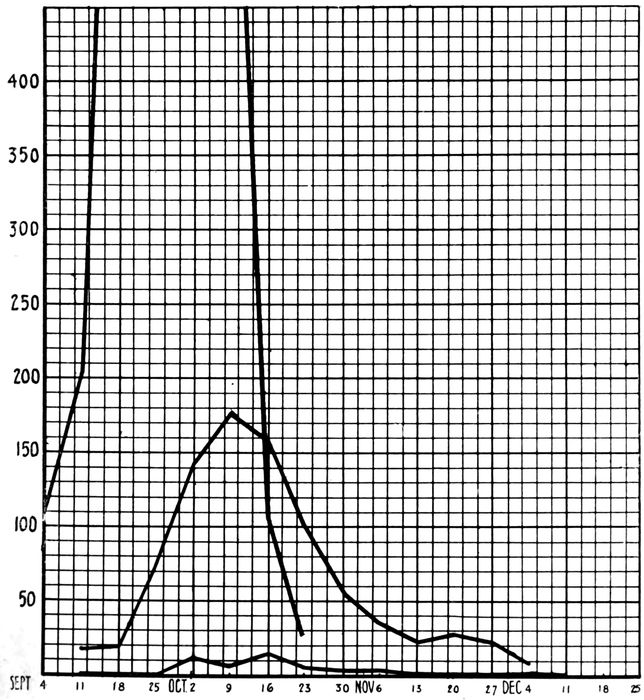
Chart 3.—Shows the relation of the epidemic of measles to that of influenza at Camp Pike, and the relations of the pneumonia following measles to both measles and influenza. The large incomplete curve represents influenza; the intermediate curve, measles; the small curve, pneumonia following measles.
294It will be noted from the overlapping of the two curves
in Chart 3 that a considerable portion of the measles cases
appeared before the influenza had subsided in Camp Pike.
This occurrence of the two epidemics at the same time
makes it impossible to separate the parts played by each
disease in producing the pneumonias and other complications
following measles. Analysis of the chart, however,
shows that the pneumonia with measles occurred in large
part during the first half of the measles epidemic. This
is of particular significance since it was during this period
that the effects of the influenza wave were felt most severely.
In Table LIX the cases of measles are grouped into
fifteen day periods according to their dates of onset and
the pneumonias arising from each group are tabulated.
This tabulation shows very clearly that the pneumonia
complications developed in large part in patients with
measles entering the hospital during the influenza period,
that is, late in September and during the first half of
October.
| Table LIX |
|---|
| |
| Patients with Measles and with Subsequent Pneumonia |
|---|
| |
| DATES |
TOTAL CASES OF MEASLES DURING INTERVALS OF 15 DAYS |
TOTAL CASES PNEUMONIA FROM SAME |
OF PER CENT INCIDENCE OF PNEUMONIAS |
| Sept. 11 to 30 |
86 |
433 |
14 |
42 |
16.28 |
9.7% |
| Oct. 1 to 15 |
347 |
28 |
8.07 |
| Oct. 16 to 31 |
270 |
434 |
8 |
14 |
2.96 |
3.2% |
| Nov. 1 to 15 |
91 |
2 |
2.2 |
| Nov. 16 to 30 |
56 |
4 |
7.15 |
| Dec. 1 to 15 |
17 |
0 |
|
The high incidence of pneumonia among measles patients
coming into the hospital prior to, with, or immediately following
the height of the influenza epidemic is very striking.
It so happens that half of the total number of measles cases
295considered, date their onsets prior to October 15. From the
433 cases included in this first half, 42 cases of pneumonia
arose, while from the 434 cases arising during the two
months following October 15, only 14 or one-third as many
cases of pneumonia developed. These figures very strongly
suggest that influenza played a large part in the production
of the pneumonia with measles in this group of cases.
Again the 9.7 per cent incidence of pneumonia in the first
half of cases considered, approaches the 12 per cent incidence
of pneumonia following influenza observed in the epidemic
at Camp Pike, while the incidence of 3.2 per cent in
the second half of the cases conforms more nearly to figures
for pneumonia following measles in the army prior to the
pandemic of influenza.
It has been shown that the prevalence of B. influenzæ at
Camp Pike increased with the passing of the wave of influenza
(p. 40) and that this increase applied to the
measles admissions. For a time the separation of measles
patients carrying B. influenzæ as identified by throat culture
on admission, from those free from it, was practiced.
All cases were then followed up by weekly throat cultures,
and cases in negative wards on being identified as positives
were transferred.
This practice was discontinued as impractical when it
became apparent that about 80 per cent of patients with
measles would be found positive for B. influenzæ when repeated
throat cultures were made during their hospital
treatment. The dissemination of B. influenzæ through the
wards from which we were attempting to exclude it took
place much faster than we could follow its spread by cultural
methods. When this became evident, the practice
of separating the two groups of patients with reference to
B. influenzæ was discontinued and the great inconvenience
of repeated transfer of patients was largely eliminated.
Table LX gives the findings in 426 cases of measles
cultured for B. influenzæ during the period when the practice of separating measles patients carrying B. influenzæ
from those not carrying the organisms was followed.
296
| Table LX |
|---|
| |
| Results of Repeated Throat Cultures for B. Influenzæ on 426 Cases of Measles, Camp Pike, Sept. 15 to Oct. 20, 1918. |
|---|
| |
| GROUPS |
TOTAL NUMBER CULTURED IN GROUP |
GROUP NO. NEGATIVE FOR B. INFLUENZÆ ON ADMISSION |
RESULTS OF CULTURES TO DATE |
GROUP NO. POSITIVE FOR B. INF. TO DATE |
GROUP OF POSITIVES DEVELOPING TO DATE IN CASES NEGATIVE FOR B. INF. ON ADMISSION |
PER CENT OF GROUP POSITIVE FOR B. INF. TO DATE |
GROUP PER CENT OF POSITIVES TO DATE AMONG CASES NEGATIVE FOR B. INF. ON ADMISSION |
| 1ST CULTURE |
2ND CULTURE |
3RD CULTURE |
4TH CULTURE |
NO. IN EACH CLASS |
| I |
|
|
|
|
|
|
|
|
|
|
|
| 1st culture on admission |
426 |
|
− |
|
|
|
274 |
152 |
|
35.6 |
|
| + |
|
|
|
152 |
| II |
|
|
|
|
|
|
|
|
|
|
|
| 1st and 2nd culture, after one week in hospital |
201 |
143 |
− |
− |
|
|
75 |
126 |
68 |
62.7 |
47.5 |
| − |
+ |
|
|
68 |
| + |
+ |
|
|
29 |
| + |
− |
|
|
29 |
| III |
|
|
|
|
|
|
|
|
|
|
|
| 1st, 2nd and 3rd cultures after two weeks in hospital |
94 |
69 |
− |
− |
− |
|
22 |
72 |
47 |
77.7 |
68.1 |
| − |
− |
+ |
|
18 |
| − |
+ |
− |
|
13 |
| − |
+ |
+ |
|
16 |
| + |
+ |
+ |
|
8 |
| + |
− |
+ |
|
6 |
| + |
+ |
− |
|
4 |
| + |
− |
− |
|
7 |
| IV |
|
|
|
|
|
|
|
|
|
|
|
| 1st, 2nd, 3rd and 4th cultures after three weeks in hospital |
25 |
19 |
− |
− |
− |
− |
4 |
21 |
15 |
84 |
79. |
| − |
− |
− |
+ |
3 |
| − |
− |
+ |
+ |
3 |
| − |
− |
+ |
− |
2 |
| − |
+ |
+ |
+ |
2 |
| − |
+ |
− |
+ |
2 |
| − |
+ |
+ |
− |
2 |
| − |
+ |
− |
− |
1 |
| + |
+ |
+ |
+ |
2 |
| + |
− |
− |
+ |
1 |
| + |
− |
+ |
+ |
1 |
| + |
+ |
+ |
− |
1 |
| + |
− |
− |
− |
1 |
297On admission 35.6 per cent of the patients were found
positive for B. influenzæ. Repeated throat cultures were
not confined to those appearing negative on this initial culture,
but were made on all patients without regard to their
being previously positive or negative. By a summation
of the results of the weekly cultures of all patients, the percentage
of patients carrying B. influenzæ rises from 35.6
per cent on admission, to 62.7 per cent after one week;
to 77.7 per cent after two weeks; to 84 per cent after three
weeks in the hospital.
To gain some idea of the rate of spread of B. influenzæ
in wards receiving only patients whose throat cultures were
negative for B. influenzæ on admission, a similar summation
of the results of repeated throat cultures on patients
in negative wards shows weekly increases from 47.5 per
cent after one week, to 68.1 per cent after two weeks; to
79 per cent at the end of three weeks.
These results demonstrate quite clearly that the measles
wards were saturated with B. influenzæ during the period
of the influenza epidemic. Conditions within the measles
wards with regard to B. influenzæ were not at all different
from those in the camp community during this period.
While no clinical methods could be relied upon to
diagnose influenza in the presence of an acute attack of
measles, there is every reason to believe that the occurrence
of clinical influenza with measles was no less frequent than
was its incidence in the camp at large, that is, about 20 to
25 per cent. That influenza played a large part in determining
predisposition to the complications of measles in
this series seems evident.
Hemolytic Streptococci with Measles at Camp Pike
Between September 15 and December 15, 1918, 867 cases
of measles, admitted to the wards of the base hospital, were
298studied and handled according to the system outlined
above. About one half of these cases appeared during the
first month of the study. During this month hemolytic
streptococci played a very insignificant rôle. This microorganism
did not appear with alarming prevalence until
after the wards had been thoroughly overcrowded. After
the emergency, when better ward conditions were provided,
S. hemolyticus carriers continued to develop in the wards
and were removed when identified. The first S. hemolyticus
carriers to develop in the wards were identified on October
8. The first case of streptococcus pneumonia developed
on October 17, while streptococcus otitis as a complication
of measles did not begin until a little later. During
the latter two months of the study, S. hemolyticus became
rampant in the wards. The streptococcus complications
date their onset at some time during these two
months.
Table LXI shows the number of admissions to the measles
wards by weeks and the patients among them found to be
carrying hemolytic streptococci. It also shows the number
of S. hemolyticus carriers developing each week among
patients under treatment in the “clean” wards, as identified
by throat cultures repeated at weekly intervals. For
purposes of orientation, the number of cases developing
streptococcus pneumonia and otitis media with its subsequent
mastoiditis are given for each week during the period
of observation.
An admission to the measles ward can generally be regarded
as an acute case of measles. There are a few exceptions
to this statement and these are cases of measles
treated in barracks and afterwards transferred to the base
hospital. A relatively small number of such cases furnished
16 of the cases positive for hemolytic streptococci
on admission to the measles ward.
299
| Table LXI |
|---|
| |
| S. Hemolyticus Carriers Identified by Throat Culture Among Admissions; Those Developing Among Patients Under Treatment in the Streptococcus “Clean” Measles Wards; S. Hemolyticus Complications According to Their Dates of Onset |
|---|
| |
| GROUPING OF CASES BY WEEKS |
ADMISSION CASES |
HEMOLYTIC STREPTOCOCCI HOSPITAL CASES DEVELOPING |
PRINCIPAL COMPLICATIONS DUE TO HEM. STREP. |
| NO. CASES CULTURED |
NO. POS. HEM. STREP. |
PER CENT POS. HEM. STREP. |
NO. CASES CULTURED |
NO. POS. HEM. STREP. |
PER CENT POS. HEM. STREP. |
PNEUM. |
OTITIS |
MASTOIDITIS |
| Sept. 15 to Sept. 21 |
23 |
252 |
1 |
3 |
1.2 |
0 |
0 |
0 |
0 |
0 |
0 |
| Sept. 22 to Sept. 29 |
25 |
1 |
23 |
0 |
0 |
0 |
0 |
0 |
| Sept. 30 to Oct. 6 |
95 |
0 |
24 |
0 |
0 |
[91]1 |
0 |
0 |
| Oct. 7 to Oct. 13 |
109 |
1 |
121 |
4 |
3.3 |
0 |
0 |
0 |
| Oct. 14 to Oct. 20 |
223 |
494 |
7 |
19 |
3.8 |
175 |
8 |
4.6 |
1 |
0 |
0 |
| Oct. 21 to Oct. 27 |
156 |
5 |
451 |
35 |
7.7 |
2 |
3 |
0 |
| Oct. 28 to Nov. 3 |
71 |
6 |
333 |
29 |
8.7 |
1 |
12 |
1 |
| Nov. 4 to Nov. 10 |
44 |
1 |
263 |
45 |
17.1 |
3 |
8 |
11 |
| Nov. 11 to Nov. 17 |
31 |
117 |
4 |
13 |
11.1 |
149 |
46 |
30.8 |
0 |
5 |
5 |
| Nov. 18 to Nov. 24 |
41 |
4 |
93 |
7 |
7.5 |
0 |
2 |
2 |
| Nov. 25 to Dec. 1 |
19 |
0 |
48 |
7 |
14.6 |
0 |
3 |
2 |
| Dec. 2 to Dec. 8 |
26 |
5 |
52 |
12 |
23.1 |
0 |
3 |
0 |
| Dec. 9 to Dec. 15 |
4 |
|
2 |
|
|
47 |
12 |
25.5 |
1 |
0 |
0 |
300An admission to the measles ward does not indicate admission
to the hospital, because a considerable number of
cases of measles developed from time to time among patients
under treatment in the hospital for other conditions.
Since these patients remained in other wards not subject to
the same ward management and with no distinction between
those positive and those negative for hemolytic
streptococci, they cannot be included in figures to show the
incidence of hemolytic streptococci in patients with measles
at the time of admission to hospital from the camp. Two
classifications of the 37 cases, positive when first observed,
are necessary.
1. Division of cases according to days in the hospital
before first culture was taken:
| Days in Hospital |
No. of cases |
| 0–1 (admission) |
15 (2 not acute) |
| 2–7 |
10 |
| More than 7 |
12 |
2. Classification according to stage of the disease:
| During acute stage |
21 cases |
| After acute stage |
16 cases |
The first classification shows only 13 cases positive
when cultured on admission to the hospital and also during
the acute stage of the disease; the incidence of S. hemolyticus
in patients on admission is very low (1.76 per cent).
The second classification shows a slightly higher incidence
for cases during the acute stage of the disease, regardless
of whether they were admitted to the measles service
from camp or from another service of the hospital
(2.4 per cent). These findings conform with those at Fort
Riley in a smaller series of cases and support the opinion
that the hemolytic streptococci temporarily disappear from
the throat during the acute onset of measles. Unfortunately
controls among normal men in Camp Pike were not
taken at intervals throughout the period of three months
represented by this study of measles, but all controls taken
show a higher incidence than that found among measles
301patients on admissions over a period of time comparable to
that of the control series.
The gradual increase in the percentage of patients developing
hemolytic streptococci in their throats in wards
receiving only streptococcus free cases demonstrates that
the admission culture and the subsequent weekly cultures,
with the separation of all patients identified as carriers,
did not suffice to control the spread of streptococcus in this
group of cases. It is interesting to note that the greatest
incidence of streptococcus carriers among these patients
occurred three weeks after the height of the measles epidemic,
when it became about four times that observed at
the height of the measles epidemic.
When we consider the time relations of the streptococcus
complications, it is noteworthy that they begin to
appear somewhat after the appearance of streptococcus
carriers and then increase parallel with the increase in the
numbers of carriers. The relative number of complications
developing among the first carriers which were identified is
less than that among the carriers appearing later. This
suggests an increase in virulence of hemolytic streptococci
attending their wider dissemination.
Tables LXII and LXIII are introduced for the purpose of
showing to what extent duration of stay in the hospital
increases the individual’s chances of acquiring hemolytic
streptococci. Table LXII includes all cases admitted to and
treated in the measles wards. On repeated cultures, previous
positives and negatives were cultured alike and the
total positives reported for each week.
Table LXIII includes only those cases treated in the
“clean” wards and known to be negative on previous culture.
| 302 |
| Table LXII |
|---|
| |
| Incidence of Hemolytic Streptococci in Throats of Measles Cases with Reference to Period in Hospital |
|---|
| |
| (All cases treated in the wards) |
|---|
| |
| PERIOD IN MEASLES WARD |
NO. CASES CULTURED |
NO. POSITIVE FOR HEMOLYTIC STREPTOCOCCI |
PER CENT POSITIVE FOR HEMOLYTIC STREPTOCOCCI |
| (Admission) |
867 |
37 |
4.2 |
| 1 week |
768 |
84 |
10.9 |
| 2 weeks |
479 |
109 |
22.8 |
| 3 weeks |
240 |
63 |
26.2 |
| 4 weeks |
133 |
44 |
33.1 |
| 5 weeks |
82 |
26 |
31.7 |
| 6 weeks |
53 |
14 |
26.4 |
| 7 weeks |
25 |
8 |
32.0 |
| 8 weeks |
13 |
1 |
7.7 |
| 9 weeks |
9 |
1 |
11.1 |
| 10 weeks |
6 |
0 |
0 |
| 11 weeks |
5 |
0 |
0 |
| |
| Table LXIII |
|---|
| |
| Weekly Development of Hemolytic Streptococci in Throats of Patients Treated in “Clean” Wards |
|---|
| |
| PERIOD IN MEASLES WARD |
NO. CASES CULTURED |
NO. POSITIVE FOR HEMOLYTIC STREPTOCOCCI |
PER CENT POSITIVE FOR HEMOLYTIC STREPTOCOCCI |
| 1 week |
738 |
67 |
9.1 |
| 2 weeks |
424 |
74 |
17.4 |
| 3 weeks |
195 |
34 |
17.4 |
| 4 weeks |
92 |
16 |
17.4 |
| 5 weeks |
46 |
7 |
15.2 |
| 6 weeks |
26 |
4 |
15.4 |
| 7 weeks |
14 |
3 |
21.4 |
| 8 weeks |
8 |
0 |
|
| 9 weeks |
5 |
0 |
|
| 10 weeks |
4 |
0 |
|
| 11 weeks |
3 |
0 |
|
A comparison of Tables LXII and LXIII gives some indication
of what might have been expected if the carriers had
not been removed from the treatment wards at weekly intervals.
With the carriers removed from the “clean”
cases and segregated in a separate ward so as to be removed
effectively as sources of spread of the S. hemolyticus
infection to clean cases, the percentage incidence with
all cases considered rose to a point nearly twice as high
as that ever reached in the wards where clean cases alone
were allowed to remain. Had these carriers not been separated,
and remained in contact with cases free from hemolytic
streptococci, they would have served as just so many
more sources of infection, and an incidence of at least twice
303that recorded for all cases combined, or four times that
of the treatment wards, might have been expected. These
results indicate that the weekly separation of carriers from
clean cases did, to a considerable extent, lower the individual’s
danger of acquiring S. hemolyticus infection
while in the hospital.
Complications of Measles
In Table LXIV the complications developing in the measles
patients under observation at Camp Pike are tabulated.
In the division of the complications developing in “carriers”
and “noncarriers” of the hemolytic streptococci, reference
is made only to the records of the throat cultures.
The division is therefore not dependent upon the bacteriology
of the complications. For example, only 9 of the 12 cases
of pneumonia developing in “carriers” were streptococcus
pneumonias. On the other hand, the cases of mastoiditis
following otitis media were almost invariably due to hemolytic
streptococci. Of the 10 otitis cases occurring in “noncarriers,”
4 developed mastoiditis and 3 of these showed
hemolytic streptococci on culture from the mastoid cells
at operation. Missed cases of identification of S. hemolyticus
by throat culture in cases which develop S. hemolyticus
complications may arise from a number of causes.
It is desired here only to direct attention to these discrepancies.
Pneumonia Following Measles.—Fifty-six cases of pneumonia
following measles occurred during the period of observation
in this group of 867 cases of measles. Of these,
9 were streptococcus pneumonias. This gives an incidence
for streptococcus pneumonias of 1.04 per cent, while that
for all the pneumonia is 6.4 per cent. There were 8 cases
of lobar and 48 cases of bronchopneumonia. Seventeen
fatal cases occurred giving a mortality rate of 30.4 per cent
for the group. Five of these fatal cases occurred among
the 9 streptococcus pneumonias. The mortality rate for
the streptococcus pneumonia thus was 55.5 per cent; that
for the nonstreptococcus group was 25.5 per cent. All 9
cases of streptococcus pneumonia developed empyema. In
7 cases it was diagnosed clinically; in 2 at autopsy only.
No cases of empyema developed in the group of nonstreptococcus
pneumonias.
304
| Table LXIV |
|---|
| |
| Complications Developing in 867 Cases of Measles at Camp Pike. Distribution of Complications Between 242 “Carriers” and 625 “Noncarriers” of Hemolytic Streptococci from September 15 to December 15, 1918 |
|---|
| |
| NAME OF COMPLICATION |
NUMBER OCCURRING IN |
TOTAL NUMBER |
PER CENT IN |
| “CARRIERS” OF HEM. STREP. |
“NONCARRIERS” OF HEM. STREP. |
CASES WITH INCOMPLETE RECORD OF THROAT CULTURES |
ALL CASES |
HEM. STREP. “CARRIERS” |
“NONCARRIERS” OF HEM. STREP. |
| Pneumonia |
12 |
44 |
0 |
56 |
6.4 |
5.0 |
7.0 |
| Otitis media |
31 |
11 |
6 |
48 |
5.5 |
12.8 |
1.8 |
| Mastoiditis (following otitis media) |
15 |
4 |
4 |
23 |
2.6 |
6.2 |
0.6 |
| Local meningitis (extension from mastoid) |
2 |
0 |
0 |
2 |
|
|
|
| Frontal sinusitis |
1 |
0 |
0 |
1 |
|
|
|
| Ethmoidal sinusitis |
0 |
1 |
0 |
1 |
|
|
|
| Suppurative arthritis |
1 |
0 |
0 |
1 |
|
|
|
| Cervical adenitis |
1 |
0 |
0 |
1 |
|
|
|
| Acute bronchitis |
4 |
2 |
0 |
6 |
|
|
|
| Acute tonsillitis |
4 |
1 |
0 |
5 |
|
|
|
| Acute laryngitis and aphonia |
1 |
0 |
0 |
1 |
|
|
|
| Acute pleurisy |
2 |
1 |
0 |
3 |
|
|
|
| Erysipelas of face |
0 |
1 |
0 |
1 |
|
|
|
| Epidemic meningitis |
0 |
1 |
0 |
1 |
|
|
|
| |
| Note.—The percentages of incidence of pneumonia and otitis media in the “carrier” and “noncarrier” groups are at direct variance. It would appear from these findings that streptococci very readily invade the middle ear from the throat and set up grave disorders. The invasion of the lung from the throat occurs with less frequency. Hemolytic streptococci perhaps never initiate the pneumonic processes and can be regarded as more or less accidental secondary invaders. |
305The relation of these pneumonias following measles, to
the influenza epidemic has been discussed. The time relations
between the onsets of measles and that of the subsequent
pneumonia vary widely. There appears to be
nothing constant in the length of time between the onset
of measles and that of the pneumonia. In 30 of the cases
this period is less than ten days; in the remaining 26 cases,
it ranges from ten to thirty-two days (Chart 4).
In the ward treatment of these cases of pneumonia, they
were divided into three groups according to their clinical
characters and according to the results of throat and
sputum cultures.
| (a) |
Streptococcus pneumonias |
9 cases |
| (b) |
Pneumonia with hemolytic streptococci in the throat without symptoms referable to the streptococcus |
13 cases |
| (c) |
Pneumococcus pneumonias not carrying hemolytic streptococci |
34 cases |
The streptococcus-free cases were treated in a separate
ward. Cases were admitted to this ward directly from the
“clean” measles wards, but only after a throat culture
taken prior to their transfer had been negative for the
hemolytic streptococcus.
The other two groups were treated together in another
ward, but in strictly separate compartments of it. This
precaution was carried out on the assumption that patients
with an acute streptococcus pneumonia were real sources
of danger in the ward because of a heightened virulence of
the organism causing the grave symptoms. The pneumonias
subsequently developing hemolytic streptococci in
their throats, without their presence modifying the course
of the pneumonia, came to be regarded as being in the same
class with uncomplicated cases of measles carrying hemolytic
streptococci, in so far as their being potential sources
of danger in a ward is concerned.
306
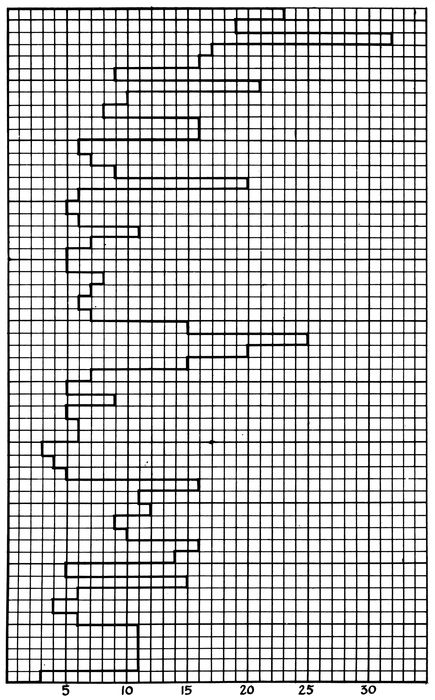
Chart 4.—Shows the time interval between the onset of measles and the onset of the subsequent pneumonia in the 56 cases of pneumonia following measles at Camp Pike. Each case is represented by one of the small blocks measured along the ordinate. The onset of measles in all cases is represented by the line at the extreme left of the chart. The onset of pneumonia in each case is indicated by the limit of the block marked off in days to the right of this line.
307(a) Streptococcus Pneumonias.—Nine cases of streptococcus
pneumonia developed. Of the 867 cases of measles
studied, 242 showed throat cultures positive for the hemolytic
streptococci at some period of their stay in the hospital.
It appears then that 3.7 per cent of the patients
carrying hemolytic streptococci in their throats developed
streptococcus pneumonia. Thirty-seven cases had positive
throat cultures when first observed on admission to the
measles wards. It is significant to note that not a single
case of pneumonia of any kind developed among these
cases.
MEASLES PNEUMONIA; STREPTOCOCCUS GROUP
Case 98, O. McN. Onset of measles, Sep. 19; admitted to hospital Sep. 21;
onset of bronchopneumonia, Oct. 21; of empyema, Oct. 23. Recovered from
pneumonia; convalescent in empyema ward.
Bacteriology.—1. Throat culture for: (a) S. hem.: Sep. 21, −; 28, −; Oct.
9, −; 20, −; 23, +; Nov. 2, −; 9, −; 15, −; (b) B. influenzæ: Sep. 21, +; 28, −;
Oct. 9, +. 2. Pleural fluid (culture) S. hem. Oct. 23, +.
Case 141, J. G. G. Autopsy No. 438. Onset of measles, Sep. 28; admitted
to hospital, Oct. 1; onset of bronchopneumonia, Oct. 6; of otitis media (bilateral),
Oct. 12; died, Oct. 18.
Bacteriology.—1. Throat culture for: (a) S. hem., Oct. 2, −; 6, −; 8, −;
(b) B. influenzæ, Oct. 2, −; 6, +; 8, +. 2. Autopsy cultures: Heart blood, negative;
left lung, Pneumococcus II atypical, B. influenzæ and S. viridans; right
lung, S. hem. and B. influenzæ; right bronchus, S. hem. and B. influenzæ.
Case 147, S. W. Autopsy No. 442. Onset of measles, Oct. 1; admitted to
hospital, Oct. 2; onset of bronchopneumonia, Oct. 17, with chill and rapid
development; died, Oct. 18.
Bacteriology.—1. Throat culture for: (a) S. hem., Oct 2, −; 9 −; 15, −;
18, +; (b) B. influenzæ, Oct. 2, −; 9, −; 15, −; 18, −. 2. Autopsy cultures:
Heart blood, S. hem.; right main bronchus, S. hem. and B. influenzæ.
Case 281, T. M. Onset of measles, Oct. 6; admitted to hospital Oct. 9; onset
of bronchopneumonia, Oct. 21; of empyema, Oct. 23; recovered from pneumonia;
convalescent in empyema ward.
Bacteriology.—1. Throat culture for: (a) S. hem., Oct. 10, −; 20, −; 24, +;
Nov. 2, +; 9, +; 15, +; (b) B. influenzæ, Oct. 10, −; 20, +. 2. Culture from
pleural fluid, Oct. 23, S. hem.
Case 285, J. H. Onset of measles, Oct. 4; admitted to hospital, Oct 9;
onset of lobar pneumonia, Oct. 29; of empyema, Nov. 9; convalescent in empyema
ward.
Bacteriology.—1. Throat cultures for: (a) S. hem., Oct. 11, −; 20, −; 24,
+; 29, −; Nov. 2, −; 9, −; (b) B. influenzæ, Oct. 11, −. 2. Cultures from pleural
fluid, Nov. 9 and 13, S. hem.
308Case 714, W. H. Onset of measles, Oct. 26; admitted to hospital, Oct. 28;
otitis media, Nov. 8; onset of bronchopneumonia, Nov. 9; of empyema, Nov.
17; convalescent in pneumonia ward.
Bacteriology.—1. Throat cultures for: S. hem., Oct. 28, −; Nov. 4, −; 12, +;
23, +; 30, +; Dec. 7, +; 12, −. 2. Sputum: Nov. 10, Pneumococcus II atypical,
S. hem. and B. influenzæ.
Case 730, W. S. Autopsy No. 491. Onset of measles, Oct. 26; admitted to
hospital, Oct. 29; onset of bronchopneumonia, Nov. 10; of empyema, Nov. 11;
of cervical adenitis, Nov. 5; died, Nov. 15.
Bacteriology.—1. Throat culture for: S. hem., Oct. 30, −; Nov. 4, +. 2.
Sputum: Nov. 10, S. hem. 3. Pleural fluid: Nov. 11, S. hem. Autopsy bacteriology:
Heart blood, S. hem.; right main bronchus, B. influenzæ, B. coli;
right lung, S. hem. and B. influenzæ; right pleura, S. hem.; peritoneum, S. hem.
Case 751, P. B. Autopsy No. 492. Entered hospital, Oct. 19; onset of
measles, Oct. 30; of bronchopneumonia, Nov. 5; of right empyema, Nov. 12;
died, Nov. 16.
Bacteriology.—1. Throat cultures for: S. hem., Nov. 1, −; 4, +; 15, +.
2. Sputum: Nov. 13, B. influenzæ and S. hem. 3. Autopsy cultures: Heart
blood, S. hem.; right lung, S. hem., Pneumococcus IV, B. influenzæ, B. coli;
pericardium, negative; right pleura, S. hem.; peritoneum, S. hem.
Case 880, B. McN. Autopsy No. 507. Onset of measles, Nov. 30; entered
hospital, Dec. 3; onset of bronchopneumonia, Dec. 11; of empyema, Dec. 14;
died, Dec. 14.
Bacteriology.—1. Throat cultures for: S. hem., Dec. 3, −; 5, −; 12, +.
2. Cultures from pleural fluid, Dec. 14, S. hem. 3. Autopsy cultures: Heart
blood, S. hem.; right main bronchus, S. hem., B. influenzæ, staphylococcus (a
few); left lung, S. hem.; left pleura, S. hem.
The average period in the hospital before the development
of the streptococcus pneumonia is about two weeks.
Cases 98 and 285 were in the hospital thirty and twenty
days respectively before the onset of pneumonia. There
is a record of from one to four negative throat cultures
on each case before streptococcus was found in the
throat. This enables us to fix the onset of the pneumonia
with reference to the appearance of the streptococcus in
the throat.
Case 141 stands alone as representing a class in which
S. hemolyticus was implanted upon a pneumococcus pneumonia
during its course. In this instance two throat cultures
on alternate days after the onset of the pneumonia
were negative for hemolytic streptococci. Unfortunately
309the last record of a throat culture is for one taken ten days
before the fatal termination of the case, and it can only
be stated that the S. hemolyticus infection was implanted
within the last ten days of the course of the pneumonia,
perhaps on or about October 12 when bilateral otitis media
developed.
In Cases 285 and 730 hemolytic streptococci were found
in the throats five and six days respectively before the onset
of pneumonia. They represent the 2 cases of pneumonia
which developed in patients isolated in the streptococcus
“carrier” ward. Case 285 is of particular interest for
several reasons. It is the only case of lobar pneumonia
in the group and happens also to be the only case from
which B. influenzæ was not obtained. S. hemolyticus was
found only once on throat culture, i.e., five days before the
onset of the pneumonia. Three throat cultures after the
onset of the pneumonia were negative. The case ran the
course of a lobar pneumonia. Eleven days after the onset
(November 9) a small amount of pleural fluid was diagnosed.
Aspirated fluid on this date and again four days
later showed many streptococci in smears and pure cultures
of S. hemolyticus.
The remaining 6 cases belong to a group in which hemolytic
streptococci were first identified in the throats after the
cases had been reported to the laboratory as pneumonia suspects
to be examined by culture before transfer from the
measles ward. In all these cases the culture taken at this
time was positive while all cultures taken before were negative.
In some cases, e. g., Cases 98, 147, and 281, throat
cultures taken only one or two days before the onset of the
pneumonia were negative. In these cases the onset of the
pneumonia and the appearance of the streptococcus in the
throats appear to be simultaneous.
It should be noted that the period between the appearance
of the hemolytic streptococci in the throat and the development
of the pneumonia is very short in all cases. In this
310small group of cases S. hemolyticus infection which has
complicated pneumonia has been acquired at or near the
time of onset of the pneumonia.
(b) Pneumonia with Hemolytic Streptococci in the
Throat without Symptoms Referable to the Streptococcus.—Thirteen
cases of pneumonia associated with measles developed
into S. hemolyticus “carriers” without having the
course of the disease affected by the presence of the organism
in the throat. Cases 705, 872, and 188 are of interest
in that hemolytic streptococci were identified in the throats
from one to six days prior to the onset of the pneumonia.
In spite of their presence, the symptoms, course and outcome
of the pneumonia were apparently unaffected. One
of these cases (Case 872) died. Autopsy showed lobar
pneumonia with no signs of invasion of the lung by hemolytic
streptococci. Cultures at autopsy showed that pneumonia
was due to a pneumococcus, Type II atypical. A
few hemolytic streptococci were found in culture from the
right main bronchus.
Of the remaining 10 cases 1 developed S. hemolyticus
in a throat culture at the end of the first week of the pneumonia;
3 during the second week; 1 during the third week,
and 5 further along in the convalescent period. In 8 cases
hemolytic streptococci appeared in the throat, at a time
when invasion of the lower respiratory tract by the streptococcus
might be expected, and yet none of them developed
evidence of streptococcus pneumonia. The 9 cases with
hemolytic streptococci appearing late in convalescence are
not of particular interest, since the dangers of lower respiratory
invasion are much reduced after the acute stage
of the pneumonia has passed. Three of these cases (Cases
678, 725 and 398) did however develop ear complications
directly referable to the streptococcus invasion of the
throat. Two of them terminated in mastoiditis with operation.
These cases emphasize the greater tendency of S.
hemolyticus to invade the middle ear rather than the lung.
311In 3 fatal cases of pneumococcus pneumonia in which during
life no hemolytic streptococci were found by throat culture,
a few hemolytic streptococci were found at autopsy
in culture from the main bronchi, along with predominating
growths of pneumococci and B. influenzæ. In 2 instances
there was frank lobar pneumonia and in the third bronchopneumonia;
there was no evidence to show that hemolytic
streptococci had any relation to the pneumonia which was
found.
MEASLES PNEUMONIAS; GROUP CARRYING HEMOLYTIC STREPTOCOCCI
Case 705. Onset of measles, Oct. 25; admitted to hospital, Oct. 27; onset
of bronchopneumonia, Nov. 10; acute pleurisy, Nov. 16; convalescent in pneumonia
ward.
Bacteriology.—1. Throat cultures for: S. hem., Oct. 27, −; Nov. 4, −; 11,
+; 15, +; 23, −; 30, −; Dec. 7, −; 12, −. 2. Sputum: Nov. 10, Pneumococcus II
atypical, S. hem. and B. influenzæ.
Case 872. Autopsy No. 508. Onset of measles, Nov. 29; admitted to hospital,
Nov. 30; onset of lobar pneumonia, Dec. 10; died, Dec. 14.
Bacteriology.—1. Throat cultures for: S. hem., Nov. 30, −; Dec. 5, +;
10, +; 12, +; 14, +. 2. Autopsy culture: Heart blood, Pneumococcus II atypical;
right main bronchus, Pneumococcus II atypical, B. influenzæ, S. hem. (a
few); left lung, Pneumococcus II atypical; left pleura, Pneumococcus II
atypical.
Case 188. Onset of measles, Oct. 3; admitted to hospital, Oct. 4; onset of
bronchopneumonia, Oct. 14; recovered and discharged from hospital, Nov. 24.
Bacteriology.—1. Throat cultures for: (a) S. hem., Oct. 5, −; 8, +; 12, +;
19, +; 20, +; 27, −; Nov. 2, −; 9, +; 15, −; (b) B. influenzæ, Oct. 5, −; 8, −;
12, +; 19, +.
Case 678. Onset of measles, Oct. 23; admitted to hospital, Oct. 25; onset
of bronchopneumonia, Nov. 2; of otitis media, Nov. 9; of mastoiditis, Nov.
13; mastoid operation, Nov. 20; still under treatment.
Bacteriology.—1. Throat cultures for: S. hem., Oct. 25, −; Nov. 4, −; 5, −;
12, +. 2. Sputum: Nov. 3, Pneumococcus Type IV, and B. influenzæ. 3. Culture
from mastoid bone at operation, Nov. 20, S. hem.
Case 389. Admitted to hospital, Oct. 2, with diagnosis of influenza; onset
of bronchopneumonia, Oct. 7; onset of measles, Oct. 13; phlebitis (right leg),
Oct. 22; otitis media, Oct. 31; recovered.
Bacteriology.—1. Throat cultures for: (a) S. hem., Oct. 16 −; 20, −; 27, +;
Nov. 2, +; 9, +; 15, −; 23, −; 30, −; Dec. 7, −; 12, −; (b) B. influenzæ, Oct.
16, −.
Case 725. Onset of measles, Oct. 18; one week in measles barracks; admitted
to hospital, Oct. 27; onset of lobar pneumonia, Oct. 23; otitis media,
Nov. 7; mastoid operation, Nov. 20; still under treatment.
312Bacteriology.—1. Throat cultures for: (a) S. hem., Oct. 29, −; Nov. 1, −;
5, −; 12, +; (b) B. influenzæ, Oct. 29, +. 2. Sputum: Nov. 2, Pneumococcus
II atypical. B. influenzæ. 3. Culture from mastoid at operation, Nov. 20,
S. hem.
(c) Pneumococcus Pneumonias not Carrying Hemolytic
Streptococci.—Thirty-four cases of pneumonia following
measles went through their entire course in the hospital
with no throat culture positive for hemolytic streptococci.
In some of these cases there are records of twelve negative
throat cultures. Eleven fatal cases occurred in this group.
Autopsy findings and bacteriology showed in each instance
that S. hemolyticus was not the cause of the pneumonia.
Measles During the Course of Pneumonia.—Eleven cases
of pneumonia which developed measles during the course
of the pneumonia came under observation. Hemolytic
streptococci appeared in the throats of 3 of these patients
during convalescence, but there was no evidence that it invaded
the lung. In one fatal case autopsy showed that
there was no streptococcus pneumonia; pneumonia followed
influenza and the onset of measles occurred three days after
the onset of bronchopneumonia.
Bacteriology of Pneumonia Following Measles.—When
observations made during life are combined with the results
of postmortem cultures, the bacteriology of 35 of the 56
cases is available and is as follows: Pneumococcus Type II
atypical in 36 per cent, Type IV in 22.9 per cent, Type I in
2.8 per cent, Type III in 2.8 per cent, hemolytic streptococci
in 22.4 per cent, and B. influenzæ in 88.6 per cent of these
cases.
Otitis Media and Mastoiditis Complicating Measles.—The
occurrence of otitis media and mastoiditis complicating
measles in patients harboring hemolytic streptococci in
their throats has already been presented (Table LXIV).
The bacteriology of these complications was not studied
by this commission. The records of the base hospital laboratory
at Camp Pike contain reports of twenty-nine cultures
made at operation from pus in the middle ear and
313the mastoid bone. Hemolytic streptococci were found in
22 of these cases. Throat cultures were in accord with
these positive findings in all except a few instances. The
throat culture serves as a fairly reliable index of the bacterial
nature of these complications. By combining our
records of throat cultures with the results of the cultures
from the lesions, hemolytic streptococci were obtained from
37 of the 48 cases of otitis media. In 23 cases of mastoiditis
following the otitis media, hemolytic streptococci were demonstrated
in all except 2. It is evident that the great majority
of these complications were due to hemolytic streptococci.
The relation between the appearance of hemolytic streptococci
in the throat and the onset of the otitis is recorded
in all except 4 of the 31 instances of otitis media occurring
in patients with throat cultures positive for hemolytic
streptococci. These four patients had positive throat cultures
when first observed and represent the only patients
who carried hemolytic streptococci when admitted to
measles wards and developed complications.
The first of these patients had been under treatment in
an otologic ward during a month before measles developed.
Measles caused a recurrence of disease of the ear with
double mastoiditis requiring bilateral operation. Two
other patients had been in the hospital ten and eleven days
respectively before they were admitted to the measles
ward; on admission to the ward otitis media was present
in one patient and in the other it developed six days later.
The fourth patient was admitted to the measles wards directly
from the camp, and culture from the throat on the
day of admission showed the presence of S. hemolyticus.
Two weeks later at the time of onset of otitis media, culture
from the throat contained no hemolytic streptococci. Repeated
cultures during the next three weeks were negative.
No complications of otitis media developed and no direct
cultures from the ear are recorded.
314
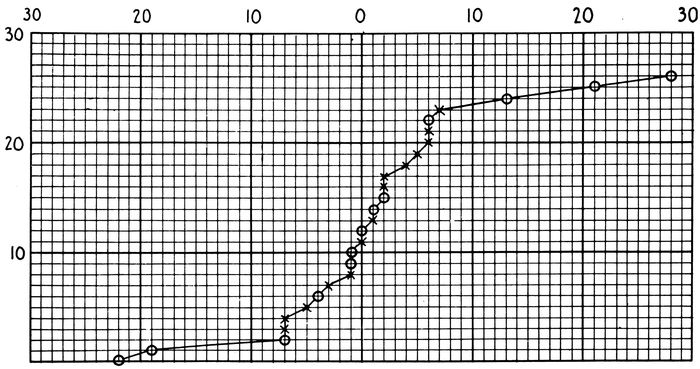
Chart 5.—Shows the time relation between the identification of hemolytic streptococci in the throats and the development of otitis media in 27 cases shown to be due to hemolytic streptococci. The onset of otitis media is represented by the ordinate marked ○. The number of days before or after the onset of the otitis, within which the throat culture which proved positive for hemolytic streptococci was taken, is marked off along abscissæ to the left and right of ordinate ○ respectively. On the curve plotted these symbols are used: A circle represents a throat culture positive for hemolytic streptococci in a case of otitis media without extension to mastoid. The plus sign represents a throat culture positive for hemolytic streptococci in a case of otitis media with mastoiditis and osteitis.
315In this series of cases (Chart 5) the appearance of S.
hemolyticus in the throat and the onset of otitis media are
very closely associated in those patients in whom further
extensions of the streptococcus infection occurred. In instances
in which appearance of streptococci and of otitis
media are separated by an interval of more than seven days,
no further extension occurred. In 8 cases in which this interval
is seven days or less there has been no further extension
of the infection.
The Dissemination of Hemolytic Streptococci in Wards
Beginning October 24 cultures for the identification of
carriers of hemolytic streptococci were made from all patients
in a ward and repeated at intervals of one week.
Prior to this time individual patients had been examined at
intervals of one week, so that an entire ward was never
studied on any particular day. This system did not identify
and remove all “carriers” in a ward at a given time
and was abandoned because it failed to show the conditions
present. Investigation of wards as units proved much
more satisfactory.
The studies made in four of the double wards used for
the care of patients with measles are presented in Table
LXV. During the time of this study hemolytic streptococci
were more prevalent than at an earlier period.
Cultures from the throats of all patients entering these
wards were negative for S. hemolyticus on admission. The
table showing the incidence of “carriers” of hemolytic
streptococci each week in these wards demonstrates:
1. The separation of “carriers” and “noncarriers” by
throat culture made on admission does not prevent the increase
of streptococcus “carriers” in wards.
2. Removal of all “carriers” found by cultures on admission
and at weekly intervals is inadequate.
| 316 |
| Table LXV |
|---|
| |
| Ward Conditions with Reference to Hemolytic Streptococcus Infection |
|---|
| |
| DATE OF CULTURE |
NO. PATIENTS CULTURED |
NO. POSITIVE HEM. STREP. |
PER CENT POSITIVE HEM. STREP. |
COMPLICATIONS ASSOCIATED WITH HEM. STREP. WITH DATES OF ONSET |
REMARKS |
| Ward 57 |
|
|
|
|
|
| 11–3 |
35 |
1 |
2.8 |
|
|
| 11–10 |
13 |
2 |
15.5 |
None |
|
| 11–17 |
16 |
6 |
37.5 |
|
|
| Ward 58 |
|
|
|
|
Wards 57 and 58 served by same ward staff. |
| 11–3 |
38 |
7 |
18.4 |
Otitis media: |
| 11–10 |
11 |
4 |
36.4 |
11–8 1 case |
Members of staff cultured on 11–5, 11–12 and 11–19. No positives |
| 11–17 |
6 |
2 |
33.0 |
11–7 1 case |
| Ward 49 |
|
|
|
|
|
| |
|
|
|
Otitis media: |
|
| 10–25 |
37 |
7 |
18.9 |
10–25 2 cases |
|
| 11–1 |
31 |
3 |
9.7 |
10–26 1 case |
|
| 11–8 |
35 |
9 |
25.7 |
10–28 1 case |
|
| 11–15 |
32 |
18 |
56.3 |
11–15 1 case |
|
| 11–22 |
16 |
7 |
43.8 |
11–18 1 case |
|
| |
|
|
|
11–27 1 case |
|
| Ward 50 |
|
|
|
|
Wards 49 and 50 served by same ward staff. |
| 10–25 |
29 |
2 |
3.4 |
Otitis media: |
| 11–1 |
43 |
2 |
4.6 |
11–8 1 case |
Ward staff cultured:
11–5 1 positive
11–12 1 positive
11–26 2 positives |
| 11–8 |
32 |
3 |
9.4 |
11–13 1 case |
| 11–15 |
20 |
11 |
55.0 |
11–22 1 case |
| 11–22 |
11 |
0 |
0.0 |
|
| Ward 41 |
|
|
|
|
Case of pneumonia developing on 11–9 was transferred to the “clean” pneumonia ward without a throat culture to warrant its transfer; last culture 11–4 negative; culture 11–12 in pneumonia ward positive |
| 10–28 |
45 |
4 |
8.9 |
Streptococcus pneumonia: |
| 11–4 |
34 |
9 |
26.5 |
(11–9 1 case) |
| 11–11 |
12 |
8 |
66.6 |
11–10 1 case |
| Ward closed—No patients. |
Otitis media: |
| 11–21 |
13 |
0 |
0.0 |
10–29 1 case |
| 11–28 |
8 |
4 |
50.0 |
11–4 1 case |
| 12–5 |
12 |
4 |
33.3 |
11–5 1 case |
| 12–12 |
4 |
3 |
75.0 |
11–11 1 case |
| |
|
|
|
11–27 1 case |
| |
|
|
|
12–3 1 case |
| Ward 42 |
|
|
|
|
Wards 41 and 42 served by same ward staff. |
| |
|
|
|
Streptococcus pneumonia: |
| 10–28 |
32 |
0 |
0 |
11–10 1 case |
| 11–4 |
43 |
7 |
16.3 |
12–11 1 case |
| Ward closed—No patients. |
Otitis media: |
Ward staff cultured:
11–5 2 positive
11–12 2 positive
11–26 2 positive
12–2 1 positive |
| 10–21 |
16 |
4 |
25.0 |
10–29 1 case |
| 11–28 |
12 |
1 |
12.5 |
12–3 1 case |
| 12–5 |
20 |
10 |
50.0 |
12–6 1 case |
| 12–12 |
14 |
7 |
50.0 |
|
| 317Ward 59 |
|
|
|
|
The 3 cases of streptococcus pneumonia acquired S. hemolyticus infection while patients in the 16 bed south section of this ward |
| |
|
|
|
Streptococcus pneumonia: |
| 10–24 |
37 |
6 |
16.2 |
10–17 1 case |
| 10–31 |
27 |
5 |
18.5 |
10–21 1 case |
| 11–7 |
9 |
3 |
33.3 |
10–29 1 case |
Case developing 10–29 was removed from section a few days before onset of pneumonia |
| 11–12 |
7 |
1 |
14.3 |
Otitis media: |
| |
|
|
|
11–1 1 case |
| Ward 60 |
|
|
|
|
Wards 59 and 60 served by same ward staff. |
| |
|
|
|
Streptococcus pneumonia: |
| 10–24 |
22 |
1 |
4.5 |
10–21 1 case |
Ward staff cultured:
11–5 0 positive
11–12 1 positive
11–19 0 positive |
| 10–31 |
17 |
2 |
11.7 |
Otitis media: |
| 11–7 |
8 |
1 |
12.5 |
10–31 1 case |
| 11–12 |
6 |
1 |
16.6 |
|
When the streptococcus complications are traced back to
the wards in which the streptococcus infection of the throat
was acquired, it is found that with the exception of Case
141 (already cited) all the streptococcus pneumonias arose
from two double wards. Wards 41 and 42 furnished 4
cases at times when streptococcus was rampant in them and
3 of these cases arose within a period of a few days.
Wards 59 and 60 furnished 4 cases, very closely associated.
In 3 cases the streptococcus infection was acquired in a
section of Ward 59 containing 16 beds. These patients
were in beds, of which the positions are represented by numbers
2, 5, and 7, along one side of the ward. The fourth
instance of pneumonia appeared at the same time in Ward
60, which was attended by the same ward personnel, but
no other connection can be established between this case
and the other three.
The otitis media appeared in patients scattered throughout
those wards for measles in which the weekly incidence
of “carriers” was rising rapidly. This relation is illustrated
by Wards 58, 50, and 41. The same observation applies
to streptococcus pneumonia arising in Wards 41 and
42. In Ward 41 the weekly percentage of carriers are
October 28, 8.9, November 4, 26.5 and November 11, 66.6.
318On November 9 and 10 the first 2 cases of streptococcus
pneumonia arising from this ward developed. At the same
time, November 10, a third case appeared in another part
of this same ward unit (Ward 42) where the spread of
hemolytic streptococci had been very active. These observations
suggest that hemolytic streptococci may build
up its virulence as the result of rapid dissemination to
such a degree that it is capable of causing grave complications.
The relation of complications to “carriers” in Wards
59 and 60 is different from that in the wards just cited.
Wards 59 and 60 were opened on October 9 and before October
17; when the first case of fulminating streptococcus
pneumonia occurred, only three “carriers” had been found
in them. From October 17 to 24 when the record in Table
LXV begins eight “carriers” were removed. The appearance
of a case of severe streptococcus pneumonia in an
unusually clean ward was followed by the rapid development
of “carriers,” and the appearance within twelve days
of 3 other cases of streptococcus pneumonia, 2 of which
were in beds close to the first case. This sequence suggests
focal dissemination of a streptococcus from a case in which
it had suddenly assumed high virulence.
An outbreak of infection with S. hemolyticus was recognized
on November 12 in a measles-pneumonia ward which
had been opened for several weeks and had continued free
from streptococcus. In three patients hemolytic streptococci
were found by throat cultures. Inquiry revealed that
a nurse in this ward, recognized as a streptococcus “carrier”
the week before, had been retained on duty. Two
patients well advanced in the course of their pneumonias,
had acquired S. hemolyticus demonstrated by throat examination.
Both patients developed otitis media with mastoid
extension requiring operations. Cultures from both
at operation showed hemolytic streptococci.
319The third patient, with acute pneumonia, had been sent
into the ward on November 11 from Ward 42, which at the
time was a highly infected ward; no culture of the throat
was made before transfer. This patient developed streptococcus
pneumonia with empyema requiring subsequent operation.
Discussion.—At Camp Funston, where the prevalence of
S. hemolyticus in the measles wards did not rise above that
among normal men in the camp at large, 112 consecutive
cases of measles were treated without a single complication
due to hemolytic streptococci.
At Camp Pike, the investigation began at the onset of
a small epidemic of measles at a time when hemolytic streptococci
were an almost negligible factor. The epidemic of
measles was followed throughout its course; and, with the
passing of the epidemic, there was an increase in the prevalence
of hemolytic streptococci which assumed alarming
importance in the production of complications.
The epidemic of measles was in part superimposed upon
the epidemic of influenza, so that deductions concerning
complications strictly due to measles became impossible.
It is evident that influenza played a considerable part in
producing the complications of measles at Camp Pike.
The dissemination of hemolytic streptococci through
measles wards was controlled only in part by the methods
used. This partial control may have served to limit the
incidence of streptococcus pneumonia, nine instances occurring
among 867 cases of measles.
In the ward treatment of measles effort should be directed
to prevent the exposure of patients free from hemolytic
streptococci to S. hemolyticus “carriers.” By this
means the rate of development of S. hemolyticus “carriers”
may be reduced.
Measures which should be adopted are as follows:
1. Adequate wards should be prepared in advance for
the treatment of measles. The rather gradual onset of
epidemics of measles makes this provision possible.
3202. The separation of S. hemolyticus “carriers” from
other patients should be enforced. Observation wards,
where strict technic to prevent transfer of infection is
practiced and where throat cultures are made on admission,
are essential. Those wards should be promptly evacuated
to wards for the care of S. hemolytic “carriers” on the one
hand and for “noncarriers” on the other. As far as possible
patients should be admitted to a ward until it is filled
and then another ward should receive consecutive cases in
the same manner. It is desirable to have all cases in each
treatment ward in the same stage of the disease. With
this system of ward rotation convalescent wards are necessary,
so that cases requiring a period of hospitalization
longer than the average may be segregated, thus rendering
treatment wards available for another levy of acute cases.
3. Strict ward technic elaborated to prevent transfer of
bacterial infection from one patient to another must be
employed.
4. Throat culture for identification of “carriers” is laborious
but essential. An accurate method for identifying
and reporting “carriers” as speedily as possible must be
employed. A competent bacteriologist is essential. A
twenty-four hour interval between culture and its report is
desirable. The following scheme is recommended:
(a) A culture from the throat made on admission to the
observation ward (first day in hospital).
(b) A culture made on the first day in the treatment
ward (third day in hospital).
(c) A culture made one week later (tenth day in hospital).
If the ward incidence of hemolytic streptococci reaches
10 per cent, especially in a filled ward, the cultures should
be repeated on the thirteenth day in the hospital. If the
incidence of “carriers” of hemolytic streptococci increase
rapidly, cultures on alternate days should be made so that
“carriers” may be removed from the ward. Wherever
321possible, culturing of the treatment wards as units should
be practiced.
5. Patients developing acute symptoms in any way suggestive
of infection with S. hemolyticus should be immediately
isolated; culture from the throat should be made at
once and final disposal of the patient should depend upon
its result.
Carriers of Hemolytic Streptococci
During the winter of 1917–18, with the establishment of
the army camps, it very soon became evident that in many
of the serious and fatal complications of measles and other
respiratory diseases, hemolytic streptococci were playing
a very important rôle. The epidemic prevalence of hemolytic
streptococci among hospital cases, and later among
men on duty in the camps, was established by bacteriologic
studies. Prior to this time in civil life, hemolytic streptococci
under epidemic conditions had been studied in milk-borne
epidemics of septic sore throat, such as are reported
from Chicago in 1911–13[92]; from Boston in 1911[93]; and from
Baltimore in 1911–12[94]. Contact air-borne infection has not
been emphasized in considering the dissemination of hemolytic
streptococci. Smillie[95] reports a few cases of hemolytic
streptococcus throat infections which he attributes
to contact infection. Conditions within the army camps
were such as to suggest the dissemination of hemolytic
streptococci by contact air-borne infection. Some knowledge
of the percentage of individuals showing positive
throat cultures became desirable at the very beginning of
studies of contact dissemination of hemolytic streptococci.
Smillie found that only one of 100 normal throats harbored
the Beta hemolytic streptococci of Smith and Brown.
Levy and Alexander[96] report the presence of hemolytic
322streptococci in 83.2 per cent of healthy men at Camp Taylor,
and hemolytic organisms (not definitely identified as
streptococci) in 14.8 per cent of recruits arriving at Camp
Taylor. Irons and Marine[97] found hemolytic streptococci
among 70 per cent of healthy men at Camp Custer.
Among measles patients on admission to the hospital at
Fort Sam Houston, Cole and MacCallum[98] report 11.4 per
cent and Cummings, Spruit and Lynch,[99] 35 per cent of
throat cultures positive for hemolytic streptococci. At
Camp Taylor, Levy and Alexander report 77.1 per cent
positive among 388 cases of measles on admission to the
hospital.
The spread of hemolytic streptococci in measles wards
was shown by Cole and MacCallum when on admission 11.4
per cent of cases had positive throat cultures, 38.6 per cent
after from three to five days, and 56.8 per cent after from
eight to sixteen days in the ward. In our study of hemolytic
streptococci with measles at Camp Funston, 2.6 per
cent of the cases had positive throat cultures on admission,
12.8 per cent after three to ten days, and 24.1 per cent after
eight to twenty-three days in the hospital. In a similar
study at Camp Pike we found 1.7 per cent positive on admission;
10.9 per cent after one week; 22.8 per cent after
two weeks; 26.2 per cent after three weeks; and, 33.1 per
cent after four weeks in the hospital.
Hemolytic Streptococci in the Throats of Normal Men.—The
percentage of normal individuals harboring hemolytic
streptococci in their throats was investigated in three distinct
classes of men, classified according to the degree of
exposure to contact infection.
The first group includes men largely from country districts,
cultured within an hour after being assembled by
their local draft board. The laboratory car “Lister” was
sent to Hot Springs, Ark. to meet the November draft of
323men to be sent to Camp Pike. These men were returned
to their homes when the armistice was signed, so that there
was no opportunity to study them after they had lived under
camp conditions.
The second group includes men on duty in Camps Funston
and Pike. These men, while largely from country districts,
had been living crowded together in the camp for a
period varying from a few weeks to several months.
The third group includes normal men resident in the
base hospitals at Ft. Riley and Camp Pike. This group
includes at Camp Pike the medical personnel of the measles
and measles pneumonia wards and represents individuals
most exposed to contact infection with hemolytic streptococci.
On the other hand, the group includes doctors,
nurses and seasoned medical detachment men who are perhaps
less susceptible to respiratory infections than are raw
recruits.
The results of studies of these groups are presented in
Tables LXVI and LXVII.
| Table LXVI |
|---|
| |
| Hemolytic Streptococci in Throats of Normal Men Not Resident in the Base Hospital |
|---|
| |
PLACE OF STUDY
DATE |
NO. OF CASES |
NO. POSITIVE FOR HEM. STREP. |
PER CENT POSITIVE FOR HEM. STREP. |
REMARKS |
Camp Funston, Kan.,
Aug., 1918. |
274 |
60 |
21.9 |
Men on duty in camp including 201 white and 73 colored; in great part newly drafted men |
Camp Pike, Ark.,
Nov. 5 to Dec. 10, 1918 |
337 |
25 |
7.4 |
Largely white men on duty in camp |
Hot Springs, Ark.,
Nov. 12, 1918 |
[100]64 |
0 |
0.0 |
Men from country districts, assembled by the local draft board |
| |
| Table LXVII |
|---|
| |
| Hemolytic Streptococci in Throats of Normal Men Resident in the Base Hospital |
|---|
| |
PLACE OF STUDY
DATE |
NO. OF CASES |
NO. POSITIVE FOR HEM. STREP. |
PER CENT POSITIVE FOR HEM. STREP. |
REMARKS |
Ft. Riley, Kan.,
Aug., 1918 |
24 |
7 |
29.2 |
14 convalescent patients in a surgical ward; 10 laboratory workers |
Camp Pike, Ark.,
Sept. 10 to Nov. 30, 1918. |
153 |
22 |
[101]7.5 |
Personnel of measles wards |
324The group of men studied at Hot Springs represents
individuals among whom there was little chance for contact
dissemination of hemolytic streptococci. It is a control
series of men from outlying districts examined before their
throat bacteriology has been complicated by the interchange
of mouth organisms which occurs when a group of
men are crowded into close quarters. The entire absence
of hemolytic streptococci by the throat culture method is
noteworthy. By multiplying the chances of identifying
hemolytic streptococci by making parallel cultures from
the saliva, and from the peritoneal exudates of mice inoculated
with saliva, hemolytic streptococci were found,
in small numbers, in 3 instances. The findings in this
group were only three throats lightly infected with hemolytic
streptococci. They are in direct contrast with the
findings among individuals living in camps under crowded
conditions and are in accord with the findings among recruits
arriving in camp as recorded by Levy and Alexander.
In the second group, men living for a time in camp, the
findings at Camp Funston and at Camp Pike show rather
325striking differences. The lower percentage incidence at
Camp Pike is the more remarkable since the studies were
made soon after the influenza epidemic had swept the camp
and made necessary the hospitalization of about 20 to 25
per cent of the camp population.
In the third group, namely, individuals resident in the
hospital, percentage rates at Camp Funston are slightly
higher than for men resident in camp. This difference
disappears for the entire group at Camp Pike if we consider
a single throat culture, as we must for the sake of
comparison. The majority of these individuals at Camp
Pike served in measles wards from which patients carrying
hemolytic streptococci were removed at weekly intervals.
Seven and one-half per cent of the ward personnel
were positives when first cultured. An additional 7.5 per
cent acquired the streptococcus while under observation.
Duration of the “Carrier” State.—Unfortunately there
are very few observations with regard to the duration of
the “carrier” state which can be determined only by repeated
cultures at short intervals. We have made no observations
of the duration of the “carrier” state in healthy
men. Two hundred and forty-two individuals carrying
hemolytic streptococci were identified in the ward treatment
of measles. All except 37 of these cases were “noncarriers”
when first observed. The remaining 205 include
166 contact “carriers” and 39 patients with acute symptoms
of infection by hemolytic streptococci.
The complete record of throat cultures on these cases is
presented in Table LXVIII.
Group I includes 37 cases positive for hemolytic streptococci
on admission.
(a) Twenty-two of these remained positive throughout
the period of observation. Four patients became negative
after one or two weeks and later showed positive findings,
leaving the hospital as positives. These are classified as
“irregular.” The results of culture were as follows: Cultured once only, 7; positive after one week, 7; positive after
two weeks, 6; positive after three weeks, 2; irregular, 4.
326
| Table LXVIII |
|---|
| |
| Results of Throat Cultures in 242 Hospital Patients Identified as “Carriers” of Hemolytic Streptococci; Cultures Taken at Weekly Intervals |
|---|
| |
| GROUP |
1st Culture |
2nd Culture |
3rd Culture |
4th Culture |
5th Culture |
6th Culture |
7th Culture |
8th Culture |
9th Culture |
10th Culture |
11th Culture |
12th Culture |
No. of Contact “Carriers.” |
No. with Acute Hem. Strep. Complications |
| I |
37 |
Cases |
|
|
|
|
|
|
|
|
|
|
|
| |
+ |
|
|
|
|
|
|
|
|
|
|
|
7 |
|
| |
+ |
+ |
|
|
|
|
|
|
|
|
|
|
7 |
|
| |
+ |
+ |
+ |
|
|
|
|
|
|
|
|
|
6 |
|
| |
+ |
+ |
+ |
+ |
|
|
|
|
|
|
|
|
2 |
|
| |
+ |
− |
|
|
|
|
|
|
|
|
|
|
8 |
|
| |
+ |
− |
− |
|
|
|
|
|
|
|
|
|
1 |
|
| |
+ |
− |
− |
− |
− |
|
|
|
|
|
|
|
1 |
|
| |
+ |
+ |
− |
|
|
|
|
|
|
|
|
|
1 |
|
| |
+ |
− |
+ |
|
|
|
|
|
|
|
|
|
2 |
|
| |
+ |
− |
− |
− |
− |
+ |
+ |
+ |
|
|
|
|
1 |
|
| |
+ |
+ |
− |
− |
+ |
+ |
+ |
|
|
|
|
|
1 |
|
| II |
67 |
Cases |
|
|
|
|
|
|
|
|
|
|
|
| |
− |
+ |
|
|
|
|
|
|
|
|
|
|
26 |
3 |
| |
− |
+ |
+ |
|
|
|
|
|
|
|
|
|
12 |
5 |
| |
− |
+ |
+ |
+ |
|
|
|
|
|
|
|
|
2 |
2 |
| |
− |
+ |
− |
|
|
|
|
|
|
|
|
|
9 |
1 |
| |
− |
+ |
− |
− |
|
|
|
|
|
|
|
|
0 |
1 |
| |
− |
+ |
+ |
− |
|
|
|
|
|
|
|
|
2 |
1 |
| |
− |
+ |
+ |
+ |
+ |
− |
− |
+ |
− |
|
|
|
1 |
|
| |
− |
+ |
− |
+ |
|
|
|
|
|
|
|
|
2 |
|
| III |
74 |
Cases |
|
|
|
|
|
|
|
|
|
|
|
| |
− |
− |
+ |
|
|
|
|
|
|
|
|
|
38 |
5 |
| |
− |
− |
+ |
+ |
|
|
|
|
|
|
|
|
5 |
3 |
| |
− |
− |
+ |
+ |
+ |
|
|
|
|
|
|
|
4 |
1 |
| |
− |
− |
+ |
+ |
+ |
+ |
|
|
|
|
|
|
0 |
2 |
| |
− |
− |
+ |
− |
− |
− |
|
|
|
|
|
|
0 |
1 |
| |
− |
− |
+ |
− |
|
|
|
|
|
|
|
|
4 |
|
| |
− |
− |
+ |
+ |
− |
− |
− |
− |
|
|
|
|
1 |
|
| |
− |
− |
+ |
+ |
− |
|
|
|
|
|
|
|
0 |
2 |
| |
− |
− |
+ |
+ |
− |
− |
− |
|
|
|
|
|
1 |
|
| |
− |
− |
+ |
+ |
+ |
+ |
− |
|
|
|
|
|
0 |
1 |
| |
− |
− |
+ |
− |
+ |
|
|
|
|
|
|
|
1 |
|
| |
− |
− |
+ |
− |
+ |
+ |
|
|
|
|
|
|
2 |
|
| |
− |
− |
+ |
− |
+ |
+ |
+ |
|
|
|
|
|
1 |
|
| |
− |
− |
+ |
− |
− |
+ |
+ |
|
|
|
|
|
1 |
|
| |
− |
− |
+ |
+ |
+ |
− |
− |
+ |
|
|
|
|
1 |
|
| 327IV |
34 |
Cases |
|
|
|
|
|
|
|
|
|
|
|
| |
− |
− |
− |
+ |
|
|
|
|
|
|
|
|
12 |
4 |
| |
− |
− |
− |
+ |
+ |
|
|
|
|
|
|
|
5 |
|
| |
− |
− |
− |
+ |
+ |
+ |
|
|
|
|
|
|
4 |
|
| |
− |
− |
− |
+ |
− |
|
|
|
|
|
|
|
3 |
1 |
| |
− |
− |
− |
+ |
− |
− |
|
|
|
|
|
|
1 |
|
| |
− |
− |
− |
+ |
+ |
− |
|
|
|
|
|
|
1 |
|
| |
− |
− |
− |
+ |
+ |
+ |
− |
|
|
|
|
|
1 |
|
| |
− |
− |
− |
+ |
− |
− |
+ |
+ |
|
|
|
|
1 |
|
| |
− |
− |
− |
+ |
+ |
− |
− |
− |
− |
− |
|
|
0 |
1 |
| V |
16 |
Cases |
|
|
|
|
|
|
|
|
|
|
|
| |
− |
− |
− |
− |
+ |
|
|
|
|
|
|
|
1 |
1 |
| |
− |
− |
− |
− |
+ |
+ |
|
|
|
|
|
|
1 |
1 |
| |
− |
− |
− |
− |
+ |
− |
|
|
|
|
|
|
3 |
1 |
| |
− |
− |
− |
− |
+ |
− |
− |
|
− |
|
|
|
0 |
2 |
| |
− |
− |
− |
− |
+ |
− |
− |
− |
− |
− |
|
|
1 |
|
| |
− |
− |
− |
− |
+ |
+ |
− |
|
|
|
|
|
1 |
|
| |
− |
− |
− |
− |
+ |
− |
+ |
|
|
|
|
|
2 |
|
| |
− |
− |
− |
− |
+ |
+ |
− |
|
+ |
|
|
|
1 |
|
| |
− |
− |
− |
− |
+ |
+ |
− |
− |
− |
+ |
|
|
1 |
|
| VI |
7 |
Cases |
|
|
|
|
|
|
|
|
|
|
|
| |
− |
− |
− |
− |
− |
+ |
|
|
|
|
|
|
1 |
|
| |
− |
− |
− |
− |
− |
+ |
+ |
|
|
|
|
|
2 |
|
| |
− |
− |
− |
− |
− |
+ |
− |
|
|
|
|
|
3 |
|
| |
− |
− |
− |
− |
− |
+ |
− |
− |
|
|
|
|
1 |
|
| VII |
4 |
Cases |
|
|
|
|
|
|
|
|
|
|
|
| |
− |
− |
− |
− |
− |
− |
+ |
|
|
|
|
|
2 |
|
| |
− |
− |
− |
− |
− |
− |
+ |
+ |
|
|
|
|
1 |
|
| |
− |
− |
− |
− |
− |
− |
+ |
− |
− |
− |
− |
− |
1 |
|
| VIII |
3 |
Cases |
|
|
|
|
|
|
|
|
|
|
|
| |
− |
− |
− |
− |
− |
− |
− |
+ |
|
|
|
|
2 |
|
| |
− |
− |
− |
− |
− |
− |
− |
+ |
+ |
+ |
|
|
1 |
|
328(b) Eleven of the patients entering as positives became
negative, 10 after one week and 1 after two weeks.
This group of cases furnishes no data concerning the
duration of the “carrier” state, since all cases were positive
when first observed. In 30 per cent of instances, hemolytic
streptococci disappeared within the first two weeks
of observation.
Groups II to VIII include 205 patients who became positive
at some time during their stay in the hospital. The
arrangement in groups depends upon the length of time
the patients remained in the hospital before acquiring S.
hemolyticus. Ninety-five of these patients had no further
cultures after the initial positive culture. Fourteen appear
as “irregular,” as defined above. These two classes of
cases are omitted in the following summary of these groups.
The initial positive culture is arbitrarily considered the
day of infection and subsequent cultures mark off weekly
intervals.
(a) Thirty-nine patients had acute infections due to
hemolytic streptococci. Thirteen of these patients passed
from observation after their initial positive culture. The
cases with repeated cultures after initial positive may be
summarized as in Table LXIX.
| Table LXIX |
|---|
| |
|
NO. PATIENTS CULTURED |
NO. BECOMING NEGATIVE |
PER CENT BECOMING NEGATIVE |
| Recultured after one week |
26 |
7 |
26.9 |
| Recultured after two weeks |
14 |
8 |
57.1 |
| Recultured after three weeks |
7 |
4 |
57.1 |
| Recultured after four weeks |
2 |
2 |
100.0 |
The records within this small group of cases indicate
that hemolytic streptococci tend to disappear with the passing
of the acute infection.
329(b) One hundred and sixty-six contact “carriers” are
included in Groups II to VIII. Eighty-two of these passed
from observation after their initial positive culture and
14 appear as “irregular.” The cases with repeated throat
cultures after the initial positive are summarized in Table
LXX.
| Table LXX |
|---|
| |
|
NO. PATIENTS CULTURED |
NO. BECOMING NEGATIVE |
PER CENT BECOMING NEGATIVE |
| Recultured after one week |
70 |
26 |
37.1 |
| Recultured after two weeks |
22 |
9 |
40.9 |
| Recultured after three weeks |
5 |
5 |
100.0 |
| Recultured after four weeks |
4 |
4 |
100.0 |
These records indicate that contact carriers in great part
harbor hemolytic streptococci during short intervals. A
longer period of observation after the disappearance of
hemolytic streptococci would have been desirable in many
instances. Some patients were followed with consistently
negative cultures during three, four and five weeks after
hemolytic streptococci had disappeared.
It is difficult to explain those instances in which negative
cultures are interposed between positives. Where one
negative interrupts positive cultures, it is possible that the
throat culture failed to demonstrate hemolytic streptococci
which were present. Such cases in this series fall within
the limits of the percentage error of throat culture identification.
Where two or three, or even four negative cultures
intervene, reinfection is not impossible.
Relation of S. Hemolyticus “Carriers” to the Complications
of Acute Respiratory Diseases.—In the present
study of measles it has been shown that pneumonia following
measles has been no more common in “carriers”
than in “noncarriers.” Nevertheless, pneumonia occurring
in badly infected wards has been modified by streptococcus
complications.
More cases of otitis media have appeared in “carriers”
than in “noncarriers.” The possibility that mild otitis
330media, which would ordinarily pass unnoticed, might become
evident as the result of streptococcus invasion must
be considered. Levy and Alexander have made an important
contribution to our knowledge of the rôle of hemolytic
streptococci in measles. They find that “carriers” of
hemolytic streptococci among measles patients are especially
predisposed to complications following measles.
Their cases were drawn from a camp population highly
saturated with S. hemolyticus “carriers.” In the organization
from which 89 per cent of their patients with
measles came, there were 83 per cent hemolyticus “carriers”
among men on duty. Among patients with measles,
throat cultures were positive for hemolytic streptococci on
admission in 77 per cent. It is evident that all patients
with measles have been exposed to hemolytic streptococci
during the first day or two after admission. Failure to
carry streptococcus would appear to be dependent upon
ability to resist it rather than upon lack of opportunity for
acquiring it. Of 388 cases observed by Levy and Alexander
only 79 were “noncarriers” of hemolytic streptococci on
admission, and of these, 27 became positive while under
observation; only 52 remain as “noncarriers” of hemolytic
streptococci. This small group must be regarded as a
highly selected one, composed of individuals more than ordinarily
resistant to hemolytic streptococci and perhaps to
all complications of measles. The chances are that these
52 cases placed under any circumstances might very well
have been among the large number of measles cases in
which no complications develop.
Furthermore, it is not unlikely that any complication of
measles may be modified by a streptococcus secondarily
when about 85 per cent of the cases show S. hemolyticus in
the throat. The complications in the cases of Alexander
and Levy appear to have been caused in large part by
streptococcus, but a complete bacteriologic study of them is
not recorded. Complications among streptococcus “carriers”
331are not identical with complications due to the
streptococcus, and it is desirable to know what percentage
of complications actually due to hemolytic streptococci occurred
among the 85 per cent of patients with measles who
carried hemolytic streptococci.
Summary.—No hemolytic streptococcus complications
occurred in 112 cases of measles observed at Ft. Riley,
among which streptococcus “carriers” rose from 2.6 per
cent on admission to 24.1 per cent before discharge from
the hospital. The percentage of “carriers” of hemolytic
streptococci among normal men in the camp supplying these
cases was about 25.5 per cent.
The influenza epidemic and a small epidemic of measles
occurred in part simultaneously at Camp Pike during September
and October, 1918. The complications following
measles at Camp Pike were to a considerable extent dependent
upon the combined effects of influenza and measles.
Thirty-five per cent of the measles patients showed throat
cultures positive for B. influenzæ on admission to the
hospital. On repeated cultures, this rose to 84 per cent before
discharge.
Ward separation of cases of measles carrying hemolytic
streptococci in their throats and cases not carrying these
organisms were practiced in handling this epidemic. Of
867 cases of measles treated in this manner, 37 were positive
for hemolytic streptococci on admission, and 205 developed
positive throat cultures for these organisms during
their period of observation in the hospital.
At Camp Pike, the percentage incidence of S. hemolyticus
“carriers,” on admission to the measles wards, was
4.2 per cent. In cases recultured after one week, it was
10.9 per cent; after two weeks 22.8 per cent; after three
weeks 26.2 per cent; and after four weeks 33.1 per cent.
The weekly development of “carriers” in the “clean”
treatment wards was during the first week 9.1 per cent;
during the second week 17.4 per cent; during the third
332week 17.4 per cent; and during the fourth week 17.4 per
cent.
The principal complications of these 867 cases of measles
at Camp Pike were: pneumonia, 56 cases; otitis media, 48
cases, with subsequent mastoiditis in 23 cases, 2 of which
had extensions to the meninges and brain. The greater
part of the pneumonia occurred early in the period of observation,
while most of the otitis media occurred later.
Incidence of hemolytic streptococci was low during the
pneumonia period and high during the prevalence of otitis
media.
Hemolytic streptococci complicated 9 of these pneumonias;
caused a large percentage of otitis (bacteriology incomplete),
and 21 of the 23 cases of mastoiditis.
The bacteriology of 35 of the 56 pneumonias showed:
Pneumococcus Type II atypical, in 36 per cent, Type IV in
22.9 per cent, Type I in 2.8 per cent and Type III in 2.8 per
cent; hemolytic streptococci in 22.4 per cent; and B. influenzæ
in 88.6 per cent.
The culturing of wards as units revealed widespread contact
dissemination of hemolytic streptococci, at times 25
to 50 per cent of the patients in a ward becoming “carriers”
within the period of a week. Streptococcus pneumonias,
otitis media and its complications were furnished
in large part by wards in which active dissemination
occurred.
Streptococcus complications did not occur among 37 patients
who were “carriers” of hemolytic streptococci when
admitted to the hospital.
The epidemic dissemination of hemolytic streptococci occurs
in measles wards, and is a serious danger. Many, patients
whose throats become infected, develop no symptoms.
In some instances streptococcus invades, and renders much
more serious lesions caused by other microorganisms.
Methods to prevent transfer of infection within the ward
and separation of “carriers” from “noncarriers” in different
333wards are efficient in keeping epidemic dissemination
of hemolytic streptococci under control. Frequent
throat cultures and prompt report of the results of cultures
are essential.
The dissemination of B. influenzæ in patients with measles
was not controlled by segregation of “carriers” and
“noncarriers” of this organism as identified by throat cultures
in separate wards.
334
CHAPTER VI
THE PATHOLOGY AND BACTERIOLOGY OF PNEUMONIA FOLLOWING MEASLES
Eugene L. Opie, M.D.; Francis G. Blake, M.D.; James C. Small, M.D.; and Thomas M. Rivers, M.D.
Among 18 autopsies upon men who have died with pneumonia
following measles there are pulmonary lesions representing
almost every type of pneumonia which has been
found in association with influenza. In most instances
pneumonia made its appearance during the second week of
measles and death occurred during the third week. Of 16
instances in which the record is definite, pneumonia had its
onset during the first week of measles in 4 instances, during
the second week in 11 instances, and in one instance (Autopsy
390) perhaps not referable to measles in the fifth
week. The duration of pneumonia varied from three to
thirty-two days; in 10 instances it did not exceed one week,
in 5 instances it was between one and two weeks and in one
instance, thirty-two days. When the duration of pneumonia
exceeded ten days some evidence of chronic pulmonary
disease was found at autopsy.
The same lack of correspondence between clinical diagnosis
and pulmonary lesions noted with influenza was found
following measles. In accordance with the prevailing
opinion concerning the character of pneumonia following
measles, the diagnosis of bronchopneumonia was made in
13 instances and in all of these cases bronchopneumonia was
found at autopsy. The diagnosis of lobar pneumonia was
made 5 times and was correct only once. Nevertheless,
lobar pneumonia was present 4 times, but was recognized
only once (Autopsy 486.) Failure to recognize lobar pneumonia, was doubtless due in part at least to its association
with purulent bronchitis and peribronchiolar pneumonia
(Table LXXI).
335
| Table LXXI |
|---|
| |
| NO. OF AUTOPSY |
RACE |
LENGTH OF MILITARY SERVICE |
DURATION OF ILLNESS |
DURATION OF PNEUMONIA |
CLINICAL DIAGNOSIS |
PURULENT BRONCHITIS |
LOBAR PNEUMONIA |
PERIBRONCHIOLAR CONSOLIDATION |
HEMORRHAGIC PERIBRONCHIOLAR CONSOL. |
LOBULAR CONSOLIDATION |
PERIBRONCHIAL CONSOLIDATION |
ABSCESS |
INTERSTITIAL SUPPURATIVE PNEUMONIA |
MULTIPLE ABSCESSES IN CLUSTERS |
EMPYEMA |
BRONCHIECTASIS |
UNRESOLVED BRONCHOPNEUMONIA |
ORGANIZING BRONCHITIS |
BACTERIA IN SPUTUM |
BACTERIA IN BRONCHUS |
BACTERIA IN LUNG |
BACTERIA IN BLOOD OF HEART |
| 390 |
W |
1m. |
35 |
6 |
L |
|
|
M |
|
+ |
|
|
|
|
|
|
|
|
No S. Hem. |
|
|
Pneum. II a |
| 438 |
W |
2m. |
22 |
12? |
B |
P |
|
+ |
|
+ |
|
+ |
|
|
E |
|
+ |
|
B. inf. |
S. hem., B. inf. |
Pneum. II, S. vir., |
0 |
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. inf., S. hem. |
|
| 439 |
W |
10d. |
14 |
11? |
B |
P |
|
M |
+ |
+ |
|
|
|
|
|
+ |
|
+ |
No S. hem. |
B. coli |
Pneum. IIa, S. aur. |
0 |
| 441 |
W |
1m. |
16 |
11 |
B |
P |
|
+ |
+ |
+ |
M |
|
|
|
|
+ |
|
|
|
B. inf., S. aur. |
B. inf., S. aur. |
0 |
| 442 |
W |
1m. |
17 |
2+ |
L |
P |
|
M |
|
+ |
|
N |
+ |
|
E |
|
|
|
No S. hem. |
B. inf., S. hem. |
|
S. hem. |
| 443 |
W |
21d. |
23 |
14 |
B |
P |
|
+ |
|
|
M |
|
|
|
|
+ |
+ |
|
No S. hem. |
B. inf., B. coli. |
B. coli. |
0 |
| 444 |
W |
1m. |
9 |
3 |
B |
P |
|
M |
+ |
+ |
|
|
|
|
|
|
|
|
B. inf. |
Pneum. IIa, B. inf. |
Pneum. IIa, B.inf. |
Pneum. II a. |
| 450 |
W |
29d. |
19 |
5 |
B |
|
+ |
M |
|
|
|
|
|
|
|
|
|
|
B.inf., No. S. hem. |
B. inf., Staph. |
B. inf. |
Pneum. IV. |
| 453 |
W |
36d. |
13 |
6 |
B |
P |
|
+ |
|
+ |
M |
|
|
|
|
+ |
|
|
|
Pneum. I, B. Inf. |
Pneum. I. |
Pneum. I. |
| 481 |
W |
54d. |
4+ |
3? |
B |
P |
|
+ |
|
+ |
|
|
|
|
|
+ |
+ |
|
No S. hem. |
B. inf., Pneum. IIa, S.hem. |
B. inf. |
0 |
| 484 |
W |
42d. |
20 |
7 |
B |
P |
|
+ |
|
+ |
M |
|
|
|
|
+ |
+ |
|
Pneum. IV, B. inf. |
B. inf., Diploids |
|
0 |
| 486 |
C |
6d. |
17 |
8 |
L |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
No S. hem. |
B. inf., Pneum. IIa, S. hem., Staph. |
B. inf. |
0 |
| 491 |
W |
2m. |
19 |
5 |
B |
|
|
|
+ |
|
|
|
+ |
|
E |
|
|
|
S. hem. |
B. inf., B. coli. |
S. hem., B. coli. |
S. hem. |
| 492 |
W |
49d. |
20? |
11? |
L |
P |
|
M |
+ |
+ |
M |
+ |
|
|
E |
+ |
+ |
|
S. hem., B. inf. |
|
S.hem., Pneum. IV, B. coli., B. inf. |
S. hem. |
| 496 |
W |
1m. |
43 |
32 |
L |
P |
|
+ |
|
+ |
|
|
|
|
|
+ |
+ |
+ |
B. inf., no S. hem. |
B. inf. |
0 |
0 |
| 505 |
C |
4m. |
16 |
6 |
B |
P |
+ |
|
|
|
|
|
|
|
|
|
|
|
No S. hem. |
Pneum. II a., S. hem. |
Pneum. II a. |
Pneum. II a. |
| 507 |
C |
5m. |
14 |
3 |
B |
|
|
|
|
|
|
N |
+ |
|
E |
|
|
|
S. hem. |
S. hem., B. inf., S. aur. |
S. hem., S. aur. |
S. hem. |
| 508 |
C |
2m. |
16 |
5 |
B |
|
+ |
M |
|
|
M |
|
|
|
|
|
|
|
S. hem. |
Pneum. IIa, B. inf., S. hem. |
Pneum. II a. |
Pneum. II a. |
336Changes in Bronchi.—The changes in the bronchi do not
differ in character from those associated with pneumonia
following influenza. Purulent bronchitis recognized at autopsy
by the presence of mucopurulent material in the
small bronchi was found in a much larger proportion of
instances in this group of autopsies occurring in 13 of 18
instances (72.2 per cent), whereas it was present in only
55.6 per cent of autopsies on individuals with pneumonia
following influenza. There was peribronchial hemorrhage
recognizable on gross examination in 3 autopsies and microscopically
in 3 additional instances.
Bronchiectasis was present in a considerable proportion
of these autopsies, dilatation of bronchi being noted in 7,
but it was usually moderately advanced and at times limited
to the bases of the lungs. The short duration of respiratory
disease perhaps explains the infrequency of advanced
bronchiectasis. The incidence of the lesion is greater with
measles (43.7 per cent) than with influenza (22.4 per cent).
Microscopic changes in the bronchi do not differ from
those found after influenza. Evidence of acute inflammation,
often hemorrhagic in character, is found within the
lumen of the bronchus and in the tissues immediately in
contact with the lumen. Not infrequently the epithelium
is lost; there is superficial necrosis and deposition of fibrin
upon the surface and within the tissue. In the deeper tissues
of the bronchial wall there is infiltration with lymphoid
and plasma cells, which in the larger bronchi is particularly
advanced about the mucous glands of which the acini exhibit
degenerative changes. With the onset of chronic
changes new formation of fibrous tissue occurs in the wall
of the bronchus and in the contiguous interalveolar walls.
The lining epithelium often loses its columnar cells and
assumes a squamous type.
337Changes in the bronchi with bronchiectasis have been
similar to those following influenza. Weakening of the
wall permitting dilatation is brought about by necrosis extending
outward from the lumen a varying distance into
the bronchial wall and permitting the formation tears which
diminish resistance to intrabronchial pressure.
Lobar Pneumonia.—Lobar pneumonia following measles
occurred in 4 instances. Onset in these cases was on approximately
the 9th, 10th, 11th, or 14th day of measles; the
onset of bronchopneumonia bore a similar time relation to
the onset of measles, the average interval being nine days.
Hepatization with lobar pneumonia was in 1 instance red, in
3 instances gray, and in all save 1 instance the consolidation
was firm and coarsely granular on section. In the exceptional
instance the greater part of the right upper lobe was
laxly consolidated and rather finely granular but the microscopic
appearance was in all instances that of lobar
pneumonia. Lobar pneumonia in 2 of these cases was associated
with purulent bronchitis present in parts of the
lung that had not undergone consolidation, whereas in the
other 2 instances there were acute bronchitis and peribronchiolar
pneumonia recognized by microscopic examination.
In one instance hepatization of the lung presented some
noteworthy features.
Autopsy 450.—G. D., white, aged twenty-one, a farmer, resident of Arkansas,
had been in military service twenty-nine days. Onset of illness began
on October 2, nineteen days before death, and on admission on the same day
the diagnosis of measles was made. Signs of pneumonia, regarded as bronchopneumonia,
were recognized five days before death. Three days later
there was otitis media and paracentesis was performed. On October 3 and 10
neither S. hemolyticus nor B. influenzæ was found in the sputum; on October
17 and 20 S. hemolyticus was not found but B. influenzæ was present.
Anatomic Diagnosis.—Acute lobar pneumonia with gray and red hepatization
in right upper and lower lobes; edema and peribronchial hemorrhage
in left lung.
338

Fig. 29.—Lobar pneumonia following measles, showing extension of gray hepatization from lower to upper lobe through a defect in the septum separating the two lobes. Autopsy 450.
339The entire lower lobe of the right lung (Fig. 29) with the exception of
a narrow air-containing zone in contact with basal surface is firmly consolidated.
The greater part of the consolidated tissue is yellowish gray,
firm and coarsely granular. The uppermost part of the consolidated tissue
is softer than elsewhere as if it has undergone autolysis. The lowermost
part of the consolidated tissue in a zone from 2.5 to 3.5 cm. in breadth is
firmly consolidated but deep red. The bronchi contain stiff plugs of fibrin.
In the upper lobe continuous with the consolidated part of the lower is a
semicircular patch of yellowish gray consolidation. It overlies the line of
the interlobular cleft at the site of a break in its continuity. Consolidation
appears to have spread from the lower lobe into the upper at the site where
the alveolar tissue of the two lobes is continuous but is absent from that
part of the upper lobe separated from the lower by the interlobular cleft.
This semicircular patch of yellowish gray consolidation is separated from
air containing tissue of the upper lobe by a zone of red hepatization about
1 cm. in thickness.
Bacteriologic examination showed the presence of Pneumococcus IV in
the blood of the heart; B. influenzæ alone was obtained from the right
lower lobe and B. influenzæ and staphylococcus from the left main bronchus.
The distribution of lobar pneumonia in the foregoing
autopsy indicates that it has spread like a wave from the
upper part of the lower lobe (Fig. 32) penetrating into the
upper where the alveolar tissue of the two lobes is in contact;
gray hepatization is everywhere separated from air
containing tissue by an advancing zone of red hepatization.
It may be assumed that lobar pneumonia was caused by
Pneumococcus II atypical in 3 instances although it was
recovered from the lungs only twice, for in the third instance
(Autopsy 486) it was found in the bronchus and in
the inflamed pleural cavity; pneumococci were doubtless
previously present in the lung, but had disappeared at least
from that part from which the culture was made. Pneumococcus
IV was evidently the cause of pneumonia in 1
instance (Autopsy 450), for it was found in the blood of
the heart although it was absent in the culture from the
lung.
Little significance can be attributed to the observation
that B. influenzæ was present in pure culture in the lungs
from Autopsies 450 and 486, for the presence of Pneumococci
IV in the blood of the heart in Autopsy 450 and of
340Pneumococcus II atypical in the pleura in Autopsy 486 furnishes
evidence in view of the occurrence of lobar pneumonia
that pneumococci had disappeared from the lungs.
B. influenzæ was found both in the lungs and bronchus or
in the bronchus alone in 3 of these 4 cases.
The relation of hemolytic streptococci to the lesion is of
interest. In 3 of 4 instances of lobar pneumonia this microorganism
had entered the bronchi but was not found in
the lungs or in the heart’s blood; and gross and histologic
examination showed none of the lesions which are usually
caused by it. In 1 instance (Autopsy 508) hemolytic streptococci,
absent from the throat when the patient was admitted
to the hospital with measles sixteen days before
death, appeared in a culture made five days later and was
subsequently found three times; it had penetrated into
the bronchus but failed to reach the lung. Observations
made upon lobar pneumonia following influenza have shown
the relative insusceptibility of lobar pneumonia with gray
hepatization to secondary infection with hemolytic streptococci
(p. 160). Autopsy 508 demonstrates that occurrence of
hemolytic streptococci in the sputum of a patient with pneumonia
does not furnish conclusive proof of the existence of
streptococcus pneumonia.
Bronchopneumonia.—Bronchopneumonia has been found
in every instance of pneumonia following measles save 3,
namely in Autopsy 486, Autopsy 505 with lobar pneumonia
and Autopsy 507 with interstitial suppurative pneumonia.
It is not improbable that further histologic study might
have demonstrated small patches of peribronchiolar pneumonia,
for purulent bronchitis was present in the two autopsies
with lobar pneumonia. This small group of cases has reproduced
all of the important features of bronchopneumonia
following influenza. Hemorrhagic peribronchiolar consolidation
characterized by the presence of small gray spots
clustered about terminal bronchi upon a homogeneously
red background has been found in 5 of 18 instances of pneumonia
341with measles. Pfeiffer regarded this lesion as characteristic
of the pneumonia of influenza. Peribronchiolar
patches of consolidation with no surrounding hemorrhage
were found in 14 instances, being recognized first by microscopic
examination in half of this number. Lobular
consolidation occurred in 11 autopsies and peribronchial
fibrinous pneumonia was present in a third of the autopsies
on patients with pneumonia of measles.
Bronchial, peribronchial and intraalveolar hemorrhage
is much more commonly associated with the pneumonias of
influenza than with the more familiar types of acute bronchopneumonia.
Exuded blood may undergo absorption;
and with bronchopneumonia which, persisting unresolved,
has assumed the characters of a chronic lesion, it is common
to find mononuclear cells often in great abundance
filled with brown pigment derived from the hemoglobin of
red blood corpuscles.
Autopsy 439 is an example of acute hemorrhagic bronchopneumonia;
there are red lobular and confluent lobular
patches of consolidation which upon the pleural surface
have a blue or purplish color. In the dependent part of
the left lung occupying a large part of the lower lobe there
is lax, red consolidation marked by gray or yellowish gray
spots of peribronchiolar pneumonia and in this lobe bronchi
are encircled by zones of hemorrhage. Pneumococcus II
atypical was obtained from the lung. In Autopsy 444 the
lesion has the same hemorrhagic character although lobular
patches are in a stage of grayish red hepatization.
Pneumococcus II atypical has been found in the heart’s
blood, and with B. influenzæ in lungs and bronchus. Autopsy
441 is an example of the occurrence of conspicuous
nodules of peribronchiolar consolidation in some parts of
the lungs with the same lesion in other parts on a background
of hemorrhage. B. influenzæ and S. aureus have
been found in both lungs and bronchi.
342Steinhaus[102] states that the pneumonia of measles is never
lobular inflammation but occurs in small patches several
of which may be found in a single lobule.
Chronic fibroid pneumonia following measles characterized
by cellular infiltration and proliferation of the interstitial
tissue of the lung has been described by Bartels,[103] Steinhaus,[104]
Hart,[105] MacCallum[104] and others.
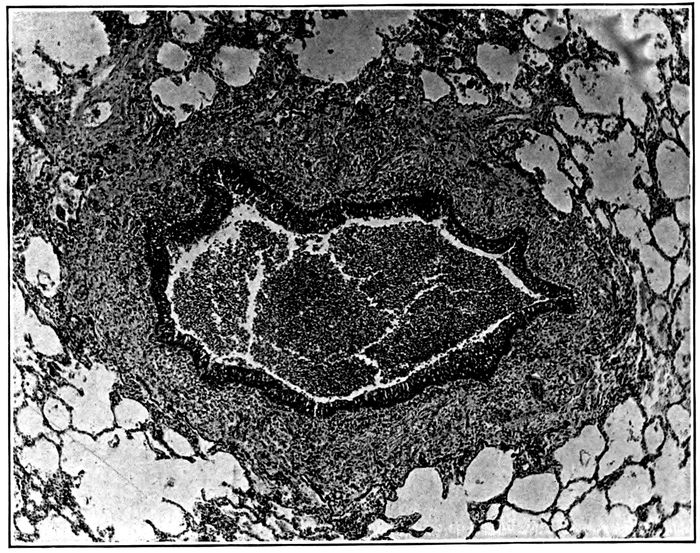
Fig. 30.—Unresolved bronchopneumonia with measles showing new formation of fibrous tissue about a bronchus and in immediately adjacent alveolar walls; partially obliterated alveoli occur in the peribronchial fibrous tissue. Autopsy 481.
343
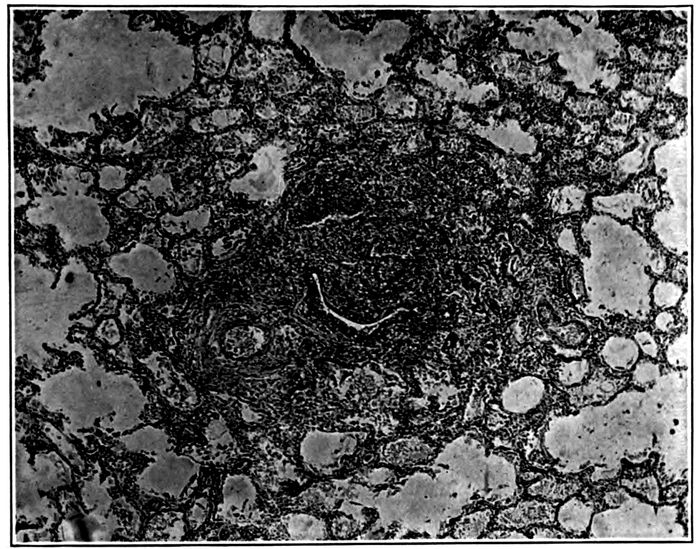
Fig. 31.—Unresolved bronchopneumonia with measles showing a nodule of chronic fibrous pneumonia surrounding a respiratory bronchiole. Autopsy 481.
The incidence of unresolved bronchopneumonia among
instances of bronchopneumonia following measles is higher
than that among bronchopneumonias following influenza.
There have been 6 instances of chronic or unresolved bronchopneumonia
among 18 pneumonias following measles,
namely 33.3 per cent. The incidence of unresolved bronchopneumonia
among 241 autopsies on pneumonia following influenza
has been 21, namely 8.7 per cent. The essential features
of this chronic lesion have been as follows: (a) chronic
peribronchiolar pneumonia indicated by the presence of
firm nodules of peribronchiolar consolidation which have
considerable resemblance to miliary tubercles. Induration of
the nodule occurs because the walls of alveoli surrounding
and adjacent to a respiratory bronchiole (Fig. 31) become
thickened and infiltrated with cells and there is organization
of exudate within the alveoli. New formation of
fibrous tissue (Fig. 32) occurs where the acute inflammatory
reaction of peribronchiolar consolidation is most advanced
(p. 169 and compare with Figs. 3 and 4), namely,
about the respiratory bronchiole, alveolar duct and the
344proximal parts of the infundibula, disappearing as the distal
half of the infundibulum is approached. Distention of
the alveoli explaining the distention of the lung and its failure
to collapse on section is a noteworthy feature of the
lesion. (b) Chronic peribronchial inflammation (Fig. 30)
with new formation of fibrous tissue about the smaller and
medium-sized bronchi extending into immediately adjacent
alveolar walls and often associated with organization of
peribronchial fibrinous pneumonia. (c) Chronic lobular
inflammation with changes similar to those just cited, distributed
throughout entire lobules. (d) Moderate thickening
of interlobular septa. Bronchiectasis may be associated
with the chronic lesion (Autopsies 443, 481, 484, 492
and 496) but with one exception (Autopsy 443) has been
only moderately advanced. Suppurative pneumonia with
abscess formation has occurred twice (Autopsies 438 and
492).

Fig. 32.—Unresolved bronchopneumonia with measles showing chronic pneumonia about a respiratory bronchiole and alveolar duct; alveoli about the proximal parts of three distended infundibula are filled with polynuclear leucocytes, whereas inflammatory changes disappear as the distal parts of the infundibula are approached. Autopsy 481.
345With acute bronchopneumonia following measles the average
duration of pneumonia, determined by the date upon
which physical signs of pneumonia were first recognized
and in consequence subject to some error, was seven days;
in instances of chronic bronchopneumonia the average
duration of pneumonia has been fifteen days.
The bacteriology of acute bronchopneumonia following
measles is shown in Table LXXII.
| Table LXXII |
|---|
| |
| WITH NO SUPPURATION |
SPUTUM IN LIFE |
BACTERIA IN BLOOD OF HEART |
BACTERIA IN LUNGS |
BACTERIA IN BRONCHI |
| Autopsy 390 |
|
Pneum. II atyp. |
|
|
| 439 |
|
0 |
Pneum. II atyp. S. aur. |
B. coli |
| 441 |
|
0 |
B. inf., S. aur. |
B. inf., S. aur. |
| 444 |
B. inf. |
Pneum. II atyp. |
Pneum. II atyp. B. inf. |
Pneum. II atyp. B. inf. |
| 453 |
|
Pneum. I |
Pneum. I |
Pneum. I, B. inf. |
| With suppuration: |
|
|
|
|
| 442 |
S. hem. |
S. hem. |
|
B. inf., S. hem. |
| 491 |
S. hem. |
S. hem. |
S. hem., B. coli |
B. inf., B. coli |
| 507 |
S. hem. |
S. hem. |
S. hem., S. aur. |
S. hem., B. inf., S. aur. |
It is noteworthy that pneumococci have been recovered
from the heart’s blood or lung in all but 1 (Autopsy 441) of
5 instances of acute bronchopneumonia with no suppuration
and is doubtless the cause of this pneumonia. Pneumococcus
II atypical has been found in 3 of 4 instances of lobar
pneumonia following measles and is present in 3 of these
5 instances of bronchopneumonia.
Where suppuration has been found, hemolytic streptococci
have been present in the sputum, in the heart’s blood
and either in the lungs (Autopsy 491) or in the bronchi (Autopsy
442) or in both (Autopsy 507). In these instances
pneumococci have not been found, though in view of the
readiness with which pneumococci disappear from the lungs
346it is possible that they have been the primary cause of
bronchopneumonia.
The bacteriology of 6 instances of unresolved bronchopneumonia
following measles is given in Table LXXIII.
| Table LXXIII |
|---|
| |
| WITH NO SUPPURATION |
SPUTUM IN LIFE |
BACTERIA IN BLOOD OF HEART |
BACTERIA IN LUNGS |
BACTERIA IN BRONCHUS |
| Autopsy 443 |
|
0 |
B. coli |
B. inf., B.coli |
| 481 |
|
0 |
B. inf. |
B. inf., Pneum. II, atyp., S. hem. |
| 484 |
Pneum. IV., B. inf. |
0 |
0 |
B. inf., diphtheroids |
| 496 |
Pneum. IV., B. inf. |
0 |
0 |
B. inf. |
| With Suppuration: |
|
|
|
|
| Autopsy 438 |
B. inf. |
0 |
Pneum. II atyp., S. vir. B. inf. S. hem. |
S. hem., B. inf. |
| 492 |
St. hem., B. inf. |
S. hem. |
S. hem., Pneum. IV, B. coli, B. inf. |
|
Whereas with acute bronchopneumonia death has been
accompanied and perhaps caused by bacterial invasion of
the blood by pneumococci or streptococci in 5 of 7 instances,
with unresolved or chronic bronchopneumonia, bacteriemia
has been present only once, namely, in Autopsy 492 in which
with suppurative pneumonia hemolytic streptococci have
entered the blood. It is probable that pneumococci have
likewise had an important part in the causation in these
instances of bronchopneumonia which have run a chronic
course but in all save 2 cases (Autopsies 438 and 492) have
disappeared from the lungs. Pneumococcus II atypical has
been found twice.
B. influenzæ has been found in association with acute
bronchopneumonia in the lungs in 1 of 6 examinations and
in the bronchi in 5 of 6 examinations. These figures indicate
that it is present in small numbers if at all in the consolidated
lung tissue but is relatively abundant in the bronchi.
With chronic bronchopneumonia B. influenzæ has been
347found in every instance, in half of the examinations of lungs
and in all of the examinations of bronchi. In 1 instance
(Autopsy 481) B. influenzæ has been found in pure culture
in the lung; Pneumococcus II atypical has been found in
the bronchus and has perhaps disappeared from the pneumonic
lung, since this microorganism is often destroyed
in the late stages of pneumonia so that its demonstration
at autopsy is no longer possible. In 1 instance B. influenzæ
found in the bronchus has been the only microorganism
isolated at autopsy, although the sputum during life contained
B. influenzæ and Pneumococcus IV.
Suppurative Pneumonia.—Suppurative pneumonia with
formation of abscesses has occurred in 2 autopsies with
pneumonia following measles (Autopsies 438 and 492), both
instances of chronic bronchopneumonia. In Autopsy 438
the lower and posterior part of the left lower lobe has been
consolidated and has had on section a cloudy, grayish red
color; within this area of consolidation and immediately below
the pleural surface there have been opaque, yellow
spots where the tissue has been softer than elsewhere. Microscopic
examination shows that the tissue has here undergone
widespread necrosis so that all nuclear stain has disappeared;
at the edges of the necrotic tissue polynuclear
leucocytes are often present in large numbers, but necrosis
is much more conspicuous than suppuration. In the necrotic
tissue and at its edges streptococci are present in vast numbers.
Hemolytic streptococci have been grown both from
the lung and from the bronchus, but these have not been
the only microorganisms present, for Pneumococcus II atypical
and S. viridans have been obtained from the lungs and
B. influenzæ from lungs and bronchus.
In Autopsy 492 with chronic bronchopneumonia the posterior
half of the right lower lobe is laxly consolidated, deep
red in color and with the cloudy appearance often associated
with streptococcus pneumonia; upon this background
are peribronchiolar spots of yellow color, in places well
348seen below the pleura; in the corresponding part of the left
lower lobe similar nodules have been converted into small
abscesses by central suppuration. There is empyema on
the right side, fibrinopurulent pericarditis, and purulent
peritonitis. Hemolytic streptococci had been found in the
sputum three times, the first examination being thirteen
days before death. This microorganism is found in pure
culture in the blood of the heart and with Pneumococci IV,
B. coli and B. influenzæ in the lung. Hemolytic streptococci
were found in the right pleural exudate and peritoneum.
The pneumonias following measles give opportunity to
consider the relationship of suppurative interstitial pneumonia
to unresolved or chronic bronchopneumonia, which
is characterized by infiltration and proliferation of the
fibrous tissue of the lungs. A number of those who have
studied the pneumonia of measles have recognized that this
chronic interstitial lesion is a common sequela of measles.
MacCallum has designated the lesion “interstitial bronchopneumonia,”
and has included under this name its acute
stage in which the interstitial character of the lesion is not
more evident than with other forms of acute bronchopneumonia.
He has regarded S. hemolyticus as the cause of
“interstitial bronchopneumonia” following measles. A
review of the autopsies which he has described shows that
he has included under the same designation typical instances
of interstitial suppurative pneumonia associated
with suppurative lymphangitis. Instances of unresolved,
chronic or “interstitial” bronchopneumonia and of interstitial
suppurative pneumonia which we have observed after
measles, demonstrate that the two lesions are distinguishable
both by their anatomic characters and by their etiology.
Three instances of suppurative interstitial pneumonia
occurred among the pneumonias following measles (Autopsies
442, 491 and 507). The lesion is characterized by
suppuration of the interlobular septa and particularly noteworthy
is the occurrence of suppurative lymphangitis,
349lymphatics being immensely dilated and distended with
purulent fluid so that their irregularly dilated, beaded appearance
is recognizable upon the section of the lung. In
the group of pneumonias following measles this lesion has
not been associated with unresolved or chronic bronchopneumonia;
no nodular tubercle-like foci of bronchopneumonia
have been found at autopsy, and there has been no
thickening of the interstitial tissue. The lesion has accompanied
confluent lobular pneumonia in 2 instances (Autopsies
442 and 491). In the third instance (Autopsy 507)
there was in the neighborhood of the suppurative lesions
diffuse consolidation which had the cloudy, gray red color
of streptococcus pneumonia, but this consolidation was not
lobular in distribution.
The etiology of interstitial suppurative pneumonia established
by study of instances following influenza is confirmed
by Table LXXII (p. 345) showing the bacteriology
of instances of acute bronchopneumonia following measles.
Pneumococci are almost invariably found in uncomplicated
instances of bronchopneumonia and hemolytic streptococci
have been absent, whereas in 3 instances of suppurative
interstitial pneumonia hemolytic streptococci have been
found in the sputum during life, in pure culture in the blood
of the heart and in the lungs and bronchus (missed in the
bronchus in one instance, Autopsy 507). In the 3 instances
of the disease B. influenzæ has been found in the bronchi.
Table LXXIII shows that suppuration has accompanied
unresolved bronchopneumonia (“interstitial bronchopneumonia”)
in 2 instances (Autopsies 438 and 492), but in
these instances the interlobular tissue of the lung has not
been the site of suppuration and there has been no suppurative
lymphangitis. Localized abscesses have been formed;
hemolytic streptococci, as with abscesses following influenza,
have been found.
Empyema has occurred only 5 times in association with
pneumonia following measles and in these 5 instances has
350been associated with suppurative pneumonia caused by
hemolytic streptococci. In Autopsy 492 there was fibrinopurulent
pleurisy on both sides. Aspiration had been performed
3 times and at autopsy the right pleural cavity contained
150 c.c. of purulent fluid. In small pockets, corresponding
to shallow oval depressions upon the anterior
surface of the lung, fluid was walled off from the general
cavity. The pericardial cavity contained 25 c.c. of turbid
yellow fluid containing yellow flakes of fibrin and the peritoneal
cavity contained thick purulent fluid. Hemolytic
streptococci present in the heart’s blood and lung were recovered
from the right pleural cavity and from the peritoneum.
Among 3 instances of empyema accompanying
interstitial suppurative pneumonia, in 1 (Autopsy 491)
there were walled off pockets of fluid similar to those just
described. Aspiration of the right pleural cavity had been
performed 3 times; at autopsy 100 c.c. of fibrinopurulent
fluid was found on the right side and 450 c.c. on the left.
There was general purulent peritonitis and the peritoneal
cavity contained 350 c.c. of thick yellow pus. Hemolytic
streptococci were obtained from the heart’s blood, right
lung, right pleural cavity and peritoneum.
Among 4 instances of lobar pneumonia following measles
there was serofibrinous pleurisy 3 times; in 1 instance there
is no record of pleural change. In 1 instance of lobar
pneumonia (Autopsy 505) the right pleural cavity contained
800 c.c. of serofibrinous exudate and the pericardial
cavity contained 510 c.c. of opaque, yellow seropurulent
fluid; Pneumococcus II atypical in pure culture was obtained
from the blood, lung and pleural and pericardial
exudates. Among 9 instances of bronchopneumonia following
measles there was fibrinous pleurisy 3 times, serofibrinous
3 times, and no recorded lesion of the pleura 3 times.
Empyema, like suppurative pneumonia following measles,
is in most instances, but not constantly, caused by invasion
of hemolytic streptococci.
351The foregoing study has shown that pneumonia which
has followed measles has reproduced all of the lesions
usually found after influenza. There is no pulmonary
lesion peculiar to measles. Lobar pneumonia follows the
disease in some instances, but bronchopneumonia with
purulent bronchitis is more common. The same tendency
to hemorrhagic inflammation found with the pneumonia of
influenza is seen after measles. Unresolved pneumonia
with chronic inflammatory changes in the interstitial tissue
of the lung has all of the characters of the similar lesion
following influenza but has been found in a larger proportion
of the pneumonias of measles.
B. influenzæ has been found in the bronchi in 14 of 16
examinations, namely in 87.5 per cent of fatal instances of
pneumonia. In 1 instance in which B. influenzæ has not
been found at autopsy, it has been isolated from the sputum
during life. It is not improbable that B. influenzæ has
been constantly present in the inflamed bronchi both after
influenza and measles. It is noteworthy that the outbreak
of pneumonia following measles has been in part coincident
with, in part slightly subsequent to, an epidemic of influenza
which has exposed every individual in the camp to infection
with this disease.
B. influenzæ has been found in the lung with the pneumonia
of measles in 7 of 17 examinations, namely, in 41.2 per
cent of instances. The microorganism with measles, as
with influenza, is found in the inflamed lung only half as
frequently as in the bronchi. It appears to be peculiarly
adapted for multiplication within the bronchial tubes, and
its isolation from the inflamed lung in less than half of the
cases of pneumonia is perhaps referable to its presence in
the small bronchi and bronchioles. The presence of B. influenzæ
in the lungs in pure culture in 3 instances at first
sight suggests that the microorganism produces pneumonia,
but a more intimate survey of these cases gives little
support to this view. In Autopsy 450 B. influenzæ has been
352found in pure culture in the lung, but Pneumococcus IV has
been isolated from the blood of the heart and has been with
little doubt the cause of typical lobar pneumonia present in
this instance. In Autopsy 486 the condition is almost identical,
for in the presence of lobar pneumonia B. influenzæ
has been found in the lung in pure culture, but Pneumococcus
II atypical has been isolated from the pleural cavity
and from the bronchus; in both autopsies the pneumococci
which have caused lobar pneumonia have disappeared from
that part of the consolidated lung from which a culture has
been made; and here doubtless its invasion has been effectively
resisted although it is still present in other organs. In
Autopsy 481 in which B. influenzæ has been isolated from
the lung in pure culture, the part of pneumococci in the
production of the fatal disease is less evident; in this instance,
Pneumococcus II atypical, S. hemolyticus and B. influenzæ
have been isolated from the bronchus.
The presence of microorganisms which have a well-established
etiologic relation to pneumonia explains the occurrence
of pneumonia and makes unnecessary the assumption
that B. influenzæ, which is present in the lungs in less than
half of the instances examined, is essential to the production
of the pneumonic consolidation. In view of the well-recognized
etiology of lobar pneumonia we may conclude that
this lesion is referable to the pneumococci (Pneumococcus
II atypical in 3 instances and Pneumococcus IV in 1 instance)
isolated from the autopsies in which this lesion occurred.
Pneumococcus (Pneumococcus II atypical in 3 instances
and Pneumococcus I in 1 instance) has been isolated
from the lungs or heart’s blood in 4 of 5 instances of acute
bronchopneumonia unaccompanied by suppuration. With
unresolved bronchopneumonia with no suppuration, pneumococci
have been in no instance found in the lungs or blood
though their presence in the washed sputum during life or
in the bronchus at autopsy suggests the possibility that
they may have disappeared from the lungs.
353In all instances in which suppuration has occurred
hemolytic streptococci have been found in the lungs or
blood, or in both. The occurrence of pneumococci in the
lungs in 2 of 5 instances of suppurative pneumonia indicates
that infection with S. hemolyticus is in some instances
at least superimposed upon acute bronchopneumonia caused
by pneumococci. Bronchopneumonia in 3 instances has the
character of that caused by pneumococci. It is probable
that the sequence of infection frequently observed after influenza,
namely, bronchial infection by B. influenzæ, followed
by pneumonia caused by pneumococci, followed in
turn by infection by hemolytic streptococci with necrosis
or suppuration, is not uncommon after measles.
Pneumonia Associated with Acute Infectious Diseases
Other than Influenza and Measles.—A small group of autopsies
have been excluded from the list of those which
accompanied the epidemic of influenza, because pneumonia
has been associated with an acute infectious disease to
which it is perhaps secondary. These few instances of
pneumonia, like those following measles reproduce characters
of the pneumonia following influenza and may be in
part referable to influenza which has attacked an individual
suffering with typhoid fever, mumps or scarlet fever.
In 2 instances pneumonia followed typhoid fever and appeared
on September 23 and 26 shortly after the epidemic
of influenza had become evident. In the following autopsy
there was acute lobar pneumonia which appeared ten days
after onset of typhoid fever.
Autopsy 245.—O. H., white, aged twenty-one, a farmer, resident of Oklahoma,
had been in military service twenty-one days. Onset of illness was
on September 13 with chill, headache, cough and nausea. The patient was
admitted two days later with the diagnosis of acute bronchitis. On September
20 the abdomen was tense, the spleen was enlarged and rose spots
were present. Signs of lobar pneumonia were found September 23. Death
occurred September 25, twelve days after onset of typhoid fever and two
days after recognition of pneumonia.
Anatomic Diagnosis.—Typhoid fever with necrotic ulcers in lower ileum
and in colon; hyperplasia of ileocecal lymphatic nodes; acute splenic tumor;
354parenchymatous degeneration of liver and kidneys; acute lobar pneumonia
with gray hepatization in left lower lobe and red hepatization and edema
in left upper lobe and in right lung; serofibrinous pleurisy on left side.
The left pleural cavity contains 75 c.c. of yellowish gray turbid fluid.
Over the left lower lobe there is a layer of fibrin. The upper half of the
lobe is firmly consolidated, pinkish gray and coarsely granular; the bronchi
contain plugs of fibrin. The lower and posterior part of the lower lobe is
consolidated deep red and edematous. The left upper lobe is edematous and
a layer in the lowermost part in contact with the lower lobe is deep red
and consolidated. The left lung weighs 1,490 grms. The lower half of the
right upper lobe and the posterior border of the lower is consolidated deep
red and edematous; the lung weighs 970 grms.
Bacteriologic examination shows that the blood of the heart contains
Pneumococcus II atypical.
The foregoing autopsy is of interest because typical lobar
pneumonia appears to have spread from the left lower lobe,
where consolidation is firm and gray, to the adjacent part
of the upper lobe where consolidation is red and edematous.
The second instance of pneumonia following typhoid
fever is an instance of suppurative pneumonia caused by
S. aureus.
Autopsy 329.—J. B., white, aged twenty-two, laborer, resident of Oklahoma,
had been in military service two days before onset of symptoms of
typhoid fever. He was admitted to the hospital on August 27 and B.
typhosus was found in cultures from the blood on September 2 and 3.
Acute bronchitis appeared on September 26 when the epidemic of influenza
had almost reached its height. A diagnosis of bronchopneumonia was
made on the day preceding death, which occurred forty-one days after
onset of typhoid fever and eleven days after onset of bronchitis.
Anatomic Diagnosis.—Typhoid ulcers of ileum; acute splenic tumor;
acute bronchopneumonia with red hemorrhagic peribronchiolar and lobular
consolidation in right lung; multiple abscesses forming a circumscribed group
in left upper lobe; purulent bronchitis.
The pleural cavities contain no excess of fluid. The lungs are voluminous
and there is interstitial emphysema. Below the pleura are bluish red spots
of lobular consolidation; in the right upper lobe is a large patch of red
consolidation marked by yellowish gray spots in clusters. In the external
and upper part of the left upper lobe is a patch of gray consolidation
within which, beneath the pleura, there are small abscesses grouped to form
a cluster 1.5 cm, across.
Bacteriologic examination demonstrates no microorganisms in the blood
of the heart; of two cultures from the left lung one contains S. aureus in
pure culture, the other S. aureus and a few colonies of Pneumococcus IV.
355Cultures from the left main bronchus and from the mucopurulent exudate
in a small bronchus both contain B. influenzæ, S. aureus and Pneumococcus IV.
In the foregoing case bronchitis has appeared thirty
days after onset of typhoid fever on September 26, immediately
preceding the height of the epidemic of influenza.
In association with hemorrhagic bronchopneumonia there
is suppurative pneumonia with small abscesses forming a
circumscribed group below the pleura; there is no empyema.
The lesion has the characters of the staphylococcus
abscesses following influenza, and S. aureus is found
in association with the lesion; B. influenzæ is identified in
two cultures from the bronchi.
In 2 instances pneumonia was associated with parotitis
which was diagnosed mumps.
Autopsy 403.—C. T., colored, aged twenty-five, a laborer, resident of Arkansas,
had been in military service one month. Illness began September
27 with swelling of face behind jaw and difficult mastication; the patient
was admitted to the hospital on the same day with the diagnosis of mumps.
Pneumonic consolidation was recognized on October 8. Death occurred October
13, sixteen days after onset of illness and six days after recognition of
pneumonia.
Anatomic Diagnosis.—Acute lobar pneumonia with red and beginning
gray hepatization of lower and parts of upper and middle right lobes; acute
bronchopneumonia with lobular consolidation in left lung; purulent bronchitis;
bronchiectasis in left lung.
The lower lobe of the right lung with the exception of the anterior and
basal edge is firmly consolidated; the posterior part of the middle lobe and
a small corner at the posterior and lower part of the upper lobe is similarly
consolidated. The consolidated tissue is gray and coarsely granular on
section. The remainder of the lung is dry and voluminous, and the bronchi
contain purulent fluid. The left lung contains red and gray patches of
consolidation, from 0.2 to 3 cm. across. Bronchi contain purulent fluid and
in the lowermost parts of both upper and lower lobes are moderately
dilated.
Bacteriologic examination shows that the blood of the heart contains
Pneumococcus III.
It is noteworthy that there was in this case, as in many
instances of influenza, both lobar and bronchopneumonia.
Purulent bronchitis was present and there was bronchiectasis
throughout one lung.
356In the following case the diagnosis of mumps may be
questioned since the lesion of the parotid has characters of
terminal suppurative parotitis.
Autopsy 417.—H.W.D., white, aged twenty-four, a farmer, resident of
Oklahoma, had been in military service one month. He said that he had
had pneumonia four times. He was admitted to the hospital delirious and
the diagnosis of lobar pneumonia was made. Parotitis regarded as mumps
appeared five days before death and suppuration occurred on the right
side of the face. Death of the patient occurred thirteen days after admission
to the hospital.
Anatomic Diagnosis.—Acute bronchopneumonia with lobular consolidation
in both lungs; suppurative pneumonia with necrosis and beginning abscess
formation in left lung; purulent pleurisy in left side; purulent bronchitis;
bronchiectasis; acute parotitis.
The left pleural cavity contains 100 c.c. of purulent fluid of creamy consistence.
The left lung is voluminous and bound to the chest wall in places.
There are numerous patches of lobular consolidation. At the apex of the
lung there is a large area of consolidation, 7 cm. across, where the tissue
is cloudy gray and soft in consistence. In the upper lobe is a well-defined
patch of grayish yellow color, 6 by 2 cm., with opaque yellow edges; purulent
fluid escapes from the cut surface. Bronchi throughout the lung are
widely dilated and contain purulent fluid. The right lung is voluminous
and contains lobular patches of consolidation; bronchi of this lung are widely
dilated.
Bacteriologic examination shows the presence of hemolytic streptococci
in the blood of the heart; hemolytic streptococci and B. influenzæ in the
lung, and hemolytic streptococci, B. influenzæ and S. aureus in a main
bronchus.
In association with bronchopneumonia there have been
necrosis and beginning abscess formation with empyema,
the suppurative lesions being caused by hemolytic streptococci
which had finally entered the blood stream. There
was purulent bronchitis, and the lungs had the voluminous
character often associated with this lesion; there was beginning
bronchiectasis. B. influenzæ was obtained both
from the lung and from the bronchus.
In 2 instances (Autopsies 323 and 335) the diagnosis of
scarlet fever was made in patients suffering with pneumonia
following influenza. These lesions have been included
in the list of influenzal pneumonias. In the following
instance the patient was admitted with scarlet fever,
357later developed acute follicular tonsillitis, and finally suppurative
pneumonia caused by hemolytic streptococcus.
Autopsy 311.—E. J., white, aged twenty-two, a tinsmith and automobile
repairer, resident of Arkansas, had been in military service three months.
Onset of illness was on September 18 with headache and sore throat. The
patient was admitted September 24 with the diagnosis of scarlet fever; two
days later there was acute follicular tonsillitis. Pneumonic consolidation
on the right side was recognized October 2, three days before death.
Anatomic Diagnosis.—Acute suppurative pneumonia with three small abscesses
below pleura of right lower lobe; acute fibrinopurulent pleurisy on
both sides; serous pericarditis.
The right pleural cavity contains 1500 c.c. of turbid, dirty yellow fluid
containing masses of fibrin; the left cavity has 500 c.c. of similar contents.
The pericardium contains 30 c.c. of turbid fluid containing a small quantity
of fibrin; there are ecchymoses below the epicardium. The right lung is collapsed
and in the lower lobe contains three small subpleural abscesses, the
largest of which is 1.5 cm. across.
Bacteriologic examination shows the presence of hemolytic streptococci in
pure culture in the blood of the heart and in the right lung. From the
right main bronchus are obtained hemolytic streptococci, B. influenzæ,
Pneumococcus IV and a few staphylococci.
In this instance there has been infection with streptococcus
which is a common sequela of scarlet fever. In the
absence of evidence of bronchopneumonia there has been
abscess formation below the pleura with empyema and
pericarditis. B. influenzæ has been found in the bronchus.
The pneumonias found in association with measles reproduce
the characters of the pneumonias described in association
with influenza. Particularly noteworthy is the
occurrence of lobar pneumonia, hemorrhagic peribronchiolar
pneumonia, interstitial suppurative pneumonia, severe
bronchitis with bronchiectasis and unresolved bronchopneumonia.
In the presence of an epidemic of influenza attacking
more than one fourth of the population of a camp,
those suffering with diseases, such as measles, typhoid
fever, mumps, etc., are unlikely to escape entirely, and it
is probable that the tendency to the occurrence of pneumonia
present in association with these diseases will be
increased. The close resemblance between the pneumonias
358which we have found with the diseases mentioned, on the
one hand, and the pneumonias of influenza on the other,
both being characterized by the occurrence of hemorrhagic,
suppurative and chronic pulmonary lesions, indicates that
influenza has had a part in the production of the pneumonia
found with measles and some other infectious diseases during
the progress of the epidemic of influenza.
359
CHAPTER VII
SUMMARY OF THE INVESTIGATION AND CONCLUSIONS REACHED
There is no reason for believing that the influenza which
prevailed in this country differed in any essential feature
from that of previous epidemics and particularly of the
pandemic of 1889–90. Our studies have shown that an organism
with the morphologic and cultural characters of B.
influenzæ of Pfeiffer has been constantly found in association
with the disease, and so frequently demonstrated in
association with its pulmonary complications that there is
little doubt of its constant presence. The bronchial and
pulmonary complications of influenza present characters
which, while varied, are not usually observed in the absence
of epidemic influenza, and in this pandemic agree with those
of the former pandemic so far as it is possible to determine
from the descriptions available.
Especially noteworthy is the severity of the changes
within the bronchial passages. Clinical studies have shown
that purulent bronchitis has occurred in 36 per cent of instances
of influenza. The sputum with this condition has
contained B. influenzæ in all instances, but although there
were no signs of pneumonia it has been constantly associated
with other microorganisms, namely, pneumococci (in
11 of 13 instances), S. hemolyticus, S. viridans, M. catarrhalis,
etc.
Identification of the bacteria which have been present
in the bronchi of those dead with pneumonia following influenza
have determined what microorganisms have penetrated
into the lower respiratory passages. B. influenzæ
360has been found so frequently (80 per cent) that there is
good reason to believe that it has been constantly present
and has not been isolated in every instance because it has
been overgrown by other microorganisms on the plates or
after long continued illness has disappeared from the bronchi.
Mixed infections of B. influenzæ and other microorganisms
are constantly found in the inflamed bronchi; combinations
of B. influenzæ and pneumococci, B. influenzæ and
hemolytic streptococci or these combinations with staphylococci
or the four organisms together are common. Other
microorganisms such as B. coli, S. viridans, M. catarrhalis
and diphtheroid bacilli are not infrequently associated with
those which have been mentioned.
Purulent bronchitis has been found in 137 of 241 autopsies;
its bacteriology differs in no respect from that which
has just been described and indeed no line can be drawn
between this condition and the bronchitis invariably present
with the pneumonias of influenza. Other evidence of
profound injury to the bronchi is the frequent occurrence
of hemorrhage in a zone ensheathing the smaller bronchi,
and the common occurrence of bronchiectasis when the
fatal disease has lasted more than two or three weeks.
Microscopic study demonstrates that the changes in the
bronchial walls are such as destroy the defences against
invasion by microorganisms. The bronchial epithelium
undergoes destruction which is not infrequently limited to
the superficial ciliated cells, but often complete loss of epithelium
occurs. The mucous glands of the larger bronchi
exhibit a special susceptibility to injury, and in the early
stages of the lesion profound degenerative changes are
found in the secreting cells, whereas at a later stage chronic
inflammatory changes are almost invariably present.
Pneumonia following influenza is in most instances bronchopneumonia,
but typical lobar pneumonia has been found
in autopsies representing 40.7 per cent of pneumonias of influenza.
Lobar pneumonia is frequently accompanied by
361purulent bronchitis, and in a considerable number of autopsies
(34 of 98 with lobar pneumonia) lobar and bronchopneumonia
have occurred in the same individual.
Statistics based upon the clinical diagnosis of lobar and
bronchopneumonia following influenza are so inaccurate
that they have little if any value. Notwithstanding careful
study of the symptomatology of the disease, lobar
and bronchopneumonia following influenza are not accurately
distinguishable by the means usually employed,
and an erroneous diagnosis has been recorded on the patient’s
history in 36.6 per cent of 227 fatal cases with autopsy.
A diagnosis of suppurative pneumonia is rarely if
ever made. The difficulties of diagnosis are in part explained
by the frequent association of lobar pneumonia
with purulent bronchitis, with bronchopneumonia or with
both, and by the occurrence of bronchopneumonia with confluent
lobular consolidation involving a large part of a lobe
or whole lobes.
There are many defects in the present knowledge of
the symptomatology of the pneumonias under consideration.
The symptoms of suppurative pneumonia are not
clearly defined. Many of these deficiencies might be supplied
by further application of the time-honored method of
comparing the clinical course of the disease with the
changes found at autopsies, supplemented by bacteriologic
studies made during life and confirmed after death.
With peribronchial pneumonia bronchi of medium size,
on the cut surface of the lung, are surrounded by sharply
defined zones of pneumonic consolidation perhaps 0.5 cm.
in radius, and this lesion furnishes conclusive proof that
the inflammatory process can extend directly through the
bronchial wall reaching all alveoli within a limited distance
for these alveoli bear no relation to the distribution
of the terminal bronchi of the affected bronchus. This
peribronchial pneumonia is usually characterized by fibrinous
exudate, and pneumococcus has been found either in
362the blood of the heart or in the lung in all of 6 instances in
which peribronchial consolidation has been recognized at
autopsy; in half of these autopsies Pneumococcus Type II
has been isolated and this relationship is especially noteworthy
because Type II has been uncommonly associated
with the pneumonias of influenza.
Lobar Pneumonia.—The distribution of lobar pneumonia
has repeatedly furnished evidence that the process spreads
like the peribronchial lesion directly through the tissue of
the lung and is not necessarily disseminated by way of the
bronchial tree. Pneumococci doubtless enter the lung by
way of the bronchi; the occurrence of lobar pneumonia in
frequent association with influenza which exhibits a peculiar
capacity to destroy the defences of the lower respiratory
passages is in harmony with this view. The presence
of pneumococci in the blood furnishes no evidence that
infection is hematogenous, for bacterial infections, particularly
at their onset, are frequently accompanied by bacteriemia.
The wave-like spread of lobar pneumonia may be
indicated by a narrow zone of red hepatization separating a
large patch of firm, gray consolidation from engorged but
air containing lung tissue. A semicircular patch of consolidation
not infrequently extends from the left lower lobe
into the upper lobe at the site where the interlobular cleft
is absent. This patch may be firm and gray in continuity
with similar consolidation in the lower lobe but surrounded
over its convex surface by a zone of red hepatization.
There is no reason to doubt that the lobar pneumonia
which we have found with influenza has been constantly
caused by pneumococci. We have encountered no instance
of lobar pneumonia caused by the capsulated bacillus of
Friedländer. The incidence of different types of pneumococci
in the lung with lobar pneumonia has been as follows:
Type IV, 32.4 per cent; Type II, atypical, 26.5 per cent;
Type III, 17.6 per cent; Type II, 5.9 per cent; Type I, 2.9
per cent; no pneumococci found 14.7 per cent. It is noteworthy
363that this distribution of types is in sharp contrast
with the lobar pneumonia of civil life with which Types I
and II constitute the cause of two-thirds of all instances,
and is in agreement with the etiology of the pneumonias
found in an army camp (Funston) in the absence of influenza
in epidemic proportion.
Bronchopneumonia.—Bronchopneumonia is associated
with intense bronchitis penetrating to the finest bronchioles
and is characterized by consolidation distributed in such
definite relation to the bronchial tree that dissemination
of the inflammatory irritant by way of the bronchi is evident.
Consolidation occurs (a) in foci affecting alveoli
in immediate proximity to the respiratory bronchioles and
in consequence clustered about the terminal bronchi, the
intervening alveolar tissue containing air; (b) in foci of
the same character surrounded by intraalveolar hemorrhage
which occupies all alveolar tissue between adjacent
foci; (c) throughout whole lobules or groups of lobules,
intervening lobules being unaffected; (d) surrounding bronchi
of medium size like a sheath.
The lobar pneumonia of influenza is characterized by
frequent association with purulent bronchitis and bronchopneumonia.
The bronchopneumonia of influenza exhibits
characters which serve to distinguish it from other forms
of bronchopneumonia; (a) The associated lesions of the
bronchi are unusually severe; purulent exudate accumulates
within the lumen and the lining membrane is destroyed.
(b) Pneumonia is frequently hemorrhagic with accumulation
of blood within the alveoli and within and surrounding
the bronchi. (c) There is unusual susceptibility of the injured
bronchi and of the pulmonary tissue to secondary invasion
by streptococci and staphylococci with consequent
necrosis and suppuration. (d) Bronchiectasis frequently
accompanies bronchitis. (e) Bronchopneumonia frequently
fails to resolve and the lesion assumes the character of a
chronic pneumonia.
364With bronchopneumonia pneumococci are found with B.
influenzæ in the bronchi and lungs in nearly half and in
the blood in approximately one-third of instances of the
disease, but hemolytic streptococci, staphylococci, S. viridans,
B. coli, M. catarrhalis and other microorganisms are
very frequently found in various combinations: they undoubtedly
have a part in the production of the lesion.
Mixed infection of the lung and even of the blood with pneumococci
and hemolytic streptococci is often found, and
study of the sputum during life has repeatedly shown that
pneumococci alone are present shortly after the onset of
the disease, whereas hemolytic streptococci appear later
or are first discovered at autopsy. In such instances pneumococci
have not infrequently disappeared from the lung
and at autopsy hemolytic streptococci alone are demonstrable.
The part which B. influenzæ has in the production of
bronchopneumonia is of great interest. This microorganism
is demonstrable by cultures in at least three-fourths
of all instances of bronchopneumonia but is obtained from
the inflamed lung tissue in less than half. In no instance
of pneumonia have we found B. influenzæ unassociated with
other microorganisms, whereas repeatedly pneumococci
have been the only microorganism demonstrable in the
lung and very frequently the only organism present in the
blood. In view of the difficulty of demonstrating the microorganism
in plates overgrown by other bacteria, it is
probable that its incidence in the bronchi is much higher,
if it is not constantly present, whereas its isolation from
the lung is in part referable to its presence in the small
bronchi where it can be readily demonstrated by cultures
or by microscopic preparations. We have been almost uniformly
unsuccessful in demonstrating the microorganism in
the alveoli of the lung. Goodpasture and Burnett,[106] who
365have devised a special method for the demonstration of B.
influenzæ in tissues, have found few of these microorganisms
in the alveoli of the lungs.
Pneumonia characterized by the occurrence of small
(peribronchiolar) spots of leucocytic pneumonia upon an
almost homogeneous background of intraalveolar hemorrhage,
was regarded by Pfeiffer as the characteristic lesion
produced by his microorganism. B. influenzæ in our autopsies
has borne the same relation to this lesion which it has
exhibited to other forms of bronchopneumonia; pneumococci
have been present with approximately the same frequency
and hemolytic streptococci have often been found.
Streptococcus Pneumonia.—The occurrence of streptococcus
pneumonia with suppuration occurring in the trail
of influenza was frequently observed during the pandemic
of 1889–90. It is now well recognized that the streptococcus
concerned is one capable of causing hemolysis. Suppurative
pneumonia referable to hemolytic streptococci is of
two types which are readily separable by their anatomic
characters: (a) One or several abscesses are situated below
the pleura and accompanied by empyema. Their relation to
severe lesions of the bronchi is not infrequently demonstrable,
for a destructive lesion of the bronchial wall has
penetrated into the surrounding alveolar tissue so that necrosis
of tissue and subsequent abscess formation occur in
continuity with the bronchial lumen. The localization of
the abscess below the pleura is referable to the greater
severity of the lesions of the small bronchi which are most
numerous at the periphery, to the greater severity of these
bronchial lesions at the bases of the lung, and to the relation
of lymphatics within the interior of the lung to those
of the pleura. It is not improbable that stasis of lymph
caused by thrombosis of the lymphatics has a part in the
production of abscess. Preceding or accompanying abscess
formation, the lung tissue undergoes consolidation and
in a wide area about the abscess has a homogeneous gray
366cloudy appearance occasionally mottled by opaque patches
of necrosis. (b) Interstitial suppurative pneumonia is a
lesion not infrequently found in association with influenza
(21 times among 241 autopsies) and rarely, if ever, seen in
its absence. There are few references to this lesion in the
pathologic literature of the English language and those of
German origin in great part refer to the period of the pandemic
of 1889–90. The lesion is essentially suppurative
lymphangitis, and both thrombosis and suppuration of the
lymphatics are widespread throughout the affected lung. In
proximity to the inflamed lymphatics and the surrounding
interstitial septa, lung tissue throughout parts of the lobes
or even throughout a whole (lower) lobe has undergone
consolidation and has the gray, cloudy appearance of streptococcus
pneumonia.
Staphylococcus Pneumonia.—Abscesses produced by
staphylococci differ in anatomic characters and sequelæ
from those caused by hemolytic streptococci. Small abscesses
occur in one or several localized clusters; these abscesses
are grouped about a bronchus and have their origin
in its terminal branches. This relation may be readily demonstrated
in microscopic sections. The lesion tends to remain
localized and pneumonic consolidation is limited to
the immediate neighborhood of the group of abscesses.
There is no lymphangitis and the lesion is not accompanied
by empyema.
Empyema.—Empyema is almost invariably associated
with suppurative pneumonia caused by hemolytic streptococci.
Among our autopsies purulent fluid has been
found in the pleural cavity 55 times; it occurred 15 times
among 178 instances of lobar or bronchopneumonia and 50
times among 60 instances of suppurative pneumonia referable
to S. hemolyticus. In our experience hemolytic
streptococci and pneumococci are the only microorganisms
which exhibit a noteworthy capacity to penetrate from the
lung to the pleural cavity. We have not found nonhemolytic
367streptococci (e. g., S. viridans) in association with empyema.
Staphylococcus has failed to invade the pleural cavity
even when a pulmonary abscess has been present below the
pleura, and in the only instances in which staphylococci
have been isolated from the pleural cavity thoracotomy had
been performed for empyema caused by hemolytic streptococci
(2 instances) or an abscess communicating with both
bronchus and pleura. B. influenzæ has been found in the
pleural cavity with empyema only once and in this instance
cannot be regarded as the cause of the lesion, for it has
accompanied hemolytic streptococci.
Bronchiectasis.—Bronchiectasis has been frequently
found as a sequela of the severe bronchitis of influenza and
there has been abundant opportunity to study the lesion
in process of development. These observations have furnished
a satisfactory explanation of its etiology and pathogenesis.
Infection of the bronchi by B. influenzæ, accompanied
by a variety of other microorganisms, notably hemolytic
streptococci and staphylococci, has caused profound
changes in the bronchial wall beginning with destruction
of the epithelial surface, and followed by necrosis penetrating
partially or completely through the wall and occasionally
extending into the surrounding alveolar tissue.
The difference between the atmospheric pressure within
the bronchi and the lower inspiratory pressure within the
surrounding alveoli, accentuated by forced inspiration at
intervals and by occlusion of the bronchioles with mucopurulent
exudate, ruptures the necrotic tissue and produces
longitudinal fissures which are recognizable both macroscopically
and microscopically. In consequence of the separation
of the edges of these fissures by intrabronchial pressure
the circumference is increased. These rents in the
wall are limited and partially healed by fibrinous pneumonia
about them, by new formation of fibrous tissue from
the bronchial wall, and adjacent interalveolar septa, by
368organization of fibrin within adjacent alveoli and finally by
growth of epithelium over the denuded surfaces.
Bronchitis caused by B. influenzæ and pyogenic micrococci
with necrosis of the bronchi wall is the essential factor
in the production of bronchiectasis, but advanced bronchiectasis
is found only in those individuals who have survived
the onset of illness during several weeks, for dilatation
under the influence of positive intrabronchial and
negative extra-bronchial pressure occurs slowly.
Unresolved Bronchopneumonia.—Unresolved lobar pneumonia
has not been recognized among instances of pneumonia
following influenza, but unresolved bronchopneumonia
is of frequent occurrence and has well definable gross
and microscopic characters. There are purulent bronchitis,
bronchiectasis and distention of the lung tissue, so that it
fails to collapse; particularly characteristic are the indurated
foci of peribronchiolar pneumonia, which being firm
and sharply defined, have the appearance of miliary tubercles.
When the process is sufficiently long continued
there are recognizable patches of fibroid pneumonia. Microscopic
examination shows that the lesion is characterized
by organization of fibrinous exudate not only within the
alveoli but within bronchioles as well, and by thickening
of the alveolar walls, thickening of fibrous tissue about
the bronchi and blood vessels, and thickening of interstitial
septa. These changes may occur as peribronchiolar patches
of consolidation, producing tubercle-like nodules, or may involve
areas of hemorrhagic peribronchiolar or of lobular
consolidation, or may be limited to the immediate neighborhood
of bronchi (peribronchial).
No peculiarity of the bacterial flora of the bronchi or of
the lung offers a satisfactory explanation of the failure of
pneumonic exudate to resolve. Mixed infections have been
common and S. hemolyticus, staphylococci, pneumococci,
S. viridans, B. coli, etc., have been found in association with
B. influenzæ but the incidence of these microorganisms has
369not been greater than with bronchitis. The lesion has occurred
in association with B. influenzæ and pneumococci
unassociated with other microorganisms. It seems probable
that the severity of injury to the bronchial and alveolar
walls accompanied by recurring bacterial invasion
or by continued infection with B. influenzæ and one or several
cocci, is the factor concerned in the inhibition of resolution
and the production of chronic pneumonia. If the
disease does not result in early death, chronic pneumonia
has an opportunity to manifest itself.
In this investigation of the bacteriology and pathology
of influenza and its complications, certain microorganisms
have been found so frequently that it is desirable to discuss
the pathogenicity of each and to define the character of
the lesions which it causes.
Bacillus Influenzæ.—The microorganism has been constantly
found in association with influenza when cultures
and animal inoculations have been made from various parts
of the respiratory tract within from one to five days after
the onset of the disease at a time when there have been
acute symptoms of the disease.
It is often identified with difficulty in the presence of
other microorganisms and may be overlooked when a single
culture is made. Repeated cultures from the throat alone
made from the fourth to the eighth day after admission to
the hospital, at a time when temperature had fallen to normal,
have demonstrated the presence of B. influenzæ in
30.5 per cent, whereas the incidence of the microorganism
in similar cultures on admission had been 63.4 per cent.
The incidence of B. influenzæ in the present epidemic of
influenza is not less than that found by Pfeiffer in the epidemic
which he studied in 1892.
Nevertheless we have found that B. influenzæ is frequently
an inhabitant of the mouth and throat of normal individuals.
By inoculation of mice with the saliva or
sputum of 76 patients with influenza, the microorganism
370has been found in 80.3 per cent; by inoculation of mice
with the saliva of 185 normal men at army cantonments, it
was found in 41.6 per cent; by inoculation of mice with
saliva from 50 recruits immediately after they were assembled
from isolated farming communities where only a
few cases of influenza had occurred, it was found in 22 per
cent. Figures for the same groups examined by a single
throat culture were as follows: 65.7 per cent, 25.9 per cent
and 0 per cent.
Experiments which we have performed on monkeys show
that inoculation of the nasopharynx with B. influenzæ obtained
from patients with influenza is followed by ill-defined
symptoms associated with the presence of B. influenzæ
within the throat. After from two to eleven days
the symptoms and the microorganism disappear. Injection
of B. influenzæ into the trachea causes bronchitis and the
microorganism may be recovered from the inflamed bronchi
two or three days after inoculation.
The constant association of B. influenzæ with influenza
suggests that it is the cause of the disease. Its widespread
occurrence in the throats of normal individuals does not
contradict this view, since pneumococci long indistinguishable
from those which usually cause lobar pneumonia are
commonly found in the throats of healthy men. It is possible
that B. influenzæ is a secondary invader, entering the
respiratory tract when susceptibility is increased by an unknown
virus causing influenza; but there is no convincing
evidence in favor of this view. It is desirable to determine
if microorganisms having the characters of B. influenzæ
found with influenza differ in type from those found in the
throats of healthy men and if the invasion of the respiratory
tract by B. influenzæ is followed by the appearance of immunity
reactions in the serum of the patient. Experiments
on monkeys demonstrate the pathogenicity of the microorganism.
371The relation of B. influenzæ to the bronchitis of influenza
indicates that it has a part in the production of the pulmonary
sequelæ of influenza. The microorganism has
been found by a single culture from the bronchial passages
in 80 per cent of instances of bronchitis with fatal pneumonia
following influenza and is probably constantly present,
usually in immense number, in the bronchial mucus.
It is obtained from the pneumonic lung in only about 40
per cent of instances, and microscopic examination of prepared
tissue shows that a bacillus with the morphology of
B. influenzæ is often demonstrable in the bronchial passages
but seldom in the alveoli of the lung. The microorganism
is well adapted to multiply under conditions present
in the bronchi but doubtless readily disappears from the
alveoli which are the site of an inflammatory reaction. The
microorganism has an important part in the production of
the associated mucopurulent and hemorrhagic inflammation
of the bronchi, but it is rarely if ever found in pure culture,
being associated with a considerable variety of pyogenic
cocci and occasionally bacilli. Infection of the bronchi
with B. influenzæ in immense numbers offers an explanation
of the severity of the inflammatory process within
the bronchi, and of the subsequent dilatation and other
chronic changes which occur in them. The presence of
the microorganism and the accompanying injury to the ciliated
epithelium and mucous glands are important factors
in lowering the resistance of the bronchial passages to
secondary bacterial infection.
We have obtained no evidence that B. influenzæ alone
is capable of causing pneumonia. Its occurrence in less
than half of all pneumonic lungs is explainable, in part at
least, by its presence in the terminal bronchi which are cut
across whenever the lung is punctured for culture. B. influenzæ
alone has been found only once among 153 pneumonic
lungs from which cultures were made, and in this
instance (Autopsy 487) S. hemolyticus present in the blood
372of the heart, pleural cavity and bronchus doubtless had a
part in the production of the associated pneumonia. Pfeiffer
maintained that the lesion we have designated hemorrhagic
peribronchiolar consolidation was characteristic of
infection with his microorganisms. With this lesion B.
influenzæ has been found in the lungs in slightly more than
half of our autopsies but never alone, pneumococci being
found in a third, hemolytic streptococci in more than a half
and staphylococci in a fourth of the lungs examined.
B. influenzæ has relatively little capacity to penetrate
from the bronchi into the lung tissue and rarely penetrates
into the pleural cavity (once with Pneumococcus III, once
with S. hemolyticus and once in pure culture), and only
once has it been found in the blood of the heart, in this
instance in company with S. hemolyticus. Capacity of the
microorganism to penetrate from the bronchi into other
tissues, both in man and as our experiments have shown
in the monkey, is increased by association with pyogenic
cocci.
Pneumococcus.—Lobar pneumonia following influenza,
like lobar pneumonia in civil life unassociated with influenza,
has been caused by pneumococci, but there is the
notable difference that the pneumococci usually found are
those types which are commonly present in the mouths of
healthy men, namely, Types IV, III and atypical II and
not the so-called fixed types, namely, Types I and II, which
represent the usual cause of lobar pneumonia unassociated
with influenza. It appears that influenza increases susceptibility
to lobar pneumonia, so that it is frequently caused
by microorganisms which under other conditions are less
capable of producing this lesion. The association of the
pneumococci usually found in the mouth with the lobar
pneumonia of influenza does not exclude the possibility that
pneumococci transmitted from one individual to another,
when newly recruited troops are brought together, have
an important part in the production of pneumonia.
373Bronchopneumonia is frequently caused by pneumococci
and the types which are recovered from the lung and blood
do not differ from those found with lobar pneumonia, those
usually present in the mouth being predominant, but the
incidence of pneumococci with bronchopneumonia has been
much less than with lobar pneumonia. Both lobar and
bronchopneumonia caused by pneumococci have undergone
secondary infection with hemolytic streptococci in a large
proportion of instances and both pneumococci and streptococci
are often recovered at autopsy. Nevertheless, the
bacterial flora of the bronchi and lungs is much more varied
with broncho than with lobar pneumonia, and it is evident
that microorganisms other than pneumococci are capable
of causing bronchopneumonia.
In instances of bronchopneumonia associated with pneumococci,
fibrin has been abundant in the alveolar exudate.
The pneumococcus exhibits a notable tendency to produce
an inflammatory process which extends through the
bronchial walls and from one alveolus through the alveolar
walls to those adjacent, for in 6 instances in which the
bronchi were surrounded by pneumonic consolidation recognizable
at autopsy, pneumococci were uniformly the
causative agent, Pneumococcus Type II, otherwise rarely
found, being present in half of these cases.
Pneumonia caused by one type of pneumococcus does
not necessarily confer immunity from other types of pneumococci,
and with somewhat limited opportunity we have
observed a number of instances in which, following recovery
from pneumonia caused by one type of pneumococcus,
a second attack of pneumonia, usually fatal, has been associated
with pneumococci of a different type. This recurring
pneumonia in a considerable proportion of the relatively
small number of instances observed has been produced
by Pneumococcus Type II which otherwise has been
seldom found among the cases which we have studied. The
374virulence of this microorganism doubtless explains its ability
to cause recurrent pneumonia.
Streptococcus Hemolyticus.—Secondary infection with S.
hemolyticus is a common event during the course of lobar
pneumonia following influenza. It is noteworthy that this
streptococcus infection of the lung has almost invariably
occurred in the stage of red hepatization, whereas with gray
hepatization, when the alveoli are filled with polynuclear
leucocytes, S. hemolyticus rarely invades the lung. It is
possible that infection with S. hemolyticus tends to prolong
the stage of red hepatization.
The most significant change produced in the pneumonic
lung by streptococci is necrosis. When after death with
lobar pneumonia hemolytic streptococci, usually associated
with pneumococci, are found both in the lungs and blood
of the heart, the lung contains patches of necrosis recognized
microscopically, in which the alveolar walls and exuded
cells have uniformly lost their nuclei. Microscopic
examination demonstrates the presence of chains of streptococci
in immense number in these necrotic foci; elsewhere
chains of streptococci occur but are much less abundant.
In some instances streptococci exhibit a tendency to enter
lymphatics and to cause acute lymphangitis with lymphatic
thrombosis and edema of the adjacent interstitial tissue.
Hemolytic streptococci have been more frequently found
in association with broncho- than with lobar pneumonia.
In 24.5 per cent of instances of lobar pneumonia, doubtless
in all instances caused by pneumococci, hemolytic streptococci
have invaded the lungs and in 12.6 per cent of instances
have found their way into the blood. With bronchopneumonia
hemolytic streptococci have been obtained
from the lungs in 29.8 per cent of instances and from the
blood of the heart in 34.3 per cent.
With lobar pneumonia there is little doubt that pneumococcus
has been the primary cause of pneumonia, but
with bronchopneumonia pneumococci have been less frequently
375found. It is difficult to determine how often hemolytic
streptococci have invaded a bronchopneumonic lesion,
caused by pneumococci because pneumococci tend to disappear.
In numerous instances in which the sputum had been
studied during life, it was evident that pneumonia was primarily
referable to pneumococci, and hemolytic streptococci
made their appearance in the sputum late in the disease or
were first recognized at autopsy.
When hemolytic streptococci occur in association with
bronchopneumonia, foci of pulmonary necrosis similar to
those found under the same conditions with lobar pneumonia
have been repeatedly found by microscopic examination.
In the patches of necrosis, cocci in chains are
much more abundant than in the tissue elsewhere.
In some instances of pneumonia, caused by hemolytic
streptococci, opaque gray or yellowish gray patches of
necrosis occur upon a background of flaccid homogeneous
consolidation which has a peculiar cloudy, gray color.
This mottled consolidation may implicate an entire lower
lobe and has the characteristic features neither of lobar
nor of bronchopneumonia. More frequently the lesion is
less widespread and necrosis occurs in one or several spots
which undergo softening so that finally a small abscess
cavity may be formed; it is surrounded by pneumonic consolidation
which is soft and has the cloudy appearance described
above. These pulmonary abscesses are almost invariably
situated below the pleural surface; the adjacent
pleural cavity is infected by streptococci and there is purulent
inflammation of the pleura.
Streptococcus infection, which has been described, doubtless
has its origin in the bronchi, for in favorable sections
it is not infrequently possible to demonstrate that necrosis
extends through the bronchial walls into the surrounding
alveolar tissue and is followed by suppuration with abscess
formation. Localization of abscesses below the pleura is
376in part at least referable to transmission of streptococci
by way of the lymphatics.
Streptococci in the lung, as in other tissues, often invade
lymphatics and produce an acute inflammatory reaction
within and about these vessels. The peculiar lesion which
may be designated suppurative interstitial pneumonia is
a suppurative lymphangitis associated with inflammation
and edema of the interstitial tissue. Lymphatics invaded
by streptococci are the site of acute lymphangitis; occlusion
by fibrinous thrombi occurs and finally the immensely distended
lymphatics, filled with purulent fluid, take a characteristic
nodular or beaded form and pus flows from them
when they are cut. Streptococci are present in vast numbers.
Suppurative inflammation may extend to the surrounding
interstitial tissue which is distended by inflammatory
edema. This interstitial suppurative pneumonia
extends up to the pleural surface and empyema is almost
invariably associated with it. The lesion is seldom seen
in the absence of influenza.
One of the most significant characters of S. hemolyticus
is its ability not only to enter the bronchi and penetrate
into the tissue of the lung, but to find its way into more
distant structures, namely, the pleural cavity, pericardial
sac and peritoneal cavity and to penetrate into the blood.
Among 121 examinations, hemolytic streptococci were
found in the bronchi in 47.9 per cent; among 153 examinations
of the lung it was present in approximately the same
proportion, namely, 50.3 per cent; among 218 examinations
of the blood it was found in 39 per cent. In 4 of 5
fatal pneumonias in which the organism has penetrated into
the bronchi it has ultimately found its way into the blood.
Nonhemolytic Streptococci.—In contrast with S. hemolyticus
nonhemolytic types have rarely been encountered
in association with the pneumonias of influenza. S. viridans
has been found only 5 times among 153 autopsies in
which cultures have been made from the lung and has been
377invariably associated with other microorganisms. In no
instances have nonhemolytic streptococci been found with
empyema. In one autopsy with lobular bronchopneumonia
S. viridans has been isolated from the blood of the heart
and in this instance it has been found in the bronchus and
lung as well. This type of streptococcus is evidently little
adapted to invade the bronchi and produce lesions of the
lung and adjacent tissues.
Staphylococci.—Staphylococci have been very frequently
isolated from the bronchi in association with the pneumonias
of influenza, being found in approximately half of
our autopsies. Their isolation in cultures from the lung
in a fourth of the autopsies examined is in part perhaps
referable to their presence in the small bronchi cut across
when the lung is punctured for cultures. S. aureus shows
little ability to invade the pleura, being found in association
with empyema only 3 times; in these autopsies there
has been opportunity for entrance from the exterior
through thoracotomy wounds in 2 instances and from a
bronchus in free communication with an abscess which had
ruptured into the pleural cavity in 1 instance.
Abscesses of the lung caused by staphylococci have been
found in a small number of autopsies and have exhibited
characters which differ from those ordinarily seen in association
with S. hemolyticus. Small, sharply defined abscesses
are grouped about terminal bronchi, so that they
occur in one or several isolated clusters. Microscopic examination
demonstrates that these abscesses have arisen
by destruction of the bronchial walls and extension of suppuration
into the surrounding alveolar tissue; clumps of
staphylococci are found in sections through the abscess,
and cultures made from the pus within the abscess cavity
demonstrate the presence of S. aureus or albus, but the
microorganism may be missed if the culture is made from
the adjacent lung tissue. It is noteworthy that there is
little tendency for the staphylococcus to infect the pleura
378for even though these clusters of abscesses have been situated
just below the pleura, there has been no associated empyema.
Staphylococci have scant tendency to enter the blood and
have been obtained from the blood of the heart only once, in
this instance with hemolytic streptococci.
Pneumonia of Measles.—Pneumonia following measles
has been responsible for a considerable part of the deaths
occurring in the United States Army during the period of
the war. The importance of measles as a factor in the
production of pneumonia is illustrated by the history of
pneumonia at Camp Funston from the establishment of
the camp in September, 1917, until September, 1918. Pneumonia
following measles occurred throughout the year;
but in association with the high incidence of measles during
the second half of November and the first half of December,
1917, there was an outbreak of related pneumonia
characterized by frequent empyema and a mortality of 45.3
per cent.
During the period of our investigation at Camp Funston
there were 112 cases of measles, but no pneumonia occurred
among them. At Camp Pike, during the period of observation,
there was an outbreak of measles almost coincident
with the epidemic of influenza, and among 867 cases pneumonia
occurred in 56, otitis media in 48, and mastoiditis in
23. Pneumonia following measles was almost coincident
with that of influenza, and it is not improbable that the epidemic
of influenza had an important part in the production
of pneumonia in individuals suffering with measles.
In 9 of 56 instances of pneumonia following measles at
Camp Pike, S. hemolyticus had invaded the lung and caused
pneumonia; among 48 instances of otitis media following
measles a very large proportion were caused by hemolytic
streptococci, and 21 of 23 instances of mastoiditis were
caused by the same microorganism. No complication
379caused by S. hemolyticus occurred among 37 patients who
carried this microorganism when admitted to the hospital.
A special study has been made to determine if those patients
with measles who carry S. hemolyticus in their
throats are especially susceptible to complications during
the course of measles. The low incidence of streptococcus
“carriers” among those admitted to the hospitals with
measles was noteworthy both at Camp Funston (2.67 per
cent) and at Camp Pike (4.2 per cent). Indeed, it was
found at both places that the incidence of hemolytic streptococci
in the throats of normal men in the camp was higher
(Camp Funston 21.9 per cent; Camp Pike 7.4 per cent)
than that in the throats of those admitted with measles.
While in the hospital there was a gradual increase of the
incidence of S. hemolyticus, so that in three weeks it had
risen to 19 per cent at Camp Funston and to 26.2 per cent
at Camp Pike. It seems not improbable that hemolytic
streptococci disappear from the throat in the early stages
of measles, so that they are not demonstrable by cultural
methods. During the course of the disease in the hospital
ward the number of those with S. hemolyticus has increased
in some wards with great rapidity, infection being apparently
transmitted from one individual to those adjacent.
At Camp Funston the incidence of S. hemolyticus in the
throats of those convalescent with measles was almost
identical with that among normal men in organizations from
which the patients had come, but at Camp Funston the
percentage of hemolytic “carriers” among convalescents
was much higher than that obtained among normal men
in the camp.
The demonstration of S. hemolyticus in the throat of a
patient suffering with pneumonia is not conclusive proof
that the lungs have been invaded by this microorganism.
Pneumonia in individuals carrying S. hemolyticus in the
throat may pursue a favorable course and exhibit no evidence
that the microorganism has found its way into the
380lung. In some instances hemolytic streptococci have been
found in the bronchi at autopsy yet none have entered the
lung or blood and the lung exhibits none of the lesions which
are referable to hemolytic streptococci. Nevertheless, the
occurrence of S. hemolyticus in cultures from the throat of
a patient with pneumonia suggests the probability that he
is suffering with streptococcus pneumonia.
Pneumonia following measles studied in 18 autopsies
upon patients who died during or shortly after the epidemic
of influenza, exhibited all the characters exhibited by
the pneumonias of influenza. In 4 instances there was typical
lobar pneumonia; bronchopneumonia was found in all
but 3 instances, being associated with lobar pneumonia
twice. All the noteworthy features of the bronchopneumonia
of influenza have been reproduced among these instances
of pneumonia with measles; there is severe injury
to the bronchi, and purulent bronchitis has been present in
13 instances; pneumonia has frequently had a hemorrhagic
character, hemorrhagic peribronchiolar pneumonia occurring
in 5 instances; secondary infection of the pneumonic
lungs with hemolytic streptococci has been common; bronchiectasis
has been associated with bronchitis (in 8 instances)
when purulent bronchitis has persisted several
weeks; and unresolved bronchopneumonia has been more
frequent (6 instances or one-third of the autopsies) than
with influenza.
The bacteriology of pneumonia following measles has
been the same as that of influenzal pneumonia. B. influenzæ
is found with few exceptions in the bronchi and much
less frequently in the pneumonic lungs.
Pneumococci have been obtained from the blood or lungs
in 5 of 13 instances of lobar or bronchopneumonia unaccompanied
by suppuration; when suppuration has been absent
no hemolytic streptococci have been found. Pneumococci
concerned in the production of pneumonia of measles,
as with influenzal pneumonia, have been types usually
381found in the mouth; Pneumococcus II atypical has been
found 6 times, Type IV once, Type I once.
Hemolytic streptococci have invaded the pneumonic lung
in 5 instances. They have produced subpleural abscesses
accompanied by empyema in 2 instances. Interstitial suppurative
pneumonia, a lesion repeatedly found in consequence
of secondary infection with S. hemolyticus following
influenza and rarely found in this country, at least
in the absence of an epidemic of influenza, has occurred
3 times among 18 instances of pneumonia following measles.
The foregoing observations show that the pneumonia following
measles, which has occurred almost coincidentally
with pneumonia accompanying epidemic influenza has reproduced
the lesions found with influenzal pneumonia.
They indicate that influenza attacking patients with measles
has had a part in the production of this pneumonia.
The Transmission of Streptococcus Pneumonia.—The importance
of streptococcus as a cause of pneumonia following
influenza was recognized during the pandemic of 1889–90.
Patients suffering with pneumonia following influenza
or measles are susceptible to infection by S. hemolyticus
and this streptococcus pneumonia may be transmitted from
one patient to another throughout a ward in which patients
with pneumonia are assembled. There is no evidence that
primary pneumonia caused by S. hemolyticus has prevailed
as an epidemic in the army or elsewhere in the absence of
preceding infection with influenza or measles.
Our autopsies demonstrate that at least half of all deaths
which have occurred at Camp Pike have been caused by
hemolytic streptococci which have invaded the lung and
entered the blood. It is significant that this mortality had
its origin in the first half of the epidemic of influenza at a
time when the military and medical organization of the
camp was confronted with an unforeseen emergency which
overwhelmed all agencies for the care of disease. Curves
prepared by referring cases of pneumonia in which autopsy
382demonstrated the nature of the fatal infection back
to the date of the onset of influenza, demonstrate that fatal
streptococcus pneumonia was frequently acquired during
the early period of the epidemic, the maximum number of
cases occurring September 23 and 24 and became gradually
less common as a sequela of the influenza which began
at a later period. Fatal pneumococcus pneumonia had
its origin with increasing frequency at a later period, the
maximum incidence following influenza which had its onset
September 29 and 30. Overcrowding of influenza patients
in infirmaries, ambulances and hospital had an important
part in the dissemination of streptococcus pneumonia
among influenza patients whose disease might otherwise
have pursued a benign course.
The most important factor in the high incidence of streptococcus
pneumonia has been the spread of the disease in
the hospital wards. On September 24 the base hospital
contained 2,789 patients, although it had been planned to
care for only 2,009. With the progress of the epidemic the
number of admissions increased very rapidly, so that on
September 30 the hospital contained 3,587 patients and on
October 5, 4,233. After September 24 the milder cases of
influenza were treated in barracks. The pressing need of
diminishing the overcrowding of the hospital was fully recognized
and adjacent barracks were transformed into hospital
wards; between October 3 and 6, 1,362 patients were
transferred from the hospital to these quarters.
In the main hospital, during the period of overcrowding
20 wards for patients with pneumonia were added to the two
which already existed. These hastily organized and overcrowded
wards have been attacked by outbreaks of streptococcus
pneumonia, which during certain periods have
been fatal to more than two-thirds of those who have been
admitted with pneumonia, whereas in the two long established
wards for pneumonia isolated cases of streptococcus
infection, which have appeared, have failed to spread to
383other patients and pneumococcus pneumonia with few exceptions
has been found in those who have died. In one
newly established ward 67.5 per cent of those admitted
within a period of three days have died, and in all of the
23 autopsies which have been performed, streptococcus
pneumonia has been found. In another ward 50 per cent
of all who have been admitted during a period of one week
have died, and among the autopsies performed on these
individuals pneumococcus pneumonia has been found in
6 and streptococcus pneumonia in 14. The sputum of 9
patients in this ward has been examined on admission, and
pneumococci, but no streptococci, have been found. All
these patients have died, and infection with S. hemolyticus
has been found at autopsy in 7.
Transmission of Pneumococcus Pneumonia.—Our study
of secondary ward infection has not only shown that patients
with pneumococcus pneumonia following influenza
are susceptible to infection by S. hemolyticus, but that
patients suffering with pneumonia caused by one type of
pneumococcus may be infected with another type during
the course of the disease or after convalescence has begun,
the second infection being acquired from patients in adjacent
beds. Pneumonia caused by Type IV has ended in
crisis and has been followed by a period of normal temperature;
recurrent pneumonia has been fatal and Pneumococcus
Type II has been found in the organs at autopsy.
Pneumonia caused by Type I has been followed by recurrent
pneumonia caused by Pneumococcus II atypical acquired
from a patient in the next bed. These secondary
pneumococcus infections acquired within the hospital are
apparently not uncommon.
Prevention of the Transmission of Pneumonia.—The essential
factor in the management of influenza and pneumonia
is such isolation of each patient that microorganisms
cannot be transmitted from one to another or from attendants
or others to patients. This condition may be fulfilled
384by the separation of patients in rooms or isolated compartments
especially constructed for the treatment of pneumonia
and by the employment of all possible means to prevent
the transmission of infection from one patient to another
by physicians, nurses and orderlies. It is desirable
to examine attendants to determine if they carry hemolytic
streptococci in their mouths and to exclude those who are
found to be “carriers.”
Influenza is a self-limited disease which, in the absence
of complications implicating the lower respiratory tract,
is of relatively mild character. When death occurs as the
result of influenza it is with very rare, if any, exceptions
referable to pneumonia; we have invariably found pneumonia
in those who have died in consequence of influenza.
The individual attacked by influenza may carry within his
upper respiratory passages pneumococci or hemolytic
streptococci capable of invading the bronchi and causing
pneumonia, but in most instances the microorganism which
produces serious pulmonary complications is derived from
others with whom the influenza patient has come into contact.
The greatest source of danger to one with influenza
is contact with patients who have acquired pneumonia, and
this danger is immensely increased when infection with S.
hemolyticus makes its appearance among pneumonic patients.
Hospital epidemics of streptococcus pneumonia
will be prevented when the disease is dreaded as much as
puerperal fever or the hospital gangrene of former years,
and widespread knowledge of the suppurative pneumonias
of influenza will bring a clear recognition of the fatal character
of streptococcus infection in patients suffering with
pneumococcus pneumonia.
Overcrowding of barracks has been an important factor
in the propagation of acute respiratory disease and
in the transformation of otherwise trivial influenza into
fatal pneumonia. Crowded troop trains have doubtless
had a part in disseminating infection among newly assembled
385recruits. Should these dangers be recognized they
may be avoided by appropriate measures which will promote
rather than retard those military aims which must be
placed foremost in time of war. It may be possible by adequate
expenditure to avoid the death of thousands of recruits
within one month of their entrance into military
service.
A second factor in the increase of death rate from pneumonia
is the overcrowding and confusion of hospital facilities
in the presence of an epidemic disease. When troops
are maintained in camps precautions should be taken to provide
effective safeguards against the overcrowding of the
base hospital.
Isolation of each patient with pneumonia is the most effective
way of protecting him from infection and of preventing
him from becoming a possible source of danger to
others. The effectiveness of this isolation will depend upon
the separation of patients by some means more effective
than the cubicles composed of sheets heretofore employed,
upon an aseptic technic sufficiently rigid to prevent the
transfer of pyogenic infection to pneumonia patients, and
upon the exclusion from the ward of those who harbor S.
hemolyticus.
Even should each patient be completely isolated from
his neighbors, no effort should be neglected to determine,
as far as possible, the nature of the infection with which
he suffers. In the presence of an overwhelming epidemic
such as that which attacked our army camps, the bacteriologic
work which is required may be far beyond the facilities
which are available and in many instances it may be
wholly impossible. Nevertheless effective control of streptococcus
pneumonia will depend upon its recognition as
soon as it appears, and bacteriologic examination of the
sputum offers the readiest means for its identification.
The routine performance of autopsies will furnish an index
of the success of the measures in force, and the discovery
386of suppurative pneumonia will suggest the presence of imminent
danger.
However perfect the organization of pneumonia wards
and however accurate the aseptic technic in force, it is
desirable to separate as far as possible those infected with
streptococcus from those who are free from this infection,
so that the accuracy of the technic in force may not be put
to too severe a test. When streptococcus pneumonia has
appeared in a ward it should be closed to further admissions.
Those who are concerned in the planning and construction
of military and other similar hospitals might well give
special attention to the possibility of epidemics such as
those which we have experienced, and special provision
might be made to avoid overcrowding in the presence of a
demand far in excess of the routine need for hospital facilities.
In the construction of these hospitals appropriate
provision should be made for the care of patients with
pneumonia. Medical officers should receive detailed instruction
in the organization and conduct of wards designed
for the treatment of pneumonia.
387
APPENDIX
EXPERIMENTAL INOCULATION OF MONKEYS WITH BACILLUS INFLUENZÆ AND MICROORGANISMS ISOLATED FROM THE PNEUMONIAS OF INFLUENZA
Eugene L. Opie, M.D.; Allen W. Freeman, M.D.; Francis G. Blake, M.D.; James C. Small, M.D.; and Thomas M. Rivers, M.D.
Experiments were undertaken at Camp Pike in December,
1918, to determine whether bacteria freshly isolated
from patients suffering with influenza and pneumonia during
the outbreak of influenza and its associated pneumonias
were capable of producing similar diseases when introduced
into the respiratory passages of monkeys. The
number of animals available for the study was limited.
The attempt was made (a) to determine if B. influenzæ
produces in monkeys a disease comparable to influenza of
human beings, and (b) to determine so far as possible,
with the limited opportunity, the character of the lesions
produced by combinations of pneumococcus or S. hemolyticus
with B. influenzæ and to compare these lesions with
lesions produced by pneumococcus or by hemolytic streptococcus
alone.
Pfeiffer[107] found monkeys alone susceptible to invasion
by B. influenzæ and obtained no evidence of multiplication
of the microorganism within the body of any other animal.
A suspension containing mucus from the sputum of a patient
with influenza was injected into a monkey. There was
elevation of temperature and the animal died after seven
days. Lobular patches of atelectasis occurred along the
sharp edges of the lungs and the adjacent bronchial
388branches contained mucus. Cultures on agar from the
bronchi remained sterile. Microscopic examination showed
the presence of bacilli resembling B. influenzæ. Death was
caused, the author states, by an abscess at the site of inoculation
and not by the process in the lungs. Three monkeys
received each 0.5 c.c. of bouillon containing a blood
agar culture injected into the lung through the chest wall.
There was elevation of temperature lasting from three to
five days with return to normal every morning. There
was cough but little evidence of illness. B. influenzæ was
introduced by a platinum loop into the nose of a monkey.
Febrile reaction is recorded lasting four or five days.
Pfeiffer found that guinea pigs and mice were resistant to
the microorganism. Large doses injected intravenously
caused in rabbits intoxication with dyspnea and evidence
of profound muscular weakness.
Kamen[108] used a culture of B. influenzæ which was nonpathogenic
for mice, but when it was inoculated into the peritoneal
cavity with streptococcus both influenza bacilli and
streptococci appeared in the blood. Jacobson[109] found that
B. influenzæ appeared in the blood and viscera of mice
killed by intraperitoneal inoculation of B. influenzæ mixed
with cultures of streptococcus either living or killed by
heat. B. influenzæ which had successively passed through
mice, simultaneously inoculated with killed streptococci,
acquired such virulence that it was capable of producing
septicemia when inoculated alone.
Richie[110] introduced by lumbar puncture a suspension of
two blood agar cultures of B. influenzæ obtained from the
meninges of a patient with influenzal meningitis into the
subdural space of a rhesus monkey. Death occurred in
eighteen hours and there was beginning meningitis. B. influenzæ
was present in the exudate in abundance.
389In two species of monkeys Wollstein[111] produced fatal
meningitis by injecting suspensions of B. influenzæ into the
subdural space by lumbar puncture.
During the course of our investigation of pneumonia and
influenza, sputum of approximately 400 normal individuals
or patients with influenza was injected into the peritoneal
cavity of mice. B. influenzæ was found in approximately
150 instances. In only 4 instances was B. influenzæ found
in pure culture in the blood; in all other mice in which B.
influenzæ appeared in the blood it accompanied pneumococcus
or S. hemolyticus.
Before experiments were performed cultures were made
from the throats of all monkeys in order to exclude the
presence of B. influenzæ. Blood agar plates inoculated with
a swab applied to the nasopharynx failed to show in any
instance B. influenzæ, pneumococci, or hemolytic streptococci.
Streptococci causing green discoloration of blood
agar were usually found.
Inoculation of the Nose and Pharynx with B. Influenzæ.—B.
influenzæ was introduced into the nose and pharynx of
two healthy monkeys. An actively growing culture of the
microorganism made on alkaline blood agar and sixteen
hours old was used. The culture was the first subculture
from a growth obtained from the nose and throat of a
patient with influenza. A cotton swab moistened with
broth was applied to the surface of the culture. It was
introduced into the nostrils and smeared over the pharynx
of the animals. A swab moistened with sterile broth was
applied to the nose and pharynx of a third monkey as a
control; cultures from this animal kept in a cage removed
from those inoculated failed to show B. influenzæ.
Experiment 1
November 21, 1918.—Small female monkey; throat culture: negative. November
23.—10:20 A.M.—White blood corpuscles, 16,700; polynuclear leucocytes,
68 per cent; small lymphocytes, 17.5 per cent; large lymphocytes, 8 per
390cent; large mononuclears, 1 per cent; eosinophiles, 2.5 per cent; basinophiles,
0.5 per cent. 10:30 A.M.—Mucous membranes of nose and throat were inoculated
with B. influenzæ as described above. November 25.—The animal appears
sick and is huddled in back of its cage; the nose is running. White blood
corpuscles, 13,500; polynuclear leucocytes, 44 per cent; small lymphocytes, 30
per cent; large lymphocytes, 22 per cent; large mononuclears, 3 per cent; eosinophiles,
1 per cent. 3:40 P.M.—Free epistaxis occurred after culturing of nose;
the swab was discolored with old brownish blood indicating previous epistaxis.
Nose culture: B. influenzæ present in abundance; Gram-positive cocci present.
Throat culture: negative for B. influenzæ. November 28.—Monkey is more
active and appears to be fairly well. Nose and throat cultures: negative for
B. influenzæ. December 4.—Monkey is apparently well.
Experiment 2
November 21, 1918.—Small male monkey. Throat culture: negative. November
23.—10:10 A.M.—White blood corpuscles, 10,900; polynuclear leucocytes,
52 per cent; small lymphocytes, 18 per cent; large lymphocytes, 25 per
cent; large mononuclears, 3 per cent; eosinophiles, 2 per cent. 10:15 A.M.—Mucous
membranes of nose and throat were inoculated by means of moist
swab with 4 strains of B. influenzæ recently isolated from acute cases of influenza.
November 24.—Monkey is quiet and takes no interest in surroundings.
November 25.—Animal appears sick and remains huddled at back of its cage.
Nose culture: B. influenzæ present. Throat culture: B. influenzæ present.
Swab applied to nose is stained brown with old blood indicating previous
epistaxis. November 26.—Animal is still sick; nose is running. White blood
corpuscles, 14,400; polynuclear leucocytes, 61 per cent; small lymphocytes, 23
per cent; large lymphocytes, 15 per cent; large mononuclears, 1 per cent. November
27.—White blood corpuscles, 11,300. November 28.—Nose culture:
negative for B. influenzæ. Throat culture: B. influenzæ present. November
29.—Animal is active, but still appears sick. White blood corpuscles, 19,300.
December 4.—Monkey appears well. Throat culture: B. influenzæ present.
These animals were sick two and six days following inoculation.
There was discharge from the nose. In both instances
there was epistaxis. The temperature of the animals
was subject to such wide variation in relation to external
temperature that it could not be used as an index of
the progress of the disease. There was no leucocytosis, but
in one animal there was some increase in the numbers of
leucocytes during recovery. In one animal B. influenzæ
present in the nose after two days was absent after four
days. In the other animal the organism was repeatedly
found in the nose and throat and was still present in the
throat eleven days after inoculation. The two animals suffered
391with a self-limited disease resembling many cases of
influenza.
Introduction of Bacillus Influenzæ into the Trachea.—In
the attempt to reproduce the bronchitis which occurs in a
considerable proportion of all cases of influenza and is almost
invariably associated with B. influenzæ, this organism
was introduced into the trachea of monkeys. In Experiment
3 a suspension containing young cultures of freshly
isolated B. influenzæ was introduced into the trachea by a
silver catheter passed through the glottis and larynx into
the trachea.
Young cultures of B. influenzæ, subcultured only once
after isolation from early cases of influenza, were used. The
microorganism was recovered in abundance by throat swab
two days later and again from the bronchus at autopsy
three days after inoculation. Tuberculosis of mesenteric
lymph nodes, of intestine and of liver and several small
tuberculous nodules in the lung were found at autopsy. A
secondary invasion of the lung by staphylococci had occurred.
There was bronchitis with an inflammatory infiltration
of the subepithelial tissue of the bronchi by lymphoid
and plasma cells. Bronchopneumonia was present,
and the bronchi and many of the alveoli contained blood.
These changes do not differ essentially from the changes
found in many instances of pneumonia following influenza.
In three instances cultures of B. influenzæ were injected
into the trachea by means of a hypodermic syringe.
In one of these experiments (Experiment 4) intratracheal
injection of 2 c.c. salt solution suspension of B. influenzæ
(isolated at autopsy from bronchus of the monkey
used in Experiment 3), representing growth on 1½ blood
agar plates, was made with a needle inserted into trachea
just above the suprasternal notch. On the following day a
throat culture contained B. influenzæ in abundance. Three
days after inoculation the monkey appeared to be very sick
and there was profuse nasal discharge. The animal
392coughed and sibilant râles were heard over the chest.
There was no leucocytosis. A throat culture contained
B. influenzæ. Four days after inoculation the monkey was
still sick and weak, but appeared much improved and was
killed. The trachea and large bronchi contained thick viscid
mucus. In the middle lobe of the right lung was a patch
of grayish red, airless tissue, firmer than the lung substance
elsewhere. Cultures from the trachea, bronchus and lung
contained a variety of microorganisms, but B. influenzæ was
not recovered.
In two additional experiments (Experiments 6 and 7)
cultures of B. influenzæ forty-eight hours old were injected
into the trachea of monkeys. The microorganism was recovered
in cultures made from the pharynx two days later.
These animals were only slightly sick.
Introduction of B. Influenzæ and S. Hemolyticus into the
Trachea.—In view of the frequent association of B. influenzæ
and S. hemolyticus in the sputum of patients with streptococcus
pneumonia following influenza and in the bronchi
and lungs of those who have died with this disease, the two
microorganisms were injected simultaneously into the trachea
of monkeys.
B. influenzæ and S. hemolyticus in Experiment 7 produced
bronchitis and bronchopneumonia. There was acute
inflammation of the interstitial tissue of the lung, and acute
lymphangitis with numerous polynuclear leucocytes within
the lumen of the lymphatics was present. B. influenzæ and
S. hemolyticus were present in the trachea at autopsy four
days after inoculation. It is probable that part of the injected
culture entered the tissue outside the trachea, for an
abscess was formed in this situation. It is noteworthy that
acute pericarditis occurred and both S. hemolyticus and B.
influenzæ were found in the pericardial exudate. B. influenzæ
not infrequently exhibits this tendency to penetrate in
association with other bacteria localities which it does not
invade independently.
393In a second experiment (Experiment 8) in which B. influenzæ
and S. hemolyticus were injected into the trachea,
both microorganisms were recovered from the throat on
the day following inoculation; on the fifth day S. hemolyticus
alone was recovered and on the sixth day a throat
culture was negative both for S. hemolyticus and B. influenzæ.
Introduction of B. influenzæ and of Pneumococcus or of
Pneumococcus Alone into the Trachea.—In two experiments
B. influenzæ and Pneumococcus Type III were simultaneously
injected into the trachea.
In Experiment 9 a large male monkey was used and intratracheal
injection made with syringe and needle of 5 c.c.
salt solution suspension of Pneumococcus Type III and B.
influenzæ (growth on 5 blood agar plates of mixed cultures
of Pneumococcus III and B. influenzæ). On the following
day the animal was very sick, lying on the floor of its cage,
and was dead two days after inoculation.
The dosage of bacteria in this experiment was large. The
lesions in gross appearance and microscopically resembled
those seen in many instances of pneumonia following influenza.
In the trachea there was loss of ciliated epithelium,
congestion of the subepithelial tissue, hemorrhage and infiltration
with plasma cells. The lungs were consolidated and
red and there were hemorrhage and edema. B. influenzæ,
as in human cases, was abundant in the bronchi, less abundant
in the consolidated lung, being present though scant
in the left lung, and absent in cultures from the right. B.
influenzæ as in Experiment 8 with streptococcus had entered
the left pericardial cavity in company in this experiment
with Pneumococcus III.
In Experiment 10 a very large monkey received by intratracheal
injection, made with syringe and needle, 5 c.c. salt
solution suspension of Pneumococcus III and 3 strains of
B. influenzæ, (2 recently isolated from cases of influenza
394and 1 from autopsy in a case of postinfluenzal pneumonia).
The animal died twenty-four hours later.
This simultaneous introduction of B. influenzæ and Pneumococcus
III in large quantity has produced rapidly fatal
pneumonia with lobar distribution. Hepatization was
homogeneous and red, and outside the consolidated parts
of the lung there was hemorrhage and edema. The lesion
resembled that found when death has occurred within a few
days after the onset of pneumonia following influenza, but
had no distinctive characters establishing its relation to
pneumonia following influenzæ.
In Experiment 11 Pneumococcus III alone in small
amount was introduced into the trachea of a small monkey.
The animal was very sick, but its condition improved and
recovery seemed probable. The animal was killed seven
days after inoculation, and typical lobar pneumonia with
gray hepatization was found at autopsy.
Experiment 11
November 20, 1918.—Small monkey; throat culture: negative for B. influenzæ,
pneumococcus and S. hemolyticus. November 28 and December 6.—Nose
and throat cultures again negative for B. influenzæ. December 9—4:30
P.M.—Intratracheal injection with syringe and needle of 0.33 c.c. of an
eighteen hour broth culture of Pneumococcus Type III. December 10.—The
animal is sick, huddled up in his cage with head down; there is rapid respiration
with expiratory grunt and the mucous membranes are moderately cyanotic.
There is frequent cough. Throat culture: Pneumococcus III present
in abundance. December 15.—The animal appears to be better. Respirations
are still rapid but less labored. December 16.—The animal is improving but
very weak and emaciated.
Autopsy.—The pleural cavities contain no fluid. On the right side are several
strands of fibrin. The right lower lobe with the exception of a small
patch at the summit and the lower part of the middle lobe are voluminous,
have a dull gray surface covered by a scant layer of fibrin and are firmly consolidated.
On section the consolidated tissue has a gray color and is conspicuously
granular, the granulation resembling, on a slightly smaller scale,
that seen in human lobar pneumonia. The bronchi contain a small amount of
viscid fluid.
Bacteriology.—Direct smears from the trachea and the lower lobe of the
left lung contain Gram-positive diplococci. Cultures from the trachea and
from the blood of the heart contain Pneumococcus III. Cultures from the
left lower lobe, from the liver and from the spleen remain sterile.
395Microscopical Examination.—There is abundant infiltration of the subepithelial
tissue of the trachea with plasma cells. Superficial ciliated epithelium
is in places lost. At one point is a small focus of hemorrhage. Alveoli in the
consolidated part of the lungs contain polynuclear leucocytes and fibrin and
exhibit the appearance seen in lobar pneumonia in man.
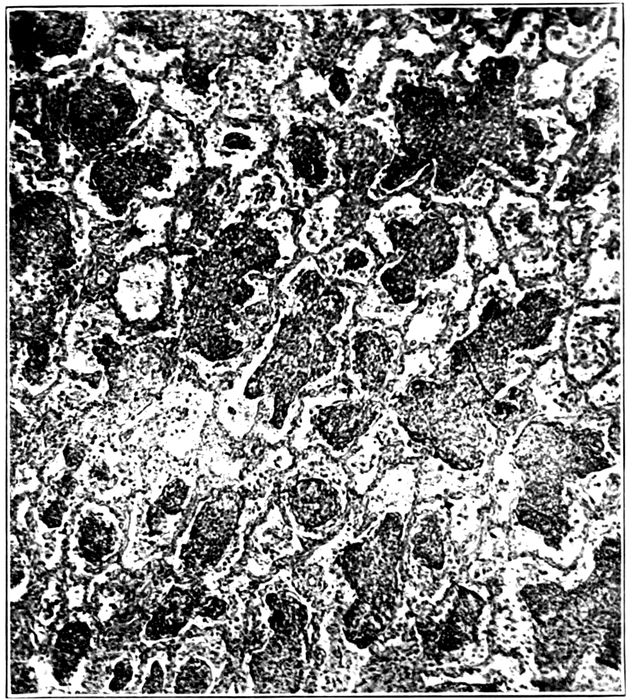
Fig. 33.—Experimental lobar pneumonia in the stage of gray hepatization produced by injection of Pneumococcus III into the trachea of a monkey (Experiment 11). The alveoli are uniformly filled with plugs of fibrinous exudate.
In Experiment 12 B. influenzæ was injected into the trachea
and two days later identified in a culture made from
the pharynx; four days after inoculation Pneumococcus IV
was injected into the trachea. The animal was killed seven
days after the first inoculation, and three days after inoculation
with pneumococcus. The lower half of the upper
lobe of the right lung and the greater part of the lower and
396middle lobes were consolidated. The pleural surface of the
consolidated areas was dull red and covered by a small
amount of fibrin. The lower lobe, with the exception of a
small part at the summit, was very firmly consolidated, on
section pinkish gray in the anterior part and deep red in a
small zone at the posterior border. The cut section was
conspicuously granular. The trachea and bronchi contained
mucus. Cultures from the trachea, the right lung
and the right pleural cavity contained Pneumococcus IV in
pure culture. Alveoli in the consolidated part of the lung
were filled with polynuclear leucocytes and fibrin.
Lobar pneumonia has been produced by the introduction
of Pneumococcus IV into the trachea. It is doubtful if preceding
inoculation of B. influenzæ has influenced the course
of the disease.
The foregoing experiments have shown that B. influenzæ
introduced into the nasopharynx or into the trachea of
monkeys is capable of causing lesions of the mucosa of
these structures; the microorganism persists within the
nasopharynx or trachea and is recoverable during a variable
period of from two to eleven days after inoculation.
Spontaneous infection of monkeys with B. influenzæ has
not been observed. The animals infected with the microorganism
are ill during several days, but the experimental
disease like most instances of human influenza is self limited.
Following inoculation of the nose and throat of monkeys
with B. influenzæ there is discharge from the nose,
tendency to epistaxis and absence of leucocytosis.
Bronchitis was produced by the introduction of B. influenzæ
into the trachea of monkeys, and the microorganism
was recovered from the nasopharynx two and three days
following inoculation. There was no leucocytosis. In two
experiments death occurred following inoculation, and in
both instances it was found that the animal suffered with
tuberculosis which had produced only trivial lesions of the
397lungs. In both animals staphylococci were obtained from
the internal organs. There was bronchitis with changes in
the bronchi which, although not characteristic, resembled
those found in association with B. influenzæ in man. It is
noteworthy that B. influenzæ is usually found mixed with
other bacteria in the bronchi of those who have died with
bronchitis and pneumonia following influenza. In the experimental
animals there was in places superficial loss of
ciliated epithelium, exudation of polynuclear leucocytes, infiltration
of the subepithelial tissue with plasma cells and
hemorrhage into this tissue.
In one instance simultaneous injection of B. influenzæ and
S. hemolyticus, freshly obtained from autopsy upon a man
dying with pneumonia following influenza, caused bronchitis
and bronchopneumonia; there were acute lymphangitis
and infiltration of the interstitial tissue of the lung with
polynuclear leucocytes such as occurs in human cases, but
the lesion had not proceeded to suppuration.
In man B. influenzæ is usually found in greatest abundance
upon the mucosa of the respiratory passages, less
frequently it invades the alveoli of the lungs and is almost
invariably found in association with other microorganisms.
In company with other microorganisms B. influenzæ penetrates
into tissues outside the lungs. In Experiment 7 it
has entered the pericardium, with streptococcus, and in
Experiment 9 with pneumococcus. When B. influenzæ and
streptococcus are injected into the peritoneal cavity of a
mouse both organisms appear in the blood, whereas in the
absence of streptococcus, B. influenzæ seldom leaves the
peritoneal cavity.
Typical lobar pneumonia has been produced for the first
time in monkeys by injecting pneumococci (in quantity as
small as 0.33 c.c. of suspension) into the trachea. With the
animals available it has not been possible to adjust the dosage
of the two microorganisms so that the influence of one
398upon the other might be determined. Pneumococcus III, in
small quantity, introduced into the trachea has produced
typical acute lobar pneumonia in the stage of gray hepatization.
A similar lesion has been produced with Pneumococcus
IV obtained from the lung of a man dead with pneumonia.
399
INDEX
- A
- Abscess of lung, bacteriology of, 203
- empyema with, 233
- healing of, 208
- measles with, 347
- parotitis with, 356
- pathogenesis of, 205, 375
- scarlet fever with, 357
- staphylococcus causing, 199, 225, 366, 377
- S. hemolyticus causing, 199, 365
- Autopsies, table of, 118, 120, 335
- Autopsy protocols, No. 280, 226;
- No. 286, 226;
- No. 312, 254;
- No. 322, 228;
- No. 330, 214;
- No. 333, 229;
- No. 370, 229;
- No. 376, 206;
- No. 379, 215;
- No. 380, 204;
- No. 387, 206;
- No. 397, 223;
- No. 406, 204;
- No. 416, 204;
- No. 420, 279;
- No. 425, 229;
- No. 428, 280;
- No. 433, 280;
- No. 445, 257;
- No. 465, 238;
- No. 467, 208;
- No. 473, 236;
- No. 474, 221;
- No. 487, 273;
- No. 499, 224;
- No. 504, 238
- B
- Bacillus influenzæ, 369
- bronchi and, 178, 215, 346
- bronchitis and, 153, 371
- experimental inoculation with, 389
- history of, 25
- influenza and, 30, 42, 43, 46, 49, 76, 370
- isolation of, 30, 32, 38, 44
- measles with, 26, 40, 43, 295, 351
- meningitis and, 26
- normal men carrying, 34, 42, 45, 369
- pathogenicity of, 26, 48, 370, 387, 396
- pneumococcus pneumonia with, 62, 178
- pneumonia with, 72, 75, 76, 173, 364, 371
- Bronchi, inflammation of mucous glands of, 146
- Bronchiectasis, 239, 269, 355, 367
- abscess with, 254
- bacteriology of, 244
- bronchitis with, 245
- measles with, 336
- pathogenesis of, 245, 259
- Bronchiolitis, organizing, 264
- Bronchitis, 40, 142, 195, 359
- bacteriology of, 56, 150, 164, 359, 371
- bronchiectasis with, 245
- chronic, 262
- clinical course of, 58
- measles with, 336
- organizing, 264
- purulent, 47, 56, 60, 63, 74, 143, 149, 153, 360
- Bronchopneumonia, 60, 63, 66, 162, 360, 363
- bacteriology of, 68, 163, 171, 176, 181, 184, 189, 194, 197, 345, 364
- fibrin with, 182
- lobar pneumonia with, 155, 157
- measles with, 340
- secondary infection by S. hemolyticus with, 172, 177, 181, 374
- C
- Carriers of B. Influenzæ, 46, 101, 369
- of S. hemolyticus, 99, 285, 287, 298, 303, 309, 310, 315, 319, 321, 332, 379
- Cartilage, atrophy with bronchiectasis of, 254
- Contact infection in influenza, prevention of, 98
- in measles, 289
- in pneumonia, prevention of, 98
- Cubicles to prevent contact infection, 98, 290
- 400Cyanosis, 144
- E
- Empyema, 64, 67, 224, 226, 233, 304, 366
- abscess of lung and, 233
- encapsulated, 235
- interstitial suppurative pneumonia with, 216, 234
- measles with, 349
- pneumococcus, 236, 350
- streptococcus, 233, 350
- Endophlebitis, 219
- H
- Hemorrhagic and edematous consolidation with bronchopneumonia, 188
- peribronchiolar consolidation with bronchopneumonia, 163, 173, 272, 340
- Hepatization with bronchopneumonia, 179, 181
- with lobar pneumonia, 160
- I
- Influenza, B. influenzæ with, 30, 73
- bronchitis with, 55, 56
- clinical course of, 28, 53, 73, 80
- coryza with, 54
- cyanosis with, 54
- epidemic in fall of 1918, 52, 108, 359
- epidemic in spring of 1918, 47
- fever with, 53
- gastrointestinal symptoms with, 55
- laryngitis with, 54
- lobar pneumonia and, 161
- measles and, 292, 319, 331, 351, 357, 380
- pandemic of 1889–90, 109, 115
- pandemic of 1918–19, 27, 359
- pharyngitis with, 54
- pneumococcus with, 33
- pneumonia with, 55, 59, 74, 81, 139
- pulmonary lesions of, 137
- pulse with, 54
- secondary infection with, 28, 45, 57, 95
- sputum with, 55
- S. hemolyticus with, 103
- Interstitial bronchopneumonia, 261, 278, 348
- suppurative pneumonia, 199, 209, 366, 376
- bacteriology of, 214
- chronic inflammation with, 221
- empyema with, 216, 234
- healing of, 222, 224
- measles with, 348
- pericarditis with, 237
- L
- Lobar pneumonia, 60, 63, 154, 360, 362
- bacteriology of, 64, 156, 164, 339, 362
- bronchopneumonia with, 155, 157
- experimental production in monkeys of, 394, 397
- influenza and, 161
- measles with, 337
- purulent bronchitis with, 60, 63, 66
- secondary infection by hemolytic streptococci with, 64, 159, 340, 374
- spread in lung of, 339, 354
- typhoid fever with, 353
- Lobular consolidation, confluent, 188, 341
- Lymphatics, suppurative inflammation of, 217, 218, 376
- Lymphangitis, experimental production with S. hemolyticus of, 392
- M
- Masks to prevent contact infection, 98, 290
- Mastoiditis, 303, 312, 332
- Measles, 119, 288
- B. influenzæ with, 26, 40, 43, 295
- bronchiectasis with, 336
- bronchitis with, 336
- bronchopneumonia with, 340
- complications of, 303, 378
- empyema with, 349
- influenza and, 292, 319, 331, 351, 357, 380
- interstitial suppurative pneumonia with, 348
- lobar pneumonia with, 337
- pneumococcus pneumonia with, 312
- pneumonia and, 292, 303, 312, 332, 334, 378
- secondary infection with, 282
- 401S. hemolyticus with, 285, 287, 297, 319, 330, 331, 353, 378
- suppurative pneumonia with, 345, 347
- unresolved bronchopneumonia with, 342
- Methods, 29, 51, 283, 291
- Mortality of pneumococcus pneumonia, 140
- of pneumonia following influenza, 139
- of streptococcus pneumonia, 140
- Mumps, 119, 355
- N
- Necrosis with bronchopneumonia caused by S. hemolyticus, 186, 375
- with lobar pneumonia caused by S. hemolyticus, 160, 374
- with S. hemolyticus, 199, 200
- O
- Oedema, interstitial, 209
- Organization of pneumonic exudate, 197
- Otitis media, 289, 303, 312, 317, 329, 332
- P
- Peribronchiolar consolidation with bronchopneumonia, 163, 166, 267, 340
- Pericarditis, 64, 237
- Peribronchial consolidation with bronchopneumonia, 163, 192, 361
- Peritonitis, 238
- Phagocytosis of red blood corpuscles, 272
- Pneumococcus, 372
- bronchitis and, 153
- bronchopneumonia with, 165, 184, 373
- empyema, 236
- experimental lobar pneumonia with, 393
- influenza with, 33
- lobar pneumonia with, 158, 372
- pneumonia, 60, 75, 104
- clinical course of, 62
- measles and, 312, 332
- mortality of, 140
- secondary pneumococcus infection with, 61
- secondary streptococcus infection with, 62
- transmission of, 91, 383
- secondary infection in pneumonia with, 91
- Pneumonia, B. influenzæ causing, 72, 76, 371
- bacteriology of influenza and, 60, 74, 107
- bacteriology of measles and, 351
- chronic fibroid, 273
- clinical course of influenza with, 62
- diagnosis of, 136, 334, 361
- dissecans, 209
- immunity following, 373
- influenza with, 59, 76, 81, 109, 360
- measles and, 119, 292, 303, 312, 332, 334, 378
- mumps and, 119
- pneumococcus, see Pneumococcus pneumonia
- prevention of, 98, 319, 383
- scarlet fever and, 119
- secondary infection with, 83, 106
- spread through lungs of, 194, 373
- staphylococcus, see Staphylococcus pneumonia
- streptococcus, see Streptococcus pneumonia
- S. hemolyticus in throat with, 310, 329, 379
- Pseudoinfluenza bacilli, 26
- S
- Scarlet fever, 119, 356
- Squamous transformation of bronchial epithelium, 149, 251, 275, 336
- Staphylococcus, 153, 377
- Streptococcus empyema, 233
- hemolyticus, 374
- bronchitis with, 153
- dissemination in wards of, 315
- experimental production of acute
- lymphangitis with, 392
- identification of, 283
- influenza with, 103
- lobar pneumonia with, 64, 159
- measles with, 285, 287, 297, 330, 331, 345, 353, 378
- 402normal men with, 285, 322
- secondary infection in pneumonia with, 84, 106, 178, 204, 374
- nonhemolytic, 376
- peritonitis, 238
- pneumonia, 60, 70, 75, 115, 307, 365
- bacteriology of, 71
- clinical features of, 71
- measles with, 303, 305, 307, 318
- mortality of, 140
- transmission of, 84, 381
- viridans, 377
- Suppurative pneumonia, 199, 347
- T
- Thrombosis of capillaries with bronchopneumonia, 184
- Typhoid fever, lobar pneumonia with, 353
- staphylococcus pneumonia with, 354
- U
- Unresolved bronchopneumonia, 261, 266, 342, 368
- bacteriology of, 276
- interstitial suppurative pneumonia with, 278
- Silently corrected typographical errors and variations in spelling.
- Archaic, non-standard, and uncertain spellings retained as printed.
- Footnotes have been re-indexed using numbers and collected together at the end of the
last chapter.
*** END OF THE PROJECT GUTENBERG EBOOK 62429 ***