Patient’s Chart. Cardboard, five by eight inches
Transcriber’s Note:
The cover image was created by the transcriber and is placed in the public domain.
To tuberculosis, more than to any other infectious disease, the parable of the seed and the soil is strictly applicable. Without the tubercle bacillus there can be no tuberculosis, but for tuberculosis to develop, many factors of great complexity and as yet but little understood must facilitate the implantation of the bacillus and augment its growth. It is true that though we may emphasize the rôle of the bacillus, still we cannot completely ignore those personal factors that contribute to make the infection fruitful, and likewise though we focus our attention upon individual resistance, still we cannot keep out of sight the invader that is being resisted. The two viewpoints meet and run together, but are sufficiently separate to lead to different methods in our efforts to eradicate tuberculosis.
On the one hand are those who direct their efforts toward the annihilation of the tubercle bacillus. We are sufficiently instructed about the life history and habits of this organism to lay our viplans upon a firm, scientific basis—a basis so firm and at first sight so simple and so plausible that over-enthusiasm led to predictions that have been sadly disappointed. The principles are sound indeed, but in practice their application has met with insuperable difficulties. These obstructions have sharpened our wits to find new avenues that now promise a more ready approach to the goal. To put the matter briefly, the tuberculosis campaign of the past fifteen years has taught us two important lessons: first, that the tuberculous cannot be isolated in their homes; second, that they cannot be cured in or out of sanatoria. I am shocked myself to read these bald statements, particularly the second, and still I am convinced that they are true. Some patients can be isolated in their homes, and many patients recover from tuberculosis and remain well. Tuberculosis is very amenable to treatment and under proper conditions the results of treatment are very gratifying. The difficulty is that the proper conditions are in most instances wanting, and when they are absent sanatorium recovery is almost invariably followed, after a brief period, by relapse. The records of cases with tubercle bacilli in the sputum establish this fact. Concerning the value of statistics of cases without tubercle bacilli in the viisputum I entertain the gravest doubt. While I am heartily in favour of treating such patients, the personal equation enters too largely into the diagnosis to give the results convincing value as evidence of the lasting benefits of treatment. Experience has taught me that the educational value of sanatoria has been grossly exaggerated, and that this value is of small account in a broad plan of prevention. Our present knowledge, fortified by the costly experience of the past fifteen years, forces us to believe that the most direct and effective way of dealing with the tubercle bacillus is to isolate as many advanced consumptives as is possible. The hospital, perhaps supplemented by colonies, is the rational method of procedure. Other factors are of importance; all other factors are, but this is the fundamental and essential factor in the campaign.
On the other hand are those who direct their efforts towards cultivating the soil. Reliable studies inform us that ninety per cent. of the human race is tuberculosis infected, and that infection occurs at a very early age, so that at twelve years few children have escaped it. Relatively a small number of those infected subsequently become tuberculous, so that something more than infection is necessary for tuberculosis to develop. viiiWhat this something is we do not know. Time, manner, frequency, and intensity of infection play an important part. Apparently too there is a wide personal variation in susceptibility. To just what this personal factor is due we are not in a position to say, but certain general facts known about the distribution of tuberculosis afford us a clue to its interpretation. Tuberculosis, like most infectious diseases, thrives under the conditions that poverty induces. Inadequate housing facilities, insufficient food, filth, and sordid care are a few of these. If, as all must admit, the tubercle bacillus is more or less ubiquitous and few escape contact with it, then an important part of our campaign of prevention will be the raising of personal resistance so that when infection occurs it may be successfully overcome. Here is the field for wide social activity. Everything that makes for higher standards of living and for improved personal hygiene is a valuable arm against tuberculosis. Housing laws, child-labour laws, the wage question, municipal recreation centres, the liquor question, social service in all its departments, vacation lodges, open-air schools, factory inspection, and so on and so on, are all indirectly valuable anti-tuberculosis agitation.
It is not my purpose to discuss the relative ixmerits of the various phases of the anti-tuberculosis campaign. The death-rate from tuberculosis is falling steadily and rapidly, and it has fallen most rapidly in just those centres where the campaign has been vigorously pushed on a broad basis. Which phase of the work is responsible for the decrease or deserves the greatest credit, it is impossible to conclude from a study of available evidence. The same statistics are interpreted by one, for instance Cornet, as evidence of the efficiency of sputum prophylaxis; by another, for instance Hoffman, as evidence of the influence of improved economic conditions; by yet another, for instance Newsholme, as evidence of the value of hospitals for advanced cases; and finally by many, for instance Fränkel, as evidence of the undisputed value of all three factors. Which factor one emphasizes will depend largely upon one’s training and the field of activity in which one is engaged.
Being a physician and by training accustomed to view problems from a medical standpoint, it is natural that I should emphasize the attacks upon the bacillus. As I have said, it seems to me to be firmly established that the most efficient, the most direct, and the cheapest way to enforce isolation and prevent infection is by hospital segregation of cases of advanced pulmonary tuberculosis. While xearly diagnosis, sanatorium treatment, and education are valuable features of the campaign, their value will be but slight if this one essential feature is neglected. Indeed I am inclined to see the chief value of economic improvement in the indirect influence this improvement exercises upon the facility for infection. With economic advance the æsthetic value of general and personal hygiene grows apace, and the dictates of ordinary cleanliness offer a very strong barrier to infection. Poverty itself does not produce tuberculosis, but the conditions that poverty fosters do, and the advantages of better living reside not so much in an improved personal fitness as in the eradication of the conditions that facilitate infection. This view is in accord with what we have learned of other infections. Plague has been notoriously a scourge to the poor. To improve living conditions lessens plague, and this general fact was known before we learned that cleanliness produced results indirectly by eliminating rats. Malaria has always been particularly prevalent amongst labourers living in unprotected huts. To improve living conditions reduces malaria, but we gain the result more surely and directly by an intelligent campaign against mosquitoes. Unfortunately, we are not sufficiently instructed about tuberculosis to pick out of the xiwhole mass of ills that poverty entails those few essential features that control infection. Perhaps some day we will, and then we shall be able to manage the social campaign more efficiently and economically. For instance, we are quite at sea to know what prophylactic use to make of the firmly grounded fact that tuberculosis infection establishes a strong resistance to reinfection. Upon an analogous principle rests the conquest of smallpox by vaccination. No doubt this immunity reaction has an important influence upon the development of tuberculosis, but as yet we know too little about it to control it and use it to advantage in our fight with the disease.
In the anti-tuberculosis campaign the nurse must look to medical science for the plan and inspiration of her work. Her attitude in the tuberculosis campaign must always conform to the medical attitude, although she may and indeed has added valuable material for building up this attitude. It is because this intimate relation exists that I have briefly outlined the medical impression of the tuberculosis campaign. It is quite natural that it should represent at the same time the nurse’s attitude. My object was to point out the numerous factors concerned in the anti-tuberculosis crusade, their interrelation, and the quite xiinatural and necessary specialization that must occur. The field of the nurse and particularly the municipal nurse is circumscribed, but it is large enough to engage all her energy and devotion. It is not necessary nor even desirable that she should diffuse her interest and energy over the adjoining fields.
For more than ten years Miss La Motte and I have been engaged in working at the same problems, from the same broad though different personal viewpoint. Our work has brought us into almost daily contact. I acknowledge, with gratitude, the many valuable suggestions that I have borrowed from her experience, and in reading her book I note with the greatest satisfaction what I believe to be evidence of influence from the experience I have gained. It is a pleasure to find that after years of arduous work we agree at least upon what is the fundamental problem of the tuberculosis campaign, namely—institutional care of the advanced cases of pulmonary tuberculosis. I think it is right and proper that Miss La Motte has made this fact the guiding principle of her book, and that she has shown the relation of nursing activity to its furtherance, and that she has held all other phases of tuberculosis work subservient to it. To avoid misunderstanding it may be xiiinecessary to point out that other features of the anti-tuberculosis campaign have been merely touched upon or entirely ignored. This apparent slight is not offered, I am sure, as a reflection upon the value of these features; they are omitted simply to accentuate more boldly the dominant idea of the nurse’s work.
Another noteworthy feature of the book is the purely personal and local character of the experience presented. It details the problems that have offered themselves here in Baltimore, how these problems have been met, and how an effective nursing staff has been built up, first under private and then under municipal control. What has been accomplished abroad and in other localities in this country is not considered. In a way this is a disadvantage, for the book loses somewhat in breadth and erudition. However, I am convinced that what may be lost in this respect is more than compensated for by the gain in force and conciseness. After all, the fundamental problems are the same everywhere, and though local conditions will necessitate adjustment of details, still I believe the adjustment will be stimulated and facilitated more by a spirited account of what has been done under specific conditions than by a colourless review of the whole field of activity.
xivNo doubt many will find personal views expressed with which they disagree. This is unavoidable before such a frank and radical presentation of the situation. One is impressed by the honesty and enthusiasm of the book, but some may wish that certain of the statements, and particularly some strictures, had been a little mollified. The book will be interesting and helpful and, what is more important, stimulating to all engaged in tuberculosis work. All the better if some parts of it cause surprise and opposition,—we will then review more critically our own attitude.
During eight successive years the writer has been engaged in special tuberculosis work, first as field nurse of the Visiting Nurse Association of Baltimore, later as organizer and director of the Tuberculosis Division of the Baltimore Health Department. Entering the field in the pioneer days of 1905, she has seen the work pass through the struggling stages of private enterprise into the well organized, almost automatic grooves of the city machinery. This continuity of service has been an experience of unique value. During this period we have walked into and backed out of many blind alleys or “No Thoroughfares,” and have acquired wisdom through the loss of infinite time, effort, and money. Although the material for the following pages was gathered in Baltimore, and is therefore, strictly speaking, of a local character, yet since practically all of the conditions indicated or dealt with are common to all towns and cities, this need not limit the application of the ideas and principles set forth.
xviIt is also hoped that though the work of tuberculosis nursing is dealt with chiefly as done under the auspices of a Visiting Nurse Association, or as part of the work of a City Health Department, what is here presented will be of value to nurses working under private associations, and to private associations themselves. Therefore, in presenting this book to the public—to nurses, physicians, social workers, anti-tuberculosis associations, and all those engaged in public health work—the writer has two objects in view. First, to offer a working model by which any community can gain some idea as to how to organize and conduct tuberculosis work; second, to offer conclusions, gained through practical experience, as to the nurse’s part in the anti-tuberculosis campaign.
The object of the anti-tuberculosis campaign is the eradication of tuberculosis. Our experience has been to prove that the simplest and most direct method of controlling this disease is through the segregation—the voluntary segregation—of the distributor, and that to remove the patient from an environment where he is dangerous to one where he is harmless is the function of the public health nurse. This is her chief and foremost duty, and all others are subsidiary to it.
The writer wishes to express her appreciation xviiand deep indebtedness to those friends and fellow-workers who have given her guidance and assistance during these years of service. These are: Mary E. Lent, Superintendent of the Visiting Nurse Association of Baltimore, and Susan Edmond Coyle, “lay member” of that Association; Dr. Louis Hamman, Physician-in-Charge of the Phipps Dispensary, Johns Hopkins Hospital; Dr. Samuel Wolman, First Assistant to the Phipps Tuberculosis Dispensary; Dr. Gordon Wilson, Physician-in-Charge of the Maryland University Dispensary and of the Municipal Tuberculosis Hospital; Dr. Martin F. Sloan, Superintendent of Eudowood Sanatorium; Dr. Victor F. Cullen, Superintendent of the Maryland Tuberculosis Sanatorium; and my Chief, Dr. Nathan R. Gorter, Health Commissioner of Baltimore.
| CHAPTER I | |
| PAGE | |
|---|---|
| Statement of the Case—Beginning the Work—Reaching the Patients—Supervision of the Work—Necessity for Experienced Nurses | 1 |
| CHAPTER II | |
| The Nurse’s Training—Health—Hours Off Duty—Afternoons Off—Character | 11 |
| CHAPTER III | |
| Salary—Increase of Salary—Carfare—Transportation—Telephone—Vacation—Sick Leave—Uniforms—Badges | 20 |
| CHAPTER IV | |
| Object of Work—Districts—Hours on Duty—Number of Daily Visits—The Nurse’s Office—Lunch and the Noon Hour—Bags—Prophylactic Supplies—Cups, Fillers, and Napkins—Disinfectant—Waterproof Pockets—Books of Instruction—Stocking the Bag and Distributing Supplies—Nursing Supplies | 33 |
| xx | |
| CHAPTER V | |
| Records and Reports—The Patient’s Chart—The Card Index—Nurse’s Daily Report Sheet—Weekly and Monthly Reports—Examination of Charts—Taking the Patient’s History | 48 |
| CHAPTER VI | |
| Finding Patients and Building up the Visiting List—Increasing the Visiting List—Social Workers—Dispensaries—Patients’ Families and Friends—Nurses’ Cases—Physicians | 61 |
| CHAPTER VII | |
| The General Practitioner and the Public Health—Responsibility of the Private Practitioner in Tuberculosis—Impossibility of Fulfilling this Obligation—Failure because of the Nature of Tuberculosis—Failure because of the Personal Equation | 74 |
| CHAPTER VIII | |
| The Nurse in Relation to the Physician—Municipal Control of Infectious Diseases—The Nurse’s Difficulties—A Waiting Game—Undiagnosed Cases—The Nurse’s Responsibility to the Ethical Practitioner Only | 87 |
| xxi | |
| CHAPTER IX | |
| Obtaining a Diagnosis—The General Dispensary—Sputum Examinations—Tuberculin Tests—Registration of Cases | 105 |
| CHAPTER X | |
| Prevention of Tuberculosis—Sources through which Calls are Received—Entering the Home—Telling the Truth to the Patient—Truth for the Family—Disposal of Sputum—Danger of Expired Air—Isolation of Dishes—Linen, Household and Personal—Disinfectant and Other Supplies—Phthisiphobia | 117 |
| CHAPTER XI | |
| Inspection of the House—The Patient’s Bedroom—Porches—Gardens and Tents—Flat Roofs—Clothing and Bedclothing—Artificial Heat—Rest—Fresh Air—Food—Cooking—The Bedridden Patient | 136 |
| CHAPTER XII | |
| Care of the Family—Examination of the Family—Taking Patients to Dispensaries—Children—Tuberculosis in Children—Open-Air Schools—The Danger of Sending Patients to the Country | 154 |
| xxii | |
| CHAPTER XIII | |
| Disinfection of Houses—Value of Fumigation—Formaldehyde—Housecleaning—Burning and Sterilizing—Boiling—Carpets, Rugs, and Mattings—Painting, Papering, and Whitewashing—Temporary Removals—Vacant Houses—Concessions—Compulsory Cleaning | 169 |
| CHAPTER XIV | |
| The Tuberculosis Dispensary—Equipment—Medicines—Hours—Consideration for Patients—Function of the Dispensary—The Physician’s Service—The Physician’s Qualifications—The Physician and the Patient—Duties of the Nurse—Tuberculin Classes—The Nurse in Home and Dispensary—The Nurse as a Community Asset | 184 |
| CHAPTER XV | |
| The Nurse in Relation to the Institution—Reports Made to the Institution—Procuring Patients for it—The Value of the Sanatorium—Sanatorium Outfit—Return from the Sanatorium—Work for the Arrested Case—Light Work—Outdoor Work | 203 |
| CHAPTER XVI | |
| xxiiiHospitals for Advanced Cases—The Careful Consumptive—Chief Duty of the Nurse—Responsibility of the Institution—Home Care of the Advanced Case—Exceptions to Institutional Care—Compulsory Segregation | 218 |
| CHAPTER XVII | |
| The Problem of Relief-Giving—The Relief-Giver—Co-operation between Agent and Nurse—General Rules for Nurses and Agents—Conditions of Asking for Relief—Wrong Conditions of Relief-Giving—Incidental Assistance—Withdrawal of Relief—Milk and Eggs | 230 |
| CHAPTER XVIII | |
| Home Occupations of Consumptives—Sewing and Sweatshop Work—Food—Milk and Cream—Lunch Rooms and Eating-Houses—Laundry Work—Boarding and Lodging-Houses—Miscellaneous Occupations—The Consumptive Outside the Home—Cooks—Personal Contact in the Factory—Supervision Outside the Home | 252 |
| CHAPTER XIX | |
| Municipal Control of Tuberculosis—The Danger of “Political” Control—“Politics” in Co-operating Divisions of the Health Department—Results in Baltimore—Tuberculosis and Poverty | 273 |
Statement of the Case—Beginning the Work—Reaching the Patients—Supervision of the Work—Necessity for Experienced Nurses.
Statement of the Case. Pulmonary tuberculosis is a communicable disease, transmitted from person to person by means of the tubercle bacilli contained in the sputum of infected patients, or in the breath expired during paroxysms of coughing. The bacilli thus liberated, find their way into the system of another individual, either through the respiratory or alimentary tract, or both. The enormous prevalence of tuberculosis is due to the fact that its infectious nature was not recognized until 1882 when Koch discovered the bacilli. Since that time it has been classed as a transmissible disease, and during the past ten years a vigorous effort has been made to eradicate it. This agitation is popularly known as the anti-tuberculosis 2campaign, and associations for the suppression of tuberculosis have sprung up in all parts of the country. So far, no serum or vaccine has been found by which this disease may be controlled, as was the case when smallpox and diphtheria were checked. The sole way of overcoming it is to overcome the ignorance concerning its nature, its transmissibility, and the means by which it is spread.
At the beginning of the campaign it was believed that simple education along these lines was all that was needed to obtain results. These results were expected to follow as soon as the patient was informed of the nature of his disease, and how to avoid spreading it, and as soon as those in contact with him were given like information and taught how to avoid infection. Ten years ago, in the optimism of the moment, tuberculosis was freely proclaimed a “curable” disease; so that together with the campaign of prevention went a campaign of teaching the patient how to become a “cured,” or as we now call it, an arrested, case. The mechanics of cure were equally simple—rest, fresh air, and food were all that was needed, provided the disease was taken in the early stages. And all that was necessary for “cure,” just as all that was necessary for prevention, was to tell the patient what to do, 3and those about him what to do, and the thing was done. This is the theory upon which the work was founded, and in theory this is still a sound principle upon which to continue it. Unfortunately, a series of unlooked for conditions interposed themselves between this theory and our ability to put it into practice. At the time when the crusade was begun these conditions were not recognized, and it is only through long study of the situation, from its social, economic, and legal as well as clinical aspects that we get some idea of the difficulties and complexities of the task before us.
In the first place, tuberculosis is largely a disease of the poor—of those on or below the poverty line. We must further realize that there are two sorts of poor people—not only those financially handicapped and so unable to control their environment, but those who are mentally and morally poor, and lack intelligence, will power, and self-control. The poor, from whatever cause, form a class whose environment is difficult to alter. And we must further realize that these patients are surrounded in their homes by people of their own kind—their families and friends—who are also poor. It is this fact which makes the task so difficult, and makes the prevention and cure of a preventable and curable disease a matter of the utmost complexity.
4People of this sort, however, constitute almost the entire problem—otherwise the situation would be so simple that the word problem would not apply.
This is why “cure” is not the solution of the matter. Too few people are cured, in comparison to the numbers annually infected, to make any impression on a disease of such wide prevalence. The sanatorium, valuable as it may be for certain cases, is of little use to those who relapse upon return to an environment they will not or cannot control. This is also why mere instruction in preventive measures, unaccompanied by effective isolation, is barren of results.
Experience has taught us the unsatisfactory nature of so-called cures, and the futility of that prevention which allows the distributor of tuberculosis to remain at large in the community and heedless of his obligations. Hence we must look to segregation as the only reasonable course to pursue. If segregation can be obtained in the home, well and good. If not, then we must look to the institution to provide the proper care. This segregation, most of it voluntary, some of it enforced, is the only way to do preventive work on a scale large enough to count. To this end, we need dispensaries where the disease may be recognized 5and diagnosed, nurses to visit the patients in their homes, and hospitals for advanced cases, the function of the nurse being to teach patients and their families the necessity for segregating the former in hospitals.
Beginning the Work. Let us suppose that a certain community, town or country, suddenly becomes aware of tuberculosis in its midst, and in consequence wishes to get rid of it. It is but a fraction of the community which is enlightened enough for this, but from this nucleus must come all that awakening of public sentiment needed to facilitate the campaign. To estimate the number of tuberculous persons in any locality, multiply the yearly tuberculosis death-rate by five or ten—authorities differ as to the exact figures. The result will be the approximate number of those afflicted. The public press will help in disseminating this information, which is the basis from which we must work. Since the beginning of the campaign, newspapers have been wonderfully helpful allies in giving wide publicity to facts concerning tuberculosis. As a result of this newly aroused interest, an Anti-Tuberculosis Society may be created, and into its fold are gathered all those willing to help in the work, each with his dollar. Lectures, exhibits, open-air speaking, 6lantern-slide exhibitions, meetings in churches and others held before various societies are given in various parts of the town, and in this way information about tuberculosis is spread far and wide.
There are two classes of the community, however, that must be reached—those who have tuberculosis and those who have not. The people who go to lectures and exhibits belong chiefly to the latter class. Frequently, of course, the sick ones find their way in, in an endeavour to learn something which may be helpful to them; unfortunately, they are able to take away but little, and the little they do get they often misapply. We recall the case of a man who went to a tuberculosis exhibit, and learned that fresh air was good. As a result, he walked several miles a day in order to get it, and nearly killed himself. He had succeeded in learning one important fact—that fresh air was valuable—but another, of equal importance, that exercise was harmful, had escaped him.
To make the undertaking succeed, it is necessary to reach both the sick and the well, since that strong, intelligent public opinion, which is the motive force behind all new movements, must be aroused among the sick as well as among the healthy. But as we have seen, the former are not 7those who go largely to lectures, so they must be reached through some other means. The most effective way of reaching them is through the employment of a special nurse, who shall give eight hours a day, week in and week out, to visiting in the homes where tuberculosis exists, and giving instruction adapted to each individual case. By this means the people most in need of assistance are reached without loss of time and effort, and case after case is uncovered. This is shooting straight for the bull’s-eye—namely, the infected home from which tuberculosis is spread.
There may be laws on the statute books compelling doctors to notify the local health authorities of their tuberculosis cases, but these laws are not lived up to. Nor will the establishment of a hospital for advanced cases bring these patients to light; neither will the sanatorium, nor even the special tuberculosis dispensary. The surest and most effective way of unearthing them is through the visiting nurse. Therefore the nebulous plans of the newly formed anti-tuberculosis association may well crystallize themselves into a decision to put such an effective agent into the field.
Supervision of Work. After this decision has been made, the question arises, by whom is the nurse to be directed? Is she to be placed under 8the local health department, under a dispensary, under the charity organization society, or under the visiting nurse association, if such an organization exists in the town? If supported by a church or special association of some sort, should not the governing board of such organization direct her work? Or is she to be a free lance and manage herself?
Unless taken over by the local health department (which in that case becomes responsible for her salary and expenses incurred in the work), the nurse should be affiliated with the Visiting Nurse Association, rather than with any lay organization. Better results will be obtained if her work is directed by a superintendent of nurses who is accustomed to dealing with and judging nurses, and familiar with their duties along technical lines. The credit of supporting the nurse would still rest where it belonged—with the church, with the anti-tuberculosis association, or whatever group of people might be responsible for her maintenance,[1] but this arrangement would relieve the lay organization of much responsibility, for no matter how good their intentions, such a group 9cannot direct nursing work as well as this can be done by one qualified for the purpose. Another advantage gained by placing the new nurse with the Visiting Nurse Association is that it keeps together the various branches of public health service, and the tuberculosis nurse realizes more fully than she otherwise might, how completely her own specialty is interlocked with and dependent upon other forms of social activity.
1. For five years the Maryland Tuberculosis Association supported five nurses, which it placed under the management of the Superintendent of the Visiting Nurse Association of Baltimore.
There is still another advantage in placing the new nurse with the established organization, for then a nurse may be selected with regard to her ability alone, leaving it to the Superintendent of Nurses to give her the necessary careful training in social work, and the proper supervision.
If there is no Visiting Nurse Association in the community, under whose auspices the new special nurse may be placed, the lay organization will have to do the best it can. In this event, it will be absolutely necessary to select a nurse thoroughly trained in social work, and since the number of women with this equipment falls far short of the demand, a delay of some duration may take place. This delay is always borne with great impatience by the newly formed group of people, anxious in their enthusiasm to attack the tuberculosis problem at once. Yet policy would counsel postponing 10the undertaking until a suitable person can be found, for it is usually a fatal mistake to begin new work with an inexperienced worker. Moreover, a situation which has existed for years may be tolerated a few months longer without undue alarm as to consequences.
If it is impossible to obtain a nurse fully trained in public health work, the community may select a good nurse and send her for a few months’ experience to some well recognized centre of public health work, such as New York, Chicago, Boston, Baltimore, etc. The money thus spent will prove a valuable investment to a community thus far-seeing, and an ample return will be manifest in the efficiency of the nurse’s work.
A wrong start in choosing a nurse has driven many an enthusiastic organization into deep waters, and caused trouble and misunderstanding of a most grievous sort. In several instances, the local campaign against tuberculosis has come to a disappointed end; in others, public interest has been so antagonized and repelled that the movement received a check from which it did not recover for several years.
The Nurse’s Training—Health—Hours off Duty—Afternoons off—Character.
Training. One of the first qualifications of the nurse should be proper training. She should be a graduate of a first-class general hospital, which gives a three-years’ course. In States where registration is established, she should be a registered nurse as well. This means that she has passed the examinations set by the State Board of Examiners for Nurses, and has attained at least the minimum degree of efficiency prescribed by that body. Of course, it is well if she far exceeds this minimum, but she must not fall below it in any case.
It is sometimes said that a woman trained in a sanatorium or special tuberculosis hospital will make as good a tuberculosis nurse as one who has been trained in all branches of nursing work. This claim is often made by those sanatoriums which seek to find positions for their ex-patients, to whom they have given a more or less sketchy 12training and a diploma. Needless to say, if a community undertakes to support a nurse, it should procure the best that can be found. There is no economy in employing a half-trained woman. In social work the nurse occupies a unique position in the patient’s household—she must be able not only to gain but to retain the family’s confidence, and this cannot be done by a half-educated woman, not sure of herself and unable to carry conviction to her hearers.
Health. Next to thorough training, the health of the nurse is of utmost importance. All nurses should be examined before they undertake tuberculosis work. This should be done for two reasons: first, for the obvious reason of protecting the nurse herself; secondly, for the protection of the work. There is already sufficient prejudice against tuberculosis work, and it is well not to increase it by having a nurse break down soon after going on duty. In Baltimore, all applicants are examined by a specialist before they are accepted. Note that this is done by a specialist, and that the applicant is not permitted to go to her own “family physician” who may or may not be able to make a proper examination. The candidate is given a choice of several specialists, to any one of whom she may go. The report of 13her physical condition, mailed to the superintendent, determines her eligibility from the standpoint of health. In this way, the responsibility is assumed by those most capable of assuming it, and neither the health of the nurse nor the prestige of the work is jeopardized.
After the preliminary examination, it is well for the nurse on duty to be re-examined every six months. If suspicious symptoms present themselves, this should be done oftener. Part of the superintendent’s duties are to watch the health of her workers, and keep a sharp look-out for suspicious symptoms—symptoms which the nurse herself may be unaware of or afraid to acknowledge. Each nurse, however, should assume the responsibility for her own health; she should remember that she is dealing with a highly infectious disease, and that it behooves her to keep in as good physical condition as possible. Nurses with a predisposition to tuberculosis should not undertake this work.
The question often arises as to whether this visiting work is suitable employment for arrested cases—for nurses who have had tuberculosis and recovered. It is not suitable. It is far too hard and trying, for it must be done day in and day out, at all seasons and in all weathers, and involves 14severe physical strain. For that reason it is not proper occupation for one whose health is in any way precarious. The danger of relapse is too great. Nor should this work be done by those who are afraid of tuberculosis. If fear of tuberculosis develops after a nurse goes on duty, she should be released at once. Under such circumstances she cannot do good work, while to persuade her to remain on duty, contrary to her instincts, is a responsibility too grave for any one to assume.
Hours off Duty. At this point we should like to speak of the nurse’s hours off duty, though strictly speaking they are not within our scope. As a rule, the hours on duty are eight—from 9 a.m. till 5 p.m., with an hour in the middle of the day for lunch. This is a long day, and at the end of it, any woman is in a condition of mental and physical fatigue. The constant nervous strain occasioned by contending with the ignorance and stubbornness which a nurse must encounter, is particularly wearing.
The hours off duty are for recuperation from the day’s toil, and if this recuperation is insufficient, it will manifest itself in various ways. A tired nurse is of no use as a teacher—she cannot cope successfully with the obstinate wills of her patients, nor with the trying demands of the daily 15routine. Moreover, a physically tired person is one who offers ready soil for the development of tuberculosis. These two facts must be constantly borne in mind. Therefore we should like to impress upon all nurses who undertake this work that they must take excellent care of themselves. Rest, sleep, and food are the three essentials to good health, and any scheme of life which reduces these below a certain level is bound to lead to disaster.
No one condemns reasonable pleasures, and in no other work is relaxation and recreation so much required, but one must be careful not to burn the candle at both ends. It is no part of the superintendent’s duties to regulate the life of her nurses outside of working hours, but when their life off duty diminishes their working ability, she is then called upon to interfere. Tuberculosis work is trying, serious, and difficult, and demands a high degree of mental and physical strength and freshness. If a nurse is not willing to give this, she should not undertake public health work.
Afternoons Off. Each nurse should be given one afternoon a week off duty. It is more satisfactory to give this half-day in the middle of the week, on Wednesday or Thursday, rather than on Saturday, at the week’s end. In this way, the rest period breaks the long stretch of days, and the 16nurse is enabled to rest before she becomes too tired. Sundays, of course, should always be free. Under no consideration should the nurse be subject to night calls and it is well to have this fact understood at the outset of the work. A nurse cannot be on duty night and day both, and certain rules should be established, regarding her hours on duty, and be rigidly adhered to.
Character. The questions of training and of health having been satisfactorily answered, there remains a third great essential to be considered—the question of personality. Social nursing differs from all other branches of nursing, since in this specialty there is a wider departure from the routine and mechanical duties which form so large a part of nursing work. Those qualities which make a good institutional, or a good private nurse, do not necessarily make a good social or public health nurse. Something more is demanded.
Broadly speaking, apart from professional training, the more highly educated and cultivated the woman, the better will she be qualified. This, one may say, would apply to all branches of the profession, but we believe these qualities are more necessary in the tuberculosis nurse than in the operating-room nurse, for example. The latter does work which demands mechanical quickness 17and coolness; the former requires a personality capable of dealing with human beings in all stages of refractoriness, over whom she has no authority, but from whom she is expected to obtain results. As every one knows, it is far easier to deal with things than with people.
The qualities of a teacher are requisite. No matter how well one may know a subject, if one cannot present it clearly and impressively, small progress will be made. Nor is it the patient alone that the nurse is called upon to deal with. Her activities bring her into close relations with physicians, social workers, politicians, boards of directors, and “benevolent individuals” of all classes, whose interest and good-will it is necessary to secure. She must be as well able to meet people of this sort, as to teach the humblest patient in her district.
Since this is social work, the so-called social virtues are a necessity—and these exclude a bad temper or a quarrelsome disposition. It is as essential to work in harmony with other social workers as with the patients themselves—the two relationships are interdependent.
Needless to say, a nurse who cannot get on with her patients is a failure. No matter how experienced she may be, or how well trained, if she cannot gain the confidence and friendship of her 18families she is unfitted to deal with them. It frequently happens that for the first few visits a family may be uncordial and suspicious, but within a short time a well trained, sympathetic nurse should be able to change this attitude into one of confidence and appreciation. A few, a very few families remain unchangeable of course, but their number is so small that they form a negligible quantity.
Neither should a nurse fraternize with her patients. Through familiarity she loses the personal dignity which means so much to her authority. Authority is a term somewhat subtle in its definition—it means that hint of power, of sureness, of knowledge, which enables one to speak with a confidence which transmits itself to others, and compels them to accept one’s point of view. A strong personality easily conveys this sense of authority, but it may also be conveyed by a personality less strong, when the nurse is well assured of her facts and cannot be caught tripping. It is the hall-mark of the successful teacher—this ability to impress her points upon others, and to make them see that what she proposes is right, reasonable, and advantageous.
It seems hardly necessary to speak of the qualities of honesty, loyalty, and conscientiousness. 19When they are lacking, all or any one of them, the nurse is useless. The nurse is alone in her district all day long, from early morning till late in the afternoon, and she must be a woman with a high sense of responsibility and worthy of her trust. Patience, that despised virtue, is also an essential part of the nurse’s equipment, for she must listen to long details of illness, and must be willing to reiterate, over and over again, without show of annoyance, the rules which have been needlessly and exasperatingly ignored. No one knows better than the nurse the awful hiatus that exists between preaching and practising—the glib promise and the broken pledge—but she must never show her irritation. We have known many excellent nurses who gave up this work because they could not stand discouragement of this sort, and who had not vision enough to look into the future for results.
This standard of requirements may seem high, but it is not impossible. In fact, it is the minimum from which successful work can be expected. A superintendent who has a choice of nurses will of course approximate it as nearly as possible, in choosing her staff. The higher and finer the type of woman, the more valuable she will be—probably in no other field do fine instincts and fine feeling tell so strongly.
Salary—Increase of Salary—Carfare—Transportation—Telephone—Vacation—Sick-Leave—Uniforms—Badges.
Salary. A good nurse should command a good salary—she is worth it. There is a tendency to underpay nurses even at the present day, because of the tradition handed down from the Middle Ages, that nursing service should be given largely as a matter of love or charity. A woman who gives up her whole time to district nursing, doing highly specialized work, should at the very least receive a living wage. Associations are often asked to supply nurses at a salary of forty or fifty dollars a month, and surprise and indignation have been expressed because such a woman was not forthcoming. Salaries should be large enough to attract and retain efficient women; a small salary does not attract desirable applicants, as a rule, and this limits the field of selection. Large sums are appropriated for hospitals, sanatoriums, dispensaries, and physicians’ services, but retrenchment takes place when it comes to the nurse. Her work seems to be the one point where economy prevails.
21In Baltimore, the staff nurses are paid seventy-five dollars a month, and this is the very least that any woman should receive. A small town or country community would doubtless have to pay more than this, especially if it looks to the city for an experienced nurse. The reason is simple enough—other things being equal and the character of work the same, one would hardly expect a nurse to prefer an unknown locality, away from home and friends, unless some extra inducement were offered. A nurse might be willing to organize work in a small city, at a low salary, for the sake of the experience. In that case, it is the experience which offers the inducement. This once gained, however, she would shortly be in a position to demand more salary or seek a wider field of service.
Increase of Salary. The question constantly arises whether or not it is well to increase the salary of the staff nurse from year to year. If she enters the work at seventy-five dollars a month for the first year, is it well to increase this to eighty dollars a month for the second year, eighty-five dollars the third, and so on till a definite maximum has been reached? To this question there are two answers.
Undoubtedly a nurse becomes more valuable as her experience ripens. Her first six months on 22duty are largely spent merely in acquiring rudimentary knowledge concerning her work. As she learns to know her district, her patients, the doctors, the institutions, the social workers, her value to the community increases. Each succeeding year, therefore, which increases her knowledge of social conditions, should make her in so far more valuable. It would seem but just, under these conditions, that her remuneration should be raised accordingly. But at this point there enters a factor which we must recognize. To specialize in tuberculosis work makes peculiar demands upon one’s strength. Quite apart from the physical strain, which is always great, it demands the expenditure of a vast amount of nervous force, required in the constant combat with opposition. For this reason it is peculiarly wearing and exhausting. Also, by its nature, it tends to become monotonous. These two factors—one of which tends to wear out the individual, the other to make her indifferent and stale—make us hesitate to say that the nurse’s value keeps increasing year after year. It undoubtedly does increase up to a certain point, but after that point has been reached, it tends to diminish. Such being the case, the obligation of raising the salary is debatable.
Two kinds of nurses are usually found on the 23staff. One is the ambitious nurse, who comes for the experience and training, to fit herself for an executive position elsewhere. To such a woman, the routine of field work will not be desirable for long—not for more than a year or two, or until she has gained enough experience to prepare herself for a wider field of service. That point being reached, her executive ability will seek an outlet in work where she herself may become the organizing and directing force. To such a nurse, salary increase will offer no inducement, since she will seek that increase through work which provides greater opportunities and responsibilities.
There is another sort of nurse on the staff however, who has no such ambition; no executive ability, no desire to occupy any other than a subordinate position. This one will never venture into a position of responsibility, such as her experience might warrant, but prefers instead the easier path, choosing to be guided rather than to guide. She prefers to work under direction, rather than to direct others. To such, an increase in salary would seem but a just reward for faithful service. But, as we have said before, the monotony of tuberculosis work tends to produce stale workers. There is danger, after a time, that the first alertness and energy may wear off, the nurse may settle 24down into a rut, and her daily task, though faithfully performed, tends to become one of mechanical routine.
One of the chief duties of the superintendent is to train new nurses, and she should renew the personnel of her staff whenever the welfare of the work demands a change. Sometimes, when a nurse shows flagging energy and interest, sufficient stimulus may be given by removing her to another district, where she will encounter new patients and new problems, and so regain her old keenness and ability. When one once becomes thoroughly tired of this work, however, it is unwise and futile to attempt to continue it. Therefore, in the interest both of the nurse and of her work, it does not seem wise to offer inducements for prolonged service, unless the individual characteristics of any given nurse make this wholly desirable.
Carfare. In addition to salary, a reasonable sum of money should be allowed for carfare. This allowance should vary in accordance with the territory to be covered, those nurses who visit in smaller areas naturally having a smaller allowance for the purpose. While economy in this matter is always necessary, it must be remembered that undue economy in carfare is wasteful of something still more important,—the nurse’s time and 25strength. If she is obliged to walk long distances between cases, this will greatly reduce the number of visits she can make in a day. Moreover, she will spend so much energy in mere walking that she will become too tired for effective teaching. Only fresh, energetic people can teach; those who are physically tired are apt unconsciously to let the obstinate patient have his own way.
Transportation. In small towns and country districts the problem of transportation is often a difficult one. There are either no street cars, or their service is very restricted and inadequate. Under such circumstances it will be necessary to provide the nurse with a horse and runabout, especially if she is expected to cover a large territory. Unless there is proper provision for transportation, it will be impossible for her to visit the patients often enough to make any impression,—her teaching will be laid on too thin to have much value. And to depend upon haphazard, volunteer offers of transportation is almost as bad as to expect her to make her rounds on foot. She should be given proper facilities for going from case to case, and should be able to plan a day’s work unhampered by any considerations as to if or how she can reach her patients.
Telephone. In making up the budget of necessary 26expenses, a reasonable sum should be set aside for telephone calls. The nurse has constant occasion to communicate with doctors, institutions, social workers, and so forth, and this item of expense should not come out of her own pocket. A careful weekly account of all expenditures, including telephone calls and carfare should be rendered by her.
Vacation. A vacation of at least one month should be given during the year. Less than a month is not sufficient time in which to recover the physical and nervous energy expended during the rest of the year. This holiday should be taken all at one time, rather than split up into shorter vacations, taken at intervals throughout the year. We all know that a week or two is not sufficient time in which to restore a thoroughly tired person; at the end of such a short period, one is just beginning to feel rested, and there has been no margin left over for amusement, which is a necessary part of all holidays.
Strong emphasis must be laid on the fact that if a nurse expects to return to her work and continue it successfully for another year, she should use this vacation as a means of fitting herself for another year’s close contact with an infectious disease. She should return to work thoroughly rested, with 27her resistance increased by rest and recreation, not lowered by injudicious use of this time off duty.
Sick-Leave. While a nurse is supposed to be sufficiently well and strong to go on duty every day, in all weathers and at all seasons of the year, a reasonable allowance for illness should nevertheless be made. Two weeks’ annual sick-leave is a good allowance. If a woman is off duty for longer time than that, needless to say her work must suffer and her patients must be neglected. If a nurse is constantly off duty for small ailments, this shows that she is not strong enough to undertake this arduous work. A fixed allowance for sick-leave, therefore, will tend to work automatically, and will eliminate the unfit, whose burden of work is otherwise added to that of the steady working members of the staff.
In the case of acute illness, such as typhoid fever or appendicitis, it would be perfectly possible to appoint a substitute until the nurse was able to resume her duties. If no time has been taken off for sick-leave during the year, the two weeks should be added to the time granted for vacation. If exceeded during the year, the salary for every day thus lost should be deducted from the monthly salary. This procedure may seem harsh, but with a large staff it is necessary. It places a double 28incentive on keeping well, and nurses who would otherwise have been thoughtless and careless as to their health, will take excellent care of themselves, in order not to lose one day of their coveted vacation.
In Baltimore, the municipality gives two weeks’ vacation, and two weeks’ sick-leave. If the sick-leave is unused, a reasonable vacation is the result.
Uniforms. The question as to whether or not a nurse shall wear a uniform is one which usually excites much discussion. The one or two disadvantages of such a dress are more than offset by the numerous reasons in its favour. Two objections are usually raised to wearing it: by the nurse, because it makes her conspicuous; and by the patient, because the uniform makes him a target for neighbourly gossip.
Let us consider the first objection, that made by the nurse. A nurse does not feel conspicuous when on duty in her district. Her busy, daily routine, taking her in and out of homes where she is needed, soon causes her to forget her personal appearance. A self-conscious woman is hardly the right sort for this work. The only rub comes when she is off duty and going to and from her district, but this cannot be held to constitute a serious objection.
29As for the patient’s objection—he would be equally conspicuous if regularly visited by any woman unknown to the neighbourhood, no matter how attired. Prying eyes would recognize her as an alien, and the neighbours would speculate accordingly. We have often heard of patients who for fear of what the neighbours would say objected to being visited by agents of the Charity Organization Society. Yet the agents of that Organization wear no sort of uniform. The truth is, it is usually really the visit itself which is objected to, rather than the costume of the visitor—the costume merely serving as an excuse. On analysing the objections of a group of patients who disliked the uniform, they were found to be, without exception, patients who strongly resented every suggestion made to them. Their one desire was to be let alone, to be as careless as they chose.
On the other hand, the advantages of the uniform are many. In the first place, all effective care given to a consumptive has to include nursing as well as teaching. Now, one can “educate” in a woollen dress, but one certainly cannot give bed-baths in anything but a cotton dress, which can be plunged into a tub and washed. And whether she enters the home to give a bed-bath, or whether she goes in merely to distribute prophylactic supplies, the 30fact remains that a nurse spends some eight hours a day in contact with an infectious disease. Good technique demands that she be dressed in washable material.
In summer, a dress of washable material is not conspicuous. In winter, it may be covered with a long coat. And if we admit that such a dress is necessary, what objection can there be to making it of simple and uniform design? A single nurse so arrayed looks neat and business-like; a staff of nurses looks equally so. Moreover, uniformity of dress suggests uniformity of method, standard, and character of work, and hence inspires confidence. A staff of nurses, each one dressed according to the hazard of her own fancy, would hardly create the same impression.
In itself, the uniform is a protection to its wearer. It enables her to go freely and without molestation into all kinds of tenements and lodging houses, into side alleys and back streets. The well-known dress surrounds her with recognition, affection, and respect.
The uniform is also of value to the patients and to their friends. It enables them to recognize the nurse as she passes, and to call upon her as she goes by.
The uniform worn in Baltimore consists of a 31plain shirtwaist suit, worn with white linen collar and black necktie. The dress is made of blue denim, such as is used for overalls. Denim of this sort has two sides, a light and a dark; the dress is made up with the light side out, as in washing it seems to “do up” better than the darker side. Black sailor hats are worn, and in winter long, dark coats protect the dresses. This uniform is not necessarily the last word as to what a uniform should be, but it is simple and inexpensive, and the nurses look well in it.
Badges. The staff of a municipal nursing force is usually provided with badges to denote that they are connected with the Health Department. These badges should never be worn conspicuously, although they should be readily accessible. They are only occasionally needed, however, as when entering some lodging or rooming houses, or houses of prostitution, or other places where there may be marked opposition. To show them when entering a private home would be bad policy. A nurse usually enters a private house as a friend, but a public house she is sometimes obliged to enter in her official capacity. In dealing with all her patients, however, no matter where they are situated, the less show made of officialdom the better. By the time her patient finds out that she 32is connected with the Health Department, she should be already firmly established as his friend, and then the discovery will have no terrors. Indeed, at that stage, it very often enhances her value, and patients often feel intense pride at being visited by the “city nurse.”
Object of Work—Districts—Hours on Duty—Number of Daily Visits—The Nurse’s Office—Lunch and the Noon Hour—Bags—Prophylactic Supplies—Cups, Fillers, and Napkins—Disinfectant—Waterproof Pockets—Books of Instruction—Stocking the Bag and Distributing Supplies—Nursing Supplies.
Object of Work. The object of tuberculosis nursing is the home supervision of all persons suffering from pulmonary tuberculosis. This supervision should include patients in all stages of the disease, and not be limited to those who are in some particular stage, such as early, in contradistinction to advanced, cases. No organization which expects to do effective work should deal with one class of patients alone, since the boundary lines between the different stages are constantly shifting; the ambulatory case of to-day may be the bed-ridden case of to-morrow, and vice versa, and any attempt to limit the nurse to one class or the other would mean neglect of both. Unless the work is planned on such inclusive lines, it will be necessary to place a second organization in the field, to care for those cases 34which have been thrown out by the first. Policy of this sort would mean a number of similar organizations, duplicating and overlapping each other’s work at every turn. Thus, in the same household, we should see the early, ambulatory patient “advised” by the nurse of one organization, while the advanced, bed-ridden, more infectious case is being bathed and cared for by the nurse from another. Invidious comparisons would doubtless be made by the family, with the decision in favour of “deeds, not words.” True, there would be co-operation between these two societies,—which would mean, as a rule, double work, duplication of visits, endless transferring of cases backwards and forwards, and opening and closing of records. From whatever point of view we consider it, this is a very poor plan of work, and a wasteful method. The nurse should be in a position to follow the fortunes of her patients for months and years. Any scheme which involves transferring him to a stranger, from an old friend to a new, at the moment when he slips from an early into a most infectious stage, is to lose sight of him and of his family at a most critical time.
Adequate supervision means that the nurse must teach, nurse, and ferret out patients, and her patients must include advanced, early, and suspicious 35cases. The care should be of two kinds—instruction as to the nature of tuberculosis, with general teaching along the lines of prevention and prophylaxis; as well as actual nursing service, rendered to advanced and bed-ridden cases. The Baltimore nurses take charge of all tuberculous patients, in whatever stage, and we feel that this is the most effective way to carry on the work.
Districts. A small town, of course, constitutes but one district in itself. A larger town may be divided into two or three districts; a city, into as many as may be necessary. The principles upon which the work is conducted are the same in each case. The nurse is responsible for every consumptive in her district, and her constant endeavour should be to bring under supervision every case of tuberculosis that exists. She must visit all patients referred to her—give them instruction, prophylactic supplies, and nursing care; unearth suspicious cases and send them to a physician for diagnosis; secure hospital or sanatorium treatment for those who are eligible, and arrange all details connected with their admission. To accomplish these duties, she must know the physicians of her district, the dispensaries and institutions where she may send her patients, the philanthropic or relief-giving agencies whose aid is so often needed, 36and all social workers whose co-operation is necessary for the furtherance of the work in hand.
Hours on Duty. Eight hours should constitute the working day, from eight or nine in the morning, till four or five in the afternoon. With a large staff, the day will probably not begin till 9 A.M., while a single nurse, in a small community, may prefer to begin earlier and so finish earlier, especially in summer. It is a mistake to work overtime, no matter how interested and enthusiastic one may be. A peculiarity of tuberculosis work is its unending character—there is always more to do than can be crowded into the longest day, and even after working ten, twelve, fourteen hours, one would always feel that some important thing was being left undone. It is well to recognize this fact in the beginning, although the temptation to make “just one more” visit is often hard to resist. The nurse who habitually works overtime only wears herself out the faster, and in the end her patients will suffer through her loss of health and energy.
Number of Daily Visits. This is a variable factor, and depends in great measure upon the size of the district, as well as the number of patients it contains. The character of the service rendered also determines the number of visits, as 37new patients and bed-ridden patients always demand considerable time. If a nurse calls on ten patients in a block, and finds none of them in, she naturally can make more visits than when compelled to spend a long time in each house. As in everything else, it is the quality that counts, rather than the quantity; the day which shows few visits may have been spent more profitably than that on which she scored a high total. There is no general rule as to a nurse’s capacity, yet it is always well to suspect the value of a large total of daily visits; if a nurse dashes in and out of a house, spending but a few moments with her patients, she has probably done her work so superficially that nothing has been accomplished.
On the other hand, some nurses pay far too few visits because they have no head for planning their work, but linger, past all necessity, over unimportant details. To judge if a district is being properly visited, the superintendent should know the district, and she should also know her nurse’s capacity. To estimate the value of the day’s work by the number of visits alone, is like those societies who reckon their value by the number of pieces of literature they distribute, totally regardless as to whether any of it bears fruit.
Roughly speaking, each patient should be visited 38once a week; failing this, once every ten days or two weeks. In a few exceptional instances, this time between visits may be still further extended, but this should happen only when the patient is doing extremely well, following all the rules, and giving efficient and intelligent co-operation. There are not many patients in this class—for the average, supervision to be adequate must be frequent.
Very ill patients, however, must be seen two or three times a week—every day would not be too often, did the work permit. Unfortunately, if the visiting list is large, these sick patients can be visited only at the expense of other cases better able to take care of themselves. For this reason, the visits to ambulatory patients may become as infrequent as once every three weeks. If the visiting list grows so large that these infrequent visits are all that the nurse can give, then her instruction is laid on so thin as to be nearly worthless, a condition of affairs which calls for another nurse.
The Nurse’s Office. An office is a necessity for the nurse as a place where she may keep her nursing and prophylactic supplies, and at which she will report at certain hours of the day, say at 9 A.M., at lunch time, and possibly again in the afternoon before going off duty. At certain specified hours, therefore, it will be possible to reach her, 39either in person or by telephone, and her office hours should be known to doctors, social workers, patients, or to any who have need to call upon her. In a small town or country district, there will of course be only one office, but in a city it will be necessary to have several branch offices, accessible to the nurses of the different districts. These branch offices should be situated on the border lines of two or three adjoining districts, so that one office may be used in common by several nurses. In a city there is also the central office, from which the superintendent directs the work, and where the staff nurses report daily.
In Baltimore[2] these branch offices are usually in the same building which houses a branch of the Federated Charities, the branch office of the Visiting Nurse Association, the Infant Welfare Association, and other similar agencies. In this way, the various social workers learn to know each other, and to secure close co-operation and understanding. The different agencies, however, each have their separate rooms or offices.
2. Baltimore is divided into sixteen nursing districts, with eight branch offices or sub-stations, for the use of the sixteen nurses.
The nurse’s office should be simply but comfortably furnished. It is used for several purposes—as a store room for supplies, and as a rest room, 40where she takes her lunch and spends an hour off duty in the middle of the day. The furniture should consist of a large writing table, which may also be used for a dining table; chairs, a lounge or couch, and a small gas stove or Bunsen burner for cooking simple meals. If there is no available closet, there will have to be a commodious cupboard for storing the prophylactic supplies. A large stock of these must always be kept on hand, so that the nurse may refill her bag before starting out again on her afternoon rounds. A telephone in the office, or at least in the same building, is of course necessary.
Lunch and the Noon Hour. It is not within the province of a superintendent to dictate to her nurses as to what they shall eat. The association, be it private or municipal, furnishes the office and the hour, but the nurse must provide her own lunch and select it according to her fancy. A word, however, in regard to this lunch. It should be as nourishing as possible, and should consist of such wholesome food as eggs, milk, cocoa, and so forth. If a nurse substitutes a pint of milk for a cup of tea or coffee, she is wise.
In addition to nourishing, wholesome food (in contradistinction to unprofitable pie and buns from the neighbouring bakeshop), a short period of 41relaxation on the lounge or couch is a wise way in which to spend a portion of the noon hour. In dealing with tuberculosis, food and rest are necessary to keep one strong and well, and no nurse can afford to trifle with her health when engaged in this serious work. On no account should the noon hour be cut short, no matter how little tired she may be. Better work can be done if one is well fed and rested.
Bags. The association which employs the nurse should also provide her with the bag for carrying the supplies. The kind of bag needed is a much discussed question. It should be strong, even though this necessitates its being heavy. There is no other way out of it—for unless the bag has the first qualification, strength, the weight of the supplies will soon wear it out. Very light bags are not practical.
The bags used in Baltimore are made somewhat like the ordinary Boston bag, about fourteen inches long, and of good black leather. They weigh a few more ounces than those used by other associations, but they last longer. It must also be remembered that the bag used by the tuberculosis nurse, no matter how heavy it is when she starts forth on her rounds, grows lighter and lighter as she goes from house to house, leaving the supplies. 42Thus, at the end of the day, when she is most tired, it is practically empty.
Prophylactic Supplies. The prophylactic supplies used for the patients consist of tin sputum cups, cardboard fillers, paper napkins, waterproof pockets, disinfectant, and books of instruction. The first three are of primary importance. The Health Department of a community usually provides these supplies, even when the nursing work is carried on by a private association. Thus, in Baltimore, where for six years the tuberculosis work was done by the Visiting Nurse Association, an arrangement was entered into between this Association and the State Board of Health, according to which, the latter paid for and provided the supplies which the nurses distributed. The only condition imposed was that each case should be reported to the Health Department, and that the Health Department should be constantly advised as to the number of cases under supervision. If no such arrangement is possible, then the private association supporting the nurse must be put to the additional expense of buying the supplies.
It is impossible to make the patients themselves pay for them. Naturally, they consider them a nuisance and a bother, and it is difficult enough to 43persuade them to use them, even when given free. The cost is not great, however.
| Tin sputum cups, (in lots of 5000) | 7 cents apiece. |
| Fillers, (in lots of 1,000,000) | $3.50 per thousand. |
| Paper napkins, (in lots of 5,000,000) | $.55 per thousand. |
| Disinfectant, | 10 cents a bottle. |
| Waterproof pockets | 4 cents apiece. |
| Books of instruction | 2 or 3 cents apiece. |
Disinfectant. The most expensive of the supplies is the disinfectant, which is also probably the least valuable. That used in Baltimore is a special preparation, consisting largely of creolin; it is put up in pint bottles by one of the large wholesale drug houses. For use, it is diluted in water, a tablespoonful to a pint, and used in wiping up floors, furniture, and so forth. It is of necessity too dilute to have much germicidal action, and the patients place far too much reliance upon its odor—which, to the ignorant mind, is of prime importance. Although we use this disinfectant, we prefer to teach our patients that better results may be obtained by the lavish use of hot water, brown soap, and a scrubbing brush, and that thorough cleaning of this kind is of more value than the most malodorous drug ever dispensed. Disinfectant to be of real use must be strong and powerful, and it is dangerous 44to distribute such powerful drugs promiscuously. Several of our patients have tried to commit suicide by drinking even the weak preparation that we gave them. On the whole, we believe that an anti-tuberculosis society would lose nothing by omitting disinfectant from its list of prophylactic supplies, and better results could be obtained by substituting a thorough grounding as to the value of soap and water.
Waterproof Pockets. These are little calico bags, dipped in paraffin, or some similar preparation which makes them fairly waterproof. These are pinned inside the coat pocket, and the patient uses them as a receptacle for his soiled napkins, when he is out on the street, or in other places where he cannot carry his sputum cup. The napkins are burned upon his return.
Books of Instruction. These little books are more or less valuable, but are by no means intended to take the place of the verbal instruction which it is the nurse’s duty to give. They serve merely to refresh the memory after she has gone. They can be procured at small cost through the various anti-tuberculosis organizations, and most Boards of Health print them for their own distribution. The best of them are inadequate.
Stocking the Bag and Distributing Supplies. 45When the nurse starts forth on her morning rounds, her bag should contain enough supplies for the patients she proposes to call on. Each should be given enough to last until her next arrival. It is sometimes possible to direct either the patient himself, or some member of his family, to come to the office and get a fresh stock whenever necessary. By putting this slight responsibility on the family, it is made to realize how necessary are these supplies, but it should not relieve the nurse of her obligation to visit such a household, and keep it under as close observation as any other case. If a nurse thus trains a certain number of patients to come themselves for the supplies, she will be able to reserve the contents of her satchel for those patients who cannot call for them, or who are too indifferent to do so.
Supplies should always be given out freely, and the patient should not feel that he is put under any obligation by accepting them. They are intended for his personal use and convenience, and he should be made to realize this. Otherwise, some patients may hesitate to accept all that they really need. If a patient needs four or five fillers a day, he should unquestionably have them—otherwise he may practise small economies which will mean unnecessary exposure for his family. On the 46other hand, the nurse must see that the supplies are used for the purpose intended—we have sometimes known handkerchiefs used as a decoration for kitchen shelves, simply because the nurse had given away far more than was necessary.
Nursing Supplies. In addition to the prophylactic supplies, the bag also contains a number of articles used in caring for bed-ridden or very ill cases. Naturally, these articles are not given to the patients, but are used from case to case, as necessity arises. They include a bottle of alcohol, boracic ointment, talcum powder, gauze, adhesive strapping, absorbent cotton, and a thermometer. The nurse should always carry an apron, to be worn when doing any nursing work.
The most common dressing is that of bedsores; many patients with pleurisy have to be strapped; others have drainage tubes, which must be taken out and cleaned. These extensive dressings are not those which the nurse should properly be required to attend to, since a patient ill enough to require an extensive dressing, is a patient who should be sent to a hospital. Hospital accommodation, however, is unfortunately very limited, and the nurse is often obliged to do these dressings while waiting for a vacancy to occur. It is no part of the programme to keep these advanced cases at home 47rather than in an institution; on the contrary, the nurse must make every effort to get them away—but until this can be accomplished, it is her duty to care for them at home.
Records and Reports—The Patient’s Chart—Closing the Chart—The Card Index—Nurse’s Daily Report Sheet—Weekly and Monthly Reports—Examination of Charts.
Records and Reports. Every association, whether it be private or municipal, supporting one nurse or fifty, should keep careful records concerning its patients, and concerning its nurses’ work. These two sets of records should dovetail and form a cross file; by looking at the patient’s chart, one should be able to note the condition of each individual case, and how often and on what dates he was visited. By looking at the nurse’s record, one should be able to know exactly how she had employed every moment of her day, and to see the number of patients she had visited during the course of it. The patients’ charts account for the patients—the nurse’s daily report accounts for her work among them.
The Patient’s Chart. Each patient should have a chart made out for him at the moment when he is taken on the visiting list. This also applies to suspects, 49or those for whom the diagnosis is not positive, but whom the nurse is required to visit and care for. This also applies to those moribund patients, who may live but a few hours after being reported, and who die before a second visit can be made. Whether he has been on the list a year or an hour, it is necessary to account for every patient who passes under supervision, and to record the result in each case. Unless this is done, accurately and promptly, it will be impossible to estimate the amount of work, and its value to the community.
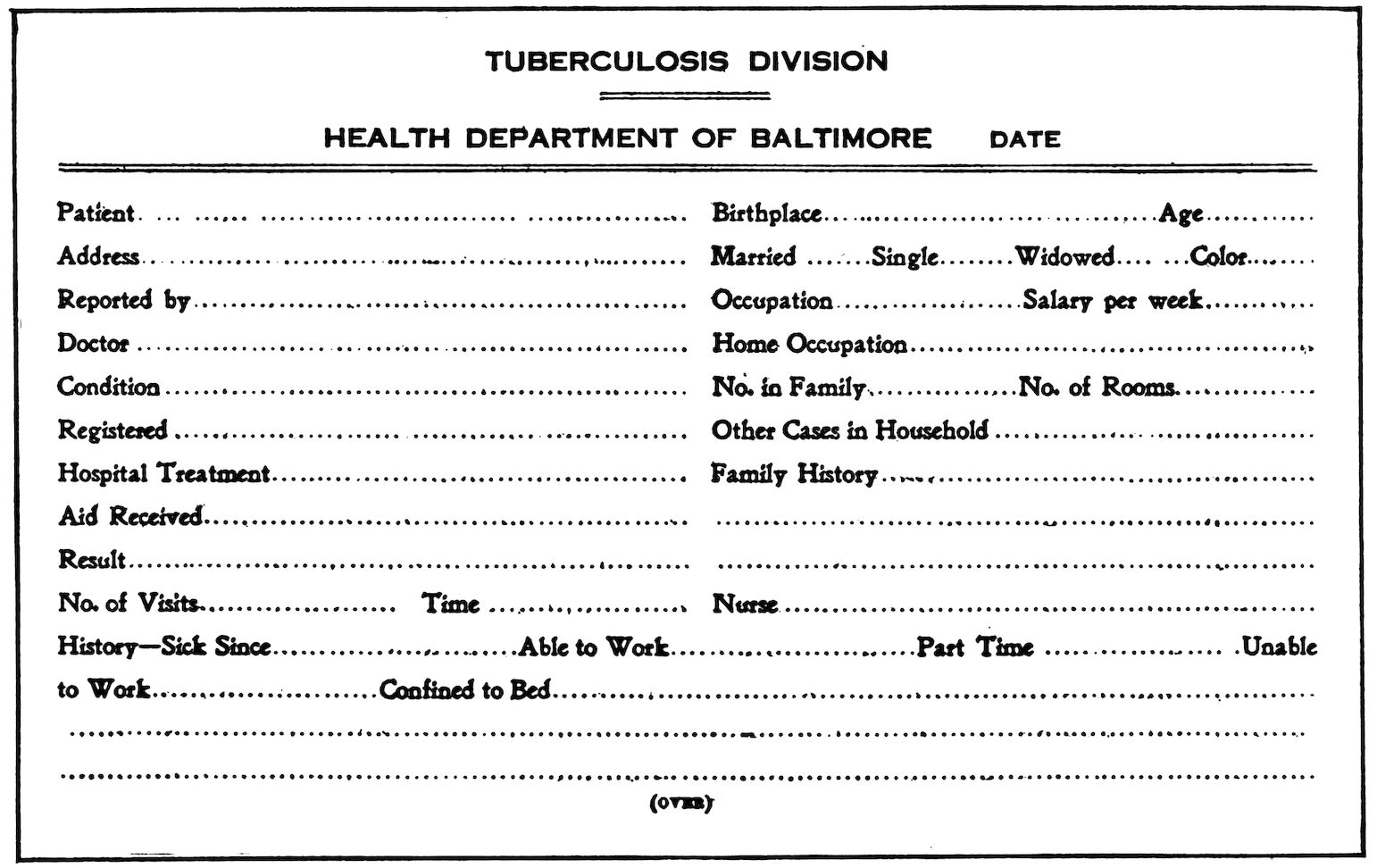
The patient’s chart should contain name, sex, age, colour, address, occupation, social status (married, single, or widowed), and a brief history concerning the onset and progress of his disease. These charts may be as simple or as elaborate as one desires. Herewith is submitted a specimen chart, such as are used in Baltimore; they are not perfect, nor the acme of all that is or might be desirable in a record of this kind, but they have proved simple and fairly satisfactory. There is much left out which with advantage might have been added, but in this connection it is well to remember that an elaborate and exhaustive history, one demanding dozens of intimate details, is apt to alarm the patient excessively. To collect exhaustive statistics would be valuable for the sociologist, but to do so at the expense of the patients’ confidence and trust would be to defeat the object of the work itself.
Patient’s Chart. Cardboard, five by eight inches
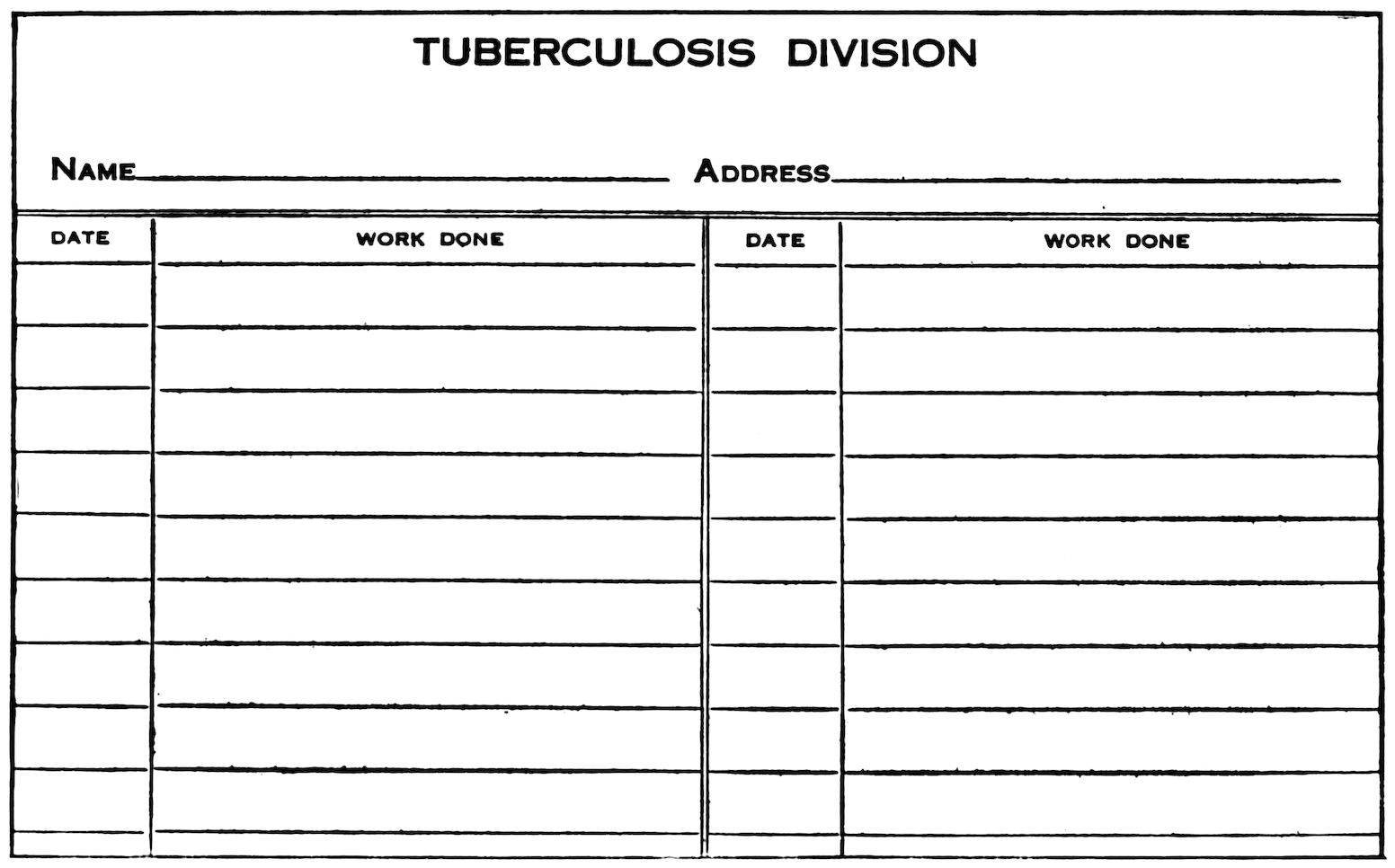
Reverse side of Patient’s Chart, showing spaces for recording visits. The Second Chart Sheets are similar to this, but alike on both sides
52The reverse side of this chart contains spaces in which each visit may be recorded. Sometimes these charts are kept up for months and years, and it is therefore necessary to have what are called second sheets—alike on both sides, and resembling the reverse side of the first sheet, which contains the patient’s history. These sheets are fastened together, and the chart of a chronic case may thus record hundreds of visits. Each nurse is responsible for keeping up the charts of all patients under her supervision. The notes should be carefully recorded at the end of each day’s work, for it is bad policy to let this charting accumulate for even two or three days. The entries should be brief and concise, and should describe the patient’s condition, or the work done for him.
Each nurse should have a filing box or drawer in which to keep these charts; they should be arranged in alphabetical order, and kept at the central office, where the superintendent may have ready access to them. These charts are the property of the association, and under no circumstances are to be removed from the central office. The nurse may make her entries upon them either at 53the end of the day’s work, or before she goes on duty the next morning.
Closing the Chart. Patients are removed from the visiting list when they die, or when they are discharged. They are discharged only for one of three reasons—either they leave the city, or they move and their address is lost, or they prove not to be tuberculous. When a patient dies or is discharged, a suitable entry is made on his chart, which is then turned in to the superintendent of nurses, or to whomever is responsible for the records. If there is only one nurse, it is of course her duty to file these closed histories. These records should be rich mines of sociological information, and should contain valuable material for those who have access to them, such as municipal authorities, physicians, and social workers. Except for the access allowed to these, the files should be confidential.
The Card Index. All offices should contain a card index, giving the name and address of each patient under supervision. Change of address should always be noted, since it is only by means of this card index that the particular chart desired can be referred to. For example: the card index contains the names of some 3000 cases, all under supervision, and each one having its own chart. 54The charts themselves, however, are distributed among the filing boxes of several nurses. If particulars are wanted concerning John Doe, it would be necessary to turn first to the card index, find his address and the district in which he lives, and then turn to the filing box of that district and take out the chart. If it were not for the card index, it would be necessary to search through all the filing boxes before finding the desired chart.
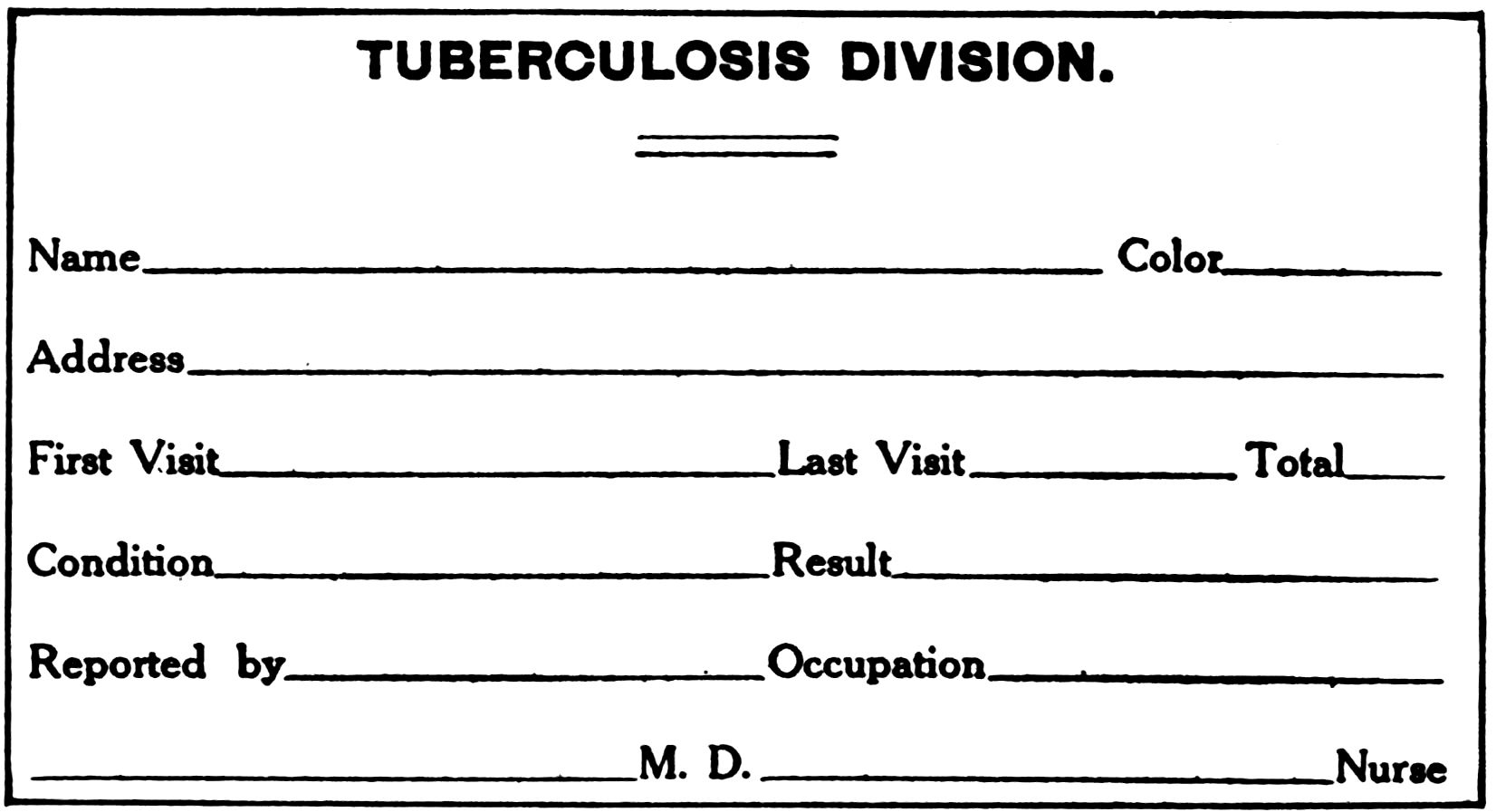
Card, three by five inches, used in Card Index
As the discharged charts are handed in, the corresponding card in the index is withdrawn and filed away in a drawer containing either the dead or the discharged cases according to circumstances. This is a very simple way of keeping records, and of balancing from day to day the number of patients on the visiting list. This balance may be made 55every week or every month, as desired, for it is a simple method and reduces to a minimum the opportunities for mistakes in addition and subtraction. Needless to say, no one but the superintendent or her secretary should have access to, or touch these files in any way.
Nurse’s Daily Report Sheet. Beside the patients’ charts, the nurse must fill in a day sheet, or daily report of her work, to be handed to the superintendent, or to whomever she is responsible. This sheet accounts for her time and occupation all through the day. Beginning with the time she goes on duty in the morning, she will record each visit to each patient, the service rendered, and the time spent on him. She will also record the time she reached her office for lunch, and the time she left it for her afternoon rounds, also the hour at which she went off duty for the day. A record of this kind means additional clerical work, but how else is the nurse to account for her day? And be it noted, it is always a satisfaction to the nurse to place on record the summary of her day’s work.
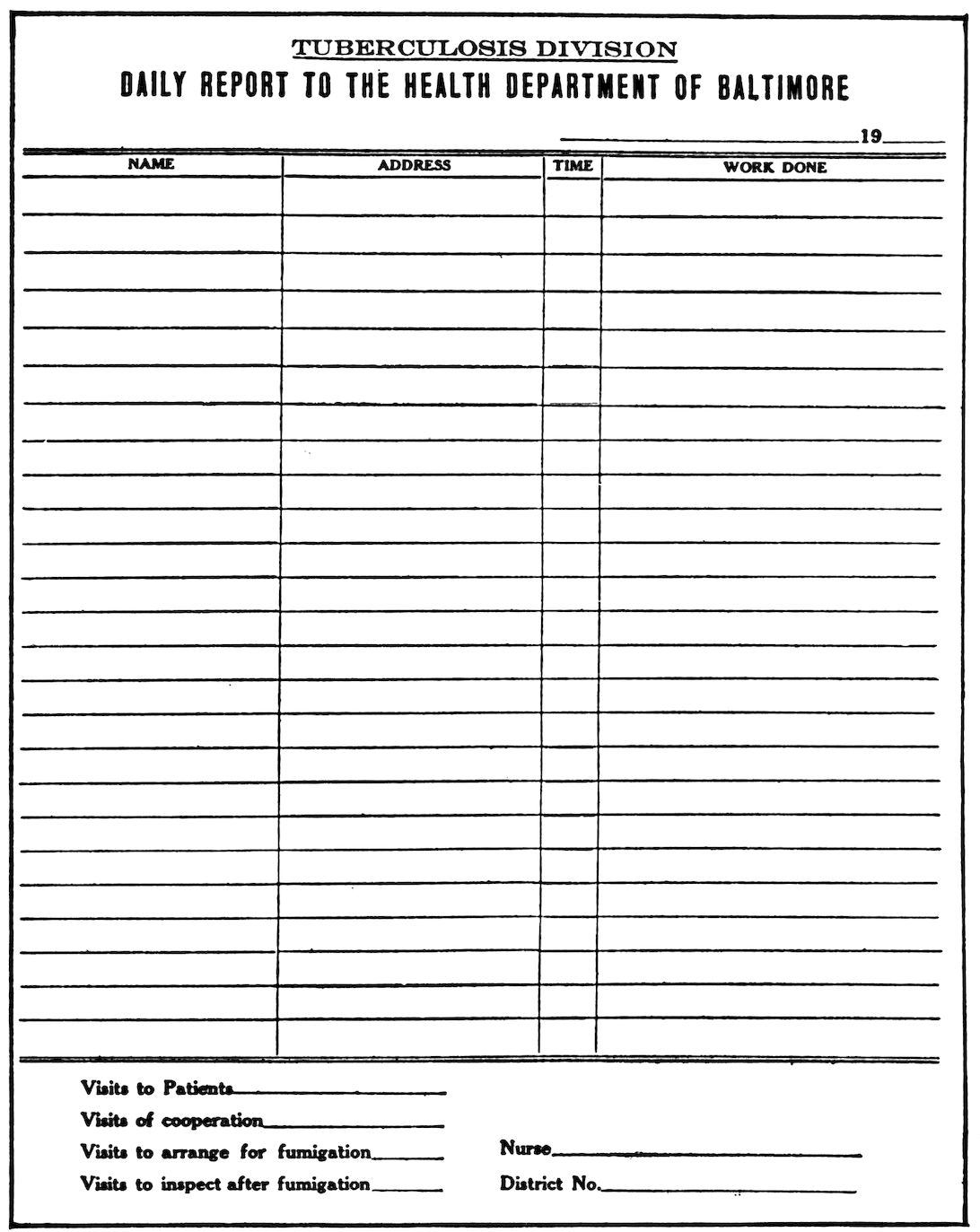
Nurse’s Daily Report Sheet, seven by nine inches
This daily report sheet is of great value to the superintendent: without it, there is no way in which she can estimate either the quality or the quantity of each nurse’s work. A glance at the report will show whether the day has been light or heavy; it will show the number of new patients and ill patients, and how many bed-baths and dressings were given; how much time was spent in calling on doctors, dispensaries, social workers, and so forth, and arranging houses for fumigation. In short, a record of this kind shows the day’s work at a glance, and is the only way in which it can be satisfactorily accounted for, and if necessary verified.
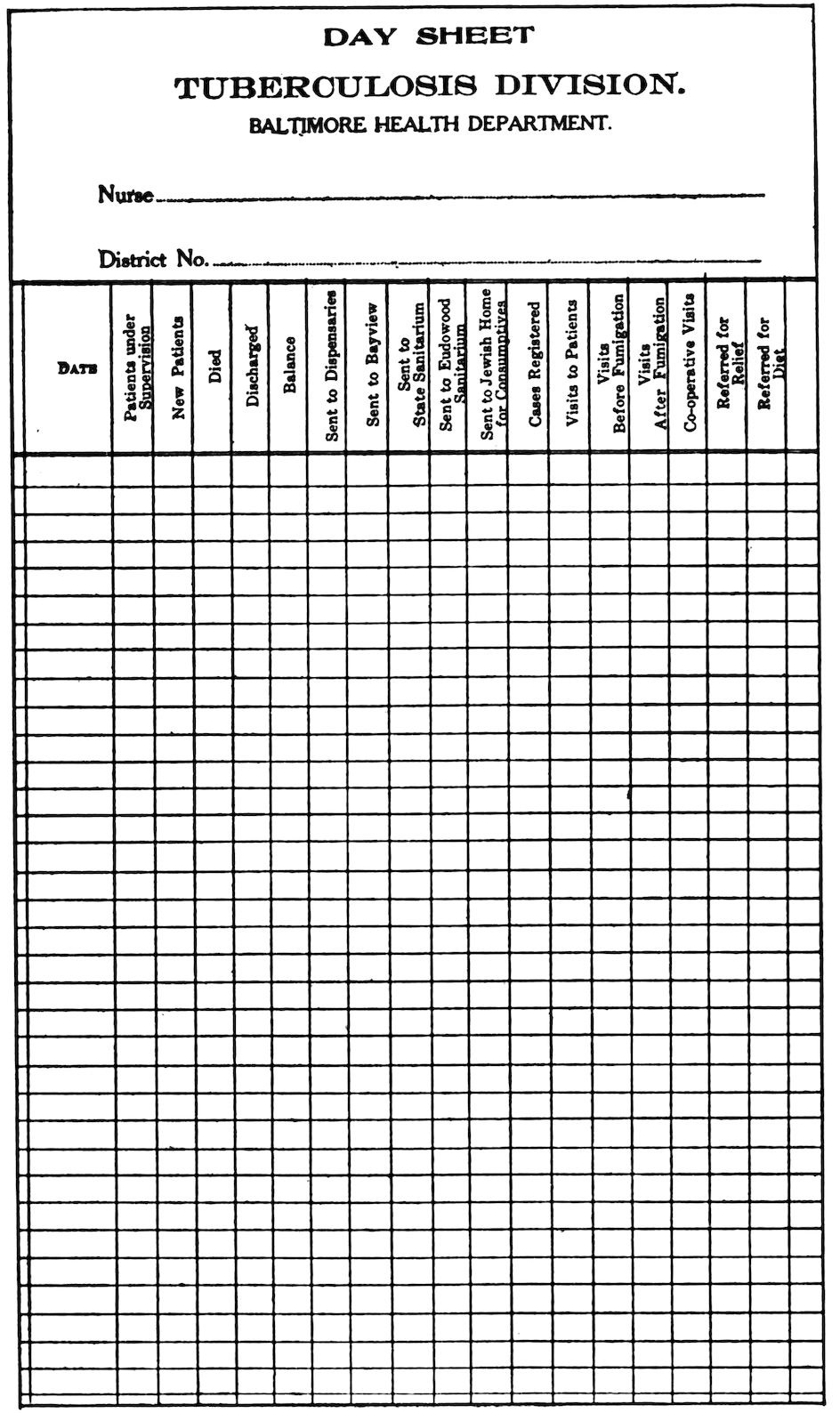
Day Sheet, used for summarizing the day’s work. From this sheet the weekly and monthly reports are made out
58True, this information may be obtained by going over the charts one by one, and verifying the records made upon them. But this is a clumsy and laborious way of doing it. If a nurse has two hundred charts in her box, and pays fifteen visits a day, it would be necessary to search through the whole boxful of charts in order to find the fifteen cases visited. A day sheet therefore, is not only a simple and practical way of recording a day’s work, but it is a protection both to the nurse and the work itself.
Weekly and Monthly Reports. From her daily report sheet, the nurse should make up a weekly or monthly report, to be turned in at specified intervals. This weekly or monthly balance sheet should be presented to the superintendent, or to the officers of the association to whom the nurse is responsible. Herewith is given a sample of the monthly report cards used in Baltimore, but again attention is called to the fact that these are not the last word in desirability. In using them as models, they would of course be altered to meet local needs or conditions, and enlarged or changed to 59suit other requirements. These monthly reports should be carefully filed away; they are needed for the construction of the annual report, and it may be necessary to refer to them on other occasions.
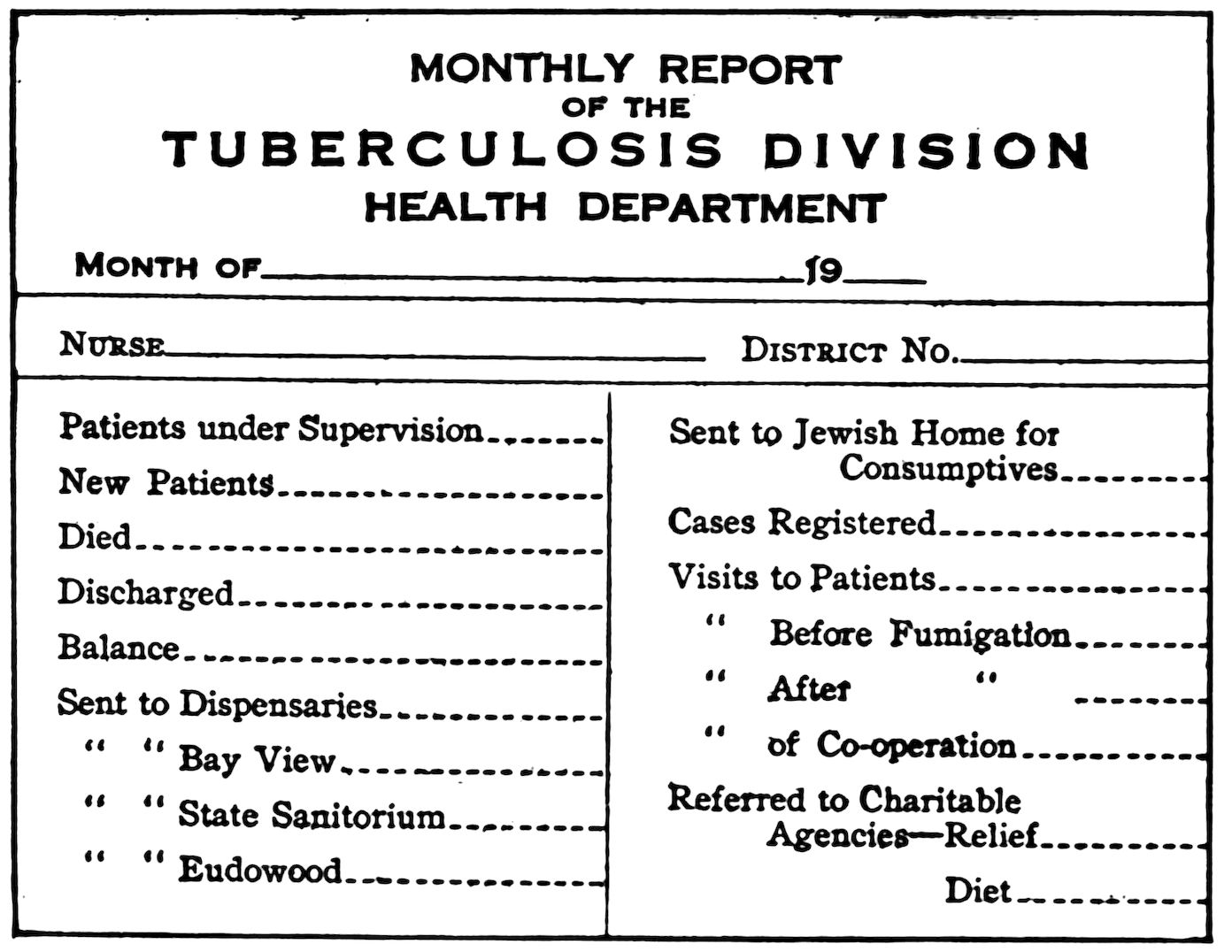
Card, four by six inches, used for summarizing the weekly and monthly reports
Examination of Charts. One of the duties of the superintendent is to examine the patients’ charts from time to time, to see how well the nurses do the clerical work, which is quite as important as the visiting itself. By carefully examining the charts, the superintendent is able to call the nurse’s attention to any lapses in them—incomplete histories, long intervals between visits, 60and so forth. If, for any reason, the nurse allows considerable time to elapse between her visits to a patient, the reasons for this should be fully noted on his chart. For example: some one wants to know when Mrs. Jones was last visited. On looking at the chart, we find the last visit was made on June first—and it is now August first. A two-months’ gap between visits looks like careless and inattentive work. The nurse, being questioned, however, is able to give a satisfactory explanation—Mrs. Jones had gone to pick berries, leaving the city the first of June, and not due to return till the first of September. This important fact, however, should have been noted on the chart, since it is almost as careless not to have made this entry, as it would have been to neglect the patient for so long a time. If a chart is to have any value, it should tell its own story, briefly and clearly.
These charts, therefore, should be examined every two or three weeks. It is the duty of the superintendent to go over these records, just as it is her duty to make rounds from time to time among the patients, and visit them in their homes. This is done by the superintendent, not in a spirit of distrust or suspicion, but because she is the person responsible for the work, and it is her duty to oversee it, and bring it to its highest degree of efficiency.
Finding Patients and Building up the Visiting List—Increasing the Visiting List—Social Workers—Dispensaries—Patients’ Family and Friends—Nurses’ Cases—Physicians.
Finding Patients and Building up the Visiting List. The first thing for a nurse to do when she begins her work in a new community is to find the patients she is to instruct and care for. And the question naturally arises; how are these patients to be discovered?
The campaign of propaganda concerning the need of tuberculosis work has aroused the interest of people of all classes. The funds to support the nurse are evidence of this. But the people who pay the bills are not those who can produce the patients. To get in touch with the patients, it is necessary to approach people of another class, those whose work brings them in contact with the very poor. For, as a rule, in beginning tuberculosis work, it is only patients of the poorest class who find their way to the nurse’s visiting list. Later, as the work becomes more firmly established, and better known and understood, her visiting list will 62include not only the poor, but those in well-to-do and comfortable circumstances.
The Board of Managers of the new association may interest themselves in finding the patients, but in the end it is the nurse herself upon whom this responsibility rests. Upon her initiative and ability depends the success of the work. Her first step, therefore, should be to call upon all those who can in any way be of service, and who can direct her to the patients she is anxious to reach. She should call upon the physicians of the community, the dispensaries and hospitals (if there are any), social workers, such as the agents of charitable associations; priests, clergymen, and all those who come into contact with the suffering and the destitute. Her visits should be made in person, since a personal interview makes a stronger appeal to the memory of the busy man than the most convincing letter or the most eloquent report. This involves one great reason why the nurse should be thoroughly equipped in character and training; the colourless, uneducated, unconvincing woman carries with her no conviction, and inspires no confidence either in herself, or in what she proposes to do. A physician may well hesitate about turning over his patients to a woman who is unable to put her case before him.
63It may be that considerable time will thus have to be spent in calling upon all those likely to know of tuberculous patients, and therefore able to furnish the nurse with the necessary names and addresses. That the response is not great should cause no discouragement. As we have said elsewhere, the tuberculosis death-rate, multiplied by five, will give a conservative estimate of the number of tuberculous individuals in a community. It is the nurse’s duty to unearth them. They exist—she must find them, and the greater the obstacles, the greater the incentive to overcome them. The total result of a two or three weeks’ campaign may be a mere handful of cases reluctantly handed over by a few physicians, and a few undiagnosed suspects, reported by an earnest priest. In this way the visiting list is begun.
Increasing the Visiting List. To increase the visiting list—that is, to bring under her care an increasingly larger proportion of the total number of tuberculous patients, even though the list becomes so large and unwieldy that she cannot manage it, should be the ambition of every tuberculosis nurse. At present, in every city in the country, there is so much undiscovered and unreported tuberculosis, that the failure of the nurse to increase the visiting list is an indication of poor 64work, not an indication that a full round-up has been made of all those suffering from this disease. This is especially true in a new community; a small or stationary visiting list is a sure sign, not necessarily of lazy or unconscientious work, but at least that the undertaking is being managed by someone who does not know how.
To illustrate this: A nurse is sent to a certain house, to see a specified patient. She does her work well—gives him a bed-bath, shows the family what to do, and makes considerable impression along lines of general hygiene. As far as it goes, her work is satisfactory and good. Another nurse, however, sent into this same house, would not only do all these things equally well, but, in addition, she would discover that the patient’s wife was coughing and probably infected, while his old mother, retired in the chimney-corner, was in even worse plight than the patient himself. These suspects, therefore, she sends to the dispensary, where her suspicions are confirmed by the doctor’s findings. Thus, if a community possesses a nurse of the first type, it may rejoice to find the amount of tuberculosis so small. If, on the other hand, it has a woman of the second type, it will become alarmed and anxious at the increasing number of patients who need care and control.
65Nothing should diminish the enthusiasm for gaining new patients. The mere fact that a nurse has more than she can manage should never deter her from continually trying to find more. More patients, more patients, and even then, more patients, should be her constant aim—and then the chances are that she has not found all that exist. In Baltimore, when pioneer work was begun under the Visiting Nurse Association, that organization had a visiting list of some 1700 consumptive patients, divided among five nurses. As five nurses represented the largest number the Association could support, and as 1700 patients was only about one-fourth of those who needed care and attention, some other method of caring for the latter had to be devised. It was at this critical moment that the Health Department was persuaded to assume the tuberculosis work of the private association, and to incorporate it as part of the city machinery. If the need for this transfer had never been proved, it is hardly possible that the change would have been made. If the first nurses had confined their visits to the patients they could reasonably manage, and had refused to accept others, it would have been impossible to prove how great the number of infectious patients was, and how inadequate the care given them by 66the five struggling nurses of the private association. Therefore, each community which undertakes tuberculosis work should endeavour to unearth all the cases that exist, if for no other reason than to show the size of the problem, and the necessity of adequate measures for handling it. New patients, positive and suspicious, should be sought for from every possible source. This is better policy than to confine the work to the conscientious care of a handful of manageable cases.
Social Workers. The agents of the Charity Organization Society, or similar associations, continually come across cases of tuberculosis. The new nurse should canvass all these agencies, and ask that all cases of this kind be referred to her. If a case is not positively diagnosed, that should be no drawback to reporting it; while the agents of these associations are laymen and therefore not able to make diagnoses, laymen, nevertheless, are able to make very shrewd guesses. It is the nurse’s duty to take charge of these doubtful cases, and get them examined and diagnosed by the proper agencies. The mere fact that a patient presents suggestive symptoms makes it all the more urgent that he be examined as soon as possible, and lack of positive diagnosis should be no reason for the agent to withhold, or for the nurse to refuse to take 67charge of, such a case. To visit a suspect does not necessarily classify him as a consumptive, while not to visit him might be to deprive him of assistance at a most critical time.
In finding cases, extensive co-operation should be invited; almost every one whose work brings him into contact with numbers of people, knows one or two among them who are tuberculous. Thus settlement workers, school teachers, school attendance officers, juvenile court officers, clergymen, Salvation Army workers, and so forth, are all people whose aid and interest should be solicited. It makes no difference whether or not the case is positively diagnosed—any sick person, with the symptoms of a consumptive, is a person whose case should be looked into. It is the nurse’s business to obtain the diagnosis.
Dispensaries. If there is a hospital or dispensary (not necessarily a tuberculosis dispensary), the nurse should visit these institutions and ask to have all positive and suspicious cases referred to her. Since the patients who come to these places are usually those of the poorer classes, the doctors will not be likely to object to giving their names to the nurse. Indeed, they may be glad to accept the assistance she offers. One visit to these institutions, however, is not enough. Every week or 68two the nurse must present herself and renew her request for patients—she must not trust to the busy physician to report them by letter or telephone. Even when tuberculosis work is conducted on a large scale, as in Baltimore, it is always part of the nurse’s duty to visit these institutions regularly, to remind the doctors of their existence and of their unquenchable desire for more patients.
Patients’ Families and Friends. After the nurse is well established, and her position in the community recognized and assured, she will find that a certain number of new cases are referred to her through the families and friends of those already on her visiting list. This is a high tribute, and should be valued accordingly. She should not rely entirely upon this voluntary assistance, however, but from time to time should question her patients, and find out whether they have any friends who are ill, who would like to be visited. Surprising revelations often follow. There was in Baltimore one old coloured woman who took special pride in discovering patients, and who made an indefatigable agent in hunting up cases in the neighbourhood. The accuracy of her diagnosis was wonderful—her son had died of tuberculosis, so she knew all the symptoms, and she did 69not refer us to a single case, which, upon examination, failed to be tuberculous. We must remember that while in its early stages tuberculosis is difficult to detect, when it is so advanced that a layman can recognize it, in nine times out of ten he is right. And as these advanced cases are the chief distributors of the disease, the alert nurse should be keen to learn of these patients through any source that presents itself. Of course many calls from such sources send one on mere wild-goose chases, but it is better to go on a dozen fruitless errands, than to overlook one real case of tuberculosis.
Nurse’s Cases. A large proportion of her cases will be unearthed by the nurse herself. In Baltimore, the nurses themselves discover nearly thirty-three per cent. of the cases under supervision. Thus, on being sent to see a certain patient, before her visit is over the nurse may discover one or two others of the family whose condition is such as to call for immediate examination. The nurse should look with suspicion upon every member of a household which has been exposed to tuberculosis. The prolonged and intimate contact which is necessary for the transmission of this disease has unfortunately, in most families, existed for months before her arrival. The nurse should be particularly keen in questioning the parents of tuberculous 70children since it is from the parents that most children contract this disease.
Physicians. In considering the various sources from which patients are recruited, we have purposely left until the last that which most people would have deemed the first and most important source of all, namely, the physicians of a community. While the medical profession has blazed the way, and has indicated the paths along which the work must be carried on, it is unfortunately only the greater men in the profession who have done this. The others, through ignorance, through indifference, or through that spirit which according to Dr. Cabot makes medicine “the greatest profession, the meanest of trades,” have succeeded in placing effective if temporary barriers in the path of the anti-tuberculosis worker. The rigid adherence to the old Hippocratic oath, by which the physician was sworn to keep inviolate the confidence of his patient, and to place foremost the welfare of the individual, has for the most part been very nobly lived up to. This oath, however, antedates our knowledge concerning infectious and communicable disease. With the knowledge as to the nature of transmissible diseases, there has come a change in medical ethics, a change manifested by laws in which the welfare of the community 71is placed above that of the individual. We see this reflected in the regulations governing diphtheria, smallpox, scarlet fever, and so forth—diseases which are distinctly the concern of the community, as well as of the patient himself. But with tuberculosis, which has but recently become recognized as a communicable disease, we find a halting reluctance to consider anything but the rights of the individual. This feeling is particularly strong among physicians of an older generation, hold-overs from a passing régime. To such as these the nurse is nothing less than an impertinence. Even if physicians of this sort are unable to see their patients oftener than once or twice a year, or know them to be in need of supplies which the nurse will gladly furnish, they refuse to call upon her, and consider her advent as intolerable.
Again, there are physicians who do not object to the nurse on this score, but who resent her as a subtle menace to their practice. They feel that if a layman is able to preach rest, fresh air, and food, and distribute prophylactic supplies, that the ground will be cut out from under them, and that they will lose a chronic and fairly lucrative class of patients. As a matter of fact, the physician who preaches this simple doctrine has nothing to fear 72from the tuberculosis nurse—if her words echo his they only add force.
There are other physicians, however, who have received an inferior medical education; they are neither sure of themselves, nor able to diagnose tuberculosis until it is in an advanced state. These object to the nurse on the ground, implied rather than expressed, that she is supervising and criticizing their work, and this self-consciousness often takes the form of a violent antagonism. It is always the badly trained physician who fears the well-trained nurse.
Furthermore, there are certain practitioners who frankly exploit their patients. They may be competent enough but they are in medicine to make a living, and are often brutally unethical as to how this is done. If through self-interest it seem best to them to withhold from the patient the nature of his disease, they do not hesitate to do so, regardless of the danger to which others may be exposed. By a strange paradox, the same profession which gives us the noblest, the most unselfish workers in the interests of public health, also gives us its most implacable enemies.
However, the new nurse must call upon all the physicians of the community, and endeavour to obtain their assistance and support. But, for the 73reasons mentioned, she must not be discouraged if she is not always cordially received by them. There will always be among them many who are enlightened and progressive, and who will assist generously in the anti-tuberculosis campaign. If a community can boast of only one or two such men, even, success is assured. And later on, as the nurse progresses quietly in her work, she will come into contact with other doctors, who promise her aid, but ignore their promises because they think she is trying to steal away their patients. As it gradually dawns on them that this is not the case, their opposition will wear off. To conquer this prejudice as soon as possible is part of the nurse’s work.
Furthermore, the community itself should not be daunted if the physicians as a body do not endorse the prospect of a tuberculosis nurse. This prejudice against public health nursing is the common experience in all cities where visiting work has been established, but it gradually wears off as the nurse is able to demonstrate her value. Little by little the doctors are won over, as they begin to realize that she is not a rival but an assistant. In Baltimore, our experience has been that those physicians who were at first our worst opponents have now become our staunchest and warmest friends.
The General Practitioner and the Public Health—Responsibility of the Private Practitioner in Tuberculosis—Impossibility of Fulfilling this Obligation—Failure because of the Nature of Tuberculosis—Failure through the Personal Equation.
The General Practitioner and the Public Health. Roughly speaking, we may say that the medical profession is divided into three or four branches—private practice, hospital or laboratory work, and public health service. A man who takes up one of these branches is not necessarily interested in or equipped for another. While all physicians are supposed to have approximately the same medical education, and therefore to be interested in those measures which tend to raise and improve the standard of public health, it is only those who are most keenly interested in this work who have made it a special study. For it must be remembered that public health work is as much a specialty and calls for as much training and ability along certain lines as laboratory work, or the administration of an institution. This being so, a man who goes in 75for it does so because he is more interested in it than in private practice, or in research work. And the converse of this is also true. The selection of one field rather than another is a matter of individual taste or inclination. Yet curiously enough, the State does not take note of this fact. It places certain obligations upon all members of the medical profession, and expects them all to live up to the responsibilities thus arbitrarily imposed.
Responsibility of the Private Practitioner in Tuberculosis. In the pursuit of his calling, the private practitioner comes into contact with certain diseases which by their nature are a matter of public as well as private concern. In so far, therefore, he is expected to interest himself in the general welfare of the community, but there is no way of compelling him to do this. The State grants him a licence to practice medicine, and in exchange for this licence or permission, he is expected to serve the State more or less gratuitously. At best, it is volunteer service, and therefore intermittent and unsatisfactory. That the State expects this service is shown by laws referring to transmissible diseases, the notification of births and deaths, and other matters which in one sense belong to his private business, but which in another sense are part of his public responsibility.
76Physicians who have no taste for research work are not forced to undertake it, nor are they coerced into any other line of service. Yet the State obliges those who are least inclined, as well as the others, to assume a graver responsibility; care of the public health. It takes no account of the many reasons which may prevent their doing this, or prevent their willingness to assume any part of this responsibility. It is thrust upon them just the same, but the expected results are not forthcoming. The State, therefore, is in the position of making an unfair demand upon the private practitioner, and at the same time relying upon an unfulfilled requirement for the security of the public health. In regard to tuberculosis, there are certain regulations which all physicians are supposed to comply with, no matter how little interested they may be in public welfare, or how unwilling to consider any other than their personal interests. These laws require, first, that all cases of tuberculosis be registered with the local or state health department, since in dealing with a transmissible disease it is necessary to learn its distribution and prevalence. Second, the physician in charge of a tuberculous patient must give this patient full prophylactic supplies, and teach him how to use and dispose of them. These supplies are furnished 77free of charge by the Health Department, so that the physician is under no expense in distributing them. Third, all houses vacated by a consumptive, either through death or removal, must be reported to the Health Department for fumigation. If these regulations could have been thoroughly complied with, they would doubtless have insured a system of complete and satisfactory supervision of tuberculosis. As it is, most of our large cities have found it necessary to place special workers in the field, to give exactly the same supervision and control which these regulations were designed to secure. The private practitioner, endowed with special education, special opportunity, and special authority, has not used these endowments, or else has used them to so slight an extent that the community has received no benefit.
If the physicians of a community have been able to diagnose tuberculosis, and have been required by law to report it, why has it become necessary to establish municipal dispensaries for this purpose? Can the dispensary physician make a better diagnosis? Or is he more willing to fill in a blank and report the case?
And if the physicians, required by law to instruct and keep careful watch over their consumptive patients, had been able to do this, why 78has it become necessary to place tuberculosis nurses in the field, designed to give just such service? Is the special nurse better fitted to explain the nature and danger of the disease? Is she a more efficient distributor of prophylactic supplies? To all these questions there should be but one answer—there is, or should be, no difference between the two. The private practitioner should be as well able to make a sure diagnosis as the municipal physician. He should be as ready to report the case. The private practitioner should be as capable a teacher, as careful a distributor of supplies, as alive to the danger of tuberculosis as the municipal nurse. The only difference between these two groups of people is that one acts and the other does not—or acts in such intermittent and irregular manner as to be productive of no results. And it is because of this lack of action on the part of the physicians in private practice, their failure to recognize, report, teach, and continually supervise consumptive patients, that our cities are placing the care of tuberculosis under municipal control. The care of tuberculosis is gradually being withdrawn from the man in private practice, and placed in the hands of specialists, who devote their entire time to the welfare of the community. And although now as always the latter solicit the 79support of the private physician, if he withholds his co-operation they can do without him, and reach their goal through other means.
Impossibility of Fulfilling this Obligation. We may ask why the private practitioner is being supplanted by municipal control. Undoubtedly he once held the key of the tuberculosis situation, as he holds it of many other problems involving the public health. He is being supplanted for two reasons: because of the peculiar nature of tuberculosis, and because of the failure of the medical profession to act as a united whole.
Failure because of the Nature of Tuberculosis. Let us first consider the nature of the disease. Tuberculosis is a prolonged, chronic disease, which may be drawn out over a period of months or years. The patient has many ups and downs, being sometimes so ill that he places himself under the care of a physician, sometimes so much better that he does not see a doctor for months. We have known patients who have not been to a physician for years, yet during that time they were infectious cases, as proved by sputum examination. During a hiatus of this kind, how can we possibly hold the doctor responsible for the tuberculous patient? How can we hold him responsible for the conduct, training, and surroundings 80of a case he never sees? Undoubtedly a very large number of patients pass completely from under the observation of their physicians, and are utterly lost to them. With the best intentions in the world, the private practitioner cannot follow and supervise a disease of this character, not acute, but chronic and ambulatory in nature. If he attempted this, it would leave him little time for anything else.
Nor can we assume that the patient who closes his account with one doctor necessarily places himself in the hands of another. He frequently drifts along without any medical advice whatsoever, and only seeks it again when his symptoms become alarming. These facts alone, exclusive of all other considerations, show the necessity for centralized control of these ambulatory patients.
Tuberculosis is largely a disease of the poor, as we have remarked before. A poor consumptive must consider the spending of every dollar, and the doctor’s fee is a matter of grave importance. For this reason, the patient will pay just as few visits to the physician as he possibly can. A doctor who sees a case only once or twice may well hesitate to pronounce it tuberculosis, and may wish to keep the patient under observation for a time, but the poverty of the patient prevents this.
Again, patients of the poorer classes continually 81change their doctors. Unlike people in more fortunate circumstances, they have no one physician to whom they always turn when in trouble. To such as these, the “family doctor” is unknown. Their fickle interest is attracted by the newest shingle, and they pay a visit or two to its owner and they depart. We knew one patient who visited five different doctors within the week. Small wonder that the doctor forgets these patients—mere transients—and that, even if he has time to diagnose them, he does not consider himself their physician, or responsible for them in any way. It is for just such cases, however—those patients who come into fleeting and haphazard relation with their physician, that municipal control is required. It is no reflection upon the private practitioner that he has failed to make headway against tuberculosis. It simply proves that people with this disease must be watched and cared for by those who are able to devote their entire time to it.
So much for the disease itself, and for the sociological and psychological conditions which complicate it, and make it a matter which cannot be handled successfully by the man in private practice. For no matter how conscientious he may be, or how willing to assume the full responsibility imposed by the State, he cannot do this when the 82patients refuse him the opportunity. He cannot follow them up at the expense of his private obligations. While the State expects service from those whom it licenses to practise, it does not expect the impossible.
Failure through the Personal Equation. We must now consider the second reason for removing tuberculosis from private into public control. For while the nature of the disease itself explains in large measure why it cannot be dealt with by the private practitioner, that is not the entire explanation. And here we must put the blame where it belongs—at the door of the physician himself.
When we think of the medical profession, we unconsciously think of its finest members—not only of the leaders in thought and achievement, but the numbers of highly educated, advanced, efficient, and conscientious men who form so large a part of it. In thinking of these, however, we are apt to overlook men of another sort, who are less well equipped, or who are imbued with commercialism, yet who are none the less members of this great profession. Yet even the least of these is armed, and has the sanction of the State in bearing these arms, which may be used either against a common enemy, or in a guerilla warfare in behalf of his own interests. The wide diversity among its 83individual members is the reason why the medical profession has been unable to act as a united whole in the warfare against tuberculosis.
In the first place, all physicians, no matter how well they may be trained, are not necessarily good teachers. No matter how keenly aware of the danger of tuberculosis, they are often unable to impress it upon their patients. Again, the busy physician has usually too little time to be a careful teacher. When conscious of a crowded waiting-room, or of the urgency of his next call, he is unable to give any but the most superficial and hurried instructions about the nature of tuberculosis, or the use of the prophylactic supplies. He does not realize that that which is obvious to him is frequently unintelligible to those less enlightened. We have often found patients possessing bundles of prophylactic supplies, given conscientiously enough, but without sufficient instruction to enable them to fold the fillers or to dispose of them afterwards. We recall one such case, where the doctor had given his patient a package of supplies, but had hurried off without opening the bundle or explaining its contents. A week later, we found the package still unopened. The patient, however, had torn a small hole in the wrapper, through which opening he had seen enough to 84convince himself that the strange objects within were no concern of his. We do not mean to say that no physicians are good teachers, but we do say that even where they are, and are moreover highly conscientious men, that they frequently give inadequate instruction to the patients under their charge, because they are too busy.
There is another class of practitioners, who, while willing enough, are nevertheless unable to contribute much towards the anti-tuberculosis campaign. These are the men whose education is limited, who are unable to recognize tuberculosis until it is advanced, and even then hesitate to commit themselves. The patient under these circumstances has ample opportunity to infect others, to say nothing of losing his own life into the bargain. No amount of conscientiousness, of integrity, and of honest intention can compensate for lack of skill. Indeed, many men of this sort come perilously near the border-line of quackery. Yet the State has granted them a licence, though thereby it entrusts them with obligations which they cannot fulfil.
We have spoken before of the unethical practitioner, who, while competent enough, feels himself under no obligation to protect the community from an infectious disease. There is sometimes 85a reason for this indifference, this failure to tell the patient he has tuberculosis, and to inform those who surround him of their danger. This reason is because many a patient is afraid to know the truth about his condition. If the physician tells him he has tuberculosis, he at once changes his doctor and seeks another who will give a more comforting diagnosis. Thus, the struggling physician, to whom this may mean the loss of livelihood and prestige, is forced to a decision between self-interest and the interest of a community which he learns to despise, because it has forced him to dishonesty. We grow cynical about the welfare of those who force us to trim our ideals.
We have tried thus briefly to review the main reasons why tuberculosis is emphatically a disease which should be removed from private practice and placed under municipal control. On the one hand, this is necessary because of the nature of the disease, since ambulatory patients cannot be followed except by those able to devote their whole time to it. On the other hand, it is necessary because of the wide diversity within the ranks of the medical profession. The greater number of private practitioners are either too busy, too intent on earning a living, too indifferent, or too poorly educated to assume effective supervision 86of an infectious disease which requires masterful handling. And since they themselves have not been able to deal with this great issue, they should not object to placing it in the hands of those qualified to do so. The greatest contribution that the private physician can make to the anti-tuberculosis campaign, is to do what he can to hasten the advent of full municipal controls.
The Nurse in Relation to the Physician—Municipal Control of Infectious Diseases—The Nurse’s Difficulties—A Waiting Policy—Undiagnosed Cases—The Nurse’s Responsibility to the Conscientious Physician Only.
The Nurse in Relation to the Physician. In the foregoing chapter, we have seen that the task of preserving and improving the public health is one which rests, theoretically, on the medical profession as a whole. As a matter of fact, however, this task is assumed only by certain members of the profession. We have pointed out the reasons for this—that physicians vary greatly as to personal character, ability, and ideals. In the field of public health, the nurse finds herself in contact with physicians of all classes. Some are able, high-minded, and skilful, and whether working as public officials or private practitioners, have nevertheless the same end; improvement of the public health. Others have standards quite the reverse. This brings us to the question: When the nurse’s duties bring her in contact with men of the latter class, how is she to meet the situation? In what 88relation does she stand to these men? What shall be her attitude to them, as regards her work? They are not numerous fortunately, but there are enough to constitute a serious problem, and one which sooner or later the nurse must face. This question will also have to be faced by those who are responsible for the nurse, and for her work.
In our opinion, the answer is simple enough—or, rather it will be, twenty years hence. For at present, public opinion is in a transition state and needs moulding. The nurse should work under the direction of, and in co-operation with, all those physicians who, whether as public officials or private practitioners, are working for a higher standard of public welfare. To all such, without discrimination, the public health nurse is the faithful, efficient, and tireless ally. But to all those other physicians who have no such aims or desires, the nurse stands in but remote and casual relation. The old teaching that she is the handmaiden of the doctor is gone. Both are now co-workers in the field of public health. The nurse still carries out the doctor’s orders, but there is this difference—she discriminates as to doctors. As a public servant, she obeys the orders of the municipal authorities, or of the private practitioner when the object of both is the same, that is, the welfare of 89the community. But she is not responsible to those physicians who try to defeat this object.
For this reason, the nurse can do more effective work if she is connected with the Health Department, since it is the Health Department of a city which must formulate standards of efficiency, and clothe its employees with authority to carry them out. The authority of the Health Department physicians should be superior to that of any private physician, should there be any conflict of opinion between them.
If the nurse cannot be established in connexion with the local Health Department, she will yet be responsible to a group of public-spirited citizens, which group will undoubtedly include many advanced and enlightened physicians. This group of people will represent advanced public opinion on the subject of tuberculosis, and the authority which the nurse gets from them will be of almost equal value to that which she would get from the municipality. Municipal authority, or the authority of enlightened public opinion, is a dangerous thing to oppose.
Municipal Control of Infectious Diseases. In the case of smallpox, diphtheria, or scarlet fever, the private practitioner attends the patient under the immediate supervision of the Health Department. 90Thus, in diphtheria and scarlet fever, he notifies the Department of each case that comes under his notice. A municipal physician is at once sent to take cultures from the patient’s throat, as well as from all the other members of the household. He placards the house, and instructs the family in such preventive measures as shall insure their safety and that of the community. The patient is then left in the charge of the original physician, who notifies the Health Department when, in his opinion, the infection is over. His opinion, however, is verified by the municipal physician, who takes another series of throat cultures, and ascertains, quite independently, whether or no the danger is past. If it is, he orders the placard taken down, and arranges for the fumigation of the house.
In the case of smallpox much more drastic measures are observed. The patient is summarily removed to quarantine, and all those who have come in contact with him are vaccinated and kept under observation for a definite period. In this way the strong hand of authority protects the community from infection—the private physician has been merely the means of calling attention to the danger. The time will come, indeed it is rapidly approaching, when enlightened public 91opinion will demand this same care in the matter of tuberculosis. By reason of the chronic nature of the disease, the care given must include long-continued supervision, extending if need be, over months and years. This supervision will be given by municipal physicians and nurses. Furthermore, the private practitioner will no more resent this, nor consider it interference with his private business, than he resents municipal care of smallpox or scarlet fever. The readjustment of the point of view is necessarily slow, but it is coming, none the less. Those of us on the firing line, however, who daily witness the loss and sacrifice due to this slow readjustment, cannot but wish for revolution instead of evolution in medical ethics.
In this chapter, however, we must deal with the situation as it exists to-day. The infectious nature of tuberculosis has become known comparatively recently, hence we find ourselves confronted with a delicate and difficult situation, as must always be the case when public opinion is evolving. To-day if a private physician forbids a nurse to visit his patient (and for nurse, read also Health Department), the present status of public opinion will usually uphold him in his decision. It is for us, therefore, to find out the reasons which prompt him to this decision, and to 92lay them frankly before the public, and let the public pass judgment. In no other way can opinion be altered, or can we gain for tuberculosis the same supervision and control that we have obtained for the other infectious diseases.
The Nurse’s Difficulties. Let us take a few examples of the difficulties the nurse meets. A boy of fifteen had been diagnosed by the Phipps Dispensary as a moderately advanced case, and the nurse was asked to follow him up. On her first visit, the patient’s mother refused to let the nurse enter, saying that her son had since called in a private physician, who assured him that the dispensary diagnosis was all nonsense. The dispensary man had counselled rest; the newcomer told the mother to buy her son a bicycle and let him take all the exercise he could. This treatment was followed out, and, still acting on the physician’s advice, the nurse was refused admission to the house. The mother was friendly enough when they met on the street, and she even permitted the nurse to stop and inquire for her son, always cheerfully replying that he was doing well. Useless as they were, the nurse continued these visits, since she was anxious to see the outcome of the case. Finally, one day six months later, the mother threw open the door, and in deep distress, begged 93the nurse to come in. “Do what you can for my boy,” she pleaded, and led the way to an upper bedroom, where the young fellow was lying in a moribund condition. A few days later he died. The mother bitterly accused herself for her folly in refusing the disinterested advice of the dispensary physician, and her grief, remorse, and opinions were given wide circulation in the neighbourhood. At no time during his illness had instruction been given as to the nature and danger of the disease, and not until a week before death did the attending physician admit that something was seriously wrong. In consequence of this wrong diagnosis, the boy lost his life, and the physician’s reputation was damaged. Apparently he had not taken into sufficient consideration the risk of contradicting a diagnosis that came from such an expert source.
In this particular case, it was impossible for the nurse to force her way in, or to do anything except await developments. As it happened, there was no one in the family likely to become infected, since the patient had no brothers or sisters, no one except his mother with whom he came in contact. The sacrifice of this boy to the ignorance, obstinacy, jealousy, or stupidity of the local physician proved a striking object lesson to the neighbourhood. 94The bereaved and indignant mother was a factor in forming public opinion in this particular vicinity.
Another case is that of a woman who had in her employ a favourite coloured servant, whom she suspected to be tuberculous. Accordingly, she sent for the nurse, asking her to take all necessary steps towards getting the case diagnosed. As the patient was too ill to go to a dispensary and could not afford a doctor, the nurse brought a specimen of sputum to the laboratory of the Health Department, where it was proved positive. So far, all was clear going. The patient was given her prophylactic supplies, put to bed in a clean, airy room, and the nurse called daily to give her a bath and such attention as she required. This should have been a hospital case, but at that time the hospital was crowded and there was no available bed. One day, when the nurse called as usual, she found the patient suddenly become very impudent. She was lying in a room with all windows closed, and a coal oil stove in full blast; no supplies were in sight and the patient was expectorating at random over the floor. This change had occurred because the patient had taken some of the money given by her employer, and had called in a “private doctor,” who declared she had nothing but a passing 95cold. He also told her the supplies were nonsense, and that he could cure her in two or three weeks. Furthermore, this physician himself came down to the Health Department, and forbade the nurse to continue her visits, and all “interference” with his case. A few days later, the employer also came to the Health Department, in considerable heat, and wished to know why the nurse was neglecting her duty. The explanation was satisfactory, and a visit to her servant amply corroborated the statements that had been made. This woman had been paying her servant full wages while off duty, as well as providing her with many little luxuries and necessities. She was therefore in a position to dictate the terms upon which she would continue this assistance, and these terms did not include visits from a physician of the calibre of the man now in attendance. In every case, however, it is not so easy to obtain the whip-hand of the situation.
In these two instances, there was little danger of spreading the infection, since neither patient was in close contact with children, or other persons likely to contract the disease. The young boy suffered an early death, while the coloured woman suffered personal inconvenience and discomfort, due to lack of nursing, care, and attention. In 96neither case, however, was there danger to other people. Whenever other people are involved, it is less easy to stand by and do nothing, while waiting for that slow change in public sentiment which shall give one the right to interfere. Thus, a physician diagnosed a case as tuberculous, and asked the nurse to take charge of the patient, telling her that he had carefully examined all the other members of the family, and found them in apparently good condition. He added, however, that he had been dismissed as soon as he had told the family the disease from which the patient was suffering. For this reason, he feared the nurse would find difficulty in entering the home. His fears were only too well grounded. The family had straightway called in another doctor, who calmed their anxiety by denying the previous diagnosis. He also advised them to turn away the nurse, which they did.
The patient lived some eight months after this, during which time she was given no supplies, no instructions of any sort, and the family were kept in ignorance of the nature of her illness. When she died, the nurse as agent of the Health Department went to the house to arrange for the fumigation. The front door was opened by a young girl obviously tuberculous—the nurse was struck with 97her appearance; further search revealed still another member of the household who presented suggestive symptoms. In their distress, the family turned to the nurse and asked for advice and assistance, and she at once referred them to the physician who had diagnosed the original patient, eight months ago. The family obediently presented themselves to him, and he found that three more members had become infected. Since they were all in the early stages, it is probable that they had become infected during the last few months of the patient’s life—during which time not one precautionary measure had been observed. The day will surely come when the possibility of treating tuberculosis lightly, at the option of the attending physician, will not be allowed. Public sentiment will finally insist upon full municipal control, which will do away with such malpractice and sacrifice of human life.
A Waiting Policy. As matters stand to-day, we can do nothing but accept the situation as we find it, and do the best that circumstances will permit. Which brings us to the question of the hour—What is to be done if the physician refuses to let the nurse visit his patient? Is she to accept his dismissal and turn away, or is she to continue her 98visits in spite of his objections, on the ground that the patient is hers as well as his?
If the case is a positive one, diagnosed on unquestionable authority, and if the nurse has been sent by a dispensary, the Federated Charities, or through some other disinterested source, she should be readily able to gain admission. Having gained this, she should be able to hold her own against all comers. As a rule, it is the opposition she encounters before, rather than after her first visit, which determines her ability to do her work in the home. Once in the home, however, it should make little difference whether or not the patient changes doctors. If he does, she should continue her visits as usual—her knowledge of his condition makes it advisable to hang on to the family at all costs. If this change brings a friendly doctor, he will not object to the nurse. If it brings a prejudiced one, she should do nothing to excite his hostility. Thus, if the new doctor denies the presence of tuberculosis, it may become necessary for her to seem to assent to this opinion—for a time she may have to visit merely in the capacity of a friend, offering no advice, and distributing no supplies. She must be careful not to antagonize the family, for after all, it is the family, at the doctor’s instigation, which is able to turn her out. Thus, when 99they triumphantly tell her that the patient no longer has consumption, she should not contradict them. Time will do it for her. She may express pleasure at the happy change, and ask for permission to stop in now and then, in passing, in the capacity of an old acquaintance. This request will seldom be denied, and at all costs she must keep in touch with the family which now, more than ever, needs her supervision and aid. She must stand by, ready to give this as soon as it is wanted. During this time it will be very hard to wait, to see the patient relax all vigilance, and to see the family recklessly exposed. But this waiting policy will pay in the end. As we have said elsewhere, the consumptive changes doctors more often than any other class of patients, and the nurse must realize this, and be ready to follow him through the vicissitudes which these changes involve. She must avoid all criticism when the family is fallen upon evil times, and be ready to uphold and encourage them when they are fallen upon good times.
Undiagnosed Cases. In the matter of suspected or undiagnosed cases, there is greater difficulty. In these cases the nurse has nothing to go on but her own keen observation of symptoms, therefore the physician in charge may make it very difficult 100for her to continue her visits. He can withhold his diagnosis, ignorantly or wilfully, and there is nothing to do but to accept this state of affairs. As before, the nurse must quietly hold on to the case, saying nothing that can possibly imply criticism or involve her in difficulty with the doctor. Time must be trusted to clear the situation—either the patient will get better, or he will get so much worse that a diagnosis may be forthcoming. Or else he may change doctors. When a nurse is visiting a case in charge of one doctor, she must be exceedingly careful never to advise another or to suggest a dispensary. All this involves infinite waste of time and loss of life, but as matters stand to-day, there is no other course to pursue. When a nurse is visiting a case of this kind—it may be one who presents every symptom of tuberculosis, including even hemorrhage—she must be particularly careful. She may call up the doctor, tell him that she has been called to his case through such and such an agency (these cases are usually referred by a layman) and ask if there are any orders he would like carried out. She may also ask him to tell her the nature of the disease. If he refuses, it is then a question of further “watchful waiting.” If the patient is expectorating a great deal, she may provide him with a sputum cup and other 101supplies, taking care, however, never to use the word “tuberculosis” in connection with them. She simply offers them as a convenience for a distressing symptom. We have known patients of this kind who died after being ill for months, most of the time being spent in bed. Meanwhile, they had extreme emaciation, night sweats, fever, cough, profuse expectoration, even hemoptysis, yet the death certificate read “bronchitis.” It is true, that these patients may really have died of bronchitis; as nurses, we cannot make diagnoses, therefore we have no right to question the physician’s findings. But it is impossible for an intelligent nurse to look on at a case of this kind without wishing it were possible to obtain a second opinion. As public health nurses we cannot but object that the last word on so serious a disease should be said by men whose diagnoses we distrust. That the health of the community should be endangered by even a few physicians of this sort,—either ignorant, or dishonest, or both,—is grave commentary upon the medical ethics of the day. It is a severe criticism on that “professional courtesy” which forbids intervention, even by the health authorities, with a physician who drives his trade at the community’s expense. The war against tuberculosis cannot be fought to a successful 102finish until the public refuses to countenance ethics of this sort.
The Nurse’s Responsibility to the Conscientious Physician Only. In all tuberculosis work, the nurse is singularly independent. When the patient is in charge of the dispensary physician, or is in charge of a doctor in sympathy with the tuberculosis movement, she may be said to be acting under their orders. Or rather, there are no special orders, except in individual instances, for the routine prescribed is always practically the same. When a doctor reports a case, with the laconic statement, “John Smith, such and such an address, usual thing,” he has fully stated the situation. The doctor knows what should be done, and the nurse knows what to do, and further words are unnecessary. Therefore, when for any reason the patient gives up his doctor, the nurse can still continue to supervise and direct. Months may pass before the patient revisits a physician, and during these months the nurse is the only person in touch with him. She also knows how to advise and direct those who are in contact with him. When he finally calls upon a doctor again, her visits still continue without a break—there should be nothing in her teaching that is at variance with that of the newly arrived physician. The chronic 103nature of tuberculosis makes this situation possible, and also makes for the extremely independent position of the nurse.
Whenever the physician is in the vanguard of the anti-tuberculosis movement, he will recognize the nurse as an ally, not a rival. He will know that she will make no attempt to supplant him with the patient, since the chances are that she has been caring for the patient for months before he, the doctor, has been called in. He will regard her, therefore, as a highly efficient ally, who will relieve him of tiresome, time-consuming details connected with the case. She will take charge of routine matters that he has no time for, and thus set him free for larger and more important tasks.
If, on the contrary, the physician is one who exploits his patients, who keeps the nature of the disease hidden, whether through ignorance or design, and fails to give proper instruction as to its infectiousness, then we must look for nothing but opposition and antagonism. We must hear objections as to the nurse’s interference, to her uniform, to her tactlessness, to her scaring the patient to death—and we must consider the motives which underlie them. This brings us once more to the question—under these circumstances, what is the nurse to do? Is she to discontinue her visits, or is 104the value of her instruction to be nullified by contradictory advice? Is a physician, who has consideration for neither the patient nor the community to be allowed to jeopardize both?
To men of this stamp, the tuberculosis nurse owes nothing. Her business is to do her duty, even when it brings her to cross-purposes with them. She has been taught her work by the most advanced and progressive members of the medical profession, and in the homes of patients she is but carrying out the orders of these abler men. That they themselves may have no direct connection with the patient does not alter the situation. She is their agent, not the agent of the hold-overs from a passing régime. Therefore, we look to the former to establish their agent, the public health nurse, in a position of unassailable dignity and authority.
Obtaining a Diagnosis—The General Dispensary—Sputum Examinations—Tuberculin Tests—Registration of Cases.
Obtaining a Diagnosis. As we all know, it is not the business of the nurse to make diagnoses, but it is emphatically her business to select cases which should be diagnosed, and to send them where this may be done. Therefore, if a community supports a tuberculosis nurse it will also find it necessary to establish a place where she may send her patients for examination—a special dispensary for the recognition of pulmonary tuberculosis. If there is no such dispensary, in charge of a capable physician, she may find it exceedingly difficult to obtain a diagnosis for her patients, without which her hands are tied. She cannot preach fresh air and prophylaxis to a person who has nothing but a “heavy cold,” no matter how serious may be the symptoms in connection with it. If the physician in charge of such a case is unable or unwilling to make a diagnosis, it is necessary to have some court of appeal to which the patient may be sent 106the moment he gives up his doctor or his doctor gives him up. As we have said before, the nurse must never influence a patient to change his doctor—on the contrary, she must be exceedingly punctilious in this regard—but when the patient is fickle and inconstant in his allegiance, she must take advantage of the opportunities offered to send him where he may be skilfully examined. The question of the special dispensary will be treated more fully in another chapter—here it is simply our purpose to show the need of such a place.
In a community which is beginning tuberculosis work, there are usually a few physicians who will generously volunteer their services in examining suspected cases. The nurse, however, will feel some hesitation in accepting these kindly offers, since to take full advantage of them would be to swamp these physicians with a class of patients which would leave them but little time for their private practice. These offers, however, may well be utilized in the formation of a special dispensary, since the same men would doubtless be equally willing to examine patients at some central locality. No matter how humble the quarters, how imperfect the equipment, it is necessary to establish as soon as possible a special place where these patients 107may be freely examined without any sense of intrusion or of incurred obligation.
The General Dispensary. In many cities, general dispensaries exist for the treatment of minor medical and surgical diseases. It is possible to send tuberculous patients to these dispensaries, and to get them examined and diagnosed, but as a rule this is not satisfactory. These general dispensaries are usually crowded, and the physicians in charge are unable to give sufficient time to the protracted, careful examination which the consumptive requires. However, failing a special dispensary, the nurse must take advantage of these general clinics and accept all the help they are able to give.
Sputum Examinations. In many States, the local or State Departments of Health maintain laboratories for the examination of sputum. The nurse as well as the doctor should be allowed the privilege of sending specimens for examination. If the findings are positive, the result is a diagnosis from which there can be no appeal. The difficulty with this means of diagnosis, however, is that many specimens are negative upon first examination. It may require repeated examinations to find the bacilli, or before their continued absence may be considered evidence that the patient is not 108tuberculous. Dr. Victor F. Cullen, Superintendent of the Maryland Tuberculosis Sanatorium, writes:
“We had one case that was examined sixty-seven times before tubercle bacilli were found, and this was a far advanced case, with both lungs involved from top to bottom, and cavities in each lung.
“We have at the present time (September 14, 1914) a patient in the Sanatorium, with both lungs diffusely involved, with a huge cavity in her left lung, expectoration about two boxes daily, whose sputum was examined twenty-four times, with only three positive findings.
“These advanced cases with a lot of bronchial secretion are usually the ones in which it is difficult to find tubercle bacilli in one or two examinations.”
The nurse, therefore, should send in specimens frequently, every week or so, and should never be satisfied with a negative report. As we have said before, finding the bacilli is proof positive that the patient has tuberculosis, but not finding them is no proof to the contrary. Countless lives have been sacrificed by considering a negative return as evidence that the patient was not tuberculous.
The nurse should carry in her satchel specimen bottles for collecting sputum. These bottles are provided by the Health Department. If the nurse has been called to a patient by the Federated 109Charities, or through some similar source, or if the patient is one whom she herself has discovered, she may send the specimen to the laboratory on her own initiative. But if the patient is already under the care of a physician who has not made a diagnosis, the nurse may call upon him and ask if she may take such a specimen to be examined. This courtesy will doubtless ensure better co-operation and understanding, but if the physician refuses, the nurse is then in an awkward position. In a short time she will learn the various physicians of her district, those whom she may call upon, and those whom she may not, and she will learn to exercise considerable discretion concerning them.
Valuable as these sputum examinations may be in the case of a positive finding, they should never take the place of a careful physical examination. It is only when this examination is not to be had, when the diagnosis can be obtained in no other way, that the nurse will be obliged to rely upon sputum examinations alone in dealing with her patients. A positive sputum should confirm the diagnosis made by physical examination—it is not, or should not be, the only means of obtaining this diagnosis. Therefore, the fact that a Health Department is equipped to make sputum examinations should never for a moment supplant the dispensary, in 110charge of a specialist or expert. A specialist is able by auscultation, percussion, and an ear finely trained to detect changes in the breath sounds, and to recognize tuberculosis weeks before the diagnosis is confirmed by sputum findings. In this way it is possible to place a patient under treatment long in advance of the time when the average physician would have recognized the disease—an advantage to the patient and to the community as well.
Tuberculin Tests. There are two tuberculin tests commonly used, which enable the specialist to diagnose doubtful cases. These are the eye and the skin test. Strictly speaking, the public health nurse has nothing to do with these tests, since they are entirely within the realm of the physician, but she should at least understand their significance. The Von Pirquet, or Skin Test, consists of inoculating the forearm with a drop of tuberculin of a certain strength. A positive reaction is manifest by a slight redness appearing within twenty-four hours and this may persist for a day or two, after which it disappears. This test has no value in the case of adults, since all adults are supposed to possess some slight tuberculous focus, and therefore a reaction has no significance. In the case of children, however, a positive skin test has some 111value. Children are not as a matter of course supposed to possess tubercular foci, and a positive reaction would therefore indicate that they have become infected. A reaction, however, gives no indication as to the location of the focus—it only proves its existence.
The Calmette, or Eye Test, has more importance. A drop of tuberculin is placed inside the lower eyelid of one eye, and if a reaction occurs, it does so within twenty-four hours. The conjunctiva becomes slightly red and inflamed, which condition persists for a day or two and then disappears. In adults as well as children, this is a positive indication of tuberculosis—not necessarily of a mere latent focus, but of a possible lesion which must be watched and guarded against. It gives no indication, however, of the location of the lesion.
These tests are useful to specialists in helping them to highly refined diagnoses. Dr. Hamman, however, questions the validity of these extremely early diagnoses, unless they are confirmed by sputum findings. If the bacilli are not found the diagnosis rests entirely with the examiner, and is therefore dependent upon the personal equation.
Registration of Cases. Most States have laws which require the notification of infectious diseases, 112including tuberculosis. This means that all physicians are required to report their cases of tuberculosis to the Health Department, filling in a card, more or less complex, in which is set forth the patient’s name, age, address, occupation, and the duration and stage of the disease. In Baltimore, the nurses also are allowed to register their tuberculous patients in this way, with the city as well as the State Health Department. The card used is the same as that used by the physicians, but with this difference—since a nurse is unable to make a diagnosis herself, she is required to place in the corner of the card the name and address of the physician or dispensary responsible for the diagnosis. In this way the authorities are enabled to know how many patients are under the nurses’ supervision, and the sources of the diagnosis.
Many of these registration cards are duplicates, the case having already been registered by the attending physician, or the dispensary. If they are not duplicates, it is necessary to have the official registration in the handwriting of the physician himself—it is often needed when trouble arises over the fumigation of houses, and so forth. There is nothing official or authoritative about the nurse’s registration cards—these merely call attention to the fact that certain patients are under her 113supervision, attended by such and such a doctor. In most cases, the diagnosis given is a verbal one. Should any difficulty arise, this verbal diagnosis would not be valid, although it furnishes an excellent basis from which to instruct the patient and his family. Therefore the nurse’s registration card, if it is not a duplicate, serves to call attention to the fact that a certain physician is in charge of a case which he has not reported. The Health Department at once writes and asks him to report, and in this way the diagnosis is officially recorded.
In Maryland, the law calling for the registration of tuberculosis had been on the statute books some years, but was generally disregarded. The physicians failed to report their cases, and it was therefore impossible to estimate the amount or distribution of tuberculosis. To do this was the object of the law. How generally this regulation had been ignored may be judged from the fact that in 1909, the year before the Baltimore municipal nurses went on duty, the number of cases of tuberculosis registered by physicians was only 919, while the deaths from tuberculosis for that same year were 1400. In 1910, the first year that the nurses were on duty, the cases registered jumped up to 3202, while the deaths fell to 1234. This sudden increase in the registrations—an increase 114of over three hundred per cent.—shows the stimulating effects of a staff of active public health nurses.
How necessary it is to have the diagnosis recorded in the physician’s own handwriting may be judged by the following incident. There was a coloured man on our list, referred to us by a private physician. This patient was a model in a school of painting and drawing, and after a time the Health Department was flooded with complaints concerning him. These complaints came from pupils, who declared they were afraid to go to the classes, because the patient coughed so violently and spat so profusely. The students did not know he was tuberculous, but they suspected it, and therefore asked us to look into the matter. Finding that the man was one of our patients, we at once wrote to the directors of this school, telling them of this, and of the complaints that had been made against him. We further suggested that if he continued to pose as a model he should use the prophylactic supplies that the nurse had given him, and which he used faithfully enough in his own home. The Directors, however, would not take our word for this; they sent the patient to another physician, not the one who had originally examined him. To this man, the darkey protested 115that he had never seen a doctor in his life. The second physician declared that the patient did not have tuberculosis, wrote a note berating us for our interference, and called upon us for proof. A hurried search of the files brought forth the original registration card, sent in by the physician who had first diagnosed the case, and transferred it to the nurses of the Health Department. This fact at once threw a different light upon the matter, and we were able to uphold our contention. The first physician, however, had completely forgotten this patient, and had it not been for his registration card, on file at the office, we should have been in a very disagreeable position.
Since there is nothing authoritative about the nurse’s registration card, she must be exceedingly careful never to register a case unless it has been properly diagnosed. This information should be obtained from the physician himself, whether in writing, verbally, or over the telephone. She should never accept a third person’s word for the diagnosis, no matter how accurate it may seem. For example, if a patient’s mother tells the nurse that the doctor has just been in, and said her son had tuberculosis, the nurse must not accept this statement as sufficient. She must call upon the physician and ask him herself. Again, suppose the 116nurse has sent a patient to the dispensary, and, meeting him on the street an hour later, she learns that the doctor’s verdict was consumption. She must not take the patient’s word for this, obvious as its truthfulness may seem. It is necessary to be thus punctilious, to prevent unpleasant occurrences from taking place. The diagnosis of tuberculosis is too serious a matter to be accepted through any such irresponsible medium as the patient or his family.
To fill in the registration cards is the nurse’s work. To supervise these cards, and note their correctness and accuracy, should be the work of the superintendent of nurses, in whose name they should be signed. This transaction is one of the most important tasks of the office, and extreme care should be taken that non-tuberculous patients are not registered by mistake.
Prevention of Tuberculosis—Sources through Which Calls are Received—Entering the Home—Telling the Truth to the Patient—Truth for the Family—Disposal of Sputum—Danger of Expired Air—Isolation of Dishes—Linen, Household and Personal—Disinfectant and Other Supplies—Phthisiphobia.
The Prevention of Tuberculosis. The object of the nurse’s work is to prevent the spread of tuberculosis—it is not to cure the disease. In doing the preventive work, it often follows that the patient himself is immensely benefited, and his disease apparently arrested. This arrest, however, is incidental—it is not the real object of the work, which is the protection of individuals as yet uninfected. In no other branch of nursing is there so much misunderstanding, so much placing of the cart before the horse, and so much emphasis laid on the wrong thing. Nurses themselves when they first begin the work fail to recognize the real issue, and think that it is the actual care of the patient which is the thing to be considered. This is totally wrong—we work through the 118patient to gain our ends, but he himself is not the main object. It is necessary to grasp this fact firmly, and keep it constantly in mind. This will not only prevent much disappointment and discouragement, but it will lay the foundation for more intelligent work.
On entering the home of the consumptive, the nurse has before her two responsibilities, the family and the patient. The former is infinitely larger and more important, since it is the family, as yet uninfected, which must be protected from the patient, or source of the disease. Instead of “family” substitute the word “community” and we have the crux of the situation—the protection of the community from the danger to which it is exposed. This protection may be accomplished largely through care of the patient, but care of the patient, only, as such, is a secondary matter. The vital and important concern is the welfare of his family. To confuse these two issues, and put the patient first, and the family, which means the community, second, would delay indefinitely the result we hope to attain. As far as possible, the interests of the two, patient and family, should be identical, but whenever a choice must be made between them, the welfare of the community has the right of way.
119This is why effective tuberculosis work must place the emphasis on the control of the last-stage cases, since it is the advanced case which is of most danger to society. For example: we have two families, one of which contains a moderately advanced case, whose outlook is favourable, while the second contains a last-stage case with a hopeless prognosis. Both patients are equally intractable; the nurse has but a limited time at her disposal, and must choose between the two, since she cannot divide her days equally between them. From the point of view of the individual, care of the earlier case would better repay her time and effort; from the standpoint of the greatest good to the greatest number, she must concentrate her efforts on the advanced case, since it is this one which is immediately dangerous. The earlier case is less of a menace to those about him; his obstinacy and refusal to follow advice mean loss of that precious time in which life and death are determined—but if he chooses, however wilfully, to waste this time, it is his own loss after all. It involves no one else. On the other hand, much more is involved in the advanced case. Here the patient’s death is inevitable, but it can be kept from occurring amid circumstances which would drag down others with him.
120In the majority of cases, the death of the patient is the issue to be expected, however much it may have been delayed or postponed—a result saddening and discouraging to those whose previous training has been to preserve life. What nurses are not trained to see, and what many of them have neither imagination nor faith enough to see, is the number of lives that are probably saved through the safeguarding of a dying individual. It has been said that the world would be infinitely better off if every consumptive in it could die to-day, since by this loss the people of to-morrow would be saved. The nurse must cease to reckon in terms of hundreds of patients—she must reckon in terms of the thousands who come in contact with these patients. The amount that can be done to protect these thousands is the standard by which the work must be judged a failure or a success. If she bears this constantly in mind, she will not become so easily discouraged.
Therefore, to sum up once more: upon entering the home, the nurse’s first care is the family, and her second is the patient himself. But it is by working through the latter that the former may be reached. The patient himself is the point of attack, and if in the ensuing pages he becomes so prominent as to delude one into thinking that 121his welfare alone is the final goal, he is only made prominent in order that we may reach our goal more quickly.
Sources through Which Calls are Received. The nurse goes to the patient’s home, in the first instance, at the request of some one who has sent her. This may be a physician, a dispensary, a neighbour, or she may even go on her own shrewd suspicion that some one is ill. When the door is opened to her knock, she must be careful how she explains her coming. If a municipal nurse, she should never say that she has come from the Health Department, for this conveys a suggestion of authority which is often most alarming. Since the patient has been referred to the Health Department from one of the sources just mentioned, it would be more tactful to name the agency through which the call was received.
When calls are anonymous, such as by letter or telephone message, or when the sender gives his name but asks that it be withheld from the patient, the task of gaining an entrance is often one of considerable difficulty, and requires much strategy. Calls of this sort should never be refused, since in this way many advanced cases are brought to light. It is also a wholesome indication that the community is learning to take an intelligent 122interest in an infectious disease, whose presence is recognized as a menace. These cases can best be managed if the nurse assumes the responsibility herself, saying that in a roundabout way she has heard that there is illness in the house, and so has called to offer her services. As a rule, her offer will be readily accepted, for a case reported in this manner is usually advanced, and, as we have said before, when the neighbours diagnose tuberculosis, they are frequently right.
Entering the Home. As a rule, when a nurse presents herself at a house and explains her errand, the door is opened wide and she is cordially asked in. In some instances, it is held half-shut, in a dubious manner, and she is admitted with reluctance. Sometimes it is banged in her face. It is a great satisfaction to gain an entrance into homes of the latter class; to win the confidence of such patients is a victory worth having. The surest formula for entering all homes is a broad smile; to stand on the doorsteps and grin like a Cheshire cat disarms suspicion, and once across the threshold, the victory is won.
Taking the Patient’s History. The facts concerning the patient must be gathered in his home, and they are of two kinds, those concerning his physical and those concerning his social condition. 123The first thing to be done is to establish a feeling of trust between the patient and the nurse. As a rule, all patients are communicative, and a few adroit questions will open a flood-gate of confidence from which can be gathered full details concerning their personal and family affairs. This gives the nurse much of the information which she needs not only for her charts and records, but also in order to deal intelligently with each case. For unless she understands the patient, and knows something of his social and economic condition, she will not be able to give helpful advice. But the nurse must also bear in mind that tuberculous persons are frequently shy and sensitive, and it may be difficult to obtain their true histories. They may be more ready to describe their physical symptoms than their social condition, and facts about their employment, hours, wages, life insurance, and so forth are not always forthcoming. It is inadvisable to make notes in the presence of the patient, for among the poorer classes there is a fear that their words, when noted in a book, may in some mysterious manner be used against them. Occasionally, in a matter of some importance, distrust may be quieted by asking, “May I just write that down? The doctor will be interested in that and I want to get it right,” but it is well to 124remember that suspicions once aroused are difficult to quiet, and that for the welfare of the community it is better to teach them to use their sputum cups, than to antagonize them by too many questions. The nurse should get all the facts the chart calls for, but with certain patients this may take considerable time. At each succeeding visit she can ask another question and a more intimate one, until she collects, little by little, all the data she requires. But it is a mistake to keep on asking questions—collecting statistics—at the expense of confidence and good-will.
It is true that when a patient goes to a dispensary, he is prepared to answer many questions, but there is this difference—it is he who seeks the dispensary. When the tables are reversed, when he is not the seeker but the one sought, he must be handled carefully. There are of course many patients to whom this does not apply, and who willingly volunteer every detail of their lives, but these are not the majority. The others, the more sensitive ones, make up three quarters of the visiting list. The antagonizing of a patient by tactless questioning is an unfavourable commentary on the method of handling him.
Telling the Truth to the Patient. The most difficult of the nurse’s duties, and the saddest, is 125to tell the patient the nature of his disease. Yet this must be done, for unless he knows from the very beginning, it is impossible to exact from him that intelligent co-operation upon which rests his sole hope. Only on the rarest occasions is there any justification for withholding this knowledge. If a patient has but a few more days to live, or if a hopeless case is surrounded by scrupulous care and attention, this information may, if it seems best, be withheld. But these are exceptional instances. To hide the truth from an early or moderately advanced case would be criminal. Apart from the first shock, people are never really injured by being told the truth, and we all know of hundreds of cases in which lives have been ruthlessly sacrificed through the policy of silence.
The truth need not necessarily be brutal—it can be made full of hope, interest, and encouragement. In her efforts to encourage the patient, however, the nurse must be exceedingly careful never to use the word “cure.” Tuberculosis is never cured in the sense that typhoid fever is cured, for example. At best, it is only arrested—that is, brought to a standstill, to a point where the destruction of the lung tissue goes no farther. Thus, if a person loses one or two fingers from a hand, a cure would imply that these lost fingers 126could be made to grow again. The lung tissue destroyed by tuberculosis can not be replaced or renewed any more than lost fingers can be renewed. Yet a lung, in spite of this loss, is still able to serve its owner well and enable him to lead a useful and happy life, just as a hand which has lost a finger or two may still be a fairly useful hand, and serve its owner well. This distinction between arrest and cure must be made perfectly clear to the patient, and he must also be taught that whether the arrest of the disease is temporary or permanent depends in large measure upon himself. His improvement depends upon his thorough understanding of his illness, and upon his ability or willingness to co-operate as to treatment. According to Dr. Minor,[3] it is not so much what a patient has in his lungs, as what he has in his head; namely, common-sense, which determines his recovery. Therefore to keep a patient in the dark concerning his condition, and yet expect him, without knowing the reason, to do over and over again the tiresome routine things necessary to improvement, is to expect the impossible.
3. Dr. Charles L. Minor, Asheville, North Carolina.
In making the best of things, the nurse must never over-encourage the patient. A half-starved, overworked person, suddenly put on a 127régime of fresh air, rest, and abundant food, will often make surprising advances—up to a certain point. This improvement may be so marked that it will raise false hopes of its continuance and the nurse must never jeopardize her reputation and the confidence imposed in her, by extravagant statements as to what may be accomplished. The overconfident patient mistakes temporary improvement for permanent cure. Tuberculosis is like a concealed enemy, crouched and ready to spring the moment one turns one’s back, and it requires constant vigilance to guard against it. If this fact could be securely drilled into the patients, there would probably be fewer relapses.
Truth for the Family. If now and then an exception may be made in informing the patient of his condition, there are no conceivable circumstances under which this knowledge should be withheld from his family. The significance and danger of tuberculosis must be fully explained to all who are exposed to it. It is the “family” who constitute public opinion as far as the patient is concerned, and we must depend upon it to keep the patient up to the standard of living which means his improvement and their protection. The nurse should fully explain the situation to some older, responsible member of the household. 128This can best be done out of the patient’s presence. She must speak very plainly, using words within the comprehension of her hearers, so that they cannot fail to grasp her meaning. The patient needs this knowledge in order to get better—the family need it in order to protect themselves. It is a sad fact, but a frank appeal to the selfish instinct is usually productive of better results than one made upon higher grounds. Both points should always be made, but the instinct of self-preservation may be aroused with less prodding than is needed to awaken rudimentary altruism.
Disposal of Sputum. The nurse has by this time prepared the way for the prophylactic supplies, which she carries in her bag. These consist of a tin cup, fillers, paper napkins, disinfectant, and so forth. She must teach the patient how to use and dispose of them, as well as their advantages—the latter reason not being always apparent to the ambulatory case. She must teach that danger to himself and others lies in the sputum coughed up from his sick lungs, and that the simplest way to receive it is in the little tin cup, whose waterproof filler can easily be burned. To the advanced case, with profuse expectoration, these light, convenient little cups are a great 129improvement over the household spittoon, which should be banished at once. Bed patients, or those too weak to raise even this light cup to their lips, may be taught to expectorate into the paper napkins, of which they should be given a large supply. A simple way of disposing of these napkins is to pin to the bedclothes a large paper bag (such as are used for groceries), into which they may be thrown. Failing a paper bag, a cornucopia made of newspaper will answer the purpose, the object being to let the patient himself place this infective material in a receptacle which can be burned in its entirety, without its contents being handled by anyone else.
The problem of destroying sputum cups and their contents is often difficult. The proper and only sure way is to burn them, and no other course should be considered. Yet in summer, when many patients have no coal fires, but merely gas or oil stoves, many difficulties arise. Under such circumstances the patient may wrap his cup in a newspaper, place it in a galvanized iron bucket, and then set it on fire. This is a nuisance, as well as somewhat dangerous, and since these fillers and their contents are hard to burn, the simpler method of throwing them in the gutter becomes an irresistible temptation. To see that these 130fillers are properly destroyed requires constant supervision and instruction and is one of the most important of the nurse’s duties.
The patient should destroy the fillers himself—they should be handled by no other member of the family, unless of course he is too weak and ill to do it. Even when very ill, however, it is nearly always possible for him to remove the filler from the cup and place it in a newspaper, which is then rolled up by someone else and carried out to the fire. Needless to say, the nurse must teach those who touch or handle this cup how important it is to wash their hands thoroughly afterwards.
Danger of Expired Air. After giving him the tin cup and fillers, the nurse must then give the patient a supply of paper napkins, and explain their purpose. These are primarily intended to hold over the mouth when coughing. The nurse must explain that bacilli are liberated in great numbers during these coughing attacks, and that it is harmful to live in a room filled with these invisible organisms. Most patients, knowing themselves to be infected, are indifferent to the welfare of those about them. Therefore, in trying to make him careful, the nurse will have to appeal to his selfish instincts, and show that what is bad 131for other people is equally bad for him, and so diminishes his chances of improvement.
It is comparatively easy to instruct a patient in the use of his sputum cup, but to obtain any sort of carefulness in this equally grave matter—liberation of bacilli in the expired air—is well-nigh impossible. This is partly due to the nature of the disease—in its most infectious stages, the patient is so racked with paroxysms of coughing, that it is impossible for him to keep his mouth covered, or to think of anything except his own sufferings.
On the street, these paper napkins may be used to spit into, the patient carrying them home again in the waterproof pocket pinned inside his coat. Fine details of this sort are difficult to insist upon, however—the convenience of the street and of the gutter making a stronger appeal than any newly acquired æsthetic valuations. This is of minor importance, however; the real danger lies in the home.
Isolation of Dishes. The consumptive should have special dishes provided for him, which should never be used by any other member of the household. If the family can afford it, they should buy dishes of a special pattern, unlike those in general use, since in this way the chances of mixing them 132are greatly lessened. Otherwise, constant care must be taken to keep them apart. The patient’s dishes should stand on their own corner of the shelf, be washed in a separate dishpan, and dried with a special towel. Once a week, for general cleanliness’ sake, they should be boiled. Any dish which may have got mixed with them, or has inadvertently been used by the patient, should be boiled before being used again in the household. The patient need not necessarily know that his dishes are isolated, since details of this kind are explained to the family rather than to the sick man.
If he is a bed patient, it is an easy matter to isolate his dishes, without his knowledge; when he is up and about, it is much harder. Patients are particularly sensitive about this, and some families, rather than risk hurting the feelings of the invalid, prefer to boil the dishes after every meal. This adds so much to the work of the busy household that after a time all attempts at isolation are dropped. This matter calls for considerable vigilance on the part of the nurse.
Linen, Household and Personal. All linen, including clothing and bed linen that has been used by the patient, should be boiled before it is washed. There seems to be some prejudice 133against this previous boiling, as the family are apt to maintain that it makes it more difficult to get the linen clean afterward. The nurse should overcome their objections, and emphasize the necessity for the utmost caution in regard to this infective material.
Disinfectant and Other Supplies. At a later visit, the disinfectant may be given, as well as the waterproof pockets and books of information. During the first visit, it is better to give only the most important of the supplies—the tin cup, fillers, and napkins—and to save the rest for another time. For on her first visit the nurse is a stranger—later, she becomes a friend. Therefore she will make better headway if on her first appearance she does not burden the family with too much instruction and too much detail. It is better to say too little than too much, better to leave something unsaid until the next time, rather than overwhelm those she visits with a mass of advice which they cannot assimilate. Her first visit has been made as the bearer of distressing news, no matter how gently and carefully it may have been broken, and the distress and confusion which often arise fill the minds of her hearers to the exclusion of nearly everything else.
During her later visits, she will have ample 134opportunity to say all that should be said—and at each succeeding call she will find that much of what she said the time before has been forgotten, misapplied, or altogether ignored. Tuberculosis work means the constant and incessant repetition of the same thing, trying by every device imaginable to point the way, to make an impression, to obtain some slight degree of carefulness which may mean the protection of other people.
Phthisiphobia. People frequently reproach the nurse with the fact that her teaching tends to alarm the patient and his family, and to produce a community phthisiphobia which works great hardship in individual cases. As far as the community is concerned, fear of tuberculosis is a good, wholesome sentiment, and infinitely preferable to ignorance and indifference. We cannot have too much of a public opinion which declines to be exposed to this disease, and which will therefore provide the machinery to cope with it. As far as the family is concerned, we have never been able to produce enough fear of tuberculosis. It would greatly facilitate the campaign if the first feeling of alarm and apprehension could become permanent, instead of very transitory and fleeting. Tuberculosis is so slow and insidious in its onset,—there is nothing spectacular, by which we can demonstrate 135to the ignorant mind the relation between cause and effect, exposure and infection,—that the educational method alone is inadequate to deal with the situation. If the alarmed patient and his household could or would continue the preventive measures which at first so strongly appeal to them, and which in the beginning they apply with boundless enthusiasm, we should have comparatively little difficulty. But the disease is chronic and slow; the scare wears off, and the cry of “Wolf, Wolf” loses its value. And then follows a relaxation of prophylactic measures. Each time the nurse must stir them up anew—encourage, threaten, alarm, coax, bribe,—do everything in her power to awaken them from their mental apathy and drowsiness, which, as in morphia poisoning, precedes death.
Inspection of the House—The Patient’s Bedroom—Porches—Gardens and Tents—Flat Roofs—Clothing and Bedclothing—Artificial Heat—Rest—Fresh Air—Food—Cooking—The Bedridden Patient.
Inspection of the House. On her first visit the nurse must inspect every room in the patient’s home, with a view to knowing what possibilities it affords for treatment and isolation. Some contain no facilities whatsoever; some but meagre ones, while in others may be found excellent opportunities which the patient must be taught to use. Before advising any change or rearrangement, several factors must be considered: the stage of the disease, number in family, financial condition, home surroundings and the institutional facilities of the community. The course to be taken depends whether or not there is a hospital, or whether or not the patient must wait some time before admission. The first object is the protection of the family, but all those measures which bring this about, offer at the same time the maximum advantage to the patient himself. To 137remove him to an institution is the best way to accomplish both ends. If this cannot be done, the nurse must endeavour to secure conditions in the home which as nearly as possible approach those of an institution. The closer this approximation, the greater the gain to both patient and those who surround him.
The Patient’s Bedroom. The first thing to be considered is the patient’s bedroom, or sleeping quarters. He should have this room to himself, sharing it with no one. If this cannot be arranged, he should at least have a bed to himself. This bed, and that of the other person, or persons, should be placed at opposite ends of the room, and as far apart as possible.
The more windows in the room the better; these should be kept open to their fullest extent. In some houses, where the windows are small, it is often possible to lift out the entire sash, thereby admitting more air. The bed should be placed directly at the window, so that the patient may lay his pillow on the window sill if he chooses. He should be instructed to sleep facing the opening, in order to get all the air he can. The nurse should rearrange the furniture as she wishes it, otherwise misunderstandings may occur. If the family object to her moving it but promise to do 138this themselves, she must be careful to inspect the room again on her next visit, to see that this has been properly done. Even with families that have been under supervision a long time, it is well to inspect the bedrooms occasionally, for the patient’s bed always has a tendency to retreat into a remote corner of the room, especially in winter.
The floor should be bare, and this, together with all other plane surfaces should be washed several times a week with hot water and soda. Great caution must be exercised in making a sanitary sick-room, but, in her enthusiasm to produce ideal conditions, the nurse must remember that articles used for months by the patient, and suddenly banished from his proximity, may be very deadly elsewhere. In advising that carpets and curtains be removed, she must be careful what becomes of them. If germ-laden carpets are sold, or given to the neighbour next door, they would better remain where they are. Poor people find it hard to withstand the temptation to sell or give away serviceable articles, which is of course but natural, but the nurse must be on guard against such occurrences.
To have an ideal sick-room, there is no necessity for its being depressing by its bleak ugliness, or bare and dismal as a cell. Washable muslin curtains may be permitted, and there is no objection 139to pictures and ornaments in moderation. It is bad enough to have tuberculosis, without penalizing the patient by removing from him all those little treasures which give him pleasure and harm no one.
In selecting a good room for the patient, the nurse may find it necessary to have him exchange with some other member of the household. In this event, great care must be taken that the room vacated by the patient is thoroughly cleaned and disinfected before being occupied by anyone else. There are also circumstances which render it unwise to make this exchange: for example, say that we have a moderately advanced case, whose improvement is doubtful. He is occupying a room with one window—not ideal, but fair enough. There is also another room in the house, containing several windows, altogether brighter and larger, but occupied by three or four people, so far healthy and sound. To exchange rooms under such conditions would be bad policy—it would be of little advantage to the patient himself, while the other people would be subjected to overcrowding and bad ventilation, which would decidedly lower their resistance. Those in prolonged, intimate contact with a consumptive must not be allowed to reduce their vitality in any way.
140To arrange a good sanitary room for a patient does not in the least mean that he will use it. Such a room would doubtless appear well in a photograph, illustrating the “before and after” phases of the nurse’s activity, but this does not necessarily mean that the patient is isolated and harmless. He will probably use his nice room for sleeping purposes only, and it is what he does with the remainder of his time that counts. He comes into contact with the household at meals, in the evenings, and on innumerable other occasions, and the consciousness of an immaculate bedroom should not lessen the nurse’s anxiety about the kitchen, the living-room, and the family sofa. There is where the danger lies.
Porches. In some houses we find a porch readily available for the patient’s use, where he can sleep and spend most of his daylight hours. It is sometimes difficult to induce him to make use of it, however. We must also remember that there is a great difference in porches. Some are narrow, unroofed, exposed to sun and wind, have disagreeable outlooks, for instance, as on unsavoury alleys, and in other ways are unfit to be used as living-rooms. They should be used, of course, whenever practicable, since undoubtedly the patient will get more air, and more constantly 141changing air, than if he sleeps indoors. Yet it is well to realize that a place where the patient is unsheltered, uncomfortable, and where he cannot sleep or have a quiet mind, is often far less valuable than a good bedroom which may give him all of these necessities.
Patients in well-to-do circumstances can equip their porches admirably, both with awnings and with canvas screens. These latter should roll up from the floor, rather than down from the roof. Screens and awnings can be made to order by any awning or sail maker; the price varies with their construction, from about five dollars upward. To teach a patient to use a porch for sleeping and also to use it as a living-room should be the nurse’s constant endeavour. Even an ideal porch is like an ideal bedroom—only valuable if it is used.
Gardens and Tents. Many houses have little yards or gardens, easily adaptable for open-air living. A tent may be erected for sleeping purposes, if the space is large enough and the family can afford it. Women and children are usually afraid to sleep under such exposed conditions, and in consequence refuse to make use of what would otherwise be an excellent opportunity. These gardens may be used during the day, however, and the patient made comfortable in a reclining 142chair or lounge. But excellent as they appear theoretically, the extremes of our climate, excessive heat and cold, often make them unpractical for the consumptive’s use. Under such circumstances, these little back yards often become anything but ideal places in which to “take the cure.”
Flat Roofs. We also find flat roofs or sheds attached to certain houses in the tenement districts. These sometimes offer excellent conditions for long hours out-of-doors, and may also be used as sleeping-porches. The nurse must be alert to seize all opportunities which present themselves, and to teach her patients to utilize them.
Clothing and Bedclothing. In her effort to teach her patient to sleep out-of-doors, and to spend most of his waking time there, the nurse must remember that in winter this is impossible, if he is insufficiently clad. The vitality of the consumptive is always below par, consequently he needs much more clothing than would a healthy person under the same conditions. It is impossible to expect patients to remain out-of-doors if they are cold and uncomfortable, and before insisting upon open-air treatment the nurse must see that it is possible for them to take it. If they lack the necessary clothing—underwear, blankets, sweaters, 143overcoats—these may be procured through some charitable association. It is a part of the nurse’s duties to arrange for this assistance, the question of which will be dealt with in a later chapter.
Artificial Heat. In addition to extra clothing, artificial heat is nearly always necessary, and this may be procured by means of hot-water bottles, hot bricks, stove lids, and so forth. The clothing itself may be sufficiently warm, and a hot brick may be all that is necessary to keep the patient in the yard, rather than in the kitchen. The patient must learn to live in the open-air—and the family must also learn that their safety lies in keeping him there, and is well worth the trouble of filling a hot-water bottle now and then. A hot kitchen is the worst place in the world for a coughing consumptive—and a coughing consumptive is the worst thing in the world for a hot kitchen—and the inhabitants thereof. It is fortunate that the rule works both ways, so that both sides may be appealed to.
Rest. The three things necessary to improvement are rest, fresh air, and food. Not one alone, nor two alone, but all three together, if results are to be obtained. It is very difficult to impress upon the patient that rest is not exercise, and that nothing is as bad for him as exertion. He 144instinctively associates fresh air with exercise, and does not realize that fresh air and rest is the combination required. If a physician is in charge of the case, he of course would direct the amount of exercise to be taken, but if, as often happens, there is no doctor in attendance, the nurse must use her own knowledge of what is best. In a sanatorium the usual rule is that all patients with more than 99 degrees of fever shall stay in bed. After a hemorrhage, absolute rest is of course indicated.
Therefore the nurse should try to induce her patients to rest as much as possible—not to walk about, or to drag themselves to a park, and so tire themselves out. Exertion increases fever, and this will counteract what benefit might have been gained through the fresh air. They should be taught to sit comfortably in their gardens, on their front sidewalks, on their porches, at their open windows. Best of all, they should go upstairs to their bedrooms, and lie at full length on the bed placed next to the open window. By thus emphasizing the importance of rest—synonymous in this case with outdoor rest—the nurse is not only giving sound advice to her patient, but she is protecting the community from the ambulatory consumptive.
145Whenever possible, the patient should be induced to remain in bed permanently. The sooner the weary, advanced case gives up his painful wanderings, stops dragging himself from his own to his neighbour’s kitchen, or to the hospitable bar, the better for him and for the community. If he were to go to bed in a hospital, instead of at home, greater still would be the gain. The part of the community constituted by his family would be freed from danger, while he himself would be adequately cared for. Again we are struck by the coincidence of what is best for the patient being also best for those who surround him.
Fresh Air. Fresh air is the second great essential in the treatment of tuberculosis, and every patient should be taught to spend as many hours as possible out-of-doors. The nurse must explain in words of one syllable why this is necessary—that clean, pure air contains life-giving oxygen, and that to breathe it entails little exertion on the part of the sick lungs. On the other hand, impure air contains no upbuilding principle, but greatly taxes the lungs and makes breathing difficult. Outdoors, every breath of air is clean and pure; indoors, especially in a closed room, one is soon reduced to rebreathing expired air, with all its impurities. Just as tainted meat or 146spoiled fruit or vegetables are unwholesome, and bad for the stomach and general system, so is impure air harmful to the lungs and general health. One organ surely deserves as much consideration as another. And when the lungs become impaired through disease, it is still more necessary to take care of them. They need to be strengthened in every way, in order to defy the inroads of tuberculosis. The nurse must make her points clear and emphatic; if the patient takes an intelligent interest in his treatment, it will become less irksome.
But it is not enough to tell the patient why he needs fresh air—the nurse must show him how to get it. He is singularly helpless and unable to recognize such ways for himself. Also she must overcome his objections and bring him to her way of thinking. Thus, he objects to his porch because it is shaky, or because it may only be reached by passing through another person’s room. Investigation may prove the shakiness imaginary, or at least not dangerous, while the other person may be only too willing to let his room be used as passageway to this desirable goal. Again, he objects to sitting in the yard, or on the sidewalk, or even at his window, for fear of what the neighbours may say. It should be pointed out that his 147health is more important than their comments—whatever they may or may not be—and that his interest, not theirs, should come first. The nurse must plan every little detail; she must select his chair or sofa; must show how he can be warmly tucked up, and sit out of the wind or sun, as the case may be. She must teach the family about the hot brick and how to place it at the patient’s feet—or two hot bricks, if need be. It is not enough to say: Do thus and so—she must herself demonstrate how the thing is done. The consumptive is sick and helpless and needs constant reassuring. If he belongs to the very poor, he has little to do with, and is so ignorant that he cannot make the most of what he has. This teaching is one of the chief duties of the nurse.
Food. The third great essential in the trilogy is food. The patient’s diet is of the utmost importance, since his ability to take and assimilate nourishing food determines his ability to build up enough resistance to cope with tuberculosis. Generally speaking, he should be encouraged to eat every kind of nourishing food that he can digest—for tuberculosis does not call for a special diet as does typhoid or diabetes. Anything which specifically disagrees with him should, of course, be excluded. The question of food values 148must be considered; with the poor, this requires careful teaching and explanation. The nurse should point out the difference between food which merely fills the stomach, and food which nourishes and upbuilds. In the first class may be instanced cabbage, turnips, doughnuts, pies—all highly esteemed by the poor, and cheap and indigestible. In the second class are meat, eggs, milk, fish, rice, beans, hominy, oatmeal, and so forth. Some of these nourishing foods—rice, beans, hominy, oatmeal—are no more expensive than cabbage and pie. The family should be taught the difference. Very harmful and indigestible are the products of the corner bakery, the penny candies, the enormous pickles, and the copious strong brews of tea and coffee which form so large a part of the dietary of those near the poverty line. Considerable money is spent on these things—often money enough to provide a wholesome meal, if the family but knew how to discriminate. In planning a patient’s diet, the nurse will have to do as much exclusive as inclusive propaganda.
It is not necessary to insist on milk and eggs, certainly not in the abnormal quantities which a few years ago were considered indispensable in the treatment of tuberculosis. If a patient likes these and can afford them, well and good, but they 149need by no means be made the staple article of diet. This rich and highly concentrated food has a tendency to cause indigestion, and since this is one of the gravest and most distressing complications of tuberculosis, it must be prevented at all costs. A patient unable to digest his food has but slim chance of increasing his vitality, and little hope of improvement. Therefore, in advising raw eggs, the nurse must be very careful; one or two a day will be sufficient, over and above the regular meals.
Milk should be substituted for tea and coffee. Three or four glasses a day will be enough, and even that may be too much if the patient eats well of other things. In place of raw milk, it may be peptonized, malted, given hot, made into junket, taken in cocoa, or as one of the flavoured milkshakes, or turned into clabber or buttermilk. These varieties of milk are good for advanced patients, who may also be given egg albumen, flavoured with lemon, orange, ginger ale, grape juice, and so forth. The family must be taught to make these little innovations, in the ordinary diet, and instruction in these is part of the nurse’s work.
By careful supervision and attention, the nurse can procure a very satisfactory dietary, one both nourishing and digestible. Three good meals a day, with a little nourishment between meals and 150at bedtime (a glass of milk or its equivalent), will be found quite satisfactory. If a doctor is in attendance, he will of course arrange such diet as he thinks best, but if the nurse is left to herself, she will not overstep the boundaries if she advises some such plan as we have outlined.
As we have said, indigestion is one of the most frequent complications of tuberculosis. In some cases this can be overcome or relieved by advising rest in the reclining position for an hour before, and immediately following meals. If the patient lies flat on the bed or lounge, this will be more effective that if he sits in a rocking-chair.
Cooking. Cooking and the preparation of food also require supervision, for, especially among the poor, dense ignorance of these important matters prevails. Through improper cooking, wholesome, excellent food is often turned into something quite the reverse, indigestible and injurious to a high degree; or, if not ruined, it may lose so much of its food value as to be practically worthless. Thus, a hard-boiled egg or a fried egg (especially if fried on both sides) is less easy to digest than a soft-boiled one. A good piece of meat may have its entire value removed by overcooking. All nurses have had training in dietetics, and this special knowledge is of immense value in 151public health work, where for the most part they come in contact with a class of people whose ignorance of culinary matters is profound.
Alcohol. The question of giving alcohol frequently arises in this work. If a doctor is in attendance, he will prescribe it or not as he chooses. But if the nurse alone is in charge of the case, and the matter is left to her decision, we feel that the ruling of the Phipps Dispensary of the Johns Hopkins Hospital is a wise one to follow—no alcohol for the consumptive under any circumstances. This means that there shall be no eggnogs, made with brandy, sherry, rum, etc.; no sherry with raw eggs—no indulgence in wine, beer, or alcoholic stimulants of any sort.
The Bedridden Patient. When the patient is confined to bed, the nurse’s task becomes easier. Isolation, therefore better protection to the family, is more readily secured than when he wanders from room to room, leaving a trail of germs behind him. It is well to exclude from the sick-room every one except those in actual attendance upon the patient; this is especially necessary in the case of children, to whom the danger is greatest. Neighbours and friends should also be excluded, and if they refuse to consider the risk, the plea for exclusion should be made on the 152ground that visitors are disturbing and harmful to the patient.
In the sick-room we sometimes find the young children of neighbours, whose mothers are all unconscious of the danger to which they are exposed. If through sheer indifference, the patient’s family does not exclude these children, it would then become the nurse’s duty to seek out their parents and warn them. When a patient’s household becomes indifferent to community welfare, the nurse should then extend her teachings farther afield—into the next house or block if need be—and try to protect others who are unknowingly exposed to infection.
In brief, these are the duties of the nurse in the home of the patient. At her first visit, she cannot say everything she wishes, but later it will be possible to do so. In many cases, the household will be suspicious, antagonistic, or not inclined to want her, so that she must feel her way cautiously, step by step. It may take two, three, four, or even a dozen visits to accomplish her object, and before she can drive her points home with the requisite vigour. When the situation is acute, and the danger great, it is difficult and discouraging to make haste slowly, yet this policy will pay in the end. It is better to proceed cautiously 153with an uneasy family, winning them gradually from point to point, than to arouse their resentment by an impatient enthusiasm which sees no wisdom in delay.
In dealing with patients, the nurse must speak plainly; it will not do to insinuate or imply. What she has to say must be said straightforwardly, in simple words adapted to the intelligence of her hearers. The situations one encounters in this work are often sad and trying to a degree, and it would be far easier to insinuate a disagreeable or painful thing than to speak out plainly. The nurse who cannot express herself clearly, forcibly, and convincingly will get poor results. She must be able to meet prejudice with reason, to impose her view upon another, and to convince the ignorant that what she says is right.
There is an old fable which all public health nurses should remember—the old story of the Wind and the Sun, who both tried to remove the Traveller’s cloak. The Wind tried first, and he blew and blustered, but his frantic efforts only made the Traveller clutch it tighter. And then the Sun tried. He shone, blandly, warmly, gently, and in a few moments off came the cloak. It is the method of the Sun, rather than of the Wind, which usually wins out.
Care of the Family—Examination of the Family—Taking Patients to Dispensaries—Children—Tuberculosis in Children—Open-Air Schools—The Danger of Sending Patients to the Country.
Care of the Family. We have already said that the first consideration is the patient’s family, or those individuals who come in contact with him. Therefore, as soon as he himself is under satisfactory supervision, the nurse must turn her attention to the other members of the household who need her even more. A majority of the nurse’s patients are either advanced or last-stage cases, many of them having a history extending over months or perhaps even years of illness. If during this time the nature of the disease has been unknown; or known, and no precautions have been taken, there is great likelihood that other members of the family have also become infected. To discover these suspicious cases and get them examined and under treatment as soon as possible, is one of the nurse’s first responsibilities. Next, she must give careful attention to those other 155members of the family who so far have apparently escaped. She must not over-alarm or frighten them, but she must keep before them the fact that they are in close contact with a highly infectious disease, and that whatever lowers their resistance, increases in like manner their chances of contracting it. They must employ every means in their power to raise their vitality to a point where they cannot be reached. An infectious disease does not, as a rule, gain entrance into a constitution strong enough to resist it.
To this end, the nurse should pay particular attention to the personal hygiene of the exposed family. Their bedrooms and sleeping quarters should receive as careful consideration as do those of the patient. Every one in the house should be taught the value of fresh air, and the necessity of sleeping with wide-open windows; the measures needed to get people well are equally necessary to keep them well.
The family also needs careful instruction as to food and rest: food, nourishing and well cooked; rest, which should at least mean that at the end of a day’s work they do not exhaust their vitality in crowded poolrooms, dance halls, and saloons. The need of recreation is one of the fundamental needs of mankind, but there is a difference between 156that which refreshes and that which undermines the constitution. Whether this fatigue comes from work, play, or excesses of any kind, it is usually the worn-out individual who first succumbs to exposure. In all households there is great need for instruction along these lines. There are weary, indifferent parents, and heedless boys and girls whose ignorance of personal hygiene is profound. The fact that much of this teaching falls on apparently stony ground shows the need for redoubled effort—which will in time bear fruit. Those in contact with tuberculosis must be continually on their guard against it—disease does not, as a rule, attack those who are in sound health.
In this preventive work, the nurse will be greatly aided if she knows what agencies she can call upon to reinforce her instruction. She must be familiar with all the forces of social service, and know how to reach them, and how to place her families in touch with them. Just as she must have sufficient knowledge of dietetics to suggest rice as a substitute for cabbage, bread instead of pie; so must she understand the social agencies within call, and know what substitutes they offer for the things that she condemns. A great gain will have been made if instead of the poolroom, the young boy can be given the Settlement club 157or gymnasium; or instead of the saloon dancehall, the young girl can be offered that of the schoolroom or the church. The aim should not be to deprive, but to substitute. Preventive work consists largely in teaching how to substitute the harmless for the harmful, the healthful for the unhealthful. In some communities, no such agencies exist; in others, they are inadequate to the needs they try to fill. But if they exist, they should be called upon.
Examination of the Family. Every person constantly exposed to tuberculosis should be examined periodically, whether or not he presents symptoms. The nurse should endeavour to get all members of the patient’s household examined. This is sound in theory, but not always feasible in practice, especially when there are a large number of patients under supervision. When one is working with small numbers, with ten, twenty, or a hundred families, it might be possible to get every member of these households examined, but when one is working with large numbers it becomes proportionately difficult. In Baltimore some 5000 consumptives are annually dealt with by the Tuberculosis Division; if every one of these patients comes in contact with five other persons—a most modest estimate—that would give us a 158total of 25,000 people to bring forward for physical examination. This task would swamp our dispensaries and leave no time for anything else. After all, it is the positive rather than the potential cases which are a menace to the community. Thus, however much we may advocate the need for general examination of all exposed persons, this course has its drawbacks when it comes to actual practice. The best we can do is to get the suspicious cases examined. The examination of those who have no symptoms would furnish interesting statistics, but they are hardly dangerous enough to the community to warrant the outlay of time and energy.
To induce a patient to be examined often requires weeks or months of effort and persuasion. The less the apparent necessity, the more difficult it often becomes. If a person has no symptoms he will not go, and if he has symptoms, he is afraid to go, to a physician. Therefore, whenever it is possible to get exposed persons examined, well and good; when this is not possible, the nurse may confine her efforts to those with suspicious symptoms. One of the foremost requisites in this work is the ability to distinguish between essentials and unessentials, and having made the distinction, to concentrate on the most important.
159Taking Patients to Dispensaries. Unless the nurse has abundance of time and a very light district, it is not well that she should spend time in taking reluctant patients to a dispensary for examination. To do this, means to give up from one to several hours, which she can ill afford to spend in this manner. Nor is it necessary to waste her expert service in this way—it is always possible to find some one willing to take these patients, some friendly visitor, settlement worker, or even a kindly, intelligent neighbour.
Children. It is conceded nowadays that people usually become infected with tuberculosis in the first ten or twelve years of life, or during childhood. The disease itself may or may not develop in later life, according to the circumstances or environment in which the individual is placed. It may light up later, if his resistance becomes lowered, or he is reinfected, and cannot carry the extra load. For this reason, it is a vastly important thing to protect children from infection, as well as to protect those exposed in childhood from later undue strain.
The children the nurse sees are usually those in contact with a tuberculous father or mother. What is gained if we teach the parent to sleep alone, and spend part of the time away from them, yet permit him at other times to remain in close 160contact with the children? Intermittent contact, repeated often enough, is as bad as constant contact. If a mother nurses, feeds, cooks for, and handles her child, there are untold opportunities of infection. If the parent is intelligent and unselfish, it may be possible to bring about a relative degree of carefulness, and a minimum exposure, but there is no such thing as adequate carefulness while these conditions continue. Among the very poor, where it is impossible to regulate living conditions, there is practically no doing away with the danger of infection.
Whenever the parents are sick, selfish, or ignorant; when the children are undisciplined and uncontrolled, and where the grind of poverty has reduced ethics to the most primitive basis, one cannot expect much. When a child is in constant contact with a tuberculous individual, no matter how careful that individual may try to be, there is always some danger. By the very nature of his disease, a consumptive cannot be a hundred per cent. careful. An adult living in contact with tuberculosis may be able to resist it, a child has infinitely less chance.
The only way to ensure absolute safety for the child is to remove it from the danger, or to remove danger from it. Either the child must be removed 161from the house, or the patient must be removed from the house, it makes little difference which. The patient may be sent to an institution, or the child may be sent to a relative, to the country, to a neighbour, or to one of the child-saving agencies that are to be found in most communities. We are aware that in advocating this policy we are advocating what is called by the unthinking “breaking up the home,” as if tuberculosis had not long ago preceded us in this. Sending away the parent or the child is merely a belated effort to save what is left of the home.
Whenever an institution is possible, the patient should go there. In many communities, however, there are no such facilities, or else their capacity is limited. In this case, the child is the one to be removed. This often becomes a matter of extreme difficulty, since it is hard to overcome the parent’s very natural resistance. In urging this separation, we are making a choice between two lives—one already doomed, and the other which may be saved from a similar fate.
Tuberculosis in Children. Although children become infected at an early age, it is often most difficult to obtain a diagnosis for them. The most competent specialist hesitates to pronounce a child tuberculous until he has repeatedly examined it, 162and kept it under constant observation—and even then he may prefer to call it “suspicious only.” By the aid of the eye test and the skin test he may finally arrive at a positive diagnosis, but even then, he may not be sure of the location of the lesion. The child, therefore, though diagnostically a positive case, is not necessarily an infectious one.
All these doubts and difficulties in connection with the diagnosis of tuberculosis in children serve to show that in a way this question may be called a negligible one, negligible, that is to say, as a menace to public health. It is important for the individual that a diagnosis be made, in order to do intensive work in upbuilding his resistance, but he is negligible as a distributor of infection. About ten per cent. of the visiting list is made up of children. On entering a home where there are two children, one tuberculous and one not, the nurse’s efforts should be concentrated on separating the two—the emphasis being placed on the care of the one as yet uninfected.
The question frequently arises, Should these tuberculous children be sent to school? Is it well for them as individuals, from the standpoint of their own health, and is it well for those who are thrown in contact with them? This decision rests solely with the physician, and can be made 163by him alone. As far as danger to others is concerned, it must be remembered that while a person may be tuberculous, he is not necessarily infectious, and it is upon the infectiousness of a case that the danger depends.
It is difficult to care for these tuberculous children. Most nurses become deeply distressed because of this. The children are frequently undisciplined, and their parents often weak and lacking in self-control. The nurse becomes discouraged and annoyed when she sees her directions unheeded or disobeyed. But, after all, these cases constitute but a minor part of the problem, and they are not patients who do much harm. It is sad to stand by and see the individual throw away his chances, or to see them thrown away for him—but this standing by is part of the work.
Open-Air Schools. During the past five or six years, open-air schools or classrooms have been established in several of our large cities. This is an excellent affirmative answer as to whether a tuberculous child should attend school. At these places, careful, systematic attention is given the child for several hours a day. Non-tuberculous children are also admitted—they may be called pre-tuberculous, since they are anæmic, run-down, undernourished children, who come from homes 164where tuberculosis exists in active form. For such cases, the open-air school does excellent preventive work, in raising the child’s resistance to a point where it can cope with the exposure at home. These open-air classes are always in charge of a physician and a nurse; their management does not come within the range of this discussion, any more than does that of the hospital or the sanatorium.
The public health nurse must always take advantage of these schools, if they exist, and must see that her children are sent there. She must avail herself of every agency and of every opportunity which will improve or secure the welfare of those under her charge.
Schools of this kind are extremely valuable, but are not the solution of the tuberculosis problem, any more than the sanatorium for the early case is its solution. Both of these institutions deal with results, not causes. To fight tuberculosis, we must strike deep at the cause—the advanced case who scatters the disease. Open-air schools always make a strong appeal to people—it is easy to obtain money to support them, and easy for public sentiment to exaggerate their value in the anti-tuberculosis campaign. Since the public mind generally grasps but one idea at a time, it is 165not well to dissipate its facile interest on side issues. When a community has established on adequate scale the machinery for combating tuberculosis, it may then establish such effective allies as the open-air school. But to bring them on first, before the fundamentals, is to misdirect public sentiment, and to place the cart before the horse.
The Danger of Sending Patients to the Country. Sooner or later, the nurse will be called upon to decide whether the tuberculous patient shall be sent to the country. This will be urged by earnest, well-meaning people—and sometimes by social workers who should know better. Needless to say, this policy calls for strong condemnation. Whatever good the patient himself might gain from going to the country, must be offset by the fact that the disease is spread elsewhere. To create new centres of infection is not the result at which the tuberculosis campaign is aimed.
In his own home, under immediate and constant supervision, it is difficult to obtain from the patient anything better than relative carefulness. To get even that requires unceasing vigilance and continual training, both of the patient and of his family. Therefore, to free him of this restraint by sending him to a distant farm, would mean his immediate relapse into carelessness, and a 166danger to those among whom he is quartered. To send a consumptive into another household is to send him where he may infect other people. Pity for the patient should not obscure our interest in his possible victims.
Moreover, the welfare of the patient himself is not as a rule secured by this method. These journeys to the “country” are usually to out-of-the-way little farm-houses, with various shortcomings both as to food and accommodation. They are often anything but satisfactory places for a sick man; or, if they happen to possess advantages, the patient may not know enough to use them. In making these statements, we are not speaking entirely at random, or from general surmises as to probabilities. A few years ago, we had on our visiting list some fifty-five patients who went to the country for the summer. They were in all stages of the disease, and it is well to note, in this connexion, that it is usually the advanced case who is most anxious to get away. Of the fifty-five cases, two were really benefited by their sojourn; thirteen were temporarily improved, but lost it all within a few weeks after their return; thirty-two came back to town worse than when they went away, and eight died while in the country.
167Of these fifty-five removals, it is safe to assume that fifty-five centres of infection were established in consequence. The families where they were quartered were doubtless unaware of the nature of the disease, or how to protect themselves in any way. Nor is it likely that any of these fifty-five farm-houses were afterwards properly cleaned or disinfected. It was of course impossible to follow the results in these scattered centres of infection—remote counties of Maryland and Virginia—but we succeeded in doing so in one instance out of the fifty-five. In this case, the patient had gone to a farm in Virginia; as a result of his visit, three members of a hitherto healthy family became infected, all of whom have since died, as well as the original patient, the “city boarder” who carried infection among them.
Of course, if patients insist upon going to the country, nothing can prevent them, although the nurse must do her best to dissuade them. One patient who had a large airy room in town, decided that she would be better off on a farm. She was questioned as to conditions at the farm, and it transpired that she was to occupy an attic room, with one window, and that this room was to be shared with three other people. It then became an easy matter to dissuade her from going. It is 168not always thus easy to deflect them. Should they insist, they should be given plentiful supplies, and if the nurse can obtain the address of the family where they are to stay, she should send full information as to the patient’s condition. It is a regrettable fact, but when a patient is removed from surroundings where his condition is known, he is apt to discard his sputum cup and all other precautions by which he is rendered conspicuous.
We cannot be too emphatic in refusing to send consumptives to the country. If a sanatorium or day camp is not available, they would better remain in the city. If the patient has money, he cannot of course be prevented from going. If he has no money, no appeal should be made for funds to send him away. To ask for money for such use is a wrong the public health nurse should have no hand in. Her business is to prevent scattering infection, not to aid in it.
Disinfection of Houses—Value of Fumigation—Formaldehyde—House-Cleaning—Burning and Sterilizing—Boiling—Carpets, Rugs, and Mattings—Painting, Papering, and Whitewashing—Temporary Removals—Vacant Houses—Compulsory Cleaning.
Disinfection of Houses. One of the most important of the nurse’s duties is her arrangement for the fumigation and cleaning of premises that have been vacated by a consumptive. This takes place after death, or upon the patient’s removal to an institution, to another house, or to another room in the same house.
Since tubercle bacilli are not confined to the sputum, but are discharged in great numbers during coughing attacks, and to a less extent during sneezing, speaking, and so forth, a patient not confined to one room, but who wanders freely about the house, scatters bacilli everywhere. No matter how careful he may be about the sputum, the nature of the disease makes it practically impossible to be equally careful about the expired air. Moreover, these organisms do not die of 170themselves, at the end of a few weeks. They are singularly tenacious and persist for months, virulent and active. A case is recorded in which they were found in a room six months after the patient’s removal, alive and virulent enough to cause tuberculosis in guinea-pigs inoculated with them. For this reason it takes drastic measures to rid a house of these tenacious germs.
In indicating the rooms to be fumigated, it is necessary to include all those that have been occupied by the patient within the past six months. If he dies in his bedroom, it is not enough to do merely that one room. It is equally necessary to fumigate the kitchen, in which he sat until two months ago; the parlour, where he spent a few hours a day, and the second bedroom, to which he was now and then removed. All are infected, and all need the utmost care to free them from germs. The family must be taught why these rooms are dangerous, and made to understand the necessity for full and complete disinfection. It is better to err on the side of too much, rather than of too little care.
In Baltimore, the actual fumigation is not done by the nurses, but by the employees of the Fumigation Division of the Health Department. The nurse indicates the rooms, instructs the family, 171and makes all the preliminary arrangements, after which she reports the premises to the fumigator, who disinfects them next day. It would be well if this fumigation could be done by the nurses or by a special corps of nurses; this would probably ensure more intelligent and conscientious work than that which the average city employee bestows upon this important task.
As a matter of routine, every death from pulmonary tuberculosis is reported to the Tuberculosis Division; the nurse in whose district this death has occurred then inspects the house and arranges for the fumigation. Four times out of five the patient is already known to us and already under supervision, which makes the duty easier than if he were unknown. In either case, however, the nurse visits the home and arranges all the details.
In like manner, all patients who enter either hospital or sanatorium are reported to the Health Department, the institutions furnishing their names and addresses so that the fumigation may be attended to. When a patient changes his address and moves to other quarters, the nurse is the only one who knows of this change, hence it is her responsibility to report these houses and see that they are fumigated. To arrange for all 172these fumigations, whether after death or after removal, means that a large amount of time is spent upon this work of trying to rid the community of dangerous centres of infection.
Value of Fumigation. The actual value of fumigation is a debatable point. Under the best conditions, its efficacy is not a hundred per cent.—far from it—while under unfavourable conditions, when poorly done, its efficacy is so low as to be almost nil. The house whose cracks have been improperly stopped, and the old house, with open chimneys, loose windows, and apertures which cannot be closed, are not made safe by this process. Under such conditions, fumigation not only fails to remove the danger, but it produces a false sense of security. Unless properly done, it were better not to do it at all. We should prefer instead to depend upon vigorous house-cleaning, the use of hot water, soap, and the scrubbing brush, and the destruction of all infective material. Moreover, even under the best conditions, formaldehyde has no powers of penetration. Its action is purely superficial, and only useful for plane surfaces, such as walls, ceilings, and so forth. The most dangerous articles, such as clothing, carpets, bedding, and the like, are totally unaffected by it. We ought to stop teaching 173that fumigation alone will clear up these infected houses and make them safe for future habitation. The public has been misled as to the value of this measure, and allowed to place far more reliance upon it than has been justified by experience. It is high time for enlightenment. The most that can be said for fumigation is that undoubtedly it kills some germs—so many that it is worth while to continue the practice of it, but too few to afford adequate protection. It must be supplemented by other and more radical measures.
Formaldehyde. Formaldehyde in one of its preparations is the chemical most generally used, and is more valuable than sulphur, which is now discarded. In most cities, the Health Department attends to the fumigation. In small towns or rural districts, where there is no fumigating corps, formaldehyde is usually given upon application to the local or State Board of Health. In some localities, especially in country districts, there may be no appropriation for this disinfectant, which the householder must then buy himself.[4]
4. There are many formaldehyde preparations on the market, simple and easy to use, but these may be unobtainable. In this case, an effective method is the combination of formaldehyde with potassium permanganate. For a room containing 1000 cubic feet of air space (a room 10 feet long, 10 feet wide, and 10 feet high), the amount needed is: Potassium permanganate, oz. 111.; liquid formaldehyde, pint 1. Place the formaldehyde in a large galvanized iron bucket (holding 8 to 10 quarts), and drop the permanganate into it. The room should be left closed for six hours; a longer time is unnecessary, a shorter time ineffectual. All cracks, of course, should have been previously stopped.
174Since fumigation is only a matter of six hours’ duration, it will cause no great hardship or inconvenience to the family which for this short period must be turned out of the house. Yet many people complain bitterly over this trial, and raise every possible objection. They are willing enough to have one room done, but refuse to allow more. The nurse must explain that a six hours’ inconvenience is better than risking health and life, and she should also explain that in insisting upon fumigation the Health Department is neither arbitrary nor vindictive. Fumigation is a rather costly affair, and this expense is incurred, not to annoy but to protect the community. In winning over a reluctant family she has a chance to do excellent educational work. It is always better to secure their intelligent co-operation, even though it take long and patient argument, than to end the discussion by abruptly informing them that fumigation is compulsory, and will be done whether desired or not.
House-Cleaning. Fumigation must always be followed by most searching and thorough house-cleaning, which important task must be done by 175the family itself. All floors should be scrubbed with hot water containing lye or soda solution and all washable surfaces should be likewise treated. This includes furniture, doors, door knobs, windows, stairs, banister rails, and so forth. The necessity for this house-cleaning cannot be too strongly emphasized.
Burning and Sterilizing. The most highly infective material is the bedding, mattress, pillows, clothing, and so forth, which have been used by the patient. Since these articles cannot be made safe by formaldehyde fumigation, and since most of them cannot be washed and boiled, there are but two methods of disposal. The most drastic and wasteful is to burn them, yet this must always be advised unless we can offer the alternative of sterilization under high pressure steam. To burn infective material involves a loss which few people can afford, and they are loth to make the sacrifice; most of these articles, while laden with germs, are nevertheless serviceable and in good condition. To expect that they will be burned, therefore, is to expect the impossible. If the family consent to destroy certain articles, they reserve others, equally unsafe for use. The only alternative is the municipal sterilizer, and any community which expects to do effective 176preventive work must establish this as a factor of first importance.
In Baltimore there is such a sterilizer, and the use of it is very simple. When the nurse arranges about the fumigation, she selects at the same time whatever articles are to be sterilized—pillows, mattresses, blankets, clothing, and so forth. These are then called for by the men from the Fumigation Division. They are placed in large canvas bags, inventoried, labelled, and carried to the sterilizer. Here they are steamed and dried, and returned a day or two later in good condition. The householder signs a receipt to this effect.[5]
5. Certain articles are ruined by sterilization, and the nurse must be careful not to include these, or there will be a suit for damages. Leather and furs, can never be steamed. Straw mattresses are also injured. Nor is it possible to sterilize carpets and matting, because of their bulk. The sterilizer should be reserved exclusively for material which lends itself readily to treatment of this kind. In selecting what is suitable, the nurse should exclude old and filthy articles, which should be burned.
Unfortunately, steam sterilizing plants are rare, and in most communities the nurse will have to protect her patients in other ways. As we have said before, the only alternative is burning, and this often works great hardship on many families. With the very poor, the Federated Charities may be called upon to supply new mattresses, etc., in place of those that have been destroyed, and as 177a rule this response is prompt. Yet there are many cases where the family is too poor to suffer this loss, yet not poor enough to come within range of a charitable association. These cases constitute a difficult problem—a problem that is entirely solved only by the municipal sterilizer.
Except through sterilization, there is no way in which these articles may be made safe. Carbolizing will not do this, neither will sunshine. Valuable as sunshine is, it is difficult to secure prolonged exposure, especially in tenement districts. It is possible, of course, to take a mattress apart and wash and boil the ticking; feathers or hair may be sent to an upholsterer, who has means of steaming them. Pillows may be put into a large wash-boiler, and boiled for half an hour, after which they may be washed—it will take a week or more before they become thoroughly dry and usable. All these alternatives involve a great outlay of time and energy, and we cannot but feel sceptical as to the thoroughness with which this cleaning is likely to be done. A family which objects to parting with dangerous articles, and prefers risk to inconvenience or deprivation, is hardly likely to be scrupulous as to details of this character.
In Baltimore, before the advent of the steam 178sterilizer, the amount of material burned was never more than a third of the amount which should have been burned. Still, under the circumstances, we were thankful to have achieved this third. Since the establishment of the sterilizer, we now succeed in getting over two thirds (70 per cent.) of the infective material sterilized. This is a triumph for the nurse’s teaching, since there is no law making sterilization compulsory.
Boiling. Everything which can be boiled will of course be made safe, whether these articles be of wool, linen, china, rubber, etc. Even blankets may be boiled, although the family will object to this on the ground that it shrinks them. The nurse must explain that not to boil them may have consequences even more disastrous. The nurse must never permit her patients to make indiscriminate bonfires, and wantonly destroy harmless articles, or those which may readily be made so. We know one family which destroyed a whole set of dishes, not from painful association, but from a misdirected desire to do the right thing. For this reason, the nurse must look over all articles carefully, giving thoughtful counsel as to the proper disposition of each.
Carpets, Rugs, and Mattings. As the sterilizer cannot be used for carpets, rugs, and mattings, 179there is nothing to do but advise that these articles be burned. As a rule, this destruction is agreed to with more readiness than in the case of pillows and mattresses.
Painting, Papering, and Whitewashing. Whenever possible, the rooms used by a consumptive should be repapered, painted, or whitewashed as the case may be. The more thorough and complete the measures taken to eliminate tuberculosis, the greater the chances of success. It is a costly disease, and costly measures, both as to money, energy, and time, are required to get rid of it. Half-way methods are poor economy.
Temporary Removals. The foregoing directions apply mainly to those cases in which the patient has either died, or has been permanently removed elsewhere. If his return is not expected (as when an advanced case enters the hospital), the amount of cleaning, burning, repapering, etc., would naturally be as great as that required after death.
On the other hand, when his removal is but temporary and the patient expects to return home after a few months, the amount of disinfection would be considerably modified. When he enters a sanatorium, his house must be fumigated and cleaned, so that for a few months at least the family 180may be relieved of danger. Under such circumstances, it would not be necessary to counsel the destruction of the mattress and bedding that he is to use upon his return. Meanwhile, no other member of the family should use these things, although in certain instances it is almost impossible to prevent their doing so. For such cases the municipal sterilizer is needed—indeed no community can make much headway against tuberculosis until it provides a means of removing the danger without causing loss to the individual.
Vacant Houses. When a family’s removal leaves a vacant house, there is naturally no one left to do the cleaning. The Health Department will do the fumigation, but the more essential house-cleaning remains undone. These houses often stand idle for weeks or months before finding a new tenant. Even if it were possible to discover the landlord or owners (a task which in itself would require a staff of employees), it is doubtful whether they would clean these houses themselves, or notify their new tenants of the need for extra vigilance. Legislation compelling house-cleaning would be difficult to put through. The landlord feels relieved of all responsibility when once the fumigation is accomplished, and that this fumigation is not a hundred per cent. effective is no concern 181of his. He, together with the general public, has been misled as to its true value. Nor is thorough cleaning, painting, and papering an expense that he would willingly incur. The question of the fumigated but not necessarily safe house is one that causes considerable anxiety. We feel that the only way to deal with it, is that the nurse keep these vacant houses on her visiting list, so to speak, and watch for the time when they are re-let. This entails considerable loss of time, which she can ill afford to spare from her patients, but the information she can give the new tenant will have distinct preventive value. She must tell the newcomer that he has moved into a house in which there has been tuberculosis, and that only by the most exact and painstaking efforts can it be made safe.
Concessions. In carrying out this important work, the nurse sometimes becomes so enthusiastic that her common-sense gives way under the strain. She wishes to carry her point, without fully realizing the prejudices, ignorances, sometimes even the comfort, of the family she is dealing with. After a death, she comes upon a household in a most upset, distressed, and often irresponsible condition, and she must be very gentle and patient in her relations with them. She must accomplish what 182is necessary, without undue disturbance of their prejudices and feelings. For example: Orthodox Jewish people observe a mourning period of several days following death, during which time they wish to remain undisturbed. Fumigation should be postponed until this time is past. A few days’ delay will not injure the health of a family which has been exposed to infection for months. By thus respecting their religious customs, it will be possible to gain better co-operation as to cleaning and so forth; co-operation which would have been jeopardized by riding roughshod over their feelings and beliefs.
Sometimes people raise objections because they have nowhere to go for the six hours required for fumigation, during which time they must leave the house. If there is no kindly neighbour to take them in, the nurse may arrange with a Settlement or other social agency, to give them shelter. We have often asked for hospitality in this way, and have always met a ready response. Sometimes, if a house is a large one, it is possible to have it fumigated in sections, a few rooms being done one day, a few the next.
Compulsory Cleaning. In most communities, fumigation is compulsory. But there is no regulation whatever concerning the after-care of the 183premises—the cleaning, sterilization, and destruction of infective material. The relatively unimportant part is obligatory, while the essential part is optional. And that this essential part is done, and well done, depends almost entirely upon the teachings of the public health nurse.
If, however, the family remains obdurate, refusing to clean and disinfect, nothing can be done. Since it is now generally acknowledged that fumigation falls far short of what it was once expected to do, we need laws making adequate disinfection compulsory; until such laws are enacted, we can only rely on the ability of the nurse to teach the necessity for cleaning and disinfecting. How valuable is this teaching may be gathered from these figures (Report, 1913, Tuberculosis Division of the Baltimore Health Department): “After death: houses cleaned, 80 per cent.; bedding, etc., either burned or sterilized, 70 per cent.” With adequate laws, the nurses would make even a better showing.
The Tuberculosis Dispensary—Equipment—Medicines—Hours—Consideration of Patients—Function of the Dispensary—The Physician’s Service—The Physician’s Qualifications—The Physician and the Patient—Duties of the Nurse—Tuberculin Classes—The Nurse in Home and Dispensary—The Nurse as an Asset to the Community.
The Tuberculosis Dispensary. No community can make definite progress against tuberculosis until it establishes a place where suspicious patients may be sent for examination and diagnosis. Unless this disease be promptly and definitely recognized, it is impossible to give advice, or take authoritative action concerning the treatment of the patient and his family. If in connection with the dispensary there was also a corps of municipal physicians, who could visit the patients in their homes, and examine all suspects called to their attention, diagnoses could be obtained even more promptly. As it is now, considerable interval often elapses between the time when the patient is advised to go to a dispensary and the time when he follows this advice. The existence of a corps of visiting 185physicians would prevent such delays. The patient would be allowed a reasonable time in which to present himself, at the expiration of which period he would be sought out by the officer of the municipality. This prompt recognition of tuberculosis would save the community from an enormous amount of exposure. The time may yet come when Departments of Health will see the wisdom of such measures.
Until that time, the special dispensary represents the only means of obtaining a diagnosis; it is the only place where patients may freely be sent, and where an expert and frank opinion may be had. Such a dispensary may be established in connection with the general dispensary of a hospital, or by the local Health Department, or it may be supported by the same group of people or association which supports the special nurse. In Baltimore, we have had dispensaries of all three kinds, and the nurses have worked in connection with each one, on exactly the same terms.
Equipment. The great tuberculosis dispensaries run in connection with the large hospitals and medical schools are usually very completely and elaborately equipped. They contain large waiting rooms, examining rooms, special rooms for the giving of tuberculin, for X-ray examinations, 186for throat examinations, for laboratory work, and so forth. All these are needed in teaching centres, where it is necessary to collect certain scientific data. But for the purpose of making an ordinary physical examination a simpler equipment will do equally well.
In Baltimore there are several small municipal dispensaries, all under the control of, and managed by, the Department of Health. They are situated in different parts of the city, readily accessible to the patients of different localities. Each dispensary consists of two or three rooms, which are in the same building which houses the Federated Charities, and other social agencies. This arrangement has several advantages, from the point of view of both economy and co-operation. To have rented similar rooms in another building or in a private house would have meant a much greater outlay of money, to say nothing of the opposition encountered in obtaining the use of these rooms for dispensary purposes.
The furnishings of these little municipal dispensaries are extremely simple, but they lack nothing of comfort and convenience. The outer or waiting room contains two or three dozen chairs, or benches to accommodate an equal number of people. A corner of this room is screened off for the nurse’s table, where she keeps her charts and records, and writes the patients’ histories. A couple of filing cabinets, a medicine closet, and a pair of scales complete the outfit.
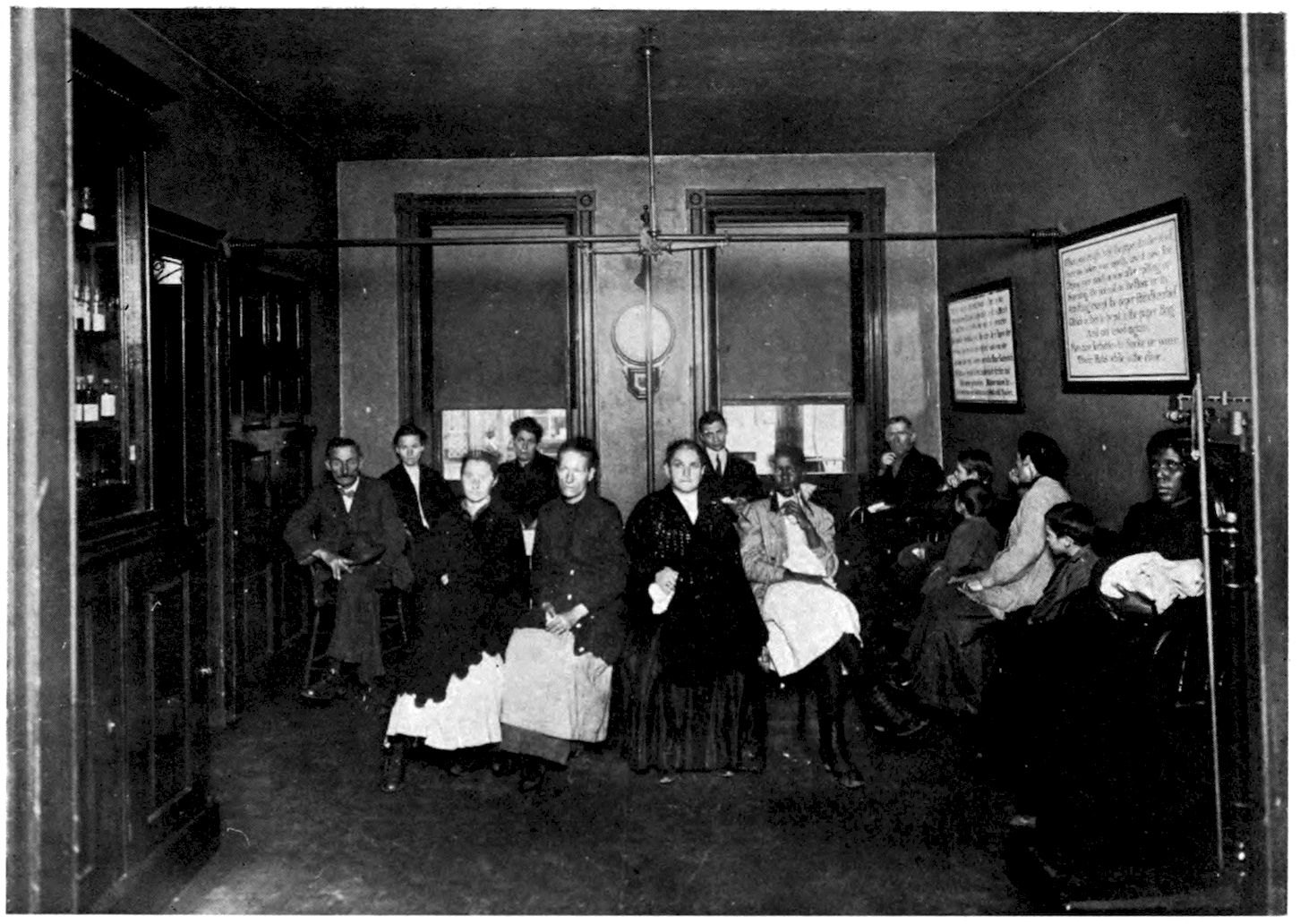
Waiting Room in Municipal Dispensary
187The inner, or examining room, is also simple and inexpensively furnished. It is divided into several compartments by means of gas piping, each compartment being large enough to hold a revolving stool and a wicker lounge. Unbleached muslin curtains hang from these gas-pipe rods, making several little cubicles in which the patients are examined. It is thus possible for the doctor to examine a patient in one cubicle, while another patient undresses in the adjoining one—an arrangement which saves considerable time. Sheets, towels, and blankets complete the necessary furnishings, which may be cheap or costly according to the means available. The doctor’s table stands in one corner of this examining room.
This is not necessarily the last word as to what tuberculosis dispensaries should be, but we have found the ones described practical. No tuberculin tests are given here, and all sputum examinations are made at the Health Department laboratory.
Medicines. A supply of simple drugs is kept in the medicine closet. This includes a few of the standard tonics, such as iron, quinine and strychnia, 188nux vomica, gentian and alkali, and so forth; there are also cough syrups, and heroin, codeine, cascara, etc. The tonics are usually bought in large quantities, in gallon jugs, and in her leisure moments the nurse pours them into four- or six-ounce bottles. If these bottles are filled by the druggist, the expense is somewhat greater. This medicine is given free of charge, although now and then a patient may wish to make a small payment of ten cents or so. In themselves, these drugs cannot be said to constitute treatment, yet it has been found advisable to dispense them. Patients are so accustomed to being dosed, that they have no faith in an institution which does not prescribe for them. It is above all things necessary to make these dispensaries popular, so that patients will freely seek them, and recommend them to their friends. Only through wide publicity and extensive patronage can they become effective factors in the fight against tuberculosis.
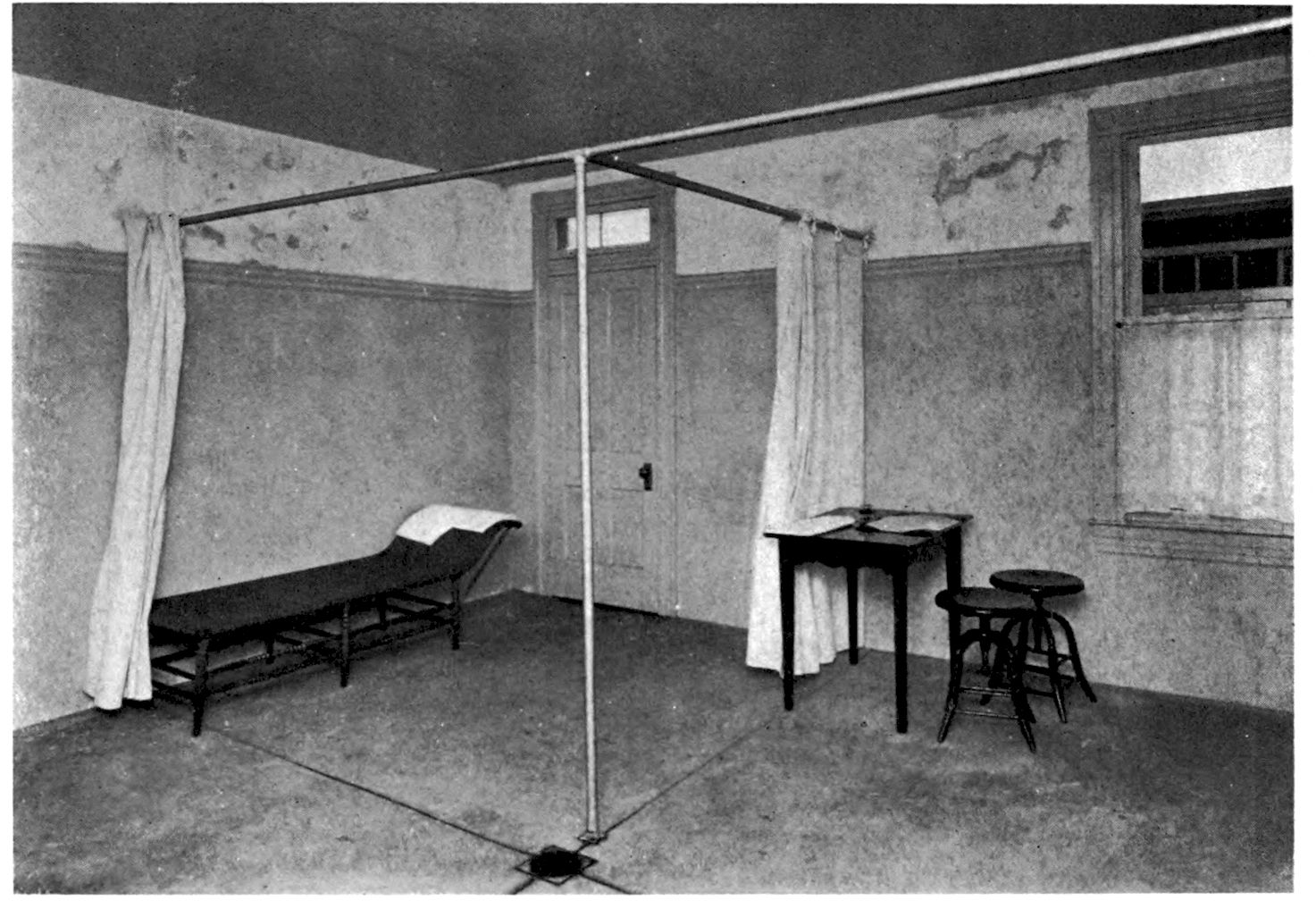
Examining Room in Municipal Dispensary, showing the room divided into cubicles, by means of gas-piping
189Hours. The hours at which a dispensary is open will depend somewhat upon its location, also upon whether or not the physician’s services are volunteered; in the latter case, it will depend upon the time he is able to give to it. If it is open in the morning, the workingman cannot attend without losing a whole day from his work, nor are these hours convenient for schoolchildren, or for the busy housewife who does most of her work before noon. If the dispensary is open in the afternoon, all three classes of patients may be accommodated; the workingman will lose half, not an entire day, while women and children can attend with no inconvenience at all. Afternoon hours, say from two till five, not only permit patients to be examined by daylight instead of artificial light, but the doctor will be further aided in his diagnosis by the presence or absence of that characteristic symptom, an afternoon temperature. Night clinics are necessary in certain localities, when they may be patronized by men and women, employed during the day, who would otherwise be unable to come to them.[6]
6. Night clinics are in existence in New York, Hartford, Boston, Chicago, and other cities, and are well attended.
Consideration for Patients. The first consideration of the dispensary should be the comfort and welfare of the patients. We have known many dispensaries where the first consideration was the experience of the students or physicians, the patient being regarded merely as good clinical material. In dispensaries connected with medical schools, which are essentially used for teaching purposes, this condition is unfortunately necessary, 190yet we cannot believe that it is necessary to the extent to which it is sometimes carried. We have often known of “interesting” cases being held up for hours, in order that they might be examined by certain men, or groups of students; moreover, this detention, prolonged examination, and exposure often took place when the patient was very weak, when he lost his job through the delay, or when a husband’s dinner, a nursing baby, or a houseful of children made such detention intolerable. Patients often refuse to return to a large dispensary on the ground that “they keep you all day, everyone in the place examines you, and you get so tired and sick you have to stay in bed for a week afterward.” This lack of consideration—failure to look upon the patient as a human being—is what tends to make dispensaries unpopular. We have known patients to come straight from such an experience and deliver themselves into the hands of a quack. However necessary it may be to use certain dispensaries as teaching centres, the tuberculosis campaign demands clinics of another kind. If the tuberculosis dispensary is to be a factor in the fight against this disease, it cannot afford to be a training school as well—it should be in charge of men already trained.
Function of the Dispensary. It follows, then, 191that the function of the municipal dispensary is of necessity different from that established for teaching purposes. The larger dispensary serves a double purpose, the little dispensary serves but one; it is an examining station for making diagnoses. Here the patient should come as informally as he would to a doctor’s office, and here he should be able to consult experienced men. We feel that the informality of these little clinics constitutes their strong point. The patients are not afraid of them, and their great advantage lies in their social rather than their scientific value. They are merely places where a communicable disease may be discovered at the earliest possible moment.
The Physician’s Service. If a community decides to establish a dispensary, the first step must be to secure the services of a physician. At first this may be voluntary, and many doctors will gladly offer an hour or two of their time, once or twice a week. Should there be great pressure of work, it may be possible to find several men willing to offer their time. But however willingly and freely offered—for most physicians are generous in response to calls of this sort—it must be remembered that, after all, this service is gratuitous. The busy physician will often be obliged to side-track his dispensary obligations, in favour 192of urgent private calls. This is only to be expected, yet too many such side-trackings are bad for the dispensary. The patients lose confidence in it; it is discouraging for a roomful of sick people to find no one to receive them.
Experience teaches us to look askance at all volunteer work, no matter how generously or sincerely offered. Under certain conditions it may have to be accepted, but whenever possible, the physician in charge of the dispensary should be paid. It is fairer to him, and fairer to the patients.
The Health Department of Baltimore has three special tuberculosis dispensaries, each open twice a week, for two hours at a time. The physician in charge is paid a good salary, and as a result, the regularity of his attendance is in sharp contrast to that in certain other dispensaries, where the work is done by well meaning but overworked men who volunteer their services. Tuberculosis is a disease that cannot be overcome by volunteer work or economical methods.
The Physician’s Qualifications. The success of the dispensary depends upon the ability and character of the physician in charge. He should be able to make a diagnosis by means of auscultation and percussion, without hesitating to commit 193himself until a sputum examination reveals the bacilli.[7] For if finding the bacilli is to be the sole test by which tuberculosis may be recognized, it would be possible for the nurse to obtain specimens of sputum from her patients and submit them to the laboratory direct—thus doing away with the doctor and proving the dispensary superfluous.
Nor is this all. The physician must have a strong social sense, and be able to inspire his patients with confidence. In no other work does the personal character play so large a part, and this applies to the doctor as well as to the nurse. One of our patients, enthusiastic in her praise of one of the dispensary men, summed this up with homely accuracy: “He couldn’t have been nicer to me if I’d paid him fifty cents in his office.”
The Physician and the Patient. After the patient has been examined, the doctor carefully explains to him the nature of his disease, and the precautions necessary. Since these directions must often be brief and hurried, he will further add that he is sending a nurse to the patient’s home, to act under his orders, and see that certain directions are carried out. In this manner, the doctor prepares the way for the nurse’s visit, and gives her an authority which greatly facilitates 194her work. With this assistance, it is far easier to gain the patient’s confidence than if it has been forgotten or withheld. The orders concerning the patient are then given to the nurse, and if these include admission to an institution, it is her duty to arrange all the necessary details, and so relieve the physician of much time-consuming work.
Duties of the Nurse. If a community has a special dispensary as well as a special nurse, the nurse’s duties are twofold, and should include not only the home supervision of the patients, but attendance at the dispensary as well. She is the connecting link between the two. In this way, her intimate knowledge of home conditions is placed at the physician’s disposal, who is then able to give sounder advice and deal more intelligently with his patients if he has some knowledge of their environment.
The nurse’s presence at the dispensary is often a considerable assistance in persuading patients to come. Patients are often frightened and shy, and dread the unknown, consequently it is better if the nurse can give them the comforting assurance that she will be on hand to welcome them. From her knowledge of their home conditions, she also knows which cases can afford to wait, and which should be taken out of turn and given immediate 195attention. It is thus possible to deal with them in a personal and intelligent manner. Since at present the control of tuberculosis lies largely with the patients themselves, and depends almost wholly upon their good-will and co-operation, it is necessary to establish this co-operation as firmly as possible.
The duties of the nurse consist in taking the history of the patient; taking his weight and temperature, and preparing him for physical examination. If the patient is a woman, she must be present while this examination is made. She also gives such drugs as may have been prescribed. On his arrival, each patient receives a paper napkin to hold over his mouth during coughing attacks, and to use for expectoration. A special receptacle should be provided for these soiled napkins, and they should afterwards be burned. The nurse should come to the dispensary half an hour before it opens, in order to put it in readiness,—to take out the charts and histories, attend to the drugs, place towels and sheets in the examining rooms, and so forth. Whenever the clinic becomes large enough to require it, it will become necessary to place the clerical work in charge of a clerk.
In these informal clinics considerable trouble is 196often caused by patients who arrive just before closing time, and expect to be examined. It is unwise to encourage this sort of tardiness, and a time limit should be set and strictly adhered to. All patients arriving after a specified hour should be directed to come another day, except such patients as are recognized by the nurse as worthy of exception from this rule. The most frequent offenders are not the patients who come from a distance, but those who live just around the corner. Unless punctuality be insisted upon, there will be endless overtime work for both doctor and nurse.
Tuberculin Classes. At some of the large dispensaries, selected cases are formed into what are called Tuberculin Classes, and given special treatment. These patients are very carefully chosen, both from a financial as well as a physical standpoint, and intensive work, of a curative rather than a preventive nature, is put upon them. The treatment is carried out in their homes, where as nearly as possible sanatorium conditions are attained. Unruliness, or failure to comply with the regulations, means being dropped from the class. These patients live on a carefully planned routine, carried out under close supervision of both doctor and nurse. They report to the dispensary 197at certain intervals, once a week or so, and there tuberculin is administered, weights taken, and examinations made. Each patient keeps a little book containing a daily record of his doings, including the number of hours spent in the open-air, food—kind and amount, exercise, temperature, cough, and other symptoms. This book is presented at each visit to the dispensary, and the nurse also inspects it when she visits his home. These class patients often do extremely well, and excellent results are often obtained. Like all work of a curative nature, however,—in which the subjects are carefully selected and as carefully rejected,—it deals with so few people that it makes no real impression on the situation. The tuberculosis problem is, what can be done for a thousand patients, not for twenty. It is always possible to select a handful of cases and maintain them indefinitely at a high level of health, by a considerable outlay of money, energy, and time—an expenditure from which the community as a whole derives little benefit.
To establish a tuberculin class is purely a physician’s affair, and all directions in regard to it come from the doctor himself.
The Nurse in Home and Dispensary. When the staff is large and there are several nurses, it 198may seem advisable, upon first consideration, to assign one nurse solely to dispensary duty, and leave the others to work in the homes. It is a better plan, however, to let all the nurses combine service of both kinds, as the single nurse in the small community must do. The intimate connection between home and dispensary should never be broken—it is much too valuable. Moreover, as far as the nurse herself is concerned, the monotony of dispensary work becomes extremely wearing, and it is well to vary it with duty in the home. It is a regrettable fact that a nurse confined to mere mechanical routine, is apt to lose that fine understanding and sympathy which she needs in her work, and which is always lost whenever human beings become merely “cases.”
In Baltimore this service is arranged in the following manner: There are three Municipal Dispensaries, and one other clinic, managed on the same lines, although not connected with the Health Department. These are situated at the boundary lines of two or more adjoining districts, and are thus accessible to the patients as well as the nurses of the adjacent areas. All four clinics are served by certain nurses of the Health Department, who are on duty on alternate days or alternate weeks, as the case may be. Thus, the nurse 199from any one district is on dispensary duty for two afternoons a week, every other week. This deprives the home of her services to only a very slight extent—a deprivation which is counter-balanced by her increased opportunities for effective work. We should never advocate any greater curtailment of home work, however, since the home, or centre of infection, is always the chief point of attack.
From another standpoint it is well that the nurses combine both kinds of service. Through sickness or other reasons, it may become necessary to substitute one nurse for another, and it is an advantage to have nurses trained and able to relieve each other when necessary.
The Nurse as an Asset to the Community. We have hitherto considered the nurse as a public health nurse, or servant of the entire community. Whether supported by public or private funds, whether connected with the Health Department or a private association, we have considered her as ready to answer all calls made upon her. We have regarded her as at the service of all physicians, dispensaries, institutions, social workers, and laymen, ready to respond to all calls without hesitation or discrimination. Her unattachment to any claims but those of the community as a whole gives her this broad field.
200If, however, her work be limited to the patients of any one institution, association, or sect, she is no longer an asset to the community. For example, if she is employed by a certain dispensary to visit its patients only, her work is circumscribed. Her usefulness will be restricted—her service will be valuable to the physicians of such an institution, and she will collect data for their records, but her duties will be localized for the good of the dispensary, rather than for society as a whole. The same would be true if she be employed by a St. Vincent de Paul Society to care for Catholic consumptives, or by a Jewish organization to follow up Jewish patients—any arrangement through which she visits one patient in a block, but refuses the case next door, means a narrow field of service. She then becomes the nurse of an institution, or a sect, rather than a public health nurse. The object of her work is not the welfare of the community, but the welfare of certain individual patients. Incidentally, her work may benefit the community, but it falls far short of its possibilities. It must be supplemented by new agencies, with the consequent duplication and waste of effort that this always involves.
Our experience in Baltimore will illustrate this point. In 1904, when tuberculosis nursing was 201first organized, two nurses were placed in the field. One was attached to the dispensary, of the Johns Hopkins Hospital, the other placed in charge of the Visiting Nurse Association. Between them the city was divided into halves, one nurse working in the eastern, the other in the western portion of the town. The dispensary nurse visited only patients who had been to the dispensary. The nurse of the Visiting Nurse Association visited not only dispensary cases, but all patients reported from whatever source. Thus, in East Baltimore, if two consumptives lived in the same tenement, one a dispensary case and the other under no supervision at all, only one of these two was visited. In West Baltimore, both patients were cared for on equal terms. At the end of a year, another nurse was added to the Visiting Nurse Association staff, but not to the dispensary. The city was then redivided, this time into thirds, and again the patients were cared for under the same conditions. The dispensary nurse served the Johns Hopkins Dispensary; the Visiting Nurses served the dispensary and the community as well. Finally, in 1910, the tuberculosis work of the Visiting Nurse Association was taken over by the city, thus creating a new municipal department, the Tuberculosis Division of the City 202Health Department. At that time the dispensary nurse gave up visiting in the homes of the patients, and confined herself entirely to routine dispensary duties. This left all visiting work to the Health Department nurses, who were as punctilious in making reports to the dispensary as was the dispensary nurse herself. By this arrangement, the Phipps, in common with every other dispensary in the city, has had a large staff of nurses placed at its disposal. Both the dispensaries and the community gain through this co-operation.
The Nurse in Relation to the Institution—Reports Made to the Institution—Procuring Patients for it—The Value of the Sanatorium—Sanatorium Outfit—Return from the Sanatorium—Work for the Arrested Case—Light Work—Outdoor Work.
The Nurse in Relation to the Institution. As the nurse is the go-between from patient to physician, and from patient to dispensary, so also does her service link together patient and institution. This, of course, is only possible if she is a public health nurse—not if she is the agent for one institution alone, or if she is employed to serve one set of people instead of the community as a whole. Just as she should be at the service of every physician, dispensary, and layman who chooses to call upon her, so in like manner should she serve both hospital and sanatorium. She will act as beater-up in the matter of sending patients into these institutions; will arrange all details connected with their admission, and finally, upon their discharge, will take them again under her supervision and care. By this co-operation, the patient 204himself profits, likewise the community, while the institutions are enabled to keep in touch with their discharged cases, learn of their condition, and, through the nurse’s reports, add to their histories and records from time to time in a way which will greatly enhance their value.
There is complete co-operation between the various institutions of Baltimore and the nurses of the Health Department. Of the five institutions near the city, four admit both early and late cases, while one is for advanced cases only. Whenever a patient is admitted to or discharged from one of these institutions, either hospital or sanatorium, the Health Department is at once notified of the fact. Following admission, the nurse visits the home and arranges for the fumigation. Two thirds of the patients admitted are already known and under supervision, but whether known or unknown, the visit is made and fumigation arranged for in the usual manner. In homes where the patient is unknown, the nurse often finds suspicious cases, which she sends for examination and diagnosis. By means of this sharp look-out the visiting list is considerably augmented.
When the discharge of a case is reported, the patient may or may not have been under previous supervision. If already on the visiting list, the 205nurse merely resumes her visits. If not on the list, he is taken on at once. Needless to say, the physician in charge of the institution should prepare the way for the nurse’s coming, as should the physician of the dispensary. If he forgets to do so, the nurse may have some difficulty, especially with patients discharged in good condition, who see no need for her services. When discharged in bad condition, the reason is obvious enough, but in either case co-operation with the institution is necessary.
Reports Made to the Institution. The reports made to the institution vary in accordance with the wishes of the physician in charge. Sometimes they are informal, made on certain specified cases; sometimes they are extensive and deal with large numbers of individuals. The value of these reports is indicated by the following examples: Two months ago a young girl was admitted as a paying patient, but she is now at the end of her resources, which consisted of a small fund subscribed through contributions of her fellow-workers. If she is to remain longer at the sanatorium, she must be transferred to the free list. Or we find that a young man, admitted erroneously to the free list, is in a position to pay; in justice to the institution and those who perforce must accept 206its hospitality, this patient should be transferred to the paying side. Or we receive a letter from the superintendent, saying that a certain patient has failed to arrive on the day specified, and asking us to look into the matter. Upon investigation we may find that a death in the family, an accident, or the lack of railway fare has been the cause of his non-arrival. Provision for him to go can then be made—his place is not forfeited, but held for him until a more favourable time. These personal relations between the nurse and the institution bring a great sense of cordial understanding and mutual good-will.
The more extensive reports are managed as follows: Once a year, or oftener if necessary, certain institutions send to the Health Department a full list of their discharged patients, whom they wish looked up. The names and addresses are written on separate slips of paper, which contain a printed list of questions to be answered. These are distributed among the nurses of the different districts, each nurse being responsible for the patients in her own territory. Within a week or ten days all the slips are filled in, and a full return made on all cases submitted for investigation. This involves little extra work on the part of the nurses, since in nearly every instance 207the patients are already under supervision—and if through any oversight they are not, it affords a means of finding them. The superintendents of the various institutions find this a satisfactory way of keeping in touch with their ex-patients, and we think that this work is well within the field of the visiting nurse. Each gains by this co-operation—the Health Department, which wishes to supervise all consumptive patients, and the institution, which wishes accurate data for its reports. In effective social work the keynote of success is reciprocity.
Procuring Patients for the Institution. In still another way does the nurse serve the institution and that is by procuring patients for it. Large, well organized, and well equipped institutions have little difficulty in filling their beds, but this is often the reverse with those less known and less attractive. It takes much persuasion to induce a sick man to leave his home, and it often takes still more to persuade his family to let him go. To point out the necessity for institutional care, and induce the patient to take advantage of this, is the chief duty of the public health nurse. Only when she does this duty thoroughly and well does the demand for hospital beds exceed the supply. For example: in Baltimore, before the nurses went 208on duty, the large hospital for advanced cases was never more than half full. The community was not well enough educated to take advantage of it. Since the nurses have been on duty, however, not only has this hospital been filled to capacity, but the capacity itself has been enlarged to nearly double—while a long waiting list is constantly maintained. A small sanatorium was recently opened in Maryland, with a capacity of twenty beds; at the end of five months, it had only five patients. The nurses’ aid was solicited, and within a week it was full. This situation has also occurred in other cities, which found themselves equipped with excellent hospital accommodations, which the patients refused to make use of. Co-operation between the institution and the municipal or visiting nurses would doubtless have promptly remedied this state of affairs. Incidentally we may observe, the better managed and more comfortable the institution, the less difficulty there is in keeping it full. It must offer substantial advantages over the home—attractions which even the most ignorant and prejudiced must be trained to appreciate.
The Value of the Sanatorium. The sanatorium for the treatment of hopeful cases is by no means as valuable as was at first expected. The cure 209of tuberculosis is at best very problematical, and the sanatorium is chiefly useful to those who can control their environment upon discharge. Unless this can be done, treatment will be of little avail, although it will delay the inevitable end. The patient who comes from the alley and returns to the alley is foredoomed. And as most patients come from the alley, figuratively speaking, and are afterwards obliged to return to it, the results obtained by these sanatoriums are by no means commensurate with the expense involved in maintaining them. Whatever benefit is derived from them is for the individual, rather than for the community.
In the tuberculosis campaign, the sanatorium occupies a place of secondary importance. We could fight quite as successfully without it—possibly better, since the money devoted to the upkeep of these very costly institutions could then be diverted to more radical purposes. However, the sanatorium exists, and every patient should be given his individual opportunity. It is usually more difficult to get a patient into a sanatorium than into a hospital. The former is for early or moderately advanced cases, who have a reasonable chance of improvement, therefore it would seem a simple matter to induce them to go. Yet to persuade a patient that he needs such 210treatment, especially when he feels well and has few symptoms, is often a difficult task. The peculiar psychology of the consumptive, his optimism and refusal to believe that he has tuberculosis, is as well marked in the early as in the later stages of the disease. On the other hand, the difficulty is often of an economic nature. When the patient stops work, his income ceases, and this often determines his refusal. This is why many patients work until they drop in harness. Through the Charity Organization, or other similar agencies, it is possible to solicit aid for a certain number of these cases, and this must always be done. Such relief, however, is very uncertain, and latent periods of considerable duration often intervene between the time it is asked for and such time as it may be given. Even when given, it very seldom approximates the wages that the patient himself has been able to earn. Thus, a patient earns twenty dollars a week; with luck, we may obtain for his family an income of eight or ten. This is no reflection upon the Charity Organization Society, which has probably pulled every conceivable wire in order to raise even that amount—but it explains why the patient refuses the sanatorium and hangs on to his job until he can work no longer.
211In many cases on the other hand, there is no question of poverty to contend with—neither the wage-earner’s reluctance to stop work, nor the mother’s unwillingness to leave a houseful of little children. Instead, we must contend with ignorance, prejudice, and mental inertia—a moral alley quite as dark as that of the slum. One of the most discouraging features of this work is having to stand by and see the patient throw away his chances. Tuberculosis waits for no one, and it requires not only physical, but mental and moral strength to resist it. Before we can remake and reconstruct a supine individual, the disease wins out in the race.
There is one consolation, however; hopeful cases are usually far less dangerous than advanced ones. The refusal of sanatorium treatment is a loss to the individual only. Furthermore, we have this grim solace—when they finally consent to go, after weeks and months of delay, they do so, too late to help themselves, it is true, but at a time when they are most dangerous to other people.
Sanatorium Outfit. When a patient enters a sanatorium, the nurse must see that he is supplied with clothing heavy and warm enough for outdoor living. If he has money, he should be instructed what to buy. If he has none, these things must 212then be procured through some charitable association. No patient should be permitted to enter a sanatorium unless properly equipped, and frequently his decision against going is due to lack of such equipment.
In winter, he naturally requires much more than in summer. Roughly speaking, his wardrobe should contain at least two changes of flannel underclothing, a sweater, overcoat, woollen cap, woollen gloves, overshoes, flannel night clothing, a dressing-gown, toilet articles, and a hot-water bottle. Some institutions have a printed list of the articles required, which is sent to the patient when his application is accepted. A steamer rug is usually necessary, a cheap substitute for which may be found in the large horse-blanket, sold in saddlery shops.
Return from the Sanatorium. When a patient returns from a sojourn in an institution, he may or may not be better, but he has certainly received a liberal education in what to do, and how to take care of himself. Often, however, he is totally unable to apply this knowledge, or to adapt his home environment to his needs. So carefully is the institutional life planned, and so smoothly does he fit into it, that he has no conception of the time and thought that have gone into this planning. 213When he comes home, he knows theoretically what to do, but in comparison with the institution his home surroundings seem so poor and so inadequate, that he becomes hopelessly bewildered and confused. It is at this point that the nurse has her great opportunity. She teaches him to apply what he has learned, and how he may approximate sanatorium conditions and routine. She goes to work much as she does upon her first visit to the home, but this time she is working in a soil already ploughed. The patient himself may be almost as helpless, but he will follow suggestions, and co-operate with an intelligent enthusiasm gained through his sanatorium education.
Work for the Arrested Case. When a patient returns from the sanatorium able to work, the question of employment is a serious one. Our experience has been that of Dr. Lyman:[8] as a rule, unless it is an exceedingly injurious employment, it is better to let him return to his former occupation than to seek a new one. He understands his old work, and for this reason it will be easier for him than one to which he is unaccustomed. The difficulty of finding suitable employment for arrested cases, and the number of relapses that occur in consequence, serve once 214more to emphasize the value of prevention rather than cure.
8. Dr. David R. Lyman, Wallingford, Connecticut.
There is one point which must always be brought out. It is not so much what the patient does with his working hours, as what he does with his leisure hours, which determines his ability to hold his own. An arrested case may work eight or ten hours a day, in office, factory, or shop, and still remain well, provided he spends the remaining hours of the twenty-four in a proper manner. The ex-sanatorium case, rejoicing in his apparently restored health and in his regained liberty, feels that he can resume life on exactly the same terms as before. This he can never do. He has tuberculosis, and he always will have tuberculosis, although it may be latent at the moment. The fact that it is quiescent does not mean that it will not light up again at the slightest indiscretion. He must bear this fact constantly in mind and order his life accordingly. If he expects to work and remain well, he cannot burn the candle at both ends, even in the mildest manner. He must forego late hours, moving picture shows, poolrooms, saloons, dance halls—everything, no matter how harmless in itself, which places an extra strain upon his vitality. At the end of the day’s work he should rest quietly, preferably in 215the open-air. Eight or ten hours’ sleep at night is a necessity. The most critical time in a patient’s career is that which follows his return from a sanatorium, and it is at this particular moment that the nurse’s supervision and encouragement are so greatly needed.
Light Work. Many patients return from the sanatorium, unable to work at their former occupation, yet sufficiently strong to do “light work,” if such a thing can be found. In my experience, suitable “light work” for these cases has yet to be discovered. We all know of patients who have been given easy positions as night watchmen, elevator-men, corridor-men, office work, gardening, and so forth, and who have done well at such employment. The number of such positions, however, is so small and so out of proportion to the number of those who seek such occupation that it forms no adequate answer to the question; what light work can we find for the arrested case? Our present industrial system, which produces the class of people from which the consumptive is so largely recruited, also fails to provide proper employment for him after his so-called recovery. The pressure of this system makes it sufficiently difficult for an able-bodied man or woman to find work that pays, or even any work at all, but to find such work for the handicapped 216is almost impossible. Light work means light pay, and light pay means an insufficiency of food, clothing, and shelter, all three of which are needed for the maintenance of health. In these days when the physically fit cannot always earn a living wage, what chance has the poor consumptive?
Outdoor Work. Another favourite fallacy is the advantage of outdoor work for the returned patient. The sole value of outdoor work lies in the opportunity to breathe fresh air, but this benefit may be more than offset by the strain of long hours, exposure to heat, cold, and rain, the lifting of heavy weights, and so forth. All these objections apply to farm-work, driving delivery or freight waggons, the occupation of motorman, conductor, and so forth. Now and then, patients undertake work of this character and do well at it, but we cannot but believe that this is in spite, of, rather than because of, their occupation.
In summing up the nurse’s value to these discharged cases, we find her able to give immense assistance at a most crucial period in the patient’s life. By this help and advice, she can often prevent his relapse, or at least delay it for a long time. Her supervision provides incentive and encouragement, and her careful watchfulness, both of the 217patient and his household, is of value in detecting further danger signals. If, as too often happens, he is eventually swept under by currents too strong for him, she is still on the spot, tried counsellor and friend, to make safer and easier the downward path.
Hospitals for Advanced Cases—The Careful Consumptive—Chief Duty of the Nurse—Responsibility of the Institution—Home Care of the Advanced Case—Exceptions to Institutional Care—Compulsory Segregation.
Hospitals for the Advanced Case. The crux of the tuberculosis problem lies in the segregation of the advanced case. Until the distributor is removed from his family, and separated from the intimate circle surrounding him, we can make but little progress in the fight against this disease. No community can protect itself from the ravages of tuberculosis until it provides a place to which these advanced cases may be sent. Not only do we need large special hospitals for these patients, but we need special wards for consumptives in connection with every general hospital which receives either city or State appropriations. These special wards would be of even greater benefit to the community than large special hospitals situated in the environs of a city, since it would be easier to persuade a patient to enter an institution just “round the corner” than to go to one far 219distant from his home. A dying man dreads being separated from his family, and his family is equally reluctant to part from him; furthermore, if a hospital is remote from the city, his family can afford neither time nor carfare for frequent visits. These facts play an important part in influencing a patient’s decision, and due consideration should be accorded them.
It would probably cost less to build and maintain special wards in connection with hospitals already existing than to erect and support an entirely new institution. The greatest objection to special wards is that the coughing of the consumptives is disturbing to the other patients, but if the ward is sufficiently isolated (a separate building, if the hospital is planned on the cottage system) this objection would not apply. Furthermore, these wards would offer good teaching centres, where both doctors and nurses could learn more about pulmonary tuberculosis than the average hospital teaches to-day.
In attempting to secure ground for the erection of a tuberculosis hospital, there is usually great opposition from laymen. They are not only afraid of tuberculosis, but they fear the depreciation of property which may arise in the vicinity of such an institution. Considerable education 220is required to calm them to a realization that the consumptive sheltered and cared for is less dangerous than the consumptive at large and unrecognized. When it comes to a special ward in connection with a city hospital, we may again encounter great opposition, really from the same reason, though the objections expressed are expense of such a ward, the lack of nursing facilities, that the room is needed for acute diseases, and so on. All of which is a grave commentary, from the people who best understand it, upon the infectious nature of this disease. Yet the medical profession tells us with apparent sincerity that “the careful consumptive is not a menace.” If this be true, where can he be more careful and less of a menace than in a place specially provided for him?
The truth of the matter is, there is not, nor can there be, a careful enough consumptive. The very nature of the disease precludes such a possibility, however much we educate him, or however earnestly he himself may try to co-operate to that end. And for the vast majority of patients, from whom we can obtain but little or only spasmodic co-operation, there is even less to be said. There is one simple method of determining whether or not a patient is careful—it consists in asking the question: Under these circumstances, would I, 221myself, feel safe? Would I be satisfied as to the safety of my nearest and dearest friend?
At the beginning of the year 1912, the nurses of the Tuberculosis Division of Baltimore had on their visiting lists about 2800 patients. Of these 2020 were positively diagnosed, and had been under supervision for over three months. Undiagnosed cases, and positive ones who had been under supervision less than three months were excluded. These 2020 cases were then classified according to their willingness or ability to follow instructions, the groups being: Fairly Careful, Careless, and Grossly Careless. We purposely omitted a “Careful” class, since adequate carefulness would imply a condition in which there was absolutely no danger, a condition hardly possible with this disease. In Fairly Careful we included all those patients who really tried to follow advice, doing so to the best of their ability. Careless included those who tried intermittently, or who were badly hampered by circumstances. Grossly Careless speaks for itself.
The results of this analysis are here given:
| Patients visited over three months | 194 | ||
| Fairly Careful | 98, or 50.5% | ||
| Careless | 75, or 38.65% | ||
| Grossly Careless | 21, or 10.82% | ||
| 222 | |||
| Patients visited over six months | 346 | ||
| Fairly Careful | 171, or 49.43% | ||
| Careless | 151, or 43.64% | ||
| Grossly Careless | 24, or 6.84% | ||
| Patients visited over one year | 623 | ||
| Fairly Careful | 300, or 48.15% | ||
| Careless | 267, or 42.85% | ||
| Grossly Careless | 56, or 8.98% | ||
| Patients visited over two years | 857 | ||
| Fairly Careful | 443, or 51.69% | ||
| Careless | 339, or 39.55% | ||
| Grossly Careless | 75, or 8.75% | ||
| Total Number of Patients | 2020 | ||
| Fairly Careful | 1012, or 50.09% | ||
| Careless | 832, or 41.13% | ||
| Grossly Careless | 176, or 8% | ||
It will be noticed that these percentages vary but slightly, or to a negligible extent. Roughly speaking, about half the patients try to be careful, and half do not try, or do not succeed if they attempt it. Furthermore, it will be noticed that the time element has little to do with making a patient careful. The natural supposition would be that a patient visited for one or two years would show a marked increase of carefulness over those 223who had been under supervision but a few months. Yet there is virtually no difference between them, 50.5% of the three-months class being careful, as against 51.69% of the two-years class. These figures, we believe, show conclusively that long-continued teaching does not necessarily lead to satisfactory results. They also show that the patient left in his own home, even under constant supervision, is unable to achieve a degree of technique which means positive protection to those around him. There is but one conclusion to be drawn from these facts—not that the nurse is useless, but that the patient at large is dangerous. It proves the necessity for hospital care.
The hospital for a patient to die in appeals less to public sympathy than as a place in which he may get well. But it is better economy. Care of the open case, during his last and most infectious stages, is care which strikes at the very root of the evil. Until this fact is realized and full provision made for these cases, it will be a waste of time and money to spend them on superficial or half-way measures. If our goal is the elimination of tuberculosis, we should concentrate our efforts upon radical and fundamental methods.
At present, however, we can conceive of no community sufficiently advanced or far-seeing to 224make adequate provision for these last-stage cases. Therefore, the patients who make up the difference between the number of those needing hospital care, and those receiving hospital care, must be cared for in their homes by the nurse. Never for a moment should home supervision be considered a satisfactory substitute for hospital accommodation. The nurse’s efforts, no matter how thorough and conscientious, can never entirely remove the danger. Her care often lessens it to a marked degree, but never absolutely eliminates it. It is at best a makeshift, a stopgap—better than nothing, often much better than nothing, but never for a moment the proper alternative to removing the patient from his home. No one knows better than the nurse herself the inadequacy, the futility, of even the closest supervision.
Chief Duty of the Nurse. For this reason, the chief, the absolutely most important duty of the nurse is to induce the infectious patient to go from his home into an institution. To accomplish this end, she must bring every effort to bear upon the patient and his family, and appeal to them from every conceivable angle. This is her one great duty—the paramount reason for her existence.
225To accomplish this, is as difficult as it is important. A patient does not willingly give up his home, however poor and humble it may be, while his family often cling to him with an obstinacy open to no argument. As a rule, the difficulty of removing him is in inverse ratio to his intelligence, and to the danger to those surrounding him.
Responsibility of the Institution. In overcoming this prejudice, a great deal depends upon the character of the institution itself. It is not enough to establish hospitals:—they must be attractive and comfortable to such a degree that they become highly desirable to prospective patients. They must be well run, well managed, the food must be good, and the patients well treated. To obtain segregation, we must have hospitals which offer great advantages over the home.
Home Care of the Advanced Case. If there are no hospital facilities, it then becomes the nurse’s duty to give nursing care to the bed-ridden patient. This is also done when the hospital accommodations are limited, and the patient must wait to be admitted. During this waiting period, which may extend over weeks, he should be visited every day (or at least as often as the work will permit), and given such care as he requires, including bed-baths, 226care of the back, and so forth. The nurse must also teach some older, responsible member of the family how to care for him in the intervals between her visits. Sometimes, when a vacancy finally occurs, the patient may be contented with home treatment and refuse to enter the institution, or his family may refuse to let him go. The nurse must do her utmost to persuade them. She must explain that in the hospital he will receive constant, not intermittent care, and that her work will only permit her to render nursing service to those who cannot otherwise be provided for. Should he still refuse, she must continue her visits of supervision, but must stop all nursing care. No premium whatever should be placed on his remaining at home. This may seem like a harsh and unfeeling policy, but it is the only course to pursue when we take into consideration the fact that the institution is the proper place for an infectious disease. If a patient has become accustomed to a daily bath and other attentions, he will miss them; when he misses them badly enough, he will consent to go where they may be had. This plan does not mean that the nurse neglects the patient,—if he suffers, it is through choice. An excellent alternative has been offered, and his refusal to accept it should not entitle him 227to continue infecting his family, assisted by the nurse to do it in comfort.
Exceptions to Institutional Care. A few exceptions may be made in advising institutional care. For example, if a family is in good circumstances, with excellent home conditions, and the patient is surrounded with every care and attention, it would hardly be necessary to counsel his removal. On the contrary, with our present lack of hospital facilities, to urge such a patient to leave his home might mean taking a hospital bed from another who needed it infinitely more. Again, if a tuberculous child is being cared for by his mother, or some one equally unlikely to contract the disease, it might not be worth while to remove him. An exception might also be made in the case of a childless couple, advanced in years. The nurse must use her judgment and common-sense in such cases, where the chances of infection are slight, or non-existent. On the other hand, if there is ample hospital accommodation, and cases like the above ask for admission, they should always be taken in.
The cases in which separation is imperative are those in which there is great exposure, inability to control the home surroundings, extreme poverty and neglect, or undue and 228prolonged strain upon other members of the household.
Compulsory Segregation. Not until our hospital facilities are so large that we can accept every case which applies for admission, can we consider forcing people to enter these institutions against their will. It is illogical to consider compulsory segregation, while we cannot accommodate all those who voluntarily ask for it. The patient who refuses to go to an institution is probably no more dangerous than he who clamours in vain for a bed. The docile, well intentioned, kindly consumptive is doubtless as much a menace as the selfish, vicious, avowedly careless one; in fact, the former may be more harmful, since his kindly nature surrounds him with friends, whereas the latter forces people to avoid him.
As for the tramp, the homeless man who wanders from pillar to post, sleeping in saloons and lodging-houses, he is far less of a menace than people suppose. He comes into but casual relationship with his fellows, and no one is in prolonged and intimate contact with him, as is the case of the man in the home, the centre of the family circle. Until we can accommodate the latter, we must let the former do as seems best to him. If ten anxious people are clamouring for 229every hospital bed at our disposal, why force it upon the reluctant one who refuses? When we can handle the problem of voluntary segregation, it will be time to consider compulsory measures.
The Problem of Giving Relief—The Giver of Relief—Co-operation between Agent and Nurse—General Rules for Nurses and Agents—Conditions of Asking for Relief—Wrong Conditions of Relief-Giving—Incidental Assistance—Withdrawal of Relief—Supplying Milk and Eggs.
The Problem of Relief-Giving. Giving financial assistance or relief to patients on or below the poverty line is a question which sooner or later confronts the nurse who undertakes social work. Long hours, overwork, and low wages produce a class of people who offer little or no resistance to disease, and when tuberculosis once gets a foothold amongst them, it is passed on from one devitalized individual to another. This is why it is necessary to remove a disease-distributor from among a group of highly susceptible individuals. For example: let us take a family consisting of father, mother, and four children. The father contracts tuberculosis and stops work—his income also stops. Even at best, it was a pitifully inadequate income, and in consequence the entire family is undernourished, anæmic, and generally run down. With 231the income gone, their resistance is still further lowered, and their chances of infection are correspondingly increased. The result is a patient surrounded by a group of people able to offer but slight opposition to this insidious disease. The environment, bad as it was originally, grows worse. The family moves into smaller, fewer, cheaper rooms, and food, heat, clothing are all reduced to a minimum. This increasing poverty means diminished vitality, and heightened susceptibility to the threatening danger. In attempting to relieve this situation we are dealing not with a simple, but with a twofold problem—poverty, plus an infectious disease.
Because of its complex nature, the question of giving assistance is a difficult and delicate matter. In our efforts to relieve distress and want, we must be careful to do nothing which will result in spreading tuberculosis. The paramount consideration is the prevention of infection, and for this reason, relief should be made conditional upon the removal or reduction of the danger. If we keep this idea firmly before us, the problem will be much simplified.
In Baltimore, from one third to one half of the families under supervision are on or below the poverty line. This means that they are registered 232on the books of some charitable association, and are, or at times have been, dependent upon these organizations for food, rent, fuel, clothing, or other assistance. In other words, the gap between the income and the cost of living has needed to be bridged over by outside aid. In a new community when the nurse’s first patients are the “poor people” of the locality, she will find that nearly a hundred per cent. of her cases are on the poverty line. This was our experience in Baltimore, when the work was first organized, but now that it is well established the percentage is much reduced. The nurses are now working in homes where economic conditions are not acute, hence the number of those receiving or rather of those needing relief (the terms are not always synonymous) is less than a few years ago. Still, distressing poverty is found in from one half to one third of the families, which means that the problem of fighting tuberculosis is gravely complicated.
The Relief-Giver. When people need financial assistance, the question arises, by whom shall it be given? a point which provokes much discussion. Many people think that the nurse should give this relief, because of her intimate knowledge of the home conditions of the families under her charge—a knowledge far more extensive than that gained 233in any other way. Some think if she is socially trained, i.e., supplements her hospital training by a course in a school of philanthropy, that she can combine the duties of both nurse and charity organization agent, and become in this way a most effective social worker. By this combination, the family will be spared the infliction of two visitors, nurse and agent, a desirable result, since the advice given by these two workers is often flatly contradictory. Other people think that instead of having a nurse, it would be better to have a graduate from a school of philanthropy, with a training supplemented by a six months’ hospital course. The superficial nature of this course is sufficient commentary on its value. Moreover, more than one half of the patients with tuberculosis do not come within the reach of a relief-giving agency.
These two people, nurse and agent, are both specialists in their own lines, and they are equally needed. They have had a different training and are equally valuable in the field of social service. Even if it were possible, we should not like to see these two offices combined in one person—somewhere there would be a loss. It is difficult enough to get a first-class tuberculosis nurse, and it is equally difficult to find a first-class charity organization 234agent. How much more difficult to find these combined in one person. There is full warrant for saying that under no circumstances whatever should the nurse become a relief-giver, or even remotely identified as such. In the foregoing pages we have learned something of the extent and responsibility of her work, and if she concentrates her attention upon bringing it to the highest degree of efficiency, she will find time for nothing else. Moreover, if she becomes known as one able to give material assistance, her value as a public health nurse will decline. That she can give or withhold relief will become known to her patients, who will follow or reject advice according to what they receive from her. Her prestige as impartial, disinterested adviser will at once diminish, and the force and authority of her opinion be lost. Never, even by the gift of a five-cent piece, should she jeopardize her unique position. The well-to-do patients will scorn her services, and resent the implication of her visits, while the others will follow advice when they are bribed, so to speak, and do as they like when for any reason this bribe is withdrawn. And other patients will be disobedient or resentful if they cannot obtain what their neighbours have, or what they believe themselves entitled to.
235Co-operation not Interference. To concentrate on one’s specialty is all we should ask of anyone. Any social agency which scatters instead of concentrates, produces superficial work, which is open to well-deserved criticism. As well expect a nurse to become a kindergarten teacher, because she sees the need for kindergartens, or to become a playground teacher or settlement worker, as to take upon herself the rôle of charity-organization agent. And the reverse of this is true. We should not expect a relief-giver to undertake a nurse’s duties. It is not the combination of various effective qualities in one person, but the co-operation of various effective persons or specialists, which counts in social service. Furthermore, each set of workers should recognize its own limitations. The line of demarcation should be sharply drawn between the work of one agency and that of another.
One sometimes encounters an intense zeal which causes one social worker to try to do her own, and everyone else’s work as well; or even worse than this, to neglect her own work in order to do that of another person. All social workers should learn where to stop—where to transfer the case to someone else better fitted to deal with another phase of it. We sometimes hesitate to call in other agencies, 236because they do not recognize their boundaries. Co-operation should be substituted for rivalry and interference; when this is brought about, petty bickerings and jealousies among the social agencies will cease.
To become an effective co-operator, instead of a critical interferer, the public health nurse must familiarize herself with all the agencies in the wide field of social service. She should try to understand the object and method of their work, and to know where her own work interlocks with theirs. In a way, they are all interdependent, one upon the other, and have the same object in view—to relieve distress and raise the sum total of human happiness. Whether their work is effective or superficial is not our concern. The nurse should understand what each of them has to offer, and by picking here and there among them, secure valuable assistance for the families under her charge. She can thus reinforce her own efforts, and supplement her own work in behalf of their well-being and security.
Since nurses come in almost daily contact with the Charity Organization Societies it should be part of their duties to attend the local district meetings of these associations, for during the discussions which take place, the nurses are able 237to give most helpful information concerning their own cases, while in regard to other cases, not complicated by a communicable disease, they learn much as to the methods and theory of relief-giving. For this reason, these district meetings are useful to both nurse and agent alike; the interchange of opinion enlarges the outlook of both workers, and each gains an insight into the difficulties of the other’s work. This interest and understanding promotes good feeling, tolerance, and personal friendliness—the basis of successful team work.
General Rules for Nurses and Agents. In a small community in which there is but one nurse and no Charity Organization Society or its equivalent, it is well to form a Relief Committee, to whom the nurse may refer such of her cases as need assistance. In cities where relief-giving organizations are already established, a few general rules should govern the relation between nurse and agent; the observance of these will prevent much trouble and misunderstanding. Under no circumstances should the nurse give material assistance—neither money, food, clothing, nor anything of the sort. When these things are needed, the agent should be asked for them, and no case is so acute but that it may wait until this consultation takes 238place. In a city where there is no emergency or night bureau, it may be necessary to make an occasional exception to this rule, in which case the nurse may tide the patient over till the following morning, when the agent may be conferred with. Such instances will be so rare, however, that they are merely noted as exceptions to the general rule—under no consideration whatever should the nurse give any material relief.
It sometimes happens that the nurse has been given a small sum to buy food, clothing, or special articles for some of her patients. This fund was perhaps intended for a specified case, or to be used at discretion. It is wiser to give this money to the agent, with the request that it be spent (if circumstances warrant) as the nurse suggests. This course may involve additional trouble, a little extra work for both nurse and agent, but it is necessary to be extremely punctilious in order to avoid serious misunderstandings.
When a nurse has been in the work a long time, and is dealing with agents whom she knows and understands, a feeling of mutual trust and dependence will arise. Under such circumstances, both may take far more leeway than should be granted a new worker—but unfortunately this happy and comfortable state is not always reached. 239The safest plan is that each should follow her own line with utmost precision, being rigidly careful not to overstep the boundaries between her own and another’s duties.
For example: a benevolent individual may give the nurse an overcoat, to be used for any patient who needs it. The nurse knows a patient who is expecting to enter a sanatorium in a few days. Her first inclination would be to give him the coat and say nothing. Apparently it concerns no one but herself and her patient. In adherence to the rules laid down, however, she must first consult the agent before giving away the coat. This consultation may reveal the fact that the family (new to the nurse) is well known to the Federated Charities, and that but a short time ago this patient was given an overcoat which he sold for drink. At this time, be it said, he was not known to be tuberculous. Of course, this constitutes no argument against giving him another chance, inasmuch as he depends upon it to enter the sanatorium, but it gives the nurse a side light on her patient’s character. She should make sure that he will not play fast and loose again; also upon entering the sanatorium the physician must be informed that the man is addicted to alcohol—a tendency to be considered in his treatment.
240Tuberculosis, like poverty, is a chronic condition, and the delay required for wholesome co-operation will seldom prove fatal.
The agents, likewise, should be governed by one very simple rule, which will obviate all misunderstandings and ill feeling. This rule should be—no advice, suggestions, or interference in regard to medical attention, nursing, or treatment. All this lies strictly within the nurse’s province and should be left absolutely to her. For example: if an agent enters a house and finds a consumptive, she should make no suggestions as to changing doctors, going to this or that dispensary, or to such and such an institution. If the case is already known to the nurse, the agent may consult her, and find out what plans and arrangements have been made and then aid in bringing them about. If the case is unknown to the nurse, the agent should report it at once, leaving the nurse to take all necessary steps as to diagnosis and treatment. Grave results often follow the abuse of this one simple rule. For example: an agent enters a patient’s home, and finds him in charge of a certain doctor. Without knowing anything of the circumstances, she may advise him to change doctors, go to a dispensary, or even to a sanatorium. She does not know that the patient is in charge of a physician with a large 241private practice, and that this is the first time he has called upon the tuberculosis nurse. His co-operation and help in the tuberculosis campaign depends upon the way this first case is handled. His indignation at finding the nurse has played him false (for it is apt to be the nurse who is credited with these objectionable things) may be so great that months of explanation cannot wipe it out. As we have said before, tuberculosis is like poverty—a chronic complaint—and the delay needed for co-operation will not prove fatal.
If nurses and agents will follow strictly this one simple rule—the former to give no material assistance, the latter to offer no advice concerning the patient’s treatment—the chief cause of friction between these two sets of workers will be eliminated.
Conditions under which Relief is Asked. The nurse who visits a family every week or two is in a position to know when they have come to the end of their resources and need relief. When this point is reached, she should report the case to the agent of the Federated Charities. She must always bear in mind that her chief work is the prevention of tuberculosis; it is not necessarily the prolongation of human life, although the two are sometimes coincident. Relief should be asked for if it brings 242about the prevention of tuberculosis, but under no circumstances if it means increased opportunities for scattering the disease. Under the latter conditions, assistance should be withheld or withdrawn as the case may be.
For example: we have a family consisting of father, mother, and several children. The income ceased when the father, the wage-earner, became too ill to work. The family is in great need of fuel, rent, and groceries. The giving of this assistance should be made conditional upon the removal of the danger—that is, upon the patient’s going to an institution where he will be better cared for than in the home. By insisting upon this removal, the Federated Charities can play an important part in the suppression of tuberculosis.
Suppose there are no hospital facilities, and it is necessary to keep the patient at home. In this case, the most susceptible members of the household, namely, the children, should be removed. To place out children is a difficult matter, since it is hard to get the parents’ consent; this can be done, however, with time.
If this turns out to be impossible, relief may be given on condition that the strictest precautions are observed. This assistance may be given as long as both patient and family follow rigidly all 243directions given by the nurse; failure to do so should be a signal for the withdrawal of all aid. To assist the patient who has no choice but to remain at home, means to give relief under the least favourable conditions, but it must answer when there are no hospital facilities. When such facilities exist, no alternative should be permitted. When a family reaches the point where outside interference—social interference—is needed, we think it not unreasonable that this assistance should be given upon terms which tend to promote, rather than diminish the welfare of its members.
Wrong Conditions of Relief-Giving. Relief is sometimes given in a way that makes it defeat preventive work, and tends to create new sources of infection. For example: we recall a case in which the father of a family was in the last stages of consumption. His wife took in washing, and was general drudge for the patient and five small children. This man refused to go to a hospital, and also refused to use his sputum cup, or take any other precautions. Most of his time was spent in bed, and beside him in the bed were his two small children, whose presence gave him pleasure. Neither doctor, nurse, nor agent could bring about a better state of things, yet the family was desperately 244poor and in great need of help. In consequence, assistance was given upon the patient’s own terms of being allowed to carry out his right to infect his family. Groceries were given in large amounts, and the patient himself was supplied with abundant milk and eggs, which kept him alive for weeks beyond the point where his own manner of living would have ended the matter. Soon after his death, one of the children died of tubercular meningitis, while his wife developed a pulmonary lesion. All the family are now public charges.
We recall another case: The family consisted of the patient, his wife, and eight children. The patient was grossly careless, declining to observe the slightest precautions, and flatly refused to enter a hospital. After his death, his wife and five of the eight children were found to have tuberculosis. During the last six months of his life, a certain agency had poured in unceasing relief, thereby subsidizing a centre of infection.
Still a third case is that of a widow, with two small children. She would not part from these children, and refused to go to a hospital, or to let them go to the country. A separate bed was provided, so that for part of the time at least the children might be away from her, but she declined 245to let them occupy it. She kept them in bed with her. Neither would she use a sputum cup nor follow advice in any way. All this time, some benevolent old ladies kept her well supplied with groceries, milk, eggs, coal, rent, and so forth, by means of which assistance she was able to drag out a moribund existence for eight or ten months. Pitiful as this case was, the utter selfishness and immorality of this sort of “mother love” is something which should repel rather than attract the sympathies of thinking people.
These are perhaps extreme instances, yet in a lesser degree this is what usually happens unless relief is made conditional upon removal of the danger. Charitable associations should be careful not to act as accessories in the spread of tuberculosis, and should not prolong conditions under which this is practically inevitable. If centres of infection are thus perpetuated, through sources over which the associations in question have no control, nurse and agent, at least, should not countenance such “benevolence.”
Incidental Assistance. There are many occasions when the nurse should ask for relief, and when this should be freely and generously given. When a patient enters an institution, it may be necessary to pension his family during his absence; 246assurance of their welfare will enable him to leave with an easy mind. Unless such provision is made, we are threatened with the alternative of seeing him sit at home, unable to work, but engaged in the minor though highly dangerous occupation of caring for the children while his wife goes out to service.
Relief may also be of a temporary nature. While a patient waits for admission to a hospital he may be too sick to remain alone at home. This may mean that his wife, the breadwinner, is forced to give up work in order to care for him. Assistance should be given during this waiting period, after which time the wife will return to her employment and the family affairs readjust themselves.
Again, we may have a family in which the patient himself is the only one who needs help, the income sufficing for all ordinary demands, but not for the extraordinary demands of illness. While awaiting admission to an institution, it may be necessary to give him extra food, extra clothing or bed clothing, an overcoat, railway fare, or something of like nature, either to make him comfortable, or to facilitate his removal when the time comes. The patient must not be allowed to suffer during this enforced wait, but this assistance must 247not be interpreted as encouragement to remain at home.
In the foregoing instances, relief has been conditional upon removal. We must sometimes give assistance under other circumstances. If there are no hospital facilities, or if he will not avail himself of them, we are doing good preventive work if we give the patient an extra bed, since this may result in his partial separation from the children or other members of the household. Extra clothing may also be given under like conditions. On the other hand, if we gave milk and eggs to the patient, we should be supplying food which would maintain indefinitely a centre of infection. (Good preventive work may be accomplished by ample feeding of the other members of the household, thus increasing their resistance. In this case we should be sure that this food is taken by the children, or by those for whom it was intended, since otherwise it would be wasted.) Let us put the matter very frankly: it is wrong to prolong a patient’s life, unless at the same time we can make him harmless to those about him. If the two are coincident, well and good. If not, then the shorter the exposure, the better for all those who must submit to it. We repeat what was said at the beginning of the chapter: the patient 248on the poverty line is surrounded by a group of individuals whose vitality is at a very low ebb. Our first duty is to protect these individuals.
Withdrawal of Relief. When relief is given with the understanding that certain conditions be complied with, it should be withdrawn if this compact be violated. The nurse is in a position to know of any breach of faith, and should notify the agent accordingly. The objection is sometimes raised that assistance given in this way is a bribe, or a threat, or a means of coercion, and is therefore wrong. This rather overstates the case. Let us say, rather, that under these circumstances we have in our hands a powerful lever, by which mountains of ignorance and prejudice may be removed. By the use of this lever, we can work quickly and well for the best interests of the family and the community. We constantly see families who are not on the poverty line, and over whom we have no control, yet who are equally obstinate, ignorant, and dangerous, and regret infinitely that we have no such lever as in the case of patients who are below the poverty line.
When asking for relief, the nurse must be sure that her patients will take advantage of it, and that she is not sending the agent on wild-goose chases. Patients have sometimes been supplied 249with cots, window-tents, reclining chairs, and other similar and expensive articles, which they subsequently declined to use. An indifferent, careless patient, unwilling to co-operate in any way, is not one for whom to demand such an outlay.
Milk and Eggs. Ten years ago, milk and eggs for consumptives was an integral part of the tuberculosis campaign. In those early days, they were considered as necessary as was fresh air itself. They were prescribed as a matter of routine, and if the patient could not afford to buy them, they were at once supplied by some charitable association. We have come a long way since then.
Attention has already been called to the fact that, in the past few years, medical opinion has undergone a great change as to the value of milk and eggs. This rich and highly concentrated food is considered far less advantageous than was at first supposed. By reason of their fat content (especially the case with eggs), they tend to cause indigestion, always a serious complication in pulmonary tuberculosis. For this reason, the old idea of living on enormous quantities of milk and eggs has been largely abandoned. Some sanatoriums do not give them at all—other food is substituted, equally nourishing but less apt to 250upset the stomach. Yet the idea that they are necessary for consumptives dies hard.
In Baltimore, there is now no question of providing them. During the past year, nearly five thousand consumptives passed under the supervision of the Tuberculosis Division; we asked that milk and eggs be given to only thirty-eight of this number. Of these thirty-eight cases, thirteen were advanced, waiting admission to a hospital; two were early cases, waiting admission to a sanatorium; nine were suspects, and extra nourishment was needed in order to facilitate diagnosis; and fourteen were chronic cases, to whom this diet was given as a valuable tonic.
Quite apart from their value, the real reason that we have ceased to give milk and eggs is because of our policy of removing the patient to an institution. The furnishing of this diet, or of anything else which tends to keep him at home, is something we do not endorse. We do not wish to place any premium upon the home, or to offer any inducements to remain in it. If our patient wants milk and eggs, we can send him where they may be had.
If there is no hospital for the tuberculous patient in a community which is able to furnish one, the maintenance of the patient by charity as a centre 251of infection, makes little difference, one way or the other. In this case, the absence of a hospital means that the community is merely sentimentalizing and pottering over the tuberculosis problem.
Home Occupations of Consumptives—Sewing and Sweatshop Work—Food—Milk and Cream—Lunch Rooms and Eating-Houses—Laundry Work—Boarding- and Lodging-Houses—Miscellaneous Occupations—Summary—The Consumptive Outside the Home—Cooks—Personal Contact in the Factory—Supervision Outside the Home.
Home Occupations of Consumptives. Up to this point we have considered the patient solely in relation to his own family, or to those with whom he comes in immediate, constant contact. The people surrounding him are in their turn infected, transmitting the disease to others who in like manner are intimately exposed. Roughly speaking, all of this infection takes place within the four walls of the home. The home, therefore, is the centre of infection,—the focus from which tuberculosis radiates into the community. The further one is removed from this focus, the less the danger.
There are certain ways, however, in which danger from the home threatens people who live outside, people in no wise connected with the patient, and unaware of his existence. This 253occurs when the patient leaves his home to seek employment in the community, or when he makes or handles certain articles which go forth into the community as carriers of bacilli. Infections of this sort may be termed accidental. They are infrequent as compared to house infections, but infrequent as they are, they should be prevented.
In Baltimore, nearly fifty per cent. of the patients under supervision are able to work. They seek a livelihood in office, factory, shop, hotel, and private home. We also find that nineteen per cent. of the families under supervision carry on some sort of gainful occupation within the confines of their own homes. As a rule, the patients who conduct these little home industries or occupations are more advanced cases than those able to find employment in shops and factories. In some instances, this home industry was carried on before the patient became ill; in others, by far the greater number, it is the direct result of an illness which has modified his earning power and compelled him to eke out a scanty income by this means. In many cases the actual work is not done by the patient himself but by some other member of the household. Sometimes these industries are not dangerous to other people, or the risk is so slight as to be negligible. At other times, the menace 254is grave. Each case must be considered upon its individual merits—one must not generalize and condemn in wholesale fashion.
Sewing and Sweatshop Work. A number of our patients are dressmakers, or do factory sewing at home. Much has been written about the danger of clothing made under such conditions, either by the patient himself or by other members of his family. This output is not as dangerous as many people suppose, although such an admission would deprive the campaign of much picturesque photography. Much of this clothing is of washable material, such as cotton shirts, blouses, overalls, and the like, therefore any germs they might carry would be removed in the first washing. The danger has also been exaggerated in the case of woollen materials, such as coats, trousers, etc. Any organisms contained in these articles would soon die, or their virulence become so attenuated that little harm would result. This also applies to artificial flowers. It is not the occasional dose of bacilli, conveyed in this or any other manner, but the large and repeated implantations which do the damage.
Infected clothing doubtless plays considerable part in the spread of the acute contagious diseases, such as measles, diphtheria, and scarlet 255fever, but in tuberculosis the risk is so slight that it may almost be called non-existent. Under such conditions, the danger is not to the wearers, or probable buyers, but to workers who make this clothing while in contact with the consumptive himself.
Food. There are other home occupations about whose danger to the public there can be little doubt. Many patients keep small grocery stores, confectionery shops, and lunch rooms, and prepare and handle foodstuffs of all kinds. Again we must discriminate. The consumptive who sells tinned foods (which he does not handle), or meat, fish, or vegetables which are cooked before they are eaten, is not necessarily spreading disease among his customers. On the other hand, he who sells and handles milk, cream, ice-cream, bread, cake, candy, and so forth, is a decided danger to all who buy his wares. The alimentary tract is one of the main portals of entry for the tubercle bacilli, and every precaution must be taken to prevent the contamination of food. The patrons of these little shops are the people of the neighbourhood, who are regular customers, and their health is endangered not by occasional but by repeated doses of germ-laden food.
Milk and Cream. There is an ordinance in Baltimore forbidding the sale of milk and cream 256in a house where there is an infectious disease; this includes tuberculosis. In order to sell milk, it is first necessary to obtain a permit from the Health Department, but this permit may be revoked whenever occasion demands. If the nurse finds that one of her patients is selling milk (as is often done in connection with a small grocery business), she reports this fact to the Health Department. It may be that the patient himself never comes near the shop, and is out at work or away all day. This sometimes happens, but not often. Usually he waits upon the customers himself, selling milk in penny amounts, with a dirty finger inside the measuring cup. Or he may be too ill to attend the shop, but sits or lies in an adjoining room, so that his wife may wait upon him and upon the customers alternately. Under such conditions, the danger may be almost as great as if he himself handled the milk, since she does not take time for proper cleanliness.
To revoke a permit usually occasions considerable hardship, and the reduction of an already pitiful income. Yet summary measures must be taken unless the milk is sold without risk to the purchasers. The patient should be removed to a hospital, and the family must choose between 257letting him go and giving up the permit. When there are no hospital facilities and the permit must be withdrawn, leaving the family under financial stress, the nurse should ask assistance of the Federated Charities. This assistance, however, should never be offered as an alternative to removing the patient to a hospital.
There are other foods besides milk and cream liable to contamination, the sale of which is not controlled in any way. Thus as we have seen, while a consumptive may be prohibited from selling milk, he may sell ice-cream without let or hindrance. And furthermore, an ice-cream cone or “snow-ball,” handled by dirty, germ-laden fingers, is most often sold to the most susceptible of all customers—the child.
Lunch Rooms and Eating-Houses. Many patients earn their living by keeping eating-houses, oyster-parlours, ice-cream saloons, and so forth. There is danger to the customer whenever the cooking and serving of food are done by a consumptive, or by those in contact with a consumptive. A community to be well protected should enact comprehensive legislation controlling every aspect of the food supply, and special emphasis should be laid upon the handling of food by those with a transmissible disease.
258Laundry Work. Another home occupation is laundry work—unskilled labour requiring no capital and largely resorted to, especially among negroes. This is heavy work, hence not always done by the patient, but often by some other member of the household. Whether the patient irons the clean clothes or sits coughing in the same room where this is done (we have often seen newly ironed clothes spread upon the bed of a last-stage case), the result is much the same. Under such circumstances clothes become contaminated. Since this sort of laundry work is usually done for regular customers, they week after week wear clothing that has come from an infected house. It is dangerous to sleep constantly on pillow cases that have been coughed on by a consumptive, and to use towels and napkins that have been subjected to a like infection.
Since there are no laws to govern conditions of this sort, the question arises, what is the nurse to do in such a case? Must she look on and say nothing, or must she warn those for whom this laundry work is being done? It would be futile to argue with the patient’s family—they would refuse to recognize the danger to others, seeing instead the financial loss from giving up the work. The nurse must first try to remove the patient to 259a hospital, thus doing away entirely with the danger. Failing in this (through lack of hospital facilities), the family may be willing to give up the work on condition that an income be substituted by some charitable agency. Simple as the latter course may seem, so many obstacles to procuring this aid will arise, that it offers no practical solution of the matter. If the home surroundings cannot be altered and the danger reduced, then the patrons or customers should be told of the conditions under which their laundry work is done. It is not always possible, however, to locate these customers, since the patient is very wary of giving information upon this subject. Whenever possible, nevertheless, they should be told; if they prefer to continue the risk, they are at least not in ignorance of it.
It is deeply regrettable that exposure to infection by tuberculosis is still an optional matter, and that the necessary curtailment of individual liberty has not yet been made in regard to all opportunities for it. In the case of impure milk, for instance, the law at least makes an effort to curb the preference which any individual may entertain for it.
Boarding and Lodging Houses. There are other home occupations in which the menace is of 260a personal nature, and does not come through contaminated articles. Many patients take in boarders—an occupation which frequently entails considerable overcrowding of the home. This brings healthy individuals directly within the danger zone, and subjects them to the same risks incurred by the family itself. Other patients take in lodgers; here the risk is less, because meals are not included. In either case, there is great personal exposure, with equally great opportunities of infection.
Summary. To sum up: Among 3107 patients under supervision, we find 608, or 19 per cent., carrying on some sort of gainful industry within the confines of their own homes. The resultant danger is of two kinds: from personal contact with the patient, and the remoter possibility of infection through articles which he makes or handles. The most serious risk is that incurred in boarding- and lodging-houses, where the inmates are subjected to a high degree of personal exposure. In other occupations there may be some personal risk, but it is slight and transitory, and therefore insignificant. In considering contaminated articles, we find there also two classes: those dangerous to a high degree, and those but slightly so, if indeed they may be called dangerous at all. 261Among the former, the most harmful are the contaminated foodstuffs, in which the risk is almost as great as through personal contact. Next comes laundry work, where the risk is in the repetition of infection, as in the use of household linen. Then comes the output of clothing, cotton and woollen, where also the risk is slight. In the case of other articles handled by the consumptive the risk involved is so insignificant as not to be worth mentioning.
The following table shows the nature of these various Home Occupations, ranged in order of their risk to the community:
| Personal: | Boarders | 104 | ||
| Lodgers | 18 | 122 | ||
| Food: | Bakeries | 4 | ||
| Confectioneries | 4 | |||
| Cook shops | 6 | |||
| Groceries | 73 | |||
| Oyster-parlours | 1 | |||
| Saloons | 13 | 101 | ||
| Clothing: | Laundry work | 222 | ||
| Sewing | 109 | |||
| Millinery | 1 | |||
| Tailor shop | 4 | 114 | ||
| 262Miscellaneous: | Barbers | 8 | ||
| Basket-maker | 1 | |||
| Cigar store | 2 | |||
| Cleaning and Dyeing | 1 | |||
| Drygoods | 10 | |||
| Second-hand shop | 1 | |||
| Shoemaker | 21 | |||
| Umbrella-mender | 1 | |||
| Wall-paper shop | 1 | 46 | ||
| Total, | 605 |
The Consumptive Outside the Home. We must now consider the patient who is employed outside the home. As we have said before, nearly fifty per cent. of our patients are able to work. The danger to the public is of two kinds, that arising through personal contact, and through certain articles which the consumptive may make or handle. In the latter case, just as we find it among the home occupations, the risk to the community depends upon the articles themselves. Whatever affects food, is far more dangerous than the contamination of articles not taken into the alimentary tract.
To prevent the possibility of food infection, we should enact and enforce laws forbidding the employment of consumptives in any factory, shop, or establishment of any kind in which food is 263either prepared or sold. This would include candy factories, bakeries, cake, biscuit, and cracker factories, canning and preserving establishments, as well as dairies, restaurants, lunch rooms, sodawater stands, candy shops, and the like. We must never forget that the home is the chief centre of danger, the place responsible for the vast majority of infections, and that every infection which occurs outside the home is accidental, so to speak. Yet accidental infections, while relatively few in number, are still plentiful enough to make it necessary to safeguard the community in every way. An effective tuberculosis campaign demands the stoppage of all leaks.
For example: on our visiting list was a girl employed in a biscuit factory, packing cakes. She was an advanced case, and every now and then had a hemorrhage which compelled her to stop work, though sometimes only for a few hours. Between hemorrhages, she worked steadily. The cakes packed under these conditions doubtless carried a full quota of germs. We tried to induce her to go to a hospital, but she declined. The manager was appealed to but he wanted to keep her—she was a quick worker; besides, he did not have to eat the cakes—so he refused to add his influence to ours to get the patient to an institution. The 264public should be protected by law from the possibility of such infection.
The saving phase of the situation is this: while the patient who keeps a bakeshop and sells his wares day after day to practically the same customers, fulfils the condition that repeated implantations are necessary to contract the disease; on the other hand, the cakes distributed by a factory cover a wider range of territory—thus, while many more people get doses of germs, the doses themselves are probably too small to be harmful. This also may be said for other kinds of foodstuffs, handled in factories by tuberculous persons; these articles are distributed so widely that no individual consumer is really endangered. In this way, the risk is minimized. But still we must remember that every factory in the country has its tuberculous employees, with their output of bacilli to be reckoned with. The consumer is thus threatened on every side. No wise community should tolerate such chances of infection.
Cooks. There is considerably more danger from the tuberculous cook employed in a private family. Under such conditions the household is steadily infected day by day, not through personal contact, but by small, repeated doses of bacilli received into the alimentary tract.
265If typhoid fever permitted a patient to work—if it were a chronic instead of an acute disease—we should consider it a highly dangerous expedient to permit such a patient to handle food in any way, and we should be exceedingly wary of restaurants which employed typhoids as cooks or waiters. This argument applies with equal force to tuberculosis. In typhoid, there is but one portal of entry—the digestive tract. In tuberculosis there are two—the respiratory as well as the alimentary—and they are equally important.
Personal Contact in the Factory. While the patient in the factory is a menace, he is less dangerous than the patient in his home. A man well enough to work is seldom in the most advanced and infectious stages of tuberculosis. Moreover, his fellow-workers, unlike the members of his household, are not in constant but rather in casual and intermittent contact with him. These two conditions tend to diminish the risk to his associates; still, it always exists. The consumptive does not seek employment from a malicious desire to spread tuberculosis—he seeks it because of economic conditions compelling him to work until he falls in harness. We must recognize this driving necessity, but at the same time we must protect the workers who perforce surround him. 266They too are impelled by the same need, and their rights equal his.
When a patient is visited at home, he and his family are often stimulated to a high degree of carefulness. The patient uses a sputum cup for his own convenience, and the family insist upon this for their own interest and safety. The result is a lessening of danger, and an improvement upon a neglected and uninstructed case. In the factory, these conditions are reversed. His cup is no longer a convenience, and he dreads being conspicuous through its use. Moreover, since his illness is unknown to his fellow-workers, there is no one to insist upon precautions of any kind. The result is that we maintain in the factory conditions which we seek to abolish in the home. We give one set of people information whereby to protect themselves, and we withhold this information from another group of people who need it almost as much, which is illogical and stupid and costly. Enormous sacrifices have been made to this policy of silence, and it is time for these sacrifices to cease.
Those in contact with a consumptive, whether this contact takes place in the home or in the factory, are entitled to know the nature of his disease. It is not the degree of consanguinity, but the degree of contact which should determine this 267knowledge. We cannot trust the patient to protect others—it is a trust too often violated. We must surround him in the shop with a public opinion even more potent than that which he finds at home. His fellow-workers will be less tolerant of breaches of technique, will make less excuse for whims and temper, than does the tired family. We knew of one patient who insisted on spitting on the floor—at home; when his wife remonstrated, he knocked her down. In the shop, such conduct would cost him his place, and rightly.
Supervision Outside the Home. Whenever the infectious case is at large in the community, his whereabouts should be known to those most exposed to the danger. This applies alike to employer and employee. The head of the department in which the consumptive is at work should see that those in contact with him know of his condition. The patient should be compelled to use his sputum cup when he expectorates. Knowledge of the patient’s condition does not necessarily mean that he should be dismissed—it should merely mean that he will be held up to the required standard of carefulness. For example: the Baltimore Health Department received a letter from a certain firm in the city, stating that 268many cases of tuberculosis had developed among the employees on a certain floor in their factory—and on this one floor alone. This led them to suspect that a consumptive might be among these workers, distributing the disease. A list of all the employees was submitted. Investigation promptly showed that on this particular floor was a chronic case of tuberculosis of long standing, a man who had been under supervision at home for several years. In his home, this patient was exceedingly clean and punctilious in the use of the sputum cup; at his work, however, he was absolutely the reverse. On receipt of this information, the employer had a sound talk with this man, which resulted in the use of the sputum cup and all other precautions. The patient did not lose his place, but he was no longer permitted to jeopardize the health of his fellow-workers.
Patients with chronic tuberculosis are also found in domestic service, and go in and out of private homes, carrying infection with them. This danger is especially great in the South, where there is a large negro population, and we constantly find consumptives employed as cooks, housemaids, nursemaids, and butlers, as the case may be. For the most part, the employers are 269entirely ignorant as to their condition. In these cases, just as in the factory, office, department store, and so forth, the employer should be notified of the presence of tuberculosis.
To give this information should be the duty of the Health Department. The municipal nurses are aware of the facts, and they also know when a patient changes his occupation, or place of employment. But to give this information without following it up, would not be enough. To notify an employer of the presence of a tuberculous worker, would not necessarily mean that any action resulted. A poor workman might be summarily dismissed, and a good one retained, without those in his vicinity being enlightened as to the nature of his disease. To make this information of value, it would be necessary to supervise the patient in the factory, just as he is supervised in the home. This double supervision would demand a greatly increased staff of nurses, since factory visiting should not be done through curtailment of the nurse’s other duties. We must once more emphasize the fact that the home is the fountainhead of tuberculosis, and that every infection which occurs outside the home circle (or its equivalent) is practically an accidental infection. But, as we have already said, a comprehensive 270plan for checking tuberculosis must include the stoppage of all leaks, and the unknown, unsupervised consumptive, at large in the community, is a leak which should be recognized by common-sense.
Yet certain conditions must be complied with before we can extend this municipal supervision. Outside-the-home supervision will create an enormous amount of phthisiphobia. Consumptives are now tolerated because their presence is either unknown or but dimly guessed at; when this ignorance is dispelled—as it must be if the nurse visits them at their places of employment, and their presence and numbers are made known, a great wave of fear will spread over the community. Such a result is inevitable when for the first time the public realizes, suddenly and concretely, the extent to which it is threatened. Tuberculous workers will be discharged by hundreds, and there will be widespread suffering in consequence.
On the other hand, however, thousands of non-tuberculous workers will be relieved of a great danger. Our factories already produce workers so worn out and devitalized as to fall ready victims to any disease that presents itself. Would not these same factories be somewhat 271less dangerous if swept clear of consumptive employees?[9]
9. However bad certain factory conditions may be, these of themselves cannot produce tuberculosis any more than they can produce scarlet fever or diphtheria. The disease itself must be brought into the factory by a carrier—someone who is himself infected.
Outside-the-home supervision is the next logical step in the anti-tuberculosis campaign. But valuable as this would be, from the point of view of the general health, it cannot be done until the community is prepared to care for all who would undoubtedly suffer as a result. Some patients, of course, would not lose their situations, but the majority would be turned adrift without a moment’s hesitation. These the community must take charge of. Therefore, before we can supervise tuberculosis beyond the boundaries of the home, we must have ample hospital facilities. Hospital accommodation must be so extensive, so complete, and so excellent that institutional care can be given to all who need it.
In this way, the community will be relieved automatically of a vast amount of danger. Patients will either seek institutional care, or, if they continue at work, will do so under conditions which do not jeopardize other people. For the reaction from the first intense phthisiphobia will be a demand 272for carefulness on the part of the consumptive, and sane toleration of him.
The one objection to this policy of supervision and publicity is the seeming interference with the personal liberty of the individual, but to curtail the liberty of the patient to transmit a communicable disease, is to increase the liberty of hundreds to escape it. There should be no question as to which has the superior claim.
Municipal Control—The Danger of “Political” Control—“Politics” in the Co-operating Divisions—Results in Baltimore—Tuberculosis and Poverty.
Municipal Control. Tuberculosis is a communicable disease in which the patient himself must be relied upon to protect the community. We depend upon him for whatever protection he chooses to give, and whether this is much or little is determined by his circumstances, temperament, and environment. Whenever his ability or good-will breaks down, we are at his mercy. We may try to overcome his ignorance by education; to substitute ethical for unethical standards, and in a more or less unsatisfactory way to reconstruct his immediate surroundings. But the success of these efforts depends, in the last analysis, upon the patient himself. The public is exposed to a communicable disease, the control of which lies with the transmitter.
For this reason, a disease which may be contracted by a neighbour becomes as much his affair 274as it is that of the patient or possessor. Should the interests of the two conflict, it is obvious that we must have some impartial arbiter to decide between them. At such a point—the right of one person to transmit, of another to acquire an infectious disease—the matter becomes one of public as well as private concern. The arbiter between these two interests should be the Health Department of a community, and the control of all infectious diseases should be placed completely under the municipality.
In the first chapters of this book, we considered the special nurse as supported by a group of private individuals, in connection with some privately maintained association. Social experiments frequently begin in this way; when their value is proved, it should be the aim of the promoters to transfer this special work to the department of the municipality in which it belongs. Upon looking over the various municipal departments, we realize that much of what is now freely recognized to be municipal work, was originally carried on through private enterprise and initiative. This is the case with school nursing, playground work, juvenile court and probation work; which in many cities has passed through the stage of private enterprise and become firmly incorporated 275into the city machinery. In all public health nursing, the aim of the founders should be, first to prove its worth to the community, and then make the community (municipality) assume full charge of it as soon as possible. It is particularly necessary to transfer tuberculosis work from private to municipal control.
The Danger of “Political” Control. The question of doing this, however, is often a matter of great concern to the founders. They are usually deeply interested in the work, and have maintained it upon a basis of efficiency, in spite of many obstacles. They fear, and often rightly, that to transfer it to the municipality will be to transfer it from the basis of efficiency in its own line, to the basis of politics, and they dread that sinister condition known as “political control.” And yet the administration of public affairs is not necessarily “political” in the bad sense of the term. On the contrary, municipal control may, and in many cities does mean, that work is conducted with the force, authority, and financial backing of a great department, such as the Health Department. Under such conditions, it can attain a far greater degree of efficiency than could ever have been reached through private administration. Under municipal control, it is possible to have a large 276staff of nurses and pay them good salaries—which latter always means a wide choice of applicants. It is also possible to establish many and well equipped dispensaries, in charge of salaried, qualified physicians. Money will be forthcoming for all necessary expenses connected with the development and extension of the work—in short, the financial handicap will be removed, and the work can go forward with increased facilities, enlarged opportunities, and heightened dignity and authority.
On the other hand, if the administration of the Health Department is “in politics,” the reverse of this will take place. Unfortunately, in many American cities, the business of “politics” is the business of providing people with jobs at the taxpayers’ expense, regardless of the fitness of the applicant. Many of our cities are managed in this way. Moreover, in the same city, this corruptness may affect certain departments only, some being negligently and dishonestly conducted, others cleanly and efficiently. Or we may find both conditions existing in a single department, some of whose branches or divisions may be well conducted and on a high level, while other divisions may be grossly mismanaged and worthless. If a Health Department is hampered by politics, either as a 277whole or in certain mismanaged branches or divisions, it is useless to expect results. Placed under such a handicap, tuberculosis work would fail. Not only would the taxpayers’ money be wasted, but the community would suffer through a false sense of security, gained through its faith in, or rather its ignorance concerning, a badly conducted department. To trifle with the health of a community is a criminal act, and a Health Department which is “in politics” is the most immoral of all corrupt city departments.
Evil results of a Health Department being “in politics” may be of several sorts. For example: the Superintendent of Nurses may be an inexperienced, incapable woman, appointed by a ward politician to clear off political debts. A ward politician is hardly one whose judgment—in nursing matters at least—should be relied upon.
On the other hand, the Superintendent herself may be capable and efficient, but she may not be permitted to select the members of her staff. Instead of being able to choose them herself, according to their fitness and ability, she must accept any unqualified woman whom the ward boss may appoint. A staff of incompetent nurses, appointed without regard to character or education, is not a 278force from which to expect results. Moreover, nurses chosen in this manner feel that they are “protected” and can do as they like, subject to neither restraint nor discipline. This means that their work cannot be controlled, corrected, or directed in any way. Dismissal can be made only for the most flagrant offences—not for any such trifle as incompetence, laziness, or stupidity. When the Superintendent’s hands are thus tied—when she cannot select her nurses, cannot control them, and cannot dismiss the worthless as well as the unscrupulous, the result is a low grade of work. No able and self-respecting woman could hold the position of superintendent under such circumstances, thereby making herself responsible for work which she cannot control.
The acceptance of registered nurses only, and the requirement of Civil Service Examination in addition, would do much to raise the level of efficiency. These requirements, however, valuable as they are, would by no means ensure the suitability of the applicant, or guarantee the selection of nurses best adapted to public health work. Over and above this, the Superintendent should have free choice in selecting her workers, not only from the point of view of education, but also that of personal worth.
279“Politics” in the Co-operating Divisions. Sometimes the Tuberculosis Division itself may not be on a political basis, but the various other divisions of the Health Department may be conducted in such a manner as to nullify much of the nurses’ work. For example: much depends upon the co-operation of the Fumigation Division. If the men employed to fumigate houses do their work badly or improperly—if they are too lazy to stop chinks and crevices, thus permitting the disinfectant to leak out; if too ignorant to properly measure the rooms, and unable to calculate the necessary amount of formaldehyde, this work will be valueless. Worse still if they are the kind that can be “bought off” and so shirk work entirely.
Or the trouble may be with the Sterilization Division, where the duty of the employees is to carry mattresses, etc., from the patient’s home to the city sterilizer. When there is no law compelling this sterilization, and it is an optional matter with the householder, if done, its doing is altogether the result of the nurse’s teaching and advice. If the waggon drivers are lazy and do not wish to carry the heavy mattresses, they can shirk work by means of false excuses often difficult to detect. For example: they can report that when 280a certain mattress was called for, the family had changed their minds about having it sterilized and refused to have it done. Upon investigation, we find that this refusal was at the instigation of the waggon driver himself—he had assured the family that sterilization was an unnecessary and stupid proceeding. To ignorant minds, one Health Department employee is as good as another, and when the advice is conflicting, they choose that which best pleases them.
Again, the fumigators or drivers may report that they cannot get into a certain house; the key could not be found; there was no one to admit them, or give them the articles to be removed. In innumerable ways they may compel the nurse to return again and again to the same house, to make arrangements which they try to frustrate by every conceivable device.
If, therefore, the employees of the various co-operating divisions are mere jobholders—if they are neither honest nor intelligent, nor interested in anything but pay-day—it is a heartbreaking task for the honest and efficient division to work with them. All of these activities interlock, and must work together to gain a common goal. If all are operated at their highest level, working in close and intelligent accord, then indeed we 281may expect results. But if the reverse is the case—if the co-operating divisions are a drag and a hindrance—then the task is overwhelming. The weak are corrupted and the strong discouraged.
Those responsible for placing tuberculosis work under the city’s administration—where it rightfully and logically belongs—should continue their interest still further. It is not enough to transfer it from pioneer, private control, and then drop the responsibility.
If a Health Department is clear of politics, and all its divisions work together harmoniously, magnificent results may be obtained. Power, prestige, and efficiency is a combination which results in forceful work.
Results in Baltimore. Results have been achieved in Baltimore by reason of a well-managed Health Department, acting in close co-operation with the institutions of both city and state. The tuberculosis machinery consists of a staff of seventeen special nurses; three special dispensaries with a physician in charge; a laboratory for sputum examinations; a fumigation corps and a steam sterilizer. With this force, we work in connection with three other tuberculosis dispensaries, and six institutions for the care of early and advanced cases. Some of these institutions are maintained 282by state appropriations, others by both public and private funds. The co-operation between these institutions and the Health Department is absolute; if the control was all through one, instead of a dozen different centres, it could not be more complete or harmonious. Failure in any one direction is felt down the line, consequently each is stimulated to its best effort. Thus, the nurse knows that if she fails to persuade her patient to enter the hospital, the hospital is useless, or that if the bad food of the hospital drives the patient back again to his home, the nurse’s work goes for nothing. Each reacts upon the other, and as all are working for the same end, there is constant incentive to become a strong, rather than a weak link in the chain. The results obtained cannot be measured in terms of individuals—we cannot point to so many patients improved, so many working, and so forth. Individual welfare is too shifting and too questionable a standard by which to judge. The only absolute standard is that afforded by the death-rate. A declining death-rate means also a decreasing morbidity—fewer people die of tuberculosis and fewer are infected. While our tuberculosis death-rate is still enormously high, it is nevertheless falling year by year. Thus we see:
| 283 | |
| Deaths from Pulmonary Tuberculosis: | |
|---|---|
| 1909 | 1400 |
| 1910 | 1234 |
| 1911 | 1165 |
| 1912 | 1189 |
| 1913 | 1129 |
There is nothing spectacular about this. It is heartbreakingly slow—needlessly, uselessly slow work. Yet it is progressing in the right direction.
Tuberculosis and Poverty. Throughout the foregoing pages we have considered the direct method of dealing with tuberculosis—the removal or segregation of the distributor. But there is also an indirect method of dealing with tuberculosis, namely the abolishment of poverty. Tuberculosis recruits full fifty per cent. of its ranks from people of a certain social level—the very poor. This class is composed of people habitually overworked, underpaid, and subject to all the deteriorating influences of unsanitary and vicious environment, and to the ignorance and degradation which follow in the wake of extreme distress. The root cause of these conditions is our present unjust economic system, which produces an excess of luxury and frivolity on the one hand, and on the other an army of people who must forego the barest necessities of life. One class is 284maintained at the expense of the other. Every movement which seeks to abolish this injustice, and to substitute a fairer and more equable system, is a movement which at the same time tends to raise the standard of public health. Any legislation, social or revolutionary, which makes for the improvement of industrial conditions, raises the level of public health through raising the welfare (i.e., resistance) of the individual. Therefore, sweeping readjustment of social and economic conditions would automatically eliminate an enormous amount of disease, by reducing the number of highly susceptible individuals. To increase the number of people with high resistance—or to decrease the number of people with low resistance, whichever way one chooses to put it—would probably diminish the amount of tuberculosis by about one half.
This indirect method—the readjustment of social conditions and the abolishment of poverty—valuable as it would be, would still leave the problem unsolved. Even diminished by one half, the amount of tuberculosis would still be formidable, and we should have to attack it as vigorously as ever, if not to the same extent. The disease would still exist, just as it now exists in well-to-do families in small towns, in rural districts, and in other circumstances 285attributable to neither poverty nor bad industrial conditions.
A thousand years ago, industrial conditions were as distressing as those which exist to-day—yet in those days the poor staggered under the additional burden of leprosy. A hundred and fifty years ago poverty was complicated by smallpox, the scourge of Europe. The rigid segregation of lepers in the Middle Ages relieved the situation of leprosy, while the discovery of vaccine has practically eliminated smallpox. The submerged classes, while their economic condition remained unchanged, were at least relieved of the added weight of these two great diseases. So in our present fight against tuberculosis. An aggressive campaign against this disease will not necessarily improve industrial conditions, but those who suffer most from these conditions will be relieved of one more handicap.
In our present warfare against tuberculosis we are not impelled by the blind fear that made society in the Middle Ages demand segregation, and refuse to tolerate an infectious disease at large in the community. Nor has any vaccine or similar agent been discovered by which the disease may be wiped out. Instead, we must depend upon a campaign of education—wholesale, widespread 286education, conducted amongst all classes of society. We know the path to be travelled, and the machinery by which we may gain our ends. If at any time we become impatient with our slow rate of progress, we can accelerate our speed by the extension and multiplication of the three fundamental agencies in the anti-tuberculosis campaign—the Hospital, the Dispensary, and the Public Health Nurse.
No one could be better fitted to produce this book, filling a long-felt want, than Miss Pope, because of her large practical experience as a nurse, instructor, and author. Without question this volume must quickly be recognized as indispensable to the students of her great profession.
| NEW YORK | LONDON | |
| 2–4–6 | G. P. Putnam’s Sons | 24 Bedford St. |
| W. 45th St. | Strand |
Author, with Anna Caroline Maxwell, of “Practical Nursing,” and Former Instructor in Practical Nursing and Dietetics in the Presbyterian Hospital School of Nursing.
The object of this work is to provide a text-book containing more physiology than the books on anatomy and physiology hitherto provided for nurses. The book is very fully illustrated and contains a number of questions for each chapter; also an extensive glossary, which includes a detailed explanation of all the chemical and physical terms used.
Formerly Instructor in the Presbyterian Hospital School of Nursing; Instructor in School of Nursing, St. Luke’s Hospital, San Francisco, Cal.
Over 50,000 copies of Practical Nursing had been sold up to January 1st, 1914. This new edition has been entirely reset, revised, and enlarged, and contains over 50 per cent. more material than the previous editions. An important feature of the new edition is, that the authors have not confined themselves to one method of treatment where experience has shown that other methods may be more effective in certain cases. Detailed instructions have been given, thus bringing the book in line with the latest developments in practical nursing.
“The work is interesting, valuable, and worthy of a position in any library.”—N. Y. Medical Record.
“It is written very concisely, and little can be found in it to criticize unfavorably, except the inevitable danger that the student will imagine after reading it that the whole subject has been mastered. The subject of therapeutics has been omitted as not a part of a nurse’s study, and this omission is highly to be commended. It will prove a valuable book for the purpose for which it is intended.”—N. Y. Medical Journal.